board of directors meeting 08.30am 12.20pm, wednesday … 31 05 17 part 1 (e... · presentation...
TRANSCRIPT

Board of Directors Meeting
08.30am– 12.20pm, Wednesday 31 May 2017 Seminar Room, Children’s Centre, Dorset County Hospital
AGENDA DEVELOPMENT SESSION
Patient Experience Feedback To discuss
08.30 Sophie Jordan
PART 1 (PUBLIC SESSION)
Page No.
Approx. timings
1 Welcome and Apologies for Absence:
8.50 Chair
2 Declarations of Interest All
3 Chairman’s Remarks
Oral 8.55 Chair
4 Minutes of Board of Directors 29 March
2017 To approve
Enclosure 9.00 Chair
5 Matters Arising from those Minutes and
Actions List To receive
Enclosure 9.05 Chair
QUALITY AND PERFORMANCE ITEMS
6 Chief Executive’s Report To receive
Oral 9.10 PM
7 Integrated Performance Report: (to
include comments from Committee Chairs)
a. Quality b. Performance c. Finance d. Workforce
To receive and agree any necessary action
Enclosure 9.20 NL JP LW MW
Age
nda
Page 1 of 132

8 Medical Revalidation Progress Report To receive
To follow 10.20 PL
COFFEE BREAK 10.30
9 Inpatient Survey To receive
Enclosure and Presentation
10.45 NL
STRATEGIC ITEMS
10 Trust Vision – update To approve
Enclosure 11.00 NJ
11 Strategy – Board oversight
To note Enclosure 11.10 NJ
GOVERNANCE ITEMS
12 Corporate Risk Register and Board
Assurance Framework To note
Enclosure 11.20 NL/LW
13 Committee Work Plans
To receive Enclosure 11.35 Committee
Chairs
14 Board Self-Assessment of Effectiveness To review
Enclosure 11.45 Chair
CONSENT SECTION
The following items are to be taken without discussion unless any Board Member requests prior to the meeting that any be removed from the consent section for further discussion.
11.55
15 Report on Use of the Trust Seal
To receive Enclosure PM
16 Safe Staffing Return (previously reviewed at
Quality Committee) To approve
Enclosure NL
17 Annual Complaints Report (previously
reviewed at Quality Committee To note
Enclosure NL
18 Any Other Business
Chair
Date of Next Meeting (open to the public): Wednesday 26 July 2017, 8.30 a.m., Seminar Room, Children’s Centre, Dorset County Hospital
Age
nda
Page 2 of 132

Questions from the Council of Governors and Members of the Public – 12.05- 12.20. Fifteen minutes will be allowed for questions, with priority being given to Governor questions submitted in advance of the meeting. Note: The Board will now adopt the resolution that “Governors, members of the public and representatives of the press are excluded from the next part of the meeting because publicity would be prejudicial to the public interest by reason of the confidential nature of the business about to be transacted”.
Age
nda
Page 3 of 132

1
BOARD OF DIRECTORS PART 1 (PUBLIC SESSION)
Minutes of the Meeting of 29 March 2017
Seminar Room, Children’s Centre, Dorset County Hospital
Present: Mr Mark Addison (Trust Chair) Mr Peter Greensmith (Vice Chair) Prof Sue Atkinson (Non-Executive Director) from BoD17/022 Mr Graeme Stanley (Non-Executive Director) Mr Matthew Rose (Non-Executive Director) Ms Victoria Hodges (Non-Executive Director) Ms Judy Gillow (Non-Executive Director) Ms Patricia Miller (Chief Executive) Ms Libby Walters (Director of Finance and Resources) Mr Mark Warner (Director of Organisational Development (OD) and Workforce) Ms Julie Pearce (Chief Operating Officer) (COO) Mr Paul Lear (Medical Director) Ms Nicky Lucey (Director of Nursing and Quality) (DoN)
In Attendance: Mr Nick Johnson (Director of Strategy and Business
Development) Dr Richard Jee (Divisional Director Designate) Dr Will McConnell (Divisional Director Designate) Ms Lindsey Perryman (Trust Secretary) Ms Catherine Abery- Williams (Divisional Manager for Family Services) for BoD17/022 Ms Anna Ekerold (Paediatric Matron) for BoD17/022 Ms Sarah Knight (Divisional Manager) for BoD17/030 Ms Sophie Jordan (Divisional Manager) for BoD17/030
Apologies: None Observers: 1 member of the public
BoD17/022 Board Development Session – Patient Experience Feedback
Catherine Abery- Williams, Divisional Manager for Family Services and Anna Ekerold, Paediatric Matron, joined the meeting. Anna advised of a 19 day old baby admitted to Kingfisher Ward in December 2015 with suspected pyloric stenosis. She advised the baby required intravenous fluids which were administered through a peripheral cannula in the foot. The following day, an extravasation injury was confirmed upon the realisation that the baby’s leg was swollen above the knee. The baby was then transferred to Southampton for surgical management of pyloric stenosis. She advised that the root cause analysis had highlighted missed opportunities which may have prevented the extravasation injury become as severe these included;
Staff nurse did not respond to prompts from Health Care Support Worker that
Min
utes
Page 4 of 132

2
the patients name band was tight on the ankle 4 hours prior to detection of extravasation.
No Visual Infusion Phlebitis scores were carried out
The baby’s bandage was not removed to visualise the cannula site
The baby’s crying was attributed to hunger rather than pain. Anna advised that the following recommendations from the root cause analysis were implemented:
Risk summary circulated to all Kingfisher staff highlighting the main points of the incident
Extravasation teaching provided to all staff on annual updates
Staff competency developed and implemented for all staff who are signed off to administer fluids or medication via the intravenous route
Yearlong peripheral cannulation audit undertaken, amongst other criteria this also included recorded of VIP scores and documentation.
Anna highlighted that the good news was that there had been no further extravasations since implementation of actions. Patient had follow up daily dressings for 3 weeks post extravasation injury by the CCN team who delivered exceptional care. There was no lasting injury from the extravasation. Anna advised that the baby was readmitted days afterward with bronchiolitis. She highlighted that the parents had expressed some concerns but that staff were able to reassure them and provide safe effective care during this admission. [Sue Atkinson joined the meeting at this point] The Chair questioned how the original incident had been handled. Anna advised that both the consultant and the staff nurse had spoken to the parents and apologised. She advised that she felt the parents were shocked at the time but that their concern surfaced on the second admission. The DoN advised that compliance with cannula checks was now embedded across the organisation. The Chair thanked Anna and Catherine for attending the meeting and for the straightforward and clear explanation of what had gone wrong and how lessons had been learnt.
BoD17/023 Welcome and Apologies for Absence
The Chair welcomed everyone present to the meeting. There were no apologies. The Chair particularly welcomed Will McConnell and Richard Jee who he advised had been invited to attend the Board in advance of their appointment as Divisional Directors from 1 April following which they would be present at Board meetings as non-voting attendees.
BoD17/024 Declarations of Interest
There were no declarations of interest in relation to items on the agenda. The Chair reminded members that declarations of interest could be raised at any time during the meeting should they arise.
BoD17/025 Chairman’s Remarks
The Chair highlighted to the Board that the Trust was now able to report that it would
Min
utes
Page 5 of 132

3
be achieving its financial control total for 2016/17. He highlighted the achievement this had been in light of the position the Trust had been in 9 months previously and thanked everybody for their hard work in achieving this. The Chair highlighted the Charity events taking place and in particular the “Walk for Wards”. He advised that he was meeting Canon Eric Woods on 20 March and that he was also hopeful that the Lord Lieutenant would be able to be present at the Trust on 5 April for the photoshoot. The Chair reported that the date for the AGM had been set for the 11 July with a slightly different format. The Trust Secretary advised that the Council of Governors meeting would be held in the afternoon followed by tea and cake prior to the start of the AGM. The Chair advised that he had now met the three new Dorset Chairs and that they would be making arrangements to meet and develop links.
BoD17/026 Minutes of the Previous Meeting held on 25 January 2017
With the correction of a typo, the minutes of the previous meeting held on 25 January 2017 were accepted as a true and accurate record.
BoD17/027 Matters Arising and Actions
BoD17/010 – the Medical Director advised that the Guardian of Safe Working would report to the Quality Committee as well as the Board. The Chair recalled that the Board had agreed that it would receive a written report quarterly with Jonathan Chambers attending on an annual basis to present his report – close. BoD16/109 – Comments from long service awards – the Chief Executive confirmed that these were on display – close. BoD16/109 – Key actions in integrated performance report – the Chair reminded the Board of the need to include the key points from Board committees in the summary of papers. It was noted that there was an issue of timing and that Execs, NEDs and the Trust Secretary would need to work together to ensure these were drawn out, possibly by discussing at the end of the meetings. BoD16/088 – Committee Work programmes – the Chair advised that work on these was almost complete following which they would be presented to the Board. BoD16/092 – STP modelling – the Director of Strategy and Business Development reported that one of the overriding responses to the CSR from all providers was a need for more modelling and that there was a lack of clarity as to what had been modelled. Peter Greensmith advised he had heard that the CCG would be looking at the impact of new homes on GPs which might imply that this was the first time this had been modelled. The Chief Executive highlighted that the CCG had clearly articulated a reduction in acute beds but had not yet responded to the query raised regarding the basis of this. The Chair confirmed that the issue of modelling would be raised when he next met with the CCG.
BoD17/028 Chief Executive’s Report
The Chief Executive presented a previously circulated report providing the Board with information on strategic developments across the NHS and more locally within Dorset. The Chair thanked her for the more personal style of report.
Min
utes
Page 6 of 132

4
The Chief Executive highlighted the announcement by NHS England that provider deficits were being covered by the 1% funding that CCGs had been required to retain for supporting system working. She highlighted the NHS cap on new drugs and reported that the statement by Simon Stevens during the last few days about prescription was directly related to supporting the funding of drugs. The Chief Executive highlighted the announcement in the budget of £2.4bn over 3 years but advised that the Local Government Association had indicated that an additional £2B of funding was required in 2017/18 alone to meet current needs She advised that there was no assurance as to where the additional funding would be spent. In respect of the additional £100m of capital funding to support the delivery of the 4 hour standard through closer working with GPs, the COO reported that the Trust had considered how it might bid for capital. The Chief Executive highlighted the report by the CQC which gave a flavour of the findings from their inspections and expressed concern in respect of the number of trusts which were finding themselves rated as inadequate and had not made significant improvements at re-inspection. The Chief Executive drew the Board’s attention to the timetable in respect of the CSR consultation and the expectation of the final decision in September. She advised that the CCG were having two away days in April to consider the responses to the consultation and that the themes would be presented to the Senior Leadership Team. The Chief Executive highlighted the attendance detailed in the report of the divisional management teams at Board and Committees. She advised that that the Divisional Heads of Nursing would also be attending the Quality Committee. The Chief Executive reported that the Trust had had its quarterly meeting with NHS Improvement on 28 March where reasonable confidence had been expressed in the ability of the Trust to deliver but with concern in respect of the short to medium term financial situation and RTT. She confirmed that the Trust had been given approval to delay its external Well-Led review. The Board resolved to note the content of the report.
BoD17/029 Integrated Performance Report
The COO presented a previously circulated report providing an overview of operational performance and highlighting areas of under-performance and risks including the 9 “must dos”. She advised that the new style report was a compilation of input from all of the Executive Team. The COO highlighted the following areas of good performance:
Access standards for ED and 62 day cancer pathway
Access to diagnostic tests – predicted to meet standard for March
Predicted achievement of financial control total The COO highlighted the main performance risks facing the Trust for 2017/18:
Maintaining RTT performance above 90% and demonstrating improvement against an agreed trajectory
Improvement in mortality reporting and coding The COO reported that only the ED 4 hour standard would be linked to STF funding for 2017/18
Min
utes
Page 7 of 132

5
. Quality – the DoN highlighted the continued good performance in respect of Infection Prevention and Control. She advised that the Trust continued to underperform against the Dementia standards and that she would be requesting support from the Divisional Directors in embedding this. The DoN reported that work was continuing to try and improve the turnaround time of complaint responses. Sue Atkinson, who had chaired the most recent meeting of the Quality Committee, advised that stroke and dementia standards were both being scrutinised in detail by the Quality Committee. She reported that the last meeting had received a report on mortality and coding but that there was still some reservation that the work in hand would resolve the issues. Judy Gillow asked for an update on the weekend HSMR scores. The Medical Director advised that the understanding was that the level of diagnosis made at the weekend was lower than that during the week. He advised that clinicians had been asked to make a definitive diagnosis. Judy Gillow gave an update on mortality from the National Mortality Review meeting she had attended. She advised that the responsibility of the Board would increase in respect of monitoring a more detailed mortality dashboard, learning and how reviews were undertaken. Judy Gillow confirmed that she was preparing a briefing note for Board members. The Medical Director confirmed to the Board that, although reviews showed a small number of cases where patients could have been managed differently, he was confident there were no issues in regard to the quality of care. Judy Gillow advised that she felt the Trust did not yet have full assurance that there was not an issue. Richard Jee highlighted that, in respect of critical care, assurance could be obtained from the Intensive Care National Audit and Research Centre (ICNARC) data. The Chief Executive confirmed that there were a number of national audits that showed the Trust mortality rates were at or below the expected rates and that there was a need for this information to be pulled together as an assurance piece. Performance – the COO advised that the Trust was considering the feasibility of delivery of the RTT standard by the end of quarter 2. She advised that there were some risks mainly in respect of Ophthalmology and Paediatrics. The COO highlighted that if Ophthalmology was taken out of the equation the Trust achieved the 92% target. Matthew Rose confirmed that RTT was one of the key areas of focus for the Finance and Performance Committee and would continue to be. He advised that the Committee also wanted to enhance the work around activity and the triangulation of contract activity, budget and RTT. The Director of Finance and Resources expressed some concern that the Trust had underperformance against contract, had national funding to support the delivery of RTT but had still not achieved the target. The Chief Executive report that last week it had been announced that STF funding for quarter 4 would be paid purely on the achievement of financial targets. Finance – the Director of Finance and Resources confirmed that the Trust was now forecasting achieving the £1.8m deficit control total due the changes in payment of STF funding for quarter 4 and being able to claim the back payments for the ED 4 hour target. She advised that the overpayment of £750k from the CCG had still to be finalised. The Director of Finance and Resources reported that the cash position was better than planned due to the management of capital payment, delaying payment of creditors and chasing debtors. She advised that the Trust was forecasting requiring
Min
utes
Page 8 of 132

6
cash support in July but that it was likely this would be later due to the tendency for slippage in capital expenditure. The Director of Finance and Resources highlighted the need to the Trust to assess whether the activity in the contract and the financial envelope would enable the Trust to achieve the RTT target. She highlighted that there was currently just under £5m of unidentified CIP for 2017/18. Workforce – the Director of Organisational Development and Workforce reported that the Trust had seen a spike in sickness levels for January, however, it was the lowest level of sickness seen in January for four years. He reported that the Trust had seen a reduction in fill rates for agency staff which was reflective of the changes in the market place partially due to the changes in HMRC rules for those engaged on personal services contracts. The Director of Organisational Development and Workforce reported that the level of appraisals had remained constant. He advised that the Trust were now beginning the appraisal cycle with band 7s and above to align with the business planning cycle. The Director of Organisational Development and Workforce reported that a new approach for refresher training for essential skills was being introduced where staff would complete an assessment on line for all refresher modules. He advised that the Trust did not do a cut by staff group but by staffing area. He confirmed that where there was a particularly low compliance in a subject an action plan was put in place. The Director of Organisation Development and Workforce reported that the government had announced this week a 1% pay rise for staff on Agenda for Change payscales and doctors and dentists. The Chair welcomed the excellent new summary dashboard for the Board and requested that any comments were provided to the COO.
Action: ALL The Board resolved to note the issues raised and agree the actions to ensure compliance.
BoD17/030 Trust Performance Management Framework
Sarah Knight and Sophie Jordan attended the meeting for this item. The COO advised that this report had been discussed at Finance and Performance Committee and complemented the Governance Framework to ensure robust processes around all of the Trust’s business. She advised that the Executive Team wanted to work towards earned autonomy for the divisions and that Sophie and Sarah would give a presentation at a high level about work in the divisions and how the framework would help. Sarah and Sophie highlighted the structure of the performance matrix and gave an outline of the structure of the two new divisions each containing 4 care groups. They advised that the divisions would be trying to mirror the processes at a Board level and set the same standards across both divisions. They gave an outline of the priorities for quarter 1:
• Agree metrics and align with performance dashboards • Work with new Transformation Lead to establish levels of intervention and
roles of the team • High Level review of Divisions using established metrics (peer review)
Min
utes
Page 9 of 132
7
• Divisions to report at Quarterly Performance Meeting • Agree reporting framework for Care Groups • Implement the Trust Clinical Governance Framework to complement the
performance framework. They advised that during quarter 2 the performance processes would be cascaded to the 8 care groups. The divisional managers confirmed that both divisions had identified HR, finance and information support. In terms of underperformance the divisional managers advised that peer review would be used as an interventional tier. Peter Greensmith highlighted the need for staff at ward level to understand the process and to have given “consent” to follow. The DoN advised that the ward leaders were engaged in the dashboard but that there was a need for the divisional management to coach to embed the change. It was acknowledged that work was required to change the culture. It was agreed that a quality priority should be added to the annual priorities for 2017/18 with the suggestion that this was learning from deaths.
Action: JP
The Director of Strategy and Business Development highlighted the need to look at how performance was aligned to strategic outcomes. The Chief Executive advised that the Executive Team recognised that there was a need to streamline the management processes to support earned autonomy and highlighted the need to ensure that the Head of Transformation was used for transformation and not to tackle poor performance. She reminded the Divisional Managers that it was proposed for the divisions to present to the Board following their quarter 1 self-assessment. In response to a question from the Chair, Richard Jee advised that to some extent the consultant community were not yet engaged but that he was meeting individually with divisional leads. It was agreed that it would be helpful to have a simple assessment tool listing the six or so key things the new model was designed to achieve to enable review in a year. The Board noted the content of the report and agreed to the trial of the first iteration of the framework.
BoD17/031 2016 National Staff Survey Findings
The Chair advised that one of the discussions which had taken place with the Leadership Academy was to have some items presented to the Board where all members were reviewing them at the same time ie they had not been presented to a Board committee or to Executive Directors. This report had accordingly come directly to the Board. The Director of Organisational Development and Workforce reported that the Staff Survey was the most important metric that the Trust had in terms of staff engagement. He advised that it was based on a full paper census which had had a 54% response rate. The Director of Organisational Development and Workforce advised that the Trust was considering the use of a mixture of electronic and paper based survey for the coming year dependent on staff group.
Min
utes
Page 10 of 132
8
The Director of Organisational Development and Workforce highlighted the Staff Engagement Index which he advised showed no significant change from last year and was consistent with the national average. He advised that there was no statistically significant change in any of the key findings. The Director of Organisational Development and Workforce advised that it was important to share the outcomes with the divisions and for them to develop their action plans. He highlighted that the People Strategy was focused on staff engagement but that it would be helpful for the Trust to identify 2 or 3 areas to focus on. The Chief Executive advised that she felt there was a need for the Trust to ask staff what would change their level of engagement. The following comments were made in the course of a full discussion:
We should avoid a major new action plan but focus on trying to identify what lies beneath the responses and what local teams could do to address these issues
There was a need to promote front line conversations about what was driving the feedback
Some of the responses and the low level of movement overall from last year seemed at odds with the general feel and culture of the hospital
There was a theme about leadership
We should move towards a “You said, we did” style of feedback and communication
Visibility of middle and senior management appeared to be an issue
The new performance and governance frameworks give the opportunity to link responses to the survey to link to existing initiatives
There need to be a link between the management response and the strategy (to be in the top quartile).
The Board noted the content of the report and the actions in response to the survey set out in the Staff Engagement Action Plan.
BoD17/032 Freedom to Speak Up Guardian
The Director of Organisational Development and Workforce presented a previously circulated report which he advised set out a change to the approach to the requirement to have a Freedom to Speak up Guardian. He advised that Graeme Stanley had been undertaking this role linked to his role as the SID and the Whistleblowing NED but that recent guidance made it clear that this role should not be undertaken by a NED. The Director of Organisational Development and Workforce advised that the proposal was to invite two or three staff to volunteer to take on the role and that it was proposed that these staff would meet with Graeme Stanley, the Chief Executive and himself on a bi-monthly basis. It was agreed that, in terms of the role description, the language should be less formal. The Board approved the proposal for the appointment of Freedom to Speak up Guardians and as for the communication of the new roles to be as straightforward as possible.
Min
utes
Page 11 of 132
9
BoD17/033 Easy Guide to Dorset Health The Director of Strategy and Business Development spoke to a single slide which aimed to condense the Dorset landscape onto one page all fitting under the umbrella of the Five Year Forward View. He explained the relationship between the Dorset wide STP with its five work streams, the CSR which he advised was a subset of the STP with the Vanguard delivering some of the CSR. The Director of Strategy and Business Development highlighted the Trust’s five strategic objectives and the corresponding strategic programmes. The Board welcomed the one page explanation.
BoD17/034 Trust response to the Dorset CCG Mental Health Acute Care Pathway
Consultation Questionnaire The Director of Strategy and Business Development presented a previously circulated paper detailing the proposed Trust response based on views from the Senior Management Team and the Emergency Department. The following comments were made:
Concern was expressed regarding the predominance of beds in the East
There should be more data to support the comments in respect of Out of Hours and Crisis
There was a need for better/more data on need
There was no mention of integration
Consideration of changing the response on the degree of support for the proposals from “to some extent” to “not very much”
The Board:
agreed the Mental Health Acute Care Pathway Consultation response subject to amendment to take account of the comments above
delegated authority to the Director of Strategy and Business Development to make any final minor adjustments, in consultation with the Chief Executive, and submit the response on behalf of the Trust by the deadline of 31 March.
BoD17/035 Corporate Risk Register and Board Assurance Framework
The Director of Finance and Resources advised that it was felt it may be useful to bring the Corporate Risk Register and Board Assurance Framework into one document so that operational risks that were becoming so significant they could impact on objectives could be identified. BAF- the Director of Finance and Resources highlighted the two red risks in relation to the ability to deliver transformational change and having sufficient cash. She reported that the Trust had appointed to the Head of Transformation but had failed to recruit a CIP Manager. The Director of Finance and Resources advised that the risk relating to opportunities for services to be tendered not arising had been reduced to green due to looking to the market for business not being key to the Trust at the current point in time. The Director of Finance and Resources highlighted the two risks that had increased from green to amber:
personal records including medical records should be accurate and kept safe and confidential – due to internal audit on the IG Toolkit showing that
Min
utes
Page 12 of 132

10
assurance was not as robust as the Trust had thought
trust being open to fraud – due to the need to ensure that cyber security risks had been addressed.
CRR – the DoN reported that the Emergency Department risk had been reduced due to the Trust now meeting the 4 hour standard. She highlighted that there were two new risks:
ENT medical staff – although there had been some mitigation since the report and also return from sick leave
Fire alarm reliability and capability – the DoN advised that this risk had been identified in 2014 but due to plans to resolve being deferred the risk had increased. She advised that the risk was currently being managed with repairs but that these were becoming more frequent.
The DoN advised that in terms of the risk around RTT this was included on the risk register under Ophthalmology. Discussion took place in respect of the current and mitigated risk ratings, particularly in respect of the fire alarm risk. It was agreed that there was a need to consider renaming the current risk rating and to look at clarifying the definitions.
Action: NL
The Director of Finance and Resources confirmed that she had requested a formal update to be presented to the Board on fire safety. It was agreed that the financial sustainability risk should be reviewed considering the cash position and the level of required CIP.
Action: LW The Board noted the Corporate Risk Register and Board Assurance Framework
BoD17/036 Guardian of Safe Working Quarterly Report
The Medical Director presented a previously circulated report outlining the work undertaken to implement the new contact and the potential risks over the next 6 months. It was noted that this report was not in the consent section due to lack of full assurance due to the risk in terms of middle grades particularly in medicine. Will McConnell suggested that the Trust should consider taking an overstaffing risk on the basis that there would always be gaps. He confirmed that the divisions were looking at different staffing models. The Chief Executive advised that the Trust were considering how medical staffing might be reported as there was a need for the Board to be aware of the possible clinical risk and the need for pace in terms of the development of alternative models. The Board noted the content of the report.
BoD17/037 Review of Bi-Monthly Board Meetings
The Chair presented a previously circulated report detailing the output from the survey of Board members regarding the changes to the Board meeting cycle. He advised that there was almost unanimous support of continuing with bi-monthly meetings although there was an understandable concern as to risks of many items
Min
utes
Page 13 of 132
11
appearing on the agenda. The Board noted the feedback and agreed to the continuation of holding formal Board meetings on a bi-monthly basis.
BoD17/038 Consent Section
The Chair confirmed that no requests had been received to remove items from the consent section for discussion, and therefore the following were taken as agreed:
Staffer Staffing Return (previously reviewed by the Quality Committee): approved
Vanguard Update: noted
BoD17/039 Any Other Business
Insight Programme – the Chair introduced this initiative which he advised was aimed at developing aspiring but inexperienced potential NEDs. The Board agreed to participate in the programme.
BoD17/040 Date of Next Meeting
The date of the next meeting was scheduled for Wednesday 31 May 2017, Seminar Room, Children’s Centre, Dorset County Hospital, 8.30am.
BoD17/041 Questions from Governors and Members of the Public
The Chair confirmed that no questions had been received in advance of the meeting. The following question/comment was received from Governors/Public present:
The CCG has consistently talked about population projections and having higher than average numbers of elderly people and babies. His own GP surgery had 100 new patients per annum which would result in several thousand new patients across the region. Poundbury has been built fairly recently and the local plan was being reviewed as it was not showing enough land for new housing. Query as to why health did not benefit from section106 payouts as part of the planning permission process.
The Board adopted the resolution that “members of the public, Governors and
representatives of the press are excluded from the next part of the meeting because publicity would be prejudicial to the public interest by reason of the confidential nature of the business about to be transacted”.
…………………………. ……………………. Chair Date
Min
utes
Page 14 of 132

ACTIONS LIST – BOARD OF DIRECTORS PART 1 31 MAY 2017
Minute Action Owner Timescale Outcome
BoD17/029 Integrated performance report – comments on new dashboard to be provided to COO
All April 2017
BoD17/030 Performance Management Framework - It was agreed that a quality priority should be added to the annual priorities for 2017/18 with the suggestion that this was learning from deaths
JP April 2017 This indicators has been added to the framework and the framework policy and guidelines have been finalised for use by the Divisions & care groups
BoD17/035 Risk Register - Discussion took place in respect of the current and mitigated risk ratings, particularly in respect of the fire alarm risk. It was agreed that there was a need to consider renaming the current risk rating and to look at clarifying the definitions.
NL May 2017 Reviewed with Estates
BoD17/035 Risk Register - It was agreed that the financial sustainability risk should be reviewed considering the cash position and the level of required CIP.
LW May 2017
Actions carried forward from previous meetings
BoD16/088 Committee chairs to review work programmes and bring to board for approval
MA/PM/ committee
Chairs/ lead execs
March 2017
On agenda
BoD16/092 Sustainability and Transformation Plan – details of modelling to be obtained from CCG
NJ Oct 2016 March - issue of modelling to be raised when trust next meets
Act
ions
Lis
t
Page 15 of 132

with the CCG
Act
ions
Lis
t
Page 16 of 132

Title of Meeting
Board of Directors
Date of Meeting
31 May 2017
Report Title
Performance Report
Author
Executive Team
Responsible Executive
Chief Executive
Purpose of Report (e.g. for decision, information) To inform the board of operational performance for month 1 (April) 2017 and to identify areas of concern and risk
Summary The overall performance demonstrated that improvements in quality and access achieved during Q4 and March 2017 was not sustained during April 2017. This was due to service capacity constraints resulting from key gaps in the medical workforce. In addition, the impact of the transition to the new organisational structure placed extra stress on operational teams. A change in staff and teams taking responsibility for specific services and care groups within the divisions has had an impact on sustaining performance improvement. It is anticipated that this will settle down during May and June. The continued poor and deteriorating performance in ophthalmology means that this service is now subject to internal ‘special measures’ regime as described in the performance management framework, and this means that the service will be subject to close scrutiny by both the divisional and executive team and specific interventions will be required until the service becomes more stable. The improvement regime will be overseen by FPC.
Paper Previously Reviewed By Quality Committee and Finance and Performance Committee on 23rd May 2017 Items for escalation from Quality Committee
Mortality – ongoing focus. It was agreed that a verbal update would be provided in May with a deep dive to include timescales for actions to be presented to the June meeting.
CQC report - assessment of any additional risks since the CQC visit eg current risk regarding middle grade medical staffing
The provision of face to face specialist palliative care service 7 days a week, as identified within the CQC Action plan. An internal pilot provided this service over a 7 day period, and audited the support required by the Trust. This is being discussed with the palliative care team in early June.
Timeliness of complaints. The Trust has not been able to demonstrate the improvements required. A detailed action plan was presented and discussed
There has been a positive improvement in dementia screening, and although the standards are not at the level required, the Committee recognised that significant progress had been made and were presented with the draft Dementia Strategy in support of these improvements.
Inte
grat
ed P
erfo
rman
ce R
epor
t
Page 17 of 132
Items for escalation from FPC
Overall RTT performance - main area of concern is ophthalmology; further presentation to FPC and Quality Committee in June.
CIP gap
Triangulation of contract/performance from budgeted activity compared with actual delivery – we are behind budget plan and this is a potential contractual risk with CCG
Workforce – survey of nurses, committee asked if this could be cut to show results for those approaching retirement and also detail of comments re lack of support of managers
Strategic Impact The performance of the Trust impacts on two strategic objectives related to sustainability of services and ability to provide good and outstanding care in relation to quality and access.
Risk Evaluation The extreme risk level in ophthalmology and overall poor performance on RTT with a lack of pace to improve the service has placed the service into ‘internal special measures’ as defined in the Trusts performance management framework. The Executive team are working with the division and specialty to over-see the improvement and will be receiving an options paper 1st June
Impact on Care Quality Commission Registration and/or Clinical Quality Performance focuses on all five domains linked to the standards of services underpinning registration and quality of services.
Governance Implications (legal, clinical, equality and diversity or other): Operational performance is governed through the policy and performance management framework and deals with all forms of performance.
Financial Implications Poor performance can result in additional cost associated with a shortfall in capacity in order to improve access for patients. Any patient safety and quality concerns may also carry additional cost
Freedom of Information Implications – can the report be published?
Yes
Recommendations
a) To note the report b) To discuss the issues escalated by quality committee and FPC c) To agree any additional actions
Inte
grat
ed P
erfo
rman
ce R
epor
t
Page 18 of 132
1 | P a g e
Balanced-Score Card Performance Report
Report to Board: 31 May 2017
Performance Summary:
The overall performance demonstrated that improvements in quality and access achieved during Q4 and March 2017 was not sustained during April 2017. This was due to service capacity constraints resulting from key gaps in the medical workforce. In addition, the impact of the transition to the new organisational structure placed extra stress on operational teams. A change in staff and teams taking responsibility for specific services and care groups within the divisions has had an impact on sustaining performance improvement. It is anticipated that this will settle down during May and June. The continued poor and deteriorating performance in ophthalmology means that this service is now subject to internal ‘special measures’ regime as described in the performance management framework, and this means that the service will be subject to close scrutiny by both the divisional and executive team and specific interventions will be required until the service becomes more stable. The improvement regime will be overseen by FPC. Main Performance Risks facing the Trust in 2017/18 Quality and Access risks:
- Medical workforce in Medicine, Ophthalmology, Gastroenterology, ENT and Obstetrics/Gynaecology and impact on waiting times for patients; and due to the national supply shortage in medicine and nursing presents a risk in terms of agency usage and cost
- EDS completion partially linked to the IT system configuration between the clinical system and patient administration system - Complaints timeliness - C.difficile annual position due to peak in month - Dementia screening rate – improvement not yet embedded - Access to and waiting times in Ophthalmology – the service is now subject to internal ‘special measures’ - Impact of loss of locum breast radiologist on the fast-track cancer waiting times in the breast service - Data accuracy and quality related to the reporting of mandatory training and appraisal rates
Financial risks
- Gap in cost improvement programme and pace at which the system transformation programme can be prioritised and mobilised to support divisional teams in closing the CIP gap.
- Ability to meet the trust control total and access to sustainability and transformation funding
Inte
grat
ed P
erfo
rman
ce R
epor
t
Page 19 of 132

2 | P a g e
Quality and FPC Recommendations Escalation from Quality Committee in April and May:
Mortality – ongoing focus. It was agreed that a verbal update would be provided in May with a deep dive to include timescales for actions to be presented to the June meeting.
CQC report - there was a discussion regarding the risks re middle grade staffing but also acknowledgement of the need to assessment whether any additional risks had arisen since the CQC visit
The provision of face to face specialist palliative care service 7 days a week, as identified within the CQC Action plan. An internal pilot provided this service over a 7 day period, and audited the support required by the Trust. This is being discussed with the palliative care team in early June, and a meeting has been arranged with Weldmar Hospice.
Timeliness of complaints. The Trust has not been able to demonstrate the improvements required. A detailed action plan was presented and discussed with the Quality Committee in May, with divisions confirming that this is now discussed at the divisional Governance meetings. Improvements are expected with the incoming Divisional Heads of Nursing/Quality, supported by the new Quality Managers for each division. The introduction of the Datix system will also allow more transparency.
There has been a positive improvement in dementia screening, and although the standards are not at the level required, the Committee recognised that significant progress had been made and were presented with the draft Dementia Strategy in support of these improvements.
Escalation from FPC in April and May:
Overall RTT performance - main area of concern is ophthalmology; further presentation to FPC and Quality Committee in June.
CIP gap
Triangulation of contract/performance from budgeted activity compared with actual delivery – we are behind budget plan and a potential contractual risk with CCG
Workforce – survey of nurses, committee asked if this could be cut to show results for those approaching retirement and also detail of comments re lack of support of managers
Inte
grat
ed P
erfo
rman
ce R
epor
t
Page 20 of 132

