biomed 370: the neurobiology of mood disorders march 3, 2005 lawrence h. price, m.d. professor of...
TRANSCRIPT

BIOMED 370: The Neurobiology BIOMED 370: The Neurobiology of Mood Disorders of Mood Disorders
March 3, 2005March 3, 2005
Lawrence H. Price, M.D.Lawrence H. Price, M.D.Professor of Psychiatry and Human BehaviorProfessor of Psychiatry and Human Behavior
Brown University School of MedicineBrown University School of Medicine
Clinical Director and Director of ResearchClinical Director and Director of Research
Butler HospitalButler Hospital
345 Blackstone Blvd345 Blackstone Blvd
Providence, RI 02906Providence, RI 02906
EmotionEmotion A complex feeling state, with A complex feeling state, with psychological, somatic, and psychological, somatic, and behavioral components, that is behavioral components, that is related to mood and affect.related to mood and affect.
MoodMood The subjective experience of The subjective experience of feeling or emotion as described by feeling or emotion as described by the individual; tends to be the individual; tends to be pervasive and sustained.pervasive and sustained.
AffectAffect Feeling or emotion as Feeling or emotion as expressed by expressed by the individual and the individual and observed by others; tends to be observed by others; tends to be variable even over short time variable even over short time intervals.intervals.
DEFINITIONSDEFINITIONS
NEUROANATOMY AND MOODNEUROANATOMY AND MOOD
The maintenance of a normal mood The maintenance of a normal mood
state (euthymia) depends on the state (euthymia) depends on the
interactions of a widely distributed interactions of a widely distributed
network of cortical-limbic and network of cortical-limbic and
cortical-striatal pathways.cortical-striatal pathways.
THE NEUROBIOLOGY OF EUTHYMIATHE NEUROBIOLOGY OF EUTHYMIA
StructuresStructures •Cingulate cortexCingulate cortex
•HippocampusHippocampus
•AmygdalaAmygdala
•(Hypothalamus)(Hypothalamus)
•(Orbitofrontal cortex)(Orbitofrontal cortex)
•(N. accumbens, septal n.)(N. accumbens, septal n.)
THE LIMBIC SYSTEMTHE LIMBIC SYSTEM

Beatty, The Human Brain, 2001

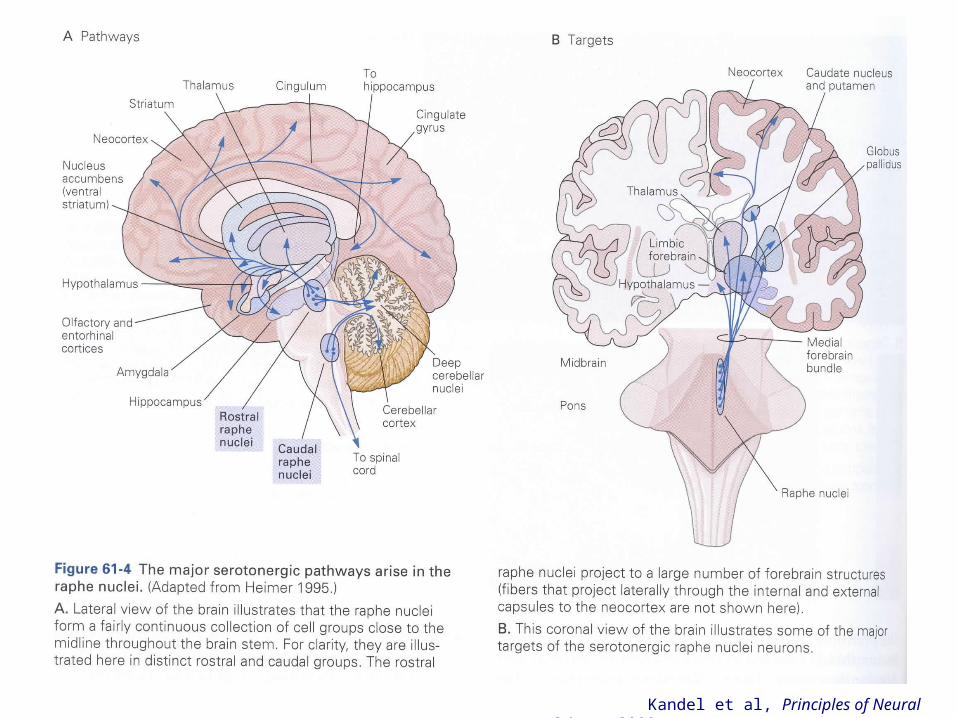
Kandel et al, Principles of Neural Science, 2000

FunctionsFunctions Integration of internal and Integration of internal and external inputs relevant to the external inputs relevant to the coordination of the followingcoordination of the followingneurobehavioral processes: neurobehavioral processes:
•EmotionalEmotional
•CognitiveCognitive
•VegetativeVegetative
•AutonomicAutonomic
•MotorMotor
THE LIMBIC SYSTEMTHE LIMBIC SYSTEM
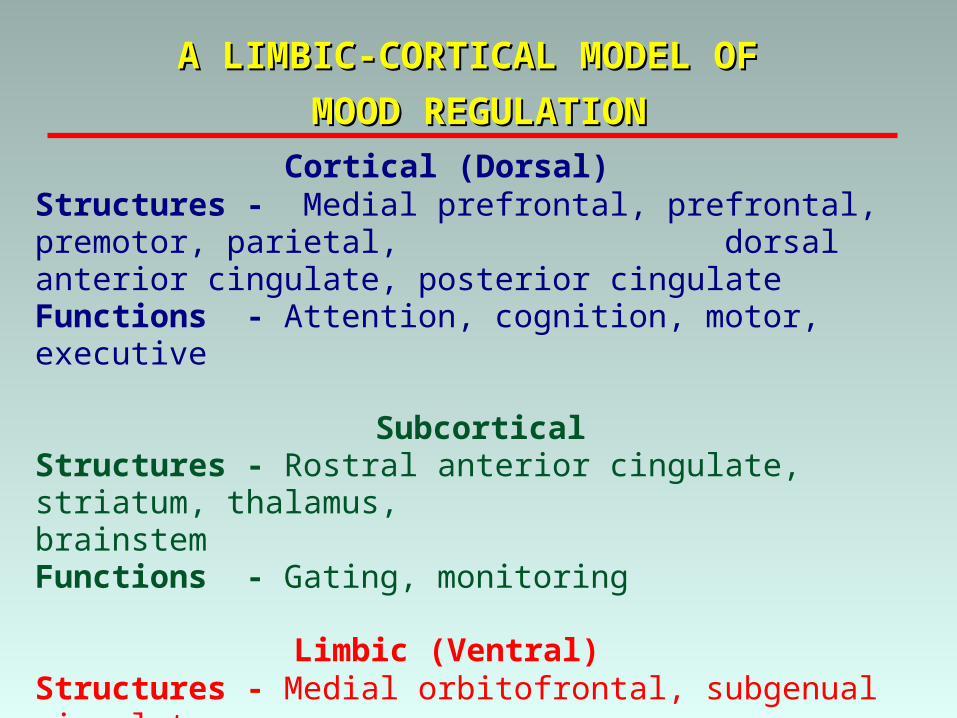
Cortical (Dorsal) Structures - Medial prefrontal, prefrontal, premotor, parietal,
dorsal anterior cingulate, posterior cingulateFunctions - Attention, cognition, motor, executive
SubcorticalStructures - Rostral anterior cingulate, striatum, thalamus,
brainstemFunctions - Gating, monitoring
Limbic (Ventral) Structures - Medial orbitofrontal, subgenual cingulate,
hypothalamus,hippocampus, anterior insula, amygdala, posterior cingulate
Functions - Autonomic, vegetative, somatic
A LIMBIC-CORTICAL MODEL OF A LIMBIC-CORTICAL MODEL OF
MOOD REGULATIONMOOD REGULATION
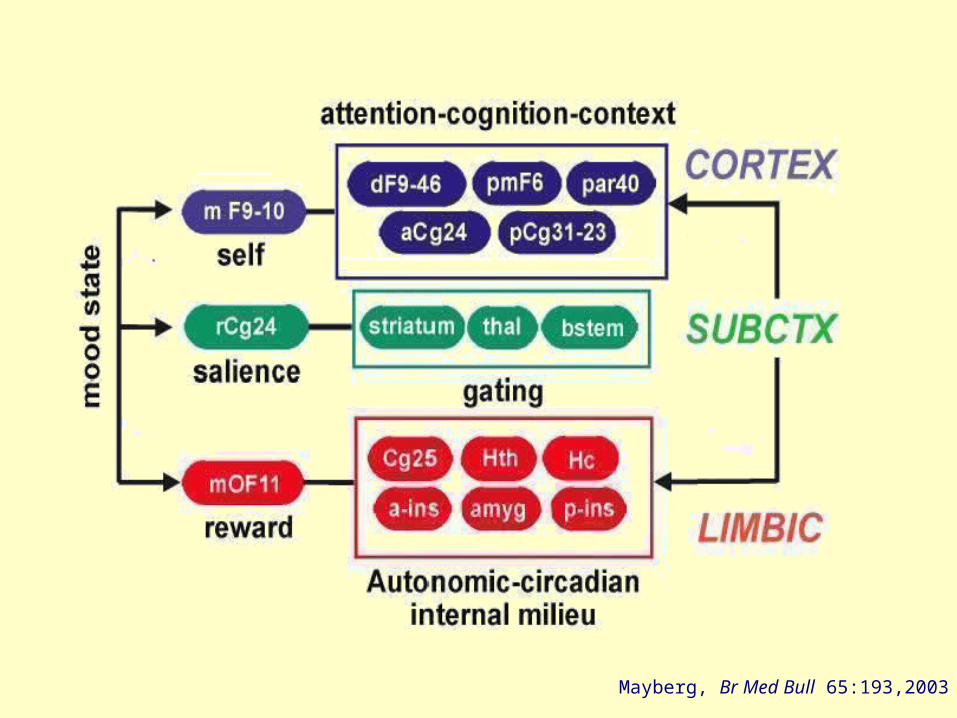
Mayberg, Br Med Bull 65:193,2003

