brain stimulation potential with intranasal light...
TRANSCRIPT

1
THE POTENTIAL OF INTRANASAL LIGHT THERAPY FOR BRAIN STIMULATION
By Lew Lim, MedicLights Research Inc., Toronto, Canada.
January 2013
Abstract
Available evidence supports intranasal light therapy for brain-related conditions such as mild
cognitive impairment, Parkinson’s Disease, migraine, stroke. However, the present set of
parameters have been based on optimising the results for blood irradiation; which may be
holding back its potential for better neurological outcomes. We analysed the literature to arrive
at reference parameters for optimum brain stimulation with low level light. MedicLights then
developed intranasal light therapy devices based on these parameters, which we then used to
develop case reports with a growing group of subjects for neurological outcomes, which include
those already using legacy intranasal light therapy devices. Studies lead us to select parameters
that involve low level light in the near infrared red (NIR) range that pulses at 10 Hz to draw
superior neural response. More specifically, the parameters could include a wavelength of 810
nm from a LED source, supported by a power density of 10 mW/cm², over daily treatment
session of 25 minutes, and a duty cycle of 50 percent. The LED beam footprint spans the
underside of the brain, including the mid-brain area. With these specifications, the energy is 7.5
J/cm² (net of duty cycle) per session. Users reported improved neurological outcomes, although
the results are more mixed (but without negative effects) from those without prior medical
conditions. The findings suggest that intranasal light therapy is promising as a brain stimulation
method, to be validated with more specific and rigorous clinical studies.
Introduction
Figure 1: Intranasal light therapy in use

2
Available evidence supports intranasal light therapy for brain-related conditions such as
insomnia, mild cognitive impairment, Alzheimer’s Disease, Parkinson’s Disease, schizophrenia,
migraine and stroke. However, the present set of parameters have been based on optimizing
the results for blood irradiation; which may be holding back its potential for better neurological
outcomes. Further analyses of available studies on the effect of photo-neurostimulation and
observations suggest that a new approach would point to a new set of parameters that would
draw greater brain stimulation.
Existing evidence of brain stimulation based on intranasal light therapy
The evidence in this section are selected based specifically on low level light irradiation treatments
through the intranasal (via the nasal cavity) pathway,
Insomnia
In China, intranasal light therapy with low level laser has been used to treat insomnia. Wang et al (2006)
treated 50 patients with insomnia with low level laser at 650 nm, powered with 3 mW for 60 minutes
per each session per day, over 10 – 14 days. They found that the symptoms improved significantly for 82%
of the patients.1
Mild cognitive impairment
Jin L et al (2001) randomly divided 93 patients with cerebral infarction into three groups, 30 in a drugs-
only group (A Group), 32 in intranasal low level laser therapy + drugs group (B Group) and 31 in an
intravascular low energy laser therapy + drugs group (C Group), and then treated B Group with low level
laser at 670 nm and 7 -10 mW for 40 min each time and C Group with He-Ne (632.8 nm) laser at 1.5 mW
for 90 min each time, once daily for ten days. They found a decrease in the peak latency potential of the
P300 waveform, and greater erythrocyte deformity after the treatment in either B or C Groups than A
Group.2
Alzheimer’s disease
Xu C et al (2002) divided the objects into two groups, 47 patients with Alzheimer’s disease (AD) and 22
patients with gastric ulcer, and treated the patients with intranasal low level laser therapy with He-Ne
source at 3.5 - 4.5 mW for 30 minutes each time, which was done once every morning for 30 days. They
found that melatonin, score in mini-mental state exam (MMSE) and score in Wechsler memory scale for
adult (WMS) increased in the AD group, but there was no significant change for the gastric ulcer group.3
Parkinson’s disease
Li Q et al (1998) treated 43 patients with Parkinson’s disease (PD) with intranasal low level He-Ne laser
therapy at 3.5 - 5.5 mW for 30 minutes per treatment session per day for ten days, and found serum

3
cholecystokinin-octapeptide (CCK-8 - which high levels have a deleterious effect on cognitive ability in
PD)4 decreased to normal levels. When referencing to Webster Scale scores (WSS), they found the
improvements to be significant for 26 of the 43 patients. 5
Xu C et al (2003), treated 47 patients with PD with intranasal low level He-Ne laser therapy at 3.5 to 4.5
mW for 30 minutes per session, every morning for 20 days, and found the PD symptoms improved for 31
(66%) of the patients. Out of these, 14 (29.8%) were significant while 27 (57.4%) were mild. Presence of
superoxidase dismutase (SOD) and melatonin increased and malondialdehyde (MDA – a marker for
oxidative stress) decreased. 6
Zhao G et al (2003) treated 36 patients with PD with intranasal low level He-Ne laser therapy at 3.5 - 5.5
mW for 30 minutes per session per day for ten days, and found improvements in PD symptoms for 31
(89.1%) of the patients; out of whom 10 (27.8%) of them were significant and 21 (58.35) mild.7
Schizophrenia
Liao Z et al (2000) randomly divided 80 patients with schizophrenia into two groups, 40 in drugs-only
group (A Group) and 40 in intranasal low level He-Ne laser therapy +drugs group (B Group). The B Group
was treated with energy of 2 mW for 60 minutes per session per day for ten days. They found that
significant improvement was achieved more quickly with the B Group - on the 18th day versus the 26th
day for the A Group.8
Migraine and headaches
Li Q et al (1998) treated 39 patients with chronic headache, migraine and trigeminal neuralgia with
intranasal low level He-Ne laser therapy at 3.5 - 4.5 mW for 30 minutes per session per day over two 5-
day sessions with a 2-day break in between. They found improvements in 35 (89.8%) of the patients, out
of whom 26(66.7%) were significant. The blood β endorphin in the blood of the 35 improved patients
were also found to have increased.9 10
Stroke (cerebral infarction)
Qiao Y et al (2004) treated 68 patients with cerebral infarction with intranasal low level He-Ne laser
therapy at 10 - 15 mW for 60 minutes per session per day over 10 days. The more severe cases had 3
sessions per day. They found improvements in 61 (89.7%) of the cases, out of which 34 (50.0%) were
significant.11
Xiao X et al (2005) treated 21 patients with cerebral infarction by intranasal low level laser therapy with
650 nM wavelength at 3.5 - 4.0 mW energy for 30 minutes. Single photon emission computed
tomography (SPECT) in brain perfusion imaging indicated that the ratio of local regional cerebral blood
flow (rCBF) vs whole brain rCBF and brain blood flow function change rate (BFCR%) increased on the
treated side of the brain, and there was no change in the mirrored regions. 12
Dou Z et al. (2003) treated 50 patients with cerebral infarction or traumatic brain injury with intranasal
low level He-Ne laser therapy group The devices were powered at 2.4 mW for 30 minutes per session

