blepharitis
TRANSCRIPT
177
INTRODUCTIONBlepharitis, first described by Elschnig in 1908,1 is one of the most commonly encountered ophthalmic conditions. It poses a significant challenge to the managing clinician due to its chronic nature and avail-ability of diverse treatment options but lack of scientific evidence for their use. Nonetheless, given the prevalence of blepharitis, its associa-tion with dry eye disease (DED), and its vision-threatening sequelae, better understanding and management of this condition is essential for reducing ocular discomfort and improving the patient’s quality of life.
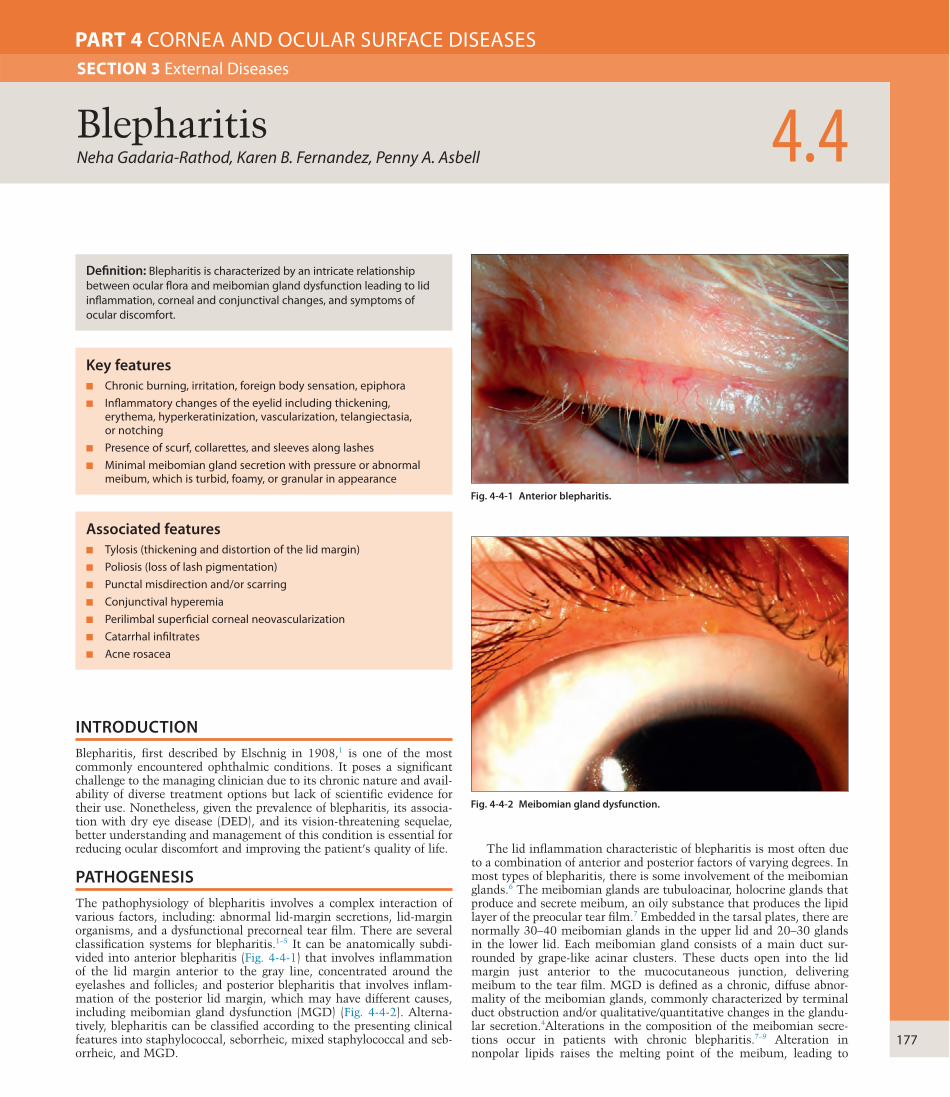
PATHOGENESISThe pathophysiology of blepharitis involves a complex interaction of various factors, including: abnormal lid-margin secretions, lid-margin organisms, and a dysfunctional precorneal tear film. There are several classification systems for blepharitis.1–5 It can be anatomically subdi-vided into anterior blepharitis (Fig. 4-4-1) that involves inflammation of the lid margin anterior to the gray line, concentrated around the eyelashes and follicles; and posterior blepharitis that involves inflam-mation of the posterior lid margin, which may have different causes, including meibomian gland dysfunction (MGD) (Fig. 4-4-2). Alterna-tively, blepharitis can be classified according to the presenting clinical features into staphylococcal, seborrheic, mixed staphylococcal and seb-orrheic, and MGD.
