biomedical sciences - mucosal immunology...biomedical sciences 23 february 2015 celiac disease and...
TRANSCRIPT

Biomedical Sciences
23 February 2015
Celiac Disease and Malabsorption
Christoph MuellerInstitute of Pathology

Malabsorption
Definition Malabsorption represents the pathological interference with the normal physiological sequence of digestion (intraluminal process), absorption (mucosal process) and transport (postmucosal events) of nutrients.
Intestinal malabsorption due to:
•Mucosal damage (Enteropathy) e.g. celiac disease
•Acquired or congenital reduction in absorptive surface
•Defects of specific hydrolysing enzymes
•Defects of ion transport
•Pancreatic insufficiency
•Impaired entero-hepatic circulation
Celiac disease(Gluten-induced Enteropathy)
• Incidence: highly variable: Ireland, Scandinavia: 1 in 300; in most other European countries: 1 in 3000 ; Female : male: 1.3 : 1.
• Sites involved: Small intestinal mucosal villi, particularly in the distal duodenum and proximal jejunum.
• Age. Most are diagnosed in childhood after first feedings of cereals, a subgroup of patients develops disease only in adulthood. Complications: Malnutrition almost immediately, later, malignant lymphoma of the small intestine may develop.
• Prognosis: there is almost always a good response to gluten – free diet.

Tommasini et al., 2011
“Evolution” of our understanding of the etiopathogenesis of celiac disease

Celiac Disease Histopathology
L. Sollid Nature Rev Immunol 2: 647; 2002

Celiac Disease Histopathology

MN Marsh Gastroenterology 102: 330;1992
Immunopathogenesis of Celiac Disease

Modellvorstellung der Interaktionen zwischen Protein-Prozessierung und spezifischen Immunreaktionen im Darm bei Zoeliakie. Gluten wird aus der Nahrung durch Verdauungsenzyme (z.B. Prolin-Endopeptidasen) in stabile Peptide gespalten (mit Prolin-reichen PQPQLPY Motiven) Die Peptide werden absorbiert und in die Lamina propria transportiert, wo sie durch eine Transglutaminase (tTG2, tissue transglutaminase-2) modifiziert werden und in Assoziation mit HLA-DQ2 oder -DQ8 Molekülen auf Antigen-praesentierenden Zellen an CD4 T Zellen praesentiert werden. Diese aktivierten T Zellen produzieren Interferonγ und weitere entzündungsfördernde Zytokine, welche die charakteristischen Veränderungen (z.B. Villus - Atrophie, Kryptenhyperplasie) vermitteln (A. Mowat, Lancet 361:1290; 2003)

A vast majority of celiac patients express the HLA-DQ2 heterodimer encoded by the DQA1*05 and DQB1*02 genes. These two genes are carried either in cis on the DR3-DQ2 haplotype, or in trans in individuals who are DR5-DQ7 and DR7-DQ2 heterozygous. Most DQ2-negative patients express DQ8 encoded on the DR4-DQ8 haplotype. Qiao, Sollid Blumberg; Curr Opinion Immunol 2009
HLA association in celiac disease

Peptide binding signatures of DQ2 and DQ8 molecules
The DQ2-restricted γ-III epitope and the DQ8-restricted γ-I epitope recognized by lesion derived T cells of CeD patients share the same 9 amino acid core sequence. This sequence contains three glutamate residues formed by TG2-mediated deamidation in positions P1, P4 and P9. DQ2 prefers negatively charged glutamate residue in P4 (shaded) whereas DQ8 prefers glutamate in P1 and P9 (shaded). Qiao, Sollid Blumberg; Curr Opinion Immunol 2009

The coeliac small-intestine lesionThe coeliac small-intestine lesionNature Rev Immunol 2: 647; 2002
TG
HLADQ
CD3
Epithelium

Gluten peptides that are highly resistant to intestinal proteases reach the lamina propria, via either epithelial transcytosis or an increased epithelial tight junctional permeability. Deamidation of gluten peptides by TG2 creates potent immunostimulatory epitopes that are presented via HLA-DQ2 or HLA-DQ8 on antigen-presenting cells. Subsequently, CD4+ T cells are activated, secreting mainly Th1 cytokines such as IFN-γ, which induces the release and activation of MMPs by myofibroblasts, finally resulting in mucosal remodeling and villus atrophy. Additionally, Th2 cytokines are produced driving the production of (auto-)antibodies to gluten and TG2. Other cytokines such as IL-18, IFN-α, or IL-21 seem to play a role in polarizing and maintaining the Th1 response. The scheme is simplified. It does not show that T cells circulate to mesenteric lymph nodes where they encounter and are primed by antigen-presenting cells (mainly dendritic cells) and from where they home back to the lamina propria, a process that is driven by the lymphocyte homing receptors CCR9 and integrin α4β7.
Pathogenesis of celiac disease.
Gastroenterology 137: 1912-1933; 2009

