blood transfusion safety: the potential role of the patient
TRANSCRIPT

Blood Transfusion Safety: The Potential Role of the Patient
Rachel E. Davis, Charles A. Vincent, and Michael F. Murphy
There are many initiatives to reduce transfusion-relatederrors. However, one important intervention that remainslargely unexplored is that of patient involvement. Thisarticle considers the patients' role in ensuring safe carealong the transfusion trajectory. Study Design andMethods: Empirical data on patients' attitudes to, andinvolvement in, transfusion-related behaviors were sys-tematically reviewed. Opportunities for patient involve-ment in transfusion processes were identified by extantnational guidelines and expert consultation. Results: Anumber of transfusion-related behaviors inwhich patientscan participate were highlighted, but to date, little isknown about patients' preferences for taking on an activerole. Many patients have no recollection of consenting toa blood transfusion, and some are not even aware theyhave been transfused. Information provided to patientsabout transfusion is often poorly understood. Patientshave a number of misconceptions about the safety ofblood transfusion, and the way in which information ispresented to patients can significantly affect their level of
From the Clinical Safety Research Unit, Department ofSurgery and Cancer, QEQM, St. Mary's Hospital, London, andNHS Blood & Transplant/Oxford Radcliffe Hospitals, and theNuffield Department of Clinical and Laboratory Sciences,University of Oxford.This research was supported by NHS Blood and Transplant.
The Clinical Safety Research Unit is part of the Imperial Centrefor Patient Safety and Service Quality, which is funded by theNational Institute of Health Research.Address reprint requests to Rachel E. Davis, Clinical Safety
Research Unit, Department of Surgery and Cancer, 10th Floor,QEQM, St. Mary's Hospital, South Wharf Rd, W2 1NY London,UK. E-mail: [email protected]/$ - see front matter© 2011 Published by Elsevier Inc.doi:10.1016/j.tmrv.2010.08.003
Transfusi12
confidence and subsequent acceptance in receiving ablood transfusion. Summary: One important interventionthat could help to improve the quality and safety of theblood transfusion process is involvement of the patientthemselves. This article considers the patients' role inensuring safe care at different stages of the transfusiontrajectory. The literature on patients' attitudes to, andinvolvement in, transfusion-related behaviors was sys-tematically reviewed and opportunities for patient invol-vement were identified. The evidence suggests thatalthough there is considerable potential for patients tobe involved in different blood transfusion processes, it isvery unclear at present how able and willing patientswould be to take on an active role in this aspect of theirhealth care management. Research in this area isparamount in helping to inform the design and implemen-tation of interventions aimed at encouraging patientinvolvement in this very important but largely under-researched area.© 2011 Published by Elsevier Inc.
B LOOD TRANSFUSION IS a remarkably safeprocedure, but like many other clinical
procedures, it is associated with clinical risks.These include transfusion-transmitted infectionand unexpected clinical complications such astransfusion-related acute lung injury. In addition,adverse effects occur due to error and suboptimalcare during the transfusion process. In the last20 years, many studies have documented errorsat all stages in the transfusion process,1-6 and
there have been many initiatives to minimize theoccurrence of errors. These initiatives haveprimarily focussed on education and training,but a variety of technological innovations inclu-ding bar coding and the use of hand heldcomputers have reported promising results.7
Technological solutions may facilitate good trans-fusion practice, but the expertise, rigor, andmonitoring of the process by experienced staffprovide the final protection for the patient. Findingbetter ways to train and support the staff directlyinvolved in the many steps of the transfusionprocess remains essential.
In this article, we suggest that, in addition totraining staff in transfusion safety, there is consi-derable potential for a role for patients in ensuringsafe practice. Within the wider arena of patientinvolvement, many opportunities for patients toparticipate in safety-related aspects of their healthcare have been identified,8-11 but the specificcontext of transfusion safety remains unexplored.This is a complex issue, and the whole questionof patient involvement in transfusion requiresdetailed consideration. We do not know, forinstance, how willing patients are to be involved,what they could reasonably be expected to do, orhow much their involvement might be affected or
on Medicine Reviews, Vol 25, No 1 (January), 2011: pp 12-23

13PATIENT INVOLVEMENT IN BLOOD TRANSFUSION SAFETY
curtailed by age, illness, culture, and familiaritywith the transfusion process. In this review, wepresent an overview of the sparse existingliterature on patient experience and involvementin transfusion, and then systematically consider theways in which patients might be more involved.Finally, we propose a research agenda for patientinvolvement in blood transfusion.
PATIENT EXPERIENCE AND ATTITUDESTOWARD TRANSFUSION
To provide a foundation for this assessment ofthe potential for patient involvement in improvingtransfusion practice, we carried out a systematicsearch of the medical literature. We searched forarticles that contained empirical data related topatients' attitudes and/or experiences of allogeneicblood transfusions and/or attitudes toward parti-cipating in transfusion-related behaviors (the spe-cific search strategy is available from the authors).Empirical articles on patients' attitudes towardautologous blood donation or domiciliary transfu-sion services were not considered. Fifteen articleswere of relevance (from 2018 retrieved). On closerinspection of the findings, data could be catego-rized into 6 main areas of interest. Here wesynthesize the key findings for these studies inrelation to these different areas. For a more detailedaccount of the findings and information on thedesign and methodologies of the studies, pleaserefer to Table 1.
