board of directors public meeting - amazon web services · (chief financial officer /dr tim...
TRANSCRIPT

Board of Directors Public Meeting Board Room, The Royal Marsden, Chelsea
Wednesday 1st June 2016, 10am – 12pm
Agenda 1. Apologies for Absence None
2. Declarations of Interest (All)
Verbal
3. Minutes of Public Board Meeting held on the 23rd March 2016 (Chairman)
Enclosed
4. Report from the Chief Nurse and Medical Director 4.1. Senior Medical Appointments 4.2. Annual Medical Revalidation Report 4.3. Junior Doctors Briefing (Medical Director) 4.4. Initial feedback on CQC inspection 4.5. Nurse revalidation (Chief Nurse)
Enclosed Enclosed Enclosed
Verbal Enclosed
5. Review of the Trust Balanced Board Scorecard 5.1. KPIs for Q4 5.2. Proposed KPIs for 2016/17 (Chief Operating Officer)
Enclosed Enclosed
6. IM&T Strategy (Chief Financial Officer /Dr Tim Wigmore, Chief Clinical Information Officer)
Enclosed
7. Quality and Performance 7.1. Quality Account for April 2016 7.2. Duty of Candour Report 2015/16 (Chief Nurse)
Enclosed Enclosed
8. Financial Performance Report for 1 month ending April 2016 (Chief Financial Officer)
Enclosed
9.
Audit and Finance Committee Annual Report (Ian Farmer, Non-Executive Director)
Enclosed
10. Board Assurance Framework (Nancy Hallett, Non-Executive Director)
Enclosed
11. Trust Membership Report – for information
Enclosed
12. Any other business
Date of next meeting: 21st September 2016, 10am – 12pm


Minutes of The Royal Marsden Board of Directors Public Meeting Wednesday 23rd March 2016 Board Room, Chelsea
Present R. Ian Molson Chairman Cally Palmer Chief Executive Ian Farmer Non-Executive Director Dame Nancy Hallett Non-Executive Director Professor Dame Janet Husband Non-Executive Director Richard Turnor Non-Executive Director Professor Paul Workman Non-Executive Director Dr. Liz Bishop Chief Operating Officer Dr. Shelley Dolan Chief Nurse Professor Nick van As Medical Director Marcus Thorman Chief Financial Officer In Attendance: Syma Dawson (minutes) Trust Secretary Nina Singh Director of Workforce – item 6 only The meeting was quorate.
1/15 Apologies for absence None.
2/15 Minutes of the Public Board held on the 22nd September 2015 The minutes were approved as an accurate record.
3/15 Declarations of Interest No declarations of interest were made.
4/15 Board Self-Assessment The Chairman reminded the Board of its decision to conduct a rigorous self-assessment process based on the relevant guidance from Monitor instead of an external review of governance. He thanked the Trust Secretary and Board members for their efforts in completing this exercise. It was reported that the results were positive overall, particularly in relation to the Board’s understanding and confidence on quality issues and matters which are fundamental to the Board’s obligations. In terms of self-improvement, it is agreed that Board members could benefit from a more formal training and development programme which the Trust Secretary will review with the Chairman. The Chair of the Audit and Finance Committee, Ian Farmer, commented that the Audit and Finance Committee would be conducting a similar self-assessment in due course with the Trust Secretary’s assistance. The Board noted the results of its self-assessment process and in particular, the actions relating to Board development.
5/15 Finance 5.1. Financial Performance Report for 11 months ending February 2016 The Chief Financial Officer (CFO) reported on the Trust’s reduced capital spend and variance of £2.6m against the Financial Plan. He explained the Trust’s income position which has

Page 2 of 4
benefitted from Trust efforts to reduce agency spend. Debt levels in Private Care have stabilised at £20m despite overall income increasing. The Trust is expecting a break even position at the end of the year. The Board noted the Financial Performance Report for 11 months ending February 2016. 5.2. Financial Plan 2016/17 The CFO presented the report and reminded the Board that it has already received the draft Financial Plan which was submitted on the 8th February with a view that the final Plan will be submitted on the 11th April 2016. He reported that the timeline for submission has been brought forward and in light of the Board meeting schedule, requested that authority is delegated to the Audit and Finance Committee to approve the final version of the Financial Plan 2016/17 on behalf of the Board. The regulatory requirements to submit a one year operational plan as well as a five year Sustainability and Transformation Plan were noted. With regards to the latter, due to a lack of clarity on Monitor’s part, the Trust has submitted its plan based on the national submission for specialist trusts. In addition, Monitor is offering the Trust £1.5m contribution to achieve a surplus of £5.6m and achieve the conditions specified. The Board discussed the position, including the impact this will have on the Trust’s Capital Plan as well as the Cancer Vanguard programme. The CFO expressed his concern about the growing funding gap because of medical equipment (replacement) needs, IT development and backlog maintenance costs. The CFO also highlighted the risk of not signing contracts with Commissioners as the Trust has not yet received an offer for 2016/17 because discussions are taking place on activity and cost levels. If contracts are not agreed and signed by the 15th April 2016 then negotiations will move to the arbitration stage. The CFO also reported on the position in Private Care, the BRC risk if the Trust does not achieve renewal of this and the financial impact of junior doctor contract negotiations which is yet to be confirmed. A discussion ensued about the efficiency programme which the Transformation Board is closely monitoring through its key work streams with help and support from the new Clinical Business Units. It was agreed that a report regarding the work and progress of the Transformation Board would come back to the Board at a future meeting. The CFO gave the Board assurance that according to a Deloitte report, the Trust benchmarks well on its financial performance in comparison with other Trusts. The Trust still maintains its Risk Rating of ‘3’ which Monitor is aware of and has accepted. The Board agreed to delegate authority to the Audit and Finance Committee in reviewing and approving the final Financial Plan on behalf of the Board prior to submission on the 11th April 2016. The Board also agreed to not pursue the £5.6m STP Fund and the conditions which must be satisfied in order to receive the £1.5m contribution from NHS England due to concerns that these are not achievable in light of the current financial climate. A briefing on the Transformation Board’s work and progress, particularly in relation to targeting efficiencies within the Trust is to be presented to the Board at a future meeting.

Page 3 of 4
6/15 Quality and Performance 6.1. Key Performance Indicators Q3 The Chief Operating Officer reported the Trust’s ongoing challenge with the 62 day target and commented on Trust efforts to address this issue. The Trust is currently reviewing the Board scorecard metrics. Any proposals to change these will be presented to the Board by June 2016. Suggestions or comments from Board members prior to this are welcome. The Board discussed the new scorecard and possible integration of the CQC categories of performance measurement. The Chief Executive noted that the Trust needs to consider not only the CQC standards but also national standards and policy changes around cancer. Research metrics will also be reviewed as this is critical to a research active centre. It was agreed that the Chief Nurse would review the information presented to the Board about complaints to ensure it provides the correct type and level of information the Board receives. The Board noted the Trust KPIs for Quarter 3. It was agreed that the revised Board scorecard will be presented to the Board at its meeting in June 2016 which will include a revision of the complaints metric, consideration of the new CQC categories as well as the information needs of the Board. 6.2. NQB Safer Staffing Report The Chief Nurse explained that the NQB Safer Staffing Report is a mandatory report for Boards following issues arising from Mid-Staffordshire and Morecambe Bay. She explained the tool which the Trust uses to record the information and how this makes benchmarking difficult. However, the Trust will be switching to a different tool this year which will help address this issue as recommended by NICE. She was pleased to report that the Trust was top in England for the amount of time band 5 nurses directly spent with patients. However, indirect time particularly spent on documentation varied across the Trust but in some areas was higher than the national average. The enclosed report shows that the Trust is well staffed and above the national average with a richer skill mix of band 6 nurses. The Key Performance Indicators on ward nursing reveal the areas where the Trust is doing well but also those areas where the Trust may be short staffed. The Chief Nurse proposed that once the report has been finalised, this will be presented to the Board Sub-Committees with any recommended changes in staffing. The Board noted the results of the NQB Safer Staffing Report. 6.3. Quality Accounts for January and February 2016 The Chief Nurse reported on healthcare associated infections. It was noted that there were no MRSA cases to report. The Trust has met its target in relation to patient falls and is seeing more medication errors being reported in the category of “less than significant harm”. Work is underway on pressure ulcers in the community and quality outcomes have improved as a result of the pharmacy partnership with Boots. An action plan has been established as a result of the Friends and Family Test results. With regard to recruitment efforts, the Chief Nurse was pleased to report that the Trust attended another national recruitment day where 28 nurses attended resulting in 15 staff appointments. The Chief Nurse assured the Board that she does not expect any decision to leave Europe will pose a risk to nursing given the recent national effort to reduce recruitment restrictions for candidates from abroad. The Trust is carefully reviewing the exit interview feedback to better understand the reasons
Page 4 of 4
for nurses leaving the Trust. The Board noted the Quality Accounts for January and February 2016.
6/15 Equality Report The Director of Workforce attended for this item and presented the enclosed report. The following points were highlighted:
• Equality Objectives for both patients and staff have been established; • A survey of the experiences of patients over the age of 65 has been conducted as well
as a survey on capacity for care and patients over the age of 75 with dementia, the results of which can be found on page 27;
• A mediation service has been launched to support staff in conflict at work. The Board discussed the Workforce Equality Standards and the statistics on ethnicity in recruitment. It was also noted that a system of mentorship by the members of the Leadership Team will be established with specific encouragement to BME staff. The Board noted the Equality Report and in particular, the Equality Objectives and Trust’s aim to provide a fair and inclusive working and patient environment for staff and patients.
7/15 Any other business
No other business was raised.
Signed as a true and accurate record Chaired by: Date:

BOARD PAPER SUMMARY SHEET
Date of Meeting:
1st June 2016
Agenda item 4.1
Title of Document: Senior Medical Appointments
To be presented by
Medical Director
Executive Summary The attached report provides the Board with the summary of senior medical appointments since January 2016. There have been three appointments since that time:
1) Honorary Consultant in Medical Oncology/Clinical Scientist (February 2016)
2) Consultant Histopathology post (April 2016)
3) Consultant Medical Oncologist for Drug Development Unit (May 2016)
Recommendations The Trust Board is asked to note these appointments. Author: Nina Singh, Director of Workforce
Contact Number or E-mail: 2141
Date: 17th May 2016


Senior Medical Appointments
1. Introduction
The purpose of this report is to provide the Trust Board with an update on senior medical appointments.
2. Senior medical appointments
Since January 2016, the following consultant appointments have been made: Dr Chiara BRACONI – Honorary Consultant in Medical Oncology/Clinical Scientist. She started on the 31st March 2016. Dr Braconi was appointed to the post of Clinical Scientist by the Institute of Cancer Research on a full time permanent contract. Her role requires her to undertake approximately 20% of her at The Royal Marsden through an honorary contract. An AAC was arranged to enable her to fulfil the duties as an NHS consultant in accordance with the NHS guidelines. Dr Braconi qualified as a doctor in Italy in 2002 and completed a PhD in Oncology in 2009. She obtained her CCT in 2006 and has been on the GMC Specialist Register since 2006. She has a strong background in research. She has trained in research institutions in Italy, US and the UK. Her PhD was done jointly with Italy and the University of Ohio, where she spent time until it was completed. Dr Monica TERLIZZO – Consultant Histopathologist The Trust has been fortunate in making an appointment in Histopathology, despite this speciality being a difficult to recruit to nationally. Dr Terlizzo qualified as a doctor in Italy in 1997 and completed her FRCPath qualification in 2007. She is on the GMC Specialist Register. She has worked as a consultant for 8 years in both Italy and the UK. Her specialist interest is in Gastrointestinal and Hepatobiliary pathology. Her current position is consultant at St Helen and Knowsley Teaching Hospitals NHS Trust where she has worked for the past year. Her previous positions were at the Royal Liverpool University Hospital and the University Hospital Aintree where she worked as a Consultant. She also competed 3.5 years as a Specialist Registrar in the UK whilst working towards her CCT. Dr Juanita LOPEZ – Consultant Medical Oncologist, Drug Development Unit Dr Lopez qualified as a doctor at Cambridge University in 2001; she completed her MRCP in 2005, her PhD in 2011 and is on the GMC Specialist Register with CCT in Medical Oncology. She has a strong research background. She is currently working as a locum consultant in medical oncology at the RM and has been in post since August 2015. Prior to this post she was Senior Clinical Fellow to Prof De Bono at the RMH from September 2014-August 2015. Her previous posts were part of the Specialist Registrar rotation in Oncology at the RM, Guy’s and St Thomas’ hospital, St Georges and Maidstone. The Board is asked to note these appointments.


BOARD PAPER SUMMARY SHEET
Date of Meeting:
1st June 2016
Agenda item 4.2.
Title of Document: Annual Medical Revalidation Report
To be presented by
Medical Director
Executive Summary The Board is required by the NHS to receive an annual report on medical appraisal and revalidation. As at 31st March 2016, there were 281 doctors with a prescribed connection to The Royal Marsden NHS Foundation Trust. Of those, 79 are honorary doctors employed by the Institute of Cancer Research (ICR). The Trust is responsible for supporting these doctors with their appraisal and revalidation. There has been a significant improvement in the appraisal completion rate from 73% in 2014-15 to 89% in 2015-16, which exceeded the in-year target of 85%. The consultant appraisal rate was 92% for 2015-16. 78 positive recommendations were made to the General Medical Council (GMC). An Appraisal and Revalidation Lead was appointed in May 2016 to support the Medical Director in his role as the Responsible Officer for the organisation. The focus of this role will be in maintaining or further improving the appraisal completion rate particularly for non-consultant grades and improving the quality of the appraisal process. The improvement plan for 2016-17 is shown at appendix A. Recommendations The Board is asked to:
1) Note progress with implementation of appraisal and revalidation in 2015; 2) Note key areas for improvement and detailed action plan; 3) Approve the Chief Executive and Chair to sign off a statement of compliance by 31
August 2016. Author: Nina Singh, Director of Workforce
Contact Number or E-mail: Nina. [email protected]
Date: 17 May 2016


1
Annual Medical Revalidation Report
1. Introduction
The purpose of this report is to provide assurance that there is a system in place that meets General Medical Council (GMC) requirements for the appraisal and revalidation of all medical staff for whom the Trust is the Designated Body. The Framework of Quality Assurance for Responsible Officers and Revalidation (2014) requires organisations employing doctors (Designated Bodies) to receive annual reports at the Board on the implementation of medical revalidation and submit an annual statement of compliance to their higher level responsible officers, which in the case of London Trusts is NHS England South Region. This report follows the format prescribed by NHS England.
2. Background
Medical Revalidation was launched in 2012 to strengthen the way that doctors are regulated, with the aim of improving the quality of care provided to patients, improving patient safety and increasing public trust and confidence in the medical system. Each NHS provider is required to have a Responsible Officer, who leads on appraisal and revalidation and makes recommendation to the GMC. This role is undertaken by the Medical Director on behalf of the Royal Marsden and Institute of Cancer Research. NHS provider organisations have a statutory duty to support their Responsible Officers in discharging their duties under the Responsible Officer Regulations and it is expected that Trust Boards will oversee compliance by:
a) monitoring the frequency and quality of medical appraisals in their organisations;
b) checking there are effective systems in place for monitoring the conduct and performance of their doctors;
c) confirming that feedback from patients is sought periodically so that their views can inform the appraisal and revalidation process for their doctors; and;
d) Ensuring that appropriate pre-employment background checks (including pre-engagement for Locums) are carried out to ensure that medical practitioners have qualifications and experience appropriate to the work performed.
3. Governance Arrangements
The Medical Director is the designated Executive Lead for medical appraisals and revalidation. One of the recommendations from last year’s report was to consider the support required for Responsible Officer. To this end, an Appraisal and Revalidation Lead, Dr Jonathan Handy, was appointed in May 2016. The focus for this clinical leadership role will be to support the Trust to maintain a high level of compliance (90%+) with appraisals and improve the quality of the appraisal. The metrics for determining the latter have yet to agreed but are likely to include indicators suggested by NHS England.
The Medical Workforce Committee, led by the Director of Workforce was established in 2015-16 and this group is responsible for tracking progress with appraisal and revalidation and implementation of the improvement plan shown at appendix A. Monitoring is tracked through regular reporting as follows:- • Monthly and quarterly reports to NHS England South Region

2
• Annual Organisational Audit to NHS England South Region • Monthly reporting to the Performance Review Group and quarterly reporting to Integrated
Governance and Risk Management Committee
4. Policy and Guidance
The Trust has a policy on medical appraisals and revalidation in line with NHS requirements. The policy also covers doctors that employed by the ICR and hold an honorary contract with The Royal Marsden.
5. Medical Appraisal
a) Appraisal and Revalidation Performance Data
As of 31 March 2016, of the 281 doctors who have a prescribed connection to the Trust, 251 had an appraisal meeting. There has been a significant improvement in the appraisal completion rate from 73% in 2014-15 to 89% in 2015-16, which exceeded the in-year target of 85%. The consultant appraisal rate was 92% for 2015-16. The details are shown in the table 1 below. Table 1 shows appraisal and revalidation performance data -2015/2016
Doctors with a prescribed connection Trust Honorary Total
No of completed appraisals variance
Cancer Services 125 47 172 159 13 Clinical Services 69 25 94 81 13 Clinical Research 1 7 8 5 3 Corporate 1 0 1 1 0 Community 3 0 3 3 0 Private 3 0 3 2 1 Total 202 79 281 251 30
Number of positive recommendations to the GMC for revalidation between 1/04/2015 - 31/03/2016 i.e. these are doctors who have met all the requirements and have actually been revalidated by the GMC 78 Number of deferrals between 01/04/15 - 31/03/2016 i.e. these are doctors who were due to be assessed for revalidation but the assessment has been deferred by the Trust 25
Reasons for deferrals Long term sickness/personal reasons 2 Maternity leave 1 New Starter 4 Relinquish license to practice 1 Incomplete Appraisal 17
3
b. Appraisers
There are currently 80 trained consultant appraisers in the Trust. This figure is reviewed annually as part of the appraisal audit process to ensure there is sufficient capacity to deliver a high completion rate for appraisals.
c. Quality Assurance
Quality assurance systems are in place including:
• Audit reviews - KPMG undertook an internal audit in January 2014, which provided assurance that there are robust systems in place. There is also a Trust local audit review process in place;
• Appraisal portfolios are reviewed prior to submission to the Responsible Officer to ensure documentation is complete and up to date;
• Monthly review of the appraisal completion rate is undertaken by the Medical Workforce Committee and Performance Review Group;
• A process to link complaints information to the appraisal process is being established; • A process to link significant clinical events to appraisals. There is a positive reporting
mechanism to confirm if there have been no significant events. Concerns and performance issues are dealt with under the Maintaining High Professional Standards Policy, (Appendix B).
6. Risk and Issues
In addition to those doctors with a prescribed connection to the Trust, there are other doctors working for the Trust through a service level agreement or contract for service, who have a prescribed connection to another organisation. There is a need to confirm that service level agreement(s) make adequate reference to appraisal/revalidation requirements.
7. Responding to Concerns and Remediation
Information about the number and type of concerns raised about individual clinical practitioners during 2015-16 (Appendix B).
8. Areas for improvement
Each year the Trust reviews the processes that support medical appraisal and revalidation. The detailed action for improvement is shown at appendix A. In summary the areas for improvement in 2016-17 include: a. Improve performance by further reducing the number of deferrals; b. Improve processes for non-consultant grades; c. Agree methodology and metrics for auditing quality of appraisals; d. Ensure that service level agreement(s) for doctors working for the Trust but with a
prescribed connection with another organisation make adequate reference to appraisal/revalidation requirements.
9. Recommendations
The Board is asked to:
1) Note progress with implementation of appraisal and revalidation; 2) Note key areas for improvement and action plan; 3) Approve the Chief Executive and Chair to sign off a statement of compliance by 31
August 2016 (Appendix C)

4
Appendix A - Improvement Plan for 2016-17
No. Item
Actions Timescales* Monitoring by
Priority April - September 2016 (next 6 months)
1 Review process to reduce deferral rate from 25 in 2015-16 to 20 in 2016-17
Investigate further reasons for incomplete appraisal and process changes required for improvement
June 2016 Medical Workforce Committee
2 Maintain appraisal at 90% or above
HR scorecard to continue to be reviewed at PRG Appraisal overdue reports to be discussed at Medical Workforce Committee Issue to be escalated to Appraisal and Revalidation Lead Review processes for non-consultant grades
On-going On-going June 2016 August 2016
Medical Workforce Committee
3 Training and support for appraisers and doctors
Review communications to doctors on appraisal and revalidation to ensure these are up to date / consistent with recommendations from previous audits Review system for allocating of appraisees to appraisers
June /July 2016 September 2016
Medical Workforce Committee
4 Annual board report on appraisal and revalidation detailing assurance and concerns
Six month report to IGRM
September 2016
IGRM
5 Monitor quality of appraisals completed
Agree methodology and KPIs for reviewing quality of appraisals Audit random sample of appraisals to review information used is in line with Trust policy and inclusion of education supervision as part of appraisal process
September 2016 September 2016
Medical Workforce Committee and IGRM

5
* Please note the timescales for action are subject to review with recently appointed Appraisal and Revalidation Lead.
Medium priorities - October to March 2016/17 6 Review of medical
appraisal and revalidation policy
Review existing policy in light of quality audit completed in April 2016
December 2016 Medical Workforce Committee
7 Feedback / Survey on the appraisal / MSF process/use of Zicardian system
Seek qualitative feedback from appraiser/appraises on the appraisal process Seek feedback on use of Zicardian system and discuss with Allocate
January 2017
Medical Workforce Committee
8 Service level agreements for doctors with prescribed connection with another organisation(s)
Ensure that the service level agreement made adequate reference to appraisal/revalidation requirements
March 2017 Medical Workforce Committee and IGRM

6
Appendix B - Audit of concerns about a doctor’s practice
Concerns about a doctor’s practice High level
Medium level
Low level
Total
Number of doctors with concerns about their practice in the last 12 months Explanatory note: Enter the total number of doctors with concerns in the last 12 months. It is recognised that there may be several types of concern but please record the primary concern
0
Capability concerns (as the primary category) in the last 12 months
0
Conduct concerns (as the primary category) in the last 12 months
1 1
Health concerns (as the primary category) in the last 12 months
0 0
Remediation/Reskilling/Retraining/Rehabilitation
Numbers of doctors with whom the designated body has a prescribed connection as at 31 March 2015 who have undergone formal remediation between 1 April 2015 and 31 March 2016 Formal remediation is a planned and managed programme of interventions or a single intervention e.g. coaching, retraining which is implemented as a consequence of a concern about a doctor’s practice A doctor should be included here if they were undergoing remediation at any point during the year
0
Consultants (permanent employed staff including honorary contract holders, NHS and other government /public body staff)
0
Staff grade, associate specialist, specialty doctor (permanent employed staff including hospital practitioners, clinical assistants who do not have a prescribed connection elsewhere, NHS and other government /public body staff)
0
General practitioner (for NHS England area teams only; doctors on a medical performers list, Armed Forces)
0
Trainee: doctor on national postgraduate training scheme (for local education and training boards only; doctors on national training programmes)
0
Doctors with practising privileges (this is usually for independent healthcare providers, however practising privileges may also rarely be awarded by NHS organisations. All doctors with practising privileges who have a prescribed connection should be included in this section, irrespective of their grade)
0
Temporary or short-term contract holders (temporary employed staff including locums who are directly employed, trust doctors, locums for service, clinical research fellows, trainees not on national training schemes, doctors with fixed-term employment contracts, etc) All DBs
0
Other (including all responsible officers, and doctors registered with a locum agency, members of faculties/professional bodies, some
0

7
management/leadership roles, research, civil service, other employed or contracted doctors, doctors in wholly independent practice, etc) All DBs
TOTALS 1
Other Actions/Interventions 0
Local Actions: 0
Number of doctors who were suspended/excluded from practice between 1 April and 31 March: Explanatory note: All suspensions which have been commenced or completed between 1 April and 31 March should be included
0
Duration of suspension: Explanatory note: All suspensions which have been commenced or completed between 1 April and 31 March should be included
Less than 1 week 1 week to 1 month 1 – 3 months 3 - 6 months 6 - 12 months
0
Number of doctors who have had local restrictions placed on their practice in the last 12 months?
0
GMC Actions: Number of doctors who:
0
Were referred to the GMC between 1 April and 31 March 0
Underwent or are currently undergoing GMC Fitness to Practice procedures between 1 April and 31 March
0
Had conditions placed on their practice by the GMC or undertakings agreed with the GMC between 1 April and 31 March
0
Had their registration/licence suspended by the GMC between 1 April and 31 March
0
Were erased from the GMC register between 1 April and 31 March 0
National Clinical Assessment Service actions: 0
Number of doctors about whom NCAS has been contacted between 1 April and 31 March:
0
For advice 0
For investigation 0
For assessment 0
Number of NCAS investigations performed 0
Number of NCAS assessments performed 0

8
Appendix C – Designated Body Statement of Compliance
The board / executive management team – [delete as applicable] of [insert official name of DB] can confirm that
• an AOA has been submitted, • the organisation is compliant with The Medical Profession (Responsible Officers)
Regulations 2010 (as amended in 2013) • and can confirm that:
1. A licensed medical practitioner with appropriate training and suitable capacity has been nominated or appointed as a responsible officer;
Yes
2. An accurate record of all licensed medical practitioners with a prescribed connection to the designated body is maintained;
There is a process to regularly review the list of medical practitioners with a prescribed connection to the Trust.
3. There are sufficient numbers of trained appraisers to carry out annual medical appraisals for all licensed medical practitioners;
The numbers of trained appraisers is detailed in the annual report.
4. Medical appraisers participate in ongoing performance review and training / development activities, to include peer review and calibration of professional judgements (Quality Assurance of Medical Appraisers1 or equivalent);
There is a process to quality assure completed appraisals. A Revalidation and Appraisal Lead was appointed in May 2016 to support the Trust to achieve further improvements with the quality of medical appraisals.
5. All licensed medical practitioners2 either have an annual appraisal in keeping with GMC requirements (MAG or equivalent) or, where this does not occur, there is full understanding of the reasons why and suitable action taken;
Compliance is at 89% for all medical practitioners and 92% for consultants and there is a process for monitoring non-compliance.
6. There are effective systems in place for monitoring the conduct and performance of all licensed medical practitioners1 (which includes, but is not limited to, monitoring: in-house training, clinical outcomes data, significant events, complaints, and feedback from patients and colleagues) and ensuring that information about these matters is provided for doctors to include at their appraisal;
The Trust has robust systems for clinical governance and a process to link this information to the appraisal process.
7. There is a process established for responding to concerns about any licensed medical practitioners1 fitness to practise;
1 http://www.england.nhs.uk/revalidation/ro/app-syst/ 2 Doctors with a prescribed connection to the designated body on the date of reporting.

