brad esarey vp business operations. a need for personalized medicine
TRANSCRIPT

Brad EsareyVP Business Operations
A need for Personalized Medicine

PGx Integration:Role of the Clinical Laboratory
• Catalyze the delivery of biotechnology products to healthcare consumers
• Overcome barriers to genotyping
• Develop genetic profiling strategies to maximize sensitivity and specificity of predicting phenotype
• Provide availability of testing• Develop methods to reduce technical difficulty, cost • Improve interpretations

Pharmacogenetics
Links differences in gene structure (inherited polymorphism) to drug metabolism and response
(Genotype) (Phenotype)
Genetic
polymorphism
Drug metabolism
& response
Why is this important ?
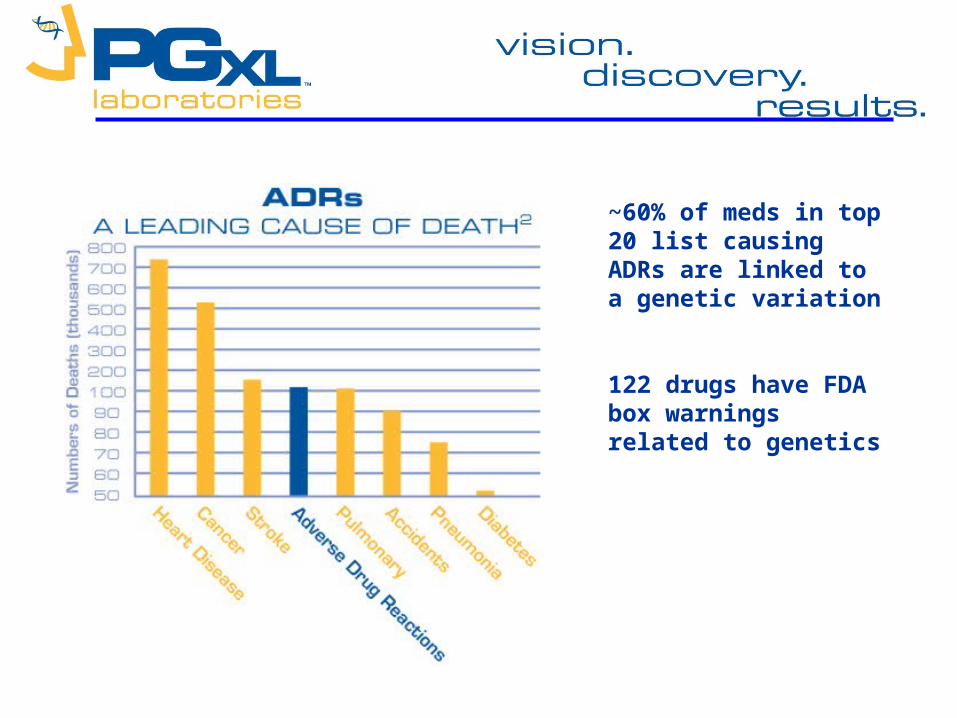
~60% of meds in top 20 list causing ADRs are linked to a genetic variation
122 drugs have FDA box warnings related to genetics

Explanatory Use
Decision forDrug Treatment
CYP Genotyping
Therapy Refractorinessor Adverse Events
Dose Adjustment Accordingto Efficacy and Adverse Events
Standard Drugand Dose
Predictive Use
Decision forDrug Treatment
CYP Genotyping
Further Adjustment Accordingto Efficacy and Adverse Events
Drug Selection and DosageBased on Genotype
Key:
This
Connection

IntuitiveMedicine
PrecisionMedicine
Indicators Suggest: Diagnostic services will trump therapeutics (Clayton M Christenson in: The Innovator’s Prescription, MacGraw Hill, 2009)
PGXL Enables Transformation

8
Applications of pharmacogenomics
• Individualizing drug therapy selection
• Predicting adverse reactions, dosing, response
• Identify increased sensitivity to drug interactions

