bronchial asthma · • definition of asthma exacerbation = episodes of progressive increase in...
TRANSCRIPT
Bronchial asthma MUDr. Mojmír Račanský
Odd. Alergologie a klinické imunologie FNOL Ústav Imunologie LF UPOL
ASTHMA BRONCHIALE
DEFINITION
= Asthma is a chronic inflammatory disorder of the airways
in which many cells and cellular elements play a role
Inflammation is connected with BRONCHIAL HYPERREACTIVITY and REVERSIBLE OBSTRUCTION OF BRONCHI.
Bronchial asthma is just local sign of pro-inflammatory state of organism = Asthma is systemic disorder!
• CHRONIC INFLAMMATORY DISORDER
• HYPERREACTIVITY OF BRONCHI
• REVERSIBLE OBSTRUCTION OF BRONCHI

• World • Prevalence: 1-18% with maximum in developed countries • Incidence: in adults 1% • Mortality approx. 250 000 persons per year • The most common chronic disease in childhood • Coincidence with allergic rhinitis in 80% of patients- ARIA
• CZE • Prevalence: 8% in whole population, in children 12-15% • Incidence: up to 30% = 30 000 new diagnoses • Very low mortality due to quality of health care (2006 + 101 per.)
EPIDEMIOLOGY

• BY CONTROL OF DISEASE- GINA 2006
CLASSIFICATION
Parameters CONTROLED PARTLY CONTROLED NOT CONTROLED
Day signs None(max 2x week) ≥ 2x week
≥ 3 signs of partly controled asthma in one week
Disruption of daily routine
None Anyone
Night signs/wake up None Anyone
Need of rescue mediacation
None(max. 2x week) ≥ 2x week
Lung function tests Normal < 80% FVC
Number of exacerbation
None ≥ 1x per year
1x in one week
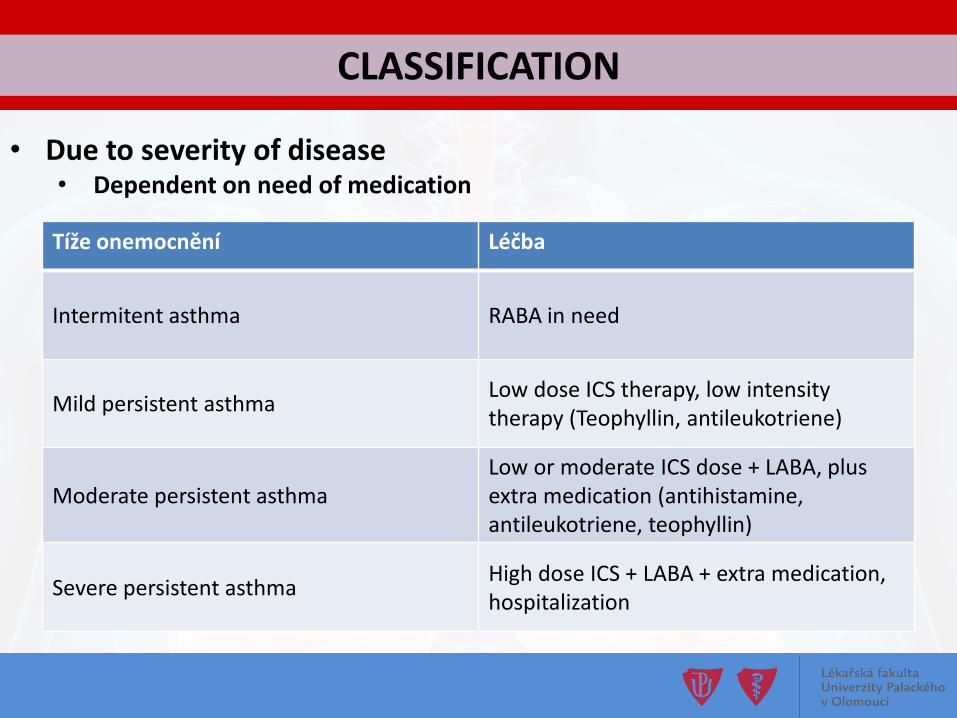
• Due to severity of disease • Dependent on need of medication
CLASSIFICATION
Tíže onemocnění Léčba
Intermitent asthma RABA in need
Mild persistent asthma Low dose ICS therapy, low intensity therapy (Teophyllin, antileukotriene)
Moderate persistent asthma Low or moderate ICS dose + LABA, plus extra medication (antihistamine, antileukotriene, teophyllin)
Severe persistent asthma High dose ICS + LABA + extra medication, hospitalization