4
over 10 days with a 2-day break in after the first 5 days. Fugl Meyer movement scale and Barthel index
scores were significantly increased and the brain damaged area was reduced.13
Jin L et al. (2001) randomly divided patients with cerebral infarction into a group with 30 patients that
are treated with drugs only and 32 patients in another group that was treated with drugs plus low level
laser intranasal light therapy. The laser used had a wavelength of 670 nm powered with 7 - 10 mW over
40 minutes per session per day over 10 days. The group with the intranasal device saw the peak latency
potential of the P300 waveform decreased at a higher level than the drugs-only group. 14
Section summary
The evidence above have deployed intranasal light therapy have all deployed the relatively
short parts of the visible red to near infrared red spectrum as lasers (mainly from He-Ne gas
source at 632.8 nm or GaInP/AIGaINP source at 670 nm). Yet the results are already efficacious.
The foregoing sections below will examine whether the outcomes can improve with a new set
of parameters, taking advantage of the range of wavelengths available from semi-conductor
based diode sources today.
Legacy and shortcomings
In summary, the present state of the art of intranasal light therapy produces a measure of brain
stimulation/therapy. However, these have been based on the historical intravenous blood
irradiation model invented by Russians and came into commercial use in the 1980s. So far, the
intranasal pathway parameters have evolved out of the parameters used by the legacy
intravenous method, modified to penetrate the cutaneous layers to reach the blood capillaries.
With a new approach that focuses on brain irradiation as opposed to blood irradiation, we can
arrive at a new set of parameters that could could improve efficacy, which is the subject of
discussion in this paper. Although the studies cited above were based on low level laser, it is
now widely accepted that non-laser light emitting diodes (LEDs) should draw the similar cellular
response and outcomes, offering us the option of the less regulated LEDs.15
Other light-based brain stimulation pathways as predicates
Other brain stimulation pathways that deploy light for brain stimulation are optogenetics, ear
canal light therapy, and transcranial light therapy. Optogenetics are solely experimented on
animals (laboratory mice and rats), using light to react with photosensitizers; and ear canal light
therapy involves the deployment of bright light to address seasonal affective disorder (SAD) or
winter depression. Transcranial light therapy is the closest predicate for intranasal light therapy.

5
Transcranial light therapy (TLT)
Transcranial light therapy (TLT) is enjoying more attention in recent years due to the increasing
understanding of the underlying mechanism of action, successful outcomes, lack of side-effects
and being non-invasive. This method involves directing light to the brain from the outside of the
skull. The source of light can be light emitting diodes (LED) or low level laser, usually in the red
or near infrared-red (NIR) sections of the spectrum. The NIR band would be the choice to
provide deeper penetration through the meninges, cranial material and then through the brain
matter in order to reach the deeper parts of the brain. Recent research supports TLT’s potential
for treating stroke, traumatic brain injury, Parkinson’s disease, mild cognitive impairment,
Alzheimer’s disease, depression, and some other cognitive issues.16 The TLT pathway should be
superior to the alternatives, even the intranasal pathway, for traumatic injuries at specific
locations at the top side of the brain.
The TLT devices are available commercially. See Figure 2 below.
Figure 2: Transcranial light therapy (source: http://topnews.us/content/237119-transcranial-light-therapy-
may-help-tbi-patients)
The intranasal pathway as a solution
In the past, the challenge of intranasal light therapy was to make the applicator small enough to fit comfortably and safely within the restricted size of the nostril. All things being equal, this pathway shares many advantages of the transcranial method because they irradiate the brain in similar ways. Furthermore the light source in intranasal light therapy is located closer to the all-important mid-brain area where much of the autonomic functions lie, with little barrier in between the light source and the target.
The issue now shifts to selecting the specifications that can achieve the most desired outcomes. Clinical studies show that there is no one universal set of parameters for all indications, although it is widely accepted that the red to near infrared-red section of the electromagnetic spectrum stimulates cellular activities in general. It is now a question of being specific about the specific parameters.

6
Summary of device specifications proposed for brain stimulation
In summary, based on relevant literature and ensuing discussions, the choice for balanced and effective set of parameters are:
Landed beam footprint: Whole underside of the brain Light source: Semiconductor light emitting diode (LED) Wavelength: 810 nm (near infrared red or “NIR”) Energy output: 10 mW/cm² Pulse mode: 10 Hz at 50% duty cycle Exposure time: 25 minutes
The bases for these parameters are expounded below.
Potential Impact of Intranasal Irradiation
Key Targeted Areas
Specific parts of the brain govern specific functions of the mind and body. Since every part is important, a beam with a footprint that spans the whole brain would be most beneficial. The most efficient way to achieve this with a single light point source would be through the nasal cavity. To achieve the same landed dosage, other methods of delivering the photons to the brain would need to come from a large area source, or be invasive or have enough energy to penetrate thicker layers of dense materials. When compared to alternative methods of irradiating the brain from the outside of the cranium, the intranasal method has a distinct advantage: the concave shape of the underside of the brain envelopes the convex shape of the light beam coming off a single light source in the nasal cavity.
The diencephalon (in the mid-brain area) is the seat of some of the most essential autonomic and survival functions, and holds some keys to the physical well-being of the person. This is a hard-to-reach region for light to access from outside the skull but is more easily reached from the nasal cavity, especially with longer wavelengths (that are closer to the infrared red spectrum). The hypothalamus located in this area, is the control center for many auto-regulatory functions. It is connected with structures of the endocrine systems to support its vital role in maintaining homeostasis throughout the body. It is also part of the limbic system that influences various emotional and pleasure responses, storing long-term memories, regulating hormones, sensory perception, motor function, and olfaction. The other components of the limbic system are the amygdala, cingulate gyrus, hippocampus, olfactory cortex and the thalamus.

7
Longer wavelengths may also reach deeper underlying areas such as the substantia nigra (its dysfunction leads to Parkinson’s disease) which is located at the bottom of the mid-brain area. In addition, the prefrontal cortex in a separate location, could be targeted to improve higher order cognitive functions.
The anatomical advantages of intranasal irradiation
A light source that is inserted into the nasal cavity will be in close proximity (about 3 inches of mainly air and soft tissue) to the mid-brain area. See Figure 3.
When the light source 1 in this position is pointed as shown, it requires little energy for effective irradiation because much of the physical pathway to the brain is air. 2. For the purpose of illustration, the mid-brain areas highlighted are the amygdala 3, hippocampus 4, hypothalamus 5, septal area 6 and the cingulated cortex 7. The portion of the neo-cortex that is easily illuminated by the light source is the prefrontal cortex 8.
The brain is encased by a bony skull. Other than the area of the brain stem 9 which connects the spinal cord to the brain, the thinnest part of the protective skull is the thin perpendicular plate of the ethmoid bone 10.
As testament to its low barrier to the brain, it is also the part of the skull that is broken during the ancient Egyptian mummification process to drain out brain matter. Surgery involving the
Figure 3: Irradiation with intranasal light
source
1
10 2
8
7
6
5 4
3
9

