bleeding tendency
TRANSCRIPT
APPROACH TO BLEEDING TENDENCY
Hamad Emad H. Dhuhayr
CONTENT
• Overview
• approach to bleeding tendency
1. Taking history
2. Physical examination
3. Laboratory
• references
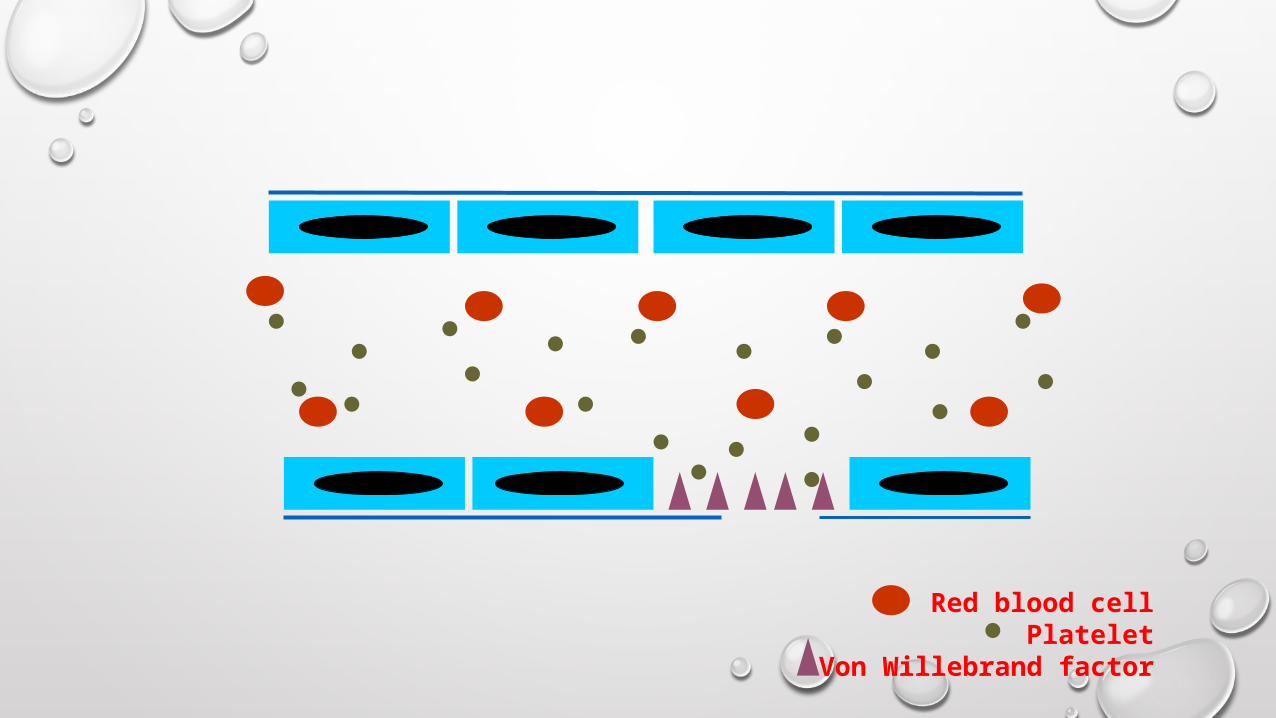
VASCULAR CONTRACTION
1. Local myogenic spasm
2. Local autacoid factors from traumatized tissue and blood platelets
3. Nervous reflexes
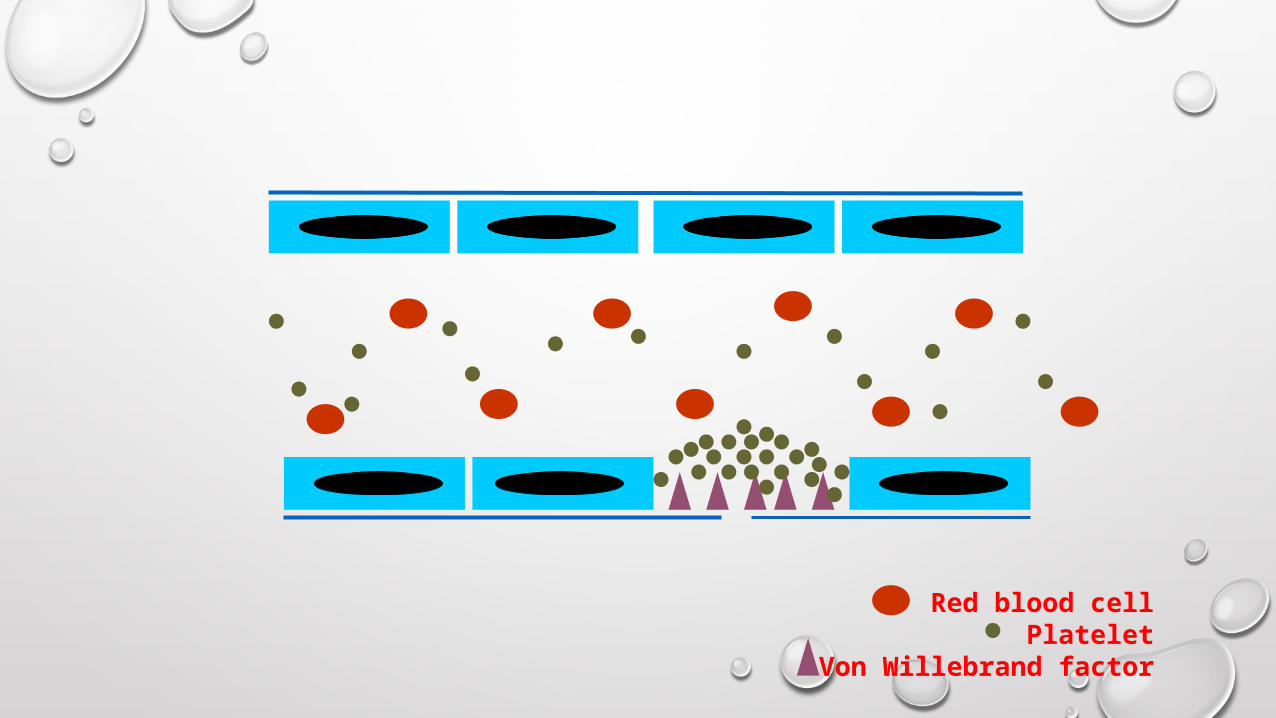
Red blood cellPlatelet
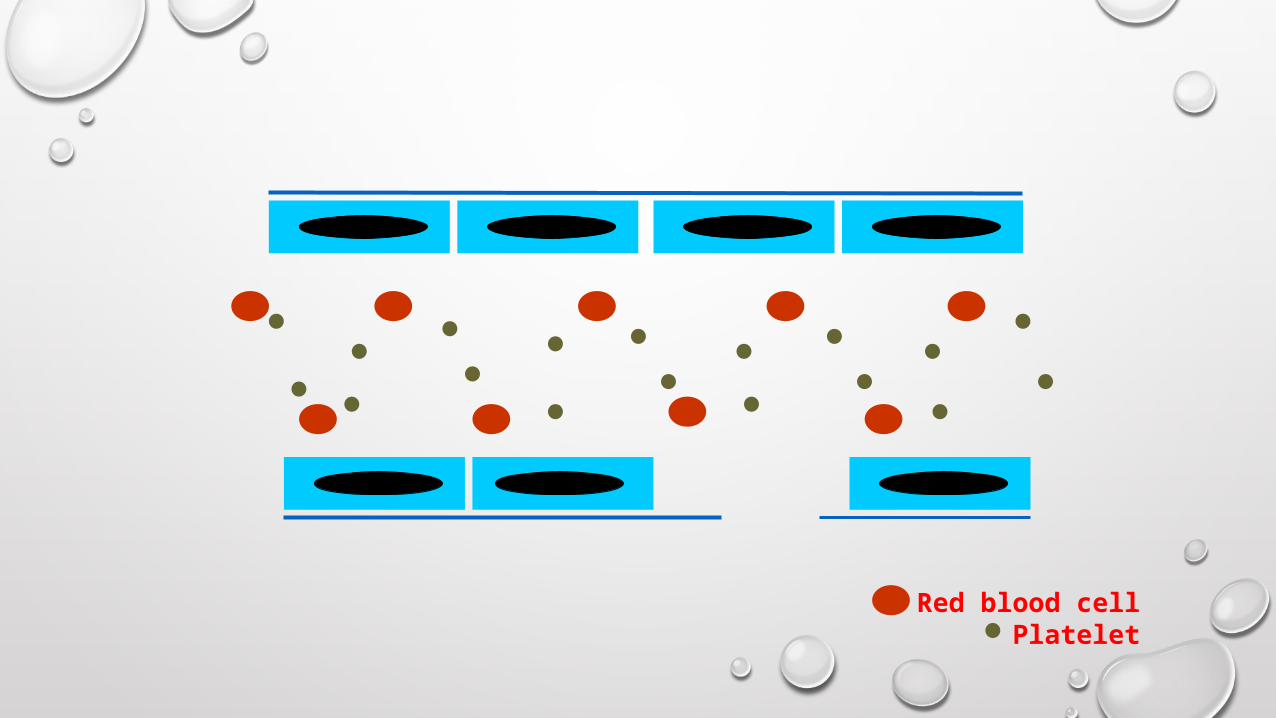
Red blood cellPlatelet

Red blood cellPlatelet
Von Willebrand factor
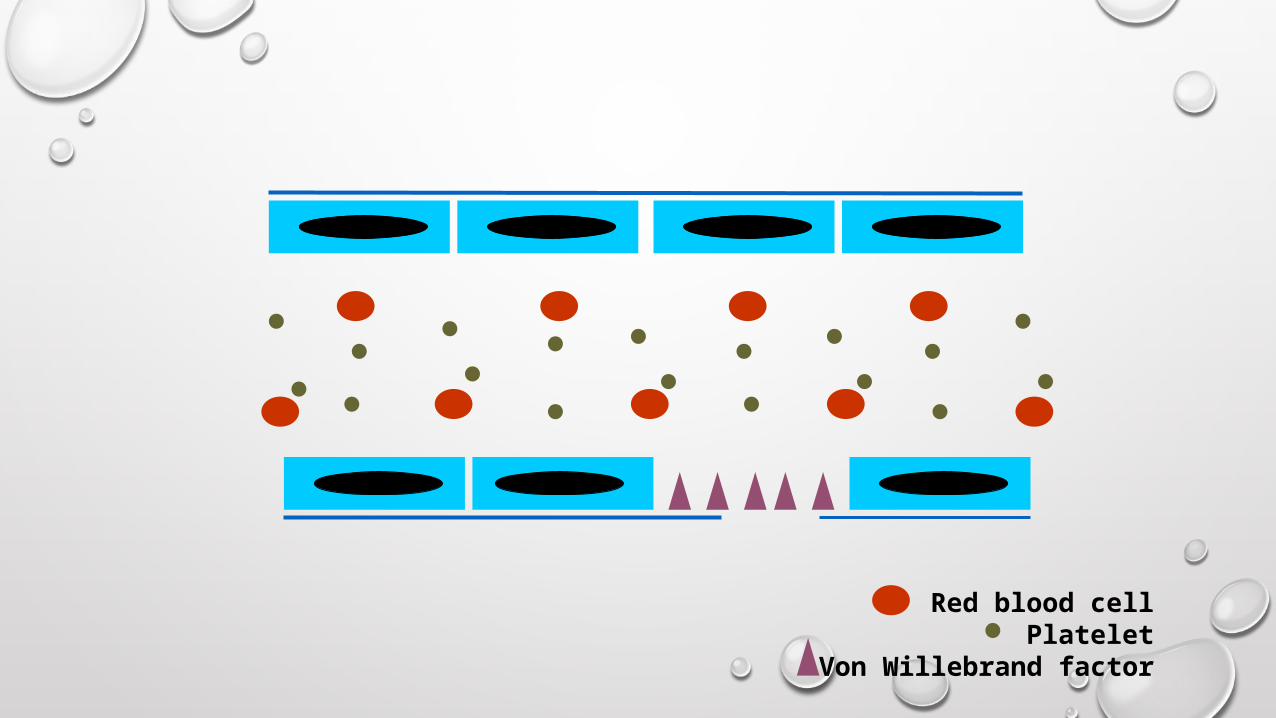
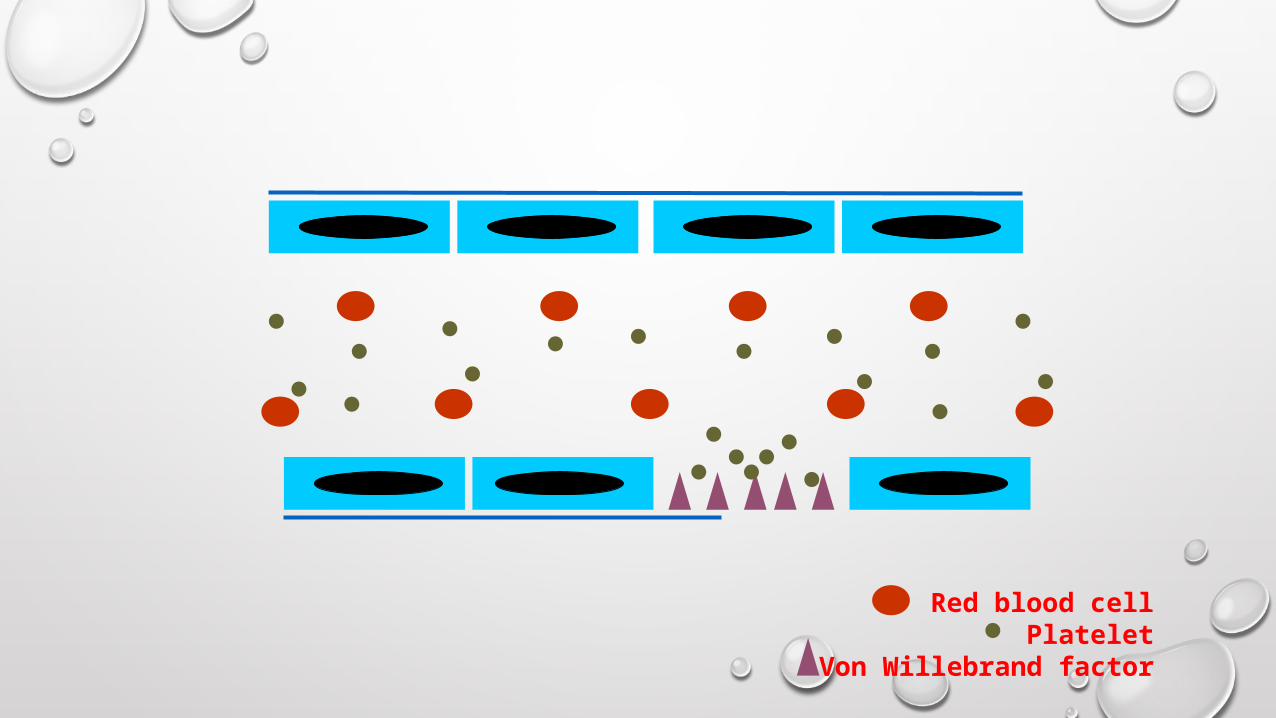
Red blood cellPlatelet
