biology of aging carmel bitondo dyer, md kathleen pace murphy, phd the university of texas health...
TRANSCRIPT

Biology of AgingCarmel Bitondo Dyer, MDKathleen Pace Murphy, PhDThe University of Texas Health Science Center at HoustonDepartment of Internal MedicineConsortium on Aging

Successful students will be able to :
A. Define “aging” and four main characteristics of the aging process.B. Describe changes that occur in the aging cell.C. Describe theories of aging.D. Differentiate between normal aging, usual aging, and successful
aging – Practical Aspects
Learning Objectives
What does AGING mean to the healthcare provider?
¨ Great heterogeneity in the older population¨ Increased attention to biological age versus
chronological age¨ No “one size fits all” approach to treating older adults

Define “aging” and four main characteristics of the aging process.
1. Destructive processes2. Progressive, irreversible and ongoing 3. Intrinsically determined 4. Universal
Strehler, 1959
Biological vs Chronological Age

From age 25 – 85: a 130 fold risk of death
Your organs decrease in capacity – linearly
Reduced response to stimuli – example?
Increased susceptibility to disease
Destructive Processes

Homeostenosis

Chronological Age vs. Biological Age
How long have You lived?
How old is Your body?

The average number of years remaining for a living being (or the average for a class of living beings)of a given age to live.
Life Expectancy

Improved public hygiene and the discovery of antibiotics in the early to mid 1900s led to significantly prolonged lifespan
Further prolongation occurred in 1970’s and 1980’s with improved treatments for cardiovascular disease
Life Expectancy

Mortality increases exponentially Biochemical composition of tissue changes Physiologic capacity decreases Ability to maintain homeostasis diminishes Susceptibility and vulnerability to disease increases
Environmental and genetic factors influence the rate of aging
Characteristics of Aging (1 of 2)

Loss of physiologic reserve and decreased homeostatic control may result from:
Allostatic load (persistent activation of normal neuroendocrine, immune, and autonomic responses to stress)
Development of homeostenosis (altered response to physiologic stresses)
Changes are generally irreversible
Characteristics of Aging (2 of 2)

Progeria is a disease of premature aging Death typically by age 13 and usually due to atherosclerotic
disease, stroke, heart attack. Hutchinson-Gilford Progeria linked to mutations in the nuclear
structural protein lamin A. caused by a tiny, point mutation in a single gene, known as
lamin A (LMNA).
Developmental-Genetic Progeria

Disease of premature aging. Patients appear normal for first two decades of life but develop arteriosclerosis, malignant neoplasms, DMII, osteoporosis, cataracts very young
Werner’s Syndrome
Disorder isolated to a single gene on chromosome 8 which encodes for a DNA helicase
This gene has been cloned and is an area of great research DNA helicases are involved in the repair, replication and
expression of genetic material

Aging research has turned away from a single gene answer to the cause of aging.
Increasing understanding that aging is a consequence of complex interactions within differing systems of the body and the surrounding environment.

Describe changes that occur in the aging cell Morphological alterations Enzyme function Gene expression Telomere shortening
Learning Objectives

Aging is caused by changes in gene expressions, affecting both aging and development
Gene Regulation Theory

Compared with younger adults, the elderly can have decreased, unchanged, or increased rates of gene expression
Mechanisms that influence gene expression with aging: Mutations in DNA sequences in/around certain genes Latent viral infections (eg, herpes viruses) Accumulation of environmentally induced cell damage
It is unknown whether age-related changes in gene expression are functionally significant
Gene Expression (1 of 2)

Primary changes in gene expression with age: Decreased transcription rates for key genes Decreased messenger RNA (mRNA) turnover Decreased inducibility of genes, such as immediate early genes,
acute phase reactants, and stress genes Expression of genes related to stress response is up-regulated
during senescence Consequences unknown May be adaptations to accumulated environmental or oxidative
stress
Gene Expression (2 of 2)

Accuracy of mRNA translation is impaired due to inability to decode codons in mRNA
Codon Restriction Theory

Decline in fidelity of gene expression over time resulting in increased portion of abnormal proteins
Error Catastrophe Theory

A gradual accumulation of random molecular damage over time impairs regulation of gene expression
Dysdifferentiation

