britt berger, ms sodexo di february 2014 medical nutrition therapy in the patient with hiv/aids: a...
TRANSCRIPT

Britt Berger, MSSodexo DIFebruary 2014
MEDICAL NUTRITION THERAPY IN THE
PATIENT WITH HIV/AIDS: A CASE
STUDY

HistoryStatisticsBiologyDisease Course and LifecycleAntiretroviral TherapyMedical Nutrition TherapyCase Study PatientMedical Hospital CourseNutritional Hospital CourseCommentsQuestions
OUTLINE

Late 1800s: fi rst human infection
Likely source: chimpanzees in West Africa infected with Simian Immunodefi ciency Virus (SIV)
Humans hunted chimpanzees for their meat and were infected by contact with their blood
Virus slowly spread across Africa and to other parts of the world
HIV in the US: since at least the mid- to late 1970s
First cases of AIDS described in 1981
HISTORY OF HIV/AIDS

More than 1.1 million people are living with HIV Almost 1 in 5 are unaware of their infection
Gay, bisexual, and other men who have sex with men (MSM) are most aff ected
Blacks/African Americans face the most severe burden of HIV
HIV incidence has remained relatively stable in recent years at about 50,000 new infections per year
15,529 people in the US with an AIDS diagnosis died in 2010
636,000 people in the US with an AIDS diagnosis have died since the epidemic began
UNITED STATES STATISTICS
33.4 million people are currently living with HIV/AIDS
More than 25 million people have died of AIDS since the fi rst cases were reported in 1981
2 million people died due to HIV/AIDS in 2008
2.7 million people were newly infected in 2008
Cases have been reported in all regions of the world Almost all those living with HIV (97%) reside in low- and middle-
income countries Sub-Saharan Africa (10% of world’s population/68% of HIV)
Prevention has helped reduce HIV rates in small but growing numbers New infections are believed to be on the decline
GLOBAL STATISTICS

HIV = retrovirus
Retroviruses Contain RNA as their genetic material Use reverse transcriptase to convert RNA into DNA Replicate using the cell’s machinery
Lentivirus “Slow” viruses Long period of time between initial infection and beginning of
serious symptoms Many people unaware of their infection and spread the virus
to others
BIOLOGY OF HIV

CD4 cells: Critical part of the immune system Type of white blood cell (fight infection) Send signals to activate the body’s immune response Normal CD4 count = 500 – 1000 As HIV infection progresses, CD4 count decreases Also known as T cells
Viral load: Measurement of the amount of HIV in the blood As HIV infection progresses, viral load increases
TWO IMPORTANT TERMS

HIV infection has a well documented progression
If an HIV-infected person does not get treatment, HIV will eventually overwhelm their immune system
When used consistently, antiretroviral therapy (ART) prevents the HIV virus from multiplying and destroying the immune system
Research has shown that taking ART can help prevent the spread of HIV to others
COURSE OF DISEASE

2 – 4 weeks after HIV infection
Many, but not all, people develop flu-like symptoms Often described as “the worst flu ever”
Body’s natural response to HIV infection “Acute antiretroviral syndrome” (ARS) Or “primary HIV infection”
Large amounts of virus being produced
High risk of transmitting HIV to sexual or drug using partners during this stage
STAGE 1: ACUTE INFECTION
Period where the virus is living/developing in a person without producing symptoms
No HIV-related symptoms Some people experience mild symptoms
Virus continues to reproduce at low levels
Clinical latency may last for several decades for people who take ART
Lasts an average of 10 years for people not on ART
Still possible to transmit HIV to others
STAGE 2: CLINICAL LATENCY STAGE

1. CD4 cells <2002. Opportunistic infection
Regardless of CD4 count
Immune system is badly damaged Vulnerable to infections
Without treatment, people typically survive 3 years
Once a person has an opportunistic infection, life-expectancy without treatment falls to about 1 year
If a person takes ART and maintains a low viral load, they may have a near normal lifespan and never progress to AIDS
STAGE 3: AIDS

