blood vessel suture: its use instead of the ligature in war surgery
TRANSCRIPT

BLOOD VESSEL SUTURE
ITS USE INSTEAD OF THE LIGATURE IN WAR SURGERY
CHARLES GOODMAN, M.D.
NEW YORK,
ATAS M must be accredited with hav- ing first stressed the importance of the preservation and carefuI ap-
NEW YORK
France) and assigned to a CasuaIty CIear- ing Station in the Ypres district, I found that Iigature was the accepted method for
FIG. I. End-to-end suture of carotids. Dog No. 108. Surg. Path. No. 3846. Operation January 20, 1916. Specimen removed February 9, 1916. Cicatricial tissue firmly unites one vesse1 end to that of the other. One extremity is sIightIy everted and the other is implanted upon it. The recess is so obtiterated by connective tissue that the intimaI Iining is compIetely regenerated. The suture line is hardly discernible on account of the merging of the cicatrix with the sutured ends. Smooth muscte ceIIs as demonstrated in a Van Gieson stain infiltrate the cicatrix. (Good- man, Charles. Ann. Surp., July, 1917.)
proximation of the edges of the endothe- hum during vascuIar repair. This was emphasized in his description of aneurism- orrhaphy in I 888. Fifteen years Iater CarreI stimuIated renewed interest in vascuIar surgery by his brihiant animaI research which led to the successfu1 deveIopment of bIood transfusion and the simpIified technic of bIood vesse1 suture.
In 1913, a symposium on the subject of bIood vesse1 suture was heId during the session of the InternationaI MedicaI Con- gress in London. At that session I had reported my technic for arteriovenous anastomosis in fifteen consecutive cases.
In November, 1917, whiIe overseas with the Presbyterian HospitaI Unit (B.E.F.
the treatment of bIood vesse1 injuries. It was recognized that Iigature of the popIi- tea1 or posterior tibia1 artery was aImost invariabIy foIIowed by gangrene, but ap- parentIy no one in the British Service had attempted suture in the treatment of such wounds at the CasuaIty CIearing Station. At that time I used the CarreI suture in five cases on the popIitea1 vesseIs. In these cases the restoration of the continuity of the vesseIs resuIted in tibia1 puIsation, and gangrene was averted. The foIIowing is a brief report of two of these cases:
CASE I. On November IO, 1917, Private M. C. K. G., age twenty-eight, was brought in
with the hamstring mu&es badIy Iacerated. The popIitea1 vessek were exposed and the
196

NEW SERIES VOL. LX, No. z Goodman-Hood Vessel Suture American Journal or surgery 197
artery and vein were found Iacerated. BIeeding in the popIitea1 artery just beIow Hunter’s was temporariIy controIIed by the use of ffexibIe clamps, and a JongitudinaI opening measuring
cana with Ioss of an ova1 segment of the waI1 of the vessel. The opening was cIosed by suture
FIG. 2. Microphotograph, mag. 415. AutotranspIantation of vein into carotid. Surg. Path. No. 2283. Operation January 3, Specimen removed January 17. Vessel par- tiaIIy occluded by coaguIum. Surface of coagulum pre- sents connective tissue ~11s and apparentIy no accretion has taken pIace. Blood coaguIum covered by growing tibroblasts also infiItrating coagulum. No further tend- ency for bIood to form a clot in the coagulum which presents a smooth surface as shown here. (Goodman, Charles. Ann. Surg., July, 1917.)
3 mm. in the waJ1 of each of these vesseIs was repaired with a continuous siIk suture. A flap of mu&e was reflected over the line of suture for protection, and a CarreI-Dakin dressing ap- plied. Forty-eight hours after the operation the foot was warm, the dorsaIis pedis artery per- ceptible and puJsations normal. Eight days Iater the dorsaJis pedis and posterior tibia1 arteries were puJsating vigorousIy; his tempera- ture and pulse were normaJ and the soldier was tra.nsferred to the Base HospitaI.