8
mid-brain area, say the pituitary gland, is accessed through the nasal cavity – an example of the accessibility of this area. There is some tissue material as part of the nasal septum wall in the pathway leading to the mid-brain region, but is of low density.
Having little tissue between the light source and the targeted areas matters because red and infrared red penetration as covered by Beer-Lambert law, suffer optical power decay of up to 80% at 1 mm from the surface.17 Yet we want to maintain low energy intensity to avoid mitochondrial damage.
Based on 810 nm low level laser irradiation done transcranially on mice, Ando T et al measured the average penetrative power, which showed that only 15% of the of the laser power was transmitted through the skin and 6% of that penetrated through a combination of skin and skull, despite the relatively better penetrative quality of this wavelength.18 The intranasal pathway only has the much thinner perpendicular plate of the ethmoid bone between the brain and the light, hence allowing more light penetration into the brain, all else being equal.
The engineering advantages of intranasal irradiation
The above anatomical advantages now allow for a system that contains a low energy, single diode for the light source. With a light source carrying the correct parameters pointing in the right direction, it would be a potent and efficient brain stimulation modality.
Scientific bases and evidence for use in neurostimulation
Recent relevant research evidence based on transcranial modality
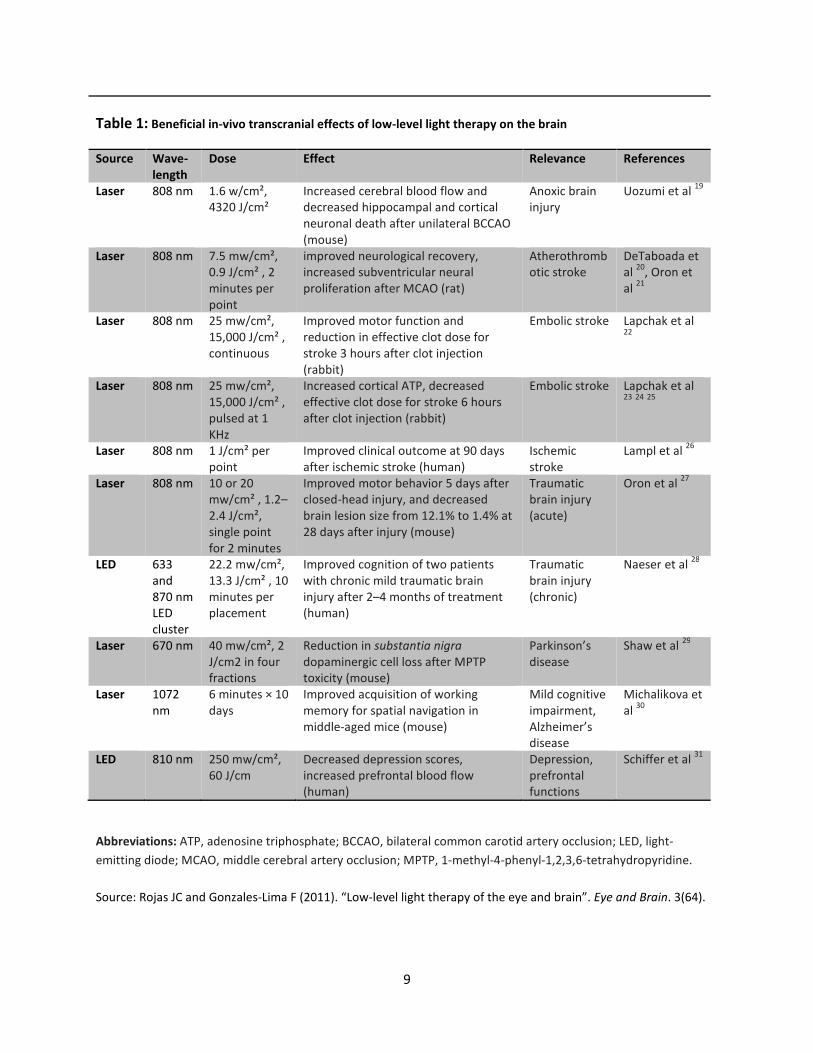
A summary of recent research into the beneficial in-vivo transcranial effects of low-level light therapy on the brain is shown in Table 1 below. In animal studies, the technology has been found to be promising for treating anoxic brain injury, atherothrombotic stroke, embolic stroke, Parkinson’s disease, mild cognitive impairment and Alzheimer’s disease. In human studies, it has been found to be promising for healing the damages of ischemic stroke, traumatic brain injury, depression and dysfunctions of the prefrontal cortex.
The potential for addressing more outcomes may be revealed with more future research on selected indications. For the time being, an understanding of the mechanism of action could reveal the potential for the technology.
9
Table 1: Beneficial in-vivo transcranial effects of low-level light therapy on the brain
Source Wave-
length
Dose Effect Relevance References
Laser 808 nm 1.6 w/cm², 4320 J/cm²
Increased cerebral blood flow and decreased hippocampal and cortical neuronal death after unilateral BCCAO (mouse)
Anoxic brain injury
Uozumi et al 19
Laser 808 nm 7.5 mw/cm², 0.9 J/cm² , 2 minutes per point
improved neurological recovery, increased subventricular neural proliferation after MCAO (rat)
Atherothrombotic stroke
DeTaboada et al
20, Oron et
al 21
Laser 808 nm 25 mw/cm², 15,000 J/cm² , continuous
Improved motor function and reduction in effective clot dose for stroke 3 hours after clot injection (rabbit)
Embolic stroke Lapchak et al 22
Laser 808 nm 25 mw/cm², 15,000 J/cm² , pulsed at 1 KHz
Increased cortical ATP, decreased effective clot dose for stroke 6 hours after clot injection (rabbit)
Embolic stroke Lapchak et al 23
24
25
Laser 808 nm 1 J/cm² per point
Improved clinical outcome at 90 days after ischemic stroke (human)
Ischemic stroke
Lampl et al 26
Laser 808 nm 10 or 20 mw/cm² , 1.2–2.4 J/cm², single point for 2 minutes
Improved motor behavior 5 days after closed-head injury, and decreased brain lesion size from 12.1% to 1.4% at 28 days after injury (mouse)
Traumatic brain injury (acute)
Oron et al 27
LED 633 and 870 nm LED cluster
22.2 mw/cm², 13.3 J/cm² , 10 minutes per placement
Improved cognition of two patients with chronic mild traumatic brain injury after 2–4 months of treatment (human)
Traumatic brain injury (chronic)
Naeser et al 28
Laser 670 nm 40 mw/cm², 2 J/cm2 in four fractions
Reduction in substantia nigra dopaminergic cell loss after MPTP toxicity (mouse)
Parkinson’s disease
Shaw et al 29
Laser 1072 nm
6 minutes × 10 days
Improved acquisition of working memory for spatial navigation in middle-aged mice (mouse)
Mild cognitive impairment, Alzheimer’s disease
Michalikova et al
30
LED 810 nm 250 mw/cm², 60 J/cm
Decreased depression scores, increased prefrontal blood flow (human)
Depression, prefrontal functions
Schiffer et al 31
Abbreviations: ATP, adenosine triphosphate; BCCAO, bilateral common carotid artery occlusion; LED, light-
emitting diode; MCAO, middle cerebral artery occlusion; MPTP, 1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine.
Source: Rojas JC and Gonzales-Lima F (2011). “Low-level light therapy of the eye and brain”. Eye and Brain. 3(64).