Von Willebrand factor
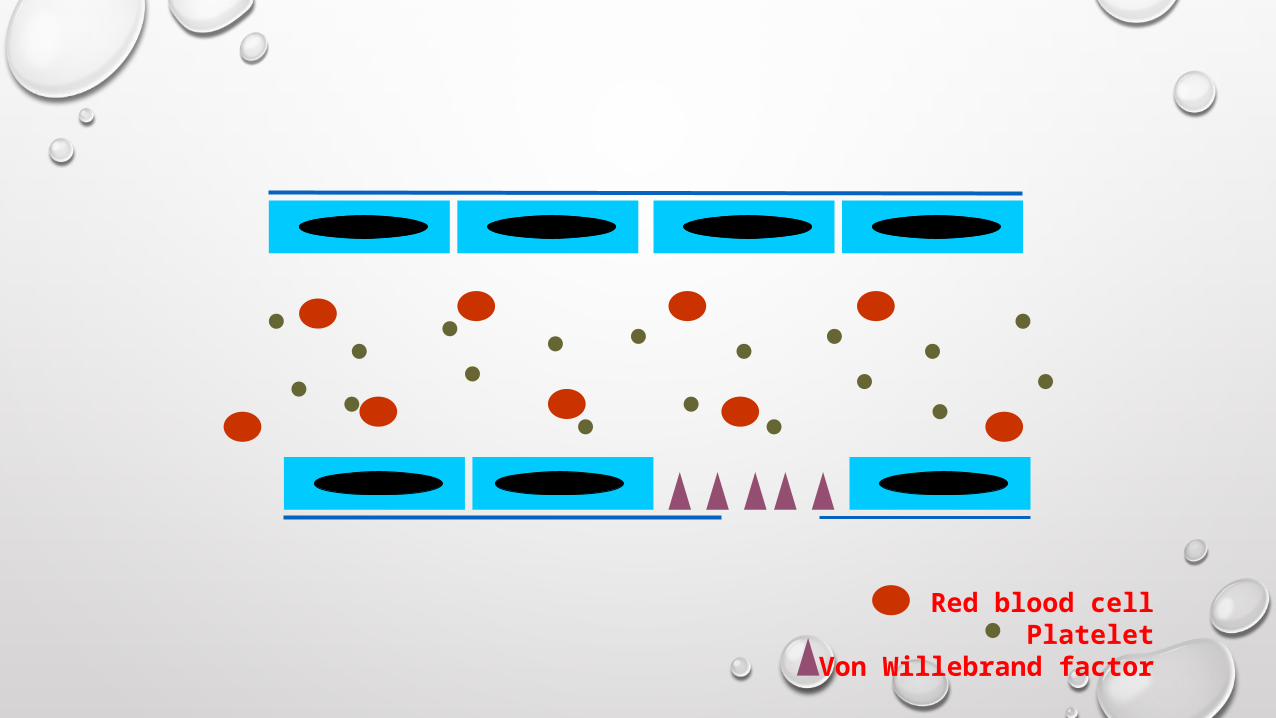
Red blood cellPlatelet
Von Willebrand factor
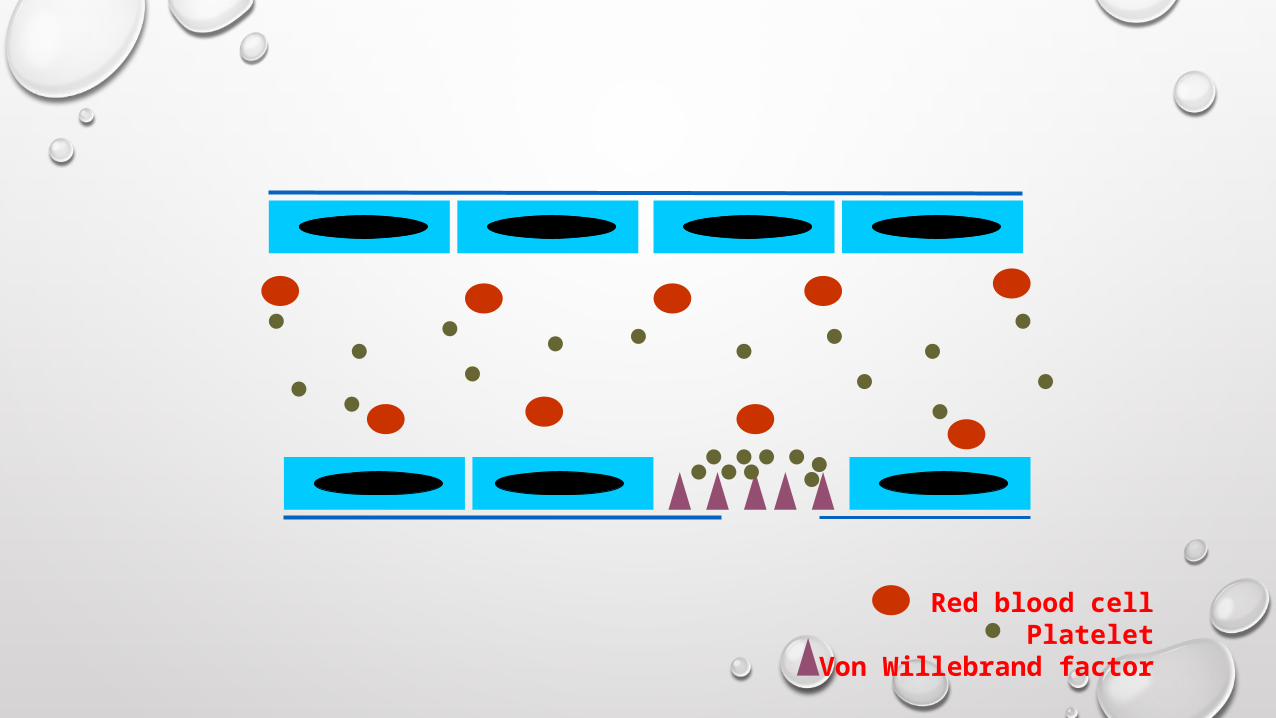
Red blood cellPlatelet
Von Willebrand factor
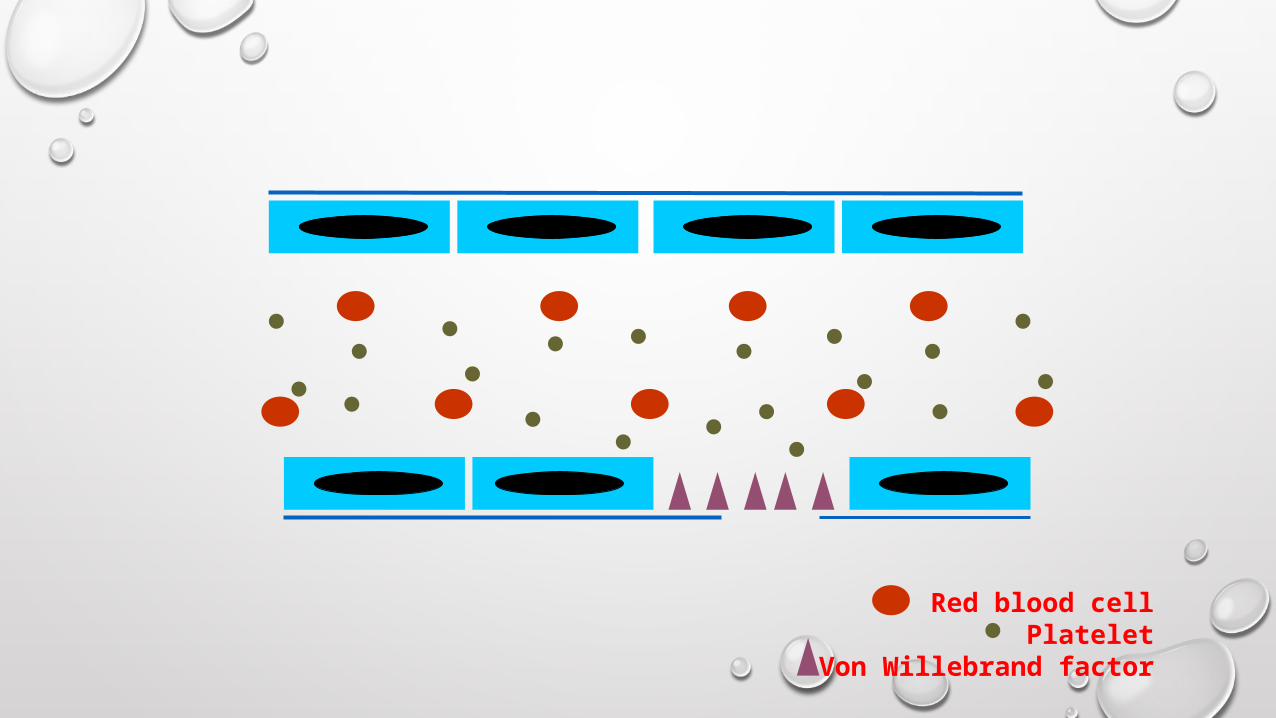
Red blood cellPlatelet
Von Willebrand factor
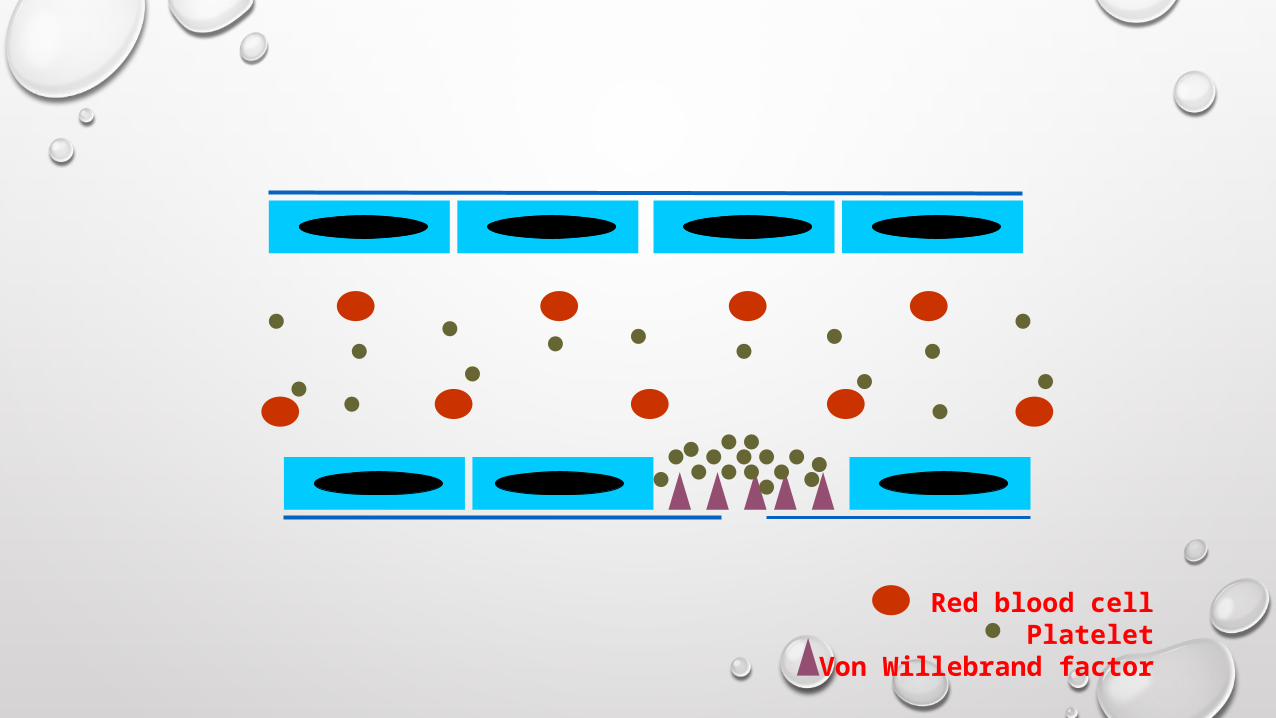
Red blood cellPlatelet
Von Willebrand factor
Red blood cellPlatelet
Von Willebrand factor
Red blood cellPlatelet
Von Willebrand factor
Red blood cellPlatelet
Von Willebrand factor
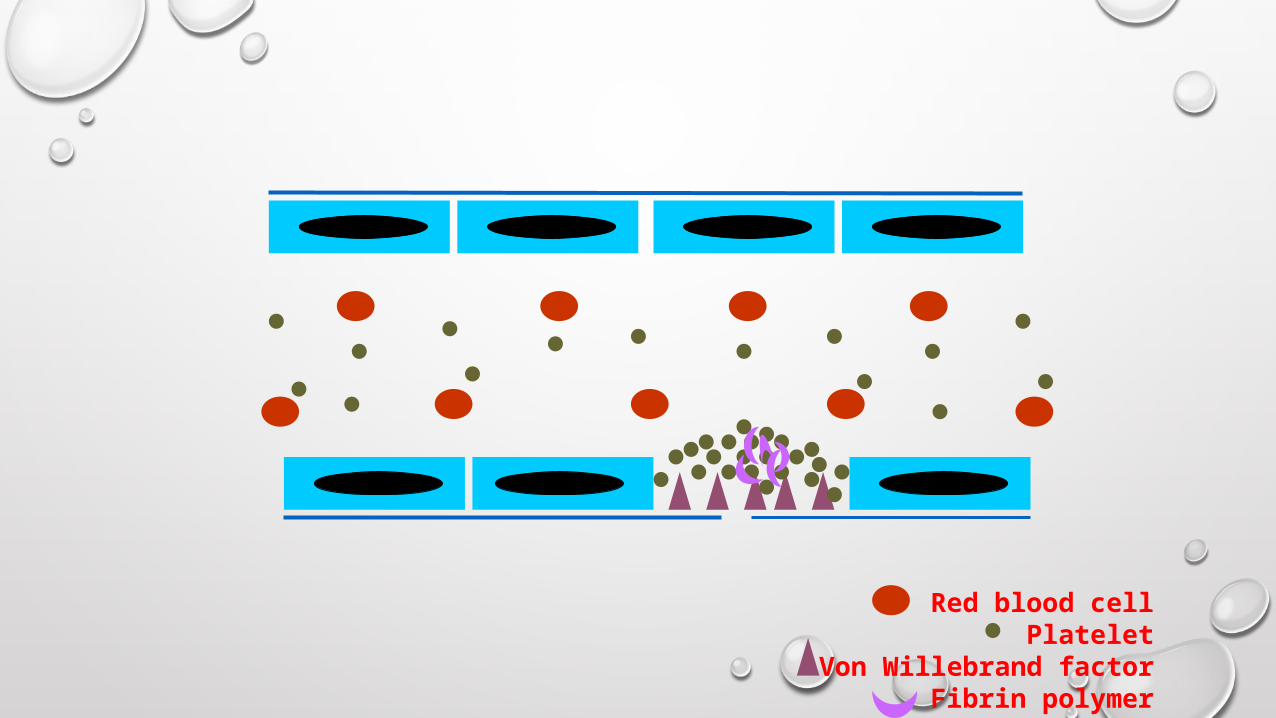
Red blood cellPlatelet
Von Willebrand factorFibrin polymer
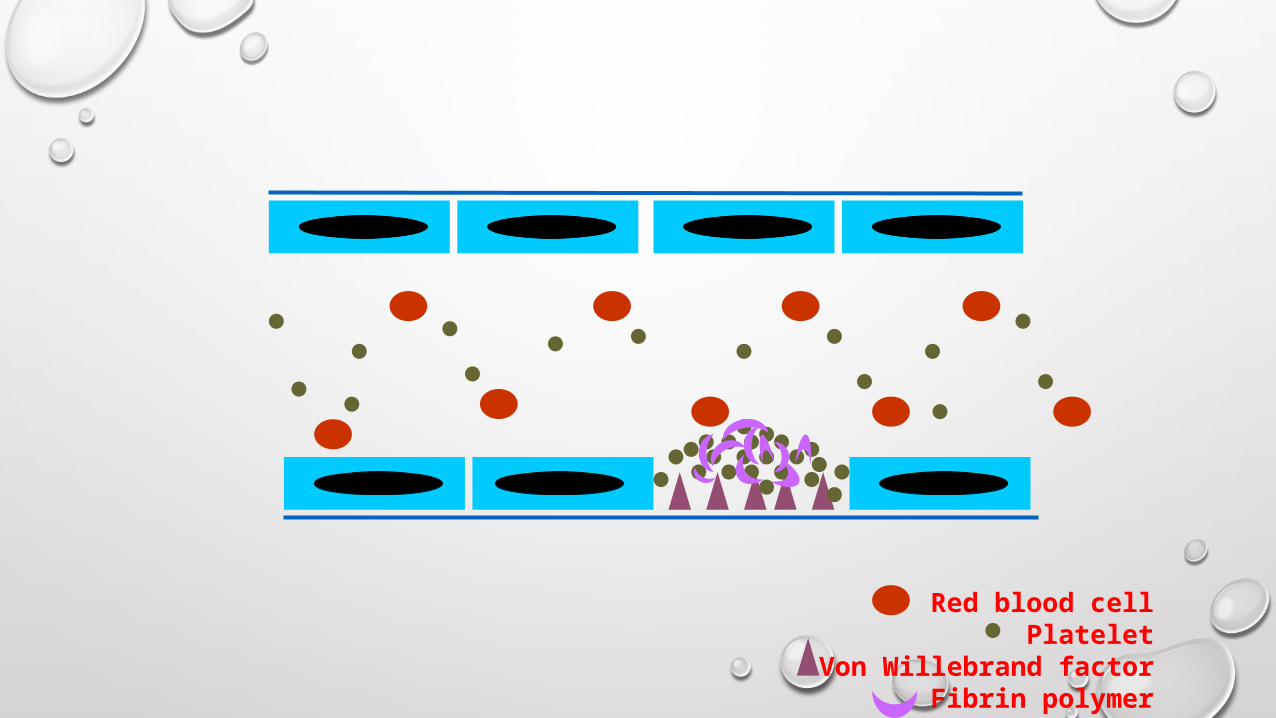
Red blood cellPlatelet