Given that patient involvement in health care isa fairly recent phenomenon, particularly in some(less developed) communities, we considered itimportant to provide the time and place where thestudy occurred, as these could affect patients'attitudes and/or participation in the transfusionprocess. The attitudes, expectations, and involve-ment of patients in Pakistan, for example, arelikely to be culturally different to those patients in,for example, Canada. For these reasons, whenreferring to the different studies in our discussion,we highlight the time (ie, the year) the work waspublished in parentheses and the place (ie, country)the study took place.
ISSUES RELATED TO CONSENT ANDCOMMUNICATION OF RISKS AND BENEFITS
OF TRANSFUSION
Studies from a number of countries suggest thatthe process of consent (including the discussion of
risks and benefits) is often poorly recalled, thoughwhether this is because the consent was notproperly given or simply not remembered is notclear. Data derived from adult patients at a tertiarycare centre in Canada (published in 2005) showedthat while 80% of patients recalled talking withhealth care professionals about blood transfusionand signing a separate consent form for transfusion,44% had no recollection of the discussion oftransfusion risks (such as the risk of viral infectionsor bacterial contamination). In addition, 75%reported not being given information on the risksof being given the wrong blood, and 88% stated thatalternatives to a transfusion had not been discussed.As could be expected, patients who were given apamphlet on blood transfusions felt well informedand comfortable with the decision to accept blood,although only 19% recalled receiving such infor-mation.12 A study (in 1997) of postoperativecardiac surgery patients in England reported that71.5% said that they received no or little informa-tion before the operation on risks related withtransfusion.13 In parallel studies from Scotlandand England (published in 1993 and 1997,respectively), 47% of transfusion patients from 3different specialities (orthopedics, pediatric cardiacsurgery, and obstetrics) did not recall being told thatthey might require a transfusion14, and only 27% ofa group of medical and surgical patients recalledthat their verbal consent to transfusion had beenobtained.15 Many of these patients would haveliked to receive more information, specifically inthe area of complications, so they could have abetter understanding of the risks associated withthe transfusion itself. However, despite thesefindings, the majority felt they had received enoughinformation and understood why the transfusionwas necessary (82% and 92%, respectively).15
Other favorable findings from members of theSwedish public (published in 1998) reportedthat 95% were positive toward consenting toa transfusion.16
Transfusion Risk-Related Attitudes
It is likely that patients' transfusion-related riskperceptions will affect the extent to which they willconsent to a blood transfusion. Four studies haveshown that many patients are worried about thesafety of transfusions.17-20 One study (published in2001) on orthopedic patients in Ireland showed thatonly 11% had no concerns about the safety of blood

Table 1. Key Findings of Papers in the Review
First author, date Aims Methods Subjects Key findings of relevance to review
Al-Drees, 200818 To determine the attitude, belief,and knowledge about blood donationand transfusion
Quantitativequestionnaire
609 patients and membersof the public in Saudi Arabia
• 55.1% (n = 336) thought blood in blood banks was safe.• 17.4% (n = 106) believed all surgical procedures requiretransfusion.
• 20% (n = 122) of patients would refuse a transfusion evenif they were in need of one because of the risk of acquiring aninfectious disease.
• 49 % (n = 298) stated they would only accept a bloodtransfusion from a relative, the belief being that this wouldreduce the likelihood of acquiring an infection.
• 58% of women (n = 159) and 65% of men (n = 217)preferred to receive a blood transfusion from the same sex,as they believed this would reduce the likelihood of infection.
Chan, 200512 To characterize patients' recalland knowledge of the consent processfor a blood transfusion
Quantitativequestionnaire
344 patients at London HeathSciences Centre in Canada
• 80% (n = 275) of patients recalled discussing bloodtransfusion with a health care professional and signing aconsent form.
• 44% (n = 151) did not recall the discussion of specifictransfusion risks (of these, 61% reported no information on therisks of being given the wrong blood and 88% statedthat alternatives to a transfusion had not been discussed).
• 19% (n = 65) recalled receiving a pamphlet; these patientsfelt better informed and more comfortable with the decisionto accept blood (P b .05).
• 35% (n = 119) felt better informed and happier with thedecision to accept blood after the written consent process.
Farrell, 200224 To investigate public perception of riskof HIV infection associated withblood donation
Quantitativequestionnaire
168 undergraduate studentsin England
• All students were given information on the transfusion processas being safe, but those patients that were also giveninformation on the small risk of HIV were 11 times more likelyto think they could catch HIV than those that were not giventhis information.
Farrell, 200121 The effects of message framing onpatients' confidence in safety oftransfusion
Quantitative survey 254 undergraduate studentsin England
• Patients who are given information in a gain frame format(n = 85) were significantly more likely to have confidence inblood safety than those given information in a loss frameformat (n = 86).
• There were no differences between levels of confidence forthose patients that were given information in a loss frameformat or combined frame format (n = 83).
• As perceptions of the risks of transfusion increased, thewillingness to accept blood was reduced.
