british society for histocompatibility and · pdf filebshi volume 96 – 2014 issue 3...
TRANSCRIPT

BSHI Volume 96 – 2014 Issue 3 ©2014 The British Society for Histocompatibility & Immunogenetics
1BSHI
ISSUE 3 September 2014
British Society for Histocompatibility and Immunogenetics
NEWSLETTER 96
BSHI
This year’s One Lambda European Clinical Histocompatibility Workshop took place in the Andalusian city of Marbella, located on the Spanish Costa del Sol. The venue for the workshop was the spectacular Villa Padierna Palace Hotel and golf resort
Supported byAbbott Diagnostics, Alpha Biotech Ltd,Life Technologies, Quest Biomedical,Savant Ltd, StemCell Technologies and VH Bio Ltd.
Continued on page 3
One Lambda European Clinical Histocompatibility Workshop19th-22nd May 2014, Marbella, SpainAndrew Lemin – Trainee Clinical Scientist, Welsh Transplantation and Immunogenetics Laboratory, Pontyclun.
Like us on Facebook!
The event was extremely well organised and comprised both an excellent scientific and social programme.
The first morning of presentations was on the topic of non-HLA antibodies in renal transplantation with particular focus on angiotensin II type I receptor (AT1R) antibodies. A highlight included Magali Giral’s presentation which focused on work from three independent studies which demonstrated the role of AT1R pre-sensitisation in acute rejection and renal graft failure (Giral et al., 2013; Am J Transplant. 13; 2567-76). Dr Giral suggested that, as a result of these studies, pre-transplant AT1R antibodies are a novel and independent risk factor for acute rejection. In the afternoon we took a trip to the historic mountainous city of Ronda, famous for the canyon upon which the city is built. After lunch overlooking the canyon, the delegates were treated to a guided walking tour of the old town area. An evening lecture charting the evolution of antibody-mediated rejection diagnosis and risk stratification was well received.
The second morning of presentations was on the theme of antibody-mediated rejection.
The dizzying view from the top of the canyon in Ronda.
I was lucky enough to be awarded a bursary from VH Bio Ltd to attend the workshop which took place on 19th-22nd May 2014. Applications for the bursary were open to trainee clinical scientists who had passed their BSHI diploma in the preceding twelve months. Submitted abstracts are usually related to a trainee’s BSHI Diploma project or MSc project. Abstracts were assessed by the BSHI Education Board and the successful candidate was chosen to present an oral presentation at the workshop.

BSHI Volume 96 – 2014 Issue 3 ©2014 The British Society for Histocompatibility & Immunogenetics
2BSHI
British Society for Histocompatibility and ImmunogeneticsBritish Society for Histocompatibility and Immunogenetics
Editorial Board:Kelly Williamson – Production Editor Steven Jervis – Web Designer Sharon Vivers – Co-editor Sarah Corbett – Co-Editor Laura Roche – Co-Editor Janet Mackman – Co-Editor Louise Onions – Co-Editor Arthi Anand – Co-Editor
Submissions to: David McKenzie. Histocompatibility & Immunogenetics Service, Gartnavel General Hospital, Level 1, Laboratory Medicine Building, 21 Shelley Road, Glasgow, G12 0XL. Tel: 0141 301 7755 Email: [email protected]
Advertising Enquiries to: Janet Mackman, Tel: 0113 206 4579 Email: [email protected]
Deadline for submission of articles in 2014 Volume 97, Issue 4 - 3rd November
British Society For Histocompatibility and Immunogenetics, all rights reserved.(No part of this publication may be reproduced or transmitted in any form or by any means, including photocopying and recording, without the written permission of the publishers, or where appropriate, the author of the article. Such written permission must also be obtained before any part of this publication is stored in a retrieval system of any nature, except those directed by BSHI itself.)Opinions expressed by any contributor to this Newsletter are not necessarily those of the Editor, or of the BSHI, and neither the Editor nor BSHI accepts any responsibility or liability for any article or part thereof.
CONTENTS One Lambda Workshop 1, 3
Editorial 2
Chair’s Report 5
BSHI Committee Report 6-7
Julia Bodmer travel award 7
Science Watch 8-9
28th EFI Conference 10-11
Susan Corbin retirement 12
10th IDRC 13-14
GenDx Training School 15
Journal Based Learning 16-18
Call for Case Studies 19
Editorial
British Society for Histocompatibility and Immunogenetics. A company limited by guarantee. Company No. 6078396. Registered in England and Wales at Executive Business Support Ltd, City Wharf, Davidson Road, Lichfield, Staffs. WS14 9DZ.
Registered Charity Number: 1123760
BSHI CORPORATE MEMBERSAbbott Diagnostics, Alpha Biotech Ltd, Life Technologies, Quest Biomedical, Savant Ltd, StemCell Technologies and VH Bio Ltd
Charity No. 1123760
Welcome to the autumn edition of the Newsletter.
It was good to see so many of you at our successful 25th Annual Meeting in Manchester last month. For those who couldn’t be there we will have reports on the scientific and social highlights in the next edition of the Newsletter. In the meantime you can get a flavour of the events from the photos on the BSHI Facebook page.
Each year the BSHI Diploma candidate who submits the best abstract is awarded a bursary by VH Bio to attend the One Lambda European Clinical Histocompatibility Workshop. This year’s winner was Andrew Lemin from the Welsh Transplantation and Immunogenetics Laboratory. Andrew’s report from the workshop in Marbella starts this issue, and you can also read his winning abstract.
Allele-level HLA matching has been shown to be important for success following unrelated adult donor haematopoietic stem cell transplantation, but is it also important for cord blood transplants? In our Science Watch feature Mian Chen considers a study which provides some answers and discusses the implications for donor selection.
One of the ways in which BSHI supports its members is by providing bursaries to attend scientific meetings and training courses. In the past few months, members have attended meetings in Stockholm, London and Utrecht, which illustrate the breadth of interest and activities undertaken in UK labs. Thanks to the attendees for their reports.
We hope you enjoy these and the other regular features in this issue. If there is anything else you would like to see covered in the Newsletter please get in touch.
The Editorial Team

