blood physiology - zona.fmed.uniba.sk · blood physiology lecture 1 objectives 1. blood composition...
TRANSCRIPT
Blood physiology
for the dentistry students
© Katarina Babinska, Institute of Physiology, FM CU 2020
Blood tests
• a routine examination in medicine
• help to make diagnosis and to treat
Physiology
• studies the function of a healthy human body
• if you know what is normal, you can detect
abnormalities/diseases and treat them
Is the result of the blood test normal?
What is my patient's diagnosis?
Is it an inflammation?
Transfusion for my patient– what blood type?
..........
http://t3.gstatic.com/images?q=tbn:ANd9GcSK0IRJLCYguw
O1YN9x2EA02zYEqub-9-NJ2tnvC9Fh5apPtJnS
Blood Physiology
Lecture 1
Objectives
1. Blood composition and functions
2. Erythrocytes – composition, function, haemoglobin
3. Blood groups – ABO system, Rhesus system
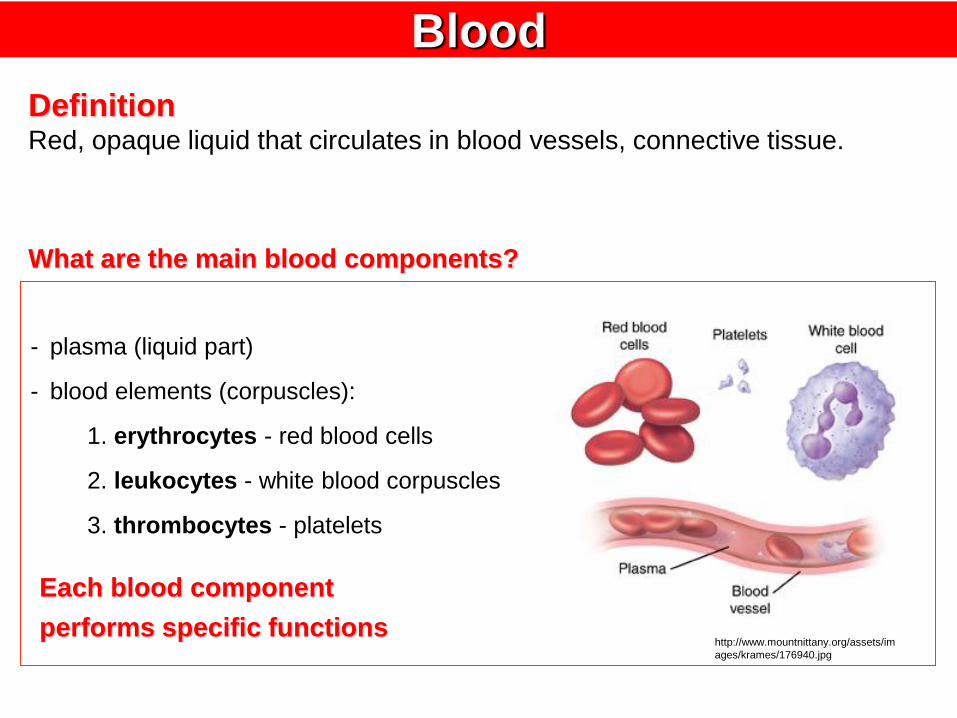
Blood
- plasma (liquid part)
- blood elements (corpuscles):
1. erythrocytes - red blood cells
2. leukocytes - white blood corpuscles
3. thrombocytes - platelets
Each blood component
performs specific functionshttp://www.mountnittany.org/assets/im
ages/krames/176940.jpg
DefinitionRed, opaque liquid that circulates in blood vessels, connective tissue.
What are the main blood components?
1. transportation (from one part of the body to another):
- O2 and CO2 (lungs tissues)
- nutrients (gut – liver/tissues)
- waste products to places of their elimination
- hormones
- immune cells and molecules
- heat (produced mainly in liver, muscles → all over the body)
- medicaments, etc.
Functions of blood
Normal blood volume
7-8 % of body weight
male 6 l
female 4,5 l
2. haemostasis
= bleeding arrest
- components of blood (platelets, clotting factors) are
activated in case of bleeding in order to stop the bleeding
3. Blood generates blood pressure (hydrostatic pressure)
- blood is pressing on the vessel walls
Functions of blood
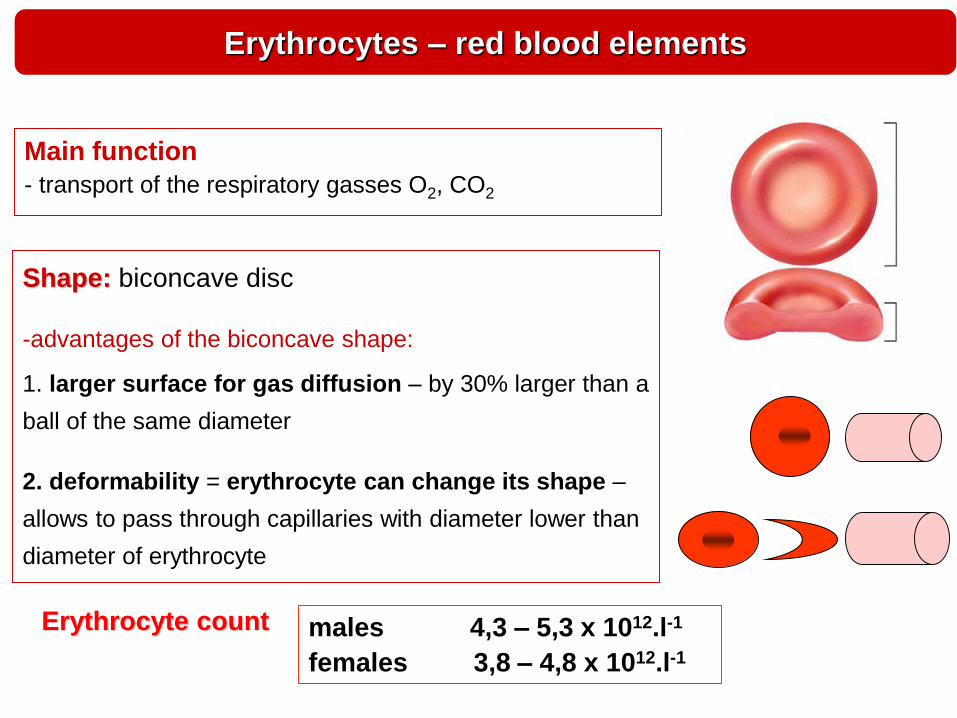
Erythrocytes – red blood elements
Main function
- transport of the respiratory gasses O2, CO2
Shape: biconcave disc
-advantages of the biconcave shape:
1. larger surface for gas diffusion – by 30% larger than a
ball of the same diameter
2. deformability = erythrocyte can change its shape –
allows to pass through capillaries with diameter lower than
diameter of erythrocyte
Erythrocyte count males 4,3 – 5,3 x 1012.l-1
females 3,8 – 4,8 x 1012.l-1
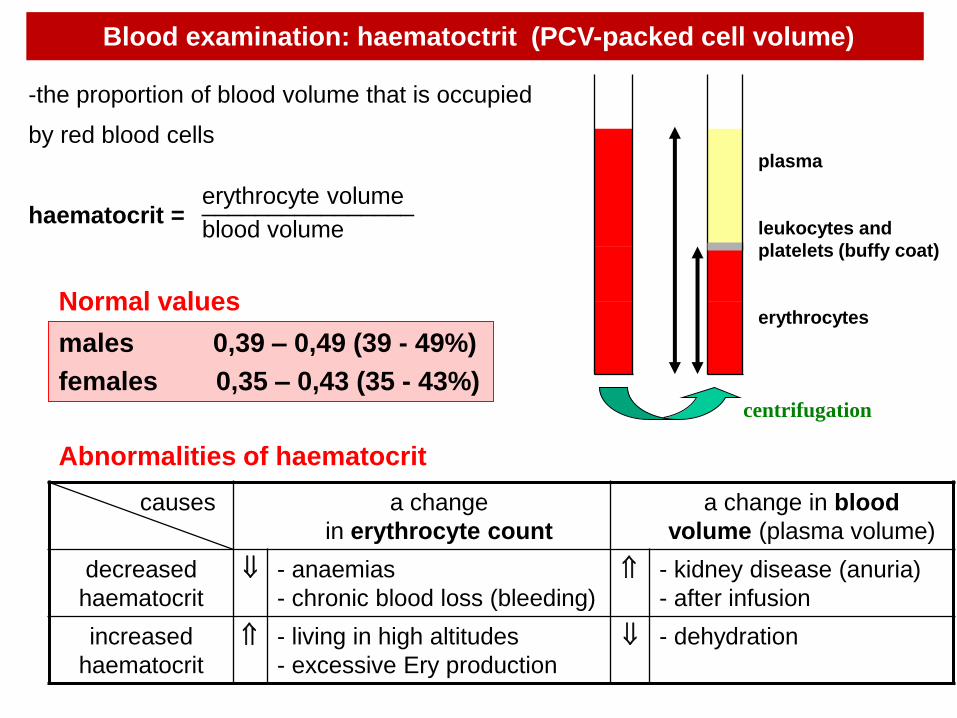
-the proportion of blood volume that is occupied
by red blood cells
haematocrit =
plasma
leukocytes and
platelets (buffy coat)
erythrocytes
erythrocyte volume________________blood volume
causes a change
in erythrocyte count
a change in blood
volume (plasma volume)
decreased
haematocrit
- anaemias
- chronic blood loss (bleeding)
- kidney disease (anuria)
- after infusion
increased
haematocrit
- living in high altitudes
- excessive Ery production
- dehydration
centrifugation
males 0,39 – 0,49 (39 - 49%)
females 0,35 – 0,43 (35 - 43%)
Normal values
Abnormalities of haematocrit
Blood examination: haematoctrit (PCV-packed cell volume)
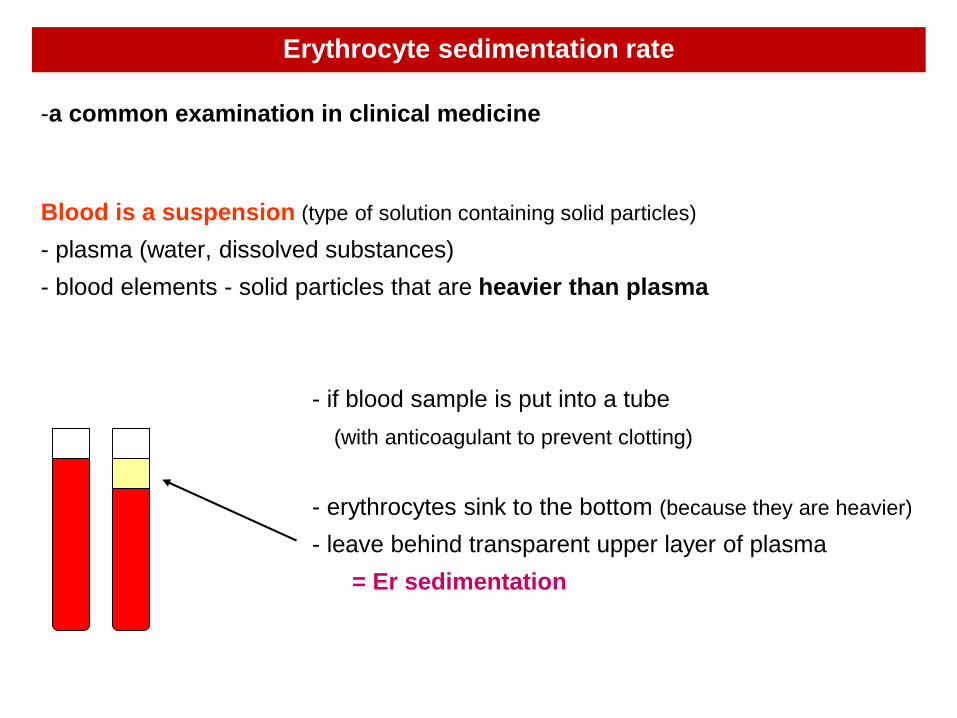
Erythrocyte sedimentation rate
-a common examination in clinical medicine
Blood is a suspension (type of solution containing solid particles)
- plasma (water, dissolved substances)
- blood elements - solid particles that are heavier than plasma
- if blood sample is put into a tube
(with anticoagulant to prevent clotting)
- erythrocytes sink to the bottom (because they are heavier)
- leave behind transparent upper layer of plasma
= Er sedimentation
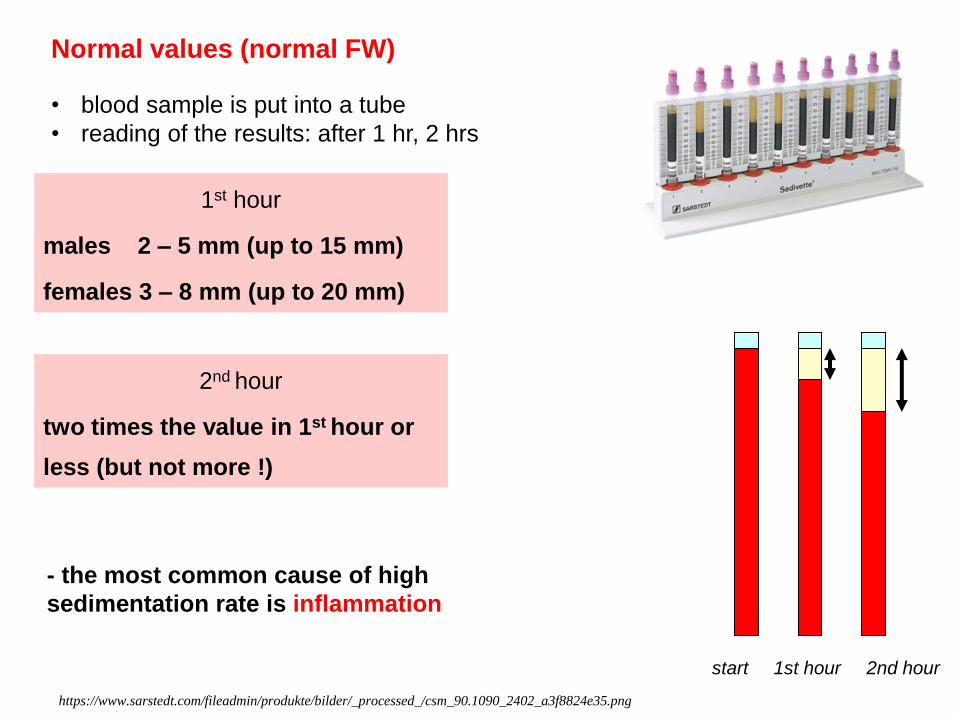
start 1st hour 2nd hour
Normal values (normal FW)
https://www.sarstedt.com/fileadmin/produkte/bilder/_processed_/csm_90.1090_2402_a3f8824e35.png
• blood sample is put into a tube
• reading of the results: after 1 hr, 2 hrs
1st hour
males 2 – 5 mm (up to 15 mm)
females 3 – 8 mm (up to 20 mm)
2nd hour
two times the value in 1st hour or
less (but not more !)
- the most common cause of high
sedimentation rate is inflammation
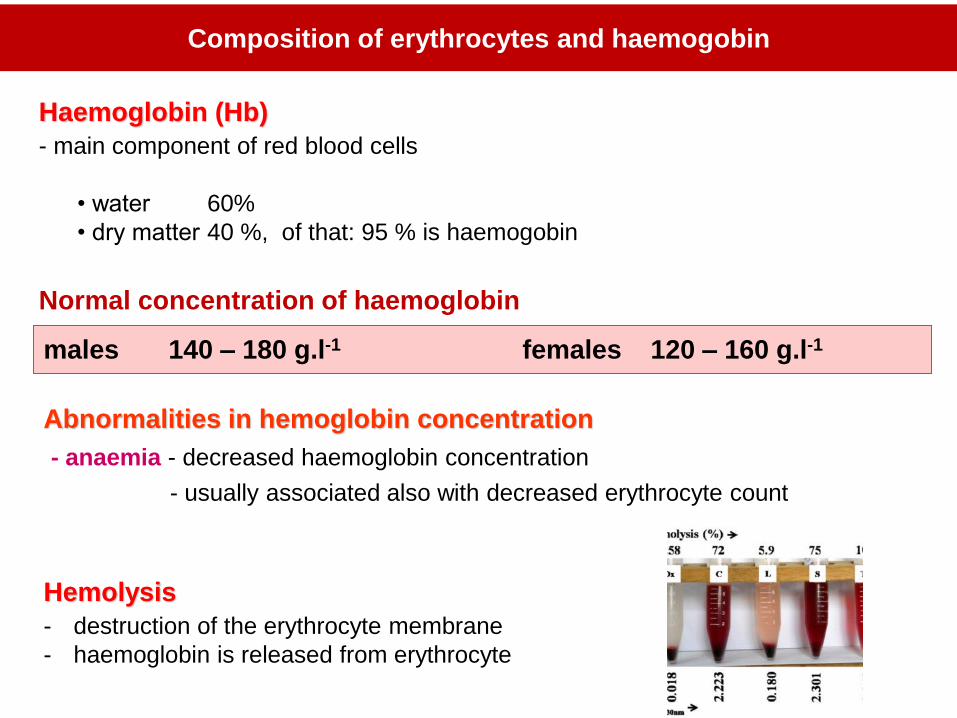
Haemoglobin (Hb)
- main component of red blood cells
• water 60%
• dry matter 40 %, of that: 95 % is haemogobin
Composition of erythrocytes and haemogobin
Abnormalities in hemoglobin concentration
- anaemia - decreased haemoglobin concentration
- usually associated also with decreased erythrocyte count
males 140 – 180 g.l-1 females 120 – 160 g.l-1
Normal concentration of haemoglobin
Hemolysis
- destruction of the erythrocyte membrane
- haemoglobin is released from erythrocyte
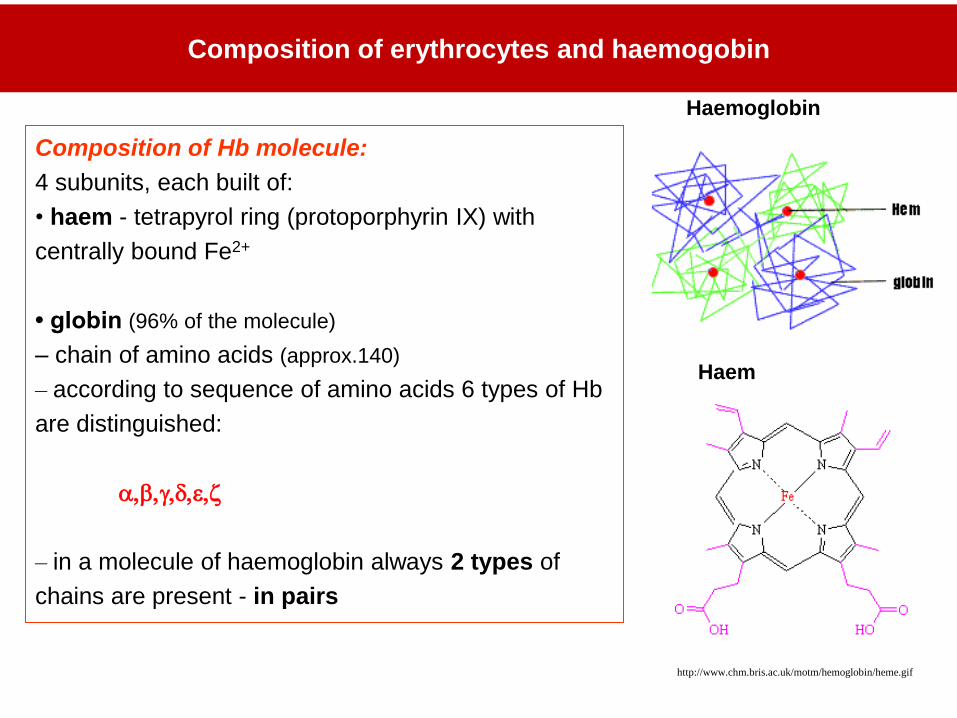
Composition of Hb molecule:
4 subunits, each built of:
• haem - tetrapyrol ring (protoporphyrin IX) with
centrally bound Fe2+
• globin (96% of the molecule)
– chain of amino acids (approx.140)
– according to sequence of amino acids 6 types of Hb
are distinguished:
a,b,,d,e,
– in a molecule of haemoglobin always 2 types of
chains are present - in pairs