14
DAVIS
ETAL

Finucane, 200020 To investigate perception of risksrelated to transfusion
Quantitativetelephone survey
1204 members of the public in theUnited States
• 46.6 (n = 401) gave a moderate or high rating for theperc ed risk of blood transfusions
• 60.9 (n = 260) agreed or strongly agreed that bloodsup in the United States is safe and 36.2% (n = 154)disa ed or strongly disagreed.
• Patie who felt they had little control over their health(n = 28) were more likely to perceive transfusion as riskythan ose that felt they had a lot of control (n = 417).
• Patie that were female or educated to less than degreeleve ere more likely to perceive blood transfusion as risky.
Fitzgerald, 199925 To investigate patients' perspectivesof blood transfusions
Qualitative interviewstudy
19 hospital patients in Australia • Som mergency patients could not remember being toldthey ere to have a transfusion.
• Heal care professionals talked about transfusion and thesafe of transfusions but did not really give patients a chanceto v e any concerns—patients were given factualinfo tion before they consented but they were givenlittle portunity to discuss it.
• Ther ere numerous incidences of patients saying they hadbee ld something they did not understand—those who hadbes derstood were those with prior experience of transfusion.
• Patie were dissatisfied when they were not given enoughinfo tion
• One tient actually said they sneaked a look at the blood tomak ure it was the right one.
• In te s of self-care, 2 patients took an interest in the timingof t lood to ensure they received it at the correct time andone tient monitored the transfusion kept dripping,
Gerbert, 199122 Patients' perceptions of risk of AIDsin health care settings
Quantitativetelephone interviews
2000 members of the public in theUnited States
• 72% = 1440) of patients thought you could get AIDs froma bl transfusion.
Gray, 199314 Patients' experiences of bloodtransfusion
Quantitativeinterview
350 patients (or parents in the caseof pediatrics) who underwentsurgery in Scotland
• 12% = 42) of patients did not know a transfusion hadbee iven—20 of these patients thought they should havebee formed.
• 47% = 166) of patients could not recall being told theymig eceive a transfusion during their hospital stay.
• 16% = 55) of patients were concerned at having atran sion, 22 of these had discussed concerns with staffand felt they received a satisfactory answer.
(continued on next page)
15
PATIEN
TINVOLV
EMENTIN
BLO
OD
TRANSFU
SIO
NSAFET
Y
%eiv%plygrents4thntsl we ew
thtyoicrmaope wn tot unntsrmapae srmhe bpa(n
ood(n
n gn in(n
ht r(n
sfu18
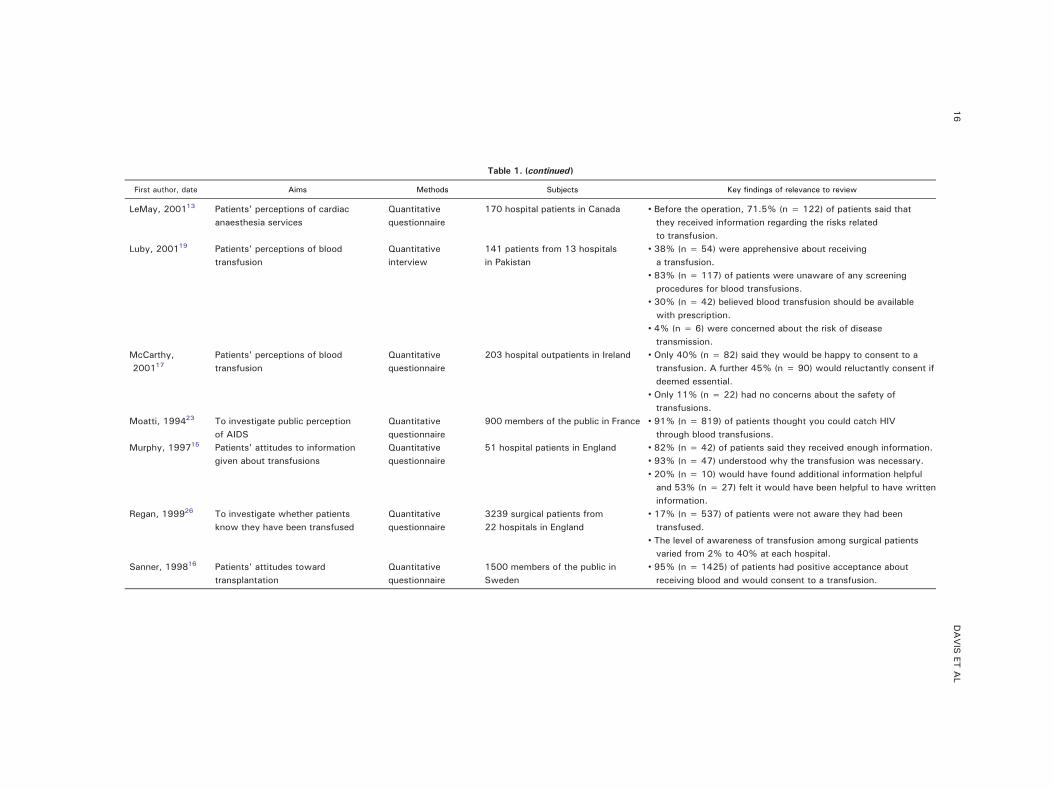
Table 1. (continued)
First author, date Aims Methods Subjects Key findings of relevance to review
LeMay, 200113 Patients' perceptions of cardiacanaesthesia services
Quantitativequestionnaire
170 hospital patients in Canada • Before the operation, 71.5% (n = 122) of patients said thatthey received information regarding the risks relatedto transfusion.
