bone healing in critical-size defects treated with bioactive glass/calcium sulfate: a histologic and...
TRANSCRIPT

Bone healing in critical-size defectstreated with bioactive glass/calciumsulfate: a histologic and histometricstudy in rat calvaria
Flavia A. C. FurlanetoMaria J. H. NagataStephen E. FuciniTatiana M. DeliberadorTetuo OkamotoMichel R. Messora
Authors’ affiliations:Flavia A. C. Furlaneto, Maria J. H. Nagata, TatianaM. Deliberador, Tetuo Okamoto, Michel R.Messora, Division of Periodontics, Department ofSurgery and Integrated Clinic, Dental School ofAracatuba, University of the State of Sao Paulo‘‘Julio de Mesquita Filho’’ – UNESP, BrazilStephen E. Fucini, Private Practice, Hanover,NH, USA.
Correspondence to:Maria Jose Hitomi NagataRua Afonso Pena, 325 – Apt. 51CEP: 16010-370 Aracatuba, SP, BrazilTel.: þ55 18 3621 7932Fax: þ55 18 3621 7932e-mail: [email protected]
Key words: bioactive, bone regeneration, bone substitutes, calcium sulfate, glass
Abstract
Objective: The purpose of this study was to analyze histologically the influence of bioactive
glass (BG) with or without a calcium sulfate (CS) barrier on bone healing in surgically
created critical-size defects (CSD) in rat calvaria.
Material and methods: A CSD was made in each calvarium of 48 rats. They were divided
into three groups: C (control): blood clot only; BG: defect filled with BG; and BG/CS: defect
filled with BG covered by a CS barrier. Animals were euthanized at 4 or 12 weeks. Formation
of new bone was evaluated histomorphometrically.
Results: No defect completely regenerated with bone. BG particles were observed in
Groups BG and BG/CS at both periods of analysis. The thickness throughout the healing area
in Groups BG and BG/CS was similar to the original calvarium, while Group C presented a
thin connective tissue in the center of the defect in both periods of analysis. At 4 weeks,
Groups C and BG/CS presented significantly more bone formation than Group BG. No
significant differences were found between Groups C and BG/CS. At 12 weeks, no
significant differences in the amount of bone formation were observed among the three
groups. When comparing 4 and 12 weeks, there was a significant increase in new bone
formation within groups BG and BG/CS, but not C.
Conclusion: BG particles, used with or without a CS barrier, maintained the volume and
contour of the area grafted in CSD. However, they did not lead to a significant difference in
bone formation when compared with control at 12 weeks post-operative.
A variety of graft materials and bone sub-
stitutes have been placed in bony defects in
order to facilitate and/or promote bone
regeneration (Lang et al. 1999). The syn-
thetic materials, or alloplasts, have been
largely used for their unlimited availability
and because they do not require additional
surgery of a donor site (Topazian et al.
1971; Norton & Wilson 2002).
Among the group of synthetic materials
used as bone substitutes, particulate bioac-
tive glasses (BG) have been studied consid-
erably. They act by forming a chemical
union with the surrounded tissues (Hench
et al. 1971; Hench & Paschall 1973). The
bonding between BG and the surrounding
bone tissue is the result of a series of
interfacial reactions that lead to the forma-
tion of a Si-rich layer covered by a Ca–P
rich layer. It has been suggested that osteo-
blasts deposit the organic matrix of bone on
this Ca–P layer, and that the bonding
results from cross-linking between ionic
sites on the collagen and the mucopolysac-
charides with those of the Ca–P rich layer
(Hench & Paschall 1974). Besides being
osteoconductive (Schepers et al. 1991;
Furusawa et al. 1998; Froum et al. 2002),
Date:Accepted 15 May 2006
To cite this article:Furlaneto FAC, Nagata MJH, Fucini SE, DeliberadorTM, Okamoto T, Messora MR. Bone healing in critical-size defects treated with bioactive glass/calcium sulfate.A histologic and histometric study in rat calvaria.Clin. Oral Impl. Res. 18, 2007; 311–318doi: 10.1111/j.1600-0501.2006.01331.x
c� 2007 Blackwell Munksgaard 311

BG particles have demonstrated an osteos-
timulatory effect (Schepers et al. 1991;
Schepers & Ducheyne 1997; Furusawa
et al. 1998; Froum et al. 2002; Norton
& Wilson 2002). Their use with barriers,
such as calcium sulfate (CS; Camargo
et al. 2000; Sottosanti & Anson 2003;
Melo et al. 2005), has been suggested.
When CS was used as a barrier in
conjunction with other bone graft materi-
als, such as demineralized freeze-dried
bone allograft and autogenous bone graft,
it resulted in favorable bone and perio-
dontal responses (Sottosanti 1992; Kim
et al. 1998; MacNeill et al. 1999).