Mood disordersMood disorders • Structural changes Structural changes have been associated with have been associated with
specific brain regions (e.g., hippocampus).specific brain regions (e.g., hippocampus).
• Functional changes Functional changes have been associated with have been associated with specific brain regions.specific brain regions.
• Unclear Unclear whether primary or secondary to whether primary or secondary to pathogenesis.pathogenesis.
Biological treatments for mood disordersBiological treatments for mood disorders• Effective treatments have been associated with Effective treatments have been associated with
functional changesfunctional changes in specific brain regions. in specific brain regions.
• Effects on brain Effects on brain structurestructure notnot yet yet establishedestablished..
NEUROANATOMY AND MOOD DISORDERSNEUROANATOMY AND MOOD DISORDERS

A. At least 5 of the following for A. At least 5 of the following for >>2 weeks2 weeks, including , including (1) depressed mood or (2) loss of interest or pleasure.(1) depressed mood or (2) loss of interest or pleasure.
1. 1. depresseddepressed mood mood 2. decreased interest ( 2. decreased interest (apathyapathy) or pleasure () or pleasure (anhedoniaanhedonia)) 3. weight loss or decreased ( 3. weight loss or decreased (anorexiaanorexia)/increased )/increased
appetiteappetite 4. 4. insomniainsomnia or or hypersomniahypersomnia 5. psychomotor 5. psychomotor agitationagitation or or retardationretardation 6. fatigue ( 6. fatigue (anergiaanergia)) 7. worthlessness or 7. worthlessness or guiltguilt 8. decreased 8. decreased concentrationconcentration or indecisiveness or indecisiveness 9. recurrent thoughts of death or 9. recurrent thoughts of death or suicidalsuicidal ideation/plan/ ideation/plan/
attemptattempt
B. Clinically significant B. Clinically significant distressdistress or social/occupational/ or social/occupational/other other functionalfunctional impairmentimpairment..
DSM-IV MAJOR DEPRESSIONDSM-IV MAJOR DEPRESSION
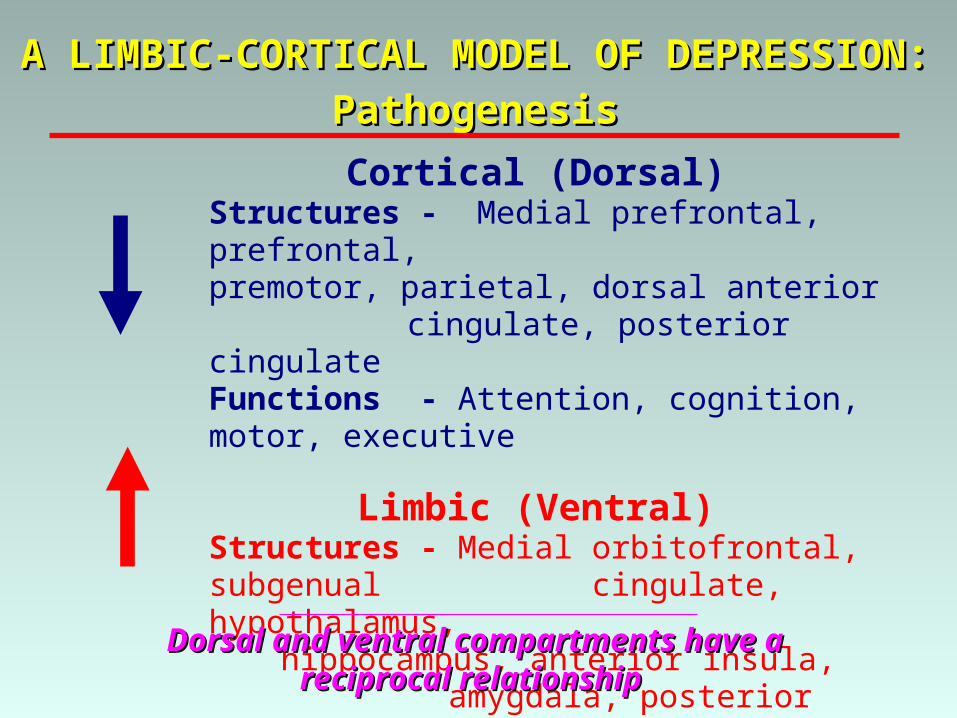
Cortical (Dorsal) Structures - Medial prefrontal, prefrontal,
premotor, parietal, dorsal anterior cingulate, posterior cingulate
Functions - Attention, cognition, motor, executive
Limbic (Ventral) Structures - Medial orbitofrontal, subgenual
cingulate, hypothalamus, hippocampus, anterior insula,
amygdala, posterior cingulateFunctions - Autonomic, vegetative, somatic
A LIMBIC-CORTICAL MODEL OF DEPRESSION:A LIMBIC-CORTICAL MODEL OF DEPRESSION:
PathogenesisPathogenesis
Dorsal and ventral compartments have a Dorsal and ventral compartments have a reciprocal relationshipreciprocal relationship

Cortical (Dorsal) Structures - Medial prefrontal, prefrontal,
premotor, parietal, dorsal anterior cingulate, posterior cingulate
Functions - Attention, cognition, motor, executive
Limbic (Ventral) Structures - Medial orbitofrontal, subgenual
cingulate, hypothalamus, hippocampus, anterior insula, amygdala, posterior cingulate
Functions - Autonomic, vegetative, somatic
A LIMBIC-CORTICAL MODEL OF DEPRESSION:A LIMBIC-CORTICAL MODEL OF DEPRESSION:
TreatmentTreatment
DisinhibitionDisinhibition
InhibitionInhibitionInhibition of ventral activity may Inhibition of ventral activity may
disinhibit dorsal activitydisinhibit dorsal activity
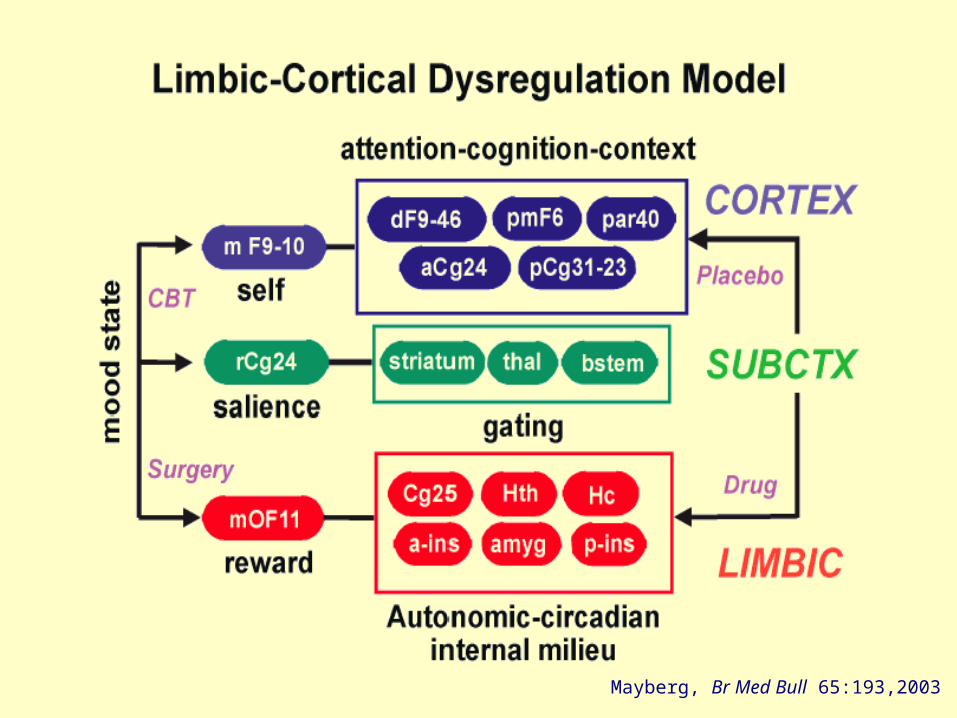
Mayberg, Br Med Bull 65:193,2003

