brain tumor treatment - abnv
TRANSCRIPT

1
TREATMENT OF BRAIN TUMORS
Simon R Platt BVM&S MRCVS Dipl. ACVIM (Neurology) Dipl. ECVN
Professor, Dept. Small Animal Medicine & Surgery College of Veterinary Medicine, University of Georgia
Current Problems in Veterinary Neuro-Oncology Literature
• Case numbers • Owner Finances • Pets >> animals • Stage of disease is often late at presentation • CT guided biopsy • Radiation therapy • Surgical Techniques • Treatment trials flawed by inclusion criteria and measures of
outcome
Classification & Grading Systems
Histologic Classification of Tumors of the Nervous System of Domestic Animals. A Koestner et al; 1999, Armed Forces Inst. Of Pathology, WHO, Washington DC.
Classification based on characteristics of constituent cell type & pathologic behavior
Canine Brain Tumors: Classification
1. Neuroepithelial ¡ Astrocytic ¡ Oligodendroglial ¡ Mixed Gliomas ¡ Ependymal ¡ Choroid-plexus ¡ Neuronal ¡ Embryonal ¡ Unclassified
2. Meningeal • Meningioma • Histiocytic sarcoma • Granular cell tumor
3. Primary CNS Lymphoma
4. Germ-cell
5. Metastatic
Classification & Grading Systems
• WHO Grading = 1 component of criteria to predict response to therapy and outcome
I – Low proliferation potential – surgical cure II – Infiltrative / low proliferation – may recur or progress III – Histological evidence of malignancy – adjuvant therapy required IV – Cytologically malignant / necrosis / mitoses
WHO Grade I II III IV
Astrocyte Pilocytic astrocytoma
(Diffuse) astrocytoma
Anaplastic astrocytoma
GBM
Oligodendroglia Oligodendroglioma
Anaplastic oligo GBM
Mixed Glial
Oligoastrocytoma Anaplastic oligoastrocytoma
GBM
Ependymal Sub-ependymoma
Ependymoma Anaplastic ependymoma
Choroid Plexus CP Papilloma Atypical CPP CP Carcinoma
Meningeal Meningioma Atypical meningioma
Malignant meningioma

2
Canine Brain Tumors
• Canine brain tumors have a similar incidence (14.5/100,000?;2-4.5%) to humans (20.5;2-3%)
• The types and classes of canine brain tumors seen are similar to those seen in humans
• The diagnostic and therapeutic options are also similar but outcome more variable
• Variables shown to influence the outcome include age, neuro status, extent of surgery possible, lesion location, histo type, molecular expression
• Most tumors (1) affect telencephalon [60%] (2) solitary (3) primary (4) affect dogs >7yr (95%: mean age 9.4 yr)
Meningioma
• Most common brain tumor (45-50%) in dogs / median age 10-11 yr / G Ret & Boxer /no sex predilection?