Camargo et al. (2000) clinically evalu-
ated the use of BG particles with a CS
barrier in extraction sites. According to
the authors, the combination of the two
materials was beneficial for preserving the
dimensions of the alveolar ridge follow-
ing extraction of teeth. Melo et al. (2005)
conducted a histomorphometric study in
rat tibias to evaluate the combination of
materials used by Camargo et al. (2000).
Surgically created bone defects were treated
with either BG, a CS barrier over the blood
clot or a combination of BG with a CS
barrier. The defects of the control group,
filled only with blood clot, presented sig-
nificantly more bone formation than the
defects of the experimental groups. These
results were attributed to the non-critical-
size nature of the surgically created defects.
The purpose of this study was to analyze
histologically the influence of BG with
or without a CS barrier on bone healing
in surgically created critical-size defects
(CSD) in rat calvaria.
Material and methods
Experimental model
Forty-eight 3–4-month-old, male rats (Rat-
tus norvegicus, albinus, Wistar) weighing
350–400 g (University of State of Sao Paulo
– UNESP, Dental School of Aracatuba,
Animal Care Unit) were used. The rats
were kept in a room with a 12 h light/dark
cycle and temperature between 22 and
241C. The experimental protocol was
approved by the UNESP – Dental School
of Aracatuba Institutional Animal Care
and Use Committee. They were randomly
assigned to one of three experimental
groups: Group C (control), Group BG
(BG implant; Biograns
, 3i Implant Innova-
tions Inc., Palm Beach Gardens, FL, USA)
and Group BG/CS (BG implant and CS
barrier; Calcigent Oral, Biomet Orthope-
dics Inc., Warsaw, IN, USA/3i Implant
Innovations Inc.).
Surgical procedure
Animals were anesthetized by an intra-
muscular injection of xylazine (6 mg/kg
body weight) and ketamine (70 mg/kg
body weight). After aseptic preparation, a
semilunar incision was made in the scalp
in the anterior region of the calvarium
allowing reflection of a full-thickness
flap in a posterior direction. A 5 mm in
diameter CSD was made with a trephine
(3i Implant Innovations Inc.) used in a
low-speed handpiece under continuous
sterile saline irrigation. The defect included
a portion of the sagittal suture. Reference
marks were made 2 mm anterior and 2 mm
posterior to the margins of the CSD, both
of which were located on a longitudinal
axis bisecting the surgical defect. The
marks were made using a small tapered
carbide fissure bur and then filled with
amalgam (Bosch et al. 1998; Fig. 1). Their
purpose was to allow identification of the
center line of the original defect during
laboratory processing and also to be used
as references to locate the original bone
margins of the surgical defect during histo-
metric analysis.
In Group C, the surgical defect was filled
with a blood clot only. In Group BG, the
surgical defect was filled with BG particles
(Biograns
). In Group BG/CS, it was filled
with BG particles (Biograns
) and covered
with a CS barrier (Calcigent Oral). The
BG particles were composed of 45% SiO2,
24.5% Na2O, 24.5% CaO and 6% P2O5
by weight percentages, and had a size range
limited to 300–355mm.
The soft tissues were then repositioned
and sutured to achieve primary closure
(Silk 4.0, Ethicon, Sao Paulo, SP, Brazil).
Each animal received an intramus-
cular injection of 24,000 IU penicillin
G-benzathine (Pentabioticon Veterinario
Pequeno Porte, Fort Dodges
Saude Animal
Ltd., Campinas, SP, Brazil) post-surgically.
Tissue processing
Each group of animals was divided into
two sub-groups for euthanasia at either
4 or 12 weeks post-operative. The area of
the original surgical defect and the sur-
rounding tissues were removed en bloc.
The blocks were fixed in 10% neutral
formalin, rinsed with water and then dec-
alcified in 16% ethylediaminetetraacetic
acid solution. After an initial decalcifica-
tion, each specimen was divided longitud-
inally into two blocks exactly along the
center line of the original surgical defect
using the amalgam reference marks. Trans-
verse cuts were made perpendicular to the
longitudinal axis at the medial edge of each
amalgam reference mark. Each specimen
then measured 9 mm in length along
the longitudinal axis running through the
center of the defect, allowing for identifica-
tion of the original surgical defect margins
during both histologic and histometric
evaluations (Fig. 2). After additional
decalcification, they were processed and
embedded in paraffin. Serial sections 6mm
thick were cut in a longitudinal direction
starting at the center of the original surgical
defect. The sections were stained with
either hematoxylin and eosin or Masson’s
Trichrome for analysis by light microscopy.
Histomorphometric analysis
Before the analysis, criteria were estab-
lished in order to conduct a more object-
ive evaluation of the acute (neutrophils)
and chronic (macrophages, lymphocytes
and plasma cells) inflammatory infiltrates.
The following criteria were used to describe
the inflammatory infiltrate in each field
using a light microscope with a � 40
objective: (a) light: 1–100 cells; (b) moder-
ate: 100–250 cells; and (c) intense: more
than 250 cells.