CASE IT. On November 25, 1917, a private, age twenty-one, was admitted with a through- and-through sheJ1 wound of the Ieft thigh. A Iarge ova1 opening I >/a cm. in length was found
and the caIiber of the Iumen was reduced to about one-haIf its norma size. A branch of the femora1 vein was ligated. FolIowing dCbride- ment of the wound, the suture line in the vesse1 was covered with a ffap of fascia Iata to protect it from erosion by the CarreI-Dakin tubes. The circuIation of the Iimb was satisfac- toriIy restored and he was transferred to the Base Hospital. Seventeen days Iater the soIdier wrote me that he had no pain and was making exceIIent progress.
Subsequently, a few French surgeons empIoyed earIy suture of bIood vessel in- juries in war wounds.

198 American Journal of Surgery Goodman-BIood VesseI Suture MAY. 1943
In reviewing the treatment of bIood vesse1 injuries at the ambuIance Chirurgi- tale under the command of Proust, the
FIG. 3. End-to-end suture of carotid. Dog. no. 27.
Surg. Path. No. 3729. Operation, November I 3, 1915. Specimen removed November ZZ, ,915. Sutured ends separated by $6 mm. of con- nective tissue on one side; on the other side by 2 mm. This connective tissue at some points is dense; at other points it is loosely constructed. The intima regenerates everywhere. At one point, one of the sutures Iies within the vessel Iumen, and is compIeteIy covered by connective tissue with an endotheIia1 surface. Where there was wide separation of the vesse1 ends, there is a considerabIe mass of reIatively Ioose con- nective tissue on the surface which is covered with intima. In the depths the repaired vesse1 wall is dense and suggests osteoid structures. In the depths of the suture Iine at another point, veri definite osteoid structure exists. There is a distinct dilatation of the lumen present at the site of the suture Iine. (Good- man, Charles. Ann. Surg., July, 1917.)
French Surgeon, Maurier, notes that he successfulIy sutured the popIitea1 artery in two cases. Learmonth, the Edinburgh sur- geon, stated in his demonstration, that suture is the idea1 method of repairing wounds of bIood vesseIs and restoring their
continuity. He adds “hitherto it has had a Iimited appIication in miIitary surgery.”
During the first WorId War a number of surgeons of the CentraI Powers stressed the importance of earIy suture of bIood vesseIs in the treatment of war wounds. Before the end of the war Von Haberer had reported zoo cases of bIood vesse1 injuries treated by this method, with onIy one faiIure. Re- centIy, he again advocated suture as the best method for repair of bIood vesse1 injuries.
On the basis of experiences in the first WorId War and in civiIian practice, I want to emphasize the fact that suture of the bIood vessels shouId have a wider appIica- tion in war surgery. Despite extensive Iacerations resuIting from the missiIes of war, repair of the arteries of the extremities can be advantageousIy undertaken in the advanced operating centers. Most of the wounded arrive at such centers within twenty-four hours-a time most favorabIe for repair of the damaged bIood vesseIs. The wounds may be contaminated but the infection has not yet become invasive. Elaborate instruments are not required for bIood vesse1 suture. The simple equipment can easiIy be kept in readiness at the advanced operating centers. Fine straight cambric needIes (Kirby 16) threaded with fine siIk are empIoyed; fIexibIe bIood vessel clamps are best for the temporary contro1 of the injured vesseIs but other devices may be used. The threaded needIes are steriIized in minera oi1. These shouId be kept on hand ready for immediate use. A needIe hoIder is not an absoIute necessity. I have adopted an epiIating forceps as a conveni- ent instrument for guiding the needIe when working in a narrow fieId. The threaded siIk sutures are wound Ioosely about a smaII square of cardboard to keep them
from becoming snarIed. In the treatment of war wounds with
injured vesseIs, dkbridement with the remova of al1 damaged and necrotic tissues shouId be compIeted before the repair of the injured vesseIs is undertaken. Where the vessel is deepIy situated, ligation of one

NEW SERIES VOL. LX, No. 2 Goodman-Blood VesseI Suture American Journal of Surgery ‘99
0.r two of its branches wiIl render the vesse1 ShouId the adventitia be incIuded in the more accessibIe. The injured vesse1 is eIe- suture it may invite thrombosis. The seg- vated to the surface on two pieces of tape ment between the temporary clamps or
FIG. 4. Microphotograph, mag. zoo. Auto- transpIantation of jugular to carotid, two weeks. Dog No. 201. Surg. Path. No. 2340. Specimen removed January 31, 1913. WaIIs of the vessels are separated by about one milIimeter. The interval is filled in by dense connective tissue. Scar tissue is somewhat irreguIar but not cov- ered by fibrin, except at one point. A uni- form and regular layer of cells covers the cicatricial scar tissue. (Goodman, CharIes. Ann. Surg., July, 1917.)