Luby, 200119 Patients' perceptions of bloodtransfusion
Quantitativeinterview
141 patients from 13 hospitalsin Pakistan
• 38% (n = 54) were apprehensive about receivinga transfusion.
• 83% (n = 117) of patients were unaware of any screeningprocedures for blood transfusions.
• 30% (n = 42) believed blood transfusion should be availablewith prescription.
• 4% (n = 6) were concerned about the risk of diseasetransmission.
McCarthy,200117
Patients' perceptions of bloodtransfusion
Quantitativequestionnaire
203 hospital outpatients in Ireland • Only 40% (n = 82) said they would be happy to consent to atransfusion. A further 45% (n = 90) would reluctantly consent ifdeemed essential.
• Only 11% (n = 22) had no concerns about the safety oftransfusions.
Moatti, 199423 To investigate public perceptionof AIDS
Quantitativequestionnaire
900 members of the public in France • 91% (n = 819) of patients thought you could catch HIVthrough blood transfusions.
Murphy, 199715 Patients' attitudes to informationgiven about transfusions
Quantitativequestionnaire
51 hospital patients in England • 82% (n = 42) of patients said they received enough information.• 93% (n = 47) understood why the transfusion was necessary.• 20% (n = 10) would have found additional information helpfuland 53% (n = 27) felt it would have been helpful to have writteninformation.
Regan, 199926 To investigate whether patientsknow they have been transfused
Quantitativequestionnaire
3239 surgical patients from22 hospitals in England
• 17% (n = 537) of patients were not aware they had beentransfused.
• The level of awareness of transfusion among surgical patientsvaried from 2% to 40% at each hospital.
Sanner, 199816 Patients' attitudes towardtransplantation
Quantitativequestionnaire
1500 members of the public inSweden
• 95% (n = 1425) of patients had positive acceptance aboutreceiving blood and would consent to a transfusion.
16
DAVIS
ETAL

17PATIENT INVOLVEMENT IN BLOOD TRANSFUSION SAFETY
transfusion.17 Three other studies from SaudiArabia (published in 2008), Pakistan (publishedin 2001), and the United States (published in2000), respectively, have reported that only55.1% of hospital patients believed that blood inblood banks was safe,18 38% of hospital patientswere apprehensive about receiving a transfu-sion,19 and 45% of the general public provideda moderate or high rating for perceived risksassociated with transfusion for self and family.20
In this latter study, more than 36% of respondentsalso “disagreed” or “strongly disagreed” with thestatement that “the blood supply in the UnitedStates is safe,” and a third of respondents wouldnot accept blood because they viewed this bloodas potentially “unsafe.” This finding was partic-ularly evident in women and those educated toless than degree level. As might be expected,people who perceived transfusion as risky wereless likely to accept transfusion as an interven-tion.20 This finding was also reflected in anotherstudy in England (published in 2001) on students'risk perceptions toward blood transfusions.21
Further data obtained from orthopedic patientsin Ireland (published in 2001) reported that only40% of those questioned said they would behappy to have a transfusion; another 45% wouldagree to it reluctantly only if it was consideredabsolutely essential.17
Patients are of course correct that there are risksassociated with transfusion, but these studiessuggest that some patients perceive transfusionas frankly dangerous. The variation in theperception of risk associated with transfusion inthese studies may be associated with a realvariation in the actual risk in different countriesor by media coverage of specific high-risk cases.The studies of transfusion risk in Ireland17 and theUnited States20 may have been stimulated by thepublicity given to the high risks of hepatitis Cvirus (HCV) and human immunodeficiency virus(HIV) in the 1990s.
Why Patients May Refuse Transfusions
In some cases, the perceived risk of transfusionmay be so high that patients might actually refusea transfusion. Indeed, this was revealed in datacollected from patients and members of the publicin Saudi Arabia (published in 2008) in which 20%would refuse a transfusion even if they were inneed of one because of the perception of risk of
acquiring an infectious disease. In addition, 49%stated that they would only accept a bloodtransfusion from a relative, the belief being thatthis would reduce the likelihood of acquiring aninfection.18 Alternative data from the public(published in 1991) derived from the United Statesfound that 72% of those questioned thought that itwas “likely” that a patient could contract HIVinfection from having a blood transfusion.22
Analogous findings were yielded on 2 face-facesurveys (also on members of the public in France(published in 1994); 91% of those interviewedthought patients were at risk of contracting HIVfrom a blood transfusion.23 However, contrary tothe above findings, data derived from hospitalpatients in Pakistan (published in 2001) reportedthat although 38% were apprehensive about recei-ving a transfusion, only 4% were concerned aboutthe risk of disease transmission.19 As in theprevious section on patients' attitudes to transfu-sion, the likelihood of refusing a transfusionbecause of a perception of a high risk of infectionassociated with transfusion is almost certainlyassociated with the actual risk of infection, and thisvaried in the studies described in this section indifferent countries and at different times.