Von Willebrand factorFibrin polymer
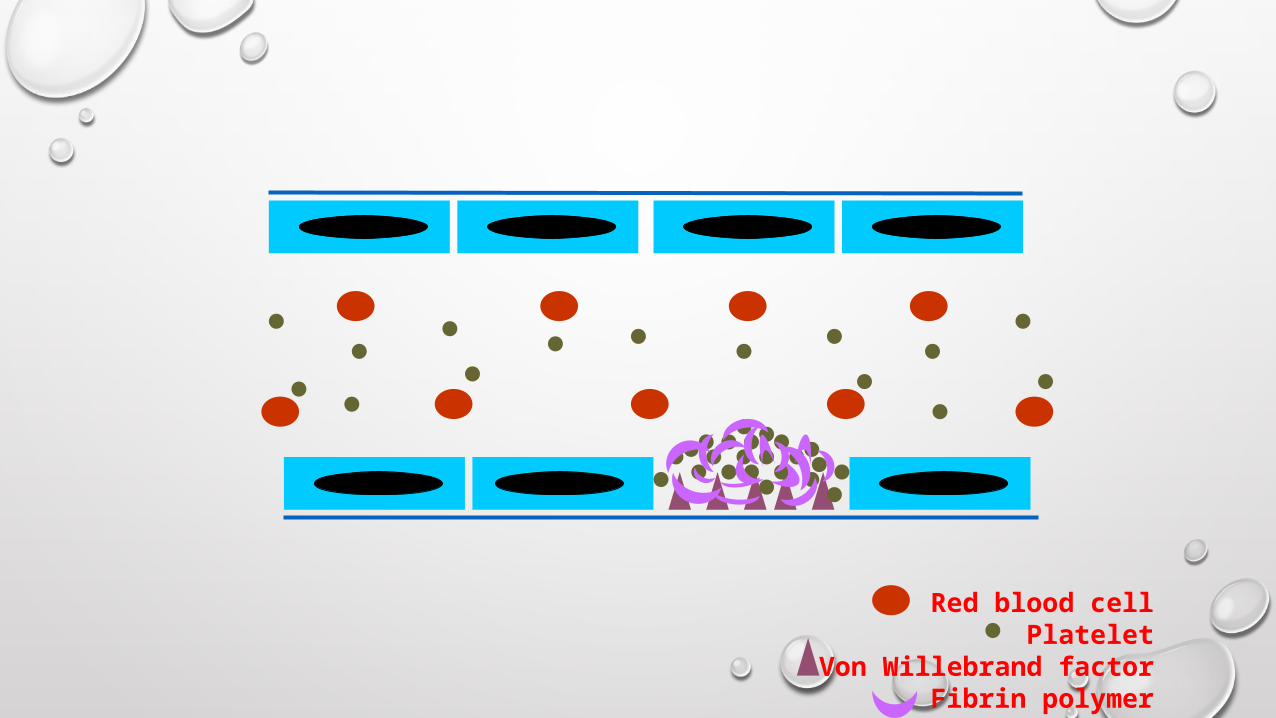
Red blood cellPlatelet
Von Willebrand factorFibrin polymer
EVALUATION OF THE PATIENT•HISTORY
•PHYSICAL EXAMINATION
•LABORATORY EVALUATION
History taking
Identify if the bleeding problem is due toLocal vs. Systemic defect
Location: single vs. Multiple sitesSeverity: spontaneous? Appropriate to trauma?
Hereditary vs. Acquired disorderOnsetFamily historyUnderlying diseaseMedication
Primary vs. Secondary hemostatic disoder
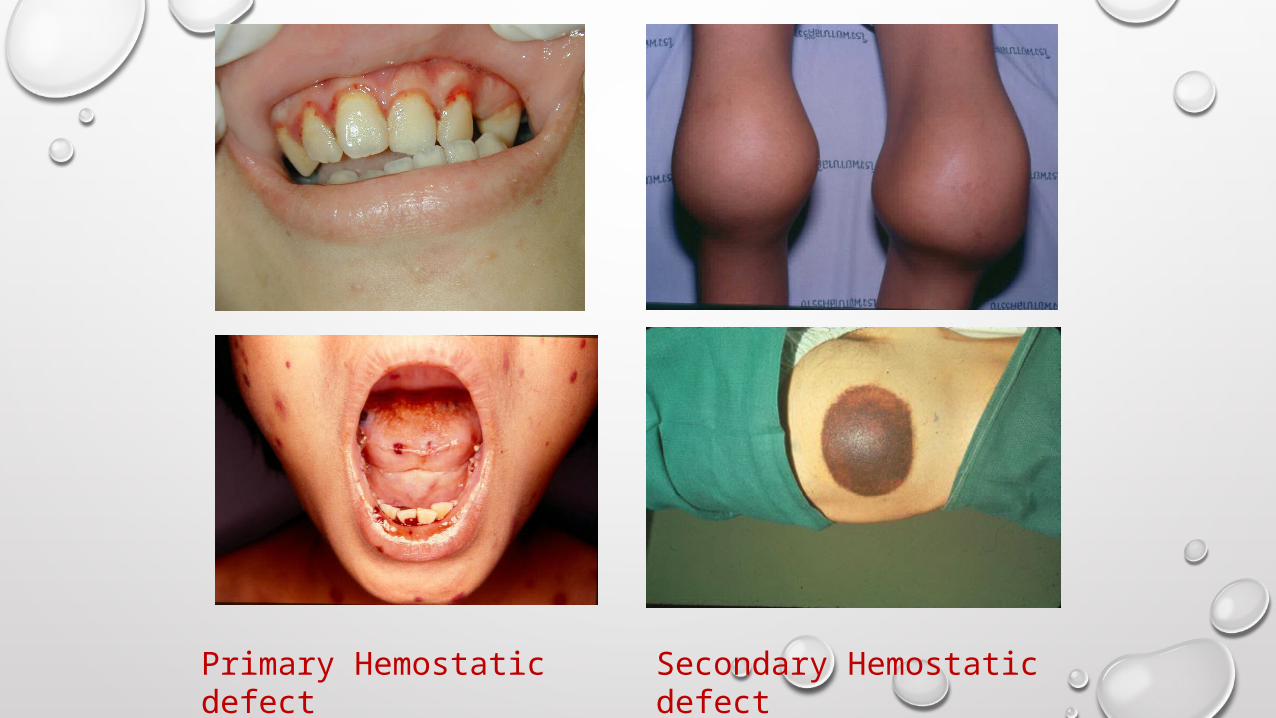
Primary Hemostatic defect
Secondary Hemostatic defect
PHYSICAL EXAMINATION• Current hemorrhage
• Nature and extent
• Intercurrent illnesses