http://www.chm.bris.ac.uk/motm/hemoglobin/heme.gif
Haemoglobin
Haem
Composition of erythrocytes and haemogobin
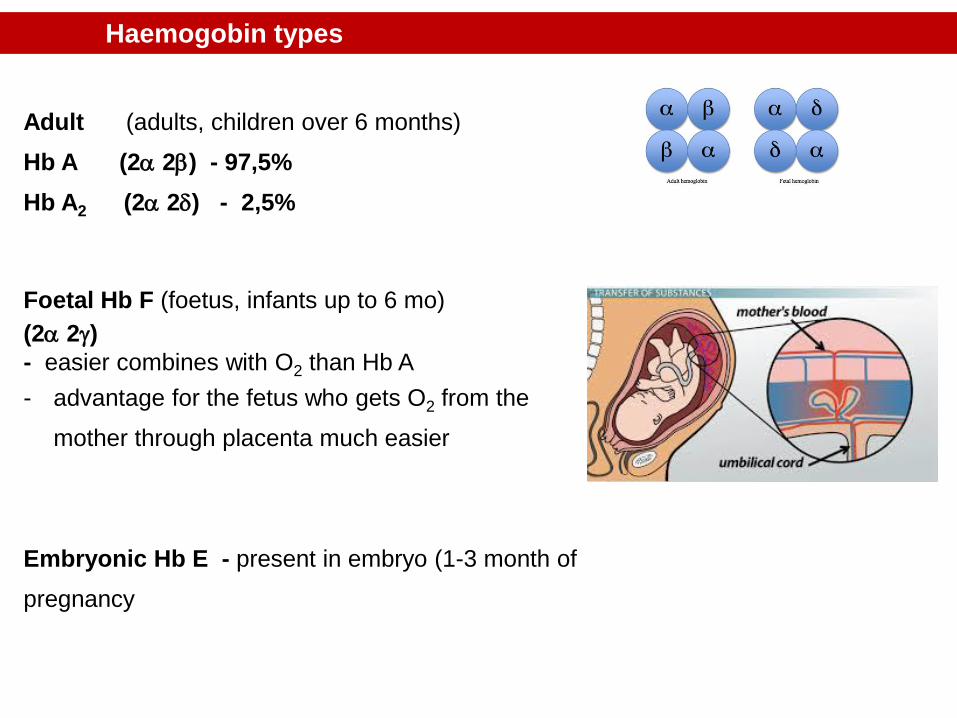
Adult (adults, children over 6 months)
Hb A (2a 2b) - 97,5%
Hb A2 (2a 2d) - 2,5%
Foetal Hb F (foetus, infants up to 6 mo)
(2a 2)
- easier combines with O2 than Hb A
- advantage for the fetus who gets O2 from the
mother through placenta much easier
Embryonic Hb E - present in embryo (1-3 month of
pregnancy
Haemogobin types
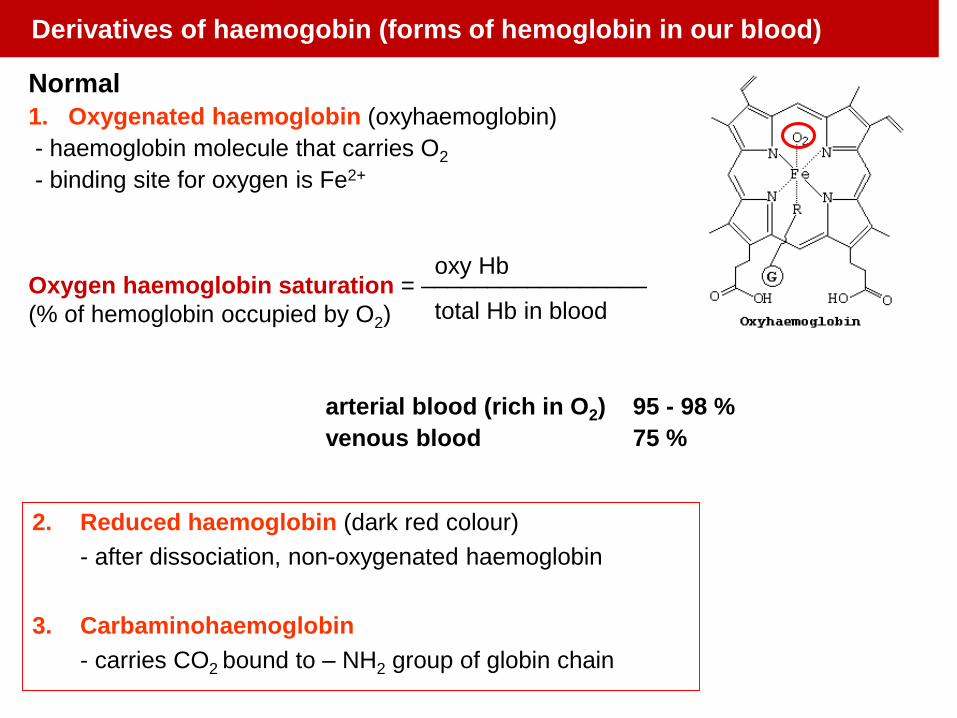
Normal
1. Oxygenated haemoglobin (oxyhaemoglobin)
- haemoglobin molecule that carries O2
- binding site for oxygen is Fe2+
oxy Hb_________________
total Hb in blood
arterial blood (rich in O2) 95 - 98 %
venous blood 75 %
2. Reduced haemoglobin (dark red colour)
- after dissociation, non-oxygenated haemoglobin
3. Carbaminohaemoglobin
- carries CO2 bound to – NH2 group of globin chain
Oxygen haemoglobin saturation =
(% of hemoglobin occupied by O2)
Derivatives of haemogobin (forms of hemoglobin in our blood)
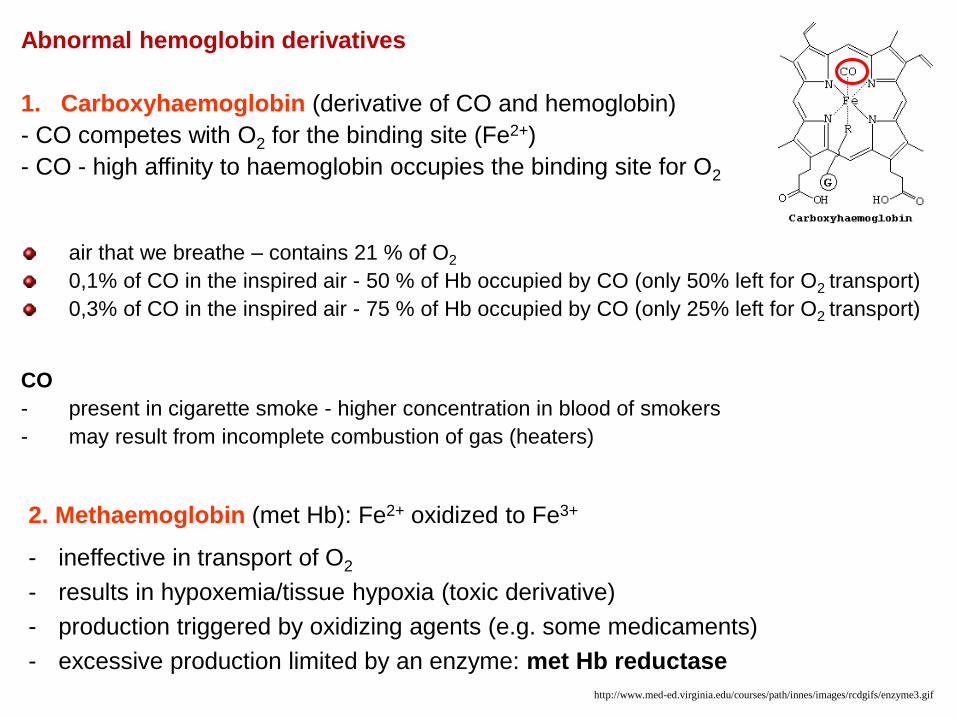
2. Methaemoglobin (met Hb): Fe2+ oxidized to Fe3+
- ineffective in transport of O2
- results in hypoxemia/tissue hypoxia (toxic derivative)
- production triggered by oxidizing agents (e.g. some medicaments)
- excessive production limited by an enzyme: met Hb reductase
Abnormal hemoglobin derivatives
1. Carboxyhaemoglobin (derivative of CO and hemoglobin)
- CO competes with O2 for the binding site (Fe2+)
- CO - high affinity to haemoglobin occupies the binding site for O2
air that we breathe – contains 21 % of O2
0,1% of CO in the inspired air - 50 % of Hb occupied by CO (only 50% left for O2 transport)
0,3% of CO in the inspired air - 75 % of Hb occupied by CO (only 25% left for O2 transport)
CO
- present in cigarette smoke - higher concentration in blood of smokers
- may result from incomplete combustion of gas (heaters)
http://www.med-ed.virginia.edu/courses/path/innes/images/rcdgifs/enzyme3.gif
Blood groups (blood types)
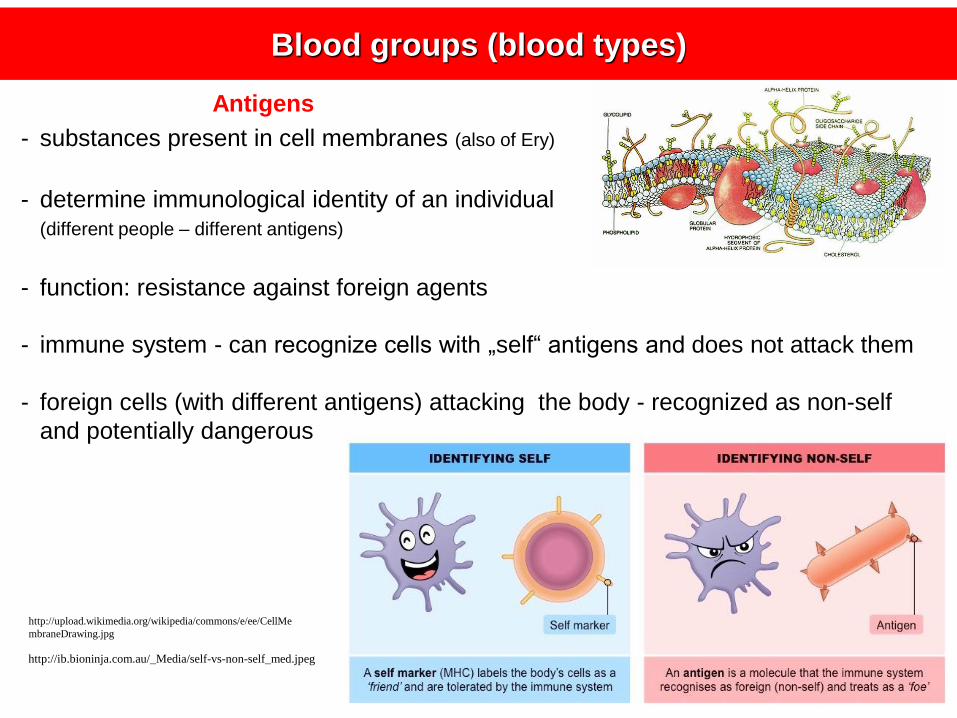
Antigens
- substances present in cell membranes (also of Ery)
- determine immunological identity of an individual(different people – different antigens)
- function: resistance against foreign agents
http://upload.wikimedia.org/wikipedia/commons/e/ee/CellMe
mbraneDrawing.jpg
- immune system - can recognize cells with „self“ antigens and does not attack them
- foreign cells (with different antigens) attacking the body - recognized as non-self
and potentially dangerous
http://ib.bioninja.com.au/_Media/self-vs-non-self_med.jpeg
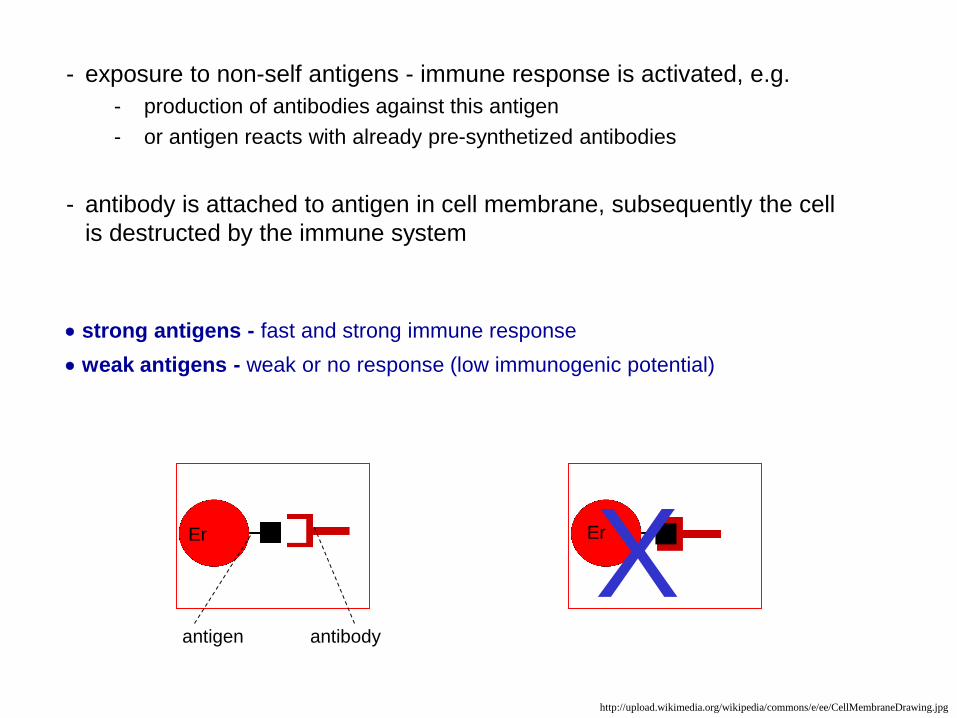
- exposure to non-self antigens - immune response is activated, e.g.
- production of antibodies against this antigen
- or antigen reacts with already pre-synthetized antibodies
- antibody is attached to antigen in cell membrane, subsequently the cell
is destructed by the immune system
strong antigens - fast and strong immune response
weak antigens - weak or no response (low immunogenic potential)
antigen antibody
XEr Er
http://upload.wikimedia.org/wikipedia/commons/e/ee/CellMembraneDrawing.jpg
Presence of antigens in the membrane of erythrocytes
(blood group substances) determines the blood group
Blood type must be considered in:
- transfusions
- transplantations
- gynaecology and obstetrics
Major clinical importance (out of all existing blood systems):
1. ABO system 2. Rh system
- antigens of these systems are strong antigens
(i.e. may cause a strong and rapid immune reaction)
- in case of mismatching transfusion – high risk of
- serious health consequences
- death
GENERAL RULE: IN A TRANSFUSION ALWAYS USE A MATCHING BLOOD
what is a „matching blood“?
http://2.bp.blogspot.com/_mIFBm1eVxx8/SojwvPgHAnI/AAAAAAAAAi0/K19gpgiaz8Y/s400/BloodTransfusion.jpg
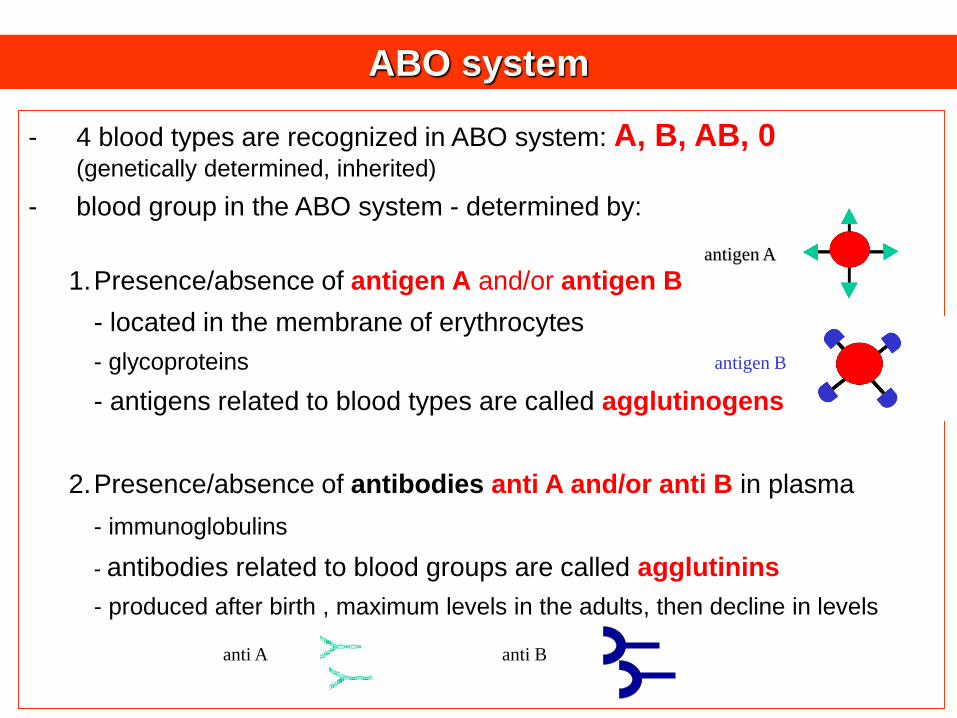
- 4 blood types are recognized in ABO system: A, B, AB, 0 (genetically determined, inherited)
- blood group in the ABO system - determined by:
1.Presence/absence of antigen A and/or antigen B
- located in the membrane of erythrocytes
- glycoproteins
- antigens related to blood types are called agglutinogens
2.Presence/absence of antibodies anti A and/or anti B in plasma
- immunoglobulins
- antibodies related to blood groups are called agglutinins
- produced after birth , maximum levels in the adults, then decline in levels
ABO system
antigen A
antigen B
anti A anti B
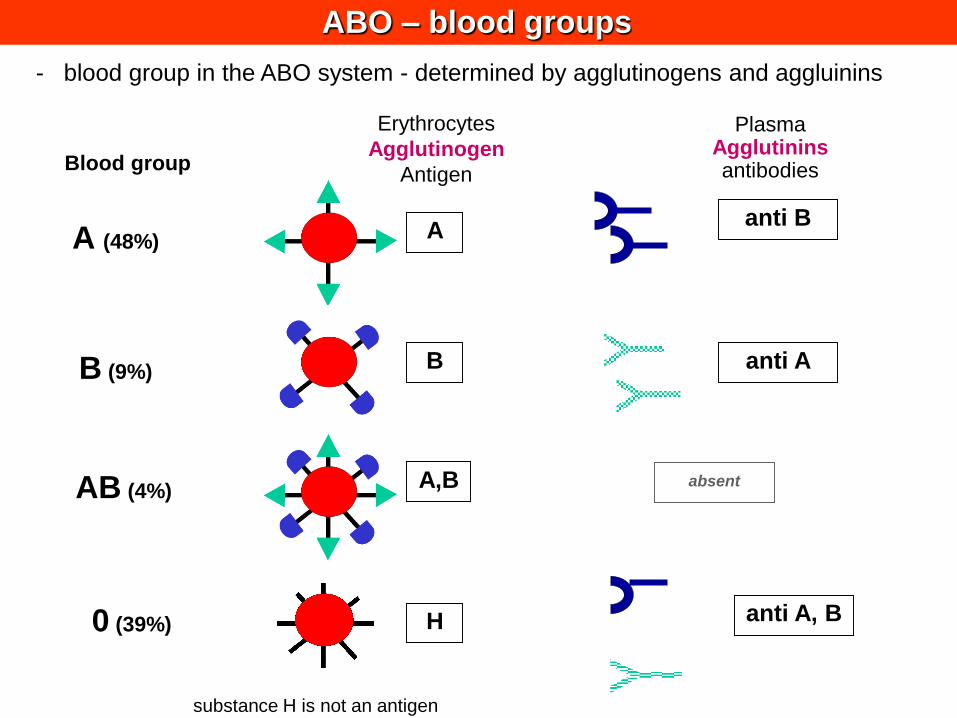
ABO – blood groups
Blood group
A (48%)
B (9%)
AB (4%)
0 (39%)
A
B
A,B
H
anti B
anti A
anti A, B
absent
substance H is not an antigen
- blood group in the ABO system - determined by agglutinogens and aggluinins
Erythrocytes
Agglutinogen
Antigen
PlasmaAgglutininsantibodies
+
+
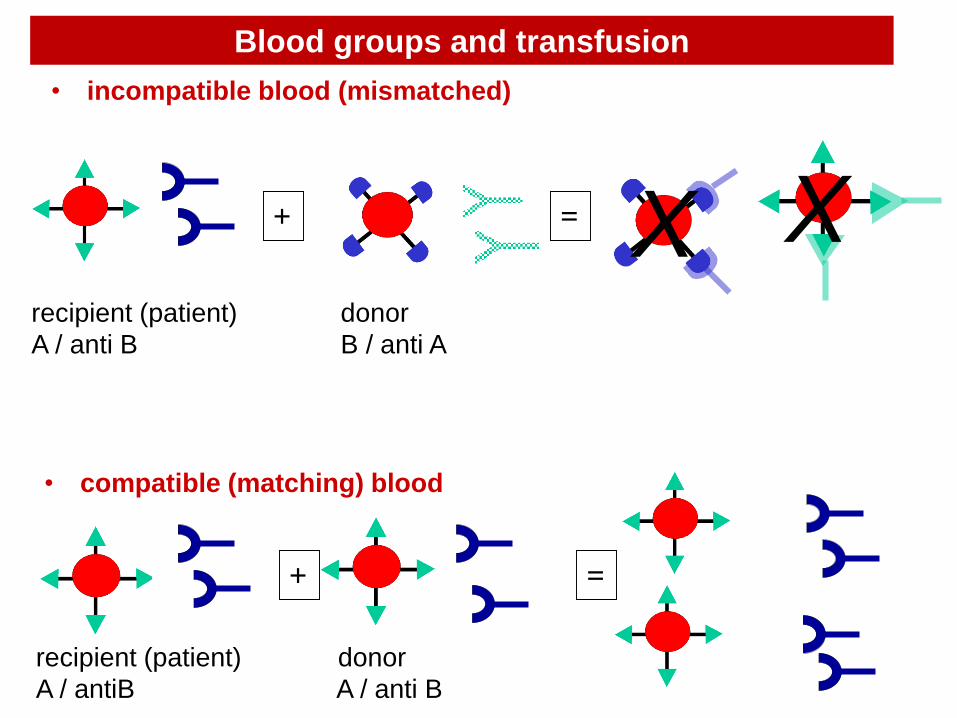
recipient (patient) donor
A / anti B B / anti A
recipient (patient) donor
A / antiB A / anti B
=
=
• incompatible blood (mismatched)
• compatible (matching) blood
Blood groups and transfusion
X X
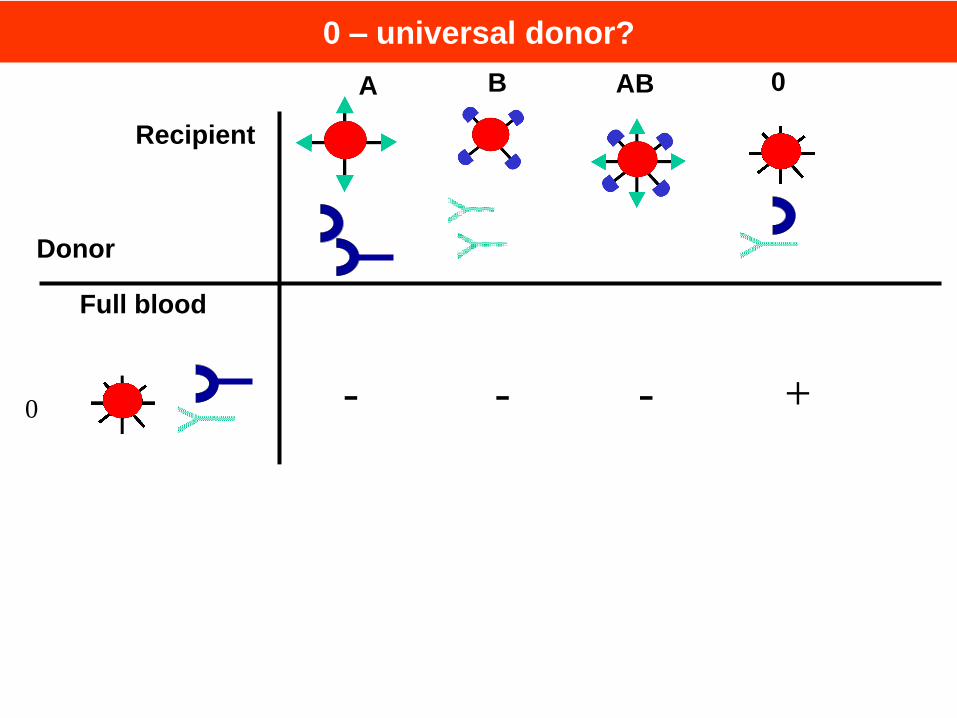
0 – universal donor?