3 | P a g e
Are we on track to deliver the 9 Must Dos? Key Performance Metrics Summary
Metric Met? Metric Standard Mar-17 Apr-17 Q1/YTD
MRSA hospital acquired cases (post 48hrs) 0 0 0 0
C-Diff hospital acquired cases (post 72 hours) - Due to lapses in care 14 0 2 2
Never Events 0 0 0 0
Serious Incidents declared on STEIS (under investigation)51
(4 per month)6 2 2
SHMI - Rolling 12 months, 6 months in arrears (Oct-15 to Sep-16) <1.12 N/A N/A 1.15
HSMR - Rolling 12 months, 2 months in arrears (Mar-16 to Feb-17) 100 N/A N/A 99.42
RTT incomplete pathways within 18 weeks (Quarter/Year = Lowest 'in
month' position)92% 89.2% 86.0% 86.0%
All cancers maximum 62 day wait for first treatment from urgent GP
referral85% 89.4% 71.4% 71.4%
Maximum 6 week wait for diagnostic tests 99% 99.4% 95.4% 95.4%
ED maximum waiting time of 4 hours from arrival to admission/transfer/
discharge (Including MIU/UCC activity from November 2016)95% 99.1% 98.7% 98.7%
Elective levels of contracted activity (£)2017/18 = 26,674,034
M1 = 2,222,8362,592,431 2,118,414 2,118,414
Surplus/(deficit) (1,208) 1,138 (497) (497)
CIP - year to date (aggressive cost reduction plans)2017/18 = (8,774)
Q1 = (464)6,794 (154) (154)
Agency spend in month2017/18 = 3,122
Q1 = 1,212216 248 248
Rating Key
Develop and implement an affordable plan to make improvements in
quality. In addition, providers will be required to publish avoidable
mortality rates annually.
Partially
Achieve and maintain the two new mental health waiting time targets.N/A
Improve care for people with learning disabilities including improved
community services and reducing inpatient facilities.Yes
Improve and maintain performance against 18 weeks RTT target. No
Deliver the 62 day cancer waiting time target including two week referral
and 31 day treatment targets and make progress in improving one year
survival rates by increasing the proportion of cancers diagnosed early.
Partially
Qu
ality
Perf
orm
an
ce
Fin
an
ce
Produce a sustainability and transformation plan for the health economy Yes
Return to "aggregate financial balance", deliver savings through the Lord
Carter productivity programme and cap agency spendPartially
Develop and implement a local plan to address the sustainability and
quality of general practice, including workforce and workload issues.N/A
Achieve waiting time targets for A&E patients and ambulance response
times.Yes
Inte
grat
ed P
erfo
rman
ce R
epor
t
Page 21 of 132

4 | P a g e
INTEGRATED PERFORMANCE REPORT – Exception Reports by Domain Safe In relation to Infection Prevention and Control, the Trust has not reported any cases of MRSA Bacteraemia, but has seen an increase in cases of C Difficile during this month. Initial analysis of these cases has identified an issue in the prompt isolation of patients experiencing symptoms and this has been cascaded to all staff. The individual cases will be presented to the Infection Prevention and Control Committee once full investigation has been completed. There were 5 patient safety risk events reported resulting in potential severe harm/death during this period; 2 have been reported as Serious Incidents, 3 are to undergo full root cause analysis and presentation to the Learning from Incidents Panel to determine the level of harm caused. These related to 1 failure to escalate a deteriorating patient, 1 Missed follow up appointment, 1 Incorrect suturing post procedure, 1 potential of missed diagnosis of spinal injury on presentation to ED. These are all due to be presented to the Learning from Incidents panel to ascertain if procedures need to be amended and identify where improvements are required. There was also one fall reported during this period which resulted in severe harm. This unfortunate case related to an individual with a prosthetic limb who fell whilst transferring. All correct procedures were followed. Effective The mortality indicators for the Trust remain of concern. There is a detailed action plan to address the areas of improvement and this has been discussed and analysed by the Quality Committee. Although the standards for dementia screening were not achieved during the month, a significant improvement has been identified. This has been discussed through the Dementia Working Group. There remains a risk in fully achieving and sustaining the standards for all elements, which continues to be addressed via the Divisions. Caring Both the response rates and recommendation rates of Inpatient, Emergency Department and Outpatients have been above the agreed standards for this reporting period. Themes of this feedback are discussed at the Patient Experience Group in order to identify any areas of further improvement. The timeliness of complaint responses remains of concern. A full detailed Improvement will be discussed at this month’s Quality Committee for assurance that this standard will meet its improvement trajectory. Well Led The Trust delivered an Income and Expenditure deficit of £497,000 at the end of April which was £711,000 better than planned. This positive variance is due in the main to the majority of the savings plan being expected to be delivered towards the end of the financial year. The Trust has to
Inte
grat
ed P
erfo
rman
ce R
epor
t
Page 22 of 132
5 | P a g e
achieve a deficit of no more than £2.9 million in 2017/18 which will require £8.7 million of savings to be delivered. There is currently £4.5 million of savings still to be identified. Temporary staffing spend increased in Month 1 but was below prior year. Sickness absence remained unchanged at 3.35% in March. There was a further decrease in the appraisal rate (-4%) to 74% sitting below the Trust target of 90% and a significant decrease in essential skills compliance (-7%) to 83%. The data quality for both of these metrics is being reviewed: the essential skills data has been subject to updates from the national system which has presented some errors, and the internal process for recording appraisal data is being updated. Significant work has been ongoing to mitigate medical workforce gaps resulting from expected shortfalls in junior doctor placements. Preparation for the Trusts second phase of the Leadership Development programme are well advanced, with the programme for all Band 3-6 team leaders commencing on 21 June.
Inte
grat
ed P
erfo
rman
ce R
epor
t
Page 23 of 132

6 | P a g e
Integrated Scorecard 2017/18 - April 2017
MetricThreshold/
StandardType of Standard Mar-17 Apr-17 Q1/YTD
Movement on Previous
period
12 Month
Trend
Safe
Infection Control - Methicillin Resistant Staphylococcus Aureus (MRSA)
bacteraemia hospital acquired post 48hrs0
Contractual (National
Quality Requirement)0 0 0 ↔
Infection Control - C-Diff hospital acquired (post 72 hours) - Due to lapses in
care14
Contractual (National
Quality Requirement)0 2 2 ↓
NEW Harm Free Care (Safety Thermometer) 95% Local Plan 98.3% 98.9% 98.9% ↑
Never Events 0Contractual (National
Requirement)0 0 0 ↔
Serious Incidents investigated and confirmed avoidable 0 1 1 ↓
Duty of Candour - Cases completed Contractual (National
Quality Requirement)?0 3 3 ↓
Duty of Candour - Investigations completed with exceptions to meet compliance 0 1 1 ↓
NRLS - Number of patient safety risk events reported resulting in severe harm or
death35 (2 per month)
Local Plan
(2015/16 outturn)1 5 5 ↓
Number of falls resulting in fracture or severe harm 8 for year
Local Plan (10%
reduction on 2015/16
outturn)
1 1 1 ↔
Pressure Ulcers - Hospital acquired (grade 2) confirmed avoidable TBC 0 0 0 ↔
Pressure Ulcers - Hospital acquired (grade 3) confirmed avoidable TBC 0 0 0 ↔
Emergency caesarean section rate 17.6% 17.3% 17.3% ↑
Sepsis Screening - percentage of patients who met the criteria of the local
protocol and were screened for sepsis.90% CQUIN target 66.0% N/A N/A ↑
Effective
Mortality Indicator SHMI (in-hospital and those occurring 30 days post
discharge) - Rolling 12 months [source HSCIC] - 6 months in arrears (Oct-2 or 3
Contractual (Local Quality
Requirement)N/A N/A 1 ↔
Mortality Indicator SHMI (in-hospital and those occurring 30 days post
discharge) - Rolling 12 months [source HSCIC] - 6 months in arrears (Oct-<1.12
Contractual (Local Quality
Requirement)N/A N/A 1.15 ↔
Mortality Indicator HSMR from CHKS - 2 months in arrears (Mar-16 to Feb-17) 100Contractual (Local Quality
Requirement)100.55 99.42 N/A ↑
Mortality Indicator Weekend Non-Elective HSMR from CHKS - 2 months in
arrears (Mar-16 to Feb-17)100
Contractual (Local Quality
Requirement)111.60 110.01 N/A ↑
Stroke - Overall SSNAP score C or aboveContractual (Local Quality
Requirement)N/A N/A N/A
Dementia Screening - patients aged 75 and over to whom case finding is applied
within 72 hours following emergency admission 90%
Contractual (Local Quality
Requirement)70.8% 80.5% 80.5% ↑
Dementia Screening - proportion of those identified as potentially having
dementia or delirium who are appropriately assessed90%
Contractual (Local Quality
Requirement)100.0% 100.0% 100.0% ↔
Dementia Screening - proportion of those with a diagnostic assessment where
the outcome was positive or inconclusive who are referred on to specialist 90%
Contractual (Local Quality
Requirement)61.9% 95.7% 95.7% ↑
Caring
Compliance with requirements regarding access to healthcare for people with a
learning disabilityCompliant Compliant Compliant Compliant ↔
Complaints - Number of formal & complex complaints 217 (18 per month)Local Plan
(2015/16 outturn)23 10 10 ↑
Complaints - Percentage response timescale met (1 month in arrears)60% Apr-16
90% Jul-16
Trajectory (monthly
10% increments to 44.0% N/A N/A ↔
Friends and Family - Inpatient - Recommend 95% Mar-16 National Average 99.4% 98.6% 98.6% ↓
Friends and Family - Emergency Department - Recommend 84% Mar-16 National Average 88.8% 88.3% 88.3% ↓
Friends and Family - Outpatients - Recommend 92% Mar-16 National Average 93.7% 92.9% 92.9% ↓
Number of WOW! Award applications received 559 (46 per month)Local Plan
(2015/16 outturn)28 12 12 ↓
Inte
grat
ed P
erfo
rman
ce R
epor
t
Page 24 of 132

7 | P a g e
Responsive
Referral To Treatment Waiting Times - % of incomplete pathways within 18
weeks (QTD = Lowest 'in month' position)92%
Contractual (National
Operational Standard)89.2% 86.0% 86.0% ↓
Cancer (ALL) - 14 day from urgent gp referral to first seen 93%Contractual (National
Operational Standard)97.2% 77.4% 77.4% ↓
Cancer (Breast Symptoms) - 14 day from gp referral to first seen 93%Contractual (National
Operational Standard)100.0% 28.6% 28.6% ↓
Cancer (ALL) - 31 day diagnosis to first treatment 96%Contractual (National
Operational Standard)97.1% 97.3% 97.3% ↑
Cancer (ALL) - 31 day DTT for subsequent treatment - Surgery 94%Contractual (National
Operational Standard)77.8% 100.0% 100.0% ↑
Cancer (ALL) - 31 day DTT for subsequent treatment - Anti-cancer drug regimen 98%Contractual (National
Operational Standard)100.0% 100.0% 100.0% ↔
Cancer (ALL) - 31 day DTT for subsequent treatment - Other Palliative 98%Contractual (National
Operational Standard)100.0% 100.0% 100.0% ↔
Cancer (ALL) - 62 day referral to treatment following an urgent referral from GP
(post)85%
Contractual (National
Operational Standard)89.4% 71.4% 71.4% ↓
Cancer (ALL) - 62 day referral to treatment following a referral from screening
service (post)90%
Contractual (National
Operational Standard)100.0% 100.0% 100.0% ↔
% patients waiting less than 6 weeks for a diagnostic test 99%Contractual (National
Operational Standard)99.4% 95.4% 95.4% ↓
ED - Maximum waiting time of 4 hours from arrival to admission/transfer/
discharge 95%
Contractual (National
Operational Standard)98.1% 97.1% 97.1% ↓
ED - Maximum waiting time of 4 hours from arrival to admission/transfer/
discharge (Including MIU/UCC activity from November 2016)95%
Contractual (National
Operational Standard)99.1% 98.7% 98.7% ↓
Well Led
Annual leave rate (excluding Ward Manager) % of weeks within threshold 11.5 - 17.5% 50.81% 29.84% 29.84%
Sickness rate (one month in arrears) 3.3%Internal Standard
reported to FPC3.35% N/A N/A ↑
Appraisal rate 90%Internal Standard
reported to FPC78% 74% 76% ↓
Staff Turnover Rate 8 -12%Internal Standard
reported to FPC11.6% 11.3% 11.3% N/A
NHS Staff Survey
CQC Inpatient Survey
GMC Survey
Total Workforce Capacity 2,394Internal Standard
reported to FPC2,245.0 2,248.0 2,248.0 N/A
Vacancy Rate (substantive) <5%Internal Standard
reported to FPC3.4% 6.1% 6.1% ↓
Total Pay Cost 9,634.0Internal Standard
reported to FPC8,965.7 9,065.1 9,065.1 ↓
Number of formal concerns raised under the Whistleblowing Policy in month N/AInternal Standard
reported to FPC0 0 0 N/A
Essential Skill Rate 90%Internal Standard
reported to FPC90% 83% 83% ↓
Elective levels of contracted activity (activity)2017/18 = 26,874
M1 = 2,240 2,468 2,076 2,076 ↓
Elective levels of contracted activity (£)2017/18 = 26,674,034
M1 = 2,222,836 2,592,431 2,118,414 2,118,414 ↓
Surplus/(deficit) (year to date)2017/18 = (2,904)
Q1 = (3,633)Local Plan 1,122 (497) (497) ↑ N/A
Surplus/(deficit) (in month/quarter) (1,208) Local Plan 1,138 (497) (497) ↑
Cash Balance 901 4,427 5,356 5,356 ↑
CIP - year to date (aggressive cost reduction plans)2017/18 = (8,774)
Q1 = (464)Local Plan 6,794 (154) (154) ↑ N/A
Agency spend in month2017/18 = 3,122
Q1 = 1,212216 248 248 ↓
Agency % of pay expenditure2017/18 = 2.9%
Q1 = 4.2%2.4% 2.7% 2.7% ↑
Movement Key
Favourable Movement ↑ Achieving Standard
Adverse Movement ↓ Not Achieving Standard
No Movement ↔
Inte
grat
ed P
erfo
rman
ce R
epor
t
Page 25 of 132

Title of Meeting
Trust Board
Date of Meeting
May 31st 2017
Report Title
2016 Picker Inpatient Survey Report
Author
Neal Cleaver, Deputy Director of Nursing and Quality
Responsible Executive
Nicky Lucey, Director of Nursing and Quality
Purpose of Report (e.g. for decision, information) To provide a summary of the Picker Inpatient 2016 survey results. The complete report is attached as an appendix for information.
Summary In comparison to the 2015 Inpatient Survey results , the trust was significantly better on 2 questions and worse on 0 questions:
The Trust has improved significantly on the following questions:
2015 2016
Doctors: did not always have confidence and trust 19 % 14 %
Nurses: talked in front of patients as if they weren't there 20 % 14 %
In comparison to other trusts within the 2016 Inpatient survey, the Trust was significantly better on 19 questions, and worse on 3 questions; therefore the key areas for improvement are:
DCH results were significantly worse than the ‘Picker average’ for the following questions:
Trust Average
Hospital: patients using bath or shower area who shared it with opposite sex 26 % 12 %
Hospital: not always able to take own medication when needed to 40 % 34 %
Surgery: not told how to expect to feel after operation or procedure 46 % 40 %
Paper Previously Reviewed By This paper has been reviewed by the previous Learning From Patients Committee.
Strategic Impact This information will be public and may determine where patients prefer to be treated.
Risk Evaluation 1. Patients care and recovery may be compromised if staff are not communicating what
to expect to them following procedures/operations.
Inpa
tient
Sur
vey
Page 26 of 132
2. Patients care and recovery may be compromised if they are unable to take their own medication when needed.
Impact on Care Quality Commission Registration and/or Clinical Quality This information will be used by the Care Quality Commission to review the quality of care at the Trust.
Governance Implications (legal, clinical, equality and diversity or other): Inability to achieve progress or sustain set standards could lead to a negative reputational impact and inability to improve patient safety, effectiveness and experience. The report highlights that patients perceive that they share bathroom/shower room accommodation with patients of the opposite sex.
Financial Implications Undetermined, but could incur penalty if unable to achieve agreed standards/targets.
Freedom of Information Implications – can the report be published?
Yes
Recommendations a) To note the report; b) To review the findings
Inpa
tient
Sur
vey
Page 27 of 132

1
Title of Meeting
Trust Board
Date of Meeting
31st May 2017
Report Title
Inpatient Survey 2016 Summary Paper (Full Survey as Appendix)
Author
Becky Protopsaltis, Head of Public and Patient Experience Nicola Lucey, Director of Nursing and Quality Neal Cleaver, Deputy Director of Nursing and Quality
INTRODUCTION
1. Introduction:
This document summarises the findings from the Inpatient Survey 2016, carried out by
Picker Institute Europe, on behalf of Dorset County Hospital NHS Foundation Trust.
The Picker Institute was commissioned by 83 trusts to undertake the Inpatient Survey
2016. A total of 1250 patients from our Trust were sent a questionnaire. 1207 patients
were eligible for the survey, of which 622 returned a completed questionnaire, giving a
response rate of 52%.
2. Have we improved our results since the 2015 survey?
A total of 63 questions were used in both the 2015 and 2016
surveys.
Compared to the 2015 survey, DCH is:
Significantly BETTER on 2 questions
Significantly WORSE on 0 questions
The scores show no significant difference on 61 questions
Inpa
tient
Sur
vey
Page 28 of 132

2
The Trust has improved significantly on the following questions:
2015 2016
Doctors: did not always have confidence and trust 19 % 14 %
Nurses: talked in front of patients as if they weren't there 20 % 14 %
3. How do we compare with other Trusts?
The survey showed that your Trust is:
Significantly BETTER than average on 19 questions
Significantly WORSE than average on 3 questions
The scores were average on 45 questions
Inpa
tient
Sur
vey
Page 29 of 132
3
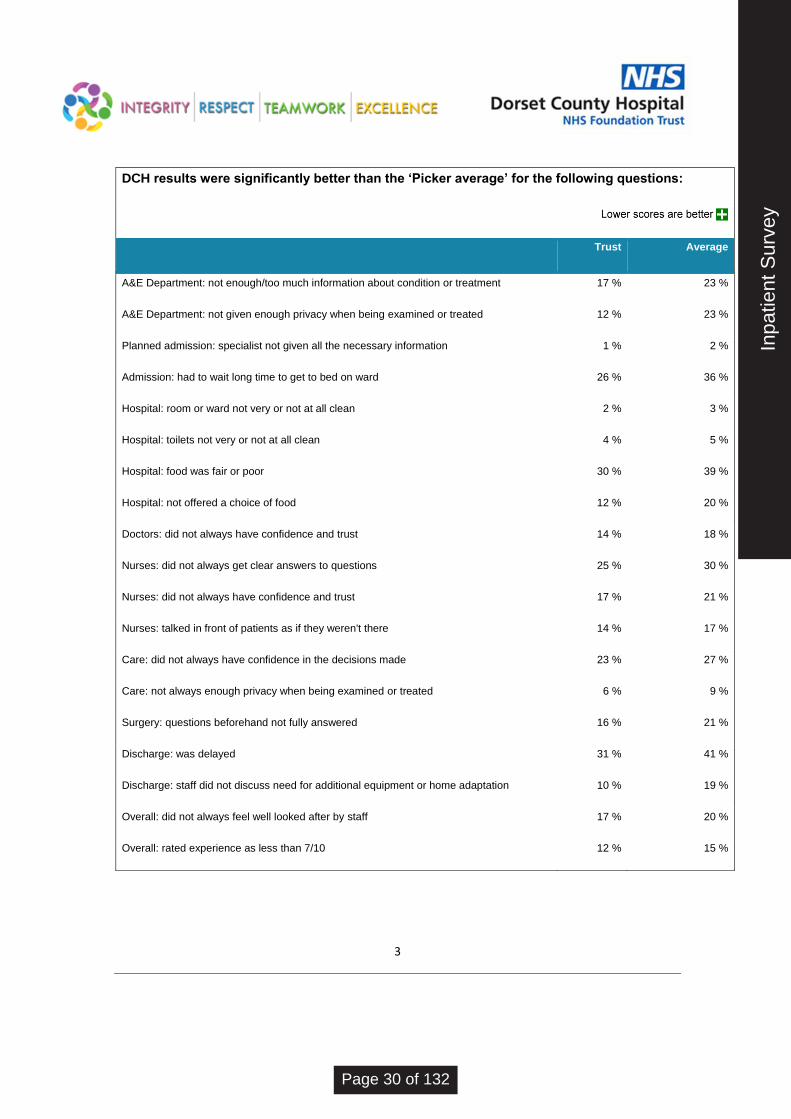
DCH results were significantly better than the ‘Picker average’ for the following questions:
Trust Average
A&E Department: not enough/too much information about condition or treatment 17 % 23 %
A&E Department: not given enough privacy when being examined or treated 12 % 23 %
Planned admission: specialist not given all the necessary information 1 % 2 %
Admission: had to wait long time to get to bed on ward 26 % 36 %
Hospital: room or ward not very or not at all clean 2 % 3 %
Hospital: toilets not very or not at all clean 4 % 5 %
Hospital: food was fair or poor 30 % 39 %
Hospital: not offered a choice of food 12 % 20 %
Doctors: did not always have confidence and trust 14 % 18 %
Nurses: did not always get clear answers to questions 25 % 30 %
Nurses: did not always have confidence and trust 17 % 21 %
Nurses: talked in front of patients as if they weren't there 14 % 17 %
Care: did not always have confidence in the decisions made 23 % 27 %
Care: not always enough privacy when being examined or treated 6 % 9 %
Surgery: questions beforehand not fully answered 16 % 21 %
Discharge: was delayed 31 % 41 %
Discharge: staff did not discuss need for additional equipment or home adaptation 10 % 19 %
Overall: did not always feel well looked after by staff 17 % 20 %
Overall: rated experience as less than 7/10 12 % 15 %
Inpa
tient
Sur
vey
Page 30 of 132
4
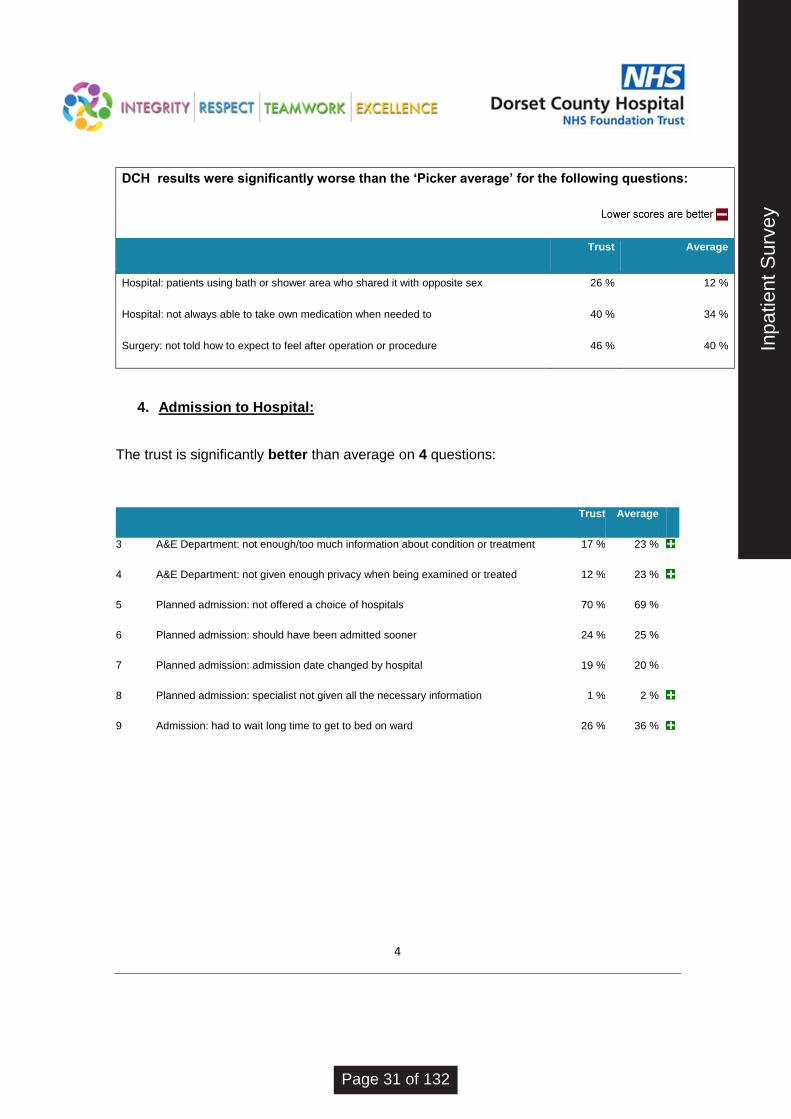
DCH results were significantly worse than the ‘Picker average’ for the following questions:
Trust Average
Hospital: patients using bath or shower area who shared it with opposite sex 26 % 12 %
Hospital: not always able to take own medication when needed to 40 % 34 %
Surgery: not told how to expect to feel after operation or procedure 46 % 40 %
4. Admission to Hospital:
The trust is significantly better than average on 4 questions:
Trust Average
3 A&E Department: not enough/too much information about condition or treatment 17 % 23 %
4 A&E Department: not given enough privacy when being examined or treated 12 % 23 %
5 Planned admission: not offered a choice of hospitals 70 % 69 %
6 Planned admission: should have been admitted sooner 24 % 25 %
7 Planned admission: admission date changed by hospital 19 % 20 %
8 Planned admission: specialist not given all the necessary information 1 % 2 %
9 Admission: had to wait long time to get to bed on ward 26 % 36 %
Inpa
tient
Sur
vey
Page 31 of 132

5
There is no significant difference historically:
2011 2012 2013 2014 2015 2016
3 A&E Department: not enough/too much information about
condition or treatment 15 % 21 % 18 % 14 % 19 % 17 %
4 A&E Department: not given enough privacy when being
examined or treated 22 % 19 % 16 % 12 % 14 % 12 %
5 Planned admission: not offered a choice of hospitals 70 % 70 % 72 % 66 % 65 % 70 %
6 Planned admission: should have been admitted sooner 23 % 27 % 19 % 24 % 21 % 24 %
7 Planned admission: admission date changed by hospital 21 % 27 % 26 % 25 % 22 % 19 %
8 Planned admission: specialist not given all the necessary
information - - 2 % 3 % 3 % 1 %
9 Admission: had to wait long time to get to bed on ward 27 % 33 % 34 % 23 % 24 % 26 %
Inpa
tient
Sur
vey
Page 32 of 132

6
5. The Hospital and Ward:
The trust is significantly better than average on 4 questions and worse on 2 questions:
Trust Average
11a Hospital: shared sleeping area with opposite sex 7 % 7 %
13a Hospital: patients in more than one ward, sharing sleeping area with opposite sex 4 % 5 %
14+ Hospital: patients using bath or shower area who shared it with opposite sex 26 % 12 %
15 Hospital: bothered by noise at night from other patients 42 % 39 %
16 Hospital: bothered by noise at night from staff 19 % 20 %
17 Hospital: room or ward not very or not at all clean 2 % 3 %
18+ Hospital: toilets not very or not at all clean 4 % 5 %
19 Hospital: felt threatened by other patients or visitors 3 % 3 %
20+ Hospital: did not always get enough help from staff to wash or keep clean 26 % 29 %
21+ Hospital: not always able to take own medication when needed to 40 % 34 %
22+ Hospital: food was fair or poor 30 % 39 %
23 Hospital: not offered a choice of food 12 % 20 %
24+ Hospital: did not always get enough help from staff to eat meals 29 % 36 %
Inpa
tient
Sur
vey
Page 33 of 132

7
There is no significant difference historically:
2011 2012 2013 2014 2015 2016
11a Hospital: shared sleeping area with opposite sex 8 % 5 % 7 % 6 % 10 % 7 %
13a Hospital: patients in more than one ward, sharing sleeping
area with opposite sex 7 % 3 % 3 % 5 % 5 % 4 %
14+ Hospital: patients using bath or shower area who shared it
with opposite sex 30 % 26 % 21 % 20 % 26 % 26 %
15 Hospital: bothered by noise at night from other patients 39 % 45 % 45 % 38 % 44 % 42 %
16 Hospital: bothered by noise at night from staff 19 % 24 % 19 % 19 % 21 % 19 %
17 Hospital: room or ward not very or not at all clean 1 % 2 % 1 % 1 % 1 % 2 %
18+ Hospital: toilets not very or not at all clean 3 % 4 % 3 % 2 % 4 % 4 %
19 Hospital: felt threatened by other patients or visitors 2 % 2 % 2 % 2 % 3 % 3 %
22+ Hospital: food was fair or poor 30 % 30 % 30 % 29 % 28 % 30 %
23 Hospital: not offered a choice of food 10 % 10 % 14 % 17 % 13 % 12 %
24+ Hospital: did not always get enough help from staff to eat
meals 26 % 41 % 40 % 20 % 36 % 29 %
6. Doctors:
The trust is significantly better than average on 1 question and worse on 0 questions:
Trust Average
25+ Doctors: did not always get clear answers to questions 30 % 30 %
26 Doctors: did not always have confidence and trust 14 % 18 %
27 Doctors: talked in front of patients as if they were not there 19 % 22 %
Inpa
tient
Sur
vey
Page 34 of 132

8
There is significant improvement historically in 1 question:
2011 2012 2013 2014 2015 2016
25+ Doctors: did not always get clear answers to questions 31 % 31 % 30 % 28 % 30 % 30 %
26 Doctors: did not always have confidence and trust 16 % 21 % 20 % 16 % 19 % 14 %
27 Doctors: talked in front of patients as if they were not
there 23 % 27 % 27 % 22 % 23 % 19 %
7. Nurses:
The trust is significantly better than average on 3 questions and worse on 0 questions:
Trust Average
28+ Nurses: did not always get clear answers to questions 25 % 30 %
29 Nurses: did not always have confidence and trust 17 % 21 %
30 Nurses: talked in front of patients as if they weren't there 14 % 17 %
31 Nurses: sometimes, rarely or never enough on duty 41 % 40 %
32 Nurses: did not always know which nurse was in charge of care 51 % 51 %
There is significant improvement historically in 1 question:
2011 2012 2013 2014 2015 2016
28+ Nurses: did not always get clear answers to questions 26 % 26 % 24 % 22 % 27 % 25 %
29 Nurses: did not always have confidence and trust 24 % 23 % 20 % 17 % 20 % 17 %
30 Nurses: talked in front of patients as if they weren't there 18 % 18 % 15 % 15 % 20 % 14 %
31 Nurses: sometimes, rarely or never enough on duty 36 % 43 % 46 % 34 % 39 % 41 %
Inpa
tient
Sur
vey
Page 35 of 132
9
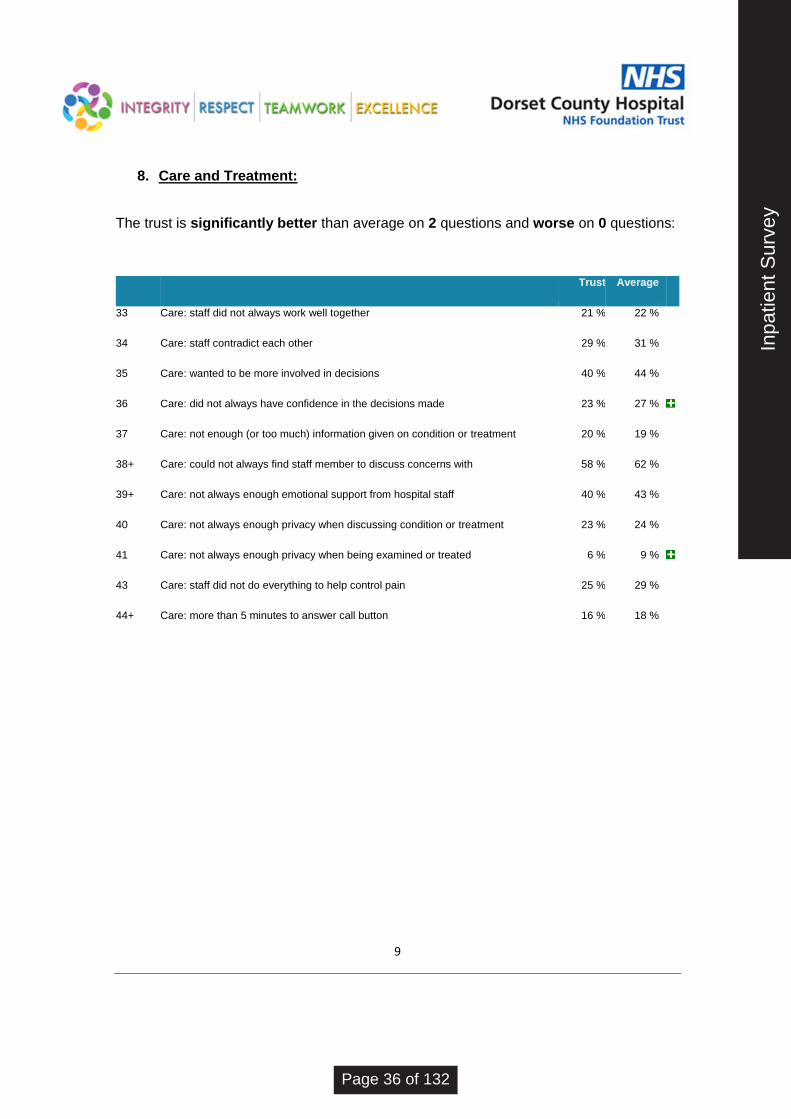
8. Care and Treatment:
The trust is significantly better than average on 2 questions and worse on 0 questions:
Trust Average
33 Care: staff did not always work well together 21 % 22 %
34 Care: staff contradict each other 29 % 31 %
35 Care: wanted to be more involved in decisions 40 % 44 %
36 Care: did not always have confidence in the decisions made 23 % 27 %
37 Care: not enough (or too much) information given on condition or treatment 20 % 19 %
38+ Care: could not always find staff member to discuss concerns with 58 % 62 %
39+ Care: not always enough emotional support from hospital staff 40 % 43 %
40 Care: not always enough privacy when discussing condition or treatment 23 % 24 %
41 Care: not always enough privacy when being examined or treated 6 % 9 %
43 Care: staff did not do everything to help control pain 25 % 29 %
44+ Care: more than 5 minutes to answer call button 16 % 18 %
Inpa
tient
Sur
vey
Page 36 of 132

10
There is no significant difference historically:
2011 2012 2013 2014 2015 2016
33 Care: staff did not always work well together - - - - 22 % 21 %
34 Care: staff contradict each other 31 % 32 % 31 % 26 % 32 % 29 %
35 Care: wanted to be more involved in decisions 42 % 46 % 42 % 41 % 39 % 40 %
36 Care: did not always have confidence in the decisions
made - - - 24 % 26 % 23 %
37 Care: not enough (or too much) information given on
condition or treatment 20 % 22 % 19 % 18 % 20 % 20 %
38+ Care: could not always find staff member to discuss
concerns with 55 % 63 % 64 % 59 % 61 % 58 %
39+ Care: not always enough emotional support from hospital
staff 39 % 47 % 40 % 31 % 38 % 40 %
40 Care: not always enough privacy when discussing
condition or treatment 28 % 28 % 25 % 21 % 23 % 23 %
41 Care: not always enough privacy when being examined or
treated 8 % 11 % 8 % 6 % 7 % 6 %
43 Care: staff did not do everything to help control pain 29 % 28 % 23 % 19 % 27 % 25 %
44+ Care: more than 5 minutes to answer call button 14 % 21 % 19 % 14 % 17 % 16 %
Inpa
tient
Sur
vey
Page 37 of 132