Four histologic sections, representing the
center of the original surgical defect, were
selected for the histologic and histomor-
phometric analyses in order to increase the
reliability of the data used in the statistical
analysis. The images of the histologic
Fig. 1. Critical-size defect (5 mm diameter) and the
two reference marks created on the calvarium.
Furlaneto et al . Bone healing with bioactive glass/calcium sulfate
312 | Clin. Oral Impl. Res. 18, 2007 / 311–318 c� 2007 Blackwell Munksgaard
sections were captured by a digital camera
connected to a light microscope with an
original magnification of � 32. The digital
images were saved on a computer and then
copied to ‘ImageLab 2000’ software (Dir-
acon Bio Informatica Ltd., Vargem Grande
do Sul, SP, Brazil), which was used for
histomorphometric analysis.
The following criteria, based in part on
the work of Melo et al. (2005), were used to
standardize the histomorphometric analy-
sis of the digital images:
(1) The total area (TA) to be analyzed
corresponded to the entire area of the
original surgical defect. This area
was determined by first identifying
the external and internal surfaces of
the original calvarium at the right and
left margins of the surgical defect, and
then connecting them with lines
drawn following their respective curva-
tures. The center of the histologic
section (considering its total length)
was localized and 2.5 mm were mea-
sured to the right and to the left of this
center point in order to determine the
limits of the original surgical defect
(Fig. 3). The newly formed bone area
(NFBA) and the areas of the remnants
of the implanted materials, named
bioactive glass area (BGA) (Fig. 3) and
calcium sulfate area (CSA), were deli-
neated within the confines of the TA.
(2) The TA was measured in mm2
and was considered 100% of the
area to be analyzed. The NFBA, the
BGA and the CSA were also measured
in mm2 and calculated as a percentage
of TA.
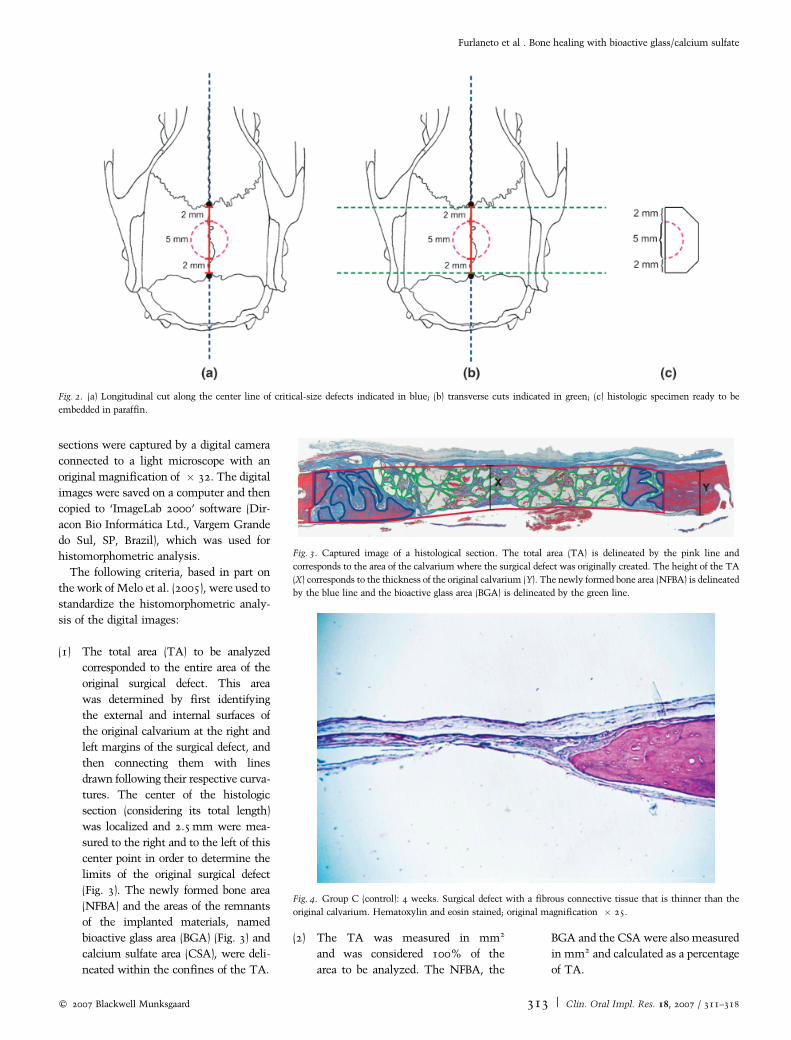
Fig. 2. (a) Longitudinal cut along the center line of critical-size defects indicated in blue; (b) transverse cuts indicated in green; (c) histologic specimen ready to be
embedded in paraffin.
Fig. 3. Captured image of a histological section. The total area (TA) is delineated by the pink line and
corresponds to the area of the calvarium where the surgical defect was originally created. The height of the TA
(X) corresponds to the thickness of the original calvarium (Y). The newly formed bone area (NFBA) is delineated
by the blue line and the bioactive glass area (BGA) is delineated by the green line.