• From arachnoid tissue (caps cells) in multiple
locations - mesenchymal and epithelial composition
• Invariably lack demarcation from normal brain (27%) in dogs and demonstrate necrosis & cystic in 25-30% of dogs
• Falx/convexity/parasellar/cerebellar /brainstem
• Benign (56%) vs. Atypical (43%) vs. Anaplastic (1%) • {Sturges et al; 2008 JVIM;596}
Meningioma • > 90% Vimentin and S100 positive
• Most positive for Neuron specific enolase
• Infrequent GFAP & cytokeratin positive
• 70-100% have progesterone receptors
• All express VEGF, PCNA & Ki-67
• >90% express VEGFR-1&2 & EGFR-1
• Expression relates to grade and prognosis Theon et al; 2000; JAVMA;p701 Adamo et al:2003; AJVR; p1310 Montoliu et al: 2006; J Comp Path; p200 Platt et al: 2006; JVIM; p663 Dickinson et al 2006; Vet Comp Onc;p132 Mandara et al: 2002; J Comp Path; p214 Rossmeisl et al; 2007; AJVR; p1239
Meningioma - Comparative Genomic Hybridization
possible tumor DNA
amplification
possible tumor DNA
deletion
Astrocytomas • 2nd most common brain tumor (17% ) in dogs / mean age 8.6 yr / Border Terrier, Boston terrier, Bulldog & Boxer (21%) /no sex predilection
• Most in cerebrum & diencephalon (8x more likely) / 28% in cerebellum
• Variants of astrocytoma reported include fibrillary, protoplasmic, pilocytic, anaplastic and gemistocytic
• Intratumoral hemorrhage is uncommon

3
Progression of Glial Tumors
Criteria Diffuse Astrocytoma
Anaplastic astrocytoma
Glioblastoma multiforme
Hyper-cellularity
Slight Moderate Moderate
Pleomorphism Slight Moderate Moderate
Mitosis None Present Present
Vascular proliferation
None Present Present
Necrosis None None Present
Astrocytomas • 35% of canine astrocytomas exhibit positive immunolabeling for p53 alteration
• 23% of canine astrocytomas exhibit positive EGFR labeling
• 84% GFAP positive (especially in differentiated areas) – chemical subunit of intracytoplasmic intermediate filaments
Stoica et al; Vet Pathol; 2004;p10 Snyder et al; JVIM: 2006; p 669
Oligodendrogliomas
• Median age 8.1yr • 14% of all primary CNS tumors / 28% of gliomas • >50% border ventricle • Capillaries tend to proliferate • Do not stain vs. all stain with GFAP?? • Ki67 correlates with degree of malignancy
• Vandevelde et al; 1985: Acta Neuropathol p111 • Higgins MA et al; 2007 ACVIM abstracts
Glioblastome Multiforme
• Mean age 8.4 yr • 3% of all primary CNS tumors / 12% of all neuroglial
tumors • Can be de novo or result from progression • Infiltrative and destructive / well vascularized and
necrotic • 5/5 GFAP positive • 6-26% Ki67 expression • 40% VEGF expression / 60% EGFR expression Lipsitz et al: 2003; Vet Path:p659
Secondary Neoplasia
• 50% of all intracranial tumors • Mean age 9.6yr • Most in telencephalon • 29% HSA • 25% pituitary tumors • 12% LSA • 12% metastatic carcinomas
Snyder et al; 2008: JVIM; p172
Canine Brain Tumors: Treatment Options
• Conservative / Palliative • Definitive Therapy 1. Surgical Debulking 2. Chemotherapy 3. Radiotherapy 4. Radiosurgery 5. Gene Therapy 6. Immunotherapy

4
Treatment Options Palliative Care
Corticosteroids -Mean Survival Canine Meningiomas
Ø 75 days (n=13; range 1-405d) Foster ES, et al: JVIM 1988
Canine Astrocytomas Ø 77 days (n=7; range 7-150d)
Foster ES, et al: JVIM 1988
Canine 1’ Brain Tumors Ø 6 days (n=45) Heidner GL, et al: JVIM
1991 Ø 81 days (n=8) Turrel JM, et al: JAVMA
1981 Ø 59 days (n=8) Turrel JM, et al: JAVMA,
1984
Treatment Options Intracranial Surgery
Role of surgery 1. Reduce mass effect 2. Establish a diagnosis 3. Cytoreduction 4. Deliver local treatment
Contraindications 1. Deep locations 2. Poor status 3. Metastasis? 4. Multiple lesions?