9
Clinical Applications of Pharmacogenetic Information
• Anti-coagulation– Warfarin– Plavix (clopidogrel)
• Psychiatry– Anti-depressants
• Oncology– KRAS– Tamoxifen– EGFR’s
• Pain management– Codeine– Hydrocodone– Oxycodone
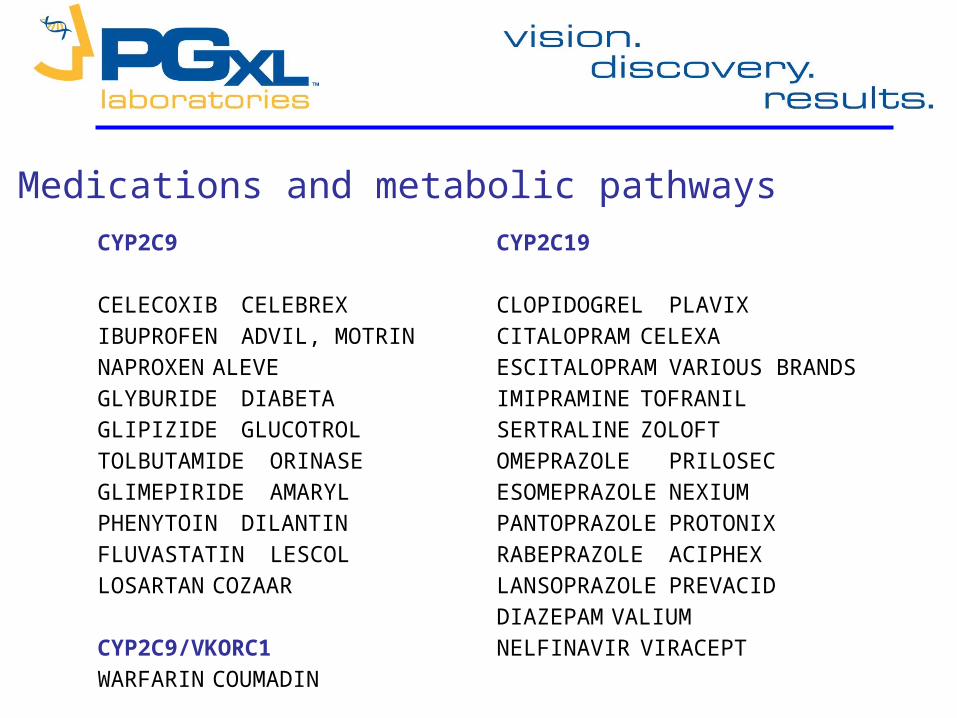
CYP2C9
CELECOXIB CELEBREX
IBUPROFEN ADVIL, MOTRINNAPROXEN ALEVEGLYBURIDE DIABETA
GLIPIZIDE GLUCOTROL
TOLBUTAMIDE ORINASE
GLIMEPIRIDE AMARYLPHENYTOIN DILANTIN
FLUVASTATIN LESCOLLOSARTAN COZAAR
CYP2C9/VKORC1
WARFARIN COUMADIN
CYP2C19
CLOPIDOGREL PLAVIX
CITALOPRAM CELEXA
ESCITALOPRAM VARIOUS BRANDS
IMIPRAMINE TOFRANIL
SERTRALINE ZOLOFT
OMEPRAZOLE PRILOSEC
ESOMEPRAZOLE NEXIUM
PANTOPRAZOLE PROTONIX
RABEPRAZOLE ACIPHEX
LANSOPRAZOLE PREVACID
DIAZEPAMVALIUM
NELFINAVIR VIRACEPT
Medications and metabolic pathways
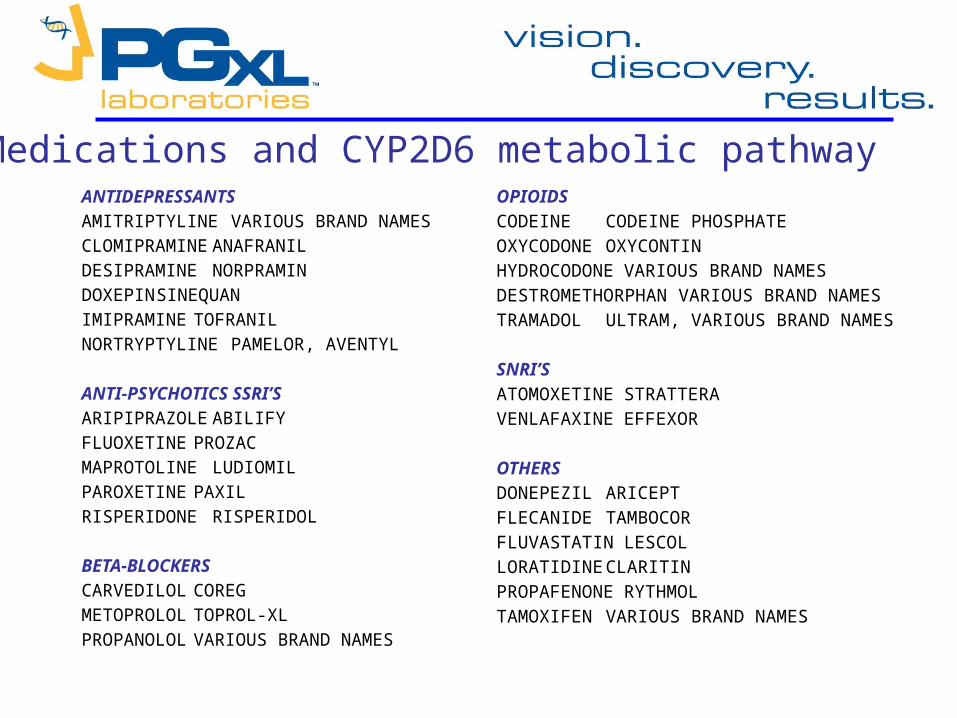
