brucella infection in total hip replacement: case report and review of the literature
TRANSCRIPT

gene sequence types from clinical isolates: emm103 to emm124.
Clin Infect Dis 2002; 34: 28�/38.
9. Johansson A, Flock JI, Svensson O. Collagen and fibronectin
binding in experimental staphylococcal osteomyelitis. Clin
Orthop 2001; 382: 241�/6.
10. Ryden C, Tung HS, Nikolaev V, Engstrom A, Oldberg A.
Staphylococcus aureus causing osteomyelitis binds to a non-
apeptide sequence in bone sialoprotein. Biochem J 1997; 327:
825�/9.
Submitted October 14, 2003; accepted November 20, 2003
DOI: 10.1080/00365540310018824
Brucella Infection in Total Hip Replacement: CaseReport and Review of the Literature
R. A. KASIM1, G. F. ARAJ2, N. E. AFEICHE1 and Z. A. TABBARAH3
From the Departments of 1Surgery, Division of Orthopaedic Surgery; 2Pathology and Laboratory Medicine, and 3Internal
Medicine, Division of Infectious Diseases, American University of Beirut Medical Center. P. O. Box, 113-6044, Beirut, Lebanon
A 47-y-old female underwent revision of a left total hip replacement because of loose prosthesis. Routine intraoperative culture of
the hip site grew Brucella sp. The patient was treated with a combination of vibramycin and rifampicin for 5 months. At 4-y
follow-up, her condition is good. Though prosthetic infection with Brucella spp. is an extremly rare condition (only 1 case each of
femur and hip, and 3 cases of knee had been previously reported in the English literature), brucella infection of prosthetic joints
should be considered in brucella endemic areas.
Z. Tabbarah, Department of Internal Medicine, Division of Infectious Diseases, American University of Beirut Medical Center,
P.O. Box, 113-6044, Beirut, Lebanon (Fax. �/961 1 355 043, e-mail. [email protected])
INTRODUCTION
Infection is one of the most serious problems complicating
total joint replacement. Prosthetic joint infection has been
discussed extensively in the literature whereby staphylococci,
streptococci and Gram-negative bacilli have been reported to
be the most common causative organisms (1, 2). Prosthetic
infection due to Brucella spp. is extremly rare, and only 5
cases have been reported in the English literature: 1 case
involved the hip (3), 3 cases involved the knees (4�/6) and 1
case involved a femur fracture (7). In this communication we
report the second case of brucella infection involving a
prosthetic hip and a review of the literature.
CASE REPORT
A 47-y-old female patient underwent left total hip replacement in
1985 for osteoarthritis secondary to dysplasia. In July 1999 she
presented to the American University of Beirut Medical Center
(AUBMC) because of isolated left hip pain of 3 months duration.
No fever was reported. Her pain was continous, waking her at night
and interfering with her daily activities. The pain did not respond to
conservative measures such as analgesics and rest. X-rays of the left
hip revealed a loose prosthesis. She underwent revision of left total
hip replacement using revision components (SOLUTION-HOW-
MEDICA). The postoperative course was smooth. Routine intrao-
perative cultures grew Brucella sp. The patient reported eating
home-made cheese, prepared from unpasteurized fresh milk, a few
months prior to presentation. Laboratory studies indicated the
following: white blood cell count (WBC) 10200/mm3 (70% poly-
morphonuclear cells), erythocyte sedimentation rate (ESR): 88 mm/
first h, Brucella standard tube agglutination test titer of 1:80
(positive]/1:40) and the Antihuman Globulin Test (Indirect Bru-
cella Coombs test) titer of 1:640 (positive]/1:40). Both of these tests
employed B. abortus whole cell antigen (Immuno/Bactacol Febrile
Antigens, Immunostics, Inc. Ocean, N.J., USA) The patient received
vibramycin (100 mg P.O. bid) and rifampicin (600 mg P.O. daily) for
5 months and responded well. At follow-up, around 4 y later, the
patient was still doing well and her laboratory data showed negative
Brucella titers and a normal ESR. X-rays showed no evidence of
loosening of prosthetic elements.