9
This is covered in the revalidation and appraisal policy and wider HR policies.
8. There is a process for obtaining and sharing information of note about any licensed medical practitioner’s fitness to practise between this organisation’s responsible officer and other responsible officers (or persons with appropriate governance responsibility) in other places where the licensed medical practitioner works;3
Information is shared through the Responsible Officer Network
9. The appropriate pre-employment background checks (including pre-engagement for locums) are carried out to ensure that all licenced medical practitioners4 have qualifications and experience appropriate to the work performed;
The Trust is compliant with NHS pre-employment checks for substantive and locum medical staff.
10. A development plan is in place that ensures continual improvement and addresses any identified weaknesses or gaps in compliance.
The annual improvement plan forms part of the annual report to the Board.
Signed on behalf of the designated body
Official name of designated body: The Royal Marsden NHS Foundation Trust
Name: Cally Palmer Signed:
Role: Chief Executive
Date: 24 May 2016
3 The Medical Profession (Responsible Officers) Regulations 2011, regulation 11: http://www.legislation.gov.uk/ukdsi/2010/9780111500286/contents


BOARD PAPER SUMMARY SHEET
Date of Meeting:
1st June 2016
Agenda item 4.3.
Title of Document: Junior Doctors Briefing
To be presented by
Medical Director
Executive Summary
This attached report provides the Trust Board with an update on the impact of industrial action in April 2016 and information on the latest developments with the junior doctor contract negotiations. The British Medical Association (BMA), NHS Employers and the Secretary of State have reached agreement on negotiated terms and conditions. The parties will now work over the next two weeks ahead of the referendum of BMA members to finalise the details, which if agreed would see some elements of the contract implemented in August 2016, with doctors moving on to the contract between October 2016 and August 2017.
Trusts have been asked to put on hold any work on the implementation of the junior doctor contract, pending outcome of the referendum and publication of the revised terms and conditions of the employment. Recommendations
To note impact of junior doctors industrial action and latest developments in contract negotiations.
Author: Nina Singh, Director of Workforce
Contact Number or E-mail: 2141
Date: 19 May 2016


1
Junior Doctors Briefing
1. Introduction This report provides the Trust Board with an update on the national junior doctor contract negotiations, industrial action and proposed implementation of the new contract in 2016-17.
2. Background and context The Trust Board received an updated on the background and context of junior doctors pay negotiations in March 2016. At that stage contract negotiations had broken down and the Secretary of State had confirmed that the new junior doctor contract would be introduced in August 2016.
Following this, a set of terms and conditions were launched and the Trust convened a working group to oversee the roll out and developed a local implementation plan. The implementation plan is now on hold following an agreement reached by the BMA, NHS Employers and the Secretary of State on negotiated terms and conditions. The parties will now work over the next two weeks ahead of the referendum of BMA members to finalise the details, which if agreed would see some elements of the contract implemented in August 2016, with doctors moving on to the contract between October 2016 and August 2017.
Both parties have resolved the outstanding issues taken forward from previous discussions, finalised and confirmed areas already agreed, and developed further measures that address the wider concerns of junior doctors. The agreement includes:
• A new approach to pay and reward. It is reported that the overall base pay may be lower than anticipated (10% instead of previously reported figure of 13%) with changes agreed to flexible pay
• Actions to support equality dimensions of the contract. The Board will recall that the equality impact assessment formed the basis of the BMA judicial review
• Refinements to previous rota rules • Improvements to flexible pay premia (FPP) and other terms • Clarification of the role of the Guardian of Safe Working • A commitment from Health Education England to review how it places doctors in
training to help provide a better family life and commitments from the General Medical Council.
3. Industrial action and impact on The Royal Marsden
To date there have been six days of industrial action between January – May 2016. Over that period a number of junior doctors have taken strike action as detailed below. For those that took strike action, their pay was amended accordingly. The most recent two days of industrial action included the withdrawal of emergency care provided by junior medical staff. In preparation for this, the GMC revised their guidance to reiterate the need for juniors to work in partnership with Trusts to ensure patient safety at all times. The Trust also asked all consultants to prioritise their NHS work and be available on-site. The Trust’s response to the industrial action was well planned and well executed. An emergency care model was supported by junior medical staff not taking strike action and Consultants. The Trust reported that it had not cancelled any operations and there had been no adverse impact on our patients.

2
Dates 12/01/2016
(24 hours) 10/02/2015 (24 hours)
9-10/03/2016 (48 hours)
26-28/04/2016 (48 hours – no emergency cover)
% junior doctors on strike
29% 32% 34% (9th) 33% (10th)
34% (26th) 37% (27th)
The percentage of juniors taking strike action is broadly similar to other London acute specialist Trusts (Great Ormond Street Hospital – 35%) and below acute hospitals (Chelsea and Westminster Foundation - 45%).
4. Appointment to the Guardian of Safe Working
Part of the new terms and conditions require Trusts to appoint a Guardian of Safe Working. The Guardian will be a senior person within the Trust, independent of the management structure and responsible for protecting the safeguards outlined in the terms and conditions of service for doctors in training. The Guardian will work with the Trust to ensure that issues of compliance with safe working hours are addressed, as they arise and will provide assurance to the Trust Board that doctors' working hours are safe.
Although expressions of interest from the Consultant body have been sought, the process will now be on hold pending BMA members referendum.
5. Medical staffing workforce plan
At the last meeting the Trust Board was updated on the programme of work to develop a sustainable medical staffing workforce model. This piece of work serves to address a number of medical staffing concerns including, recruitment and retention and the experience of our trainees. In addition, although the specific numbers are not yet known, it is expected that the number of trainees allocated to the Trust will decrease over the next few years. The Trust needs to review alternative models to mitigate the current workload pressures and the impact of a reduced workforce in the future. This project is progressing as planned and a further update will be provided in the autumn.
6. Conclusion
The Board is asked to:
• Note the impact of most recent industrial action on The Royal Marsden • Note that the latest developments with junior doctor contract negotiations • Note that future Board updates are scheduled on the junior doctor workforce plan
and the implementation of junior doctor contract. The further updates will reflect the financial information requested by the Board.

BOARD PAPER SUMMARY SHEET
Date of Meeting:
1st June 2016
Agenda item 4.4
Title of Document: Initial feedback on CQC inspection
To be presented by
Chief Nurse
Executive Summary Initial feedback on CQC inspection that occurred on the 19th to the 22nd April 2016. Over 50 Inspectors visited services and held individual and focus group sessions with all services across the RM at Sutton, Chelsea and the community services. The Chief Nurse will provide a verbal update on the inspection and the high level feedback that the Executive Directors received on the last day. The full written report is expected in about two months’ time for a factual accuracy check, this report will include the first indication of the ratings that will be applied to individual services and the overall proposed rating. Recommendations
To note the Chief Nurse’s initial feedback on the CQC inspection.


BOARD PAPER SUMMARY SHEET
Date of Meeting:
1st June 2016
Agenda item 4.5
Title of Document: Nurse Revalidation
To be presented by
Chief Nurse
Executive Summary This summary paper provides the national framework for Nurse revalidation and the RM response. Nurse Revalidation commenced mandatorily in April 2016 following national pilots. Thus far the RM has revalidated 38 of its 982 nurses. There have been no problems encountered to date. The RM actively engaged with the national preparation to ensure that it was ready as an organisation and that it’s nurses were also prepared. Recommendations
To note the RM response to the national Nurse Revalidation Framework.
Author: Chief Nurse
Contact Number or E-mail: 2121
Date: 19 May 2016


1
Nurse Revalidation
1.0. Introduction The following paper provides board members with the background to Nurse Revalidation and the current status of revalidation at The Royal Marsden NHS Foundation Trust (RM)
2.0. Background Nurse Revalidation is the process that permits nurses to maintain their mandatory registration with the Nursing and Midwifery Council (NMC). Revalidation has been introduced to improve public protection by guaranteeing individuals are fit to practise. It has been developed following a number of high profile failures in care highlighted in reports such as the Francis Report (2013). It sets out guidelines and requirements that a nurse or midwife must abide by to maintain professional registration throughout their career.
Revalidation also provides benefits for nurses and midwives as it encourages a culture of sharing, reflection and improvement and will be an on-going process throughout a nurse’s career.
Revalidation builds on the previous requirements for nurses to register including 45o hours of nursing practice and 35 hours of continuous professional development, over a three year period. Nurse revalidation in England became mandatory on the 1st April 2016 and the first nurses at the RM completed the process in April 2016.
3.0. Revalidation – requirements to be achieved over a 3 year period
- 450 hours practice (no change from previous requirement) - 35 hours continuous professional development - (no change from previous
requirement) however an additional requirement is that 20hrs of this must be participatory learning
- 5 Reflections – Write 5 pieces of reflection on different aspects of practice as a nurse (a new requirement)
- Reflective discussion – Meet with another registered nurse and discuss the reflections and learning that has occurred (a new requirement)
- 5 Pieces of practice related feedback - feedback from colleagues, patients, audits, appraisals etc. about the individual nurse or unit within which they work which relates to their practice (a new requirement)
- Confirmation - Line manager to review and confirm that the evidence above has been provided (a new requirement).
4.0. Governance A revalidation steering group chaired by the Deputy Chief Nurse was set up in November 2015 meeting monthly to provide rigour and support to the RM process. Membership includes all Clinical Nurse Directors, and representation from Human Resources, Matrons, Practice Educators and Temporary Staffing
A revalidation lead was identified and commenced in October 2015 working closely with registrants and their managers to support the process.
5.0. Risks There is a risk that nurses fail to revalidate in time. The NMC has a facility to allow a nurse to delay or extend their revalidation date. The criteria are specific and refer to “exceptional circumstances”. A nurse can only delay or provide an exemption to revalidation date if:
- They have been on maternity or sick leave for a significant amount of time and have had insufficient time to complete the require criteria;
- They can only extend the revalidation date by up to 6 weeks if there is documented exceptional circumstance.

2
Regular monitoring by the revalidation lead and liaising with managers/matrons should reduce this risk occurring at RM.
6.0. Revalidation numbers 2016/2017
The RM employs 982 nurses, in 16/17 450 nurses are due to revalidate.
No of RN to revalidate 2016/2017
RN revalidated & NMC records updated Status
TOTAL to Revalidate 2016/2017 450
April 23 21 All nurses revalidated – two nurses were due to retire in April and will therefore not revalidate.
May 18 17
One temporary (bank) nurse has requested an extension from the NMC and will revalidate in mid-July.
June 30 3
July 30 0
August 28 0
September 144 0
October 26 0
November 39 0
December 22 0
January 22 0
February 31 0
March 37 0
7.0. Conclusion The Board is invited to note the progress on Nurse Revalidation at the RM and to ask any questions about implementation or impact at The Royal Marsden.

BOARD PAPER SUMMARY SHEET
Date of Meeting: 1st June 2016
Agenda item 5.1
Title of Document:
Key Performance Indicators for Quarter 4
To be presented by Chief Operating Officer
Executive Summary This paper provides a report on the Trust’s performance for quarter 4 2015/16 including the balanced scorecard for the Trust and a commentary on the red rated indicators and actions underway to improve performance. Recommendations The Board is asked to discuss and note the Trust’s performance against the balanced scorecard indicators for quarter 4 2015-16. Author: Steven Francis, Director of Performance and Information
Contact Number or E-mail: Ext 8260
Date: 20th May 2016


1
KEY PERFORMANCE INDICATORS
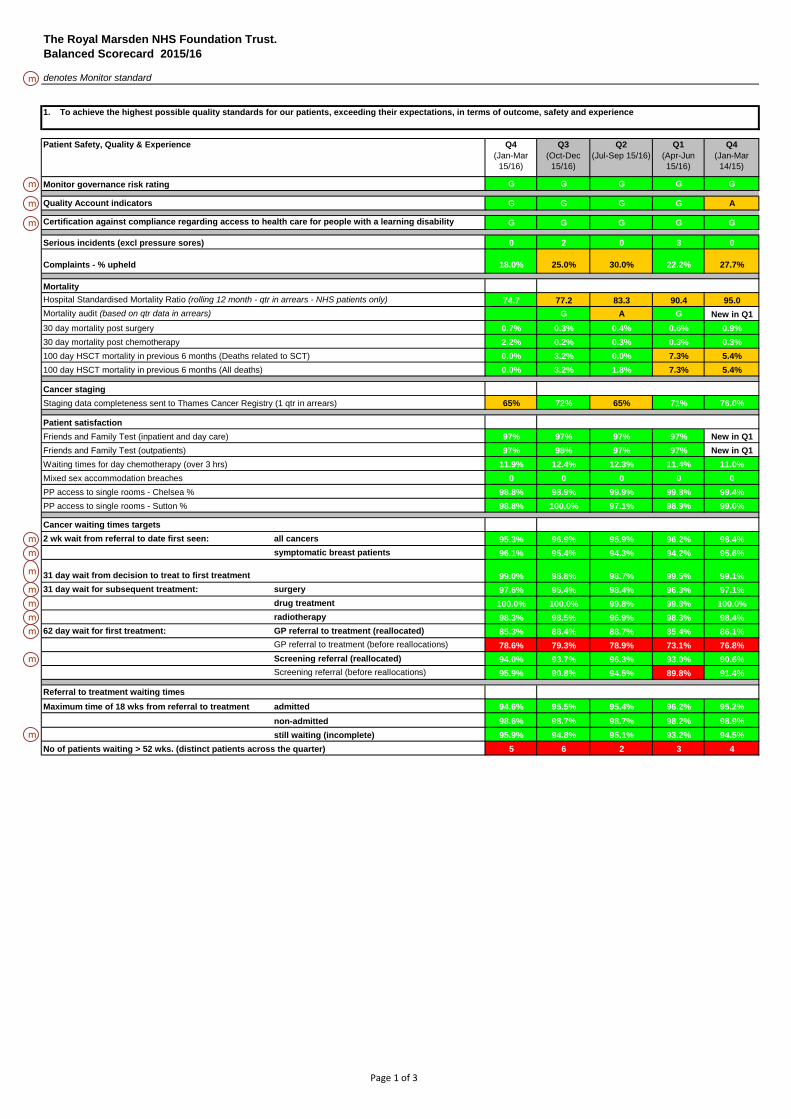
QUARTER 4 2015/16 1. PURPOSE This paper is intended to provide the Board with an update on the Trust’s performance for quarter 4 2015/16. The scorecard and narrative is also submitted to the Council of Governors. The report includes the balanced scorecard for the Trust and a commentary on the red-rated indicators in the quarter 4 report including actions underway to improve performance. The Staff Friends and Family Test did not take place in quarter 3 as the annual staff survey is undertaken during this time period and therefore this is intentionally left blank on the scorecard.
2. KPI REVIEW
A full review of the scorecard metrics, definitions and thresholds has now been completed and is being presented in a separate paper to the Trust Board. 3. PERFORMANCE FOR QUARTER 4 Attachment 1 shows the balanced scorecard report for quarter 4 for 2015/16. The Trust met all of the Monitor indicators and targets for quarter 4, although two were rated amber (financial sustainability risk and nursing agency spend). The Monitor targets are indicated on the scorecard. A commentary is only provided for indicators where performance is ‘red’ rated.
3.1
Q4
62 day wait for first treatment – GP referral to treatment (before reallocation)
Actual: 78.6% Target: 85% Forecast: Meet new reallocation target
RMH did not meet the 62 day urgent GP referral standard (before reallocations) with performance at 78.6%. The Trust met the standard following LCA reallocations at 88.4%. A new national reallocation policy has now been launched which will allow the Trust to reallocate all late referrals received after day 38 providing treatment takes place within 24 days of referral. The Trust will begin reporting in line with this standard in shadow form from Q1 onwards.

2
During Q4 there were 39.5 accountable breaches prior to reallocation. Of those, 22.5 accountable breaches were received late in the pathway (defined as on or after day 43). Out of the Trust’s control
• Late notification of target (1) • Patient fitness (2) • Patient choice (4.5) • In appropriate referral (0.5) • Complex pathway (4)
Within the Trust’s control
• Administrative delays (3) • Capacity (0.5) • Lack of tracking (0.5) • Delay to diagnostics (0.5) • Surgical planning (0.5)
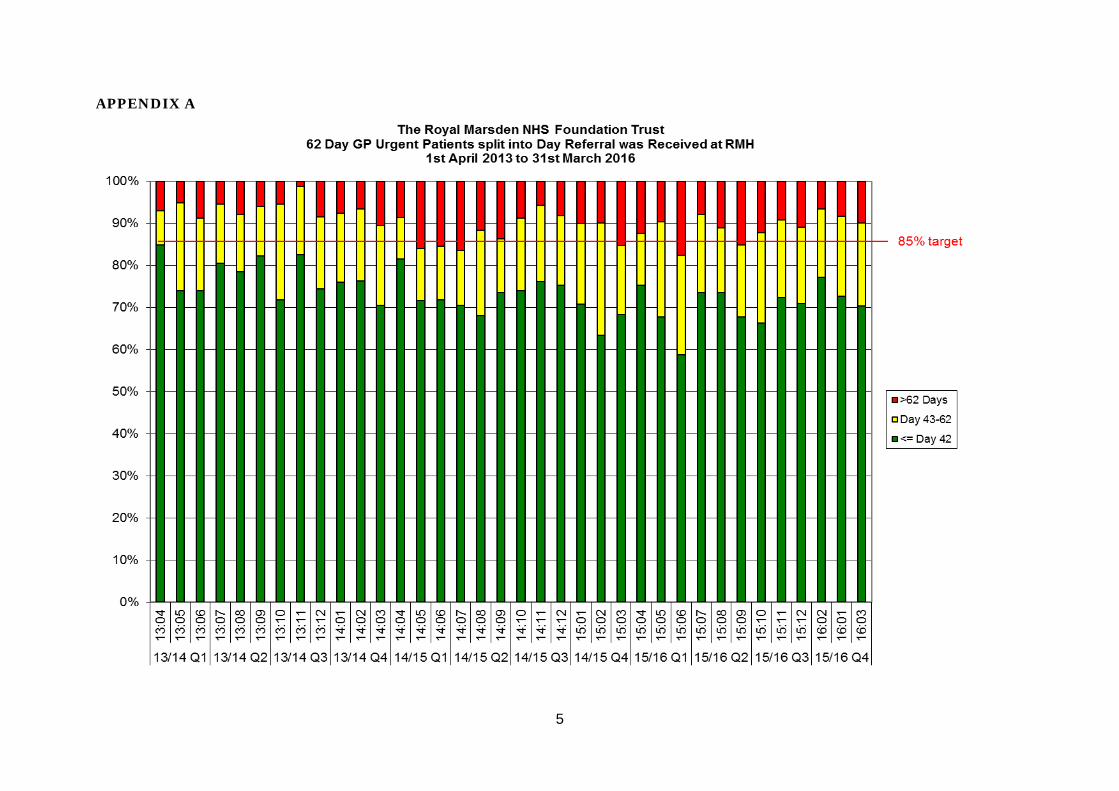
RMH continues to receive a high number of late referrals, as shown in the graph at Appendix A. A full action plan is in place and has been shared with commissioners and covers internal improvements and work with referring Trusts. In addition, the Trust continues to work closely with its referrer trusts through the System Leadership Forum and the South West London Providers’ Group. The Trust expects to continue to meet the standard post-reallocation. The full breakdown of performance by tumour site prior to reallocation can be found in the table at Appendix B.
3.2
Q4
No. of patients waiting >52 weeks (distinct patients across the quarter)
Actual: 5 Target: 0 Forecast: The Trust will continue to report 52 week waiters due to patient choice
RMH reported five 52 week waiters at the end of March as incomplete pathways. All patients were benign patients on plastics pathways awaiting delayed reconstructions. Four patients have opted to wait for surgery. One patient’s surgery was cancelled for an urgent case. An alternative date was offered with a different surgeon however the patient chose to wait for a specific surgeon. Each of these pathways has been carefully reviewed and shared with commissioners.

3
3.3 Q4 PP Debtors over 90 days (% of total PP-debtors) Actual: 46% Target: <25% Forecast: N/A Private Care Debt over 90 days has remained consistent around 47% for most of the year, driven by the increased volume of embassy work which constitutes the majority of this balance. The growth strategy of Private Care is to expand this customer group further, so different approaches will need to be taken to reduce the payment times from the sector standard of 6 months.
3.4 Q4
Capital expenditure variance (£000) Actual: -12, 007 Target :between 85%-
115% of plan Forecast: N/A
The capital programme for 2015/16 was significantly under plan but had no associated clinical risk impact. Some schemes were delivered through alternative means (such as Sphere). There was a reduction in the requirement for a second loan due to the charity funding for a new Linac. There was also tight control of contingency budgets and finally some schemes slipped into 16/17 which has contributed to the variance.
3.5 Q3 (1Q in arrears)
Percentage of closed commercial interventional trials meeting contracted recruitment target
Actual : 57% Target : >85% Forecast : N/A A deep dive analysis has been undertaken to understand the factors that are driving the underperformance of this metric. While it had previously been reported that older trials with unrealistic recruitment targets had been the main cause of the underperformance other factors have emerged. A significant number of trials failed to meet recruitment targets as a result of the sponsor closing recruitment early. In addition, there are a large number of extremely specialised trials with small recruitment targets and narrow eligibility criteria for patient participation. Both of these factors are outside the control of the Trust. It is proposed that the Board continues to have oversight of this metric as it is reported externally. The level of performance against this measure is not peculiar to RMH and under-performance is a common amongst other organisations. The NIHR has recognised this issue and is reviewing the methodology and metric to ensure it is a suitable and achievable measure. A more detailed analysis of this metric can be found in Appendix C.

4
4.0 Conclusion The Board is asked to note the Trust balanced scorecard and commentary for Q4 2015/16 and is invited to discuss the position. Appendix A shows the Trust 62 Day GP Urgent pathways by month since April 2013, cohorted by the pathway-day the referral was received at RMH. Appendix B shows the Trust 62 Day GP Urgent performance, split by tumour type. Appendix C shows the results of the deep dive analysis of the recruitment to trials measure
5
APPENDIX A

6
APPENDIX B 62 Day Wait for First Treatment (GP Urgent). Performance by Tumour Type. Tumour site Q1 15/16 Q2 15/16 Q3 15/16 Q4 15/16
Breast 93.5% 97.5% 96.5% 95.7%
Children's N/A 100.0% 100.0% N/A
Gynaecological 73.1% 74.1% 85.7% 66.7%
Haematological (excl. Acute Leukaemia) 64.3% 87.5% 100.0% 77.3%
Head & Neck 48.0% 35.7% 47.6% 81.3%
Lower GI 40.0% 61.5% 75.0% 62.96%
Lung 60.7% 86.0% 83.3% 58.3%
Referred elsewhere for treatment 100.0% N/A 100.0% N/A
Other 33.3% 100.0% 71.4% 100.0%
Sarcoma 66.7% 69.6% 58.3% 65.7%
Skin 73.3% 66.7% 72.7% 91.3%
Testicular N/A 100.0% 50.0% N/A
Upper GI 80.6% 62.5% 70.0% 72.7%
Urological 40.7% 45.0% 40.5% 64.9%
7
APPENDIX C NIHR Performance Metrics Report - Quarter 3 2015/16 1.0 Background
Each quarter, the Trust reports the percentage of closed commercial trials meeting their recruitment target as part of the Balanced Board Scorecard. This metric is calculated using NIHR methodology and has continued to be RAG rated red since its inception. This paper explores the Trust’s trial accrual performance and the current issues with the reported metric. 2.0 Measuring Recruitment of Closed Trials Currently, 56.7% of closed trials at RMH met their recruitment target which equates to 102 out of 180 trials meeting recruitment targets. This is better than the mean for League 1 institutions which stands at 55.5%. The Trust is currently ranked ninth out of 22 institutions in League 1. Once closed to recruitment, a study moves into a follow-up phase and this continues to be reported in the “closed to recruitment” metric until 12 months after the trial is completely closed. In many cases, the follow-up phase can be anything up to 11 years. Many of the older trials were set up when investigators were encouraged to set optimistic targets, which were subsequently not met and these continue to be reported in the metric until closed. In late 2013 the Trial Set-up Meeting was established as a facilitatory meeting to aid the set-up process between the trial coordinators and the support services. The meeting encourages frank and honest discussion around targets to ensure an achievable target has been set. 3.0 Trials Failing To Meet Their Target Whilst it is acknowledged that some trials historically have failed to meet their recruitment due to ambitious target-setting, as reported to the Board, further analysis has established that the single biggest factor determining recruitment failure in Q3 was sponsor-related issues. The following pie chart shows that the sponsor is responsible for almost 50% of those studies which did not reach the recruitment target.

8
4.0 Future reporting of research metrics
The Trust will continue to report the metric “percentage of closed trials meeting their recruitment target” in the Board Scorecard. However, from Q4 2015/16 the NIHR will only collect information on studies which have closed in the last 12 months. This will remove older studies which are in follow up for many years. The NIHR will also collect information relating to the reason for not reaching target, however, it is not clear how this will be used and reported, nor what the likely impact of these changes on RMH’s performance. In addition, further research metrics are proposed for the scorecard to provide more assurance around this important area.
Page 1 of 3
The Royal Marsden NHS Foundation Trust. Balanced Scorecard 2015/16
m denotes Monitor standard
Patient Safety, Quality & Experience Q4(Jan-Mar
15/16)
Q3(Oct-Dec
15/16)
Q2(Jul-Sep 15/16)
Q1(Apr-Jun 15/16)
Q4(Jan-Mar
14/15)
m Monitor governance risk rating G G G G G
m Quality Account indicators G G G G A
m G G G G G
Serious incidents (excl pressure sores) 0 2 0 3 0
Complaints - % upheld 18.0% 25.0% 30.0% 22.2% 27.7%
MortalityHospital Standardised Mortality Ratio (rolling 12 month - qtr in arrears - NHS patients only) 74.7 77.2 83.3 90.4 95.0Mortality audit (based on qtr data in arrears) G A G New in Q130 day mortality post surgery 0.7% 0.3% 0.4% 0.6% 0.9%30 day mortality post chemotherapy 2.2% 0.2% 0.3% 0.3% 0.3%100 day HSCT mortality in previous 6 months (Deaths related to SCT) 0.0% 3.2% 0.0% 7.3% 5.4%100 day HSCT mortality in previous 6 months (All deaths) 0.0% 3.2% 1.8% 7.3% 5.4%
Cancer stagingStaging data completeness sent to Thames Cancer Registry (1 qtr in arrears) 65% 72% 65% 71% 76.0%
Patient satisfaction Friends and Family Test (inpatient and day care) 97% 97% 97% 97% New in Q1Friends and Family Test (outpatients) 97% 98% 97% 97% New in Q1Waiting times for day chemotherapy (over 3 hrs) 11.9% 12.4% 12.3% 11.4% 11.0%Mixed sex accommodation breaches 0 0 0 0 0PP access to single rooms - Chelsea % 98.8% 98.9% 99.9% 99.8% 99.4%PP access to single rooms - Sutton % 98.8% 100.0% 97.1% 98.9% 99.0%
Cancer waiting times targetsm 2 wk wait from referral to date first seen: all cancers 95.3% 96.9% 95.9% 96.2% 98.4%m symptomatic breast patients 96.1% 95.4% 94.3% 94.2% 95.6%
m 31 day wait from decision to treat to first treatment 99.0% 98.8% 98.7% 99.5% 99.1%m 31 day wait for subsequent treatment: surgery 97.6% 96.4% 98.4% 96.3% 97.1%m drug treatment 100.0% 100.0% 99.8% 99.8% 100.0%m radiotherapy 98.3% 98.5% 96.9% 98.3% 98.4%m 62 day wait for first treatment: GP referral to treatment (reallocated) 85.3% 88.4% 88.7% 85.4% 86.1%
GP referral to treatment (before reallocations) 78.6% 79.3% 78.9% 73.1% 76.8%m Screening referral (reallocated) 94.0% 93.7% 96.3% 93.0% 90.6%
Screening referral (before reallocations) 95.9% 90.8% 94.5% 89.8% 91.4%
Referral to treatment waiting timesMaximum time of 18 wks from referral to treatment admitted 94.6% 95.5% 95.4% 96.2% 95.2%
non-admitted 98.6% 98.7% 98.7% 98.2% 98.9%m still waiting (incomplete) 95.9% 94.8% 95.1% 93.2% 94.5%
No of patients waiting > 52 wks. (distinct patients across the quarter) 5 6 2 3 4
1. To achieve the highest possible quality standards for our patients, exceeding their expectations, in terms of outcome, safety and experience
Certification against compliance regarding access to health care for people with a learning disability