ANTIDEPRESSANTSAMITRIPTYLINE VARIOUS BRAND NAMESCLOMIPRAMINE ANAFRANILDESIPRAMINE NORPRAMINDOXEPIN SINEQUANIMIPRAMINE TOFRANILNORTRYPTYLINEPAMELOR, AVENTYL ANTI-PSYCHOTICS SSRI’SARIPIPRAZOLE ABILIFYFLUOXETINE PROZACMAPROTOLINE LUDIOMILPAROXETINE PAXILRISPERIDONE RISPERIDOL BETA-BLOCKERSCARVEDILOL COREGMETOPROLOL TOPROL-XLPROPANOLOL VARIOUS BRAND NAMES
OPIOIDS
CODEINE CODEINE PHOSPHATE
OXYCODONE OXYCONTIN
HYDROCODONE VARIOUS BRAND NAMES
DESTROMETHORPHAN VARIOUS BRAND NAMES
TRAMADOL ULTRAM, VARIOUS BRAND NAMES
SNRI’S
ATOMOXETINE STRATTERA
VENLAFAXINE EFFEXOR
OTHERS
DONEPEZIL ARICEPT
FLECANIDE TAMBOCOR
FLUVASTATIN LESCOL
LORATIDINE CLARITIN
PROPAFENONE RYTHMOL
TAMOXIFEN VARIOUS BRAND NAMES
Medications and CYP2D6 metabolic pathway
Vision: enable transition of pharmacogenetic diagnostics into actionable healthcare results
Mission and Core Business Strategies:
• Provide Clinical Diagnostic Services (healthcare providers for direct patient care)
• Support Development of Diagnostics (discovery & translation of biological markers)

