bugs drugs & asp - central plains...
TRANSCRIPT

7/30/2013
1
K AT I E B U R E N H E I D E , M S , P H A R M D , B C P S , F C C MP H A R M A C Y C L I N I C A L M A N A G E R / T R A U M A P H A R M A C I S T
P G Y 1 P H A R M A C Y R E S I D E N C Y D I R E C T O R
A D J U N C T A S S I S T A N T C L I N I C A L P H A R M A C Y P R O F E S S O R – U N I V E R S I T Y O F K A N S A S
S T O R M O N T - V A I L H E A L T H C A R E T O P E K A , K S
BUGS, DRUGS & ASP
• Review SCCM Guidelines for antibiotic management in sepsis.
• Review the most common infections that are identified in sepsis and treatment.
• Discuss procalcitonin use to determine antibiotic duration of therapy.
• Discuss Antibiotic Stewardship Programs.
OBJECTIVES
ANTIBIOTIC MANAGEMENT
• Need blood cultures 45 minutes prior to antibiotic administration
• Give antibiotic within 1 hour• Watch CMS standard for pneumonia
• Suggest Procalcitonin levels for de-escalation • No evidence for empiric therapy.
• Source control (AKA surgical procedures) within 12 hours of diagnosis.
• Selective oral decontamination and selective digestive decontamination to prevent VAP

7/30/2013
2
What needs to be done STAT?
IV access
IV fluids
Identify a infectious source
Obtain Cultures
Antibiotics
Give with in the first hour
SCCM ANTIBIOTICS
RETHINKING:IV & PO
ANTIBIOTIC STORAGE
WHAT ABOUT CULTURES?

7/30/2013
3
WHEN SWITCH TO PO?
• Hemodynamically stable and improved clinically
• Able to injest meds
• Have normally functioning GI tract
• Inpatient observation while on PO therapy not necessary.
ANTIBIOTIC SELECTION
IDSA/ATS CONSENSUS GUIDELINES ON MANAGEMENT OF COMMUNITY ACQUIRED PNEUMONIA IN ADULTS
Diagnosis & Management of Complicated
Intra-abdominal Infection in Adults & Children: Guidelines by the Surgical Infection Society &
the Infectious Diseases Society of America