11
9. Operations and Procedures:
The trust is significantly better than average on 1 question and worse on 1 question:
Trust Average
46+ Surgery: risks and benefits not fully explained 15 % 17 %
47+ Surgery: what would be done during operation not fully explained 26 % 23 %
48+ Surgery: questions beforehand not fully answered 16 % 21 %
49 Surgery: not told how to expect to feel after operation or procedure 46 % 40 %
51 Surgery: anaesthetist / other member of staff did not fully explain how would put to
sleep or control pain 13 % 14 %
52 Surgery: results not explained in clear way 31 % 30 %
There is no significant difference historically:
2011 2012 2013 2014 2015 2016
46+ Surgery: risks and benefits not fully explained 13 % 20 % 13 % 20 % 17 % 15 %
47+ Surgery: what would be done during operation not fully
explained 23 % 28 % 23 % 28 % 27 % 26 %
48+ Surgery: questions beforehand not fully answered 20 % 26 % 20 % 21 % 21 % 16 %
49 Surgery: not told how to expect to feel after operation or
procedure 47 % 46 % 43 % 43 % 44 % 46 %
51 Surgery: anaesthetist / other member of staff did not fully
explain how would put to sleep or control pain 13 % 14 % 12 % 14 % 14 % 13 %
52 Surgery: results not explained in clear way 38 % 35 % 30 % 32 % 35 % 31 %
Inpa
tient
Sur
vey
Page 38 of 132

12
10. Leaving Hospital:
The trust is significantly better than average on 2 questions and worse on 0 questions:
Trust Average
53+ Discharge: did not feel involved in decisions about discharge from hospital 45 % 45 %
54 Discharge: not given notice about when discharge would be 44 % 44 %
55 Discharge: was delayed 31 % 41 %
57 Discharge: delayed by 1 hour or more 80 % 85 %
59+ Discharge: did always get enough support from health or social care professionals. 46 % 46 %
60+ Discharge: did not always know what would happen next with care after leaving
hospital 48 % 48 %
61 Discharge: not given any written/printed information about what they should or
should not do after leaving hospital 37 % 36 %
62+ Discharge: not fully told purpose of medications 25 % 25 %
63+ Discharge: not fully told side-effects of medications 64 % 61 %
64+ Discharge: not told how to take medication clearly 23 % 24 %
65+ Discharge: not given completely clear written/printed information about medicines 26 % 28 %
66+ Discharge: not fully told of danger signals to look for 55 % 57 %
67+ Discharge: family or home situation not considered 34 % 37 %
68+ Discharge: family not given enough information to help 49 % 53 %
69 Discharge: not told who to contact if worried 18 % 20 %
70+ Discharge: staff did not discuss need for additional equipment or home adaptation 10 % 19 %
71+ Discharge: staff did not discuss need for further health or social care services 15 % 18 %
Inpa
tient
Sur
vey
Page 39 of 132

13
There is no significant difference historically:
2011 2012 2013 2014 2015 2016
53+ Discharge: did not feel involved in decisions about
discharge from hospital 39 % 49 % 44 % 45 % 43 % 45 %
54 Discharge: not given notice about when discharge would
be - 44 % 42 % 43 % 43 % 44 %
55 Discharge: was delayed 31 % 40 % 35 % 44 % 34 % 31 %
57 Discharge: delayed by 1 hour or more 81 % 84 % 76 % 83 % 79 % 80 %
59+ Discharge: did always get enough support from health or
social care professionals. - - - - 41 % 46 %
61 Discharge: not given any written/printed information about
what they should or should not do after leaving hospital 35 % 35 % 23 % 33 % 36 % 37 %
62+ Discharge: not fully told purpose of medications 25 % 26 % 23 % 23 % 25 % 25 %
63+ Discharge: not fully told side-effects of medications 58 % 64 % 62 % 58 % 62 % 64 %
64+ Discharge: not told how to take medication clearly 24 % 22 % 21 % 24 % 24 % 23 %
65+ Discharge: not given completely clear written/printed
information about medicines 28 % 26 % 20 % 23 % 26 % 26 %
66+ Discharge: not fully told of danger signals to look for 55 % 61 % 52 % 51 % 57 % 55 %
67+ Discharge: family or home situation not considered - 36 % 34 % 28 % 34 % 34 %
68+ Discharge: family not given enough information to help 55 % 57 % 41 % 45 % 54 % 49 %
69 Discharge: not told who to contact if worried 21 % 21 % 14 % 17 % 20 % 18 %
70+ Discharge: staff did not discuss need for additional
equipment or home adaptation - 21 % 9 % 17 % 15 % 10 %
71+ Discharge: staff did not discuss need for further health or
social care services - 17 % 9 % 14 % 18 % 15 %
Inpa
tient
Sur
vey
Page 40 of 132

14
11. Overall:
The trust is significantly better than average on 2 questions and worse on 0 questions:
Trust Average
72 Overall: not treated with respect or dignity 14 % 16 %
73 Overall: did not always feel well looked after by staff 17 % 20 %
74+ Overall: rated experience as less than 7/10 12 % 15 %
75 Overall: not asked to give views on quality of care 72 % 70 %
76 Overall: did not receive any information explaining how to complain 60 % 60 %
There is no significant difference historically:
2011 2012 2013 2014 2015 2016
72 Overall: not treated with respect or dignity 17 % 21 % 17 % 14 % 15 % 14 %
73 Overall: did not always feel well looked after by staff - - - 17 % 18 % 17 %
74+ Overall: rated experience as less than 7/10 - 19 % 15 % 11 % 13 % 12 %
75 Overall: not asked to give views on quality of care 85 % 83 % 73 % 68 % 75 % 72 %
76 Overall: did not receive any information explaining how to
complain - 65 % 59 % 58 % 62 % 60 %
12. Recommendations:
To note the findings of the report
Analysis of patients comments is taking place, and divisional action plans are in
development
To delegate monitoring of the action plan to the newly formed Patient Experience
Group (which will report to the Quality Committee).
Inpa
tient
Sur
vey
Page 41 of 132
Title of Meeting
Trust Board
Date of Meeting
31 May 2017
Report Title
Mission and Vision Statements Review
Author
Susie Palmer
Responsible Executive
Nick Johnson
Purpose of Report (e.g. for decision, information) For decision
Summary The Trust Strategy mission and vision statements were reviewed at a Board development session. The output from that session was tested with staff at a focus group and the feedback incorporated into the suggestions outlined here.
Paper Previously Reviewed By N/A
Strategic Impact The mission and vision are an integral part of the strategy
Risk Evaluation Risk to delivery of our strategic aims if we don’t have agreed vision and mission statements to circulate
Impact on Care Quality Commission Registration and/or Clinical Quality The implementation of the strategy is key to delivery of high quality, sustainable care to our patients
Governance Implications (legal, clinical, equality and diversity or other): None
Financial Implications None
Freedom of Information Implications – can the report be published?
Yes
Recommendations
a) The Board agrees the proposed mission and vision statements b) c)
Tru
st V
isio
n up
date
Page 42 of 132

Trust Strategy Mission and Vision Statements Review
Introduction
The Board reviewed the Trust’s current purpose, vision and mission statements at the April
2017 development session to ensure that they were still relevant and written in a way which
could be communicated simply and effectively to staff at all levels of the organisation and
beyond.
The Board felt that it was time to move on from the current ‘purpose’ of ‘delivering
compassionate, safe and effective healthcare’ and refine the ‘mission and ‘vision’
statements:
Mission: Playing a leading role, in collaboration with our partners, in the development of an
integrated, patient-centred health and care system.
Vision: Providing and enabling outstanding care for our patients and communities in ways
which matter to them.
Board Development Session Outcome
Following group discussions several mission and vision statement options were proposed:
Mission:
Outstanding care for people in ways which matter to them.
The outstanding DGH at the heart of serving the people of central Dorset.
Our outstanding hospital at the heart of the health and care system, improving the
health of people in Dorset.
Vision:
Our hospital, working with our health and social care partners, will be at the heart of
improving the health and wellbeing of our communities.
Dorset County Hospital is now and will be at the heart of a health and care system
providing outstanding care to people in ways which matter to them.
Dorset County Hospital, working with our health and social care partners to improve
the health and wellbeing of our communities.
Tru
st V
isio
n up
date
Page 43 of 132

These ideas were then refined to present to staff during a focus group to gauge reaction to
specific wording and concepts.
Staff Focus Group Feedback
We ran a focus group of several staff from different areas of the hospital, which included
representatives from clinical and support teams.
Attendees were given some background on the strategy as well as information about what
we mean by a ‘mission’ and ‘vision’ and the key concepts we are trying to get across.
Attendees were also taken through the strategic objectives to check they made sense to
them:
Strategic Objectives
Feedback was positive - the group felt the wording was clear and concise, and the short
explanation under each title was sufficient to explain what each meant.
Mission and Vision
The following options were shared with staff to test how they felt about specific wording:
Mission:
1. Outstanding care for our patients in ways which matter to them
2. Outstanding care for people in ways which matter to them
3. An outstanding district general hospital at the heart of our communities
Vision:
1. Working with our health and social care partners to improve the wellbeing of our
communities – living our values every day.
Tru
st V
isio
n up
date
Page 44 of 132

2. Our hospital, working with our health and social care partners, will be at the heart of
improving the wellbeing of our communities.
3. Dorset County Hospital will be a key partner in developing a joined-up, patient-
centred health and care system for Dorset.
The group initially favoured Option 1 for the mission statement but after discussion decided
that Option 2 was more appropriate as ‘people’ was a better word as it reflected how we care
for the whole person rather than labelling people as patients. It also reflects that we care for
families and carers as well as the patient themselves.
The group also liked the use of the word ‘outstanding’ as it reflects what we are striving to
achieve.
Some members of the group liked Option 3 but it was felt that not everyone understood what
was meant by a ‘district general hospital’.
There was much discussion around the wording used in the vision options. The group
favoured the use of the words ‘communities’, ‘heart’, ‘partners’ and ‘wellbeing’ as they felt
this reflected our aims. There was also a preference for using the hospital’s name in full.
A line about the Trust values was added to one option to gauge opinion about how we tie in
the values with the strategy. Although the group recognised the values were an integral part
of how the Trust expects staff to behave, they didn’t feel they needed to be specifically
mentioned in the statements. There was positive feedback about how well the values were
being embedded within the organisation, and externally – staff commented that candidates
for vacancies were using them to illustrate why they were suitable for posts.
Recommendation
Based on the feedback received from staff the following options for the mission and vision
statements are proposed for agreement:
Mission: Outstanding care for people in ways which matter to them.
Vision: Dorset County Hospital, working with our health and social care partners, will
be at the heart of improving the wellbeing of our communities.
Next Steps
The Trust Strategy will be launched in the first week of July 2017 with a programme of
activity following to inform staff, governors, members, general public and stakeholders.
Activity will include but is not limited to:
Distribution of supporting materials, including a booklet, leaflet, credit card and poster
Team Brief presentation
Tru
st V
isio
n up
date
Page 45 of 132

Programme of visits to key departmental staff meetings
Open staff sessions
Restaurant information stand
Dedicated StaffNet page
Screensaver
CEO Brief messages
Social media
Council of Governors meeting presentation
Membership newsletter article
Presentation at AGM/AMM
Dedicated public website page
Annual Review section
Open Day stand/presentation
News release
Message to GPs
Tru
st V
isio
n up
date
Page 46 of 132

Title of Meeting
Trust Board
Date of Meeting
31 May 2017
Report Title
Strategy Update Report
Author
Nick Johnson
Responsible Executive
Nick Johnson
Purpose of Report (e.g. for decision, information) For information
Summary This purpose of this report is to provide Board with an update on strategy implementation and activity and enable the Board to monitor progress towards its agreed strategic objectives. It will also ensure Board has regular sight of the core strategy and prompt issues for debate and discussion (either immediately or at a later date). It is intended that the SUR is presented to Board on a quarterly basis. It is expected that the form and content of the SUR will evolve as Board requires.
Paper Previously Reviewed By EMT
Strategic Impact This report will help monitor implementation of the Trust Strategy.
Risk Evaluation Strategic risks will be identified as a result of discussions around this report and will inform BAF updates.
Impact on Care Quality Commission Registration and/or Clinical Quality None arising as a result of this report
Governance Implications (legal, clinical, equality and diversity or other): None arising as a result of this report.
Financial Implications None arising as a result of this report.
Freedom of Information Implications – can the report be published?
Yes.
Recommendations It is recommended that Board:
Note and discuss the Strategy Update Report content and design
Str
ateg
y -
Boa
rd o
vers
ight
Page 47 of 132
1 | P a g e
DCH Strategy Update Report
For 31st May 2017 Trust Board
Outstanding Care for people in ways which matter to them
Board Quarterly May17, September 17, January 18, March 18 (part of 18/19 review)
Execs Bi-monthly Focus on corporate priorities progress June, August, October, December, February
SMT Bi-monthly Focus on strategic programmes progress June, August, October, December, February
Str
ateg
y -
Boa
rd o
vers
ight
Page 48 of 132

2 | P a g e
6
OutstandingDelivering
outstanding services everyday
IntegratedJoining up our
services
Collaborative Working with our
patients and partners
EnablingEmpowering our
staff
SustainableProductive,
effective and efficient
New care modelsDevelop a sustainable service and financial model for all our services
Strategic Objectives 17/18 Corporate Priorities
System integrationEnsure a clear STP and ACS delivery
plan and drive forward the mid-Dorset hub
VanguardImplement key Vanguard
workstreams – Pathology, Business Support Services , Health Informatics
and Stroke
Commercial developmentDevelop and implement key
commercial ventures – Private Patients, Damers, Pharmacy
Better Information Deliver our Information Strategy
Front-line leadershipDevelop and embed the new Divisional leadership model
- Rated Outstanding- Meeting our
performance targets
- Reduced ED admissions and
hospital bed days per 100,000 population
97+% Friends and Family
Top quartile staff engagement
1% Operating surplus
Strategic Measures
Strategic Service Transformation
Programme
Strategic Programmes
Governance Framework and New Divisional
Structure
Digital Patient Record
Accountable Care System
One Acute Network of services
Acute Care Collaborative Vanguard
Damers Joint Venture
Dorset Care Record
Business Support Services and Health
Informatics
Syste
mO
rganisa
tional
Demand Management
Mid-Dorset Hub
Str
ateg
y -
Boa
rd o
vers
ight
Page 49 of 132

3 | P a g e
1. Summary
System working continues at pace. The One Acute Network Programme is being established and DCH must ensure the right engagement
and involvement given the majority of the programme will be focussed on any changes in acute provision in east Dorset as a result of the
CSR.
The Trust continues to make progress in delivering key strategic programmes which contribute towards the achievement of our strategic
objectives.
The key issue for the Trust is the ability to deliver all of the key programmes – system wide and internally – at the pace required in order to
impact demand, financial and workforce pressures in the timeframes required.
National
The result of the general election is awaited which may bring a new Health Secretary. The timing of the general election has upset
assumptions that there may have been some extra funding for the NHS in 2018 to mark the NHS’ 70th Birthday.
The purdah period arising due to the general election has limited recent national activity, however, the recent release of the Five Year
Forward View Next Steps document on 31st March which was designed to set clear priorities around urgent and emergency care, primary
care, mental health, and efficiency (briefing at appendix 1).
The Naylor Review of NHS Property and Estates was published on 31st March setting our recommendations for better management of
property and estates. The Trust is reviewing the document to ensure its plans – in particular around Damers site – align to the Naylor
review recommendations where applicable (e.g. a drive to use land for key worker housing). (briefing at appendix 2)
System-wide & Sustainability and Transformation Partnership
An expression of interest was submitted to NHS England by the Dorset SLT to be considered a wave one STP/Accountable Care System.
A Programme Director has been appointed by Poole Hospital and RBCH for the One Acute Network Programme. Discussions are taking
place between DCH, Poole and RBCH over the Terms of Reference for the One Acute Network Programme Board.
A high-level Business Case was submitted to NHSE/I for capital funding for acute reconfiguration in the east.
Str
ateg
y -
Boa
rd o
vers
ight
Page 50 of 132

4 | P a g e
DCH staff have been working closely with system partners on developing an Accountable Care System programme and delivering key
ACC Vanguard workstreams on pathology, stroke, Health informatics and business support services.
DCH
The new divisional structure, performance framework and governance structure have been implemented and are now being embedded.
The development of an internal Transformation Programme following the Strategic Service Review has not yet been finalised as a result of
competing system wide-priorities.
The procurement for the Strategic Estates Partner for the Damers site development and wider site master planning is currently on
programme and due to be completed in June.
Key commercial strategy milestones/achievements with signing of Costa lease, agreement with NHS England to set up the Pharmacy
Sub-Co and DCH Pharmacy being awarded the Dorset Healthcare Pharmacy contract.
A Staff Focus Group was held in May to test the Mission and Vision (separate report forthcoming).
Str
ateg
y -
Boa
rd o
vers
ight
Page 51 of 132
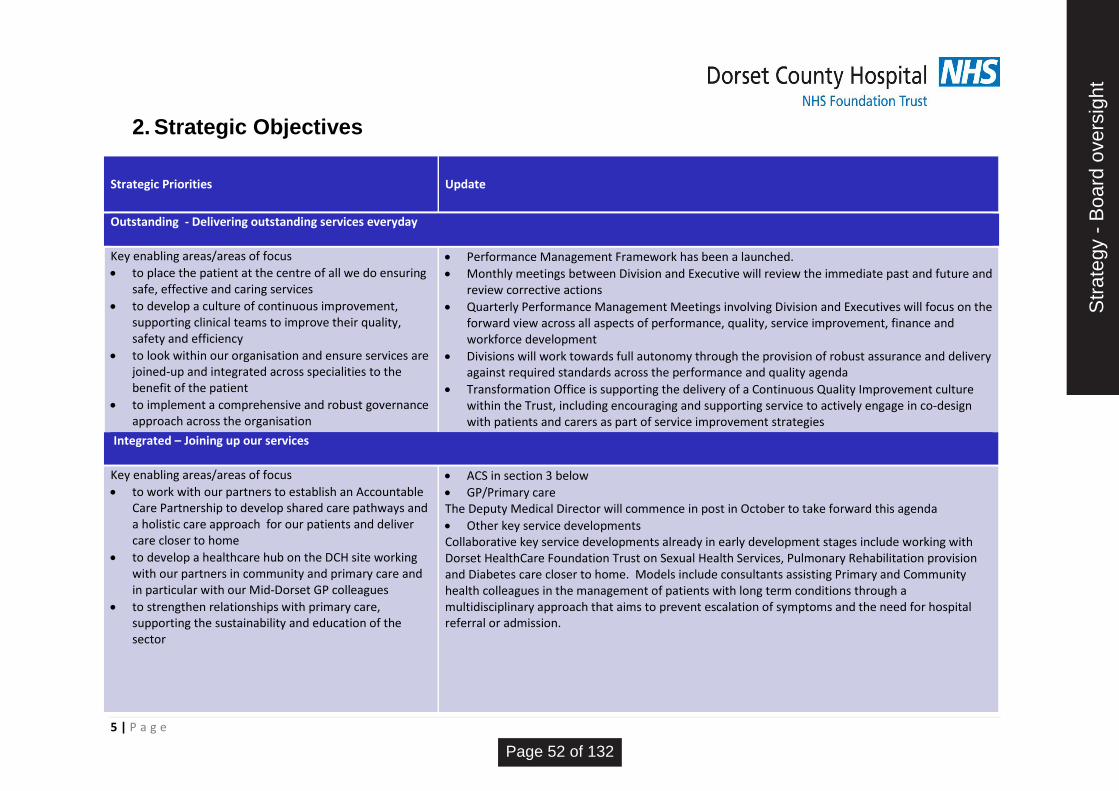
5 | P a g e
2. Strategic Objectives
Strategic Priorities Update
Outstanding - Delivering outstanding services everyday
Key enabling areas/areas of focus
to place the patient at the centre of all we do ensuring safe, effective and caring services
to develop a culture of continuous improvement, supporting clinical teams to improve their quality, safety and efficiency
to look within our organisation and ensure services are joined-up and integrated across specialities to the benefit of the patient
to implement a comprehensive and robust governance approach across the organisation
Performance Management Framework has been a launched.
Monthly meetings between Division and Executive will review the immediate past and future and review corrective actions
Quarterly Performance Management Meetings involving Division and Executives will focus on the forward view across all aspects of performance, quality, service improvement, finance and workforce development
Divisions will work towards full autonomy through the provision of robust assurance and delivery against required standards across the performance and quality agenda
Transformation Office is supporting the delivery of a Continuous Quality Improvement culture within the Trust, including encouraging and supporting service to actively engage in co-design with patients and carers as part of service improvement strategies
Integrated – Joining up our services
Key enabling areas/areas of focus
to work with our partners to establish an Accountable Care Partnership to develop shared care pathways and a holistic care approach for our patients and deliver care closer to home
to develop a healthcare hub on the DCH site working with our partners in community and primary care and in particular with our Mid-Dorset GP colleagues
to strengthen relationships with primary care, supporting the sustainability and education of the sector
ACS in section 3 below
GP/Primary care The Deputy Medical Director will commence in post in October to take forward this agenda
Other key service developments Collaborative key service developments already in early development stages include working with Dorset HealthCare Foundation Trust on Sexual Health Services, Pulmonary Rehabilitation provision and Diabetes care closer to home. Models include consultants assisting Primary and Community health colleagues in the management of patients with long term conditions through a multidisciplinary approach that aims to prevent escalation of symptoms and the need for hospital referral or admission.
Str
ateg
y -
Boa
rd o
vers
ight
Page 52 of 132

6 | P a g e
Collaborative – Working with our patients and partners
Key enabling areas/areas of focus
to work with our Acute Care Collaborative Vanguard partners to deliver outstanding services which reflect the needs of our local populations
to strengthen links between health and social care and mental health providers to provide joined-up services
to establish a comprehensive transformation programme for our services focussed on co-design and outcomes
One Acute Network & Vanguard progress – see section 3 below
Transformation Programme – see section 3 below
Enabling – Empowering our staff
Key enabling areas/areas of focus
to implement our ‘People Strategy 2015’ to develop the our ability to deliver safe, effective and compassionate care
to review our enabling and support services to ensure they support the delivery of our aims and objectives and meet the needs of our patients and staff
to ensure relevant data is easily accessible, in multiple locations using technology, and enabling a culture of evidence based decision making
to speed up the adoption of relevant research and innovation and define our role within science, education and training, and research and development, working with the AHSN.
to appreciate and further develop our social responsibility in the community
People Strategy update – implementation of 3 year plan continues on track. Values developed and re-launched, appraisal paperwork relaunched to include assessment against behaviours, induction re-viewed, phase one of Leadership Development Programme delivered, and second phase commencing June2017, Workforce planning governance reviewed and in place. Support Services
DCH is engaged in the system wide work exploring the potential to join-up support services across Dorset where appropriate. This covers, estates, procurement, finance, HR and Health Informatics (ICT).
DPR/DCR The Digital Patient Record is due to go live in June and will be rolled out to all staff by the end of June. Clinical and support staff have been involved in the design of the solution to ensure it enables staff in delivery of our aims and objectives including support for integrated care across care settings. As an ongoing development the solution will be responsive in enabling continuous improvement.
The Dorset Care Record Programme has selected a supplier. The programme is currently over budget. R&D and/or Innovation updates – none to report
Social/community engagement activity – none to report
Str
ateg
y -
Boa
rd o
vers
ight
Page 53 of 132

7 | P a g e
Sustainable – Productive, effective and efficient
Key enabling areas/areas of focus
to embed a culture of value management and deliver efficiency projects across the organisation, using the Carter principles as a foundation
to develop our commercial capacity and capability building commercial partnerships to help achieve this
to drive value from our assets, in particular our estates and property, and enhance the patient experience
A Finance Improvement Team is in place and working with the divisions to support them in delivering CIPs and developing a culture of value management. The Better Value Better Care Group is reviewing the Carter metrics to ensure efficiencies are maximised.
The commercial strategy is being implemented with a year one review due to take place shortly. The Costa commercial concession is due to open on 26th June. The Pharmacy Subsidiary Company will be established shortly and the Pharmacy Team recently won the DHC Pharmacy contract. Other commercial initiatives are in early planning phases.
We are currently undergoing a procurement dialogue process to identify a Strategic Estates Partner to take forward the development of the estate.
Str
ateg
y -
Boa
rd o
vers
ight
Page 54 of 132

8 | P a g e
3. Strategic programmes
Strategic Programme Update and progress since last report Key issues affecting delivery and resolution approach
Accountable Care System
Dorset was named as one of the 9 potential STPs which could apply to be a wave 1 ACS/ACO. A short Expression of Interest has been submitted to NHSE/I. Dorset County Hospital is working with partners in Primary, Community, Social and Urgent Care sectors to agree key steps towards creation of an Accountable Care System for West Dorset. Numerous programmes across the providers to integrate and simplify pathways will be launched in the first Quarter of 2017/18.
-An agreed definition/blueprint for a Dorset ACS has not yet been developed and delivery plan is not yet in place. -Consideration needs to be given to how the west/east split for any ACS is dealt with
One Acute Network of Services
Discussions with Poole and RBH regarding the Programme approach for delivery of the One Acute Network workstream are ongoing.
The major programme in the workstream will be re-configuration in the east. There is a risk that all the focus is on this reconfiguration rather than the wider goal of sustainable networks across Dorset.
Acute Care Collaborative Vanguard (a sub-programme of One Acute Network)
Agreement on the direction of travel for Business Support Services and Health Informatics is agreed. Pathology and Stroke workstreams are progressing
The evolution and sustainability of Vanguard after funding expires in 17/18? How the Vanguard programme will merge into One Acute Network Programme?
Demand Management – Right Referral, Right Care
9 specialties across 4 providers are involved in an iterative change program. The first Learning Week, testing assumptions or new pathways will be held in mid-May and this will inform the next iteration of the work-program. There are Learning Weeks planned for each Quarter in 2017/18.
Clinical capacity to engage with change program involving cross-county collaboration Understanding the current provision and pathways in place across multiple partners Weekly management and service improvement teleconferences in place to mitigate project slippage.
Mid-Dorset Hub
Dorset County Hospital is working with partners in Primary, Community,
and Social Care. 4 key workstreams have been identified to progress the
initial integrated working. There is senior clinician input from secondary
and primary care to each group and a dashboard will be developed to
monitor outcomes.
Identification of resource savings across the health
economy linked to the hub development proves a
challenge. The workstreams are anticipated to reduce
activity across the system but are not isolated from other
initiatives complicating the ability to measure impact.
Expanding the hub and establishing a permanent base
Str
ateg
y -
Boa
rd o
vers
ight
Page 55 of 132

9 | P a g e
within DCH and as close to ED as possible.
Service Transformation Programme
Transformation office is now fully staffed. Two members have been released to take part in the training program for Quality Service Improvement and Redesign run by NHS Improvements. Once qualified in September and as associate members of the QSIR College they will be able to deliver the program locally and grow quality service improvement knowledge and engagement within the Trust. Colleagues at the CCG and Dorset HealthCare Trusts have expressed an interest in taking part in this program alongside DCH personnel.
A methodology for accessing Transformation Office support at the appropriate level to be signed off in Quarter 1 Program content for 2017/18 Patient Flow Transformation to be agreed, this program needs to compliment the external agenda supporting the development of the Integrated Primary and Community Care Services and Accountable Care System programs with the STP partners.
Damers Joint Venture
The Damers Joint Venture procurement is progressing well and on schedule. Subject to approvals a JV partner is due to be selected in June and a site masterplan will be finalised in the autumn.
Procurement challenge risk is thought to be low but always possible. Wider system interest may have an impact but is being managed.
Str
ateg
y -
Boa
rd o
vers
ight
Page 56 of 132

10 | P a g e
4. Strategic measures
Strategic measure Narrative Update Baseline (April 2017) Current
2020/21 Target
Exec Lead Source
Rated outstanding by the Care Quality Commission
CQC action plan to address gaps in assurance progressing well with significant assurance from Internal auditors on action plan Quality Committee priorities in work plan drafted for board approval, includes: - Mortality surveillance - Sepsis and the deteriorating patient - Board triangulation of quality assurance - Quality assessment of STP and new models - Governance embedding of new framework and ward to board exemplar for well-led.- Quality account/report priorities agreed with partners and all have plans in progress: - SAFE: Avoidable falls reduction/ mortality surveillance and reducing variation (Including End of Life care)/ Sepsis - CLINICAL EFFECTIVENSS: Electronic discharge/ promote health and wellbeing staff and patients/ Volunteers and social isolation improved support to improve outcomes - PATIENT EXPERIENCE: Dementia/ Timely and compassionate response to complaints/ Information for patients
Requires Improvement
Requires Improvement
Outstanding NL CQC report Quality Report
Meeting our key performance targets
ED Achieving Achieving
Achieving 4/4
JP IPR/BI team
RTT – improvement plans to be presented at Finance Performance Committee in June 2017.
Requires improvement
Requires improvement
Cancer, referral levels in March and April outstripped available capacity in addition to unplanned absences in key areas.
Achieving Requires improvement
Diagnostics – two areas only experiencing capacity constraints
Requires improvement
Requires improvement
Str
ateg
y -
Boa
rd o
vers
ight
Page 57 of 132

11 | P a g e
Reduced ED admissions per 100,000 population
Patient Flow Program (internal) and Better Care Program (external) initiatives in development to further improve non-elective flow through the system
ED Attendances 3,753 TBD TBD JP IPR/BI team Admissions via ED 1,240
Reduced number of hospital bed days per 1000,000
population
Patient Flow Program (internal) and Better Care Program (external) initiatives in development to further improve non-elective flow through the system
Bed Days (total excluding Regular Day Admissions) 12,297
TBD TBD JP BI Team
Bed Days (Non-elective Only) 9,190
Achieving a top quartile%* our friends and family test
*National benchmark
publication 1st June 2017
Inpatients: FFT well-embedded. Paediatrics trailing new
ways to engage children and young people in FFT
returns
CQUIN 95% 96%*
85%*
96%*
92%*
96% NL BI Team
Emergency department: Well-embedded and
performing well against set CQUIN based on national
benchmark
CQUIN 84%
Maternity: Not achieving and to be refreshed on the
engagement to complete returns
CQUIN 96%
Outpatient: Embedded and achieving CQUIN 92%
Top quartile for staff engagement
The People Strategy is the strategic programme to raise
levels of staff engagement. The delivery of the people
Strategy is on track, as described above, however the
overall staff engagement metric currently remains a the
national average for Acute Trusts. Annual action are
developed and managed centrally and within divisions.
3.80 3.80, compared
to national
average for
Acute Trusts of
3.81
Top quartile MW Workforce
report/HR
team
Financially sustainable; self-sufficient in cash terms with an operating surplus of 1%
The control total for 17/18 of a £2.9 million deficit will
not enable us to achieve this in the current financial
Forecast for
17/18 £2.9
£7.4 million
deficit 1% surplus LW Finance report/finance team
Str
ateg
y -
Boa
rd o
vers
ight
Page 58 of 132
12 | P a g e
without funding support year. A cash loan will be required this financial year. million deficit
Str
ateg
y -
Boa
rd o
vers
ight
Page 59 of 132

13 | P a g e
Appendix 1 – Dorset System and DCH Strategy programmes
Prevention at Scale
One Acute Network
Integrated Community
Services
Leading and Working
Differently
Digitally Enabled Dorset
toprovide
services to meet the
needs of local people and
deliver better outcomes
Accountable Care
Acute Hospital Re-
Configuration
Maternity and
Paediatrics with Yeovil
Community Hubs
Mid-Dorset Community
Hub
Clinical Services Review
Vanguard
STP Workstreams
Sustainability and Transformation Plan
System Implementation Programmes
Dorset Care Record
Mental HealthStrategy
Primary Care Strategy
Outstanding Care for our patients in ways which matter to
them
Outstanding
Collaborative
Integrated
Sustainable
Enabling
CIP
Digital Patient Record
Damers Road JV
Div Structure
Service T’mation
Governance
GP E’ment
People Strategy
Business Support Services
Right Care
Continuous Quality Improvement
DCH Strategy
Service T’mation
Service T’mation
STP VisionDCH
Strategic objectives
DCH Vision
Five Year Forward View
DCH Strategic Programmes
Right Care and Demand
Management
Str
ateg
y -
Boa
rd o
vers
ight
Page 60 of 132

Title of Meeting
Board of Directors
Date of Meeting
31 May 2017
Report Title
Corporate Risk Register and Board Assurance Framework
Author
Mandy Ford, Head of Risk Management and Quality Assurance Lindsey Perryman, Trust Secretary
Responsible Executive
Nicky Lucey, Director of Nursing and Quality Libby Walters, Director of Finance and Resources
Purpose of Report (e.g. for decision, information) For information.
Summary
Corporate Risk Register The Risk Items on the Corporate Risk Register have been reviewed by the appropriate risk leads and the Executive Team.
The Trust Risk Register outlines the current position regarding all of the active Risk Items which have been identified by the Trust. There are currently 15 Risk Items on the Corporate Risk Register. Summarised below are key changes;
Increased Risks Impact
1009 Added 01/12/2016 No compliant mental health interview room, no footprint available.
Increased 14.4 HIGH RISK Ongoing
1045 Added 01/12/2016 Opthalmology Service Capacity
Increased 20.0 EXTREME RISK Ongoing
1009 Added 01/12/2016 Financial Sustainablity
Increased 13.6 HIGH RISK Ongoing
NEW
1059 Added 11.05.17
Recruitment and retention of staff across specialities
NEW Risk Rating 16 EXTREME RISK Outstanding
1060 Added 05/05/2017
Temporary Medical Workforce planning and capacity
NEW Risk Rating 12 HIGH RISK Outstanding
Cor
pora
te R
isk
Reg
iste
r
Page 61 of 132

Board Assurance Framework Following the development of the Trust’s Strategy, the Board Assurance Framework has been reworked and mapped against the Trust’s Strategic Objectives and the priorities for achievement of the objective. The following risks are rated as RED:
Not being able to deliver transformational savings at a fast enough pace
Insufficient cash to ensure the continuity of services
An unsustainable financial position could result in a reduced quality of both clinical and support services and reduce the autonomy the Trust has in providing high quality services to its population.
Opthalmology: An unsustainable financial position could result in a reduced quality of both clinical and support services and reduce the autonomy the Trust has in providing high quality services to its population.
There have been changes to risk ratings of the BAF since the last review by Audit Committee.
Risks or emerging risks that are or could impact on the strategic priorities The following risks have been identified above as having the potential to impact on “outstanding”:
Emergency Department Target, Delays to Care & Patient Flow
ENT Medical Staffing
Waiting lists and staffing for Gastroenterology
Staffing within ED
Ability to meet targets because of staffing issues
Previously Reviewed by Corporate Risk Register - appropriate risk leads and the Executive Team.
Board Assurance Framework - Audit Committee, March 2017 - no changes to the BAF were requested at this meeting
Strategic Impact The Corporate Risk Register outlines the identified risks to the achievement of quality and performance standards. Failure to identity and control risks could lead to the Trust failing to meet its strategic objectives.
Risk Evaluation Each risk item is individually evaluated using the current Trust Risk Matrix.
Impact on Care Quality Commission Registration and/or Clinical Quality
Cor
pora
te R
isk
Reg
iste
r
Page 62 of 132

