biological membranes and transport simple diffusion simple diffusion - no transporter protein...
TRANSCRIPT

Biological Membranes and TransportSimple diffusion
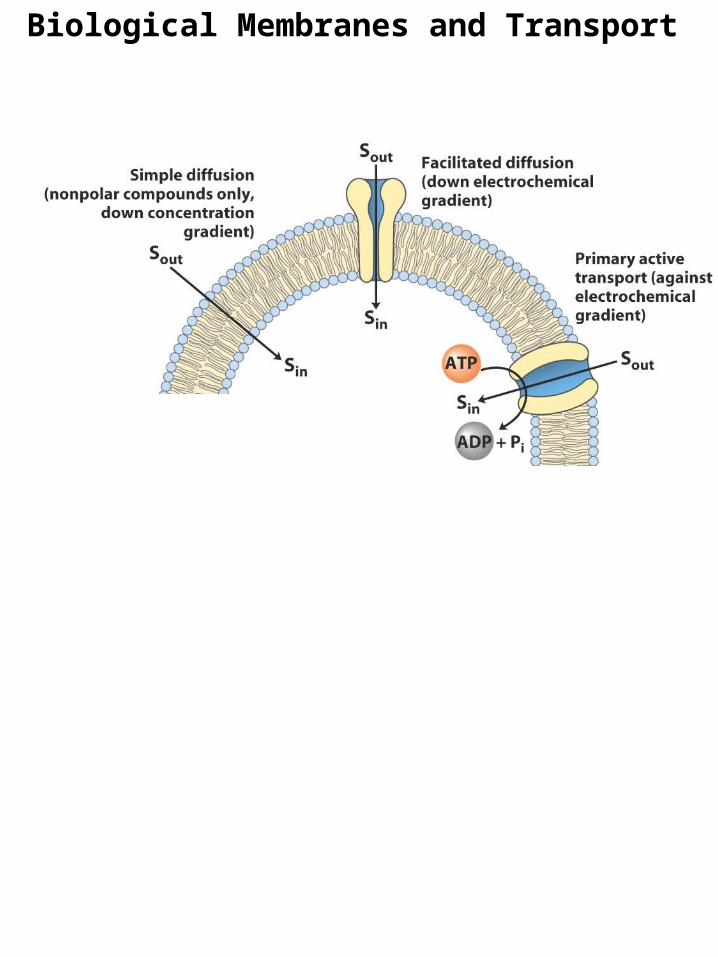
Simple diffusion - No transporter protein needed, no energy expended
Simple diffusion of gases (O2, N2, CH4), slow diffusion of water (high concentration)

Simple diffusion in living organismsImpeded by selectively permeable membranes (high G‡)
permease
Facilitated diffusionPassive transport
Bind substrate with stereochemical specificity, lots weak interactionsSpan bilayer, channel lined with hydrophilic amino acids
Biological Membranes and TransportSimple & Facilitated diffusion

Biological Membranes and TransportFacilitated diffusion (Passive transport)
Aquaporins (AQPs)Create hydrophilic transmembrane channel for passage of water (no ions)Erythrocytes (red blood cells), proximal renal tubule cells, vacuole

Biological Membranes and TransportFacilitated diffusion (Passive transport)
Glucose transporter of erythrocytesWith glucose transporter glucose enters erythrocyte at rate ~50,000 higher than without the transporter

Biological Membranes and TransportGlucose transporter of erythrocytesThink back to enzyme/substrate kineticsGlucose outside cell = substrateGlucose inside cell = productGlucose transporter = enzyme
Kt = constant similar to Km, combination of rate constants characteristic of each transport system (measure of affinity of transporter for glucose)
Lower Kt, higher affinity

Biological Membranes and Transport
Glucose transporter of erythrocytesGluT1 specific for D-glucose, Kt = 1.5 mMD-mannose (Kt = 20 mM), D-galactose (Kt = 30 mM), L-glucose (Kt > 3000 mM)
Hallmarks of passive transporter:(1) high rate of diffusion down concentration gradient(2) saturability (GluT1 is nearly sat’d with substrate and operates near Vmax )(3) specificity
High [glucose]~5 mM, 3x Kt
Lower [glucose]