Neha Gadaria-Rathod, Karen B. Fernandez, Penny A. Asbell 4.4Blepharitis
SECTION 3 External Diseases
PART 4 CORNEA AND OCULAR SURFACE DISEASES
Definition: Blepharitis is characterized by an intricate relationship between ocular flora and meibomian gland dysfunction leading to lid inflammation, corneal and conjunctival changes, and symptoms of ocular discomfort.
Key features■ Chronic burning, irritation, foreign body sensation, epiphora■ Inflammatory changes of the eyelid including thickening,
erythema, hyperkeratinization, vascularization, telangiectasia, or notching
■ Presence of scurf, collarettes, and sleeves along lashes■ Minimal meibomian gland secretion with pressure or abnormal
meibum, which is turbid, foamy, or granular in appearance
Associated features■ Tylosis (thickening and distortion of the lid margin)■ Poliosis (loss of lash pigmentation)■ Punctal misdirection and/or scarring■ Conjunctival hyperemia■ Perilimbal superficial corneal neovascularization■ Catarrhal infiltrates■ Acne rosacea
Fig. 4-4-1 Anterior blepharitis.
Fig. 4-4-2 Meibomian gland dysfunction.
The lid inflammation characteristic of blepharitis is most often due to a combination of anterior and posterior factors of varying degrees. In most types of blepharitis, there is some involvement of the meibomian glands.6 The meibomian glands are tubuloacinar, holocrine glands that produce and secrete meibum, an oily substance that produces the lipid layer of the preocular tear film.7 Embedded in the tarsal plates, there are normally 30–40 meibomian glands in the upper lid and 20–30 glands in the lower lid. Each meibomian gland consists of a main duct sur-rounded by grape-like acinar clusters. These ducts open into the lid margin just anterior to the mucocutaneous junction, delivering meibum to the tear film. MGD is defined as a chronic, diffuse abnor-mality of the meibomian glands, commonly characterized by terminal duct obstruction and/or qualitative/quantitative changes in the glandu-lar secretion.4Alterations in the composition of the meibomian secre-tions occur in patients with chronic blepharitis.7–9 Alteration in nonpolar lipids raises the melting point of the meibum, leading to

4
178
CORN
EA A
ND
OCU
LAR SU
RFACE DISEA
SES
rosacea. In ocular rosacea dilated and telangiectatic vessels at the lid margin, and interpalpebral hyperemia may be seen.
DIAGNOSIS AND ANCILLARY TESTINGBlepharitis is mainly a clinical diagnosis. However, ancillary testing may be considered in those who have chronic disease or are unrespon-sive to therapy, to monitor treatment effect, and for research purposes.
Cultures taken from the eyelid margins may grow the typical bacteria associated with blepharitis, as well as viruses, such as herpes simplex, herpes zoster, and molluscum contagiosum. Microscopic examination of the epilated lashes may show demodex eggs, and adult mites.17
Meibomian gland secretion can be analyzed by its quality and expressibility. This can be done by digital pressure or with the use of a device that applies a standard pressure that is equivalent to the pressure exerted on the lids during a normal blink.22 This device is supposed to target a standard area of one-third of the total number of glands (8–10 glands). Expressibility is graded according to the number of glands that express fluid, and decreased expressibility indicates disease. Although it sounds simple, a marked variability exists between individuals, hence a definite cut-off cannot be defined. Also, the location of the glands along the lid margin has influence in their expressibility. It was found that nasal glands tend to express most actively, followed by central glands, and then temporal glands.22 There is also evidence of diurnal fluctuation of meibomian gland expression that may affect diagnosis using this method.23 Quality of glandular secretion can be evaluated in terms of appearance. It can be graded according to how cloudy or vis-cous the secretion is. It can be classified as clear, cloudy opaque, vis-cous, or toothpaste-like using various grading schemes.17,24
Changes in meibomian gland morphology and gland dropout can be assessed using meiboscopy. This is done by transillumination through the skin and observing the glandular silhouette through the everted mucosal side. Photodocumentation of the same is called meibogra-phy.17 Disadvantage of the transillumination method is that it may be tedious and time-consuming. Non-contact meibography applies the same principle but is easier and more rapid than transillumination. It uses an infrared transmitting filter attached to a slit lamp and video camera.25 Photographs are taken and meibomian gland morphology and dropout are then analyzed. In vivo laser scanning confocal micros-copy can be used to examine the microstructure of meibomian gland acinar units and measure their size. These serve as new parameters that significantly correlate with the clinical ocular surface and tear function findings of MGD.26
TREATMENTTreatment strategies include a combination of lid hygiene, manage-ment of MGD, reducing bacterial colonization of the lids, suppression of inflammation, and restoring tear function.27 It is crucial to educate patients about the chronic, recurrent nature of the disease and the need for long-term intervention. Despite the availability of diverse treatment options, very few treatments have been extensively evaluated for safety and efficacy in randomized controlled trials, and most are typically not FDA approved for use in blepharitis specifically. Treatment recommen-dations are largely dependent on clinical experience and published case reports.