and these may be used for the contro1 of the circuIation above and beIow the laceration. If ffexibIe bIood vessel cIamps are not at hand, rubber bands or smooth forceps without teeth tied with a Iigature may be substituted. A smaI1 rubbed- buIb or piston syringe with saIine or Ringer’s soIution is used to wash away the cIot presented at the opening. The adventitia or outer coat of the vesse1 is then trimmed away about the edges of the wound with the aid of smaI1 forceps and scissors. Adventitia contains considerabIe thrombokinase or ferment.
FIG. 5. Microphotograph, mag. 415. Auto- transplantation of jugular to carotid; two weeks. Dog No. 201. Surg. Path. No. 2340. @E!ratiOn January 31, 1913. WalIS of the vessels are separated by about I millimeter. The interva1 is fiIIed in by dense connective tissue. Scar tissue is somewhat irreguIar but not covered by fibrin except at one point. A uniform and reguIar Iayer of ceIIs covers the cicatricial scar tissue. (Goodman, Charles. Ann. Surg., July 1917.)
tape Iigatures is perfused thoroughly with saIine or Ringer’s soIution foIIowed by a few drops of vaseIine or minera oiI. The minera oi1 keeps the vesse1 from drying. The rent in the vesse1 is then cIosed with a simpIe overhand suture. With the suture compIeted, the temporary compression clamps or tapes are removed and gentIe pressure applied with a pIedget of gauze dipped in minera oi1. Slight oozing may prevail for a few seconds. ShouId there be a spurt of bIood because of the unevenness of the suture, an additiona suture introduced
200 American Journal of Surgery Goodman-BIood VesseI Suture MAY, 1943
and tied at the point of hemorrhage will effectiveIy controI the spurt. The waIIing off of the operating field with pieces of
guide sutures wiI1 usuaIIy be foIIowed by reIaxation. This overcomes the tendency to retraction of the segments, and the circuIar
FIG. 6. Microphotograph, msg. 100. Arteriovenous anastomosis (human vessets). Surg. Path. No. 3550. The artery in cIose apposition with vein, especially the adventitia and media. Mass of connective tissue which has grown beneath the intima reinforces the junction. In the sec- tion at points the endothelium is intact. A thin layer of fibrin with a few round celIs in it is in the venous portion of the section. (Good- man, CharIes. Ann. Surg., July, 1917.)