HIV enters the body through sexual contact, transfusions with infected blood, or by injection
Virus attaches to dendritic cells (type of immune system cell) Found in the mucosal membranes that line the mouth,
vagina, rectum, penis, and upper GI tract
Dendritic cells transport the virus from the site of infection to the lymph nodes where HIV can infect other immune system cells
The steps of the lifecycle are important to understand Medications used to control HIV infection act to interrupt
the cycle
HIV LIFECYCLE ANDANTIRETROVIRAL THERAPY
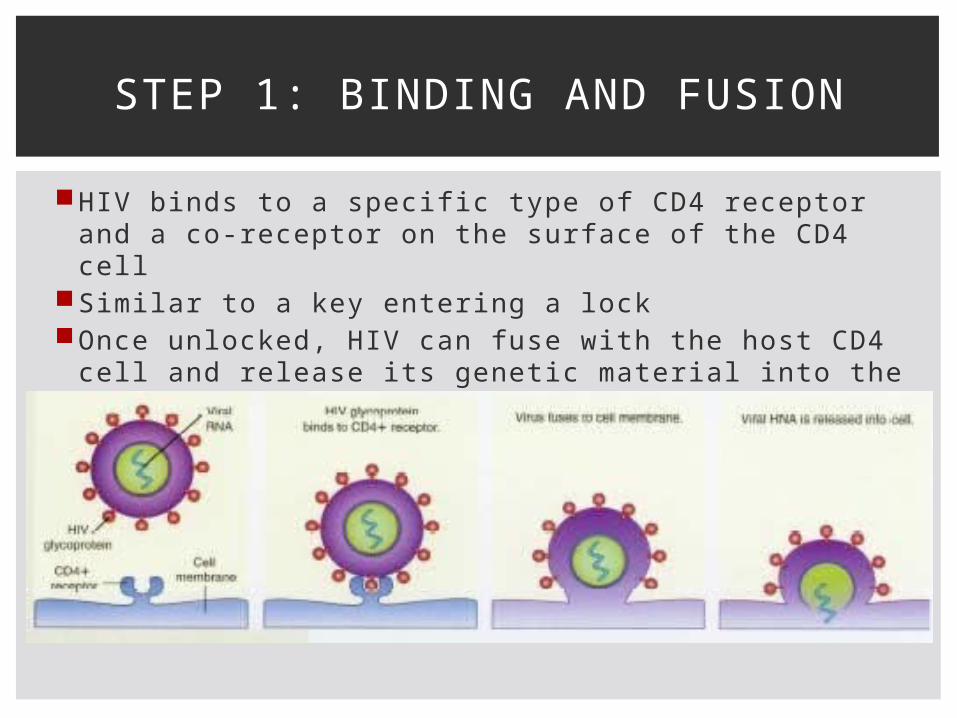
HIV binds to a specific type of CD4 receptor and a co-receptor on the surface of the CD4 cell
Similar to a key entering a lockOnce unlocked, HIV can fuse with the host CD4 cell
and release its genetic material into the cell
STEP 1: BINDING AND FUSION

The enzyme reverse transcriptase changes the genetic material of the virus so it can be integrated into the host DNA
STEP 2: REVERSE TRANSCRIPTION

The virus’ new genetic material enters the nucleus of the CD4 cell and uses the enzyme integrase to integrate itself into the body’s own genetic material where it may “hide” and stay inactive for years
STEP 3: INTEGRATION

When the host cell becomes activated, the virus uses the body’s own enzymes to create more of its genetic material
Also creates a more specialized genetic material which allows it to make longer proteins
The enzyme protease cuts the longer HIV proteins into individual proteins
When these come together with the virus’ genetic material, a new virus has been assembled
STEP 4: TRANSCRIPTIONSTEP 5: ASSEMBLY
Final stage of the virus’ lifecycleVirus pushes itself out of the host cell, taking part of
the cell membrane with itOuter part covers the virus
Contains all of the structures necessary to bind to a new CD4 cell
Process begins again
STEP 6: BUDDING