Morphological Cell Changes – CELL SUICIDE. Replicative senescence - irreversible arrest of cell proliferation
and altered function. A greater heterogeneity of cell sizes A shift to larger cell sizes An increase in the size of the nucleus, nucleolus, number of
multinucleated cells. Prominent Golgi apparatus, evacuated endoplasmic reticulum,
increased number of cytoplasmic microfilaments, vacuolated cytoplasm, and large lysosomal bodies observed in senescent human fibroblasts.
Cellular Theory of Aging

Each cell has a maximum number of divisions before it enters senescence
The length of the telomere end of the DNA chain shortens with each division and less telomerase activity is observed
A telomere is a region of highly repetitive DNA at the end of a chromosome that functions as a disposable buffer
Cellular Theory of Aging

Telomeres are protein-DNA structures that comprise the terminal ends of eukaryotic chromosomes. In humans, telomeres are composed of repeats of the sequence TTAGGG reiterated in tandem for up to 15 kilobases at birth.
Telomeres stabilize chromosomal ends by binding to proteins that prevent them from being recognized as double-stranded breaks by repair enzymes.
This function protects chromosome ends against degradation and end-to-end fusion and prevents inappropriate activation of checkpoint pathways that respond to chromosome breaks.
Telomeres may also play a role in the determination of chromosomal localization within the nucleus and regulation of cellular replicative capacity.
Telomere

Aged cells with proliferative potential exhibit telomere shortening and loss of telomerase activity
Conversely, telomerase hyperactivity is linked to cellular transformation and cancer
Telomere length and telomerase activity might be clinical markers of human aging and oncogenesis
Telomere

Oxidative metabolism produces reactive oxygen species which damage protein, lipids and DNA
Oxidative Stress Theory

In support: Mutations in oxidative stress pathway can extend life span Mutations in other pathways that increase longevity resist
oxidative damage In opposition: Antioxidants do not delay human senescence or
disease
Oxidative Stress Theory
Genetically determined, programmed cell death.
“Genome Crisis”
Apoptosis Theory
Changes in the neuroendocrine control of homeostasis result in aging-related physiologic alterations
Neuroendocrine Theory
Synopsis: Hypothalamic and pituitary responses are altered (TRH, GNRH, GHRH, TSH, LH, FSH, GH, ACTH)
In support: No direct support as causative of healthy aging, and supplementation does not alter aging in humans

Changes in the immune system with aging lead to increases in infectious disease and increase in autoimmune disease in older adults.
Immune Senescence Theory

Synopsis: Time-acquired deficits, primarily in T-cell function, increase susceptibility to infections and cancer Slower onset of lymphocyte proliferation Diminished cloning efficiency of individual T cells Fewer population doublings of fibroblasts
In support: Some diseases are associated with aging In opposition: Immunologic function is apparently not directly
related to healthy aging
Theories of Aging: Immune Senescence

There appears to be endocrine regulation of aging In a range of species, mutations in certain genes, especially
those that appear to play roles in metabolic and insulin signaling (eg, GH, IGF-1), extend life span
In contrast, life span is shorter in humans with untreated isolated GH deficiency (but normal age-related GH decline may have little to do with healthy aging)
Low-expressing IGF-1 receptor alleles are more highly represented among long-lived humans
These pathways are potential targets for drugs to delay or prevent age-related changes
Life Span Extension: Metabolic And Insulin Signaling

Can all of this knowledge be used to extend lifespan?

50% of seniors use them Research is confounded Elders excluded Daily multivitamin? Folate? Glucosamine? Vitamin D?
Vitamins?