Page 2 of 3
The Royal Marsden NHS Foundation Trust. Balanced Scorecard 2015/16
m denotes Monitor standard
Finance & Efficiency Q4(Jan-Mar
15/16)
Q3(Oct-Dec
15/16)
Q2(Jul-Sep 15/16)
Q1(Apr-Jun 15/16)
Q4(Jan-Mar
14/15)m Monitor financial sustainability risk rating 3 3 3 3 4
Agency spend (% of total pay) 5.6% 5.8% 7.1% 6.7% New in Q1m Nursing agency spend (% of nursing pay bill) 5.1% 6.9% 5.1% 4.3% New in Q1
Cash (£m) 24.1 34.7 33.9 30.6 New in Q1NHS activity Income Variance YTD (£000) -4487 -3257 -3685 -2000 2,740PP activity Income Variance YTD (£000) -537 -568 -664 -95 -4,144PP Debtors over 90 days (% of total PP debtors) 46% 49% 37% 47% New in Q1Non-PP Debtors over 90 days (% of total non PP-debtors) 35% 36% 43% 41% New in Q1Achievement of Efficiency Programme YTD (%) 87% 89% 89% 93% 63%Capital Expenditure Variance YTD (£000) -12,007 -5,684 -4,429 -414LQIS % achievement (formerly CQUINS) Acute TBC 100% 100% 100% 99.5%LQIS % achievement (formerly CQUINs) Sutton and Merton Community Services TBC 100% 100% 100% 100%
Asset utilisationBed occupancy - Chelsea 82% 82% 83% 82% 88%Bed occupancy - Sutton 83% 80% 82% 82% 84%Theatre utilisation - Chelsea 93% 96% 95% 93% 93%Theatre utilisation - Sutton 72% 75% 87% 77% 77%
Clinical and Research Strategy Q4(Jan-Mar
15/16)
Q3(Oct-Dec
15/16)
Q2(Jul-Sep 15/16)
Q1(Apr-Jun 15/16)
Q4(Jan-Mar
14/15)New referralsTotal new referrals 5791 5914 5971 5849 5471Total GP referrals 2577 2655 2609 2643 2436GP referrals - urgent suspected cancers for diagnosis 1720 1760 1584 1638 1486Referrals from Surrey 969 940 971 994 916
Personalised care - building molecular diagnosticsInternal referrals to the service 1341 1241 1452 1837 1549External referrals to the service 1043 1008 1036 1423 973Number of samples sent from patients recruited to CRUK Stratified Medicine Programme 109 164 215 192 66
Private carePP referrals 1027 1024 1075 1056 997
Efficient clinical modelsNo of inpatients discharged whose LOS > 15 days On hold
NHS Radiologist reporting time – variance to target (new measure) 1.9% -4.4% -3.1% -6.6% New in Q1PP Radiologist reporting time – variance to target (new measure) 3.4% -2.5% -2.3% -4% New in Q1Research (1 Qtr in arrears)70 day target (for externally sponsored trials) NIHR Adjusted figure (excluding delays attributed to
sponsor/neither sponsor or trust) 98.0% 90.9% 88.0% 90.0% 95.0%Accrual to target (1Q arrears) % of closed commercial interventional trials meeting
contracted recruitment target (excluding trials that had )
57% 57% 60% 64% 61%
2. To improve the productivity and efficiency of the Trust in a financially sustainable manner, within an effective governance framework
3. To deliver the Trust's clinical and research strategy; redefining our market position to better meet the needs of patients and commissioners, and increasing market penetration
Radiology

Page 3 of 3
The Royal Marsden NHS Foundation Trust. Balanced Scorecard 2015/16
m denotes Monitor standard
Workforce Q4(Jan-Mar
15/16)
Q3(Oct-Dec
15/16)
Q2(Jul-Sep 15/16)
Q1(Apr-Jun 15/16)
Q4(Jan-Mar
14/15)
Workforce productivityVacancy rate 6.3% 6.4% 6.8% 5.8% 5.8%Staff turnover rate 14.6% 14.3% 13.6% 13.6% 13.4%Stability rate (new measure) 88.3% 88.5% 88.8% 88.8% New in Q1Sickness rate 3.1% 3.2% 2.7% 2.8% New in Q1
Quality & developmentConsultant appraisal (number with current appraisal) 90.0% 72.9% 84.7% 81.8% 81.4%Appraisal & PDP rate 85.4% 84.8% 84.2% 78.4% 73.3%Completed induction 78.6% 73.4% 57.2% 46.7% New in Q1Statutory and Mandatory Staff Training 89.5% 86.8% 85.8% 84.2% 80.3%
Q4(Jan-Mar
15/16)
Q3(Oct-Dec
15/16)
Q2(Jul-Sep 15/16)
Q1(Apr-Jun 15/16)
Q4(Jan-Mar
14/15)m Community care data completeness referral to treatment information 75.0% 75.0% 75.0% 75.0% 75.0%m referral information 75.0% 75.0% 75.0% 75.0% 78.6%m activity information 76.2% 76.2% 76.2% 76.2% 76.2%
Q4(Jan-Mar
15/16)
Q3(Oct-Dec
15/16)
Q2(Jul-Sep 15/16)
Q1(Apr-Jun 15/16)
Q4(Jan-Mar
14/15)Recommend – Care 96.3% N/A 96.5% 94.7% 96%Not recommend – Care 1.8% N/A 0.5% 1.7% 1%
5. Monitor Community Measures
6. Staff Friends and Family Test - How likely are you to recommend this organisation to friends and family… as a place to receive care or treatment ('care')… as a place to k (' k')
4. To recruit, retain and develop a high performing workforce to deliver high quality care and the wider strategy of the Trust

BOARD PAPER SUMMARY SHEET
Date of Meeting:
1st June 2016
Agenda item 5.2
Title of Document: Proposed KPIs for 2016/17
To be presented by Chief Operating Officer
Executive Summary The Trust Balanced Board Scorecard is presented quarterly to both the Trust Board and Council of Governors. The scorecard aims to provide assurance and give an over-arching picture of Trust performance and any keys risks or issues. It is important, therefore, that the scorecard remains relevant. To this end a number of changes are proposed, and a more rigorous process of agreeing metric targets & thresholds is being introduced. This paper outlines the proposed changes to the scorecard for 2016/17. Recommendations The Board is asked to approve the proposed changes to the Board Scorecard for 2016/17. Author: Steven Francis, Director of Performance and Information
Contact Number or E-mail: ext 3451 / ext 8557
Date: 17th May 2016


Page 1
Proposed KPIs for 2016/17
1.0 Background
The Trust balanced board scorecard is presented quarterly to both the Trust Board and the Council of Governors. It is presented in the form of a RAG rated dashboard along with a narrative to explain any issues or areas of under-performance. Last year the format of the scorecard was updated to show the trend over 5 quarters and to simplify the layout. The metrics themselves have not been subject to any major revisions for over a year. It was agreed at the last Executive Board (EB) Away Day that the thresholds for Red/Amber/Green would be signed off by EB. This paper summarises the proposed changes to the scorecard metrics and their associated thresholds. The full proposed scorecard for 2016/17 is shown at Appendix B. 2.0 Rationale for Metrics
The scorecard comprises both nationally and locally defined metrics. The national metrics should always reflect the standards set for the Trust by the NHS and by Monitor. Accordingly the scorecard may change in-year in order to remain relevant if guidance or national requirements change. Locally defined metrics must be selected carefully and should meet the following criteria :-
• As a whole, the set of metrics must define the success criteria of the Trust for the year. A scorecard that is fully green would indicate a Trust this is performing well, meeting its key ambitions and has no major issues.
• The metrics must give the Board and Council of Governor an accurate picture of how the Trust is performing. That is to say metrics must not be chosen based on whether they would present performance in a favourable light. Indeed if the Trust is red-rated externally against a key target the Board and CoG should be aware of this.
• The scorecard is not a proxy for routine monitoring across all services. Only metrics that represent key standards or key ambitions should be included.
• Metrics on the board scorecard should not be unique to the board scorecard, and therefore should be part of regular review & action planning at a lower level in the Trusts performance framework.
Finally it should be noted the purpose of the quarterly Board Scorecard is different from the purpose of monthly departmental/CBU scorecards. The Board scorecard is intended to provide assurance to the board and gives an over-arching picture of performance and any key issues/risks. The CBU scorecards are a tool to show KPI performance and track improvement through local action plans to ensure successful delivery of the Trusts objectives. 3.0 Proposed Changes to Metrics for 2016/17
A number of changes are proposed to the metrics included in the scorecard for 2016/17. These changes align with a number of themes :-
1. In February 2016, Lord Carter of Coles published his review of Operational Productivity in NHS hospitals. In response to this, we intend to add a number of metrics to give the board visibility of some aspects of Trust productivity. In some

Page 2
cases these metrics are novel and have not been produced before, as such the value and stability of the data is untested. It is therefore proposed to introduce new productivity metrics cautiously, with a view to evolving this area further in the future when the data and potential definitional issues are better understood. For example, Lord Carter has suggested a 7% cap on corporate & administrative staffing costs, but there is currently no clear definition on what constitutes “administrative staff” in this context, nor are we clear on the applicability of this measure in a specialist Trust with both NHS and Private patients.
2. The Trust’s research portfolio is of significant strategic importance, and yet to date the scorecard has only included two metrics, one of which has not proved to be particularly informative. It is proposed that the range of research metrics is increased to give a more comprehensive view of the Trust’s successes and risks in this important area.
3. Some of the metrics previously published have become out of date or simply less relevant, these have therefore been updated. This includes changes such as replacing Local Quality Improvement Scheme (LQIS) achievement metrics with CQUINs (Commissioning for Quality and Innovation); removing CRUK recruitment and adding GEL recruitment; removing the downgraded Admitted & Non-Admitted RTT targets; simplifying metrics relating to referrals and adding in a metric on contract sanctions in recognition of the more financially punitive stance now adopted by commissioners.
A summary of the main proposed changes to the scorecard metrics are shown at Appendix A. 4.0 Thresholds for Metrics 2016/17
The Red, Amber and Green rating is set according to predetermined thresholds for each metric. National metrics are typically accompanied by national targets and these are used as the thresholds wherever these are applicable. National targets are either red or green, and do not have a concept of ‘amber’. The thresholds for locally defined metrics are set locally and will be approved by the Executive Board prior to the publication of Q1 data. The thresholds will be set with full knowledge of current baseline performance, and should be based on at least one of the following, in descending order of preference :-
(i) commissioned or contracted levels (ii) benchmarking data from comparable Trusts , where available (iii) accepted national levels of ‘gold standard’ or ‘best practice’ (iv) EB agreed levels set to be achievable but ‘stretching’ given current baseline
In previous years the Board and CoG have not been sighted on the actual thresholds and the basis upon which they has been set. It is proposed that this year, the set of thresholds is published alongside the Q1 report to aid assessment and interpretation.
Page 3
5.0 Summary
It is important that the board-level metrics and their associated thresholds for 2016/17 accurately reflect The Trust’s ambitions and appropriate quality standards for the coming year. The Board scorecard must remain a relevant document, however, and accordingly metrics may be changed throughout the year if required, with the approval of the Executive Board. More specifically the national and Monitor metrics may need to change if guidance changes, and will be reviewed in this light once the Monitor Risk Assessment Framework for 16/17 is published. The Board is asked to discuss and approve the proposed changes to the quarterly Balanced Board Scorecard for 2016/17.


Page 4
Appendix A
The following are recommended as new metrics for inclusion in 2016/17. Theme Description Rationale Finance CQUIN Performance (%) This was removed in 15/16 as
the Trust was not eligible for CQUINs. This year CQUINs return as part of the Trust’s contract and performance against this is both a quality and finance measure.
Finance Contractual Sanctions incurred (£) Commissioners are now enforcing contractual sanctions against key performance targets. The Trust stands to incur substantial financial penalties for both 18 week (RTT) and 62 days, among other targets.
Productivity Maintenance / m2 Following the publication of the report by Lord Carter, the Board has requested sight of some productivity metrics. The 8 listed here cover estates, medicines and activity.
Productivity Utilities / m2 Productivity Care Hours per Patient Day Productivity MDU patients per chair Productivity Imaging scans per machine
Medicines/ Productivity
%Unintended omitted critical medicines
These are both Carter review medicines optimisation metrics as well as being patient safety related.
Medicines/ Productivity
%Medicines reconciliation on admission
Research Local accrual against target The board scorecard has been traditionally light on research metrics, despite the relative importance of this area. These brand new metrics are proposed to give a fuller picture of the Trust’s research portfolio.
Research No. of 1st European patients in last 12mths
Research Patients on interventional trials as %age of new cancer patients
Research %age of trials with RMH as lead vs as participant
Strategy GEL Recruitment The Trust has now started recruiting patients to the 100k genome project.
Strategy Elective LoS Management of inpatient discharges and beds continues to be of key strategic importance. We have previously struggled to find metrics that monitor this adequately. The combination of Elective LoS and proportion of Elec/Non-Elec patients may be a better way to demonstrate if we are managing elective discharges and controlling the influx of non-elective patients.
Strategy % of Admissions that are Non-Elective

Page 5
The table below shows proposed amendments to existing metrics.
Theme Description Change Rationale Quality PP access to single rooms Merge Sutton &
Chelsea into a single trustwide metric
Performance continues to be good against both these metrics. Therefore a single trustwide view should be sufficient to ensure performance continues, and changes in performance can be investigated down to a branch level if required.
Finance LQIS % achievement Remove Replaced by CQUINs above Efficiency Radiologist time Remove The current presentation of
this metric was confusing. It is proposed that this is replaced by the new productivity metrics above (imaging scans/machine).
Strategy GP urgent suspected cancer
Remove Referrals are tracked in detail through PRG. It is important to retain a referral metric as this provides an important view of any changes to patient flows into the Trust. However, there is no need to retain 5 different referral measures. These should be condensed into 2 - NHS and PP.
Strategy Referrals from Surrey Remove Strategy GP Referrals Change to “Total
NHS Referrals”
Strategy Referrals to molecular diagnostics
Remove Currently this service is in Business As Usual and no requirement to track this at board level.
Strategy Recruitment to CRUK SMP
Remove No longer in active recruitment.
Waiting Times
Referral to Treatment – Admitted and Non-Admitted
Remove These are no longer active targets, only the “still waiting” target remains.
Workforce Stability rate Remove Finance Agency Spend (%)
Nursing Agency Spend (%)
Replace with “Total Spend Cap” %age +/- £9,074m
New Guidance issued by Monitor/NHSI

Page 1 of 2
The Royal Marsden NHS Foundation Trust APPENDIX BBalanced Scorecard 2016/17 (Proposed)
m denotes Monitor standard
Patient Safety, Quality & Experience Q1(Apr-Jun 16/17)
Q4(Jan-Mar
15/16)
Q3(Oct-Dec
15/16)
Q2(Jul-Sep 15/16)
Q1(Apr-Jun 15/16)
m Monitor governance risk rating G G G
m Quality Account indicators G G G
m G G G
Serious incidents (excl pressure sores) 2 0 3Complaints - % upheld 25.0% 30.0% 22.2%
MortalityHospital Standardised Mortality Ratio (rolling 12 month - qtr in arrears - NHS patients only) 77.2 83.3 90.4Mortality audit (based on qtr data in arrears) G A G30 day mortality post surgery 0.3% 0.4% 0.6%30 day mortality post chemotherapy 0.2% 0.3% 0.3%100 day HSCT mortality in previous 6 months (Deaths related to SCT) 3.2% 0.0% 7.3%100 day HSCT mortality in previous 6 months (All deaths) 3.2% 1.8% 7.3%
Medicines Management% Medicines reconciliation on admission New in Q1%Unintended omitted critical medicines New in Q1
Cancer stagingStaging data completeness sent to Thames Cancer Registry (1 qtr in arrears) 72% 65% 71%
Patient satisfaction Friends and Family Test (inpatient and day care) 97% 97% 97%Friends and Family Test (outpatients) 98% 97% 97%Waiting times for day chemotherapy (over 3 hrs) 12.4% 12.3% 11.4%Mixed sex accommodation breaches 0 0 0PP access to single rooms - Chelsea % 98.9% 99.9% 99.8%PP access to single rooms - Sutton % 100.0% 97.1% 98.9%
National waiting times targets
m 2 wk wait from referral to date first seen: all cancers 96.9% 95.9% 96.2%m symptomatic breast patients 95.4% 94.3% 94.2%m 31 day wait from diagnosis to first treatment 98.8% 98.7% 99.5%m 31 day wait for subsequent treatment: surgery 96.4% 98.4% 96.3%m drug treatment 100.0% 99.8% 99.8%m radiotherapy 98.5% 96.9% 98.3%m 62 day wait for first treatment: GP referral to treatment (reallocated) 88.4% 88.7% 85.4%
GP referral to treatment (pre-reallocations) 79.0% 78.9% 73.1%m Screening referral (reallocated) 93.7% 96.3% 93.0%
Screening referral (pre-reallocations) 90.8% 94.5% 89.8%m 18 wks from Referral to Treatment still waiting (incomplete) 94.8% 95.1% 93.2%
18 wks pathways - patients waiting > 52 wks. (distinct patients across the quarter) 6 2 3
Q1(Apr-Jun 16/17)
Q4(Jan-Mar
15/16)
Q3(Oct-Dec
15/16)
Q2(Jul-Sep 15/16)
Q1(Apr-Jun 15/16)
Recommend – Care N/A 96.5% 94.7%Not recommend – Care N/A 0.5% 1.7%
Q1(Apr-Jun 16/17)
Q4(Jan-Mar
15/16)
Q3(Oct-Dec
15/16)
Q2(Jul-Sep 15/16)
Q1(Apr-Jun 15/16)
m Community care data completeness referral to treatment information 75.0% 75.0% 75.0%m referral information 75.0% 75.0% 75.0%m activity information 76.2% 76.2% 76.2%
Certification against compliance : access to health care for people with a learning disability
3. Monitor Community Measures
2. Staff Friends and Family Test - How likely are you to recommend this organisation to friends and family… as a place to receive care or treatment
1. To achieve the highest possible quality standards for our patients, exceeding their expectations, in terms of outcome, safety and experience

Page 2 of 2
The Royal Marsden NHS Foundation Trust APPENDIX BBalanced Scorecard 2016/17 (Proposed)
m denotes Monitor standard
Finance, Productivity & Efficiency Q1(Apr-Jun 16/17)
Q4(Jan-Mar
15/16)
Q3(Oct-Dec
15/16)
Q2(Jul-Sep 15/16)
Q1(Apr-Jun 15/16)
m Monitor financial sustainability risk rating 3 3 3m %age variance from Agency Spend Cap New in Q1
Cash (£m) 34.7 33.9 30.6NHS activity Income Variance YTD (£000) -3257 -3685 -2000PP activity Income Variance YTD (£000) -568 -664 -95PP Debtors over 90 days (% of total PP debtors) 49% 37% 47%Non-PP Debtors over 90 days (% of total non PP-debtors) 36% 43% 41%Achievement of Efficiency Programme YTD (%) 89% 89% 93%Capital Expenditure Variance YTD (£000) -5,684 -4,429 -414Contractual Sanctions incurred (£000) New in Q1CQUIN %age achievement Acute New in Q1CQUIN %age achievement Sutton Community Services New in Q1
Productivity & Asset UtilisationBed occupancy - Chelsea 82% 83% 82%Bed occupancy - Sutton 80% 82% 82%Care Hours per Patient Day New in Q1Theatre utilisation - Chelsea 96% 95% 93%Theatre utilisation - Sutton 75% 87% 77%MDU Patients per Chair New in Q1Imaging scans per machine New in Q1Maintenance - Building, Engineering, Equipement (£000/sqm) New in Q1Utilities - Electricity, Gas, Oil, Coal (£000/sqm) New in Q1
Clinical and Research Strategy Q1(Apr-Jun 16/17)
Q4(Jan-Mar
15/16)
Q3(Oct-Dec
15/16)
Q2(Jul-Sep 15/16)
Q1(Apr-Jun 15/16)
Total NHS referrals New in Q1Total PP referrals 1024 1075 1056RMH Patients recruited to 100K Genome Project New in Q1
Efficient clinical modelsNHS Average (mean) Elective LoS New in Q1
NHS Non-Elective Admissions as %age of all NHS Admissions New in Q1
Research70 day target (for externally sponsored trials) NIHR Adjusted figure (excl delays attributed to
sponsor/neither sponsor or trust) 90.9% 88.0% 90.0%Accrual to target (1Q arrears) - National definition % of closed commercial interventional trials
meeting contracted recruitment target (excluding
57% 60% 64%Accrual to target (1Q in arrears) - Local definition New in Q1No. of 1st European patients in previous 12 months New in Q1Patients on interventional trials as %age of new cancer diagnoses New in Q1Trials lead by RMH as %age of all trials with RMH involvement
New in Q1
Workforce Q1(Apr-Jun 16/17)
Q4(Jan-Mar
15/16)
Q3(Oct-Dec
15/16)
Q2(Jul-Sep 15/16)
Q1(Apr-Jun 15/16)
Workforce productivityVacancy rate 6.4% 6.8% 5.8%Staff turnover rate 14.3% 13.6% 13.6%Sickness rate 3.2% 2.7% 2.8%
Quality & developmentConsultant appraisal (number with current appraisal) 72.9% 84.7% 81.8%Appraisal & PDP rate 84.8% 84.2% 78.4%Completed induction 73.4% 57.2% 46.7%Statutory and Mandatory Staff Training 86.8% 85.8% 84.2%
6. To recruit, retain and develop a high performing workforce to deliver high quality care and the wider strategy of the Trust
4. To improve the productivity and efficiency of the Trust in a financially sustainable manner, within an effective governance framework
5. To deliver the Trust's clinical and research strategy; to better meet the needs of patients and commissioners

BOARD PAPER SUMMARY SHEET
Date of Meeting:
1st June 2016
Agenda item 6
Title of Document: IM&T Strategy 2015-20
To be presented by
Chief Financial Officer/Dr Tim Wigmore
Executive Summary The Board reviewed the draft direction of the Information Management &Technology (IM&T) Strategy at its away day in November 2015. The Audit and Finance Committee had a ‘deep dive’ into the key elements at its January meeting and will continue to review progress against timetable. This paper includes a summary of the background, next steps and the financial requirement of the strategy, as well as the IM&T Strategy as a summarised brief. The brief focuses on the six IM&T strategic objectives the Trust will need to meet if it wishes to achieve its future organisational vision. The document provides the direction of travel for IM&T, which will be reviewed and updated as necessary, and highlights the key components required for successful delivery. The brief will be published for staff to understand the strategic direction of the IM&T strategy. It is presented for approval by the Trust Board. Recommendations The Board is asked to discuss and approve The Royal Marsden IM&T Strategy 2015-20. Author: Sam Ball – Director of IT
Contact Number or E-mail: 4250
Date: 24th May 2016


Information Management & Technology Strategy Introduction The purpose of this report is to request formal approval of the Information Management & Technology Strategy (IM&T) 2015-20 and outline the plan, timescales, financial requirements and next steps in delivering the IM&T objectives. Background The IM&T Strategy has been completed following significant input across the Trust. This paper includes the Strategy itself as a summary brief in brochure format, and timescales for the achievement of key milestones. The Trust has already undertaken a number of activities including the development of a draft EPR requirements specification, appointment of an EPR Programme Manager, appointment of a Chief Clinical Information Officer (CCIO) and establishment of the IT Programme Board (ITPB). The IT Programme Board meets monthly and is chaired by the CCIO. As a central Trust governance body it is made up of Executive Directors and other staff members from the leadership and senior management teams. All areas of the Trust e.g. clinical, patient administration, operations, corporate, IM&T are represented as well as Sphere and the ICR. Financial Requirements The strategy will require significant investment over the next five years in order to deliver the full programme. An indicative summary is set out in the table below which details the current capital investment in IT as well as an additional £30m required in order to deliver the Electronic Patient Record. This outline investment was discussed at the Board away day in November 2015.
The Executive Board have reviewed the capital requirement over the next five years and with the priority schemes and the investment in IT the Trust will need to consider alternative funding for its major equipment replacement programme, as the current financial position does not cover the complete capital requirement.

Next Steps Subject to Board approval of the IM&T Strategy, a dedicated multi-disciplined team reporting to the IT Programme Board will form to take forward the implementation of the IT Strategy. An Outline Business Case will be presented to the Audit & Finance Committee in January 2017. The case will assess each investment action against solution options, strategic fit, value for money, potential funding sources and return on investment in a format that will aid decision-making. Subject to approval, assurance and the recommendations of the Full Business Case, The Trust will proceed to procurement presenting a full business case for Board approval in January 2018. All documentation will use Trust HM Treasury green book compliant templates. Summary To remain a world-leader in cancer treatment and research it is recommended that The Royal Marsden continues to invest in IM&T. Approval and implementation of the IM&T Strategy will enable the Trust to improve its clinical care, patient safety and experience, and make IM&T fit for the future. The Board is asked to:
• Approve the IM&T Strategy 2015-20; • Approve the prioritisation of capital investment on the replacement of the
EPR; • Note the timeframe for delivering the Outline & Full Business Cases to deliver
the IM&T objectives.

1
IM&
T S
trategy
Authors: Samantha Ball, Director of IT and Dr Tim Wigmore, Associate Medical Director, and Chief Clinical Information OfficerDate: March 2016


Contents
1 Context of this document 4
2 Vision and strategic objectives 4
3 Alignment between Trust strategic themes and IM&T objectives 14
4 High level action plan 14
5 Conclusion 15
IM&
T S
trategy

4
1. Context of this Document
This document is a Strategic Brief and summarises the full IM&T Strategy. It focuses on the six IM&T strategic objectives that The Royal Marsden NHS Foundation Trust will need to meet if it wishes to achieve its future organisational vision.
2. Vision and Strategic Objectives
The Royal Marsden and The Institute of Cancer Research (ICR) work in partnership to translate science from bench to bedside and together are ranked in the top four centres worldwide for cancer research and treatment. Without state of the art technologies to enable research and support ‘Big Data’ initiatives, The Royal Marsden could risk falling behind the curve within the international research community. The Provision of Private Care is integral to the Trust’s strategic growth. Successful delivery of partnership and international models will be dependent on cutting edge technology.
Through extensive stakeholder engagement the Vision, Mission and Strategic Objectives for IM&T during the next five years have been define.
2.1 Vision & Mission
The strategic vision for IM&T is:
‘A world leading Trust in both treatment and research initiatives enabled and underpinned by world leading technologies’
The strategic mission for IM&T is:
‘To provide a robust and responsive IM&T service to the Trust, built on a solid infrastructure. To enable a world leading organisation through the implementation and support of innovative technologies, to deliver treatment and enable ground breaking bench to bedside research’
2.2. IM&T Strategic Objectives
2.2.1 Overall IM&T Strategic Objective
The Royal Marsden’s overall IM&T Strategic objective is to adopt an approach based on shared IT functional components and services. This will apply equally to both clinical and corporate systems. Wherever possible the components and services will be industry standard. Software as a Service (SaaS) and cloud based hosting will be utilised where this is cost-effective. Selection will be based on the component or service that meets the greatest number of the The Royal Marsden’s requirements. They will be combined to create solutions for individual specialties and functions and will be accessed through a common front end. The development resources within the The Royal Marsden will focus on integrating the functionality and filling any functional gaps.
2.2.2 Detailed IM&T Strategic Objectives
To achieve the IM&T Vision, Mission and respond to both local and national initiatives The Royal Marsden has identified six Strategic Objectives. These are explored in more detail below:
2.2.2.1 Replacement Electronic Patient Record (EPR)
As the diagram below illustrates an EPR is typically broken down into four major functional areas: Registration and Referral; Scheduling and Patient Management; Clinicals; and Coding, Reporting and Contracting. Workflow and Clinical Decision Support increase from left to right. Departmental and Specialist Systems for example Pathology, Radiotherapy and Chemotherapy etc. are usually integrated into the EPR using an interface engine. The grey boxes surrounding the EPR list additional services, which can typically be purchased to support the implementation, adoption and maintenance of the solution.