0 +- - -
A B AB 0
+ +
Full blood
Erythrocytes
0 + +
Donor
Recipient
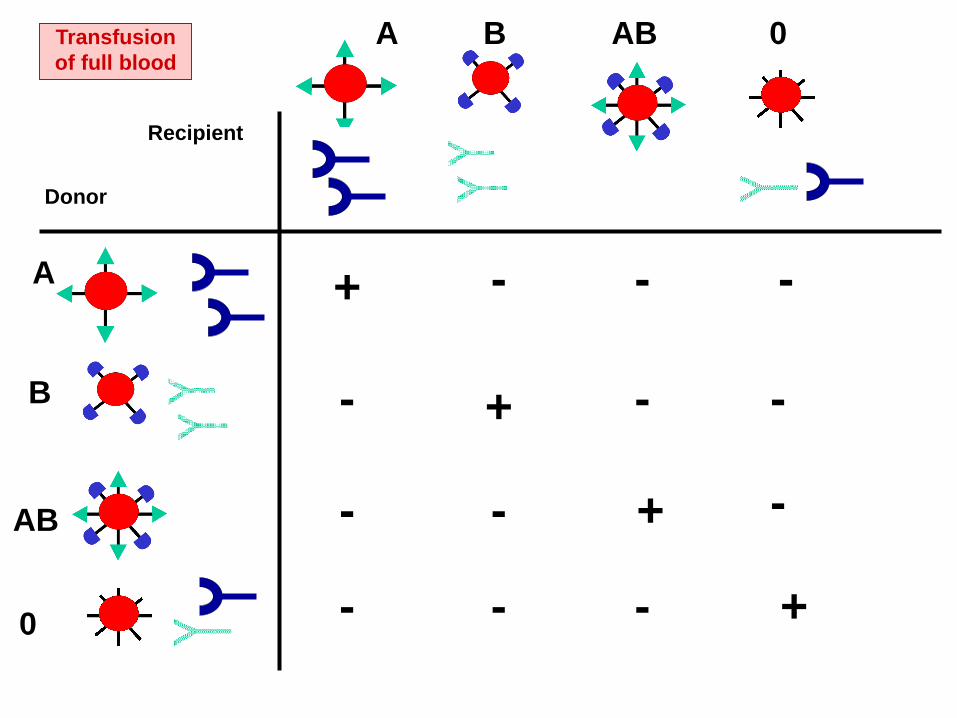
Transfusion
of full blood
A
B
AB
0
A B AB 0
+
+
+
+
-
-
-
-
- -
--
Donor
Recipient
--
-
-
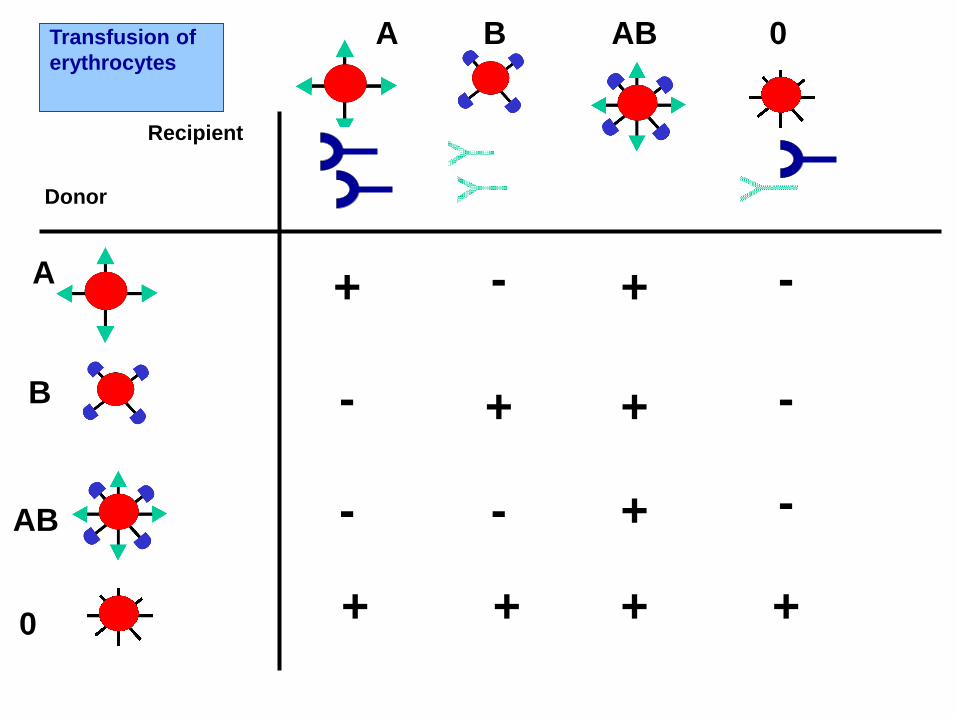
Transfusion of
erythrocytes
A
B
AB
0
A B AB 0
+
+
+
+
-
-
-
--
Donor
Recipient
-
-
+
+
+++
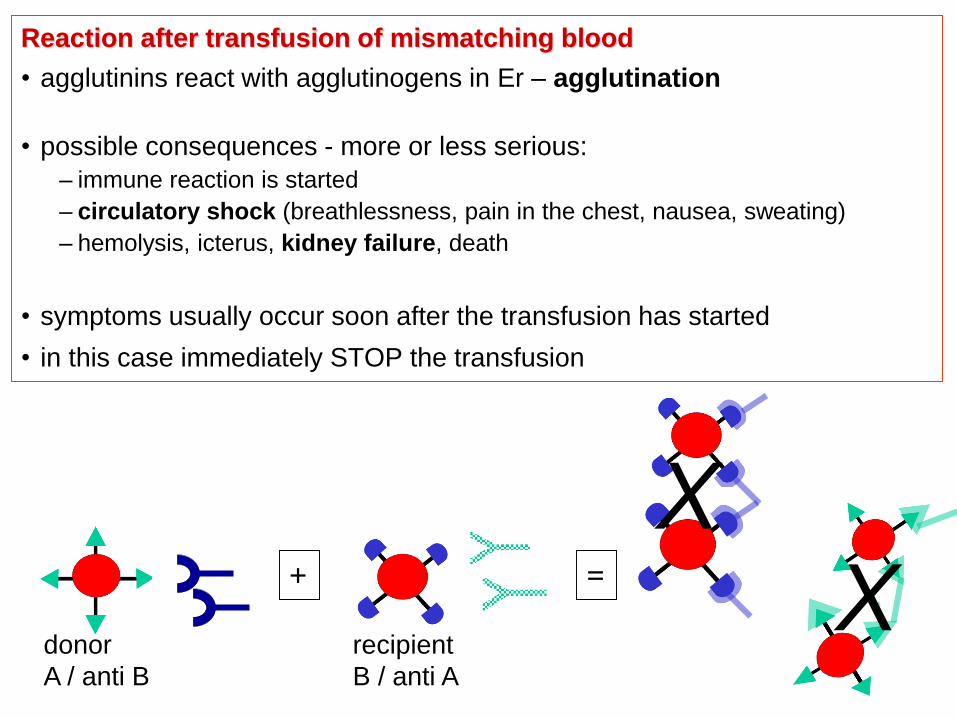
Reaction after transfusion of mismatching blood
• agglutinins react with agglutinogens in Er – agglutination
• possible consequences - more or less serious:
– immune reaction is started
– circulatory shock (breathlessness, pain in the chest, nausea, sweating)
– hemolysis, icterus, kidney failure, death
• symptoms usually occur soon after the transfusion has started
• in this case immediately STOP the transfusion
donor recipient
A / anti B B / anti A
=+
XX
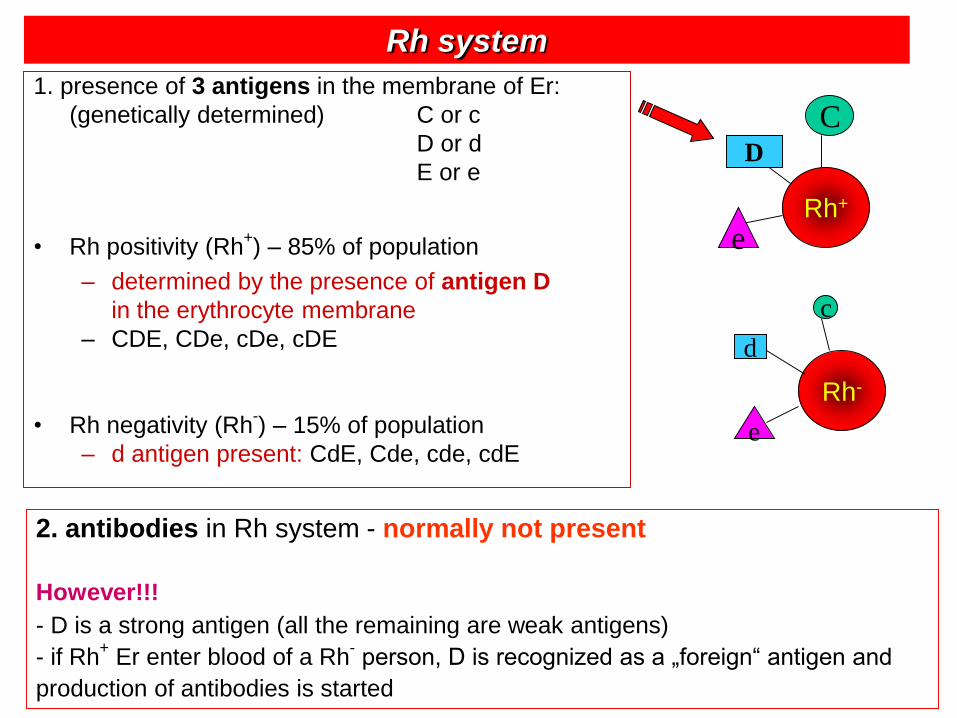
Rh system
1. presence of 3 antigens in the membrane of Er:
(genetically determined) C or c
D or d
E or e
• Rh positivity (Rh+) – 85% of population
– determined by the presence of antigen D
in the erythrocyte membrane
– CDE, CDe, cDe, cDE
• Rh negativity (Rh-) – 15% of population
– d antigen present: CdE, Cde, cde, cdE
Rh-
Rh+
C
c
D
d
e
e
2. antibodies in Rh system - normally not present
However!!!
- D is a strong antigen (all the remaining are weak antigens)
- if Rh+
Er enter blood of a Rh-person, D is recognized as a „foreign“ antigen and
production of antibodies is started
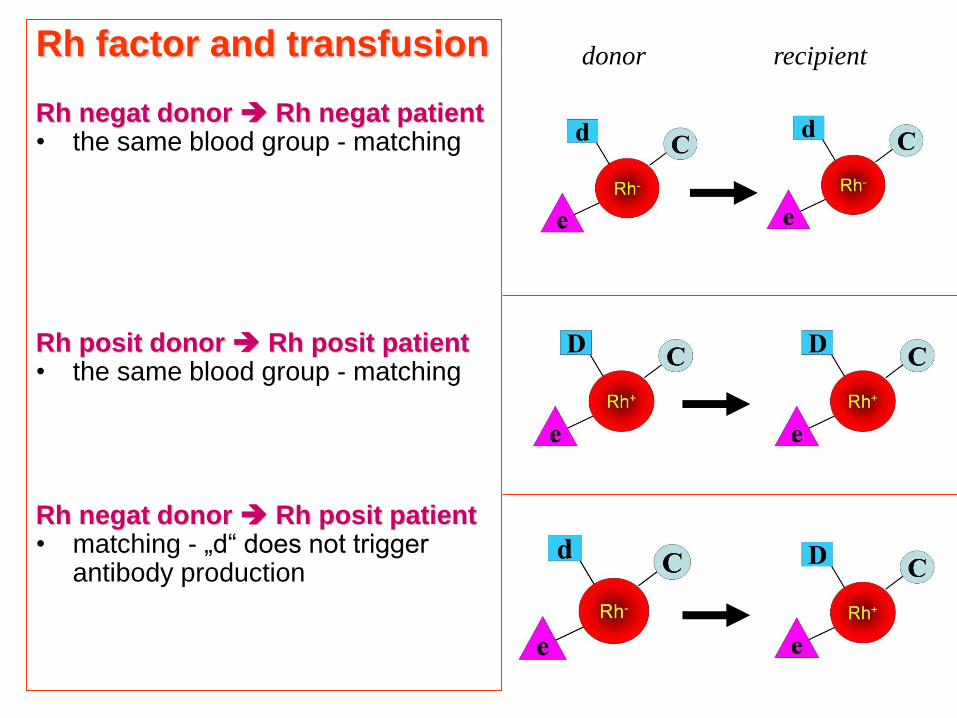
Rh factor and transfusion
Rh negat donor Rh negat patient• the same blood group - matching
Rh posit donor Rh posit patient• the same blood group - matching
Rh negat donor Rh posit patient• matching - „d“ does not trigger
antibody production
donor recipient
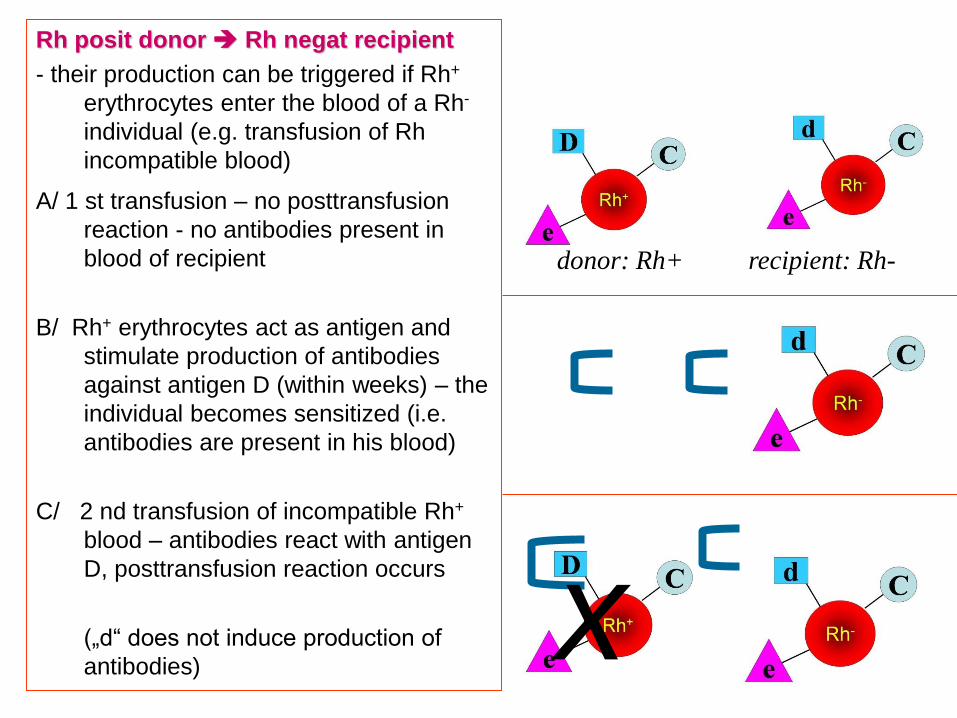
Rh posit donor Rh negat recipient
- their production can be triggered if Rh+
erythrocytes enter the blood of a Rh-
individual (e.g. transfusion of Rh
incompatible blood)
A/ 1 st transfusion – no posttransfusion
reaction - no antibodies present in
blood of recipient
B/ Rh+ erythrocytes act as antigen and
stimulate production of antibodies
against antigen D (within weeks) – the
individual becomes sensitized (i.e.
antibodies are present in his blood)
C/ 2 nd transfusion of incompatible Rh+
blood – antibodies react with antigen
D, posttransfusion reaction occurs
(„d“ does not induce production of
antibodies)x
donor: Rh+ recipient: Rh-
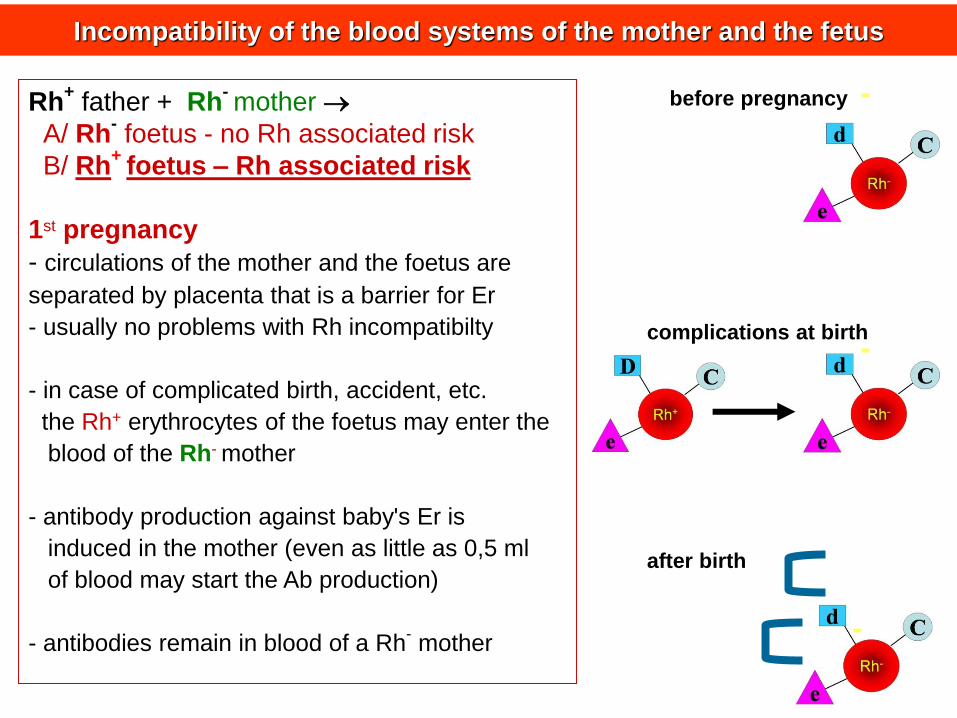
Rh+
father + Rh-mother
A/ Rh-foetus - no Rh associated risk
B/ Rh+
foetus – Rh associated risk
1st pregnancy
- circulations of the mother and the foetus are
separated by placenta that is a barrier for Er
- usually no problems with Rh incompatibilty
- in case of complicated birth, accident, etc.
the Rh+ erythrocytes of the foetus may enter the
blood of the Rh- mother
- antibody production against baby's Er is
induced in the mother (even as little as 0,5 ml
of blood may start the Ab production)
- antibodies remain in blood of a Rh-mother
Incompatibility of the blood systems of the mother and the fetus
before pregnancy
after birth
complications at birth
placenta
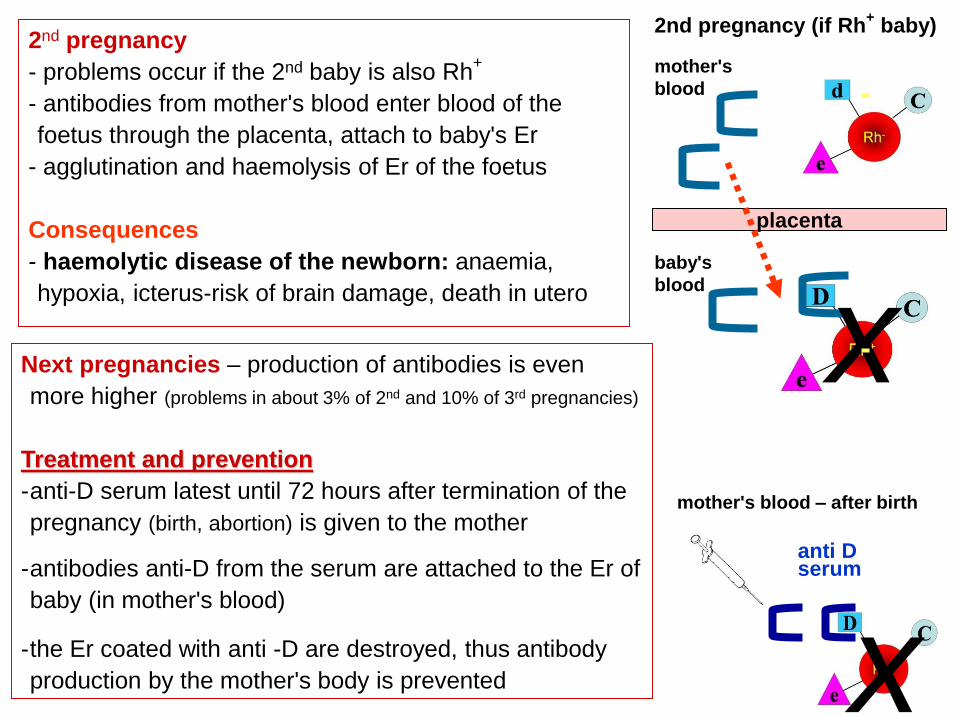
xNext pregnancies – production of antibodies is even
more higher (problems in about 3% of 2nd and 10% of 3rd pregnancies)
Treatment and prevention
-anti-D serum latest until 72 hours after termination of the
pregnancy (birth, abortion) is given to the mother
-antibodies anti-D from the serum are attached to the Er of
baby (in mother's blood)
-the Er coated with anti -D are destroyed, thus antibody
production by the mother's body is prevented
anti D serum
mother's
blood
baby's
blood
2nd pregnancy (if Rh+
baby)2nd pregnancy
- problems occur if the 2nd baby is also Rh+
- antibodies from mother's blood enter blood of the
foetus through the placenta, attach to baby's Er
- agglutination and haemolysis of Er of the foetus
Consequences
- haemolytic disease of the newborn: anaemia,
hypoxia, icterus-risk of brain damage, death in utero
mother's blood – after birth
x
Other blood systems
- about 30 blood systems exist
- clinically significant:
Kell (K, k) MNSs Kidd
Lewis (Lewisa, Lewisb) Diego Lutheran, etc.
• may cause mismatch of donor´s and recipient´s blood despite compatibility in
ABO and Rh system
• may cause mother/fetus incompatibility
• may cause transfusion reaction in individuals who often receive transfusion
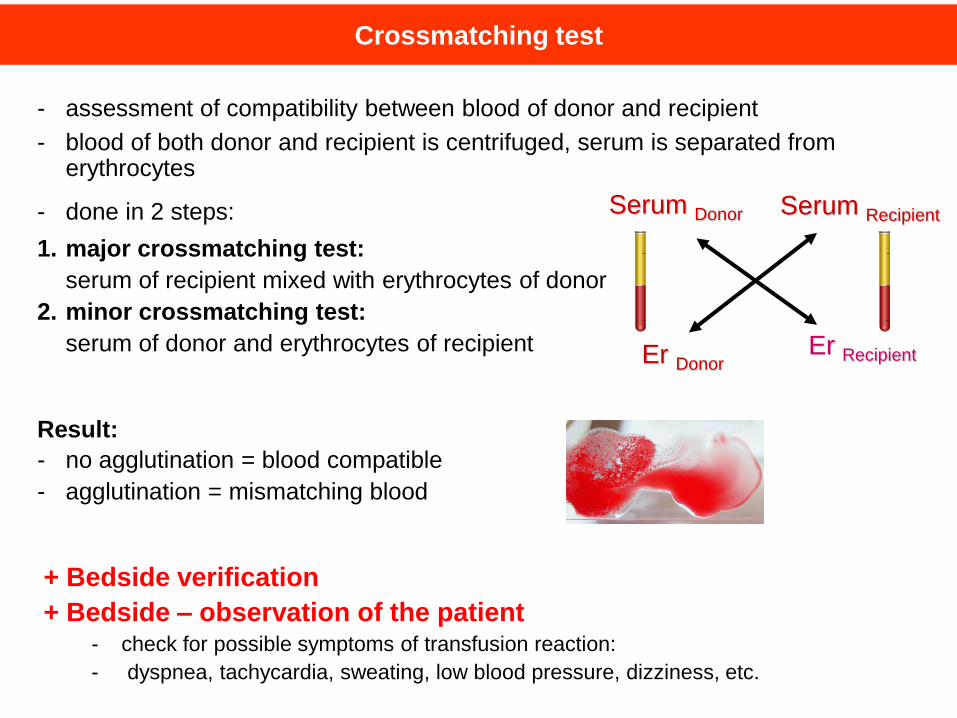
Crossmatching test
- assessment of compatibility between blood of donor and recipient
- blood of both donor and recipient is centrifuged, serum is separated from erythrocytes
- done in 2 steps:
1. major crossmatching test:
serum of recipient mixed with erythrocytes of donor
2. minor crossmatching test:
serum of donor and erythrocytes of recipient
Result:
- no agglutination = blood compatible
- agglutination = mismatching blood
Er DonorEr Recipient
Serum RecipientSerum Donor
+ Bedside verification
+ Bedside – observation of the patient- check for possible symptoms of transfusion reaction:
- dyspnea, tachycardia, sweating, low blood pressure, dizziness, etc.
