breast cancer update miss b.n. shah consultant surgeon ealing hospital
TRANSCRIPT
Breast Cancer Update
Miss B.N. Shah
Consultant Surgeon
Ealing Hospital
Current Incidence of breast cancer
• Common disease
• 8% risk of development up to 74y
• Varies between countries
• Rare <20y
• 25 per 100,000 from 30-34y
• 200 per 100,000 from 45-50y
• 463 per 100,000 from 70-79y
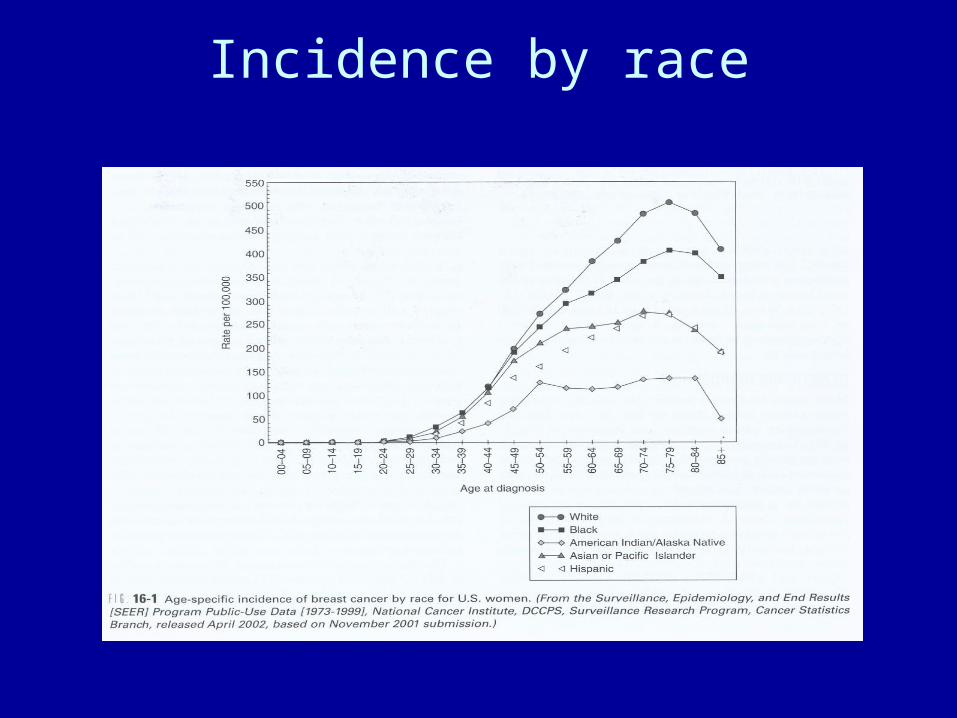
Incidence by race

Bad news
• Commonest cause of death in women aged 40-50y
• Second commonest cause of death from cancer in women overall
• Only 20-50% at most, related to attributable risk

Good news
• Breast cancer mortality has fallen both in the UK and USA for the past decade
• 56% 5 year relative survival (1968-72)
• 70% 5 year relative survival (1988-92)
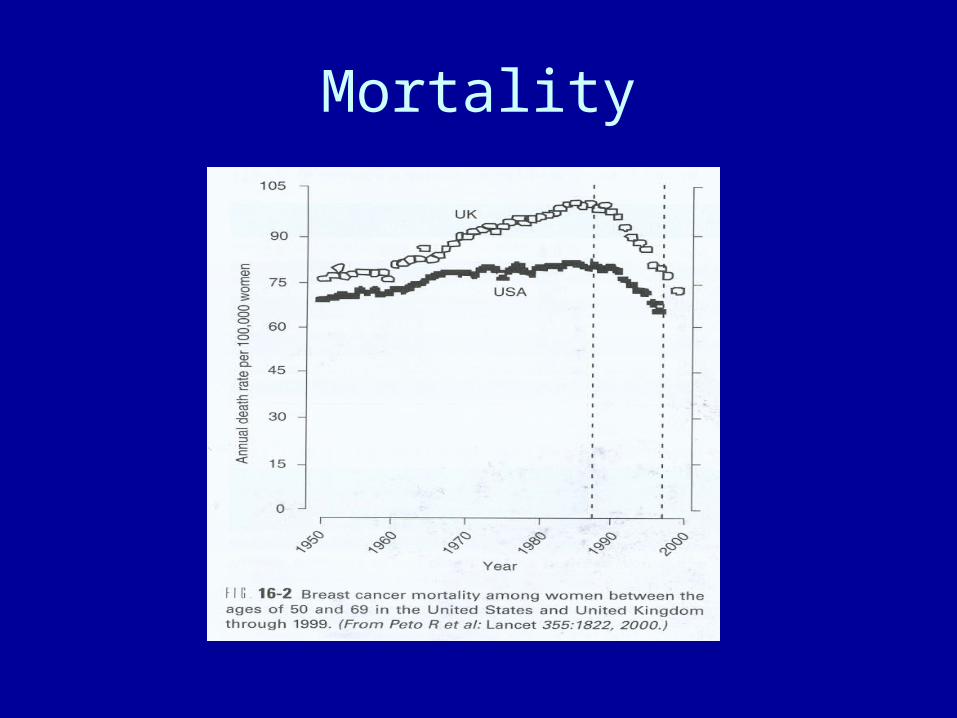
Mortality