DISCUSSION
Brucellosis is a zoonotic disease caused by a Gram-negative
coccobacillus. It is prevalent in many parts of the world,
especially in the Mediterranean region including Lebanon
(8�/10).
The main mode of transmission is by ingestion of fresh,
unpasteurized milk, milk products and raw meat. Brucellosis
may also be transmitted through the respiratory tract,
conjunctiva and skin abrasions. Human brucellosis is a
systemic febrile illness with a plethora of somatic complaints
and few physical abnormalities including mild splenomegaly,
hepatomegaly and lymphadenopathy (8, 9, 11). The course
of the disease may be complicated by localization of the
infection to 1 or more body organs. Osteoarticular affection
is the most common complication of brucellosis (20�/60%),
mostly involving the sacroiliac, hip and knee joints (12, 13).
Scand J Infect Dis 36 Case Reports 65
Scan
d J
Infe
ct D
is D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y N
orth
Car
olin
a St
ate
Uni
vers
ity o
n 04
/30/
13Fo
r pe
rson
al u
se o
nly.
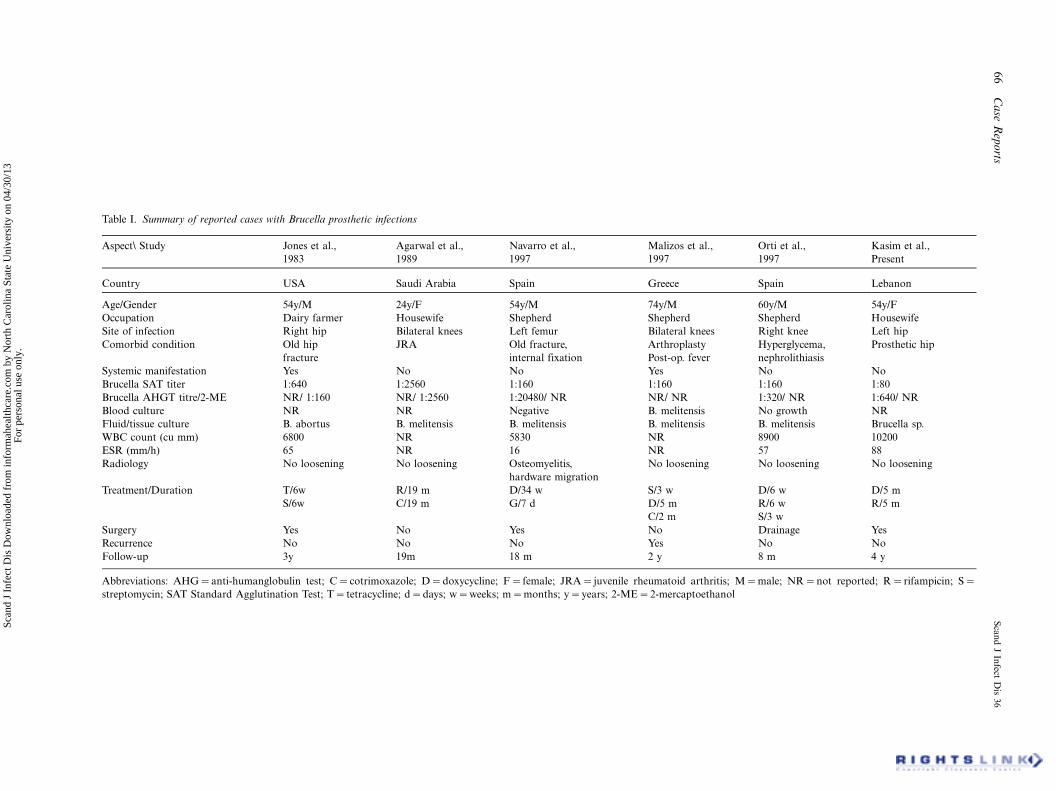
Table I. Summary of reported cases with Brucella prosthetic infections
Aspect\ Study Jones et al., Agarwal et al., Navarro et al., Malizos et al., Orti et al., Kasim et al.,
1983 1989 1997 1997 1997 Present
Country USA Saudi Arabia Spain Greece Spain Lebanon
Age/Gender 54y/M 24y/F 54y/M 74y/M 60y/M 54y/F
Occupation Dairy farmer Housewife Shepherd Shepherd Shepherd Housewife
Site of infection Right hip Bilateral knees Left femur Bilateral knees Right knee Left hip
Comorbid condition Old hip
fracture
JRA Old fracture,
internal fixation
Arthroplasty
Post-op. fever
Hyperglycema,
nephrolithiasis
Prosthetic hip
Systemic manifestation Yes No No Yes No No
Brucella SAT titer 1:640 1:2560 1:160 1:160 1:160 1:80
Brucella AHGT titre/2-ME NR/ 1:160 NR/ 1:2560 1:20480/ NR NR/ NR 1:320/ NR 1:640/ NR
Blood culture NR NR Negative B. melitensis No growth NR
Fluid/tissue culture B. abortus B. melitensis B. melitensis B. melitensis B. melitensis Brucella sp.