BSHI Volume 96 – 2014 Issue 3 ©2014 The British Society for Histocompatibility & Immunogenetics
3BSHI
British Society for Histocompatibility and Immunogenetics
Jacqueline O’Leary and Hugo Kaneku presented excellent work on the role of DSA in liver transplantation (O’Leary et al., 2014; Am J Transplant. 14; 779-87. Kaneku et al., 2013; Am J Transplant. 13; 1541-48). Selected abstracts were also presented during the morning session and covered many topics including de novo HLA antibodies in renal transplantation. Lunch was served at La Navilla Del Mar on the Marbella beachfront and many delegates took advantage of the location by taking a postprandial stroll along the promenade. The evening lecture was given – with much enthusiasm – by Adam Bingaman on the topic of antibody identification in kidney paired donation (KPD) (Bingaman et al., 2012; Am J Transplant. 12; 2125-32). Dr Bingaman presented the approach of the San Antonio KPD programme in transplanting highly sensitised patients (HSP). He also discussed some of the challenges of the programme including the requirement to ‘manipulate’ antibody assignments to transplant HSPs and the requirement for complex software to run daily matching algorithms.
The last morning was a shorter session and included presentations from selected abstracts. Diverse topics were discussed including HLA and non-HLA antibodies in heart transplantation, HLA typing strategies in cord blood banks and the use of sera pre-treatment to disrupt the prozone effect for single antigen bead antibody analysis. I also had the opportunity to present my BSHI project work at this session. My presentation was titled ‘A group-specific sequence-based typing (SBT) method for HLA-DQA1 and the prevalence of DQA1 alleles and haplotypes in blood donors resident in Wales’.
Overall, the workshop was an excellent educational opportunity and my thanks go to the organisers and to VH Bio Ltd for supporting my attendance
One Lambda.... continued
End
Accurate HLA-DQA1 typing is essential for evaluating transplant patients with DQ antibodies and determining risk haplotypes in some HLA class II-related diseases.
We developed SBT for DQA1 reliant on group-specific primary amplification. A problem with DQA1 SBT is that DQA1*02, 04, 05, 06 have a deletion of codon 56 causing an out-of-phase sequence during testing of heterozygotes for alleles with and without the deletion. Thus, both alleles were amplified and sequenced separately producing an unambiguous homozygous sequence for each. This reduced cis/trans ambiguities and circumvented the codon deletion issue. DQA1 polymorphism outside of exon 2 necessitates analysis of exon 3 and, for some of the six DQA1 allele groups, exons 1 and 4 to achieve an unambiguous second-field type. For each sample twelve separate template PCR reactions were conducted simultaneously to amplify appropriate exons for each of the DQA1 groups. Amplicons were linearly amplified bidirectionally with nine generic DQA1 sequencing primers using the BigDye Terminator kit (Applied Biosystems).
Successful validation used 50 reference samples, mostly from the UCLA International DNA Exchange Program.
For further validation and to improve our understanding of class II haplotypes we determined DQA1 frequencies and DRB1/DQA1/DQB1 haplotypes in 202 random subjects. These were HLA-A, B, C, DRB1, DQB1 second-field typed for the Welsh Bone Marrow Donor
Registry. All were aged <25 years, resident in Wales and from a largely UK European (UKE) population.
For all six loci the fit to Hardy-Weinberg equilibrium (all p>0.94) and the number of likely homozygotes identified (all p>0.12) was good (DQA1 p=0.95 and 0.96, respectively).
15 DQA1 alleles were found. Frequencies were: DQA1*01:01-0.12624, 01:02-0.20545, 01:03-0.04703, 01:04-0.02228, 01:05-0.01733, 02:01-0.13366, 03:01-0.06683, 03:02-0.0198, 03:03-0.08663, 04:01-0.01485, 04:02-0.00248, 05:01-0.14851, 05:02-0.00248, 05:05-0.10149, 05:09-0.00495.
Overall, the 2 and 3 loci haplotypes were typical of a UKE population. 15 DQA1/DQB1 haplotypes with significant corrected (p<0.01) D values were found. The five most frequent were: DQA1*05:01/DQB1*02:01- haplotype frequency (HF)-0.14818, 01:02/06:02-0.13338, 01:01/05:01-0.12326, 05:05/03:01-0.10128 and 02:01/02:02-0.08415.
27 DRB1/DQA1/DQB1 haplotypes with significant D values and HF >0.05 % were identified. The most frequent were: DRB1*03:01/DQA1*05:01/D Q B 1 * 0 2 : 0 1 - H F - 0 . 1 4 7 0 9 , 1 5 : 0 1 / 0 1 : 0 2 / 0 6 : 0 2 - 0 . 1 3 0 0 9 , 0 1 : 0 1 / 0 1 : 0 1 / 0 5 : 0 1 - 0 . 0 8 6 6 6 , 0 7 : 0 1 / 0 2 : 0 1 / 0 2 : 0 2 - 0 . 0 8 4 1 6 , 11:01/05:05/03:01-0.05296.
These findings usefully add to the HLA information of local donors and provide valuable insights into HLA Class II associations.
A group-specific sequence-based typing (SBT) method for HLA-DQA1 and the prevalence of DQA1 alleles and haplotypes in blood donors resident in WalesAndrew J Lemin, Jayne Johnson and Chris Darke
Welsh Transplantation and Immunogenetics Laboratory, Welsh Blood Service, Wales, United Kingdom

BSHI Volume 96 – 2014 Issue 3 ©2014 The British Society for Histocompatibility & Immunogenetics
4BSHI
British Society for Histocompatibility and Immunogenetics
LABScan3D™
Advanced Multiplex Analyzer
Features & Benefits
Advanced Multiplexing and Expanded Coverage
To learn about LABScan 3D™ contact
VH Bio’s HLA Product Specialists on 0191 495 8210
• Multiplexing capability with 500 unique beads for broader analyte detection
• Accelerated acquisition with dualsamplefluidicspathsandincreased syringe injection rate
• High throughput testing with reduced turnaround time
• Compatible with classic Luminex®-based assays along with the next generation of assays
LABType XRThe LABType XR (RUO) assay is designed exclusively for LABScan3D™
• 500 bead multiplexing
• Locus and Exon Coverage:
• A locus: Exons 2-5
• B locus: Exons 2-5
• C locus: Exons 2-7
• DRB1 locus: Exon 2
LABType CWDThe LABType CWD (RUO) assay was designed exclusively for LABScan3D™
• Developed based on the current CWD catalogue
• Locus and Exon Coverage:
• A locus: Exons 2-5
• B locus: Exons 2-5
• C locus: Exons 2-7
• DRB1 locus: Exon 2
VH Bio Ltd. Unit 11b Station Approach Team Valley Trading Estate Gateshead NE11 0ZF
T: +44(0) 191 495 8210 | F: +44(0)191 487 4285 | E: [email protected] www.vhbio.com

BSHI Volume 96 – 2014 Issue 3 ©2014 The British Society for Histocompatibility & Immunogenetics
5BSHI
British Society for Histocompatibility and Immunogenetics
Chair’s ReportDear colleagues I am writing this letter soon after returning from the 25th Anniversary BSHI Conference, BSHI 2014. Over the years the BSHI Conferences have been hosted in many locations throughout the UK and Eire but it was fitting that we returned to Manchester as the first Conference was held in Ashburne Hall, Manchester on 11th and 12th January, 1990. Kay Poulton had compiled a poster giving a brief summary of the early days of BSHI using material kindly provided by Phil Dyer and Steve Marsh. It was interesting to see many familiar faces on the photographs from the first conference. The poster will be published in a future edition of the newsletter.
BSHI 2014 was a great success as you will see when the reports from the Conference are published in the next Newsletter. The Manchester Conference centre was an excellent venue in the city centre and we enjoyed high quality scientific presentations. Prizes and certificates were presented at the Gala Dinner held in the impressive Manchester Town Hall. I would like to thank all those who worked so hard to ensure the success of the Conference, especially the Meetings Secretary, Arthi Anand, John Girdlestone, Luke Foster and members of the RE for programme planning and reviewing the abstracts, Kay Poulton, the Local Organiser and Jill Hitchenor and the
Events team at Sheffield Hallam University for providing the Secretariat support. We are extremely grateful to our Corporate Sponsors and Exhibitors for their support without which the Conferences would not be possible.
The AGM was held at BSHI 2014 on 4th September and the slides presented summarising all the activities of the Society will be available on the website. It is impressive to see how much work is undertaken by Members for the Society and to see the wide range of forums in which the profession is represented. We thanked the Committee members who have completed their term of office. Aliyye Karasu completed her term of office as an Ordinary Committee member and Sue Martin as Chair of the Education Board. Sue deserves special thanks as she has worked tirelessly for the Society in this role, which has been particularly challenging at this time when there are so many developments at all levels within Education. We are grateful that Deb Sage is now joining the Committee to Chair the Education Board.
I, too, completed my term of office as the Chair of BSHI at the AGM. It has been a privilege to serve in this role over the last 3 years. It has been a busy period and I have really enjoyed working with colleagues on the Committee on BSHI matters and over the last year with Kay Poulton during the time she has been Chair Elect. I wish Kay and the members of the Committee every success for the future. I do encourage all members to get involved in the work of the society. It is rewarding and involvement of the members will ensure that the society goes from strength to strength.
Best wishes,
Sue FuggleSeptember, 2014
BSHI Committee Members (from 2014 AGM)
Hon President: Prof John Forsythe Start: AGM 2012 Finish: AGM 2016
Chairperson: Kay Poulton Start: AGM 2014 Finish: AGM 2017 Tel: 0161 276 6667 Email: [email protected]
Secretary: David Turner Start: AGM 2012 Finish: AGM 2015 Tel: 0131 2427534 Email: [email protected]
Treasurer: John Smith Start: AGM 2013 End: AGM 2016 Tel: 01895 828774 Email: [email protected]
Meetings Secretary: Arthi Anand Start: AGM 2011 Finish: AGM 2014 Tel: 020 8258 2820 Email: [email protected]
Membership Secretary/BSHI Secretary Elect: Deborah Pritchard Start: AGM 2012 Finish: AGM 2015 Tel: 01443 622179 Email: [email protected]
Ordinary Members:
Richard Battle Start: AGM 2012 Finish AGM 2015 Tel: 0113 2064579 Email: [email protected]
James Robinson Start: AGM 2013 Finish: AGM 2016 Tel 020 7284 8307 Email: [email protected]
Chair BPAG: Brendan Clark Start: AGM 2013 Finish: AGM 2016 Tel: 0113 2066490 Email: [email protected]
Chair BEB: Deborah Sage, Start: AGM 2014 Finish: AGM 2017 Tel: [email protected]