Introduction of 3-drug combination ART in 1996 revolutionized treatment Significantly decreased AIDS-related morbidity and mortality
5 classes of HIV drugs Each class attacks the virus at a different point in the
lifecycle
A person taking ART will generally take 3 diff erent drugs from 2 diff erent classes Best job of controlling the amount of virus in the body and protecting the immune system Protects against resistance
Nutritional implications
HIGHLY ACTIVE ANTIRETROVIRAL THERAPY (HAART or ART)
Blocks a very important step in HIV’s reproduction process
Act as faulty building blocks in production of viral DNA
Blocks HIV’s ability to use reverse transcriptase to correctly build new DNA Without reverse transcriptase the virus is unable to make
copies of itself
NUCLEOSIDE/NUCLEOTIDE REVERSE TRANSCRIPTASE INHIBITORS (NRTIs)
Work in a very similar way to NRTIs
Also block reverse transcriptase and prevent HIV from making copies of its own DNA
NRTIs work on the genetic material
NNRTIs act directly on the enzyme itself to prevent it from functioning correctly
NON-NUCLEOSIDE REVERSE TRANSCRIPTASE INHIBITORS
(NNRTIs)

When HIV replicates it creates long strands of its own genetic material
These long strands must be cut into shorter stands in order for HIV to create more copies of itself
Protease acts to cut up these long strands
Protease inhibitors block this enzyme Prevent the long strands of genetic material from being cut
up into functional pieces
PROTEASE INHIBITORS

Block the virus from entering the cells in the fi rst place
HIV needs a way to attach and bond to CD4 cells Special structures on cells called receptor sites Found on both HIV and CD4 cells
Fusion inhibitors can target those sites on either HIV or CD4 cells and prevent HIV from attaching onto healthy cells
ENTRY/FUSION INHIBITORS

HIV uses the cells’ genetic material to make its own DNA Reverse transcription
The virus then has to integrate its genetic material into the genetic material of the cells Uses the enzyme integrase
Integrase inhibitors block this enzyme and prevent the virus from adding its DNA into the DNA of the CD4 cells
Preventing this process prevents the virus from replicating and making new copies
INTEGRASE INHIBITORS

Overall goals of MNT for HIV and AIDS patients are to:
Optimize nutritional status, immunity, and well-being
Maintain a healthy weight and lean body mass
Prevent nutrient deficiencies
Reduce the risk of comorbidities
Maximize the effectiveness of medical and pharmacological treatments
MEDICAL NUTRITION THERAPY

Good nutrition is important to all people, whether or not they are living with HIV
Eating well is key to maintaining: Strength Energy Healthy immune system
Some conditions related to HIV/AIDS and treatment mean that proper nutrition is EXTREMELY IMPORTANT Wasting Diarrhea Lipid abnormalities
Immune suppression Food safety and proper hygiene
MEDICAL NUTRITION THERAPY

Adequate intake of macro- and micronutrients is essential to restoration and maintenance of body cell mass and normal body function, including immunity
The benefi ts of providing adequate amounts of energy, protein, and micronutrients for people living with HIV are clear However, the EXACT amount of each type of nutrient needed
is less clear
Long-term clinical trials are needed to provide evidence-based formal recommendations for all nutrients
There is no single “diet” that is appropriate for all individuals living with HIV
ESTIMATED NUTRITIONAL NEEDS

Studies show that low energy intake combined with increased energy demands due to HIV are the major driving forces behind HIV-related weight loss and wasting
Asymptomatic HIV-infected adults: Goal = maintain body weight 10% increase in energy needs 25 – 30 kcal/kg 28 – 33 kcal/kg
Symptomatic HIV-infected adults (with opportunistic infections): 20 – 30% increase in energy needs 30 – 40 kcal/kg Intake should be increased to the extent possible during
recovery phase
ENERGY