Blood Physiology
Lecture 2
Objectives
1. Platelets and haemostasis
2. White blood cells and their immune functions
3. Hemopoiesis
4. Blood plasma and osmotic pressure
Dental procedures and bleeding
• a small segment of the population - an increased risk of bleeding
(e.g. inherited bleeding disorders, secondary bleeding due to medication)
• relatively minor invasive procedures can trigger a prolonged bleeding
– distressing for the patient
– hinders the completion of the procedure (e.g., suture insertion)
– can compromise wound healing.
• Dental treatment in bleeding disorders
– a challenge for dentists
• Special management of the patient needed
dental procedures - amongst the most common
invasive procedures
often associated with bleeding - in most cases self-
limiting and non-problematic
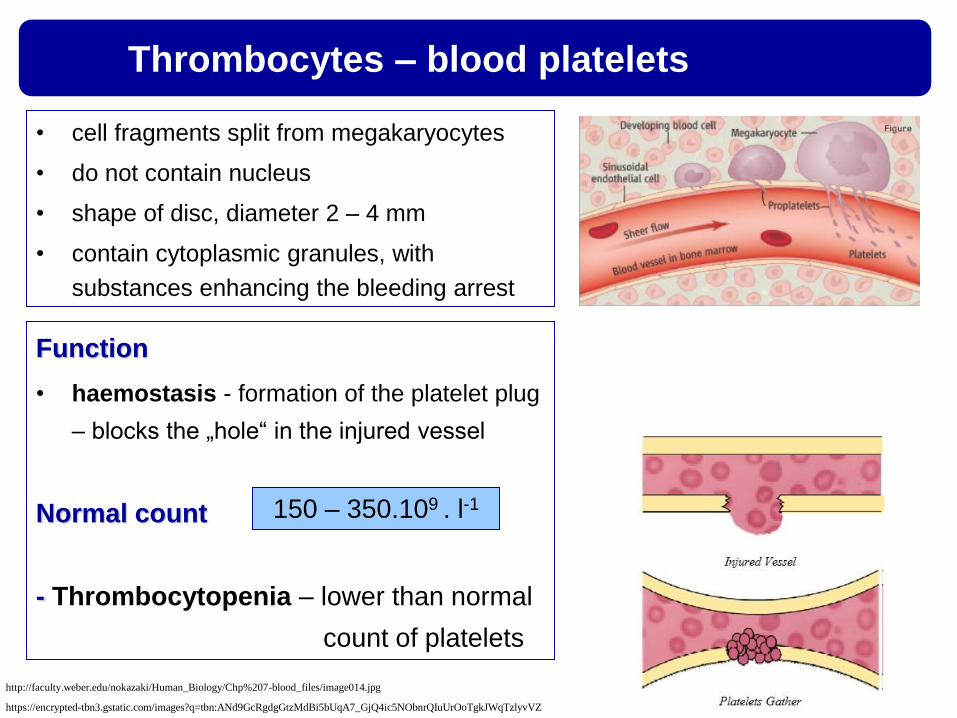
Thrombocytes – blood platelets
• cell fragments split from megakaryocytes
• do not contain nucleus
• shape of disc, diameter 2 – 4 mm
• contain cytoplasmic granules, with
substances enhancing the bleeding arrest
Function
• haemostasis - formation of the platelet plug
– blocks the „hole“ in the injured vessel
Normal count
- Thrombocytopenia – lower than normal
count of platelets
150 – 350.109 . l-1
https://encrypted-tbn3.gstatic.com/images?q=tbn:ANd9GcRgdgGtzMdBi5bUqA7_GjQ4ic5NObnrQIuUrOoTgkJWqTzlyvVZ
http://faculty.weber.edu/nokazaki/Human_Biology/Chp%207-blood_files/image014.jpg
Haemostasis – bleeding arrest
- a complex process that makes a bleeding to stop
maintenance of normal blood volume – vital
massive bleeding may lead to cardiovascular collapse and death
- haemostasis includes 3 simultaneous interrelated processes
1/ reaction of the injured vessel
2/ activity of the platelets (platelet plug formation)
3/ blood clotting (haemocoagulation)
https://encrypted-tbn0.gstatic.com/images?q=tbn:ANd9GcSZ-
gNE_9HuievzBVNFIM4o0N_rFuR0MGyPK_eezc-Klu_rU8_goQ
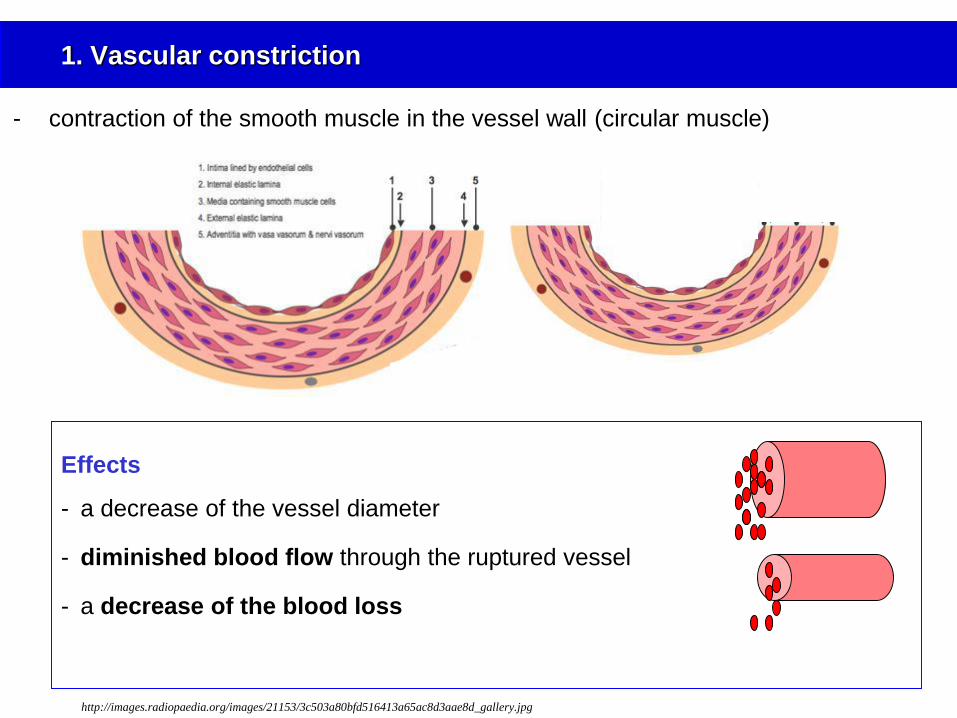
1. Vascular constriction
Effects
- a decrease of the vessel diameter
- diminished blood flow through the ruptured vessel
- a decrease of the blood loss
- contraction of the smooth muscle in the vessel wall (circular muscle)
http://images.radiopaedia.org/images/21153/3c503a80bfd516413a65ac8d3aae8d_gallery.jpg
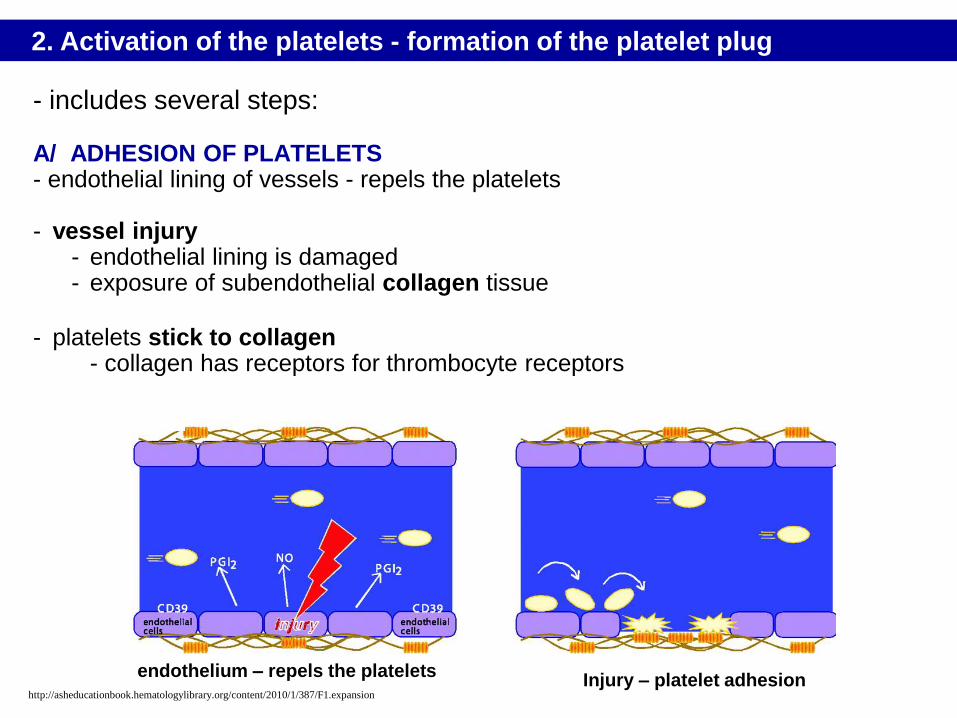
- includes several steps:
A/ ADHESION OF PLATELETS - endothelial lining of vessels - repels the platelets
- vessel injury- endothelial lining is damaged - exposure of subendothelial collagen tissue
- platelets stick to collagen- collagen has receptors for thrombocyte receptors
2. Activation of the platelets - formation of the platelet plug
Injury – platelet adhesionendothelium – repels the platelets
http://asheducationbook.hematologylibrary.org/content/2010/1/387/F1.expansion
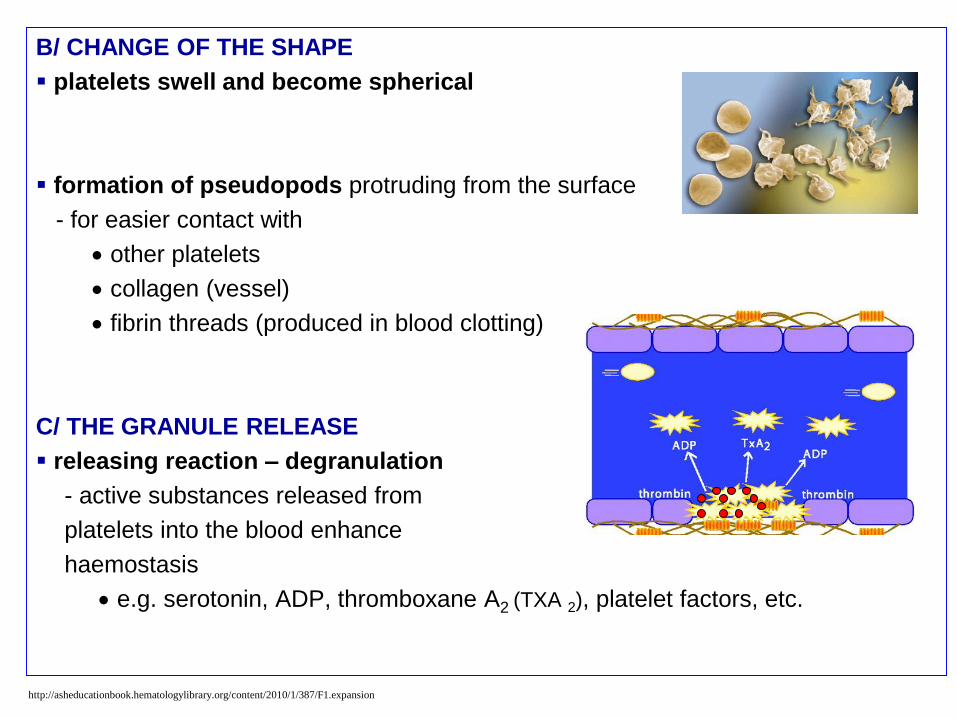
B/ CHANGE OF THE SHAPE
platelets swell and become spherical
formation of pseudopods protruding from the surface
- for easier contact with
other platelets
collagen (vessel)
fibrin threads (produced in blood clotting)
C/ THE GRANULE RELEASE
releasing reaction – degranulation
- active substances released from
platelets into the blood enhance
haemostasis
e.g. serotonin, ADP, thromboxane A2 (TXA 2), platelet factors, etc.
http://asheducationbook.hematologylibrary.org/content/2010/1/387/F1.expansion
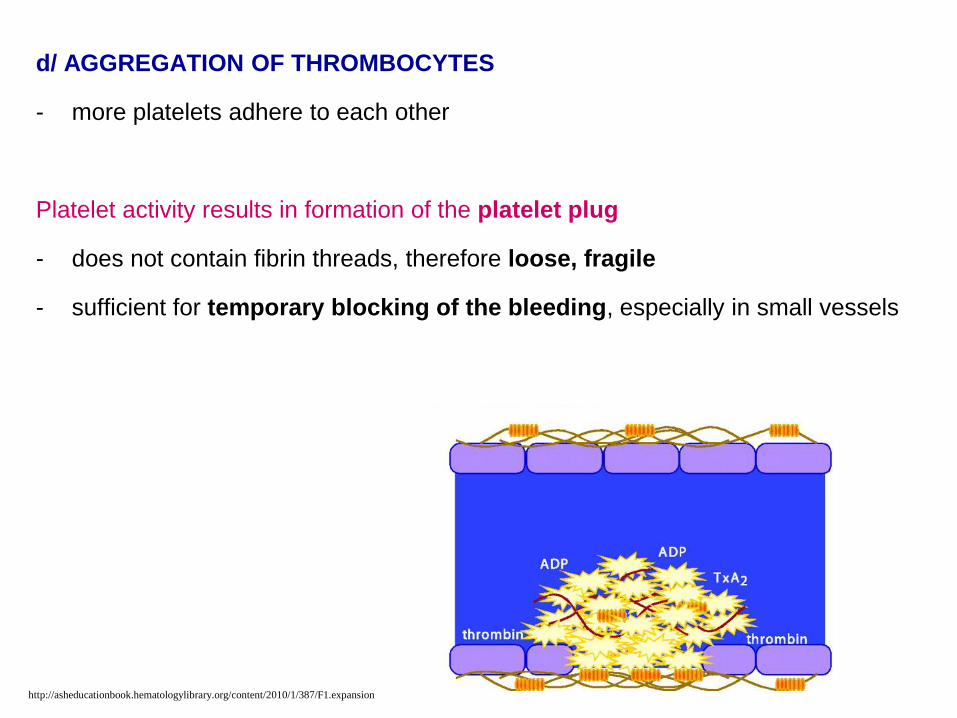
d/ AGGREGATION OF THROMBOCYTES
- more platelets adhere to each other
Platelet activity results in formation of the platelet plug
- does not contain fibrin threads, therefore loose, fragile
- sufficient for temporary blocking of the bleeding, especially in small vessels
http://asheducationbook.hematologylibrary.org/content/2010/1/387/F1.expansion
- series of enzyme reactions following in definite and rapid sequence
Result of haemocoagulation:
formation of fibrin threads - strengthen and stabilize the platelet plug
network of fibrin threads + platelet plug (+ trapped cells) = blood clot
- blood clot - seals the broken vessel until the tissue is repaired
- blood contains more than 50 substances related to blood clotting
- major role - plasma clotting factors (12 substances)
3. Blood coagulation (haemocoagulation, blood clotting)
https://encrypted-tbn2.gstatic.com/images?q=tbn:ANd9GcSYzcTvcBDveHieyeGqbHSBuVEQa7DocinF5r3gFj32IPSCJIJxKQ
http://www.alphalabs.co.uk/cms/site/images/Page-Header_Coag.jpg
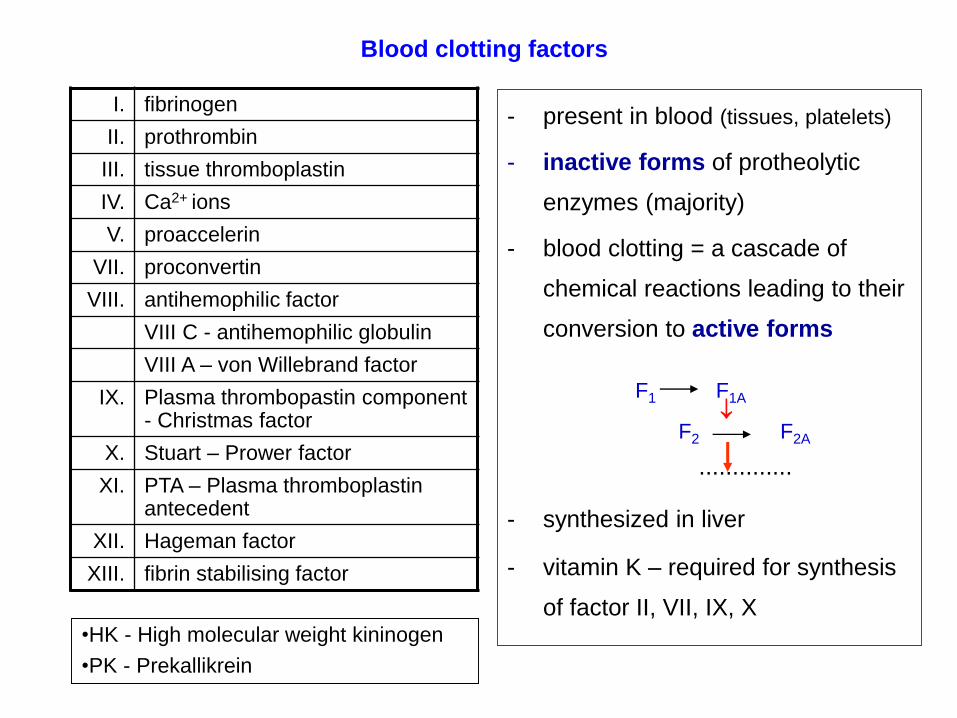
Blood clotting factors
I. fibrinogen
II. prothrombin
III. tissue thromboplastin
IV. Ca2+ ions
V. proaccelerin
VII. proconvertin
VIII. antihemophilic factor
VIII C - antihemophilic globulin
VIII A – von Willebrand factor
IX. Plasma thrombopastin component - Christmas factor
X. Stuart – Prower factor
XI. PTA – Plasma thromboplastin antecedent
XII. Hageman factor
XIII. fibrin stabilising factor
- present in blood (tissues, platelets)
- inactive forms of protheolytic
enzymes (majority)
- blood clotting = a cascade of
chemical reactions leading to their
conversion to active forms
..............
