bone suture technique for prevention of post-operative...
TRANSCRIPT

Journal of International Oral Health 2015; 7(10):6-9
6
Bone suture technique … Rahpeyma A et al
Original ResearchReceived: 19th May 2015 Accepted: 12th August 2015 Conflicts of Interest: None
Source of Support: Nil
Bone Suture Technique for Prevention of Post-operative Hematoma after Removal of Palataly Impacted Maxillary CaninesAmin Rahpeyma1, Saeedeh Khajehahmadi2
Contributors:1Associate Professor of Oral and Maxillofacial Surgery, Oral and Maxillofacial Diseases Research Center, School of Dentistry, Mashhad University of Medical Sciences, Mashhad, Iran; 2Assistant Professor of Oral and Maxillofacial Pathology, Dental Research Center, School of Dentistry, Mashhad University of Medical Sciences, Mashhad, Iran.Correspondence:Dr. Khajehahmadi S. Dental Research Center of Mashhad University of Medical Sciences, Vakilabad Blvd, Mashhad, Iran. Tel: +98(51)38829501. Email: [email protected] to cite the article:Rahpeyma A, Khajehahmadi S. Bone suture technique for prevention of post-operative hematoma after removal of palataly impacted maxillary canines. J Int Oral Health 2015;7(10):6-9.Abstract:Background: Maxillary canine palatal impaction is a common entity. After tooth removal, prevention of subperiosteal hematoma in widely elevated palatal mucoperiosteal flap is important.Materials and Methods: In a respective study, all patients with maxillary canine palatal impaction that were treated by surgical removal of the impacted tooth between 2008 and 2012 were recalled, in these patients, bone suture technique was used for management of palatal flap, based on the space between maxillary permanent lateral tooth and first premolar. This article suggests a classification in four types.Results: A total of 147 palatal impacted canines were surgically removed by a surgeon (83 unilateral and 32 bilateral). The most prevalent space classification between permanent lateral and first premolar was Type II (47.6) followed by Type I (34%), Type III (13.6%), and Type IV (4.7%). There was no case of root damage to the adjacent teeth, during buccal overmucosal hole preparation.Conclusion: The bone suture technique, introduced to overcome the problem of subperiosteal hematoma after removal of palatally impacted canine, is simple, effective, and harmless, for the patients.
Key Words: Hematoma, tooth impaction, maxillary canine
IntroductionMaxillary canine palatal impaction is a common entity. Estimated prevalence of this impaction is between 1% and 3% in general population.1,2 About 80% of maxillary impacted canines are palatally impacted.3,4 Surgical removal of these tooth often needs envelope flap. After tooth removal, prevention of subperiosteal hematoma in widely elevated palatal mucoperiosteal flap, especially in bilateral impactions, is important (Figure 1). The suggested ways include; deep
bite of elevated palatal tissue with sutures, removable acrylic splints, acrylic splints wired to the dentition, gauze pack under horizontal mattress wiring and changing the soft tissue incision in palatal region from marginal incision to submarginal incision.5-7 Firm pressure by the patients thumb through a pad of gauze for 5-10 min is the simplest suggested way.8 All of these suggested procedures have their own disadvantages. Bone suture technique is presented in this article to overcome the problem of subperiosteal hematoma after removal of palatally impacted canine.
Materials and MethodsIn a respective study, all patients with maxillary canine palatal impaction were recalled. These patients were all treated by the first author between 2008 and 2012. The procedure was surgical removal of the impacted tooth, in which bone suture technique was used for management of palatal flap. This study was approved by the Vice Chancellor of Research of Mashhad University of Medical Sciences regarding ethical and methodological issues. Periapical radiography was done in all patients post-operatively. Adjacent Root damage by probable accidental injury during preparation of bone hole was recorded. During post-operative period space classification could change (orthodontic space closure, deciduous canine extraction, and replacement of the space with dental implant), and hence the first situation before surgery was considered. If the archive file has no pre-operative radiography, then the case was excluded from the study. Other exclusion criteria were
Figure 1: Hematoma after removal of bilateral impacted maxillary canine 2 weeks after operation.
7
Journal of International Oral Health 2015; 7(10):6-9Bone suture technique … Rahpeyma A et al
intermediate maxillary canine impaction, systemic diseases that interfere with wound healing such as diabetes mellitus and anticoagulant therapy. Smokers were not excluded from the study.