DRI for healthy adults = 0.8 grams/kg Likely adequate for asymptomatic HIV-infected adults
Patients with wasted lean body mass Increased protein intake may be beneficial 1.2 – 2.0 grams/kg Currently no evidence to support protein intake in excess of
this range
Sources of dietary protein include both animal and plant-based sources Strict vegetarians need to consume a wide variety of foods
to ensure that they obtain adequate amounts of all essential amino acids May benefit from protein, energy, iron, and vitamin B12
supplementation
PROTEIN

No evidence that total fat needs are increased beyond normal requirements
Special advice regarding fat intake may be required for patients undergoing antiretroviral therapy or experiencing persistent diarrhea
Malabsorption syndromes may require changes in timing, quantity, and type of fat intake
Researchers are currently studying the potential of omega-3 fats in immune function Recommendations are currently no different than for the
general population
FAT

Foods rich in micronutrients are likely to help fight infections and improve overall health
Studies suggest that deficiencies and/or high intakes of certain micronutrients may aff ect the course of HIV Selenium deficiency may increase HIV-related mortality Excessive intake of zinc may be linked to poorer survival Increased intake of vitamins B1 (thiamin) and B2
(riboflavin) may enhance survival Other micronutrient deficiencies may exacerbate oxidative
stress associated with HIV infection
The patient is likely to benefit from consuming a varied diet that is rich in micronutrients
MICRONUTRIENTS

WHO’s position on micronutrient supplementation in HIV-infected individuals:
Healthy diet is best
Dietary intake of micronutrients at RDA levels may not be suffi cient to correct nutritional deficiencies
Legitimate use of dietary supplementation is to restore nutritional status to normal
No conclusive evidence to support use of dietary supplements to improve outcomes
Risk of adverse reactions with other medications
MICRONUTRIENT SUPPLEMENTATION

Food and nutrient intakeLifestyleMedical history
Important medical factors to consider with HIV/AIDS patients: Stage of disease (CD4 count, viral load) Comorbidities (CV disease, DM, hepatitis) Opportunistic infections Metabolic complications (DLD, insulin resistance) Biochemical measurements (CD4 count, viral load, albumin,
hemoglobin, iron status, lipid profile, LFTs, renal function, glucose, vitamin levels)
NUTRITION ASSESSMENT

Very important Noted and documented during initial assessment and all follow-
up assessments
Patients must be made aware of possible body shape changes Medical team (including RD) should ask patients about body
shape changes every 3 – 6 months
Anthropometric measurements Measure changes in body shape and fat redistribution
Physical changes = HIV-associated lipodystrophy syndrome
Unintentional weight loss often indicates progression of disease
PHYSICAL APPEARANCE

Mental status and psychosocial issues may take precedence over nutrition counseling
Depression is common
Habits, food aversions, and timing of meals with medications must be taken into consideration
Access to safe, aff ordable, and nutritious food?
Common barriers: Cost, location of supermarkets, lack of transportation, lack
of knowledge of healthier choices Antiretroviral medications are expensive and often compete
with food for available monetary resources
SOCIAL AND ECONOMIC FACTORS
All HIV patients should have access to a Registered Dietitian Baseline nutrition assessment after HIV diagnosis Reassessment 1 – 2x per year for asymptomatic patients 2 – 6x per year for symptomatic but stable patients Patients that have been diagnosed with AIDS usually need to be
seen more frequently and may require nutrition support
RD must implement MNT and coordinate care with the interdisciplinary medical team and community resources
Many cities/towns/communities have resources available for HIV and AIDS patients Food assistance programs Support systems Recreational facilities
INTERDISCIPLINARY CARE