BSHI Volume 96 – 2014 Issue 3 ©2014 The British Society for Histocompatibility & Immunogenetics
6BSHI
British Society for Histocompatibility and Immunogenetics
Chair’s Report
• National H&I Review: Terms of Reference for the review were commented on by Sue Fuggle (SF) and KayPoulton(KP)andafinalversionwassent to NHS England. Further progress and updates are awaited.
• KAG paper on defining significance of HLA Abs for renal Tx: Variationin practice in listing of unacceptableantigens has been identified by theChairoftheODTKAG.SFasScientificAdvisor has been asked to undertake a review. KAG will discuss the Terms of reference and process at the KAG meetingon10thJune.Suggestedthatresultingguidancecouldbeincludedinlatest version of BSHI/BTS Guidelines. ABSHI‘AbSIGworkinggroup’meetingis to be organized to discuss.
• RCPath Workforce planning: SF representedBSHIatameetingon7thMay to discuss the role of the College andSocieties inworkforceplanningofClinicalScientists.BSHIdatawasnotedas being of high quality. College will pursuecollectionofdataandaskedfora Rep from each society. Brendan Clark (BC) agreed to represent BSHI on this group.
• Renal CRG: SF has pushed for H&I activity to be included in futurecapacity planning. Work is ongoing withthenationaltariff.
• National Lab Medicine Catalogue: KP attendedmeetingattheCollege.Itwassuggested that Sarah Peacock would be asked if she could take this forward for BSHI (supported by others).
Continued on next page
BSHI Committee ReportSecretary’s Report from the meeting held on the 04/06/14. The following issues were discussed:
Secretary’s Report
• Electronic archiving of material: Richard Battle and James Robinsonhave set up a system on Google to allow back up of BSHI records.
• BSHI Rep to RCPath H&I Specialist Advisory Committee: Sarah Peacock has agreed to take on this role.
Treasurer’s Report
• EBS: John Smith (JS) having meetingwith EBS, who provide admin support to BSHI, to look at last year’s accounts. AlistofwaystheSocietyhasbenefitedmembers is required: training, BSHI bursaries, guidelines, journals, session at BTS etc. JS also wants to improve the ability to track expenditure and income fordifferentareasofthesociety.
• Payments for SIG meetings: SIG meetings have traditionally hadregistration fees (~£50). Dave Turner(DT) to contact Bristol to explain the HSCT SIG meeting should be selffunding and should work with Arthi Anand (AA) to set budget. JS to look at costingsformeetingsingeneralwithEBS.
• BSHI 2015, Cambridge: deposit paid for Clare College.
Membership Secretary’s Report
• Membership: now stands at 382.
Meetings Secretary’s Report
• NGS SIG: SueMartin(SM)tofeedbackto SD about the possibility of a NGS SIG
• RCPath meeting in December 2014: the cost needs to come down to make this viable. AA thinks this will happen after college meeting in July.Programme planning was discussed and SM suggested the input of the RE would be useful.
BSHI Education Board Report
• AiT meeting in Warwick, Oct 2014: BSHI will endorse this meeting, butprogrammestilltobeconfirmed.
• Case studies in Newsletter: requested in Newsletters, but nothing hasmaterialized. Everyone encouraged to speak to their colleagues, especially those undertaking the ACS portfolio,to try and get something produced. GuidelinesareintheNewsletter.
• AHCS: SM represents BSHI on the Blood Sciences Professional Group. The person fulfillingthisrolehastobenominatedbyBSHI and SF recommended that, as SF will be leaving the Council and handing over to KP, to ensure continuity, SMremainsonthiscommitteeatpresent.Confirmed that 2014 STP graduateswill have to go through an equivalence route to get registered with HCPC.
• Higher Training meeting, Manchester: this will go ahead in mid November 2014. Alison Logan planning this.
• Training Manual for Support Staff and Technologists: this is progressing, Amanda Robson (AR) hoping to get outadraftbytheendoftheyear.ARto discuss with Kingston Smith and JS about how costs will be managed.

BSHI Volume 96 – 2014 Issue 3 ©2014 The British Society for Histocompatibility & Immunogenetics
7BSHI
British Society for Histocompatibility and Immunogenetics
• IBMS Specialist Portfolio: Neil Marsden and Sarah Peacock are looking to update this document
• Textbook in H&I/collaboration with IBMS: Neil Marsden taking forward.
• HSST: recruitment process is now open. Call fromtheNationalSchoolforHealth-care Science for people to get involved in recruitment. KP may be available.
Professional Advisory Group Report
• HEE: workforce planning for HCS. BC hadameetingon28thMaywithHEE.Matters discussed were low uptakeof STP in H&I and knock-on effect onworkforce. Made point to Sue Hill that H&I should form part of STP course in firstyear.OthermessagetoSueHillwasabouttraineeswhoarealreadypartiallytrained and how they could feed into new HSST. Suggestion that Part IDiplomates should be able to access funding to complete to FRCPath. BC suggested three fast track contracts per year for the next 5 years to plug future gaps. BC working with HEE on this. ThanksweregivenfromtheCommitteeto BC and KP for this work.
• HCPC Proficiency Standards: response has gone in from BSHI.
• CTAG report: 29th April 2014. Allocation guidelines to be revised.H&I terminology was amended and suggestion made that H&I should bepartofMDTmeetings.
• BSHI/BTS Guidelines:KPhassubmittedto BTS Standards Committee (PeterAndrew).KPtotidyupexistingversion,but let PA know that an update will be imminent based on discussions ongoing at KAG regarding listing ofunacceptables in renal Tx.
BSHI Website
• Coordinator: Steven Jervis has now taken on this role from John Smith
BSHI Committee Report.... continued
The BSHI Julia Bodmer Travel AwardTo commemorate the life and work of Julia Bodmer and to recognise the seminal contributions she made to the field of human histocompatibility and immunogenetics, each year BSHI makes available an award of up to £2000. This is given with the aim of promoting the interaction and exchange of ideas between laboratories, either in the UK or overseas.
The award is aimed at scientists who are at an early stage in their career working in H&I and have been members of BSHI for over three years. It is intended to facilitate visits of at least two weeks duration to another laboratory to carry out a specific piece of research or to transfer new technologies.
Applications for the Julia Bodmer Travel Award must include a short (max 2 pages) description of the proposed scientific project along with estimated costs and supporting
Applications for travel in 2015 should be sent to the BSHI secretary ([email protected]) no later than 31st March 2015. Applications will be reviewed by the Research Executive and the successful candidate ratified by the Education Board. Notification of the outcome will be given by the end of April 2015.
letters from the directors of your own and the host laboratory. The budget outline must include laboratory costs, travel and subsistence.
The successful applicant is expected to write a report of the exchange visit to be published in the BSHI Newsletter and to give a short presentation at the BSHI annual conference.

BSHI Volume 96 – 2014 Issue 3 ©2014 The British Society for Histocompatibility & Immunogenetics
8BSHI
British Society for Histocompatibility and Immunogenetics
Impact of allele-level HLA matching on outcomes after myeloablative single unit umbilical cord blood transplantation for hematologic malignancyMary Eapen et al, Blood. 2014; 123(1):133-140.
Science WatchMian Chen, Transplant Immunology Laboratory, Oxford Transplant Centre
The importance of high-level donor-recipient matching at various human leukocyte antigen (HLA) loci for the success of unrelated adult donor hematopoietic stem cell transplantation (HSCT) is well documented. The inability to identify HLA-matched volunteer unrelated adult donors has often led to the use of umbilical cord blood (UCB) as an alternative graft to tolerate greater degrees of donor-recipient HLA mismatch. However, one of the biggest limitations of UCB transplantation is the high post-transplant non-relapse mortality (NRM).
Unrelated adult donors are selected to be closely matched to recipients at HLA-A, -B, -C, and -DRB1 at the allele level, whereas UCB units are selected using lower resolution HLA typing for HLA-A and -B and at the allele level for HLA-DRB1; HLA-C is not typically considered.
In a previous study [1], the authors have identified the benefit of matching at the HLA-C locus for the outcomes of UCB transplantation. Among transplantations matched at HLA-A, -B, and -DRB1 the NRM was higher in the HLA-C mismatched group than in the matched group. The limitation of the report was that HLA matching at HLA-A, -B, and -C was defined at the antigen level.
Allele-level matching
In this multicentre collaborative study, the effect of allele-level matching at HLA-A, -B, -C, and -DRB1 was analysed based on 1568 single umbilical cord blood (UCB) transplantations performed between 2000 and 2010. The primary end point was non-relapse mortality. Other outcome indicators such as overall mortality, neutrophil recovery, GvHD, and relapse were also analysed.
Donors and recipients were typed at HLA-A, -B, -C, and -DRB1 at low resolution for HLA-A, -B, and -C, and allele-level resolution at DRB1. High resolution of HLA-A, -B and -C typing was available for around half of the donor-recipient pairs. Instead of performing retrospective high resolution HLA typing for the remainder of donor and recipient pairs, a validated HLA high-resolution imputation algorithm, Haplogic III, developed by the NMDP was used to impute allele-level match status for these pairs.
The risk of NRM was found to be independently associated with the overall degree of allele-level HLA mismatch. UCB transplantations matched at HLA-A, -B, -C and -DRB1 alleles were associated with the lowest NRM risk. Interestingly, the NRM risks were not significantly different
between transplantations mismatched at 1 and 2 alleles or between those mismatched at 3 or 4 alleles. However, compared with transplantations mismatched at 1 or 2 alleles, risks were higher after transplantations mismatched at 3, 4 and 5 alleles. This finding differed from another recent report by a group from Japan that concluded HLA matching was not associated with NRM [2]. The authors of this paper argued that the Japanese report did not consider HLA-C and only performed low resolution typing for HLA-A and -B. It is likely that the “matched” control group in that report included a high proportion of allelic disparities and/or disparities in HLA-C.
Selection strategy
It was suggested in the discussion that the common practice of reliance on HLA typing at low or intermediate resolution or the use of selection algorithms that do not consider matching at the HLA-C locus is not fully adequate for selecting optimal UCB units. When a fully allele-level HLA-matched UCB unit is not available, mismatches at 1 and 2 alleles are better tolerated than mismatches at 3, 4, and 5 alleles and should be selected. The authors pointed out that the similarity of NRM risks between 3, 4 and 5 mismatched
Continued on next page

