biodecade - media.angelnexus.commedia.angelnexus.com/pdf/ea/biodecade-april-2016-1s2.pdf ·...
TRANSCRIPT
BioDecadeEquity IntelligenceInovio Pharmaceuticals Inc. (NASDAQ:INO)
Initiating CoverageRating: Strong Buy12-Month Target Price: $12.00
Total ReturnsTo Jan 15, 2016
Five Year -14%
One Year -41%
Six Months -32%
Three Months - 16%
One Month -21%
Chart Page 2
Certification
Neither the analyst nor his family has a position, long or short, in this stock.
The analyst or his family has not been paid by any company mentioned in this report.
Inovio Pharmaceuticals was not involved in the preparation of this report.
Extraordinary Technology Targeting Cancers and Infectious Disease — Immune Therapy is All About Generating T-cells, Especially CD-8+ Killer T-cells
Inovio’s human papillomavirus (HPV) DNA vaccine, VGX-3100, met its primary efficacy endpoint in a randomized, double-blind phase 2b trial with 167 patients in cervical
intraepithelial neoplasia (CIN) (cervical dysplasia). (Press release 7/23/14)
Study was published in The Lancet, which describes VGX-3100 as the first therapy to show that activated killer T-cells (CD8+) induced in vivo can clear both the precancerousCIN and the HPV (the virus) causing the disease.
Inovio received a $27.5 million upfront payment in Q3/15 from MedImmune (unit of AstraZeneca Plc [NYSE: AZN]) for INO-3112 (VGX-3100 + DNA plasmids encoded for IL-12) for HPV-driven cancers. Inovio could receive up to $727 million in milestones, as well as double-digit royalties.
Big Pharma partners, Roche Holding AG (OTCQX: RHHBY) and MedImmune, are fundingmajor projects. Combined milestones could be worth ~$1 billion.
$70 million received in non-dilutive grants and contracts in the last 12 months. $85 million on balance sheet as of 9/30/15; cash runway through Q4 of 2018.
Value Proposition — weak global market conditions create even greater opportunity
Inovio has 14 clinical-stage pipeline candidates. VGX-3100 is entering phase 3. Inovio has major pharma partners = validation of technology. Inovio is a DNA vaccine company which can deliver DNA-encoded plasmids into cells,
inducing the cell to produce a protein — either an antigen or an antibody. Effectively Inovio’s DNA vaccine technology can cause a cell to express up to four
antigens — but theoretically many more if needed. From our perspective, Inovio’s comp is Ionis Pharmaceuticals, Inc. (NASDAQ: IONS)
(formerly Isis Pharmaceuticals), which has a different platform entirely, but is targeting many diverse disease indications that can be pharma partnered.
Partnering can ultimately produce 100% margins where licensing revenue hits the top line and drops untouched to the bottom line.
Inovio’s valuation today is $357 million. Ten years ago, Ionis’ market valuation was approximately $640 million, but today it is $5.27 billion with only one real product on the market, antisense oligonucleotide Kynamro (mipomersen), for rare disease homozygous familial hypercholesterolemia, which has been disappointing in sales.
The importance of Kynamro lies in the fact that it is a novel technology that Ionis has proven, and Ionis shares are up 221.4% between date of product approval 1/29/13 and 1/15/16, even after a very severe market downturn.
Inovio’s $375 million valuation is a particularly sweet spot. It is small enough for huge multiple gains, but large enough for quality institutional investors to own.
Inovio has only 32% institutional sponsorship, which gives it room for dramatic uptake by small-cap mutual funds and hedge funds.
VGX-3100 has demonstrated that it can induce regression of CIN and clear HPV infection with a robust T-cell response, proving mechanism of action.
Phase 3 Trial with VGX-3100 to begin in mid-2016. Clinical proof of concept has been achieved. Pipeline is bulging with candidates. Strong Buy — $12 price target
Biotechnology—Advanced Therapies
Dr. George S. MackManaging [email protected]
Ticker: NASDAQ:INOClosing Price Jan 15, 2016 $5.2152-Week Range: $4.79-$10.83Market Cap: $375 million
As of Sep 30, 2015Shares outstanding: 72.18 millionFully diluted: 78.9 million Cash and equiv: $170.8 million
OwnershipInstitutional ownership: 32%Top 10 institutions: 21.45%Mutual fund ownership: 14.47%Float: 93.8%5%/Insider ownership: 6.18%

BioDecadeEquity Intelligence
INO One Year Chart to 1/15/16
Page 3 of 28
Milestones/Catalysts2016
VGX-3100 — Early- to mid-Q1/16 end-of-phase 2 FDA meeting to settle on phase 3 design for cervical intraepithelial neoplasia.
VGX-3100 — Q2 or mid-16 begin phase 3 trial with VGX-3100 in cervical intraepithelial neoplasia
Since p values were so low in phase 2b trial, this trial will only contain 200-300 patients. INO-4212—2016 phase 1 (with GeneOne Life Science) will read out Ebola data
If positive data are generated, then Inovio and GeneOne will seek outside development funding, likely from a U.S. Government source.
INO-1800 — Hepatitis B virus therapeutic vaccine (with Roche) initiate phase 1 INO-5150 — Prostate cancer therapeutic vaccine, phase 1 safety data will read out in mid-2016 INO-3112 Therapeutic vaccine for HPV-driven cervical cancer (with EORTC & MedImmune) initiation
of phase 2 trial

BioDecadeEquity Intelligence
Product PortfolioProduct
CandidateDisease indication Type intervention Partner Comment
VGX-3100(synthetic constructs of DNA plasmids targeting antigenic proteins expressed by E6 and E7 oncogenes of HPV Types 16 and 18)
Antigens: E6, E7
Cervical dysplasia(HPV-driven cervical intraepithelial neoplasia [CIN] grade 2/3)
CIN 2/3
Therapeutic Wholly ownedby Inovio
This is Inovio’s lead candidate Phase 2 completed Phase 3 trial to be
initiated in mid-2016.
INO-3112(VGX-3100 + synthetic constructs of DNA plasmids encoding interleukin-12 [IL-12])(IL-12 is an immune activator)
Antigens: E6, E7
Cervical cancerHPV-driven
Therapeutic MedImmune & EORTC
EORTC-sponsored phase 2 trial to begin in 2016
Cervical cancerHPV-driven
Therapeutic MedImmune Phase 1/2 in progress
Head & neck cancerHPV-driven
Therapeutic MedImmune Phase 1/2 in progress
INO-3106(synthetic constructs of DNA plasmids targeting antigenic proteins expressed by E6 and E7 oncogenes)
Antigens: E6, E7
Aerodigestive cancers, HPV-driven
Affecting lips, mouth, tongue, nose, throat, vocal cords, larynx, and parts of the esophagus and windpipe.
Wholly ownedby Inovio
Phase 1 begun in Q3/2013
INO-5150(dual-antigen synthetic construct immune therapy targeting prostate-specific membrane antigen (PSMA) and prostate-specific antigen (PSA))Antigens: PSA, PSMA
Prostate cancer Therapeutic Wholly ownedby Inovio
Phase 1 begun Q3/2015Report interim data 2016
Page 4 of 28

BioDecadeEquity Intelligence
INO-1400DNA immunotherapy targeting human telomerase reverse transcriptase (hTERT), which is present in over 85% of cancer types in the world.
A “universal” cancer therapy
18-fold higher T cells generatedthan closest pharma comparator
Antigens: hTERT
Breast, lung, and pancreatic cancers
INO-1400 is a potential universal cancer therapy
Therapeutic Wholly ownedby Inovio
Report interim data 2016
Product PortfolioProduct
CandidateDisease
indicationType of
interventionPartner Comments
INO-1800
Antigens: Multiple- surface andcore
Hepatitis BClades A&C
Therapeutic Roche Phase 1 trial initiated Q2/2015
INO-8000
Antigens: NS3/4A, NS4B, NS5A
Hepatitis CGenotypes 1a & 1b
Therapeutic GeneOne Life Sciences, Inc.
Report interim phase 1 data 2016
PENNVAX®-B (synthetic constructs of DNA plasmids encoding the Gag, Pol, and Env proteins of HIV)
Antigens: gag, pol, env
HIVClade B
Prophylactic&Therapeutic
HIV Vaccine Trials Network
Excellent T-cell responses reported in 89% of phase 1 patients Data in Journal of Infectious
Diseases July 2013
PENNVAX®-GAntigens: env, gag
HIVClades A, C, D
ProphylacticTherapeutic
USMHRP/NIAID Completed enrollment in phase 1 Interim data show PENNVAX-
G + MVA boost achieves 100% antigen-specific T-cell response
PENNVAX®-GP
Antigens: gag, pol, env
Inovio’s lead HIV program
HIVClades A,B,C,D
ProphylacticTherapeutic
NIH/NIAID/HVTN Phase 1 initiated Q3/2015 Preclinical studies
demonstrate strong antigen-specific T-cell response and protection from HIV
Several in study
Antigens: HA
Influenza - universal
Prophylactic NIH Director's Office Transformative Research Award
Phase 1 Applications out for grants. Have demonstrated immune
response versus 6 unmatched H5N1 strains and9 important H1N1 influenza strains that have attacked humans over past century; includes 1918 pandemic flu.