Product Lines
Cardiovascular: - Anticoagulation - HTN/CHF
Oncology: - Cancer therapy - Prevention
Pain Management: - Opiods
PGXL is uniquely positioned
Respiratory: - Asthma - COPD
Behavioral Health: - ADHD - Schizophrenia - Depression

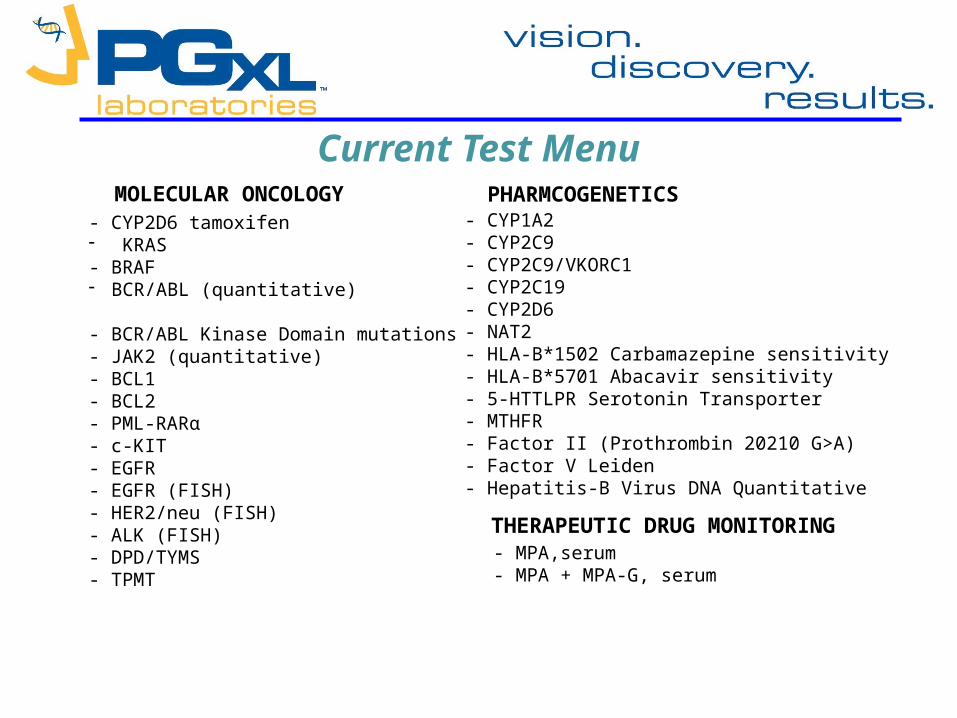
Current Test Menu
- CYP1A2- CYP2C9- CYP2C9/VKORC1 - CYP2C19- CYP2D6- NAT2- HLA-B*1502 Carbamazepine sensitivity- HLA-B*5701 Abacavir sensitivity- 5-HTTLPR Serotonin Transporter- MTHFR- Factor II (Prothrombin 20210 G>A)- Factor V Leiden- Hepatitis-B Virus DNA Quantitative
- CYP2D6 tamoxifen - KRAS- BRAF- BCR/ABL (quantitative)
- BCR/ABL Kinase Domain mutations- JAK2 (quantitative)- BCL1- BCL2- PML-RARα- c-KIT- EGFR- EGFR (FISH)- HER2/neu (FISH)- ALK (FISH)- DPD/TYMS- TPMT
MOLECULAR ONCOLOGY PHARMCOGENETICS
- MPA,serum- MPA + MPA-G, serum
THERAPEUTIC DRUG MONITORING
PGx of Warfarin Overview
• Quick review of the problem• Review of Pharmacokinetic Basics• Application of knowledge

FDA Updates Coumadin LabelGenetic Information may improve initial dosing estimate for individual
patients
The U.S. Food and Drug Administration announced today the approval of updated labeling for the widely used blood-thinning drug, Coumadin, to explain that people's genetic makeup may influence how they respond to the drug.
The labeling change highlights the opportunity for healthcare providers to use genetic tests to improve their initial estimate of what is a reasonable warfarin dose for individual patients. Testing may help optimize the use of warfarin and lower the risk of bleeding complications from the drug.
U.S. Food and Drug Administration August 16, 2007
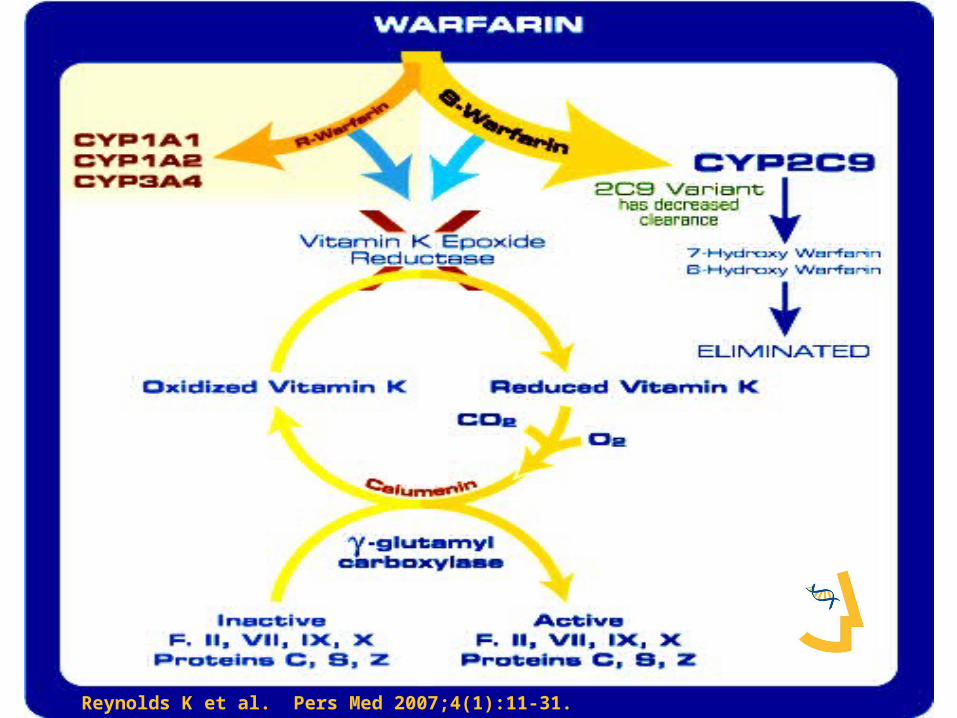
Reynolds K et al. Pers Med 2007;4(1):11-31.