bIack silk or other material wiI1 maintain a field free from contamination and wiI1 render the fine siIk sutures discernibIe, and simpIify the procedure. Where a large artery has been compIeteIy severed, the ends may be found curIed up and retracted. After the wound is dtbrided, the ends of the severed arteries are exposed and the adventitia overhanging the severed ends of the vesse1 is removed readiIy by pulling the adventitia over the end and snipping it off with one stroke of the scissors. This Ieaves the media and intima exposed for the suture. Three guide sutures are introduced, uniting the two severed ends. I have ob- served during my persona1 experience, that approximation of the severed ends by three
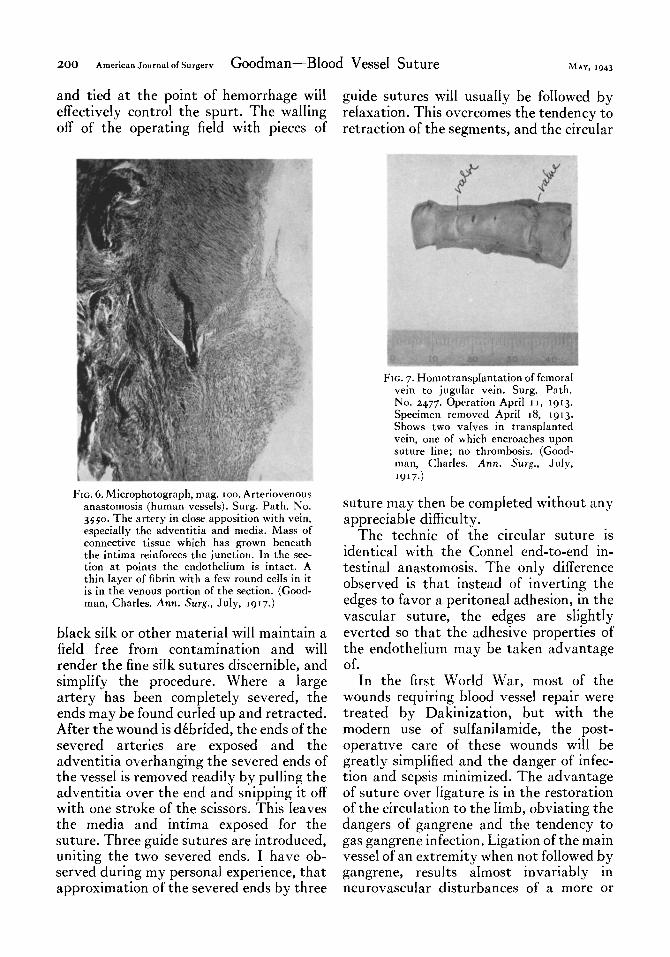
FIG. 7. Homotransptantation of femoral vein to jugular vein. Surg. Path. No. 2477. Operation ApriI 11, 1913.
Specimen removed ApriI 18, 1913.
Shows two vaIves in transpIanted vein, one of which encroaches upon suture line; no thrombosis. (Good- man, Charles. Ann. Surg., JuIy,
1917.1
suture may then be compIeted without any appreciabIe diff%uIty.
The technic of the circular suture is identical with the ConneI end-to-end in- testinal anastomosis. The onIy difference observed is that instead of inverting the edges to favor a peritoneal adhesion, in the vascuIar suture, the edges are sIightIy everted so that the adhesive properties of the endothelium may be taken advantage of.
In the first WorId War, most of the wounds requiring blood vesse1 repair were treated by Dakinization, but with the modern use of suIfaniIamide, the post- operative care of these wounds wiI1 be greatIy simpIified and the danger of infec- tion and sepsis minimized. The advantage of suture over Iigature is in the restoration of the circuIation to the Iimb, obviating the dangers of gangrene and the tendency to gas gangrene infection. Ligation of the main vesse1 of an extremity when not folIowed by gangrene, resuIts aImost invariabIy in neurovascuIar disturbances of a more or

NEW SERIES VOL. LX, No. 2 Goodman-Blood VesseI Suture American Journal of Surgery 201
less serious character. These Iate complica- tions may be avoided by suture, and the
deveIop. Thrombosis is prevented by the two important factors in the technic which
repair likewise does away with the poten- I have described: (I) bloodIess field with
FIG. 8. Arteriovenous anastomosis of femora1 vesseIs removed eighty-three days after operation; maIe adult, age thirty-five. Surg. Path. No. ~$50. (Goodman, CharIes. Ann. .%rg., July, 1917.)
ArPerio-vmoq aeuriy 01 F’emord Vpsseis. )Lacer&d wourd of FrnmraI and ProFwrda arreries. ,Propu& J#e46.