NEUROCHEMISTRY AND NEUROCHEMISTRY AND
MOODMOOD
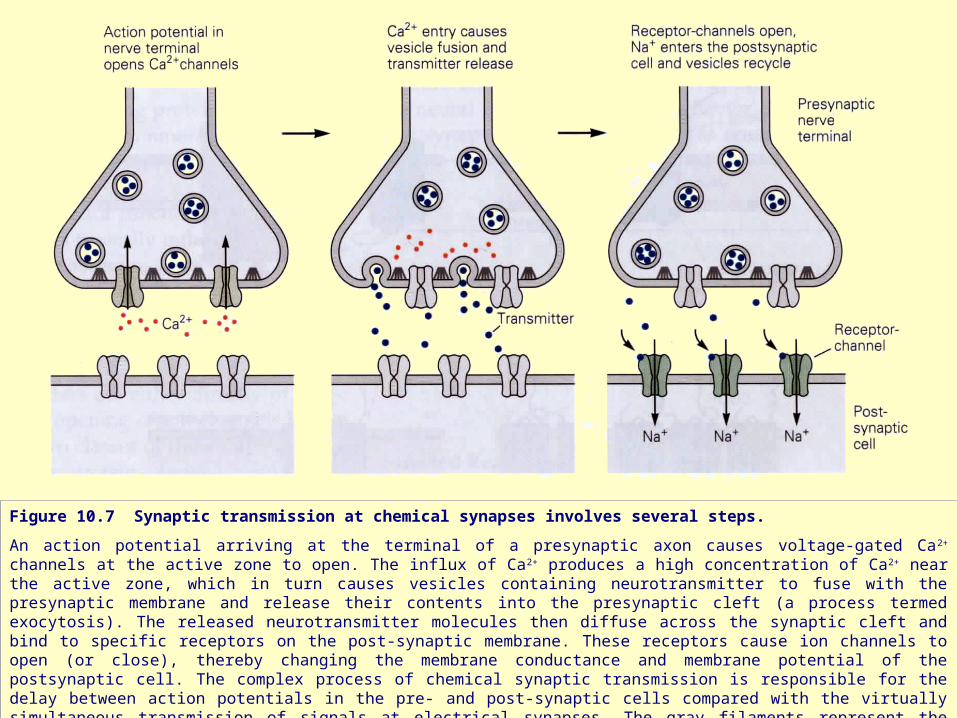
Figure 10.7 Synaptic transmission at chemical synapses involves several steps.
An action potential arriving at the terminal of a presynaptic axon causes voltage-gated Ca 2+ channels at the active zone to open. The influx of Ca2+ produces a high concentration of Ca2+ near the active zone, which in turn causes vesicles containing neurotransmitter to fuse with the presynaptic membrane and release their contents into the presynaptic cleft (a process termed exocytosis). The released neurotransmitter molecules then diffuse across the synaptic cleft and bind to specific receptors on the post-synaptic membrane. These receptors cause ion channels to open (or close), thereby changing the membrane conductance and membrane potential of the postsynaptic cell. The complex process of chemical synaptic transmission is responsible for the delay between action potentials in the pre- and post-synaptic cells compared with the virtually simultaneous transmission of signals at electrical synapses. The gray filaments represent the docking and release sites of the active zone.
Kandel et al, Principles of Neural Science, 2000
Kandel et al, Principles of Neural Science, 2000
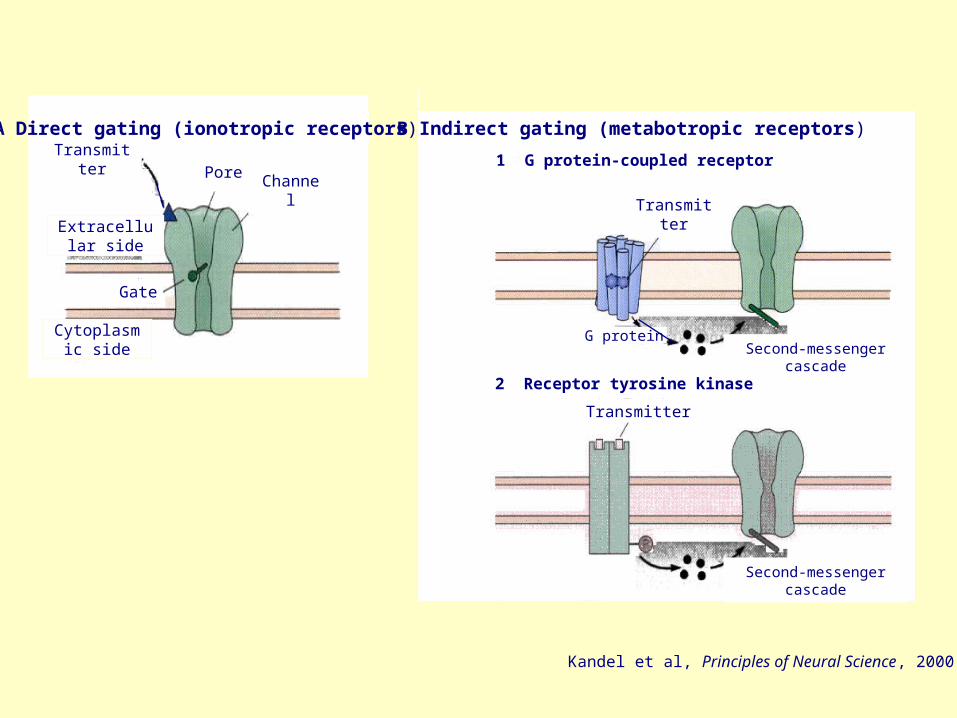
Cytoplasmic side
Transmitter
Transmitter
1 G protein-coupled receptor
2 Receptor tyrosine kinase
Gate
B Indirect gating (metabotropic receptors)A Direct gating (ionotropic receptors)
PoreChannel
Extracellular side
Second-messenger cascade
Second-messenger cascade
Transmitter
G protein
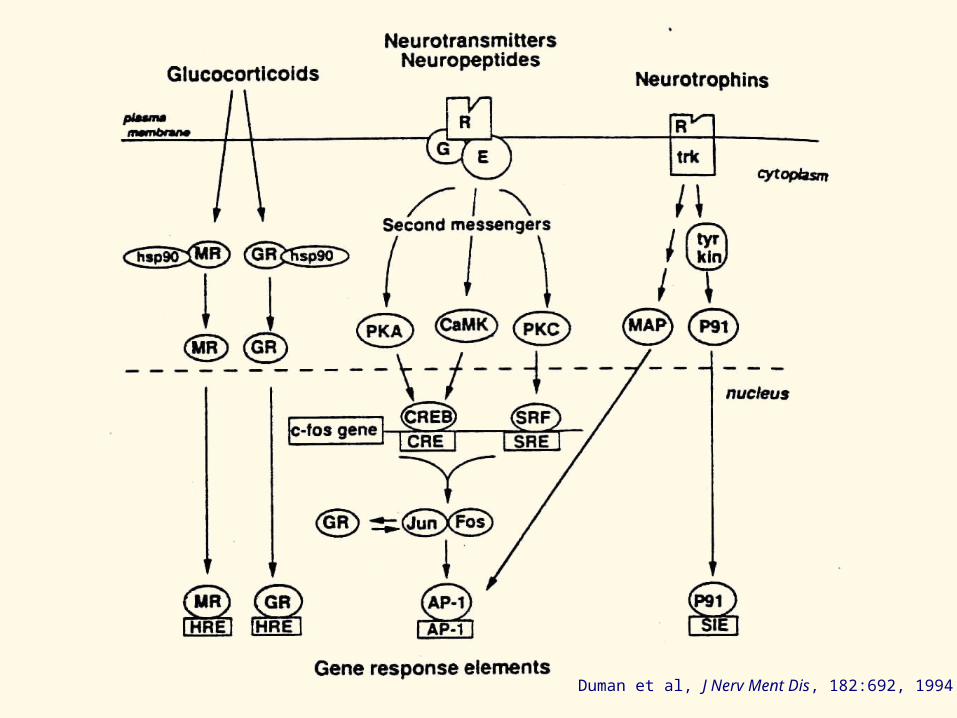
Duman et al, J Nerv Ment Dis, 182:692, 1994
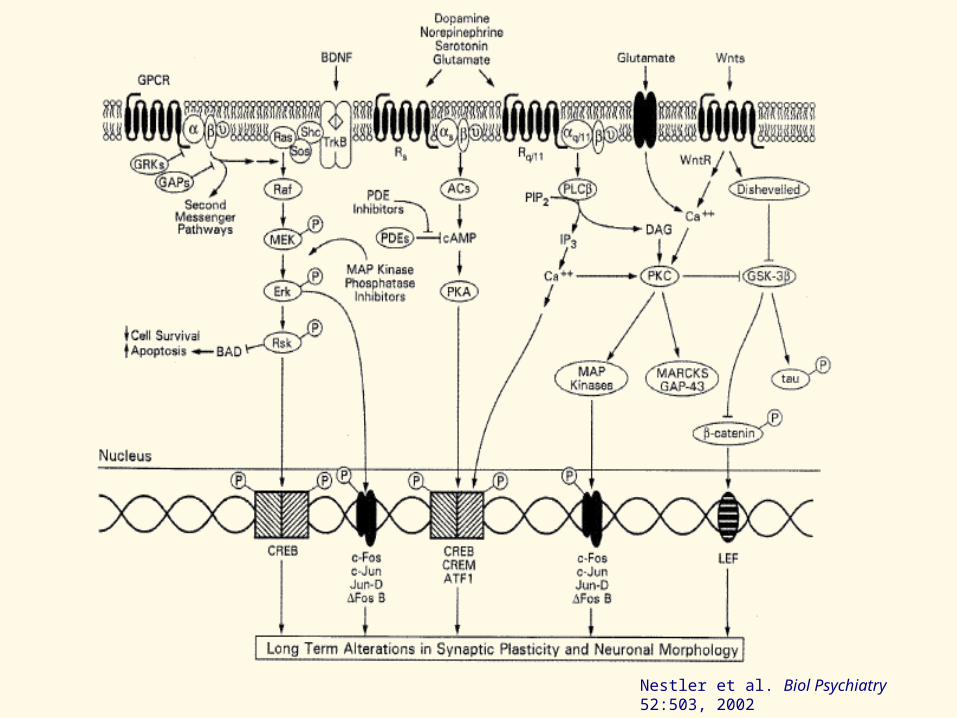
Nestler et al. Biol Psychiatry 52:503, 2002
Mood disordersMood disorders
• HypothesizedHypothesized characteristic dysfunctional characteristic dysfunctional changeschanges in specific neurotransmitter in specific neurotransmitter systems.systems.
• Good evidenceGood evidence for some such changes. for some such changes.
• HypothesizedHypothesized to be to be centralcentral to pathogenesis. to pathogenesis.
Biological treatments for mood disordersBiological treatments for mood disorders
• Effective treatments Effective treatments knownknown to cause to cause characteristic characteristic changeschanges in specific in specific neurotransmitter systems.neurotransmitter systems.
• These are their These are their primaryprimary actionsactions..
NEUROTRANSMITTERS AND MOOD DISORDERSNEUROTRANSMITTERS AND MOOD DISORDERS
Kandel et al, Principles of Neural Science, 2000