No specific medical nutrition therapy for HIV and AIDS beyond adequately meeting additional energy, protein, fluid, and micronutrients needs
MNT should be individualized for each patient
Focus on: High quality foods Variety of fruits and vegetables Problems identified during nutrition assessment (CV risk, liver disease, DM)
CUSTOMIZING A NUTRITION PLAN

Education and counseling should focus on:
Appropriate and adequate food intake Food behaviors Symptoms that may affect appropriate food intake Benefits and risk of supplemental nutrients Strategies for symptom management
Reduce effects of disease Reduce medication intolerance
NUTRITION EDUCATION

When a patient does not/cannot eat well, supplements may be necessary for getting suffi cient calories, protein, vitamins, and minerals Not perfect substitutes for food Can be helpful
Nutritional supplements can be toxic Safe limits are usually 100 – 200% of the nutrient’s DRI Vitamins A and D are most safely obtained through eating food Zinc and selenium are important for immunity, but are toxic at
fairly low doses
Patients with signifi cant weight loss may be candidates for enteral nutrition (not very common)
Unless GI function is severely abnormal, there is no reason to consider parenteral nutrition
SUPPLEMENTS AND NUTRITION SUPPORT

Diarrhea is common Causes dehydration, malabsorption, food/nutrient
losses Caused by:
Infection GI damage Increased motility Lactose/other food intolerances Medication (ART)
Short-term: Antidiarrheal medications
Long term: Large fluid losses/dehydration Investigation by MD
GI SYMPTOMS AND SIDE EFFECTS

ART medications: Diarrhea, GERD, nausea, vomiting, constipation PI and NRTI classes are most commonly associated with GI
distress Diarrhea can make it diffi cult for ART medications to be as
effective as possible Reduce caffeine and alcohol Test for lactose intolerance
Fat malabsorption Feeling full too fast, bloating, foul-smelling stools that float Low-fat diet Pancreatic enzyme supplementation
GI SYMPTOMS AND SIDE EFFECTS

Nausea Also a common problem Food, medications,
odors Psychological aversions
to food may develop Look at food-medication
interactions Add
anti-nausea/antiemetic medications if necessary
If associated with food intake, implement nutritional strategies
GI SYMPTOMS AND SIDE EFFECTS

Food safety is especially important for patients with low CD4 counts (<200) More likely to get sick from foods that are not safe to eat
Food safety rules: Avoid eating raw eggs, meat, and seafood Wash fruits and vegetables thoroughly Use a separate cutting board for raw meats Wash hands, utensils, and cutting boards with soap and water after each use Water safety is extremely important
Water can carry parasites, bacteria, and viruses
FOOD SAFETY

Dietetic internship primary site = St. Barnabas Hospital in the Bronx Urban level I trauma center
Many patients are HIV-positive in addition to condition that they are hospitalized for
Ideal opportunity to learn more about HIV and AIDS Nutritional implications
CHOICE OF CASE STUDY PATIENT
45 year-old black woman
Brought to the emergency department by EMS with shortness of breath, elevated heart rate, fevers, sweating, frequent vomiting/diarrhea, severe cough with whitish phlegm for two weeks
Past Medical History HIV (non-compliant with ART medications, last known CD4
count = 172 in January 2012) Hypertension Depression PCP pneumonia (required hospitalization) Anemia History of IV drug abuse and tobacco use
PATIENT

Height: 5’2” (62” / 156.4cm)Admission weight: 90# / 40.8kgBMI 16.4
Questionable accuracy of admission weight No mention of what type of scale was used (standing
scale, bed scale, etc.) Was the weight stated by the patient?
Visibly cachecticReport of 40# (31%) weight loss from usual body
weight 130# over the last monthSevere weight loss
PATIENT

Currently unemployedLives alone in an elevator building in the
BronxCompleted high school, did not go to
collegeBaptistPatient’s best friend/on-and-off boyfriend
spent almost every day with her during hospitalization
Sister in Staten Island
PATIENT