• Liver disease
• Petechiae/ecchymoses
LABORATORY ASSESSMENT• GUIDED BY HISTORY
• SCREENING TESTS
• PT
• APTT
• PLATELET COUNT
• FIBRINOGEN
• THROMBIN TIME
ASSESSMENT OF PRIMARY HEMOSTASISPLATELET
COMPLETE BLOOD COUNT (CBC)BLEEDING TIME/ PFA-100PLATELET AGGREGATION STUDY
BLOOD VESSELBLEEDING TIME
VON WILLEBRAND FACTOR (VWF)BLEEDING TIMEVWF ANTIGEN, VWF: RCO, VWF MULTIMER, FVIII
COMPLETE BLOOD COUNT (CBC)
PLATELET NUMBER
NORMAL PLATELET COUNT: 150,000 –400,000/UL
> 100,000/UL BLEEDING UNLIKELY
< 20,000/UL ↑ RISK FOR SPONTANEOUS
BLEEDING
MUST EXCLUDE PSEUDOTHROMBOCYTOPENIA
ASSESS FOR PLATELET MORPHOLOGY
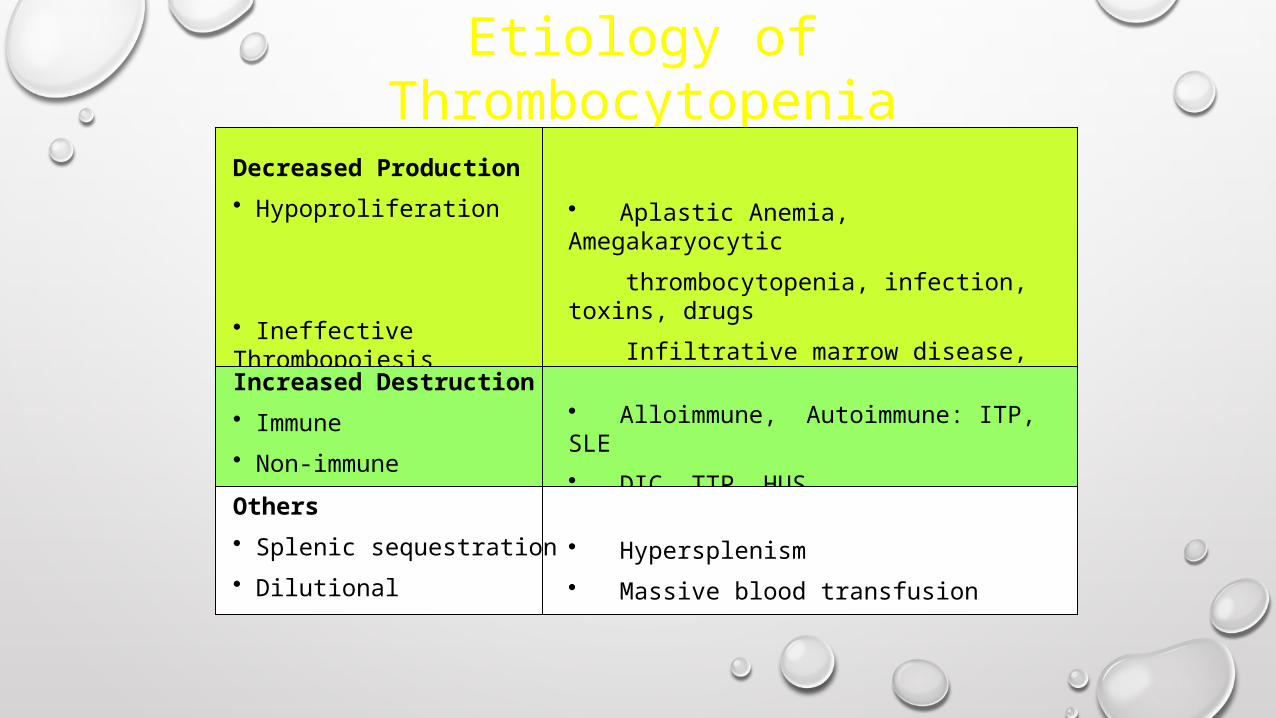
