brian russ pt, dpt, comt, faaompt matt willey pt, dpt, … · neurophysiology ! radiology ! patient...
TRANSCRIPT

1
CLINICAL REASONING AND EVIDENCE-BASED PRACTICE:THE POWER OF COMBINING BOTH
Brian Russ PT, DPT, COMT, FAAOMPT Matt Willey PT, DPT, OCS, COMT, FAAOMPT Amy Pakula PT, DPT, OCS, FAAOMPT
Objectives
Present a model of patient care guided by examination findings integrating EBP.
Demonstrate how diligent tracking of examination findings serves as the primary guide during patient management.
Discuss a model of progression based on the patient response to selected interventions and discuss how factors may alter the decision making process.
“The important thing is not to stop questioning. Curiosity has its own reason for existing.” –Albert Einstein!
34% of individuals do not fit a classification-based system
Stanton et al, PT, 2011
Permeable Brick Wall
Theoretical Clinical
§ Diagnosis
§ Pathology
§ Neurophysiology
§ Radiology
§ Patient Presentation
§ History
§ Signs
§ Symptoms
The Evidence Clinical
CPR
TBC
Test Clusters/Metrics
Psychosocial Symptoms
Signs History Patient
Presentation

2
“A process in which the therapist, interacting with the patient... helps patients structure meaning, goals, and heath care management strategies based on clinical data, patient choices, and professional judgment.”
- HIGGS AND JONES
Clinical Reasoning S.I.N.S.S
Severity Irritability Nature of the disorder Stage Stability
Key Points
Asterisks Treat Re-assess S.I.N.S.S Diligent tracking of clinical signs and
symptoms.
Evidence-informed decisions based on patient response.
Guiding force determining the vigor
of an intervention.
• Patient Profile • Body Chart • Aggravating/Easing Factors • Current History • Past History
Patient Profile § 36 year old female
referred for LBP § Parent Advocate § Jogs 3 miles 3/wk § Oswestry 28% § Married, mother of 2
children
Hypothesis Generation § Disc/Other? § OA unlikely
§ Flexion-based? § Functionally
limited?
§ Age? § Limited and in
what way?