FIG. 9. Arteriovenous aneurysm of femoral vessels. A, laceratea temoral repaired by reflecting stump of profunda and suture; B, IateraI opening in femoral vein closed with continuous suture.
tiaI danger of aneurysma formation with thorough washing away of a11 the clots its cardiovascuIar compIications. If the from the segment to be repaired; (2) the suture does not prove entireIy successfu1 remova of the adventitia from the edges of and thrombosis foIIows, the occIusion takes the wound. The condition of the soIdier pIace so sIowIy that ampIe time is afforded more or Iess exsanguinated demands trans- for an adequate coIIatera1 circuIation to fusion rather than the administration of

202 American Journal of Surgery Goodman-BIood VesseI Suture MAY, 1943
anticoagulants. Recently, the use ofheparin has been advocated for the prevention of thrombosis in blood vessel surgery. In my
P
FIG. IO. Diagram of the procedure.
opinion heparin is not of value in the severeIy wounded requiring blood vessel suture.
When a portion or segment of an artery has been destroyed or compIeteIy carried away by the missiIe so that the severed ends cannot be readiIy approximated, one may resort to the use of a paraffIned Tuffrer tube. The tube is introduced into the respective severed ends of the artery. The flanged ends are secured by simpIe Iigature which prevents them from being displaced. When removed at the end of severa days, these paraffIned tubes may be found partiaIIy or compIeteIy fiIIed with soft coaguIant, but an ampIe opportunity for the development of the coIIatera1 circuIation wiI1 have been attained.
Under favorabIe circumstances, a seg- ment of the saphenous vein can be inter- posed with the aid of a bipoIar circuIar suture. The procedure wiI1 be foIIowed by satisfactory and permanent restoration of the continuity of the vessel. In times of total war, civiIian casuaIties as we11 as casuaIties in the armed services deserve the advantageous use of the bIood vesse1 suture. What has been emphasized in
regard to blood vesseI repair in the ad- vanced operating stations of the army, appIies with equa1 force to the immediate treatment of the injured among the civiIian popuIation, as we11 as in the treatment of industria1 accidents.
During the First WorId War, surgeons of the Central Powers appreciated the advan- tages of the vascuIar suture as against the obIiterating Iigature. Among these the Iead- ing advocates were: Bier, von Haberer and Stich.
The statistica resuIts gathered and pub- Iished in the second edition of Lehrbuch der Kriegschirurgie by Car1 Franz, are iIIus- trated in the foIlowing tables:
Operator su- ture
Bier. ................. 74 Brunzel. .............. 0
Franz IS Fromme .............. 3 Graf .................. 15 v. Haberer ............ 122 Kuttner. .............. 24 Liek .................. o Muller, ............... 0
Mutschenbacher ....... Mutschenbacher-Ver- Nor
bely. report Schwieker ............. Knolle ................ : Zuckerkandl-Glas ...... GoIdammer. .......... :i
28 8
41 46 58
g
25 ‘7 67
No eport
15
90 28
: r#
TotaI. . 300 54o
1 -iga- Deaths ture
8 2
9 3
‘5 10
‘3 8
4 3
0
0
34
III
Total
102
8
56 49 72
172 93 25
z
40
I7 6
102
54
88r
DEATHS FOLLOWING LIGATURE
Operator
Bier, Franz............................ Lick............................. MuIler. BrunzeI. Y. Haberer.. Mutschenbacher.................. Fromme, Subbotisch. Zuckerkandl-Gias. Goldammer
TotaI ----- ~~- Mortality .._._............
I- I -
Deaths Total
2
7 I3 8
:
3 2
9 33
1
88
14.7%
16
41 25 I7 8
:;
46 75
s -~
463
-
-

DEATHS FOLLOWING SUTURE secondary hemorrhage folIowing suture is a negIigibIe one. The restoration of the
Operator Deaths TotaI circuIation in a damaged vesse1 obviates the danger of gas gangrene. The neuro-
Bier. 30 vascuIar disturbances frequentIy observed Franz............................ 3 v. Haberer..