Lid hygiene, the mainstay of treatment for blepharitis, consists of warm compresses, lid massage, lid scrubs, and avoidance of excessive eye make-up. Treatment with warm compresses involves the placement of a warm washcloth on closed lids daily for 5–10 minutes. Alternative sources of heat for warm compresses include eye warmer devices with infrared irradiation and moist air or eye warmer masks.27–29 The goals of heat therapy are to soften and loosen encrustations, liquefy the solidified and stagnant secretions and to dilate the ducts. This is fol-lowed by lid massage. The eyelid is held taut at the outer corner with one hand while the index finger of the other hand sweeps from the inner corner of the lid toward the ear while applying pressure. This is repeated several times to express the meibomian gland contents, which have melted during the warm compresses step. Cleansing with lid scrubs is usually done once or twice daily initially. Commercially avail-able scrubs or a cotton-tipped applicator soaked with a weak solution of baby shampoo can be used to rub along the lid margin to remove deposits and the abnormal oily secretions from the lids. Patients should
thickening of the meibum and stagnation. Decreased amounts of polar lipids result in uneven spreading of tears.10 This leads to instability of the tear film and hyperosmolarity, increased bacterial growth, evapora-tive dry eye, and ocular surface inflammation, including keratinization, scarring, and retraction of the gland orifices, thus further exacerbating MGD. Several factors can aggravate MGD such as increasing age, con-tact lens wear, and hormonal imbalance.5,6,9
Several bacteria, fungi (Pitysporum), and parasites (Demodex) have also been implicated. A phenomenon called Quorum sensing causes normally innocuous ocular flora to acquire increased virulence and become pathogenic.11,12 The most common organisms isolated from patients with chronic blepharitis include Staphylococcus epidermidis, Propionibacterium acnes, corynebacteria, and Staphylococcus aureus.13,14 S. epidermidis and S. aureus produce lipolytic enzymes such as triglyceride lipase, cholesterol esterase, and wax esterase, which hydrolyze wax and sterol esters with the release of highly irritating free fatty acids, resulting in the disruption of the tear film integrity.7 In seborrheic blepharitis, the increased amount of low viscosity meibum favors the growth of bacteria and leads to inflammation of the lids.9 Blepharitis is also frequently associated with acne rosacea, seborrheic dermatitis, psoriasis, and atopy.13 Acne rosacea is a relatively common chronic skin disease characterized by persistent erythema, telangiecta-sis, papules, pustules, and sebaceous gland hypertrophy, predominantly affecting the forehead, cheeks, and nose. Though the pathogenesis is still unclear, recent studies suggest that it is primarily due to an altered innate immune response in those with a genetic predisposition. Cer-tain reactive oxygen species and infectious agents such as Demodex folliculorum and H. pylori have also been implicated.15
OCULAR MANIFESTATIONSTypical symptoms of blepharitis include redness, itching, burning, crusting along the lid margin, loss of lashes, stickiness of lashes, and tearing. Furthermore, as MGD has been suggested to be the leading cause of DED,16 symptoms such as dryness, ocular irritation and fluctuating vision may also point a clinician to examine the lid margin. These symptoms are chronic, usually waxing and waning, and may be exacerbated by some environmental factors, such as wind, smoke, dust, cosmetic products, etc. Symptoms are usually bilateral, but may be asymmetrical. The presence of predominantly unilateral symptomatology should alert the clinician to consider other diagnoses that may masquerade as chronic unilateral blepharitis, such as sebaceous cell carcinoma.