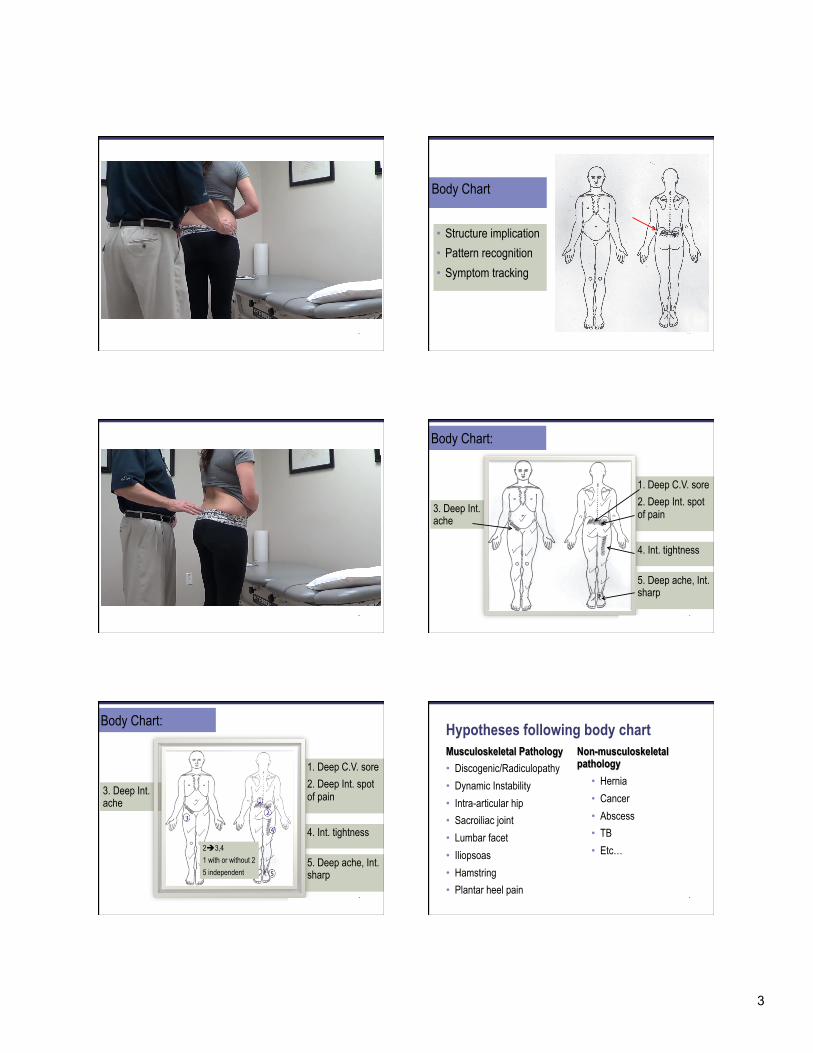
• Structure implication • Pattern recognition • Symptom tracking
Body Chart
3
• Structure implication • Pattern recognition • Symptom tracking
Body Chart
4. Int. tightness
1. Deep C.V. sore 2. Deep Int. spot of pain 3. Deep Int.
ache
Body Chart:
5. Deep ache, Int. sharp
5. Deep ache, Int. sharp
4. Int. tightness
3. Deep Int. ache
1. Deep C.V. sore 2. Deep Int. spot of pain
2è3,4 1 with or without 2 5 independent
Body Chart:
Hypotheses following body chart Musculoskeletal Pathology • Discogenic/Radiculopathy • Dynamic Instability • Intra-articular hip • Sacroiliac joint • Lumbar facet • Iliopsoas • Hamstring • Plantar heel pain
Non-musculoskeletal pathology
• Hernia • Cancer • Abscess • TB • Etc…
4
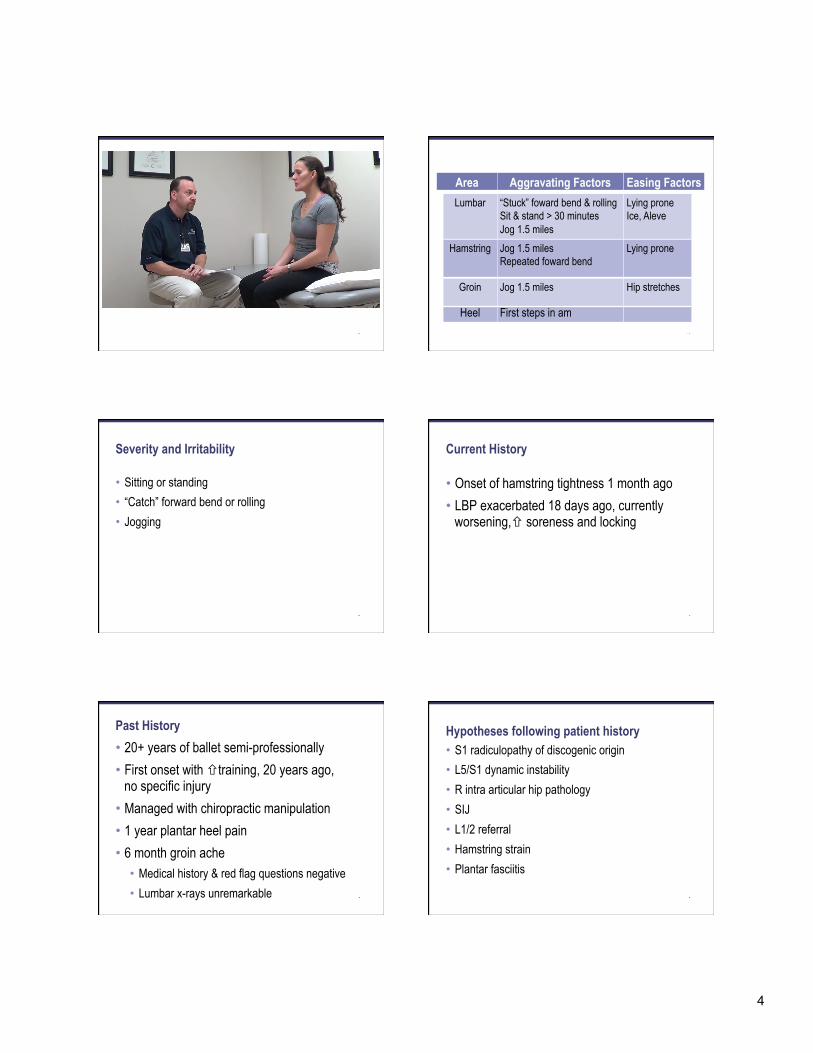
Lumbar “Stuck” foward bend & rolling Sit & stand > 30 minutes Jog 1.5 miles
Lying prone Ice, Aleve
Area Aggravating Factors Easing Factors
Hamstring Jog 1.5 miles Repeated foward bend
Lying prone