H7N9 preclinical studies shield against 100% of
Page 5 of 28
BioDecadeEquity Intelligence
animals. Vaccine is not matched to the virus subtype.
INO-4212
Antigens: various
Ebola ProphylacticTherapeutic
DARPA +international consortium
Phase 1 data Q1/2016
Others Clostridium difficile, tuberculosis, foot-and-mouth disease (for animals), malaria, dengue fever, Chikungunya virus, and other tropical infections, some with bioterrorism
Research/Preclinical
DNA-encoded antibodies (dMAb)
See page 11: “Exciting Product Category in Research” Research/Preclinical
Inovio Pharmaceuticals Technology PlatformThe vaccine, or immunization, is the closest thing there has been to a miracle in medicine. It didn’t take long tounderstand that people who got smallpox didn’t get it again. True active immunity had been conferred on these lucky survivors who had endured a critical storm. In 1796 English physician Edward Jenner created the first generally safe vaccine that would be administered to patients to prevent smallpox, a highly contagious disease that would kill 90% of its infected victims. Smallpox, the most lethal contagious disease known to humankind, would become the only infectious disease to be eradicated by immunization.
In the traditional model of immunization the patient is given an antigen or antigens in the form of an attenuated (live but harmless or much less virulent) bacterium, virus, parts of a virus, or a stand-alone protein (the antigen). An antigen coming from outside the patient is recognized by the immune system as foreign, and the mammalian immune system counters with a humoral response by inducing B-cells to produce antibodies, which are large proteins that are expressed in response to the antigenic stimulus. Antibodies combine with andneutralize or attack the antigen to keep the patient safe from disease. There is also a cellular response where antigen-specific killer (CD8+) and helper (CD4+) T-cells are mobilized to fight the disease-causing agent.
An immunization can be a preventive (prophylactic) model, as in the case of the seasonal or pandemic influenza or smallpox vaccine. In recent years we are seeing immunizations developed as therapeutic agents that leverage the immune system to kill infectious disease-causing pathogenic bacteria, viruses — such as Ebola — or even vaccines to kill tumor cells. One such cancer-causing microbe that Inovio is attacking is the human papillomavirus (HPV) that can cause neoplastic changes after infecting mucous membranes such as those in the cervix, oral cavity, and nasopharynx.
SynCon® Immunotherapy Technology
Inovio’s technology is a platform full of skill sets where plasmids are genetically engineered to include the DNA code for specific antigens chosen for their specificity to, or association with, a disease-causing agent. Found normally in bacteria, plasmids are circular sections of DNA that can be isolated in plentiful amounts, cut and spliced with whatever DNA nucleotide sequences desired. There are only four nitrogenous bases used in DNA, and each is the central molecule that embodies a nucleotide. The four bases are adenine (A), cytosine (C),
Page 6 of 28
BioDecadeEquity Intelligence
thymine (T), or guanine (G) — each of which, combined with a sugar and a phosphate group, comprises a nucleotide. Normally the nucleotides are abbreviated using only the base designation — A, C, T (or U for uracil in RNA), and G.
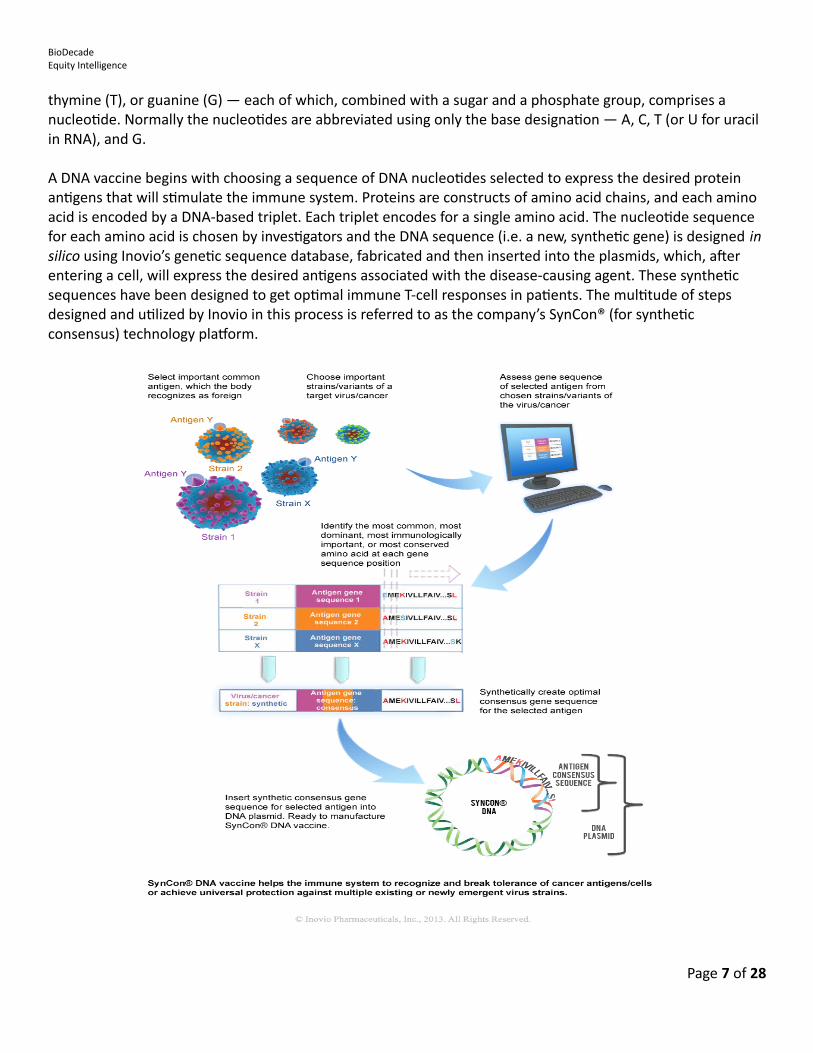
A DNA vaccine begins with choosing a sequence of DNA nucleotides selected to express the desired protein antigens that will stimulate the immune system. Proteins are constructs of amino acid chains, and each amino acid is encoded by a DNA-based triplet. Each triplet encodes for a single amino acid. The nucleotide sequence for each amino acid is chosen by investigators and the DNA sequence (i.e. a new, synthetic gene) is designed insilico using Inovio’s genetic sequence database, fabricated and then inserted into the plasmids, which, after entering a cell, will express the desired antigens associated with the disease-causing agent. These synthetic sequences have been designed to get optimal immune T-cell responses in patients. The multitude of steps designed and utilized by Inovio in this process is referred to as the company’s SynCon® (for synthetic consensus) technology platform.
Page 7 of 28
BioDecadeEquity Intelligence
Indeed, this is how Inovio’s DNA vaccine technology is differentiated from the traditional immunization model. The patient is not given the immunogenic antigen, but is rather given a specific synthetic gene via plasmid. The new gene or genes will express the desired amino acid or protein antigen or multiple protein antigens. These plasmid constructs and expressed antigens must of course be safe for the patient and not in themselves cause disease or off-target severe immunogenic adverse events.
The procedures to create a DNA vaccine begin with choosing the right, or most optimal, targets for a selected disease indication. Investigators select the amino acid sequence required for the antigens, which are chosen because of their importance or their governing capacity in the cellular pathway pathology, or in some cases those that might be the most phylogenetically conserved by evolution. Cancer cells and pathogenic organisms have the ability to mount defenses against therapies that might at first work quite well but then fail due to the ability of tumor cells to mutate and pump out cytotoxic (chemotherapeutic) agents used to treat cancers, or the ability of a bacterium or virus to mutate or modify a single locus in a gene and its expressed protein to prevent an anti-infective from performing its job of killing an infection. Inovio chooses several variants of a tumor or a pathogenic microbe, and then investigators determine the DNA sequence of nucleotides to create agene that will express these faintly dissimilar antigens. The idea here is to use a multi-faceted attack to make it more difficult for the tumor cell or the pathogen to find a workaround solution and surmount the ensuing cellular and antibody assault. Another line of defense in the oncology realm is that tumor cells are capable of masking themselves via checkpoints from the immune system’s surveillance system that screens for foreign substances. This means that tumors can teach themselves to hide from a single-agent assault. Hence, for manyreasons Inovio chooses the multi-antigen, or shotgun, approach to overwhelm the disease.
The end result is that Inovio’s SynCon platform can generate more cross-protective or universal protection against varying and mutating strains of an infectious pathogen, and it can hopefully overcome immune tolerance when it comes to the cancer immunotherapies. The magic is in the DNA sequence of nucleotides. The mammalian immune system has evolved to elicit a T-cell response to counteract foreign and detrimental substances — microbes or tumor cells — that cause devastating disease. The healthy, normally functioning immune surveillance system seeks out these harmful substances.