7/30/2013
4
ANTIBIOTIC STEWARDSHIP
WHAT IS ANTIBIOTIC STEWARDSHIP? INSTITUTIONAL PROGRAM WHICH PROMOTES AND MONITORS
APPROPRIATE SELECTION, DOSING, ROUTE AND DURATION OF
ANTIMICROBIAL THERAPY.• Primary Goals• Optimized clinical outcomes• Minimize unattended consequences of antimicrobial use
• Toxicity• Selection of pathogenic organisms (Clostridium difficile) • Emergence of resistance
• Endorsed by multiple national organizations• Infectious Disease Society of America
• Society of HealthCare Epidemiology of America • American Society of Health-Systems Pharmacists• American Academy of Pediatrics• Society for Hospital Medicine• Pediatric Infectious Disease Society• Society of Infectious Disease Pharmacist
• Infectious Disease Society for Obstetrics and Gynecology
ANTIBIOTIC STEWARDSHIP GOALS
• Improve patient outcomes by improving the overall quality of antimicrobial prescribing while minimizing unintended consequences of antimicrobial use.
• Prevent the emergence of resistant organisms by preventing unnecessary and/or inappropriate antimicrobial use.
• Reduce drug expenditures associated with inappropriate antibiotic use without adversely impacting quality of care.
• Start program in the acute care facility and expand to the outpatient settings as appropriate.
7/30/2013
5
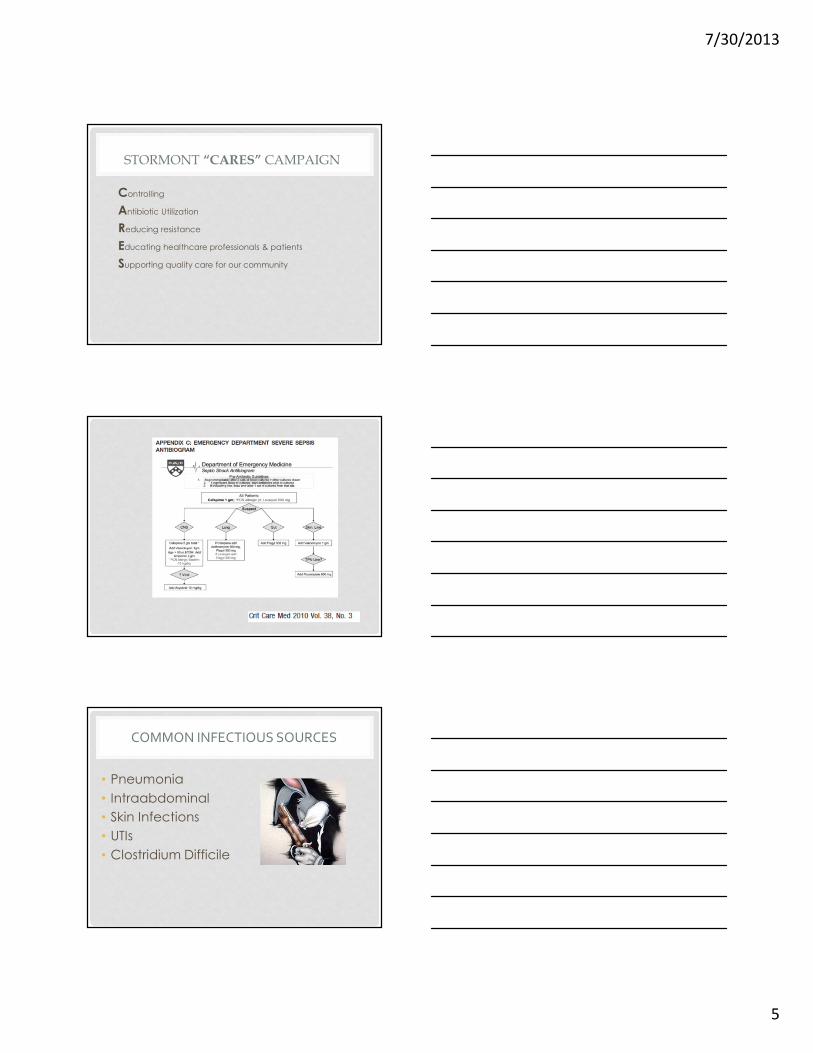
STORMONT “CARES” CAMPAIGN
Controlling
Antibiotic Utilization
Reducing resistance
Educating healthcare professionals & patients
Supporting quality care for our community
• Pneumonia
• Intraabdominal
• Skin Infections
• UTIs
• Clostridium Difficile
COMMON INFECTIOUS SOURCES

7/30/2013
6
IDSA/ATS CONSENSUS GUIDELINES ON MANAGEMENT OF COMMUNITY ACQUIRED PNEUMONIA IN ADULTS
CAP VS. HCAP
•Community acquired pneumonia
•Healthcare associated pneumonia• Nonambulatory residents in nursing homes or other long term care facilities
COMMON PATHOGENS
Outpatient
•Streptococcus pneumonia
•Mycoplasma pneumonia
•Haemophilus influenza
•Chlamydophilia pneumonia
•Respiratory viruses
Inpatient – Non ICU•Streptococcus pneumonia
•Mycoplasma pneumonia
•Haemophilus influenza
•Chlamydophilia pneumonia
•Legionella species
•Aspiration
•Respiratory viruses

7/30/2013
7
EMPIRIC TREATMENT
Outpatient• Healthy & no antibiotics X3 months
• Macrolide – strong• Doxycycline – weak
• Presence of comorbidities
• Chronic heart, liver, renal, lung, DM, alcoholism, malignancy, asplenia, immunosuppression conditions or previous antibiotics last 3 months
• Flouroquinolone• Beta-lactam +macrolide
•Inpatient – non ICU
• Quinolone
• Beta-lactam + macrolide
• Determine if additional coverage needed:
• Pseudomonal
• Aspiration
• MRSA
MRSA?
•Vancomycin 1000 mg IV Q12H• Trough after third dose• The American Thoracic Society and Infectious Disease Society of
America advocate targeting higher vancomycin trough concentrations in pneumonia and recommend vancomycin trough levels between 15-20 µg/mL.
• If Vancomycin allergy• Linezolid (Zyvox) 600 mg IV Q12H
• NEW FDA warnings Aug 2011
FDA ALERT: LINEZOLID (ZYVOX) In emergency situationsIn emergency situationsIn emergency situationsIn emergency situations requiring life-threatening or urgent treatment with linezolid• Consider linezolid treatment benefit should be weighedagainst the risk of serotonin toxicity.
• If linezolid must be administered to a patient receiving aserotonergic drug, the serotonergic drug must beimmediately stopped and the patient should be closelymonitored for emergent symptoms of CNS toxicity for twoweeks (five weeks if fluoxetine [Prozac] was taken), or until24 hours after the last dose of linezolid, whichever comesfirst.