October 21, 2013 – November 19, 2013 30 days
High nutritional risk Followed-up every 2 – 3 days Initial assessment 4 reassessments Several progress notes
Emergency department Medical/surgical fl oor ICU Step-down ICU General medicine fl oor Home
MEDICAL HOSPITAL COURSE

Admitting Diagnosis:
AIDSMultilobar/PCP pneumoniaCandida infection of the mouth and esophagus

Acquired Immunodeficiency Syndrome
Final stage of HIV infection
Badly damaged immune system One or more specific opportunistic infections Certain cancers CD4 count <200
Medical intervention necessary to prevent death
AIDS

AIDS-defining condition (opportunistic infection)
Serious illness caused by the fungus Pneumocystis jirovecii
One of the most frequent and severe opportunistic infections in people with HIV/AIDS
Symptoms: Fever Dry cough Shortness of breath Fatigue
In HIV-infected patients: Develops sub-acutely Low-grade fever
No vaccine to prevent PCP
3 week treatment with antibiotics
PCP PNEUMONIA
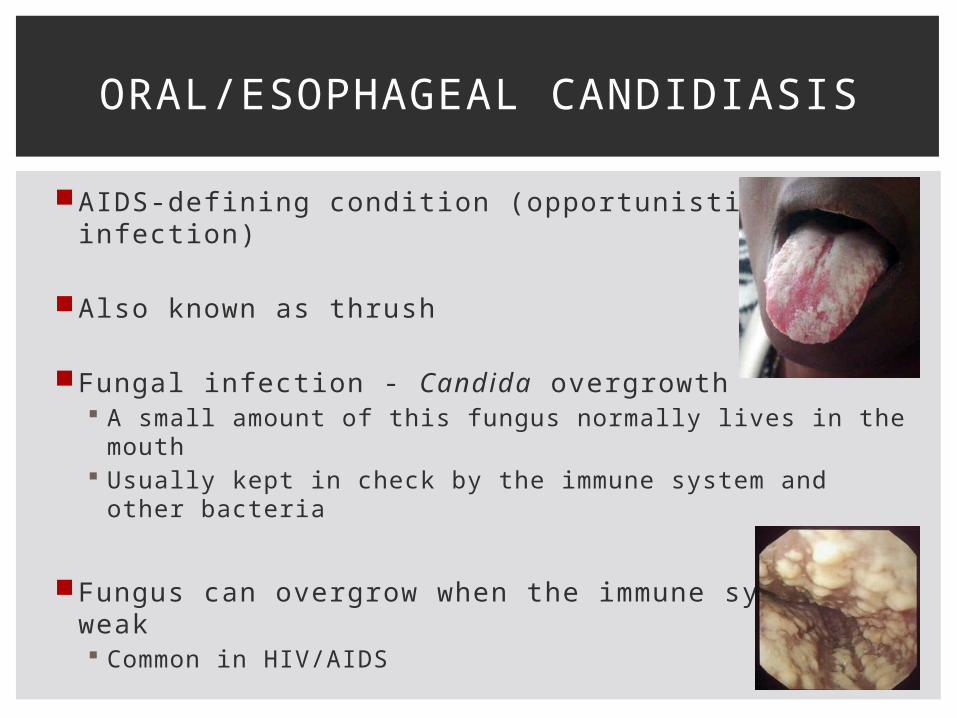
AIDS-defining condition (opportunistic infection)
Also known as thrush
Fungal infection - Candida overgrowth A small amount of this fungus normally lives in the mouth Usually kept in check by the immune system and other
bacteria
Fungus can overgrow when the immune system is weak Common in HIV/AIDS
Nutritional implications
ORAL/ESOPHAGEAL CANDIDIASIS