5

2.2.2.1.1 Case for Change
The Royal Marsden’s existing Hospital Information System (HIS) is a mixture of in-house developed applications and best of breed clinical solutions delivered through a clinical portal known as the Integrated Clinical Workstation (ICW). All patient data is captured in a single data store and stored within the Patient Event Table. There are six significant issues with the current solution which necessitate its replacement:
1. It is highly bespoke and requires specialist-programming resources to support and develop it. The limited size of available resource pool is a significant and an increasing risk to the Trust;
2. Information Technology is an obstacle to meeting regulatory requirements and supporting joined up working, because changing existing or developing new interfaces is complex;
3. Technological limitations combined with the lack of internal skills and the time consuming nature of any development make the current solution unsustainable;
4. The solution is missing capability in the following areas: e-Prescribing; Requesting and Results Reporting; Enterprise Scheduling; Aseptic Manufacturing; Theatre Management; Clinical Decision Support; and Outpatients Administration. Even if skilled resources were not a limiting factor the time to develop and get the appropriate patient safety accreditation for the functionality to fill these gaps would be prohibitive;
5. Retrieving patient data effectively is difficult because of:
a. how data is currently stored on the system;b. use of a complex multi-layered taxonomy; andc. a lack of consistent input formats and
undefined data collection processes and/or standard clinical workflow.
6. A homegrown system will continue to limit The Royal Marsden because changes and improvements can only come from the Trust’s experience. Conversely a specialist healthcare software solution will benefit from a whole industry of experience backed-up by multiple implementations in both the UK and other geographies.
EPR Components
Coding Reporting and
Contracting
Operational reporting
Clinical reporting
Clinical coding
Contracting and costing
Registration and Referral
Master patient/index
Patient registration
Referral management
waiting times
Scheduling & Patient Management
Inpatients/Daycases Bed management
Theatre management
Outpatient Management
Clinic managementTelephone contacts
Scheduling Case note tracking
Clinicals
Structured Clinical Assessments
Problems and diagnosis
Requests & Results Reporting
Allergies
Clinical decision Support
Care planning and nursing
documentation
Clinical Correspondence
Discharge planning
E-prescribingMedication
management
Rules and alerts
Clinical noting and annotation
Patient education
Vital signs
Implementation Services
Benefits Realisation
Change Management
Hosting Services
Service Management
Future Proofing R&D
Commercial Offer
Interoperability
Partnership working
Financial Offer
WORKFLOW
DECISION SUPPORT
Departmental &Specialist Systems
Electronic Document Management
Pathology PACS RIS Radiotherapy Chemotherapy
Longitudinal EPR view/External integration
6
2.2.2.1.2 Requirements & Needs
The top four strategic needs of a clinical or EPR solution to support the The Royal Marsden are:
• seamless integration with Trust systems, the wider health care economy and Strategic partners;
• strong and effective clinical functionality;
• streamlining /restructuring of clinical pathways; and
• increasing business efficiency including the enabling of easy access to research information and data.
2.2.2.1.3 EPR Options Appraisal
When considering the approach to an EPR the following four options have been considered:
1. Do Nothing – continue with the existing in-house Ethos based HIS/ICW;
2. Re-write the exist HIS/ICW – use the existing internal resources to re-write the existing solution in a more mainstream software development language;
3. Procure and implement an integrated suite of health care software from a single vendor e.g. Cerner or EPIC; and
4. Work with a partner organisation to incrementally replace the existing Hospital Information System.
Based on the options appraisal the recommendation is take options 3 and 4 forward and consider them further as part of the Outline Business Case for the EPR.
2.2.2.1.4 Proposed Roadmap
The proposed roadmap for the EPR is broken down into two stages.
Stage 1 – Replace the Integrated Clinical Workstation
This stage will be completed during 2015 – 2017 and will commence with the following two enabling activities:
1. Create an enhanced data warehouse and business intelligence/data analytics solution. This will involve restructuring the data and ensuring that it is accessible for reporting and searching. It will de-risk the later creation of the EPR because patient data will no longer be solely housed within the HIS/ICW environment;
2. Create a Vendor Neutral Archive (VNA) and implement electronic document management (EDM)1. These new systems will allow the storage, organisation/classification and retrieval of unstructured data such as pictures, videos and scanned paper documents. The EDM will be core functional component and as such will available to all users including the corporate functions e.g. Finance and HR. Its widespread use will support The Royal Marsden’s desire to remove paper from its processes.
Stage 1 will be completed by implementation of a device agnostic web based clinical portal. This will replace the current functionality of Integrated Clinical Workstation and allow access inside and outside The Royal Marsden including Community Services, helping the hub and spoke model of care and ensuring integration with other care providers including overseas organisations.
7

Stage 2 – Replace the Hospital Information System with an Electronic Patient Record
From 2016 – 2018 onwards The Royal Marsden will start to incrementally replace the internally developed Hospital Information System with the Electronic Patient Record provided by their healthcare IT partner. The Electronic Patient Record will include the following:
• Patient Administration System (including Outpatients)
• e-Prescribing (soon to be become mandatory for NHS Trusts) and e-Chemo,
• Requests and Results Reporting
• Clinical documentation (assessments, problems, allergies, diagnosis, noting and annotation)
• Nursing documentation (assessments, progress notes, care plans)
• Care Pathways
• Enterprise-wide Scheduling
• Alerts, Clinical Decision Support
• Other areas to follow for example Pathology (including Specialist Labs), Theatres, CCU, vital signs etc
• Information to support Private Care Accounts (alerts on patient’s funding status) and integration with billing systems
The diagram below shows the position of The Royal Marsden’s high-level IT System Components from 2016/17 onwards.
1
1 With Electronic Document Management the Trust would scan and digitise patient paper records to improve clinician access and reduce the cost of storing and transporting records. With EDM clinicians will have simultaneous 24/7 access to historic patient records and external paper based communication irrespective of their location.
Data Warehouse
Security Layer
Clinical Portal
Patients Other Providers GPs Clinicians
Business Intelligence
tools
Vendor Neutral Archive
Electronic Document
management
Interface E
ng
ine
Dep
artmen
tal System
s e.g
PAC
S, R
IS, C
IP, Patholog
y
Electronic Patient Record
IT Infrastructure – Sphere Shared IT Services
8
Outcome – An integrated Electronic Patient Record that supports the delivery of safe, efficient clinical care that positively impacts patient outcome and experience and enables research initiatives and consistent recording of high quality data. Implementation of core functional components that can be used to the support The Royal Marsden’s and Community Service’s clinical and administrative processes.
Benefits – High quality and reliable data supporting better patient outcomes, effective management of resources and enabling research and Private Care initiatives. Provides a cost-effective platform of functionality including EDM, Data warehouse and portal technology that can meet the requirements of both clinical and corporate users in both the hospital and community settings.
2.2.2.2 Enhanced Workflows & Processes
The current HIS/ICW does not have any standardised workflows. This poses a patient safety risk, as there is no scheduling and no workflow to ensure tests are ordered, results processed and reviewed by clinicians and standard activities are carried out as part of a pathway. It also contributes to poor quality and incomplete patient data. This means standards or “best practices” are difficult to maintain or enforce and under recovery of private patient income.
As shown in the above diagram the Electronic Document Management (EDM) system will append the EPR, and be viewable through the clinical portal to create a single electronic record for each patient. The EDM will be used for storing historic records and external paper based communications.
The importance of change management is recognised as key to the success of RMH’s future IM&T projects. Technology can never be fully optimised and fully support clinical and operational work without the appropriate change resource and funding being identified for each and every IM&T deployment. A key part of implementing successful sustainable change will be the relationships created between the clinical IT advocates and IM&T, but to realise the benefits of future IM&T projects additional resource, over and above people’s day jobs, will always be needed.
For projects of the size and impact of an EPR, expertise will be required across the full spectrum of business change including, stakeholder engagement, behavioural change, process optimisation and benefits management etc.
The most important element of any large-scale implementation is user buy in. To enable users to approach change with confidence, training and IT skills development will be essential.
IT up-skilling and knowledge transfer within The Royal Marsden’s IT department will also be of great importance to this programme and business as usual processes moving forwards. The Trust’s IT department will need to ensure that those responsible for implementation and change management employ practice methodologies such as ITIL and PRINCE2 and that their knowledge of such is continually assessed and progressed. Through the up-skilling of the IT staff, The Royal Marsden will become increasingly self-reliant, negating the need to call on external assistance for the management, implementation and review of systems, solutions or programmes of work.
Outcome – Changes to workflows and processes to improve the quality and range of data collected will be implemented at a pace that the organisation can assimilate thereby reducing the risk of the new systems being rejected or under utilised.
Benefits – Standardised data collection enabling better patient outcomes and higher quality research data. A comprehensive transformation programme empowering users to adapt easily to change. Confident use of the system enabling full optimisation of IT solutions.
2.2.2.3 Research and High Performance Computing
The acquisition, curation, management, analysis and exploration of data drives the medical research industry and is seen by The Royal Marsden as the third most important constituent after patients and staff.
The National Institute of Health Research Biomedical Research Centre at The Royal Marsden and The Institute of Cancer Research,

London currently undertakes research collaborations with Imperial College Healthcare, the Royal Brompton Hospital, the University Hospital Southampton, King’s College Hospital and the London Cancer Alliance. International collaborations include Memorial Sloan Kettering.
Data linkage is a key component to research initiatives. The Royal Marsden needs to join primary, secondary and community care with genomics and imaging data, to create true personalised medicine. This will allow it to understand a patient’s risk of genetically carried cancers and their likely response to treatment or preventative measures.
The data linkage is also paramount to understanding the use of data in answering basic questions of what The Royal Marsden does, how well research is undertaken and its cost effectiveness.
Additionally the potential of data integration technologies in aiding research initiatives has yet to be fully realised within the NHS. The creation of databases that span a cohort of Trusts would enable access to tens of thousands of patient records creating patient study cohorts in a matter of minutes rather than months. The database would be hosted within the data warehouse and accessed through the portal (these core components will be implemented as part of stage 1 of the EPR project). Through the security layer,
the portal will be able to give researchers access to an anonymised or pseudonymised data service. In this way the The Royal Marsden will be able to give appropriate self-service research datasets to the right person in the location of their choice. The Clinical Record Interactive Search (CRIS) system developed by the NIHR Mental Health Biomedical Research Centre and Dementia Unit at the South London and Maudsley (SLaM) NHS Foundation Trust has demonstrated the potential for similar data aggregation and analysis technology within the NHS2.
It is important that The Royal Marsden builds upon its world-class research portfolio through the establishment of a robust infrastructure and IM&T solutions that can support desired research activities and outcomes.
Outcome – Access to large amounts of high quality data to support the analysis of cancer and its care across multiple centres/data sets., for research purposes and to better understand resource requirements.
Benefits – Meeting of strategic objectives concerned with new models of care, health innovation and the development of new medicines and treatments. Financial stability through research generated income streams. Maintain and improve The Royal Marsden’s research collaborations and outcomes.
2.2.2.4 Mobile Working
The value of mobile technology in healthcare is now well established as the example from the Ottawa Hospital below illustrates:
“Not only has iPad increased efficiency from a provider perspective — it’s increased engagement between the provider and patient.” - Dale Potter, Senior Vice President Strategy and Transformation, The Ottawa Hospital.
The Ottawa Hospital rolled out iPads to its clinicians, managers and executive as a hospital wide solution the improvements in service included, increased patient interaction, substantial time savings and quick application development times3.
10

Mobile working is the ability to work anywhere, irrespective of place and time, enabling staff to access and update information and communicate on the go. Mobile working provides clinicians with the means to manage their time and workload better. They can communicate more freely with colleagues and patients, and have the flexibility to work in the office, at home or while travelling between the Trust’s sites.
There is increasing demand throughout The Royal Marsden for improved support for mobile working. A managed approach to the proliferation of tablet devices, users’ own devices or Bring Your Own Device (BYOD)4 and the unification of voice and data communications will be required if the introduction of mobile working is to be successful.
Mobile Device Management (MDM) solutions to monitor and support a move to mobile device and remote working will need to be procured to realise full benefits of mobile and remote working.
A strategy will be developed for supporting mobile working, which addresses the aspects mentioned above and also tackles the organisational changes that are required to operate this technology safely and cost-effectively and to maximise the benefits gained. It will also be necessary to ensure users of new technologies and devices are confident in their approach to using them.
Outcome – to be able to provide patient care at the right location at the right time by the right member of staff regardless of location.
Benefits – reduction of lost working time for staff whilst travelling, greater productivity, allowing and enabling flexible working conditions for staff.
2.2.2.5 Provision of Resilient and Robust Infrastructure
During the stakeholder interviews held as part of this engagement, the need for investment in and improvement of The Royal Marsden’s infrastructure was identified to support all IM&T initiatives moving forwards. It was stressed that often the infrastructure fails and thus impedes the work of the system users. The investment in infrastructure must also include future proofing to enable The Royal Marsden to advance in digital maturity through flexible and responsive system support. Many of the current infrastructure issues appear to have arisen from a lack of future proofing in past upgrades. The Trust’s Wi-Fi implementation, for example, was intended for computer use on the wards and access to clinical systems. However, the same Wi-Fi provisions are now being used for not only clinical needs but also for patient needs. The streaming of videos and games for inpatients, access to email, Skype and Facebook have all meant the intended use and actual use of The Royal Marsden’s infrastructure do not align. These issues mean that there is no choice but to invest in infrastructure upgrades to support the Trust wide implementations that are required as discussed in this strategy.
1
2 http://www.slam.nhs.uk/research/d-cris3 http://www.apple.com/ipad/business/profiles/ottawa-hospital/4 BYOD – Bring Your Own Device refers to the use of consumer devices and applications in the workplace. These devices can access the Trusts systems through portal or app based technologies. Data is not stored on the device and access to data sources can be monitored or removed by system administrators
11

The Royal Marsden needs to ensure that its infrastructure is:
• Adaptive and robust enough to support a Trust wide EPR solution;
• Responsive and open enough to support the needs of patient access and telehealth solutions;
• Scalable to support the growth model for private care;
• Functionally integrated so that for example the Private Care billing solution is fully connected with and accessible from the EPR, so that income from all sources can be recovered effectively;
• Secure and flexible enough so that data can be stored and retrieved to enable the Trust’s research programmes; and
• Supports more flexible working patterns e.g. hot-desking and home working by utilising technologies such as Unified Communications and Virtual Desktop Infrastructure.
Outcome – Deliver a responsive and flexible IT foundation upon which planned clinical and research and private care developments can be confidently implemented.
Benefits – Ability to fully optimise the use of all solutions. Bill private patients appropriately and recover income. Reduction in system down time and system unavailability for users. Future proofing enabling responsive changes to technologies and requirements.
2.2.2.6 Telehealth, Patient Portal and Apps
Three areas of technological innovation have been highlighted as strategic priorities:
1. Telehealth. This is use of communication and information technologies to deliver clinical care where the individuals involved (be they health care professionals or patients) are not at the same location. Telehealth also covers telecommunication to deliver non-clinical services such as research and health education promotion.
Telehealth technology is now also widely available and has been successfully implemented in numerous care settings5. Connecting patients in their home to clinicians through video technology has been proven to drastically reduce hospital admissions, reduce travel expenses, and lead to more rapid and efficient provision of health care for patients who are not able to travel easily. It has also been shown to improve the end of life care of patients who have trialled this approach at NHS Trusts.
Telehealth is essential to support the Private Care growth model, particularly in support of overseas patients and international partnership working.
During the lifetime of this strategy, The Royal Marsden intends to provide technology to facilitate telehealth including provision for self-care management, virtual clinics and consistent monitoring across the health economy.
The action plan for implementing this strategy includes the exploration and trialling or piloting of appropriate telehealth technologies.
12

13
1
5 http://www.airedale-trust.nhs.uk/services/telemedicine/case-studies/Gloucestershire Care Services NHS Trust – “For both heart failure and respiratory services, we have had increased efficiencies, larger case loads, and avoided admissions. I believe it’s been very cost effective,” Strain said. “My quick calculations are that we’ve saved £399,744 on admissions.”http://www.digitalhealth.net/news/ehi/8759/specialist-telehealth-ser-vice-a-success/6 NHS Innovations South East – App Development, An NHS Guide for Developing Mobile Healthcare Applications - May 2014.
2. Patient Portal. The NHS Five Year Forward View (FYFV) states that patients must have more access to their healthcare information and must have increased control over the care that is provided to them supporting them to manage their own health in a way that is suitable for them. One of the ways for achieving this objective is to provide a Patient Portal, which would give patients and their lay carers access to selected parts of their health care record. Used in conjunction with for example telehealth or remote monitoring solutions, the Portal will support more distributed models of care.
3. Apps. An App is a self-contained program or piece of software designed to fulfill a particular purpose. The number of apps for web-enabled mobile devices including smart phones and tablets continues to grow rapidly and this is starting to have an impact on the healthcare market. The ubiquitous nature of the devices, the ease of development and the simplicity of the user interface, which make them easy to use and deploy are putting pressure on many Trust IT departments to develop their own local Apps. However, development of Apps within a healthcare setting must be carefully controlled and tested to ensure that the applications are fit for purpose and do not pose any clinical or patient safety risks.
NHS England are in the process of developing a comprehensive quality control assessment for the development of applications, some NHS bodies, NHS Innovations South East for example, have development their own outline for the development and management of applications.6
Outcome – Care provided in locations that best suit the patient and that reduces unnecessary travel, enabling self-management, enhanced health ownership and the expansion of Private Care. Patients and their carers will be able to use a portal as an alternative/enhanced route for exchanging information between themselves and their clinical team. Apps will be developed and introduced in a controlled manager to minimise the risks to clinical/patient safety.
Benefits – Better patient outcomes through support for alternative models of care. Exploitation of technology to reduce unnecessary costly admissions and encouragement of better use of scare hospital resources and estate and closer working with international partners to deliver Private Care.

14
3. Alignment between The Royal Marsden Strategic Themes and IM&T Objectives
As the figure below illustrates there is a close alignment between the The Royal Marsden Strategic Themes and the six IM&T Strategic Objectives:
Trust Strategic Themes
Innovation and precision medicine
New systems of care
Modern infrastructure
Financial sustainability and best value
YESEPR YES YES YES
YESWorkflow & processes YES YES
YESResearch /HPC YES YES
YESMobile YES YES
YESInfrastructure YES YES
YESTelehealth/Portal/Apps YES YES
IM&
T S
trat
egic
Ob
ject
ives
4. High Level Action Plan
To achieve the strategic objectives it is recommended that The Royal Marsden implement the following high level action plan:
2015/16 2016/17 2017/18 2018/19 2019/20
Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4
Electronic Patient Record
Workflows and Processes
Research & High Performance Computing
Mobile working
Infrastructure
Telehealth Outline Business Case and Pilot
Workflow analysis
Design process improvements
Implement process improvements
Outline Bus Case Procurement Implementation
Gather requirements
Business case Procurement Implementation
Prepare strategy Deliver mobile working strategy
Complete transfer to Sphere and stabilise Procure rollout additional infrastructure
Telehealth research pilots
Lessons learnt and rollout of successful pilots
Pilot patient portal
Roll out patient portal

5. Conclusion
To remain a world-leader in cancer treatment and research it is recommended that The Royal Marsden continue to invest in IM&T. Completion of the actions outlined in this document will enable The Royal Marsden to improve its clinical care, patient safety and experience, and make it fit for the future.
Before expenditure is committed on a project an Outline Business Case (OBC) will be presented to the Trust Board for approval. The OBC will assess each investment action against solution options, strategic fit, value for money, potential funding sources and return on investment and will be presented in a format that will aid the decision-making of the Trust Board. For the larger more complex procurements e.g. the EPR or where there is uncertainty about the requirements e.g. High Performance Computing then The Royal Marsden will follow procurements based on competitive dialogue.
15


BOARD PAPER SUMMARY SHEET
Date of Meeting:
1st June 2016
Agenda item 7.1
Title of Document: Quality Account for April 2016
To be presented by
Chief Nurse
Executive Summary The monthly Quality Account reports the current Trust performance against the targets for 2016/17 described in the Annual Quality Account (2015/16) under the following three nationally agreed categories:
• Safe care; • Effective care; and • Patient experience.
Recommendations The Board is invited to note the performance of the Trust against the agreed national and local quality targets for April 2016 and the actions being taken. Author: Chief Nurse
Contact Number or E-mail: x2121
Date: 18th May 2016


1
The Royal Marsden NHS Foundation Trust Quality Account for April 2016 presented to the May 2016 Board.
Dr. Shelley Dolan, Chief Nurse
1.0. Introduction
The monthly Quality Account reports the current Trust performance against the targets for 2016/17 described in the Annual Quality Account (2016/7) under the following three nationally agreed categories:
• Safe care • Effective care • Improved Patient experience.
1.1. Data Quality Information and data at the Royal Marsden is produced by a centralised expert team separate from the clinical and operational teams. This separation and expertise is critical to ensure that the data is accurate and is not affected by the operational teams who are trying to comply with local and national improvement targets. All healthcare associated incidents, falls, medication incidents and pressure ulcers are reported locally onto the central Datix incident reporting system. The Datix analyst from the risk management team who is completely separate to the clinical care team compiles the reports for the quality account. All falls and medication incidents are also reviewed by subject matter experts to ensure accuracy and learning from themes. Every month a report is generated for each clinical area and if there is a reduction in reporting there is a central and local alert with action taken.
2.0. Safe Care
2.1. Reduction in Healthcare Associated Infections (MRSA bactereamia and C Difficile infections)
Target: <31 C Difficile infections and <1 MRSA bactereamia
The NHSE guidelines on reporting of C.Dificile infection (CDI) allows commissioners to use discretion as to whether a case is considered against the trajectory. Only cases deemed as a ‘lapse in care’ are attributed against the objective number (for the RM in 16/17 =31 cases). Where a Trust can demonstrate that the case is a single isolated case, or there are sound clinical reasons which may lead to CDI (such as chemotherapy or gut surgery) and that procedures have been correctly followed including antibiotic prescribing, hand hygiene, device care and environmental cleaning, then the commissioners are able to exclude the case from trajectory numbers. The C. difficile toxin objective for 2016/17 has been set at 31 again this year. In 15/16 there were two cases that were categorised as “lapse in care” by the commissioners and therefore counted against the trajectory of 31.

2
Table 2.1
No. Organism RM attributable April 16
YTD Trajectory
1. MRSA
bactereamia
0 0 0*
2. C.Difficile
4 4 31
*MRSA has a target of zero but Monitor has a de minimus of six cases.
In April/May there has been an increase in CDI cases on the Blood and Marrow Transplant Unit (5 cases) therefore a special case management meeting was held with the Infection Prevention and Control team and the clinical and cleaning teams. All samples have been sent off for ribotyping and once returned it will be clear whether there has been any cross infection. No lapse in case has been identified to date although there was building work being undertaken on the wards at the time.
2.2. Rate of patient safety incidents and percentage resulting in severe harm or death
To include: • Reduction of severe/moderate risk medication errors • Reduction of harm from falls
Target: Reduction in the rate of patient safety incidents per 100 admissions and the proportion that have resulted in severe harm or death
2.3. Reduction in Falls Target: < 0.7 moderate and above (resulting in harm) falls per 1000 bed days Year to date - to the end of April 2016 the Trust has met the target.

3

4

5
Severity of Patient Fall incidents: 3 - Severity - Current Period
2015 05
2015 06
2015 07
2015 08
2015 09
2015 10
2015 11
2015 12
2016 01
2016 02
2016 03
2016 04 Total
No Harm 12 12 16 8 18 13 15 10 18 18 24 9 173 Low / Minor (Minimal harm) 1 13 3 11 11 9 9 6 5 7 13 9 97 Moderate (Short term harm) 0 0 0 0 0 0 1 0 1 1 0 0 3 Severe / Major (Permanent or long term harm) 0 0 0 0 0 0 0 0 0 0 0 0 0 Death / Catastrophic (Caused by the incident) 1 0 0 0 0 0 0 0 0 0 0 0 1 Totals: 14 25 19 19 29 22 25 16 24 26 37 18 274 % Harm Patient Fall 14% 52% 16% 58% 38% 41% 40% 38% 25% 31% 35% 50% 37%
2.4. Reduction in medication errors Target: To increase the reporting of near misses and decrease the incidents that cause actual harm (low<2 per 1000 bed days and moderate <0.17 per 1000 bed days). N.B. To place medication errors in perspective, annually 0.09% of all medicines administered result in a medication error. For April 2016, the figure is 0.08%. There has been over a 3 fold increase in medication incidents categorised as near miss in comparison to the same period in 2014/2015. A streamlined near miss reporting method utilising the current IT system has now been embedded. The Pharmacy department has been raising awareness on reporting near misses and a plan has been agreed at the Executive Medication Safety Group to increase identification and reporting to ensure the organisation has more access to near miss reporting. In the current period, 1241 attributable medication incidents have been reported using the IT system Datix, of which 69% caused no harm. 372 incidents have been categorised as low severity and 7 incidents as moderate severity (resulting in harm), this represents 6.18 and 0.12 medication incidents per 1000 bed days respectively. As such, the Trust has missed the target relating to low severity medication incidents, however the target relating to moderate severity incidents has been met.

6

7
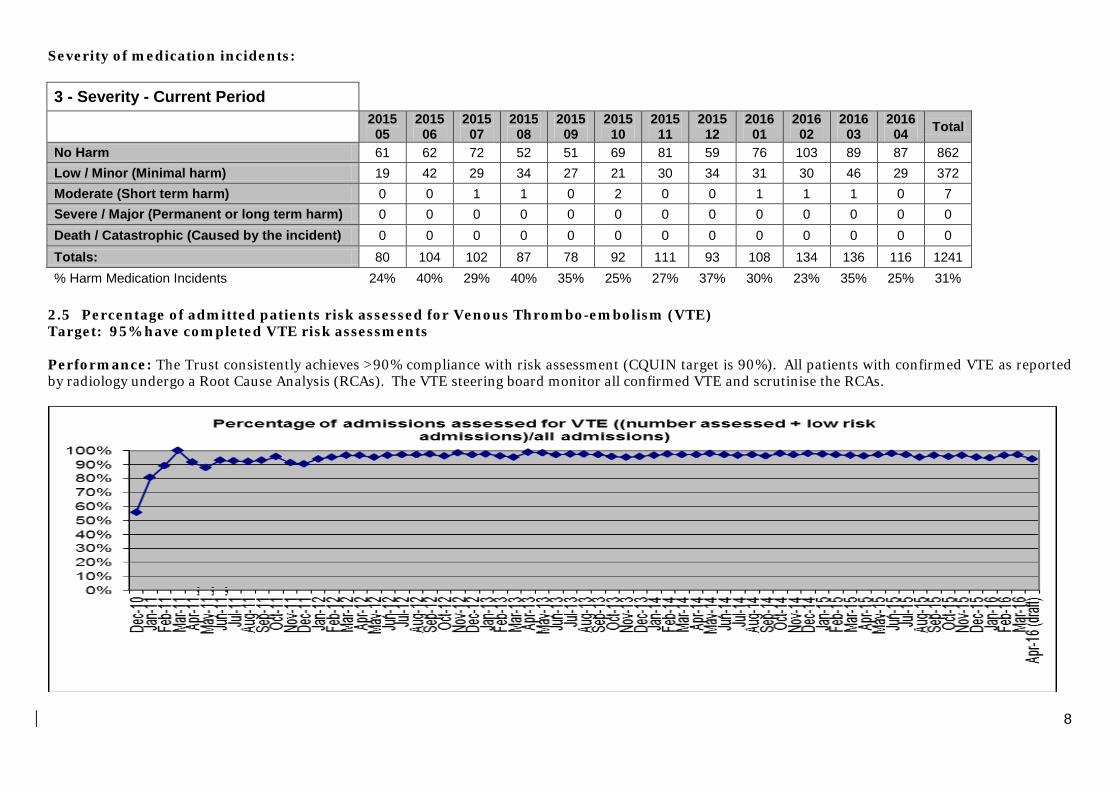
8
Severity of medication incidents: 3 - Severity - Current Period
2015 05
2015 06
2015 07
2015 08
2015 09
2015 10
2015 11
2015 12
2016 01
2016 02
2016 03
2016 04 Total
No Harm 61 62 72 52 51 69 81 59 76 103 89 87 862 Low / Minor (Minimal harm) 19 42 29 34 27 21 30 34 31 30 46 29 372 Moderate (Short term harm) 0 0 1 1 0 2 0 0 1 1 1 0 7 Severe / Major (Permanent or long term harm) 0 0 0 0 0 0 0 0 0 0 0 0 0 Death / Catastrophic (Caused by the incident) 0 0 0 0 0 0 0 0 0 0 0 0 0 Totals: 80 104 102 87 78 92 111 93 108 134 136 116 1241 % Harm Medication Incidents 24% 40% 29% 40% 35% 25% 27% 37% 30% 23% 35% 25% 31%
2.5 Percentage of admitted patients risk assessed for Venous Thrombo-embolism (VTE) Target: 95% have completed VTE risk assessments Performance: The Trust consistently achieves >90% compliance with risk assessment (CQUIN target is 90%). All patients with confirmed VTE as reported by radiology undergo a Root Cause Analysis (RCAs). The VTE steering board monitor all confirmed VTE and scrutinise the RCAs.