7/30/2013
8
FDA ALERT: LINEZOLID (ZYVOX) InInInIn nonnonnonnon----emergencyemergencyemergencyemergency situationssituationssituationssituationswhen non-urgenttreatment with linezolid is contemplated and planned;• Serotonergic psychiatric medication should be stopped, to allow itsactivity in the brain to dissipate. Most serotonergic psychiatricdrugs should be stopped at least 2 weeks in advance of linezolidtreatment.
• Fluoxetine (Prozac), which has a longer half-life compared tosimilar drugs, should be stopped at least 5 weeks in advance.• Treatment with the serotonergic psychiatric medication may beresumed 24 hours after the last dose of linezolid.• Educate your patients to recognize the symptoms of serotonintoxicity or CNS toxicity and advise them to contact a healthcareprofessional immediately.• Report adverse events to FDA MedWatch program.• Fluconazole (Diflucan) 800 mg IV X1 dose,
then 400 mg IV daily
• Drug Interactions?
• Micafungin (Mycamine) 100 mg IV Daily
SUSPECT FUNGAL INFECTION
DURATION OF ANTIBIOTIC THERAPY
• 5 days
• Afebrile for 48-72 hours
• No more than 1 CAP associated clinical sign before d/c therapy
•Longer duration• If empiric therapy not active against identified pathogen
• Complicated by extrapulmonary infection• Meningitis
• Endocarditis

7/30/2013
9
NEW AUG 2 0 1 1
BRADLY JS ET AL. MANAGEMENT OF COMMUNITY-ACQUIRED
PNEUMONIA IN INFANTS AND CHILDREN OLDER THAN 3 MONTHS
OF AGE: CLINICAL PRACTICE GUIDELINES BY THE PEDIATRIC
INFECTIOUS DISEASES SOCIETY AND THE INFECTIOUS DISEASES
SOCIETY OF AMERICA .CLINICAL INFECTIOUS DISEASES 2011:E1-E52
DIAGNOSIS & MANAGEMENT OF
COMPLICATED INTRA-ABDOMINAL INFECTION
IN ADULTS & CHILDREN: GUIDELINES BY THE
SURGICAL INFECTION SOCIETY & THE
INFECTIOUS DISEASES SOCIETY OF AMERICA
INTRA-ABDOMINAL INFECTIONS
•Includes abdominal cavity & peritoneum
• Associated w/ abscess or peritonitis
•Common
• Appendicitis alone affects 300,000/yr
• 2ndmost common cause of infectious mortality in ICU

7/30/2013
10
E. COLI

7/30/2013
11
•c
DURATION OF THERAPY
• Most: 4-7 days• Unless difficult to achieve adequate source control
•< 24hrs• Acute appendicitis w/o complications
• Penetrating, blunt, or iatrogenic bowel trauma repaired w/n 12hr
• Acute stomach & proximal jejunum perforation• Minus acid reducing tx or malignancy
• If source is controlled

7/30/2013
12
ORAL THERAPY
• May use Oral Antibiotics
• Amoxicillin-clavulanic acid
• Moxifloxacin
• Metronidazole PLUS
Ciprofloxacin, levofloxacin, cephalosporin
• If patient tolerates po diet
• Susceptibility studies do not demonstrate resistance
SKIN & SOFT TISSUE
•Streptococcus pyogenes
•Staphylococcusaureus
MOST COMMON ORGANISMS

7/30/2013
13
Antimicrobial therapy for impetigo and for skin and soft-tissue infections.
Stevens D L et al. Clin Infect Dis. 2005;41:1373-1406
© 2005 by the Infectious Diseases Society of America
NECROTIZING FASCIITIS
Treatment of necrotizing infections of the skin, fascia, and muscle.
Stevens D L et al. Clin Infect Dis. 2005;41:1373-1406
© 2005 by the Infectious Diseases Society of America

7/30/2013
14
• Most common
• Staphylococcus Aureus
• Chronic
• Gram-negative rods
• Foot ischemia or gangrene
• Anaerobic pathogens
DIABETIC FOOT
CLOSTRIDIUM DIFFICILE
AN T I B IO T IC S T EWARDSH I P & I N F EC T ION CON TROL HA S A B IGIMPACT P R EVEN T ING HEA L THCARE A S SOC IA T ED IN F EC T IONS !