Kandel et al, Principles of Neural Science, 2000

RECEPTORS
Receptors linked to second-messenger
systems
5-HT1A linked to inhibition of adenylyl cyclase5-HT1B linked to inhibition of adenylyl cyclase5-HT1C linked to inhibition of adenylyl cyclase5-HT1D linked to inhibition of adenylyl cyclase5-HT1E linked to inhibition of adenylyl cyclase
5-HT2A linked to phospholipase and PI turnover5-HT2B linked to phospholipase and PI turnover5-HT2C linked to phospholipase and PI turnover
5-HT4 linked to stimulation of adenylyl cyclase
5-HT5 unknown linkage
5-HT6 linked to stimulation of adenylyl cyclase
5-HT7 linked to stimulation of adenylyl cyclase
Receptors linked to an ion channel
5-HT3
GENE FAMILY
Superfamily of receptors with seven trans-membrane regions coupled to G proteins
Superfamily of ligand-gated channels
Serotonin Receptors
5-HT = 5-hydroxytryptamine (serotonin); PI = Phosphatidylinositide

Kandel et al, Principles of Neural Science, 2000
Kandel et al, Principles of Neural Science, 2000
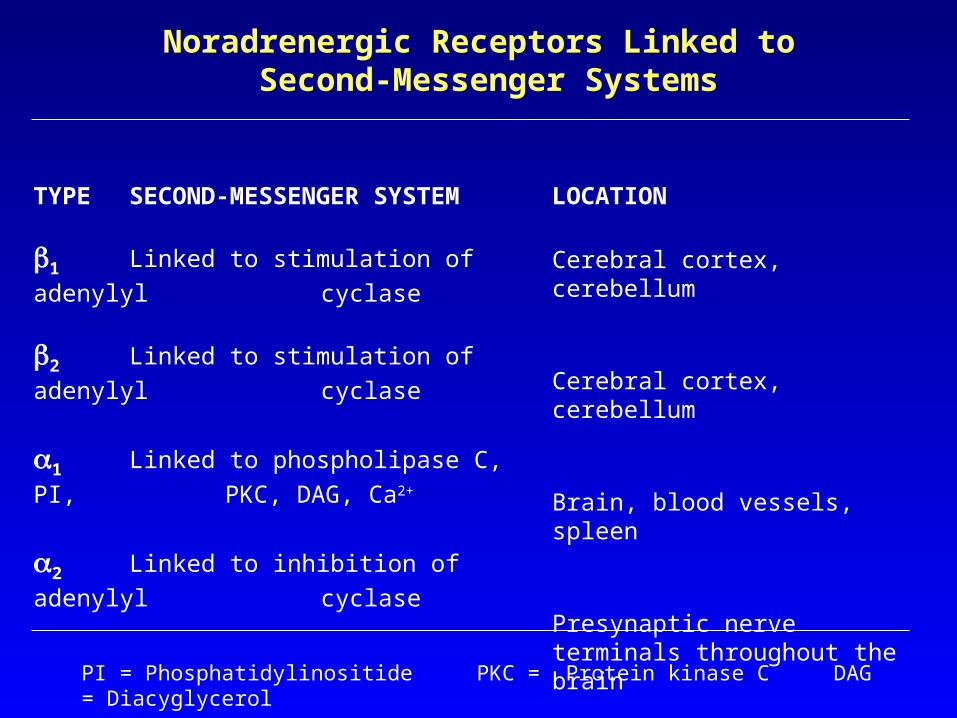
TYPE SECOND-MESSENGER SYSTEM
1 Linked to stimulation of adenylyl
cyclase
2 Linked to stimulation of adenylyl
cyclase
1 Linked to phospholipase C, PI,
PKC, DAG, Ca2+
2 Linked to inhibition of adenylyl
cyclase
LOCATION
Cerebral cortex, cerebellum
Cerebral cortex, cerebellum
Brain, blood vessels, spleen
Presynaptic nerve terminals throughout the brain
Noradrenergic Receptors Linked to Second-Messenger Systems
PI = Phosphatidylinositide PKC = Protein kinase C DAG = Diacyglycerol
MONOAMINE THEORIES OF MOOD DISORDERS
• Precursor deficit/excess
• Abnormalities in post-translational
processing
• Transporter dysfunction
• Receptor dysfunction
• Abnormalities in signal transduction,
effector activation, amplification
• Abnormalities in transsynaptic
modulation
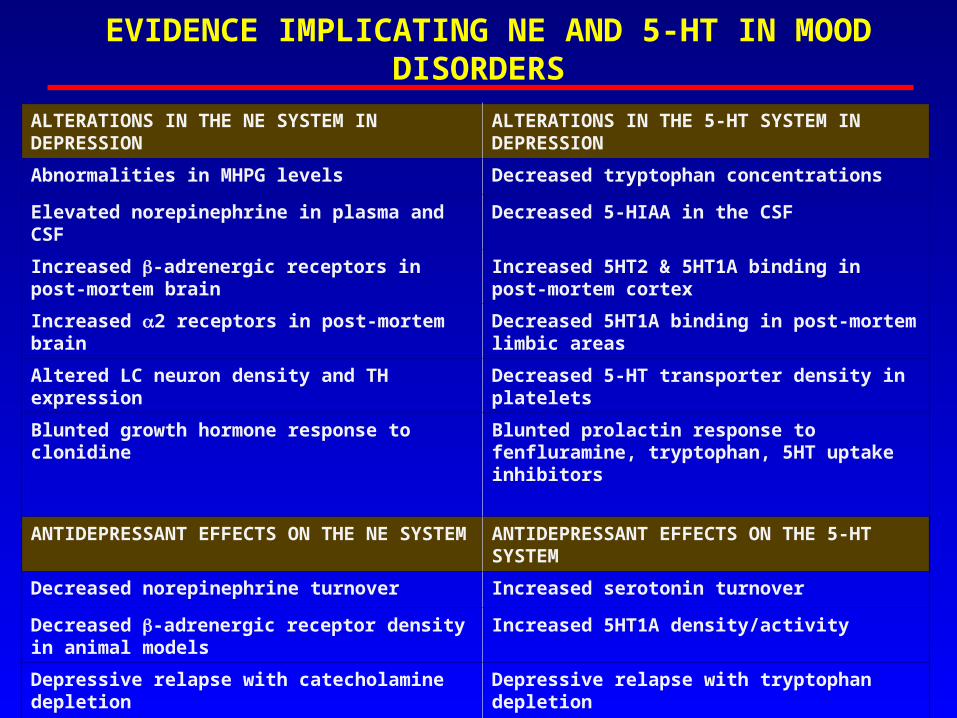
EVIDENCE IMPLICATING NE AND 5-HT IN MOOD DISORDERS
ALTERATIONS IN THE NE SYSTEM IN DEPRESSION
ALTERATIONS IN THE 5-HT SYSTEM IN DEPRESSION
Abnormalities in MHPG levels Decreased tryptophan concentrations
Elevated norepinephrine in plasma and CSF Decreased 5-HIAA in the CSF
Increased -adrenergic receptors in post-mortem brain
Increased 5HT2 & 5HT1A binding in post-mortem cortex
Increased 2 receptors in post-mortem brain Decreased 5HT1A binding in post-mortem limbic areas
Altered LC neuron density and TH expression Decreased 5-HT transporter density in platelets
Blunted growth hormone response to clonidine Blunted prolactin response to fenfluramine, tryptophan, 5HT uptake inhibitors
ANTIDEPRESSANT EFFECTS ON THE NE SYSTEM
ANTIDEPRESSANT EFFECTS ON THE 5-HT SYSTEM
Decreased norepinephrine turnover Increased serotonin turnover
Decreased -adrenergic receptor density in animal models
Increased 5HT1A density/activity
Depressive relapse with catecholamine depletion Depressive relapse with tryptophan depletion
OVERALL INCREASE IN NE TRANSMISSION IN DEPRESSION
OVERALL DECREASE IN 5HT TRANSMISSION IN DEPRESSION
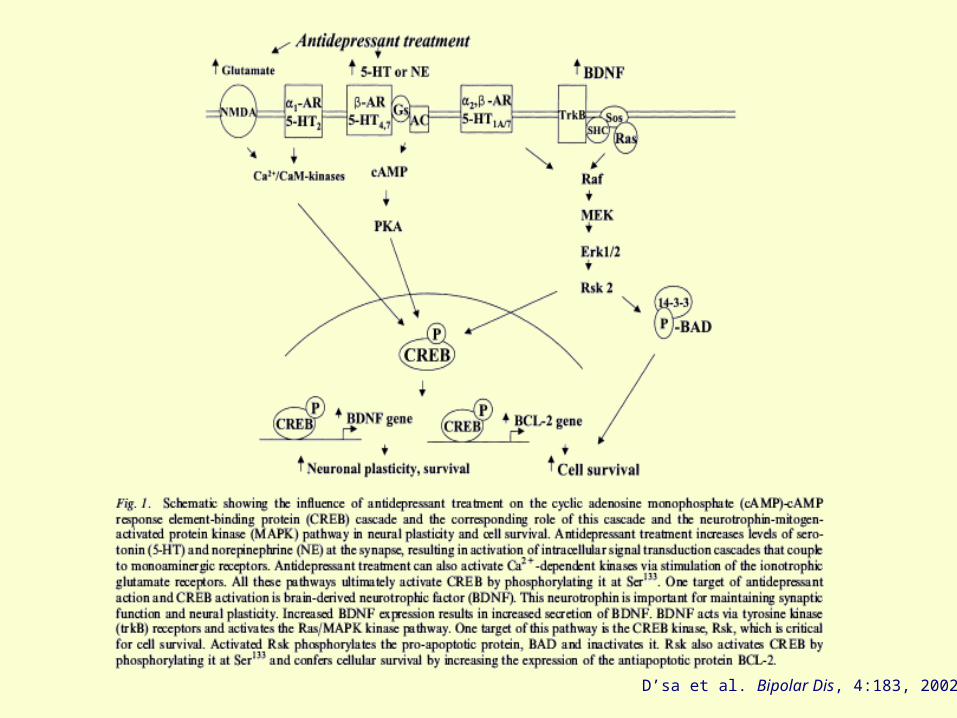
D’sa et al. Bipolar Dis, 4:183, 2002
OTHER NEUROTRANSMITTERS INVOLVED IN MOOD DISORDERS
Dopamine (DA)
Acetylcholine (Ach)
aminobutyric acid (GABA)
Glutamate
NEUROENDOCRINOLOGY NEUROENDOCRINOLOGY
AND MOODAND MOOD