Biological Membranes and TransportGlucose transporter of liverGluT2 transports glc out of hepatocytes when liver glycogen (stored sugar) is broken down to replenish blood glcGluT2 (Kt = 66 mM) can respond to increased levels of intracellular glc by n outward transport
Glucose transporter of muscle/adiposeGluT4 transporterMuscle(glycogen)/adipose(triacylglycerols) take up excess glc (> 5mM)

Biological Membranes and Transport

Biological Membranes and TransportGlucose transporter
Type I diabetes mellitus, juvenile onset, insulin-dependent diabetes
Insulin-producing cells have been destroyedInability to release insulin (mobilize glc transporters) results in low rate of glc uptakeHigh blood glucose
Type II diabetes mellitus, adult onset, noninsulin-dependent diabetes
Do make and release insulin Resistance to action of insulinNumber and affinity of insulin receptors may be reducedAbnormal activation of glc transportersObesityMedium/High blood glucose
Diabetes insipidus
genetic defect in aquaporin 2 leading to impaired water absorption by kidney

Biological Membranes and Transport
Transport of Chloride/Bicarbonate across Erythrocyte MembraneChloride-bicarbonate exchanger permeability of erythrocyte membrane to HCO3
- by 106
Two anions move at once (HCO3- and Cl- in opposite directions)
Cotransport

Biological Membranes and Transport
Chloride/BicarbonateGlucose transporter

Biological Membranes and Transport
Active transport
Movement against a concentration gradientAccumulate solute above equilibrium pointThermodynamically unfavorable, coupled to exergonic processPrimary active transport - directly coupled to ATP cleavageSecondary active transport - endergonic transport coupled to exergonic transport (went through primary first)

P-typeActive cotransport of Na+ and K+
Reversibly phosphorylated by ATP
Biological Membranes and TransportPrimary active transport: ATP-dependent active transporters
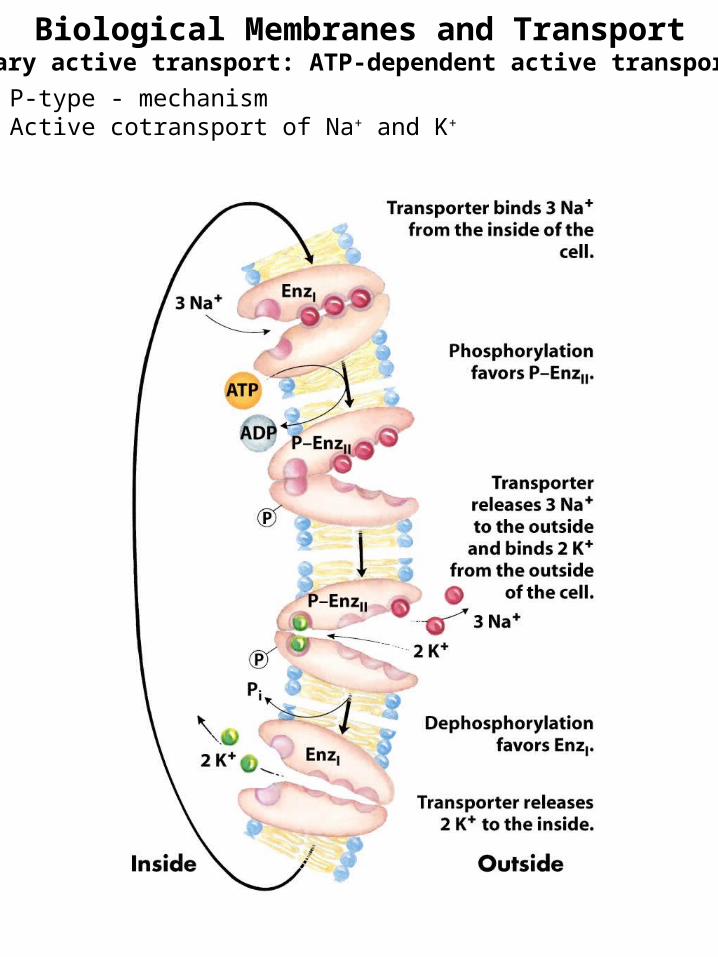
P-type - mechanismActive cotransport of Na+ and K+
Biological Membranes and TransportPrimary active transport: ATP-dependent active transporters