- synthesized in liver
- vitamin K – required for synthesis
of factor II, VII, IX, X
F1 F1A
F2 F2A
•HK - High molecular weight kininogen
•PK - Prekallikrein
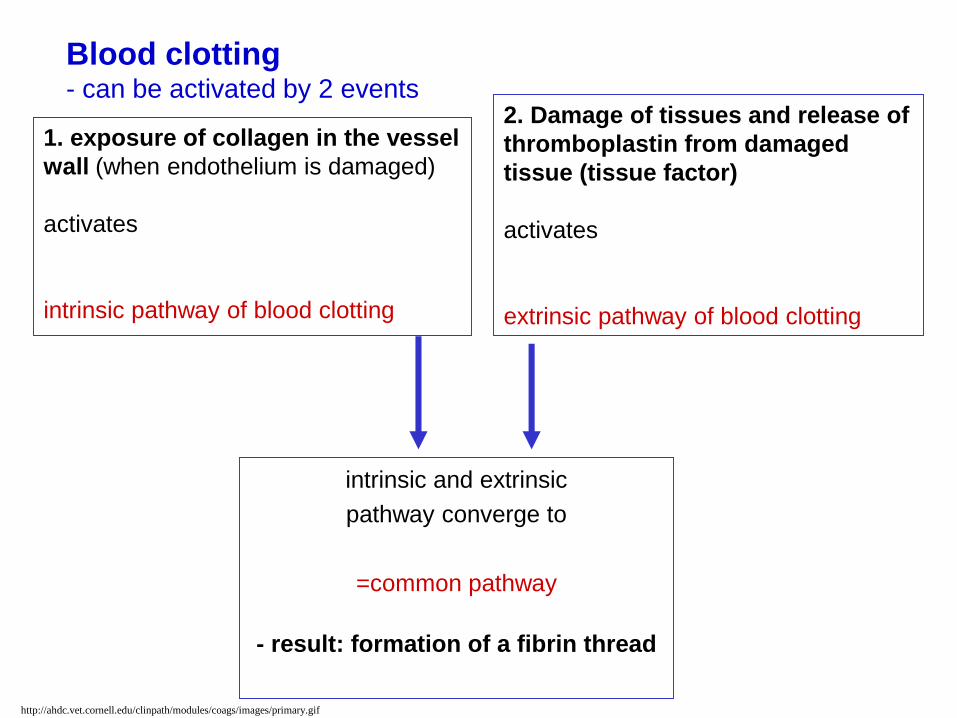
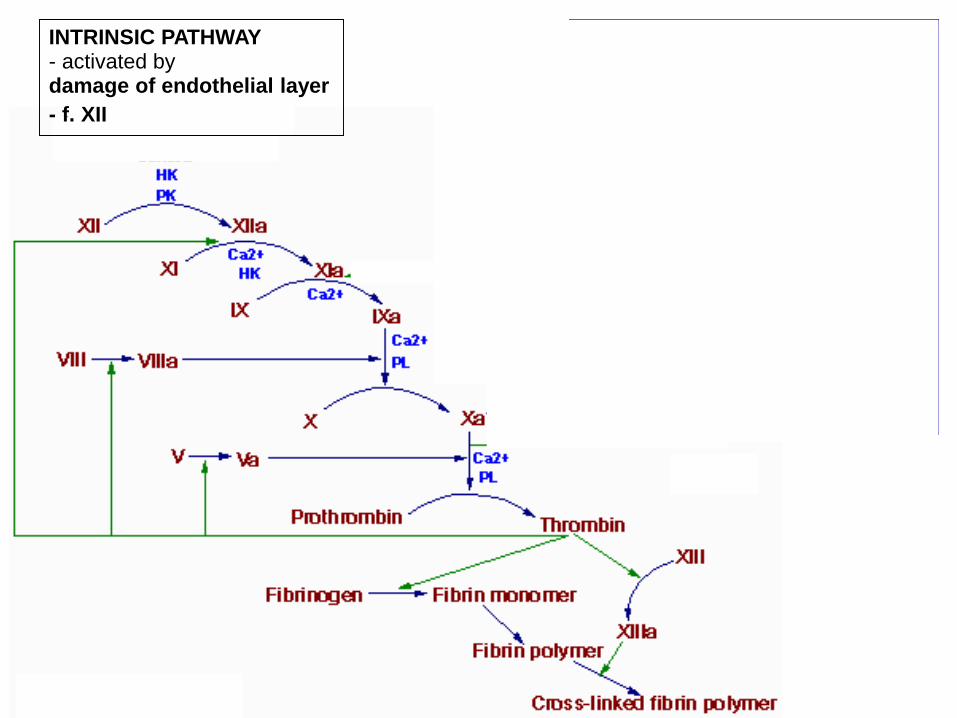
1. exposure of collagen in the vessel
wall (when endothelium is damaged)
activates
intrinsic pathway of blood clotting
2. Damage of tissues and release of
thromboplastin from damaged
tissue (tissue factor)
activates
extrinsic pathway of blood clotting
Blood clotting - can be activated by 2 events
intrinsic and extrinsic
pathway converge to
=common pathway
- result: formation of a fibrin thread
http://ahdc.vet.cornell.edu/clinpath/modules/coags/images/primary.gif
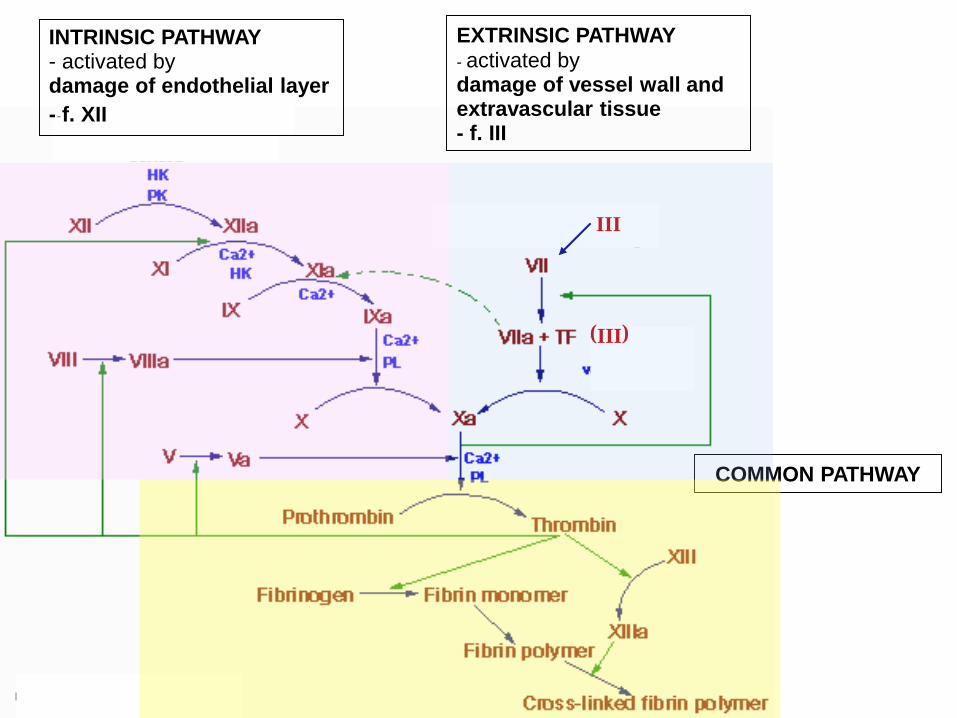
INTRINSIC PATHWAY- activated bydamage of endothelial layer
- f. XII
COMMON PATHWAY
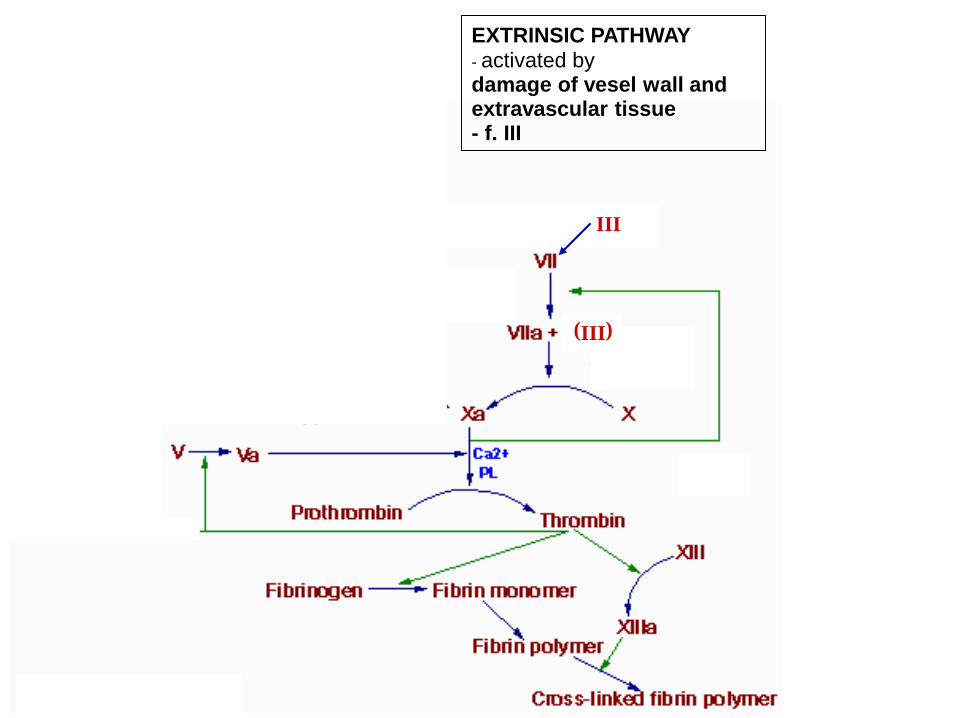
EXTRINSIC PATHWAY
- activated bydamage of vessel wall and extravascular tissue- f. III
III
(III)
INTRINSIC PATHWAY- activated bydamage of endothelial layer
- f. XII
EXTRINSIC PATHWAY
- activated bydamage of vesel wall and extravascular tissue- f. III
III
(III)
INTRINSIC PATHWAY- activated bydamage of endothelial layer
- f. XII
EXTRINSIC PATHWAY
- activated bydamage of vesel wall and extravascular tissue- f. III
III
(III)
1. fibrin monomer
2. fibrin polymer
3. cross-linked fibrin polymer
4. stabilization of the cross
linked fibrin polymer
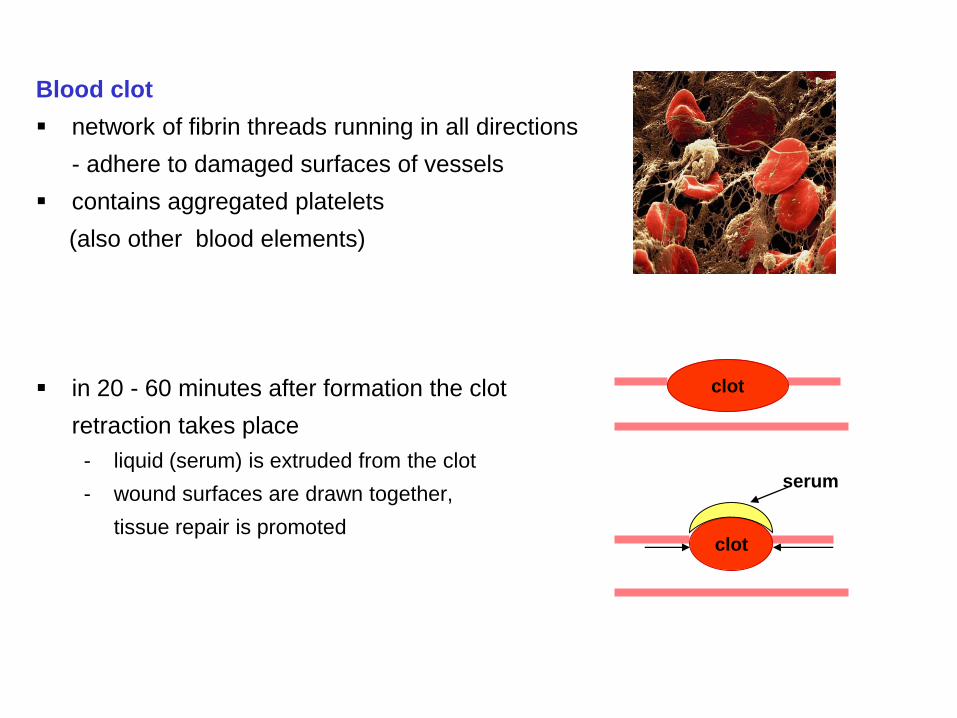
Blood clot
network of fibrin threads running in all directions
- adhere to damaged surfaces of vessels
contains aggregated platelets
(also other blood elements)
in 20 - 60 minutes after formation the clot
retraction takes place
- liquid (serum) is extruded from the clot
- wound surfaces are drawn together,
tissue repair is promoted
clot
clot
serum
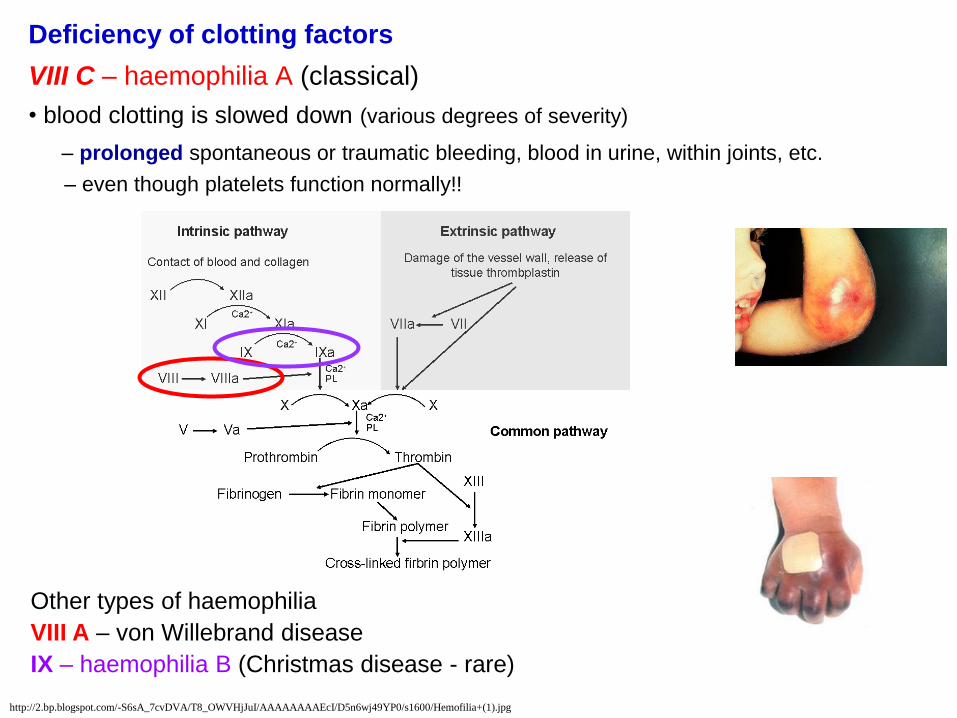
Deficiency of clotting factors
VIII C – haemophilia A (classical)
• blood clotting is slowed down (various degrees of severity)
– prolonged spontaneous or traumatic bleeding, blood in urine, within joints, etc.
– even though platelets function normally!!
http://2.bp.blogspot.com/-S6sA_7cvDVA/T8_OWVHjJuI/AAAAAAAAEcI/D5n6wj49YP0/s1600/Hemofilia+(1).jpg
Other types of haemophilia
VIII A – von Willebrand disease
IX – haemophilia B (Christmas disease - rare)
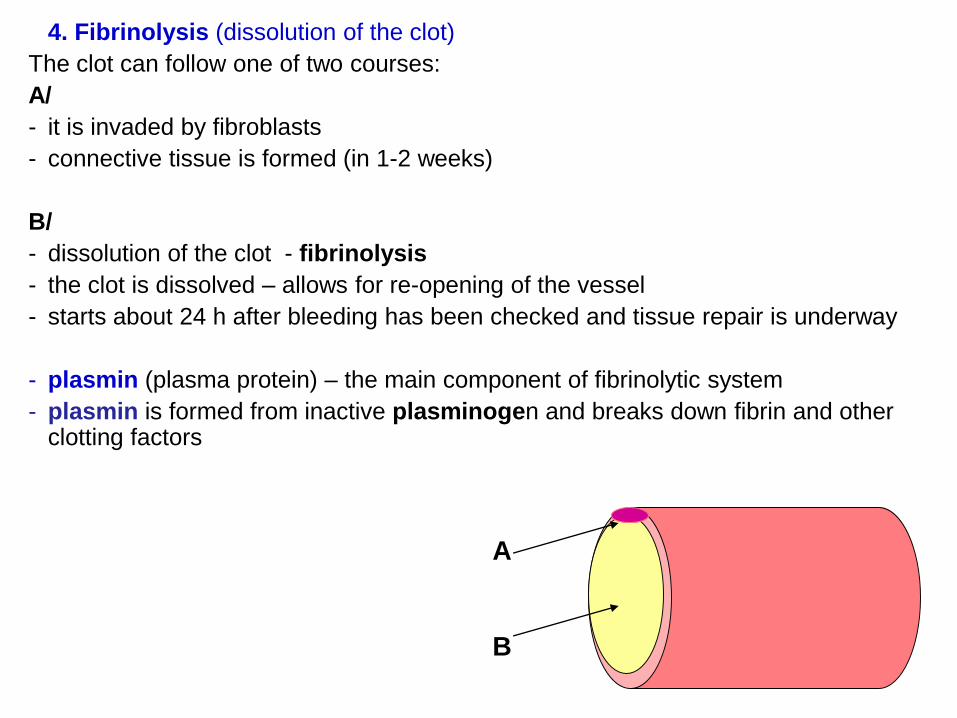
4. Fibrinolysis (dissolution of the clot)
The clot can follow one of two courses:
A/
- it is invaded by fibroblasts
- connective tissue is formed (in 1-2 weeks)
B/
- dissolution of the clot - fibrinolysis
- the clot is dissolved – allows for re-opening of the vessel
- starts about 24 h after bleeding has been checked and tissue repair is underway
- plasmin (plasma protein) – the main component of fibrinolytic system
- plasmin is formed from inactive plasminogen and breaks down fibrin and otherclotting factors
A
B
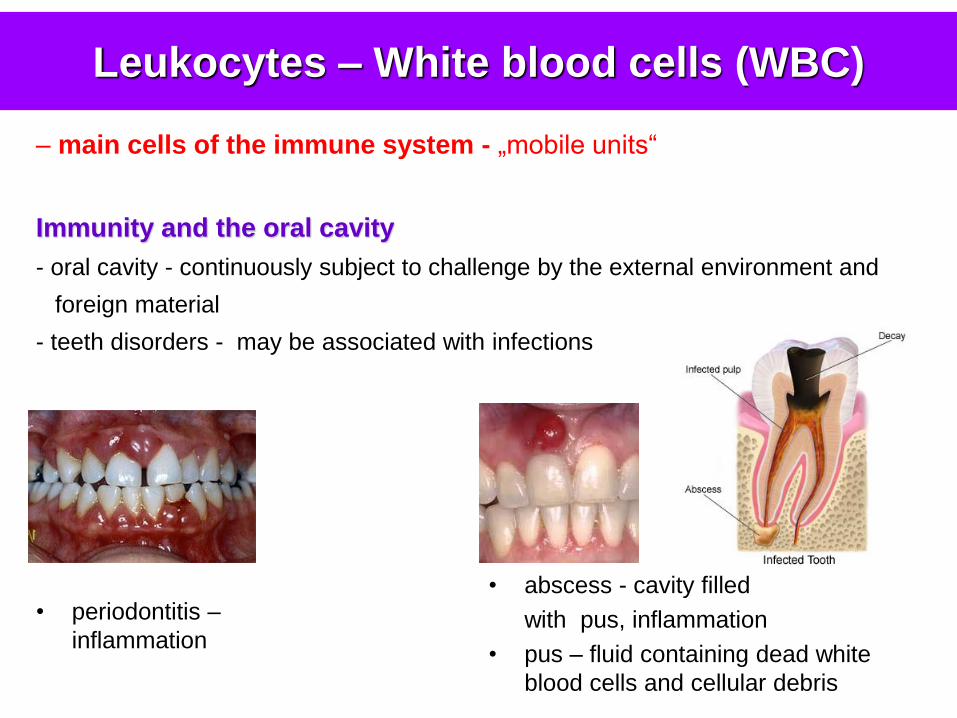
• abscess - cavity filled
with pus, inflammation
• pus – fluid containing dead white
blood cells and cellular debris
• periodontitis –
inflammation
Leukocytes – White blood cells (WBC)
– main cells of the immune system - „mobile units“
Immunity and the oral cavity
- oral cavity - continuously subject to challenge by the external environment and
foreign material
- teeth disorders - may be associated with infections
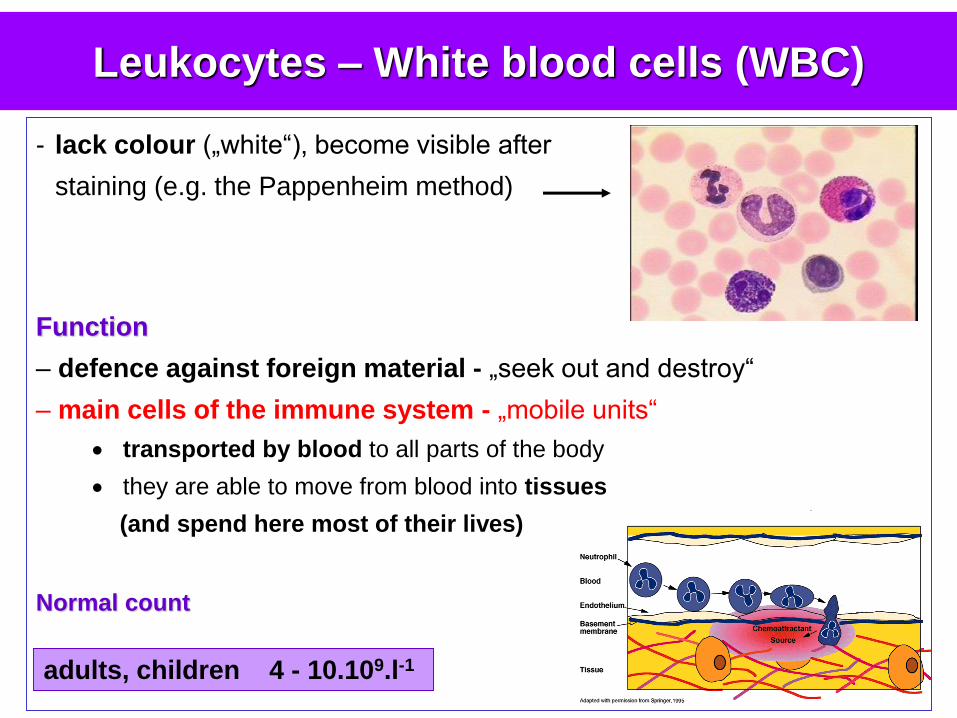
- lack colour („white“), become visible after
staining (e.g. the Pappenheim method)
Function
– defence against foreign material - „seek out and destroy“
– main cells of the immune system - „mobile units“
transported by blood to all parts of the body
they are able to move from blood into tissues
(and spend here most of their lives)
Normal count
Leukocytes – White blood cells (WBC)
adults, children 4 - 10.109.l-1
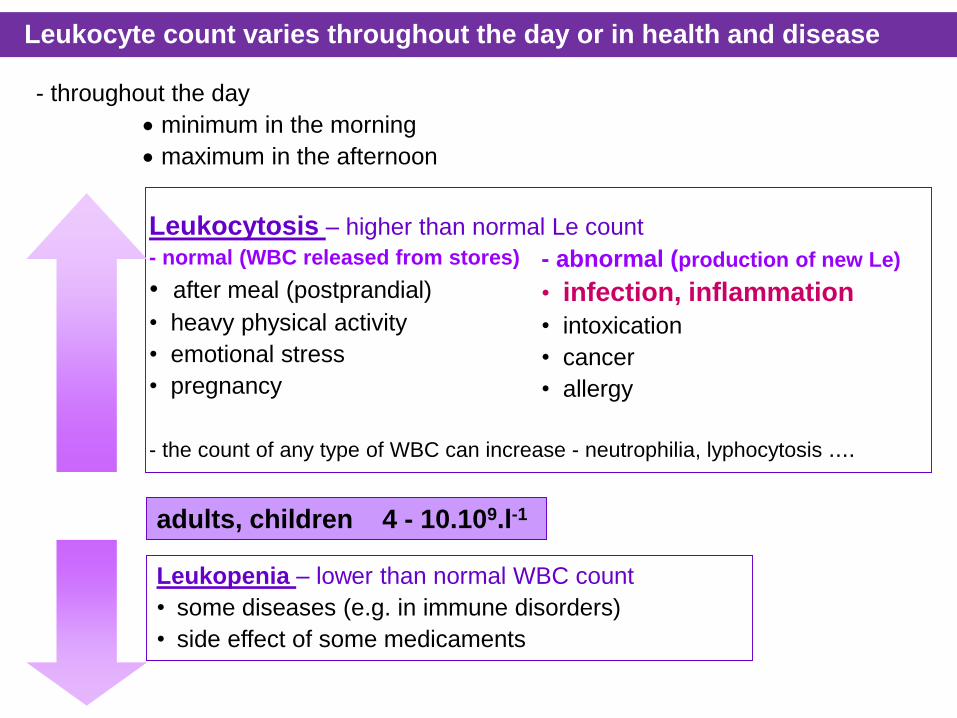
- abnormal (production of new Le)
• infection, inflammation
• intoxication
• cancer
• allergy
Leukocytosis – higher than normal Le count
- normal (WBC released from stores)
• after meal (postprandial)
• heavy physical activity
• emotional stress
• pregnancy
- the count of any type of WBC can increase - neutrophilia, lyphocytosis ....