BSHI Volume 96 – 2014 Issue 3 ©2014 The British Society for Histocompatibility & Immunogenetics
9BSHI
British Society for Histocompatibility and Immunogenetics
groups could be attributed to the small number of this study population, and postulated that a larger cohort might be able to show a significantly different effect of more mismatches.
Examination of the risk estimates of mismatching at specific loci suggests isolated allele-level mismatches at HLA-A, -C, or -DRB1 but not at HLA-B were associated with higher NRM risks. However, because of linkage disequilibrium of HLA-B and -C, the likelihood of identifying a UCB unit with only an isolated -B mismatch is relatively low. Furthermore, the “better tolerated” effect of HLA-B mismatch must be viewed with caution – the number was very small: there were only 31 pairs of isolated -B mismatch in this cohort.
It was observed that total nucleated cell (TNC) content of the unit was the only other donor characteristic associated with NRM, and its effect was independent of HLA match. NRM rates were 15-20% higher in UCB units which contained TNC <3x107/kg. Within the HLA matched transplantation group and groups mismatched at 1, 2, 3, and 4 alleles there
were no added benefits of selecting units with TNC in excess of 3 x 107/kg. This suggested that lowering the cell dose threshold to 3 x 107/kg would enable a better matched UCB unit to be found.
Conclusions
In summary, the authors concluded that the results of these analyses suggest current practice for UCB selection using only low resolution HLA-A, -B typing and high resolution DRB1 typing but disregarding HLA-C mismatch is not adequate and should be revised; single-unit UCB transplants must have a minimum pre-cryopreserved TNC of 3 x 107/kg and thereafter the best allele-level HLA-matched unit should be selected. In the absence of a fully matched UCB unit, units mismatched at 1 or 2 alleles are acceptable. The authors also acknowledged that only a small proportion of patients who may benefit from transplantation will have a fully-matched UCB unit. With similar NRM risks after 1- and 2-allele mismatched transplants, selecting a unit mismatched at 2 alleles will extend access to 80-85%
Science Watch.... continued
1. Eapen M, Klein JP, Sanz GF, et al. Effect of donor-recipient HLA matching at HLA A, B, C, and DRB1 on outcomes after umbilical-cord blood transplantation for leukaemia and myelodysplastic syndrome: a retrospective analysis. Lancet Oncol. 2011; 12(13):1214-1221.
2. Atsuta Y, Kanda J, Takanashi M, et al; Different effects of HLA disparity on transplant outcomes after single-unit cord blood transplantation between pediatric and adult patients with leukemia. Haematologica. 2013; 98(5):814-822.
3. Di Bartolomeo P, Santarone S, De Angelis G, et al. Haploidentical, unmanipulated, G-CSF primed bone marrow transplantation for patients with high-risk hematologic malignancies. Blood. 2013; 121(5):849-857.
BSHI On-line Journal AccessBSHI provides members with full-text access to the following journals:
American Journal of Transplantation Bone Marrow Transplantation Current Opinion in Organ Transplantation International Journal of Immunogenetics Transplantation
Instructions on how to access these journals is on the Members’ Section of the BSHI website: www.bshi.org.uk/
of minorities and almost all Caucasians without an added risk to NRM compared with transplantations mismatched at 1 allele. Higher graft failure and NRM associated with mismatches at 3 or more alleles also imply such transplants should be recommended with caution. The recent successes of haploidentical transplantation [3] also warrant the relative merits of transplantation with a haploidentical donor weighed against the relative merits of 3 or more allele-mismatched single UCB transplantation.

British Society for Histocompatibility and Immunogenetics
This year I attended the EFI Annual Conference which was held in Stockholm, Sweden over 4 days from 25th-28th June. The conference was organised into several themes which included plenary sessions covering cell therapies, NK cells, tolerance mechanisms, autoimmunity and immunogenetics.
Some of the highlights included a talk from Professor Fabio Ciceri from the San Raffaele Scientific Institute, Milan, Italy, about haploidentical stem cell transplantation in acute leukaemia. Haploidentical stem cell transplants can be either CD34+ selected (T cell reduced) or unmanipulated bone marrow. Both have disadvantages: patients who receive CD34+ selected donations are more susceptible to viral infections and patients receiving unmanipulated donations require more immunosuppression to prevent graft versus host disease (GvHD); however there are strategies to overcome this. In a current trial of unmanipulated haploidentical donor transplants recipients are given an immunosuppression regime containing rapamycin and other calcineurin inhibitor free drugs. Rapamycin has been found to promote generation of natural T regulatory cells and it is hypothesised that this will reduce rates of GvHD. Preliminary results have shown this to be the case although relapse rates are high due to the advanced disease stage of the patients entered into the trial.
Report from the 28th EFI Conference 2014Sophie Laflin, H and I, Cambridge
The risk of infection in CD34+ selected transplants can be reduced by providing the patient with virus specific T cells; known as adoptive T cell therapy.
Dr Michael Uhlin from the Karolinska Institutet, Stockholm, Sweden, discussed the use of adoptive T cell therapy post allogeneic stem cell transplant.
As well as boosting the immune function following stem cell transplant, reducing the chance of infection, adoptive T cell therapy can also be used to increase the graft versus leukaemia GvL effect. He described the principle of manipulated T cell infusions and MHC multimer based cytotoxic lymphocyte CTL isolation. Manipulated T cell infusions consist of T cells genetically modified to express chimeric antigen receptors specific for tumour associated antigens. When these cells are infused into the patient they directly target tumour cells. MHC multimer CTL isolation is a method of isolating CTLs that are specific for a certain virus and HLA molecule. The MHC multimer is specifically designed to replicate the HLA class I molecule the donor T cell recognises and the viral specific peptide. When mixed with donor T cells the MHC multimer only binds to CTLs specific for the virus.
The addition of paramagnetic beads, which are able to bind to the MHC multimer, allow the specific CTLs to be
isolated from the rest of the T cell population. These cells can then be infused into the patient to counter current infection or prevent infection. The advantage of this technique is the speed at which the virus specific cells can be obtained.
During the plenary session entitled “Survival of the organ transplant” Dr Menna Clatworthy from the University of Cambridge, UK, presented her research into B cell regulation in transplantation. After a clinical trial of B cell reduction using rituximab had to be stopped early, when 5 out of 6 patients developed T cell mediated rejection, she shifted her research to focus on control of B cell activation. B cell activating factor (BAFF) is a cytokine that enhances B cell survival and proliferation; if levels of BAFF are high enough B cells no longer need T cell help for activation. A study of patients undergoing HLA incompatible (HLAi) kidney transplantation found that elevated levels of serum BAFF pre-transplant increased the risk of antibody mediated rejection post-transplant. Further to this her research group is now conducting a clinical trial using belimumab, an anti-BAFF antibody, in HLAi kidney transplantation.
In the “Tolerance mechanisms” plenary session Dr Niloufar Safinia, from King’s College London, UK, discussed the role of regulatory T cells in the induction of
Continued on next page
BSHI Volume 96 – 2014 Issue 3 ©2014 The British Society for Histocompatibility & Immunogenetics
10BSHI