10
Mechanism of action and its far-reaching impact
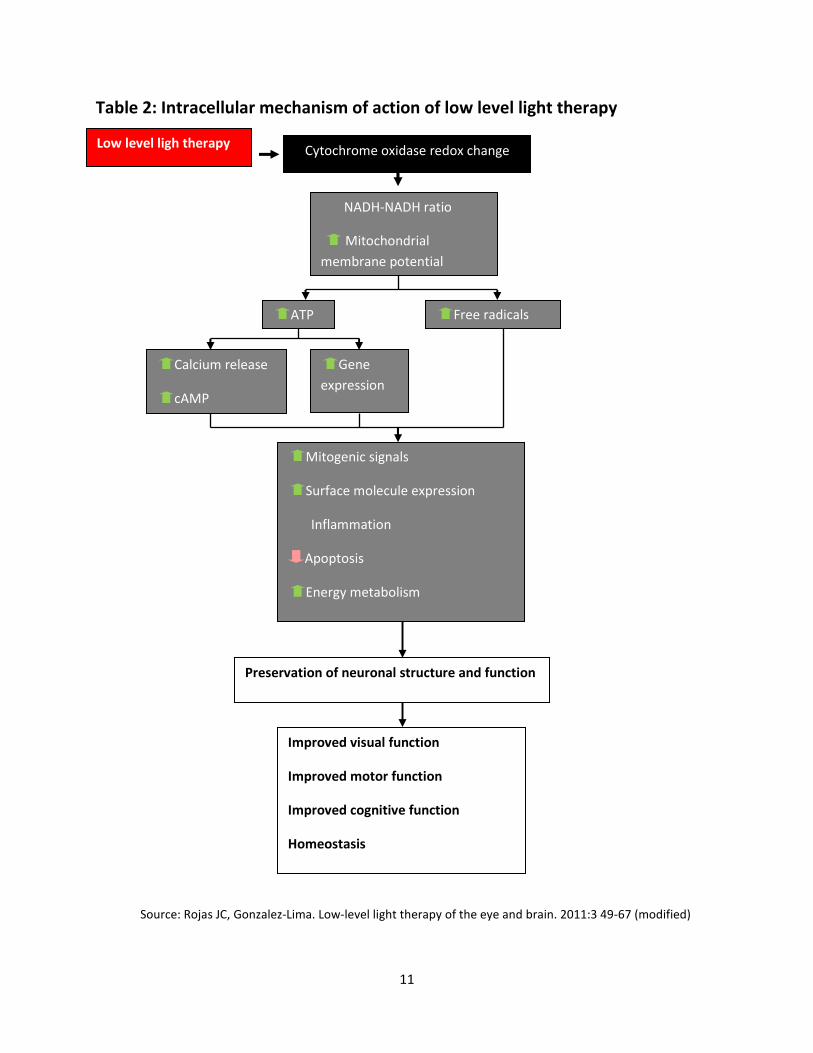
The intracellular mechanism of low level light therapy is illustrated by Table 2 below. The key to the response of the brain lies in the presence of a photoacceptor respiratory enzyme in all cellular mitochondria called cytochrome oxidase. It represents the best known intraneural marker of metabolic activity and is tightly coupled with free radical metabolism, cell death pathway and glutamatergic neurotransmitter activation, important for learning and memory. 32
When light with these wavelengths at low energy hit the cells (including nerve cells), it modulates the cells into metabolism (photobiomodulation) by regulating mitochondrial function, intraneuronal signaling systems, and redox states. The process also increases nitric oxide and cerebral blood flow,33 helping with the perfusion of oxygen and nutrients to the brain. This is assisted by the known vasodilitative quality of nitric oxide,
With the brain affecting virtually all functions of the body, the impact of exposing neurons to light (photoneurobiomodulation) could consequently affect the entire well-being of the human being.
The sensitivity of cytochrome oxidase to red and near infrared red light can be explained by the role of a chromophore in the protein structure. This chromophore is an organic cofactor that is present in all photoreceptors, such as the those in the eyes that give us the perception of colors. The chromophore absorbs particular wavelengths and rejects the others, and those in the cytochrome accept red and infrared red light.
These facts express the potential impact of light that could be correctly directed to the various parts of the brain, resulting in both therapy for, and prophylaxis against nervous disorders. At low energy levels, the therapeutic effects are not accompanied with any major side effect. Experiments show that photoneurobiomodulation of electrical activity in neurons can also be achieved independently of thermal effects.34
11
Table 2: Intracellular mechanism of action of low level light therapy
Low level ligh therapy
Source: Rojas JC, Gonzalez-Lima. Low-level light therapy of the eye and brain. 2011:3 49-67 (modified)
Improved visual function
Improved motor function
Improved cognitive function
Homeostasis
Preservation of neuronal structure and function
Mitogenic signals
Surface molecule expression
Inflammation
Apoptosis
Energy metabolism
Gene
expression
Calcium release
cAMP
Free radicals ATP
NADH-NADH ratio
Mitochondrial
membrane potential
Cytochrome oxidase redox change
12
Photoacceptors in the nervous system
Although earlier animal experiments reveal the presence of photoacceptors in the brain, it was experiments in year 2000 that demonstrated that isolated mitochondria are sensitive to irradiation with monochromatic light in the red and near infrared red spectrum. For example, illumination of isolated rat liver mitochondria with red low-powered lasers increased ATP synthesis and oxygen consumption.35
It has been demonstrated that impaired mitochondrial oxidative metabolism is associated with neurodegeneration.36 Rat neuronal cultures exposed to low level red light showed increases in cytochrome oxidase activity.37 Therefore an intervention that is aimed at improving mitochondrial metabolism is hypothesised to benefit the functions of both the diseased and normal brain. It is also clinically tested to be able to relieve pain in humans.38
The effects of the light irradiation on the brain are observed in a wavelength-specific range. The data also suggest that the primary photoacceptor mediating the effects of the light is not only localized to the mitochondria; the molecules that absorb the light in cells are probably part of the respiratory chain.39
Cellular equilibrium and homeostasis
There is a point when the photoacceptors such as cytochrome oxidase do not respond to further photostimulation: when the cytochrome oxidase is fully reduced or fully oxidized. It responds only when it is in its intermediate stage.40 Therefore further sequential low power irradiation will not yield further metabolic activity from these photoacceptors. This indicates that cells in the body have coded action potential when they are ex-homeostasis, responding positively to light irradiation until they reach homeostasis.
Potential Indications
Based on the scientific evidence (outside the earlier mentioned studies based specifically on intranasal light therapy), there are many potential indications that can be derived from the irradiation of the brain. Improvements in conditions of stroke and neurotrauma, Parkinson’s disease, cognition and emotional states are direct responses to the irradiation (as opposed to the indirectly through say, the circulatory system in the legacy hypothesis). The human and animal studies that are related to these outcomes are well documented.41
Some specific indications that are already tested in related studies are discussed below.
Stroke and neurotrauma – protection and therapy