Fig. 4. Group C (control): 4 weeks. Surgical defect with a fibrous connective tissue that is thinner than the
original calvarium. Hematoxylin and eosin stained; original magnification � 25.
Furlaneto et al . Bone healing with bioactive glass/calcium sulfate
c� 2007 Blackwell Munksgaard 313 | Clin. Oral Impl. Res. 18, 2007 / 311–318

Statistical analysis
The values of NFBA for each animal were
represented by the mean percentage of the
four histologic sections. These percentage
data were transformed into arccosine
for the statistical analysis. The significance
of differences between groups in relation
to NFBA was determined by an analysis of
variance, followed by a post hoc Tukey’s
test when the analysis of variance sug-
gested a significant difference between
groups (Po0.05). The values of BGA for
each animal in Groups BG and BG/CS and
of CSA in Group BG/CS were represented
by the mean percentage of the four histo-
logic sections. The proportion test at the
5% significance level was used to compare
the values of BGA between 4 and 12 weeks
post-operative in Group BG and in Group
BG/CS (Po0.05). The values of CSA
in Group BG/CS at both 4 and 12 weeks
post-operative were practically zero. There-
fore, statistical analysis was not performed
on this parameter.
Results
One specimen of Group BG/CS at 4 weeks
post-operative and one specimen of Group
BG/CS at 12 weeks post-operative were
lost because of problems encountered
during lab processing.
Qualitative histologic analysis
No surgical defect in any of the groups
completely regenerated with bone.
Group C (Control)
At 4 weeks, new bone formation was
restricted to areas close to the borders of
the surgical defect in most specimens. At
12 weeks, well-developed newly formed
bone surrounded by an osteoid matrix rich
in osteoblasts was observed in those areas.
In all specimens, at both 4 and 12 weeks,
the connective tissue in the central part
of the defect was thinner than the origi-
nal calvarium (Figs 4 and 5). It was
well vascularized and rich in fibroblasts
with oriented collagen fibers. The presence
of osteoid matrix was observed in some
areas. Light acute and chronic inflamma-
tory infiltrates were present throughout the
surgical defect. In a few specimens, areas
with an intense, predominantly chronic
inflammatory infiltrate were noted.
Group BG and Group BG/CS
Well-developed newly formed bone sur-
rounded by an osteoid matrix was observed
restricted to the borders of the surgical
defect in both periods of analyses. At
12 weeks, it extended toward the center
of the defect in a few specimens in Group
BG and in most specimens in Group BG/
CS. At 4 weeks, a large amount of BG
particles was distributed throughout the
defect and at 12 weeks, they were smaller
than those at 4 weeks. Most BG particles
presented with cracks, many of which had
an ingrowth of connective tissue within the
cracks and excavated centers, in both per-
iods of analysis (Fig. 6). Other particles
showed amorphous material in their exca-
vated centers instead (Fig. 7). In some
areas, BG particles were surrounded by a
fibroblast-rich connective tissue that
was organized and dense with the presence
of osteoblasts and osteoid matrix (Figs 8
and 9). In other areas, the surrounding
connective tissue was loose and not orga-
nized. In all specimens, BG particles and
the surrounding connective tissue formed
a strip with a thickness similar to that of
the original calvarium (Figs 10 and 11). In
Group BG/CS, minimal remnants of CS
were observed, sometimes surrounded by
Fig. 5. Group C (control): 12 weeks. Surgical defect with a fibrous connective tissue that is thinner than the
original calvarium. Masson’s Trichrome; original magnification � 25.
Fig. 6. Group BG/CS (bioactive glass/calcium sulfate): 4 weeks. Bioactive glass particles surrounded by
connective tissue that is also seen within cracks and excavated centers. Hematoxylin and eosin stained;
original magnification � 160.
Furlaneto et al . Bone healing with bioactive glass/calcium sulfate
314 | Clin. Oral Impl. Res. 18, 2007 / 311–318 c� 2007 Blackwell Munksgaard
newly formed bone. In Group BG/CS, in
both period of analyses and in Group BG at
4 weeks, light acute and chronic inflam-
matory infiltrates were observed in most
specimens, while a few demonstrated an
intense chronic inflammatory infiltrate
composed of lymphocytes, plasma cells
and histiocytes between the BG particles.
In Group BG, at 12 weeks, a light and
predominantly chronic inflammatory infil-
trate was dispersed throughout the defect.
Histometric and statistical analyses
The data normality and homogeneity of
variances were verified. Means and stan-
dard deviations of NFBA for each group, as
well as the comparison among the groups,
at 4 and 12 weeks post-operative are docu-
mented in Table 1. Table 2 demonstrates
the increased resorption of BG particles
from 4 to 12 weeks post-operative in
Groups BG and BG/CS.
Discussion
This study evaluated the influence of
BG particles (300–355mm) with or with-
out a CS barrier on the healing of CSD in
rat calvaria.