When the antigens are expressed by the synthetic genes created de novo to elicit an amplified or optimal humoral response, antigen-specific antibodies, as already noted, are one of the immune system’s responses; however, Inovio’s preeminent feature as a research, development, and clinical enterprise is that its gene designs are able to generate a cellular response where antigen-specific T-cells are generated to kill viruses and other infectious agents, as well as tumor cells. DNA immunizations from Inovio’s platform have demonstrated that they can produce antigens that elicit immune responses, including antibodies and robust CD4+ (helper) and especially CD8+ (killer) T-cells, the latter of which is the most critical component of the immune system’s ability to clear tumors and infections. This has already been demonstrated in a phase 2b proof of concept trial with Inovio’s DNA vaccine VGX-3100 in the precancerous cervical intraepithelial neoplasia disease indication.
There are a couple of ways to get a new gene into a cell. One is to give it through a vector, i.e. a non-pathogenic live virus, which will penetrate into cells, embed its gene and induce expression of antigen. A majordrawback of the viral vector is that antibodies will form against the virus itself, and because the vector is deactivated by the antibody, the patient will no longer be able to incorporate the desired gene. Aside from the
Page 8 of 28

BioDecadeEquity Intelligence
virus’ immunogenicity, there are problems associated with being able to reliably manufacture vectors in a predictable, reproducible manner that can be scaled for cost effectiveness.
The other method of getting a new gene into a cell is via the SynCon platform that mimics the vector approach but is devoid of the drawbacks of a viral transfer and delivery system. SynCon technology allows antigen synthesis to occur inside the cells, with no immunogenic viruses entering the cells, and protein synthesis is accomplished via a more natural cellular pathway. The expressed antigens are then sliced and diced into various peptides that will be recognized by the T-cells.
The novel gene-containing plasmids can be thought of as software, while the T-cells, which read the antigens, might be thought of as hardware. SynCon-produced plasmids enter cells with relative ease with the aid of the company’s electroporation system without the risks and consequences of a vector. Inovio’s system incorporates the efficiency of vector gene delivery while eschewing the immunogenicity and associated shutdown of efficacy.
It’s important to note that Inovio’s SynCon-produced genes are not natural products and therefore do not existin the wild, which is the reason they can be protected with intellectual property. Patents are assets that have value on a balance sheet. Moreover, the company has proven to regulators that these synthetic genes cannot replicate themselves and get into the biological ecosystem.
Electroporation delivery
Since the breakthrough characterization of the DNA structure and its configuration by James Watson and Francis Crick in 1953, investigators have thought about how the genome might be altered. As already referenced, viral delivery of nucleic acids — DNA or RNA — brings a set of potential problems, most especially immunogenicity to the virus itself. The therapeutic potential of modifying cellular DNA is vast with nearly any and every type of disease being a candidate for genetic intervention, either in the host patient or in a microbe or tumor cell. But getting genetic material into cells on a wholesale basis with predictability have long been a bottleneck in gene-based therapies. That physical and biochemical barrier figures to be a natural evolutionary protective mechanism because it is not in an organism’s best interest in most cases for foreign materials to enter the cell membrane boundary and cross into the cytoplasm or nucleus.
Page 9 of 28
Inovio's primary intellectual property includes:
SynCon® DNA vaccines in specific disease indications. This includes the gene sequences for the targeted variant antigens. These are human-made products that do not exist in the wild
DNA-based immune activators that include the cytokines — the chemokines and interleukin (IL) molecules, which boost the immune response
Formulations and processing methods Electroporation delivery systems, including the next-generation instruments. These fall under the machine
category of intellectual property Electroporation parameters and methods of application
BioDecadeEquity Intelligence
Inovio’s electroporation expertise has been demonstrated to achieve outstanding DNA vaccine penetration. Electroporation, performed with the company’s Cellectra 5PSP instrument for use with intramuscular injections or the Cellectra 3000 device for use in intradermal injections, involves a millisecond series of electrical pulses. When applied after an injection of the plasmids, these pulses initiate the opening of short-lived pores in cell membranes, which allows for large-volume cellular absorption of plasmids. After the pores close, the cell with its gene processing apparatus allows the injected DNA to encode the protein antigens on the cell surface after which dendritic cells absorb the antigens and carry them to lymph nodes. After that, antibodies, and CD8+ (killer) T-cells and CD4+ (helper) T-cells attack tumor cells or pathogens.
Inovio CELLECTRA® 5PSP Intramuscular Electroporation Delivery Device
Inovio chief Joseph Kim says Inovio has done comparisons with the SynCon DNA versus “plain vanilla” DNA vaccines. The combined technologies of Inovio’s SynCom formulation with electroporation demonstrated a five- to ten-fold higher immune responses in animals1 versus Merck & Co. Inc.’s (NYSE: MRK) viral vector Ad5, which was considered to be the best of the best. Inovio’s intellectual property portfolio is solid, and that includes patents on its Cellectra electroporation devices and the parameters surrounding their use.
Proof of concept of the total package has been achieved and was demonstrated conclusively when the company’s phase 2b, 167-patient, double-blind, randomized, placebo-controlled, multi-site, multinational study demonstrated clinically relevant efficacy where both the cervical dysplasia and human papillomavirus were actually cleared in some of the patients. These data were first reported in a press release on July 23, 2014. Cervical intraepithelial neoplasia (CIN) 2/3 actually resolved to CIN1 or to no disease in 53 of 107 (49.5%)women treated with VGX-3100 compared to 11 of 36 (30.6%) who received placebo. The result is statistically significant (p<0.025).
Page 10 of 28

BioDecadeEquity Intelligence
Optimized delivery of plasmid DNA that encodes green fluorescent protein (GFP)
Page 11 of 28

BioDecadeEquity Intelligence
The combination of the company’s synthetic DNA immunization and electroporation technology has been shown to be both safe and able to produce a reliably efficient immune response in both antibodies and T-cells without immunotoxicity, and more importantly there have been no hyperimmune, e.g. anaphylactic, responsesassociated with re-administration of the immunizations. The ability to re-administer the plasmids enables “booster” shots to enhance or sustain an effect.
1. Hirao, Lauren A, Wu, Ling, Satishchandran, Abhishek, Khan, Amir S., Ruxandra, Draghia-Akl, Ruxandra, Finnefrock, Adam C., Bett, Andrew J., Betts, Michael R., Casimiro, Danilo R., Sardesai, Niranjian Y., Kim, J. Joseph, Shiver, John W., Weiner, David B. (2010). Comparative Analysis of Immune Responses Induced by Vaccination With SIV Antigens by Recombinant Ad5 Vector or Plasmid DNA in Rhesus Macaques. Molecular Therapy 18 8: 1568–1576. doi:10.1038/mt.2010.112
Exciting Product Category in Research
DNA monoclonal antibodies (dMAbs)
One of the most exciting and hopeful research programs at Inovio is its DNA monoclonal antibody (dMAb) initiative. On July 29, 2015 the company announced preclinical proof of concept that its dengue virus-infected mouse models could be 100% protected against a lethal challenge dose of virus. The monoclonal antibody was not given to the mice as an infusion, as is done currently in cancer or autoimmune settings, but rather the animals were given the DNA-encoded plasmids which express the dMAb in vivo. This study is regarded as a major milestone, but because it is so early stage, it is not a value driver for shares.
With the noteworthy exception of Inovio’s phase 1 study of INO-4212 (INO-4201 + INO-4202 + DNA plasmids encoded for monoclonal antibody [dMAb]) as a potential Ebola virus disease therapy, the dMAb program is stillpreclinical. INO-4212 contains a dMAb with Ebola antigens, but this study is in 75 healthy volunteers and is currently a pure safety trial.
This dMAb discussion serves to highlight the versatility and power of the Inovio platform. Antibodies are very difficult and expensive to manufacture, and consistency is a hallmark of current good manufacturing practice (cGMP), but if the antibody could be expressed by the patient’s own cells, in vivo, the obvious efficiencies could render this kind of prophylactic or therapeutic intervention inexpensive and practical in a plethora of diseases and preventive settings, including a plan B-type indication where a patient may have been exposed to a potentially fatal virus but is not yet symptomatic. This has obvious bioterrorism applications — both as a prophylactic and therapeutic applications for many different types of attacks.
It is not unreasonable to suggest that Inovio’s dMAb program could be disruptive in medicine, and could be worth many billions of dollars in revenue and market valuation as a standalone platform. Inovio is currently researching and developing a basket of dMAbs targeting infectious diseases, including Ebola virus disease, dengue virus, influenza, as well as a DARPA-funded drug-resistant bacterial infection program. dMAbs are also potential blockbusters as checkpoint inhibitors in the oncology setting. One might also envision the dMAb as an adjuvant vaccine therapy to prevent recurrences or metastatic activation in at-risk patients.
Page 12 of 28
BioDecadeEquity Intelligence
At Inovio’s current market valuation, think of the dMAb platform as a free call option.
Clinical Pipeline
VGX-3100 (synthetic constructs of DNA plasmids targeting antigenic proteins expressed by E6and E7 oncogenes of HPV Types 16 and 18) Antigens: E6, E7 Disease indication: Cervical intraepithelial neoplasia grade 2/3 (CIN2/3) caused by human papillomavirus
(HPV). CIN2/3 is not cancer, but can become cancer and spread to adjacent tissues if left untreated. Type of intervention: Therapeutic Partners: None, wholly owned by Inovio Milestone ahead: Phase 3 slated to begin around mid-2016 Standard of care therapy: Can include cryotherapy, laser therapy, loop electrosurgical procedure (LEEP) or
cone biopsy to excise or ablate diseased tissue.