Reiche,Lancet Oncol, 5:617, 2004
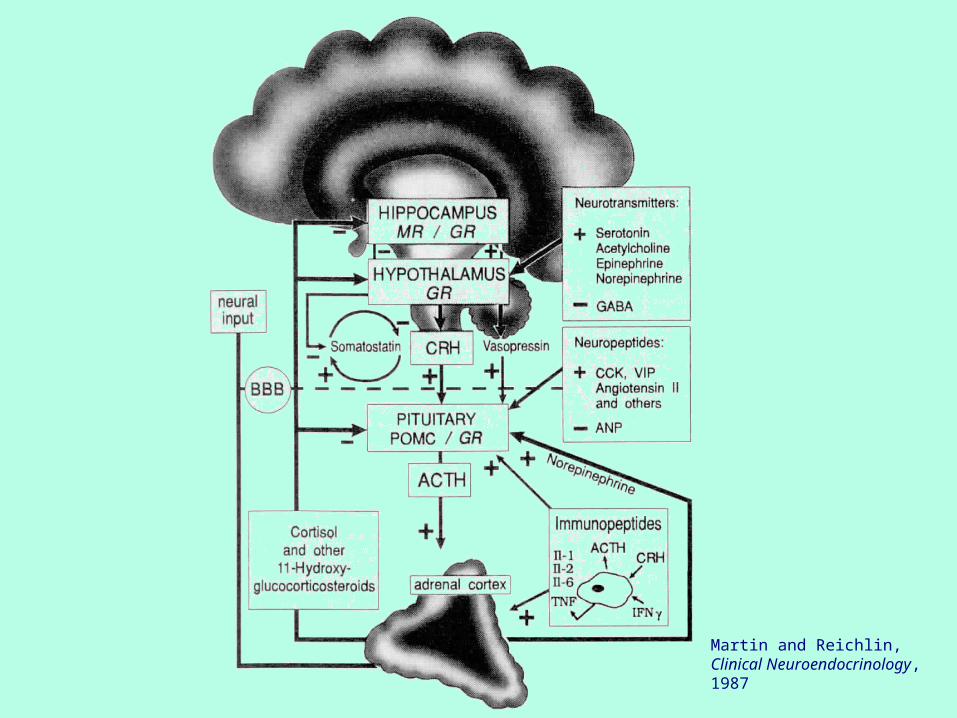
Martin and Reichlin,Clinical Neuroendocrinology, 1987
Mood disordersMood disorders • KnownKnown characteristic dysfunctional characteristic dysfunctional changeschanges in in
specific neuropeptide systems.specific neuropeptide systems.
• Unclear Unclear whether primary or secondary to whether primary or secondary to pathogenesis.pathogenesis.
Biological treatments for mood disordersBiological treatments for mood disorders• Effective treatments have been associated with Effective treatments have been associated with
changeschanges in specific neuropeptide systems. in specific neuropeptide systems.
• Most such changes believed Most such changes believed secondarysecondary..
• Efficacy of agents with Efficacy of agents with primary neuroendocrine primary neuroendocrine effectseffects under investigation, but under investigation, but notnot yet yet establishedestablished..
NEUROPEPTIDES AND MOOD DISORDERSNEUROPEPTIDES AND MOOD DISORDERS
Hypothalamic-Pituitary-Adrenal (HPA) Axis Hyperactivity in Depression
• Increased basal cortisol levels in plasma, urine, and CSF• Increased frequency, duration, and magnitude of cortisol and
ACTH secretory episodes• Resistance to suppression of cortisol and ACTH secretion by
dexamethasone• Increased cortisol response to ACTH• Blunted ACTH response to CRH• Increased CSF levels of CRH• Adrenal and pituitary gland enlargement• Decreased glucocorticoid receptor binding on lymphocytes• Decreased postmortem CRH receptor binding in frontal
cortex• Diminished glucocorticoid negative feedback

HPA Axis Function and Antidepressants
• HPA axis abnormalities in depression generally resolve with successful treatment
• In rodents, chronic treatment with conventional antidepressants causes increased:
• glucocorticoid binding• glucocorticoid receptor immunoreactivity• glucocorticoid receptor mRNA levels• glucocorticoid receptor gene promoter activity
• Suppression of HPA activity by conventional antidepressants could result from enhanced HPA axis negative feedback
• Antiglucocorticoids may have clinical antidepressant activity

NEUROIMMUNOLOGY AND NEUROIMMUNOLOGY AND
MOODMOOD
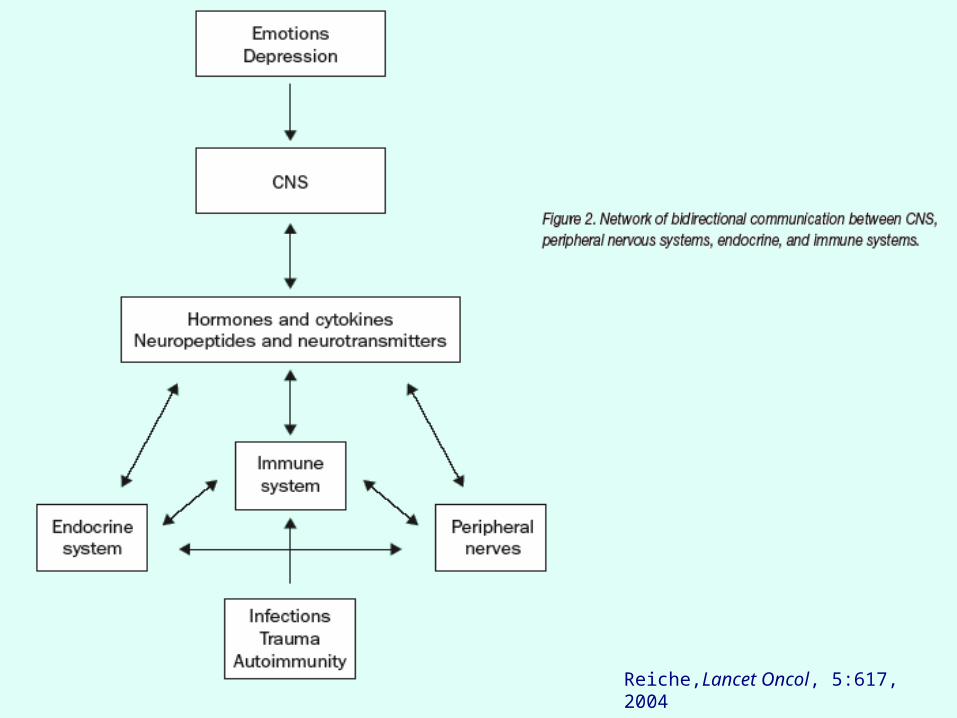
Reiche,Lancet Oncol, 5:617, 2004
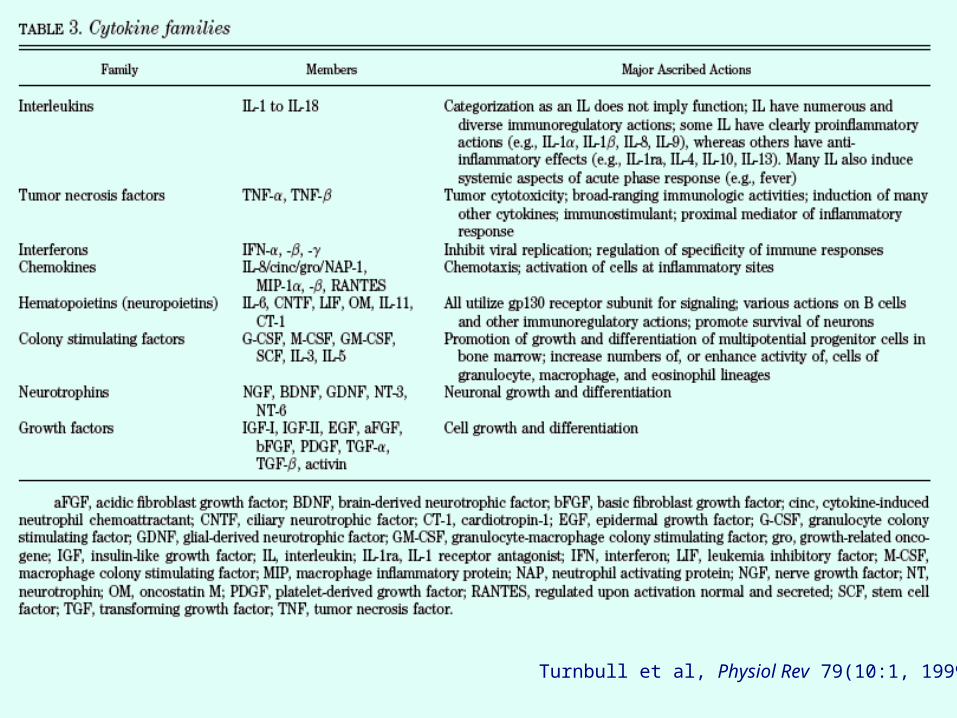
Turnbull et al, Physiol Rev 79(10:1, 1999