It is a requirement to regularly identify, capture and monitor risks to the achievement of quality and performance standards. The Trust Risk Register provides the Board with an opportunity to gain oversight of the identified risks and work streams being carried out to address them, and provide assurance to the Trust Board on these issues.
Governance Implications (legal, clinical, equality and diversity or other): The Trust Risk Register highlights that risks have been identified and capture. The Document provides an outline of the work being undertaken to manage and mitigate each risk and gives an opportunity for the Board to consider the effectiveness of the activities being undertaken. Where there are governance implications to risks on the Board Assurance Framework these will be considered as part of the mitigating actions.
Financial Implications The Trust Risk Register includes risks items relating to financial performance and the financial impact of individual quality and performance issues. The Board Assurance Framework includes risks to long term financial stability and the controls and mitigations the Trust has in place.
Freedom of Information Implications – can the report be published?
Yes
Recommendations
The Board are asked to:
note the Corporate Risk Register
note the Board Assurance Framework
consider additional emerging risks that need to be captured and monitored within the Trust Risk Register
consider whether those risk which are consider to have/potentially have an impact on the Trust’s strategic objectives should be included in the next iteration of the Board Assurance Framework
C
orpo
rate
Ris
k R
egis
ter
Page 63 of 132

1045 V3 01/12/2016 Risk Rating
20.0 EXTREME RISK POST MITIGATION
12.0 HIGH RISK
1055 V1 06/03/2017 Risk Rating
19.0 EXTREME RISK POST MITIGATION
11.2 HIGH RISK
1059 V1 11/05/2017 Risk Rating
16.0 EXTREME RISK POST MITIGATION
1056 V1 08/03/2017 Risk Rating
15.0 EXTREME RISK POST MITIGATION
3.6 LOW RISK
1009 V3 01/12/2016 Risk Rating
14.4 HIGH RISK 9.0 HIGH RISK
1017 V3 01/12/2016 Risk Rating
14.0 HIGH RISK POST MITIGATION
4.8 MODERATE RISK
1015 V3 01/12/2016 Risk Rating
13.6 HIGH RISK POST MITIGATION
7.8 HIGH RISK
1049 V3 01/12/2016 Risk Rating
13.6 HIGH RISK POST MITIGATION
6.6 MODERATE RISK
1011 V3 01/12/2016 Risk Rating
13.0 HIGH RISK POST MITIGATION
12.0 HIGH RISK
1051 V3 01/12/2016 Risk Rating
12.0 HIGH RISK POST MITIGATION
4.8 MODERATE RISK
1052 V3 08/03/2017 Risk Rating
12.0 HIGH RISK POST MITIGATION
5.4 MODERATE RISK
1060 V1 05/05/2017 Risk Rating
12.0 HIGH RISK POST MITIGATION
6.0 MODERATE RISK
1041 V3 01/12/2016 Risk Rating
11.2 HIGH RISK POST MITIGATION
4.8 MODERATE RISK
1047 V4 22/02/2017 Risk Rating
10.4 HIGH RISK POST MITIGATION
6.0 MODERATE RISK
1050 V3 01/12/2016 Risk Rating
9.6 HIGH RISK POST MITIGATION
4.4 MODERATE RISK
Workforce Planning & Capacity for Nursing/Midwifery Staff
Mortality Indicator
Temporary Medical Workforce Planning & Capacity
Medical Device Management - Training
Fire Alarm Reliability and Capacity
Financial Sustainability
Access to Care in the Community
Therapy Capacity
Sepsis: recognition, diagnosis and early management
Failure to manage the deteriorating patient effectively
This report provides a summary of the risks currently identified within the Department, Service or Function
SUMMARY
TRUST CORPORATE RISK REGISTER May 2017
Quality of Electronic Discharge Summaries
Recruitment and retention of staff across specialities
ENT Medical Staffing
Ophthalmology Service Capacity
Emergency Department Target, Delays to Care & Patient Flow
Cor
pora
te R
isk
Reg
iste
r
Page 64 of 132

Ref
CU
RR
EN
T R
ISK
R
ATI
NG
20EX
TREM
E R
ISK
1045
V3
01/1
2/20
16P
revi
ous
Rat
ing
PO
ST
MIT
IGA
TIO
N
RA
TIN
G12
HIG
H R
ISK
Add
ed to
Ris
k R
egis
ter
Ris
k S
tate
men
t
Pro
gres
s R
epor
tR
isk
Man
agem
ent
Pla
n &
Tim
esca
leD
eman
d M
anag
emen
t• G
lauc
oma
Ref
erra
l ref
inem
ent s
chem
e w
ith lo
cal o
ptom
etris
ts to
redu
ce
refe
rrals
in to
ser
vice
at s
ourc
e (J
une
2017
) • T
rain
ing
Opt
omet
rists
to s
uppo
rt in
clin
ics
with
a v
iew
to w
orki
ng a
uton
omou
sly
in th
e co
mm
unity
(Nov
embe
r 201
6)• S
topp
ing
rout
ine
post
-ope
rativ
e ca
tara
ct fo
llow
ups
to b
e pi
lote
d ad
aptin
g fra
mew
ork
used
at R
oyal
Dev
on &
Exe
ter h
ospi
tal s
ince
200
9 (J
une
2017
)• S
top
rout
ine
listin
g fo
r cat
arac
t sec
ond
eyes
and
tigh
ter g
uide
lines
to b
e in
trodu
ced
for f
irst e
ye li
stin
g (M
arch
201
7)• R
evie
w lo
ng te
rm te
nder
opt
ions
to s
uppo
rt sp
ecifi
c pa
thw
ays
or e
ntire
ser
vice
. (J
un 1
7)C
apac
ity P
lan
• R
evie
w c
apac
ity &
dem
and
mod
ellin
g w
ith n
ew p
osts
onl
ine.
(May
17)
• Und
erta
ke e
xten
sive
in d
epth
val
idat
ion
– in
itial
val
idat
ion
sugg
ests
sev
eral
pa
thw
ays
coul
d be
clo
sed.
(May
17)
• SIT
to re
view
out
patie
nt a
nd th
eatre
sta
ndar
ds a
nd e
ffien
cies
and
cre
ate
rapi
d im
prov
emen
t pla
n.• P
rocu
rem
ent r
isk
asse
ssed
inso
urci
ng/o
utso
urci
ng w
ithou
t ten
derin
g. M
edin
et
and
YDH
eng
aged
to p
rovi
de q
uote
s/av
aila
ble
capa
city
. (M
ay 1
7)• E
xten
d cu
rren
t Loc
um u
ntil
Sep
tem
ber 1
7. (M
ay 1
7)• R
evie
w c
urre
nt a
nnua
l lea
ve fo
r nex
t 3 m
onth
s to
con
side
r red
ucin
g/po
stpo
ning
w
here
pos
sibl
e. (M
ay 1
7)• E
xete
r und
erto
ok 2
00 c
atar
act
oper
atio
ns b
y Ja
nuar
y 20
17• A
dditi
onal
ope
ratin
g lis
ts in
trodu
ced
for l
ong
wai
ting
patie
nts
e.g.
Ocu
lopl
astic
s (O
ngoi
ng)
• Add
ition
al o
utpa
tient
clin
ics
to b
e in
trodu
ced
by fl
exin
g cu
rren
t con
sulta
nt jo
b pl
ans
(Ong
oing
)• A
ttem
pt to
recr
uit t
o co
nsul
tant
vac
ancy
(Mar
ch 2
017)
• Exp
lore
Joi
nt c
onsu
ltant
app
oint
men
t with
RB
H (M
arch
201
7)• R
evie
w s
kill
mix
afte
r res
igna
tion
of A
ssoc
iate
Spe
cial
ist t
o re
plac
e 1
wte
with
2
wte
spe
cial
ist n
urse
s (D
ecem
ber 2
016)
• Tra
inin
g of
Mid
dle
grad
es to
und
erta
ke a
dditi
onal
pro
cedu
res
to re
leas
e co
nsul
tant
tim
e, b
ackf
ill to
be
supp
orte
d by
new
Ban
d 6
nurs
es (A
ug 2
016)
• Int
rodu
ctio
n of
1 s
top
YAG
lase
r clin
ic (M
ay 2
017)
• Add
ition
al w
eeke
nd c
linic
cap
acity
pla
nned
thro
ugho
ut M
ay 1
7 to
see
80
Out
line
TRU
ST C
OR
POR
ATE
RIS
K R
EGIS
TER
May
201
7
This
repo
rt pr
ovid
es a
sum
mar
y of
the
risks
cur
rent
ly id
entif
ied
with
in th
e D
epar
tmen
t, S
ervi
ce o
r Fun
ctio
n
Ver
sion
Ris
k S
tate
men
t
Lead
Man
ager
Oph
thal
mol
ogy
Serv
ice
Cap
acity
19 E
xtre
me
Ris
k
Ther
e is
a ri
sk o
f adv
erse
pat
ient
out
com
es, r
eput
atio
n im
pact
and
fina
ncia
l im
pact
aris
ing
from
del
ays.
Thi
s re
late
s to
as
sess
men
t and
trea
tmen
t of o
phth
alm
olog
y pa
tient
s du
e to
dem
and
for s
ervi
ce e
xcee
ding
cap
acity
, ins
uffic
ient
sta
ffing
leve
ls,
and
chal
leng
es o
f prio
ritis
atio
n of
new
and
chr
onic
pat
ient
s us
ing
a pa
rtial
boo
king
ser
vice
. Out
patie
nt w
aitin
g tim
es to
firs
t ap
poin
tmen
t now
una
ccep
tabl
y lo
ng a
nd p
ose
a po
tent
ial p
atie
nt s
afet
y ris
k.
RTT
- Fo
rtnig
htly
mee
tings
with
the
Chi
ef O
pera
ting
offic
er to
revi
ew p
rogr
ess
agai
nst p
lan.
Mee
tings
incr
ease
d to
wee
kly
from
w
eek
begi
nnin
g 8t
h M
ay20
17
S
kills
Mix
Rev
iew
- R
evie
w c
ompl
eted
and
0.8
wte
Ass
ocia
te s
peci
alis
t & 1
wte
Nur
se c
onsu
ltant
to b
e re
plac
ed w
ith 1
wte
Nur
se
Spe
cial
ist,
2wte
Orth
opis
ts, 0
.7w
te E
CLO
& 1
wte
Clin
ical
Fel
low
. N
urse
Spe
cial
ist a
nd O
rthop
ists
pos
ts o
ut to
adv
ert i
n M
arch
17
.R
ecru
itmen
t –
• Ban
d 5
& 6
Orth
optis
ts in
terv
iew
ed a
nd a
ppoi
nted
. Sta
rt da
tes
conf
irmed
for A
ug 1
7. E
arly
mod
ellin
g su
gges
ts th
e fo
llow
ing
incr
ease
in y
early
out
patie
nt c
apac
ity o
nce
post
s on
line,
Gla
ucom
a –
5670
slo
ts, A
MD
– 6
30, I
njec
tion
(Luc
entis
) – 6
30.
• Ban
d 7
spec
ialis
t nur
se a
dver
t has
bee
n un
succ
essf
ul a
fter 3
roun
ds o
f adv
erts
. Rol
e re
view
ed a
nd to
be
rew
ritte
n as
1 W
TE
Clin
ical
Opt
omet
rist w
ith a
pla
n to
adv
ertis
e M
ay 1
7.• 2
x C
onsu
ltant
pos
ts n
ow w
ith H
unte
rs H
ealth
care
to s
earc
h fo
r sui
tabl
e ca
ndid
ates
. H
igh
Flow
clin
ics
– hi
gh fl
ow g
lauc
oma
and
AM
D c
linic
s to
be
trial
led
to in
crea
se c
apac
ity w
ithou
t ext
ra m
edic
al s
taff.
Firs
t clin
ic
plan
ned
for (
AM
D) 0
9/05
/17
with
18
patie
nts
book
ed a
s op
pose
d to
usu
al 1
2. G
lauc
oma
trial
stil
l to
be p
lann
ed.
Gla
ucom
a R
efer
ral r
efin
emen
t – C
ontra
ct d
rafte
d by
pro
cure
men
t and
sen
t ove
r to
prov
ider
(Dor
set L
OC
) to
sign
. Pla
n to
co
mm
ence
ser
vice
Jun
e 17
.B
and
6 N
ursi
ng c
ompe
tenc
ies
– C
ompe
tenc
ies
draf
ted
and
agre
ed fo
r 2x
B6
Juni
or s
iste
rs in
the
RE
I to
unde
rtake
clin
ical
wor
k.
Trai
ning
pro
gram
me
agre
ed. P
lan
for s
uper
vise
d cl
inic
s to
com
men
ce e
nd o
f Jul
y/be
ginn
ing
Aug
17
once
initi
al tr
aini
ng
com
plet
e.In
ject
ion
capa
city
– L
ead
Orth
optis
t sta
rted
unde
rtaki
ng in
ject
ion
lists
Mar
17.
Thi
s ha
s re
plac
ed th
e lo
st c
apac
ity fr
om th
e pr
evio
us a
ssoc
iate
spe
cial
ist p
ositi
on.
22/0
3/20
16
Soph
ie J
orda
n, D
ivis
iona
l Man
ager
(Div
isio
n B
)B
en L
eigh
, Dire
ctor
ate
Man
ager
(Car
e G
roup
2)
Cor
pora
te R
isk
Reg
iste
r
Page 65 of 132

Ref
CU
RR
EN
T R
ISK
R
ATI
NG
19EX
TREM
E R
ISK
1055
V1
06/0
3/20
17P
revi
ous
Rat
ing
PO
ST
MIT
IGA
TIO
N
RA
TIN
G11
HIG
H R
ISK
Add
ed to
Ris
k R
egis
ter
Ris
k S
tate
men
tLe
ad M
anag
erSo
phie
Jor
dan,
Ben
Lei
ghN
EW
Uns
afe
med
ical
sta
ffing
leve
ls w
ithin
the
EN
T se
rvic
e to
pro
vide
bot
h E
mer
genc
y an
d R
outin
e w
ork.
Ver
sion
Ris
k S
tate
men
t
ENT
Med
ical
Sta
ffing
Mid
dle
Gra
de V
acan
cies
• Job
to b
e re
writ
ten
as 2
x fe
llow
pos
ts to
try
and
mak
e P
osts
mor
e ap
peal
ing
and
put b
ack
out t
o ad
vert.
Con
sulta
nt a
ppro
achi
ng R
oyal
Col
lege
to g
et p
osts
fo
rmal
ly re
cogn
ised
Dea
dlin
e fo
r adv
erts
- 31
/03/
17• D
iscu
ssio
ns w
ith It
alia
n un
iver
sity
to s
ecur
e re
gula
r SP
R tr
aine
es. P
lan
to h
ave
2 S
PR
's a
t a ti
me
unde
rtaki
ng m
inim
al s
ervi
ce a
nd e
mer
genc
y w
ork
in-b
etw
een
train
ing
wee
ks. F
irst S
PR
sec
ured
and
join
ing
the
depa
rtmen
t for
12
mon
ths
star
ting
28/0
2/17
• Loc
um a
ppro
ved
and
secu
red
to c
over
gap
- D
elay
ed, 2
2 cl
inic
s lo
st d
ue to
no
Locu
m th
roug
hout
Dec
, onl
y se
cure
d fro
m 1
6/01
/201
7 –
31/0
3/17
.C
onsu
ltant
long
term
Sic
knes
s• L
ocum
mid
dle
grad
e co
verin
g ge
nera
l clin
ics.
Red
uced
Impa
ct, N
o Lo
cum
th
roug
hout
Dec
embe
r res
ultin
g in
loss
of 6
clin
ics
as o
ther
cov
ered
by
cons
ulta
nt
colle
ague
s.• C
onsu
ltant
retu
rned
on
phas
ed b
asis
w/c
13/
02/1
7. W
ill u
nder
take
2 s
essi
ons
1st w
eek,
3 s
essi
ons
2nd
and
will
then
revi
ew w
ith O
H. C
onsu
lt ha
s ex
pres
sed
wis
h to
retu
rn to
5 d
ay w
orki
ng u
nder
taki
ng 5
clin
ical
ses
sion
s pe
r wee
k.
Aw
aitin
g ou
tcom
e of
Occ
upat
iona
l Hea
lth v
isit
28/0
2/17
.A
dmitt
ed b
ackl
og• R
TT m
onie
s se
cure
d fro
m N
HS
Eng
land
. Pla
n to
und
erta
ke a
t lea
st 5
0 ad
ditio
nal c
ases
bef
ore
end
of th
e fin
anci
al y
ear.
Wor
k to
be
unde
rtake
n by
DC
H
cons
ulta
nts
with
ME
DIN
ET
supp
lyin
g th
eatre
sta
ff at
wee
kend
s. D
eadl
ine
for
wor
k to
be
com
plet
ed -
31/0
3/17
• Wai
ting
list r
evie
wed
regu
larly
and
pat
ient
s tre
at in
turn
of c
linic
al p
riorit
y.
Adm
itted
per
form
ance
has
see
n a
stea
dy in
crea
se o
ver p
ast 4
mon
ths.
Non
-Adm
itted
Bac
klog
• Circ
a 60
pat
ient
s aw
aitin
g 1s
t OP
A o
ver 1
8w d
ue to
nee
ding
Aud
iogr
am p
rior t
o 1s
t OP
A. A
udio
logy
& E
NT
runn
ing
addi
tiona
l cap
acity
to s
ee p
atie
nts
in
Febr
uary
17.
Thi
s w
ill e
limin
ate
this
bac
klog
and
a n
ew jo
int p
roce
ss is
in p
lace
w
ith A
udio
logy
to e
nsur
e th
is d
oes
not h
appe
n ag
ain.
• 10
extra
clin
ics
plan
ned
thro
ugho
ut M
arch
17.
Thi
s gi
ves
capa
city
for a
n ad
ditio
nal 1
20 p
atie
nts
to b
e se
en.
Em
erge
ncy
cove
r• C
onsu
ltant
s ro
ta’s
/job
plan
s re
-writ
ten
to e
nsur
e th
ere
is a
con
sulta
nt o
n si
te
ever
y da
y to
cov
er m
iddl
e gr
ades
& S
HO
’s.
Pro
gres
s R
epor
tR
isk
Man
agem
ent
Pla
n &
Tim
esca
le
06/0
3/20
17
Cor
pora
te R
isk
Reg
iste
r
Page 66 of 132

Ref
CU
RR
EN
T R
ISK
R
ATI
NG
16EX
TREM
E R
ISK
1059
V1
11/0
5/20
17P
revi
ous
Rat
ing
PO
ST
MIT
IGA
TIO
N
RA
TIN
G0
Add
ed to
Ris
k R
egis
ter
Div
isio
nal L
eads
Ris
k M
anag
emen
t P
lan
& T
imes
cale
Man
y di
ffere
nt a
ppro
ache
s ar
e be
ing
adop
ted
to m
eet t
hese
risk
s, a
nd th
e so
lutio
n w
ill va
ry d
epen
ding
on
the
spec
ialty
and
par
ticul
ar is
sues
.
We
have
est
ablis
hed
a R
esou
rcin
g S
trate
gy B
oard
to c
onsi
der o
ur s
trate
gic
appr
oach
to
long
term
med
ical
gap
s, a
nd E
xecu
tives
mee
t on
a w
eekl
y ba
sis
to re
view
all
med
ical
ga
ps a
nd p
rogr
ess
agai
nst s
peci
fic re
crui
tmen
t pla
ns.
In a
reas
whe
re w
e ha
ve k
now
n sk
ill sh
orta
ges
and
hard
to fi
ll ro
les,
alte
rnat
ive
wor
kfor
ce
mod
els
are
bein
g co
nsid
ered
and
impl
emen
ted.
For
exa
mpl
e, tr
aini
ng O
ptom
etris
ts to
su
ppor
t in
clin
ics
with
a v
iew
to w
orki
ng in
depe
nden
tly in
the
com
mun
ity.
We
are
wor
king
with
our
Van
guar
d pa
rtner
s to
mak
e jo
int a
ppoi
ntm
ents
, with
a v
iew
to
mak
ing
role
s m
ore
attra
ctiv
e to
can
dida
tes
and
deliv
erin
g be
nefit
to b
oth
orga
nisa
tions
(for
ex
ampl
e w
ithin
Oph
thal
mol
ogy.
)
Alte
rnat
ive
job
plan
s al
so b
eing
dev
elop
ed to
app
eal t
o a
wid
er a
pplic
ant p
ool.
An
exam
ple
bein
g w
ithin
EN
T w
here
2 fe
llow
pos
ts h
ave
been
dev
elop
ed in
con
junc
tion
with
th
e R
oyal
Col
lege
.
We
are
also
act
ivel
y re
crui
ting
Phy
sici
an A
ssis
tant
s to
redu
ce th
e de
man
d on
med
ical
do
ctor
s in
trai
ning
. Thi
s ha
s be
en a
suc
cess
ful a
ppro
ach
in a
naes
thet
ics,
and
we
are
wor
king
with
HE
E to
dev
elop
a tr
aini
ng p
rogr
amm
e fo
r PA
s w
ithin
Dor
set.
This
is a
long
er
term
app
roac
h, b
ut w
ill in
crea
se o
ur a
bilit
y to
recr
uit a
nd re
tain
PA
s in
the
futu
re, a
nd
bene
fit fr
om th
eir t
rain
ing
plac
emen
ts.
Car
e pa
thw
ays
are
also
bei
ng re
view
ed to
redu
ce d
eman
d w
ithin
spe
cific
spe
cial
ties,
for
exam
ple,
the
use
of O
ptom
etris
ts to
refin
e th
e re
ferra
l pro
cess
– p
artic
ular
ly in
the
case
of
Gla
ucom
a.
We
are
parti
cipa
ting
in a
sch
eme
led
by th
e C
CG
to o
ffer p
lace
men
ts to
pos
t gra
duat
e G
P
train
ees,
whi
ch p
rovi
des
a sm
all n
umbe
r of s
essi
ons
for t
hese
doc
tors
for a
12
mon
th
perio
d (C
aree
r Fle
x).
We
are
recr
uitin
g ov
erse
as m
edic
al tr
aine
es th
roug
h th
e M
edic
al T
rain
ee In
itiat
ive
(MTI
) sc
hem
e.
NE
W
Ver
sion
Ris
k S
tate
men
t
Rec
ruitm
ent a
nd re
tent
ion
of s
taff
acro
ss s
peci
aliti
esLe
ad M
anag
erTh
is ri
sk a
mal
gam
ates
risk
s id
entif
ied
prev
ious
ly re
fere
nces
: 105
5 (E
NT
Med
ical
Sta
ffing
), 10
45(O
phth
alm
olog
y C
apac
ity L
evel
s du
e to
Sta
ffing
) an
d ne
w s
taffi
ng ri
sks
bein
g id
entif
ied
in o
ther
spe
cial
ties.
11/0
5/20
17
Pro
gres
s R
epor
t
Ris
k S
tate
men
t
Pro
gres
s ag
ains
t eac
h of
thes
e ris
k m
anag
emen
t pla
ns is
at d
iffer
ent s
tage
s de
pend
ing
on th
e sp
ecia
lty.
In te
rms
of th
e ge
neric
act
ions
:G
over
nanc
e an
d tra
ckin
g no
w in
pla
ce.
Phy
sici
an A
ssoc
iate
s be
ing
activ
ely
recr
uite
d at
job
fair
on 1
5th
May
. Fur
ther
mee
ting
with
HE
E a
nd
educ
atio
n pr
ovid
ers
bein
g ar
rang
ed b
y H
EE
.. C
once
rns
with
pac
e of
pro
gres
s ra
ised
at D
orse
t Wor
kfor
ce
Act
ion
Boa
rd a
t May
mee
ting.
Re-
desi
gn o
f car
e pa
thw
ay’s
is o
ngoi
ng.
Pla
cem
ents
for C
CG
Car
e Fl
ex s
chem
e be
ing
iden
tifie
d.
MTI
recr
uitm
ent c
omm
ence
d an
d on
goin
g.
Cor
pora
te R
isk
Reg
iste
r
Page 67 of 132

Ref
CU
RR
EN
T R
ISK
R
ATI
NG
15EX
TREM
E R
ISK
1056
V1
08/0
3/20
17P
revi
ous
Rat
ing
PO
ST
MIT
IGA
TIO
N
RA
TIN
G4
LOW
RIS
K
Add
ed to
Ris
k R
egis
ter
Fire
Ala
rm R
elia
bilit
y an
d C
apac
ity15
.0 E
xtre
me
Ris
k
08/0
3/20
17
Ver
sion
Ris
k S
tate
men
t
Ther
e is
a la
ck o
f cap
acity
for e
xpan
ding
the
num
ber o
f pro
tect
ion
devi
ces,
repa
irs a
re b
ecom
ing
mor
e fre
quen
t as
the
syst
em a
ges
and
the
clos
ed p
roto
col n
atur
e of
the
syst
em m
akes
us
relia
nt o
n th
e m
anuf
actu
rer f
or m
aint
enan
ce a
nd re
pairs
. In
add
ition
, all
of E
ast W
ing
and
Leve
ls 0
, 1 a
nd 2
Sou
th
Win
g, n
eed
to b
e un
grad
ed to
L1
stan
dard
to m
eet B
S58
39 a
nd th
e R
egul
ator
y R
efor
m (F
ire S
afet
y)
Ord
er 2
005
Andy
Mor
ris
Full
revi
ew o
f req
uire
men
ts to
repl
ace
the
exis
ting
syst
em, i
nclu
ding
ope
n pr
otoc
ol.
Firs
t pha
se to
in
clud
e th
e re
plac
emen
t of t
he m
ain
fire
alar
m c
ontro
l pan
el a
nd a
ssoc
iate
d w
orks
in th
e N
orth
Win
g,
subs
eque
nt w
orks
to u
pgra
de th
e E
ast a
nd S
outh
Win
gs.
S
ub p
anel
faul
t has
bee
n re
ctifi
ed w
ith in
stal
latio
n of
a n
ew p
anel
and
has
resu
lted
in fe
wer
faul
ts.
The
E
stat
es O
ffice
r Ele
ctric
al h
as c
omm
ence
d th
e pr
oces
s of
iden
tifyi
ng a
con
sulta
nt to
ass
ist w
ith th
e re
view
pr
oces
s.
Pro
gres
s R
epor
t
Ris
k S
tate
men
tLe
ad M
anag
er
Ris
k M
anag
emen
t P
lan
& T
imes
cale
This
risk
was
firs
t ide
ntifi
ed in
ear
ly 2
014.
At t
he ti
me
we
gave
an
unde
rtaki
ng to
the
Fire
Ser
vice
that
a s
yste
mat
ic a
ppro
ach
wou
ld b
e ta
ken
to re
plac
e th
e fir
e al
arm
sys
tem
ove
r a n
umbe
r of y
ears
. Sin
ce th
en
the
fire
alar
m u
pgra
de h
as b
een
push
ed b
ack
as p
art o
f cap
ital b
udge
t al
tera
tions
. Bas
ed o
n cu
rrent
bud
gets
we
will
be
doin
g th
e fo
llow
ing:
2016
/17
- ful
l sys
tem
revi
ew to
iden
tify
wor
k ne
eded
(£10
0,00
0). B
egin
te
nder
for o
pen
prot
ocol
sys
tem
.20
17/1
8 - £
400,
000
for E
ast w
ing
upgr
ade
2018
/19
- £35
0,00
0 fo
r Sou
th w
ing
upgr
ade
Cor
pora
te R
isk
Reg
iste
r
Page 68 of 132

Ref
CU
RR
EN
T R
ISK
R
ATI
NG
14H
IGH
RIS
K
1009
V3
01/1
2/20
16P
revi
ous
Rat
ing
PO
ST
MIT
IGA
TIO
N
RA
TIN
G9
HIG
H R
ISK
Add
ed to
Ris
k R
egis
ter
Pro
gres
s R
epor
tR
isk
Man
agem
ent
Pla
n &
Tim
esca
leTo
exp
lore
all
optio
ns re
gard
ing
bette
r util
isat
ion
of c
urre
nt s
pace
and
pl
ans
to e
xpan
d ar
ea.
Fina
l wor
ks p
lan
agre
ed.
To g
o ou
t to
tend
er.
Wor
ks p
lan
to b
e ris
k as
sess
ed to
dev
elop
a b
usin
ess
cont
inui
ty p
lan
whi
le 5
maj
ors
spac
es c
lose
d fo
r con
stru
ctio
n, c
onsi
derin
g pa
tient
saf
ety
and
impa
ct o
n pe
rform
ance
. Sta
rt da
te fo
r wor
ks to
be
conf
irmed
; sta
rt da
te w
ill im
pact
on
BC
P d
ue to
cha
nges
in c
ase
mix
and
pos
sibl
e sp
ace
crea
ted
as p
art o
f the
bed
reco
nfig
urat
ion
plan
. Nur
sing
- N
ursi
ng
lead
ersh
ip s
truct
ure
revi
ewed
, with
adj
ustm
ents
to b
and
6 an
d 7
ratio
, with
a
view
to im
prov
ing
gove
rnan
ce (D
ec 2
016)
. C
reat
ion
of 2
x A
NP
role
s,
both
hav
e be
en re
crui
ted
to w
ith s
tart
date
s in
Mar
ch a
nd M
ay 2
017)
. B
and
4 nu
rsin
g ro
les
in d
evel
opm
ent t
o su
ppor
t exi
stin
g st
aff m
odel
. O
ngoi
ng re
crui
tmen
t to
vaca
ncie
s in
ban
d 5
esta
blis
hmen
t. M
edic
al
Sta
ffing
- Id
entif
icat
ion
of u
pcom
ing
gaps
in G
PTV
s ro
ta a
nd ju
nior
doc
tor
rota
, with
new
recr
uits
app
oint
ed w
ith s
tart
date
s in
Mar
ch 2
017.
E
xplo
ring
use
of p
hysi
cian
's a
ssoc
iate
s an
d m
ajor
s ad
vanc
ed
prac
titio
ners
to b
road
en w
orkf
orce
. Upc
omin
g M
G v
acan
cy o
ut to
adv
ert
sinc
e no
tice
rece
ived
; so
far u
nsuc
cess
ful.
App
oint
ed c
onsu
ltant
to
upco
min
g va
canc
y, s
tarte
d 24
Apr
il 20
17.
Wor
king
with
all
spec
ialti
es to
id
entif
y an
d de
velo
p st
ream
ing
path
way
s fo
r spe
cific
pre
sent
ing
cond
ition
s. D
evel
opm
ent o
f int
erna
l pro
fess
iona
l sta
ndar
ds to
form
alis
e an
d co
dify
the
man
agem
ent o
f spe
cial
ty p
atie
nts
in E
D. M
eetin
gs w
ith
spec
ialti
es to
dis
cuss
cha
lleng
es a
nd th
e de
velo
pmen
t of m
utua
lly
agre
eabl
e so
lutio
ns.
Red
esig
n of
mon
thly
bre
ach
repo
rt to
incr
ease
aw
are
of th
e im
pact
of e
ach
divi
sion
on
ED
per
form
ance
. O
ngoi
ng c
lose
w
orki
ng w
ith W
eym
outh
Urg
ent C
are
Cen
tre, r
otat
ing
cons
ulta
nt a
nd
mid
dle
grad
e co
ver t
o th
e U
CC
and
the
shar
ing
of le
arni
ng a
nd b
est
prac
tice.
Stre
ngth
enin
g of
rela
tions
hips
with
loca
l MIU
s.
Ris
k S
tate
men
tLe
ad M
anag
er
Ver
sion
Ris
k S
tate
men
t
Emer
genc
y D
epar
tmen
t Tar
get,
Del
ays
to C
are
& P
atie
nt F
low
10.6
Inco
nsis
tent
ach
ieve
men
t of t
he 4
-hou
r sta
ndar
d, c
ause
d by
cro
wdi
ng, h
igh
atte
ndan
ce n
umbe
rs,
insu
ffici
ent b
ed/a
sses
smen
t uni
t cap
acity
, and
sta
ffing
cha
lleng
es, l
eadi
ng to
ext
erna
l reg
ulat
or s
crut
iny,
im
pact
on
over
all p
erfo
rman
ce (l
inke
d to
STF
pac
kage
), am
bula
nce
hand
over
del
ays,
and
pat
ient
saf
ety
risks
.
Fund
ing
agre
ed to
com
plet
e a
porti
on o
f req
uest
ed e
stat
es w
ork.
Wor
k w
ill b
e pr
iorit
ised
, with
the
min
or o
ps ro
om
and
the
old
eye
room
to b
e co
mpl
eted
as
a m
atte
r of u
rgen
cy.
This
will
ens
ure
that
dep
artm
ent c
ompl
ies
with
CQ
C
requ
irem
ents
, res
olve
s th
e is
sue
with
trol
ley
acce
ssib
ility
in th
e ey
e ro
om, a
nd c
reat
es o
ne a
dditi
onal
maj
ors
spac
e.
Wor
ks o
ut to
tend
er, w
ith a
ctiv
ity p
lann
ed to
occ
ur in
Jun
-Aug
201
7. B
uild
ing
wor
ks w
ill c
ompr
omis
e m
ajor
s ca
paci
ty s
igni
fican
tly.
Pla
ns to
miti
gate
the
impa
ct o
f thi
s ar
e be
ing
expl
ored
incl
udin
g m
ovin
g E
DA
U to
a w
ard
envi
ronm
ent,
usin
g th
e E
DA
U s
pace
to re
acco
mm
odat
e th
e m
ajor
s pa
tient
s, a
nd p
ossi
bly
repu
rpos
e an
offi
ce in
to
an a
dditi
onal
trea
tmen
t spa
ce te
mpo
raril
y. A
dvan
ced
Nur
se P
ract
ition
er ro
le a
gree
d an
d su
cces
sful
ly re
crui
ted
into
, st
art d
ates
in M
arch
and
May
201
7. T
his
role
will
incr
ease
cov
er 7
day
s pe
r wee
k, in
clud
ing
until
mid
nigh
t on
Fri-
Sat
, to
cove
r pea
k ac
tivity
tim
es.
Iden
tifie
d ga
ps d
ue to
non
-allo
catio
n of
GP
VTS
hav
e be
en re
crui
ted
into
, sta
rt da
tes
in M
arch
201
7. A
ltern
ativ
e st
affin
g m
odel
s be
ing
cons
ider
ed.
Sho
rtage
of j
unio
r doc
tors
from
Aug
ust 2
017
note
d in
bus
ines
s ca
se, f
undi
ng a
ppro
ved,
and
role
s ou
t to
adve
rt w
ith o
ne a
ppoi
nted
to.
New
con
sulta
nt s
tarte
d in
po
st in
Apr
il to
sup
port
depa
rtmen
t dur
ing
perio
d of
MG
vac
ancy
and
to s
uppo
rt de
partm
enta
l per
form
ance
.
01/1
2/20
15
Sara
h K
nigh
t, D
ivis
iona
l Man
ager
(Med
icin
e)Je
ni F
ram
pton
, Ste
ph T
hom
as
Cor
pora
te R
isk
Reg
iste
r
Page 69 of 132