Treatment Options Intracranial Surgery
Surgery Alone - Mean Survival Canine Meningiomas Ø 210 days (n=14) Axlund TW, et al: JAVMA 2002
Ø 138 days (n=4; 63-203d) Kostolich M, et al: Vet Surg 1987
Ø 198 days (n=10) Niebauer GW, et al: JAVMA 1991 Ø 1254 days (n=17) Greco JJ et al: JAVMA 2006
Ø Higher median survival if transitional / meningothelial Ø 2104 days (n=39) Klopp & Rao, JVIM 2009
Treatment Options Radiation Therapy
• Deliver tumoricidal dose of radiation while sparing normal brain tissue
• Improvements in treatment planning have resulted in improved local control and a decrease in CNS side-effects • External beam megavoltage most commonly used • Superfractionation / Sensitisation / BNCT / Hyperthermia / Brachytherapy / Radiosurgery
Treatment Options Radiation Therapy
Side-effects in dogs 1. Superficial tissues Ø KCS, otitis, dermatitis, mucositis,
corneal ulcer 1. CNS
Ø Acute – wks to months 10% dogs?
Ø Early Delayed Ø Late Delayed – only 5-20% still
alive Ø risk related to total dose (<48Gy) /
fraction size (<3Gy) / number of fractions / extent of disease / neuro status
Treatment Options Radiation Therapy
Radiation Alone - Mean Survival Canine Primary Brain Tumors Ø 225 days (n=16) Turrel JM, et al:Proc VCS 1986 Ø 345 days (n=14) Evans SM, et al: JVIM 1993 (0rthoV) Ø 322 days (n=4) Turrel JM, et al: JAVMA 1984 Ø 140 days (n= 25) Heidner GL, et al: JVIM 1991 Ø 250 days (n=29) Spugnini EP, et al: Vet Radiol & US 2000 Ø 344 days (n=15) LeCouteur R, et al: Int J Rad Oncol Biol Phys
1988
Canine Extra-axial Masses Ø 370 days (n=35) Brearley, et al:JVIM 1999

5
Treatment Options Radiation Therapy
• Stereotactic radiotherapy • 1+ fractions • MST 399 days for meningioma
Mariani et al. Vet Comp Oncol. 2013 www.csuanimalcancercenter.org
Sx alone
Sx & Rad
Treatment Options Surgery & Radiation
Canine Meningiomas Ø 610 days (n=12) Axlund TW, et al: JAVMA 2002
Ø 1150 days (n=20) Theon A, et al: JAVMA 2000
Ø 441 days (n=6) Brearley MJ, et al: JVIM 1999
Prognosis Associated with: Ø PCNA expression
Ø VEGF expression
Ø Progesterone expression
Treatment Options Chemotherapy
• Nitrosurea Alkylating Agents – Carmustine (BCNU) & Lomustine (CCNU) Meta-analysis of 17 human trials showed increase in survival when used in addition to
RT but only in a sub-population: Young / Good Neuro status / Min Residual disease after surgery
Canine Clinical Trials – 5 astrocytomas CCNU mean survival 218 days Fulton et al, 1990 3 Meningiomas post surgery – median survival 552 days Bilderback et al ACVIM 2006 / 71 dogs with intracranial masses CCNU No survival benefit vs. symptomatic Meervenne et al. J Vet Comp Oncol. 2014
• Platinum-based agents – Carboplatin / Cisplatin
• Temozolamide (Temodar)– Recurrent astrocytomas and in combo with RT for GBM
• Bevacizumab (Avastin)- Anti-VEGF Ab; Recent data suggests limited survival benefit • Procarbazine – Not cross-resistant with Nitrosureas / combined with CCNU and vincristine • Hydroxyurea – 50mg/kg tid PO without side-effects in dogs
• Ribonucleotide reductase inhibitor