A Short History of VGX-3100: Proof of concept phase 2b trial data were released on July 23, 2014 (Press release) Study was published in one of the world’s most prestigious medical journals, Lancet: Safety, efficacy, and
immunogenicity of VGX-3100, a therapeutic synthetic DNA vaccine targeting human papillomavirus 16 and 18 E6 and E7 proteins for cervical intraepithelial neoplasia 2/3: a randomised, double-blind, placebo-controlled phase 2b trial
(NCT01304524) Official title of trial: Phase 2 Placebo Controlled Study of VGX-3100, (HPV16 E6/E7, HPV18 E6/E7 DNA Vaccine) Delivered IM Followed by Electroporation With Cellectra-5P for the Treatment of Biopsy-proven CIN2/3 or CIN3 With Documented HPV 16 or 18.
More than 167 women with cervical intraepithelial neoplasia grades 2 and 3 (CIN2 and CIN3) were in
the study; double-blind (subject + investigator); randomized 3:1 — 75% receiving VGX-3100 and 25% receiving placebo; more than 36 academic and private gynecological sites in seven countries.
Patients in experimental arm (those receiving VGX-3100) of the study were administered three 6 mg doses of VGX-3100 in a 1 ml intramuscular (IM) injection followed by electroporation with Inovio's CELLECTRA® device at weeks 0, 4, and 12.
Patients in the control arm (placebo) of the study received 1 ml of placebo delivered IM followed by electroporation at weeks 0, 4, and 12.
Cervical tissue was examined before starting treatment and nine months later.
VGX-3100 was shown to induce regression of biopsy-proven precancerous cervical intraepithelial neoplasia associated with HPV subtypes 16 or 18.
VGX-3100 was also shown to clear the actual virus (HPV) from the cervical tissues, as well as inducing histopathological regression of the dysplasia to CIN1 or to no disease at all in 43 of 107 (40.2%) of patients receiving the vaccine, versus 5 of 35 patients (14.3%) receiving placebo (p<0.025).
Regression and viral clearance and disease regression are correlated to a vigorous T-cell response.
VGX-3100 is the first therapeutic immunization that has shown efficacy in CIN2/3 linked to HPV-16 and HPV-18. This represents a non-invasive intervention that could change the treatment paradigm for cervical intraepithelial neoplasia (cervical dysplasia).
Page 13 of 28
BioDecadeEquity Intelligence
For investors the bottom line is that VGX-3100 will be a value driver for Inovio Pharmaceuticals, but it also opens to the door to proof of concept that a DNA immunization can be a viable therapeutic option for many other disease indications — oncology, microbial pathogen or combination (e.g. HPV-driven neoplasia) — that are amenable to T-cell activation.
In addition, a successful regulatory pathway for VGX-3100, opens the door to investors being willing to bid up INO shares as value is created in many other disease indications and therapeutic and prophylactic candidates.
INO-3112 (VGX-3100 + synthetic constructs of DNA plasmids encoding interleukin-12 [IL-12]) Antigens: E6, E7 Disease indications: Cervical cancer (HPV-driven) and Head & neck cancer (HPV-driven) Type of intervention: Therapeutic Partners: MedImmune (a unit of AstraZeneca Plc (NYSE: AZN)) and European Organization for Research and
Treatment of Cancer (EORTC) Milestone ahead: Phase 2 trial for HPV-driven cervical cancer in 2016 (sponsored by EORTC) Standard of care therapy:
For cervical cancer: surgical resection, radiation — X-rays or implants in the vaginal cavity, combination chemotherapy and radiation, chemotherapy.
For head and neck cancer: chemotherapy and radiation as well as surgical dissection of lymph nodes of the neck; potential major disfiguring surgical resection of the jaw may also be employed. This leads to very poor quality of life.
A Short History of VGX-3112: Note that VGX-3112 is a combination of VGX-3100 + synthetic constructs of DNA plasmid-encoded
Interleukin-12 (IL-12).
IL-12 has other instructive names that have been used: T-cell stimulating factor (TSF), natural-killer cell stimulatory factor (NKSF), and cytotoxic lymphocyte maturation factor (CLMF).
In mammals cytokines belonging to the IL-12 group are expressed by dendritic cells, macrophages, neutrophils, and human B-lymphoblastoid cells (NC-37) in response to antigenic challenges — bacterial or viral infections.
IL-12 is a very potent immune modulator and has the potential to dramatically enhance immunotherapies.
IL-12 is regarded as particularly applicable as a therapy or adjuvant for HPV-driven cancers, which are particularly capable of generating T-cell responses.
Aside from HPV-driven neoplasia, other highly immunogenic cancers include ovarian, melanoma, breast, and lung.
However, given directly in a drug-like fashion, IL-12 can be toxic and may cause a cascade of cytokines resulting in hyper-elevated levels in the blood stream (a cytokine storm) and can be fatally immunogenic.
INO-3112 entered into a phase 1/2a clinical trial for cervical cancer in Q2/14. MedImmune will now be driving this indication.
Page 14 of 28

BioDecadeEquity Intelligence
(NCT02172911) Official Title: Phase 2/2a, Open-Label, Safety, Tolerability, and Immunogenicity Study of INO-3112 Delivered by Electroporation (EP) in Women With Cervical Cancer After Chemoradiation for Newly Diagnosed Disease or Therapy for Recurrent and/or Persistent Disease
Patients receive a 1.1 ml IM injection of INO-3112 followed immediately by electroporation with CELLECTRA®-5P.
Open label, 30 patients, primary endpoint is safety, secondary endpoints are antigen-specific (T-cell) cellular immune responses and antigen-specific humoral (antibody) responses to HPV-E6 and -E7.
Currently there is no clinical trial data available for INO-3112 in cervical cancer; nevertheless, the vaccine drove robust CD8+ (killer) T-cell responses in 3 out of 4 patients with head and neck cancer linked to HPV subtypes 16 and 18.
The scale and features of the interim data from this trial emulate those earlier seen in subjects receiving VGX-3100 for HPV-associated cervical intraepithelial neoplasia.
April 2019 — final data collection date for primary outcome measure.
INO-3106 (synthetic constructs of DNA plasmids targeting antigenic proteins expressed by E6 and E7 oncogenes) Antigens: E6, E7 Disease indication: Aerodigestive cancer — includes cancers of lips, mouth, tongue, nose, throat, vocal
cords, larynx, esophagus, and trachea Type of intervention: Therapeutic Partners: None, wholly owned Milestones ahead: Pilot study will be completed in 2016. Presumably the company will report data from six
patients in spring or summer of 2016. Standard of care therapy: Any combinations of surgical resection, anti-viral therapy, chemotherapy, and/or
radiation therapy.
A Short History of VGX-3106: There is currently no study data on VGX-3106 A Phase 1 pilot study was begun with VGX-3106 in aerodigestive cancers in May 2014. Collaborator: University of Pennsylvania (NCT02241369) Official Title: Phase 1, Pilot Study of HPV Specific Immunotherapy in Subjects With HPV6
Associated Aerodigestive Malignancies
Open label, 6 patients (2 cohorts)
3 mg of INO-3106 (D0); 6 mg of INO-3106 (Wk3); 6 mg of INO-3106 + 1 mg of INO-9012 (Wk6); 6 mg of INO-3106 + 1 mg of INO-9012 (Wk9);Biological: INO-3106, INO-9012Experimental: Cohort II6 mg of INO-3106 in combination with 1 mg of INO-9012, or at the MTD determined above at day 0, week 3, week 6, week 9.
Patients entering this trial will have exhausted all conventional therapies.
April 2016 — final data collection date for primary outcome measure.
Page 15 of 28

BioDecadeEquity Intelligence
INO-5150 (dual-antigen synthetic construct immune therapy targeting prostate-specific membrane antigen (PSMA) and prostate-specific antigen (PSA)) Antigens: PSA, PSMA Disease indications: Prostate cancer Type of intervention: Therapeutic Partners: None, wholly owned Milestones ahead: Reporting phase 1 interim data in 2016 Standard of care therapy: Surgery, chemotherapy, radiation — X-rays or implants
A Short History of INO-5150: There is currently no human study data on INO-5150 Preclinical data, including in simian, demonstrate vigorous T-cell immune responses. In a murine study,
INO-5150 produced both a potent antibody and T-cell response. (NCT02514213): Official Title Phase I, Open-label Trial to Evaluate the Safety and Immunogenicity of INO-
5150 Alone or in Combination With INO-9012 in Men With Biochemically Relapsed (PSA) Prostate Cancer
60 patients (four cohorts), open-label
Primary endpoint is safety — severe, injection site reactions or lab assays, secondary endpoint is antigen-specific immune response.