Leukopenia – lower than normal WBC count
• some diseases (e.g. in immune disorders)
• side effect of some medicaments
adults, children 4 - 10.109.l-1
- throughout the day
minimum in the morning
maximum in the afternoon
Leukocyte count varies throughout the day or in health and disease
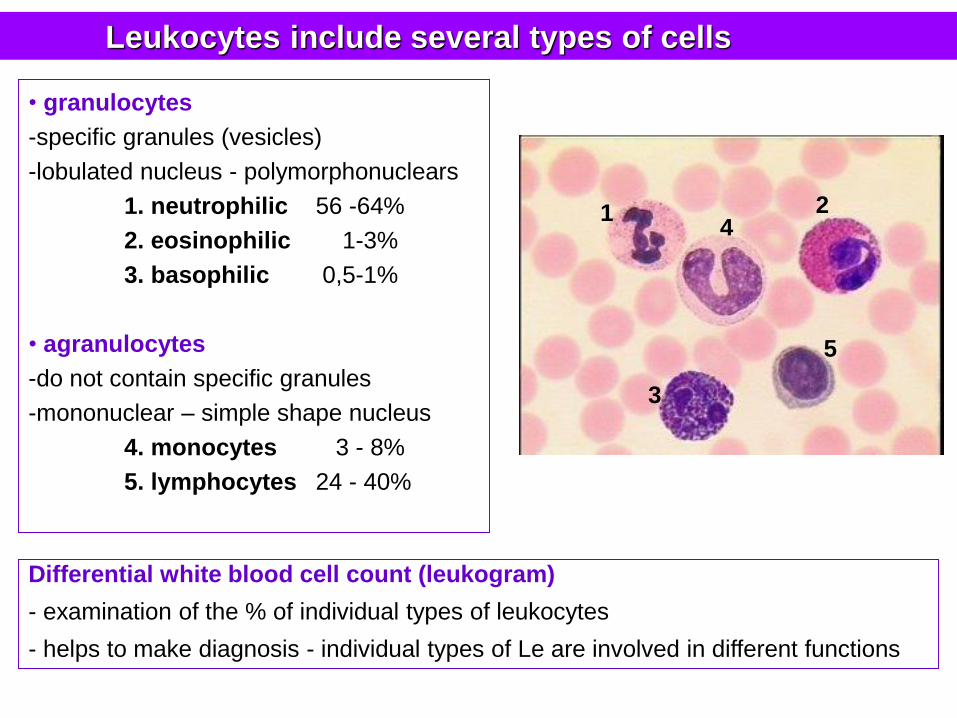
Leukocytes include several types of cells
• granulocytes
-specific granules (vesicles)
-lobulated nucleus - polymorphonuclears
1. neutrophilic 56 -64%
2. eosinophilic 1-3%
3. basophilic 0,5-1%
• agranulocytes
-do not contain specific granules
-mononuclear – simple shape nucleus
4. monocytes 3 - 8%
5. lymphocytes 24 - 40%
Differential white blood cell count (leukogram)
- examination of the % of individual types of leukocytes
- helps to make diagnosis - individual types of Le are involved in different functions
1 2
3
4
5
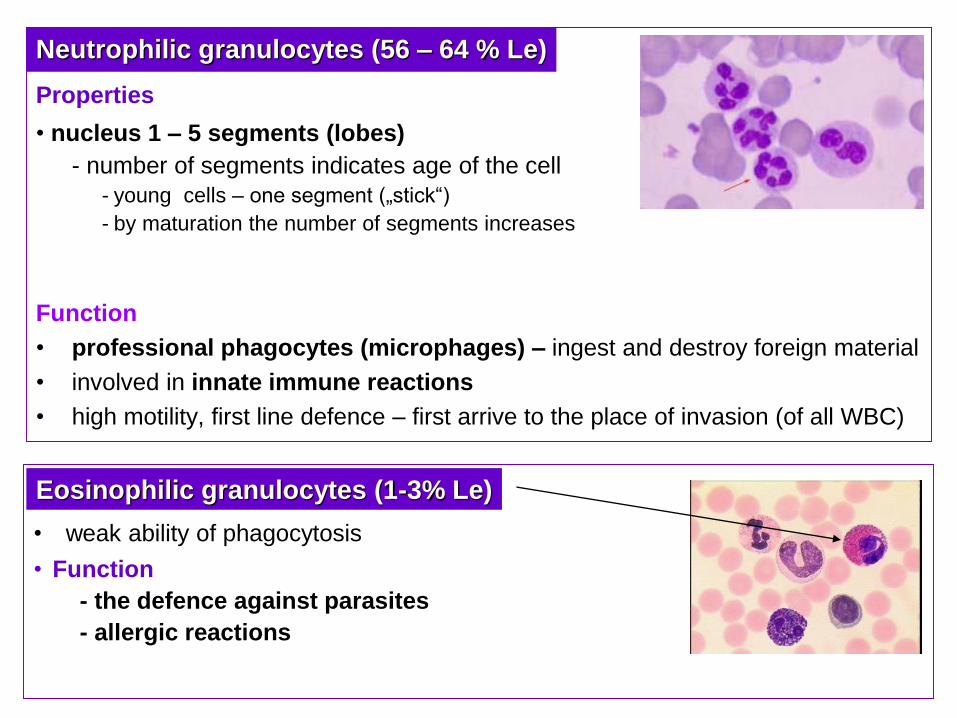
Properties
• nucleus 1 – 5 segments (lobes)
- number of segments indicates age of the cell
- young cells – one segment („stick“)
- by maturation the number of segments increases
Function
• professional phagocytes (microphages) – ingest and destroy foreign material
• involved in innate immune reactions
• high motility, first line defence – first arrive to the place of invasion (of all WBC)
• weak ability of phagocytosis
• Function
- the defence against parasites
- allergic reactions
Neutrophilic granulocytes (56 – 64 % Le)
Eosinophilic granulocytes (1-3% Le)
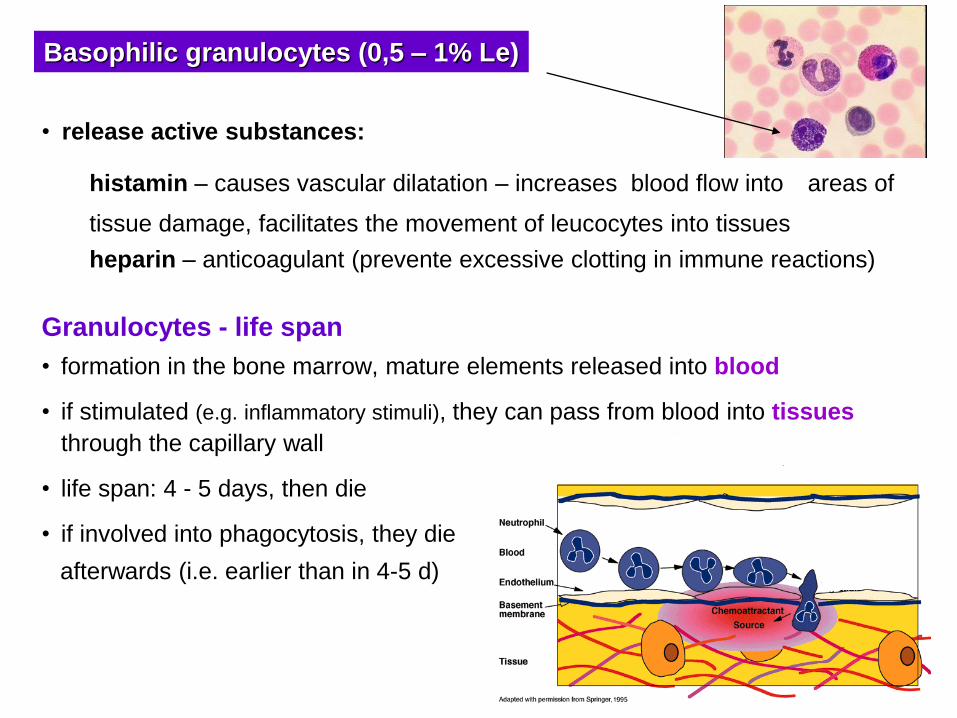
Granulocytes - life span
• formation in the bone marrow, mature elements released into blood
• if stimulated (e.g. inflammatory stimuli), they can pass from blood into tissues
through the capillary wall
• life span: 4 - 5 days, then die
• if involved into phagocytosis, they die
afterwards (i.e. earlier than in 4-5 d)
• release active substances:
histamin – causes vascular dilatation – increases blood flow into areas of
tissue damage, facilitates the movement of leucocytes into tissues
heparin – anticoagulant (prevente excessive clotting in immune reactions)
Basophilic granulocytes (0,5 – 1% Le)
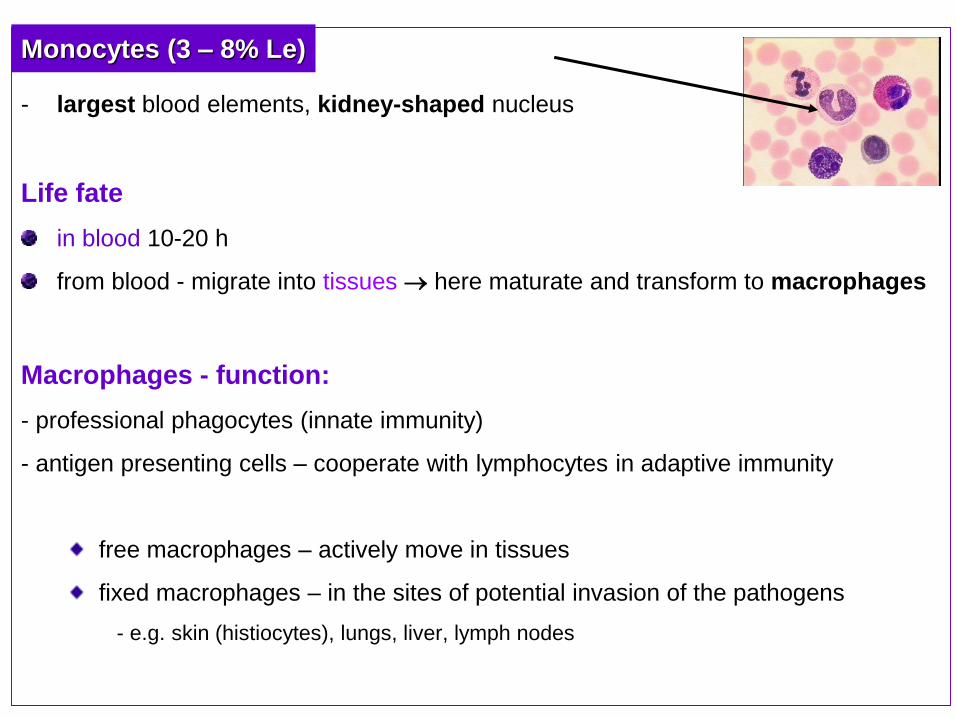
- largest blood elements, kidney-shaped nucleus
Life fate
in blood 10-20 h
from blood - migrate into tissues here maturate and transform to macrophages
Macrophages - function:
- professional phagocytes (innate immunity)
- antigen presenting cells – cooperate with lymphocytes in adaptive immunity
free macrophages – actively move in tissues
fixed macrophages – in the sites of potential invasion of the pathogens
- e.g. skin (histiocytes), lungs, liver, lymph nodes
Monocytes (3 – 8% Le)
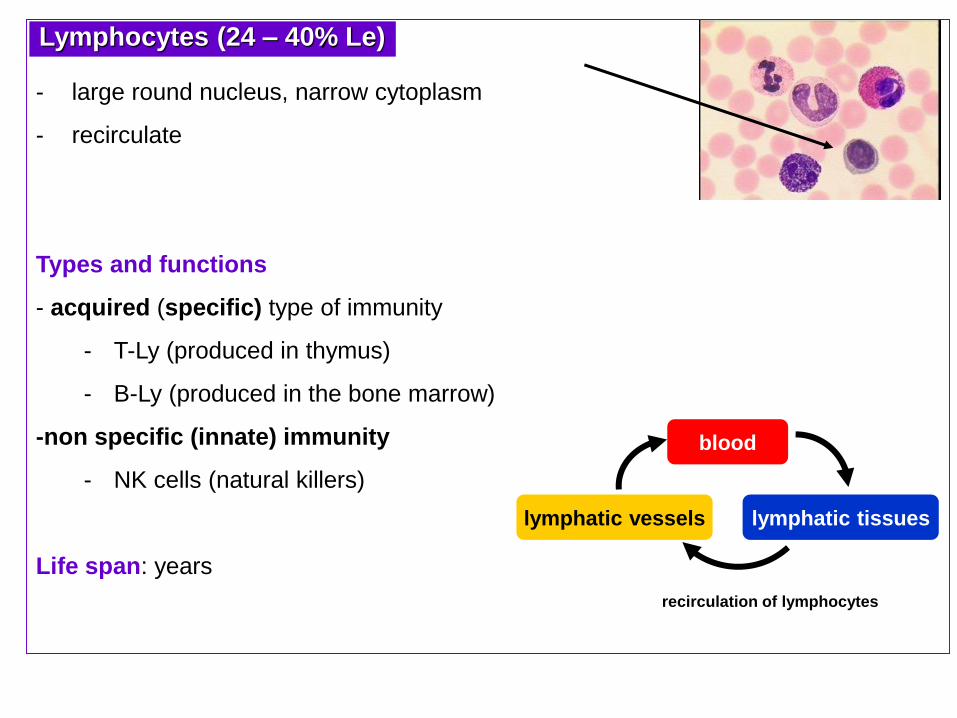
recirculation of lymphocytes
- large round nucleus, narrow cytoplasm
- recirculate
Types and functions
- acquired (specific) type of immunity
- T-Ly (produced in thymus)
- B-Ly (produced in the bone marrow)
-non specific (innate) immunity
- NK cells (natural killers)
Life span: years
Lymphocytes (24 – 40% Le)
blood
lymphatic tissueslymphatic vessels
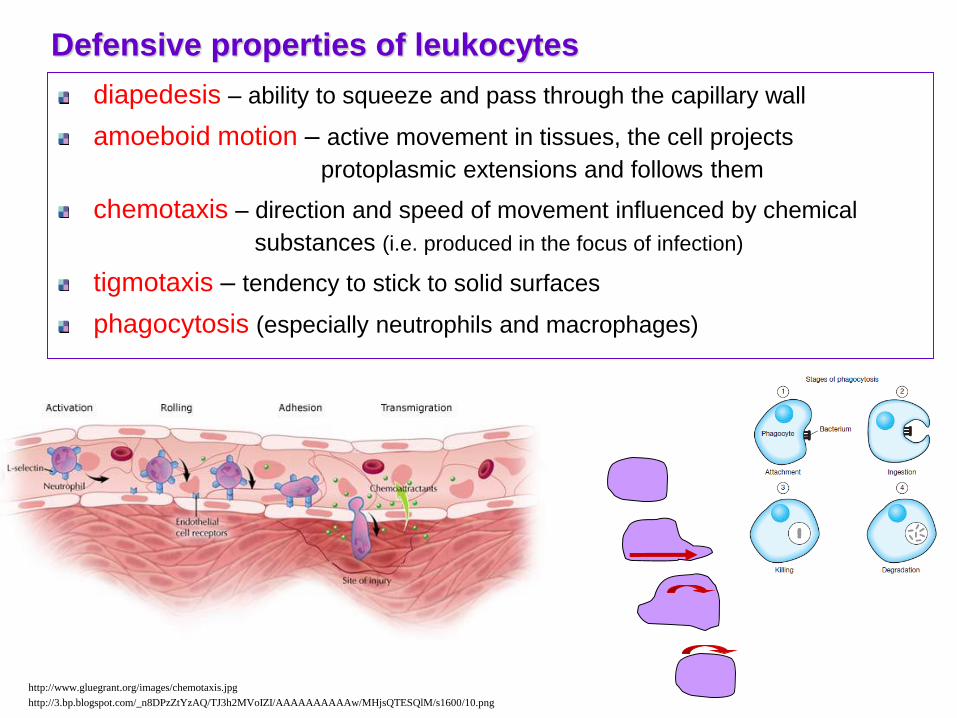
Defensive properties of leukocytes
diapedesis – ability to squeeze and pass through the capillary wall
amoeboid motion – active movement in tissues, the cell projects
protoplasmic extensions and follows them
chemotaxis – direction and speed of movement influenced by chemical
substances (i.e. produced in the focus of infection)
tigmotaxis – tendency to stick to solid surfaces
phagocytosis (especially neutrophils and macrophages)
http://www.gluegrant.org/images/chemotaxis.jpg
http://3.bp.blogspot.com/_n8DPzZtYzAQ/TJ3h2MVoIZI/AAAAAAAAAAw/MHjsQTESQlM/s1600/10.png
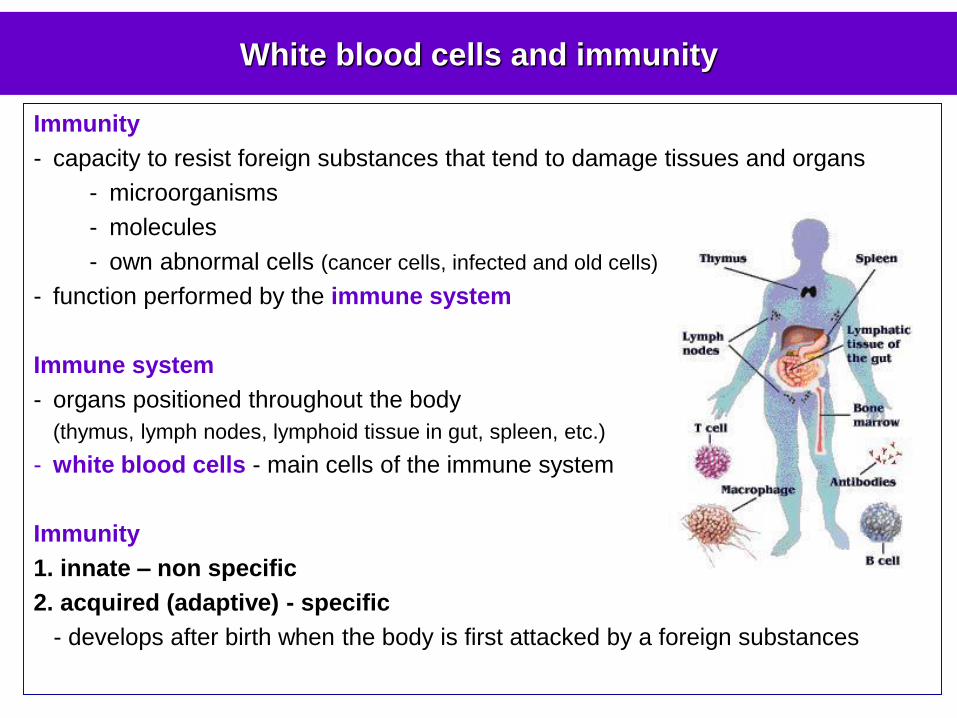
White blood cells and immunity
Immunity
- capacity to resist foreign substances that tend to damage tissues and organs
- microorganisms
- molecules
- own abnormal cells (cancer cells, infected and old cells)
- function performed by the immune system
Immune system
- organs positioned throughout the body
(thymus, lymph nodes, lymphoid tissue in gut, spleen, etc.)