Etiology of Thrombocytopenia
Decreased Production
• Hypoproliferation
• Ineffective Thrombopoiesis
• Aplastic Anemia, Amegakaryocytic
thrombocytopenia, infection, toxins, drugs
Infiltrative marrow disease, TAR
• Megaloblastic anemiaIncreased Destruction
• Immune
• Non-immune
• Alloimmune, Autoimmune: ITP, SLE
• DIC, TTP, HUS
Others
• Splenic sequestration
• Dilutional
• Hypersplenism
• Massive blood transfusion
BLEEDING TIME
BLEEDING TIME: INTERPRETATION
Normal value* : 1-9 minProlonged bleeding time:
Thrombocytopenia/ anemia (hct < 20%)Hereditary platelet dysfunctionVon willebrand diseaseSevere hypofibrinogenemiaBlood vessels disordersUremiaMyeloproliferative disordersMedication: aspirin, nsaids,other antiplatelet drugs
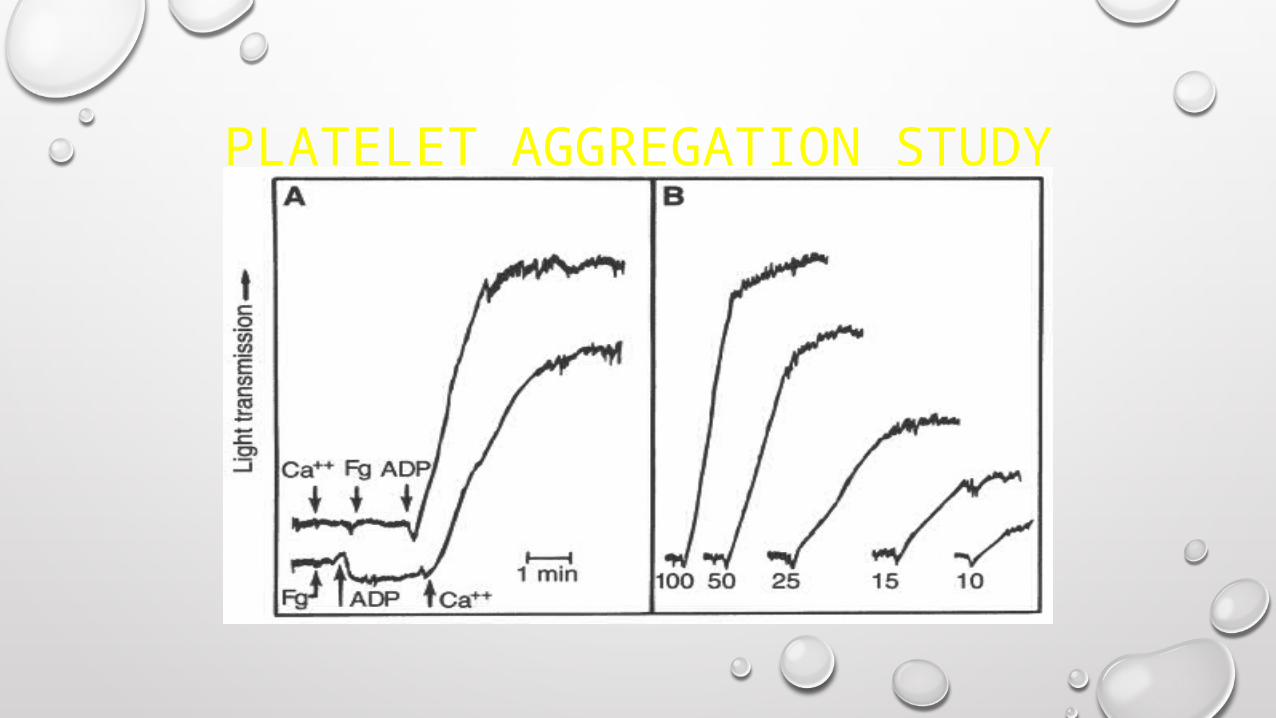
PLATELET AGGREGATION STUDY
ASSESSMENT OF SECONDARY HEMOSTASIS SCREENING TESTS:
PT
APTT
MIXING STUDY
ADDITIONAL TESTSFIBRINOGEN
THROMBIN TIME
REPTILASE TIME
COAGULATION FACTOR ASSAYS
D-DIMER
FIBRIN DEGRADATION PRODUCT
EUGLOBULIN LYSIS TIME
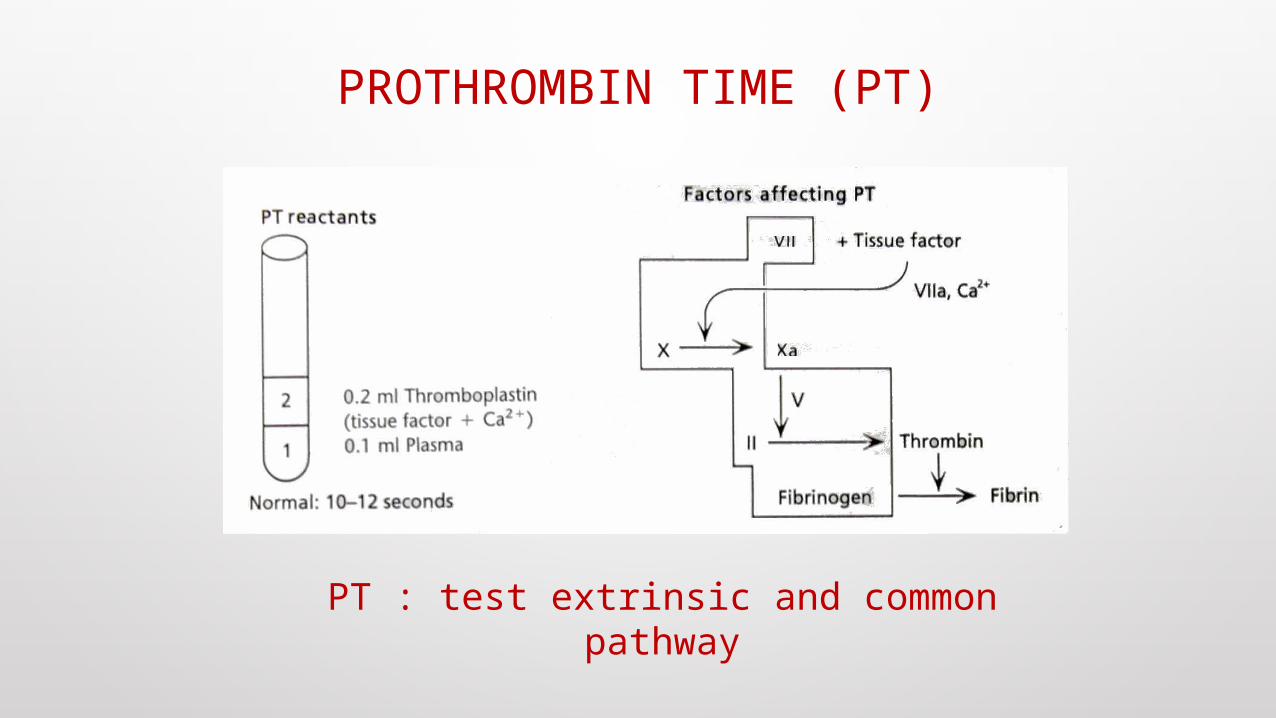
PROTHROMBIN TIME (PT)
PT : test extrinsic and common pathway
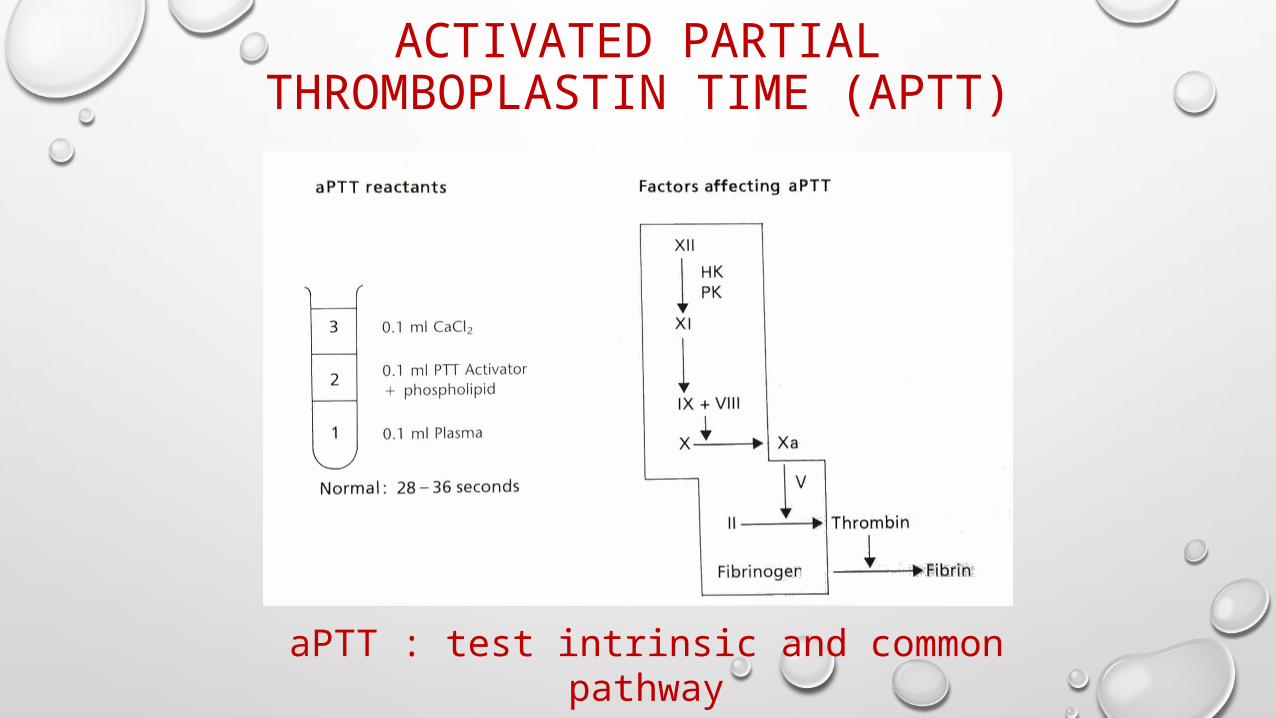
ACTIVATED PARTIAL THROMBOPLASTIN TIME (APTT)
aPTT : test intrinsic and common pathway
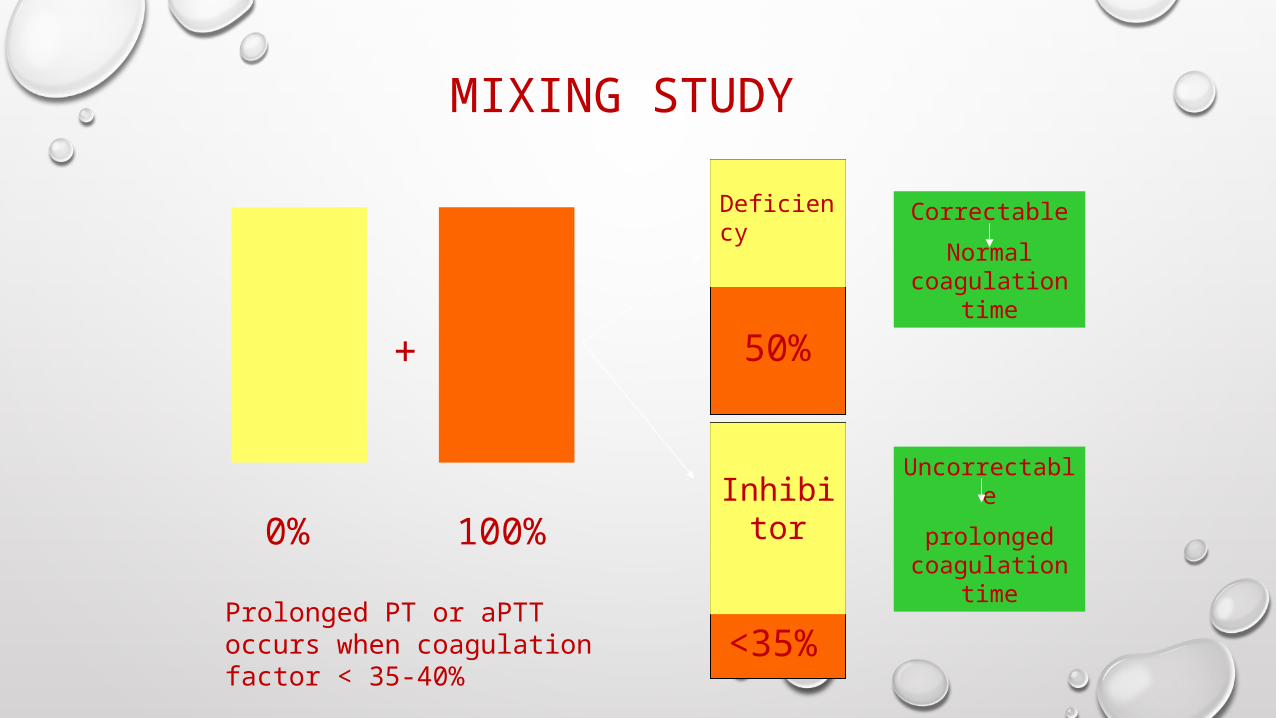
MIXING STUDY
+
0% 100%
50%
<35%
Correctable
Normal coagulation