• Pharmacogenetics of Warfarin– Inactivated and eliminated via Cytochrome
P4502C9 metabolism• 40% of populations have deficient CYP2C9
– Inhibits Vitamin K epoxide reductase complex• > 70% of population have decreased VKOR and
are more sensitive to warfarin

Linder et al. J Thrombosis & Thrombolysis 2002;14:227-232
• CYP2C9 *2 and *3 – delay time to reach
steady-state– Increase blood
concentration
• Dose effectiveness should be assessed at steady-state
0 3 6 9 12 15 18 21 24 27 30
Time (days)
0.00
0.60
1.20
1.80
2.40
3.00
S-W
arfa
rin (m
g/L)
CYP2C9*1/*3
CYP2C9*1/*2
CYP2C9*1/*1
Confidential

Variables influencing maintenance dose.
Zhu Y et al. Clin Chem 2007;53(7):1199-1205.
Optimal WARFARIN dose can be calculated based on AGE, GENDER, WEIGHT and PHARMACOGENETICS
Impact of Testing• Estimate Maintenance Dose Requirement
Guides dose selection• Estimate of Time to Reach Steady-state
Avoid Mis-interpretation of INR’s
Avoid Premature Dosage Changes

© Copyright 2007 Pharmacogenetics Diagnostic Laboratory, LLC. All rights reserved. Duplication of material prohibited.

Application of Pharmacogenomics to Anti-platelet therapy
25
Antiplatelet Response
• Clopidogrel (Plavix) is a pro-drug which is converted to an active metabolite by hepatic cytochrome P4502C19 (CYP2C19).
• ~ 30% of patients have deficiency in
CYP2C19

Influence of CYP2C19 on Clopidogrel Response

Applications of PGx in Pain Management
• Pharmacokinetics: genetic variation in cytochrome P450’s– Decreased drug clearance
• Mis-interpretation of over compliance
– Ultra-rapid drug clearance• Mis-interpretation of drug diversion• Mis-interpretation of poor compliance
Cytochrome P4502D6 Substrates • Pain management
– Hydrocodone– Oxycodone– Methadone– Propoxyphene– Codeine– Others ….
• In addition many drugs commonly co-prescribed with pain management medications– Antidepressants– Anti-anxiety

Genetic polymorphism of CYP2D6• Ultra-rapid metabolizers (UM)
– 3 – 7 % of population
• Extensive metabolizers (EM)– 55 – 60 % of population
• Intermediate metabolizers (IM)– 25 – 30% of population
• Poor Metabolizers (PM)– 5 – 10 % of population

Example: Codeine• Principal metabolism by CYP2D6• Pro-drug to morphine• CYP2D6 PM: in adequate morphine• CYP2D6 UM: morphine poisoning

Case Report:Neonatal Morphine Overdose
• Full-term healthy male infant showed intermittent periods of difficulty in breastfeeding and lethargy starting on day 7
• Day 11 pediatric visit baby regained birth weight• Day 12 gray skin and milk intake had fallen• Baby found dead on day 13• Postmortem analysis showed no anatomical
anomalies
Koren et al. Lancet 2006;368:704.