Omega-3Fatty Acids
Co-enzyme Q10
Green Tea
Growth Hormone
Other Agents

Landon Center on Aging Photo Contest

Decreased falls Improved glucose homeostasis Improved cardiovascular function Improved flexibility Better sleep Less depression and dementia Less hip and knee pain due to arthritis
Exercise

Landon Center on Aging Photo Contest

Caloric restriction increases average and maximum life spans in a variety of species
Impact of caloric restriction varies considerably in mice and flies Two robust markers of caloric restriction in rodents (reduced
body temperature, reduced plasma insulin) have been observed in older men and in caloric-restricted rhesus monkeys
Life Span Extension: Caloric Restriction (1 of 2)

Sir2, an enzyme in the sirtuin family of proteins, mediates the benefits of caloric restriction in yeast
Sirtuin-activating compounds (STACs) could conceivably enhance life span in humans Resveratrol, a plant polyphenol in red wine, is a STAC that
prolongs life span in fruit flies and worms Resveratrol has anti-inflammatory, antioxidant, anticancer,
and vasoactive effects on human cells It might be possible to develop calorie restriction mimetics to
increase human life span
Life Span Extension: Caloric Restriction (2 of 2)

Religious Participation

Differentiate between normal aging, usual aging, and successful aging.
Learning Objectives

Normal aging is associated with progressive and universal physiologic changes.
Usual aging includes age-related diseases. Successful (or healthy) aging occurs with minimal deleterious
events and is associated with preserved function until advanced age.
Normal vs. Usual vs. Successful Aging

Why is hyperglycemia in the setting of infection so common in old people?

Increased random blood sugar in the elderly
No change in fasting glucose Unaltered glucose
responsiveness to catecholamines and corticosteroids
Old have enhanced release of steroids and catecholamines in illness
Higher frequency of hyperglycemia in illness
Glu
cose
Why is hyperglycemia so common in old people?
Decreased Insulin Sensitivity

Why is apathetic hyperthyroidism essentially unique to old people?

Muted adrenergic component to hyperthyroidism.
Decreased cardiac inotropic, chronotropic and lusitropic response to isoproterenol
Decreased vasodilatation in response to beta agonist
Many manifestation of hyperthyroidism are adrenergically mediated.
Why is apathetic hyperthyroidism unique to old people?
30-50 51-70 71-90
Heart Rate>100
100% 58% 28%
New Atrial Fib.
0% 0% 20%
Lid Lag 71% 35% 12%
Fine Skin 97% 81% 40%
Tremor 97% 89% 36%
Decreased Beta Adrenergic Sensitivity

Why do lipid soluble drugs have such long half-lives in old people?

50% or more increase in percent body fat in men
Older women can be 50% fat in body composition.
Increased half-life for lipid soluble drugs
Lipid soluble meds stored in depots
100
0
10
20
30
40
50
60
70
80
90Bone Mineral - 20%Cell Solids - 35%
Water -10%
Fat + 100%
AGE 25 AGE 75
Why do lipid soluble drugs have long half-lives in old people?
Increased Fat Mass in Old Persons

Why do old people seem to get pressure sores more often than young ones?

Loss of thickness in all three layers Loss of elastin (tenting no longer reliable measure) Flattening of dermal-epidermal junction Decreased sensation of pressure related discomfort
Why do old people seem to get pressure sores so often?
Decreased Skin Thickness

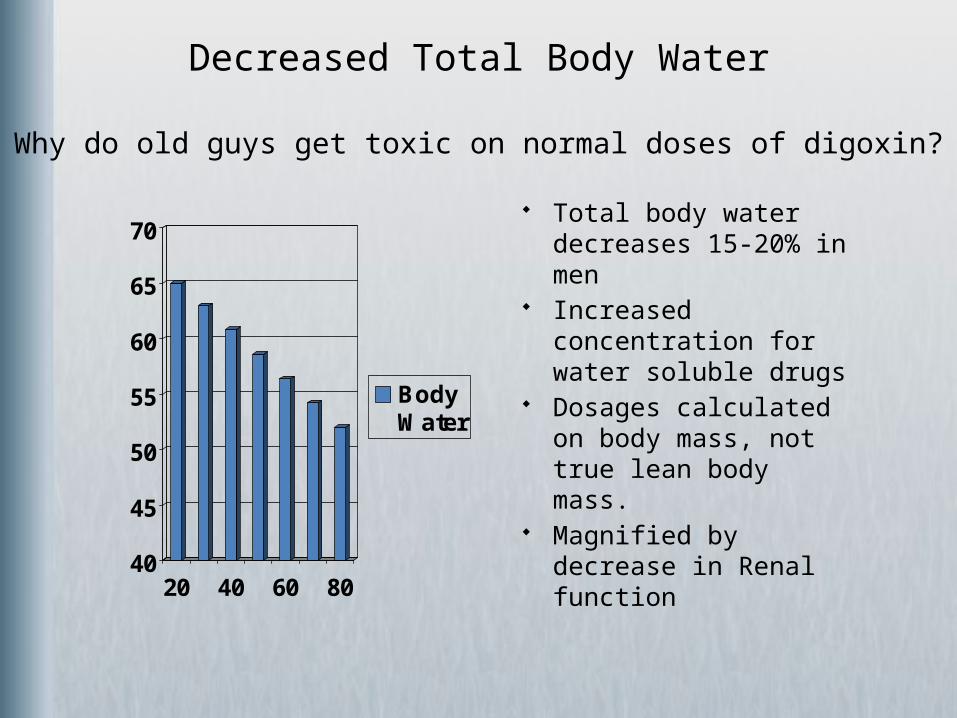
Why do old guys get toxic on normal doses of digoxin or Vancomycin?
40
45
50
55
60
65
70
20 40 60 80
BodyWater
Total body water decreases 15-20% in men
Increased concentration for water soluble drugs
Dosages calculated on body mass, not true lean body mass.
Magnified by decrease in Renal function
Why do old guys get toxic on normal doses of digoxin?
Decreased Total Body Water

