bianca moses fall 2013. -lol β-blockers for the treatment of the symptoms of attack by...
TRANSCRIPT

Bianca Moses Fall 2013

-LOL

-LOLβ-Blockers

For the treatment of the symptoms of attack by ostriches…and other ailments; including
those of the cardio-pulmonary tract
-LOLβ-Blockers

For the treatment of the symptoms of attack by ostriches…and other ailments; including
those of the cardio-pulmonary tract
-LOLβ-Blockers

For the treatment of the symptoms of attack by ostriches…and other ailments; including
those of the cardio-pulmonary tract
-LOLβ-Blockers

For the treatment of the symptoms of attack by ostriches…and other ailments; including
those of the cardio-pulmonary tract
-LOLβ-Blockers

For the treatment of the symptoms of attack by ostriches…and other ailments; including
those of the cardio-pulmonary tract
-LOLβ-Blockers

-LOLβ-Blockers
Ateno
For the treatment of the symptoms of attack by ostriches…and other ailments; including
those of the cardio-pulmonary tract

-LOLβ-Blockers
Atenolol
For the treatment of the symptoms of attack by ostriches…and other ailments; including
those of the cardio-pulmonary tract

-LOLβ-Blockers
Atenolol
Carvedi
For the treatment of the symptoms of attack by ostriches…and other ailments; including
those of the cardio-pulmonary tract

-LOLβ-Blockers
Atenolol
Carvedilol
For the treatment of the symptoms of attack by ostriches…and other ailments; including
those of the cardio-pulmonary tract

-LOLβ-Blockers
Atenolol
Carvedilol
Timo
For the treatment of the symptoms of attack by ostriches…and other ailments; including
those of the cardio-pulmonary tract

-LOLβ-Blockers
Atenolol
Carvedilol
Timolol
For the treatment of the symptoms of attack by ostriches…and other ailments; including
those of the cardio-pulmonary tract

-LOLβ-Blockers
Atenolol
Carvedilol
Timolol
Metopra
For the treatment of the symptoms of attack by ostriches…and other ailments; including
those of the cardio-pulmonary tract

-LOLβ-Blockers
Atenolol
Carvedilol
Timolol
Metopralol
For the treatment of the symptoms of attack by ostriches…and other ailments; including
those of the cardio-pulmonary tract
-LOLβ-Blockers
Atenolol
Carvedilol
Timolol
Metopralol
Proprano
For the treatment of the symptoms of attack by ostriches…and other ailments; including
those of the cardio-pulmonary tract

-LOLβ-Blockers
Atenolol
Carvedilol
Timolol
Metopralol
Propranolol
For the treatment of the symptoms of attack by ostriches…and other ailments; including
those of the cardio-pulmonary tract

-LOLβ-Blockers
Atenolol
Carvedilol
Timolol
Metopralol
Propranolol
and more…
For the treatment of the symptoms of attack by ostriches…and other ailments; including
those of the cardio-pulmonary tract

-LOLβ-Blockers
Atenolol
Carvedilol
Timolol
Metopralol
Propranolol
and more…
-LOL
For the treatment of the symptoms of attack by ostriches…and other ailments; including
those of the cardio-pulmonary tract