External examination using slit-lamp biomicroscopy is essential in establishing diagnosis and determining the type of blepharitis. Staphylo-coccal anterior blepharitis is more common in the younger population with female preponderance. Findings include vascularization and ery-thema of the lid margin, telangiectasia, eyelid edema, loss or misdirec-tion of lashes, collarettes around the base of the lashes, and crusting or hyperkeratosis. Chronic findings of ulceration, punctal misdirection, and scar formation may also be seen. There can be subtle signs of cor-neal involvement in severe cases, presenting with phlyctenulosis, cor-neal neovascularization, thinning, or marginal ulceration. Seborrheic blepharitis is more common in the older age group. It presents with scurfs, which is a term used for the scales, oily debris, and greasy mate-rial that collects along the lash shaft as a result of hypersecretion from the meibomian glands.17 In blepharitis associated with Demodex sp. infestation, the most commonly seen finding is coating of the lash with cylindrical dandruff-like material (sleeves).18
Clinical signs of MGD may include rounding, thickening, and irregularity of the eyelid margin; changes in the lid vascularity and pres-ence of telangiectasia; pouting, plugging, and narrowing of the gland orifices; reduction in volume and number of glands secreting liquid; and changes in gland secretion quality, clarity, and viscosity with greater pressure required to express secretions.18,19 ‘Nonobvious MGD’ is a common form of obstructive MGD that shows no obvious signs of inflammation, hypersecretion, or purulent secretion of the glands.20 In chronic MGD, there may be cicatricial changes along the lid margin, and the mucocutaneous junction may migrate anterior to the meibo-mian gland line.21 Subtle signs, such as frothy quality of the tear menis-cus, and decreased Schirmer’s scores and tear break-up time, may be found. Other ocular conditions, such as recurrent chalazia, trichiasis, and keratoconjunctivitis sicca, may also be seen. External examination of the face and skin may reveal associated dermatologic problems, such as seborrheic dermatitis, atopy, herpes zoster ophthalmicus, and acne

Blepharitis4.4
179
can help improve both MGD and DED. Treatment options include minimally or nonpreserved tears, gels, and ointments, environmental control, and moisture goggles. A newer class of tear substitutes involv-ing the use of lipid-containing eye drops, liposomal sprays, emulsion-type eye drops, and ointments may be more effective than artificial tears in DED associated with MGD.36,37 Dietary supplementation with omega-3 fatty acids has been shown to be effective in improving signs and symptoms of DED and MGD by reducing ocular surface inflamma-tion and improving the lipid composition of meibum.6
There are several additional methods of treatment that have been found to be helpful when used in conjunction with the core interven-tions mentioned above. Antiseborrheic shampoos such as those con-taining selenium sulfide or tar may be helpful when seborrheic dermatitis is significant. Weekly lid scrubs with 50% tea tree oil and daily lid scrubs with tea tree shampoo are effective in eradicating demo-dex infestation of the lids.38 As MGD may be related to androgen defi-ciency or receptor dysfunction, topical androgens are being evaluated as a possible therapeutic option for patients with MGD.39 A new approach for surgically treating MGD is currently being evaluated. It involves insertion of small stainless-steel probes in the meibomian orifices and ducts to remove obstruction and thus improve symptoms.40 Thus, a combination of interventions, including environmental, dietary, phar-macological, and surgical, may provide a more effective approach in future to prevent and treat this chronic disease.
KEY REFERENCESGeerling G, Tauber J, Baudouin C, et al. The international workshop on meibomian gland
dysfunction: report of the subcommittee on management and treatment of meibomian gland dysfunction. Invest Ophthalmol Vis Sci 2011;52:2050–64.
Graham JE, Moore JE, Jiru X, et al. Ocular pathogen or commensal: a PCR-based study of surface bacterial flora in normal and dry eyes. Invest Ophthalmol Vis Sci 2007;48:5616–23.
Ibrahim OMA, Matsumoto Y, Dogru M, et al. The efficacy, sensitivity, and specificity of in vivo laser confocal microscopy in the diagnosis of meibomian gland dysfunction. Ophthalmology 2010;117:665–72.
Knop E, Knop N, Millar T, et al. The international workshop on meibomian gland dysfunction: report of the subcommittee on anatomy, physiology, and pathophysiology of the meibomian gland. Invest Ophthalmol Vis Sci 2011;52:1938–78.