Delivery of Local Chemotherapy • Desire to avoid BBB, drug efflux mechanisms and high plasma protein binding
• Carmustine (Gliadel) wafers • Human glioma/GBM • Resection cavity • Gliadel wafer vs. placebo
• MST 13.9mos vs 11.6mos • CSF leak and intracranial
hypertension in Gliadel group • Anecdotal reports in dogs
• Early work on CED, microspheres and nanoparticles to deliver drugs
www.gliadel.com
Westphal et al. Neuro-Oncol. 2003
(i) Convection-Enhanced Delivery (CED)
• Approach developed to overcome BBB • High drug concentrations without toxicity to normal tissue • Distributes a product directly to the brain
• Safe, reliable, targeted, homogeneous method • Relies on bulk flow
• Driven by small hydrostatic pressure differential to distribute molecules within the interstitial spaces of the CNS
• Pressure gradient between infusion site and surrounding tissue
• Long retention and slow dispersion of agents • Agent visualization remains a challenge
• Radio-labeled agent • Co-infusion of MRI contrast agent • Liposomes containing MRI contrast agent
(i) Convection-Enhanced Delivery (CED)
• Several factors influence tissue CED drug distribution • Drug flow rate • Drug volume • Drug viscosity • Size, shape and placement of cannula
• Drug back-flow is major issue and related to catheter size, catheter position in brain and infusion rate
• Reflux prevents continued pressure in the EC space that drives bulk flow away from the catheter
• Systemic toxicity likely due to reflux into CSF
• Real-time imaging ensures treatment volumes are consistent

6
CED in Dogs
• Convection-enhanced delivery • CPT-11 (Irinotectan)
• Topoisomerase 1 inhibitor • Liposome carrier • Reduced tumor volumes in canines
• Correlated to Vd of tumor
• Cetuximab • EGFRvIII antibody • Conjugated to iron oxide in nanoparticles
Dickinson et al. Neuro-Oncol. 2010 Platt et al. Clin Neurosurg. 2012
Cetuximab (C225; Erbitux) § Monoclonal IgG1 antibody § Chimeric (65% human & 35% mouse)
§ Binds EGFR extracellularly ú Competitive inhibition ú Inhibits downstream signals ú Cell cycle arrest in G1 phase
§ NO relation between EGFR expression and response to cetuximab
§ Effects ú Enhances radiosensitivity ú Promotes RT induced apoptosis ú Decreases cell invasion & proliferation ú Reduces angiogenesis ú Inhibits radiation induced damage repair & angiogenesis
Iron Oxide Nanoparticles (IONPS)
§ 10-25 nm § Provide simultaneous imaging and therapeutic efficacy ú Tumor targeting ú Therapy with conjugated drug delivery, and/or hyperthermia
§ Biocompatible § Low toxicity § Evade immune system § Taken up by tumor cells § Decrease cell survival of human GBM cells in vitro
§ Increased survival of mice with CED of IONPs alone
Magnetic IONPs
Iron Oxide Nanoparticles (IONPS) THERMOTHERAPY
• IONPSheatduetoalternatingmagneticfield• Thermoablationofcancertissue• SCCHNinnudemice• SQflankinjection• Tumorcenterincreasedto40°Cwithin5mins• Maintainedfor20mins
Magnetic IONPs
Catheter
Cetuximab-IONPs
100x
A.
C.
B.
IR 0.5 µl/min
Day 0 24 hr
Day 30
IR 0.5 µl/min B.
D.