Toxicology Results• Blood concentration of morphine = 70 ng/mL
– neonates breastfed by mothers receiving codeine typically have morphine serum concentrations of 0–2.2 ng/mL
• Day 10 breast milk morphine concentration = 87 ng/mL– Typical range after repeated maternal codeine doses of 60
mg every 6 h is 1.9–20.5 ng/mL
• The mother was prescribed 2 weeks codeine 30 mg + acetaminophen 500 mg (Tylenol #3) after birth for episiotomy pain– 4 tabs first day, but only 2 tabs daily thereafter because of
maternal somnolence and constipation
Koren et al. Lancet 2006;368:704.
CYP2D6 Genotype Analysis
CYP2D6 *1/*2xN = Ultra-rapid Metabolizer(gene duplication) (UM)
• Leads to increased formation of morphine from codeine
• Maternal grandfather, the father, and the infant had 2 functional CYP2D6 alleles (Extensive Metabolizer, EM)
• The maternal grandmother was a UM
Koren et al. Lancet 2006;368:704.
Clinical Case Conclusions
• The clinical and laboratory picture was consistent with neonatal death from opioid toxicity
• Most of the analgesic and CNS depressant effects of codeine are secondary to its metabolism to morphine by CYP2D6
• Neonates invariably have impaired capacity to metabolize and eliminate morphine
Koren et al. Lancet 2006;368:704.
Case Conclusions, cont’d• Codeine is a commonly used analgesic after labor
– Episiotomy– Caesarean section
• American Academy of Pediatrics lists codeine as compatible with breastfeeding, despite lack of sufficient published data to support this recommendation
• Inherited differences in CYP2D6 can be life-threatening for some breastfed babies “Codeine cannot be considered as a safe drug for all infants
during breastfeeding”• CYP2D6 UM frequency
– 1.5 - 2% in Caucasians and Asians– 14% in African Americans– 29% in Ethiopians
Koren et al. Lancet 2006;368:704.
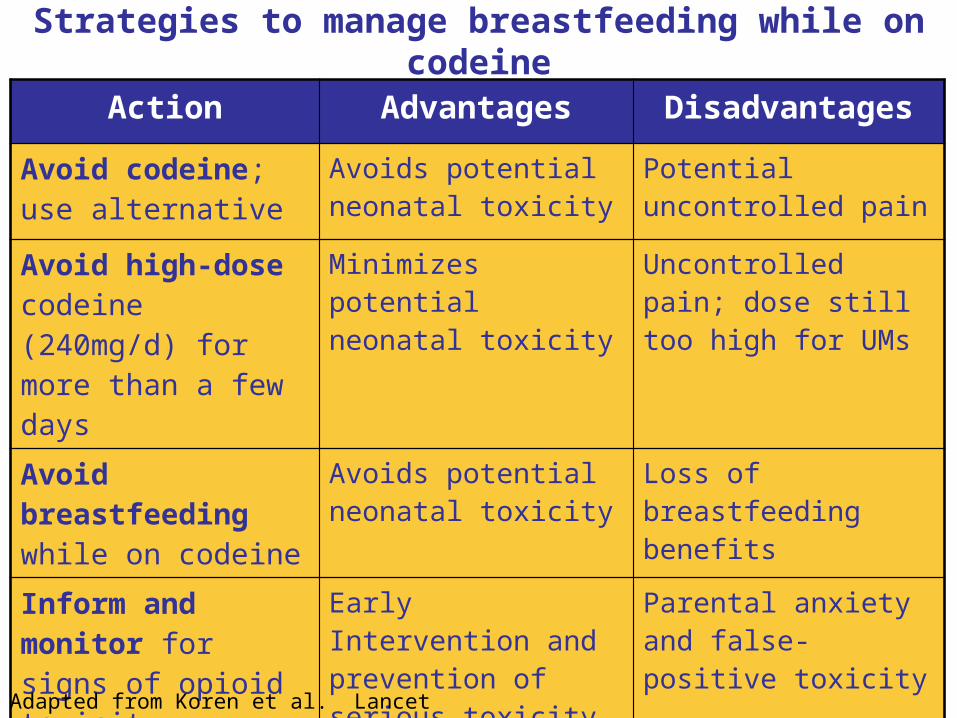
Strategies to manage breastfeeding while on codeine
Action Advantages Disadvantages
Avoid codeine; use alternative
Avoids potential neonatal toxicity
Potential uncontrolled pain
Avoid high-dose codeine (240mg/d) for more than a few days
Minimizes potential neonatal toxicity
Uncontrolled pain; dose still too high for UMs
Avoid breastfeeding while on codeine
Avoids potential neonatal toxicity
Loss of breastfeeding benefits
Inform and monitor for signs of opioid toxicity
Early Intervention and prevention of serious toxicity
Parental anxiety and false-positive toxicity
Genotype mothers for CYP2D6
Predicts risk of excess morphine production
Expensive, not presently routine
Adapted from Koren et al. Lancet 2006;368:704.