Ref
CU
RR
EN
T R
ISK
R
ATI
NG
14H
IGH
RIS
K
1017
V3
01/1
2/20
16P
revi
ous
Rat
ing
Lead
Man
ager
PO
ST
MIT
IGA
TIO
N
RA
TIN
G5
MO
DER
ATE
RIS
K
Add
ed to
Ris
k R
egis
ter
Ris
k S
tate
men
t
14 30/0
8/20
13
Ver
sion
Qua
lity
of E
lect
roni
c D
isch
arge
Sum
mar
ies
Ris
k S
tate
men
tC
athe
rine
Aber
y-W
illia
ms,
Ser
vice
Impr
ovem
ent P
rogr
amm
e M
anag
erTh
e Tr
ust p
erio
dica
lly re
ceiv
es re
ports
from
par
tner
age
ncie
s w
hich
hig
hlig
ht th
at p
robl
ems,
del
ays,
inac
cura
cy o
f det
ails
in E
DS
do
cum
ents
occ
urs
or m
ultip
le E
Ds
are
sent
. Thi
s ca
n ca
use
dela
ys in
trea
tmen
t or f
ollo
w-u
p. A
pla
n to
regu
larly
edu
cate
clin
ical
st
aff i
s in
pla
ce. T
he d
evel
opm
ent o
f a p
olic
y do
cum
ent i
s be
ing
unde
rtake
n un
der t
he g
uida
nce
of th
e M
edic
al D
irect
or.
Con
side
ratio
n of
furth
er a
reas
pur
suin
g nu
rse-
led
disc
harg
es is
und
er re
view
. A lo
ng te
rm p
lan
is in
pla
ce to
link
Ele
ctro
nic
Dis
char
ge S
umm
ary
(ED
S) t
o th
e pl
anne
d el
ectro
nic
pres
crib
ing
softw
are.
The
Tru
st c
ontin
ues
to re
ceiv
e ris
k ev
ents
from
GP
pr
actic
es in
rela
tion
to d
elay
ed o
r ina
ccur
ate
ED
S d
ocum
ents
and
mul
tiple
ED
Ss
sent
.
To p
riorit
ise
this
issu
e, w
hich
des
pite
the
cons
ider
able
wor
k st
ream
s du
ring
rece
nt y
ears
con
tinue
s to
repr
esen
t a ri
sk o
f pat
ient
ha
rm, a
task
& fi
nish
gro
up is
bei
ng le
d by
the
Med
ical
Dire
ctor
, Chi
ef O
pera
ting
Offi
cer a
nd S
ervi
ce Im
prov
emen
t Pro
gram
me
Man
ager
, Cat
herin
e A
bery
-Willi
ams.
The
grou
p ha
ve id
entif
ied
an is
sue
with
the
syst
em p
roce
ss a
nd a
re c
urre
ntly
in d
iscu
ssio
ns w
ith S
unqu
est f
or a
n up
date
to
impr
ove
the
syst
em to
rect
ify d
uplic
ate
ED
Ss
bein
g se
nt.
Ris
k M
anag
emen
t P
lan
& T
imes
cale
The
aim
is to
ach
ieve
a h
igh
stan
dard
of t
imel
y an
d ac
cura
te d
ischa
rge
sum
mar
ies.
The
re is
an
Impr
ovem
ent P
lan
whi
ch is
revi
ewed
mon
thly
in o
rder
to
mon
itor s
et m
ilest
ones
and
inte
rven
tion
requ
ired
to a
ddre
ss id
entif
ied
IT is
sues
th
at a
re c
reat
ing
issue
s or d
uplic
ates
/ del
ays.
Cor
pora
te R
isk
Reg
iste
r
Page 70 of 132

Ref
CU
RR
EN
T R
ISK
14
HIG
H R
ISK
1015
V3
01/1
2/20
16P
revi
ous
Rat
ing
PO
ST
MIT
IGA
TIO
N
RA
TIN
G8
HIG
H R
ISK
Add
ed to
Ris
k R
egis
ter
Pro
gres
s R
epor
t
Lead
Man
ager
Shar
on M
oone
y, N
urse
Con
sulta
nt
Failu
re to
man
age
the
dete
riora
ting
patie
nt e
ffect
ivel
y
Ris
k M
anag
emen
t P
lan
& T
imes
cale
It is
pla
nned
that
the
curre
nt o
utre
ach
serv
ice
will
exp
and
to b
e av
aila
ble
24hr
s/da
y fro
m A
ugus
t 201
7.
Sta
ff ar
e cu
rrent
ly b
eing
trai
ned
up to
und
erta
ke th
is ro
le.
Sep
sis
com
mitt
ee e
stab
lishe
d w
ith m
ulti-
prof
essi
onal
atte
ndan
ce a
nd is
exp
andi
ng to
cov
er a
cute
kid
ney
inju
ry.
This
has
ena
bled
coo
rdin
atio
n of
ac
tion
to m
itiga
te th
e ris
k. T
his
has
incl
uded
dev
elop
men
t of a
scr
eeni
ng to
ol, b
ased
on
Nat
iona
l gu
idan
ce, p
rodu
ctio
n of
a g
uide
line
for t
he m
anag
emen
t of t
his
grou
p of
pat
ient
s an
d pr
oduc
tion
of a
n ed
ucat
ion
mat
rix to
mon
itor a
ttend
ance
at t
rain
ing.
The
Vita
lPA
C a
lgor
ithm
will
cont
ain
guid
ance
on
whe
n to
sep
sis
scre
en p
atie
nts,
ach
ievi
ng a
cer
tain
sco
re, i
n th
e ne
xt u
pgra
de.
The
seps
is s
cree
ning
tool
is
now
an
inte
gral
par
t of t
he m
edic
al a
dmis
sion
s pr
o-fo
rma
and
the
nurs
ing
AIR
S d
ocum
ent.
As
part
of th
e W
AH
SN
pro
gram
me
a pr
ojec
t to
impr
ove
the
accu
racy
of f
luid
bal
ance
man
agem
ent,
ofte
n re
quire
d by
th
e de
terio
ratin
g pa
tient
s is
to b
e un
derta
ken.
A d
eter
iora
ting
patie
nts
grou
p is
to b
e es
tabl
ishe
d, s
peci
fical
ly to
look
at t
he ti
min
g, a
ccur
acy
and
esca
latio
n of
obs
erva
tions
. Th
e se
psis
act
ion
plan
con
tinue
s to
be
impl
emen
ted.
Scr
eeni
ng h
as a
lread
y im
prov
ed in
ED
and
use
of t
he s
cree
ning
tool
is in
crea
sing
. Fu
rther
aud
it is
pla
nned
to e
nsur
e th
at th
is
succ
ess
is ro
lling
out,
initi
ally
to o
ther
adm
issi
on a
reas
. Th
e ba
se li
ne a
sses
smen
t for
AK
I has
bee
n co
mpl
eted
and
act
ions
are
und
erw
ay to
impr
ove
the
man
agem
ent o
f thi
s gr
oup
of p
atie
nts.
The
crit
ical
ca
re o
utre
ach
serv
ice
will
be
cove
ring
twilig
ht s
hifts
from
the
mid
dle
of M
arch
with
the
plan
stil
l to
go 2
4/7
in A
ugus
t 201
7 w
hen
the
train
ees
will
have
com
plet
ed th
eir t
rain
ing.
The
WA
HS
N p
roje
ct to
impr
ove
fluid
ba
lanc
e m
onito
ring
mod
ule
of th
e V
italP
AC
sys
tem
has
bee
n re
view
ed b
y th
e gr
oup
and
this
will
be
goin
g in
to te
st s
hortl
y.19
/10/
2015
Ris
k S
tate
men
t13
.6V
ersi
on
A c
ritic
al c
are
outre
ach
serv
ice
has
been
est
ablis
hed
whi
ch c
urre
ntly
co
vers
08.
00 to
20.
00 a
cros
s th
e Tr
ust.
In a
dditi
on, t
he T
rust
is
deve
lopi
ng a
Hos
pita
l at N
ight
ser
vice
for c
over
out
side
of t
hese
hou
rs.
Crit
ical
Car
e O
utre
ach
assi
sts
war
d st
aff t
o id
entif
y an
d m
anag
e ac
utel
y de
terio
ratin
g pa
tient
s an
d su
ppor
ts th
eir e
duca
tion
in th
is.
A m
ulti-
prof
essi
onal
sep
sis
com
mitt
ee h
as b
een
form
ed, w
ith a
n E
xecu
tive
lead
, w
hich
has
ove
rsee
n th
e de
velo
pmen
t and
intro
duct
ion
of a
sep
sis
scre
enin
g to
ol to
aid
in th
e id
entif
icat
ion
and
man
agem
ent o
f thi
s gr
oup
of
patie
nts.
The
scr
eeni
ng to
ol a
lso
dire
cts
staf
f to
the
Sep
sis
6 ca
re b
undl
e to
exp
edite
app
ropr
iate
man
agem
ent.
The
Tru
st h
as s
igne
d up
to th
e W
esse
x A
cade
mic
Hea
lth S
cien
ce N
etw
ork
safe
ty p
rogr
amm
e w
hich
, thi
s ye
ar, i
s fo
cusi
ng o
n th
e de
terio
ratin
g pa
tient
.
It is
kno
wn
that
, at t
imes
, qua
lity
of w
ard
care
with
rega
rd to
the
iden
tific
atio
n an
d m
anag
emen
t of t
he
dete
riora
ting
patie
nt m
ay b
e va
riabl
e an
d st
udie
s ha
ve s
how
n th
at th
is h
as a
n ef
fect
on
patie
nt m
orta
lity
and
mor
bidi
ty.
At p
rese
nt th
ere
is a
'tra
ck a
nd tr
igge
r' (V
iEW
S) s
yste
m w
ithin
the
Trus
t to
iden
tify
patie
nts
at ri
sk o
f det
erio
ratio
n. T
his
syst
em d
oes
not o
verri
de c
linic
al ju
dgem
ent a
nd re
cogn
ition
of t
his
dete
riora
tion
and
appr
opria
te e
scal
atio
n st
ill ne
eds
to h
appe
n. T
his
is n
ot a
lway
s th
e ca
se, l
eadi
ng to
a
num
ber o
f ser
ious
eve
nts
whe
re p
atie
nts
have
det
erio
rate
d du
e to
del
ayed
reco
gniti
on a
nd in
appr
opria
te
or in
adeq
uate
trea
tmen
t. T
his
is n
ot o
nly
a cl
inic
al ri
sk fo
r the
pat
ient
s bu
t als
o ha
s im
plic
atio
ns fo
r the
pr
ofes
sion
al a
ccou
ntab
ility
of th
e st
aff c
arin
g fo
r the
m.
Ris
k S
tate
men
t
Cor
pora
te R
isk
Reg
iste
r
Page 71 of 132

Ref
CU
RR
EN
T R
ISK
R
ATI
NG
14H
IGH
RIS
K
1049
V3
01/1
2/20
16P
revi
ous
Rat
ing
PO
ST
MIT
IGA
TIO
N
RA
TIN
G7
MO
DER
ATE
RIS
K
Add
ed to
Ris
k R
egis
ter
Of t
he £
4.2
milli
on o
f CIP
sch
emes
iden
tifie
d to
dat
e th
e B
VB
C g
roup
hav
e id
entif
ied
that
£1
milli
on a
re
high
risk
and
wor
k is
und
erw
ay to
ens
ure
they
are
all
robu
st p
lans
. D
orse
t wid
e C
IP p
lans
are
bei
ng
deve
lope
d bu
t the
re a
re n
o de
taile
d pl
ans
in p
lace
as
yet.
Ris
k M
anag
emen
t P
lan
& T
imes
cale
Mar
ch 1
7 –
June
17:
A D
orse
t wid
e fin
anci
al c
ontro
l tot
al is
in p
lace
and
w
ork
is h
appe
ning
acr
oss
the
syst
em to
ens
ure
Dor
set a
s w
hole
ach
ieve
s its
fina
ncia
l con
trol t
otal
. T
he fi
nanc
ial g
ap c
an b
e re
duce
d th
roug
h th
e pr
iorit
isat
ion
of th
e st
rate
gic
serv
ices
revi
ew, m
aint
aini
ng fi
nanc
ial r
un
rate
s at
the
sam
e le
vel a
s in
201
6/17
and
clo
ser w
orki
ng w
ith o
ther
pr
ovid
ers
acro
ss D
orse
t. E
ach
divi
sion
has
a s
avin
gs ta
rget
to d
eliv
er
and
the
Fina
nce
Impr
ovem
ent T
eam
is s
uppo
rting
ser
vice
s to
iden
tify
and
deliv
er fu
rther
fina
ncia
l sav
ings
. Th
e B
ette
r Val
ue B
ette
r Car
e G
roup
co
ntin
ue to
ove
rsee
the
CIP
del
iver
y.C
ash
borro
win
g fa
cilit
ies
are
in p
lace
for w
hen
requ
ired.
Thi
s is
not
an
ticip
ated
to b
e un
til th
e se
cond
hal
f of t
he fi
nanc
ial y
ear.
28/0
1/20
16
Ris
k S
tate
men
tLe
ad M
anag
er
Pro
gres
s R
epor
t
Reb
ecca
Kin
g, D
eput
y D
irect
or o
f Fin
ance
Ver
sion
Fina
ncia
l Sus
tain
abili
ty
An
unsu
stai
nabl
e fin
anci
al p
ositi
on c
ould
resu
lt in
a re
duce
d qu
ality
of b
oth
clin
ical
and
sup
port
serv
ices
an
d re
duce
the
auto
nom
y th
e Tr
ust h
as in
pro
vidi
ng h
igh
qual
ity s
ervi
ces
to it
s po
pula
tion.
Ris
k S
tate
men
t
12.8
Cor
pora
te R
isk
Reg
iste
r
Page 72 of 132

Ref
CU
RR
EN
T R
ISK
R
ATI
NG
13H
IGH
RIS
K
1011
V3
01/1
2/20
16P
revi
ous
Rat
ing
PO
ST
MIT
IGA
TIO
N
RA
TIN
G12
HIG
H R
ISK
Add
ed to
Ris
k R
egis
ter
Pro
gres
s R
epor
tR
isk
Man
agem
ent
Pla
n &
Tim
esca
le
Acce
ss to
Car
e in
the
Com
mun
ity
Ris
k S
tate
men
t
30/0
1/20
14
Ver
sion
Jenn
ifer F
ram
pton
, Ser
vice
Man
ager
13 The
aim
is to
ach
ieve
d a
sust
aine
d re
duct
ion
in d
elay
ed tr
ansf
ers
of c
are
and
to s
usta
ined
le
vel l
ower
than
15
patie
nts
by th
e en
d of
Q3
16/1
7
The
wor
k w
ith p
artn
er o
rgan
isat
ions
has
pro
gres
sed
sign
ifica
ntly
, but
is y
et to
real
ise
a no
tabl
e re
duct
ion
in d
elay
s.A
pilo
t at Q
ueen
Cha
rlotte
Nur
sing
Hom
e co
mm
ence
d on
1st
Feb
ruar
y 20
17 fo
r ste
p-do
wn
asse
ssm
ent f
or lo
ng te
rm c
are.
Thi
s is
bei
ng d
eliv
ered
in p
artn
ersh
ip w
ith D
CC
, Wey
mou
th G
Ps
and
Kin
gsle
y H
ealth
care
. The
pro
ject
has
alre
ady
seen
a re
duct
ion
in th
e de
laye
d di
scha
rge
list (
for n
ursi
ng c
are)
, whi
ch is
the
high
est c
ateg
ory
of d
elay
at D
CH
. The
pilo
t will
be e
valu
ated
mid
-end
M
ay 2
017.
Ane
cdot
al e
vide
nce
from
the
proj
ect h
as in
dica
ted
that
pat
ient
car
e ne
eds
are
ofte
n re
duce
d fo
llow
ing
trans
fer t
o Q
ueen
Cha
rlotte
, with
ver
y po
sitiv
e pa
tient
exp
erie
nces
repo
rted.
A m
eetin
g to
det
erm
ine
a pi
lot f
or d
isch
arge
to a
sses
s (h
ome)
at s
cale
has
take
n pl
ace,
bet
wee
n D
CH
, DC
C, D
HU
FT a
nd
Tric
uro.
Res
ourc
e m
appi
ng to
be
done
follo
wed
by
a pr
oces
s m
appi
ng e
xerc
ise.
Initi
ally
, the
pilo
t has
bee
n ag
reed
to ta
ke p
lace
in
Wey
mou
th/P
ortla
nd. P
lan
to b
e pr
oduc
ed, d
ates
for p
ilot t
o be
agr
eed.
Pap
er to
be
prod
uced
to o
utlin
e In
tegr
ated
Dis
char
ge te
am, i
nvol
ving
DC
C, D
HU
FT, V
olun
tary
sec
tor.
Key
obj
ectiv
es a
re
stre
amlin
ing
proc
esse
s fo
r com
plex
dis
char
ge (p
atie
nts
who
nee
d su
ppor
t to
retu
rn h
ome)
, 7 d
ay s
uppo
rt fo
r dis
char
ge, c
o-or
dina
ting
com
plex
dis
char
ges
in h
ospi
tal a
nd in
con
junc
tion
with
com
mun
ity s
ervi
ces.
Trus
ted
prac
titio
ner t
rain
ing
has
been
del
ayed
, but
Tie
r 1 is
bei
ng re
sche
dule
d de
pend
ent u
pon
DC
C a
vaila
bilit
y.. T
rain
ing
will
be
1.5
hour
s fo
r all
inpa
tient
sta
ff. T
ier 1
trai
ning
will
prov
ide
a fo
cus
on in
form
atio
n an
d ad
vice
. Dis
cuss
ions
hav
e co
mm
ence
d on
ho
w th
is m
ay b
e lin
ked
into
Dis
char
ge tr
aini
ng c
urre
ntly
bei
ng p
rovi
ded.
Impl
emen
tatio
n of
Sup
port
at H
ome
serv
ice
in p
artn
ersh
ip w
ith th
e R
ed C
ross
is n
ow in
pla
ce, f
or a
per
iod
of 1
8 m
onth
s. A
si
mila
r sch
eme
but t
hrou
gh D
orse
t Fire
and
Res
cue
serv
ice,
usi
ng th
eir v
olun
teer
s is
due
to c
omm
ence
in J
anua
ry 2
017
as a
pi
lot o
n D
ay-L
ewis
, Pur
beck
and
Rid
gew
ay w
ards
. Th
is w
ill in
clud
e tra
nspo
rt an
d lo
w le
vel i
nter
vent
ions
suc
h as
app
lyin
g Te
d st
ocki
ngs.
DC
H w
ill be
pro
vidi
ng th
e tra
inin
g. F
urth
er m
eetin
gs a
re in
pla
ce to
dis
cuss
impr
oved
use
of v
olun
tary
sec
tor a
nd
supp
ort f
or p
atie
nts
to re
turn
hom
e. A
Dis
char
ge p
roje
ct p
lan
is in
pla
ce, w
hich
incl
udes
trai
ning
for a
ll w
ards
. Th
e co
nten
t of t
his
train
ing
incl
udes
trai
ning
del
iver
ed b
y th
e C
hapl
ain
in d
eliv
erin
g di
fficu
lt m
essa
ges
as w
ell a
s up
date
s on
CH
C, M
CA
and
ther
apy
unit.
CH
S (s
elf-f
unde
rs) –
is n
ow li
ve, t
his
is a
pilo
t sch
eme
for e
nhan
ced
supp
ort f
or s
elf-f
unde
rs is
due
to b
e in
pla
ce fr
om 3
0th
Janu
ary
2017
unt
il 30
th J
une
2017
. Th
is is
ant
icip
ated
to re
duce
sel
f-fun
ding
del
ays
by 5
0% (c
urre
nt D
CH
bas
elin
e is
10
days
, C
HS
targ
et is
5 d
ays)
. Int
erim
revi
ew o
f pilo
t has
bee
n la
rgel
y po
sitiv
e, w
ith d
elay
s re
duce
d by
app
roxi
mat
ely
50%
(dep
ende
nt
upon
met
hodo
logy
use
d).
Indi
cativ
e sa
ving
s as
com
pare
d to
ben
chm
arke
d p
erio
ds h
ave
been
sig
nific
ant a
s w
ell.
Pat
hway
s - F
railt
y pa
thw
ay h
as b
een
draf
ted
at a
hig
h le
vel,
anot
her m
eetin
g ha
s be
en c
ompl
eted
with
acu
te p
hysi
cian
s, s
ocia
l se
rvic
es a
nd o
ther
par
tner
s. D
iscu
ssio
n w
ith p
rimar
y ca
re/c
omm
unity
ser
vice
s is
pla
nned
for t
he th
ird w
orks
hop
(tbc)
. EoL
di
scha
rge
path
way
has
bee
n co
mpl
eted
in d
raft.
Com
plex
dis
char
ge p
athw
ays
will
com
men
ce in
Feb
ruar
y 20
17.
A C
are
Hom
e Fo
rum
has
bee
n ar
rang
ed fo
r 5th
Apr
il in
volv
ing
resi
dent
ial,
nurs
ing
and
dom
icilia
ry c
are
prov
ider
s fo
llow
ing
an
initi
al m
eetin
g in
Nov
embe
r. P
rovi
ders
will
be in
vite
d in
to m
eet W
ard
Sis
ters
and
bui
ld re
latio
nshi
ps to
sup
port
proa
ctiv
e di
scha
rge
path
way
s fo
r pat
ient
s. T
his
mee
ting
was
ver
y su
cces
sful
, with
sev
eral
car
e ho
mes
and
pro
vide
rs re
pres
ente
d. T
his
prov
ided
a fo
rum
for o
pen
and
frank
dis
cuss
ion
and
shar
ing
lear
ning
whi
ch is
bei
ng s
hare
d vi
a S
iste
rs’ m
eetin
gs.
Incr
ease
d de
man
ds o
n D
CH
ser
vice
s an
d po
or p
atie
nt e
xper
ienc
e ar
isin
g fro
m in
effe
ctiv
e lin
ks b
etw
een
com
mun
ity a
nd a
cute
ser
vice
pro
visi
on -
resu
lting
in in
crea
sed
acce
ss to
acu
te s
ervi
ces
and
dela
yed
disc
harg
ed to
alte
rnat
ive
care
Ris
k S
tate
men
tLe
ad M
anag
er
Cor
pora
te R
isk
Reg
iste
r
Page 73 of 132

Ref
CU
RR
EN
T R
ISK
R
ATI
NG
12H
IGH
RIS
K
1051
V3
01/1
2/20
16P
revi
ous
Rat
ing
Ris
k M
anag
emen
t P
lan
& T
imes
cale
PO
ST
MIT
IGA
TIO
N
RA
TIN
G5
MO
DER
ATE
RIS
K
Add
ed to
Ris
k R
egis
ter
Pro
gres
s R
epor
t
Lead
Man
ager
The
Trus
t has
a S
EP
SIS
gro
up w
hich
coo
rdin
ates
wor
k ac
ross
the
orga
nisa
tion
on th
is to
pic.
The
NIC
E
guid
elin
es p
ublis
hed
July
201
6 ar
e be
ing
revi
ewed
to in
form
loca
l pol
icy
and
it is
the
inte
ntio
n of
they
gr
oup
to la
unch
a n
ew T
rust
gui
delin
e to
refle
ct N
ICE
gui
danc
e w
ith s
cree
ning
tool
in S
epte
mbe
r 201
6.
The
curre
nt e
duca
tion
prog
ram
me
is b
eing
revi
ewed
to id
entif
y a
gap
anal
ysis
, with
the
inte
ntio
n of
de
velo
ping
a tr
aini
ng p
lan.
The
grou
p w
ill c
oord
inat
e an
aud
it of
com
plia
nce
with
the
scre
enin
g to
ol fo
r Em
erge
ncy
Adm
issi
ons
and
this
we
be re
peat
ed o
n a
mon
thly
bas
is fr
om O
ctob
er o
nwar
ds 2
016.
To e
nhan
ce th
e m
anag
emen
t and
scr
eeni
ng o
f det
erio
ratin
g pa
tient
s fo
llow
ing
adm
issi
on, w
here
sep
sis
may
be
the
mai
n or
con
tribu
ting
fact
or, M
atro
ns a
re to
revi
ew th
e sa
fety
han
dove
r pro
cess
, to
incl
ude
a sy
stem
atic
app
roac
h to
iden
tifyi
ng p
oten
tially
sep
tic p
atie
nts
(e.g
. Vita
lPA
C o
verv
iew
scr
een)
.
To e
nsur
e ac
cura
cy o
f the
dat
a us
ed to
mea
sure
per
form
ance
the
grou
p w
ill o
vers
ee a
revi
ew o
f the
cl
inic
al c
odin
g fo
r acc
urac
y an
d de
velo
p pr
opos
al w
ith c
linic
ians
.
Dr R
uth
Thom
as,
Anne
Sm
ith, S
haro
n M
oone
y
01/0
8/20
16
Ris
k S
tate
men
t
12 The
Trus
t is
mai
ntai
ning
the
Sep
sis
grou
p, w
hich
ove
rsee
s w
ork
on th
is
topi
c ac
ross
the
Trus
t.
New
nat
iona
l gui
danc
e ha
s be
en p
ublis
hed
and
this
is b
eing
revi
ewed
to
ensu
re th
at T
rust
gui
delin
es re
flect
the
mos
t up
to d
ate
posi
tion
and
the
scre
enin
g to
ol u
sed
for s
epsi
s is
em
bedd
ed in
to p
ract
ice.
The
edu
catio
n pr
ogra
mm
e is
bei
ng re
view
ed to
ens
ure
that
enh
ance
men
ts c
an b
e m
ade
and
impr
ove
awar
enes
s.
Ris
k S
tate
men
tR
isk
of a
void
able
dea
th o
r sev
ere
/ pro
long
ed il
l hea
lth to
pat
ient
s du
e to
del
ays
in re
cogn
ition
&
diag
nosi
s of
sep
sis
and
failu
re to
com
men
ce a
ppro
pria
te e
arly
trea
tmen
t pat
hway
s, a
risin
g fro
m li
mite
d aw
aren
ess
and
effe
ctiv
e to
ols
to a
ssis
t clin
icia
ns in
this
dia
gnos
is
Ver
sion
Seps
is: r
ecog
nitio
n, d
iagn
osis
and
ear
ly m
anag
emen
t
Cor
pora
te R
isk
Reg
iste
r
Page 74 of 132

Ref
CU
RR
EN
T R
ISK
R
ATI
NG
12H
IGH
RIS
K
1052
V3
08/0
3/20
17P
revi
ous
Rat
ing
PO
ST
MIT
IGA
TIO
N
RA
TIN
G5
MO
DER
ATE
RIS
K
Add
ed to
Ris
k R
egis
ter
Ris
k S
tate
men
tLe
ad M
anag
er
Ther
apy
Cap
acity
12
Ris
k S
tate
men
tV
ersi
on
Ther
e ha
s be
en a
sig
nific
ant r
ecru
itmen
t and
rete
ntio
n is
sue
in T
hera
py S
taff
(OT
in p
artic
ular
) rel
atin
g to
va
canc
ies
and
turn
over
. E
stab
lishm
ent o
f The
rapy
Sta
ff ha
s be
en re
view
ed a
nd b
ench
mar
king
pro
vide
d. P
riorit
ies
for t
he T
rust
ar
e to
ach
ieve
the
mai
n ob
ject
ives
to a
) avo
id a
dmis
sion
to h
ospi
tal b
) effe
ctiv
ely
and
timel
y di
scha
rge
from
hos
pita
l.
Pre
cept
orsh
ips:
2 W
TE O
T pr
ecep
tors
recr
uite
d, n
ow s
lotti
ng in
to fu
nded
est
ablis
hmen
t. P
hysi
othe
rapy
pr
ecep
tor r
emai
ns u
nfille
d. H
owev
er, r
ecru
itmen
t offi
ce h
as s
uppo
rted
iden
tific
atio
n of
pot
entia
l ca
ndid
ates
thro
ugh
a re
crui
tmen
t fai
r in
Dub
lin.
• Acc
eler
ator
Pro
gram
me:
in p
lace
and
all
acce
lera
tor p
osts
fille
d.
• Pat
ient
Pat
hway
: mee
tings
cur
rent
ly in
pro
gres
s w
ith D
UH
FT.
Join
t rec
ruitm
ent o
ppor
tuni
ties
disc
usse
d an
d be
ing
deve
lope
d, a
long
side
pot
entia
l for
rota
tion
post
s to
attr
act t
hera
py s
taff
to w
ork
for b
oth
orga
nisa
tions
. D
iscu
ssio
ns w
ith S
ocia
l Ser
vice
s ar
e pl
anne
d, a
lthou
gh th
e po
tent
ial t
o sh
are
rota
ting
post
s is
less
er d
ue to
spe
cial
ism
s in
the
field
.
• Ben
chm
arki
ng: u
nder
take
n w
ith P
GH
and
RB
H. F
urth
er c
ompa
rison
s w
ill b
e m
ade
to D
CH
figu
res
and
furth
er a
naly
sis
of th
e M
odel
Hos
pita
l will
be
unde
rtake
n w
ith s
uppo
rt fro
m th
e fin
ance
team
.
• Cur
rent
ly th
ere
are
no o
utst
andi
ng v
acan
cies
with
in th
e th
erap
y se
rvic
es.
How
ever
, due
to a
vaila
bilit
y of
se
nior
sta
ff, th
e sk
ill m
ix w
ithin
the
serv
ice
has
need
ed to
alte
r to
mee
t dem
ands
in a
diff
eren
t way
.
• Fur
ther
pro
activ
e re
crui
tmen
t pla
nnin
g an
d so
me
agre
emen
t to
risk
over
-est
ablis
hmen
t is
bein
g pl
anne
d in
ord
er to
miti
gate
the
high
turn
over
rate
. F
urth
er w
ork
is b
eing
und
erta
ken
to d
eter
min
e th
e na
tura
l ra
nge
of tu
rnov
er e
xpec
ted
and
any
proa
ctiv
e w
ork
poss
ible
to m
anag
e re
duct
ions
in tu
rnov
er.
• The
out
stan
ding
risk
rem
ains
whe
ther
the
serv
ice
is e
stab
lishe
d to
the
exte
nt re
quire
d to
pro
vide
full
inpa
tient
ser
vice
s. N
o ad
ditio
nal f
undi
ng o
r bus
ines
s ca
se h
as b
een
agre
ed fo
r 201
7/18
to th
is e
nd.
The
OT
benc
hmar
king
has
bee
n co
mpl
eted
, Phy
sio
is b
eing
revi
ewed
. Th
e m
odel
of s
ervi
ce p
rovi
sion
is n
ow
unde
r rev
iew
to d
eter
min
e w
heth
er th
e se
rvic
e ca
n be
pro
vide
d in
an
alte
rnat
ive
way
with
ble
nded
role
s an
d pa
rtner
ship
wor
k w
ith D
orse
t Hea
lth C
are.
Som
e pr
ovis
ion
for f
undi
ng is
pos
sibl
e vi
a th
e be
d m
odel
ling
busi
ness
cas
e, if
app
rove
d.
31/0
8/20
16
Chr
istin
a C
ollin
s-G
ilchr
ist
Kar
yn S
tew
art D
odd
Pro
gres
s R
epor
tR
isk
Man
agem
ent
Pla
n &
Tim
esca
le1.
Incr
easi
ng C
apac
ity
a) R
ecru
it O
ver E
stab
lishm
ent:
Pla
ns a
re in
pla
ce to
incr
ease
cap
acity
by
over
re
crui
ting
on c
urre
nt e
stab
lishm
ent l
evel
s by
mea
ns o
f a P
rece
ptor
ship
P
rogr
amm
e. T
o da
te 2
WTE
OTs
wer
e ap
poin
ted
(pla
nned
3.0
0wte
OT
and
1.00
wte
PT)
. Fin
al y
ear s
tude
nts
are
empl
oyed
as
Ban
d 3’
s an
d th
en u
pgra
ded
to
Ban
d 5’
s on
ce th
ey h
ave
been
regi
ster
ed.
This
act
ion
now
com
plet
ed.
2. S
taff
Ret
entio
n M
easu
res
a) A
ccel
erat
or P
rogr
amm
e: B
and
5’s
(OT/
PT)
are
bei
ng re
crui
ted
and
then
pr
omot
ed to
Ban
d 6
role
s af
ter 1
2 –
18 m
onth
s on
ce th
eir c
ompe
tenc
ies
have
be
en a
chie
ved.
Thi
s in
crea
ses
the
leve
l of s
kill
mix
and
resi
lienc
e. C
urre
ntly
in
plac
e.
b) R
otat
ions
with
Com
mun
ity S
ervi
ces:
OTs
/PTs
rota
te in
to th
e co
mm
unity
to
incr
ease
ski
ll le
vels
and
to b
uild
rela
tions
hips
to im
prov
e co
mm
unic
atio
n an
d fa
cilit
ate
patie
nt fl
ow. T
rain
ing
and
Sup
ervi
sion
Pro
gram
mes
are
in p
lace
to
max
imis
e st
aff c
apac
ity fo
r ser
vice
del
iver
y
3. P
atie
nt P
athw
ay
a) P
athw
ay P
lann
ing
with
Com
mun
ity a
nd S
ocia
l Car
e is
bei
ng d
evel
oped
to
desi
gn p
atie
nt p
athw
ays
to p
rom
ote
info
rmat
ion
shar
ing
to a
void
adm
issi
ons,
re
duce
LoS
and
saf
e di
scha
rge.
Joi
nt p
osts
are
bei
ng e
xplo
red
e.g.
CO
PD
, S
troke
, Hea
rt Fa
ilure
and
Tra
uma
as th
ese
are
area
s th
at h
ave
high
er th
an
expe
cted
LO
S a
nd re
adm
issi
on ra
tes.
Par
tially
impl
emen
ted
with
ant
icip
atio
n of
S
ocia
l Ser
vice
s in
volv
emen
t. b)
Ser
vice
Inte
grat
ion:
OT
and
PT
team
s w
ill b
e fu
lly in
tegr
atin
g to
incr
ease
pr
oduc
tivity
and
con
tinui
ty o
f ser
vice
del
iver
y.
4. B
ench
mar
king
a) T
o ill
ustra
te a
nd e
vide
nce
benc
hmar
king
of T
hera
py S
taff
in li
ne w
ith
obje
ctiv
es a
) adm
issi
on a
void
ance
b) e
ffect
ive
and
timel
y di
scha
rge
from
hos
pita
l us
ing
othe
r loc
al h
ospi
tals
and
Mod
el H
ospi
tal e
vide
nce
to p
rovi
de c
ompa
rabl
e.
This
will
be
achi
eved
with
in th
e ne
xt 6
mon
ths.
Cor
pora
te R
isk
Reg
iste
r
Page 75 of 132