February 2017 — final data collection date for primary outcome measure
INO-1400 (synthetic constructs of DNA plasmids encoding human telomerase reverse transcriptase [hTERT]) Antigens: hTERT Disease indications: Multiple oncology indications — breast, lung, pancreatic Type of intervention: Therapeutic Partners: None, wholly owned Collaborator: Abramson Cancer Center of the University of Pennsylvania Milestones ahead: Reporting phase 1 interim data in 2016 Standard of care therapy: Multiple
A Short History of INO-1400: Human telomerase reverse transcriptase (hTERT) protein is expressed in over 85% of cancer types, and as
such is a compelling target in the immune-oncology arena. Non-cancerous cells demonstrate undetectable levels of hTERT. hTERT activates the immune system to induce a CD8+ (killer) T-cell response against tumor cells that
express telomerase. This can result in tumor cell apoptosis (cell death). Inovio CEO Joseph Kim refers to INO-1400 as a potential “universal” cancer therapy.
Page 16 of 28

BioDecadeEquity Intelligence
INO-1400 has been demonstrated to generate an 18-fold higher T-cell concentration than the closest pharma comparator.
(NCT02327468) Official Title: Phase 1 A Study of hTERT Immunotherapy Alone or in Combination With IL12 DNA Followed by Electroporation in Adults With Breast, Lung, or Pancreatic Cancer at High Risk of Relapse Post Definitive Surgery and Adjuvant Therapy
54 patients (six cohorts), open label
Primary endpoint is safety (adverse tissue reactions at injection site; secondary endpoints are time to progression and antigen-specific cellular immune responses
December 2016 — final data collection date for primary outcome measure)
INO-1800 (synthetic constructs of DNA plasmids encoding for multiple hepatitis B antigens) Antigens: Multiple — surface and core Disease indication: Hepatitis B, Clades A&C Type of intervention: Therapeutic Partner: Roche Milestone ahead:
A Short History of INO-1800: Preclinical studies in mice demonstrate generation of a vigorous immune response — both T-cell and
antibody — that destroy targeted liver cells. Phase 1 trial initiated Q2/2015 (NCT02431312) Official Title: Phase I, Randomized, Open-Label, Active-Controlled, Dose Escalation Study to
Evaluate the Safety, Tolerability & Immunogenicity of INO-1800 Alone or in Combination With INO-9112 Delivered IM Followed by EP in Select Nucleos(t)Ide Analogue-Treated, HBeAg+, Chronic Hepatitis B Patients
126 patients, open-label,
Primary endpoint — safety, including pain, adverse events, lab assays, vital signs; Secondary endpoint — immunogenicity assessment at screening and first dose and select points up to 76 weeks after the first dose.
Magnitude of antigen-specific cellular immune responses
November 2017 — final data collection date for primary outcome measure
INO-8000 (synthetic constructs of DNA plasmids encoding for HCV nonstructural proteins 3 (NS3), 4A (NS4A), 4B (NS4B) and 5A (NS5A)) Antigens: NS3/4A, which includes HCV nonstructural proteins 3 (NS3) and 4A (NS4A), as well as NS4B and
NS5A. Disease indication: Hepatitis C virus (HCV) genotypes 1a and 1b Type of intervention: Therapeutic Partners: GeneOne Life Science Inc. (KSE: 011000), an affiliate of Inovio which owns equity in GeneOne.
Page 17 of 28
BioDecadeEquity Intelligence
Milestone ahead: Reporting phase 1 interim data in 2016
A Short History of INO-8000: A therapeutic candidate In preclinical studies, a robust HCV-specific T-cell response was generated in rhesus macaques. This is of
great interest because this observable fact is markedly similar to the phenomenon seen in human patients who have autonomously cleared the virus.
INO-8000 has potential cancer preventive activity No ClinicalTrials.gov protocol listing
PENNVAX®-B (synthetic constructs of DNA plasmids encoding the Gag, Pol, and Env proteins of HIV) Antigens: gag, pol, env Disease indications: HIV uninfected subjects, HIV infected subjects Type of intervention: Prophylactic and Therapeutic Partner: HIV Vaccine Trials Network Collaborator: National Institute of Allergy and Infectious Diseases (NIAID) Milestone ahead:
A Short History of PENNVAX®-B:
35 million people globally are infected with HIV. The developing world is in great need of immunizations to both prevent and treat the infection. Prevention is clearly the most effective means of dealing with HIV. The market for an immunization is vast.
(NCT00991354) Official Title: A Phase 1 Clinical Trial to Evaluate the Safety and Immunogenicity of PENNVAX™-B (Gag, Pol, Env) Vaccine, With or Without IL-12 DNA Plasmid, Delivered Via Electroporation in Healthy, HIV-1-Uninfected Adult Participants
48 patients (subjects), double-blind (subject, investigator)
February 2011 — final data collection date for primary outcome measure
Demonstrated best-in-class immune response
Phase 1 data published July 2013 in the Journal of Infectious Diseases — excellent T-cell responses reported in 89% of phase 1 patients
(NCT01082692) Official Title: A Phase I, Open Label Study to Evaluate the Safety, Tolerability and Immunogenicity of PENNVAX™-B (Gag, Pol, Env) + Electroporation in HIV-1 Infected Adult Participants
12 patients, open-label, conducted at the University of Pennsylvania Medical Center
Patients received a four-dose series of PENNVAX-B each containing 3 mg of DNA/dose administered via IM injection + electroporation at day 0, week 4, week 8 and week 16.
There were no adverse effects.
In March 2012, the company reported that PENNVAX-B induced a significant T-cell response — predominantly antigen-specific CD8+ (killer) T-cells, which is a critical and necessary outcome in order
Page 18 of 28
BioDecadeEquity Intelligence
to clear a chronic viral infection. It also represents a very significant biomarker correlation that can be assayed.
PENNVAX®-G (synthetic constructs of plasmids encoding HIV-1 env A, C, and D, and consensus gag plasmids)
Antigens: env, gag Disease indication: HIV Clades A, C, D Type of intervention: Prophylactic and Therapeutic Partners: United States Military HIV Research Program (USMHRP) / National Institute of Allergy and
Infectious Diseases (NIAID) Milestone ahead:
A Short History PENNVAX®-G:
(NCT01260727) Official Title: A Phase I Study of the Safety and Immunogenicity of PENNVAX-G DNA (ENV &GAG) Administered by Intramuscular Biojector 2000 or CELLECTRA Intramuscular Electroporation Device Followed by MVA-CMDR (HIV-1 CM235 ENV/CM240 GAG/POL) Boost in Healthy, HIV Uninfected Adults
92 patients (six cohorts), double-blind (subject + investigator)
December 2013 — final data collection date for primary outcome measure
Interim data revealed a strong T-cell-mediated immune response, with CD4+ (helper) and CD8+ (killer) T-cells which were specific to both the gag and env antigens encoded by the prime and boost agents. This trial was then extended to three global U.S. Military HIV Research Program sites, which enrolled 80additional healthy (uninfected) subjects in the study.
Interim data show PENNVAX-G + MVA boost achieves 100% antigen-specific T-cell response.
PENNVAX®-GP (synthetic constructs of plasmids encoding HIV-1 env A, B, C, and D)Inovio’s Lead HIV Program
Antigens: gag, pol, env Disease indication: HIV Clades A, B, C, D Type of intervention: Prophylactic and Therapeutic Partners: National Institutes of Health (NIH)/ National Institute of Allergy and Infectious Diseases
(NIAID)/ HIV Vaccine Trials Network (HVTN) Collaborators: University of Pennsylvania, University of Massachusetts, Emory University, and Duke
University Milestone ahead:
A Short History PENNVAX®-GP: PENNVAX-GP is Inovio’s lead HIV DNA vaccine candidate. Designed as a “universal,” multi-clade, multi-antigen immunization to provide coverage against all
major HIV-1 clades. PENNVAX-GP is being developed under a $25 million contract from the NIH.
Page 19 of 28

BioDecadeEquity Intelligence
(NCT02431767) Official Title: A Phase 1 Clinical Trial to Evaluate the Safety and Immunogenicity of PENNVAX®-GP (Gag, Pol, Env) DNA Vaccine and IL-12 Plasmid, Delivered Via Intradermal or Intramuscular Electroporation in Healthy, HIV-Uninfected Adult Participants
94 patients (8 cohorts), double-blind (subject, caregiver, investigator, outcomes assessor)
This trial began in Q3/2015
August 2016 — final data collection date for primary outcome measure
INO-4212 (INO-4201 + INO-4202 + DNA plasmids encoded for monoclonal antibody [dMAb]) INO-4212 (INO-4201 + INO-4202)
INO-4201 (DNA plasmid sequence that encodes for past Ebola Zaire virus outbreak strains) INO-4202 (DNA plasmid sequence that encodes for the current Ebola virus outbreak strain)
Antigens: various Disease indication: Ebola virus disease. Note that the Ebola virus is one of the most dangerous viral
infections known to humankind, and it is lethal in rates of up to 90%. Death can occur within two to 21 days after exposure. There is not currently an approved therapeutic or prophylactic agent for the Ebola infection.