CYP2D6 Genotyping
Routine CYP2D6 testing IS available
Metabolizer status (phenotype)can be predicted
Predicts risk of toxicity, therapeutic failure, and promotes optimal outcomes for patients

Other CYP2D6 Genotyping Considerations
• CYP2D6 metabolizes 20-25% of all current medications
• CYP2D6 inactivates medications– antidepressants, antipsychotics, beta- blockers, antiarrhythmics
• CYP2D6 activates medications– opioids, tamoxifen
• CYP2D6 is inhibited by medications– antidepressants (SSRIs in particular), antipsychotics, certain
antimicrobials, quinidine, amiodarone• CYP2D6 is induced by medications
– rifampin, carbamazepine, phenobarbital, ritonavir

Consultation Services
• PGXL provides state-of-the-art interpretive reports with actionable guidance
• PGXL medical directors are available for clinical consultation with ordering practitioners before and after testing
• Ongoing VIP review consultation after 50-100 patients tested
• Educational lecture series and/or CME events as needed

Diagnostic Testing• Clinical testing is available• Must be performed by high-complexity
CLIA-certified laboratory• 5-7 business day TAT• Whole blood or cheek swab samples• Genotype result with phenotype
interpretation

Patient Information: Genetic Drug Sensitivity TestingWhy test my genes before prescribing a drug?Just as gene variation controls hair or eye color, it also controls how the body reacts to certain drugs. Before prescribing one of those drugs, your physician may give you a genotype test to make sure the drug will be safe and effective for you. A genotype is an analysis of some aspect of your genetic make-up. Knowing your genotype will help you and your doctor choose the most effective treatment path.What is CYP450?CytochromeP450, abbreviated CYP450, is a complex of genes that controls liver enzymes that digest certain drugs. Those drugs include Plavix®, Coumadin®, warfarin, beta blockers, common pain medications and antidepressants, among many others. Different genes within the CYP450 complex control the metabolization of different drugs. CYP2C19, for example, indicates Plavix sensitivity, and CYP2C9 is commonly analyzed before prescribing Coumadin/warfarin.What will the test tell me?Specifically, how quickly your body filters a given drug out of your bloodstream. A high metabolizer flushes drugs out of the body quickly, and might never realize any benefit from taking a “normal” dose. A poor metabolizer is just the opposite, with a “normal” dose building to potentially dangerous levels. Understanding how quickly you will metabolize a drug helps your doctor calculate the safest, most effective dose for you.What is required to perform this test?You will need to provide a DNA sample using a buccal swab. A buccal swab is a sterile cotton swab made for DNA collection. You gather DNA simply and painlessly by rubbing the buccal swabs on the insides of your cheeks. The swabs are then sealed and shipped to the lab for testing.What happens to my DNA once the test is complete?Your privacy is assured. Samples and genetic information are stored securely in accord with HIPAA and other government regulations.Is there a cost for this test?This is a routine clinical laboratory test covered by Medicare and most private insurance plans. There may be a co-pay, depending on the specifics of your policy.How do I get my test results?Results will be sent to your doctor 3-5 business days after your sample is collected.All tests are performed by PGXL Laboratories, Louisville, KY – 877-564-2199 – CLIA License 18D0983143.

The Actual In-service


DON’T
DO’S
• Four swabs per test• One swab at a time• Two swabs per
cheek• Thirty seconds per
swab• One minute dry
• Blood is ok• Swabs in envelope • Envelopes in Ziploc • Forms in Pouch

QUESTIONS?
THANK YOU!