brecher 4 21 15 - roswellpark.org • prognosis - tumor burden. nhl (cont) • therapy -...
TRANSCRIPT
PEDIATRIC MALIGNANCIES
Martin Brecher, MD Roswell Park Cancer Institute
Women & Children’s Hospital of Buffalo !
Oncology for Scientists

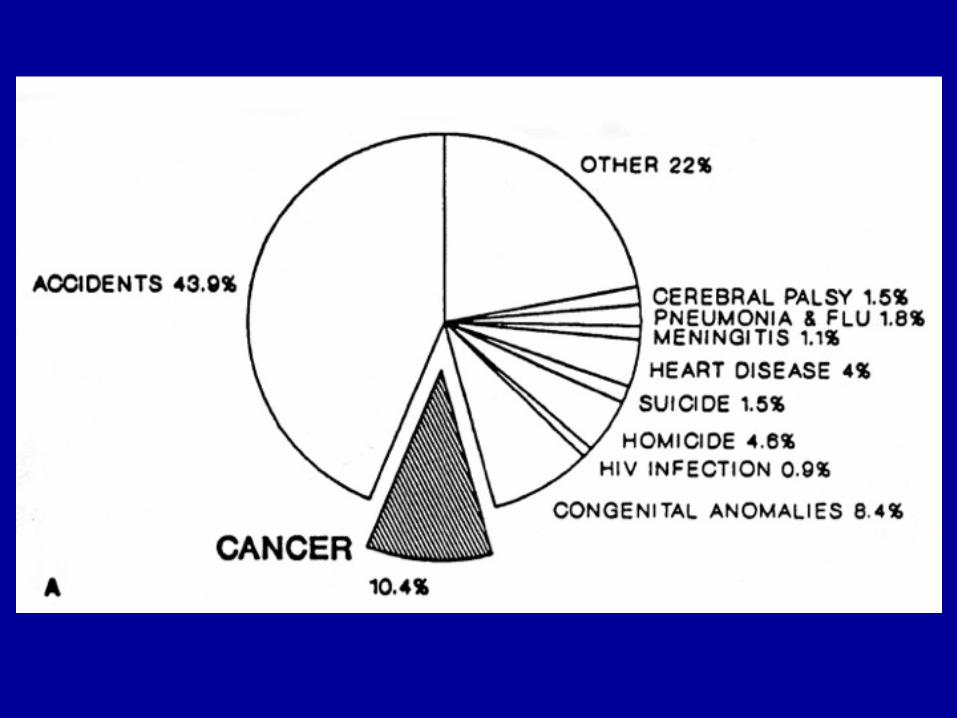
Epidemiology
• 10% of childhood deaths, most common cause of death from disease
• 10-12,000 new cases/yr in US

Etiology
• Unknown • Genetics
– incidence increased with some chromosomal abnormalities
– identical twins - 20% concordance rate for leukemia if < 6 yrs
• Environmental - prenatal vs post natal – radiation – chemical carcinogens – diet - no evidence in children

Etiology (cont)
• Viral Oncogenesis – EBV in Burkitt’s, Hodgkin’s
• Immune deficiency – increase in lymphoid malignancies with
congenital immunodeficiency – cancer in AIDS patients
Signs & Symptoms
• Solid tumors – lump, mass, pain in area of growth
• Leukemia – related to abnormal blood counts – infections/fever - WBC – fatigue, lethargy - anemia – bruising, bleeding - platelets
• Brain tumor – headache, vomiting, neurologic signs

Acute Lymphoblastic Leukemia
• Most common pediatric malignancy • 80% of pediatric leukemias • 1/25,000 • peaks at 3-5 years • boys>girls

ALL (cont)
• Presentation – bleeding/bruising, fever, irritability, bone pain,
adenopathy – high or low WBC, anemia, thrombocytopenia,
elevated LDH, elevated uric acid • Differential diagnosis
– Mono, CMV, ITP, JRA, aplastic anemia, neuroblastoma,

ALL (cont)
• Diagnosis - bone marrow – morphology, histochemistry, flow cytometry,
cytogenetics • LP for CNS disease, prognosis, prophylaxis • Prognosis
– WBC > 50K, age <2 or >10 worse – DI > 1.16 favorable – chromosomes

ALL (cont)
• FAB Classification - L1, L2, L3 • Markers - Tcell, B cell, B-lineage • Treatment based upon risk category -
standard vs high risk • Induction - clear marrow of evidence of
leukemia (CR) – 3 drug - VCR, pred, asp – 4 drug - add anthracycline

ALL (cont)
• Intensification/Consolidation • Maintenance - outpatient • CNS prophylaxis - IT meds vs CSXRT • 80% cure overall
Acute Myelogenous Leukemia
• 500 new cases/yr • No age, sex preference • FAB classification dependent upon lineage • presentation - similar to ALL, DIC,
gingivitis, chloromas • 20% with WBC > 100,000