- white blood cells - main cells of the immune system
Immunity
1. innate – non specific
2. acquired (adaptive) - specific
- develops after birth when the body is first attacked by a foreign substances
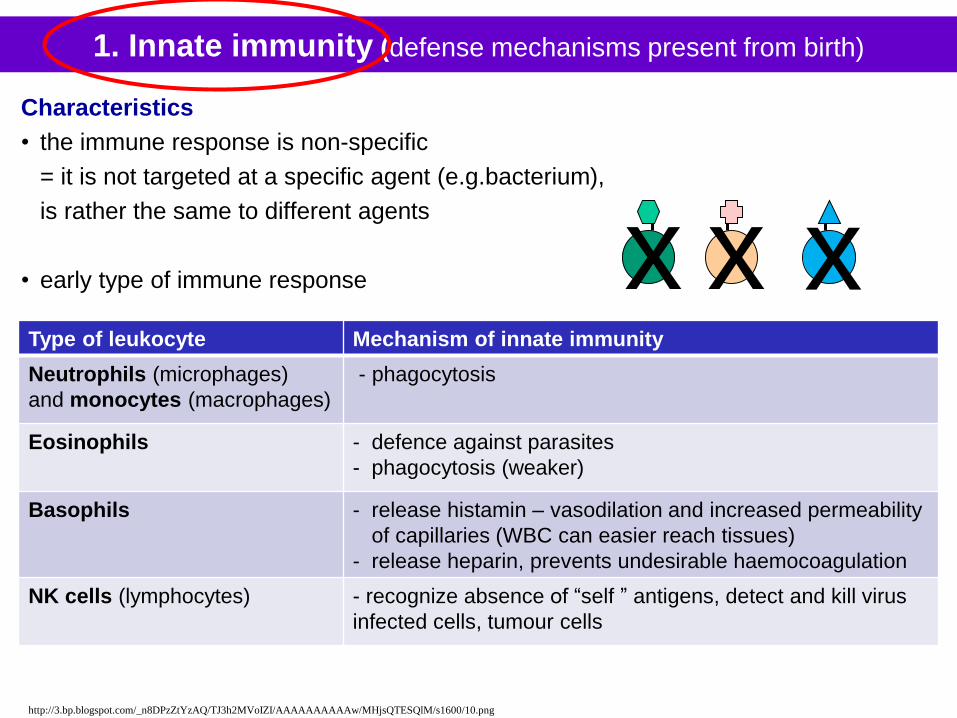
1. Innate immunity (defense mechanisms present from birth)
Characteristics
• the immune response is non-specific
= it is not targeted at a specific agent (e.g.bacterium),
is rather the same to different agents
• early type of immune response x x x
http://3.bp.blogspot.com/_n8DPzZtYzAQ/TJ3h2MVoIZI/AAAAAAAAAAw/MHjsQTESQlM/s1600/10.png
Type of leukocyte Mechanism of innate immunity
Neutrophils (microphages)
and monocytes (macrophages)
- phagocytosis
Eosinophils - defence against parasites
- phagocytosis (weaker)
Basophils - release histamin – vasodilation and increased permeability
of capillaries (WBC can easier reach tissues)
- release heparin, prevents undesirable haemocoagulation
NK cells (lymphocytes) - recognize absence of “self ” antigens, detect and kill virus
infected cells, tumour cells
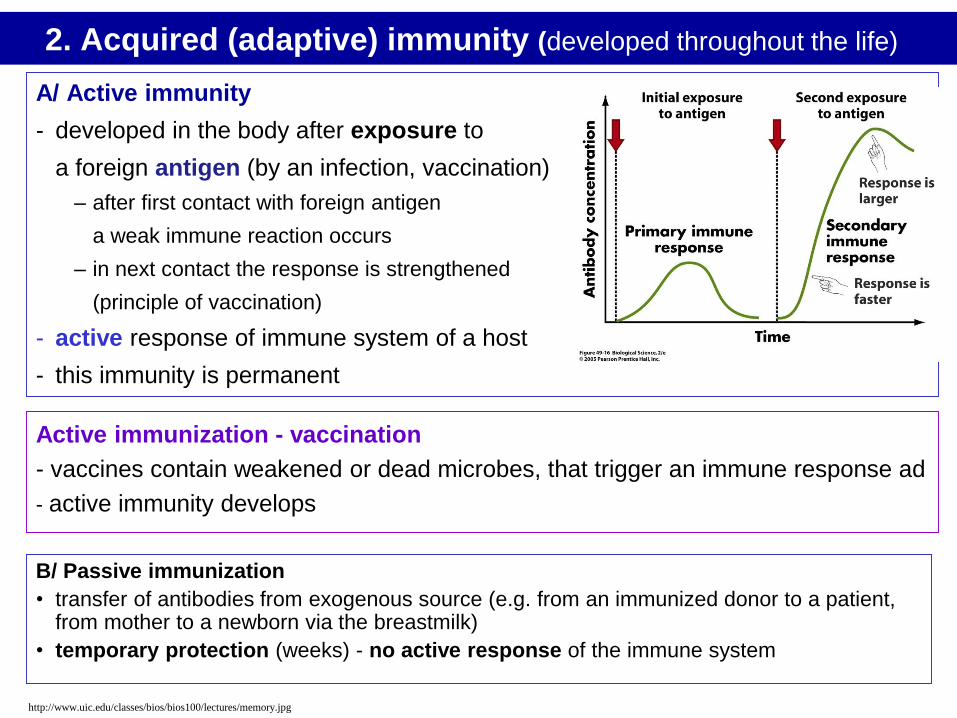
2. Acquired (adaptive) immunity (developed throughout the life)
B/ Passive immunization
• transfer of antibodies from exogenous source (e.g. from an immunized donor to a patient, from mother to a newborn via the breastmilk)
• temporary protection (weeks) - no active response of the immune system
A/ Active immunity
- developed in the body after exposure to
a foreign antigen (by an infection, vaccination)
– after first contact with foreign antigen
a weak immune reaction occurs
– in next contact the response is strengthened
(principle of vaccination)
- active response of immune system of a host
- this immunity is permanent
Active immunization - vaccination
- vaccines contain weakened or dead microbes, that trigger an immune response ad
- active immunity develops
http://www.uic.edu/classes/bios/bios100/lectures/memory.jpg
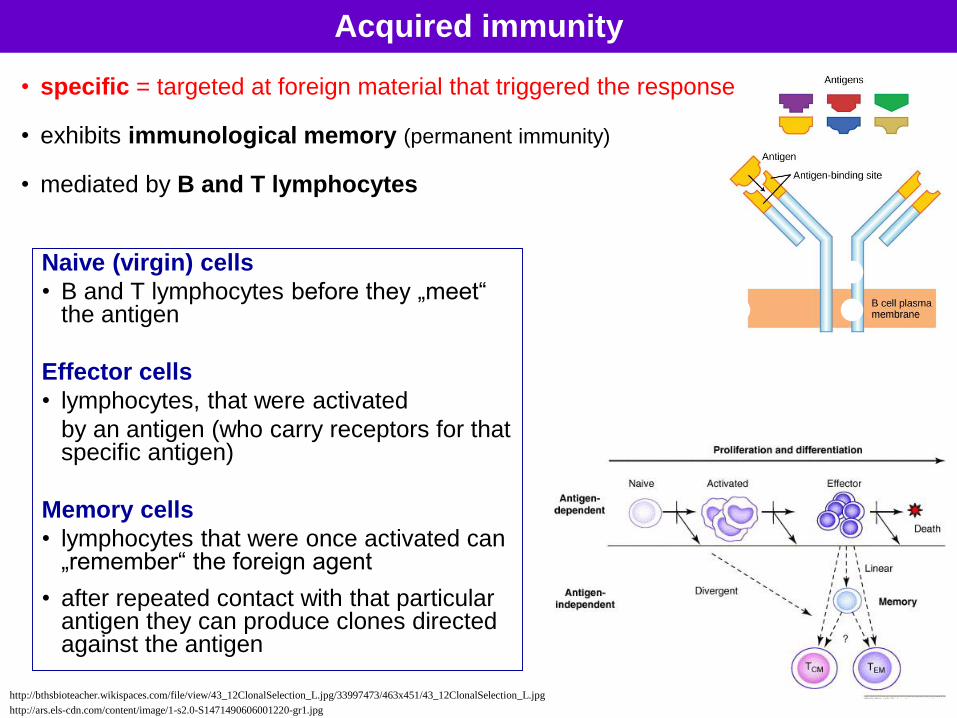
Acquired immunity
• specific = targeted at foreign material that triggered the response
• exhibits immunological memory (permanent immunity)
• mediated by B and T lymphocytes
Naive (virgin) cells
• B and T lymphocytes before they „meet“ the antigen
Effector cells
• lymphocytes, that were activated
by an antigen (who carry receptors for that specific antigen)
Memory cells
• lymphocytes that were once activated can „remember“ the foreign agent
• after repeated contact with that particular antigen they can produce clones directed against the antigen
http://ars.els-cdn.com/content/image/1-s2.0-S1471490606001220-gr1.jpg
http://bthsbioteacher.wikispaces.com/file/view/43_12ClonalSelection_L.jpg/33997473/463x451/43_12ClonalSelection_L.jpg
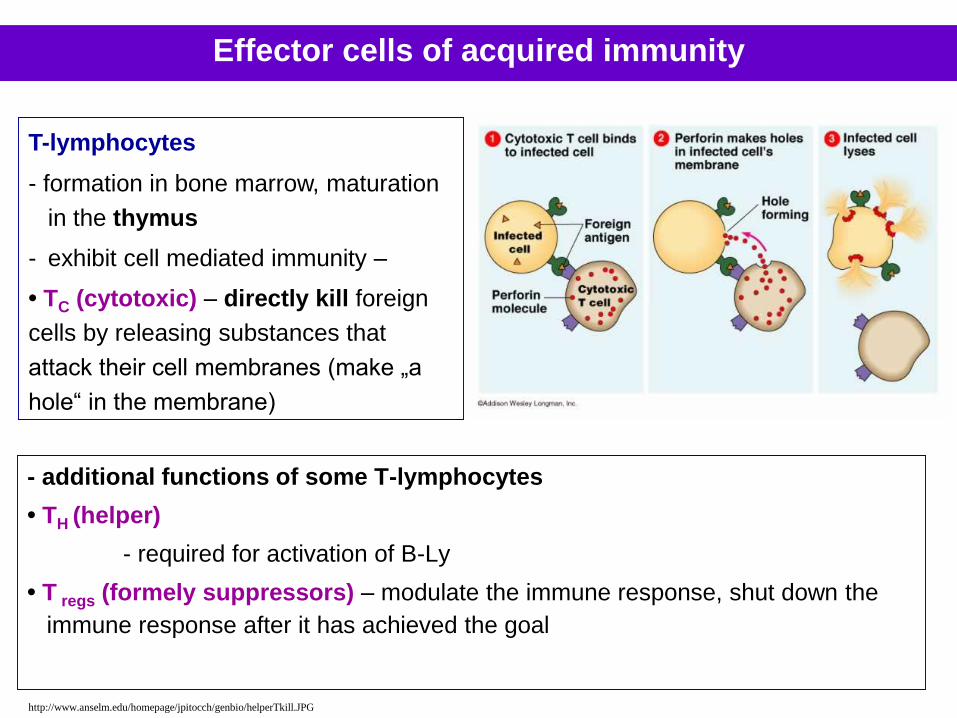
- additional functions of some T-lymphocytes
• TH (helper)
- required for activation of B-Ly
• T regs (formely suppressors) – modulate the immune response, shut down the
immune response after it has achieved the goal
T-lymphocytes
- formation in bone marrow, maturation
in the thymus
- exhibit cell mediated immunity –
• TC (cytotoxic) – directly kill foreign
cells by releasing substances that
attack their cell membranes (make „a
hole“ in the membrane)
http://www.anselm.edu/homepage/jpitocch/genbio/helperTkill.JPG
Effector cells of acquired immunity
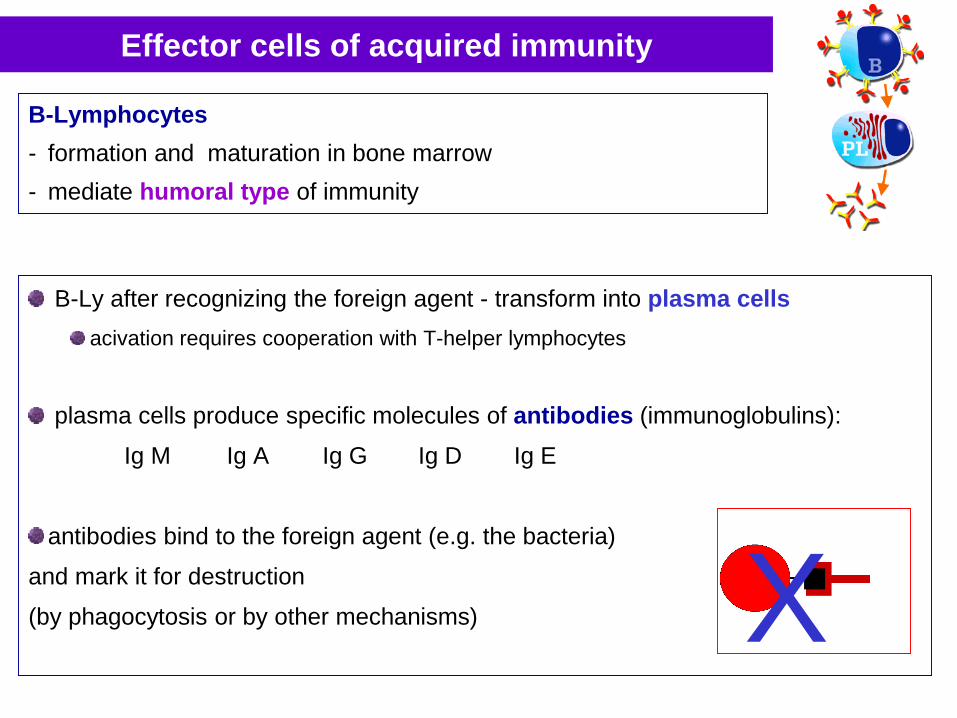
Effector cells of acquired immunity
B-Lymphocytes
- formation and maturation in bone marrow
- mediate humoral type of immunity
B-Ly after recognizing the foreign agent - transform into plasma cells
acivation requires cooperation with T-helper lymphocytes
plasma cells produce specific molecules of antibodies (immunoglobulins):
Ig M Ig A Ig G Ig D Ig E
antibodies bind to the foreign agent (e.g. the bacteria)
and mark it for destruction
(by phagocytosis or by other mechanisms) X
Hematopoiesis
Life span of formed blood elements
erytrocytes 120 days
granulocytes 4 - 5 days
monocytes weeks/months
lymphocytes months/years
thrombocytes 8 – 10 days
Hematopoiesis
- production and development of the blood elements
- maintenance of normal count of formed elements in blood
a neonate, small child- hematopoiesis in all bones
an adult- flat bones- vertebrae- epiphyses of humerus, femur
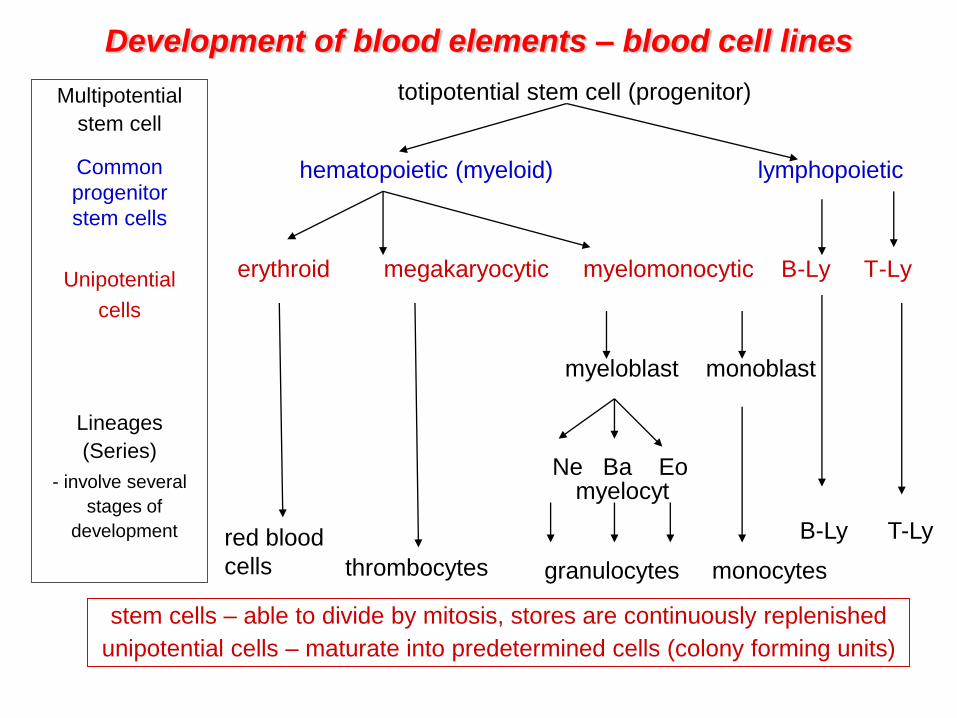
totipotential stem cell (progenitor)
hematopoietic (myeloid) lymphopoietic
erythroid megakaryocytic myelomonocytic B-Ly T-Ly
myeloblast monoblast
Development of blood elements – blood cell lines
Multipotential
stem cell
Common
progenitor
stem cells
Unipotential
cells
Lineages
(Series)
- involve several
stages of
development red blood
cells thrombocytes granulocytes monocytes
B-Ly T-Ly
Ne Ba Eomyelocyt
stem cells – able to divide by mitosis, stores are continuously replenished
unipotential cells – maturate into predetermined cells (colony forming units)
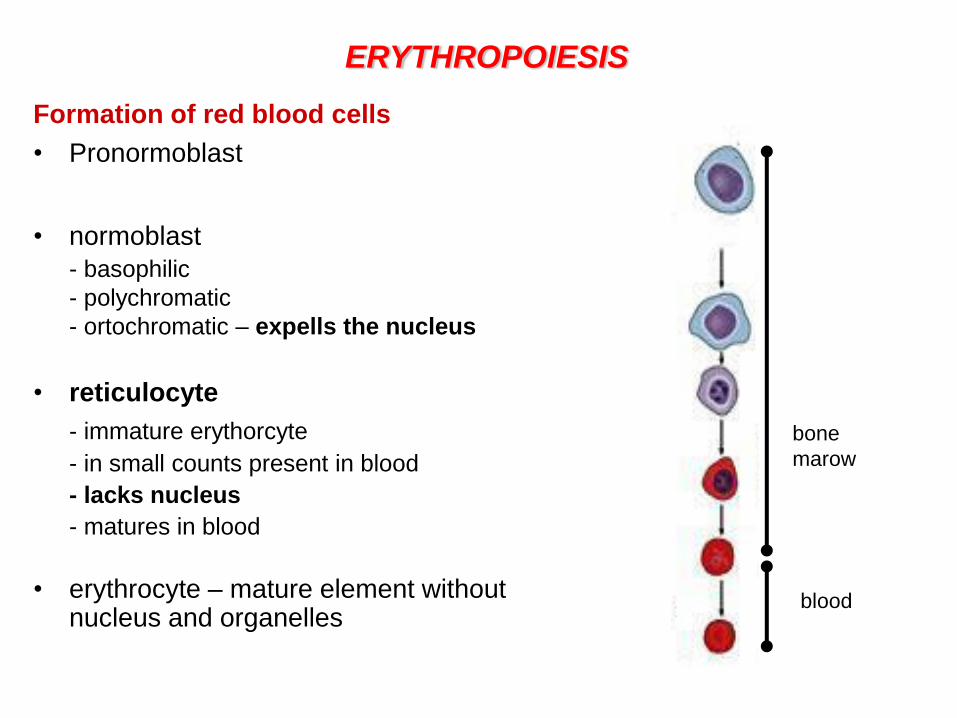
ERYTHROPOIESIS
Formation of red blood cells
• Pronormoblast
• normoblast
- basophilic
- polychromatic
- ortochromatic – expells the nucleus
• reticulocyte
- immature erythorcyte
- in small counts present in blood
- lacks nucleus
- matures in blood
• erythrocyte – mature element without nucleus and organelles
bone
marow
blood
Substances for erythropoiesis- provided by diet - nutrients
amino - acids
iron
A/ food derived - Fe3+
B/ recycled – from destroyed erythrocytes
* deficiency – hypochromic anemia
copper (plasma ceruloplasmin – stores)
- helps in utilisation of iron stores
* deficiency – hypochromic anemia
cobalt
vitamin B12 – extrinsic factor
- it can be absorbed in small intestine only if bound to intrinsic factor
produced in gastric mucosa
folic acid
- synthesis of DNA, erythrocyte maturation
* deficiency of B12 or folate – pernicious anaemia (megalocytic)
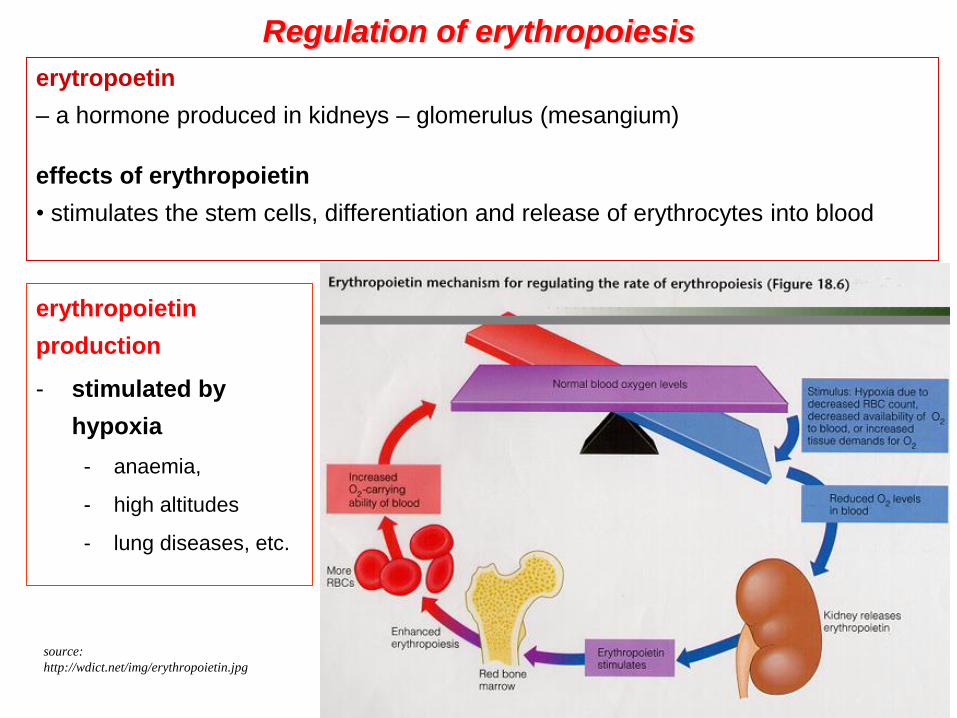
Regulation of erythropoiesis
erytropoetin
– a hormone produced in kidneys – glomerulus (mesangium)
effects of erythropoietin
• stimulates the stem cells, differentiation and release of erythrocytes into blood
erythropoietin
production
- stimulated by
hypoxia
- anaemia,
- high altitudes
- lung diseases, etc.
source:
http://wdict.net/img/erythropoietin.jpg
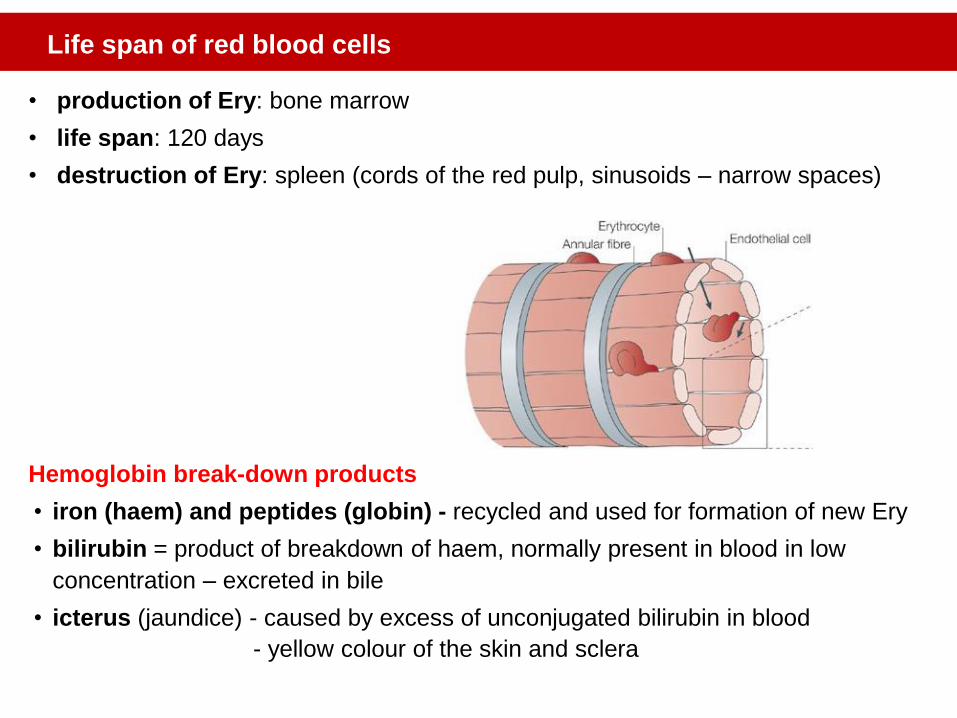
• production of Ery: bone marrow
• life span: 120 days
• destruction of Ery: spleen (cords of the red pulp, sinusoids – narrow spaces)
Hemoglobin break-down products
• iron (haem) and peptides (globin) - recycled and used for formation of new Ery
• bilirubin = product of breakdown of haem, normally present in blood in low
concentration – excreted in bile
• icterus (jaundice) - caused by excess of unconjugated bilirubin in blood
- yellow colour of the skin and sclera
Life span of red blood cells
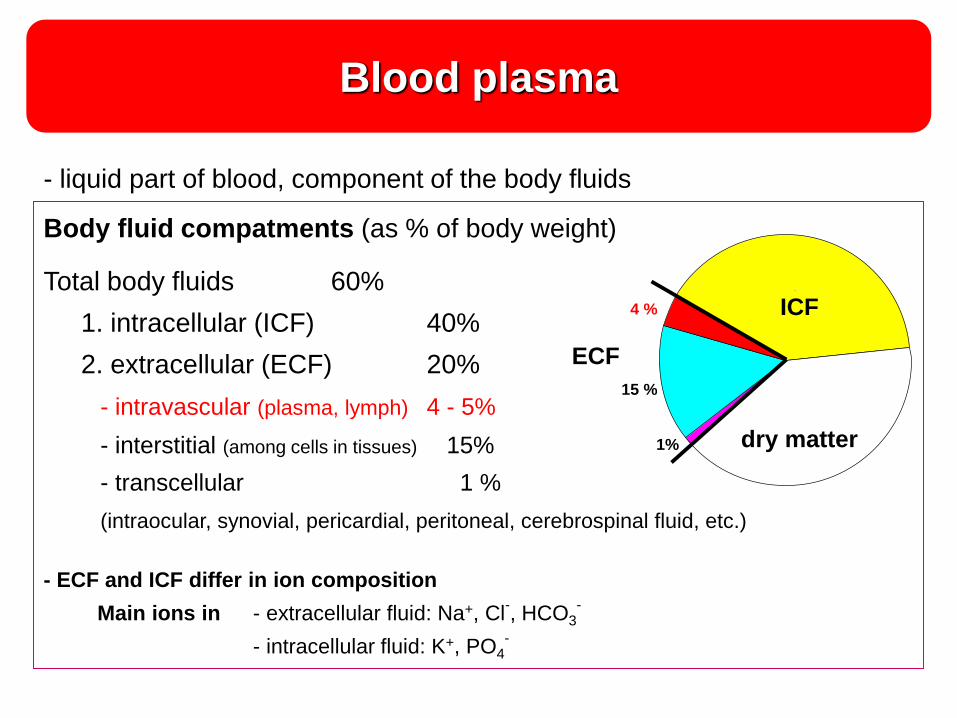
Blood plasma
- tekutá zložka krvi svetložltá
priehľadná tekutina,
- 4-5 % telesnej hmotnosti
Body fluid compatments (as % of body weight)
Total body fluids 60%
1. intracellular (ICF) 40%
2. extracellular (ECF) 20%
- intravascular (plasma, lymph) 4 - 5%
- interstitial (among cells in tissues) 15%
- transcellular 1 %
(intraocular, synovial, pericardial, peritoneal, cerebrospinal fluid, etc.)