WBC count (cu mm) 6800 NR 5830 NR 8900 10200
ESR (mm/h) 65 NR 16 NR 57 88
Radiology No loosening No loosening Osteomyelitis,
hardware migration
No loosening No loosening No loosening
Treatment/Duration T/6w R/19 m D/34 w S/3 w D/6 w D/5 m
S/6w C/19 m G/7 d D/5 m R/6 w R/5 m
C/2 m S/3 w
Surgery Yes No Yes No Drainage Yes
Recurrence No No No Yes No No
Follow-up 3y 19m 18 m 2 y 8 m 4 y
Abbreviations: AHG�/anti-humanglobulin test; C�/cotrimoxazole; D�/doxycycline; F�/female; JRA�/juvenile rheumatoid arthritis; M�/male; NR�/not reported; R�/rifampicin; S�/
streptomycin; SAT Standard Agglutination Test; T�/tetracycline; d�/days; w�/weeks; m�/months; y�/years; 2-ME�/2-mercaptoethanol
66
Ca
seR
epo
rtsS
can
dJ
Infect
Dis
36
Scan
d J
Infe
ct D
is D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y N
orth
Car
olin
a St
ate
Uni
vers
ity o
n 04
/30/
13Fo
r pe
rson
al u
se o
nly.

Prosthetic infections due to Brucella spp. are an extremely
rare condition. A Medline search of the English literature
revealed only 5 cases. Four of them involved prosthetic joint
(3�/6) and 1 had osteomyelitis of the femur (7) (Table I). Our
patient is the second case reported in the literature of a
brucella infection involving prosthetic hip. The diagnosis was
recognized postoperatively based on the routine cultures
taken at the time of her revision surgery. The diagnosis was
not suspected on preoperative evaluation, and this is not
surprising since brucellosis has a variable and wide spectrum
of clinical presentation. Moreover, the routine laboratory
data are usually normal, thus making the diagnosis of
brucellosis challenging to the physician (14).
The exact pathogenesis of brucella prosthetic hip infection
is not known. It is possible that brucella bacteremia at the
time of systemic infection (symptomatic or asymptotic) may
have led to colonization and establishment of infection on
the prosthesis. Because of the rare occurrence of prosthetic
joint infections with brucellosis, there is no protocol or
consensus on its management. Surgical intervention and
conservative management with combination of antibiotics
were reported to provide successful outcome (3, 7), as also
noted in our case. Exchange arthroplasty was performed in
the case reported by Jones (3), and in our case, in addition to
prolonged antibiotic therapy.