Heel First steps in am
Groin Jog 1.5 miles Hip stretches
Severity and Irritability
• Sitting or standing • “Catch” forward bend or rolling • Jogging
Current History
• Onset of hamstring tightness 1 month ago • LBP exacerbated 18 days ago, currently
worsening,ñ soreness and locking
Past History • 20+ years of ballet semi-professionally • First onset with ñtraining, 20 years ago,
no specific injury • Managed with chiropractic manipulation • 1 year plantar heel pain • 6 month groin ache
• Medical history & red flag questions negative • Lumbar x-rays unremarkable
Hypotheses following patient history • S1 radiculopathy of discogenic origin • L5/S1 dynamic instability • R intra articular hip pathology • SIJ • L1/2 referral • Hamstring strain • Plantar fasciitis
5
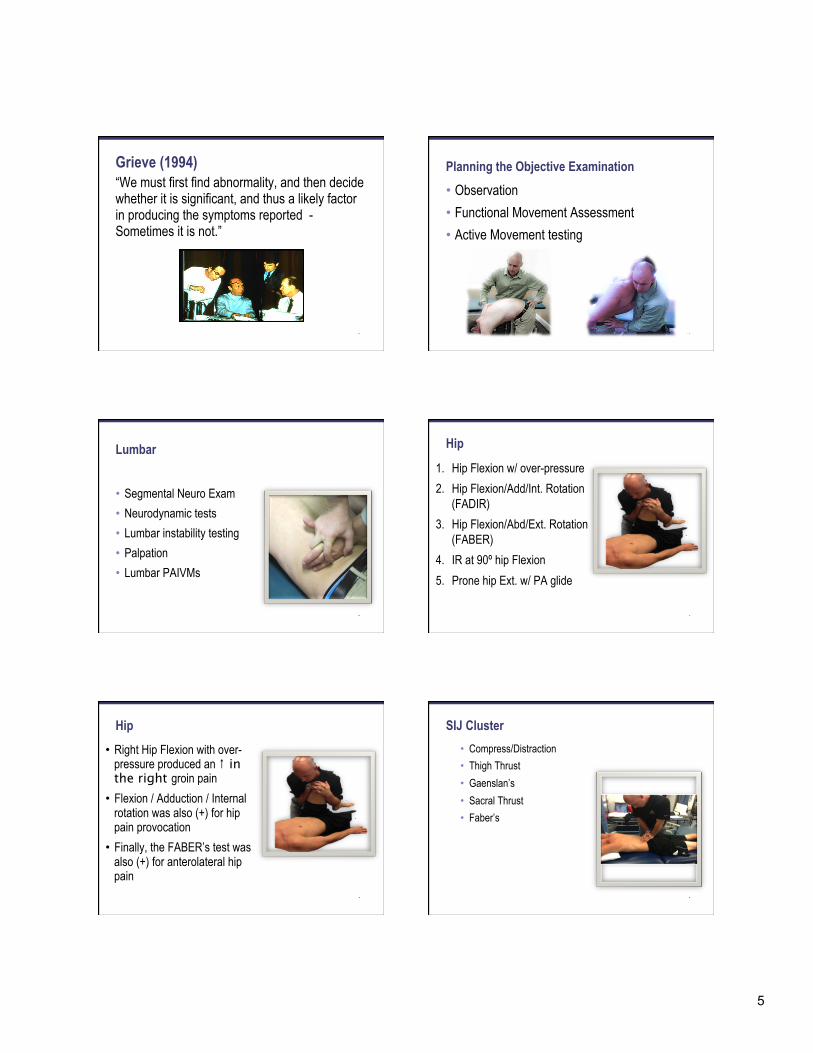
Grieve (1994) “We must first find abnormality, and then decide whether it is significant, and thus a likely factor in producing the symptoms reported - Sometimes it is not.”