anatomy
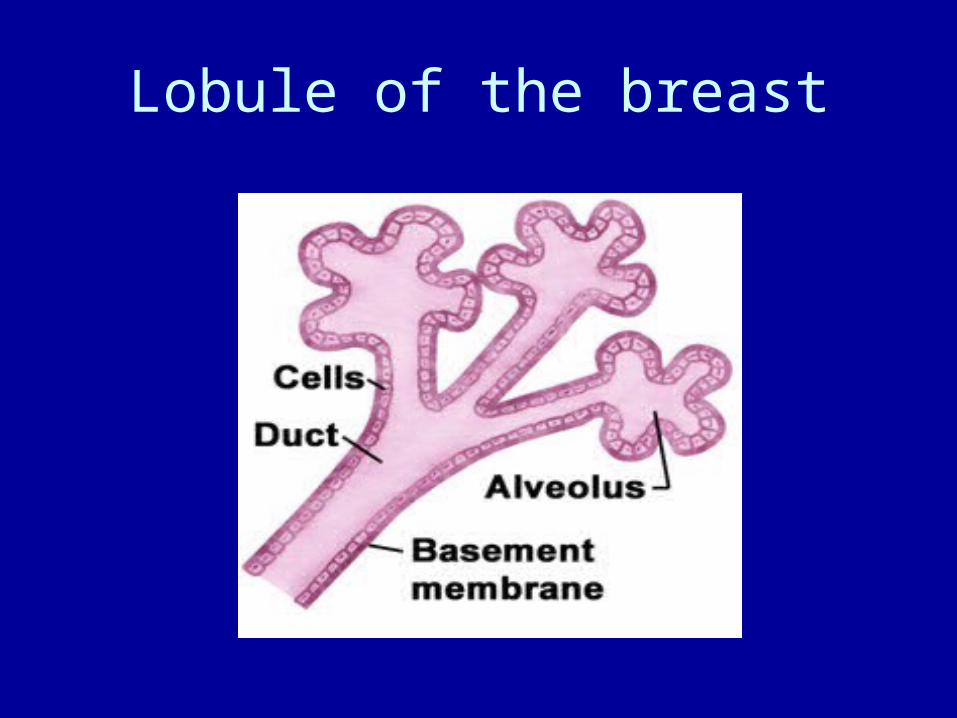
Lobule of the breast

Epidemiology
Influence of oral contraception (1)
• Weakly associated with breast cancer risk
• Single study evaluated effect on women with F.H
• Cohort –showed R.R 3.3 among sisters and daughters of probands
• Risk most evident before and during 1975
Influence of oral contraception (2)
• Population based studies don’t show this effect
• Estimated excess number of cancers between starting use and 10 years after stopping 0.5-5%
• No hard evidence of increased risk of having breast cancer diagnosed 10y or more after stopping

Influence of HRT (1)
• Data more extensive , variable, many confounding issues
• No long term RCT’s
• Collaborative group on Hormonal Factors in Breast Cancer
• Meta-analysis of 90% of world data
• 54,000 women, 33% had used HRT for 5 y or more

Influence of HRT (2)
Two main consistent findings
1. The length of time on HRT was related to extra breast cancers in users
2. This increased risk disappears within 5y of stopping
• Women who use HRT for a short time around the menopause have a very low excess risk

Influence of HRT…..nitty, gritty
Cumulative incidence for women aged 50-70y is 45 per 1,000 in ‘never users’
• 2 per 1,000 extra cancers after 5yrs on HRT
• 6 per 1,000 extra cancers after 10yrs
• 12 per 1,000 extra cancers after 15yrs