Type of intervention: Prophylactic and Therapeutic Partners: Defense Advanced Research Projects Agency (DARPA) Collaborator: GeneOne Life Science, MedImmune, VGXI, Inc, University of Pennsylvania, Emory University,
and Vanderbilt University. Milestone ahead: Reporting interim phase 1 data Q1/16
A Short History of INO-4212: INO-4212 is being developed with a $45 million grant from DARPA The company also has a preclinical study of DNA monoclonal antibodies, which is also being conducted
under the DARPA grant. In preclinical studies 100% of immunized guinea pigs were protected from death following an Ebola virus
challenge. Investigators detected a significant rise in neutralizing antibody levels with “strong and broad levels of
vaccine-induced T-cells, including "killer" T-cells.” A mouse study using a single vaccination fully protected the animal models from death following an Ebola
virus challenge. Unlike the non-immunized mice, the immunized animals did not experience weight loss. These preclinical data were published in Molecular Therapy in 2013: Induction of Broad Cytotoxic T Cells by
Protective DNA Vaccination Against Marburg and Ebola (NCT02464670) Official Title: Phase 1, Open-Label Study to Evaluate the Safety, Tolerability, and
Immunogenicity of INO-4212 and Its Components, INO-4201 and INO-4202, Given With or Without INO-9012 (DNA sequence encoded for IL-12), Administered IM or ID Followed by Electroporation in Healthy Volunteers 75 subjects (healthy, 5 cohorts), open label December 2016 — final data collection date for primary outcome measure.
Page 20 of 28

BioDecadeEquity Intelligence
Financial StatementsSource: Inovio Pharmaceuticals Q3/15 10Q
INOVIO PHARMACEUTICALS, INC.
CONDENSED CONSOLIDATED BALANCE SHEETS
September 30,
2015 December 31,
2014 (Unaudited)
ASSETS Current assets: Cash and cash equivalents $ 85,468,796 $ 40,543,982Short-term investments 85,313,556 53,075,974Accounts receivable 10,965,273 2,804,207Prepaid expenses and other current assets 1,348,890 797,973Prepaid expenses and other current assets from affiliated entity 634,326 1,382,375Deferred tax asset 342,573 342,573Total current assets 184,073,414 98,947,084Fixed assets, net 6,458,900 4,583,204Investments in affiliated entities 25,321,361 12,340,811Intangible assets, net 4,118,010 4,776,059Goodwill 10,113,371 10,113,371Common stock warrants 88,900 550,000Other assets 597,570 474,568Total assets $ 230,771,526 $ 131,785,097
LIABILITIES AND STOCKHOLDERS’ EQUITY Current liabilities: Accounts payable and accrued expenses $ 10,519,408 $ 6,383,170Accounts payable and accrued expenses due to affiliated entity 2,813,019 28,407Accrued clinical trial expenses 2,942,444 2,007,432Common stock warrants 1,093,752 2,022,729Deferred revenue 188,415 3,187,223Deferred revenue from affiliated entity 523,192 394,791Deferred rent 197,642 —Total current liabilities 18,277,872 14,023,752Deferred revenue, net of current portion 12,798,493 173,779Deferred revenue from affiliated entity, net of current portion 798,532 836,694Deferred rent, net of current portion 5,007,000 4,709,229Deferred tax liabilities 504,049 504,049Total liabilities 37,385,946 20,247,503Inovio Pharmaceuticals, Inc. stockholders’ equity: Common stock 72,181 60,741Additional paid-in capital 532,559,242 443,327,915Accumulated deficit (343,145,851 ) (331,910,290 )
Accumulated other comprehensive income (loss) 3,654,180 (251,390 )Total Inovio Pharmaceuticals, Inc. stockholders’ equity 193,139,752 111,226,976Non-controlling interest 245,828 310,618Total stockholders’ equity 193,385,580 111,537,594Total liabilities and stockholders’ equity $ 230,771,526 $ 131,785,097
Page 21 of 28
BioDecadeEquity Intelligence
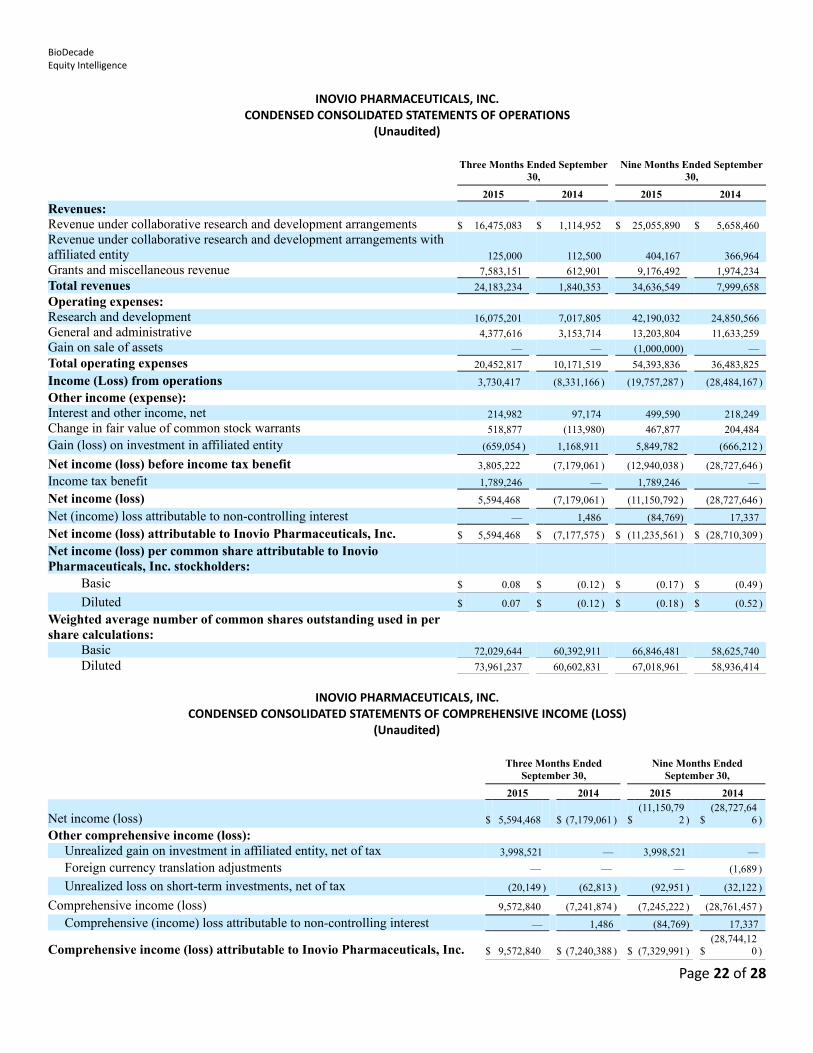
INOVIO PHARMACEUTICALS, INC.CONDENSED CONSOLIDATED STATEMENTS OF OPERATIONS
(Unaudited)
Three Months Ended September
30, Nine Months Ended September
30,
2015 2014 2015 2014
Revenues: Revenue under collaborative research and development arrangements $ 16,475,083 $ 1,114,952 $ 25,055,890 $ 5,658,460Revenue under collaborative research and development arrangements with affiliated entity 125,000 112,500 404,167 366,964Grants and miscellaneous revenue 7,583,151 612,901 9,176,492 1,974,234
Total revenues 24,183,234 1,840,353 34,636,549 7,999,658
Operating expenses: Research and development 16,075,201 7,017,805 42,190,032 24,850,566General and administrative 4,377,616 3,153,714 13,203,804 11,633,259Gain on sale of assets — — (1,000,000) —
Total operating expenses 20,452,817 10,171,519 54,393,836 36,483,825
Income (Loss) from operations 3,730,417 (8,331,166 ) (19,757,287 ) (28,484,167 )
Other income (expense): Interest and other income, net 214,982 97,174 499,590 218,249Change in fair value of common stock warrants 518,877 (113,980) 467,877 204,484
Gain (loss) on investment in affiliated entity (659,054 ) 1,168,911 5,849,782 (666,212 )
Net income (loss) before income tax benefit 3,805,222 (7,179,061 ) (12,940,038 ) (28,727,646 )
Income tax benefit 1,789,246 — 1,789,246 —
Net income (loss) 5,594,468 (7,179,061 ) (11,150,792 ) (28,727,646 )
Net (income) loss attributable to non-controlling interest — 1,486 (84,769) 17,337
Net income (loss) attributable to Inovio Pharmaceuticals, Inc. $ 5,594,468 $ (7,177,575 ) $ (11,235,561 ) $ (28,710,309 )
Net income (loss) per common share attributable to Inovio Pharmaceuticals, Inc. stockholders: Basic $ 0.08 $ (0.12 ) $ (0.17 ) $ (0.49 )
Diluted $ 0.07 $ (0.12 ) $ (0.18 ) $ (0.52 )
Weighted average number of common shares outstanding used in per share calculations: Basic 72,029,644 60,392,911 66,846,481 58,625,740
Diluted 73,961,237 60,602,831 67,018,961 58,936,414
INOVIO PHARMACEUTICALS, INC.CONDENSED CONSOLIDATED STATEMENTS OF COMPREHENSIVE INCOME (LOSS)
(Unaudited)
Three Months Ended
September 30, Nine Months Ended
September 30,
2015 2014 2015 2014
Net income (loss) $ 5,594,468 $ (7,179,061 ) $(11,150,79
2 ) $(28,727,64
6 )
Other comprehensive income (loss): Unrealized gain on investment in affiliated entity, net of tax 3,998,521 — 3,998,521 —
Foreign currency translation adjustments — — — (1,689 )
Unrealized loss on short-term investments, net of tax (20,149 ) (62,813 ) (92,951 ) (32,122 )