Based on the space between the maxillary permanent lateral tooth and first premolar we suggest the following four type classification (Figure 2).
Type I: Deciduous canine present in the arch.Type II: With edentulous space.Type III: Closed contact between adjacent teeth (lateral and first premolar).Type IV: In the edentulous patient.
In bilateral impactions, each side can have its own classification.
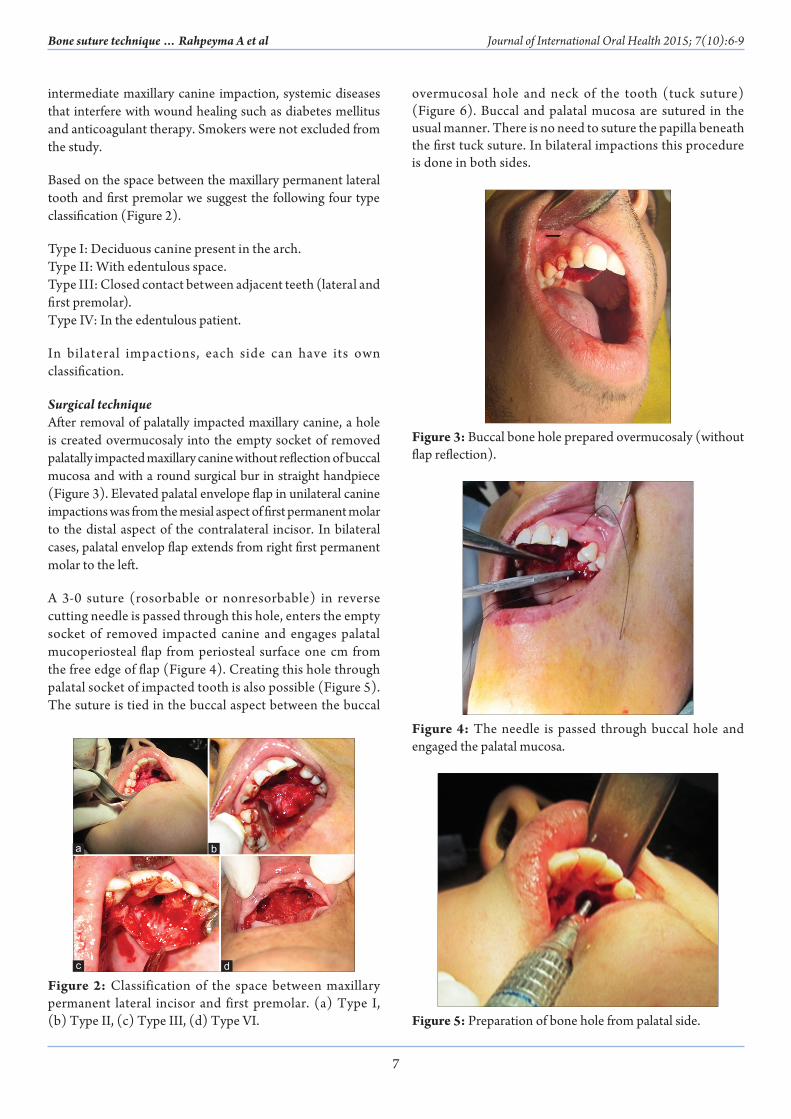
Surgical techniqueAfter removal of palatally impacted maxillary canine, a hole is created overmucosaly into the empty socket of removed palatally impacted maxillary canine without reflection of buccal mucosa and with a round surgical bur in straight handpiece (Figure 3). Elevated palatal envelope flap in unilateral canine impactions was from the mesial aspect of first permanent molar to the distal aspect of the contralateral incisor. In bilateral cases, palatal envelop flap extends from right first permanent molar to the left.