Innate immune responses in celiac disease. Upon stimulation with gliadin peptide p31-49 (and other peptides), epithelial cells, macrophages, and dendritic cells secrete IL-15, which in turn up-regulates both the NKG2D receptor on IELs and its epithelial ligand MICA. The thus stimulated cytotoxic lymphocytes induce increased epithelial apoptosis and permeability. Furthermore, the NKG2C receptor on a subset of natural killer–like IELs is stimulated by its epithelial ligand HLA-E on epithelial cells, resulting in their proliferation and cytotoxicity, whereas stimulation of γδ+ CD8+ IELs bearing the NKG2A receptor via HLA-E induces TGF-β secretion and therefore a regulatory phenotype. Gliadin peptides can also directly elicit innate immune responses in macrophages and dendritic cells via pattern recognition receptors such as Toll-like receptor 4 or other MyD88-dependent pathways. This drives maturation of these cells and secretion of inflammatory cytokines such as IL-1β, IL-8, TNFα, and MCP-1, which can potentiate the adaptive immune response to gluten.
Innate immune responses in celiac disease
Gastroenterology 137: 1912-1933; 2009

The density of CD3+ T cells (A) and TCRγδ T cells (B) IELs in patients with confirmed CD, in patients with celiac suspicion, but normal villous atrophy, and in nonceliac controls
Järvinen Am J Gastroenterol 98(6):1332-7; 2003

Buri et al., J Pathol. 2005; 206:178-85
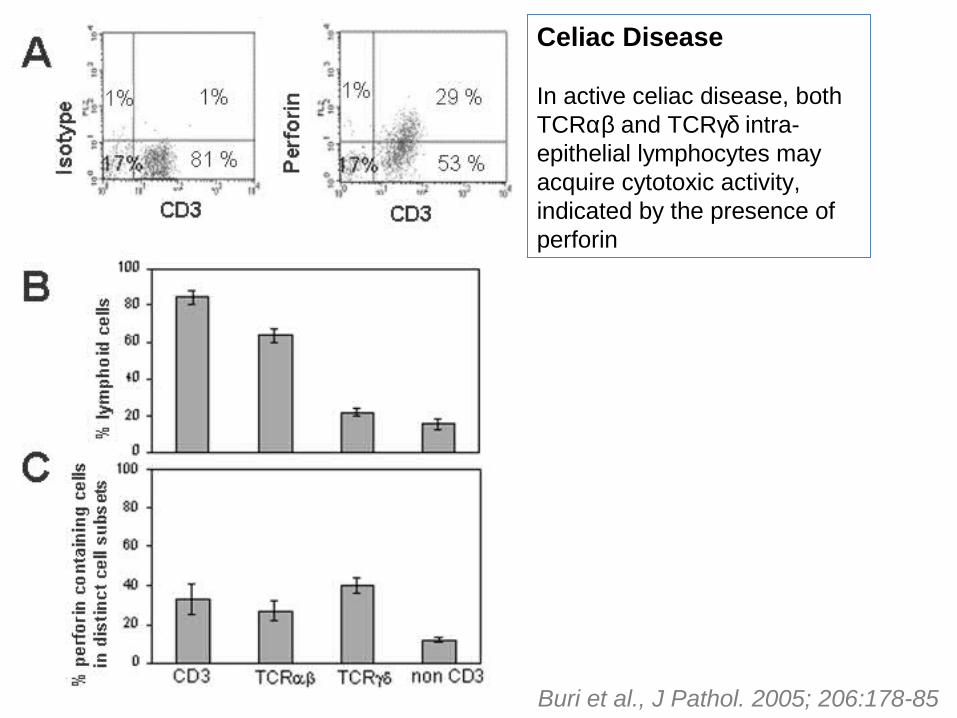
Celiac Disease
In active celiac disease, both TCRαβ and TCRγδ intra-epithelial lymphocytes may acquire cytotoxic activity, indicated by the presence of perforin
Buri et al., J Pathol. 2005; 206:178-85
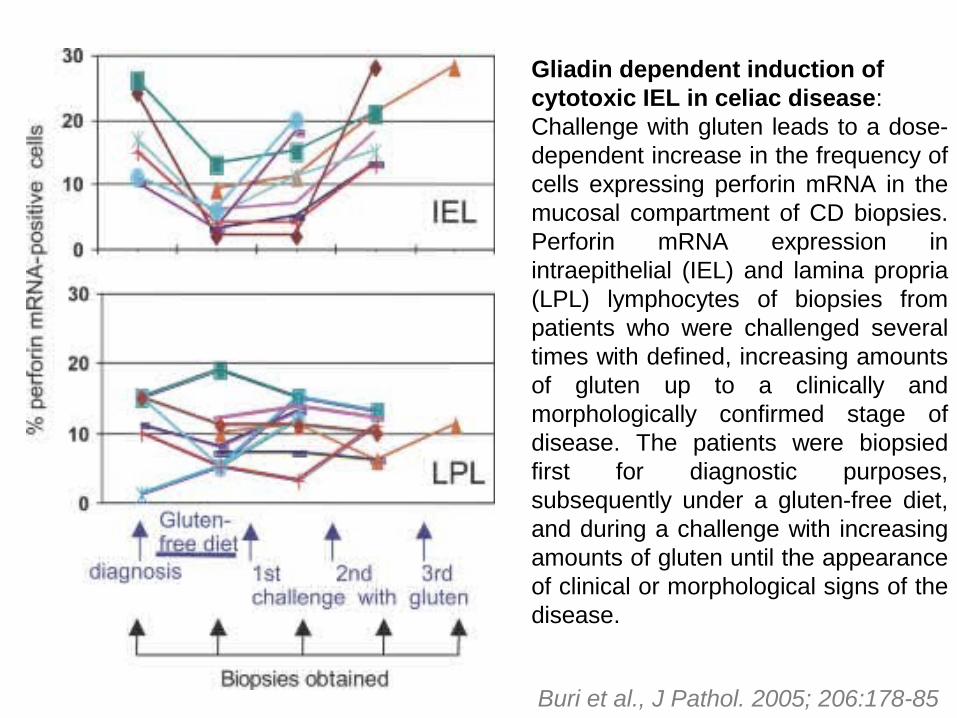
Gliadin dependent induction ofcytotoxic IEL in celiac disease:Challenge with gluten leads to a dose-dependent increase in the frequency of cells expressing perforin mRNA in the mucosal compartment of CD biopsies. Perforin mRNA expression in intraepithelial (IEL) and lamina propria (LPL) lymphocytes of biopsies from patients who were challenged several times with defined, increasing amounts of gluten up to a clinically and morphologically confirmed stage of disease. The patients were biopsied first for diagnostic purposes, subsequently under a gluten-free diet, and during a challenge with increasing amounts of gluten until the appearance of clinical or morphological signs of the disease.
Buri et al., J Pathol. 2005; 206:178-85