13
Investigations into brain irradiation (photoneurobiomodulation) has extensively covered stroke and neurotrauma. Recent studies by Uozemi et al demonstrated that low energy light delivered transcranially was able to increase blood flow by 30%.42 That would help prevent ischemic strokes. The outcomes have also been accompanied with significant increases in nitric oxide production; mentiond as a “dilatative quality” earlier, this mechanism is associated with the relaxation of vascular walls to achieve improved blood circulation. In the study, the cerebral blood flow increased in both treated and untreated hemispheres. Also, subjects pretreated with irradiation showed improved blood flow during the period of occlusion, with stable body temperature, heart rate and respiratory rates. Application of photoneurobiomodulation during a stroke event also includes significant decrease in apoptotic cells.
Regular irradiation with low level near infrared red (NIR) light has also been found to be associated with significant neurological recovery after stroke events.43 Furthermore, these effects were associated with increased neuronal proliferation and migration in the subventricular zone, which may be a key factor in recovery from stroke.44
The studies on the effect of NIR on human stroke patients will continue to grow,45 and with the evidence available, we also understand better how light irradiation therapy on the brain may affect other conditions.
Traumatic brain injury
Studies have provided in vivo evidence that the effects of low level red to NIR light irradiation on cytochrome oxidase and nitric oxide play a major role in the neuroprotective action of light irradiation therapy; not just for ischemia, but also traumatic brain injury.46
Parkinson’s disease
In a study with small animals like mice, it was found that low level light irradiation at 670 nm wavelength, helps prevent the loss of dopaminergic cells in the substantia nigra,47 features that would translate into improving the conditions of patients with Parkinson’s disease. Longer wavelengths like NIR should be more feasible for the much larger human being.
Memory and learning deficits
It has also been found that irradiation of the prefrontal cortex with near infrared red light of 1072 nm wavelength, also improves working memory.48 As this condition is common among the more elderly, using a relevant light irradiation method to irradiate the prefrontal cortex will help with an aging-related problem of working memory deficits.
Furthermore, the therapy may stimulate a reversal in learning and memory deficits because of indications that it could proliferate neural progenitor cells in the subventricular zone.49 These cells and are known to migrate to the olfactory bulb and then to the hippocampus, an area that supports memory and learning, and then mature into interneurons.50
14
Dementia and Alzheimer’s disease
The issue of memory deficits extends to the discussion on dementia and Alzheimer’s disease (AD).
Neurodegeneration can lead to cognitive impairment that is often identified with dementia. Improved blood flow with this modality demonstrates the potential for addressing vascular dementia. In a recent study on laboratory mice, Rojas et al found that when the prefrontal cortex was exposed to low level red light of 650 nm wavelength, the rate of oxygen consumption would increase. 51
AD, although a form of dementia, has various causes, though full knowledge is still lacking. The early signs of this neurodegenerative condition is revealed in the form of regional brain metabolic deficits in the form of reduced cytochrome oxidase activity – which is a sign for potential risks for Alzheimer’s disease.52 It is established that the red and infrared red lights activate cytochrome oxidase makes intranasal light therapy a potentially good candidate to help manage the onset of a full Alzheimer’s disease.
Depression and emotional deficits
Phenotypic expressions of mood disorders such as depression and post-traumatic stress disorder (PTSD) have been shown to be associated with decreased metabolic capacity in the prefrontal cortex region.53 Electrical stimulation of the prefrontal cortex has antidepressant effects .54 Irradiation of the same area with red and near infrared red light is expected to have at least similar outcomes, as well as the potential for being neuroprotective of these conditions. A pilot study showed that when the foreheads of patients with major depression and anxiety are irradiated with low level light with 810 nm wavelength, the blood flow to the frontal cortex increased and induced a 63% reduction in depression scores.55
Post-traumatic stress disorder (PTSD) and panic disorder
PTSD and panic disorders have been associated with the fear memories often triggered by stimuli identified with certain bad experience. These memories are embedded in the hippocampus. A singular neurostimulation of the hippocampus may recall the fear memories. Animal experiments combining a light source with a photosensitizer in the hippocampus (optogenetics) show that this is possible.56 There is no photosensitizer involved with normal intranasal light therapy, so the potential of this modality causing fear memory recall is much smaller.
Stimulating the prefrontal cortex (where the executive functions lie) (position 8 of Figure 3) with low level light therapy can help balance out fear memory recall from the hippocampus - the main trait of PTSD. Rojas et al hypothesized that PTSD can be overcome when combining training for extinction of fear memories with low level light illumination of the prefrontal cortex. This is due to the increased metabolic activity of that of that area of the brain.57

15
Discussion
The science and evidence supports the hypothesis that the intranasal pathway would be efficacious for brain stimulation/therapy. The potential of its apparent ability to activate neurogenesis, and to achieve cellular homeostasis could form the bases of new studies that may uncover new indications. There are neural conditions yet unexplored, such as epilepsy, migraine, chronic fatigue syndrome, encephalitis, multiple sclerosis, anxiety disorder, attention deficit disorder, schizophrenia, and learning disability.
Bases for System Specifications / Dosimetry
The relevant specifications that govern a light therapy modality include the wavelength, coherency, energy (in Joules (J)), Power (in Watts (W) or milliwatts (mw)), Irradiance (W/cm²), Radiant exposure or Dosage (J/cm²), Exposure time (seconds), Wave type/mode (continuous vs pulsed), Fraction protocol (number of component sessions), Aperture/Footprint (area of landed beam), and Delivery distance.
Determination of therapeutic wavelengths
The wavelengths shown to be most effective at inducing in vivo beneficial effects in cells that do not have specialized photopigments, have been in the optical window of the red and infrared red (NIR) range of the spectrum, between 600 – 1100 nm. Successful experiments with brain irradiation have mainly been carried out at 633-670 nm (visible red) or 808 - 1072 nm (NIR) in both animals and humans. This matches the luminous range of energy that excite susceptible intracellular molecules,58 which affects cellular metabolism.
It is also a fact that the longer the wavelength, the deeper the travel/penetration into the tissues, and the lower the energy required. Researchers recognise that it is this range of wavelengths that draw the greatest mitochondrial response as opposed to the need to have this wavelength merely for tissue penetration. Nevertheless, when tested on rats, photons between 630 nm and 800 nm have been shown to penetrate up to 28 mm even in layers of tissues with relatively low transparencies such as skin, connective tissue, muscle, bone, and spinal cord (even though much is already dissipated after the initial 1 mm) with about 6% of the total energy density being detectable at the ventral surface.59 Deeper tissue penetration obviously offers a better headstart, and hence the longer NIR should be considered for use.
The depth of light travelling through tissues depends not only on the wavelength but also on the optical properties of the target tissue. The work of Abdo A et al suggests that the maximal penetration of light in the gray and white matter of the brain occurs at wavelengths at the NIR spectrum.60

16
In this respect, in neural tissues, cytochrome oxidase is the most abundant metallaprotein; its wavelength peaks in its absorption spectrum (670 nm and 830 nm) highly correlate with its peaks in its catalytic activity and with ATP in vitro.61
Another important protein that is a photoacceptor for red and near infrared red light is the flavoprotein, reduced nicotinamide adenine dinucleotide (NADH)-dehydrogenase.62 Enzymes involved in NADH are found to be attractive targets for drug discovery against a variety of human diseases, including cancer, multiple sclerosis, neurodegeneration and Huntingdon’s disease.63
It is also in our favour to select a single monochromatic wavelength for a single application. Based on the work of Karu et al, ideal wavelengths could be around 670 nm (visible red) or 830 nm (near infrared red). It has been found that simultaneous dichromatic irradiation changes the ratio of the reduced and oxidized form of the enzyme; suggesting that one should select pure monochromatic wavelength light source for every application.64 This fits with the intranasal modality which works best with just one monochromatic light source.
Selection of the shorter wavelength of 670 nm or thereabout would require greater energy intensity to achieve longer travel through the tissues. The mitochondria and their composites are sensitive and their response to light take on a biphasic or U-shaped response; meaning that whilst low intensity would be therapeutic, high intensity would be inhibitive.65 When tested with mice, a dose of 10.9 J/cm² induced a significant 13.6% increase in mean cytochrome oxidase activity, whereas just an increase to 32.9J/cm² show no significant difference with the control group,66 This suggest that we should seek the lowest energy intensity as possible that can draw a therapeutic response (which is counter intuitive to many people).
Literature have suggested that the ideal wavelength is 830 nm for photoneurobiostimulation. However, most studies with successful outcomes have been done with 808nm and 810 nm (see Table 1), which are close enough to 830 nm for practical purposes. The choice of 810 nm one based on the large body research documented. The faint visibility at this slightly shorter wavelength is also a practical check to let the user know that the light diode is working.
Coherent vs non-coherent (or laser vs LED)
Lasers feature coherent electromagnetic radiation that is unidirectional, hence allowing more concentrated energy. Where deeper penetration is required, given the same parameters of wavelength, energy dosage and intensity, the lasers may perform better than LEDs. Once the photons land on the cell photoacceptors, it would not make any difference whether they are coherent because it is the frequency that matters. 67 However, for most therapeutic applications this coherency is not required, and where greater tissue penetration is asked for, it is better met with a longer wavelength. LED beams have the other feature of giving a larger landed footprint.