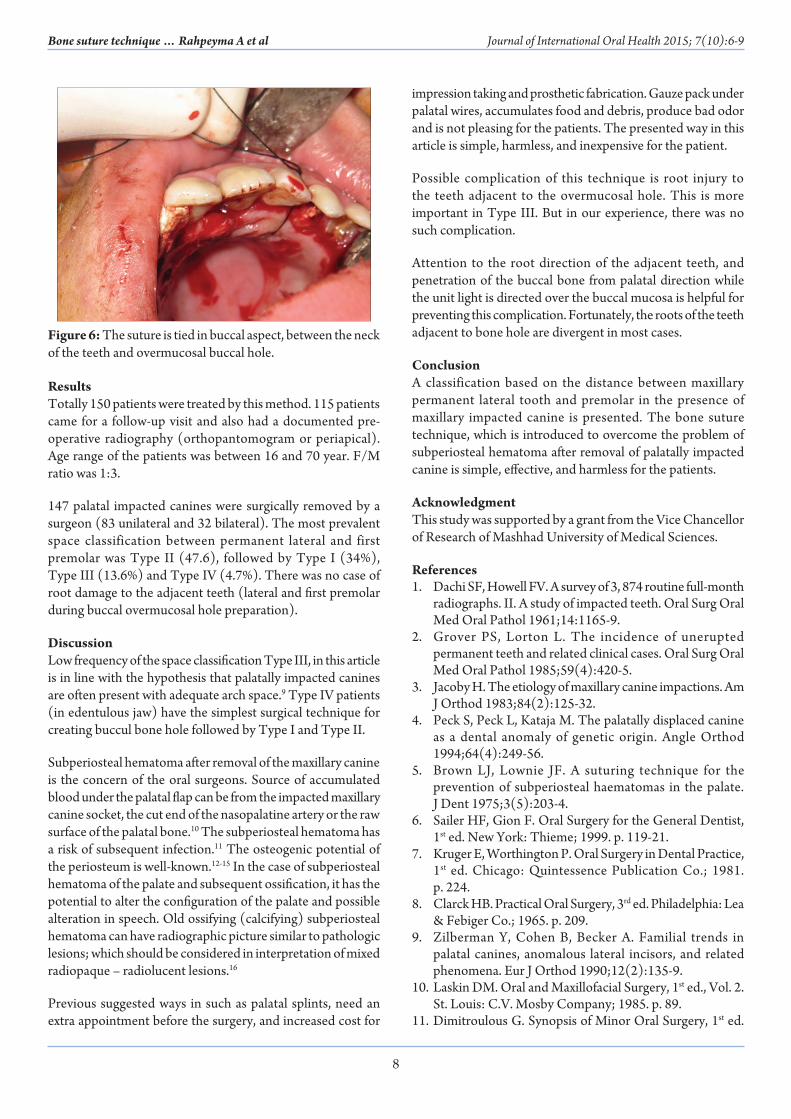
A 3-0 suture (rosorbable or nonresorbable) in reverse cutting needle is passed through this hole, enters the empty socket of removed impacted canine and engages palatal mucoperiosteal flap from periosteal surface one cm from the free edge of flap (Figure 4). Creating this hole through palatal socket of impacted tooth is also possible (Figure 5). The suture is tied in the buccal aspect between the buccal
overmucosal hole and neck of the tooth (tuck suture) (Figure 6). Buccal and palatal mucosa are sutured in the usual manner. There is no need to suture the papilla beneath the first tuck suture. In bilateral impactions this procedure is done in both sides.
Figure 3: Buccal bone hole prepared overmucosaly (without flap reflection).
Figure 4: The needle is passed through buccal hole and engaged the palatal mucosa.
Figure 5: Preparation of bone hole from palatal side.
Figure 2: Classification of the space between maxillary permanent lateral incisor and first premolar. (a) Type I, (b) Type II, (c) Type III, (d) Type VI.
dc
ba
8
Journal of International Oral Health 2015; 7(10):6-9Bone suture technique … Rahpeyma A et al
ResultsTotally 150 patients were treated by this method. 115 patients came for a follow-up visit and also had a documented pre-operative radiography (orthopantomogram or periapical). Age range of the patients was between 16 and 70 year. F/M ratio was 1:3.
147 palatal impacted canines were surgically removed by a surgeon (83 unilateral and 32 bilateral). The most prevalent space classification between permanent lateral and first premolar was Type II (47.6), followed by Type I (34%), Type III (13.6%) and Type IV (4.7%). There was no case of root damage to the adjacent teeth (lateral and first premolar during buccal overmucosal hole preparation).
DiscussionLow frequency of the space classification Type III, in this article is in line with the hypothesis that palatally impacted canines are often present with adequate arch space.9 Type IV patients (in edentulous jaw) have the simplest surgical technique for creating buccul bone hole followed by Type I and Type II.