AML (cont)
• Treatment – induction -Dauno, AraC, 6TG – intensification - HD AraC – Allo BMT vs chemo
• Cure rates - 60-70% sib allo BMT vs 30-40% chemo only

Hodgkins Disease
• Peaks in adolescence, 20’s in US, rare < 5 years
• More common in immunodeficiency • Pathology - 4 types, NS most common • Painless adenopathy -supraclavicular,
cervical • firm, rubbery nodes • 2/3 mediastinal involvement

Hodgkins Disease (cont)
• Spreads via contiguous nodal groups • Lungs, pleura, pericardium • Spleen, liver. marrow • “B” symptoms -fever, weight loss, night
sweats • Stage with CT neck/chest/abdomen,
gallium scan

Hodgkins Disease
• Bone marrow aspirate/biopsy if advanced disease
• Staging laparotomy • Therapy
– traditionally -skeletally mature, local disease - XRT
– advanced disease - chemo -MOPP, ABVD – Trend toward low dose chemo + low dose XRT
in local disease
Non-Hodgkins Lymphoma
• Very different from adults - nearly all high grade
• Small noncleaved (undifferentiated) - Burkitt’s
• Lymphoblastic • Large cell
NHL (cont)• Small non-cleaved - “Burkitt’s”
– endemic vs sporadic – B cell, express surface immunoglobulin, usually IgM – abdominal mass +/- ascites – abdominal pain/swelling – intussception, right iliac fossa mass, confused with
appendicitis – inguinal, iliac adenopathy
• Large cell – usually B cell phenotype – presentation similar to small noncleaved
NHL (cont)
• Lymphoblastic – T cell phenotype – mediastinal mass, pleural effusion – SVC syndrome, dyspnea – cervical adenopathy – abdominal involvement uncommon
• Staging - CT chest/abdomen, bone marrow, LP
• Prognosis - tumor burden

NHL (cont)
• Therapy - Chemotherapy – XRT no benefit – chemo differs, based on cell type – intensive, multiagent – CNS prophylaxis

Brain Tumors
• Most common solid tumor (1200/yr) • Associated with phacomatoses • Presentation dependent upon site of origin,
not histology • Obstructing, increased ICP - classic triad
(morning HA, vomiting w/o nausea, diplopia
Brain Tumors (cont)
• Subacute ICP - poor school performance, fatigue, personality change, HA
• Infants, toddlers - irritable, anorexia, developmental delay, loss of milestones, optic pallor, macrocephaly
• Infratentorial -balance, truncal instability, UE coordination, gait disturbance, CN findings
Brain Tumors (cont)
• Supratentorial - seizure, hemiparesis, hemisensory loss, visual field defect
• Staging - MRI brain, spine for mets, LP for cytology, +/- bone scan, BMA/bx
• Treatment - SURGERY -prognosis better • XRT • Chemo - less of role for many types
– advanced, metastatic – attempt to decrease XRT dose
Wilms Tumor
• Most common malignant renal tumor in children
• 460 cases/yr • Mean age 3-4 yrs • WAGR Syndrome - del 11p13 • Beckwith-Wiedemann

Wilms Tumor (cont)
• Abdominal swelling mass • Abdominal pain, hematuria, fever • Imaging
– US, abdominal CT – MRI for caval patency – CXR for pulmonary mets
Wilms Tumor (cont)
• Surgery upfront -nephrectomy • Chemotherapy - VCR, actino +/- doxo • XRT for advanced stages • 65-90% RFS, overall 80% • 5-7% bilateral
Neuroblastoma
• Most common extracranial solid tumor (525 cases/yr)
• Histology – Small round blue cell tumor – derived from post ganglionic sympathetic
neuroblasts • Arise in any site along sympathetic chain
Neuroblastoma (cont)
• Most primaries - abdomen (adrenal) • Infants - thoracic, cervical • < 5yrs, rare > 10 yrs • Metastasis - lymphatic, hematogenous • Infants more localized vs older children
more metastatic
Neuroblastoma
• Surgery - pivotal role • Chemotherapy - aggressive, multiagent • XRT for advanced stages • High-dose chemo with auto BMT? - delay
recurrence?
Bone Tumors
• 7th largest, 3rd largest group in adolescents
• Osteosarcoma – distal femur, proximal tibia, proximal humerus – metaphysis – RB gene deletion – pain, soft tissue mass
Bone Tumors (cont)
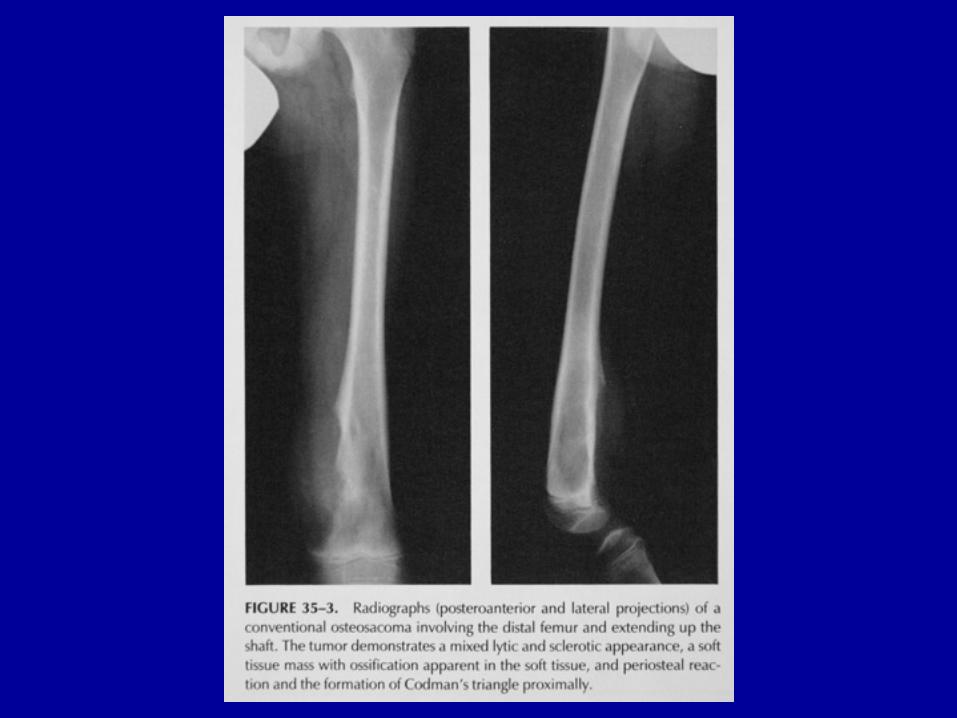
• Osteosarcoma (cont) – 20% metastatic @ dx - lung, bone – “Codman’s triangle” – stage - MRI primary, CT chest, bone scan – Neo-adjuvant chemo - limb-sparing surgery – 80-90% RFS