17
The non-coherency of the LED light creates negligible amount of heat. This allows brain tissue longer exposure to “therapeutic” wavelengths at relatively low power intensity while allowing modulation of neural metabolism, even if the treatment time is prolonged. For this reason, the LED may be favored over laser to treat traumatic brain injury which requires prolonged exposure to the light without the risk of thermal injury.68
In summary, we may desire NIR to better reach deep-lying regions of the brain such as the substantia nigra to treat Parkinson’s disease, pineal gland to regulate the circadian rhythm, and to draw a stronger response from the hypothalamus for systemic homeostasis. A LED NIR diode would have a large footprint that would cover the whole underside of the brain while it is able to reach deep lying glands too.
The risk of retina damage is always an issue with lasers even if it is low level with a 57 degree divergence that is common for the diodes used for intranasal light therapy. The issue is exacerbated with the near invisible NIR delivered as a laser; if one cannot respond with a reflex action (to blink) because it cannot be seen. This would be an overriding reason to prefer the LED over low level laser.
Therapeutic energy and other parameters
Energy is measured in Joules (J) = Power (W) X Time (seconds). For brain stimulation, very little energy is required to stimulate mitochondrial activity although a definitive threshold is yet to be established. A reference is the time-tested intravenous light irradiation method. This modality normally employs lasers with wavelength of 632.8 nm, power of 1.5 mw, time of 30 minutes per session. Treatment is usually spread over once a day for the first three days and then once every two days until a total of ten sessions is reached. For each session, dosage energy of 2.7J (1.5/1000W X 30 minutes X 60 seconds) is delivered.
If we are to use the same wavelength, the intranasal pathway calls for a higher power input than the above to penetrate additional tissues. The other factors that need to be considered are the treatment time, light coherency and whether we want continuous or pulsed wave, and for the pulsed wave, the choice of duty cycle.
Continuous wave (CW) vs Pulsed frequency
Generally, under certain conditions, ultra-short pulses can penetrate deeper into the tissues than continuous wave irradiation.69 Pushing greater power to a pulsed light source delivers more energy, which can activate more ATP, as demonstrated in a study on rabbits.70 Under a pulsed mode, the effective dosage is higher than the conventional calculation due the deeper travel into the tissues. The other mechanism of action involves the first part of a pulse containing photons to take all chromophore molecules in the upper tissue layer to excited states, opening the way for itself into tissue.71 Using 808 nm lasers on rabbits, researchers demonstrated that pulsed lasers at 100 Hz and 1000 Hz produced superior results to continuous wave (CW).72
18
Later researchers tested 810 nm laser that pulsed at 10 Hz produced even greater recovery from traumatic brain injury than 100 Hz. They suggested that the antidepressant activity of the light therapy was a contributing factor.73
The answer as to why pulsing at 10 Hz works better than 100 Hz (or any other frequency) is a matter of hypothesis: 10 Hz is the frequency of the alpha brain oscillation at rest. The pulsation at 10 Hz could be resonating with the whole brain in alpha state.
Furthermore, the hippocampus region also functions at waves in the 4-10 Hz. The hippocampus is responsible for memory, emotional well-being, behavioral management, spatial memory and navigation. It also is one of the regions that suffer damage in Alzheimer’s disease. A study showed that transcranial light therapy using a 808 nm laser diode attenuated amyloid plaque development in the transgenic mouse model, implying the possible efficacy of this therapeutic method for Alzheimer’s disease in humans.74
Apart from treating depression, researchers have had some success in treating attention deficit disorder and epileptic seizure by inducing alpha states through the process of neurobiofeedback.75
In summary, for brain therapy, particularly for the mid-brain region, a 10 Hz pulsed model promises efficacious outcomes. The profile for alpha state show even oscillations, which resembles a 50% duty cycle. We may combine this with the NIR 810 mw light source which gives good penetration depth, but only in the LED embodiment for safety reasons.
Summary of parameters
In conclusion, based on the large body of successful outcomes, the preferred set of parameters includes a 810 nm LED light source. To achieve a higher level of efficacy, it can be pulsed at 10 Hz with 50% duty cycle. Treatment time can be at 25 minutes, with the power intensity set at 10 mW. This results in the light rays from the LED light source to be delivered over a wide area. The power (as compared to lasers) can be set at 10 mW/cm².
With these parameters, the dosage per treatment is conventionally calculated at 7.5 J (10/1000W X 25 X 60 seconds X 50%). A pulsed wave gives a higher effective biomodulation, so the actual dosage should be higher than the 7.5 J though this amount is subjective. These parameters bring together what have been previously discovered to be most effective for brain stimulation when irradiating the brain through the nasal cavity.
Observations