BSHI Volume 96 – 2014 Issue 3 ©2014 The British Society for Histocompatibility & Immunogenetics
11BSHI
British Society for Histocompatibility and Immunogenetics
tolerance post solid organ transplant.
She described two clinical trials ongoing at Guy’s Hospital in London to test the safety and efficacy of regulatory T cell infusions post kidney or liver transplant.
In the same session Professor David Sachs, from Harvard Medical School, Boston, USA, gave a really interesting presentation about his experience with tolerance induction in patients receiving kidney transplantation. After a non-myeloablative conditioning regime patients received a bone marrow transplant from their live kidney donor followed by the kidney transplant. In 4 out of the 5 patients it was possible to completely stop immunosuppression at 9 to 14 months post kidney transplant and kidney function remained stable.
As well as the plenary sessions there were also several parallel sessions; I attended Educational session 1 where Professor Steven Marsh from the Anthony Nolan Research Institute, London, UK, gave an explanatory talk about NK cells and their receptors. After giving an overview of the complex genetic organisation and nomenclature of the KIR system Professor Marsh discussed some of his research, showing that specific B KIR haplotypes are associated with better outcomes following haematopoietic stem cell transplantation (HSCT) as a treatment for acute myelogenous leukaemia. He has developed a tool, available online at www.ebi.ac.uk/ipd/kir, to enable scientists to determine if the KIR haplotype combination of a particular donor-recipient pair is favourable or not. The idea is to use this to help determine which donor to select if more than one well HLA matched donor is available.
Next generation sequencing was the topic of another educational session. The methodology of the various next generation sequencing technologies available were explained by Dr Ingrid Fae from the Medical University Vienna, Austria. The session provided an opportunity for delegates to share
information about problems they have encountered while setting up next generation sequencing in their labs, for example, how to manage the large amount of data produced.
In the One lambda sponsored symposium entitled “A paradigm in flux: understanding the role of antibodies in transplant rejection” Dr Duska Dragun from the University of Berlin, Germany, presented the evidence that antibodies to angiotensin II type 1 receptor (AT1R) have a role in transplant rejection. Antibodies to AT1R have been found in patients suffering from vascular rejection after receiving an HLA matched organ; plasmapheresis to reduce the level of this antibody improved the patients’ conditions. AT1R antibodies present at the time of transplantation increase the risk of acute antibody mediated rejection. Therefore patients should be screened for AT1R specific antibodies prior to transplantation so the level of antibody can be reduced pre-transplant or immunosuppression tailored post-transplant to control rejection. Dr Carmen Lefaucheur from Hôpital Saint-Louis, Paris, France, discussed how determining the subclass, complement fixing ability, avidity and affinity of HLA specific antibodies is important and will improve immunological risk stratifications.
In the “Autoimmunity and Immunogenetics” plenary session Professor Olle Korsgren’s controversial lecture attempted to convince the audience that the current dogma for the aetiology of type 1 diabetes (T1D) is incorrect. After dissecting and dismissing some recent publications in popular medical journals, Professor Korsgren proposed that T1D is caused when the pancreas is damaged as a side effect of the immune response to bacteria in the gut. He suggested that this is due to changes in diet affecting the composition of gut microflora and increased portion size spreading the bacteria further along the digestive tract.
The final lecture was given by Professor Olle Ringden from the Karolinska Institutet,
Stockholm, Sweden, who gave an overview of his centre’s experiences with HSCT. A new approach to patient management that they are currently monitoring is the discharge of patients earlier after HSCT. If the patient has a family member able to care for them, no current infection and live within 2 hours drive of the hospital, they are able to go home sooner after HSCT. They have found patients who return home earlier have lower incidences of acute GvHD, less pro-inflammatory cytokines and better transplant related mortality figures. This is also cheaper for the transplant centre.
At the Karolinska they have also had successful experience with HSCT as a treatment for some solid tumours such as renal carcinoma, colon carcinoma, pancreatic adenocarcinoma and liver cancer. The patients receive chemotherapy or in the case of liver cancer a liver transplant and then HSCT transplant from HLA matched sibling.
As well as the many educational lectures, abstract presentations and large number of posters on display there was also the opportunity to relax and socialise. Olerup, one of the Platinum sponsors of the conference, treated many of the delegates to a mini-cruise and huge barbeque one evening with plenty of complimentary wine and beer. (This was very welcome as alcohol in Sweden is expensive!) Not to be outdone, One Lambda also hosted a party the same evening. The main event – the conference dinner party – was held the following evening in a converted old brewery on the waterfront, with a rooftop terrace overlooking the city. After the delicious buffet had been consumed many of the delegates danced the night away to the impressive live band.
At the end of the conference prizes for best abstract and poster were awarded and we were treated to an interesting promotional film produced by next year’s hosts – Geneva, Switzerland.
EFI Conference.... continued

BSHI Volume 96 – 2014 Issue 3 ©2014 The British Society for Histocompatibility & Immunogenetics
12BSHI
British Society for Histocompatibility and Immunogenetics
Susan Corbin
Susan Corbin needs little introduction to the majority of the BSHI Membership from her long service as Manager of UK NEQAS for H&I.
However, you may not be aware that she has been involved in tissue typing since 1969 when she joined the National Tissue Typing and Reference Laboratory (NTTRL) at Southmead Hospital in Bristol. It was here that she developed her passion for HLA and knew that this was what she wanted to do with her career.
She subsequently completed the IBMS special examination in blood group serology (1975) and the IBMS certificate in Medical Laboratory Management (1979) and continued to work in tissue typing when the NTTRL merged with the National Organ Matching and Distribution Service to form the UK Transplant Service in 1979 (now NHSBT-ODT).
Susan worked in the laboratories and took part in the on-call rota as an HLA specialist for the allocation of deceased donor organs for many years. She then became involved in the External Quality Assessment schemes, which at this time were being organised by UK Transplant. The EQA schemes later developed into UK NEQAS for H&I and Susan became Manager of the Service in 1991.
She continued to manage the EQA Schemes from UK Transplant after it moved to its current home at Stoke Gifford until 1999, when closure of the laboratories necessitated the re-location of UK NEQAS for H&I to the Welsh Transplantation and Immunogenetics Laboratory.
As well as Susan’s work on the UK NEQAS Executive Committee in the UK, she also greatly contributed to External Proficiency Testing (EPT) within Europe as a founder member of the European Federation of Immunogenetics (EFI). She has been a regular attendee at the annual EFI Conferences since 1983, only missing one meeting due to the birth of her son! She has been a member and co-chair on the EFI External Proficiency Testing Committee since 1998, where her work was vital to the introduction of the EFI standards for laboratories participating in EPT, as well as the EFI standards for EPT Providers.
In recognition of this, Susan has been awarded the EFI Medal which she was presented with at the EFI meeting in Stockholm. The medal is awarded annually to recognise the achievements of individuals who have made a significant contribution to EFI.
Susan retired in May 2014 and there is no doubt that she will be sadly missed from the EQA scene. On behalf of all her colleagues we wish her well for a long and happy retirement.
Deborah Pritchard, Manager of UK NEQAS for H&I.

BSHI Volume 96 – 2014 Issue 3 ©2014 The British Society for Histocompatibility & Immunogenetics
13BSHI
British Society for Histocompatibility and Immunogenetics
The IDRC was hosted by the Anthony Nolan this year at the Royal College of Physicians.
Day one
The first session was about how to best answer questions regarding transplant outcome. There were two talks, the first by Prof Charlie Craddock about randomized prospective studies and the second by Stephen Spellman on the importance of retrospective (observational) analyses. The conclusion of this session was that both can contribute towards improving outcome in HPCT.
The next educational session of the morning addressed donor availability issues and the impact on patients. Dr Alexander Schmidt (DKMS, Germany) discussed optimising the donor profile. Donors who have been HLA typed at more loci, and to higher resolution are much more likely to be selected for work-up request. A simulation overview performed on a virtual donor registry of 2.6 million donors found that 2.6% of patients had fully matched donors that could not be predicted by a virtual search.
10th International Donor Registry Conference16th-17th May 2014, Royal College of Physicians, LondonNicola Martin, Transplantation Laboratory, Manchester.
On a registry of this scale, this equates to 50 patients per year for whom the search process will be prolonged. The second talk by Dr Galen Switzer (University of Pittsburgh) discussed the donor attrition rate which is currently high, and is increasing, mostly due to ambivalence. There was some discussion about perhaps selecting better registry candidates and/or introducing a two stage recruitment process so that those on the register are more likely to proceed with donation. An interesting observation was that a 5% increase in retention offsets 2 years of recruitment so it is well worth investigating options for improving donor retention. The final talk of the session by Prof Nigel Russell described the Graft Identification and Advisory Service (GIAS) to potentially expedite donor selection, however the majority of delays documented appear to be due to patient and/or transplant centre factors.
The last session of the morning included a series of talks about alternative donor selection. First, Prof Effie Petersdorf gave a fascinating talk about novel selection mechanisms and secondary selection characteristics for unrelated donors. Non-HLA variation can be clinically relevant to transplant outcome and, after controlling for HLA mismatching, several important SNPs/genes have been identified. The patient genotype itself could be responsible for GvHD regardless of donor and in some instances an HLA mismatched donor may be more desirable due to SNPs on the extended MHC haplotype. Prof Gerhard Ehninger presented information about optimal donors ‘beyond HLA’. Some patients need a transplant very urgently and in these instances previous experience with the registry becomes especially relevant. Alternative treatment options may include haploidentical transplantation,
Continued on next page