The Effect of Information Formatting/Structuringon Risk Perception
Research also suggests that the way in whichrisk-related information is conveyed to patientscan affect their perceptions. This is reflected in 2experimental studies both conducted in Englandon an undergraduate student population. The firststudy (published in 2001) provided participantswith factual information about blood transfusion,but framed it in 3 different ways: (1) gain frame(ie, lives saved from transfusion), (2) loss frame(ie, lives lost from transfusion), or (3) a combinedframe (ie, a loss expressed in a positive context).Participants that received the gain frame infor-mation were significantly more confident with thesafety of blood transfusion than those in the other2 conditions.21 The second study (published in2002) allocated participants into 1 of 3 condi-tions: (1) information about the transfusionprocess as being safe, (2) the same informationas condition 1 but also with a small risk ofcontracting HCV, or (3) the same information ascondition 1 but with the risk of contracting HIV.The results showed that although there were no

18 DAVIS ET AL
differences in the HCV-cued condition, patientsin the HIV cued were 11 times more likely tothink that they could catch HIV through atransfusion when compared with the no-cuecondition (condition 1).24
Willingness to Participate inTransfusion-Related Behaviors
There is almost no information on whethertransfusion patients might be willing to engage intransfusion-related behaviors. However, one smallstudy in Australia (published in 1999) revealed 4examples of patients wanting to take an active rolein checking processes.25 One patient said that theysneaked a look at the unit of blood that the nursewas giving them to ensure they were being givenblood with the correct blood group. Two patientssaid that they would like to have a role in the timingof the blood to ensure that it is administered when itshould be, and one patient undergoing prolongedchemotherapy was worried about the state of hisveins and so monitored the transfusion keptdripping and the cannula site was protected so thevein could be used again.
Patients' Awareness and Understanding ofBeing Transfused
Preliminary information derived from Australia(published in 1999) indicates that patients do notalways comprehend what they have been told aboutblood transfusion, though, as would be expected,patients who had been transfused before had abetter understanding.25 In addition, a study onsurgical patients in England (published in 1999)revealed that 17% were not even aware they hadbeen transfused.26
SUMMARY OF KEY FINDINGS
Research on patient experience and involvementin transfusion is sparse and scattered acrossdifferent countries and clinical settings. However,this small group of studies suggests that manypatients have a very limited understanding of thetrue benefits and risks of transfusion. It seems thatmany people, whether current transfusion patientsor members of the public, have considerableanxieties about transfusion with patients in somesettings regarding it as so unsafe that they mightrefuse a transfusion, even though it was consid-ered clinically necessary. Patients who have
received transfusion often do not recall the consentprocess, either because they were not given fullinformation or because they rapidly forgot it.Overall, the findings suggest that communicationwith both transfusion patients and the generalpublic needs to be improved. In addition, it is clearthat patients are concerned about transfusion-related risks, which may mean that they wouldbe willing to be more actively engaged intransfusion safety. The remainder of the articleaddresses these issues.
POTENTIAL FOR PATIENT INVOLVEMENT INTHE BLOOD TRANSFUSION PROCESS
Although there is little research on these topics,the degree to which patients might be activelyengaged in the transfusion process can be assumedto depend on a number of factors. First, patientsmust have knowledge on how to be involved—wecannot expect patients to participate if they do notknow how and when they can. Second, patientsmust be able to participate—this ability in part isderived from the patient's knowledge but is alsolargely dependent on their physical and cognitivecapacity. Third, they have to be willing toparticipate—in other words, they have to want totake on an active role.
In recent years, a number of organizations in theUK have introduced initiatives (such as leaflets andposters) aimed at informing patients about bloodtransfusions, with the aim of improving theirknowledge, ability, and willingness to partici-pate.27-30 However, although these initiatives arewell intentioned, we have little information aboutwhether they are read, how effective they are, orwhether there are any adverse effects of providingsafety-related information. More importantly, theprovision of general information is only the firststep in patient engagement. We consider that itwould be useful to examine the transfusion processsystematically to identify specific ways in whichpatients can be involved. In the following sections,we consider some of the key opportunities forpatient participation in more detail before, during,and after transfusion.
Figure 1 depicts themain opportunities for patientinvolvement in the transfusion process. The ways inwhich patients could participate were identified byreferring to existing national initiatives and recom-mendations and expert consultation with consultanthematologists and nurses. The pretransfusion and

19PATIENT INVOLVEMENT IN BLOOD TRANSFUSION SAFETY
during transfusion checks would of course only beapplicable to those patients that are conscious whilebeing transfused, whereas the posttransfusion
Figure 1. Patient involvement
checks can be generalized to both those patientsconscious and unconscious during the actualadministration of the blood.
in the transfusion process.