Mood disordersMood disorders
• HypothesizedHypothesized dysfunctional dysfunctional changeschanges in in specific cytokine systems.specific cytokine systems.
• Unclear Unclear whether primary or secondary to whether primary or secondary to pathogenesis.pathogenesis.
Biological treatments for mood disordersBiological treatments for mood disorders
• Effective treatments have been associated Effective treatments have been associated with with changeschanges in specific cytokine systems. in specific cytokine systems.
• Most such changes believed Most such changes believed secondarysecondary..
CYTOKINES AND MOOD DISORDERSCYTOKINES AND MOOD DISORDERS

Kronfol et al, Am J Psychiatry 157:683, 2000
GENETICS AND MOODGENETICS AND MOOD
Mood disordersMood disorders
• Genetic factors Genetic factors knownknown to to increase riskincrease risk, but , but inheritance is multifactorial.inheritance is multifactorial.
• CentralCentral to pathogenesis. to pathogenesis.
Biological treatments for mood disordersBiological treatments for mood disorders
• Interaction of effective treatments with Interaction of effective treatments with genetic risk factors (pharmacogenetics) genetic risk factors (pharmacogenetics) under investigation, but under investigation, but notnot yet yet establishedestablished..
•EfficacyEfficacy
•Tolerability/adverse effectsTolerability/adverse effects
GENETICS AND MOOD DISORDERSGENETICS AND MOOD DISORDERS
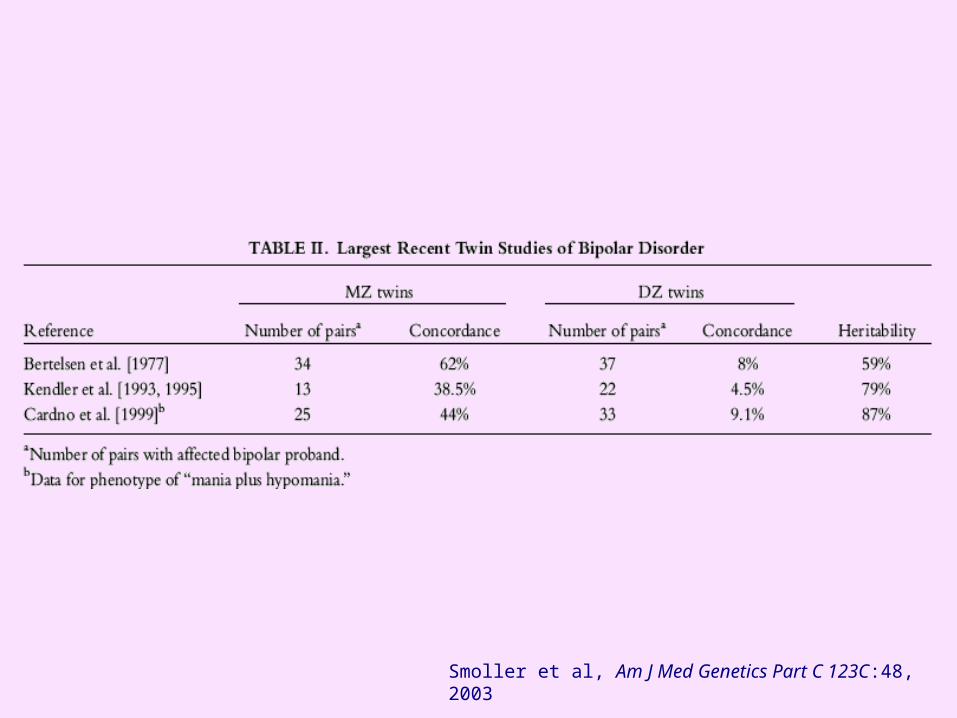
Smoller et al, Am J Med Genetics Part C 123C:48, 2003
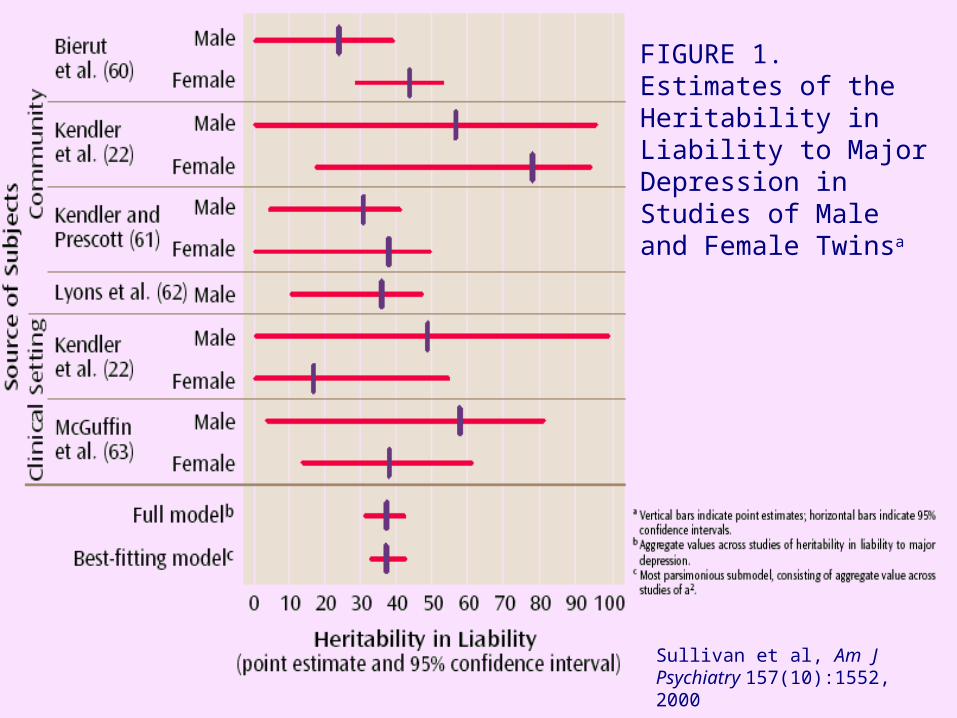
Sullivan et al, Am J Psychiatry 157(10):1552, 2000
FIGURE 1.Estimates of the Heritability in Liability to Major Depression in Studies of Male and Female Twinsa

Tsuang et al, J Psychiatr Res 38:13, 2004

Kendler et al, Am J Psychiatry 159:1133, 2002
FIGURE 2. Paths and Correlations Involving Genetic Risk for Major Depression in the Best-Fitting Model for Predicting anEpisode of Major Depression in the Last Year in 1,942 Female Twins
EXPERIENTIAL FACTORS EXPERIENTIAL FACTORS
AND MOODAND MOOD
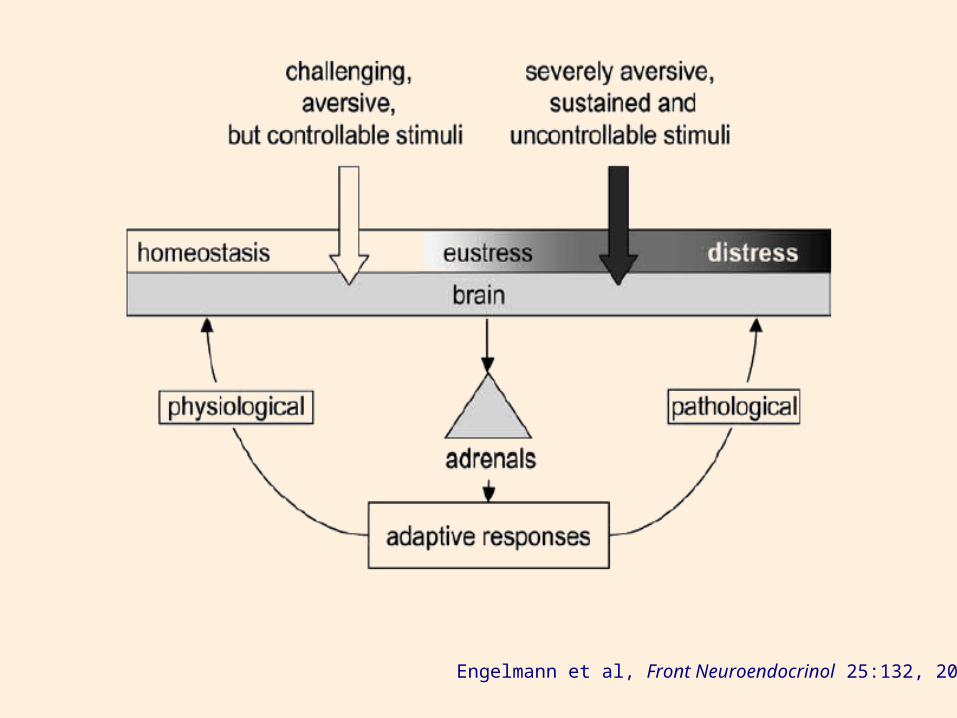
Engelmann et al, Front Neuroendocrinol 25:132, 2004
Mood disordersMood disorders
• Stressors Stressors knownknown to increase risk. to increase risk.
• Sometimes Sometimes primary to pathogenesis, but primary to pathogenesis, but often secondary.often secondary.
Psychosocial treatments for mood disordersPsychosocial treatments for mood disorders
• Effective treatments target Effective treatments target specific aspectsspecific aspects of the mood disorder (e.g., CBT, IPT).of the mood disorder (e.g., CBT, IPT).
• Effective treatments Effective treatments decreasedecrease the the subjectivesubjective experienceexperience of stress, but nonspecific stress of stress, but nonspecific stress reduction usually ineffective.reduction usually ineffective.
STRESS AND MOOD DISORDERSSTRESS AND MOOD DISORDERS