HRT…what to do?
• RCTs in UK, Italy, Scandinavia and Canada
• Each patient treated on their own merit
• Apply the principle of ‘ treatment tailored strategies’
Genes and hereditary factors (1)
• Susceptibility genes responsible for only 5-10% of breast cancers
• great strides in characterising genes responsible
• Almost nothing known about various gene interactions +/- environmental factors
Genes and hereditary factors (2)
• 1990 BRCA1 (17q) responsible for 90% of cases with autosomal dominant transmission of breast cancer and ovarian cancer
45% in breast cancer alone
• BRCA2 (13q)

Genes and hereditary factors (3)
Hereditary breast cancer• Onset <45y• excess bilateral cancer• Multiple primary cancer• 80% BRCA1, 20% BRCA2• Ashkenazi 1:100 risk of breast
/ovarian/both• Screening useful

Genes and hereditary factors
Familial breast cancer
• Positive FH
• 1 or more 1st or 2nd degree relatives that do not fit the HBCa category
• Risk ratios increase with the number of affected relatives
• Quantitative risk assessment helpful
• Genetic testing not yet feasible

Genes and hereditary factors (3)
Multiple cancer syndromes• Li-Fraumeni syndrome (p53 mutation)
• Cowden ‘s disease (mutation of PTEN gene)
• Ataxia Telangectasia (11q)
The future
• Rapid progress – clinical and molecular genetics
• find ways to cost DNA testing
• ?legislaton to prohibit discrimination
‘genetic labelling’- employers,insurance companies etc.

GP practice• The Department of Health point out that a GP with a list of 2000 patients is likely to see
only one woman a year who has breast cancer. But they will see a lot more women who have non-cancerous breast conditions such as
• Cysts - sacs of fluid in the breast tissue and most common in the 40-60 year age group
• Fibroadenomas – a collection of fibrous glandular tissue and most common in 20-30 year age group
• Diffuse nodularity – ‘lumpy’ breasts, which are common in all age groups up to the age of 50
• Breast pain – this is not a common symptom of breast cancer
• Although 9 out of 10 breast lumps are not cancer, the Department of Health recommends that any woman over 30 who has a lump in the breast that does not go away should be examined by her GP.
Early referral
• A distinct lump in women under 30
• ‘Lumpy’ breasts that do not go away after a period has finished
• A sore infected area on the breast (abscess)
• Recurrent cysts
• Breast pain that does not go away with reassurance, painkillers prescribed by your GP and wearing a well supporting bra
• Any type of nipple discharge in women over 50
• Any woman under 50 who has a blood stained discharge or a discharge from both nipples that is enough to stain clothing

Guidelines for Urgent Referral
• The symptoms that need urgent referral in 2 weeks for possible cancer of the breast are
• An area skin on the breast that is inflamed and sore (ulcerated)
• Small lumps that appear just under the skin nodules - these are often shiny and red
• Dimpling or distortion of the skin, called peau d'orange
• A rash on a nipple or surrounding area called nipple eczema
• Nipples that have turned in (inverted) within the past 3 months
Imaging
• Ultrasound (U)
• Mammagram (M)
1- normal2 - benign3 - probably benign4 - probably malignant5 - malignant

Cytology
C1 - inadequate sample
C2 - definitely benign
C3 - probably benign
C4 - probably malignant
C5 - malignant

Core Biopsy
B1 - normal
B2 - benign
B3 - probably benign
B4 - probably malignant
B5 - malignant

Management of a lump
L U M P
c lin ica l assessm en tP 1 -5
u ltrasou n dU 1 -5
cyto log yC 1 -5
u n d er 3 5 years

Management of a lump
u n d er 3 5 years
p a tien t ch o ice exc isecosm etica lly
ob serverep ea t T . A .co re b iop sy
b en ig n

Management of a lump
over 3 5 years
c lin ica lp 1 -5
m am m og ramu ltrasou n d
M 1 -5U 1 -5
core b iop syF N A cB 1 -5C 1 -5
lu m p

Management of a lump
over 3 5 years
su rg eryaxilla ry p roced u re
n eoad ju van tch em oth erap yth en su rg ery
? recon s tru c tionp rim aryd e layed
m alig n an tIn trad u c ta l ca rc in om a

Management of a lump
malignantDCIS
surgeryDXT
no clearancesentinel node
primary reconstruction

Lymphatic drainage
Management of the axilla
Clearance Levels,1, 2, 3
Sample
4 nodes
Sentinel node
50:50 divide

Sentinel Node axillary dissection
• Guided localisation
• minimally invasive alternative to traditional
axillary dissection
• Blue dye
• Radioisotope
• <5% false negative
• The future
Screening (U.K.)
• Two view
• Double reading
• 50-65years
• 3 yearly

UK Trial of early detection of breast cancer
• 1999
• 27% decreased breast cancer mortality
• 45 – 60years
• Supports Edinburgh trial (21%)

Anatomy