20 DAVIS ET AL
OPPORTUNITIES FOR PATIENT INVOLVEMENTBEFORE THE TRANSFUSION
Assessing Clinical Need
Before consenting to the transfusion, the patientcould be involved more actively in the assessmentof the clinical need for the transfusion (eg, whetherthe transfusion is appropriate or necessary). This isimportant because although there has been con-siderable progress in the avoidance of inappropri-ate transfusion, as evidenced by a near 20%decrease in the use of red cell units in Englandsince 2002/2003, audits of transfusion practiceconsistently identify that 20% or more of transfu-sions of red cells, platelets, and fresh frozenplasma are used outside the recommendations innational guidelines.31 An example of the involve-ment of patients in considering the need fortransfusion is the self-assessment of bleeding bypatients with severe thrombocytopenia undergoingintensive chemotherapy or hematopoietic stem celltransplantation for hematologic malignancies whileparticipating in a trial of different strategies forplatelet transfusion.32
New initiatives are needed to ensure that blood isonly used when it is clinically indicated. There is aneed for research to investigate the extent to whichpatients would be comfortable questioning healthcare professionals about the appropriateness ofreceiving blood, so that new initiatives for patientinvolvement in transfusion decision making can bedesigned and implemented.
Providing Informed Consent
The next step in the transfusion sequence atwhich patient engagement is critical (and is indeedrequired where possible) is by providing consent toreceiving blood. It is standard policy in everyhospital in the United Kingdom that patients,providing they are conscious, should provide theirconsent to being transfused if this is requiredduring their care. For example, patients undergo-ing surgery are required to sign a surgical consentform to indicate that they are willing to betransfused if it becomes necessary. However, forpatients to provide their informed consent, theyneed to be given information on the risks, benefits,and alternatives (if any) to the transfusion.Research we have reviewed indicates, however,that patients' often do not recall such discussionstaking place.12,14,15
Identity Check, Checking, and Administrationof Product
Perhaps the most important way that patientscould contribute to transfusion safety is by helpingto reduce misidentification errors. Blood transfusionis one of the major areas where serious clinicalconsequences, even death, related to patient mis-identification can occur.33 The annual SeriousHazards of Transfusion report for 2008 revealedthat 262 blood transfusion incidents (of a total of1040) were related to incorrect blood componenttransfusion, 47 of these were specifically adminis-tration of the wrong blood.34 Involving patients at anumber of stages in the transfusion sequence couldhelp to prevent the occurrence of these incidents.For example, before the ordering of the bloodpatients could participate in ensuring that the bloodsample for compatibility testing is correctly la-belled. Before transfusion, patients could participatein the identity check and in the administration of theproduct. At present, we do not know how willingpatients would be to engage in these checkingbehaviors. In addition, many patients may not havethe ability to participate. Often patients that aretransfused receive blood in the operating room orintensive care unit, settings where the patient wouldbe sedated or seriously ill. Under these circum-stances, the patient would clearly not have thecognitive capacity to participate.
POTENTIAL PATIENT INVOLVEMENT DURINGAND AFTER TRANSFUSION
Recording
During the transfusion itself, patients could makesure that their observations (eg, blood pressure,pulse, temperature, and respiratory rate) are taken atregular intervals as required and can notify healthcare professionals if this is not done. This of coursedepends on the extent to which patients understandthe transfusion process and what to expect.
Responding to an Adverse Event
The final point at which there are opportunitiesfor the patient to participate is by responding to atransfusion-related adverse event. If patients feelunwell, they can report this to a health careprofessional so that prompt action can be taken tomitigate the effects. Patients need to be informedthat they are expected to do this—obviously, they

21PATIENT INVOLVEMENT IN BLOOD TRANSFUSION SAFETY
can only do this if they are conscious and aware thata transfusion is taking place.
IMPLICATIONS AND SUGGESTIONS FORFUTURE RESEARCH
There are a considerable number of ways inwhich patients might be effectively engaged in thetransfusion process. In our view, the main prioritiesfor research in this area are as follows:
• Consent: Patients' attitudes toward consentand information provision could be examined.Patients often have little memory of theconsent process or of any information beingprovided. However, we do not know whetherthey were not given information or simply didnot remember it.
• Shared decision making: Transfusion may beoffered when it is not strictly necessary, and therisks of transfusion may outweigh the potentialbenefits. We could explore how patients, beinggenerally more risk averse than clinicians, canbe effectively engaged in transfusion decisions.
• Effectiveness of information leaflet: Althoughcurrent patient-focussed initiatives (eg, leaf-lets) are well intentioned, there is a significantlack of literature to indicate their effectivenessin terms of (1) imparting knowledge useful topatients, (2) encouraging patient involvement,and (3) reducing rates of transfusion-relatedcomplications and improving transfusion prac-tice as a result of patient involvement. Inaddition, and perhaps more importantly, theextent to which patients know about theseinitiatives and would be willing to adhere to therecommendations remains to be discovered.
• Perception of risk: Patients' attitudes totransfusion-related information provisioncould be explored, including which sourcesof information they trust, because this canimpact largely on patients' perceptions of risksof transfusions and their subsequent willing-ness to consent to the procedure. Research hasshown that some patients have misperceptionsabout the safety of blood transfusion, but theextent of these misperceptions or how theyinfluence willingness to have transfusionsare unknown.
• Framing of safety information: Messageframing may be a useful technique forpresenting information about the risks of
transfusion—preliminary evidence has shownthat gain frame results in higher levels ofconfidence about the safety of blood transfu-sions; this finding needs to be replicated andinvestigated in more detail.