According to Bosch et al. (1998), the use
of large bone defects results in some incon-
veniences, such as inclusion of the sagittal
suture in the calvarial defect, thereby in-
troducing the connective tissue of the su-
ture in the evaluation of bone regeneration.
Because of the size of the calvaria of the
animals used in the present study, the
experimental defect could not be made
only in parietal bone. Therefore, a location
involving the sagittal suture was chosen in
order to standardize the experimental
model. Any possible effect from the inclu-
sion of connective tissue of the sagittal
suture would be present in all groups.
Similar experimental models that included
the sagittal suture have been reported in
other studies as well (Brunel et al. 1996;
Mardas et al. 2002, Kim et al. 2004).
The outcome of any type of regenerative
procedure is strongly dependent upon the
available space under the mucoperiosteal
flap (Wikesjo & Selvig 1999). In the pre-
sent study, the flap collapse seen in Group
C was probably prevented by the use of BG
particles in Groups BG and BG/CS, similar
to what was observed by Sculean et al.
(2002). One of the advantages of BG is
the in situ formation of a calcium-phos-
phate shell, which serves to maintain the
overall volume of the particle–bone matrix
(Furusawa et al. 1998). This is an extre-
mely advantageous property for a bone aug-
mentation material where predictable
modification of the defect or deficiency is
required.
In the present study, osteoid matrix rich
in osteoblasts and fibrous connective tissue
were observed surrounding most BG parti-
cles. These collagen fibers may indicate
matrix development for future mineraliza-
tion and bone formation (Wheeler et al.
1997). This mineralization and bone
formation might have been observed if
the present study had included a longer
period of healing. Cracks and excavated
centers were observed in the BG particles,
with ingrowth of cells, probably undiffer-
entiated mesenchymal cells, at both 4
and 12 weeks post-operative, as found
in other studies (Furusawa et al 1998;
Cordioli et al. 2001; Tadjoedin et al.
2002). However, the osteostimulatory
effect described in other histological
human and animal studies (Schepers et al.
1991; Schepers & Ducheyne 1997;
Furusawa et al. 1998; Froum et al. 2002;
Norton & Wilson 2002) was not seen in
any of the specimens of the present study
at either 4 or 12 weeks post-operative.
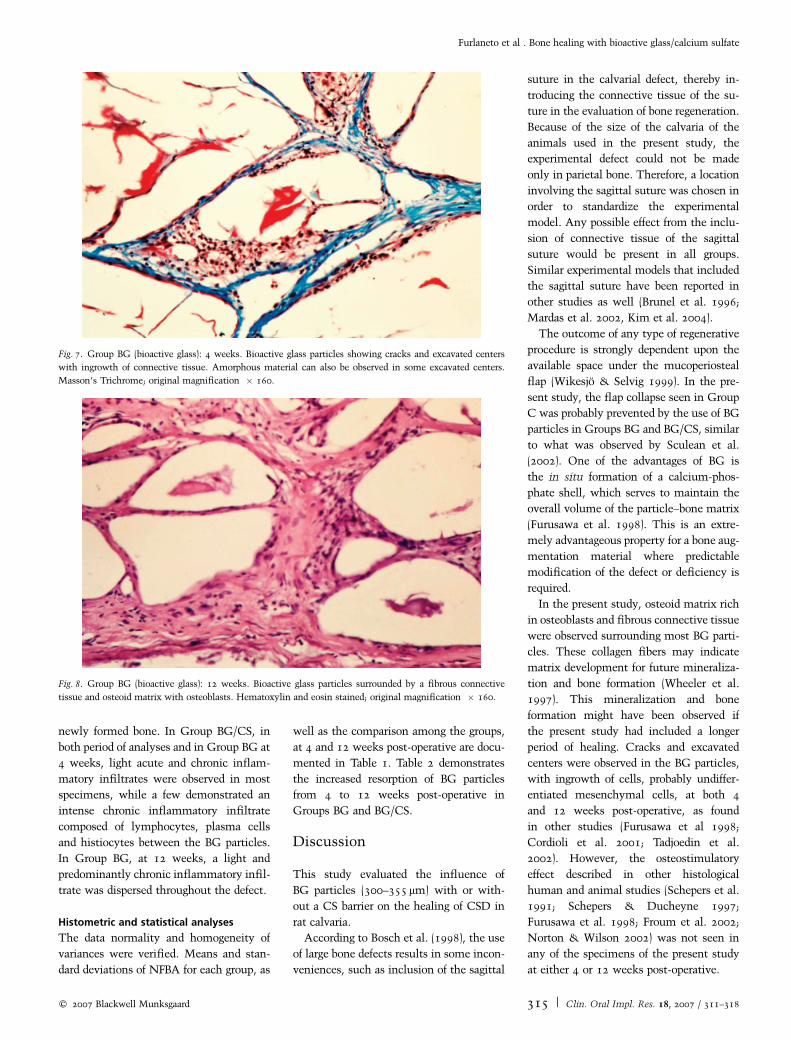
Fig. 7. Group BG (bioactive glass): 4 weeks. Bioactive glass particles showing cracks and excavated centers
with ingrowth of connective tissue. Amorphous material can also be observed in some excavated centers.