BSHI Volume 96 – 2014 Issue 3 ©2014 The British Society for Histocompatibility & Immunogenetics
14BSHI
British Society for Histocompatibility and Immunogenetics
use of cord blood, and bi-specific antibodies which have a chimeric antigen receptor which can lead to specific killing of leukemic cells. This is a potential new treatment option to rival HPCT. Prof Tony Pagliuca gave the final talk of the morning about haploidentical HPCT. Cord and haploidentical HPCT are used more often for ethnic minority patients as it can be more difficult to find an HLA matched donor. Some good outcomes have been seen especially due to a protocol utilising a high dose of cyclophosphamide post-HPCT. Some interesting case studies were discussed including mini haplo HPCT for sickle cell disease where out of 22 patients, none have suffered any GvHD. Also, a young patient with aplastic anaemia who had no matched donor received a haploidentical HSCT from a sibling and 120 months post-HPCT was very healthy and doing well. Some discussion followed this as to whether unrelated donors mismatched at several loci could be used following on from the success of haploidentical HPCT, however it is believed that due to the difference in the rate of proliferation of the CD3+ cells that the current protocol using cylophosphamide would not give a good outcome with an unrelated donor.
The afternoon session discussed donor safety with the first talk by Prof Mike Pulsipher emphasising that the process of being a related donor has been found safe and reasonable for both adults and paediatrics. Dr Etienne Baudoux presented data about how cord donation has been assessed as safe and collection should only be performed if the pregnancy and delivery are uncomplicated.
This final talk of the day was followed by the poster viewing session and then it was onto the conference dinner which was held at London Zoo.
Day two
The second day started with an educational session about the challenges and solutions for global collaboration for registries. There were three talks discussing emerging registries (Saudi Arabia) and established registries (Denmark and NMDP). There are very few registries in developing countries and there are increasing demands for unrelated donors. Funding, accreditation and effective registry software continue to be problematic. Even for established registries such as the Danish Bone Marrow Donor Registry there are problems with funding and limited resources and collaboration is needed to share experiences between registries. The NMDP is a large well-established registry, however they are the biggest importer of international donors due to the ethnic diversity of the population and other registries having donors typed to a higher resolution which leads to them being selected preferentially. A panel discussion followed in which representatives from Brazil, Kuwait and Singapore presented the progress they have made in recent years in developing their registries.
The Best Abstract session followed with interesting talks from a variety of speakers. Jügen Sauter (DKMS) gave two talks where simulations had been run to test, firstly how often a matched donor can be ‘masked’ in a registry search due to a lack of high resolution typing,and secondly, the probability of finding a suitable cord blood donor if up to two HLA mismatched alleles were accepted. The results demonstrated that this approach would not require unrealistically large cord blood banks to achieve this. Dr Neema Mayor presented a talk about Single Molecule Real-Time (SMRT) technology which has been investigated by the Anthony Nolan to provide definitive HLA allele level resolution for potential donors. The
technology and equipment has been developed by Pacific Biosciences and has the capacity to produce long reads of sequence. The data presented showed that for HLA class I definitive allele typing could be achieved: in 37/42 cases the sequences matched, in one instance the IMGT database was incorrect and in 4 cases novel alleles were identified. Therefore, in all cases the SMRT sequencing method was found to be a highly accurate method for HLA typing. Jennifer Wuchter from the DKMS presented data which confirmed that potential donors are more likely to be selected if more HLA loci have been typed, and blood group and CMV are available at the time of potential donor selection. The final talk of the session was by Dr Rachel Pawson from the BBMR who had investigated the safety of stem cell donation by donors with a high BMI and had found that all donors had recovered post-donation and that PBSC donation in donors with a BMI of up to 40 appears to be safe. The prize for the Best Abstract session was awarded to Dr Neema Mayor.
The afternoon session consisted of several presentations about working together in an ethical environment. Dr Juliet Barker presented about cord quality and cost, including the variability in viability of cord units between cord blood banks. Dr Susan Tonks presented challenges in stem cell research and Prof Jeremy Sugarman discussed the ethical hazards of stem cell tourism.
The closing talk of the day was the Shirley Nolan lecture by Awardee Dr Dennis Confer from the NMDP. This was a very enlightening presentation covering the history of the Anthony Nolan Registry and a stark reminder of why the registries exist.
This was a particularly enjoyable conference and helped to reinforce how important global collaboration of the registries is necessary in order to maximise the chance of finding matched donor for patients. I thank BSHI for their bursary which helped to enable my attendance at the conference.
IDRC Conference.... continued

BSHI Volume 96 – 2014 Issue 3 ©2014 The British Society for Histocompatibility & Immunogenetics
15BSHI
British Society for Histocompatibility and Immunogenetics
As NHSBT is currently developing and implementing Next Generation Sequencing (NGS), I had the opportunity to attend the GenDx NGS HLA training course in Utrecht, the Netherlands, to gain an insight into the GenDx NGS workflow, kits and the analysis software NGSengine®. This was the first GenDx training school for NGS, a three-day course consisting of a series of presentations, laboratory training and introduction to NGSengine®.
The course began on Wednesday morning with a course overview by the Business Development Manager, Maarten Penning followed by a summary of the participants’ background and goals. The 15 participants consisted of H&I scientists as well as GenDx and Illumina distributers from
GenDx Training School: NGS SBT HLA March 2014Zareen Goburdhun, H & I Dept., NHSBT Colindale.
India, South Africa, and Europe with little or no experience of NGS. The first presentation of the day on ‘Next Generation Sequencing Introduction’ was given by Jeroen Adema, Technical Application Specialist. This was an excellent talk explaining the basics of the NGS workflow from library preparation to clonal amplification and sequencing, comparing the Illumina and Ion Torrent approaches. Jeroen then went on to describe the GenDx NGS workflow and protocols, using NGSgo®-AmpX (HLA gene amplification primers for HLA-A, B, C, DRB1, DQB1) and GenDx reagents developed for the library preparation. The morning session was followed by group laboratory work using samples sent in by the participants prior to the start of the course. The day ended with a quiz on NGS and dinner hosted by GenDx at a local restaurant. This was a lovely opportunity to get to know Utrecht and the other delegates.
Day two started with a review of the results of the previous day’s quiz, with positive feedback for all, though I am
pleased to announce I obtained the top marks! The rest of the day alternated between presentations on setting up and monitoring a MiSeq run, MiSeq and Ion Torrent chemistry and wet work loading the MiSeq with our pooled samples. It was particularly useful to have a combination of theory and practical to understand the process, which is quite complex. After a brief lunch, we gathered in the meeting room to gain hands-on experience of NGSengine®, aided by software developer Frans Ruzius and bioinformatician Erik Rozemuller. The day ended with another quiz followed by a guided tour of the Dom tower, with spectacular views of the city once we had climbed the 465 steps! Dinner followed, organised by Wietse Mulder, GenDx co-founder, allowing us to recover from our adventure.
The last day consisted of a presentation on the “NGS experience at GenDx” by Jeroen who described the various verification experiments conducted by the technical and R&D team from testing different fragmentation enzymes to the impact of the pooling of HLA loci on final analysis and results. This was very helpful as a guide to troubleshooting and optimising our own experiments. Throughout the morning, we waited with anticipation for the MiSeq run to finish. Our data was finally ready to be analysed by midday. We spent the next few hours using NGSengine® to look at our data and generate results before leaving Utrecht after lunch.
As a NGS beginner I found the course very useful; the NGS workflow was explained very clearly and I came away with a better understanding of the basics. It was also a great opportunity to meet H&I scientists from different countries and to learn about their processes and protocols.