A. HEREDITARY FACTORS • Polygenic multifactorial inheritance • Known > 150 gens with connection to asthma and another
allergic diseases • Atopy = Ability to produced allergen specific IgE immunoglobulin
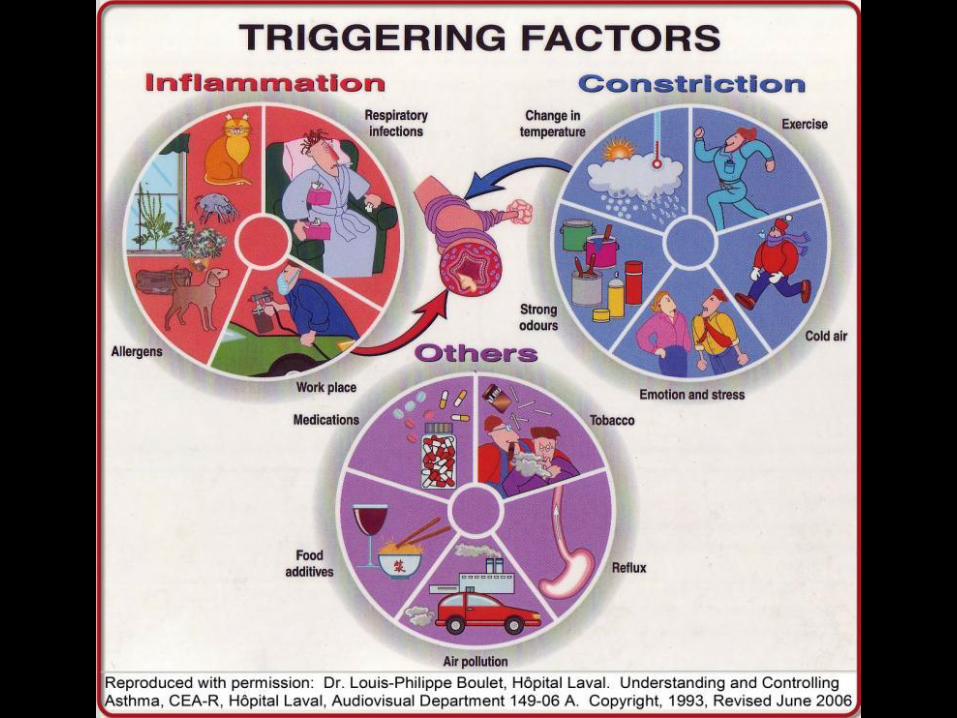
B. ENVIRONMENTAL FACTORS
• Environment, economics status, nutrition status, hygienic status, infections, working surroundings
ETIOLOGY
• Asthma = chronic INFLAMMATORY disease… • Specific picture of cellular subpopulations development
• Predominance of Th2 → enrichment of eosinophils, basophils, activation of mast cells, …
• Pro inflammatory mediators- IL-4, PGE2, LTR, PAF, …
• Bronchial hyper reactivity development • Genetically determined- chromosome 5q, ADAM23 chromosome 20q,
polymorphisms genes pro β2-rcp. ADRB2 • Consequence of chronic inflammation
• Reversible bronchial obstruction development • Acute constriction of bronchi- normally protective- irritation of bronchi • Swelling of bronchial wall • Production of high viscosity sputum • Re-modulation of bronchi due to inflammation = irreversible phase
PATOPHYSIOLOGY
CLINICAL SIGNS
https://www.vecteezy.com/vector-art/142088-free-asthma-icon-vector
• Definition of asthma exacerbation
= episodes of progressive increase in shortness of breath, cough, wheezing or chest tightness. Characterised by • decrease in expiratory airflow that can be quantified and
monitored by measurement of lung function (PEF or FEV1) • severity of asthma exacerbations: mild, moderate, severe (life-
threatening)
Background = amplification of inflammation by specific trigger
Clinical signs
1. PERSONAL HISTORY 2. LUNG FUNCTION TESTS
• Spirometry with bronchial obstruction pattern • Reversibility of bronchial obstruction and proof of hyperreactivity
• Bronchodilatační a bronchokonstrikční testy
3. FENO • Volume of NO in exhaled air- proof of eosinophilic inflammation
4. COMPLEMENTARY METHODS • Blood count + diffential count of leukocytes • Immunoglobulin profile • Allergy testing • Oesinophylic cationic protein in induced sputum
HOW TO MAKE A DIAGNOSE
PULMONARY FUNCTION TESTING
SPIROMETRY • FLOW/VOLUME curve
• Shape • FVC/FEV1 a FEV1
OBSTRUCTION PARAMETERS FEV1/VC < 75% (70%)
FEV1 < 80%
BRONCHOMOTORIC TESTS 1. Broncho dilatation test
• Prove of reversible obstruction • Administration of 400ug salbutamol x 80ug ipratropium • Positive result = after 30min after application increase of FEV1 ≥
12% and increase of 200 ml
2. Bronchoconstriction test • Prove of bronchial hyper reactivity • Nonspecific = methacholine in cumulative dose of 8mg • Specific = known allergen • Positive result = decrease of FEV1 more than 20% in comparison
with previous measurement
PULMONARY FUNCTION TESTING