Masson’s Trichrome; original magnification � 160.
Fig. 8. Group BG (bioactive glass): 12 weeks. Bioactive glass particles surrounded by a fibrous connective
tissue and osteoid matrix with osteoblasts. Hematoxylin and eosin stained; original magnification � 160.
Furlaneto et al . Bone healing with bioactive glass/calcium sulfate
c� 2007 Blackwell Munksgaard 315 | Clin. Oral Impl. Res. 18, 2007 / 311–318

BG particles were observed in Groups
BG and BG/CS in both periods of analysis,
confirming the slow process of resorption
of this material observed in histologic stu-
dies in humans (Tadjoedin et al. 2000,
2002; Cordioli et al. 2001; Norton &
Wilson 2002) and in animals (Schepers &
Ducheyne 1997; Cancian et al. 1999; Stav-
ropoulos et al. 2003). Schepers & Duch-
eyne (1997) observed the presence of BG
particles up to 24 months after their
implantation in surgically created bony
defects in mandibles of dogs.
At 4 weeks post-operative, Groups C
and BG/CS showed significantly greater
bone formation than Group BG (Table 1).
No differences were found between Groups
C and BG/CS. According to MacNeill
et al. (1999), graft materials that require
extended time periods for complete resorp-
tion will reduce the total amount of newly
formed bone due to their continued pre-
sence. The slow resorption of the BG
particles probably accounted for the greater
amount of newly formed bone observed in
Group C when compared with Group BG,
as also observed in previous studies by
MacNeill et al. (1999) and Melo et al.
(2005). In this study, Group BG/CS re-
ceived less BG particles than Group BG
because of the space occupied by the CS
barrier. Thus, in a similar manner, the
presence of a greater amount of a slowly
resorbed material in Group BG may help to
explain why Group BG/CS presented sig-
nificantly more bone formation than Group
BG in this study. Furthermore, the rapid
resorption of CS observed in the present
study probably allowed early ingress of os-
teoprogenitor cells, thus accelerating bone
regeneration. An almost complete resorp-
tion of the CS barrier was observed at
4 weeks post-operative. According to the
results observed by Pecora et al. (1997) in a
histologic study conducted in rats, the pre-
sence of the CS barrier for 3 weeks was
enough to halt ingrowth of soft connective
tissue and promote osseous formation. It
should be remembered that it is not possible
to know exactly how long the CS main-
tained its function as a barrier in the present
study. Thus, additional histologic studies
are necessary to evaluate the resorptive
process of CS when used as a barrier.
At 12 weeks post-operative, Group BG/
CS presented more bone formation than
Groups C and BG, although there were no
significant differences among the three
groups (Table 1). A statistically significant
increase in the amount of newly formed
bone was observed in the groups treated
with BG (Groups BG and BG/CS) from 4 to
12 weeks post-operative, probably due to
the combination of new bone formation
with the material resorption process (Tad-
joedin et al. 2000). The decrease in the
percentage values of BGA in Groups BG
and BG/CS from 4 to 12 weeks indicates
a clear trend, although the difference
within each group was not statistically
significant.
The time necessary for complete resorp-
tion of BG particles remains unknown.
Norton & Wilson (2002) stated that this
material can be used for filling dentoalveolar
defects and/or ridge preservation at the site
of extraction sockets before placement of
dental implants. According to the authors,
even though the BG particles are slowly
replaced by bone, there was no negative
impact on the clinical success of dental
implants placed into the graft/tissue mass.
In this study, the finding that there was
an insignificant increase in new bone for-
mation in Group C from 4 to 12 weeks
post-operative corroborates the findings of
Takagi & Urist (1982). They surgically
Fig. 9. Group BG/CS (bioactive glass/calcium sulfate): 12 weeks. Bioactive glass particles surrounded by a
fibrous connective tissue and osteoid matrix with osteoblasts. Hematoxylin and eosin stained; original
magnification � 160.
Fig. 10. Group BG (bioactive glass): 12 weeks. Bioactive glass particles and surrounding connective tissue
forming a strip with a thickness similar to that of the original calvarium. Hematoxylin and eosin stained;
original magnification � 25.
Furlaneto et al . Bone healing with bioactive glass/calcium sulfate
316 | Clin. Oral Impl. Res. 18, 2007 / 311–318 c� 2007 Blackwell Munksgaard

created CSDs in rat calvaria and found that
bone formation had terminated at 4 weeks
post-operative.
Within the limits of this study, it can be
concluded that BG particles, used either
with or without a CS barrier, maintained
the volume and contour of the area grafted
in CSD. However, they did not lead to a
significant difference in bone formation
when compared with control at 12 weeks
post-operative.
Acknowledgements: This study was
partially supported by 3i Implant
Innovationss
. The authors thank
Johnson & Johnson (Sao Jose dos
Campos, SP, Brazil) for donating the
suture materials.