LBP Heel Pain
Planning the Objective Examination
• Observation • Functional Movement Assessment • Active Movement testing
Lumbar
• Segmental Neuro Exam • Neurodynamic tests • Lumbar instability testing • Palpation • Lumbar PAIVMs
Hip
1. Hip Flexion w/ over-pressure 2. Hip Flexion/Add/Int. Rotation
(FADIR) 3. Hip Flexion/Abd/Ext. Rotation
(FABER) 4. IR at 90º hip Flexion 5. Prone hip Ext. w/ PA glide
Hip • Right Hip Flexion with over-
pressure produced an ↑ in the right groin pain
• Flexion / Adduction / Internal rotation was also (+) for hip pain provocation
• Finally, the FABER’s test was also (+) for anterolateral hip pain
SIJ Cluster • Compress/Distraction • Thigh Thrust • Gaenslan’s • Sacral Thrust • Faber’s

6
Hypotheses following objective exam • S1 radiculopathy of discogenic origin • L4/5 dynamic instability • R intra articular hip pathology • SIJ • L1/2 referral • Hamstring strain • Plantar fasciitis
Intervention Visit One
What should the first intervention be?
EBP/TBC Dilemma
Instability Manipulation ü Age
ü Instability Catch
ü + prone instability test
ü SLR > 91°
ü 18 days
ü No pain below knee
ü Hip IR > 35°
ü Lumbar hypomobility
ü Centralization
ü Symptoms
distal to buttock
Specific Exercise
Intervention Visit One: Central PA L5 Reassessment of Asterisks
• Observation • Lumbar ext with O/P • Hip flexion w/ O/P, FABER,
FADIR • SLR • PA L4 & L5 • Prone Instability Test • Palpation hamstring/heel • EHL MMT
Re-assessment of Asterisks: • Lumbar extension w/ O/P // ê hamstring and groin pain, é ext ROM
• Hip flexion w/ O/P, FADIR // ê R groin pain • FABER no change • R SLR // 100°(+ 20° to onset of hamstring tightness) • PA L5 // ê stiffness and pain • PA L4 // unchanged • Hamstring trigger point // ê • Heel palpation // no change • EHL // improved to 4+/5
Visit Two (Day 5)
How will you determine your progression?

7
Re-assessment of Subjective Asterisks
• Symptoms in standing // ê back & hamstring soreness, NPRS 1/10
• Turning over in bed // one episode • Running // groin and hamstring 2 miles • Sensation of locking // has avoided bending • Heel pain increased following intervention
Re-assessment of Objective Asterisks • Aberrant movement improved • Lumbar extension w/ OP ê hamstring and groin pain, é ROM,
R sided LBP persists • ê groin pain hip flexion and FADIR, FABER no change • SLR R 100 hamstring tightness • ê stiffness and pain PA L5, no change in muscle guarding L4 • Hamstring trigger points éto evaluation level • EHL MMT returned to evaluation level 4/5 • Heel palpation (-)
Additional testing visit two
• Foot/ankle exam • Slump test (+) R -10° knee extension with
reproduction of hamstring and heel symptoms with dorsiflexion
Intervention Visit Two: Objective Asterisks
• Aberrant movement • Lumbar extension w/ OP in
standing • Hip flexion w/ OP, FABER,
FADIR (-) • PAIVM at L4 and L5 • Hamstring/heel palpation (-) • EHL MMT 4+/5
Hypotheses following visit two intervention
• S1 radiculopathy of discogenic origin • L4/5 dynamic instability • R intra articular hip pathology
Visit Three (Day 10)
How will you determine your progression?