• Potential adverse effects of patient informationand involvement: Although the timely provi-sion of accurate, appropriate informationseems a worthy aim, it may not be appropriatefor all patients. We need to understand whethersome patients are made unduly anxious bysuch information and how to deliver informa-tion selectively and appropriately.
• Patient willingness to engage in safety checks:Patient involvement in transfusion safety willnot be appropriate for everyone. Factors thatcould affect patient involvement in the specificcontext of transfusion safety should be exam-ined. Research within the wider paradigm ofpatient involvement in safety indicates that anumber of factors will affect patients' willing-ness and ability to participate in transfusion-related behaviors. These factors include thepatient (eg, knowledge and beliefs, demogra-phics), the patient's illness (eg, stage andseverity), the health care professionals involvedin the patients care (eg, their knowledge andbeliefs about patient involvement), the settingin which care is received (eg, ambulatory vsinpatient), and the specific task that the patientis required to participate in (eg, asking ques-tions, checking procedures).9 All these need tobe explored in the context of transfusion.
• Health care professional education: In termsof health care professionals learning how tomeet patients' expectations and deliveringtransfusion-related information in a patient-centered way, there is no better individual onhow to do this than the patient themselves.Efforts therefore need to be made to investigateeffective strategies that health care profes-sionals, including doctors, can adopt to elicitand meet patients' transfusion-related needs.Implementation of the selected strategies forthe different parts of the transfusion processwill require further education and training ofthe staff carrying out that procedure.
Implications for Clinical Practice
There is considerable potential for patients tobecome more engaged in the transfusion process to

22 DAVIS ET AL
provide both a better understanding of transfusionand to support better practice. More research isneeded to assess how and in what activities patientsmight be engaged. However, the existing literature,sparse though it is, does suggest some immediatepractical steps.Patients want to be better informed about the risks
and benefits of transfusion as well as the transfusionprocess itself. Hospital processes for providinginformation could be improved to ensure thatinformation is routinely provided in advance oftransfusion to those patients who are likely to betransfused. There should be similar processes forinforming patients who are transfused in emergen-cies when they have sufficiently recovered. Hospitalstaff should be trained to provide information aboutblood transfusion and have the time to talk to thepatient as well as handing out written material. Newways of making information more accessible usingdifferent media including the Internet should also beexplored. Processes should be in place to documentthat information is provided and be subject to regularaudit. Information should be available in differentlanguages, appropriate to the local population.A number of factors may perpetuate poor patient
assimilation and retention of medical information.As well as ensuring information is readily available,it may be more effectively received if specificinformation is targeted for different types of patient,for example, for children and adults, and fordifferent patient groups (eg, surgical, leukemia,sickle cell disease). The timing of providinginformation may also play a role in how it isreceived; for example, preadmission clinics maynot be conducive to the retention of information orto provide the opportunity for asking questions asstaff are often under time pressure. Likewise, theprovision of information very close to the time oftransfusion may not be optimal, as patients may beexperiencing physical and/or mental distress fromtheir illness that may interfere with their ability toretain information.If patients are better educated about the risks of
transfusion and the steps taken to minimize the
risks, they will be able to make more informeddecisions about the safety of their care and mayhave less exaggerated perceptions of risk. Theymay also be more willing to engage in measures tosupport staff to deliver good practice. Patients whoreceive regular transfusions and are already wellinformed may be the most willing to engage withstaff in this way.
CONCLUSIONS
The concept of more active involvement ofindividual patients in steps in the transfusionpathway is a more complex issue than that ofproviding information to promote understanding. Itrequires detailed consideration and more research.How willing patients are to engage in transfusionprocedures by challenging clinical staffs' decisionsabout the need for transfusion or to participate in thebefore-, during-, and after-transfusion safety checksremains to be determined. In addition, the extentto which clinical staff would be willing to bechallenged or to support patient involvement in thiscontext needs to be explored. With the lack ofsufficient evidence, it could be argued that patientinvolvement might have the potential to causedelay, result in confrontation with clinical staff, andimpair rather than improve practice. There is muchwork to be done before the effectiveness of activepatient involvement in blood transfusion is deter-mined and before specific measures can beimplemented. We believe that this is a potentiallyimportant step in transfusion safety and, morewidely, in ensuring that the provision of transfusionservices is always centered on the needs andexperiences of patients and their families.
ACKNOWLEDGMENTS
We would like to thank all the hematology staffat St Mary's Hospital, London, and the JohnRadcliffe Hospital, Oxford, that provided feedbackon this work. In particular, we would like to thankRachel Moss for her contribution.