References
Bosch, C., Melsen, B. & Vargervik, K. (1998) Im-
portance of the critical-size bone defect in testing
bone-regeneration materials. Journal of Craniofa-
cial Surgery 9: 310–316.
Brunel, G., Piantoni, P., Elharar, F., Benque, E.,
Marin, P. & Zahedi, S. (1996) Regeneration of rat
calvarial defects using a bioabsorbable membrane
technique: influence of collagen cross-linking.
Journal of Periodontology 67: 1342–1348.
Camargo, P.M., Lekovic, V., Weinlaender, M.,
Klokkevold, P.R., Kenney, E.B., Dimitrijevic, B.,
Nedic, M., Jancovic, S. & Orsini, M. (2000)
Influence of bioactive glass on changes in alveolar
process dimensions after exodontia. Oral Surgery,
Oral Medicine, Oral Pathology, Oral Radiology
and Endodontics 90: 581–586.
Cancian, D.C.J., Hochuli-Vieira, E., Marcantonio,
R.A.C. & Marcantonio Junior, E. (1999) Use of
Fig. 11. Group BG/CS (bioactive glass/calcium sulfate): 12 weeks. Bioactive glass particles and surrounding
tissues forming a strip with a thickness similar to that of the original calvarium. Hematoxylin and eosin
stained; original magnification � 25.
Table 1. Mean percentage of newly formed bone area (NFBA) within the area of thesurgically created defect with comparison among the groups, 4 and 12 weeks post-operative
Group n Mean-NFBA(%) 4 weeks
Standarddeviation4 weeks
Mean-NFBA(%) 12 weeks
Standarddeviation12 weeks
C 8 22.04 ad � 5.14 26.88 ac � 11.83BG 8 9.21 b � 3.81 21.02 ac � 9.76BG/CS 7 19.17 a � 11.61 30.40 cd � 14.28
Same letters indicate that there is no statistical difference among the groups (P40.05).
C, control; BG, bioactive glass; BG/CS, bioactive glass/calcium sulfate.
Table 2. Mean percentage of bioactive glass area (BGA) within the area of the surgicallycreated defect for Groups BG and BG/CS with comparison between 4 and 12 weeks post-operative
Group n Mean-BGA(%) 4 weeks
Standarddeviation4 weeks
Mean-BGA(%) 12 weeks
Standarddeviation12 weeks
Proportiontest
P value
BG 8 56.18 � 6.06 20.45 � 7.74 0.27 0.6056BG/CS 7 19 � 11.75 8.26 � 7.36 0.58 0.445
BG, bioactive glass; BG/CS, bioactive glass/calcium sulfate.
Furlaneto et al . Bone healing with bioactive glass/calcium sulfate
c� 2007 Blackwell Munksgaard 317 | Clin. Oral Impl. Res. 18, 2007 / 311–318

BioGran and Calcitite in bone defects: histologic
study in monkeys (Cebus apella). International
Journal of Oral & Maxillofacial Implants 14:
859–864.
Cordioli, G., Mazzocco, C., Schepers, E., Brugnolo,
E. & Majzoub, Z. (2001) Maxillary sinus
floor augmentation using bioactive glass
granules and autogenous bone with simultaneous
implant placement. Clinical and histological
findings. Clinical Oral Implants Research 12:
270–278.
Froum, S., Cho, S., Rosenberg, E., Rohrer, M. &
Tarnow, D. (2002) Histological comparison of
healing extraction sockets implanted with bioac-
tive glass or demineralized freeze-dried bone
allograft: a pilot study. Journal of Periodontology
73: 94–102.
Furusawa, T., Mizunuma, K., Yamashita, S. &
Takahashi, T. (1998) Investigation of early bone
formation using resorbable bioactive glass in the
rat mandible. International Journal of Oral &
Maxillofacial Implants 13: 672–676.
Hench, L.L. & Paschall, H.A. (1973) Direct chemi-
cal bond of bioactive glass–ceramic materials to
bone and muscle. Journal of Biomedical Materials
Research 7: 25–42.
Hench, L.L. & Paschall, H.A. (1974) Histochemical
responses at a biomaterial’s interface. Journal
of Biomedical Materials Research Symposium
5: 49–64.
Hench, L.L., Splinter, R.J., Allen, W.C. & Greenlee,
T.K. (1971) Bonding mechanisms at the interface
of ceramic prosthetic materials. Journal of Biome-
dical Materials Research 2: 117–141.
Kim, C.K., Kim, H.Y., Chai, J.K, Cho, K.S., Moon,
I.S., Choi, S.H., Sottosanti, J.S. & Wikesjo, U.M.
(1998) Effect of a calcium sulfate implant with
calcium sulfate barrier on periodontal healing
in 3–wall intrabony defects in dogs. Journal of
Periodontology 69: 982–988.
Kim, S.Y., Kim, S.G., Lim, S.C. & Bae, C.S. (2004)
Effects on bone formation in ovarectomized rats
after implantation of tooth ash and plaster of
Paris mixture. International Journal of Oral and
Maxillofacial Surgery 62: 852–857.