time
Uncorrectable
prolonged coagulation
time
Deficiency
Inhibitor
Prolonged PT or aPTT occurs when coagulation factor < 35-40%
INTERPRETATION OF ABNORMAL COAGULOGRAM
ISOLATED PROLONGED PT
ISOLATED PROLONAGED APTT
PROLONGED PT AND APTT

Isolated prolonged PT
Mixing study
Correctable Uncorrectable Deficiency Inhibitor
Hereditary: FVII FVII (rare) Lupus anticoagulant Acquired: Early liver impairment
Vitamin K antagonist Vitamin K deficiency
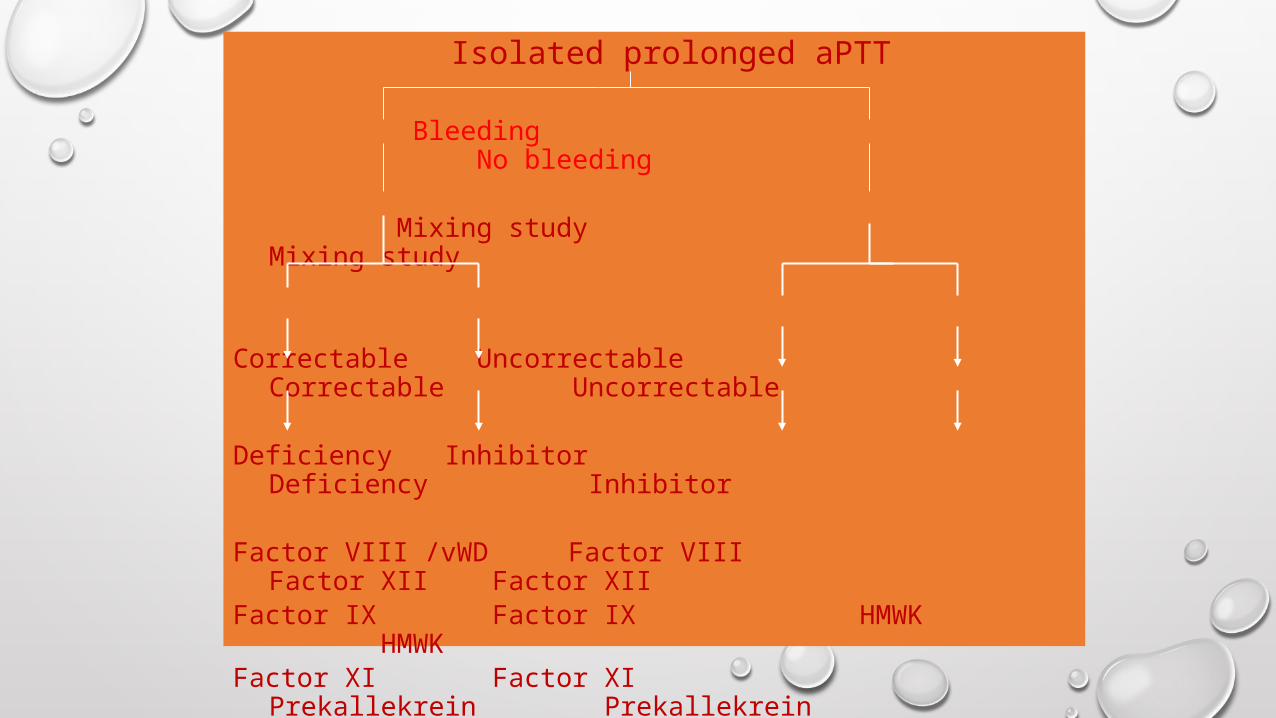
Isolated prolonged aPTT
Bleeding No bleeding
Mixing study Mixing study
Correctable Uncorrectable Correctable Uncorrectable
Deficiency Inhibitor Deficiency Inhibitor