- ECF and ICF differ in ion composition
Main ions in - extracellular fluid: Na+, Cl-, HCO3
-
- intracellular fluid: K+, PO4-
sušina
15 %
1%
4 % 40 %
40 %
ICT
ECT ECF
ICF
dry matter
- liquid part of blood, component of the body fluids
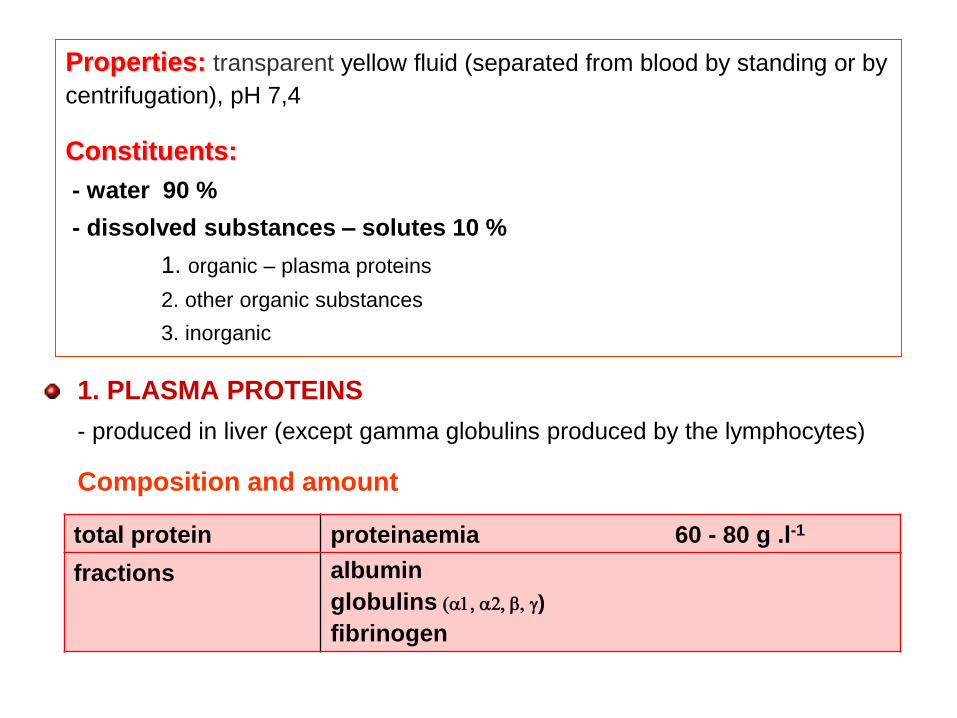
Properties: transparent yellow fluid (separated from blood by standing or by
centrifugation), pH 7,4
Constituents:
- water 90 %
- dissolved substances – solutes 10 %
1. organic – plasma proteins
2. other organic substances
3. inorganic
total protein proteinaemia 60 - 80 g .l-1
fractions albumin
globulins (a1, a2, b, )
fibrinogen
1. PLASMA PROTEINS
- produced in liver (except gamma globulins produced by the lymphocytes)
Composition and amount
Functions:
carriers for other molecules
- bind and transport substances (e.g. lipids, Fe, hormones, drugs, etc.)
blood clotting - plasma clotting factors
immune functions – immunoglobulins, complement
role the sedimentation rate
contribute to blood viscosity and normal blood flow
maintenance of constant pH of plasma
- protein buffer – can bind excess acids/bases, thus balance the pH of blood
nutritional role – rapid supply of amino-acids for tissues
generate the colloid – osmotic pressure
2. OTHER ORGANIC SUBSTANCES IN PLASMA
- include many different substances
glucose
lipids, cholesterol, triglycerides
non-protein substances containing nitrogen - creatin, creatinin, urea, uric acid
bilirubin, hormones, vitamins, etc.
- typically constant plasma concentration, e.g.
- their plasma level indicates function of various organs or systems
• hormone levels-endocrine system • creatine-kidneys
• bilirubin-liver • glucose-pancreas, etc.
Function
• influence physical and chemical properties of plasma, e.g.
- pH
- osmotic pressure,
- constant volume etc.
• role in various biologic processes, e.g.
- buffering
- permeability
- blood clotting, etc.
Serum = plasma without fibrinogen and some other clotting factors
3. INORGANIC SUBSTANCES IN PLASMA
Main cations:
sodium, calcium, potassium, iron, magnesium, copper, iodine
Main anions:
chlorides, bicarbonates, phosphates
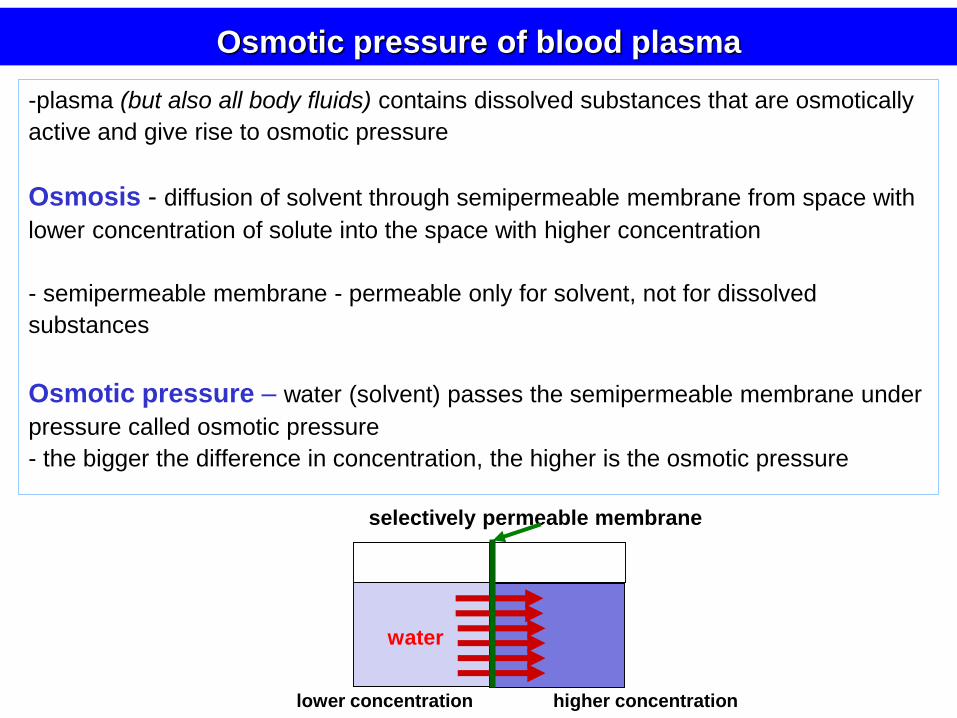
-plasma (but also all body fluids) contains dissolved substances that are osmotically
active and give rise to osmotic pressure
Osmosis - diffusion of solvent through semipermeable membrane from space with
lower concentration of solute into the space with higher concentration
- semipermeable membrane - permeable only for solvent, not for dissolved
substances
Osmotic pressure – water (solvent) passes the semipermeable membrane under
pressure called osmotic pressure
- the bigger the difference in concentration, the higher is the osmotic pressure
selectively permeable membrane
Osmotic pressure of blood plasma
lower concentration higher concentration
vodap
water
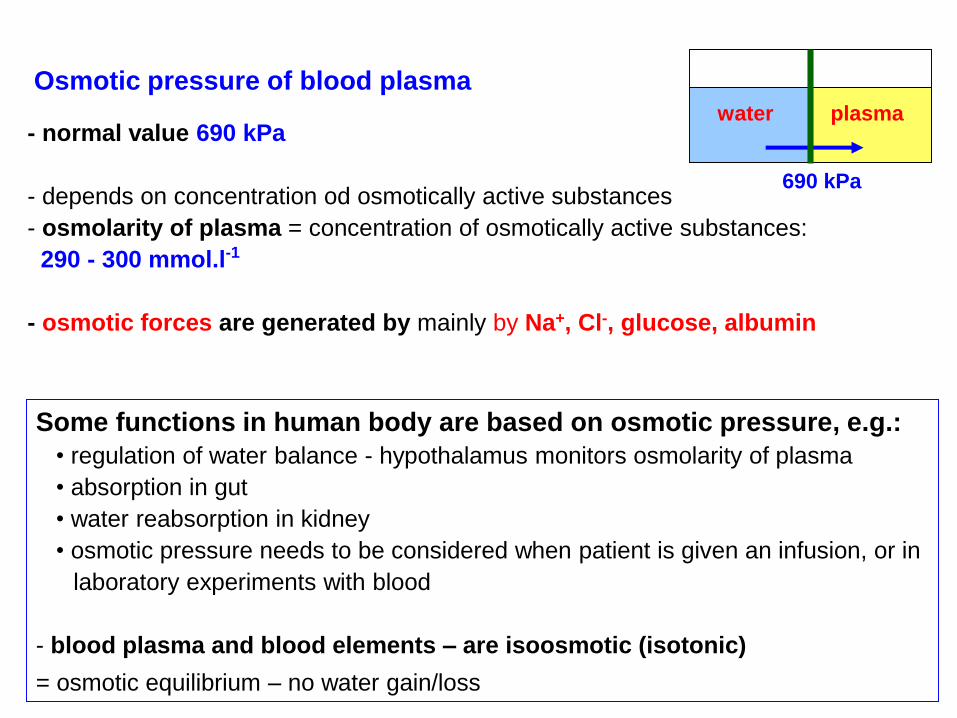
- normal value 690 kPa
- depends on concentration od osmotically active substances
- osmolarity of plasma = concentration of osmotically active substances:
290 - 300 mmol.l-1
- osmotic forces are generated by mainly by Na+, Cl-, glucose, albumin
Osmotic pressure of blood plasma
Some functions in human body are based on osmotic pressure, e.g.:
• regulation of water balance - hypothalamus monitors osmolarity of plasma
• absorption in gut
• water reabsorption in kidney
• osmotic pressure needs to be considered when patient is given an infusion, or in
laboratory experiments with blood
- blood plasma and blood elements – are isoosmotic (isotonic)
= osmotic equilibrium – no water gain/loss
water plasma
690 kPa
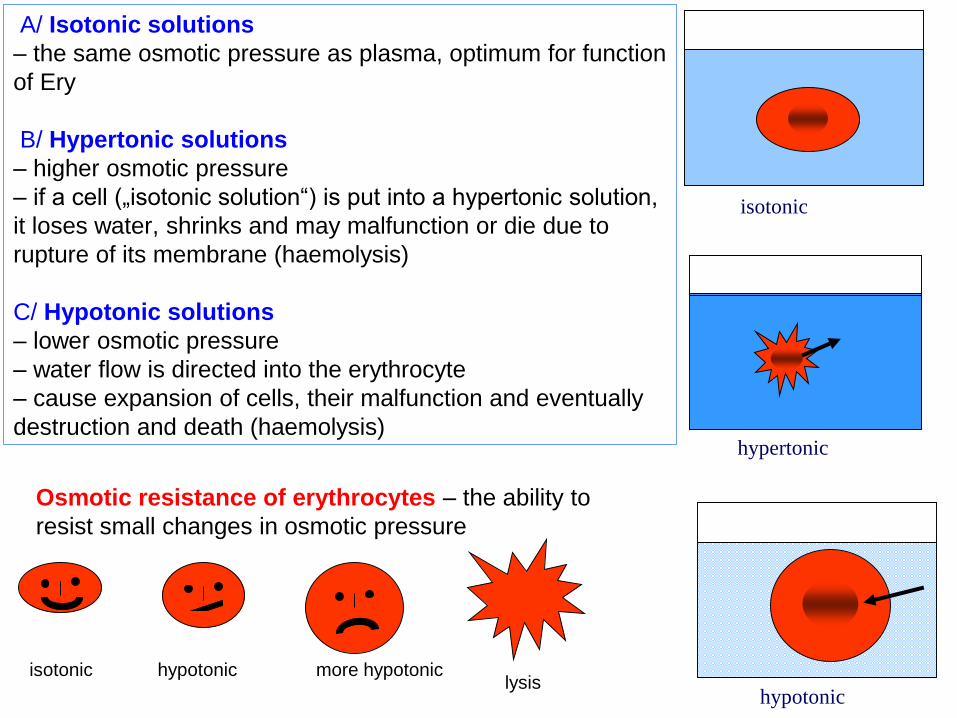
isotonic
hypertonic
hypotonic
Osmotic resistance of erythrocytes – the ability to
resist small changes in osmotic pressure
lysisisotonic hypotonic more hypotonic
A/ Isotonic solutions
– the same osmotic pressure as plasma, optimum for function
of Ery
B/ Hypertonic solutions
– higher osmotic pressure
– if a cell („isotonic solution“) is put into a hypertonic solution,
it loses water, shrinks and may malfunction or die due to
rupture of its membrane (haemolysis)
C/ Hypotonic solutions
– lower osmotic pressure
– water flow is directed into the erythrocyte
– cause expansion of cells, their malfunction and eventually
destruction and death (haemolysis)
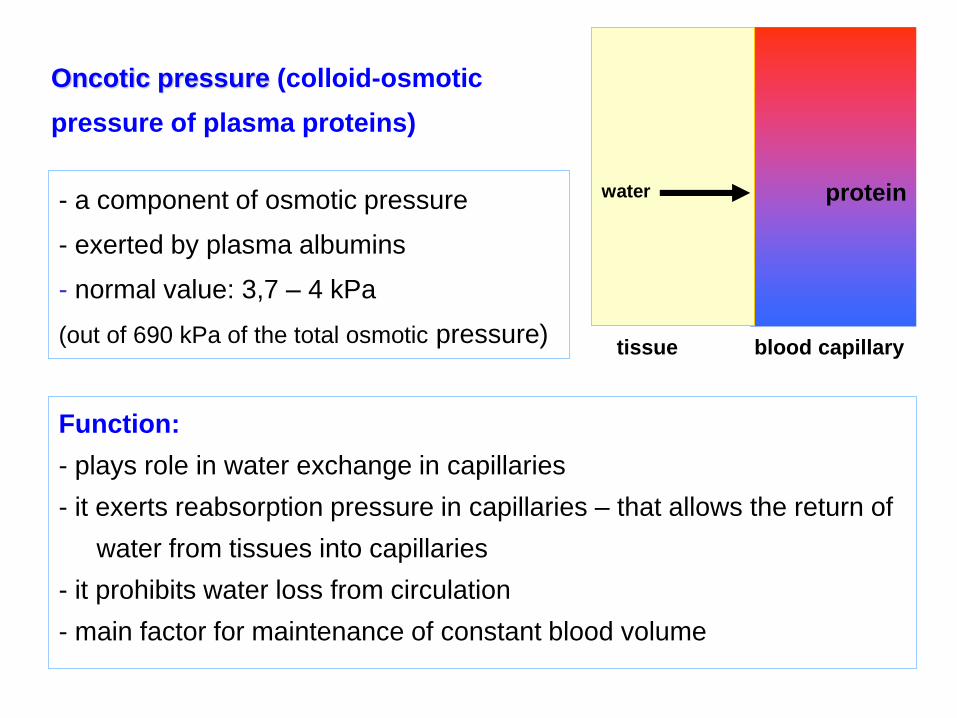
- a component of osmotic pressure
- exerted by plasma albumins
- normal value: 3,7 – 4 kPa
(out of 690 kPa of the total osmotic pressure)
proteinwater
tissue blood capillary
Function:
- plays role in water exchange in capillaries
- it exerts reabsorption pressure in capillaries – that allows the return of
water from tissues into capillaries
- it prohibits water loss from circulation
- main factor for maintenance of constant blood volume
Oncotic pressure (colloid-osmotic
pressure of plasma proteins)
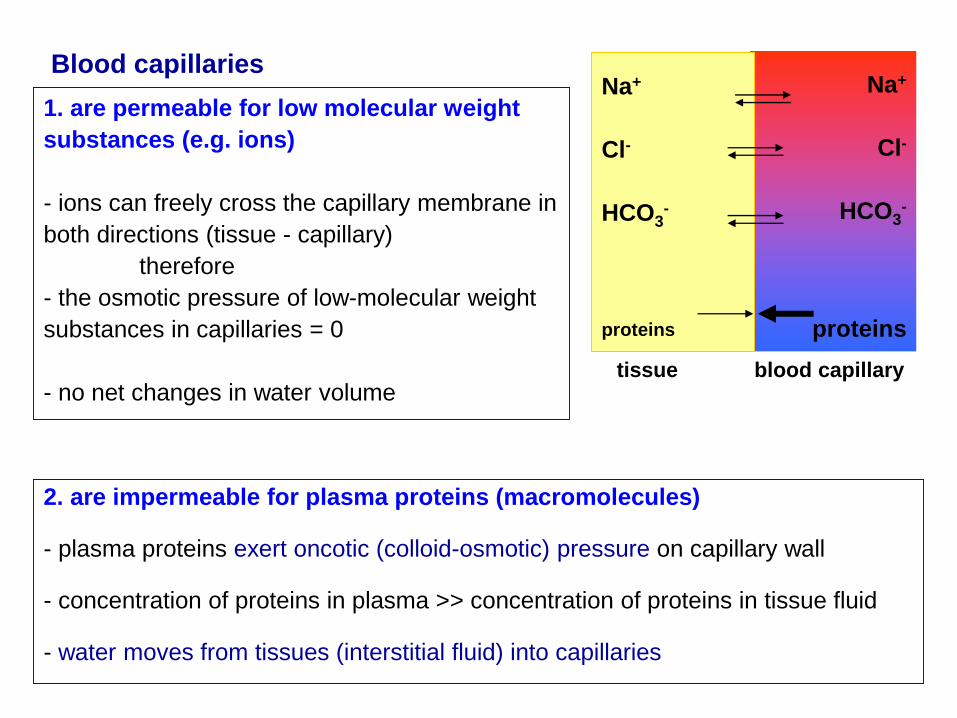
1. are permeable for low molecular weight
substances (e.g. ions)
- ions can freely cross the capillary membrane in
both directions (tissue - capillary)
therefore
- the osmotic pressure of low-molecular weight
substances in capillaries = 0
- no net changes in water volume
Na+
Cl-
HCO3-
proteins
Na+
Cl-
HCO3-
proteins
tissue blood capillary
2. are impermeable for plasma proteins (macromolecules)
- plasma proteins exert oncotic (colloid-osmotic) pressure on capillary wall
- concentration of proteins in plasma >> concentration of proteins in tissue fluid
- water moves from tissues (interstitial fluid) into capillaries
Blood capillaries
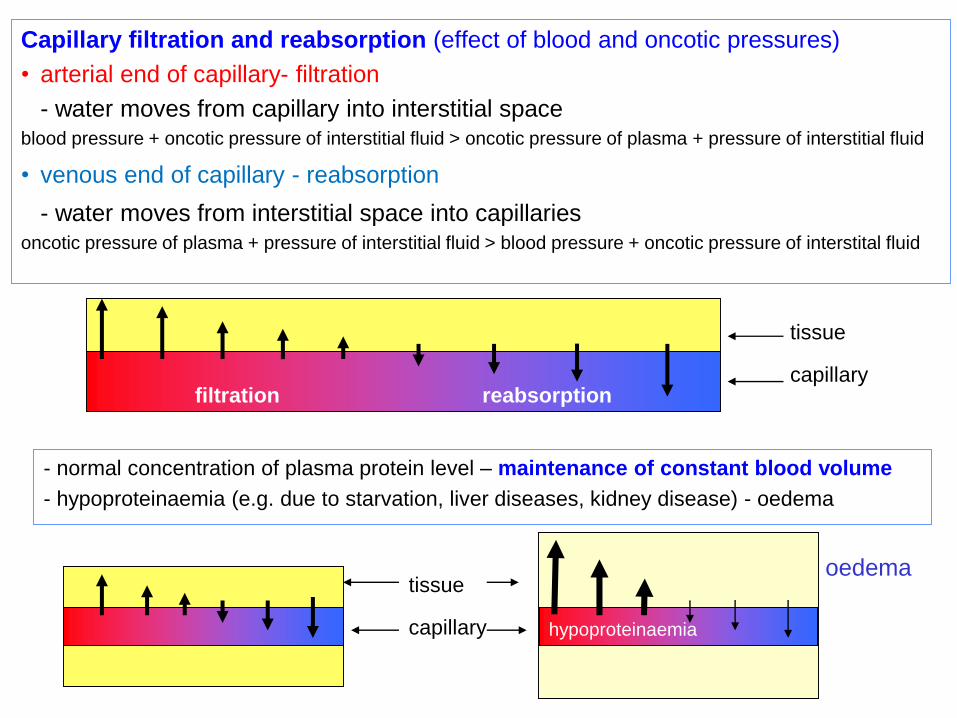
Capillary filtration and reabsorption (effect of blood and oncotic pressures)
• arterial end of capillary- filtration
- water moves from capillary into interstitial spaceblood pressure + oncotic pressure of interstitial fluid > oncotic pressure of plasma + pressure of interstitial fluid
• venous end of capillary - reabsorption
- water moves from interstitial space into capillariesoncotic pressure of plasma + pressure of interstitial fluid > blood pressure + oncotic pressure of interstital fluid
- normal concentration of plasma protein level – maintenance of constant blood volume
- hypoproteinaemia (e.g. due to starvation, liver diseases, kidney disease) - oedema
tissue
capillary
oedema
filtration reabsorption
hypoproteinaemia
tissue
capillary