9
3.0 Effective Care
Incidence of Trust acquired pressure ulcers
3.1 The number and severity of healthcare acquired pressure ulcers are used internationally as a proxy for the effectiveness of care provision. Many people with cancer and or co-morbidity are more vulnerable to tissue damage for the following reasons; multiple hospital admissions, frailty, multiple drugs including high dose steroids (decreases skin elasticity), immobility, malnutrition or susceptibility to infection.
3.2 Data for this report was taken on 3 May (hospital) and on 5 May (SCHS) 2016 from DATIX. Data may have been updated since. From 1st April 2016 community services data only contains pressure ulcers reported from Sutton Community Health Services.
3.3 Total number of patients with the Trust (hospital/community services) attributable pressure ulcers for the month of
April 2016: 32 [Hospital=19, Community services=13] For serious incident reporting to Steis [Strategic Executive Information System] as Hospital/Community Services. Number of patients with Trust attributable pressure ulcers at categories 3 and 4 for the month of April 2016: 7 [Hospital=0, Community services=7]

10
Number of patients with Trust attributable category 3 and 4 pressure ulcers
0
2
4
6
8
10
12
Apr Jun Aug Oct Dec Feb Apr Jun Aug Oct Dec Feb Apr
Number of patients with Trust attributable category 3 and 4 pressure ulcers,
April 2014- April 2016
hospital
community services

11
Number of patients with Trust attributable pressure ulcers, all categories

12
Description of European Pressure Ulcer Advisory Panel (EPUAP) pressure ulcer classification system.
EPUAP Description of Stage 1 Non blanching redness of intact skin 2 Partial thickness skin loss or blister 3 Full thickness skin loss (fat visible) 4 Full thickness tissue loss (muscle/bone visible)
3.4 Emergency re-admissions to hospital within 28 days of discharge Target: Reduction in the number of avoidable re-admissions to hospital within 28 days of discharge Some emergency re-admissions following discharge from hospital are an unavoidable consequence of the original treatment, however some can be potentially avoided through ensuring the delivery of optimal treatment according to each patient’s needs, careful planning and support for self care. It is important to note that some readmissions will inevitably include patients who are admitted with side effects of treatment therefore it may be difficult to explain any differences between RMH with other acute Trusts. Performance: Within 28 days of original admission there were the following emergency admissions:
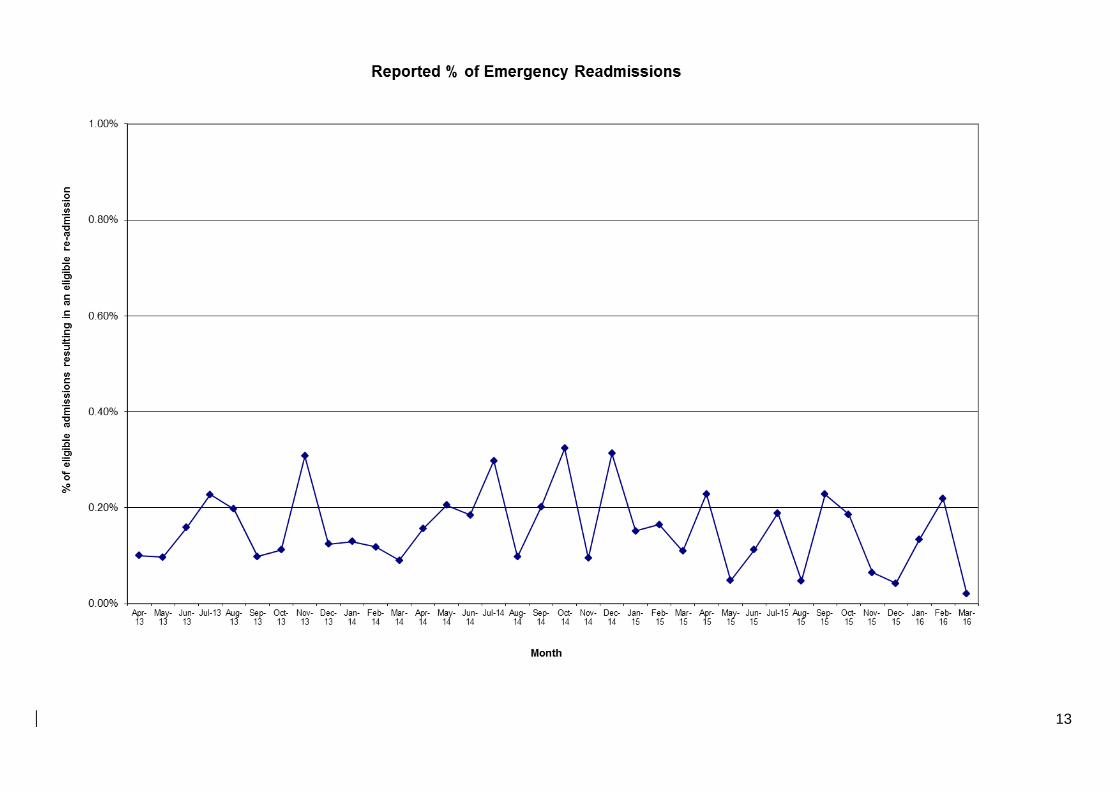
13
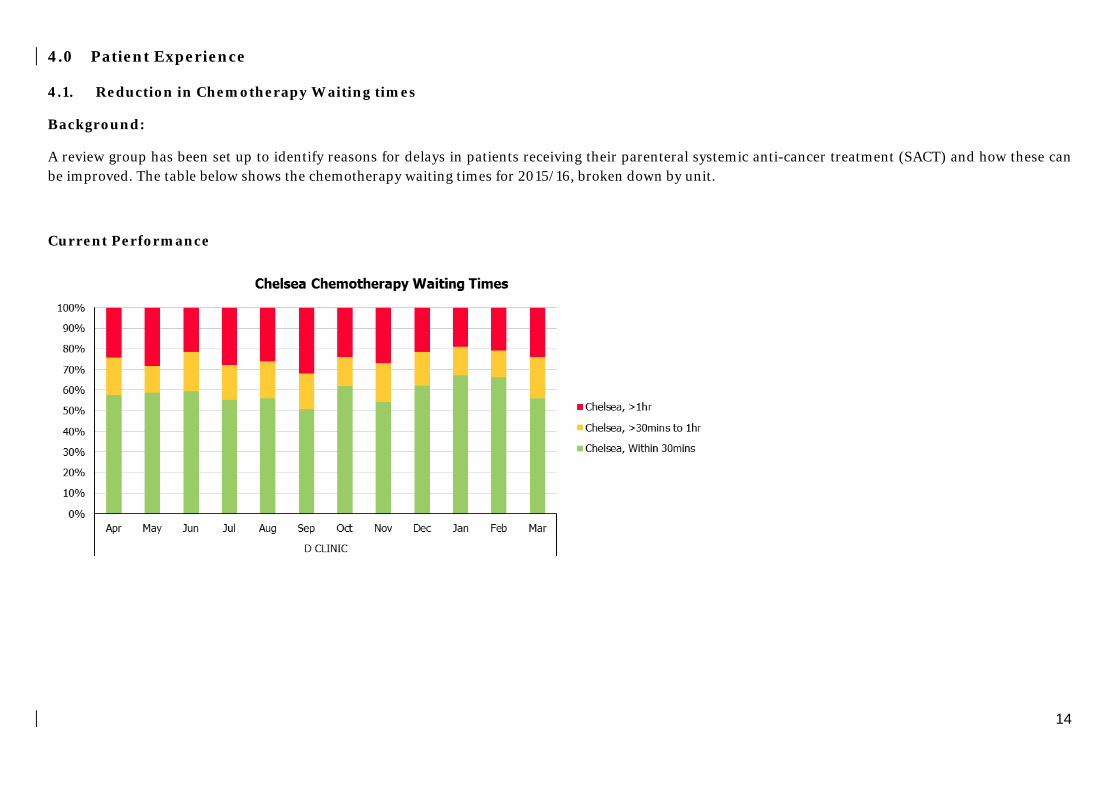
14
4.0 Patient Experience 4.1. Reduction in Chemotherapy Waiting times
Background:
A review group has been set up to identify reasons for delays in patients receiving their parenteral systemic anti-cancer treatment (SACT) and how these can be improved. The table below shows the chemotherapy waiting times for 2015/16, broken down by unit.
Current Performance

15
4.1.1. Service improvement initiatives 2015-16
Much has been done to improve the prescribing, screening, ordering and making of chemotherapy. These are summarised below
1) E-CHEMO E-chemo was introduced in October 2014 as a pilot in the Lung unit, and subsequently rolled out to all adult clinical units throughout 2015-16. E-chemo has facilitated a more streamlined patient pathway through reduction in prescription transit time, real time updates to the system, remote access. In addition, the system is able to be interrogated to provide significant audit data and enable quality improvement / route cause analysis of quality exceptions. This has also enabled production of regular reports on the efficiency of different parts of the chemotherapy prescribing and supply pathway; pre-prescribing and pharmacy pre-screening performance is now available via the Trust’s Cognos platform.
2) Pre-prescribing of chemotherapy Pre-prescribing of chemotherapy >5days in advance of patients’ appointments is well established within the Trust in recognition of the significant benefits related to chemotherapy ordering and availability for patients.
Although improvements have been made in areas, the overall pre-prescribing rates >5 days remains at 85%. Discussions have taken place with clinical units where the rates can be improved and this needs further focus and ownership by the CBUs.
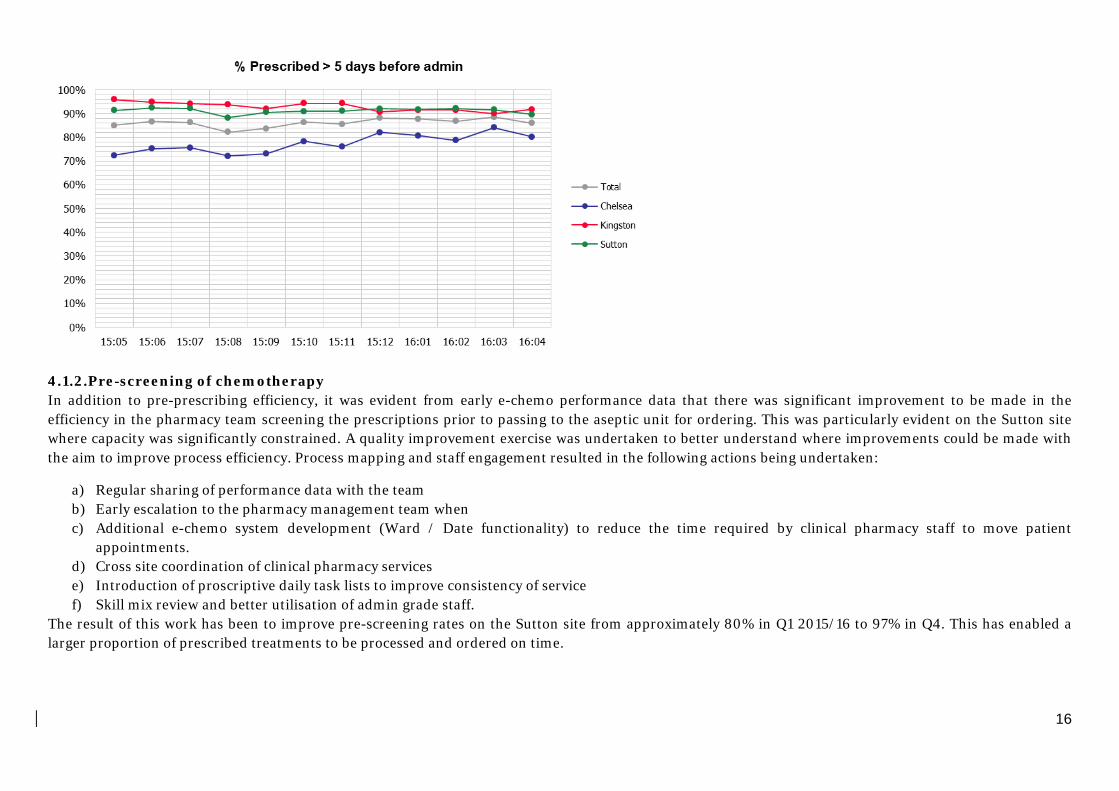
16
4.1.2.Pre-screening of chemotherapy In addition to pre-prescribing efficiency, it was evident from early e-chemo performance data that there was significant improvement to be made in the efficiency in the pharmacy team screening the prescriptions prior to passing to the aseptic unit for ordering. This was particularly evident on the Sutton site where capacity was significantly constrained. A quality improvement exercise was undertaken to better understand where improvements could be made with the aim to improve process efficiency. Process mapping and staff engagement resulted in the following actions being undertaken:
a) Regular sharing of performance data with the team b) Early escalation to the pharmacy management team when c) Additional e-chemo system development (Ward / Date functionality) to reduce the time required by clinical pharmacy staff to move patient
appointments. d) Cross site coordination of clinical pharmacy services e) Introduction of proscriptive daily task lists to improve consistency of service f) Skill mix review and better utilisation of admin grade staff.
The result of this work has been to improve pre-screening rates on the Sutton site from approximately 80% in Q1 2015/16 to 97% in Q4. This has enabled a larger proportion of prescribed treatments to be processed and ordered on time.
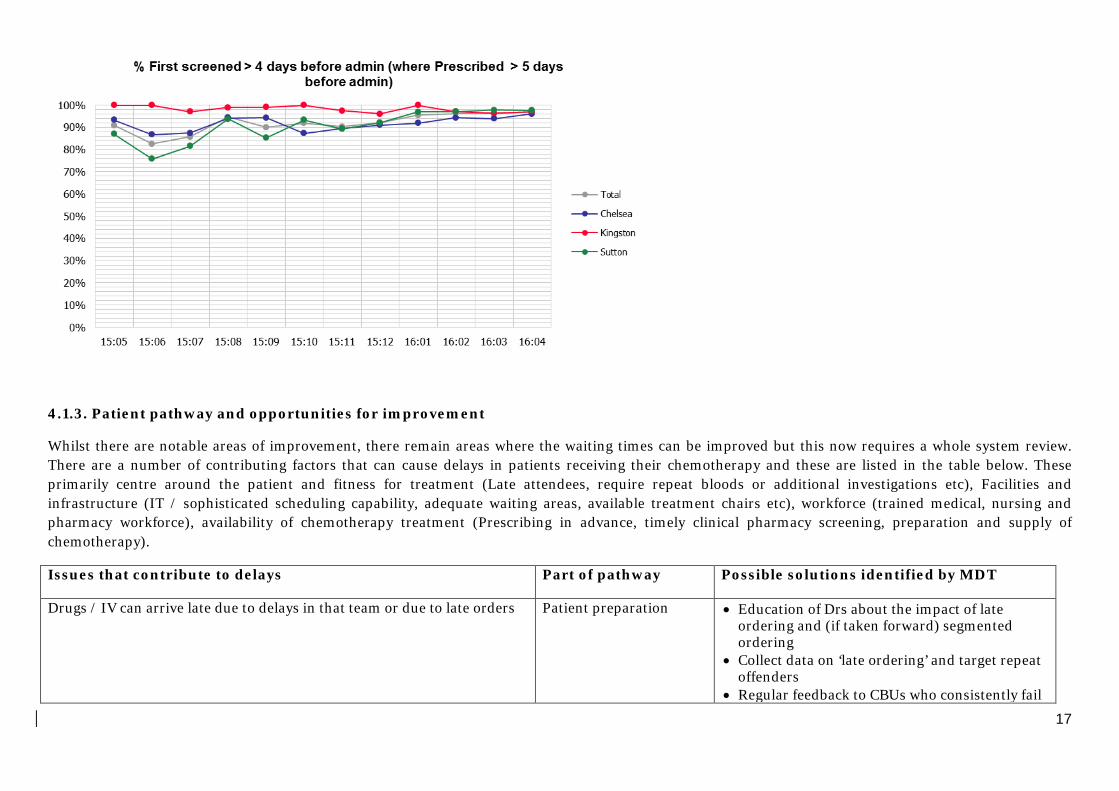
17
4.1.3. Patient pathway and opportunities for improvement
Whilst there are notable areas of improvement, there remain areas where the waiting times can be improved but this now requires a whole system review. There are a number of contributing factors that can cause delays in patients receiving their chemotherapy and these are listed in the table below. These primarily centre around the patient and fitness for treatment (Late attendees, require repeat bloods or additional investigations etc), Facilities and infrastructure (IT / sophisticated scheduling capability, adequate waiting areas, available treatment chairs etc), workforce (trained medical, nursing and pharmacy workforce), availability of chemotherapy treatment (Prescribing in advance, timely clinical pharmacy screening, preparation and supply of chemotherapy).
Issues that contribute to delays Part of pathway Possible solutions identified by MDT
Drugs / IV can arrive late due to delays in that team or due to late orders Patient preparation • Education of Drs about the impact of late ordering and (if taken forward) segmented ordering
• Collect data on ‘late ordering’ and target repeat offenders
• Regular feedback to CBUs who consistently fail

18
to meet minimum service standards
Delays in supplying SACT from pharmacy.
This is due to late orders and dose reductions, staffing constraints, aging software & facilities, multiple entries required on to three different software systems.
Patient preparation • Regular meetings now being held between Aseptic unit and MDU / wards and Clinical trial areas to improve scheduling.
• A drive on ordering well in advance from external partner (Hospira).
• Dose banding and purchasing in batches to dispense ‘off the shelf’ will speed up dispensing times.
‘Difficult’ cannulations (taking longer than 30mins); either one off or ‘repeated’ difficulties (with limited feedback about booking these patients with ‘extra’ time)
Patient preparation • Enhanced cannulation training • Re-deployment of Trust IV team for difficult
cannulations • More warm water facilities (promote
vasodilation) • Additional time built into schedule for patients
with regular challenges in venous access Bloods done >24 hrs in advance of treatment in order to facilitate 2-stop pathway – number of patients subsequently require repeat blood tests on day of treatment.
Patient preparation • Quicker blood test mechanisms for this cohort of patients (potentially ‘point of care’ testing)
Delays in getting samples to labs (possibly due to bundling of samples or delays in being transported around the hospital)
Patient preparation • Need data regarding source of delays – i.e. time taken on whole pathway, not simply turnaround within labs
Chairs are not always available (e.g. due to overrunning) Infrastructure / Space • Creation of additional space in Mobile Chemo Unit
• Build in flexibility into schedule for ‘some’ appointments
Patients arrive late (e.g. due to delays for getting a car park spot) Infrastructure / Space • Update patient information / patient education about blood requirements and ‘space issues’
Overruns / Limited flexibility of seats (due to high utilisation) / inflexible schedule
Infrastructure / Space • Build in flexibility into schedule for ‘some’ appointments
Short staffed / nursing availability Schedule / management of service
• Availability of MDU ‘supporter’ (floating / supernumerary role to support MDU nursing team)

19
Length of appointment is unrealistic / incorrect for regimen Schedule / management of service
• Measure ‘compliance’ with type of appointment
4.1.4. Aseptic preparation and supply
Significant work and review has taken place within the aseptic unit to improve the processing, ordering and manufacturing of SACT.
Improvements have been made in the ordering from the external partnership with Hospira and a new contract is about to be signed with Hospira to allow batch production of SACT for common doses used. This will significantly improve the turnaround time for supply of SACT as doses will be available ‘off the shelf’.
There is a remaining concern on the aging manufacturing facilities on both sites and these will form part of the capital works programme in the coming 2-3 years. The current manufacturing IT system that is used to order SACT needs replacing as this does not facilitate an efficient way of working. The replacement of the manufacturing system will be reviewed as part of the Trust EPR replacement programme.
4.1.5. Next steps and recommendations for 2016/17
1) Identify a lead / group to identify and improve the contributing factors to efficient prescribing, supply and administration of SACT across the Trust and target improvements in all of these.
2) Prospective Qualitative audit to establish route cause for all patients on MDUs waiting >30mins for their chemotherapy administration. June 2016. Associate Chief Pharmacist, Clinical Services.
3) Introduce batched production of dose banded SACT from Hospira. October 2016. Chief Pharmacist / Associate Chief Pharmacist. 4) Consider introduction of electronic scheduling to manage the scheduling of chemotherapy administration on MDUs.
20
4.2. Ensure that we are responding to inpatient’s personal needs: The Friends and Family Test
The NHS “Friends and Family Test” was announced by the Prime Minister on 25 May 2012. The national mandated question asked is:
“How likely are you to recommend our ward to friends and family if they need similar care or treatment?”
The patients then select their answer from the following Likert Scale:
Extremely likely; Likely; Neither likely nor Unlikely; Unlikely; Extremely unlikely; Don’t know.
The Royal Marsden has then chosen to add a second question:
What was good about your care and what could be improved?
Patients answer this question with free text comments.
4.2.1. April 841 responses overall: Inpatients 252, Day Care 278, Outpatient (OPD) 320
Inpatient: 22 patients made the following suggestions for improvement:
There could be a great improvement in toilet and showering conditions i.e not enough toilets or shower cubicles.
More advice on diet would be helpful when choosing from the menu.
Less noise during the night time period if possible i.e staff to move around quiet.
For breast surgery (which involves a lot of padding about the hospital for mammograms wires, injections etc) whether a front opening hospital grown might be better – I have to wear 2 gowns – or maybe a gown with slits like a nursing nightie.
I was watching the cleaner clean the cubicle after a patient had been discharged. She rung a cloth out dipped in antiseptic wiped down the mattress and then the tray, then the bedsides and the base of the bed. At no point was the cloth washed out.
We also asked all in-patients on discharge the following questions about their care. Score (out of 5)

21
Jan Feb Mar Apr Were you treated with dignity and respect? 4.94 4.91 4.86 4.98 Did you feel involved enough in decisions made about you? 4.79 4.79 4.80 4.84 Did you receive timely information about your care and treatment?
4.76 4.78 4.70 4.89
Was the location clean? 4.88 4.87 4.82 4.88 Were you treated well by the staff looking after you? 4.94 4.91 4.88 4.98
4.2.2. Day care 16 patients made the following suggestions for improvement:
Only one toilet in the day ward Screening over the face in theatre impeded breathing and induced sub conscious claustrophobia Arrived 8.30 am had bloods 9.00am saw doctor 11.00. It is now 4.00pm. It took 4 hours for his chemo/meds to come up from the pharmacy. Equipment’s are not working at times (eg ECG machine and OBS machine). The insertion of the cannula tool 5 attempts; this could be improved. The facility is cramped small claustrophobic and lacks any privacy therefore, dignity. We also asked all day case patients on discharge the following questions about their care. Score (out of 5) Jan Feb Mar Apr Were you treated with dignity and respect? 4.95 4.91 4.92 4.95 Did you feel involved enough in decisions made about you? 4.86 4.81 4.82 4.87 Did you receive timely information about your care and treatment?
4.84 4.77 4.77 4.88
Was the location clean? 4.91 4.88 4.88 4.90 Were you treated well by the staff looking after you? 4.97 4.92 4.94 4.98

22
4.2.3. OPD 11 patients made suggestions for improvement:
The clinical care has been fantastic; however the administration has been dreadful. I am never on the list for appointments and always have to ring to double check.
I cannot fault the medical staff at all but, the reception staff are rude and arrogant bearing in mind its most women’s first time so when you approach the reception desk and get ignored for several minutes and no eye contact or smile and looking stress.
Very polite and informative staff. Maybe some music for all the hours waits?
Please improve the gowns. It would be helpful for diabetic patients to know their sugar level must be 10 or below in order for their PET scan to go ahead.
We also asked all out-patients on discharge the following questions about their care. Score (out of 5) Jan Feb Mar Apr Were you treated with dignity and respect? 4.85 4.94 4.91 4.92 Did you feel involved enough in decisions made about you?
4.77 4.87 4.80 4.85
Did you receive timely information about your care and treatment?
4.75 4.82 4.79 4.89
Was the location clean? 4.85 4.93 4.90 4.93 Were you treated well by the staff looking after you?
4.86 4.96 4.90 4.93
4.2.4. National FFT inpatient results reporting:
From November 2014 NHS England report a percentage of those who would recommend the Trust to friends and family.
Inpatient data is collected for 170 Acute NHS trusts and independent sector providers. Nationally, the overall average inpatient percentage for those who would recommend the service to friends and family was 96% in February. The Trust is above this with an average of 97% in March.
Outpatient data was collected for 234 Acute NHS trusts and independent sector providers. Nationally the overall average outpatient percentage for those who would recommend outpatients to friends and family was 93% in February. The trust was above this with an average of 97% in March 2016.