Ref
CU
RR
EN
T R
ISK
R
ATI
NG
12H
IGH
RIS
K
1060
V1
05/0
5/20
17P
revi
ous
Rat
ing
PO
ST
MIT
IGA
TIO
N
RA
TIN
G6
MO
DER
ATE
RIS
K
Add
ed to
Ris
k R
egis
ter
NE
WTe
mpo
rary
Med
ical
Wor
kfor
ce P
lann
ing
& C
apac
ity
The
Trus
t rec
ently
mad
e tw
o si
gnifi
cant
inve
stm
ents
to im
prov
e bo
th
recr
uitm
ent a
nd te
mpo
rary
sta
ffing
:• T
he a
ppoi
ntm
ent o
f a B
and
5 Te
am M
anag
er fo
r Med
ical
Rec
ruitm
ent
adds
sig
nific
ant c
apac
ity fo
r cam
paig
n de
sign
and
del
iver
y, v
acan
cy
mon
itorin
g an
d th
e de
velo
pmen
t of n
ew re
crui
tmen
t med
ia (e
.g. C
aree
rs
Tran
sitio
n P
artn
ersh
ip, B
MJ
Jobs
, Gua
rdia
n N
etw
ork,
Lin
kedI
N e
tc.).
The
di
visi
ons
are
now
act
ing
proa
ctiv
ely
to a
ddre
ss k
now
n ga
ps in
CM
Ts
thro
ugh
the
recr
uitm
ent o
f LA
S a
nd M
TI c
over
. Thi
s ac
tivity
will
be
supp
orte
d w
ith c
opy-
writ
ten
adve
rtisi
ng a
nd re
crui
tmen
t vid
eos.
• T
he T
rust
will
laun
ch th
e Te
mpR
E a
genc
y bo
okin
g sy
stem
on
24 A
pril,
w
orki
ng w
ith L
iais
on a
nd th
e H
TE. F
ram
ewor
k to
acc
ess
a la
rger
sup
plie
r ba
se in
a ti
mel
y an
d ef
ficie
nt m
anne
r. Th
e ne
w H
ead
of W
orkf
orce
Res
ourc
ing,
join
ing
in M
ay 2
017,
has
ex
tens
ive
Med
ical
HR
and
Rec
ruitm
ent e
xper
ienc
e w
ithin
the
Lond
on
mar
ket.
It is
ant
icip
ated
that
this
will
sig
nific
antly
stre
ngth
en th
e M
edic
al
recr
uitm
ent p
lans
for 2
017-
18
Ris
k S
tate
men
tV
ersi
on
Ris
k S
tate
men
tLe
ad M
anag
erTB
D
1. J
ane
Whi
te –
Med
ical
Rec
ruitm
ent T
eam
Man
ager
, in
post
from
1 A
pril
2017
2. M
edic
al V
acan
cy L
ist w
ith c
omm
enta
ry p
ublis
hed
wee
kly
from
1 A
pril
2017
3. H
TE. F
ram
ewor
k liv
e in
Mar
ch 2
017
4. T
empR
E li
ve fr
om 2
4 A
pril
2017
5. M
edic
al fo
cuse
d H
ead
of W
ork
Res
ourc
ing
in p
ost f
rom
8 M
ay 2
017
05/0
5/20
17
Inab
ility
to s
ourc
e ap
prop
riate
ly s
kille
d an
d co
mpe
tent
sta
ff to
mee
t sho
rt te
rm re
quire
men
ts fo
r te
mpo
rary
sta
ffing
Pro
gres
s R
epor
tR
isk
Man
agem
ent
Pla
n &
Tim
esca
le
Cor
pora
te R
isk
Reg
iste
r
Page 76 of 132

Ref
CU
RR
EN
T R
ISK
11
HIG
H R
ISK
1041
V3
01/1
2/20
16P
revi
ous
Rat
ing
PO
ST
MIT
IGA
TIO
N
RA
TIN
G5
MO
DER
ATE
RIS
K
Add
ed to
Ris
k R
egis
ter
27/1
0/20
15
Ris
k M
anag
emen
t P
lan
& T
imes
cale
A w
orki
ng g
roup
was
com
men
ced
in 2
014
to o
vers
ee w
ork
stre
ams
that
ar
e in
tend
ed to
ens
ure
that
sta
ff w
ho h
ave
iden
tifie
d a
train
ing
requ
irem
ent i
n re
latio
n to
the
use
of m
edic
al d
evic
es re
ceiv
e th
e ne
cess
ary
train
ing
and
that
the
prop
ortio
n of
sta
ff re
quiri
ng tr
aini
ng is
m
aint
aine
d in
a s
imila
r way
to o
ther
man
dato
ry tr
aini
ng p
rogr
amm
esLi
mite
d tra
inin
g ha
s be
en d
eliv
ered
to e
xist
ing
staf
f dur
ing
2015
/16
and
a re
view
of t
he p
ositi
on u
nder
take
n to
out
line
next
ste
ps. M
anda
tory
trai
ning
m
onito
red
at D
ivis
iona
l Per
form
ance
revi
ews.
Ris
k S
tate
men
tLe
ad M
anag
erAn
dy M
orris
, Hea
d of
Est
ates
& F
acili
ties
Fran
k W
illia
ms,
Hea
d of
Med
ical
Eng
inee
ring
Ris
k S
tate
men
t11
.2V
ersi
onM
edic
al D
evic
e M
anag
emen
t - T
rain
ing
Pot
entia
l leg
isla
tive
impa
ct a
nd s
afet
y co
ncer
ns a
risin
g fro
m s
taff
not b
een
appr
opria
tely
trai
ned
in th
e us
e of
Med
ical
Dev
ices
. Pot
entia
l dis
rupt
ion
to s
ervi
ces
if st
aff u
nabl
e to
use
med
ical
dev
ices
unt
il th
ey
are
adeq
uate
ly tr
aine
d.
Pro
gres
s R
epor
t
An
urge
nt w
orki
ng g
roup
was
com
men
ced
to fo
cus
wor
k on
ens
urin
g th
at a
ssur
ance
can
be
gain
ed
rega
rdin
g tra
inin
g in
med
ical
dev
ices
acr
oss
the
orga
nisa
tion.
A s
uite
of t
rain
ing
prog
ram
mes
has
bee
n la
unch
ed fo
r all
devi
ce u
sers
. All
new
sta
rters
will
atte
nd th
is tr
aini
ng a
s pa
rt of
thei
r ind
uctio
n. A
se
cond
men
t pos
t fo
r a M
edic
al D
evic
e Tr
aini
ng C
oord
inat
or w
ill co
mm
ence
in D
ecem
ber 2
016.
The
y w
ill be
trai
ned
on th
e ne
w a
sset
man
agem
ent s
yste
m F
2 an
OLM
(ES
R).
The
ir pr
imar
y ta
sks
will
be
to
com
pile
a s
tand
ardi
sed
train
ing
repo
rt te
mpl
ate
and
popu
late
OLM
with
the
up to
dat
e m
edic
al d
evic
es
train
ing.
The
sta
ndar
dise
d tra
inin
g re
port
tem
plat
e w
ill be
sub
mitt
ed to
the
Med
ical
Dev
ices
Com
mitt
ee
for a
ppro
val.
Onc
e th
e te
mpl
ate
is a
ppro
ved,
repo
rts fo
r all
the
othe
r war
ds w
ill b
e pr
oduc
ed.
With
the
war
d re
ports
, tra
inin
g of
con
cern
can
be
tack
led
with
spe
cific
cou
rses
, as
requ
ired.
The
cur
rent
mon
thly
tra
inin
g co
urse
is e
xpec
ted
to c
ontin
ue th
roug
h 20
17.
A
Med
ical
Dev
ices
Tra
inin
g C
oord
inat
or s
econ
dmen
t will
be
in p
ost a
s of
12t
h D
ecem
ber 2
016.
The
y w
ill
be tr
aine
d on
the
new
ass
et m
anag
emen
t sys
tem
F2
and
OLM
(ES
R).
Thei
r prim
ary
task
s w
ill b
e to
co
mpi
le a
sta
ndar
dise
d tra
inin
g re
port
tem
plat
e, a
nd p
opul
ate
OLM
with
the
up to
dat
e m
edic
al d
evic
e tra
inin
g re
cord
s. T
he s
tand
ardi
sed
train
ing
repo
rt te
mpl
ate
will
be s
ubm
itted
to th
e M
edic
al D
evic
es
Com
mitt
ee fo
r app
rova
l. O
nce
the
tem
plat
e is
app
rove
d, re
ports
for a
ll th
e ot
her w
ards
will
be
prod
uced
. W
ith th
e w
ard
repo
rts, t
rain
ing
of c
once
rn c
an b
e ta
ckle
d w
ith s
peci
fic c
ours
es, a
s re
quire
d. T
he c
urre
nt
mon
thly
trai
ning
cou
rse
is e
xpec
ted
to c
ontin
ue th
roug
h 20
17. W
e ha
ve s
tarte
d th
e im
plem
enta
tion
actio
n pl
an to
pro
duct
the
new
risk
/ass
uran
ce b
ased
med
ical
dev
ices
trai
ning
dat
abas
e, th
e cu
rrent
Saf
e us
e of
M
edic
al d
evic
es p
olic
y is
und
er re
view
to in
corp
orat
e th
e ch
ange
s ne
cess
ary.
The
new
med
ical
dev
ices
tra
inin
g co
-ord
inat
or is
in p
ost a
nd is
bei
ng tr
aine
d to
ope
rate
ES
R/O
LM a
long
side
the
new
ass
et
man
agem
ent s
yste
m F
2. T
he n
ew c
ombi
ned
syst
em w
ill be
test
ed o
n Fo
rtune
swel
l war
d an
d th
e re
ports
ge
nera
ted
repo
rted
up to
the
Med
ical
dev
ices
com
mitt
ee in
Mar
ch 2
017
for a
ppro
val b
efor
e ro
lling
out t
he
new
sys
tem
Tru
st w
ide.
We
have
test
ed s
ever
al o
f the
key
com
pone
nts
of th
e in
tegr
ated
trai
ning
pa
ckag
e de
velo
ped
by m
edic
al e
ngin
eerin
g th
e M
edic
al d
evic
e tra
inin
g co
-ord
inat
or h
as p
rove
d se
vera
l of
the
links
to E
SR
/OLM
that
com
bine
with
the
med
ical
dev
ices
inve
ntor
y. T
he a
ctio
n pl
an h
as b
een
upda
te.
The
final
pro
cess
is th
e st
art o
f F2
the
new
ass
et m
anag
emen
t sys
tem
whi
ch is
pla
nned
for t
he 2
nd w
eek
in M
arch
this
will
giv
e us
the
repo
rting
func
tions
. The
roll
out w
ill th
en ti
e- in
with
the
new
hyb
rid m
attre
ss
syst
em a
cros
s th
e su
rgic
al d
ivis
ion
durin
g A
pril
may
Jun
e A
ctio
n pl
an a
ttach
ed.
Cor
pora
te R
isk
Reg
iste
r
Page 77 of 132

Ref
CU
RR
EN
T R
ISK
R
ATI
NG
10H
IGH
RIS
K
1047
V4
22/0
2/20
17P
revi
ous
Rat
ing
Lead
Man
ager
Ris
k M
anag
emen
t P
lan
& T
imes
cale
PO
ST
MIT
IGA
TIO
N
6M
OD
ERAT
E R
ISK
Add
ed to
Ris
k R
egis
ter
Ris
k S
tate
men
t
10.4
Ver
sion
1) R
ecru
itmen
t eve
nts
are
plan
ned
thro
ugho
ut th
e co
urse
of t
he fo
llow
ing
year
and
hav
e pr
ovid
ed li
mite
d su
cces
s.
Atte
ndan
ce a
t Uni
vers
ity o
pen
days
has
yie
lded
a g
ood
resp
onse
with
man
y ne
wly
qua
lifie
d st
aff c
urre
ntly
offe
red
posi
tions
with
in th
e Tr
ust.
2)
Exp
lora
tion
of th
e ba
nd 4
'Ass
ocia
te N
urse
' pos
t is
prog
ress
ing
and
a re
view
of t
he
Job
desc
riptio
ns fo
r ban
d 2
and
band
3 H
ealth
Car
e A
ssis
tant
s be
ing
unde
rtake
n to
ens
ure
effe
ctiv
e us
e of
re
sour
ces.
3) A
ltern
ativ
e sk
ill m
ixes
and
mod
els
of w
orki
ng a
re b
eing
pro
gres
sed
to e
nsur
e th
at th
e Tr
ust i
s ab
le to
su
stai
n an
d pr
ovid
e se
rvic
es in
the
long
er te
rm.
Iden
tific
atio
n of
sta
ff gr
oup
who
hav
e cu
rrent
regi
stra
tion
outs
ide
of th
e U
K.
4) Id
entif
icat
ion
of w
hat s
uppo
rt th
e Tr
ust c
ould
offe
r in
orde
r for
them
to g
ain
NM
C re
gist
ratio
n.
The
Trus
t has
est
ablis
hed
robu
st p
roce
sses
to re
view
recr
uitm
ent
(the
Res
ourc
ing
Stra
tegy
Boa
rd) a
nd te
mpo
rary
sta
ffing
(the
R
esou
rcin
g O
pera
tions
Gro
up) T
he T
rust
’s o
bjec
tive
is to
min
imis
e ag
ency
cos
ts th
roug
h in
crea
sed
subs
tant
ive
recr
uitm
ent,
whe
re
nece
ssar
y su
ppor
ted
by a
genc
y/se
arch
pro
vide
rs.
Initi
ativ
es h
ave
been
und
erta
ken
to e
ncou
rage
app
licat
ions
to s
ubst
antiv
e po
sitio
ns
such
as
relo
catio
n co
sts
incl
uded
, pro
visi
on o
f rot
atio
nal p
osts
for
care
er d
evel
opm
ent,
Nat
iona
l rec
ruitm
ent e
vent
s an
d th
e de
velo
pmen
t of a
robu
st P
rece
ptor
ship
pro
gram
me
for n
ewly
qu
alifi
ed s
taff.
08/1
0/20
15
Wor
kfor
ce P
lann
ing
& C
apac
ity fo
r Nur
sing
/Mid
wife
ry S
taff
Andr
ew B
lake
sley
, Nea
l Cle
aver
Inab
ility
to s
ourc
e ap
prop
riate
ly s
kille
d an
d co
mpe
tent
sta
ff to
mee
t req
uire
men
ts fo
r Nur
sing
/ Mid
wife
ry s
taffi
ng
Cor
pora
te R
isk
Reg
iste
r
Page 78 of 132

Ref
CU
RR
EN
T R
ISK
R
ATI
NG
10H
IGH
RIS
K
1050
V3
01/1
2/20
16P
revi
ous
Rat
ing
Lead
Man
ager
Ris
k M
anag
emen
t P
lan
& T
imes
cale
PO
ST
MIT
IGA
TIO
N
4M
OD
ERAT
E R
ISK
Add
ed to
Ris
k R
egis
ter
Ver
sion
Mor
talit
y In
dica
tor
Ris
k S
tate
men
t
9.6 Div
isio
nal D
irect
ors
Pot
entia
l for
incr
ease
d m
orta
lity
in p
atie
nts
acce
ssin
g se
rvic
es a
t DC
H d
ue to
out
lyin
g st
atus
of S
HM
I and
HS
MR
m
easu
res
NH
S E
ngla
nd u
tilis
es th
e S
umm
ary
Hos
pita
l-lev
el M
orta
lity
Indi
cato
r (S
HM
I) an
d th
e H
ospi
tal S
tand
ardi
sed
Mor
talit
y R
atio
(HS
MR
). Th
ese
are
colle
cted
from
dat
a pu
blis
hed
by a
ll Tr
usts
in re
latio
n to
pat
ient
s tre
ated
. The
dat
a in
dica
tes
that
DC
H is
an
outli
er in
term
s of
the
num
ber o
f pat
ient
s w
ho d
ie d
urin
g, o
r in
the
perio
d fo
llow
ing,
car
e at
th
e ho
spita
l, w
hen
com
pare
d to
sim
ilar o
rgan
isat
ions
.
An
inde
pend
ent r
evie
w o
f the
dat
a su
bmitt
ed to
the
natio
nal d
atas
et h
as b
een
unde
rtake
n an
d an
act
ion
plan
has
be
en d
evel
oped
to a
ddre
ss th
e is
sues
hig
hlig
hted
. The
re a
re c
once
rns
abou
t the
acc
urac
y of
the
codi
ng a
pplie
d to
th
e pa
tient
dat
a su
bmitt
ed b
y th
e Tr
ust,
whi
ch c
ould
be
impa
ctin
g on
the
data
.
In a
dditi
on to
con
cern
s ab
out d
ata
accu
racy
, the
pub
lishe
d da
ta a
ppea
rs to
sug
gest
that
pat
ient
s ad
mitt
ed to
DC
H
at w
eeke
nds
have
a g
reat
er ri
sk o
f mor
talit
y w
hen
com
pare
d to
thos
e ad
mitt
ed d
urin
g a
wee
kday
.Th
e Tr
ust h
as in
trodu
ced
a M
orta
lity
Sur
veill
ance
Gro
up, l
ed b
y th
e M
edic
al D
irect
or -
whi
ch w
ill re
view
the
care
of
patie
nts
who
die
in h
ospi
tal,
or w
ho d
ie w
ithin
a d
efin
ed p
erio
d of
dis
char
ge. T
his
will
pro
vide
ass
uran
ce re
gard
ing
the
natio
nal m
orta
lity
data
and
will
pro
vide
a m
ore
resp
onsi
ve e
scal
atio
n of
any
con
cern
s re
latin
g to
car
e.
An
exte
rnal
revi
ew o
f mor
talit
y da
ta, i
nclu
ding
the
codi
ng
info
rmat
ion
used
for s
ubm
issi
on to
the
natio
nal d
atas
et h
as b
een
com
plet
ed a
nd a
n ac
tion
plan
has
bee
n de
velo
ped
to a
ddre
ss th
e is
sues
rais
ed. I
ssue
s re
gard
ing
the
accu
racy
of c
odin
g in
form
atio
n ha
ve b
een
high
light
ed a
nd a
revi
ew o
f pro
cess
is b
eing
und
erta
ken
by th
e C
hief
Info
rmat
ion
Offi
cer -
this
exp
ecte
d to
hav
e re
porte
d an
d ch
ange
s im
plem
ente
d du
ring
Q1
16/1
7.Th
e M
edic
al D
irect
or
cont
inue
s to
revi
ew a
ll ca
ses
whe
re a
pat
ient
has
die
d du
ring
or
afte
r car
e at
DC
H a
nd th
e C
OO
is s
uppo
rting
a re
view
of t
hem
es
and
trend
s. A
s th
e na
tiona
l dat
aset
is re
porte
d re
trosp
ectiv
ely,
it is
an
ticip
ated
that
no
imm
edia
te c
hang
es to
the
natio
nal i
ndic
ator
s w
ill
be s
een
until
Q3
of 2
016/
17.T
he T
rust
has
intro
duce
d of
a M
orta
lity
Sur
veill
ance
Gro
up, l
ed b
y th
e M
edic
al D
irect
or -
whi
ch w
ill re
view
al
l dea
ths
whi
ch o
ccur
in h
ospi
tal o
r fol
low
ing
a de
fined
per
iod
afte
r di
scha
rge.
Thi
s w
ill p
rovi
de a
ssur
ance
of t
he m
orta
lity
data
by
iden
tifyi
ng a
ctua
l cas
es w
here
car
e ne
eds
to b
e re
view
ed.
29/0
2/20
16
Cor
pora
te R
isk
Reg
iste
r
Page 79 of 132

Board Assurance Framework (BAF) 2015/16
Strategic Objective Priorities Principal Risk Risk Owner Key Controls Sources of assuranceGaps in
control/assuranceActions for addressing gaps
RAG
Rating
Failure to engage staff in an
integrated care model
J Pearce/
M Warner
Engagement programme planned
with staff. Strategic direction for the
organisation embedded within the
Leadership development
programme.
Staff Survey
Survey Monkey
Approach to staff engagement
based on delivery of the People
Strategy, recognising that staff
engagement is a long term
endeavour.
Amber
Pace of change of the Dorset
wide review too slow.
P Miller
Executive membership on Dorset
wide review group.
Dorset STP being identified as an
early implementer
NHSE - external
assurance
Exec meetings
SMT
Trust Board
Public consultation
now delayed until
November 2016
Acute providers are now a
ACC vanguard site in order to
move the acute care
reconfiguration forward at
pace. STP operational delivery
plan in development. Further
work required on the
sequencing of key
workstreams to ensure
financial sustainability of the
provider landscape
Amber
CSR deters open
engagement with other
Trusts.
J Pearce
Dorset Cluster meetings to continue
throughout the CSR. Accountable
Care partnership meetings
established to enable and
encourage whole system
approaches to implementing the
Integrated Community Services
component of the CSR.
Exec meetings
SMT
Trust Board
CSR work-stream on
developing integrated
community services
has now started and
will form an important
part of the STP for the
county. High level
modelling only and
assurance around
predicted activity and
cost shifts not detailed
enough to provide the
assurance.
Initial meeting held to scope
Accountable Care Partnership
for West Dorset. Initial meeting
of the Accountable Care
partnership has happened and
a programme of work is being
developed to focus initially on
admission avoidance and
reducing delayed transfers of
care. It will also begin to
explore implementation of the
CSR-ICS; ICS major
component of the public
consultation to commence in
Autumn 2016. CCG due
diligence has been undertaken
and agreed with NHS-E
Green
(3) To strengthen relationships
with primary care, supporting
the sustainability and
education of the sector
Gaining access to GPs who
don't readily engage with the
Trust.
P Lear
Stakeholder engagement plan to be
developed.
Exec meetings
SMT
Trust Board
The Chair of the Medical
Staffing Committee has
established a GP and
consultant network forum
which will hold its first meeting
in March and meet bimonthly
thereafter
Develop a GP Engagement
Programme with a named
programme manager
Mid-Dorset hub project building
relationships with all mid-
Dorset GPs.
Amber
Board Assurance Framework - as at end March 2017
INTEGRATEDJoining up our services
We will drive forward more
joined up patient pathways,
particularly working more
closely with and supporting
GPs
(1) To work with our partners
to establish an Accountable
Care Partnership to develop
shared care pathways and a
holistic care approach for our
patients and deliver care
closer to home
1
BAF
Page 80 of 132

Board Assurance Framework (BAF) 2015/16
Board Assurance Framework - as at end March 2017(4) To work with our acute
Care Collaborative vanguard
partners to deliver outstanding
services which reflect the
needs of our local populations
Failure to deliver the objective
of the Acute Care vanguard
Programme
P Miller
Vanguard Governance Structure in
place.
- Vanguard Executive
Management Steering
Group
- Chairs and Chief
Executives Group
- External assurance via
NHS England
- Integration and
Collaboration Board
- No dedicated DCH
Programme
Manager/Lead
- Vanguard PMO now in place
led by a Programme Director.
Reasonable progress being
made against core work
streams. SOC agreed for
Pathology and SOC for stroke
services expected in Oct/Nov.
SOC for Health Informatics
approved Jan 17
Amber
(5) To strengthen links
between health and social
care and mental health
providers to provide joined-up
services
Failure to engage social care
and Mental health providers in
service design and
development
J Pearce
- Standardised service
development methodology
- Engagement through Accountable
Care Partnership programme
- Newly formed
Integration and
Transformation Group
- No
project/programme
structure in place.
Dorset-wide System
leadership team to
agree the toR for the
ACO/ACP and the
scope of involvement
in the implementation
of the ICS component
of the CSR. Integrated
community and primary
care services steering
group set up by CCG
ToR for ACP to be re-reviewed
to ensure clarity of purpose
and the development of an
overall project plan. System
awaiting clarification from SLT
on the approach to ACO/ACS
and the alignment to local
authority boundaries
Amber
(6) To establish a
comprehensive transformation
programme for our services
focussed on co-design and
outcomes
Not being able to deliver
transformational savings at a
fast enough pace to
safeguard quality and secure
efficiency and productivity
gains.
L Walters/
J Pearce/ N Lucey
Integration & Collaboration
Transformation Board in place
Service Transformation Group in
place.
Quality impact assessments to be
developed.
Better Value, Better Care Board in
place. Executive team providing
extra support and challenge to key
areas of CIP programme
Reports through to FPC Project management to
be strengthened.
Quality assurance to
be embedded.
Insufficient capability
and capacity to take
the savings out at the
scale and pace
required.
Quality impact assessment to be
embedded. Better Value, Better
Care Board in place. Quality impact
to be embedded into the CIP
reporting - completed. Review of
capacity and capability requirements
to be undertaken. Structure and
resources required to deliver the
Improvements and savings being re-
reviewed, capability & capacity
challenges needs to be addressed.
CIP Programme manager post
vacant and an alternative solution
being identified. Head of
Transformation appointed.
Red
COLLABORATIVEWorking with our
patients and partners
We will work with all of our
partners across Dorset to co-
design and deliver efficient
and sustainable patient-
centred, outcome focussed
services
2
BAF
Page 81 of 132

Board Assurance Framework (BAF) 2015/16
Board Assurance Framework - as at end March 2017Not having safe staffing levels
through national skill
shortages, inadequate
workforce planning and local
recruitment challenges.
Additional pressures on
medical staffing as a result of
new junior doctor contract.
P Lear/
J Pearce
M Warner
HR co-ordinate the production of
two and five-year workforce plans
which are updated on annual basis.
Divisions report on workforce
planning and recruitment issues at
monthly performance meetings.
Periodic review of worksorce issues
at FPC.
Established a Resourcing
Strategy group to look at
longer term resourcing
plans.
Twice yearly dependency
audit for nursing.
Systematic dependency
review carried out in the
latter part of 2015/16 and
recommendations for
investment presented to
SMT,FPC and Trust
Board.
Junior doctor exception
reporting and GOSW
Board report.
Nursing & Midwifery
establishment review
identified some areas
of mis-match between
the ward establishment
and the acuity (level of
care) and dependency
(nursing workload) in
some key areas of the
Trust including ED,
Medical and Surgical
Assessment Units,
Maternity Unit and
Children's ward.
Medical gaps through
low resiliance in
medical establishment,
or know areas of hard
to fill medical roles.
E-rostering to be used to
produce accurate information
for robust workforce planning
to be undertaken. Develop new
models of care with different
skills mix, to address hard to fill
medical middle grade posts.
Divisons highlighting plans for
skill mix changes and
development as part of annual
business planning cycle.
Development of longer term
workforce plans for medical
gaps, and to increase
resiliance.
Six monthly acuity and
dependency review has
highlighted areas for
investment. The case for
change to be presented to
Amber
Availability to fund backfill
training relating to new
models of care.
M Warner
Trust working with HEE Wessex to
ensure availability appropriate
SMT approving new positions.
Annaul budget setting process.
Divisional Governance
Meetings
Locum usage review.
Feedback from GMC
survey.
New junior doctor rotas
have identified a
pressure of medical
rotaos in some
specialties.
Long term medical
vacancies in hard to fill
specialities suggests a
need to invest in new
models of care.
Build into divisional workforce
plans through business
planning process. Seek
support from HEW.
Develop Trust wide approach
to investment in physician
Assistants and ANPs.
Amber
Workforce plans
unaffordable.
M Warner/
L Walters
Workforce plans built into budget
setting
FPC review of workforce plans and
agency usage
Divisional Governance
Meetings
Monthly review of medical
vacancies at SMT and
GOSW reports.
Potential risk in terms
of reduced medical
training posts provided.
Ensure DCH requirements are
fed into HEW commissioning
timetable
Review long terms resourcing
models at Resourcing Strategy
Group
Amber
(8) To review our enabling and
support service to ensure they
support the delivery of our
aims and objectives and meet
the needs of our patients and
staff
Inadequate business support
services to support clinical
services due to significant
savings required as identified
through Carter.
N Johnson
Business support services being
reviewed through the Vanguard
project.
Vanguard workstream
and Executive Steering
Group
Business support services
programme developing with
focus on quality, resilience and
efficiency. Design principles
include focus on service quality
Amber
(7) To implement our "People
Strategy 2015" to develop the
organisation and deliver safe,
effective and compassionate
care
ENABLINGEmpowering our staff
We will engage with our staff
to ensure our workforce is
empowered and fit for the
future
3
BAF
Page 82 of 132

Board Assurance Framework (BAF) 2015/16
Board Assurance Framework - as at end March 2017Poor data quality impacting
on decision making.
L Walters
Information Assurance Group in
place but further work planned to
develop its role. Information
strategy aprpoved by FPC Nov 16.
Overseen by Health Information
Programme Board.
Independent PbR Audit
raised a number of
concerns on the quality of
costing raised and these
have been addressed.
External review has
identified areas for
improving mortality data
and action plan is being
implemented.
IAG to be embedded. Coding group set up to review
quality of coding. Info strategy
approved by Board and
Information Strategy Project
Team commenced its
implementation. Mortality
coding action plan being
implemented. Mortality coding
dashboard developed to
enable impact on actions to be
seen quickly.
Amber
Personal records, including
medical records should be
accurate and kept safe and
confidential.
L Walters
Corporate Records Management
and Information Lifecycle Policy;
Data Protection and Confidentiality
Policy; Health Records Standards
including Retention Schedules
Policy; Information Governance
Strategy and Policy; Information
Risk policy; Information Security
Policy; Safe Haven Policy.
Caldicott Guardian in place. SIRO
identified. Staff training for IGC as
mandatory training.
CQC inspection identified
weaknesses ensuring all
medical records secure in
public areas. Action
taken to address this.
Internal audit on the IG
Toolkit planned 2016/17.
Standardised locked medical
records trollies have been
purchased.
Amber
(10) Implementing a Digital
Care Records for all patients
to ensure safe and efficient
care is provided
Ensuring we can continue to
deliver safe care whilst
implementing Digital Care
RecordsM Sinclair
Programme Project Board and
Team structure in place to oversee
which reports to Health Informatics
Board.
HIPB
Internal audit -
assessment of Significant
Assurance with Minor
Improvement
Opportunities
Governance process to be
embedded.
Amber
(11) To speed up the adoption
of relevant research and
innovation and define our role
within science, education and
training, and research and
development, working with the
AHSN
Loss of opportunities to
improve care and/or reduce
costs through slow adoption
of new technology and
innovative methods
P Lear
Wessex CRN annual overview and
quarterly returns. Funding
determined by recruitment numbers
into non-commercial studies.
Increased activity and
engagement by new
consultants in
Commercial trials
Potential sources of
research income
(diabetes in particular)
show little engagement
The R & D manager is retiring
in March and we have taken
the opportunity to recruit a new
manager from Bournemouth
University which will enhance
DCH working with outside
partners. We have promoted
an internal candidate to take
charge of the day to day
management within the
department.
Amber
ENABLINGEmpowering our staff
We will engage with our staff
to ensure our workforce is
empowered and fit for the
future
(9) To ensure relevant data is
easily accessible, in multiple
locations using technology,
and enabling a culture of
evidence based decision
making
4
BAF
Page 83 of 132

Board Assurance Framework (BAF) 2015/16
Board Assurance Framework - as at end March 2017
(12) To appreciate and further
develop our social
responsibility in the community
Community does not support
the Trust, affecting choice
and contributions
N Johnson
Policies and procedures Exec meetings
SMT
Trust Board
no monitoring of
activity, no guidance
for staff
Current significant support for
DCH from the local and
surrounding communities.
Possible increasing risk
depending upon Maternity and
Peadiatric developments with
Yeovil
Corporate Social Responsibility
Framework still to be
developed.
Amber
(13) Ensuring a safe and
efficient estate is provided to
enable safe service to be
delivered
Harm to patients or staff
A Morris
Policies and procedures
Maintenance programmes and
inspections
Capital Planning Group Development of estates
strategy
Development of estates
masterplan
Development of the Damers
site
Amber
ENABLINGEmpowering our staff
We will engage with our staff
to ensure our workforce is
empowered and fit for the
future
5
BAF
Page 84 of 132

Board Assurance Framework (BAF) 2015/16
Board Assurance Framework - as at end March 2017(14) To embed a culture of
value management and deliver
efficiency projects across the
organisation, using the Carter
principles as a foundation
Savings not optimised or
delivered safely
L Walters
Better Value Better Care Board
overviews this work.
CIP Internal Audit 15/16 Capacity and capability
to deliver at scale.
Service transformation function to be
developed. Finance Improvement
Team in place for 2017/18.
Amber
Loss of core business through
CCG tender exercise
N Johnson
Development of commercial
strategy focussed on increasing non
NHS income
Commercial Board
FPC
Resource to monitor
opportunities
Opportunity Pipeline has been
developed to identify potential
business and possible risks.
Strategy and Business
Development Manager
appointed to monitor pipeline
and provide facilitation for any
bids as they arise.
Currently no anticipated tender
exercises which would affect
core business of the Trust.
Some tenders which Trust
should consider pursuing for
startegic purposes
Green
Investments not resulting in
value for money. L Walters
Business cases approved at SMT
and Board of Directors as outlined
in SFI's.
FPC and Board of
Directors
Post project evaluation not undertaken.Post project evaluation to be
implemented. Amber
Opportunities for services to
be tendered not arising
N Johnson
Executive membership on Dorset
wide review group.
Strong relationships being built with
Commissioners to influence
change.
Commercial Board
FPC
Resource to take
advantage of
opportunities arising
CCG shift away from
competitive tendering.
Collaborative working with
partners is encouraged
Executives to continue to work
with and influence
Commissioners.
Development of opportunity
pipeline to identify future tender
opportunities. Beginning to
see a number of tenders
coming out or due. Do not have
the capacity to bid everything
so will have to be selective
Green
SUSTAINABLEProductive, effective and
efficient
We will ensure we are
productive and efficient in all
that we do to achieve long-
term financial sustainability
(15) To be bold in our
investment strategy to deliver
long-term financial benefit and
sustainability
6
BAF
Page 85 of 132