Mood Disorders and Psychosocial Stress
EARLY LIFE STRESSEARLY LIFE STRESS
NeglectNeglect
AbuseAbuse
ADULT STRESSADULT STRESS
Object lossObject loss (feelings of abandonment isolation (feelings of abandonment isolation
loneliness despair) loneliness despair)
FailureFailure (feelings of failure self-esteem (feelings of failure self-esteem
worthlessness guilt) worthlessness guilt)
Inadequate nurturanceInadequate nurturance
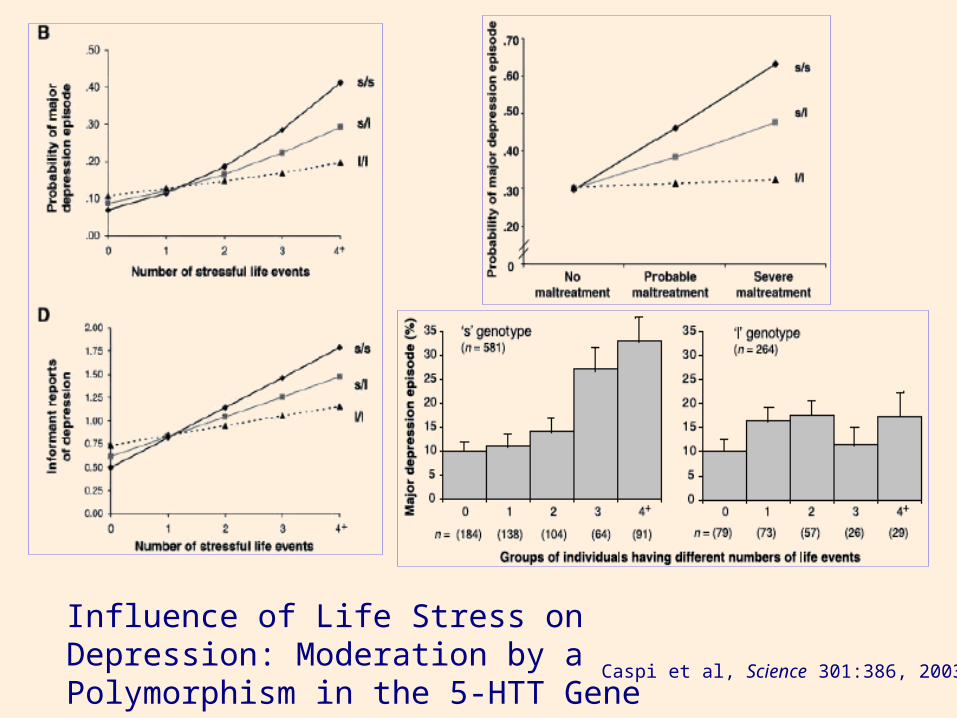
Caspi et al, Science 301:386, 2003
Influence of Life Stress on Depression: Moderation by aPolymorphism in the 5-HTT Gene
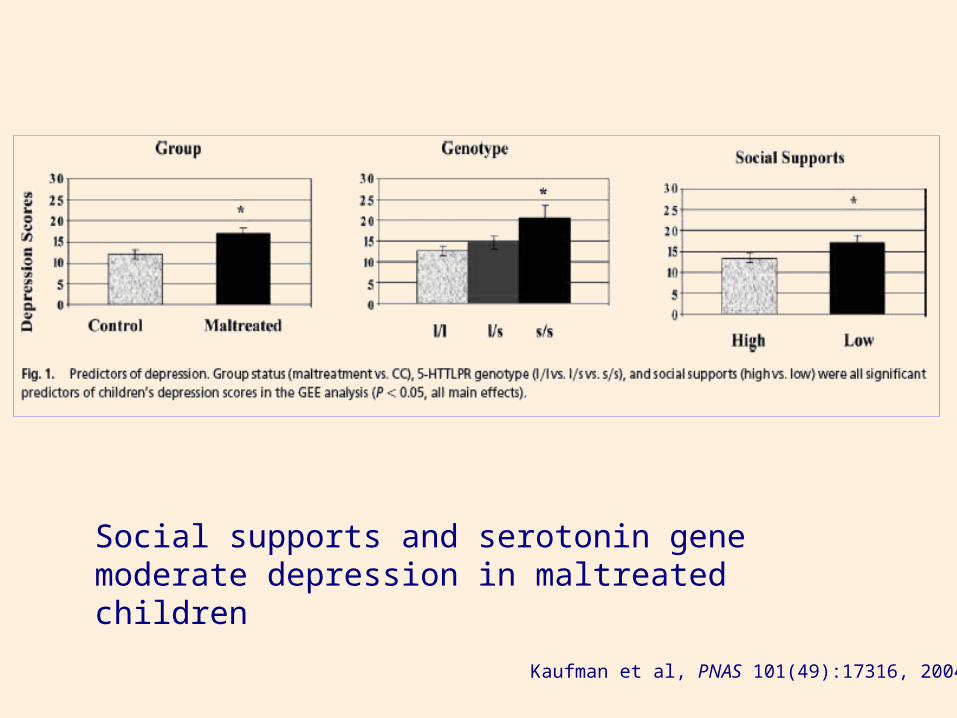
Kaufman et al, PNAS 101(49):17316, 2004
Social supports and serotonin gene moderate depression in maltreated children
INTEGRATIVE MODELS OF INTEGRATIVE MODELS OF
MOOD DISORDERSMOOD DISORDERS
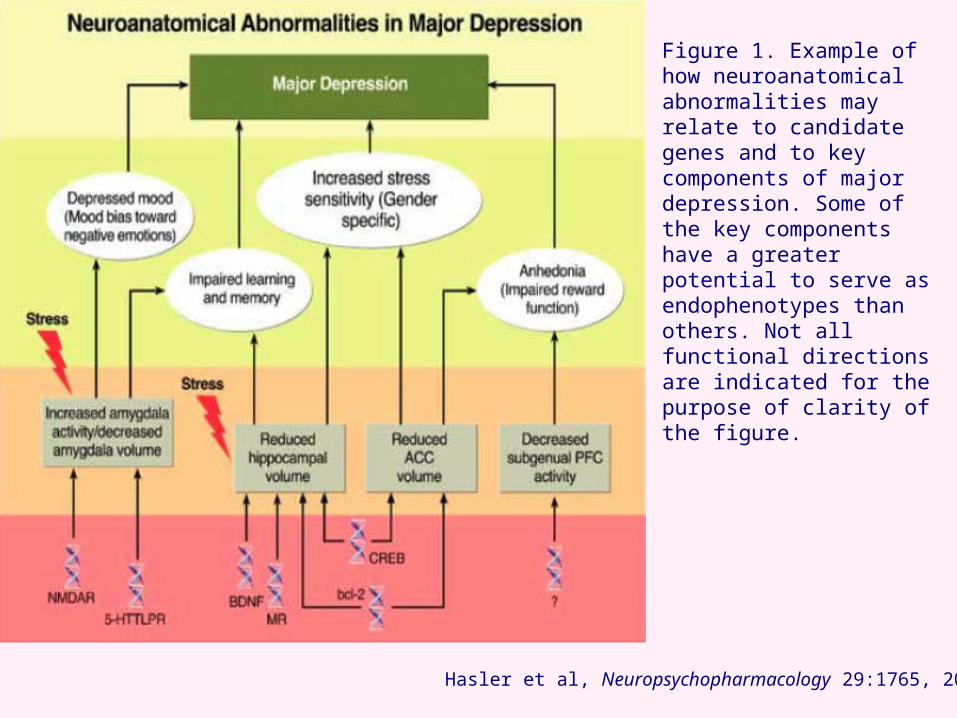
Hasler et al, Neuropsychopharmacology 29:1765, 2004
Figure 1. Example of how neuroanatomical abnormalities may relate to candidate genes and to key components of major depression. Some of the key components have a greater potential to serve as endophenotypes than others. Not all functional directions are indicated for the purpose of clarity of the figure.
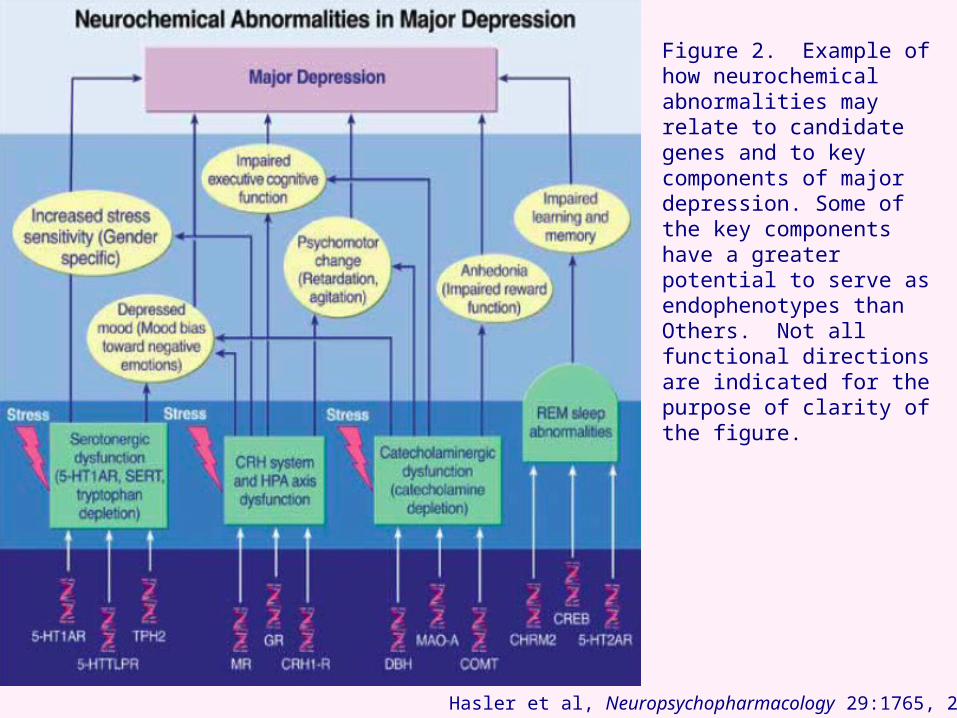
Hasler et al, Neuropsychopharmacology 29:1765, 2004
Figure 2. Example of how neurochemical abnormalities may relate to candidate genes and to key components of major depression. Some of the key components have a greater potential to serve as endophenotypes thanOthers. Not all functional directions are indicated for thepurpose of clarity of the figure.
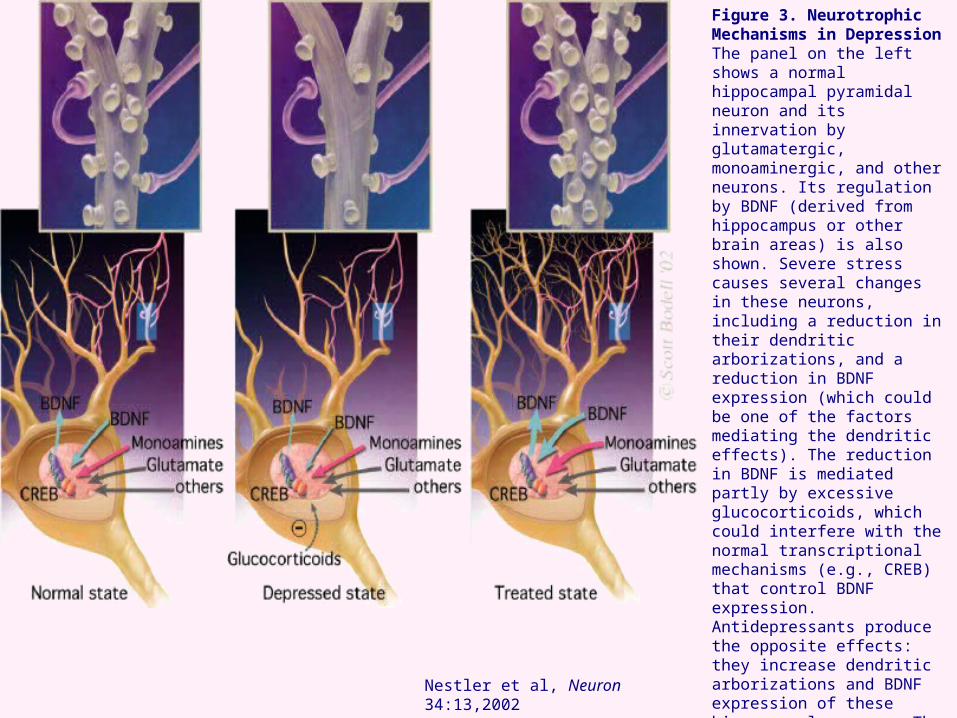
Nestler et al, Neuron 34:13,2002
Figure 3. Neurotrophic Mechanisms in DepressionThe panel on the left shows a normal hippocampal pyramidal neuron and its innervation by glutamatergic, monoaminergic, and other neurons. Its regulation by BDNF (derived from hippocampus or other brain areas) is also shown. Severe stress causes several changes in these neurons, including a reduction in their dendritic arborizations, and a reduction in BDNF expression (which could be one of the factors mediating the dendritic effects). The reduction in BDNF is mediated partly by excessive glucocorticoids, which could interfere with the normal transcriptional mechanisms (e.g., CREB) that control BDNF expression. Antidepressants produce the opposite effects: they increase dendritic arborizations and BDNF expression of these hippocampal neurons. The latter effect appears to be mediated by activation of CREB. By these actions, antidepressants may reverse and prevent the actions of stress on the hippocampus, and ameliorate certain symptoms of depression.