Bone Tumors (cont)
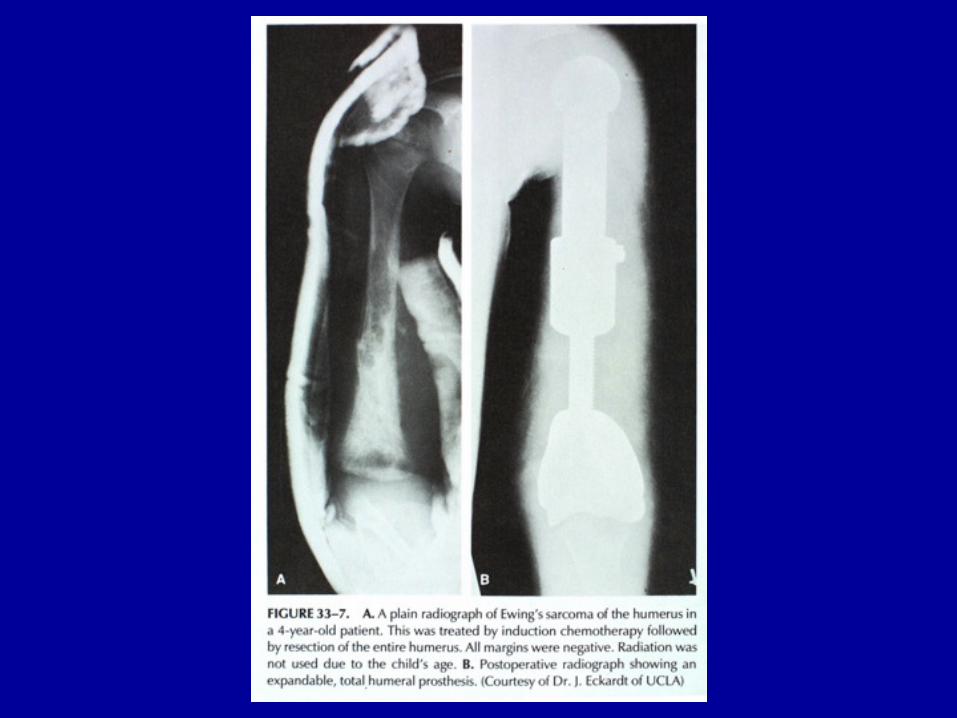
• Ewings Sarcoma – any bone - pelvis, femur, tibia, fibula, scapula,
spine, ribs (axial) – diaphysis – t(11:22) – pain, swelling, fever – mets - lungs, bone, marrow

Bone Tumors
• Ewings Sarcoma (cont) – plain film -”onion skin” – XRT effective – chemotherapy - VAC, doxo, Ifos, VP16
Late Effects
• Increasing survivors of childhood cancer • Growth abnormalities
– direct effect on bones -short stature, scoliosis – hormonal - GH from cranial XRT
• Organ damage - lung, heart, kidney, thyroid – anthracycline - cardiotoxic - late, cumulative – bleomycin -pulmonary
Late Effects (cont)
• Infertility - MOPP, XRT, BMT • Secondary malignancies - XRT, cytoxan
regimens, intensive VP16, BMT