Board Assurance Framework (BAF) 2015/16
Board Assurance Framework - as at end March 2017Insufficient cash to ensure the
continuity of services.
L Walters
Liquidity strategy in place and
reviewed by FPC.
Daily, weekly, monthly cash flows
taken. Loan facility in place with
NHS England.
Internal audit January
2017 highlighted no cash
management concerns
(rated - significant
assurance with minor
improvement
opportunities).
Formally notified NHS
Improvement of
distressed status. Monitor
undertook a site visit in
March 16 and advised we
apply for central cash
support.
Loan facility in place to use as
required.
Red
(16) To develop our
commercial capacity and
capability, building
partnerships to help achieve
this
Insufficient resources to take
advantage of opportunities to
develop commercial income
streams
N Johnson
Commercial Strategy developed
and resources identified for initial
income target. Stretch targets may
require additional resource
Commercial Board
FPC
Resource in place for PP development as
largest non-NHS income stream
Strategy and BD Manager recruited.
Resources still limited and therefore
capacity to pursue and realise commercial
income streams is limited. Capacity has to
be focussed on key areas. These are:
Private Patient Manager
- Private patients
- overseas patients
Strategy and BD Manager
- Damers development Programme
Management
- Coffee Concession
- Tender pipeline
- Active tenders and imminent- currently
Pharmacy SomPar and DHC, dermatology,
extra care, prisons, Integrated Urgent Care
Advice and Access Service
- Contract management process
Development of Commercial Estates Joint
Venture for Damers development
Amber
Not ensuring the safety,
availability and suitability of
equipment.
L Walters
Medical devised policy in place.
Regular reporting of compliance
with maintenance and training
reviewed at Medical Devices
Committee
Internal audit undertaken
2014/15. Limited
assurance given.
A lack of resilience in
the provision of
equipment training.
New system being
implemented Q3 2016/17.
Medical device training post
recruited to. Training audit to
be undertaken Q4 2016/17 and
full training programme and
recording to be in place Q1
2017/18. A review of all
departments responsible for
medical devices has taken
place and an action plan is
being developed to address a
number of gaps.
Amber
SUSTAINABLEProductive, effective and
efficient
We will ensure we are
productive and efficient in all
that we do to achieve long-
term financial sustainability
(17) To drive value from our
assets, in particular our
estates and property, and
enhance the patient
experience
(15) To be bold in our
investment strategy to deliver
long-term financial benefit and
sustainability
7
BAF
Page 86 of 132

Board Assurance Framework (BAF) 2015/16
Board Assurance Framework - as at end March 2017Trust being open to fraud.
L Walters
Counter Fraud contract in place
with external provider.; Annual fraud
plan in place based on risk
assessment;
Regular reports to the Audit
Committee; Local Counter Fraud
and Corruption Policy: Regular
report to Audit Committee.
Internal audit 2014/15
gave adequate assurance
on the main accounting
system.
Work still to be
undertaken in respect
of cyber security
Amber
SUSTAINABLEProductive, effective and
efficient
We will ensure we are
productive and efficient in all
that we do to achieve long-
term financial sustainability
(17) To drive value from our
assets, in particular our
estates and property, and
enhance the patient
experience
8
BAF
Page 87 of 132

Board Assurance Framework (BAF) 2015/16
Board Assurance Framework - as at end March 2017Not achieving required
standard of cleanliness and
robust infection control
practice, to ensure people are
cared for in a clean and safe
environment, therefore
reducing the risk of hospital
acquired infections.
N Lucey
Infection Prevention and Control
Committee reports to the Clinical
Governance Committee.
Monthly cleaning audits. Weekly
managerial audits. Monthly Patient
Safety and Quality Scorecard for
Trust Board. Annual IPC work plan.
CQC inspection raised no
concerns on infection
control.
No evidence of cross
contamination through
ribotyping.
Annual PLACE inspection
excellent.
Reduction in standards
may not be evident to
staff who are familiar
with the environment.
Weekly managerial audits,
GAT reviews and Matrons walk
about provide intelligence into
standard of cleanliness
Green
Not safeguarding people who
use services from abuse and
respecting their human rights.
N Lucey
Safeguarding Adults Committee;
Safeguarding Children's Committee;
Lead Doctors and Named Nurse in
place; safeguarding children's
policy; 3 levels of Child Protection
Training provided.
Safeguarding Adults Policy. Training
matrix in place for ADULT
safeguarding, MCA and DoLS.
Annual reports from safeguarding
adult and children to Quality
Committee.
Clinical audit highlighted a
number of actions to be
completed. Results of
clinical audit discussed at
safeguarding committees
demonstrate improvement
on the previous
recommendations. Audits
will be repeated six-
monthly
Section 11 completed for
children safeguarding.
DSCB review to take place.
Focus on training has led to
improved compliance with
training needs. CCG
inspections to support
knowledge in practice.
Compliance with
mandatory/essential training
remains an issue across the
Trust with Divisional teams
addressing.
Green
Failure of staff to engage in
Patient Charter.
N Lucey
People strategy to reflect the values
and behaviours that form the basis
for the Patients Charter.
Implementation of the
Charter and related
outcomes to be monitored
at Learning from Patient
Experience Committee,
the Quality Committee
and the Trust Board.
The ability to share
with hard to reach
groups
Patient Charter developed and
launched in line with the 175th
Anniversary of the trust.
Agreement to hold the roll out
until the people strategy values
and behaviours were finalised.
Board to agreed final version
September 2016. Launch in
progress. Patients charter has
been approved by the Trust
Board. Light launch
undertaken at Team brief with
full implementation plans being
developed. Launched and now
monitor through Patient
Experience committee
Green
(18) To place the patient at the
centre of all we do ensuring
safe, effective and caring
services
OUTSTANDINGDelivering outstanding
services everyday
We will be one of the very best
performing Trusts in the
country delivering outstanding
services for our patients
9
BAF
Page 88 of 132
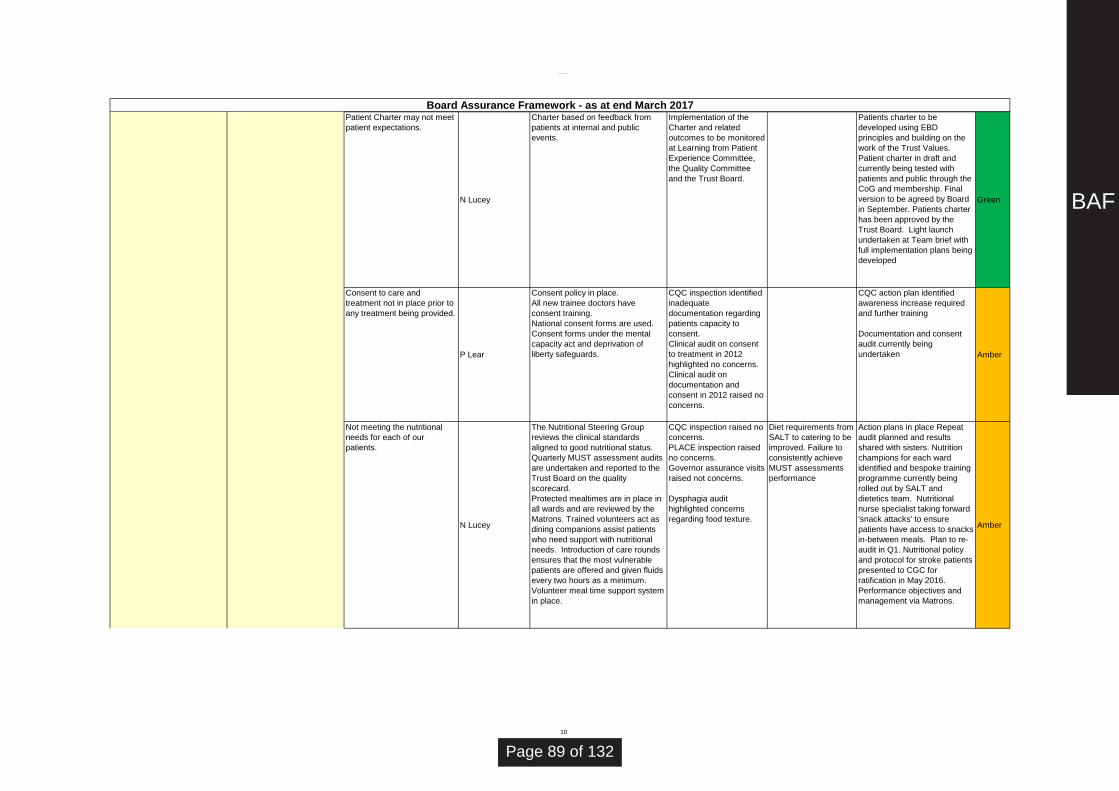
Board Assurance Framework (BAF) 2015/16
Board Assurance Framework - as at end March 2017Patient Charter may not meet
patient expectations.
N Lucey
Charter based on feedback from
patients at internal and public
events.
Implementation of the
Charter and related
outcomes to be monitored
at Learning from Patient
Experience Committee,
the Quality Committee
and the Trust Board.
Patients charter to be
developed using EBD
principles and building on the
work of the Trust Values.
Patient charter in draft and
currently being tested with
patients and public through the
CoG and membership. Final
version to be agreed by Board
in September. Patients charter
has been approved by the
Trust Board. Light launch
undertaken at Team brief with
full implementation plans being
developed
Green
Consent to care and
treatment not in place prior to
any treatment being provided.
P Lear
Consent policy in place.
All new trainee doctors have
consent training.
National consent forms are used.
Consent forms under the mental
capacity act and deprivation of
liberty safeguards.
CQC inspection identified
inadequate
documentation regarding
patients capacity to
consent.
Clinical audit on consent
to treatment in 2012
highlighted no concerns.
Clinical audit on
documentation and
consent in 2012 raised no
concerns.
CQC action plan identified
awareness increase required
and further training
Documentation and consent
audit currently being
undertaken Amber
Not meeting the nutritional
needs for each of our
patients.
N Lucey
The Nutritional Steering Group
reviews the clinical standards
aligned to good nutritional status.
Quarterly MUST assessment audits
are undertaken and reported to the
Trust Board on the quality
scorecard.
Protected mealtimes are in place in
all wards and are reviewed by the
Matrons. Trained volunteers act as
dining companions assist patients
who need support with nutritional
needs. Introduction of care rounds
ensures that the most vulnerable
patients are offered and given fluids
every two hours as a minimum.
Volunteer meal time support system
in place.
CQC inspection raised no
concerns.
PLACE inspection raised
no concerns.
Governor assurance visits
raised not concerns.
Dysphagia audit
highlighted concerns
regarding food texture.
Diet requirements from
SALT to catering to be
improved. Failure to
consistently achieve
MUST assessments
performance
Action plans in place Repeat
audit planned and results
shared with sisters. Nutrition
champions for each ward
identified and bespoke training
programme currently being
rolled out by SALT and
dietetics team. Nutritional
nurse specialist taking forward
'snack attacks' to ensure
patients have access to snacks
in-between meals. Plan to re-
audit in Q1. Nutritional policy
and protocol for stroke patients
presented to CGC for
ratification in May 2016.
Performance objectives and
management via Matrons.
Amber
(18) To place the patient at the
centre of all we do ensuring
safe, effective and caring
services
OUTSTANDINGDelivering outstanding
services everyday
We will be one of the very best
performing Trusts in the
country delivering outstanding
services for our patients
10
BAF
Page 89 of 132

Board Assurance Framework (BAF) 2015/16
Board Assurance Framework - as at end March 2017Not respecting and involving
patients in discussions about
their care and treatment.
N Lucey
Learning from Patients Committee,
quarterly report to Trust Board.
Patient Story at every Trust Board
meeting.
Cancer patients receive care plan at
appointment.
Friends and family test
feedback highlights no
significant concerns. FFT
feedback for ED is slightly
below the national
average. National patients
survey performance good
with some areas for
improvement identified.
National cancer patient
survey.
Mapping of patient
forums and
involvement groups
currently under-way to
identify where there
may be any specific
gaps
Action plan developed with a
multi professional group to
improve services aligned to
areas identified through patient
survey. Patient survey for 2015
(published March 2016) has
highlighted areas that have
improved from the previous
year and also where further
improvements can be made.
The draft improvement plan
was presented to the Quality
Committee in March.
Green
Poor management of patients'
experience leads to a
negative reputation.
N Lucey
PALs; Complaints Policy, trend
analysis of complaints, patient
stories, privacy and dignity audit; the
results of which are displayed on
individual wards.
Internal audit on learning
from issues undertaken
2014/15. High assurance
given.
Current performance
on complaints
response times is
being addressed and
an improvement
trajectory is to be
agreed with each
division. Pace of
improvement slow, a
review of the resources
supporting the
complaints handling
process underway.
Using EBD and NICE criteria
will ensure the organisation
learns from the key messages
from patient's and provide a
framework for improvement.
50% reduction in formal
complaints noted in 18 months.
Repeat complaints reducing.
Annual complaints report
prepared and will be presented
to Quality Committee in June
2016. New Datix module will
allow better analysis and
monitoring of performance.
Anticipated delivery expected
to align with new Governance
structure April 2017.
Complaints timeliness to
respond remains and issue
with an action plan being
reviewed through Quality
Committee.
Amber
(18) To place the patient at the
centre of all we do ensuring
safe, effective and caring
services
OUTSTANDINGDelivering outstanding
services everyday
We will be one of the very best
performing Trusts in the
country delivering outstanding
services for our patients
11
BAF
Page 90 of 132

Board Assurance Framework (BAF) 2015/16
Board Assurance Framework - as at end March 2017Not ensuring the care and
welfare of people who use our
services to ensure we meet
their needs and support their
rights.
N Lucey
All patients to have a plan of care
agreed on admission. Policy's on
safeguarding adults and children,
Deprivation of liberty and caring for
individuals with a learning disability
in place and enacted.
Nursing care indicators test out and
display the results at ward level.
CQC safeguarding
inspection (November
2015) highlighted a
potential risk of harm and
inadequate
documentation in some
areas of practice. Adult
safeguarding lead will be
leaving the Trust in
August.
No verbal feedback
from the full CQC
Inspection 2016
highlighted any
concerns. Awaiting the
full report to identify
any further areas that
require addressing.
CQC safeguarding action plan
to be delivered. Actions being
monitored by the CCG and
good progress noted. CCG
have signed off that all actions
associated with the action plan
for DCH have now been
completed. Successful
recruitment of adult
safeguarding lead to start in
August; specialist nurse for
Learning Disabilities post
established and has been
successfully recruited to start in
July 2016
Green
Service risks develop due to
budget holders not taking
responsibility for financial
performance.L Walters
Financial planning framework in
place;
Budgets signed off annually by
budget holders; monthly reporting of
budgetary performance as part of
integrated performance meetings.
Internal audit January
2014 highlighted no
significant concerns.
Internal audit 2014/15 on
Financial Reporting gave
adequate assurance.
Gaps remain in the
identification of CIP
scheme.
The Better Value, Better Care
Board are focusing on closing
the gap. CIP Programme
Manager recruited to January
17. Finance Improvement
Team in place for 2017/18.
Amber
Not having processes and
systems in place to ensure we
learn from complaints and
reduced quality performance.
N Lucey
Learning from Patients Committee,
quarterly report to Trust Board.
Patient Story at every Trust Board
meeting.
Nurse sensitive indicators as part of
performance management and
Divisional performance reviews,
with exception reporting to Quality
committee areas of support
required.
PALs: Complaints Policy, trend
analysis of complaints, patient
stories, privacy and dignity audit as
part of nursing care indicators, the
results of which are displayed on
individual wards EBD and NICE
indicators.
Trends in patient
feedback. Annual
programme of patient
surveys.
Internal audit.
No robust evidence
that learning from
complaints is
embedded in service
delivery. Variability in
divisional performance
management of key
improvement targets
and exception
reporting.
Internal audit planned for 2014/15
will provide independent assurance.
Revision of divisional exception
reporting and development of nurse
sensitive dashboards and
department/ward boards to drive a
culture of striving for excellence.
Divisions now required to provide
this evidence. Template to be
developed to theme issues and
produced a focused action plan.
Some signs of better engagement
within divisions and embedded
learning will be a feature of the
implementation of the improved
governance arrangements within
divisions. Complaints module on
Datix transition to enable further
learning from complaints and embed
in divisional quality management.
Amber
(19) To develop a culture of
continuous improvement,
supporting clinical teams to
improve their quality, safety
and efficiency
(18) To place the patient at the
centre of all we do ensuring
safe, effective and caring
services
OUTSTANDINGDelivering outstanding
services everyday
We will be one of the very best
performing Trusts in the
country delivering outstanding
services for our patients
12
BAF
Page 91 of 132

Board Assurance Framework (BAF) 2015/16
Board Assurance Framework - as at end March 2017Significant changes required
to implement seven day
service delivery.
J Pearce
Project board established which will
report into SMT.
Trust working with DH
Lead to complete a gap
analysis against the ten
national clinical standards.
Implementation of
nationally negotiated
changes to the consultant
contract.
Audit of 14 hour
consultant review across
7 days.
Internal audit on job
planning planned 2016/17
No assurance that the
national negotiations
will deliver changes to
the consultant contract.
Project Board in place to
implement.
Service transformation team
undertaken a gap analysis to
understand where 7 days
services delivery is required.
Action plan to be agreed to
complete the first 5 standards
across the Trust by March
2016. Some progress has
been made but the pace of
change is slow. Progress on
delivering the standards
unlikely to be achieved until the
job-plans have been reviewed.
Amber
CQUIN schemes not being
delivered
N Lucey
Each CQUIN scheme has a
responsible manager and lead
Executive Director identified.
Monthly reporting to SMT and Board
on performance.
Commissioner contract
meetings not raising any
concerns Quarterly
meetings with CCG and
providers review progress
and revise targets to
demonstrate realistic
improvements. End of
year position on CQUINs
included in Quality
Account. New set of
CQUINs agreed with
commissioners for
2016/17 contract which
are currently being
worked up for
implementation. 2017/18
has new nationally
mandated CQUIN
scheme for 2 year period
Engagement and
progress variability with
assigned leads. New
leads for the 2016/17
CQUIN programme to
be agreed. Completed
Monthly updates on action
plans to ensure progress is
being achieved. Quarterly
reports to SMT. Two areas of
CQUIN currently under-
performing against an agreed
trajectory and recovery plans
have been agreed. Final report
on CQUINs for 2015/16
included in quality account
Green
Failure to manage medicines
to ensure patients get
medicines when they need
them and in a safe way.
A Prowse
Divisional Pharmacists in place plus
ward based pharmacists to support
prescribing and dosing practice.
Drugs and Therapeutics Committee;
Training for doctors and nurses in
medicines management. Medicines
management policies and
medicines reconciliation service.
Datix reporting of clinical incident
relating to prescribing and dosing
errors. EPMA in place.
CQC inspection
highlighted issues.
Recent CQC Inspection
2016 highlighted some
issues associated with the
safe storage of
medications in maternity
Enforcement notice lifted.
Management of
medicines audit planned
2015/16.
Actions to address the issues
highlighted in the verbal
feedback by the CQC at the
time of the inspection have
been completed.
Green
(19) To develop a culture of
continuous improvement,
supporting clinical teams to
improve their quality, safety
and efficiency
OUTSTANDINGDelivering outstanding
services everyday
We will be one of the very best
performing Trusts in the
country delivering outstanding
services for our patients
(20) To look within our
organisation and ensure
services are joined up and
integrated across specialities
to the benefit of the patient
13
BAF
Page 92 of 132

Board Assurance Framework (BAF) 2015/16
Board Assurance Framework - as at end March 2017Not meeting the performance
requirements in the NHS
Standard Contract or Monitor
Risk Assessment Framework
will distract focus onto
operational recovery.
J Pearce
Divisional performance framework
in place. Performance framework to
be reviewed to align with NHS-I
appraoch
Regular report to SMT and Board of
Directors. Performance during Q3
improved for ED and cancer
standards; under-performance in
RTT and diagnostic standards
FPC, Trust Board &
Contract monitoring
meetings
Review of Divisional
governance
arrangements has
been undertaken by
PwC . Final Report
received and action
plan being developed
to address the
recommendations.
Under-performance of
key national standards
during Q1 and Q2, Q3
recovery plans in
place. Recovery
trajectories submitted
to CCG and NHS-I;
Action plans in place to recover
any performance issues.
Recommendations from the
PwC review has highlighted
areas where governance can
be strengthened. A proposal to
standardise processes
currently being developed.
Project team identified to take
forward the recommendations
from the governance review.
External support from NHS-I
has been agreed in relation to
ED performance on 4 hour
standard. Q2 appeal on RTT
successful; appeal for Q3 RTT
being prepared.
Amber
From the Francis report
actions not owned by
individuals and therefore not
delivered.
N Lucey
Quarterly review by the Quality
Committee, clinical governance
committees and trust board of the
action plan including assurance
mechanism.
Internal audit planned
April 2016. Internal audit
completed, final report to
be signed off with internal
audit
No external assurance,
PWC review of
divisional governance
will look at elements of
the Francis action plan
to look for embedded
changes
Scope of internal audit
discussed and awaiting draft
terms of reference. Terms of
reference agreed and audit will
take place during Q1. Audit has
taken place, draft report
suggests appropriate
assurances in place, final
changes to the report to be
agreed.
Green
Access and quality of services
reduces due to inadequate
emergency preparedness and
business continuity plans.
J Pearce
Major incident and business
continuity plans revised in 2013/14.
Members of the local Resilience
Forum and Executive attendance at
the Local Health Resilience
Partnership Forum.
Live testing of plans 3 yearly.
EMERGO exercise
undertaken in May 2014.
Annual review of Major
Incident Plan completed
and signed of by the
Board, CCG & NHS
England. Programme of
testing the robustness of
the emergency plans in
place. Additional training
available for key people.
Internal audit planned for
September 2016
NHS-E revised
standards framework
for 2016/17, gap
analysis to be
undertaken and any
gaps identified.
Business continuity plans for
DCH revised and updated.
Revisited Emergency planning
and business continuity policy
and plan submitted to the
Board in June 2016 and was
ratified. Testing of BCP on a
rolling programme during
2016/17.Green
(21) To implement a
comprehensive and robust
governance approach across
the organisation
OUTSTANDINGDelivering outstanding
services everyday
We will be one of the very best
performing Trusts in the
country delivering outstanding
services for our patients
(20) To look within our
organisation and ensure
services are joined up and
integrated across specialities
to the benefit of the patient
14
BAF
Page 93 of 132

Board Assurance Framework (BAF) 2015/16
Board Assurance Framework - as at end March 201721a) To achieve 'Good -
Outstanding' CQC rating as
part of our strategic excellence
ambition
Failure to complete actions as
identified in the CQC action
plan to meet the required
regulation standards in the
timescales identified
N Lucey
Action plan and tracking of actions.
Governance framework to provide
assurance on performance and
clinical/corporate governance
refined to enable delivery of the
actions. Internal inspections and
assurances processes: Mock
internal CQC inspections;
monitoring of divisional governance
and actions; Board sub-committees;
partnership Dorset Vanguard
additional good practice sharing and
development of pathway standards
CQC action plan
assurance evidence; Sub-
board committee
assurance reports to
board; Divisional
governance minutes;
CCG assurance visits
reports; internal 'mock'
inspections and deep
dives. Internal audit mock
CQC inspection against
action plan: significant
assurance.
Governance
framework needs
refreshing to enable
stronger assurance
monitoring on internal
governance. Gaps in
divisonal robust
governance and
assurance to clinical
governance and
perforamnce reviews..
Redesign of the Trust
Governance framework -
proposal by December 2016
for implementation April 2017.
On track for delivery. Divisional
performance reviews increased
to provide additional scrutiny of
governance until new divisional
structure, new performance
framework and revised
governance framework are
implemented and embedded.
Amber
(22) To develop an excellent
administrative care pathway
OUTSTANDINGDelivering outstanding
services everyday
We will be one of the very best
performing Trusts in the
country delivering outstanding
services for our patients
15
BAF
Page 94 of 132

Title of Meeting
Board of Directors
Date of Meeting
31 May 2017
Report Title
Committee Work Plans
Author
Lindsey Perryman, Trust Secretary
Responsible Executive
Patricia Miller, Chief Executive
Purpose of Report (e.g. for decision, information) To present to the Board the proposed work plans for Quality Committee, Finance and Performance Committee and Risk and Audit Committee for approval.
Summary Although committees have previously had annual work plans these have not in the past been approved by the Trust Board. For 2017/18 work plans have been reviewed by the Committee Chairs, Trust Chair and relevant executives to ensure that the work plans are robust and provide appropriate assurance.
Paper Previously Reviewed By Finance and Performance Work Plan – reviewed by Finance and Performance Committee on 21 March 2017. Risk and Audit Committee Work Plan – reviewed by Risk and Audit Committee on 18 April 2017. Quality Committee Work plan – reviewed by Quality Committee on 23 May 2017.
Strategic Impact Failure of the Trust to have robust governance arrangements could impact on the ability to achieve its Strategic Objectives.
Risk Evaluation Low
Impact on Care Quality Commission Registration and/or Clinical Quality The work of the Board committees provides assurance to the Board in respect of the quality of care and patient experience.
Governance Implications (legal, clinical, equality and diversity or other):
Com
mitt
ee W
ork
Pla
ns
Page 95 of 132

Robust governance arrangements enable appropriate decision making.
Financial Implications The Finance and Performance Committee provide assurance to the Board in respect of the Trust financial plan.
Freedom of Information Implications – can the report be published?
Yes
Recommendations To approve the work plans.
Com
mitt
ee W
ork
Pla
ns
Page 96 of 132

Quality Committee Work plan 2017/18
The Quality committee work plan reflects the Board Assurance Framework (BAF) strategic
objective ‘Outstanding: Delivering outstanding services every day’. The Priorities included in this
are 18,19, 20,21, 21(a), and 22.
Quality Committee work plan support the effective organisation management of clinical
governance including:
- Risks management relating to quality and safety, including risk management processes and
application; incident and serious incident reporting, learning and monitoring of harm.
- Assurance and identification of any gaps in control in improvement to deliver the strategic
objective
- Lessons learnt that aid improvement and learning to benefit quality, safe care and best
practice including clinical audit.
- Clinical adherence to national guidelines or standards such as NICE
- Patient and public feedback including complaints, plaudits, surveys and patient involvement
in services (such as volunteers experience and carers experience).
- Policies that apply to quality and safety principles.
The detailed reporting work plan informs sub groups of their agendas and reporting lines, as
outlined in the governance framework for the Trust.
To support the detailed reporting work plan Quality committee have agreed the following
overarching work plan priorities:
Work plan priorities CQC
1. Mortality surveillance in line with national
guidance
CQC domain: SAFE, EFFECTIVE (Regulation
12, 13, 16, 17, 20)
2. Sepsis and the deteriorating patient CQC domain: SAFE, EFFECTIVE (Regulation
12, 20
3. Board triangulation via quality visits –
board visibility and assurance
CQC domain: WELL-LED (Regulation 17)
4. Quality impact assessment of new
models for DCHFT as part of the STP
CQC domain: WELL-LED, RESPONSIVE
(Regulations 17,
5. Governance ward to board to be an
exemplar of well-led domain
CQC domain: WELL-LED (Regulation 17)
Underpinning fundamental CQC standards (Regulation8)
Com
mitt
ee W
ork
Pla
ns
Page 97 of 132

April May June July August September October November December January February March
Frequency
Quality aspect of integrated performance
report: Patient Safety, Effectiveness and
Experience Report - including safer staffing Mthly
Divisional exception reports Mthly
CQC Inspection action plans, exception reportTwice a QRT
CQC Inspection deep dive action plansQRTLY Deferred as
covered in April
Quality Accounts Quarterly ReportsQRTLY
Medicines Committee exception report (meets
first wed)BI-MTHLY
Deferred
Safety Group exception report: including
Learning from Serious Incidents, claims and legal
cases (meets first Friday)MTHLY
New start -
here
Clinical effectiveness and Innovation Group
exception reports: e.g NICE Compliance &
Clinical Audit Annual Report & Research and dev
(meets second wed)
MTHLYNew start -
here
Infection Prevention and Control Group
exception reports (meets first wed)BI-MTHLY
End of Life Care Group exception reports (meets
second wed)BI-MTHLY
Patient Experience Group exception reports
(meets third Tues): INCLUDING PATIENT
ENVIRONMENT (plus PLACE)
BI-MTHLY New -starts
here
Mortality Group exception reports (meets third
Wed) BI-MTHLY
Safeguarding Adults and Children Group
exception reportsQRTLY
TBC TBC TBC TBC TBC TBC TBC TBC TBC TBC TBC TBC
Detailed Mortality Report QRTLY
Annual Quality Report - draftANNUAL
Annual Quality Report - finalANNUAL
Committee Annual Review of Effectiveness,
Review of ToRsANNUAL
Safeguarding Children Annual ReportANNUAL
Deferred update
Safeguarding Adults Annual ReportANNUAL
update
Infection Prevention and Control annual reportANNUAL
TBC
RISK management strategy update ANNUAL
CLINICAL AUDIT plan ANNUAL
Annual patient surveys ANNUAL
Clinical Audit Annual Report ANNUAL
Information Governance Annual Report ANNUAL
Medicines Safety Annual Report ANNUAL
PLACE Annual Review ANNUAL
Complaints Annual Report ANNUAL
Annual Work Plan for Quality Committee 2017/18
SAFETY & QUALITY
ANNUAL ASSURANCE
Com
mitt
ee W
ork
Pla
ns
Page 98 of 132

1
To: Finance and Performance Committee From: Libby Walters, Director of Finance and Resources Subject: Proposed Finance and Performance Committee Work Plan 2017/18 Date: March 2017 1.0 Purpose of the Paper
The Trust Board has the responsibility to put in place governance structures and processes to:
Ensure that the organisation operates effectively and meets its statutory and strategic objectives; and
Ensure that this is the case. The Finance and Performance Committee supports the Board in fulfilling this role by:
On the ability of the Trust to meet its financial and operational performance requirements.
Ensuring performance manager processes are robust.
Providing assurance to the Board by undertaking deep dives on high risk performance issues.
Challenging relevant managers when controls are not working or data is unreliable.
To ensure the Finance and Performance Committee can fulfil its role effectively it must have in place a work programme that covers each of its responsibilities.
The purpose of this paper is to propose a work plan for the Finance and Performance Committee for 2017/18.
2.0 Current gaps in the Finance and Performance Committee Work Plan There are a number of areas that the Finance and Performance Committee are responsible for providing assurance to the Board on that they are not always covered in sufficient detail, in addition there are also opportunities to further enhance the effectiveness of the committee. The table below proposes how these gaps / enhancements are included in the work plan.
Gap in Work Plan Proposed action
Reviewing operational performance at a divisional level.
Focussing on the delivery of divisional business plans.
Divisional Managers to attend meeting on permanent basis with Divisional Directors on an as and when basis
Bi annual review of divisional business plans.
Gaining assurance from the committees/ Groups reporting to the FPC i.e.
Workforce & Resources Strategy Group
Medical Devices Group
Access & Flow Group
Template reviewed at each meeting for these 3 groups that show when last met, was meeting quorate, issues discussed, areas to escalate.
Com
mitt
ee W
ork
Pla
ns
Page 99 of 132

2
Continual opportunities to deep dive into high risk areas.
Post development appraisals not undertaken.
Increased focus on service line reporting data.
No detailed scrutiny on estates statutory compliance.
Increased focus on trend analysis and switching more time from retrospective reviews to more forward looking
Work plan to include dedicated time for deep dives on alternative agendas.
FPC to get assurance that post development appraisals are undertaken and undertake some themselves for significant developments.
Divisions to report their service line reporting to the Committee on a quarterly basis.
Head of Estates and Facilities Management to attend annually.
Monthly Finance, Operational & HR updates to include more trend analysis
3.0 Proposal
The attached work plan is a proposal for how the Finance and Performance Committee can effectively fulfil its duties in 2017/18.
Com
mitt
ee W
ork
Pla
ns
Page 100 of 132

Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Performance Reporting
Operational Performance x x x x x x x x x x x x
HR x x x x x x x x x x x x
Finance x x x x x x x x x x x x
Finance - SLR detail to be reported by divisions x x x x
Financial assurance
Business planning guidance to approve x
Draft Budgets to be approved x
Final budgets to be approved x
NHSI Draft Operational Plan to be approved x
NHSI Final Operational Plan to be approved x
Review of post investment appraisal process x x
Report from Procurement Board and Head of
Procurement attends - assurance reviewx
Report from Better Value Better Care - assurance
reviewx x
Review of cash flow reporting and borrowing
requirements - Head of Financial Accounts to attend
x x
Deep dives where required
Operational Performance assurance
Division A to attend to discuss business plans x x
Division B to attend to discuss business plans x x
Deep dives into assurance and performance issues as
and when requiredx x x x x x
Report from Access and Flow Group. Access Manager
to attendx
HR Assurance
Report from Workforce Resources Strategy Group -
assurance reviewx x
Report from Education/learning development group -
Head of Training and Education to attend.x
Deep dives where required
Estates and Facilities Assurance
Report from Medical Devices Group - Chair of Group to
attendx
Review of Estate and Capital Planning to include
reports from- Space utilisation, sustainability and
capital planning. Head of EFM to attend
x
Report on Estates Statutory compliance and travel
working group. Head of EFM to attend.x
Deep dives where required
Governance
Review meeting templates from all reporting in
committees. x x x x x x
Approval of business cases as and when
Other
Review of Terms of reference x
Review of Effectiveness of FPC x
Finance and Performance Committee Proposed Work plan -2017/18
Com
mitt
ee W
ork
Pla
ns
Page 101 of 132

1
To: Audit Committee From: Libby Walters, Director of Finance and Resources Subject: Proposed Audit Committee Work Plan 2017/18 Date: March 2017 1.0 Purpose of the Paper
The Trust Board has the responsibility to put in place governance structures and processes to:
Ensure that the organisation operates effectively and meets its statutory and strategic objectives; and
Ensure that this is the case. The Audit Committee supports the Board in fulfilling this role by:
Obtaining assurances about controls and whether that are working as they should;
Seeking assurances about the underlying data (upon which assurances are based) to ensure that it is robust, reliable and accurate;
Challenging poor and/or unreliable sources of assurance; and
Challenging relevant managers when controls are not working or data is unreliable.
To ensure the Audit Committee can fulfil its role effectively it must have in place a work programme that covers each of its responsibilities.
The purpose of this paper is to propose a work plan for the Audit Committee for 2017/18.
2.0 Current gaps in the Audit Committee Work Plan There are a number of areas where the Audit Committee must provide assurance on and currently does not spend adequate time reviewing. The table below proposes how these gaps are included in the work plan.
Gap in Work Plan Proposed action
Ensuring the risk management system and process for developing the assurance framework (BAF) is robust.
Head of Risk Management attends audit committee annually to present the risk management process.
Time on the agenda for reviewing the BAF process
Review the internal audit report on Risk Registers at the same meeting as above.
Gaining assurance from the committees reporting to Audit Committee i.e.
Information Governance Group
Information Assurance Group
Health Informatics Programme Board
Template reviewed at each meeting for these groups that show when last met, was meeting quorate, issues discussed, areas to escalate.
IG lead to attend annually to present
Com
mitt
ee W
ork
Pla
ns
Page 102 of 132