Korb DR, Blackie CA. Meibomian gland diagnostic expressibility: Correlation with dry eye symptoms and gland location. Cornea 2008;27:1142–7.
Lane SS, Dubiner HB, Epstein RJ, et al. A new system, the LipiFlow, for the treatment of meibomian gland dysfunction. Cornea 2012;31:396–404.
Macsai MS. The role of omega-3 dietary supplementation in blepharitis and meibomian gland dysfunction (an AOS thesis). Trans Am Ophthalmol Soc 2008;106:336–56.
Maskin SL. Intraductal meibomian gland probing relieves symptoms of obstructive meibomian gland dysfunction. Cornea 2010;29:1145–52.
Meadows JF, Ramamoorthy P, Nichols JJ, et al. Development of the 4-3-2-1 meibum expressibility scale. Eye Contact Lens 2012;38:86–92.
Nelson JD, Shimazaki J, Benitez-del-Castillo JM, et al. The international workshop on meibomian gland dysfunction: report of the definition and classification subcommittee. Invest Ophthalmol Vis Sci 2011;52:1930–7.
Pult H, Riede-Pult BH. Non-contact meibography in diagnosis and treatment of non-obvious meibomian gland dysfunction. J Optom 2012;5:2–5.
Rubin M, Rao SN. Efficacy of topical cyclosporin 0.05% in the treatment of posterior blepharitis. J Ocul Pharmacol Ther 2006;22:47–53.
Scaffidi RC, Korb DR. Comparison of the efficacy of two lipid emulsion eyedrops in increasing tear film lipid layer thickness. Eye Contact Lens 2007;33:38–44.
Tomlison A, Bron AJ, Korb DR, et al. The International Workshop on Meibomian Gland Dysfunction: Report of the Diagnosis Subcommittee. Invest Ophthalmol Vis Sci 2011;52: 2006–49.
Veldman P, Colby K. Current evidence for topical azithromycin 1% ophthalmic solution in the treatment of blepharitis and blepharitis-associated ocular dryness. Int Ophthalmol Clin 2011;51:43–52.
be instructed to avoid excessive scrubbing and massage, as it can lead to ocular irritation. Besides self-care, therapeutic meibomian gland expression as an in-office procedure performed by the clinician can help relieve MGD. However, therapeutic expression may be painful to the patient. Conventional heat and massage techniques are frequently inef-fective in delivering heat to the meibomian glands. Recently, a new thermopulsation device has been developed, which allows heat to be applied to the palpebral surfaces of the lids directly over the meibomian glands while simultaneously applying graded pulsatile pressure to the outer eyelid surfaces, thereby gently expressing the meibomian glands during heating.30
Topical antibiotics are added when underlying bacterial infection is suspected. Bacitracin and erythromycin ophthalmic ointments are effective agents for anterior blepharitis. Generally, ointments are applied directly to the lid margins to avoid toxicity to the ocular sur-face. Fluoroquinolone eye drops have minimal ocular toxicity with a wide coverage of organisms. However, emergence of resistant organ-isms has limited their use. Topical fusidic acid has shown efficacy in patients with ocular rosacea blepharitis. Though not yet FDA approved, topical metronidazole gel 0.75–1.0% also may be effective when used on the lid margin for treatment of ocular rosacea.27 Systemic antibiotics like cloxacillin may be added for treatment of persistent or recurrent staphylococcal blepharitis. Oral tetracyclines are commonly used in the management of rosacea and MGD. They are mainly used for their anti-inflammatory and lipid-regulating properties, rather than for their antimicrobial effects. They decrease the production of bacterial lipases, thus reducing the concentration of free fatty acids and their deleterious effects on lipid composition.31 They exert anti-inflammatory effects due to inhibition of matrix metalloproteinases (MMPs), cytokines, lym-phocyte and neutrophil activation, and chemotaxis. They also have anti-angiogenic and anti-apoptotic properties.32 They are usually used in doses ranging between 250 mg once to four times a day (tetracycline and oxytetracycline) and 50–100 mg once or twice a day (doxycycline and minocycline). Low doses of doxycycline 20 mg may be used when long-term therapy is required. A 40 mg/day slow release dose of doxy-cycline is approved for treatment of rosacea and is used by some clini-cians. Tetracycline use is limited by its common side-effects, which include sun sensitivity and gastrointestinal upset and known contrain-dications to use in pregnant women and children. Oral macrolide anti-biotics, like erythromycin and azithromycin, are safer and also have immunomodulatory and anti-inflammatory effects similar to tetracy-clines. Recently, the use of a topical azithromycin (1%) was suggested as an effective treatment of posterior blepharitis, with a significant improvement in meibomian gland secretion quality, eyelid redness, tear quality, and overall symptomatic relief, but results from studies regard-ing efficacy are mixed.33
In cases with more severe lid margin inflammation, a short-term course of topical steroids or antibiotic–steroid combinations may be utilized. However, long-term use of steroids is limited by their serious side-effects such as cataracts, glaucoma, superinfection, and corneal thinning. Topical immunomodulators like cyclosporine A 0.05%, a calcineurin inhibitor, have been shown to be beneficial in the treatment of MGD in conjunction with rosacea and/or DED, with a significant improvement in lid margin inflammation and signs of DED.34 Tac-rolimus, a potent immunosuppressive agent that inhibits the transcrip-tion of interleukin-2, may be an effective alternative for blepharitis that is refractory to traditional treatments;35 however, evidence for the same is very limited.