8
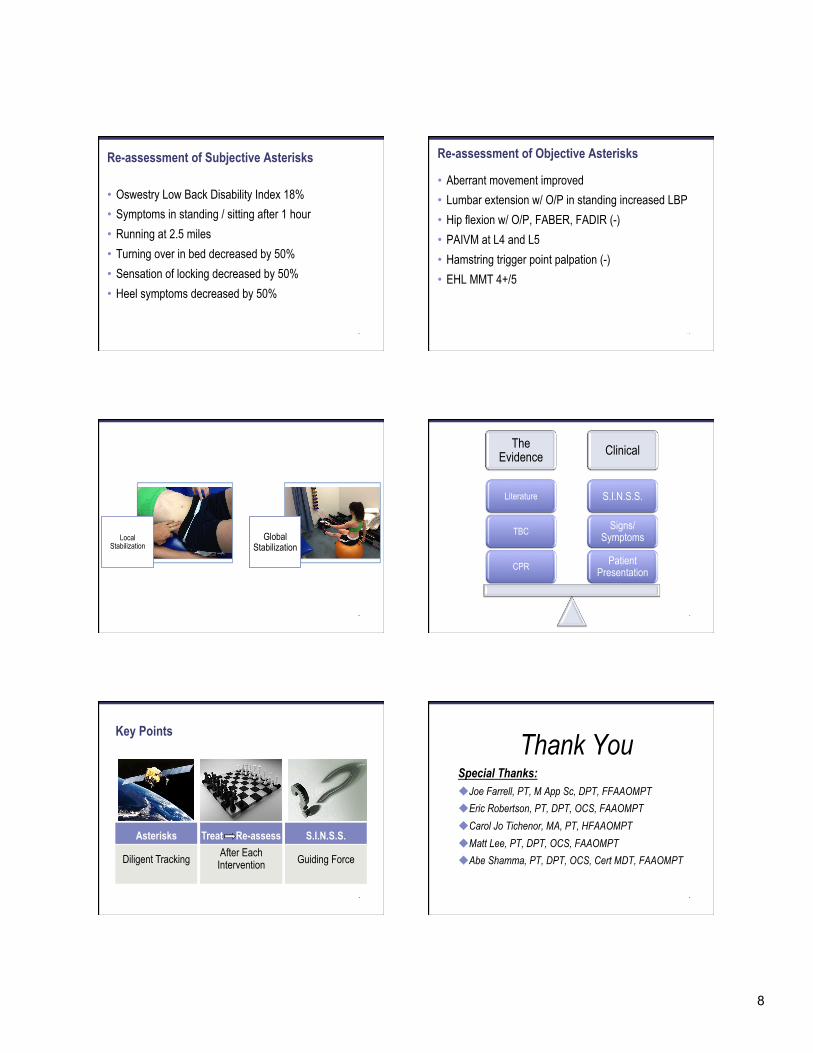
Re-assessment of Subjective Asterisks
• Oswestry Low Back Disability Index 18% • Symptoms in standing / sitting after 1 hour • Running at 2.5 miles • Turning over in bed decreased by 50% • Sensation of locking decreased by 50% • Heel symptoms decreased by 50%
Re-assessment of Objective Asterisks
• Aberrant movement improved • Lumbar extension w/ O/P in standing increased LBP • Hip flexion w/ O/P, FABER, FADIR (-) • PAIVM at L4 and L5 • Hamstring trigger point palpation (-) • EHL MMT 4+/5
Local Stabilization
Global Stabilization
The Evidence Clinical
Patient Presentation
Signs/Symptoms
S.I.N.S.S.
CPR
TBC
Literature
Key Points
Asterisks Treat Re-assess S.I.N.S.S.
Diligent Tracking After Each Intervention Guiding Force
Thank You Special Thanks: u Joe Farrell, PT, M App Sc, DPT, FFAAOMPT u Eric Robertson, PT, DPT, OCS, FAAOMPT u Carol Jo Tichenor, MA, PT, HFAAOMPT u Matt Lee, PT, DPT, OCS, FAAOMPT u Abe Shamma, PT, DPT, OCS, Cert MDT, FAAOMPT

9
References: Aina, S. May, and H. Clare, 'The Centralization Phenomenon of Spinal Symptoms--a Systematic Review', Man Ther, 9 (2004), 134-43. B. Austin, R. B. Souza, J. L. Meyer, and C. M. Powers, 'Identification of Abnormal Hip Motion Associated with Acetabular Labral Pathology', J Orthop Sports Phys Ther, 38 (2008), 558-65. J. M. Beneciuk, M. D. Bishop, J. M. Fritz, M. E. Robinson, N. R. Asal, A. N. Nisenzon, and S. Z. George, 'The Start Back Screening Tool and Individual Psychological Measures: Evaluation of Prognostic Capabilities for Low Back Pain Clinical Outcomes in Outpatient Physical Therapy Settings', Phys Ther, 93 (2013), 321-33. R. M. Burgess, A. Rushton, C. Wright, and C. Daborn, 'The Validity and Accuracy of Clinical Diagnostic Tests Used to Detect Labral Pathology of the Hip: A Systematic Review', Man Ther, 16 (2011), 318-26. M. T. Cibulka, D. M. White, J. Woehrle, M. Harris-Hayes, K. Enseki, T. L. Fagerson, J. Slover, and J. J. Godges, 'Hip Pain and Mobility Deficits--Hip Osteoarthritis: Clinical Practice Guidelines Linked to the International Classification of Functioning, Disability, and Health from the Orthopaedic Section of the American Physical Therapy Association', J Orthop Sports Phys Ther, 39 (2009), A1-25. A. Delitto, S. Z. George, L. R. Van Dillen, J. M. Whitman, G. Sowa, P. Shekelle, T. R. Denninger, J. J. Godges, and Association Orthopaedic Section of the American Physical Therapy, 'Low Back Pain', J Orthop Sports Phys Ther, 42 (2012), A1-57. M. Donaldson, K. Learman, B. O'Halloran, C. Showalter, and C. Cook, 'The Role of Patients' Expectation of Appropriate Initial Manual Therapy Treatment in Outcomes for Patients with Low Back Pain', J Manipulative Physiol Ther, 36 (2013), 276-83. Edwards, M. Jones, J. Carr, A. Braunack-Mayer, and