Why is a heart rate of 120 in an 80 year old in the setting of an infection
equivalent to 170 in a 25 year old?

Reinterpretation of Sinus Tachycardic, SOI
Underestimate response to illness
HR of 120 in 75 year old man is roughly 75% of max heart rate, the same as 170 in a 20 year old
220-age=max HR for men Men*0.85 in women Resting HR does not change
with age
100110120130140150160170180190200
20 40 60 80
Max.H.R.
Age
Why is a heart rate of 120 in an 80 year old equivalent to170 in a 25 year old?
Decreased Maximum Heart Rate

Why do the elderly develop CHF so frequently when they go into Atrial Fibrillation?

In young people, left atrial systole just “tops off” the ventricle.
In old people, atrial systole provides 40-50% of left ventricular filling.
Atrial Fibrillation, loss of a coordinated atrial contraction, is a disaster, manifest as heart failure and low cardiac output.
Why do the elderly develop CHF when they go into A Fib?
Increased Dependence on Atrial Systole for LV Filling

Why is CHF with normal left ventricular systolic function so common in old people?

Impaired relaxation of isolated muscle from old animal hearts Impaired resequestration of calcium due to decreased levels of
Sarcoplasmic Reticulum calcium pump Restoring pump protein normalizes function Impaired tolerance of Volume loads (IV fluids) because of impaired
diastolic function Diastolic measures are best predictor of maximum exercise
performance in elderly Increased diastolic heart failure because disease related changes
are superimposed on age-related ones
Why is CHF with normal LVEF so common in old people?
Aging is Associated with Impaired Diastolic Function

Why is systolic hypertension so common in older men and women?

Likely due to collagen and elastin changes
Stiffer arteries provide less cushioning function (higher peaks result)
Reflection of large artery changes not small vessels changes
Not atherosclerosis Diameter and length of aorta
increase (uncoiling of the old aorta)
Disease changes add to age changes
400
500
600
700
800
900
1000
1100
10 30 50 70 90
Age (Years)
Stiff
ness
(PW
V in
cm
/sec)
Why is systolic hypertension so common in older persons?
Large Arteries Stiffen with Age

Why are old guys so prone to orthostatic hypotension?

Predisposing Factors: Decreased baroreceptor sensitivity Decreased arterial compliance Decreased cardiac compliance Impaired brain perfusion autoregulation Decreased renal sodium conservation Decreased plasma volume Increased venous tortuosity Blunted vasopressin response to standing Decreased renin, angiotensin, aldosterone levelsProtective Factors: Impaired beta-adrenergic vasodilation Normal alpha-adrenergic vasoconstriction Elevated circulating norepinephrine levelsOrthostatic Hypotension produces falls
Why are old folks so prone to orthostatic hypotension?
The Elderly are Predisposed to Orthostatic Hypotension

Why do physical activities become harder as we age?