As change in tear composition and tear film stability is a key con-tributor to lid margin inflammation, supplementation of the tear film
Access the complete reference list online at

Blepharitis4.4
179.e1
REFERENCES1. Mathers WD, Shields WJ, Sachdev MS, et al. Meibomian gland dysfunction in chronic
blepharitis. Cornea 1991;10:277–85.2. Krachmer JH, Mannis MJ, Holland EJ, editors. Cornea: fundamentals, diagnosis, and
management. 2nd ed. St Louis, MO: Elsevier–Mosby; 2005.3. McCulley JP, Dougherty JM, Deneau DG. Classification of chronic blepharitis. Ophthalmology
1982;89:1173–80.4. Nelson JD, Shimazaki J, Benitez-del-Castillo JM, et al. The International Workshop on
Meibomian Gland Dysfunction: Report of the Definition and Classification Subcommittee. Invest Ophthalmol Vis Sci 2011;52:1930–7.
5. Jackson WB. Blepharitis: current strategies for diagnosis and management. Can J Ophthalmol 2008;43:170–9.
6. Macsai MS. The role of omega-3 dietary supplementation in blepharitis and meibomian gland dysfunction (an AOS thesis). Trans Am Ophthalmol Soc 2008;106:336–56.
7. Bron AJ, Sci FM, Tiffany JM. The contribution of meibomian disease to dry eye. Ocul Surf 2004;2:149–65.
8. McCulley JP, Shine WE. Meibomian secretions in chronic blepharitis. Adv Exp Med Biol 1998;438:319–26.
9. Knop E, Knop N, Millar T, et al. The International Workshop on Meibomian Gland Dysfunction: Report of the Subcommittee on Anatomy, Physiology, And Pathophysiology of the Meibomian Gland. Invest Ophthalmol Vis Sci 2011;52:1938–78.
10. Bron AJ, Tiffany JM, Gouveia SM. Functional aspects of the tear film layer. Exp Eye Res 2004;78:347–60.
11. Graham JE, Moore JE, Jiru X, et al. Ocular pathogen or commensal: a PCR-based study of surface bacterial flora in normal and dry eyes. Invest Ophthalmol Vis Sci 2007;48:5616–23.
12. Bassler BL, Losick R. Bacterially speaking. Cell 2006;125:237–46.13. Cher I. Chronic blepharitis: eyelid bugbear, not always bearing bugs. Mod Med Austr
1997;May:52–62.14. Yamasaki K, Gallo RL. The molecular pathology of rosacea. J Dermatol Sci 2009;55:77–81.15. Oltz M, Check J. Rosacea and its ocular manifestations. Optometry 2011;82:92–103.16. Nichols KK, Foulks GN, Bron AJ, et al. The International Workshop on Meibomian Gland
Dysfunction: Executive Summary. Invest Ophthalmol Vis Sci 2011;52:1922–29.17. Tomlison A, Bron AJ, Korb DR, et al. The International Workshop on Meibomian Gland
Dysfunction: Report of the Diagnosis Subcommittee. Invest Ophthalmol Vis Sci 2011;52:2006–49.
18. Liu J, Sheha H, Tseng, SCG. Pathogenic role of Demodex mites in blepharitis. Curr Opin Allergy Clin Immunol 2010;10:505–10.