23
The tables below show the results for the Trust each quarter or month to date. At the time of reporting (6th May 2016) national figures were available up to March 2016.
INPATIENTS Q4 2014-2015
Q2 2015-2016
Q3 2015-2016
Jan 2016
Feb 2016
Mar 2016
The Royal Marsden percentage of inpatients who would recommend
99% 96.7% 96.7% 97% 97% 97%
National average 95% 95.7% 96% 96% 96% 96% Response number 601 1986 1986 572 652 649 OUTPATIENTS Q2
2015- 2016
Q3 2015- 2016
Jan 2016
Feb 2016
Mar 2016
The Royal Marsden percentage of outpatients who would recommend
97% 98% 96% 98% 97%
National average 92% 92% 93% 93% 93% Response number 451 1084 302 309 307 5.0. Nurse Safer staffing From June 2014 all Trusts are required by the Department of Health, Monitor and the Care Quality Commission to be able to assure their Boards around the provision of nursing care on its wards and units. This requirement followed the national failings in care at Mid Staffordshire NHS Foundation Trust and other Trusts since placed on “special measures”. The final Francis report recommended that Boards regularly check that levels of nurse staffing are appropriate for good quality care. Therefore from June 2014 the RM Board has received a monthly summary of planned numbers of nurses and Health Care Assistants (HCA) during the day and at night, versus the actual numbers. It is also mandated that the Board receive a six monthly report from the Chief Nurse regarding all issues regarding Safe Nurse staffing across the Trust. The Board has received these reports since June 2014 with the last one being received in March 2016. The following data is the planned and actual nurse staffing for April 2016. Overall the percentages are as follows:

24
Average fill rate for night staff 99.3% Average fill rate for day staff 96.6% Average fill rate for Registered staff 96.7% Average fill rate for Care staff 102.1% Average Trust wide fill rate (All staff, night and day) 97.6%
5.1 Nursing Leavers and Starters Report The tables below show the number of nurse starters and leavers over a two year period. In the financial year 2013/14 the number of nurse leavers equated to 12 nurses per month on average. For the current financial year more nurses have been recruited at this point than in the last financial year. In November 2014 the Chief Nurse began a monthly recruitment meeting to address the issues around recruitment and retention of nurses. For the first time in February the meeting was able to review the results of a small exit questionnaire, questionnaires were sent retrospectively to 35 nurses who had left and nine were returned. In all but one case the nurses left for personal or financial reasons. The questionnaires are now reviewed monthly. Board members will note below that the concerted work of nursing and HR, marketing and communications is finally showing positive results from June onwards more nurses were recruited than left the Trust. The Trust is also holding national recruitment days on a Saturday which have thus far yielded 15 staff with the most recent event being held on Saturday the 19th March 2016 at Chelsea with 15 new nurses appointed.
Band 5-7 Nurses (2015/16) Apr-15 May-15 Jun-15 Jul-15 Aug-15 Sep-15 Oct-15 Nov-15 Dec-15 Jan-16 Feb-16 Mar-16 Total
Starters (wte) 6 12 16 13.6 13.8 22.49 21.27 21.45 12.8 17.59 21.08 10.57 188.65
Leavers (wte) 15 15 14 11.5 10.66 7.18 8.75 10.61 11.61 13.18 15.18 9.33 142
Variance -9 -3 2 2.1 3.4 15.31 12.52 10.84 1.19 4.41 5.9 1.24 46.62
Band 5-7 Nurses (2015/16)
Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Jan-17 Feb-17 Mar-17 Total Starters
(wte) 21.52 21.52 Leavers
(wte) 10.74 10.74 Variance 10.78 10.78

25
5.2 Nurse leavers in April 2016
Nursing Leavers Bands 5-7 April 2016
Area Job Title Leaving date LOS Band WTE Reason for leaving
Cancer Services Division
Bud Flanagan East Staff Nurse 25/04/2016 14 y 5 m XR06 1.00 Retirement - Ill-health
Children's OPD Staff Nurse 18/04/2016 4 y 8
m XR06 0.43 Voluntary Resign. – Work Life Balance - Shift Patterns Clinical Services Division
Critical Care Outreach (S) Critical Care Outreach Sister / Charge
Nurse 07/04/2016 4 y
10 m XR07 0.15 Redundancy - Compulsory
Critical Care Outreach (S) Outreach Nurse 07/04/2016 5 y 9
m XR07 0.15 Redundancy - Compulsory
Critical Care Unit (L) Senior Staff Nurse 30/04/2016 1 y 6
m XR05 1.00 End of FTC
Endoscopy Staff Nurse 01/04/2016 1 y 6
m XR05 1.00 Voluntary Resign. - To undertake further Education or Training
Endoscopy Staff Nurse 05/04/2016 0 y 6
m XR05 1.00 End of FTC - End of Work Requirement
Endoscopy Staff Nurse 28/04/2016 0 y 6
m XR06 1.00 Voluntary Resig. - Relocation Clinical Research Division
Lerner Lung & Mesothelioma Research Research Nurse 30/04/2016
0 y 2 m XR07 1.00
Voluntary Resign. – Work Life Balance - Cost of Living (Travel, Accommodation)
Community Services
HV Merton Health Visitor 31/01/2016 0 y 3
m XR06 1.00 Voluntary Resignation – Work Life Balance - Cost of Living (Travel,
Accommodation)
Respiratory Nursing Specialist Nurse Respiratory Medicine 04/01/2016 2 y
10 m XR07 1.00 Voluntary Resignation - Other Private Care
GH Ward Senior Staff Nurse 01/04/2016 0 y 8
m XR06 1.00
Voluntary Resig. - Promotion
Robert Tiffany Unit (S) Staff Nurse 17/04/2016 0 y 6
m XR05 1.00 Voluntary Resign. – Work Life Balance - Cost of Living (Travel,
Accommodation) Total WTE Leavers - 10.74

26
6.0. Board Members are invited to note the performance of the Trust against the agreed national and local quality targets for April 2016 and the actions being taken.
BOARD PAPER SUMMARY SHEET
Date of Meeting:
1st June 2016
Agenda item 7.2
Title of Document: Duty of Candour Report 2015/16
To be presented by
Chief Nurse
Executive Summary The overall number of patient safety incidents reported has increased but the percentage of these that fall into the category that require implementation of the Duty of Candour has reduced. Recommendations To note and discuss the Duty of Candour Report and the data provided within it Author: Chief Nurse
Contact Number or E-mail: x2121
Date: 19 th May 2016


1
Duty of Candour Report 2015/16
1.0 Background 1.1 Following the publication of the Francis Report in 2013 into failings at
Mid–Staffordshire NHS Foundation Trust there were many recommendations made for change throughout the NHS. One of the recommendations was for a statutory Duty of Candour, this came into force on the 27th November 2014.
1.2 Previously, there was a contractual Duty of Candour on NHS
Organisations. This meant that NHS Trusts signed up to an NHS contract and had to be open and honest with patients in order to meet the requirements of the contract.
1.3 Duty of Candour is a statutory requirement to ensure that the agreed
process is followed when a patient safety incident occurs resulting in moderate harm, severe harm or death.
2.0 Trust requirements 2.1 To meet the requirement of the regulation the Trust must:
• Inform patients or their family / carer that a suspected or actual patient safety incident has occurred within 10 working days of the incident being reported to local systems (Datix).
• The initial notification must be verbal (face to face where possible). The verbal notification must be accompanied by an offer of written notification. The notification must be recorded for audit purposes.
• An appropriate apology must be provided – a sincere expression of sorrow or regret for the harm caused both verbally and in writing;
• A step by step explanation of what happened in plain English, based on fact must be offered as soon as practicable. This may constitute an initial view pending an investigation, but patients and families must be kept informed of the process.
• Any incident investigation reports must be shared with the patient/ family within 10 days of being signed off as complete and the incident closed by the relevant authority.
• If the requirements of the Duty of Candour are not met the Commissioners can withhold the cost of an episode of care or implement a fine of £10,000 if the cost is not known.
3.0 The Royal Marsden (RM) approach to Duty of Candour 3.1 To provide a robust patient centred process for ensuring that we are
open and honest with patients with regard to incidents that fall under the regulation, the Risk Management Team review every incident that

2
is reported graded “moderate harm and above” the day that it is reported or the next working day.
3.2 If the incident is confirmed as falling into this category the Risk Management team liaises with the appropriate clinical staff to ensure that the patient is informed that an incident has occurred and that an appropriate apology has been given within 10 days of it being reported on Datix.
3.3 The patient/family is advised of the investigation and how it is being followed up. If a report is to be written the patient is asked if they would like a copy or whether they would like to meet to go through the findings.
3.4 The investigation is undertaken and the Risk Management Team with the support of the Complaints Department ensure that the report and accompanying cover letter is sent to the patient with an offer to meet to go through the findings.
3.5 The Duty of Candour process is subject to an on going six monthly audit, the results of which are submitted to the Integrated Governance and Risk Management Committee, QAR and the Trust Board.
4.0. Audit Findings 4.1. Number of incidents reported Audit period Total
number of incidents
Attributable patient safety incidents
Incidents that have caused moderate harm and above
July – Dec 15 2889 1944 45 Jan – June 15 2698 1782 54 July – Dec 14 2397 1887 67 Jan – June 14 2280 1498 63
4.2. Datix compliance Datix records state that: July –
Dec 15 Jan– June 15
July – Dec 14
Jan– June 14
The patient has been advised 89% 74% 79% 67% Staff name
89% 80% 79% 72%
Designation
89% 86% 79% 64%
Date
89% 85% 78% 78%
Is it recorded in patients record
87% 58% 81% 62%
If not recorded why not
75% NA NA NA
4.3. Electronic patient record compliance (EPR & RIO) Patient records document that:
July –Dec 15
Jan– June 15
July – Dec 14
Jan– June 14
The incident has been 93% 85% 86% 74%

3
discussed It is recorded at the time of the incident *
91% 86% 79% 77%
An apology has been given
84% 59% 11% 3%
Designation of staff
93% 90% 76% 69%
Patient has been offered a written apology
89% 38% 11% NA
Letter has been sent
88% 30% 65% NA
* Within 10 working days of the incident being reported 4.4 Compliance with follow up July –
Dec 15 Jan– June 15
July – Dec 14
Jan– June 14
Investigation was required
89% NA NA NA
Was the patient asked if they would like a copy of the report
89% 55% 5% NA
If the patient requested a report was it sent
53% 11% 33% NA
Is there evidence of incident follow up
100% 100% 75% 71%
5.0 Conclusions and Recommendations 5.1 The overall number of patient safety incidents reported has increased,
the percentage of these that fall into the category that require implementation of the Duty of Candour has reduced. The most recent National Reporting and Learning System report identifies that RM are above average reporters of incidents that fall into that category within specialist trusts so the reduction in incidents of this category is not of concern and probably down to increased scrutiny regarding the grade.
5.2 Overall compliance with the requirements of the Duty of Candour has increased with each audit. The Risk Management team continue to raise awareness of the requirements and support staff in implementing all of the different steps required by this legislation.
5.3 The audits for 2016 will include a review of the previous six months incidents to identify whether the patient are receiving the final reports as this element often falls outside the timeframe of the current audit.
5.4 There is currently no method of benchmarking compliance with Duty of Candour against other organisations, this will be discussed with Commissioners and NHS England in May as a reference tool would be useful.
Board members are invited to discuss the Duty of Candour Report and the data provided within it.


BOARD PAPER SUMMARY SHEET
Date of Meeting:
1st June 2016
Agenda item 8
Title of Document: Financial Performance Report for months ending April 2016
To be presented by
Chief Financial Officer
Executive Summary The paper provides a summary of the financial position for 1 month to April 2016. Recommendations The Board is asked to discuss the contents of the report and the risks highlighted. Author: Chief Financial Officer
Contact Number or E-mail: x2151
Date: 18th May 2016


Summary Financial Performance Report for 1 Month to April 2016
1 | P a g e
1. Introduction The paper provides a summary of the financial position for the financial year 2016/17. The reporting format has been developed to provide consistent reporting to all Trust Committees. The Board is requested to note the contents of this report and the risks highlighted.
2. Summary Financial Position In April the Trust had a deficit of £0.4m, predominantly driven by lower donated asset income. Removing the donated asset income variance, for which the Trust has little control, the Trust is broadly on plan in month. The NHS Clinical Income adverse variance to plan (£0.5m) was offset by Private Care which had a strong month with a large favourable variance to plan (£0.5m). In addition, there was increased non-clinical income in month (£0.6m) which is primarily for research grants, provider-to-provider activity and Community Services contracts, all of which report additional expenditure in relation to them. On expenditure, agency usage was £935k in month (6%) which exceeded the spend cap. 367 shifts breached the rate cap, which is low when benchmarked against other London Trusts. These shifts were all Medical and Nursing and only framework agencies continue to be used. Overall pay expenditure was however favourable to plan (£0.1m). The other key variances relate to non-pay expenditure which was adverse in month (£0.8m). Additional expenditure on research trials and in the community was incurred and funded through additional non-clinical income. The Financial Risk Rating is that the Trust is an overall 2 against a planned position of a 3. The Key Risk and Issues to highlight relate to the 2016/17 plan, which were discussed at the Board in March. These continue to be:
• NHS Commissioner Contracts – the Trust has requested that local prices are re-based as per the Monitor framework so that the income covers the cost of the services provided. In addition, the Trust runs 25 MDTs a week for which it receives only a small contribution towards four of them. Both of these issues are outstanding in the negotiations on contracts and need to be resolved in order for the Trust to achieve its financial plan in 2016/17.
• Private Care Strategy – there has been significant growth in the past few years on income, however the embassy work does fluctuate and other areas are being pursued to continue the growth ahead of the additional capacity that opens in the second half of the year.
• Junior doctors’ contract – the Trust has taken the national guidance that the contract is cost neutral for providers. The rotas are currently being reviewed and any impact will need to be discussed further with Commissioners.
• Temporary staffing – controls are in place and have been for several months, however a cap has been imposed upon the Trust which is a 35% reduction from the forecast 2015/16 expenditure, so additional measures will be required in order to deliver this target.

Summary Financial Performance Report for 1 Month to April 2016
2 | P a g e
3. Income and Expenditure The Income and Expenditure position for the Trust, in month, year-to-date and the forecast is set out in Appendix 1. Income – The income position in month 1 was a £0.6m favourable variance in month. NHS Clinical Income was adverse to plan which was largely due to CDF and High Cost Drugs pass through income (£0.3m) but also reflected lower activity levels than anticipated (£0.15m). Inpatient admissions and bed occupancy was down in month although this may be due to a coding lag which always occurs at the start of the year. Income was strong in April however compared to prior years as shown below.
Private Care had a favourable variance of £0.5m. Tariffs have been uplifted for the new financial year and activity was strong across the board. Private Care income continues to grow but the billing lag has remained at normal levels and the debt levels have stabilised. The trend chart below shows actual income compared to the 2016/17 plan, alongside 2015/16 and 2014/15 income levels.
£8.0
£9.0
£10.0
£11.0
£12.0
£13.0
£14.0
£15.0
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
NHS Acute Income for 2016/17
Acutal 14/15 Actual 15/16 Actual 16/17 Plan 16/17
£- £1.0 £2.0 £3.0 £4.0 £5.0 £6.0 £7.0 £8.0 £9.0
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Private Care Income for 2016/17
Acutal 14/15 Actual 15/16 Actual 16/17 Plan 16/17

Summary Financial Performance Report for 1 Month to April 2016
3 | P a g e
The remaining variances on income in month related to research and development (£0.5m), and other operating income (£0.1m) which included additional Community Services non-NHS contracts and provider-to-provider activity. These had equal and opposite expenditure within pay and non-pay and therefore explain the adverse variances in expenditure. Pay expenditure – was a favourable variance of £0.1m in month compared to the plan. The two charts below provide pay and temporary staffing data for 2016/17. Although costs were under plan for April indicating temporary staffing was only used to fill some vacancies, agency costs were higher than bank. Agency usage in a number of areas has been consistent across the years as recruitment remains a national issue; junior doctors, theatres and CCU staff, community nurses and AHPs. Other areas of usage have been managed down with any usage in the corporate divisions requiring COO approval. The first chart shows total pay costs are a favourable variance against the budget in April. The second chart reflects the bank and agency usage. The focus on agency staffing spend continues with NHSI requiring weekly reporting and the Trust has a spend cap that it is required to work towards as well as caps on agency rates for suppliers. The Trust is expected to utilise only agencies that apply the caps in rates although Pulse, the main nursing agency and a number of individual Medics have not conformed to the caps, so 376 cap shift breaches were recorded in April. These individuals are being managed out and converted to bank where feasible. In month the expenditure was 5.7%, above the NHSI cap by £180k (Appendix 2, chart 2.1). A number of controls, initiatives and monitoring tools are being put in place to bring this down.
£12.0
£13.0
£14.0
£15.0
£16.0
£17.0
£18.0
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Pay Cost Trend
Substantive Bank / Locums Agency Pay Budget

Summary Financial Performance Report for 1 Month to April 2016
4 | P a g e
Non-pay expenditure – is £0.8m ahead of plan in month. Additional expenditure on research trials and in the community was incurred and funded through additional non-clinical income.
4. Efficiency Programme The Trust reported that it delivered 50% of its CIP programme in April 2016. However many more of the schemes have begun but have no reporting mechanism set up yet so this figure will be lower than the final report. This is presented in Appendix 2, chart 2.1.
5. Capital Expenditure Capital expenditure showed an adverse variance of £0.2m in month. Internally funded schemes were on plan, with PDC funded schemes ahead of plan and donated asset schemes behind plan. There is no clinical risk impact with the slippage of the schemes. The total PDC schemes are still forecast to come in on plan and there is no clinical risk impact with the slippage of schemes.
6. Cash and Debt Cash – The Trust ended April with £14m cash in the bank. This was a large reduction on March as capital payments were made, to Sphere and other contractors and outstanding payables were settled. Additionally NHSE CDF revenue is two months overdue and RMCC monies were paid a day late. Chart 2.3 in Appendix 2 shows the trend of cash balances in the last four months and the forecast and plan for the next 12 months. Debt – Invoices raised but not yet paid remained stable at £47.6m at the end of April. Private Care debt decreased slightly in month, and has remained stable at c£23m over the past nine months despite increasing turnover. Notwithstanding this stabilisation, debt with embassies and overseas sponsors continues to be a concern and there is continual dialogue with each of the agencies. Chart 2.4 in Appendix 2 provides a trend of debtor balances for the last twelve months by age of debt, which shows the increase in debt over 90 days, the majority of which is with embassies.
£-
£0.2
£0.4
£0.6
£0.8
£1.0
£1.2
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Bank and Agency Spend
Bank / Locums Agency
Summary Financial Performance Report for 1 Month to April 2016
5 | P a g e
7. Governance The Board is required to sign off a number of governance statements, most of which have been dealt with through the sub-committees. However there are two new statements that require the Board’s oversight this year, these are:
• Systems for compliance with license conditions o Following a review for the purpose of paragraph 2(b) of licence condition G6,
the Directors of the Licensee are satisfied, as the case may be that, in the Financial Year most recently ended, the Licensee took all such precautions as were necessary in order to comply with the conditions of the licence, any requirements imposed on it under the NHS Acts and have had regard to the NHS Constitution; and
o The board declares that the Licensee continues to meet the criteria for holding a licence.
• Certification on AHSCs and governance The Board is satisfied it has or continues to:
o ensure that the partnership will not inhibit the trust from remaining at all times compliant with the conditions of its licence;
o have appropriate governance structures in place to maintain the decision making autonomy of the trust;
o conduct an appropriate level of due diligence relating to the partners when required;
o consider implications of the partnership on the trust’s financial risk rating having taken full account of any contingent liabilities arising and reasonable downside sensitivities;
o consider implications of the partnership on the trust’s governance processes; o conduct appropriate inquiry about the nature of services provided by the
partnership, especially clinical, research and education services, and consider reputational risk;
o comply with any consultation requirements; o have in place the organisational and management capacity to deliver the
benefits of the partnership; o involve senior clinicians at appropriate levels in the decision-making process
and receive assurance from them that there are no material concerns in relation to the partnership, including consideration of any re-configuration of clinical, research or education services;
o address any relevant legal and regulatory issues (including any relevant to staff, intellectual property and compliance of the partners with their own regulatory and legal framework);
o ensure appropriate commercial risks are reviewed; o maintain the register of interests and no residual material conflicts identified;
and o engage the governors of the Trust in the development of plans and give them
an opportunity to express a view on these plans.
8. Conclusion and Recommendation April has been a challenging start to the 2016/17 financial year with many unknowns surrounding commissioning. Agency spend continues to be closely monitored and controlled with the NHSI caps proving challenging as expected. Activity has been mixed but the Trust is broadly on plan before donated asset income variances. The Board is requested to note
• The financial performance as at month 1; • The Trust did not meet the agency cap required by NHSI; • The continued risks highlighted in section 2; and • Approve the two new governance requirements outlined in section 7.

6 | P a g e
Budget Actual Var Budget Actual Var Budget 1415 Q3 1415 Q4 1516 Q1 1516 Q2 1516 Q3 1516 Q4
£'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000
Income Actual Actual Actual Actual Actual Actual
NHS Clinical Income (1 5,999) (1 5,550) 450 (1 5,999) (1 5,550) 450 (1 94,200) (1 6,869) (20,252) (1 6,7 93) (1 7 ,362) (1 7 ,502) (1 8,593)
Non NHS Clinical Income (6,954) (7 ,440) (485) (6,954) (7 ,440) (485) (89,534) (6,850) (6,393) (6,581 ) (6,858) (7 ,1 27 ) (7 ,282)
Non Clinical Income (5,921 ) (6,529) (607 ) (5,921 ) (6,529) (607 ) (7 0,7 96) (5,580) (5,942) (5,7 02) (6,1 46) (5,37 6) (6,991 )
(28,87 5) (29,51 8) (643) (28,87 5) (29,51 8) (643) (354,530) (29,299) (32,587 ) (29,07 7 ) (30,365) (30,004) (32,866)
Expenditure
Pay 1 6,631 1 6,499 (1 32) 1 6,631 1 6,499 (1 32) 202,57 1 1 6,484 1 6,866 1 6,934 1 7 ,1 43 1 7 ,230 1 7 ,67 2
Non Pay 1 1 ,435 1 2,239 804 1 1 ,435 1 2,239 804 1 39,538 1 1 ,225 1 3,1 38 1 1 ,487 1 1 ,384 1 1 ,950 1 3,642
28,066 28,7 38 67 2 28,066 28,7 38 67 2 342,1 08 27 ,7 09 30,003 28,422 28,526 29,1 7 9 31 ,31 3
Operating Surplus (81 0) (7 80) 30 (81 0) (7 80) 30 (1 2,422) (1 ,589) (2,583) (655) (1 ,839) (825) (1 ,553)
PDC, Interest, JV 428 426 (1 ) 428 426 (1 ) 5,31 3 404 426 41 5 401 352 344
Development Reserve for Inv (382) (353) 29 (382) (353) 29 (7 ,1 09) (1 ,1 85) (2,1 57 ) (240) (1 ,438) (47 2) (1 ,208)
Donated Asset Income (945) (31 7 ) 628 (945) (31 7 ) 628 (7 ,000) (7 85) (361 ) (331 ) (387 ) (651 ) (565)
Depreciation 1 ,1 24 1 ,062 (62) 1 ,1 24 1 ,062 (62) 1 3,984 1 ,07 3 1 ,1 30 1 ,1 62 1 ,1 1 3 997 1 ,1 34
Loss Disposal Fixed Assets - - - - - - - - 283 443 - (41 0) -
Impairment - - - - - - - - 1 ,436 - - 462 491
Retained Surplus (203) 392 595 (203) 392 595 (1 25) (898) 331 1 ,035 (7 1 2) (7 4) (1 49)
Financial Risk Rating Pla n YTD A ctu a l YTD
Liqu idit y 4 4 (1) - Liquidity Ratio = Cash for liquidity purposes (net current assets excluding inventories) divided by operating expenditure expressed in days
Ca pit a l Debt Cov er Ra t io 2 3 (2) - Capital Debt Cover Ratio = revenue available for debt servicing (EBITDA plus interest receivable) divided by annual debt (PDC Dividends, Loan repayments, Loan interest)
I&E Ma rgin 2 1 (3) - I&E Margin - degree to which the Trust is operating at a surplus / deficit
V a ria n ce From Pla n 0 4 (4) - Variance between the Trust's planned I&E Margin and its actual I&E Margin year to date
Fin a n cia l Risk Ra t in g 3 2
The Trust's plan was to deliver a surplus of £203k in April, however, actual performance was a £392k deficit. This was driven by an adverse variance on Donated Asset Income, with the Development Reserve for Investment being on plan. Underperformance on NHS Income in month was offset by Private Care Income. Additional costs were largely in Research and funded through additional non-clinical income. Agency usage was 5.7 %, with 37 6 shifts exceeding the NHSI cap in month (Medical and Nursing only ). This is low when benchmarked against other London Trusts. Only framework agencies continue to be used. This delivers a Y TD Financial Risk Rating of 2, compared to a plan of 3, this being driven by the adverse variance on donated asset income.
Appendix 1: Income and ExpenditureIn Month Year to Date Year - 2016/17 Average Monthly Run Rates
-20-15-10
-505
101520
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
1.1 Liquidity Ratio 2015/16 (1)
-3-2-1012345
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
1.2 Ca pital Debt Cover 2015/16 (2)
-3%
-2%
-1%
0%
1%
2%
1.3 I&E Ma rgin 2015/16 (3)
-3%
-2%
-1%
0%
1%
2%
1.4 V ariance from plan (4)
1
2
3
4
Actual
Plan
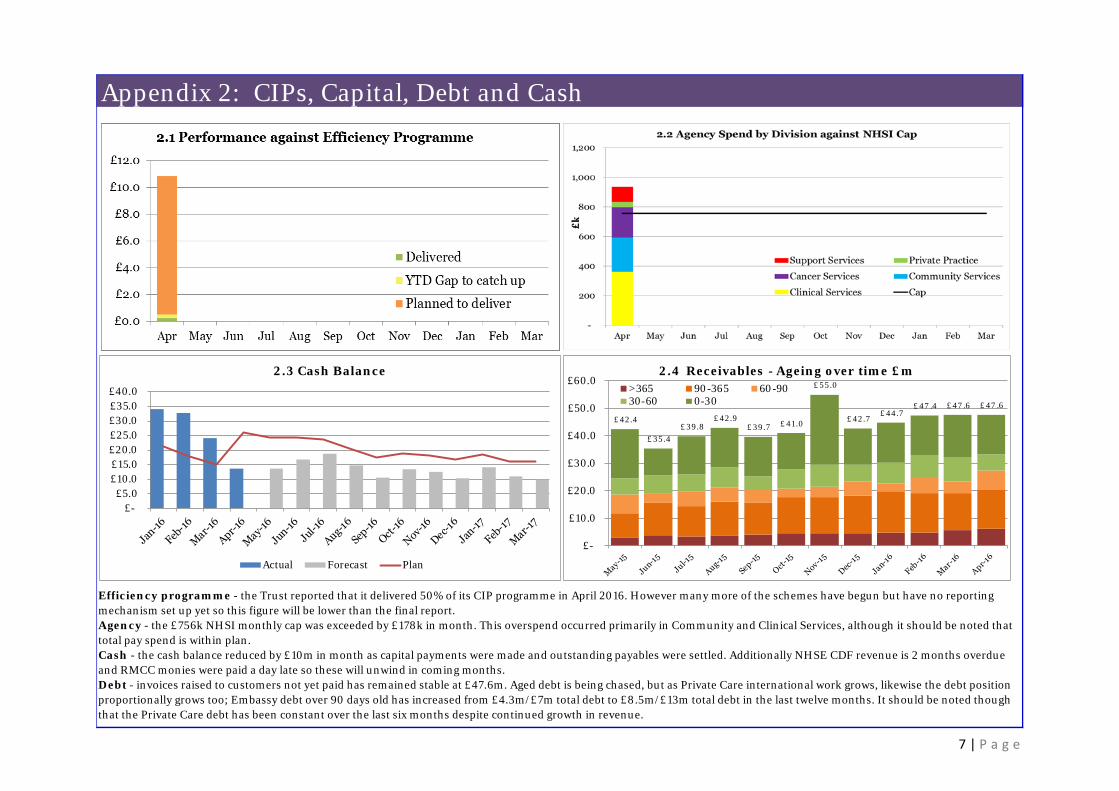
7 | P a g e
Appendix 2: CIPs, Capital, Debt and Cash
Efficiency programme - the Trust reported that it delivered 50% of its CIP programme in April 2016. However many more of the schemes have begun but have no reporting mechanism set up yet so this figure will be lower than the final report. Agency - the £756k NHSI monthly cap was exceeded by £178k in month. This overspend occurred primarily in Community and Clinical Services, although it should be noted that total pay spend is within plan.Cash - the cash balance reduced by £10m in month as capital payments were made and outstanding payables were settled. Additionally NHSE CDF revenue is 2 months overdue and RMCC monies were paid a day late so these will unwind in coming months.Debt - invoices raised to customers not yet paid has remained stable at £47.6m. Aged debt is being chased, but as Private Care international work grows, likewise the debt position proportionally grows too; Embassy debt over 90 days old has increased from £4.3m/£7m total debt to £8.5m/£13m total debt in the last twelve months. It should be noted though that the Private Care debt has been constant over the last six months despite continued growth in revenue.
£- £5.0
£10.0 £15.0 £20.0 £25.0 £30.0 £35.0 £40.0
2.3 Cash Balance
Actual Forecast Plan
£42.4
£35.4 £39.8
£42.9 £39.7 £41.0
£55.0
£42.7 £44.7
£47 .4 £47 .6 £47 .6
£-
£10.0
£20.0
£30.0
£40.0
£50.0
£60.02.4 Receivables - Ageing over time £m
>365 90-365 60-9030-60 0-30

BOARD PAPER SUMMARY SHEET
Date of Meeting: 1 June 2016
Agenda item 9
Title of Document: Audit and Finance Committee Annual Report for 2015/16
To be presented by
Ian Farmer, Chair of the Audit and Finance Committee
Executive Summary This report reviews the work of the Audit and Finance Committee undertaken in the period 1
April 2015 to 31 March 2016 and sets out how the Committee has met its terms of reference and priorities. Recommendations The Board is asked to note and discuss the annual report for Audit and Finance Committee 2015/16. Author: Ian Farmer, Chair of the Audit and Finance Committee
Contact Number or E-mail:
Date: 18th May 2016

Audit & Finance Committee
Annual Report April 2015 - March 2016
1. INTRODUCTION
The purpose of the report is to review the work of the Audit & Finance Committee (AFC) undertaken in the period 1st April 2015-31st March 2016 and to set out how the Committee has met its terms of reference and priorities.
2. COMMITTEE MEMBERSHIP
In attendance were the Chief Financial Officer together with the Chief Nurse, along with representatives of Internal Audit (KPMG) and External Audit (Deloitte). Meetings were organised and supported by the Chief Financial Officer’s team.
3. MEETINGS
Four meetings were held over the year on 1st April 2015, 27th May 2015, 9th September 2015 and 27th January 2016. Currently there are four meetings planned during 2016/17 on 6th April 2016, 25th May 2016, 7th September 2016 and 25th January 2017.
4. ASSURANCE
The Audit and Finance Committee (AFC) shares responsibility with the Quality Assurance and Risk Committee (QAR) in providing assurance to the Board that the Foundation Trust is properly governed and that risks are appropriately identified and managed across the full range of the Trust’s activities. The Committee is responsible for all matters relating to financial risk. Both Committees work collaboratively to ensure that all aspects of risk are covered and that the Board receives comprehensive assurances on the Trust’s activities. Co-ordination with Quality, Assurance and Risk Committee The Chair of AFC and QAR have discussed priorities for the respective Committees and the use of internal audit resources to provide assurance in key risk areas. In addition, forward Agendas and Minutes are regularly provided to each Committee and key items from QAR are reported at each AFC meeting. Terms of Reference The AFC Terms of Reference was presented at the 16th September 2015 meeting for the Committee’s annual review. Following some minor amendments agreed with the Committee, it was approved to be forwarded to the Board and was endorsed by the Board at 4th November 2015 Board meeting.