P-typeActive cotransport of Na+ and K+
25% of total energy consumption of a human at restInhibitors - ouabain and digitoxigenin (O+D = digitalis)Digitalis treat congestive heart failure
inhibits Na+ out, so more Na+ in cellmore Na+ activates Na+-Ca2+ antiporter in cardiac musclemore Ca2+ in cell, strengthens heart muscle contractions
Biological Membranes and TransportPrimary active transport: ATP-dependent active transporters

F-type (bacteria, mitochondria, chloroplasts) & V-type (vacuole, lysosomes, endosomes, Golgi)Acidifies organelles & pumps protons
Transmembrane pore for protons
Biological Membranes and TransportPrimary active transport: ATP-dependent active transporters

F-typeCatalyze uphill movement of protons (ATP hydrolysis)AND downhill proton flow to drive ATP synthesis (ATP synthases)
Biological Membranes and TransportPrimary active transport: ATP-dependent active transporters
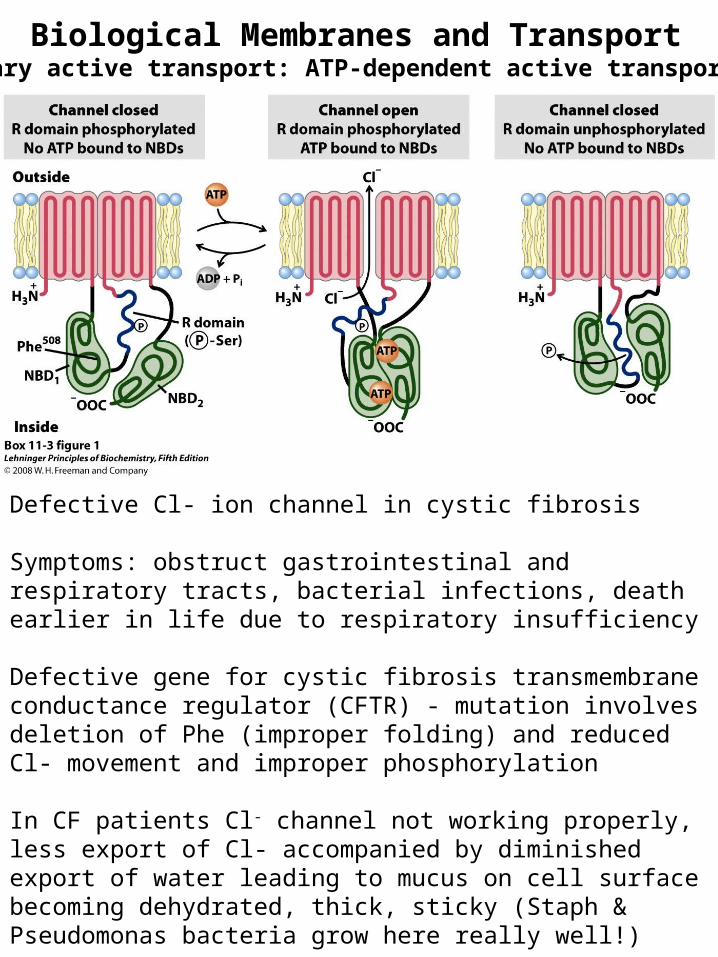
Defective Cl- ion channel in cystic fibrosis
Symptoms: obstruct gastrointestinal and respiratory tracts, bacterial infections, death earlier in life due to respiratory insufficiency
Defective gene for cystic fibrosis transmembrane conductance regulator (CFTR) - mutation involves deletion of Phe (improper folding) and reduced Cl- movement and improper phosphorylation
In CF patients Cl- channel not working properly, less export of Cl- accompanied by diminished export of water leading to mucus on cell surface becoming dehydrated, thick, sticky (Staph & Pseudomonas bacteria grow here really well!)
Normally thin layer of mucus in lungs
Biological Membranes and TransportPrimary active transport: ATP-dependent active transporters
Biological Membranes and Transport