19. Foulks GN, Bron AJ. Meibomian gland dysfunction: a clinical scheme for description, diagnosis, classification and grading. Ocul Surf 2003;1:107–26.
20. Blackie CA, Korb DR, Knop E, et al. Nonobvious obstructive meibomian gland dysfunction. Cornea 2010; Epub Sep 15. Curr Opin Allergy Clin Immunol 2010;10:505–10.
21. Yamaguchi M, Kutsuna M, Uno T, et al. Marx line: fluorescein staining line on the inner lid as indicator of meibomian gland function. Am J Ophthalmol 2006;141:669–75.
22. Korb DR, Blackie CA. Meibomian gland diagnostic expressibility: Correlation with dry eye symptoms and gland location. Cornea 2008;27:1142–7.
23. Blackie CA, Korb DR. The diurnal secretory characteristics of individual meibomian glands. Cornea 2010;29:34–8.
24. Meadows JF, Ramamoorthy P, Nichols JJ, et al. Development of the 4-3-2-1 meibum expressibility scale. Eye Contact Lens 2012;38:86–92.
25. Pult H, Riede-Pult BH. Non-contact meibography in diagnosis and treatment of non-obvious meibomian gland dysfunction. J Optom 2012;5:2–5.
26. Ibrahim OMA, Matsumoto Y, Dogru M, et al. The efficacy, sensitivity, and specificity of in vivo laser confocal microscopy in the diagnosis of meibomian gland dysfunction. Ophthalmology 2010;117:665–72.
27. Geerling G, Tauber J, Baudouin C, et al. The International Workshop on Meibomian Gland Dysfunction: Report of the Subcommittee on Management and Treatment of Meibomian Gland Dysfunction. Invest Ophthalmol Vis Sci 2011;52:2050–64.
28. Mori A, Shimazaki J, Shimmura S, et al. Disposable eyelid-warming device for the treatment of meibomian gland dysfunction. Jpn J Ophthalmol 2003;27:578–86.
29. Ishida R, Matsumuto Y, Onguchi T, et al. Tear film with ‘Orgahexa EyeMasks’ in patients with meibomian gland dysfunction. Optom Vis Sci 2008;85:684–6.
30. Lane SS, Dubiner HB, Epstein RJ, et al. A new system, the LipiFlow, for the treatment of meibomian gland dysfunction. Cornea 2012;31:396–404.
31. Dougherty JM, McCulley JP, Silvany RE, et al. The role of tetracycline in chronic blepharitis. Inhibition of lipase production in staphylococci. Invest Ophthalmol Vis Sci 1991;32:2970–5.
32. De Paiva CS, Corrales RM, Villarreal AL, et al. Corticosteroid and doxycycline suppress MMP-9 and inflammatory cytokine expression, MAPK activation in the corneal epithelium in experimental dry eye. Exp Eye Res 2006;83:526–35.
33. Veldman P, Colby K. Current evidence for topical azithromycin 1% ophthalmic solution in the treatment of blepharitis and blepharitis-associated ocular dryness. Int Ophthalmol Clin 2011;51:43–52.
34. Rubin M, Rao SN. Efficacy of topical cyclosporin 0.05% in the treatment of posterior blepharitis. J Ocul Pharmacol Ther 2006;22:47–53.
35. Joseph MA, Kaufman HE, Insler M. Topical tacrolimus ointment for treatment of refractory anterior segment inflammatory disorders. Cornea 2005;24:417–20.
36. Scaffidi RC, Korb DR. Comparison of the efficacy of two lipid emulsion eyedrops in increasing tear film lipid layer thickness. Eye Contact Lens 2007;33:38–44.
37. Goto E, Dogru M, Fukagawa K, et al. Successful tear lipid layer treatment for refractory dry eye in office workers by low-dose lipid application on the full-length eyelid margin. Am J Ophthalmol 2006;142:264–70.
38. Gao YY, Di Pascuale MA, Elizondo A, et al. Clinical treatment of ocular demodecosis by lid scrub with tea tree oil. Cornea 2007;26:136–43.
39. Sullivan BD, Evans JE, Krenzer KL, et al. Impact of antiandrogen treatment on the fatty acid profile of neutral lipids in human meibomian gland secretions. J Clin Endocrinol Metab 2000;85:4866–73.
40. Maskin SL. Intraductal meibomian gland probing relieves symptoms of obstructive meibomian gland dysfunction. Cornea 2010;29:1145–52.