2
5. INTERNAL CONTROL AND RISK MANAGEMENT
The Committee covered the following areas during the year: Efficiency Programme (standing item)
The Committee undertook in depth reviews of several work streams.
Financial Performance (standing item) The Committee reviewed the Trust’s financial performance versus plan at each meeting, discussed trends and variances and reviewed key financial assumptions. The work on service line reporting and its use across the Trust was reviewed at each meeting during the year.
Losses, Compensation and Waivers (standing item) The Committee considered and noted details of waivers in the procurement process at each meeting and received an annual report on minor losses and write-offs. Sutton & Merton Community Services (Apr15) With regard to the Community Services contract renewal, the Committee noted the request by Merton CCG to tender with the Local Authority whereas in Sutton the Local Authority and Sutton CCG requested separate tenders. The AFC endorsed a strategy to minimise financial risk to the Trust. IT Shared Services (Apr15) The executive presented a case for IT Shared Services with Chelsea & Westminster NHS Foundation Trust via a jointly owned entity named “Sphere”. The business benefits and risks were discussed in context of the Trust’s evolving IT strategy. Reference Costs (May15) The Committee approved the Annual Reference Cost submission to the Department of Health. The report was audited by PricewaterhouseCoopers who concluded that the submission was accurate and that there were good arrangements for the production and review of the submission. Minor recommendations were made and taken on board. SMCS Contract Update (Sep15) An update on the SMCS contract position was given and it was noted that Sutton CCG and Local Authority had awarded contracts to the Trust whereas Merton CCG decided to award their contract to a Community Trust. The Committee noted the process proposed for disaggregation and the risks associated with this process. Policy Review (Sep15) A new policy was adopted on
Non-audit services, and Minor amendments to policies were made where required to the following policies
Anti-Fraud, Bribery & Corruption
Conflict of Interest and Acceptance of Hospitality NED Seminars: Two “deep dive” seminars were held during the year:
Procurement Strategy Review (Dec15)
IT Strategy Review (Jan16) Draft 2016/17 Financial Plan (Jan16) The 2016/17 Financial Plan was tabled, however, due to the lack of clarity surrounding various aspects of Monitor’s letter of 15 January 2016, it was agreed that consideration and approval of the plan should be deferred until a future meeting. This matter was subsequently dealt with at the Board and the final plan was reviewed by the AFC in April 2016.

3
2016/17 National Tariff Contract (Jan16) A paper detailing management’s negotiation position was tabled and discussed. The Committee noted that the current tariff proposals do not address the underlying shortfall in funding for cancer services. Temporary Staffing & eRostering Update (Jan16) It was noted that the eRostering system was up and running. The Committee requested an update in six months’ time. Board Self-Certification Report (Jan16) The Committee reviewed and approved with one minor amendment the template to be used for self-certification purposes.
6. INTERNAL AUDIT
The Internal Audit Strategic and Operational Plan, covering the period 1st April 2015 to 31st March 2016 was discussed and agreed by the Committee at the 1st April meeting. The plan, which had been developed by the Head of Internal Audit in discussion with the Chairman of the AFC, the Chief Financial Officer and Chief Nurse, reflected the Board Assurance Framework and a number of priority areas identified by both AFC and QAR. Summary of Internal Audits Completed 2014/15 The following IA reports received during the year related to the 2014/15 audit plan:- Planned Audit Review
Completed Received by Committee
Assurance Status
Divisional governance arrangements Financial Management and Financial reporting and the benefit of subscription arrangements Review of Temporary Staffing arrangements Private Patient Income arrangements Pharmacy arrangements
Jan 2015 Jan 2015 Feb 2015 Mar 2015 Apr 2015
Apr 2015 Apr 2015 Apr 2015 Apr 2015 May 2015
Significant assurance with minor improvement potential Significant assurance Partial assurance with improvements required Partial assurance with improvements required Significant assurance with minor improvement potential
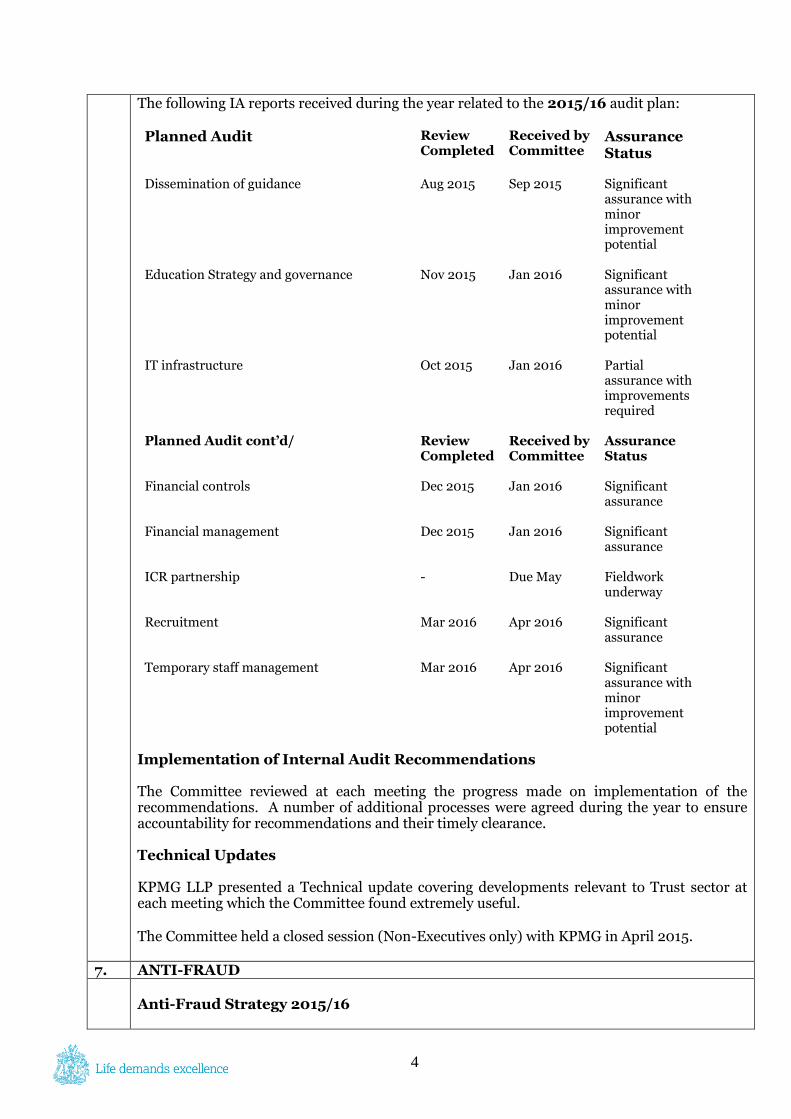
4
The following IA reports received during the year related to the 2015/16 audit plan: Planned Audit Review
Completed Received by Committee
Assurance Status
Dissemination of guidance Education Strategy and governance IT infrastructure Planned Audit cont’d/ Financial controls Financial management ICR partnership Recruitment Temporary staff management
Aug 2015 Nov 2015 Oct 2015 Review Completed Dec 2015 Dec 2015 - Mar 2016 Mar 2016
Sep 2015 Jan 2016 Jan 2016 Received by Committee Jan 2016 Jan 2016 Due May Apr 2016 Apr 2016
Significant assurance with minor improvement potential Significant assurance with minor improvement potential Partial assurance with improvements required Assurance Status Significant assurance Significant assurance Fieldwork underway Significant assurance Significant assurance with minor improvement potential
Implementation of Internal Audit Recommendations
The Committee reviewed at each meeting the progress made on implementation of the recommendations. A number of additional processes were agreed during the year to ensure accountability for recommendations and their timely clearance.
Technical Updates
KPMG LLP presented a Technical update covering developments relevant to Trust sector at each meeting which the Committee found extremely useful. The Committee held a closed session (Non-Executives only) with KPMG in April 2015.
7. ANTI-FRAUD
Anti-Fraud Strategy 2015/16

5
The Committee reviewed and approved the Anti-Fraud Strategy developed by the Trust’s Local Anti-Fraud Specialists at the 1st April 2015 meeting. The Committee noted that adopting a clear strategy enforced the Trust’s absolute commitment to countering fraud. Investigations The Committee regularly reviewed the results and progress of fraud investigations conducted during the year. Eleven new referrals were noted during the year. All were immaterial and were resolved in a satisfactory manner. Annual Report In September the Committee received and reviewed the Self-Review Toolkit which is the Anti-Fraud annual report. This was subsequently submitted to NHS Protect with an overall rating of green.
8. EXTERNAL AUDIT
The Annual External Audit Plan was presented by the Trust’s External Auditors, Deloitte LLP and approved at the 9th September 2015 meeting. Representatives from Deloitte were present at each meeting and the Committee considered written and verbal reports on the progress of their audit and issues which had arisen. The Committee held a closed session (Non-Executives only) with Deloitte in January 2016.
9. FINANCIAL REPORTING AND FINANCIAL REVIEW
Financial performance and key financial assumptions The Committee reviewed the financial performance of the Trust and tests key financial assumptions at each meeting. Financial Statements to 31st March 2015 The Committee reviewed the draft Financial Statements of the Trust for the 2014/15 financial year at the 27th May 2015 meeting, and these were recommended for approval by the Chief Executive on behalf of the Board. The Chief Financial Officer presented the draft financial statements and there followed a discussion on a number of areas including:
Asset valuation processes and impairment charges
Bad debt provisions
Presentation of the results on the Trust and clarification on the way accounting impairment adjustments were explained
Quality Accounts and local quality indicator At this meeting, the Committee also received a report from the Trust’s External Auditors and had the opportunity to discuss the results of the audit and the Letter of Representation to Deloitte LLP to be signed on behalf of the Board. The Committee received the Head of Internal Audit Opinion report from the Head of Internal Audit, who was able to give a substantial assurance opinion for 2014/15 based on the work he had undertaken.

6
10. FUTURE PLANS
The Board approved the financial plan in March 2016 for the Financial Year 2016/17. The key financial risks were identified and therefore the AFC has the following priorities for its work in 2016/17:
Tariff funding and revenue recognition
Funding of Capital Programme
R&D income
Junior doctors’ contract The Committee has also identified a number of other priorities that support the overall risk and financial operation of the Trust, which are:
Efficiency Programme
Sutton Estate developments
IT investment
Vanguard Funding In conjunction with QAR, the AFC will also review:
Quality Accounts
Risk Management Arrangements and Board Assurance Framework
Liability Insurance
Ian Farmer Chair, Audit and Finance Committee May 2016

BOARD PAPER SUMMARY SHEET
Date of Meeting:
1st June 2016
Agenda item 10
Title of Document: Board Assurance Framework
To be presented by
Nancy Hallett, Senior Independent Director
Executive Summary The purpose of the Board Assurance Framework (BAF) is to provide the Board with assurances when considered alongside the Trust’s risk management processes, the statement of internal control and the programme of internal audit. Recommendations The Board is asked to review the Board Assurance Framework and discuss accordingly. Author: Chief Nurse and Senior Independent Director Nancy Hallett
Contact Number or E-mail: 2121
Date: 18th May 2016


1
Board Assurance Framework, May 2016
1.0. Introduction
The purpose of the Board Assurance Framework (BAF) is to provide the Board with assurances when considered alongside the Trust’s risk management processes, the statement of internal control and the programme of internal audit (NHS 2015). Oversight of effective risk management by the board is underpinned by four interlocking systems of control:
• The BAF • Organisational Risk Management • Audit • The Annual Governance statement.
2.0. The Board Assurance Framework (BAF)
This is a document that sets out strategic objectives, identifies risks in relation to each strategic objective along with controls in place and assurances available on their operation. Formats vary but the framework generally includes:
- Objective - Principal risk and risk owner - Key controls - Sources of assurance - Gaps in control/assurance - Action plans for addressing gaps (NHS 2013)
3.0. The BAF at The Royal Marsden

2
The RM BAF in Appendix 1 presents the key strategic objectives for The Trust that have been identified from the four key themes identified in the Strategic Plan2015 – 2018.. Detailed operational and corporate risks can be found in The Royal Marsden Risk Register which is presented to the Quality, Assurance and Risk committee quarterly. Through an on-going consultation process with Executive Directors, Divisional Directors and some Heads of Service, the organisation is in a position to:
• Ascertain key risks associated with the strategic objectives and identify the controls in place to manage the risks; • Continuously review the Board Assurance Framework for 2016/17 and assess the risks that have either resolved or reduced significantly.
4.0. Development of The BAF at The RM In May 2013 the existing design of the BAF was discussed by the Non Executive Director Chairs for the Audit and Finance Committee (AFC), Quality Assurance and Risk Committee (QAR), the Chief Financial Officer and Chief Nurse. Although the format was fit for purpose it was felt that its length and breadth might dilute focus on key strategic risks. The Trust therefore consulted with internal and external audit and with other NHS Foundation Trusts (The Christie NHS FT, Guys and St. Thomas NHS FT, University College NHS FT) and a clearer more concise format was chosen. This new format was presented to the QAR committee in July 2013, the format was welcomed but the content needed further refinement. The BAF was further refined and brought back to the December QAR. Following further comments from QAR and KPMG further amendments were made in February 2014. The Board endorsed the new format and content of the BAF in 2014. In April 2015 the BAF has been updated to reflect the new RM five year Strategic Plan 2014/15-2018/19 which in turn takes into account the NHS Five Year Forward View (October 2015). 5.0. Recommendation The Trust Board is asked to:
• Adopt and endorse the current position of the Board Assurance Framework for 2016/17 whilst recognising that further information to support the Framework and provide assurance is submitted during the year.
• Consider gaps reported against the Board Assurance Framework where there is a risk that the Trust might not achieve one or part of its key objectives.
• Ensure identified assurances within the framework are being explicitly reported to and monitored by the Board. References Well-led Framework for governance reviews: guidance for NHS Foundation Trusts (April 2015), Monitor NHS Foundation Trust Code of Governance (2014) Monitor NHS Leadership Academy (2013) The Healthy NHS Board: Principles for Good Governance NHS Five Year Forward View (2014)

3
Assurance Score: 1 – 5 with 1-2 (Red) being minimal assurance of objective being delivered / 3-4 (Amber) Medium value assurance / 5-6 (Green) high value assurance of objective being delivered. Grey not possible to make an assessment. (EXISTING Appendix 1: The Royal Marsden Board Assurance Framework, October 2015
Strategic objectives
Annual objectives 2015-16 and Lead Director
Assurance score
Key Controls (what controls/systems are in place to assist in securing delivery of the objective)
Gaps in control (where is there failure to put controls into place. Where are they not effective)
Assurance (there is evidence that shows we are reasonably managing risks and objectives are being delivered)
Gaps in assurance (where are we failing to gain evidence that our controls/systems on which we place reliance are effective)
Actions and timescales/progress
Outcomes of discussion by relevant committee (QAR, Audit, Board)
1. Innovation and precision medicine- Clinical sustainability/Value for Money
1.1. Delivery of Biomedical Research Centres research strategy and preparation for bid in 2016. The RM /ICR CEOs.
RED Cancer Centre Strategy Board and Clinical Research Executive provide oversight of the bid preparation. Writing group established; video presentation prepared. Joint ICR/RM Research Strategy approved by both ICR/RM boards April 2016.Soft launch by July 2016
Athena Swan Silver status awarded January 2016
Oversight of progress at weekly Clinical Research Executive (CRE), chaired by Director of Clinical Research
We have been informed we may receive full funding or +10%, -10% or -50%
PQQ submitted 15 February 2016. All themes in the RM/ICR BRC have been shortlisted; RBH lung cancer theme shortlisted. Interviews to be held on 29th July; seven senior representatives from both ICR/RM allowed
Board has approved Joint Research Strategy April 2016
1.2. Maintaining top quartile
Green Fortnightly Trial Set Up meeting in place to plan/manage capacity for clinical research delivery
None; RM has been informed by
Oversight of progress at weekly Clinical Research
New research performance metrics have been
Maintain current oversight of performance

4
Strategic objectives
Annual objectives 2015-16 and Lead Director
Assurance score
Key Controls (what controls/systems are in place to assist in securing delivery of the objective)
Gaps in control (where is there failure to put controls into place. Where are they not effective)
Assurance (there is evidence that shows we are reasonably managing risks and objectives are being delivered)
Gaps in assurance (where are we failing to gain evidence that our controls/systems on which we place reliance are effective)
Actions and timescales/progress
Outcomes of discussion by relevant committee (QAR, Audit, Board)
research performance. Helping to ensure the UK is globally competitive as a centre for clinical trials. COO
Quarterly reviews of all research delivery group financial and operational performance, including accruals and 70 day target. No change
NIHR that there will be no financial penalty
Executive, chaired by Director of Clinical Research Monthly review of research targets at Performance Group, chaired by Director of Performance Reported on Trust Board scorecard.
developed as part of board scorecard annual review; to be reviewed at May Board
CRE and monthly Performance Group monitoring
1.3. Providing research leadership in cancer for local clinical research networks. COO
Amber Professor Stan Kaye appointed as director of Research in the RM Partners Cancer Vanguard
COO/CFO attendance at CRN Partnership Board
Network study accrual performance is reviewed at RM Clinical Research Leads meeting and Clinical Research Executive; both chaired by Director of Clinical Research
Decreasing CRN financial allocation; control by South London CRN Flexible workforce model enforced by NIHR/south London CRN. Assistant Director R&D managing CRN staff
Contingency funding application successful. It is important strategically that RM continues to perform well with network studies (currently deliver 51% of South CRN cancer research) but at risk due to decreasing funding. CRE and FSG
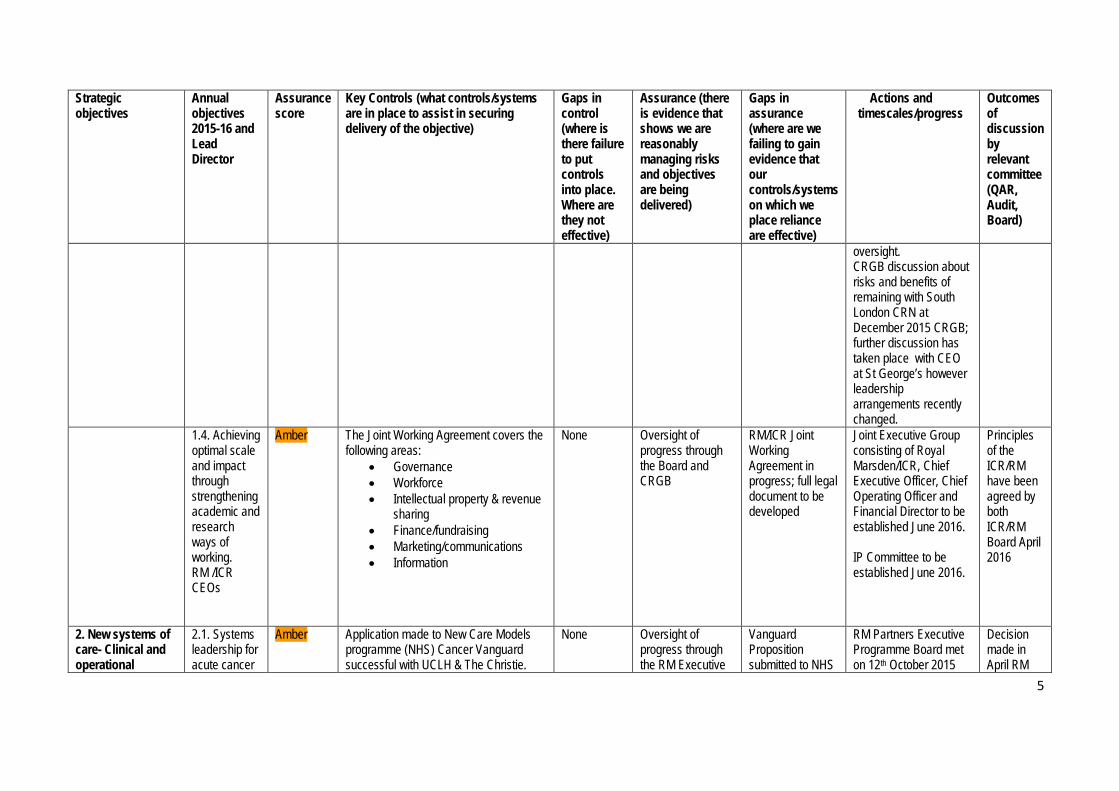
5
Strategic objectives
Annual objectives 2015-16 and Lead Director
Assurance score
Key Controls (what controls/systems are in place to assist in securing delivery of the objective)
Gaps in control (where is there failure to put controls into place. Where are they not effective)
Assurance (there is evidence that shows we are reasonably managing risks and objectives are being delivered)
Gaps in assurance (where are we failing to gain evidence that our controls/systems on which we place reliance are effective)
Actions and timescales/progress
Outcomes of discussion by relevant committee (QAR, Audit, Board)
oversight. CRGB discussion about risks and benefits of remaining with South London CRN at December 2015 CRGB; further discussion has taken place with CEO at St George’s however leadership arrangements recently changed.
1.4. Achieving optimal scale and impact through strengthening academic and research ways of working. RM /ICR CEOs
Amber The Joint Working Agreement covers the following areas:
• Governance • Workforce • Intellectual property & revenue
sharing • Finance/fundraising • Marketing/communications • Information
None Oversight of progress through the Board and CRGB
RM/ICR Joint Working Agreement in progress; full legal document to be developed
Joint Executive Group consisting of Royal Marsden/ICR, Chief Executive Officer, Chief Operating Officer and Financial Director to be established June 2016. IP Committee to be established June 2016.
Principles of the ICR/RM have been agreed by both ICR/RM Board April 2016
2. New systems of care- Clinical and operational
2.1. Systems leadership for acute cancer
Amber Application made to New Care Models programme (NHS) Cancer Vanguard successful with UCLH & The Christie.
None Oversight of progress through the RM Executive
Vanguard Proposition submitted to NHS
RM Partners Executive Programme Board met on 12th October 2015
Decision made in April RM

6
Strategic objectives
Annual objectives 2015-16 and Lead Director
Assurance score
Key Controls (what controls/systems are in place to assist in securing delivery of the objective)
Gaps in control (where is there failure to put controls into place. Where are they not effective)
Assurance (there is evidence that shows we are reasonably managing risks and objectives are being delivered)
Gaps in assurance (where are we failing to gain evidence that our controls/systems on which we place reliance are effective)
Actions and timescales/progress
Outcomes of discussion by relevant committee (QAR, Audit, Board)
sustainability care. CEO and CN.
Value proposition accepted for 15/16 and £1,000,000 awarded. VP for 16/17 submitted 8th February to NCM team, National Cancer Team and RM Executive. Draft governance framework shared with RM Exec and NCM team January 2016. Papers on rationale, governance, financial and contracting models shared with the Board from October to April 2016.
Board up to the RM Board. External oversight by NCM team and National Cancer Team – Commissioning Provision and Accountability Oversight Group 1st meeting 13th May 2016.
England awaiting financial agreement. Think Tank composed of senior clinicians across West London meets monthly. RM Partners Executive Programme Board meets monthly includes CEs from across the system.
and continues to meet monthly. 1st Clinical Partners event 25th Nov 2015. Clinicians Think Tank meet every month Frequent meetings with specialist and local commissioners and Transforming Cancer Services London throughout and involved in STP planning.
Board to ask two NEDs to be involved in planning between Board meetings. Two NEDs have agreed with first meeting 11th May and 2nd with CEO 16th May 2016.
2.2. Pathway redesign: creating efficient clinical pathways to improve quality and value and manage
Amber Access Policy; best Use of Best Resource approved November 2014 Inpatient and outpatient pathway transformation is being managed through the Transformation Board chaired by COO; started March 2015
Further refinement of Access Policy in development
Actively monitored monthly at PRG. Chaired by COO Local activity monitored through the CBUs managed by Clinical Directors & DD Cancer
Management of portfolio is dependent upon support of commissioners New medical model implemented in Chelsea and pilot
Ongoing monitoring through PRG and Transformation Board Through transformation board clinical advisory committee to be established by M D. AOS locum Consultants