05
1015
20253035
404550
25 35 45 55 65 75 85
All activities become a larger relative percent of VO2max and are perceived as harder
VO2 max decrease due to cardiac plus muscle factors
Detraining effect of bed rest may produce disability by lowering VO2 max further
Exercise will improve VO2.
Why do physical activities become harder as we age?VO
2 m
ax (m
l /kg
. min
)
Age
Decrease in VO2 Max

Why do old people develop hypoxia in response to so many challenges?

Decreased PaO2 of roughly 4 mm Hg per decade.
Worsened by lying flat in bed. No change in alveolar PO2. Preserved sensation of
hypoxia, but impaired sensation of hypercapnia in old.
50556065707580859095
100
20 40 60 80
PaO2
Why do old people develop hypoxia so frequently?
Increased VQ Mismatching in Normal Aging Lung

If we all aspirate mouth contents, why do old patients get pneumonia so often?

0
1
2
3
4
5
6
7
8
20 40 60 80
VitalCapacity
ResidualVolume
Ineffective cough Increased closing volume
which is not cleared by cough Decreased elastic recoil in old
lung Oropharyngeal Fibronectin
stickier for bacteria Decreased mucociliary
transport and slower recovery after insult
Competence of Epiglottis decreased
Immune system compromise adds to local factors
Why do old patients get pneumonia so often?
Decreased Lung Elasticity and Larger Residual Volume

Why do old people so often get confused or develop delirium in the face of infections?

Choline Acetyl Transferase (ChAT) is a marker for cholinergic pathways in brain
Decrease in ChAT in old hippocampus and neocortex No changes in ChAT with age in other parts of brain Increased frequency of delirium in normal old Marked increase in demented old Still debated as to whether delirium ever clears up
Why do old people so often develop delirium with infections?
Cholinergic Compromise

Why does a brief bout of bed rest debilitate the old patient so much?

From age 20 to 70 strength decreases 50% in legs Non-linear decline that accelerates with increasing age 30% decrease in strength from 50 to 70 80 year olds are 30% weaker at knee extensor than at 70
Upper body strength decreases less rapidly Muscle Mass Decreases with Aging, but
Young are stronger than mass predicts Old are weaker than mass predicts
Significant problems at neuro-muscular interface with motor neuron dropout, increased size muscle unit, stimulation failure. These improve with training (100% increase in strength with <10% increase in mass)
Old muscle injured more easily Loss of 5% of strength per day of immobilization
Why does a bed rest debilitate the old patient so much?
Old People have Marginal Muscle Strength

Why do old patients get hyponatremia so often?

Impaired ability to excrete water load (Minimum urine osmolality 200 instead of 75)
Impaired ability to retain salt Impaired non-osmotic stimulation of ADH release by baroreceptor Increased osmotic receptor sensitivity with enhanced ADH release Old are more susceptible to SIADH
Why do old patients get hyponatremia so often?
Increased frequency of Hyponatremia in Old

Why do old infections (TB, shingles, etc.) resurface in old people?

Thymus Involutes (essentially gone by age 70)
Thymic Hormones Decrease Decreased T-cell Proliferation Decreased Interleukin-2
production Decreased Responsiveness of
Old Memory (CD45+) cells Decreased Skin-Test Responses:
Remember Booster for TB testing
No Change in CD4/CD8 counts
IL-2 m-RNA is Decreasedafter Stimulation in Aged Humans
Y
O
Y O
Why do old infections resurface in old people?
Impaired Cellular Immunity Reduces Immuno-surveillance

Why do falls occur more frequently in old people?

Increasing sway especially without visual input Slowed reaction time Slower light dark accomodation Decreased proprioceptive input Loss of Cerebellar neurons Weakness of ankle and knee musculature Higher frequency of premonitory falls Orthostatic hypotension common 50% of falls are “accidental”
Why do falls occur more frequently in old people?
Typical Nursing Home Patients fall 1.6 times per year
Why are urinary tract infections so common in old people?

Incomplete bladder emptying with age Production of Tamm-Horsfall mucoprotein decreased Loss of bactericidal prostate secretions Decreased urine acidity and urea concentration Atrophy of Urethra in women with menopause More alkaline vaginal secretions High frequency of obstruction, stones, prostatitis, etc. Higher frequency of asymptomatic bacteriuria
Why are urinary tract infections so common in old people?
Impaired Local Defenses

Why is urinary incontinence so frequent in older women?