Subperiosteal hematoma after removal of the maxillary canine is the concern of the oral surgeons. Source of accumulated blood under the palatal flap can be from the impacted maxillary canine socket, the cut end of the nasopalatine artery or the raw surface of the palatal bone.10 The subperiosteal hematoma has a risk of subsequent infection.11 The osteogenic potential of the periosteum is well-known.12-15 In the case of subperiosteal hematoma of the palate and subsequent ossification, it has the potential to alter the configuration of the palate and possible alteration in speech. Old ossifying (calcifying) subperiosteal hematoma can have radiographic picture similar to pathologic lesions; which should be considered in interpretation of mixed radiopaque – radiolucent lesions.16
Previous suggested ways in such as palatal splints, need an extra appointment before the surgery, and increased cost for
impression taking and prosthetic fabrication. Gauze pack under palatal wires, accumulates food and debris, produce bad odor and is not pleasing for the patients. The presented way in this article is simple, harmless, and inexpensive for the patient.
Possible complication of this technique is root injury to the teeth adjacent to the overmucosal hole. This is more important in Type III. But in our experience, there was no such complication.
Attention to the root direction of the adjacent teeth, and penetration of the buccal bone from palatal direction while the unit light is directed over the buccal mucosa is helpful for preventing this complication. Fortunately, the roots of the teeth adjacent to bone hole are divergent in most cases.
ConclusionA classification based on the distance between maxillary permanent lateral tooth and premolar in the presence of maxillary impacted canine is presented. The bone suture technique, which is introduced to overcome the problem of subperiosteal hematoma after removal of palatally impacted canine is simple, effective, and harmless for the patients.
AcknowledgmentThis study was supported by a grant from the Vice Chancellor of Research of Mashhad University of Medical Sciences.
References1. Dachi SF, Howell FV. A survey of 3, 874 routine full-month
radiographs. II. A study of impacted teeth. Oral Surg Oral Med Oral Pathol 1961;14:1165-9.
2. Grover PS, Lorton L. The incidence of unerupted permanent teeth and related clinical cases. Oral Surg Oral Med Oral Pathol 1985;59(4):420-5.
3. Jacoby H. The etiology of maxillary canine impactions. Am J Orthod 1983;84(2):125-32.
4. Peck S, Peck L, Kataja M. The palatally displaced canine as a dental anomaly of genetic origin. Angle Orthod 1994;64(4):249-56.
5. Brown LJ, Lownie JF. A suturing technique for the prevention of subperiosteal haematomas in the palate. J Dent 1975;3(5):203-4.
6. Sailer HF, Gion F. Oral Surgery for the General Dentist, 1st ed. New York: Thieme; 1999. p. 119-21.
7. Kruger E, Worthington P. Oral Surgery in Dental Practice, 1st ed. Chicago: Quintessence Publication Co.; 1981. p. 224.
8. Clarck HB. Practical Oral Surgery, 3rd ed. Philadelphia: Lea & Febiger Co.; 1965. p. 209.
9. Zilberman Y, Cohen B, Becker A. Familial trends in palatal canines, anomalous lateral incisors, and related phenomena. Eur J Orthod 1990;12(2):135-9.
10. Laskin DM. Oral and Maxillofacial Surgery, 1st ed., Vol. 2. St. Louis: C.V. Mosby Company; 1985. p. 89.
11. Dimitroulous G. Synopsis of Minor Oral Surgery, 1st ed.
Figure 6: The suture is tied in buccal aspect, between the neck of the teeth and overmucosal buccal hole.

9
Journal of International Oral Health 2015; 7(10):6-9Bone suture technique … Rahpeyma A et al
Guildford: Bidles Ltd.; 1997. p. 66.12. Christofides EA, Richards P, Wall SA. Late subperiosteal
hematomata associated with craniofacial surgery. J Craniofac Surg 2006;17(2):390-4.
13. Atalla ML, McNab AA, Sullivan TJ, Sloan B. Nontraumatic subperiosteal orbital hemorrhage. Ophthalmology 2001;108(1):183-9.
14. Mizuno K, Mineo K, Tachibana T, Sumi M, Matsubara T, Hirohata K. The osteogenetic potential
of fracture haematoma. Subperiosteal and intramuscular transplantation of the haematoma. J Bone Joint Surg Br 1990;72(5):822-9.
15. Martinez-Lage JF, Esteban JA, Martinez Perez M, Poza M. Craniostenosis secondary to calcified subperiosteal hematoma: Case report. Neurosurgery 1984;15(5):703-4.
16. Wood NK, Goaz PW. Differential Diagnosis of Oral and Maxillofacial Lesions, 5th ed. Missouri: Mosby Co.; 1997. p. 445.