Factor VIII /vWD Factor VIII Factor XII Factor XIIFactor IX Factor IX HMWK HMWKFactor XI Factor XI Prekallekrein Prekallekrein Heparin Lupus anticoagulant

Acquired FVIII inhibitor
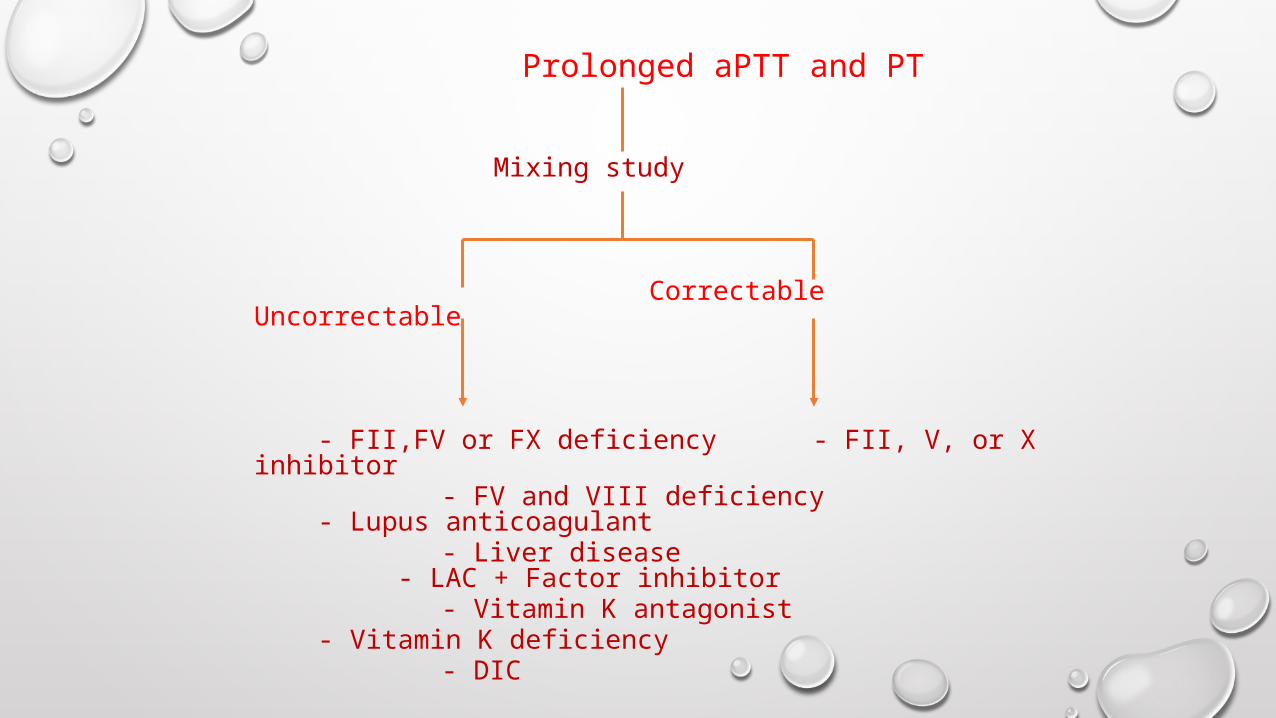
Prolonged aPTT and PT
Mixing study
Correctable Uncorrectable
- FII,FV or FX deficiency - FII, V, or X inhibitor - FV and VIII deficiency - Lupus anticoagulant - Liver disease - LAC + Factor inhibitor - Vitamin K antagonist - Vitamin K deficiency - DIC
SUMMARY
• HISTORY & PHYSICAL EXAMINATION
• LABORATORY TESTS
• SCREENING TESTS
• SPECIFIC DIAGNOSTIC TESTS
• DIAGNOSIS-SPECIFIC THERAPY
• FACTOR REPLACEMENT
• DRUGS
REFFERENCES
• KUMAR
• CECIL
• WEBSITE