Manji et al, Nature Med 7(5):541,2001
Genetic and neurodevelopmental factors, repeated affective episodes and illness progression might contribute to impaired cellular resilience, volumetric reductions and cell death/atrophy. Stress and depression likely contribute to impaired cellular resilience by reducing BDNF, increasing glutamatergic function via NMDA and non-NMDA receptors, and reducing cell energy capacity. Neurotrophic factors like BDNF enhance cell survival by activating 2 signaling pathways: PI-3–kinase and ERK–MAP-kinase. BDNF promotes cell survival by increasing expression of cytoprotective protein, Bcl-2. Bcl-2 attenuates cell death by impairing release of Ca++ and cytochrome c, sequestering proforms of death-inducing caspase enzymes, and enhancing mitochondrial Ca++ uptake. Chronic antidepressant increases BDNF and its receptor TrkB. Li and VPA upregulate cytoprotective protein Bcl-2. Li and VPA also inhibit GSK-3β, resulting in neuroprotective effects. VPA activates the ERK-MAP-kinase pathway, which may have neurotrophic and neurite outgrowth effects. BDNF, brain derived neurotrophic receptor; trkB, tyrosine kinase receptor for BDNF; NGF, nerve growth factor; Bcl-2 and Bcl-x – anti-apoptotic members of Bcl-2 family; BAD and Bax, pro-apoptotic members of Bcl-2 family; Ras, Raf, MEK, ERK, components of ERK MAP kinase pathway; CREB, cyclic AMP responsive element binding protein; Rsk-2. Ribosomal S-6 kinase; ROS, reactive oxygen species; GR, glucocorticoid receptor, GSK-3, glucogen synthase kinase.
Fig. 2 Neuroplasticity and cellular resilience in mood disorders.
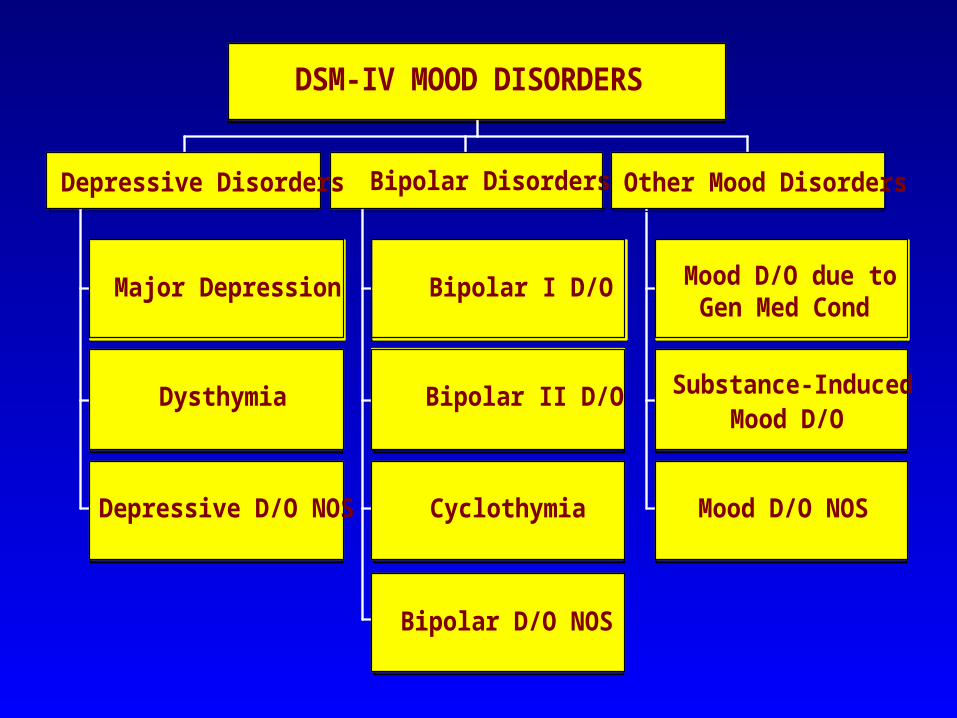
Major Depression
Dysthymia
Depressive D/O NOS
Bipolar I D/O
Bipolar II D/O
Cyclothymia
Bipolar D/O NOS
Bipolar Disorders
Mood D/O due toGen Med Cond
Substance-InducedMood D/O
Mood D/O NOS
Other Mood Disorders
DSM-IV MOOD DISORDERS
Depressive Disorders
BUTLER HOSPITAL BUTLER HOSPITAL MOOD DISORDERS RESEARCH MOOD DISORDERS RESEARCH
PROGRAMPROGRAMDepartment of Psychiatry and Human BehaviorDepartment of Psychiatry and Human Behavior
Brown Medical SchoolBrown Medical School
345 Blackstone Blvd345 Blackstone Blvd
Providence, RI 02906Providence, RI 02906
TEL 401- 455-6537TEL 401- 455-6537
FAX 401- 455-6534FAX 401- 455-6534