2
in more detail the IG processes
Providing assurance that data used has undergone quality checks to ensure it is robust
Head of BI to attend annually to present how assurance is gained on this.
Ensure effective whistle blowing arrangements are in place
Review annually the process for whistleblowing.
Noting business of other committees and reviewing inter relationships
FPC and QC chair’s attend to present how getting assurance from committees they provide assurances on.
There are a number of areas where the Audit Committee could reduce its workload as follows:
Review of tenders awarded: The audit committee needs to provide assurance that effective financial systems are in place. This can be done through the internal audit plan and does not need all tender activity to be reported to the Audit Committee. It is recommended that an annual report on tender activity is provided.
Counter Fraud: Good practice states that Counter Fraud attend Audit Committee meetings at least twice a year. Currently the Counter Fraud Service attends every meeting. This could be halved and therefore they could attend three times a year.
3.0 Proposal
The attached work plan is a proposal for how the Audit Committee can effectively fulfil its duties in 2017/18.
Com
mitt
ee W
ork
Pla
ns
Page 103 of 132

14-Feb 18-Apr 22-May 18-Jul 19-Sep 21-Nov Jan March
Governance
Review the BAF x x x x x x x
Review the significant risk register x x x x x x x
Review the assurance framework process x
- Head of Estates present x
Review of risk management system including
attendance of Head of Risk x
Review work of other committees x
Review reports from IGC, IAG and HIPB x x x x x x x
IG lead attends x
BI lead attends x
Auditors Annual Governance Report including letter of
representation x
Draft Annual Account, Quality Report and Governance
Statement x
Auditors Report on the Quality Account 2016/17 x
Review annual report and accounts x
Review whistle blowing arrangements x
Review changes to standing orders, SFI's, Scheme of
delegation x
Review losses and special payments x x
Review tender activity x
External Audit
Agree final annual report and accounts timetable and
plans x
Review audited annual accounts including the external
audit opinion x
Agree external audit plans and fees x
Review the effectiveness of external audit x
Review external audit progress reports x x x x x x x
Receive the external auditors report to those charged
with governance x
Receive/consider the external auditors annual audit
letter x
LCFS
Approve the annual work plan 2017/18 x
Progress Report x x x
Review the effectiveness of counter fraud x
Review the annual report on counter fraud x
Internal Audit
Review and agree Work plan 2017/18 x
Progress Report x x x x x x x
Recommendations Tracker x x x x x x x
Internal audit reports
-Well led review x
- Review of risk registers x
- Quality accounts/KPI quality x
- Main accounting systems x
- Financial systems - IT control x
- ICT infrastructure x
- Patient experience x
Audit Committee Proposed Work plan -2017/18
Com
mitt
ee W
ork
Pla
ns
Page 104 of 132

14-Feb 18-Apr 22-May 18-Jul 19-Sep 21-Nov Jan March
- Equality and diversity x
- Follow up x
- Quality audit tbc
Review the annual effectiveness of internal audit x
Receive the Head of Internal Audit Opinion x
Clinical Audit
Receive the annual clinical audit work plan x
Review clinical audit progress reports x x
Other
Audit Committee Annual Report x
Review of Terms of reference x
Review of Effectiveness of Audit Committee x
Register of gifts and hospitality x x
Declarations of interest x x
Draft Minutes of Quality Committee x x x x x x x
Auditors meet members without management IA IA & EA
Com
mitt
ee W
ork
Pla
ns
Page 105 of 132
Title of Meeting
Board of Directors
Date of Meeting
31 May 2017
Report Title
Board Self-Assessment of Effectiveness
Author
Lindsey Perryman, Trust Secretary
Responsible Executive
Patricia Miller, Chief Executive
Purpose of Report (e.g. for decision, information) To present to the Board the outcome of the recent self-assessment of Board effectiveness for discussion and agreement of next steps.
Summary The report contains a summary of the responses received to the Board’s self-assessment questionnaire. Responses were received from 12 Board members. Key points:
Generally there was a good consensus of opinion
Nine people said that there were sometimes surprises at Board meetings with one person stating that there were often surprises
Particularly high scores were received to the following two questions where all respondents rated the Board in the top two categories:
To what extend do Board members’ own standards of behaviours uphold these values (Trust values) and adhere to the Nolan principles?
How would you assess the balance of the Board in terms of the ranges of skills and knowledge available?
Low scores were received in respect of the following two questions: Do partners have the opportunity to influence the longer term direction
of the Trust? How would you assess the performance of the Board in assuring its
accountability to local government?
How would you rate the process for staff having a voice within the Board and access to raise their concerns and feedback?
A wide spread of answers was seen for the following questions: Do senior managers and senior clinicians have the opportunity to
contribute to the development of the strategic direction of the Trust? Do partners have the opportunity to influence the longer term direction
of the Trust? Do all Board members challenge each other in a way which can be
considered constructive? How would you assess the performance of the Board in assuring its
accountability to patients and the wider public? How would you assess the performance of the Board in assuring its
accountability to local government?
How would you rate the process for staff having a voice within the Board
Boa
rd S
elf-
Ass
essm
ent
Page 106 of 132

and access to raise their concerns and feedback?
What proportion of the Board’s time would you estimate is spent on forward looking plans; historic performance; other?
Paper Previously Reviewed By Chair and Chief Executive.
Strategic Impact None related to this report. However, failure by the Board to operate effectively could have an impact on achievement of its strategic objectives.
Risk Evaluation Low.
Impact on Care Quality Commission Registration and/or Clinical Quality None directly related to the paper.
Governance Implications (legal, clinical, equality and diversity or other): It is considered good governance practice for Boards to carry out an annual review of their effectiveness.
Financial Implications Potential financial impact if further external facilitation or development work was considered necessary to improve Board performance and effectiveness.
Freedom of Information Implications – can the report be published?
Yes
Recommendations To discuss the outcome of the self-assessment. To identify any actions required to improve effectiveness.
Boa
rd S
elf-
Ass
essm
ent
Page 107 of 132

Board Effectiveness Self Assessment Questionnaire – Collated Results
March 2017
Focus on purpose and strategy
1 How effective has the Board, as a whole, been in defining and expressing a clear purpose for the Trust?
Not Effective
0
Somewhat effective
0
Moderately effective
4
Effective
7
Highly effective
1
Unable to comment
2 How effective and transparent are the Board’s processes for developing a strategy aimed at delivering the agreed purpose?
Not Effective
0
Somewhat effective
0
Moderately effective
5
Effective
7
Highly effective
0
Unable to comment
3 Do senior managers and senior clinicians have the opportunity to contribute to the development of the strategic direction of the Trust?
Never
0
Sometimes
2
Often
0
Almost always
7
Always
2
Unable to comment
1
4 Do partners have the opportunity to influence the longer term direction of the Trust?
Never
0
Sometimes
6
Often
1
Almost always
4
Always
1
Unable to comment
Promoting values and good governance
5 How effective is the Board in establishing and promoting values for the Trust and its staff?
Not Effective
0
Somewhat effective
0
Moderately effective
2
Effective
5
Highly effective
5
Unable to comment
6 To what extent do Board members’ own standards of behaviours uphold these values and adhere to the Nolan principles?
Never
0
Sometimes
0
Often
0
Almost always
5
Always
7
Unable to comment
Boa
rd S
elf-
Ass
essm
ent
Page 108 of 132

7 How effective are the Trust’s arrangements for ensuring sound clinical quality governance?
Not Effective
0
Somewhat effective
0
Moderately effective
5
Effective
7
Highly effective
0
Unable to comment
8 What proportion of the Board’s time would you estimate is spent on:
Forward looking plans: Range 5% - 50% Mean 32 Review of historic performance: Range15% - 75% Mean 48 Other: Range 0% to 45% Mean 20
Skills and decision making
9 How would you assess the “balance” of the Board in terms of the ranges of skills and knowledge available?
Not Effective
0
Somewhat effective
0
Moderately effective
0
Effective
7
Highly effective
5
Unable to comment
10 Overall, how effective is the Board at managing organisational performance to deliver the strategy?
Not Effective
0
Somewhat effective
0
Moderately effective
5
Effective
7
Highly effective
0
Unable to comment
11 How rigorous and transparent are the Board’s decision making processes, including the information available to support their decisions?
Not rigorous
0
Somewhat rigorous
0
Moderately rigorous
2
Rigorous
9
Very rigorous
1
Unable to comment
12 What is your view of the quality of information currently received by the Board?
Very poor quality
0
Poor quality
0
Reasonable quality
8
Good quality
4
Excellent Quality
0
Unable to comment
13 Does the Board make effective use of available external information which might enhance performance?
Never
0
Sometimes
3
Often
6
Almost always
2
Always
0
Unable to comment 1
14 How effective is the Board at assuring itself that the organisation is operating effectively, efficiently
Not Effective
Somewhat effective
Moderately effective
Effective
Highly effective
Unable to comment
Boa
rd S
elf-
Ass
essm
ent
Page 109 of 132

and economically?
0 0 4 8 0
15 How effective are the Board and organisational arrangements in respect of the management of risk?
Not Effective
0
Somewhat effective
0
Moderately effective
6
Effective
6
Highly effective
0
Unable to comment
16 How effective are the Board and organisational arrangements in respect of the management of clinical safety?
Not Effective
0
Somewhat effective
0
Moderately effective
5
Effective
7
Highly effective
0
Unable to comment
17 Is sufficient time spent at Board meetings discussing and understanding key decisions so that consensus can be reached?
Never
0
Sometimes
0
Often
2
Almost always
9
Always
1
Unable to comment
18 Do all Board members leave meeting with a clear understanding of what decision has been reached, who is responsible for implementing it and how the Board will next be updated on its progress?
Never
0
Sometimes
0
Often
1
Almost always
7
Always
3
Unable to comment
1
19 Do all Board members challenge each other in a way which can be considered constructive?
Never
0
Sometimes
2
Often
3
Almost always
6
Always
1
Unable to comment
20 Are there ever surprises at Board meetings? Never
2
Sometimes
9
Often
1
Almost always
0
Always
0
Unable to comment
21 Do you think the Board is adequately trained and developed to fulfil and meet its responsibilities?
Not at all
0 Slightly
0 Partially
2 Mostly
6 Fully
4
Unable to comment
Managing and listening to stakeholders
22 How would you assess the performance of the Board in assuring its accountability to:
Boa
rd S
elf-
Ass
essm
ent
Page 110 of 132

Patients and the wider public Not Effective
0
Somewhat effective
1
Moderately effective
2
Effective
8
Highly effective
1
Unable to comment
Commissioners and other NHS Providers Not Effective
0
Somewhat effective
0
Moderately effective
0
Effective
11
Highly effective
1
Unable to comment
Staff Not Effective
0
Somewhat effective
0
Moderately effective
1
Effective
10
Highly effective
1
Unable to comment
Local Government Not Effective
½
Somewhat effective
½
Moderately effective
3
Effective
5
Highly effective
1
Unable to comment
3
Regulators Not Effective
0
Somewhat effective
0
Moderately effective
1
Effective
7
Highly effective
4
Unable to comment
23 How would you rate the Board’s working relationships with its partner organisations?
Not Effective
0
Somewhat effective
0
Moderately effective
8½
Effective
3½
Highly effective
0
Unable to comment
24 How would you rate the process for staff having a voice within the Board and access to raise their concerns and feedback?
Not Effective
1
Somewhat effective
4
Moderately effective
5
Effective
2
Highly effective
0
Unable to comment
Boa
rd S
elf-
Ass
essm
ent
Page 111 of 132

Title of Meeting
Board of Directors
Date of Meeting
31 May 2017
Report Title
Use of Trust Seal
Author
Lindsey Perryman, Trust Secretary
Responsible Executive
Patricia Miller, Chief Executive
Purpose of Report (e.g. for decision, information) To inform the Board of the use of the Trust Seal during the period 1 January 2017 to 31 March 2017.
Summary The Trust Standing Orders require that the use of the Trust’s seal is reported to the Board on a quarterly basis. During the period 1 January 2017 to 31 March 2017 the seal has been used on to May 2013 the seal was used on five occasions as set out below:
Seal number
Date of signing Description of Document Signed by
11 27 Jan 2017 Agreement for Lease and Tenant’s Works relating to the Main Entrance at Dorset County Hospital
Patricia Miller Nick Johnson
12 31 Jan 2017 Damers Road Agreement Patricia Miller Libby Walters
13 22 March 2017 Dorset Care Record Deed of Variation to Partnering Agreement
Patricia Miller Libby Walters
14 29 March 2017 Compass – Licence to carry out works relating to units at ground floor main entrance
Patricia Miller Libby Walters
15 29 March 2017 Compass – Lease relating to retail unit at ground floor entrance
Patricia Miller Libby Walters
Paper Previously Reviewed By N/A
Strategic Impact None
Risk Evaluation None
Impact on Care Quality Commission Registration and/or Clinical Quality
Tru
st S
eal
Page 112 of 132

None
Governance Implications (legal, clinical, equality and diversity or other): Reporting of the use of the seal is a requirement under Trust Standing Orders
Financial Implications None
Freedom of Information Implications – can the report be published?
Yes
Recommendations To note the report.
Tru
st S
eal
Page 113 of 132

Title of Meeting
Trust Board
Date of Meeting
31st May 2017
Report Title
Safe Staffing Return (March 2017)
Author
Neal Cleaver (DDoN and Quality)
Responsible Executive
Nicky Lucey (Director of Nursing and Quality)
Purpose of Report (e.g. for decision, information)
To report the submission to UNIFY on planned Nurse/Midwife staffing against actual hours and to provide assurance that safe staffing is managed, monitored and any gaps are mitigated to ensure patient safety.
Summary
As part of the requirement by NHS England to submit information to NHS Choices relating to planned and actual staffing levels, Trusts are required to report any areas which have a lower staffing level than planned and any specific impacts on the quality of care provided as a consequence. In the absence of clear national guidance on the thresh-hold for reporting, DCHFT Trust Board agreed that where actual registered staffing was less than 90% of the planned staffing that this should be reported to the Board with an assessment of any adverse impacts on quality that may have occurred. During this reporting period it should be noted that:
- Abbotsbury/Barnes/Day Lewis– During this period the trust saw a decrease in activity and acuity
- SCBU– Staff in this area flex up and down or are redeployed to other areas dependent on the acuity of their patients and the demand for their services.
Paper Previously Reviewed By Quality Committee on May 23rd 2017.
Strategic Impact
There is a requirement from NHS England for Trust Boards to receive this information
Risk Evaluation Staffing levels are reviewed on a daily basis, along with a review of the patient needs. If there are staffing gaps then a clinical review and effective distribution of staffing resources is applied. The National shortage of both Nursing and Midwifery registered staff continues to cause concern, and the introduction of agency caps has not yet seen the anticipated rise in nurses/midwives entering substantive posts.
Impact on Care Quality Commission Registration and/or Clinical Quality
Saf
e S
taffi
ng R
etur
n
Page 114 of 132

There is national debate as to how the information may identify a lack of clinical quality, and extra information has been included to clarify the position of DCHFT. This this information is monitored by the CQC as part of the Safe, Responsive, Effective and Well-Led domains.
Governance Implications (legal, clinical, equality and diversity or other):
Staffing shortages could lead to patient safety and experience incidents and negative reputational impact.
Financial Implications There are costs and financial benefits associated with the recommendations of the full establishment review.
Freedom of Information Implications – can the report be published?
Yes
Recommendations
a) To note and agree the contents for publication on the Trusts website. b) To receive assurance that safe staffing is monitored and managed to ensure safe care.
Saf
e S
taffi
ng R
etur
n
Page 115 of 132

Saf
e S
taffi
ng R
etur
n
Page 116 of 132

Title of Meeting
Trust Board
Date of Meeting
May 31st 2017
Report Title
Annual Complaints Report 2016/2017
Author
Neal Cleaver, Deputy Director of Nursing Becky Protopsaltis, Head of Public and Patient Engagement
Responsible Executive
Nicky Lucey, Director of Nursing and Quality
Purpose of Report (e.g. for decision, information) The annual complaints report complies with the Local Authority Social Services and National Health Service Complaints Regulations 2009, which requires each NHS Trust to produce an annual report regarding complaints received. This is also a mandated requirement of NHS Improvement in the production of the annual quality account.
Summary The paper covers the period 1st April 2016 to 31st March 2017
During this period the Trust received 283 formal complaints, an increase from 217 for 2015/16
There were 588 recorded informal issues resolved in real time during this reporting period
The Trust received 427 formal compliments during this period, a substantial increase of 41% from the previous year
Complainants have received a feedback questionnaire based on the experience based design approach in order for us to be able to understand the complaints process from a complainants perspective
There were 4 (1.4%) complaints refereed to the Parliamentary and Health Service Ombudsman (PHSO), a decrease from the previous year of 8 (4%)
A timeliness of responses action plan has been developed to be implemented in conjunction with the new governance structure and divisional restructure
Timeliness of responses to complaints remains a Quality Priority for the Trust for 2017-2018.
Paper Previously Reviewed By This paper was reviewed by the Quality Committee on 23rd May 2017 prior to providing assurance to the Trust Board. Timeliness of responses and communication/attitude themes from complaints were discussed in detail and will be monitored through the Quality Committee
Strategic Impact The delivery of improved complaints processes will require cross boundary working, MDT working and strengthened processes within the new divisional governance structure.
Risk Evaluation Improved timeliness of responses to complaints was identified as part of the quality account priorities for 2016-17. As no significant improvement has been demonstrated, this has been continued as a priority for 2017/18.
Impact on Care Quality Commission Registration and/or Clinical Quality As feedback is designed to enhance and improve both patient safety and experience, non-
Ann
ual C
ompl
aint
s R
epor
t
Page 117 of 132
delivery of improvement may result in a detrimental consequence on the quality and experience of our patients.
Governance Implications (legal, clinical, equality and diversity or other): Inability to achieve progress or sustain set standards could lead to a negative reputational impact and inability to improve patient safety, effectiveness and experience.
Financial Implications None currently identified
Freedom of Information Implications – can the report be published?
Yes
Recommendations 1. Note the report 2. Gain assurance of the scrutiny performed by the Quality
Committee
Ann
ual C
ompl
aint
s R
epor
t
Page 118 of 132

1
Title of Meeting
Quality Committee
Date of Meeting
23rd May 2017
Report Title
Annual Complaints Report 2016/17
Author
Becky Protopsaltis, Head of Public and Patient Experience Nicola Lucey, Director of Nursing and Quality Neal Cleaver, Deputy Director of Nursing and Quality
INTRODUCTION
1.1 The annual complaints report complies with The Local Authority Social Services
and National Health Service Complaints (England) Regulations 2009, which
requires each NHS Trust to produce regular reports about complaints received,
including an annual report.
1.2 This annual report includes an overview of the number and nature of complaints
received, how complaints are handled,
2.0 NUMBER OF COMPLAINTS RECEIVED
2.1 The total number of formal complaints received by the Trust for this year was 283 which has increased (30%) from the previous year. There were also 588 recorded contacts for PALS informal issues resolved, a decrease (3%) on the previous year.
2.2
373
544
352411
345
478428 452
385459
217
608
283
588
0
100
200
300
400
500
600
700
Formal complaints PALS (informal issues)
Number of Complaints and Concerns
2010/11
2011/12
2012/13
2013/14
2014/15
2015/16
2016/17
Ann
ual C
ompl
aint
s R
epor
t
Page 119 of 132

2
2.3 Each formal complaint is treated as well-founded in order to investigate and a response is
provided to the complainant outlining the findings of the investigation.
3.0 PROCESS FOR COMPLAINTS HANDLING
3.1 The Trust informs patients and carers how to raise concerns in the bedside folders, on the
website and in the “Comments, Complaints, Concerns & Compliments” leaflet.
3.2 All feedback, concerns and complaints are co-ordinated centrally and upon receipt are
screened and triaged according to the seriousness of the issues raised. The focus is to
consider each complaint from the complainant’s perspective and every complainant is
offered the opportunity to discuss the way in which their complaint is handled.
3.3 The responsibility for investigating complaints is devolved to the Divisions and their
respective teams, who are required to provide a comprehensive response within an agreed
timeframe. This outlines the response to the investigation and recommendations or actions
taken for improvement where appropriate. The final response to every formal complaint is
agreed and signed by the Chief Executive.
3.4 The complaints process allows the Trust flexibility in arranging local resolution meetings
with complainants. These meetings usually include the relevant healthcare professionals
including the Consultant or Matron in order that questions can be answered by the clinicians
delivering care and a personal apology given where appropriate. This has proved to be a
very positive and helpful process with the openness of the meetings being well received by
all participants.
3.5 Dorset County Hospital NHS Foundation Trust has been part of the NHS England
development group for the “Protocol for the Handling of Inter-Organisational Complaints in
Wessex” (Hampshire, Dorset and IoW) which will replace the “Joint NHS Complaints Policy
for Dorset”. This protocol is between NHS England (Wessex) and the NHS Trusts, CCGs,
Local Authorities and Ambulance Trusts in the Wessex area.
4.0 TIMELY AND COMPASSIONATE RESPONSE TO COMPLAINTS
4.1 This year again our task was to improve the timeliness of responses to complaints so that complainants are responded to within mutually agreed timescales and to improve the compassion in the response so that it responds to the emotions of the complainant.
4.2 We believe that when our patients or their families have cause to complain, the response
they receive should be within an agreed timescale and acknowledge the experience of the patient through their own eyes. We believe that the response should cover all the concerns that are raised, should not cause any further distress, and that our patients/families should have an identified lead who will keep them updated on the progress of any investigation.
4.3 In order to achieve improvements in this area, we:
Ann
ual C
ompl
aint
s R
epor
t
Page 120 of 132

3
4.3.1 Reviewed the Complaints Policy and Standards which includes the standards for
the complaints process and agreements of timescales for responding to complaints for non-complex complaints and concerns involving one area.
4.3.2 Met with Divisions (as per Division capacity /resource) on a weekly basis to
highlight complaints response times, and complaints in need or urgent response.
4.3.3 Sent out a weekly report highlighting which complaints and concerns are outstanding and complaint timeframes to Divisions and senior management team, Director of Nursing/ Quality, Deputy Director of Nursing/Qualityand Chief Operating Officer.
4.3.4 Put request for timescales included in complaint email from PALS. 4.3.5 Process mapped the complaint journey for the development of the Complaints
module on Datix.
4.3.6 Participate in a quarterly deep dive review from the Clinical Commissioning Group to quality check processes and responses and action any improvements identified in their report.
4.3.7 The Patient & Public Experience Lead reviews all responses to ensure compassion and timely response.
4.4 Divisions report that: 4.4.0 All complainants now receive a personal telephone call from the relevant
Manager. 4.4.1 The purpose of the call is to reassure the patient and try to deal with the matter
there and then if possible and to find out whether a written response or meeting is required in the first instance. A timescale for response will also be agreed at this time. A short confirmatory letter then is sent as a follow up.
4.4.2 If the patient wants a full and formal response this is provided and is read and signed by the CEO.
4.4.3 If this response does not meet the needs of the patient, then the patient is offered
a meeting with an appropriate person (usually the Divisional Manager). At this meeting every attempt will be made within reason to meet the patient’s needs.
4.4.4 A follow up letter is then sent after the meeting.
Ann
ual C
ompl
aint
s R
epor
t
Page 121 of 132

4
5 LEARNING FROM COMPLAINTS
5.1 Staff from across the Trust regularly reflect on complaints at divisional and departmental
meetings, in grand rounds, during junior doctors training, sisters and matrons meetings
and porters & housekeeping briefings. The training and support provided by the PALS
team enables them to understand the emotional experience from the complainant and
staff perspective and reflect upon improvements in relational aspects of care.
5.2 Patients have assisted in making videos narrating their experience of the care that they
received, and also their feelings about the complaints process. These videos are shown
to the relevant divisional leads and are available for presentation at Board when required.
The creation of patient video stories remains ongoing.
5.3 Feedback from clinicians into the delivery of complaints training and education by the
PALS team is very positive, with clinicians reporting that they have changed their practice
to deal with complaints more effectively, understand the emotions in complaints and feel
confident when dealing with them.
5.4 Complaints are an integral element of improving the patient’s overall experience of health
care and help to ensure that safe, high quality care is provided within the hospital.
5.5 The quality improvement or learning outcome following investigation of a complaint is
identified and action taken by the respective Division. This is monitored through the
Learning from Patients Committee (now Patient Experience Group) which continues to
meet quarterly. This framework enables the information gained from patient and public
feedback to be owned locally whilst providing a strategic overview with a clear focus on
improving service quality, ensuring that lessons are learnt and processes are changed to
prevent situations recurring.
6.0 FEEDBACK FROM COMPLAINANTS
Complaints Experience Questionnaire Report 2016-2017
6.1 The following charts show the responses received from the Complaints Experience Questionnaire that is sent out with each complaint response. This will be used to improve the complaint handling processes.
Ann
ual C
ompl
aint
s R
epor
t
Page 122 of 132

5
Getting complaint information
Further comments received around obtaining complaint information:
Difficult; I was not given details despite requesting a few times.
I had to ask various staff at various times to get the information I requested
Making a complaint
Ann
ual C
ompl
aint
s R
epor
t
Page 123 of 132

6
Further comments received around making a complaint:
Simple enough. I just wrote what happened and quoted when I could.
Emotionally draining and very upsetting. Only because it took me all weekend to put together all of the dates/information about the things that had gone wrong and the delays. Each department helpful in their own way but not communicating well with each other.
Staying informed
Further comments about staying informed:
Kept informed by the hospital about what was happening.
I had to chase response several times.
Unhelpful, never kept informed.
Ann
ual C
ompl
aint
s R
epor
t
Page 124 of 132

7
Response
Further comments about the complaint response:
Extremely good letter. Helpful and positive and should prevent similar situation in the future. Thank you.
Feel pacified by response. Not sure if it will make any difference as pressure on service is immense.
Frustrating. The response was full of apologies and procedural improvements; all easy to say leaving me helpless and frustrated with no compensation for the poor service.
I would make a complaint again if I needed to
Ann
ual C
ompl
aint
s R
epor
t
Page 125 of 132

8
Further comments about complaining again in future:
Without receiving complaints complacency is more likely.
To not complain only lets the NHS deteriorate further.
If people don’t speak out nothing will ever change.
The complaint was handled fairly
Further comments about the complaint being handled fairly:
Undecided. Don’t feel that the issue was dealt with in depth.
Procedurally yes. But I had no assurance that the service will improve.
7.0 REPORTING & MONITORING
7.1 The Trust Board receives a monthly summary of the number of complaints
received and the issues raised as part of the Integrated Operational Report. A
further report which contains a more in depth analysis of the issues raised in
complaints is provided quarterly to the Board.
7.2 Complaints are coded on the Datix system under a variety of categories.
Although the subject matter may vary, the root causes which result in a
complaint being raised can be associated to three main themes:
communication, staff attitude and delays.
7.3 The five main themes are shown in the graph below.
Ann
ual C
ompl
aint
s R
epor
t
Page 126 of 132

9
7.4 The graph below shows a breakdown of the largest theme of consent, communication
and confidentiality in more detail.
34
4245
62
80
0
10
20
30
40
50
60
70
80
90
Patient care - Ongoingmonitoring and review
Treatment, procedure
Diagnostic scans and tests
Access, admission, transfer,discharge (inc. missing patient)
Consent, communication,confidentiality
38
2
5
33
2
0
5
10
15
20
25
30
35
40
Employee Attitude
Breach of confidentiality
Communication failure (team)
Communication failure withpatient, parent/carer
Communication or advicegiven incorrectly
Ann
ual C
ompl
aint
s R
epor
t
Page 127 of 132

10
8.0 COMPLAINTS BY STAFF GROUPS
9.0 TIMELINESS OF COMPLAINT RESPONSES
9.1 The following chart shows the percentages achieved per division for sending a timely
complaint response (from September 2016 the target was 95%).
0
20
40
60
80
100
120
140
160
180
200
Consultant Nurse - Grade not known Administrative/Clerical
April May June July Aug Sep Oct Nov Dec Jan Feb March
Medicine
14% 83% 73% 50% 55% 46% 50% 41% 50% 38% 83% 50%
Surgery 80% 60% 68% 66% 50% 57% 41% 40% 20% 60% 60% 50%
Family n/a n/a 80% 100% 50% 0% 43% 100% 33% 50% 0% 33%
Clinical
&
Scientific
n/a n/a 0% 100% 100% 100% 50% 0% 50% 66% 0% 33% A
nnua
l Com
plai
nts
Rep
ort
Page 128 of 132
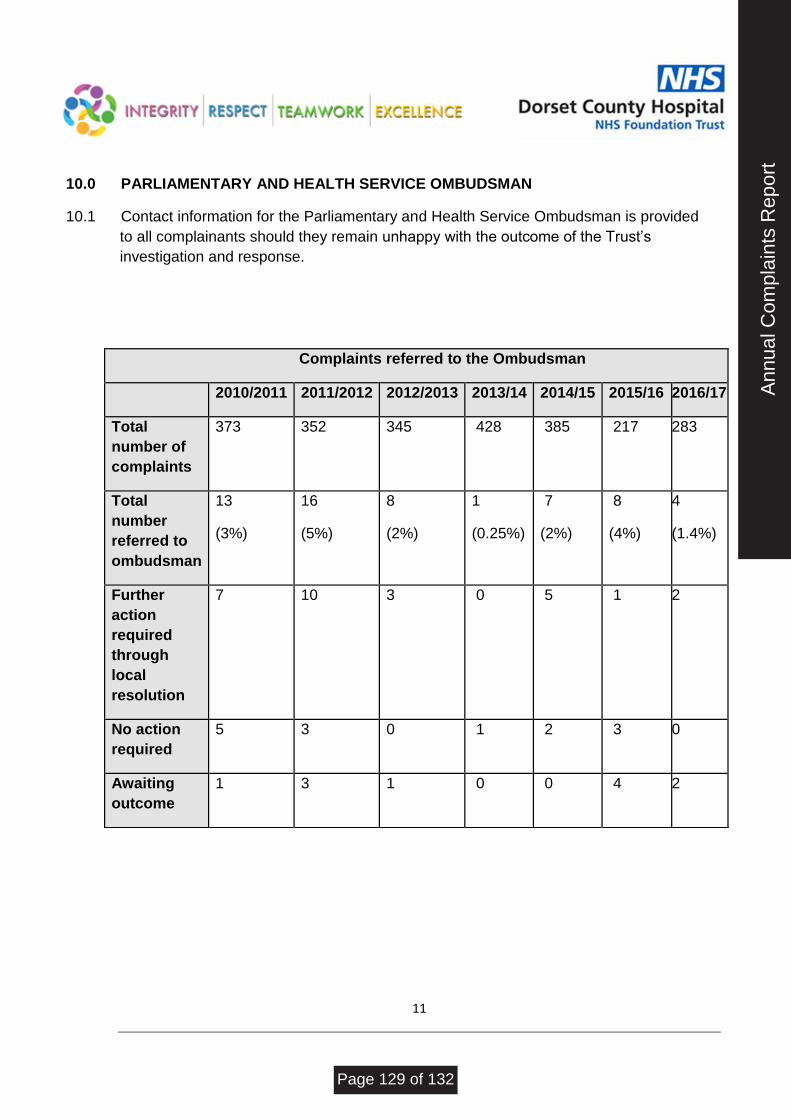
11
10.0 PARLIAMENTARY AND HEALTH SERVICE OMBUDSMAN
10.1 Contact information for the Parliamentary and Health Service Ombudsman is provided
to all complainants should they remain unhappy with the outcome of the Trust’s
investigation and response.
Complaints referred to the Ombudsman
2010/2011 2011/2012 2012/2013 2013/14 2014/15 2015/16 2016/17
Total
number of
complaints
373 352 345 428 385 217 283
Total
number
referred to
ombudsman
13
(3%)
16
(5%)
8
(2%)
1
(0.25%)
7
(2%)
8
(4%)
4
(1.4%)
Further
action
required
through
local
resolution
7 10 3 0 5 1 2
No action
required
5 3 0 1 2 3 0
Awaiting
outcome
1 3 1 0 0 4 2 A
nnua
l Com
plai
nts
Rep
ort
Page 129 of 132

12
11.0 COMPLIMENTS
11.1 The graph below shows the number of compliments received by the Trust in recent
years, with the number of compliments received this year being 427, up by 41% and a
significant increase on the usual numbers received.
12.0 CONCLUSION
12.1 Timely and compassionate response to complaints remains within the Trust’s Quality
Account Priorities for the forthcoming year as the required improvements have not been
delivered.
12.2 A detailed improvement plan is due to be presented to the May Quality Committee for
assurance on the actions required.
12.3 The new governance structure implementation which commenced in May 2017 has
identified a ‘quality’ lead position for each division. The Divisional Heads of Nursing and
Quality are also due to commence in post in June 2017, both of which will be
instrumental in delivering the improvements required.
12.4 A comprehensive action plan has been developed to implement required change and a
plan for improvement, as shown below.
Ann
ual C
ompl
aint
s R
epor
t
Page 130 of 132

13
ACTION: COMPLETION
BY:
1 To update current system used for inputting and recording complaints
(Datix Rich Client) to a web based reporting system (DatixWeb) for
complaints management.
June 2017
2 Creation of toolkit for complaints investigation to go onto intranet.
Development of toolkit to include:
How to write a statement
How to interview staff
Guidance on holding meetings with complainants
Draft response templates
Lessons learnt template
May 2017
3 Process mapping to reflect updated management of
complaints/divisional restructure to be developed and adapted as
DatixWeb rolls out to ensure continuity, accuracy and flow.
May 2017
4 On-going monthly monitoring of response timeliness. A monthly report
is already provided to reflect progress and numbers received. To be
continually monitored for improvement progress.
On-going
5 Complaints investigation training to be provided for all relevant staff.
Next steps:
• Prepare training materials for workshops.
• Identify staff requiring training.
• Trust Complaints Officer to provide 1:1 small group training as
and when required.
June 2017
6 Full quarterly report to reflect on-going progress. An on-going quarterly
report to include:
• Executive summary
• Breakdown of complaints received
• Emerging themes
July 2017 (end of
Q1)
Ann
ual C
ompl
aint
s R
epor
t
Page 131 of 132

14
• Breakdown of outcome/resolution
• Ombudsman update
• Complaints process satisfaction survey update
• PALS update
• Lessons learnt
7 Monthly complaints update meetings to be attended by Complaints
Officer and Quality Managers for each Division.
On-going from
May 2017
8 Quarterly meetings with Patient & Public Engagement Lead and
Divisional Managers to review progress and track improvement made.
On-going from
July 2017
9 Weekly report to be sent out highlighting which complaints and
concerns are outstanding and complaint timeframes to Divisions and
senior management team, Director of Nursing, Deputy Director of
Nursing and Chief Operating Officer.
Already in place;
to continue
monitoring
10 Divisional Managers and Patient & Public Engagement to review all
draft responses – the purpose of this is to check for clarity and
accuracy, as well as to ensure that the reply is sufficiently
compassionate in tone.
April 2017
13.0 RECOMMENDATIONS
13.1 The Trust Board is requested to receive and note the contents of this report.
Ann
ual C
ompl
aint
s R
epor
t
Page 132 of 132