1. NON-FARMACOLOGICAL • Limitation of exposure to risk factors
2. PHARMACOLOGICAL a) RELEAVE
• Short acting inhaled β2-agonists - SABA- salbutamol, fenoterol • Short acting inhaled anticholinergic - SAMA- ipratropium • I.v. and per oral methylxantins- teofyllin
b) CONTROLING • Inhaled corticosteroids • Long acting inhaled β2-agonists - LABA- salmeterol, formoterol, U-LABA
vilanterol • Long acting inhaled anticholinergic - LAMA- tiotropium • Antileukotriens- montelukast, zafiralukast • Per oral long acting methylxantiny • Per oral or i.v. corticosteroids • Biologic therapy - anti-IgE omalizumab, anti-IL-5 mepolizumab
THERAPY
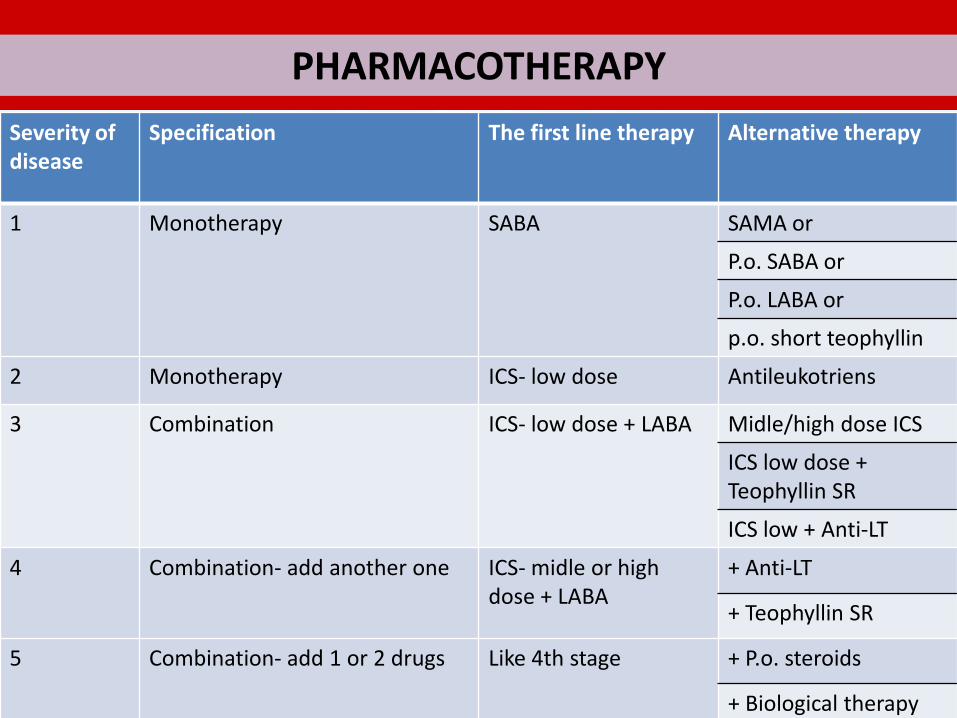
PHARMACOTHERAPY
Severity of disease
Specification The first line therapy Alternative therapy
1 Monotherapy SABA SAMA or
P.o. SABA or
P.o. LABA or
p.o. short teophyllin
2 Monotherapy ICS- low dose Antileukotriens
3 Combination ICS- low dose + LABA Midle/high dose ICS
ICS low dose + Teophyllin SR
ICS low + Anti-LT
4 Combination- add another one ICS- midle or high dose + LABA
+ Anti-LT
+ Teophyllin SR
5 Combination- add 1 or 2 drugs Like 4th stage + P.o. steroids
+ Biological therapy
HOW TO CHOOSE THE RIGT THERAPY?
PHARMACOTHERAPY
1. COMBINATION OF ACTIVE SUBSTANCES
LABA- salmeterol, formoterol U-LABA- vilanterol LAMA- thiotropium IKS- beclomethasone, fluticasone, budesonid, ciclesonid, momethasone Antileukotriens- montelukast, zafiralukast Methylxantins- theophylline, syntophylline
2. INHALE SYSTEM
Powder Aerosols