0
10
20
30
40
50
60
70
<45 45-64 65-74 >75
Atrophy of pelvic muscles Atrophy of Urethra Decreased maximum bladder
capacity Decreased bladder sensitivity Involuntary bladder
contractions more common Impaired mobility
Why is urinary incontinence so frequent in older women?
Inco
ntine
ntIncontinence is Common in Hospitalized Older Women

Why does lean body mass decrease in normal aging

Decrease IGF-1 due to loss of Nocturnal GH peaks
Inactivity Loss of androgens Major factor in decreased
muscle strength with aging Creatinine production
decreases 30-50% from 25 to 90
Loss of total number of fibers and decrease in CSA of each fiber, especially type II
Increased intramuscular fat with age
At age 40, Non-contractile tissue is 8% of CSA
At age 70, Non-contractile tissue is 18% of CSA
50
60
70
80
90
100
110
20 30 40 50 60 70 80 90
Mus
cle
Mas
s (%
)
Why does lean body mass decrease in normal aging?
Muscle Mass Decreases in Normal Aging

How does kidney function deteriorate with age?

70
80
90
100
110
120
130
140
30 40 50 60 70 80
Decreased CrCl by 35% in healthy older men. (No HTN, No Dm, No Drugs)
Decreased concentrating and diluting capacity
Increased number sclerotic glomeruli to 30% of total
Dependence on prostaglandins to maintain filtration
Decreased renal blood flow and renal mass
Decreased clearance of renal drugs
How does kidney function deteriorate with age?
CrCl
Decreased Creatinine Clearance

Why do old people get dehydrated so frequently?

Impaired recognition of thirst and serious dysregulation of thirst
Impaired retention of salt and water
Takes much longer to reach maximum retention
Maximum urine concentration for old people still poor
Dropout of longest nephrons in old kidney
Why do old people get dehydrated so frequently?
1
10
100
0 5
YoungOld
Days of salt deprivation
Na
Excr
eted
(% o
f con
trol
)Increased Loss of Water and Salt and Decreased Intake

Why do old people have increased probability of developing hyperthermia during heat waves?

Decreased sweat production Decreased numbers of sweat glands Higher core temperatures to start sweating Threshold to notice that it is hot is increased in the old Acclimatization to hot temperatures is less likely to occur in the
elderly. Decreased Heat Delivery to skin Decreased maximum skin vasodilatation
Why do old people develop hyperthermia?
Old People Cannot Dissipate Heat Well.

Why is it impossible to take a history from an old person with the TV on?

Impaired voice discrimination from background noise in noisy room
Also difficulty in phoneme discrimination Not equivalent to dementia Ability to comprehend connected speech is more impaired
than the ability to understand single spoken words. Hearing aids are ineffective as they amplify both target and
background Central processing defect is only partly related to other
changes in cognitive function. The older listener is more sensitive to accents and to varying
speakers than the young.
Why is it impossible to take an elder’s history with the TV on?
Central Processing Auditory Deficit

Which drugs are metabolized slower by the old liver?

Liver changes less magnitude and more variable then kidney changes
Decreased Hepatic blood flow induces decreased first pass metabolism of propranolol, verapamil, lidocaine, nitrates, morphine
Drug metabolism of drugs requiring Oxidation is slower including that by P450 enzymes like warfarin, diazepam, phenytoin, naproxen
Reduced inducibility of hepatic enzymes by barbiturates, rifampin, cigarette smoke
Which drugs are metabolized slower by the old liver?
Hepatic Changes

Content provided by: George Taffet, MD Mary McDonald, MD Fadi Ramadan, MD Bruce Troen, MD Adam Golden, MD Donald A. Jurivich, DO © American Geriatrics Society
Credits
Photographs use for the cover are allowed by the morgueFile free photo agreement and the Royalty Free usage agreement at Stock.xchng. They appear on the cover in this order:Wallyir at morguefile.com/archive/display/221205 Mokra at www.sxc.hu/photo/572286Clarita at morguefile.com/archive/display/33743
Images on slides 37, 44 and 99 are from the Microsoft Powerpoint clipart gallery.