PCP pneumonia Antibiotics O2 supplementation Follow-up O2
saturation Respiratory and
sputum cultures
Severe oral thrush Fluconazole and
Nystatin Swish and Swallow
Mostly resolved within the first week
AIDS (non-compliant with ART) CD4 <20
Rule out TB Airborne precautions 3 sputum cultures
Diarrhea Flagyl Stool workup
HOSPITAL DAYS 1 – 8MEDICAL/SURGICAL FLOOR

O2 saturation Red blood cells must carry suffi cient oxygen through the
arteries to all internal organs to keep a person alive Percentage of hemoglobin binding sites in the bloodstream
occupied by oxygen
95% 91% 87% 88% 75%
Possible sepsis WBC 8.2 16.7
Patient states she feels like she is going to die
Transferred to ICU
HOSPITAL DAYS 1 – 8MEDICAL/SURGICAL FLOOR

Patient appears emaciated and weak, dry crusted lips, minimal oral thrush
May require intubation if condition worsens
Discussion about end of life issues Appoints best friend as medical proxy Wishes to be intubated and resuscitated if necessary
Patient begins to feel better O2 saturation improves WBCs trend down Diarrhea resolved Medically stable Ready for transfer to general medicine floor
HOSPITAL DAYS 9 – 15ICU

Patient had episode of Ventricular tachycardia
Rapid heartbeat that starts in the ventricles 5 beats Most likely caused by medication interaction Transferred to step-down ICU instead of general
medicine floor for observation
93 – 100% O2 saturation
HOSPITALS DAYS 16 & 17STEP-DOWN ICU

C. diff negative Diarrhea resolved Flagyl discontinued
Able to walk to bathroom without significant SOB
Chest X-ray shows improvements
Reglan added for GI upset Polypharmacy
Patient tells MD she is interested in restarting ART St. Barnabas Designated
AIDS Center appointment scheduled
Patient will need home O2 when discharged Social work coordinated
with VNS for delivery
PATIENT DISCHARGED
HOSPITAL DAYS 18 – 30GENERAL MEDICINE FLOOR

Very sick
Extremely advanced AIDS CD4 <20
Two opportunistic infections Both with nutritional implications Diffi cult PO intake
First 10 days in hospital 21.6# weight loss Lowest BMI = 12.5 Cachexia and severe protein-calorie malnutrition
DISCUSSION OF MEDICAL NUTRITION THERAPY

HD 1 HD 10 HD 11 HD 12 HD 16 HD 23 HD 2950
55
60
65
70
75
80
85
90
95
Weight (in lbs.)
WEIGHT DURING HOSPITALIZATION
Chewing problem: Poor dentition
Swallowing problem: Painful/diffi cult
swallowing caused by severe oral/esophageal thrush
Vomiting: Persistent PTA, currently
resolved
Diarrhea: Persistent PTA, multiple
episodes today
Appetite/Intake: Fair, making an effort to
eat ~25% breakfast
completion
Diet PTA: <1 meal/day x2 weeks Inability to cook because
of lack of energy
Appearance: Cachectic
NUTRITION INITIAL ASSESSMENT (HD 2)

Anthropometrics BMI: 16.4 Ideal body weight: 110# / 50kg
%IBW: 82% Usual body weight: 130# / 59kg
%UBW: 69%
Estimated nutritional needs Based on current body weight 41kg Calories: 1435 – 1640 kcals (based on 35 – 40kcal/kg) Protein: 61 – 82 grams (based on 1.5 – 2.0gm/kg) Fluid: 1230 – 1435 ml (based on 30 – 35ml/kg)
High nutritional risk
NUTRITION INITIAL ASSESSMENT (HD 2)

Diagnosis: Malnutrition related to poor PO intake, persistent
vomiting and diarrhea, painful and diffi cult swallowing, and oral/esophageal thrush as evidenced by 40# (31%) unintentional weight loss x 1 month, BMI 16.4
Intervention: Discussed the importance of adequate PO intake and
strategies to achieve adequacy Recommended patient eat protein portion of meal first PO supplement use between meals, rather than meal
replacement Discussed food preferences
NUTRITION INITIAL ASSESSMENT (HD 2)