Comprehensive income (loss) 9,572,840 (7,241,874 ) (7,245,222 ) (28,761,457 )
Comprehensive (income) loss attributable to non-controlling interest — 1,486 (84,769) 17,337
Comprehensive income (loss) attributable to Inovio Pharmaceuticals, Inc. $ 9,572,840 $ (7,240,388 ) $ (7,329,991 ) $(28,744,12
0 )
Page 22 of 28
BioDecadeEquity Intelligence
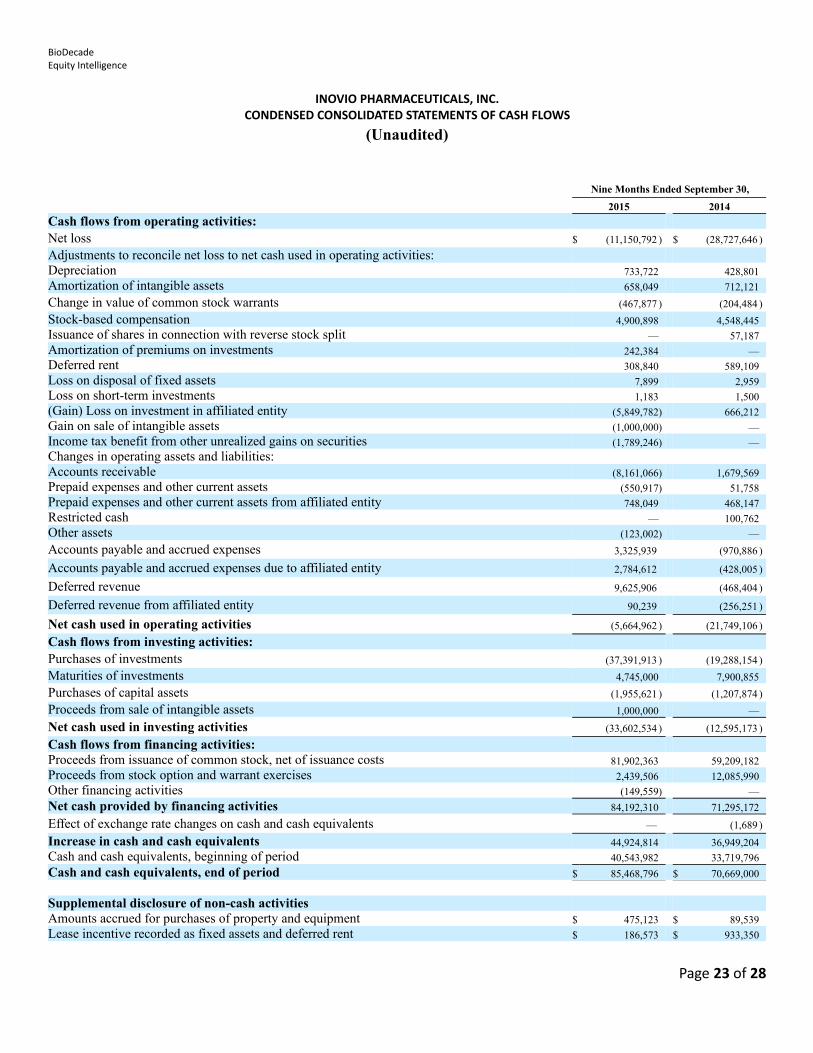
INOVIO PHARMACEUTICALS, INC.CONDENSED CONSOLIDATED STATEMENTS OF CASH FLOWS
(Unaudited)
Nine Months Ended September 30,
2015 2014
Cash flows from operating activities: Net loss $ (11,150,792 ) $ (28,727,646 )
Adjustments to reconcile net loss to net cash used in operating activities: Depreciation 733,722 428,801Amortization of intangible assets 658,049 712,121
Change in value of common stock warrants (467,877 ) (204,484 )
Stock-based compensation 4,900,898 4,548,445Issuance of shares in connection with reverse stock split — 57,187Amortization of premiums on investments 242,384 —Deferred rent 308,840 589,109Loss on disposal of fixed assets 7,899 2,959Loss on short-term investments 1,183 1,500(Gain) Loss on investment in affiliated entity (5,849,782) 666,212Gain on sale of intangible assets (1,000,000) —Income tax benefit from other unrealized gains on securities (1,789,246) —Changes in operating assets and liabilities: Accounts receivable (8,161,066) 1,679,569Prepaid expenses and other current assets (550,917) 51,758Prepaid expenses and other current assets from affiliated entity 748,049 468,147Restricted cash — 100,762Other assets (123,002) —
Accounts payable and accrued expenses 3,325,939 (970,886 )
Accounts payable and accrued expenses due to affiliated entity 2,784,612 (428,005 )
Deferred revenue 9,625,906 (468,404 )
Deferred revenue from affiliated entity 90,239 (256,251 )
Net cash used in operating activities (5,664,962 ) (21,749,106 )
Cash flows from investing activities: Purchases of investments (37,391,913 ) (19,288,154 )
Maturities of investments 4,745,000 7,900,855
Purchases of capital assets (1,955,621 ) (1,207,874 )
Proceeds from sale of intangible assets 1,000,000 —
Net cash used in investing activities (33,602,534 ) (12,595,173 )
Cash flows from financing activities: Proceeds from issuance of common stock, net of issuance costs 81,902,363 59,209,182Proceeds from stock option and warrant exercises 2,439,506 12,085,990Other financing activities (149,559) —
Net cash provided by financing activities 84,192,310 71,295,172
Effect of exchange rate changes on cash and cash equivalents — (1,689 )
Increase in cash and cash equivalents 44,924,814 36,949,204Cash and cash equivalents, beginning of period 40,543,982 33,719,796
Cash and cash equivalents, end of period $ 85,468,796 $ 70,669,000
Supplemental disclosure of non-cash activities Amounts accrued for purchases of property and equipment $ 475,123 $ 89,539Lease incentive recorded as fixed assets and deferred rent $ 186,573 $ 933,350
Page 23 of 28
BioDecadeEquity Intelligence
Management
J. Joseph Kim, Ph.D.President, Chief Executive Officer, Director
JOSEPH KIM was appointed President and CEO of Inovio Pharmaceuticals in June 2009. Dr. Kim co-founded VGX Pharmaceuticals, a synthetic vaccine company, in 2000 to develop intellectual property related to immunotherapeutics licensed from the University of Pennsylvania. He led that company for nine years and combined VGX with Inovio Biomedical in 2009 to form Inovio Pharmaceuticals. Previously, Dr. Kim was a senior vaccine developer at Merck & Co. where he successfully led efforts in manufacturing and process development for several FDA-approved products for hepatitis and developmental vaccines and therapeutics for HIV/AIDS.
Dr. Kim earned a Bachelor of Science degree in Chemical Engineering and Economics from the Massachusetts Institute of Technology (MIT), where he was a U.S. Senate Honors Scholar. He holds a PhD in Biochemical Engineering from the University of Pennsylvania and a Master of Business Administration degree in Finance from the Wharton School. Dr. Kim has published more than 100 peer-reviewed scientific papers, holds numerous patents, and sits on several editorial boards and review panels.
Dr. Kim has been recognized with numerous honors in the past several years, including:
2002: MIT's Technology Review, one of the world's Top 100 Young Innovators
2002: Philadelphia Business Journal, one of "40 under 40" dynamic professionals
2003 & 2006: Details Magazine, selected as one of "50 Most Influential Men"
2004:World Economic Forum, selection of Dr. Kim and VGX Pharmaceuticals as one of 30 Technology Pioneers
2005:Newsweek International, profiled in annual "Who's Next" issue as one of 10 leaders, scientists, and executives at the forefront of change and impact in the world
2006:Forum of Young Global Leaders, an affiliate of the World Economic Forum, named a Young Global Leader among 175 leading executives, public figures and intellectuals under the age of 40 from 50 countries.
2012:Member, The Global Agenda Council of the World Economic Forum;Life Sciences CEO of the Year
2013:Board of Trustees, International Vaccine Institute;Achievement in Drug Discovery and Development Award from the Korean American Society in Biotech and Pharmaceuticals
2015:Member, Aspen Institute Health Innovators FellowshipA group of 20 healthcare leaders challenged to generate new solutions to improvehealthcare treatments, access and delivery
2015: Entrepreneur of the Year for Greater Philadelphia; selected by Ernst & Young
Page 24 of 28

BioDecadeEquity Intelligence
Peter KiesChief Financial Officer
PETER KIES has been Chief Financial Officer of Inovio since 2002. During the prior 16 years, Mr. Kies acquired broad expertise in the functional and strategic management of biotechnology and high technology companies across the full spectrum of corporate growth, from IPO to profitability. He was previously Chief Financial Officer at Newgen Results Corporation and held positions at Cytel Corporation and Ernst & Young, LLP. Mr. Kies holds a Bachelor of Science degree in Business Administration from United States International University in San Diego, California.