7/30/2013
15
BACKGROUND
• Gram – positive, spore forming, toxin producing bacillus
• Ranges in disease severity • diarrhea ⇒ toxic megacolon ⇒sepsis ⇒ death
• 1990s - Cost to treat was > $1 billion annually but mortality < 2%
CLOSTRIDIUM DIFFICILE ON THE RISE

7/30/2013
16
REASONS WHY C DIFF ON THE RISE
•Toxic Toxin
•Antibiotics
•Proton Pump Inhibitors
•Environment

7/30/2013
17
TOXIC TOXIN
• 3 toxins produced by C Difficile
• Toxin A
• Toxin B
• NAPI/BI/027 + bilinary toxins = Severe
• Produces 16 fold more toxins then A
• Produces 23 fold more toxins then B
RAPID DETECTION
•Endotoxin – X3 stools• Can obtain false negatives
• Clinically suscpected – still treat
•Polymerase chain reaction (PCR)• 100% sensitivity and a specificity of 96.9% to diagnose clostridium difficile
•Enzyme immunoassay (EIA)• Toxin A and B is rapid but less sensitive then cell cytotoxin assay
ANTIBIOTICS
• Disrupt normal bowel flora
• 15-25% of cases
• Risk Factors:
• Increase duration
• Broad-spectrum antimicrobials
• Use of multiple agents
•Fluoroquinolones
• Increase Resistance
• NAPI/BI/027
• More resistant to fluoroquinolones
• Clindamycin resistance with J strain in early 1990s

7/30/2013
18
PROTON PUMP INHIBITOR CONTROVERSY
• Independent risk factor
• Potential mechanism of Action• Reduce the acidity of the stomach and increase the luminal pH.
• C. difficile spores are resistant to stomach acid, while the vegetative state of C. difficile is rapidly destroyed.
• Reduction in gastric acid with PPIs may lead to an environment which is unable to sterilize stomach contents, including the vegetative cells of C. difficile
PPI: OTHER POTENTIAL MOA
• Leukocyte function is altered and may reduce the bacteriocidal activity of the gastrointestinal tract.
•Colon contains proton pumps
• Role to develop C diff unknown
H2 ANTAGONIST ≠ CLOSTRIDIUM DIFFICILE ?

7/30/2013
19
ENVIRONMENTAL
COMMUNITY VS. HOSPITAL ACQUIRED CLOSTRIDIUM DIFFICILE
COMMUNITY VERSUS HEALTHCARE
Community Health Care Community Onset
/HCF
Associated
Symptoms within 48 hours of admission
> 12 weeks after discharge from HCF
Symptoms > 48 hours after HCF admission
Symptoms within 48 hours of admission
< 4 weeks since HCF discharge

7/30/2013
20
TREATMENT
METRONIDAZOLE (FLAGYL)
• First line agent – mild disease
• MOA
• After diffusing into organism, interacts with DNA to cause loss of helical DNA structure & strand breakage resulting in inhibition of protein synthesis and cell death in susceptible organisms
• Inexpensive
• Flagyl $2.18/day vancomycin $70.76/day
• Prevent VRE with using vancomycin
• Metronidazole 500 mg PO q8H X10-14 days
METRONIDAZOLE (FLAGYL)
• Failure rates
• Canada
• 1990s – 7%
• Recently - 16-38%
• US
• No reports of in vitro resistance yet

7/30/2013
21
VANCOMYCIN
• Unresolved and/or “Moderate – to Severe”
• MOA:
• Inhibits bacterial cell wall synthesis by blocking glycopeptide polymerization through binding tightly to D-alanyl-D alanine portion of cell wall precursor
• Dose:
• Vancomycin 125 mg PO QID X10-14 days
RELAPSE
1st Relapse 2nd Relapse 3rd Relapse
Flagyl
500 mg PO TID X 10
days
Vancomycin 125 mg
taper
Week one QID
Week 2 – BID
Week 3 – Daily
Week 4 – QOD
Week 5&6 – Q3D
Fidaxomicin
(Dificid™)
Fecal Transplantation – 100%
FIDAXOMICIN (DIFICID™)
• Treatment of diarrhea due to Clostridium difficile (CDAD)
• Oral: 200 mg twice daily for 10 days
•
• Mechanism of Action
• Inhibits RNA polymerase sigma subunit resulting in inhibition of protein synthesis and cell death in susceptible organisms including C. difficile; bactericidal