MRI-guided Cetuximab-IONP CED in the canine brain
IR 0.5 µl/min 24 hour
Coronal Preop w/Gad Axial Preop w/Gad Axial Preop T2 GE
Axial Postop T2 GE
Tumor
Cetuximab-IONPs
Residual Tumor Residual Tumor
Cetuximab-IONPs
Axial Postop w/Gad
7 d Postop 24 h Postop
24 h Postop
Tumor Tumor
Coronal Postop T2

7
(ii) Microsphere Delivered Therapy
• Poly(lactide-co-glycolide) microspheres • PLGA • Slow degradation
• Potential for extended-release therapy
www.controlledreleasesociety.org
PLGA Microspheres • Microparticle drug delivery
• Drugs elute via diffusion or degradation
• PLGA microspheres • Degradation via hydrolysis • Metabolized to CO2 and H2O • Degradation rate varies • γ-irridiation sterilization
Menei et al. Expert Opin Drug Deliv. 2005
PLGA Microspheres- Uses
• Initial studies • BCNU (carmustine) and carboplatin microspheres
• Increased survival rat glioma model • Injection into walls of resected tumor cavity
• For non-resectable, injection at edges of tumor may be superior
• 5-fluorouracil microspheres • Lack of toxicity/improved survival in murine model • >3 weeks drug delivery
Menei et al. Expert Opin Drug Deliv. 2005
UGA Cadaver Study- MRI
Day 1 vs. Day 5

8
UGA Cadaver Study- MRI UGA Safety study- MRI
Day 1 Day 28
UGA Safety study- Histopathology
12 microcylinders, 6.25% Gad
6 microcylinders, blank
6 microcylinders, 6.25% Gad
(iii) Nanoparticle Delivered Drug Therapy
• Platin-M: modified platinum(IV)-prodrug of cisplatin • Crosses blood-brain barrier • Delivered via biocompatible polymeric nanoparticles (NPs) • Targeted to the mitochondrial matrix of hyperpolarized cancerous
cells
OO
OO
OOO
PPh3
PLGA-b-PEG-TPP
nyx
Br-
PtH3N ClClH3N
OO
O
N
O
HN
OPh3P
ONNN
N
O NH
OPPh3
Br-
NN N
Platin-MBr-
Nanoprecipitation +
Size: 51.3±0.8 nm Zeta Potential: 44.0±1.2 mV
Marrache, et al. 2014
MTT Cytotoxicity Assay
• J3TBG Glioma Cells
• SDT3G Glioblastoma Cells
-1 0 1 20
50
100
Log Concentration (µM)
%V
iabili
ty Cisplatin
Platin-M
NT-Platin-M-NP
T-Platin-M-NPs
IC50: >50 µM
IC50: 0.87 µM
IC50: 22 µM
IC50: 12 µM
0 1 20
50
100
150
Log Concentration (µM)
%V
iabili
ty Cisplatin
Platin-M
T-Platin-M-NPs
IC50: 26 µM
IC50: 5.7 µM
IC50: 0.5 µM
MitoStress Assay by Seahorse Assay
• J3TBG Glioma
• SDT3G Glioblastoma
0 20 40 60 80 100-20
02040
100
200
300
400
500
Time (min)