Niranjan Y. Sardesai, Ph.D.Chief Operating Officer
NIRANJAN Y. SARDESAI was appointed Chief Operating Officer of Inovio in January 2012. He served as the Company’s Senior Vice President of Research and Development following the June 2009 merger with VGX Pharmaceuticals, at which company he held the same position. Dr. Sardesai joined VGX Pharmaceuticals in 2006 where he helped formulate the company’s product development and growth strategies and reorganized the company into a DNA vaccine and immunotherapies company. Across VGX and Inovio, Dr. Sardesai drove multiple M&A and licensing transactions to consolidate key technologies, establish the corporate footprint, anddevelop its immunotherapies platform and product pipeline. He led the strategic out-licensing of Inovio’s pipeline products to secure major licensing deals with big pharma companies. He has raised over $130 MM in non-dilutive grants and contract funding from government and non-government organizations and served as Principal Investigator on multi-institutional programs developing Inovio’s oncology and infectious disease products. Under his leadership, Inovio’s development stage products have been recognized by several pharmaceutical industry awards for innovation and the potential to address significant unmet needs.
Dr. Sardesai was previously the founder and President of NVision Consulting Inc., a firm providing strategic counsel to entrepreneurial life sciences companies. He served as Director of Research and Development at Fujirebio Diagnostics, Inc., where he oversaw the expansion of the company’s oncology portfolio. Products developed under his leadership include groundbreaking new tests for mesothelioma (MESOMARK™), bladder cancer and a multi-marker test for ovarian cancer.
Dr. Sardesai received a Ph.D. in Chemistry from the California Institute of Technology and an MBA (entrepreneurship and finance) from the Wharton School of the University of Pennsylvania, where he was the recipient of the Shils-Zeidman Award in Entrepreneurship. He was awarded fellowships at the Scripps Research Institute and the Massachusetts Institute of Technology (MIT). Dr. Sardesai received his Bachelor and Master of Science degrees in Chemistry from the Indian Institute of Technology, Bombay. He has authored over 100+ peer-reviewed manuscripts and book chapters with particular contributions in vaccines and immunotherapies, oncology, and medical devices; presented at over 120+ invited lectures and presentations, and filed several patents. Dr. Sardesai was recently recognized by Pharmavoice magazine as one of the top 100 most influential and inspirational leaders from across the life sciences and healthcare industry (2015).
Page 25 of 28
BioDecadeEquity Intelligence
Mark L. Bagarazzi, M.D.Chief Medical Officer
MARK L. BAGARAZZI joined Inovio Pharmaceuticals as Chief Medical Officer in January 2010 where he has responsibility for all clinical development and regulatory activities. Prior to joining Inovio, Dr. Bagarazzi was director of Worldwide Regulatory Affairs for Vaccines and Biologics at Merck Research Laboratories where he was responsible for the licensure of RotaTeq™ and led the development team for Merck’s vaccine for the prevention of herpes zoster (shingles), ZOSTAVAX™. Dr. Bagarazzi was an assistant professor of pediatrics at Drexel College of Medicine where he served as director of the pediatric HIV/AIDS program at St. Christopher’s Hospital for Children. He is a guest lecturer on vaccines and immunotherapeutics at the Perelman School of Medicine at the University of Pennsylvania and had previously been a guest lecturer at Johns Hopkins University.
Dr. Bagarazzi completed his pediatric residency at St. Christopher’s Hospital for Children and completed a fellowship in pediatric infectious diseases at the Children’s Hospital of Philadelphia. He was board certified in both Pediatrics and Pediatric Infectious Diseases. He has authored or co-authored dozens of scientific papers focused on the subject of DNA vaccines that have been published in peer-reviewed medical journals. Dr. Bagarazzi received his M.D. degree with honors from New Jersey Medical School of the University of Medicine and Dentistry of New Jersey and holds a B.S. in Electrical Engineering magna cum laude from New Jersey Institute of Technology.
Scott M. White, M.D.Vice President, Clinical Development
SCOTT M. WHITE joined Inovio Pharmaceuticals as Vice President, Clinical Development in February 2015 where he has responsibility for the clinical development of the infectious diseases portfolio. Prior to joining Inovio he was a Senior Director with GlaxoSmithKline where he had led the worldwide clinical development of several products spanning antibacterial, antiviral, hematologic, and dermatologic therapeutic areas. In 2012 hewas the industry project leader for the design and establishment of the COMBACTE EU Clinical Trial Network for antibacterial agents funded through the Innovative Medicines Initiative public private partnership program.Dr. White was an assistant professor of medicine at the University Of Pittsburgh School Of Medicine and the Baylor College of Medicine where he led NIH-funded research into the role of hematopoietic growth factors in normal and pathologic blood cell development and function.
Dr. White completed his internal medicine residency at the Hershey Medical Center and subsequent infectious diseases fellowship at the University of Pittsburgh. He has authored and co-authored several scientific papers on the topics of hematopoietic growth factors driving neoplastic transformation of blood and solid organ cells, as well as a textbook chapters regarding bacterial resistance, transplant infectious diseases and hematopoietic growth factors. Dr. White received his M.D. from the Pennsylvania State University College of Medicine and his B.S. with Honors from the Pennsylvania State University.
Page 26 of 28
BioDecadeEquity Intelligence
Zane Yang, M.D.Vice President, Clinical Development, Oncology
ZANE YANG joined Inovio as Vice President, Clinical Development, Oncology in December 2014 where he has responsibility for advancing Inovio's oncology portfolio of DNA immunotherapies through clinical trials to commercialization. Dr. Yang joins Inovio from Janssen Pharmaceuticals where he was Director, Oncology Medical Affairs in the U.S. Dr. Yang led the prostate cancer and solid tumor therapeutic area including development and commercialization of Zytiga®, for the treatment of metastatic castration-resistant prostate cancer. Prior to Janssen, he was Director of Global Medical Affairs and Clinical Development at Novartis Oncology, and Director of Clinical Development at Merck & Co.
Dr. Yang, who earned his M.D. at Beijing Medical University, was a Fellow at Emory University's Winship CancerInstitute and the Wistar Institute. Before transitioning to the pharmaceutical industry he was an associate professor at the University of Virginia Medical Center.
Risk factors There is inherent risk in owning shares of a development-stage biotechnology company. There is market risk in owning equity shares. Volatility is dependent on general market conditions as well as
fundamental data generated by the company. As of September 30, 2015 Inovio’s accumulated deficit was approximately $343.1 million. The company will continue
to sustain considerable operating losses for at least the next several years as it moves through the drug developmentprocess for its lead candidate VGX-3100 and others.
Limited revenues emanate from out-licensing and grants, as well as very limited interest income from short-term instruments on the balance sheet, but there are no revenues being generated from product sales.
Q3/15 was a profitable quarter driven by the MedImmune partnership deal for INO-3112 in cervical cancer and the cash infusion. This will not be the rule, and there are no meaningful revenues are being generated currently.
Inovio is a speculative, early-stage company that is dependent on successes in clinical trials and U.S. and foreign regulatory approvals of its synthetic DNA vaccines, a new technology that has never been commercialized before.
Proof-of-concept and statistically significant scientific proofs in clinical trials must be demonstrated to be repeatable. This may in some cases require additional capital, additional pivotal trials, and additional years of development.
Enrollment in clinical trials may be delayed. Major adverse events, including death of a subject, could occur during clinical trials, at which time the FDA could
place any human trial on hold for an indefinite period while the cause of the event is determined. After pivotal data are submitted in a new drug application (NDA) or biologic license application (BLA), the FDA or
foreign regulatory body could decide that the trial was not powered well enough to show statistical significance. There can be no assurances of clinical and regulatory successes or that any vaccine product or electroporation device
will ever be approved for sale. The company’s continued operation and drug research and development are dependent on its ability to raise debt
and equity capital or to partner its programs. If products are approved, there must be a successful marketing campaign waged by Inovio or a partner. There can be
no assurances that a partner will invest in a campaign and devote adequate resources to a successful marketing program.
Page 27 of 28
BioDecadeEquity Intelligence
FDA-approved products do sometimes fail in the marketplace for a variety of reasons, which may include competitiveforces or/and lack of acceptance.
Product labeling must be approved by the FDA. This includes the specific disease indication and if a product must be held for second or third line use. At times labeling may be less favorable for the product developer, sponsor, or marketing company than was predicted in financial models.
After a product is approved, safety signals could arise as large numbers of patients begin receiving the commercially marketed drug or vaccine.
Intellectual property, especially patents, could be challenged after a product is approved. Defending a patent could be a significant expense and could drain resources and focus from aspects of company operation.
Risks are not limited to these mentioned above.
Dr. George S. MackManaging [email protected]
Page 28 of 28