Removal of hardware was performed in the case of
brucella osteomyelitis reported by Navarro (7). In the
remaining 3 reported cases, there was no evidence of
loosening of the prosthetic elements, and antibiotic therapy
alone was reported to be successful (4�/6). Moreover, and
due to the scarcity of brucella prosthetic joint infections,
consensus antibiotic regimens and duration of treatment are
not defined. Our patient was treated conservatively for 5
months with a combination of rifampicin and doxycycline
with good response. The patient is still doing well at around
the 4-y follow-up with no evidence of recurrence of disease
or loosening of the prosthesis. The end points that may be
used include resolution of clinical signs and symptoms,
decreasing trends in titers of brucella serological tests and
the normalization of ESR.
CONCLUSION
Brucella should be considered in the differential diagnosis of
prosthetic joint infection in endemic areas and determina-
tion of brucella titers preoperatively is warranted in these
patients. Consensus on the management of brucella pros-
thetic hip infection is lacking due to the rarity of the
condition. Although our case and the previously reported
case of brucella prosthetic hip infection responded to
treatment with antimicrobial agents and 1-stage exchange
arthroplasty, it is not possible to make such a recommenda-
tion. However, in the absence of loosening of the compo-
nents of the prosthesis, an attempt to treat this infection
medically is justified.
REFERENCES
1. Tattevin P, Cremieux AC, Pottier P, Huten D, Carbon C.
Prosthetic joint infection: when can prosthesis salvage be
considered? Clin Infect Dis 1999; 29: 292�/5.
2. Salvati EA, Cheikoisky KM, Brause BD, Wilson PD Jr.
Reimplantation in infection: a 12-y experience. Clin Orthop
1982; 170:62�/75.
3. Jones RE, Berryhill WH, Smith J, Hofmann A, Rogers D.
Secondary infection of a total hip replacement with Brucella
abortus. Orthopedics 1983; 6: 184�/6.
4. Agarwall S, Kadhi SKM, Rooney RJ. Brucellosis complicating
bilateral total knee arthroplasty. Clinical Orthop 1991; 267:
179�/81.
5. Malizos KN, Makris CA, Soucacos PN. Total knee arthroplas-
ties infected by Brucella melitensis: a case report. Am J Orthop
1997; 26: 283�/5.
6. Orti A, Roig P, Alcala R, Navarro V, Salavert M, Martin C,
Merino J. Brucellar prosthetic arthritis in a total knee replace-
ment. Euro J Clin Micro Infect Dis 1997; 16: 843�/5.
7. Navarro V, Solera J, Martinez-Alfaro E, Saez L, Escalbano E,
Perez- Flores JC. Brucellar osteomyleitis involving prosthetic
extra-articular hardware. J Infect 1997; 35: 192�/4.
8. Araj GF. Human brucellosis revisited: a persistant saga in the
Middle East. Br Med J (Middle East) 2000; 7: 6�/15.
9. Young EJ. An overview of human brucellosis. Clin Infect Dis
1995; 21: 238�/90.
10. Araj GF, Azzam RA. Seroprevalence of brucella antibodies
among persons in high-risk occupations in Lebanon. Epidemiol
Infect 1996; 117: 281�/8.
11. Lulu AR, Araj GF, Khateeb MI, Mustapha Y, Yusuf AR,
Fenech FF. Human brucellosis in Kuwait: a prospective study of
400 cases. Q J Med 1988; 249: 39�/52.
12. Moussa ARM, Muhtaseb SA, Almudallal DS, Khodeir SM,
Marafie AA. Osteoarticular complication of brucellosis: a study
of 169 cases. Rev Infect Dis 1987; 9: 531�/42.
13. Khateeb MI, Araj GF, Majeed SA, Lulu AR. Brucella arthritis:
a study of 96 cases in Kuwait. Ann Rheum Dis 1990; 49: 994�/9.
14. Araj GF. Human brucellosis: a classical infectious disease with
persistent diagnostic challenges. Clin Lab Sci 1999; 12: 207�/12.
Submitted February 25, 2003; accepted October 6, 2003
DOI: 10.1080/00365540310017456
Scand J Infect Dis 36 Case Reports 67
Scan
d J
Infe
ct D
is D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y N
orth
Car
olin
a St
ate
Uni
vers
ity o
n 04
/30/
13Fo
r pe
rson
al u
se o
nly.