FARMAKOTERAPIE

1. Removal of the specific trigger 2. Oxygenotherapy- O2 in volume 4-6 l/min
3. I.v. therapy • i.v. corticoids- hydrocortison 200mg/dexo-methason 40mg • i.v. methylxantins- theophyllin 40mg (Syntophyllin®) • Possible application 4 times per day
4. Inhale therapy • β2-agonists- salbutamol (Ventolin®) • Combine solutions- salbutamol+ ipratropium (Berodual®) • Anticholinergic drugs- ipratropium (Atrovent®)
5. Laboratory tests- ABR, BC, mineralogram, sputum cultivation, serology
6. Supporting therapy- mucolytics, i.v. infusion of balanced solutions, …
THERAPY OF EXACERBATION

1. COPD 2. Pneumothorax 3. NET causes 4. Tracheal disorders (children especially) 5. Another lung diseases 6. Vasculitids 7. Pulmonary embolism
DIFFERENTIAL DIAGNOSTICS
BRONCHIAL ASTHMA is chronic inflammatory disease characterized of typical pattern- reversible obstructive disorder of ventilation and bronchial hyper reactivity. Due to known pathophysiology asthma is well treated disease. Patients are not limited with correct therapy. In diagnostics- focused on personal history, pulmonary function tests. Spirometry with obstructive pattern= typical shape + FVC/FEV1<75% (70), FEV1 <80%. Pharmacotherapy- relieving and disease controlling Combination of ICS + LABA could change life of asthmatic patient.
TAKE HOME MESSAGE

Thank you for your attention!