Lang, N.P., Becker, W. & Karring, T. (1999) For-
macao do osso alveolar. In: Lindhe, J., ed. Tratado
de periodontia clınica e implantologia oral.
3rd edition, 665–689. Rio de Janeiro: Guanabara
Koogan.
MacNeill, S.R., Cobb, C.M., Rapley, J.W., Glaros,
A.G. & Spencer, P. (1999) In vivo comparison of
synthetic osseous graft materials: a preliminary
study. Journal of Clinical Periodontology 26:
239–245.
Mardas, N., Kostopoulos, L. & Karring, T. (2002)
Bone and suture regeneration in calvarial defects
by e-PTFE-membranes and demineralized bone
matrix and the impact on calvarial growth:
an experimental study in the rat. The Journal
of Craniofacial Surgery 13: 453–464.
Melo, L.G.N., Nagata, M.J.H., Bosco, A.F., Ribeiro,
L.L.G. & Leite, C.M. (2005) Bone healing in
surgically created defects treated with either
bioactive glass particles, a calcium sulfate barrier,
or a combination of both materials. A histological
and histometric study in rat tibias. Clinical Oral
Implants Research 16: 683–691.
Norton, M.R. & Wilson, J. (2002) Dental implants
placed in extraction sites implanted with bioactive
glass: human histology and clinical outcome.
International Journal of Oral & Maxillofacial
Implants 17: 249–257.
Pecora, G., Andreana, S., Margarone, J.E., Covani,
U. & Sottosanti, J.S. (1997) Bone regeneration
with a calcium sulfate barrier. Oral Surgery,
Oral Medicine, Oral Pathology, Oral Radiology
and Endodontics 84: 424–429.
Schepers, E., De Clercq, M., Ducheyne, P. &
Kempeneers, R. (1991) Bioactive glass particulate
material as a filler for bone lesions. Journal of
Oral Rehabilitation 18: 439–452.
Schepers, E.J. & Ducheyne, P. (1997) Bioactive glass
particles of narrow size range for the treatment of
oral bone defects: a 1–24 month experiment with
several materials and particle sizes and size ranges.
Journal of Oral Rehabilitation 24: 171–181.
Sculean, A., Barbe, G., Chiantella, G.C., Arweiler,
N.B., Berakdar, M. & Brecx, M. (2002) Clinical
evaluation of an enamel matrix protein derivative
combined with a bioactive glass for the treatment
of intrabony periodontal defects in humans.
Journal of Periodontology 73: 401–408.
Sottosanti, J.S. (1992) Calcium sulfate: a biodegrad-
able and a biocompatible barrier for guided tissue
regeneration. Compendium of Continuing
Education in Dentistry 13: 226–234.
Sottosanti, J.S. & Anson, D. (2003) Using calcium
sulfate as a graft enhancer and membrane barrier.
Dental Implantology Update 14: 1–8.
Stavropoulos, A., Kostopoulos, L., Nyengaard, J.R.
& Karring, T. (2003) Deproteinized bovine bone
(Bio-Osss
) and bioactive glass (Biograns
) arrest
bone formation when used as an adjunct to guided
tissue regeneration (GTR): an experimental study
in the rat. Journal of Clinical Periodontology 30:
636–643.
Tadjoedin, E.S., De Lange, G.L., Holzmann, P.J.,
Kuiper, L. & Burger, E.H. (2000) Histological
observations on biopsies harvested following sinus
floor elevation using a bioactive glass material
of narrow size range. Clinical Oral Implants
Research 11: 334–344.
Tadjoedin, E.S., De Lange, G.L., Lyaruu, D.M.,
Kuiper, L. & Burger, E.H. (2002) High concentra-
tions of bioactive glass material (BioGran)
vs. autogenous bone for sinus floor elevation:
histomorphometrical observations on three split
mouth clinical cases. Clinical Oral Implants
Research 13: 428–436.
Takagi, K. & Urist, M.R. (1982) The reaction of the
dura to bone morphogenetic protein (BMP) in
repair of skull defects. Annals of Surgery 196:
100–109.
Topazian, R.G., Hammer, W.B., Boucher, L.J.
& Hulbert, S.F. (1971) Use of alloplastics for
ridge augmentation. Journal of Oral Surgery 29:
792–798.
Wheeler, D.L., Stokes, K.E., Park, H.M. & Hollin-
ger, J.O. (1997) Evaluation of particulate Bioglasss
in a rabbit radius ostectomy model. Journal of
Biomedical Material Research 35: 249–254.
Wikesjo, U.M.E. & Selvig, K.A. (1999) Periodontal
wound healing and regeneration. Periodontology
2000 19: 21–39.
Furlaneto et al . Bone healing with bioactive glass/calcium sulfate
318 | Clin. Oral Impl. Res. 18, 2007 / 311–318 c� 2007 Blackwell Munksgaard