OC
R (p
Mol
es/m
in)
Control Cisplatin Platin-M T-Platin-M-NPs
FCCPOligomycin Antimycin A + Rotenone
0 20 40 60 80 100-20
02040
100200300400500600700
Time (min)
OC
R (p
Mol
es/m
in)
Control Cisplatin Platin-M T-Platin-M-NPs
FCCPOligomycin Antimycin A + Rotenone
9
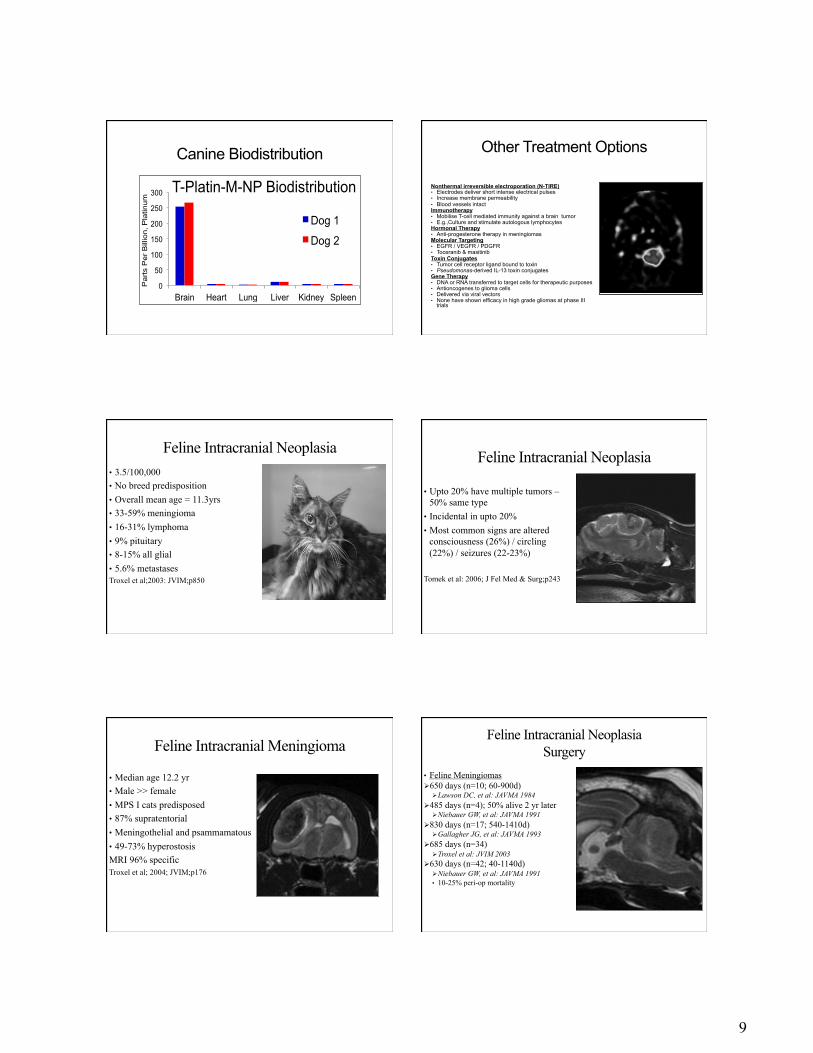
Canine Biodistribution
0
50
100
150
200
250
300
Brain Heart Lung Liver Kidney Spleen
Par
ts P
er B
illio
n, P
latin
um T-Platin-M-NP Biodistribution
Dog 1
Dog 2
Other Treatment Options
Nonthermal irreversible electroporation (N-TIRE) • Electrodes deliver short intense electrical pulses • Increase membrane permeability • Blood vessels intact Immunotherapy • Mobilise T-cell mediated immunity against a brain tumor • E.g.,Culture and stimulate autologous lymphocytes Hormonal Therapy • Anti-progesterone therapy in meningiomas Molecular Targeting • EGFR / VEGFR / PDGFR • Toceranib & masitinib Toxin Conjugates • Tumor cell receptor ligand bound to toxin • Pseudomonas-derived IL-13 toxin conjugates Gene Therapy • DNA or RNA transferred to target cells for therapeutic purposes • Antioncogenes to glioma cells • Delivered via viral vectors • None have shown efficacy in high grade gliomas at phase III
trials
Feline Intracranial Neoplasia • 3.5/100,000 • No breed predisposition • Overall mean age = 11.3yrs • 33-59% meningioma • 16-31% lymphoma • 9% pituitary • 8-15% all glial • 5.6% metastases Troxel et al;2003: JVIM;p850
Feline Intracranial Neoplasia
• Upto 20% have multiple tumors – 50% same type
• Incidental in upto 20% • Most common signs are altered
consciousness (26%) / circling (22%) / seizures (22-23%)
Tomek et al: 2006; J Fel Med & Surg;p243
Feline Intracranial Meningioma
• Median age 12.2 yr • Male >> female • MPS I cats predisposed • 87% supratentorial • Meningothelial and psammamatous • 49-73% hyperostosis MRI 96% specific Troxel et al; 2004; JVIM;p176
Feline Intracranial Neoplasia Surgery
• Feline Meningiomas Ø 650 days (n=10; 60-900d)
Ø Lawson DC, et al: JAVMA 1984 Ø 485 days (n=4); 50% alive 2 yr later
Ø Niebauer GW, et al: JAVMA 1991 Ø 830 days (n=17; 540-1410d)
Ø Gallagher JG, et al: JAVMA 1993 Ø 685 days (n=34)
Ø Troxel et al: JVIM 2003 Ø 630 days (n=42; 40-1140d)
Ø Niebauer GW, et al: JAVMA 1991 • 10-25% peri-op mortality

10
Questions??