19
To observe preliminary data, we prepared devices that contain the parameters as listed above and made these available for preliminary testing and observations, mainly to see if there are general differences with the existing devices that are operating in continuous wave mode; and with the understanding that these preliminary observations are mainly to observe whether there are risks and negative side effects related to its use. The existing devices being compared with are already being used regularly by the subjects. They are either LED devices with 633 nm diodes, powered with 8 mW/cm² of energy, timed for 25 minute treatment; or low level laser devices with 655 nm diodes, powered with 4.5 mW/cm² of energy for 25 minutes.
12 devices with the new specifications were distributed to various parties above 45 years old and who have already been using one of these devices. There was one post-stroke patient and one patient with early stage PD. The rest were generally of good health. After 2 weeks of use, the following data were collected:
• No safety issue or negative side effect were reported;
• 9 users reported a sense of improved cognitive experience, such as improved memory, and 3 reported not feeling any different;
• The recovering stroke patient reported improved sensations to the deficit side of the body.
• The PD patient reported the subjective sense of being in better overall condition.
With the small sample and lack of controls, we realize that placebo is distinctly possible These observations are encouraging bases for future rigorous studies.
Conclusion
Literature review and analysis support the proposed parameters relating to intranasal light therapy as promising for neurological. All the elements appear to have good scientific bases with sound mechanism of action. The direct and indirect evidence suggests that the parameters carry insignificant risks and insignificant side effects.
Other brain stimulation methods have their merits for treating specific neurological conditions. Evidence supporting transcranial light therapy for brain stimulation is increasing, including increasing number of indications. Intranasal light therapy using the parameters as proposed in this study is new, and as the support builds for the transcranial modality, they are also largely valid for the intranasal modality. The latter being the modality more naturally suited for irradiating from the underside of the brain, and the more primal mid-brain area. Considering that the much of the irradiating photons are dissipated soon after landing on the tissues, the combination of both the transcranial and intranasal pathways in combination would provide a comprehensive approach to holistic brain stimulation.
20
The major advantages that intranasal light therapy has over the other methods are that it is highly portable and low-cost.
References
1 Wang F. 2006. Therapeutic effect observation and nurse of intranasal low intensity laser therapy on insomnia.
Journal of Community Medicine. 4(3): 58 (in Chinese). 2 Jin L, Shi B. 2001. Compared research of laser irradiation on blood to erythrocyte deformability and P3PL
ingredient of patients with acute cerebral infarction. Chinese Journal of Rehabilitation Medicine. 16( 3) :152-153 (in Chinese). 3 Xu C, Wang L, Shang X and Li Q. 2002. The treatment of Alzheimer’s disease with hypoenergy He-Ne laser. Prac J
Med & Pharm. 19(9): 647-648 (in Chinese).
4 Smolnik R, Fischer S, Hagenah J, Kis B, Born J, Vieregge P. Brain potential signs of slowed stimulus processing
following cholecystokinin in Parkinson's disease. Psychopharmacology (Berl). 2002 Apr;161(1):70-6.
5 Li Q, Song L, Guo K, Yu Y, Ma S and Shen L. 1999. The effect of endonasal low energy He-Ne laser treatment of
Parkinson’s disease on CCK-8 content in blood. Chin J Neurol. 32(6): 364 (in Chinese). 6 Xu C, Lu C, Wang L and Li Q. 2003. The effects of endonasal low energy He-Ne laser therapy on antioxydation of
Parkinson’s disease. Prac J Med & Pharm. 20(11): 816-817 (in Chinese). 7 Zhao G, Guo K and Dan J. 2003. 36 case analysis of Parkinson’s disease treated by endonasal low energy He-Ne
laser. Acta Academiae medicinae Qingdao Universitatis. 39: 398 (in Chinese). 8 Liao Z. 2000. Nursing patients of schizophrenia treated by intranasal low energy He-Ne laser therapy. Journal of
Jiangxi University of Traditional Chinese Medicine. 12(3): 140 (in Chinese). 9 Li Q, Guo K, Kang J and Jiang B. 1998. Clinic analysis of endonasal low energy He-Ne laser treatment of 39 cases of
intractable headache. Acta Academiae medicinae Qingdao Universitatis. (1): 53 (in Chinese). 10
Li Q, Guo K, Kang J, Jiang B and Wang Y. 1998. β endorphin research for endonasal low energy He-Ne laser treatment of ache in head or face. Chin J Neurol. 31(2): 91 (in Chinese). 11
Qiao Y,Sun J, Jia F and Cheng G. 2004. Clinical Application Research of Low Power Laser Rhinal Irradiation. Applied Laser. 24(1): 64-65 (in Chinese). 12
Xiao X, Guo Y, Chu X, Jia S, Zheng X, Zhou C. 2005. Effects of low power laser irradiation in nasal cavity on cerebral blood flow perfusion of patients with brain infarction. Chinese Journal of Physical Medicine and
Rehabilitation. 27(7): 418-450 (in Chinese). 13
Dou Z, Hu X and Zhu H. 2003. The effects of two kinds of laser irradiation on patients with brain lesion. Chin J Phys Med Rehabil. 25(2): 86-88 (in Chinese).
21
14
Jin L, Shi B. 2001. Compared research of laser irradiation on blood to erythrocyte deformability and P3PL ingredient of patients with acute cerebral infarction. Chinese Journal of Rehabilitation Medicine. 16( 3) :152-153 (in Chinese) 15
Karu T (1999). “Primary and secondary mechanisms of action of visible-to-near IR radiation on cells”. J.
Photochem. Photobiol. B: Biology. 49(1):1-17. 16
Rojas JC, Gonzalez-Lima F (2011). “Low-level light therapy of the eye and brain”. Eye and Brain. 3:49-67. 17
Abdo A, Sahin M (2007). “NIR light penetration depth in the rat peripheral nerve and brain cortex”. Conf Proc
IEEE Eng Med Biol Soc 2007:1723-1725. 18
Ando T et al (2011). “Comparison of Therapeutic Effects between Pulsed and Continuous Wave 810 nm Wavelength Laser Irradiation for Traumatic Brain Injury in Mice”. Plos One. 6(10). 19
Uozumi Y, Nawashiro H, Sato S, Kawauchi S, Shima K, Kikuchi M (2010). “Targeted increase in cerebral blood flow by transcranial near-infrared laser irradiation”. Lasers Surg Med. 42(6):566–576. 20
Detaboada L, Ilic S, Leichliter-Martha S, Oron U, Oron A, Streeter J (2006). “Transcranial application of low-energy laser irradiation improves neurological deficits in rats following acute stroke”. Lasers Surg Med. 38(1):70–73. 21
Oron A, Oron U, Chen J, et al (2006). “Low-level laser therapy applied transcranially to rats after induction of stroke significantly reduces long-term neurological deficits”. Stroke. 37(10):2620–2624. 22
Lapchak PA, Wei J, Zivin JA (2004). “Transcranial infrared laser therapy improves clinical rating scores after embolic strokes in rabbits”. Stroke. 35(8):1985–1988. 23
Lapchak PA, Salgado KF, Chao CH, Zivin JÁ (2007). “Transcranial near-infrared light therapy improves motor function following embolic strokes in rabbits: an extended therapeutic window study using continuous and pulse frequency delivery modes”. Neuroscience. 148(4):907–914. 24
Lapchak PA, Han MK, Salgado KF, Streeter J, Zivin JA (2008). “Safety profile of transcranial near-infrared laser therapy administered in combination with thrombolytic therapy to embolized rabbits”. Stroke. 39(11):3073–3078. 25
Lapchak PA, De Taboada L (2010). “Transcranial near infrared laser treatment (NILT) increases cortical adenosine-5′-triphosphate (ATP) content following embolic strokes in rabbits”. Brain Res. 1306:100–105. 26
Lampl Y, Zivin JA, Fisher M, et al (2007). “Infrared laser therapy for ischemic stroke: a new treatment strategy: results of the NeuroThera Effectiveness and Safety Trial-1 (NEST-1)”. Stroke.38(6):1843–1849. 27
Oron A, Oron U, Streeter J, et al (2007). “Low-level laser therapy applied transcranially to mice following traumatic brain injury significantly reduces long-term neurological deficits”. J Neurotrauma. 24(4):651–656.

22
28
Naeser MA, Saltmarche A, Krengel MH, Hamblin MR, Knight JA (2010). “Improved cognitive function after transcranial, light-emitting diode treatments in chronic, traumatic brain injury: two case reports”. Photomed Laser
Surg. 29(5):351–358. 29
Shaw VE, Spana S, Ashkan K, et al (2010). “Neuroprotection of midbrain dopaminergic cells in MPTP-treated mice after near-infrared light treatment”. J Comp Neurol. 518(1):25–40. 30
Michalikova S, Ennaceur A, van Rensburg R, Chazot PL (2008). “Emotional responses and memory performance of middle-aged CD1 mice in a 3D maze: effects of low infrared light”. Neurobiol Learn Mem. 89(4):480–488. 31
Schiffer F, Johnston AL, Ravichandran C, et al (2009). « Psychological benefits 2 and 4 weeks after a single treatment with near infrared light to the forehead: a pilot study of 10 patients with major depression and anxiety”. Behav Brain Funct. 5:46. 32
Wong-Riley MT (1989). “Cytochrome oxidase: en endogenous metabolic marker for neural activity”. Trends
Neurosc. 12(3):94-101 33 Uozumi Y, Nawashiro H, Sato S, Kawauchi S, Shima K, Kikuchi M (2010). “ Targeted increase in cerebral blood
flow by transcranial near-infrared laser irradiation”. Lasers Surg Med 42: 566-576. 34
Fork RL (1971). “Laser stimulation of nerve cells in Aplysia”. Science. 171(974):907-908 35
Karu T (2000). “Mechanism of low-power laser light action on cellular level”. Proc SPIE. 2000;4159:1-17 36
Wong-Riley MT et al (2001). “Light emitting diode treatment reverses the effect of TTX on cytochrome oxidase in neurons”. Neuroreport. 12(14):3033-3037. 37
Wong-Riley MT et al (2005). “Photobiomodulation directly benefits primary neurons functionally inactivated by toxins: role of cytochrome c oxidase”. J Biol Chem. 280(6):4761-4771. 38
Chow Rt et al (2009). “Efficacy of low-level laser therapy in the management of neck pain: a systematic review and meta-analysis of randomised placebo or active treatment controlled trials”. Lancet. 374(9705):1897-1908. 39
Karu T (1989). “Laser biostimulation: a photobiological phenomenon”. J Photochem Photobiol B. 3(4):638-640. 40
Karu TI, et al (2008). “Absorption measurements of cell monolayers relevant to mechanisms of laser phototherapy: reduction or oxidation of cytochrome c oxidase under laser radiation at 632.8 nm”. Photomed Laser
Surg. 26(6):593-599.