7/30/2013
22
RELAPSE
1st Relapse 2nd Relapse 3rd Relapse
Flagyl
500 mg PO TID X 10
days
Vancomycin 125 mg
taper
Week one QID
Week 2 – BID
Week 3 – Daily
Week 4 – QOD
Week 5&6 – Q3D
Fidaxomicin
(Dificid™)
Fecal Transplantation – 100%
C DIF VACCINES IN THE FUTURE?
PROBIOTICS
• To prevent lower intestinal flora disruption
• Live micro-organisms which when administered in adequate amounts confer a health benefit on the host
• Include Streptococcus thermophilus, Enterococcus species, Saccharomyces species and various species of lactobacilli and bifidobacteria
• Lactobacillus casei, lactobacillus bulgaricus and S thermophilus during antibiotic course
• 7% vs 34% without drink

7/30/2013
23
PREVENTION HELPS!
ACUTE UNCOMPLICATED CYSTITIS & PYELONEPHRITIS
IN WOMEN
• Escherichia coli (75-95%)
• Proteus mirabilis
• Klebsiella pneumonia
• Staphylococcus saprophyticus
UNCOMPLICATED CYSITITS & PYELONEPHRITIS
MOST COMMON PATHOGENS

7/30/2013
24
•Hospitalization
• IV Fluoroquinolone
• Aminoglycoside ±ampicillin
• Extended spectrum Cephalosporin
• ± Aminoglycoside
• Extended spectrum penicillin
• ± Aminoglycoside
•Community
• Ciprofloxacin 500 mg PO BID 7 days ± cipro 400 mg IV X1 loading dose
• Ciprofloxacin ER 1 gram PO daily X 7 days
• Levofloxacin 750 mg PO Daily X 5 days
•Initial 1 time dose if resistance• Rocephin 1 gram IV X1
• Aminoglycoside 24 hour dose instead of a fluorquinolone
ACUTE PYELONEPHRITIS MANAGEMENT
URINE CULTURES & SENSITIVITIES – ALWAYS
RAPID DIAGNOSTIC TESTING

7/30/2013
25
MULTIPLEX BIOFILM
V I ROLOGY TEST I NG

7/30/2013
26
PROCALC I TON I N?
DURATION OF ANTIBIOTIC THERAPY
• Start Antibiotics ASAP within 1 hour
• Identify source and treat empirically
• De-escalate antibiotics when Cultures and Sensitivities are obtained
• Determine antibiotic duration
• Antibiotic Stewardship Programs Improves antimicrobial management throughout at organization.
SUMMARY

7/30/2013
27
• Healthcare team approach is vital for a successful ASP!
• Develop guidelines • Empiric Therapy
• De-escalation
• Switching for IV to Oral
• Adjusting for Renal insufficiency
• Discontinue antibiotics
• EDUCATE EDUCATE EDUCATE EDUCATE
TIPS HOW TO START AN ANTIBIOTIC STEWARDSHIP PROGRAM:
TEAMWORK!
EARLY SEPSIS IDENTIFICATION & AGGRESSIVE MANAGEMENT
IS IMPORTANT!
• Trauma
• Golden hour!
• Myocardial Infarction
• Time is tissue!
• Chain of survival
• Door to needle time
• Neurology
• Time is brain!
• Sepsis
• Time is organ function!
QUESTIONS?