G. M. Jensen, 'Clinical Reasoning Strategies in Physical Therapy', Phys Ther, 84 (2004), 312-30; discussion 31-5. J. D. Fortin, and F. J. Falco, 'The Fortin Finger Test: An Indicator of Sacroiliac Pain', Am J Orthop (Belle Mead NJ), 26 (1997), 477-80. J. M. Fritz, J. A. Cleland, and J. D. Childs, 'Subgrouping Patients with Low Back Pain: Evolution of a Classification Approach to Physical Therapy', J Orthop Sports Phys Ther, 37 (2007), 290-302. G. E. Hicks, J. M. Fritz, A. Delitto, and S. M. McGill, 'Preliminary Development of a Clinical Prediction Rule for Determining Which Patients with Low Back Pain Will Respond to a Stabilization Exercise Program', Arch Phys Med Rehabil, 86 (2005), 1753-62. G. E. Hicks, J. M. Fritz, A. Delitto, and J. Mishock, 'Interrater Reliability of Clinical Examination Measures for Identification of Lumbar Segmental Instability', Arch Phys Med Rehabil, 84 (2003), 1858-64. P. A. Huijbregts, 'Evidence-Based Diagnosis and Treatment of the Painful Sacroiliac Joint', J Man Manip Ther, 16 (2008), 153-4. C. W. MacDonald, J. M. Whitman, J. A. Cleland, M. Smith, and H. L. Hoeksma, 'Clinical Outcomes Following Manual Physical Therapy and Exercise for Hip Osteoarthritis: A Case Series', J Orthop Sports Phys Ther, 36 (2006), 588-99. C. J. Main, and S. Z. George, 'Psychologically Informed Practice for Management of Low Back Pain: Future Directions in Practice and Research', Phys Ther, 91 (2011), 820-4. G. D. Maitland, Elly Hengeveld, Kevin Banks, and Kay English, Maitland's Vertebral Manipulation. 7th edn (Edinburgh ; New York: Elsevier Butterworth-Heinemann, 2005), pp. xvii, 499 p. M. K. Nicholas, and S. Z. George, 'Psychologically Informed Interventions for Low Back Pain: An Update for Physical Therapists', Phys Ther, 91 (2011), 765-76. C. Schwarzer, C. N. Aprill, and N. Bogduk, 'The Sacroiliac Joint in Chronic Low Back Pain', Spine (Phila Pa 1976), 20 (1995), 31-7. L. Skytte, S. May, and P. Petersen, 'Centralization: Its Prognostic Value in Patients with Referred Symptoms and Sciatica', Spine (Phila Pa 1976), 30 (2005), E293-9. K. Smart, and C. Doody, 'The Clinical Reasoning of Pain by Experienced Musculoskeletal Physiotherapists', Man Ther, 12 (2007), 40-9. T. R. Stanton, J. M. Fritz, M. J. Hancock, J. Latimer, C. G. Maher, B. M. Wand, and E. C. Parent, 'Evaluation of a Treatment-Based Classification Algorithm for Low Back Pain: A Cross-Sectional Study', Phys Ther, 91 (2011), 496-509. M. W. Werneke, D. Hart, D. Oliver, T. McGill, D. Grigsby, J. Ward, J. Weinberg, W. Oswald, and G. Cutrone, 'Prevalence of Classification Methods for Patients with Lumbar Impairments Using the Mckenzie Syndromes, Pain Pattern, Manipulation, and Stabilization Clinical Prediction Rules', J Man Manip Ther, 18 (2010), 197-204.