23
41
Rojas JC, Gonzalez-Lima F. “Low-level light therapy of the eye and brain”. Eye and Brain. 2011;3:49-67. 42
Uozumi Y et al (2010). “Targeted increase in cerebral blood flow by transcranial near-infrared laser irradiation”. Lasers Surg Med. 42(6):566-576. 43
Detaboada L et al (2006). “Transcranial application of low-energy laser irradiation improves neurological deficits in rats following acute stroke”. Lasers Surg Med. 38(1):70-73. 44
Oron et al (2006). “Low-level laser therapy applied transcranially to rats after induction of stroke significantly reduces long-term neurological deficits”. Stroke. 37(10):2620-2624. 45
Lampl Y et al (2007). “Infrared laser therapy for ischemic stroke: a new treatment strategy: results of the NeuroThera Effectiveness and Safety Trial-1(NEST-1)”. Stroke.38(6):1843-1849. 46
Naeser MA et al (2010). “Improved cognitive function after transcranial, light-emitting diode treatments in chronic, traumatic brain injury: two case reports”. Photomed Laser Sur. 29(5):351-358. 47
Shaw VE et al (2010). “Neuroprotection of midbrain dopaminergic cells in MPTP-treated mice after near-infrared light treatment”. J Comp Neurol. 518(1):25-40. 48
Mikhalikova S et al (2008). “Emotional responses and memory performance of middle-age CD1 mice in a 3D maze: effects of low infrared light”. Neurobiol Learn Mem. 89(4):480-488. 49
Detaboada L et al (2006). “Transcranial application of low-energy laser irradiation improves neurological deficits in rats following acute stroke”. Lasers Surg Med. 38(1):70-73. 50
Nolte J (2009). “Formation, Modificaton, and Repair of Neuronal Connections” in The Human Brain: An Introduction to its Functional Anatomy. Mosby Inc., Elsevier. pp 633-634. 51
Rojas JC, Bruchey AK and Gonzaez-Lima (2012). “Low-Level Light Therapy Improves Cortical Metabolic Capacity and Memory Retention. J Alzheimers Dis. 32(3): 741-52. 52
Valla J et al (2001). “Energy hypometabolism in posterior cingulated cortex of Alzheimer’s patients: superficial laminar cytochrome oxidase associated with disease duration”. J Neurosci. 21(13):4923-4930. 53
Shumake J, Gonzalez-Lima F (2003). “Brain systems underlying susceptibility to helplessness and depression”. Behav Cogn Neurosci Rev. 2(3):198-221. 54
Hamani C et al (2010). “Antidepressant-like effects of medial prefrontal cortex deep brain stimulation in rats”. Biol Psychiatry. 67(2):117-124.

24
55
Schiffer F (2009). “Psychological benefits 2 and 4 weeks after a single treatment with near infrared light to the forehead: a pilot study of 10 patients with major depression and anxiety”. Behav Brain Funct. 5:46.
56 Liu X, Ramirez S, Pang PT, Puryear CB, Govindarajan, Deisseroth K and Tonegawa S (2012). “Optogenetic
stimulation of a hippocampal engram activates fear memory recall”. Nature 484: 381-385.
57 Rojas JC, Bruchey AK and Gonzaez-Lima (2012). “Low-Level Light Therapy Improves Cortical Metabolic Capacity
and Memory Retention. J Alzheimers Dis. 32(3): 741-52. 58
Hamblin MR, Demidova TN. Mechanism of low level light therapy (2006). Proc SPIE. 2006;6140:1-12. It is based on the principle that certain molecules in living systems are able to absorb photons and trigger signaling pathways in response to light [Sutherland JC (2002). “Biological effects of polychromatic light”. Photochem Phtobiol. 76(2):164-170. 59
Byrnes KR et al (2005). “Light promotes regeneration and functional recovery and alters the immune system after spinal cord injury”. Lasers Surg Med. 36(3):171-185. 60
Abdo A, Sahin M (2007). “NIR light penetration depth in the rat peripheral nerve and brain cortex”. Conf Proc
IEEE Eng Med Biol Soc 2007. 1723-1725. 61
Eells JT, Wong-Riley MT, VerHoeve J et al (2004). “Mitochondrial signal transduction in accelerated wound and retinal healing by near-infrared light therapy”. Mitochondrion. 2004;4(5-6):559-567. 62
Karu T (1999). “Primary and secondary mechanisms of action of visible to near-IR radiation on cells”. J Photochem Photobiol B. 49(1):1.17. 63
Khan JA et al (2007). “Nicotinamide adinosine denucleotide metabolism as an attractive target for drug discovery”. Expert Opin Ther Targets; 11(5):695-705. 64
Karu TI et al (1996). “Effects of monochromatic low-intensity light and laser irradiation on adhesion of HeLa cells in vitro”. Laser Surg. Med.18(2):171-177. 65
Hamblin MR, Demidova TN (2006). “Mechanism of low level laser therapy”. Proc of SPIE 6140: 1-12. 66
Rojas JC, Bruchey AK and Gonzaez-Lima (2012). “Low-Level Light Therapy Improves Cortical Metabolic Capacity and Memory Retention. J Alzheimers Dis. 32(3): 741-52. 67
Karu T (1999). “Primary and secondary mechanisms of action of visible-to-near IR radiation on cells”. J.
Photochem. Photobiol. B: Biology. 49(1):1-17.

25
68
Eells JT, Wong-Riley MT, VerHoeve J, et al (2004). “Mitochondrial signal transduction in accelerated wound and retinal healing by near-infrared light therapy”. Mitochondrion. 4(5-6):559-567. 69 Pogue BW, Lilge L, Patterson MS, et al (1997). ”Absorbed photodynamic dose from pulsed versus continuous
wave light examined with tissue-simulating dosimeters”. Appl Opt 36:7257-7269. 70
Lapchak PA, De Tabouda L (2010). “Transcranial near infrared laser treatment (NILT) increases cortical adenosine-5’-triphosphate (ATP) content following embolic strokes in rabbits”. Brain Res. 130:100-105. 71 Barolet D, Boucher A, Bjerring P (2005). “In vivo human dermal collagen production following LED-based therapy:
The importance of treatment parameters”. Lasers Surg Med 17:76 (suppl) (abstr)
72
Lapchak PA et al (2007). “Transcranial near-infrared light therapy improves motor function following embolic strokes in rabbits: an extended therapeutic window study using continuous and pulsed frequency delivery modes”. Neuroscience . 148: 907-914. 73
Ando T et al (2011). “Comparison of Therapeutic Effects between Pulsed and Continuous Wave 810-nm Wavelength Laser Irradiation for Traumatic Brain Injury in Mice”. Plos One. 6(10):e26212 (online). 74
De Taboada L, et al (2011). “Transcranial laser therapy attenuates amyloid-beta peptide neuropathology in amyloid-beta protein precursor transgenic mice”. J. Alzheimers Dis. 23. 52-59. 75
Kraft U (2006). “Train Your Brain-Mental exercises with neurofeedback may ease symptoms of attention-deficit disorder, epilepsy and depression--and even boost cognition in healthy brains”. Scientific American. 2006.