19 folIowing the obliterating Iigature are 2 122
Kuttner.......................... I 24 avoided by the restoration of the circuIa-
Fromme. I 2
tion folIowing bIood vesse1 suture. KnoIie, Hotz............................ Subbotisch. Zuckerkandl-Glas.
; I
12
30
The simpIified technic of blood vesse1 suture outIined and perfected by CarreI and
I2 taken advantage of in hundreds of cases by GoIdammer 26 the surgeons of the CentraI Powers during
Total .._....__. ..I II 284 the First World War, have been folIowed by most satisfactory and briIIiant resuIts.
Mortality folIowing suture 3.8% AmpIe observations of vascuIar sutures performed in animaIs as we11 as in human
COMPARATIVE STATISTICS OF GANGRENE FOLLOWING beings confirm the perfect heaIing of the
LIGATURE AND SUTURE Iine of suture despite the presence of a more or less scar Iine. The iIIustrations appended
Operat0r
Gan- Gan- I Liga- grene rene
Liga- Fol- Fol- Gan- demonstrate cIearIy how perfectIy the
ture and
t”re Suturt intima is reproduced by prompt endo- Suture theIiaI proIiferation.
~ i REFERENCES Rier _.. ,. 102 28 74 I I
Franz., 56 41 15 7 2 9 Goldammer.. 54 26 28
I. MATAS. Surgery of the Vascular System. Keen’s 5 5
Graf.. 72 58 15 + 2 Surgery, vol. V, 1909 and Vol. VII, 1921.
v. Haberer.. 172 I12 i; 24
,. 2. GUTHRIE, C. C. Blood Vessel Surgery and its Ap- Kuttner.. 93 I r plications. New York, 1912. Longman, Green & Liek Mutschenbacher.. 2 2; I
II II co. 2 I 3
Schwieker. Zuckerkandl.. I::
15 2 I I * 3. CARREL. Surgery of the BIood Vessels. Johns
$10 12 33 4 17 Hopkins Hosp. Bull., Jan., 1907. Fromme 49 46 3 I I 4. Abstracts of War Surgery. St. Louis, 1918. C. V.
______ _. Total.. 810 513 296 53 9 63 Mosby & Co.
63% 36.64 b 10.5% 3% 7 7 “‘4 5. GOODMAN. A histologica study of the circular suture of blood vesseIs. Ann. Surg., vo1. 65, July,
19’7.
NEW SERIES VOL. LX, No. 2 Goodman-Blood Vessel Suture American Journal of Surgery 203
According to these statistics, gangrene 6. GOODMAN. Suture of bIood vesse1 injuries from
foIIowed ligatures in 1045 per cent whiIe projectiles of war. Surg., Gynec. TV Oh., Nov.,
gangrene was observed in but 3 per cent of 1918.
7. GOODMAN. Experiments outlining the limitation of
the cases foIIowing suture. operations on the abdominal aorta. J. Exper. Med., vo1. 27, May, 1918.
CONCLUSIONS 8. GOODMAN. Surgery of the heart, blood vessels, etc.
Internat. Surg. Congress, Paris, JuIy, 1920.
The bIood vessel suture, in place of Iiga- 9. Transactions of the V. Congress of the Interna-
ture, undertaken in the advanced operating tional Society of Surgery, Paris, JuIy, 1920.
centers does not entai1 great difbculties and TO. SENCERT. Les BIessures des Vaisseaux. Univ. of
London Press, Ltd., 1918.
shouId be taken advantage of more fre- I I _ TUFFIER. L’ intubation arterieIIe. Bull. Acad. Med.,
quentIy by our army surgeons. Experiences Oct. 19, 1915.
gathered indicate that the danger of 12. FRANZ. Lehrbuch der Kriegschirurgie. 2nd ed.
BerIin, 1936. Julius Springer.