REFERENCES
1. Dzik WH: Emily Cooley lecture 2002: Transfusion safetyin the hospital. Transfusion 43:1190-1198, 2003
2. McClelland DBL, Phillips P: Errors in blood transfusionin Britain: Survey of hospital haematology departments. Br MedJ 308:1205-1206, 1994
3. Sazama K: Reports of 355 transfusion-associated deaths:1976 through 1985. Transfusion 30:583-590, 1990
4. US Food and Drug Administration: Fatalities reported toFDA following blood collection and transfusion. Annual summaryfor fiscal year 2008. www.fda.gov/BiologicsBloodVaccines/

23PATIENT INVOLVEMENT IN BLOOD TRANSFUSION SAFETY
SafetyAvailability/ReportaProblem/TransfusionDonationFatalities/ucm113649.htm
5. Serious Hazards of Transfusion: Annual report 2008.Serious hazards of transfusion scheme, Manchester, UK, 2009.www.shotuk.org
6. Linden JV, Paul B, Dressler KP: A report of 104transfusion errors in New York State. Transfusion 32:601-606,1992
7. Murphy MF, Staves J, Davies A, et al: How do weapproach a major change program using the example of thedevelopment, evaluation, and implementation of an electronictransfusion management system. Transfusion 49:829-837,2009
8. Coulter A, Ellins J: Patient-focused interventions. Areview of the evidence. London, Picker Institute Europe/ HealthFoundation; 2006
9. Davis R, Sevdalis N, Jacklin R: Patient involvement insafety: What factors influence patient participation and engage-ment? Health Expectations 10:259-267, 2007
10. Davis R, Koutantji M, Vincent C: How willing arepatients to question healthcare staff on issues related to thequality and safety of their healthcare? An exploratory study.Qual Safe Health Care 17:90-96, 2008
11. Vincent C, Coulter A: Patient safety: What about thepatient? Qual Safe Health Care 11:76-80, 2002
12. Chan T, Eckert K, Venesoen P, et al: Consenting to blood:What do patients remember? Trans Med 15:461-466, 2005
13. LeMay S, Hardy JF, Harel F, et al: Patients' perceptionsof cardiac anesthesia services: A pilot study. Can J Anesth 48:1127-1142, 2001
14. Gray A, Murphy WG: A study of patients' perceptionsand experiences of blood transfusion. Transfus Med Suppl 1:81(abstract)
15. Murphy MF, Docherty S, Greenfield P: Survey of theinformation given to patients about blood transfusion and theneed for consent before transfusion. Trans Med 7:287-288,1997
16. Sanner MA: Giving and taking – to whom and from?Patient's attitudes toward transplantation of organs and tissuefrom different sources. Clin Transplantation 12:530-537, 1998
17. McCarthy T, Butler KM, Carey M, et al: Irish orthopedicpatients' attitudes to blood transfusion. Ir Med J 94:110-111,2001
18. Al-Drees AM: Attitude, belief and knowledge aboutblood donation and transfusion in Saudi population. Pak J MedSci 24:74-79, 2008
19. Luby SP, Niaz Q, Siddiqui S, et al: Patients' perceptionsof blood transfusion risks in Karachi, Pakistan. Int J Infect Dis 5:24-26, 2001
20. Finucane ML, Slovic P, Mertz CK: Public perception ofthe risk of blood transfusion. Transfusion 40:1017-1022, 2000
21. Farrell K, Ferguson E, James V, et al: Confidence in thesafety of blood for transfusion: The effect of message framing.Transfusion 41:1335-1340, 2001
22. Gerbert B, Maguire BT, Sumser J: Public perception ofrisks of AIDS in health care settings. Aids Ed Prev 3:322-327,1991
23. Moatti JP, Dab W, Quenel P, et al: Social perception ofAIDS in French general public: 1987-1990 evolution in Parisregion. Psych Health 9:285-296, 1994
24. Farrell K, Ferguson E, James V, et al: Public perception ofthe risk of HIV infection associated with blood donation: Therole of contextual cues. Transfusion 42:679-683, 2002
25. Fitzgerald M, Hodgkinson B, Thorp D: Blood transfusionfrom the recipient's perspective. J Clin Nurs 8:593-600, 1999
26. Regan F, Hewitt P, Vincent B, et al: Do patients knowthey have been transfused? Vox Sang 76:248-249, 1999
27. ‘Please Ask' about blood transfusions and surgery http://www.npsa.nhs.uk/pleaseask/beinformed/transfusions/#RPRBaccessed 20/1/10, National Patient Safety Agency
28. Right patient, right blood: advice for safer blood transfu-sions http://www.nrls.npsa.nhs.uk/resources/?entryid45=59805accessed 20/1/10, National Patient Safety Agency
29. Is my blood transfusion necessary? http://www.transfusionguidelines.org.uk/docs/pdfs/nbtc_taw_poster_1.pdfaccessed 20/1/10, National Blood Transfusion Committee.
30. Will I get the right blood? http://www.transfusionguidelines.org.uk/docs/pdfs/nbtc_taw_poster_3_new.pdf accessed 20/1/10,National Blood Transfusion Committee
31. Qureshi H, Lowe D, Dobson P, et al: Nationalcomparative audit of the use of platelet transfusions in the UK.Transfus Clin Biol 14:509-513, 2007
32. Stanworth SJ, Dyer C, Choo L, et al: Do all patientswith hematological malignancies and severe thrombocytopenianeed prophylactic platelet transfusions? Background, rationaleand design of a clinical trial (TOPPS) to assess theeffectiveness of prophylactic platelet transfusions. TransfusMed Rev 24:163-171, 2010
33. World Health Organisation: Patient identification. PatientSaf Solut 1:2
34. Serious Hazards of Transfusion scheme: Annual report.SHOT, Manchester; 2008