BSHI Volume 96 – 2014 Issue 3 ©2014 The British Society for Histocompatibility & Immunogenetics
16BSHI
British Society for Histocompatibility and Immunogenetics
BSHI Continuing Professional Development
Journal Based Learning
The CPD JBL questions can be found on the BSHI website, and you must now submit your answers electronically via the website.
CPD PointsThequestion/answercardswillbemarkedandscoredbyanassessorappointedbythePDE.Pointswillbeawardedonthebasisof: 0-10 answers correct – 0 points, 11-14 correct – 1 point, 15 – 19 correct – 2 points, all 20 correct – 3 points.
How to participateIfyouareregisteredontheBSHICPDscheme,thenyouareeligibletoparticipateintheJournalBasedLearningscheme.Allyouneedtodoisreadthereferencearticlegivenatthetopoftheanswercard,andthenanswerthequestionstatementsbychoosingtrueorfalseforeachofthe20statementsrelatingtothearticle.Gotohttp://www.bshi.org.uk/members/cpd_questions.html
Thenfillinyourname,contactaddress,e-mailaddressandBSHImembershipnumber.Simply click on your choice. Any answers that are not clear, or are ambiguous, will not score.
John Girdlestone,NHS Blood and Transplant, [email protected]
The deadline for submission of completed cards for this cycle is: 14th November 2014
Your answers will be assessed and returned to you with the number of CPD points earned, for inclusion in your BSHI CPD folder.Any members not currently registered on the CPD scheme, but interested in joining should contact the BSHI CPD Co-ordinator; detailsintheNewsletter
If you have any comments or suggestions about the journal based learning series and the topics/articles [email protected]

BSHI Volume 96 – 2014 Issue 3 ©2014 The British Society for Histocompatibility & Immunogenetics
17BSHI
British Society for Histocompatibility and Immunogenetics
Journal Based Learning Cycle 51Paper title & reference: IMPACT Of HLA MISMATCH DIRECTION ON OuTCOMES AfTER uMBILICAL CORD BLOOD TRANSPLANTATION fOR HAEMATOLOGICAL MALIGNANT DISORDERS: A RETROSPECTIvE EuROCORD-EBMT ANALySIS. CuNHA R, LOISEAu P, RuGGERI A, ET AL. BONE MARROW TRANSPLANTATION 2014; 49: 24-29. All CPD returns to be made by the BSHI internet link. Deadline for submission of completed answers: 14th November 2014 All journals chosen are available through the BSHI access or are open access journals.
Scoring CPD points will be awarded as follows: 0-10 correct 0 points 11 – 14 correct 1 point 15 – 19 correct 2 points 20 correct 3 points
1. Leukemia-free survival is the same for fully matched high resolution typed unrelated adult donors and umbilical cord blood transplants (UCBT) with 1 to 2 HLA mismatches defined by Ag typing level for HLA-A and –B and allele typing for DRB1.
True False
2. Mismatch tolerance in UCBT may be explained by the higher number of T cells infused. True False
3. Mismatch is classified as being in the graft-versus-host direction (GVH) when the recipient is homozygous for one locus and only one of the HLA Ags/alleles is identical in a heterozygous donor.
True False
4. The patient cohort consisted of 1565 patients who received an unrelated single unit UCBT as first allogeneic transplant.
True False
5. Matching at HLA-C, -DQ and –DP was also considered for this study. True False
6. The reference group consisted of patients given grafts with 5/6 HLA compatible, classified as BID mismatch. True False
7. Fulldonorchimerismwasdefinedassustaineddonorengraftmentassessedusingchimerismassay(≥98%donor). True False
8. In this study, platelet recovery was defined as achieving platelet levels greater or equal to 20x109/L, unsupported by platelet transfusions for 7 days.
True False
9. DFS and OS were assessed using a Cox proportional hazards regression model. True False
10. 40% of patients were transplanted for AML. True False
11. Reduced intensity conditioning was used in 81% of patients. True False
12. The median infused TNC number was 3.4 x107/kg and the median CD34 cell number was 1.4x105/kg. True False
13. Neutrophil recovery rate was not significantly correlated with GVH mismatch compared with the reference group. True False
14. The risk of developing aGVHD grade 2-4 was lower for patients receiving an infused TNC cell dose >3.4x107 cells/kg. True False
15. Patients receiving a graft with 2 MM BID or 1 MM BID +1 MM HVG showed higher risk of cGVHD incidence compared with the reference group.
True False
16. HLA mismatch direction was associated with NRM. True False
17. Recipients given a 6/6 graft had a lower risk of relapse incidence. True False
18. Infection was the cause of death in 40% of deaths related to UCBT complications. True False
19. There is a need for future studies with a large well-characterised transplant population to address the role of high resolution typing and matching.
True False
20. On the basis of this study, there is evidence to support a change in the current practice for choosing CBUs, taking into account HLA mismatch direction.
True False

BSHI Volume 96 – 2014 Issue 3 ©2014 The British Society for Histocompatibility & Immunogenetics
18BSHI
British Society for Histocompatibility and Immunogenetics
1. EBV is implicated in almost all PTLDs occurring within 1 year of transplantation. True
2. All patients in the prospective study cohort received heart alone transplants. False
3. All patients received mycophenolate mofetil (MMF) as part of their immunosuppressive treatment. False
4. The effects of CMV reactivation, EBV infection and rituximab administration were assessed using a univariate Cox model.
True
5. EBV primary infection was defined as a viral load greater than 105 copies/ml of blood. False
6. A single infusion of Rituximab was administered to patients with EBV load >106 copies/ml. True
7. 37% of recipients were CMV negative at the time of transplantation. False
8. CMV primary infection was a predictive factor for EBV reactivation. False
9. All EBV-negative recipients receiving a transplant from an EBV-positive donor developed primary EBV infection.
True
10. Presentation of EBV infection is the same for primary infection and reactivation. False
11. Immunosuppressive therapy with OKT3 reduces the incidence of PTLD. False
12. The authors demonstrate a link in this study between CMV infection and EBV reactivation. False
13. All instances of post-transplant EBV infection in CMV negative recipients were due to primary infection. False
14. Diminution of immunosuppression to treat EBV infection increases the risk of graft rejection. False
15. The majority of EBV infections in transplanted adults are due to reactivation. True
16. The incidence of EBV reactivation reported in different studies is extremely variable due to the application of different viral-load thresholds.
True
17. The authors conclude that changing azathioprine for MMF results in decreased PTLD incidence in heart transplant recipients.
False*
18. There is no standardised treatment for EBV primary infection/reactivation post solid-organ transplant. True
19. Per-protocol analysis demonstrated that patients treated for EBV primary infection or reactivation were significantly less likely to develop PTLD.
True
20. This algorithm can be directly applied to recipients of any solid organ transplant. False
Journal Based Learning Cycle 50Paper title & reference: ADAPTED TREATMENT Of EPSTEIN-BARR vIRuS INfECTION TO PREvENT POSTTRANSPLANT LyMPHOPROLIfERATIvE DISORDER AfTER HEART TRANSPLANTATION. CHOQuET S, vARNOuS S, DEBACK C, GOLMARD JL AND LEBLOND v. American Journal of Transplantation 2014; 14: 857-866..
* judged to be ambiguous, all answers marked as correct.