7
Strategic objectives
Annual objectives 2015-16 and Lead Director
Assurance score
Key Controls (what controls/systems are in place to assist in securing delivery of the objective)
Gaps in control (where is there failure to put controls into place. Where are they not effective)
Assurance (there is evidence that shows we are reasonably managing risks and objectives are being delivered)
Gaps in assurance (where are we failing to gain evidence that our controls/systems on which we place reliance are effective)
Actions and timescales/progress
Outcomes of discussion by relevant committee (QAR, Audit, Board)
capacity. COO
Services Audits have been undertaken in second opinion activity and non elective admissions.
extended to Sutton approved by May FSG Non elective admission criteria has been refined
to be appointed for Sutton site.
2.3. Successful delivery of The Royal Marsden surgical strategy to ensure long term sustainability. Chief of Surgery/COO.
Red Surgical strategy implementation group in place; led by Chief of Surgery. Key work streams:
• Capacity planning through optimal resource utilisation
• Partnership plan • Portfolio management/patient
selection framework Early intervention by Palliative care and anaesthetics in OP setting.
Control of activity challenging Loss of private surgery due to other private providers due to capacity constraints;
Activity and financial monitoring through PRG; theatre utilisation processes put in place and shown early improvement
Minimum procedures mandated by CRGs and differences in coding and analysis between providers.
Ongoing Transformation Board oversight; surgical strategy mainstream Putting in place a new policy for conduct relating to private patient referrals. Ensuring RM representatives on the Surgical CRG
2.4. Development of integrated models of
Amber Sutton Community Services to be retained; Merton Services were awarded to other providers (CLCH and Connect Health).
None TUPE process completed; no redundancies Negotiating estate
Negotiation continues about the RIO IT contract (for
Disaggregation processes complete April 2016. FSG/EB oversight.
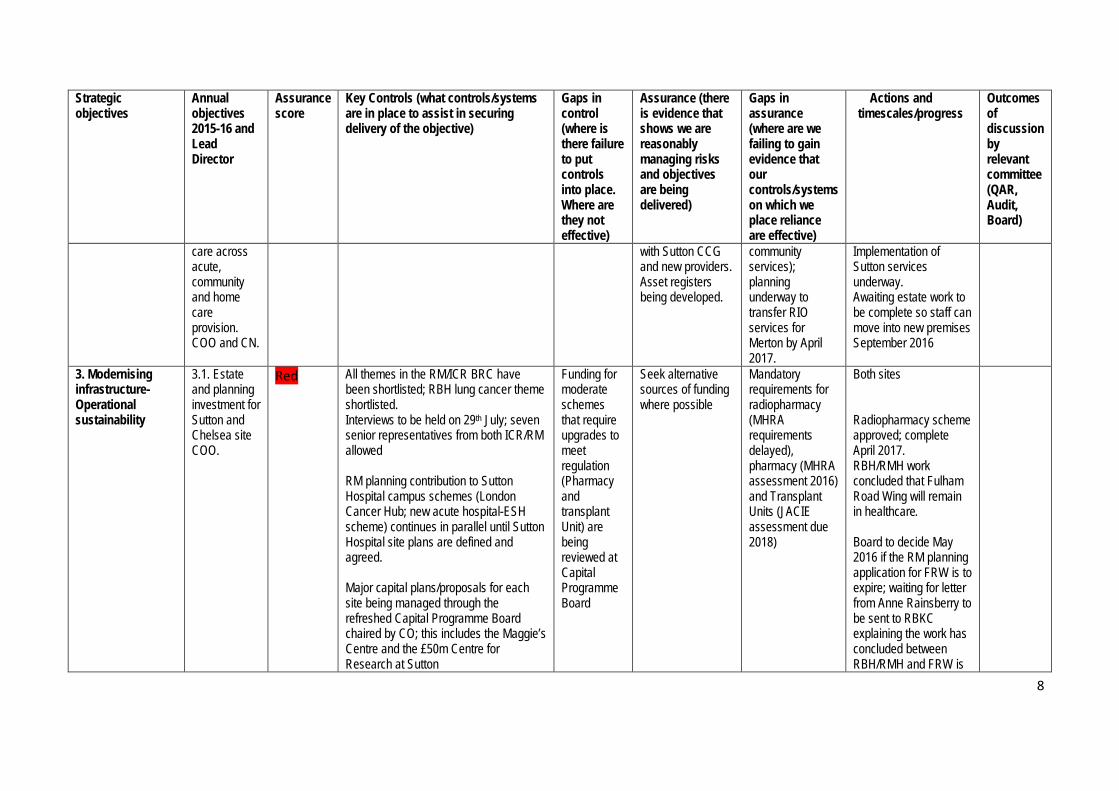
8
Strategic objectives
Annual objectives 2015-16 and Lead Director
Assurance score
Key Controls (what controls/systems are in place to assist in securing delivery of the objective)
Gaps in control (where is there failure to put controls into place. Where are they not effective)
Assurance (there is evidence that shows we are reasonably managing risks and objectives are being delivered)
Gaps in assurance (where are we failing to gain evidence that our controls/systems on which we place reliance are effective)
Actions and timescales/progress
Outcomes of discussion by relevant committee (QAR, Audit, Board)
care across acute, community and home care provision. COO and CN.
with Sutton CCG and new providers. Asset registers being developed.
community services); planning underway to transfer RIO services for Merton by April 2017.
Implementation of Sutton services underway. Awaiting estate work to be complete so staff can move into new premises September 2016
3. Modernising infrastructure- Operational sustainability
3.1. Estate and planning investment for Sutton and Chelsea site COO.
Red All themes in the RM/ICR BRC have been shortlisted; RBH lung cancer theme shortlisted. Interviews to be held on 29th July; seven senior representatives from both ICR/RM allowed RM planning contribution to Sutton Hospital campus schemes (London Cancer Hub; new acute hospital-ESH scheme) continues in parallel until Sutton Hospital site plans are defined and agreed. Major capital plans/proposals for each site being managed through the refreshed Capital Programme Board chaired by CO; this includes the Maggie’s Centre and the £50m Centre for Research at Sutton
Funding for moderate schemes that require upgrades to meet regulation (Pharmacy and transplant Unit) are being reviewed at Capital Programme Board
Seek alternative sources of funding where possible
Mandatory requirements for radiopharmacy (MHRA requirements delayed), pharmacy (MHRA assessment 2016) and Transplant Units (JACIE assessment due 2018)
Both sites Radiopharmacy scheme approved; complete April 2017. RBH/RMH work concluded that Fulham Road Wing will remain in healthcare. Board to decide May 2016 if the RM planning application for FRW is to expire; waiting for letter from Anne Rainsberry to be sent to RBKC explaining the work has concluded between RBH/RMH and FRW is

9
Strategic objectives
Annual objectives 2015-16 and Lead Director
Assurance score
Key Controls (what controls/systems are in place to assist in securing delivery of the objective)
Gaps in control (where is there failure to put controls into place. Where are they not effective)
Assurance (there is evidence that shows we are reasonably managing risks and objectives are being delivered)
Gaps in assurance (where are we failing to gain evidence that our controls/systems on which we place reliance are effective)
Actions and timescales/progress
Outcomes of discussion by relevant committee (QAR, Audit, Board)
to be retained for health use.
3.2. To ensure a sustainable paediatric service model at RM. CN
Amber Detailed submission to the Specialist Tertiary review 2014 of RM paediatric clinical and research data / quality metrics benchmarked nationally / internationally. ICR/RM succession planning for academic paediatric lead. CN & MD meetings with Clinicians, Clinical Directors and Medical Directors from across London including:
• St. Georges • The Evelina (GSTT) • Great Ormond Street / UCLH
These different models discussed with above children’s providers. RM keen to sustain a model with children’s in and outpatients at the RM site. RM acceptance may need to change admissions for some complex high risk procedures to a site with paediatric Intensive Care Unit on site. Influencing and lobbying of NHSE (London) Medical Director (Sponsor of
Further lobbying / submissions by all current London providers prohibited. The RM model without PICU on site unlikely to be the chosen model by NHSE. Current gap in senior academic leadership; appointed new Academic lead in
Verbal feedback that the external review team impressed by RM quality submission. Good and improved relationships with current PICU partner (SGH). Regular Executive Director led meetings with multi-professional paediatric clinical team leads. Successful RM leadership across the PTC with demonstrable
Awaiting outcome of external paediatric review. Review papers leaked and received by RM January. Immediate discussion with RM CE and Exec and SGH CE and Paed team. Discussion with Medical Director NHSE London 19/01/2016 and advised that they are awaiting advice from CE NHSE.
Bi-monthly meetings with clinical team leaders. QAR briefed in Jan 2016 re the leaked report. RM is preparing an omissions/factual accuracy report on the leaked paediatric review document Discussions on going between tertiary paediatric providers in London.

10
Strategic objectives
Annual objectives 2015-16 and Lead Director
Assurance score
Key Controls (what controls/systems are in place to assist in securing delivery of the objective)
Gaps in control (where is there failure to put controls into place. Where are they not effective)
Assurance (there is evidence that shows we are reasonably managing risks and objectives are being delivered)
Gaps in assurance (where are we failing to gain evidence that our controls/systems on which we place reliance are effective)
Actions and timescales/progress
Outcomes of discussion by relevant committee (QAR, Audit, Board)
review) and external Chair of Review.
February 2016 awaiting confirmation of acceptance and start date (requires move from Dana Faber, Boston, USA)
improvement in communication and clinical standards. Informal feedback from CQC Inspectors in April 2016 positive about the quality of care in the Children’s Unit.
3.3 Major equipment replacement scheme: including diagnostic (CT, MRI) and RT schemes CFO and COO
Red Major equipment schemes prioritised Major capital plans for each site being managed through the refreshed Capital Programme Board chaired by CFO
Funding gaps for replacing aging equipment. Equipment requiring replacement at similar timescales (large volume of equipment was originally
Equipment list has been merged into a single list of priorities agreed by clinical and management team
None RMCC schemes to be agreed Programme Board oversight

11
Strategic objectives
Annual objectives 2015-16 and Lead Director
Assurance score
Key Controls (what controls/systems are in place to assist in securing delivery of the objective)
Gaps in control (where is there failure to put controls into place. Where are they not effective)
Assurance (there is evidence that shows we are reasonably managing risks and objectives are being delivered)
Gaps in assurance (where are we failing to gain evidence that our controls/systems on which we place reliance are effective)
Actions and timescales/progress
Outcomes of discussion by relevant committee (QAR, Audit, Board)
funded from grants in 2004)
3.4 Development of a clear IT strategy and programme of delivery CFO and CCIO
Amber The IT strategy has been finalised and agreed by the IT Programme Board. The Board have approved the setup of a Joint venture with Chelsea & Westminster Trust that oversees and runs the technical aspects of the IT infrastructure. The CFO and COO are on the Board of the JV (Sphere). A review of the current EPR and options for replacement is currently being scoped. Monthly tracking against capital plan at ITPB
The strategy is limited by the funding available
The ITPB assesses the risk of the lack of investment and manages this within the resources available.
Recruitment of a CIO
A review of the strategy is planned for the Audit and Finance Committee later in the year. IT strategy to be approved by Board June 2016. Explore alternative funding sources such as managed service or national capital through the CSR.
3.5 Development of a sustainable medical model MD, DoW,
Amber Development of a sustainable and compliant junior medical model to support excellence in training is underway (rota review); ward based medical model; support roles) Inpatient Consultant model has been
Job planning exercise is resource intensive. Understand CMA compliance
Failure to recruit to Consultant posts in pathology although one post has been recruited to in April 2016
Action plans monitored at Workforce and Education Committee Development of new medical model forms part of the Transformation Board.

12
Strategic objectives
Annual objectives 2015-16 and Lead Director
Assurance score
Key Controls (what controls/systems are in place to assist in securing delivery of the objective)
Gaps in control (where is there failure to put controls into place. Where are they not effective)
Assurance (there is evidence that shows we are reasonably managing risks and objectives are being delivered)
Gaps in assurance (where are we failing to gain evidence that our controls/systems on which we place reliance are effective)
Actions and timescales/progress
Outcomes of discussion by relevant committee (QAR, Audit, Board)
DME, COO implemented October 2015 to support Core Medical Trainees; impact assessment to be undertaken Q4 2015-2016. Deanary visit December 2015 highlighted concerns about training in clinical oncology largely to do with workload and private patient care. Job planning review to be undertaken to ensure clarity of private/NHS planned activity sessions Succession planning and medical workforce planning processes to be agreed to ensure the medical workforce is sustainable to maintain national and international impact.
requirement Job planning is part of Medical Workforce Committee agenda
Paediatric academic leadership gap; candidate appointed awaiting confirmation of start date Haematology academic leadership gap. Planning underway
A PID is being developed and an update is due to be presented to the Board in September. Job planning approach agreed, monitoring to be undertaken at monthly by Medical Workforce Committee. Search committee with ICR being established for Haematology The Dean’s visit on the 11 April concluded that an integrated training model to incorporate both private care/NHS should be developed for Royal Marsden; this is being led by the DME/MD and trainees are involved in the process.

13
Strategic objectives
Annual objectives 2015-16 and Lead Director
Assurance score
Key Controls (what controls/systems are in place to assist in securing delivery of the objective)
Gaps in control (where is there failure to put controls into place. Where are they not effective)
Assurance (there is evidence that shows we are reasonably managing risks and objectives are being delivered)
Gaps in assurance (where are we failing to gain evidence that our controls/systems on which we place reliance are effective)
Actions and timescales/progress
Outcomes of discussion by relevant committee (QAR, Audit, Board)
4. Financial sustainability and best value.
4.1. Successful delivery of the private care Strategy which requires short and medium term initiatives to enable profitable growth. MD Private Care.
Amber Private care KPIs for financial, operational and clinical performance have been created. Reporting of these KPIs to happen quarterly to the Private Care Steering Committee (PCSC). Wider strategic initiatives taken to PCSC for approval to implement. Monthly performance review of Private care delivery as part of the PRG review. Monthly meetings to track income scheme delivery with action plans developed where under performance is identified. Major business cases supported, signed off and post implementation evaluated by FSG.
KPMG Private Care audit identified need for further training and process improvement in billing, debt collection and LOG performance.
Actions taken from KPMG audit are on track for completion. Business case for increased private care capacity approved and delivery to commence in 15/16. Introduce income/contribution targets and review performance against these.
Private care capacity from shared services needs to be more carefully monitored. Business planning for 16/17 to ensure PP shared service needs is fully resourced.
KPMG audit recommendations on track for delivery against target dates in 2016.
New capacity sought through partnership models with London PP providers. Business case to be developed in 2016.
Capital Programmes to increase capacity are being reviewed at programme board.
4.2. Ensuring fair prices for activity covered by
Red The Trust applied to Monitor for a Local price Modification in 2014, which was unsuccessful at the first hurdle as the Trust did not have a deficit greater than
There is not a clear national process for
The Trust is engaging with both Monitor and NHS England to review
The Trust is not in control of the process or timetable and
The tariff was delayed for 2016/17 and top-up payments for cancer have been deferred until
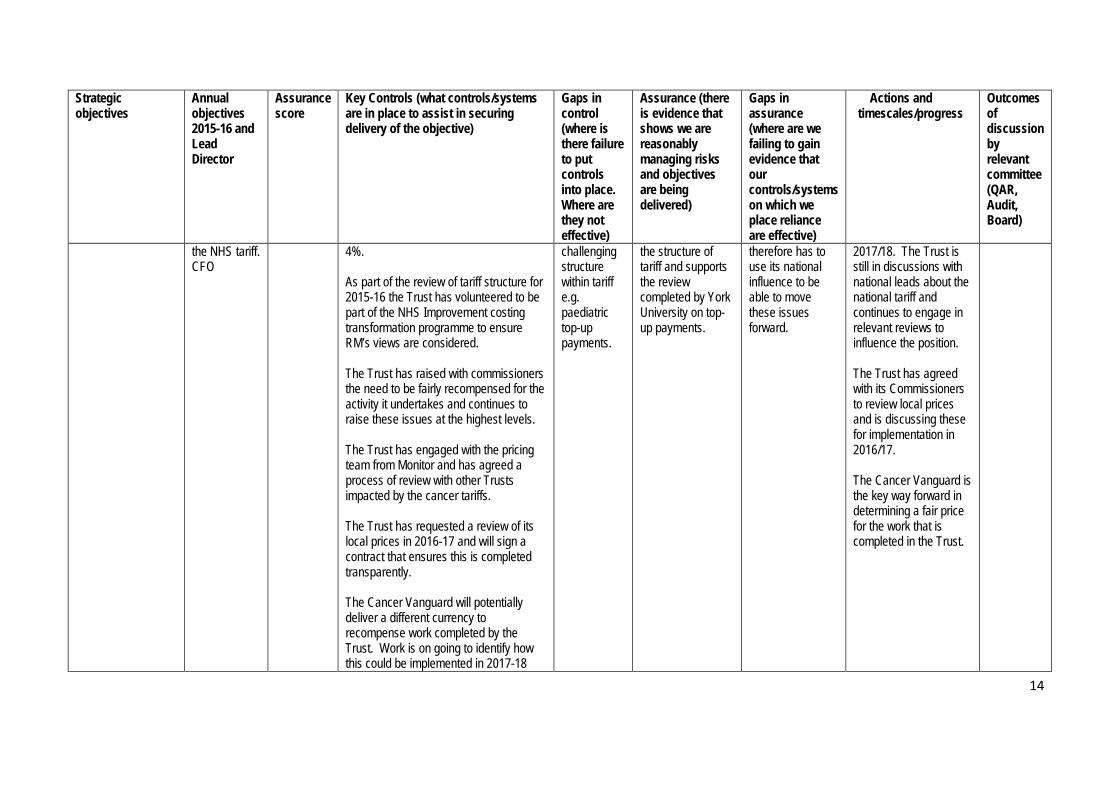
14
Strategic objectives
Annual objectives 2015-16 and Lead Director
Assurance score
Key Controls (what controls/systems are in place to assist in securing delivery of the objective)
Gaps in control (where is there failure to put controls into place. Where are they not effective)
Assurance (there is evidence that shows we are reasonably managing risks and objectives are being delivered)
Gaps in assurance (where are we failing to gain evidence that our controls/systems on which we place reliance are effective)
Actions and timescales/progress
Outcomes of discussion by relevant committee (QAR, Audit, Board)
the NHS tariff. CFO
4%. As part of the review of tariff structure for 2015-16 the Trust has volunteered to be part of the NHS Improvement costing transformation programme to ensure RM’s views are considered. The Trust has raised with commissioners the need to be fairly recompensed for the activity it undertakes and continues to raise these issues at the highest levels. The Trust has engaged with the pricing team from Monitor and has agreed a process of review with other Trusts impacted by the cancer tariffs. The Trust has requested a review of its local prices in 2016-17 and will sign a contract that ensures this is completed transparently. The Cancer Vanguard will potentially deliver a different currency to recompense work completed by the Trust. Work is on going to identify how this could be implemented in 2017-18
challenging structure within tariff e.g. paediatric top-up payments.
the structure of tariff and supports the review completed by York University on top-up payments.
therefore has to use its national influence to be able to move these issues forward.
2017/18. The Trust is still in discussions with national leads about the national tariff and continues to engage in relevant reviews to influence the position. The Trust has agreed with its Commissioners to review local prices and is discussing these for implementation in 2016/17. The Cancer Vanguard is the key way forward in determining a fair price for the work that is completed in the Trust.
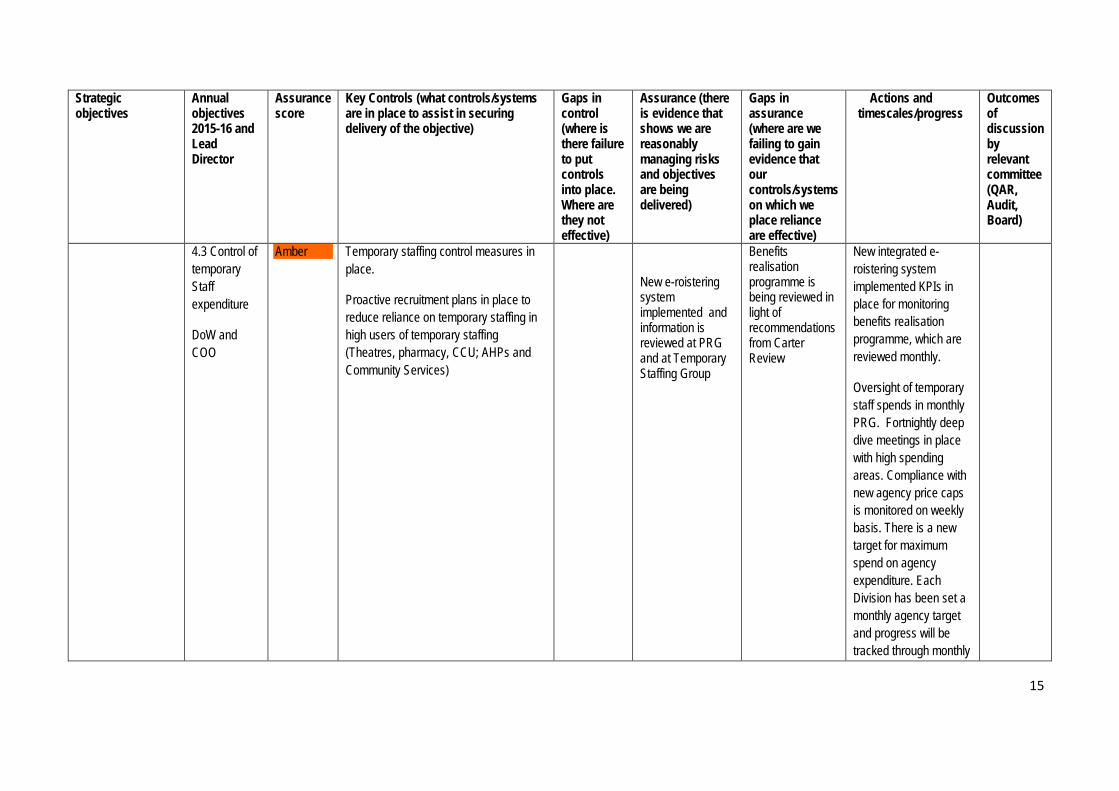
15
Strategic objectives
Annual objectives 2015-16 and Lead Director
Assurance score
Key Controls (what controls/systems are in place to assist in securing delivery of the objective)
Gaps in control (where is there failure to put controls into place. Where are they not effective)
Assurance (there is evidence that shows we are reasonably managing risks and objectives are being delivered)
Gaps in assurance (where are we failing to gain evidence that our controls/systems on which we place reliance are effective)
Actions and timescales/progress
Outcomes of discussion by relevant committee (QAR, Audit, Board)
4.3 Control of temporary Staff expenditure
DoW and COO
Amber Temporary staffing control measures in place.
Proactive recruitment plans in place to reduce reliance on temporary staffing in high users of temporary staffing (Theatres, pharmacy, CCU; AHPs and Community Services)
New e-roistering system implemented and information is reviewed at PRG and at Temporary Staffing Group
Benefits realisation programme is being reviewed in light of recommendations from Carter Review
New integrated e-roistering system implemented KPIs in place for monitoring benefits realisation programme, which are reviewed monthly.
Oversight of temporary staff spends in monthly PRG. Fortnightly deep dive meetings in place with high spending areas. Compliance with new agency price caps is monitored on weekly basis. There is a new target for maximum spend on agency expenditure. Each Division has been set a monthly agency target and progress will be tracked through monthly

16
Strategic objectives
Annual objectives 2015-16 and Lead Director
Assurance score
Key Controls (what controls/systems are in place to assist in securing delivery of the objective)
Gaps in control (where is there failure to put controls into place. Where are they not effective)
Assurance (there is evidence that shows we are reasonably managing risks and objectives are being delivered)
Gaps in assurance (where are we failing to gain evidence that our controls/systems on which we place reliance are effective)
Actions and timescales/progress
Outcomes of discussion by relevant committee (QAR, Audit, Board)
PRG meetings.
Abbreviations
CoG- Council of Governors
CEB-Clinical Executive Board
MAC- Medical Advisory Committee
NRRAC- Nursing, Radiology and Research Advisory Committee

BOARD PAPER SUMMARY SHEET
Date of Meeting: 1st June 2016
Agenda item 11
Title of Document: Trust Membership Report
To be presented by
For information
Background As an NHS Foundation Trust (FT), the Trust is expected to recruit and engage with its members i.e. patients, carers, staff and members of the public. The reason for this requirement is so that the organisation can be held to account by the community it serves but also, to help ensure that the Trust’s policy and strategy development is aligned with local and national needs. Executive Summary The purpose of this Report is to provide the Board with a summary of the Trust’s position with regard to membership and future plans to increase its membership base. Recommendations The Board is asked to note the Report and plans to increase membership recruitment and engagement. The Corporate Governance Team will continue to work closely with Governors on membership recruitment and engagement in order to ensure they are fulfilling their legal duty. Author: Syma Dawson, Trust Secretary
Contact Number or E-mail: x2826
Date: 17th May 2016


1
Membership Report
1. Introduction As an NHS Foundation Trust (FT), the Trust is expected to recruit and engage with its members i.e. patients, carers, staff and members of the public. The reason for this requirement is so that the organisation can be held to account by the community it serves but also, to help ensure that the Trust’s policy and strategy development is aligned with local and national needs. The purpose of this Report is to provide the Board with a summary of the Trust’s position with regard to membership and future plans to increase its membership base. 2. Membership 2.1. Why does The Royal Marsden have members?
Formal membership schemes were introduced for foundation trusts as a fundamental part of their governance framework. At its core, membership is simply about asking patients and public to help support the Trust. The Trust formally connects with it members through the Council of Governors and under the Health and Social Care Act 2012 Governors have a statutory role and responsibility to represent the interests of the members of the Trust. This legal responsibility implies a need for the Governors to engage with its members which through the work of the Membership and Communications group, a working group of the Council of Governors, membership recruitment and engagement is managed and monitored. 2.2. Who can become a member of The Royal Marsden?
Anyone aged 16 years old or over and lives in England can become a member of The Royal Marsden. The Trust has defined England as the geographical boundary for its membership constituencies, which is split into three constituencies: Patient and Carer, Public and Staff.
3. Current position As a specialist cancer centre with a local and national catchment area, there is recognition for the challenges the Trust will have in recruiting members, particularly to its patient and carer constituency. Furthermore, the specialist nature of the Trust’s business and the way in which membership is represented means it is difficult for the Trust to compare and benchmark its position but also benchmark its plans to recruit new members. As of the 31st March 2016, the Trust had 8,636 members, comprising of the following constituencies: • 1,579 Patient/Carer members • 3,446 Public members • 3,611 Staff members. 5. Membership Recruitment 5.1 Attract new and retain existing members
There are several ways in which a person can sign up to become a member: by completing an online form on the Trust website, picking up a form from around the hospital or contacting the Corporate Governance Office to request a form.

2
5.1.1 Current initiatives
It’s important to provide a simple and seamless process in becoming a member. The Membership & Communications Group re-designed the Trust membership form to make this more effective. Some of the recruitment activities undertaken to promote membership include: • RM magazine - advertising membership in every edition • Promoting Trust membership in official Trust literature and patient information • Reviewing and updating the membership content displayed on Trust information screens
around the hospital • Membership application forms on display across both sites • The Trust website dedicated membership pages including an online application form • Welcome letter from the Chief Executive to all new patients at registration • Volunteers of The Royal Marsden Friends being recruited as members and promoting
membership on their leaflets • Governors visiting local schools to promote the work of the Trust and encouraging young
adults to become members. 5.1.2 Recruitment options to be considered by the Membership and
Communications Group: • Installing membership message on the Patient Entertainment System • Automatically opting in new patients at registration • Approaching the volunteers of The Royal Marsden Friends to be membership champions • Promoting membership to Cancer related organisations • Promoting membership on the Boots pharmacy bags 6. Membership Engagement 6.1 Level of involvement
The Trust recognises that not all members can be or want to be active members. The Trust therefore has two levels of membership to help determine each member’s level of involvement and allows the Trust to manage resources more effectively. 6.2 Current engagement initiatives
• A welcome pack is sent to all new registered members which includes; a copy of the latest RM Magazine, letter from Chairman re: Governors, info re: membership and the two levels of membership, key contacts.
• Membership mailings - all patient/carer and public members receive a copy of the quarterly magazine which includes a covering letter from their governor(s), a copy of RM magazine and details of forthcoming events e.g. Members’ Events, Annual General Meeting, and other ad hoc engagement opportunities.
• E-bulletins - members who have given their email addresses receive ad hoc information to forthcoming events and engagement opportunities e.g. receiving the PACER survey: Patient priorities for Cancer Research.
• Holding and promoting members’ events to engage with members on the latest matters including the Quality Accounts, learning about facilities and receiving updates on key developments.
• Governors conducting structured clinical visits to gain direct experience from the perspective of patients, carers and members of staff and reporting the findings back to the Chief Nurse.
• Elections - When a vacancy arises on the Council of Governors, all members within the constituency are informed of the election and invited to stand.
In April 2016 elections were held in the following sub-constituency classes with respective candidates standing as below:

3
Constituency No. of
Candidates Standing
Patient – Kensington & Chelsea and Sutton & Merton (3 Governors) 5
Patient – Elsewhere in London (2 Governors) 8
Patient – Elsewhere in England ( 2 Governors) 12
Patient – Carer (2 Governors) 6
Public – Sutton & Merton (1 Governor) 4
Public – Elsewhere in England (1 Governor) 6
Staff – Clinical Professional (1 Governor) Elected unopposed
7. Conclusion The Board is asked to note the Report and plans to increase membership recruitment and engagement. The Corporate Governance Team will continue to work closely with Governors on membership recruitment and engagement in order to ensure they are fulfilling their legal duty.