Novel therapeutic approaches. Use of ancestral and/or modified wheat strains with lower immunogenicity. Intraluminal therapies that either bind or degrade ingested gluten peptides in the intestine (glutenases, gluten binders, neutralizing antibodies). Blocking the ZOT receptor with the octapeptide AT-1001 to decrease intestinal permeability is another option. Furthermore, because the deamidation of gluten peptides by TG2 and the subsequent presentation by HLA-DQ2/8 initiates the adaptive immune responses, TG2 inhibitors and DQ2 blocking peptides seem to be an attractive possibility to prevent inflammation. Another promising alternative, especially for patients with refractory celiac disease, is directly targeting the immune cells either by lymphocyte blocking (anti–IL-15, anti-CCR9, anti-α4β7) or tolerance induction.
Celiac Disease: potential novel therapies
Gastroenterology 137: 1912-1933; 2009

n Celiac disease:several additional susceptibility factors contribute to the patho-genesis of celiac disease

Mutationen, die zu einer erhöhten Suszeptibilität für M. Crohn und Kolitis ulzerosa führen, können auch für weitere Erkrankungen prädisponieren
Lees C W et al. Gut 2011;60:1739-1753
Schwarz: Mutationen bei Patienten mit M. Crohn und Kolitis ulzerosa
Rot: Mutationen nur bei Patienten mit M. Crohn Blau: Mutationen bei Patienten mit Kolitis ulzerosa

Current Concept of the Immunopathogenesis of Celiac Disease in Susceptible Patients
Annu Rev Immunol 2010

Celiac disease (summary)(Gluten-induced Enteropathy)
• Incidence: highly variable: Ireland, Scandinavia: 1 in 300; in most other European countries: 1 in 3000 ; Female : male: 1.3 : 1.
• Sites involved: Small intestinal mucosal villi, particularly in the distal duodenum and proximal jejunum.
• Age. Most are diagnosed in childhood after first feedings of cereals, a subgroup of patients develops disease only in adulthood.
• Histopathology: Flat mucosal surface with blunting or total loss of villi upon ingestion of gluten containing cereals; flattening and basophilia of absorptive cells, increased frequencies of intraepithelial lymphocytes, and in the intestinal lamina propria.
• Pathogenesis. Increased incidence in patients with HLA-DQ2 or DQ8, tissue transglutaminase - mediated deamidation of gliadin leads to the generation of neoepitopes that are recognized by CD4 T cells.
• Increased presence and enhanced cytotoxic activity of intraepithelial lymphocytes.
• Complications: Malnutrition almost immediately, later, malignant lymphoma of the small intestine may develop.
• Prognosis: there is almost always a good response to gluten – free diet.

Celiac Disease and Malabsorption:Key aspects
• Definition and causes of malabsortion
• Celiac disease: triggers and genetics• Celiac disease: histopathology as a rational for observer
malabsorption• Celiac disease: main imunopathological mechanisms
leading to villous atrophy – potential for the development of therapeutic interventions
• Genetics of celiac disease: (partial) overlap with other immunopathologies