7/30/2013
28
• Dellinger et al. Surving Sepsis campaign: International guidelines for Management of Severe Sepsis and Septic Shock 2012.. Crit Care Med 2013 41(2):580-647.
• Dellinger RP et al. Surviving sepsis campain:international guidelines ofr management of severe sepsis and septic shock: 2008. Crit Care Med 2008(36)297-327.
• Rivers E, Nguyen B, et al. Early Goal-Directed Therapy in the Treatment of Severe Sepsis and Septic Shock. The Early Goal-Directed Therapy Collaborative Group. NEJM 2001; 354-1368:1377.
• Angus DE et al. Epidemiology Of Severe Sepsis In The United States: Analysis Of Incidence, Outcome And Associated Costs Of Care. Critical Care Medicine 2001; 29:1303-1310.
• Surviving Sepsis Campaign Guidelines For Management Of Severe Sepsis And Septic Shock.Crit Care Med 2004 March;32 (3):858-873
• Nguyen BH. The Stop Sepsis Bundle Toolkit: Srategies To Timely Obviate The Progression Of Sepsis. http://www.llu.edu/llumc/emergency/patientcare/documents/patientcare-sepsis.pdf.
• Slides also adapted from MWCC Shared ICU Quality Improvement Files• http://www.mwcritcare.org/shared-quality-improvement-files
• Mandell LA. Community-Acquired Pneumonia in Adults: Guidelines for Management"• Clinical Infectious Diseases 2007;44:S27–S72
• Guidelines for the Management of Adults with Hospital-acquired, Ventilator-associated, and Healthcare-associated Pneumonia. Am J Respir Crit Care Med 2005; 171:388–416
• Rybak MJ et al. Vancomycin therapeutic guidelines: a summary of consensus recommendations from the infectious diseases Society of America, the American Society of Health-System Pharmacists, and the Society of Infectious Diseases Pharmacists. CID 2009 Aug 1;49(3):325-7.
• Solomkin et al. Diagnosis and management of complicated intra-abdominal infection in adults and children. CID 2010 50:133-64
• Stevens DL et al. Practice guidelines for the diagnosis and management of skin and soft-tissue infections. CID 2005 41:1373-406
• Diagnosis and Treatment of Diabetic Foot Infections“ CID 2004; 39:885–910
• Gupta K et al. International clinical practice guidelines for treatment of acute uncomplicated cystitis and pyelonephritis in women: a 2010 updated by the IDSA and European society of microbiology and infectious disease. CID 2011(52):e013-120.
REFERENCES
REFERENCES
• Nicolle LE. Infectious disease society of america guidelines for the diagnosis and treatment of
asymptomatic bacteriuria in adults. CID 2005 40:643-54.
• Tunkel AR et al. Practice Guidelines for the Management of Bacterial Meningitis. CID 2004;
39:1267–84
• O’Grady et al. Guidelines for evaluation of new fever in critically ill adult patients: 2008 update
from the American College of Critical Care Medicine and the Infectious Diseases Society of
America. Critical Care Medicine 2008 36(4): 1330-1349
• Schuetz P, Christ-Crain M, Thomann R, et al. Effect of procalcitoninbased guidelines vs standard
guidelines on antibiotic use in lowerrespiratory tract infections: the proHOSP randomized
controlled trial. JAMA. 2009;302(10):1059-1066.
• Dellit TH et al. Infectious Diseases Society of America and the Society for Healthcare
Epidemiology of America Guidelines for Developing an Institutional Program to Enhance
Antimicrobial Stewardship. CID Diseases 2007; 44:159–77
REFERENCES
• Jodlowski TZ, Oshler R, Kam LW, Meinychuk I. Emergeing therapies in treatment of clostridium difficile – associated disease. Ann Pharmacotherapy 2006; 40(12): 2161-2169
• Sunenshine RH, McDonald LC. Clostridium difficile-associated disease: new challenges from an established pathogen. Cleveland Clinic Journal of Medicine 2006 73(2):187-197
• CDC: Clostridium difficile information for healthcare professionals. http://www.cdc.gov
• Dial S, Delaney JAC, Barkun AN, Suissa S. Use of gastric acid suppressive agents and the risk of community acquired clostridium difficile associated disease. JAMA 2005 294(23): 2989-2995
• McDonald L, Owings M, Jernigan DB. Clostridium difficile infections in patients discharged from US short-stay hospitals, 1996-2003. Emerging infectious disease 2006 12(3):409-415
• Blossom DB, McDonald C. The Challenges posed by reemerging clostridium difficile infections. Clinical Infectious Disease 2007 45:222-227
• Barclay L, Vega C. Probiotic drinks prevent C difficile associated diarrhea linked to antibiotic uce. Medscape 2007 CME.
• Gilbert DN, Moellering RC, Eliopoulos GM, Sande MA. The Sanford Guide to antimicrobial therapy 2007 Antimicrobial therapy inc.