BSHI Volume 96 – 2014 Issue 3 ©2014 The British Society for Histocompatibility & Immunogenetics
19BSHI
British Society for Histocompatibility and Immunogenetics
Call for Case StudiesThis notice is an update on the process for submission of case studies for publication in the Newsletter.
The purpose of publishing case studies in the Newsletter is to highlight interesting cases from individual H&I laboratories that the community as a whole would benefit from in terms of training and education or to generate discussion. We all stand to learn from each others’ experiences.
There is no template for the submission. As a guide, it should be approximately 1000 words in length and at least at the level appropriate for inclusion in a portfolio for the Association of Clinical Scientists. Cases should include only a brief description of laboratory tests and focus primarily on the interpretation of results in the clinical context and their impact on patient management. Essentially, the more unusual and informative it is the better. Key learning points should be identified in order to highlight the educational value of the case.
Cases equals prizes!
As a replacement for the CPD prizes previously awarded for achievements in Journal Based Learning, theBSHIEducationBoardwillnowawarda£25booktokenforeachcaseselectedforpublication intheNewsletter.
Submission process
Please send your submission to the BSHI Secretary, Dave Turner ([email protected]). Cases will then be reviewed by at least two members of the Education Board to assess suitability for publication. No more than one case study will be published in each Newsletter but if there is more than one suitable case submitted for one edition then cases may be held in reserve for publication in subsequent editions.
Susan Martin, Chair, BSHI Education Board
Work Submission Deadline Application for viva deadline Viva Week
28th February 2014 28th March 2014 28th April – 2nd May 2014
20th June 2014 18th July 2014 18th-22nd August 2014
10th October 2014 7th November 2014 8th-12th December 2014
BSHI Diploma Viva dates 2014
Given the reduction in the number of trainees undertaking the BSHI Diploma it is necessary to reduce the number of viva sessions per year. The TDE have agreed that from 2015 onwards vivas will be held in the last week of April and the first week of October each calendar year
BSHI Volume 96 – 2014 Issue 3 ©2014 The British Society for Histocompatibility & Immunogenetics
20BSHI
British Society for Histocompatibility and Immunogenetics
Special Interest Groups (SIG)Haemopoietic Stem Cell(HSC )Antibody
Main BSHI CommitteeChairperson, Secretary, Treasurer, Meetings Secretary,
BEB Chairperson, BPAG Chairperson, 6 ordinary committee members
THE BRITISH SOCIETY FORHISTOCOMPATIBILITY AND IMMUNOGENETICS
Committees, Subcommittees and Working Groups
BSHI Education Board (BEB)
Training Executive (TE) Research Executive (RE)Professional Development Executive (PDE)
Professional Representatives/Contacts Group
Standards Working GroupBSHI ChairpersonSIG representativesUK members of EFI Standards Committee
BSHI Professional Advisory Group (BPAG)
BSHI Honorary President
THE BRITISH SOCIETY FORHISTOCOMPATIBILITY AND IMMUNOGENETICS
Committees, Subcommittees and Working GroupsMain BSHI Committee
Chairperson, Secretary, Treasurer, Meetings Secretary, BEB Chairperson, BPAG Chairperson, 6 ordinary committee members
BSHI Honorary President
BSHI Education Board (BEB)
Special Interest Groups (SIG)Haemopoietic Stem Cell(HSC )Antibody
Training Executive (TE) Professional Development Executive (PDE)
Research Executive (RE) Standards Working GroupBSHI ChairpersonSIG representativesUK members of EFI Standards Committee
Professional Representatives/Contacts Group
BSHI Professional Advisory Group (BPAG)
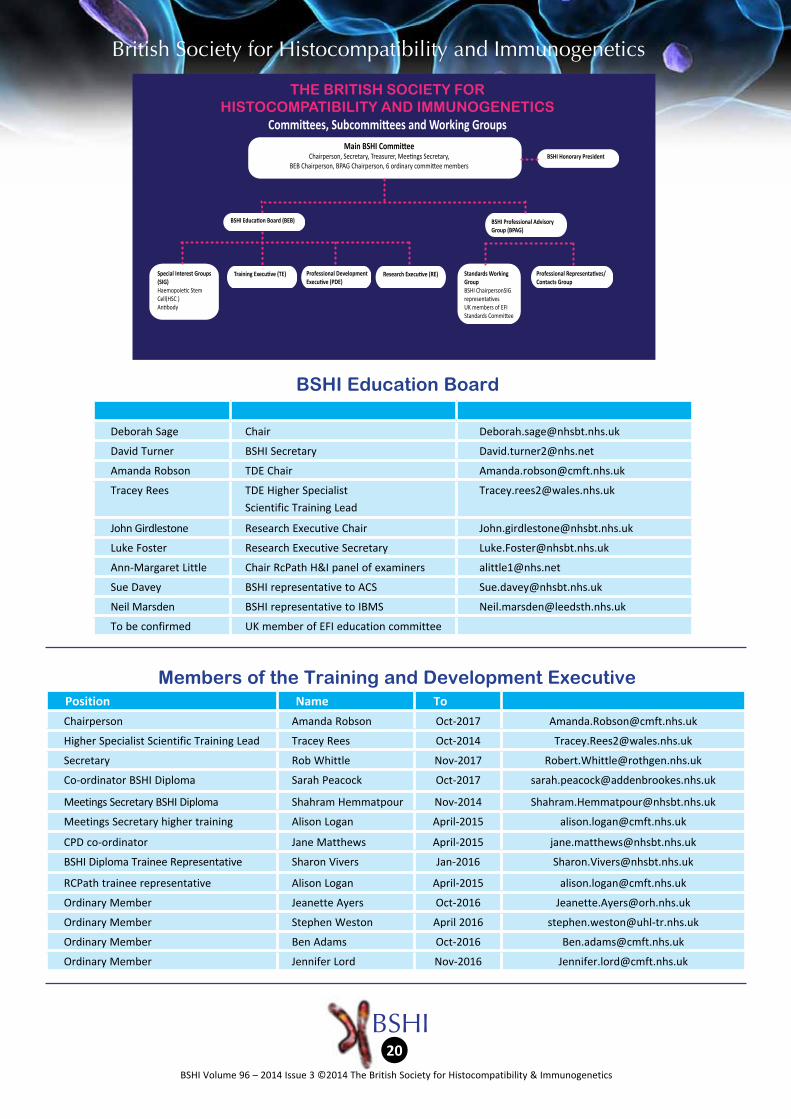
BSHI Education Board
Deborah Sage Chair [email protected]
David Turner BSHI Secretary [email protected]
Amanda Robson TDE Chair [email protected]
Tracey Rees TDE Higher Specialist Scientific Training Lead
John Girdlestone Research Executive Chair [email protected]
Luke Foster Research Executive Secretary [email protected]
Ann-Margaret Little Chair RcPath H&I panel of examiners [email protected]
Sue Davey BSHI representative to ACS [email protected]
Neil Marsden BSHI representative to IBMS [email protected]
To be confirmed UK member of EFI education committee
Members of the Training and Development Executive Position Name To
Chairperson Amanda Robson Oct-2017 [email protected]
Higher Specialist Scientific Training Lead Tracey Rees Oct-2014 [email protected]
Secretary Rob Whittle Nov-2017 [email protected]
Co-ordinator BSHI Diploma Sarah Peacock Oct-2017 [email protected]
Meetings Secretary BSHI Diploma Shahram Hemmatpour Nov-2014 [email protected]
Meetings Secretary higher training Alison Logan April-2015 [email protected]
CPD co-ordinator Jane Matthews April-2015 [email protected]
BSHI Diploma Trainee Representative Sharon Vivers Jan-2016 [email protected]
RCPath trainee representative Alison Logan April-2015 [email protected]
Ordinary Member Jeanette Ayers Oct-2016 [email protected]
Ordinary Member Stephen Weston April 2016 [email protected]
Ordinary Member Ben Adams Oct-2016 [email protected]
Ordinary Member Jennifer Lord Nov-2016 [email protected]

BSHI Volume 96 – 2014 Issue 3 ©2014 The British Society for Histocompatibility & Immunogenetics
21BSHI
British Society for Histocompatibility and Immunogenetics
BSHI representatives to other professional societies/organisationsOrganisation Member’s Name Term of office Ends Tel No./Email
Academy for Healthcare Science Blood Sciences Professional Group
Sue Martin [email protected] 0161 276 6215
Academy for Healthcare Science Council Kay Poulton [email protected] 0161 276 6667
Association of Clinical Scientists Sue Davey As required N/A [email protected] 020 8957 2997
British Society for Immunology BSHI Affinity Group
Luke Foster 3 years 2016 [email protected] 0208 957 2714
Clinical Pathology Accreditation (UK) Ltd Martin Barnardo 3 years 2016 [email protected] 01865 226102/4
International Journal of Immunogenetics Luke Foster 3 years 2016 [email protected] 0208 957 2714
NHSBT Bowel Advisory Group David Briggs 3 years 2014 [email protected] 0121 253 4099
NHSBT Cardiothoracic Advisory Group John Smith 3 years 2014 [email protected] 01895 828774
NHSBT Kidney Advisory Group Tracey Rees 3 years 2015 [email protected] 01443 622175
NHSBT Pancreas Advisory Group Vaughan Carter 3 years 2016 [email protected] 0191 202 4411
Royal College of Pathologists H&I Sub-committee Sarah Peacock Andrea Harmer (chair)
[email protected] 01223 348 833 [email protected] 0114 358 4800
UK NEQAS Quality Assurance Advisory Panel in Immunology
Helena Lee 3 years 2016 [email protected] 0161 276 6397
British Transplantation Society Martin Howell 2 years 2015 [email protected] 0191 219 4475
European Federation for Immunogenetics Standards Committee
Sue Fuggle Kay Poulton (chair)
As required N/A [email protected] 01865 226162 [email protected] 0161 276 6667
Institute of Biomedical Sciences David Wilson As required N/A [email protected] 01224 6552858
Royal College of Pathologists Standing Committee for Clinical Science
Bob Vaughan 3 years 2015 [email protected] 020 7188 1534
RE Membership
Position Name Commenced Contact detailsChairperson John Girdlestone AGM 2012 [email protected]
Secretary Luke Foster 11/07/2013 [email protected]
Ordinary member David Lowe AGM 2013 [email protected]
Ordinary Member Vivien Hanson 21/11/2013 [email protected]
Ordinary Member Catherine Cormack 21/11/2013 [email protected]
Ordinary Member Mian Chen 21/11/2013 [email protected]
Ordinary Member Zareen Goburdhun 21/11/2013 [email protected]