Recommendation plan:
SLP consult for diet consistency and upgrade from pureed consistency to soft consistency for palatability and PO intake optimization
Ensure Plus 8oz PO supplement TID (1050kcal + 39gm protein) for consumption between meals
Continue MVI supplementation, maintain hydration status, replete electrolytes as necessary
Reassess PO intake
Weekly weights
NUTRITION INITIAL ASSESSMENT (HD 2)
Poor – fair PO intake 10 – 50% meal completion
Consistency upgrade to soft foods
Added yogurt and applesauce to breakfast, lunch, and dinner trays
Food from outside Grapes, candy
Less painful swallowing
Patient seen drinking Ensure Plus supplements
HOSPITAL WEEK 1

Day after ICU transfer
0% breakfast completion, patient was told not to remove her O2 mask
Patient believes Ensure Plus supplement causes diarrhea
Weight: 74.5# / 33.8kg (bed scale) 15.5# (17%) weight loss BMI: 13.6
Estimated nutritional needs (based on IBW 50kg) Calories: 1500 – 1750 kcals (based on 30 – 35kcal/kg) Protein: 75 – 100 grams (based on 1.5 – 2.0gm/kg) Fluid: 1250 – 1500 ml (based on 25 – 30ml/kg)
NUTRITION REASSESSMENT 1 (HD 9)

Interventions and recommendations: Added tuna sandwich and gelatin to patient’s lunch and
dinner trays to give more options Continue soft diet Discontinue Ensure Plus supplements Add TwoCal HN 8oz PO supplement BID (950kcal + 40gm
protein) Reassess PO intake Daily weights
During ICU stay: Added chocolate cake to patient’s dinner trays Added Ensure pudding once daily (170kcal + 4gm protein)
NUTRITION REASSESSMENT 1 (HD 9)

Fair appetite75% breakfast completionObserved patient drinking a TwoCal supplement
Patient noted with 2.8kg (6.2#) weight gain from lowest weight
BMI: 13.6
Patient encouraged by weight gain and motivated to continue gaining weight
NUTRITION REASSESSMENT 2 (HD 17)
Good appetite 75% meal completion Finishes at least 1 TwoCal supplement per day Eats 2 sandwiches as snacks between meals Loves the chocolate cake
Weight: 91.8# / 41.6kg (bed scale) BMI: 16.8 17.3# (23%) weight gain since lowest weight during
hospitalization 2% weight gain since admission
Connection between PO intake and medical condition VERY motivated to continue gaining weight and to leave the
hospital Soft regular consistency foods Linezolid Rx added – Tyramine restriction added to diet order
NUTRITION REASSESSMENT 3 (HD 23)

Continued good appetite
Occasional diffi culty swallowing due to sore throat Patient requests mechanical soft consistency foods
Weight: 88.1# / 40kg (standing scale)BMI: 16.1
3.6# (4%) weight loss x 6 days Possibly due to bed scale vs. standing scale
Patient feels much better and is able to walk around room
Pending discharge, reinforced nutrition education
NUTRITION REASSESSMENT 4 (HD 29)

Initial diet
Discussion about end of life issues Patient realized she was not ready to die Motivated to do anything possible to get better Gaining weight became top priority SUCCESS!
Nutrition at home Supplements covered by insurance?
Trusting relationship Doctors and nurses frequently changed, but my presence and
concern remained constant Significant weight gain = big part of recovery Importance of nutrition team as part of multidisciplinary care
COMMENTS ON MNT PROVIDED

A BIG THANK YOU TO THE CLINICAL NUTRITION DEPARTMENT AT ST. BARNABAS HOSPITAL…
for being amazing preceptors, teachers, and mentors!
Amy (CNM), Allison, Rachel, Bing, Jess, Rebecca, and especially Michelle for helping me find the perfect case study patient

QUESTIONS/DISCUSSION