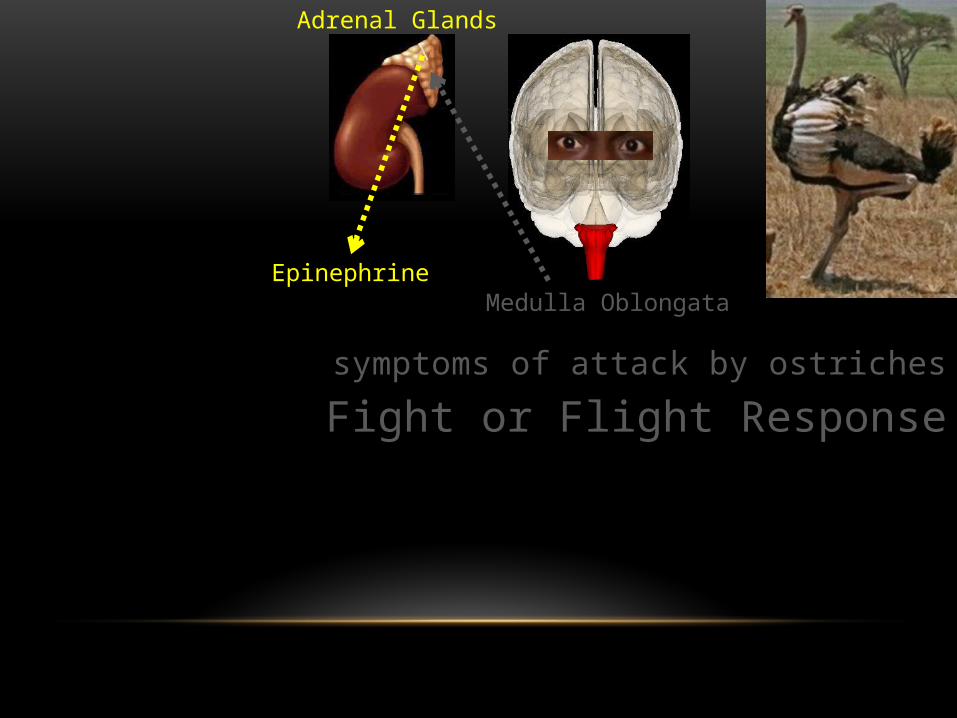
symptoms of attack by ostriches

symptoms of attack by ostriches

symptoms of attack by ostriches

symptoms of attack by ostriches

symptoms of attack by ostriches

symptoms of attack by ostriches
Medulla Oblongata

symptoms of attack by ostriches
Medulla Oblongata
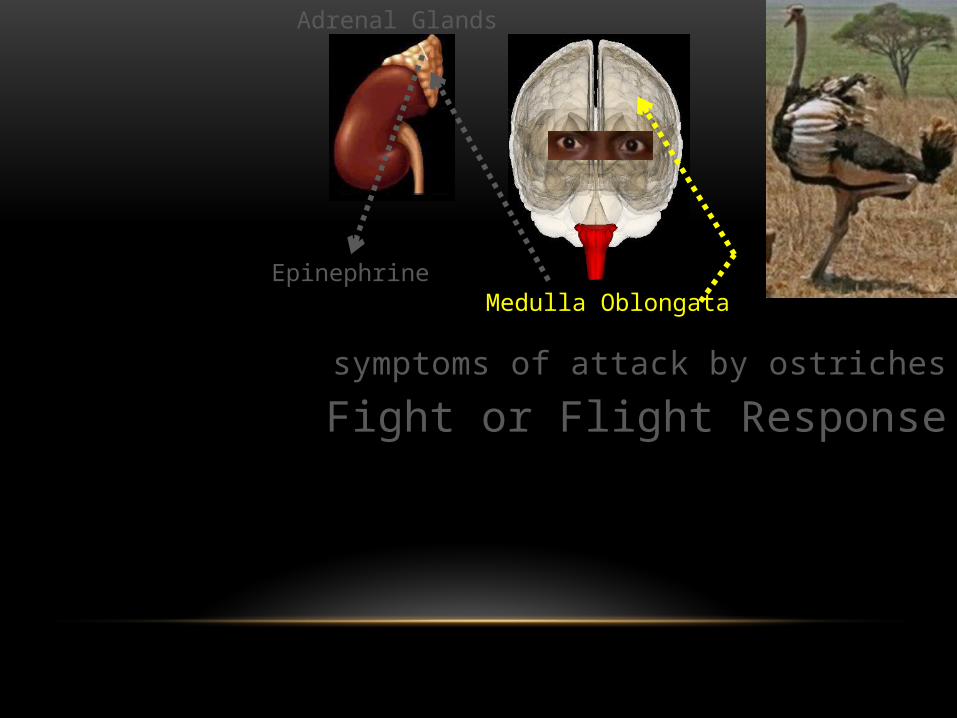
Fight or Flight Response

symptoms of attack by ostriches
Medulla Oblongata
Fight or Flight Response

symptoms of attack by ostriches
Medulla Oblongata
Adrenal Glands
Fight or Flight Response

symptoms of attack by ostriches
Medulla Oblongata
Adrenal Glands
Fight or Flight Response
symptoms of attack by ostriches
Medulla Oblongata
Adrenal Glands
Fight or Flight Response
Epinephrine

symptoms of attack by ostriches
Medulla Oblongata
Adrenal Glands
Fight or Flight Response
Epinephrine
symptoms of attack by ostriches
Medulla Oblongata
Adrenal Glands
Fight or Flight Response
Epinephrine

symptoms of attack by ostriches
Medulla Oblongata
Adrenal Glands
Fight or Flight Response
Epinephrine
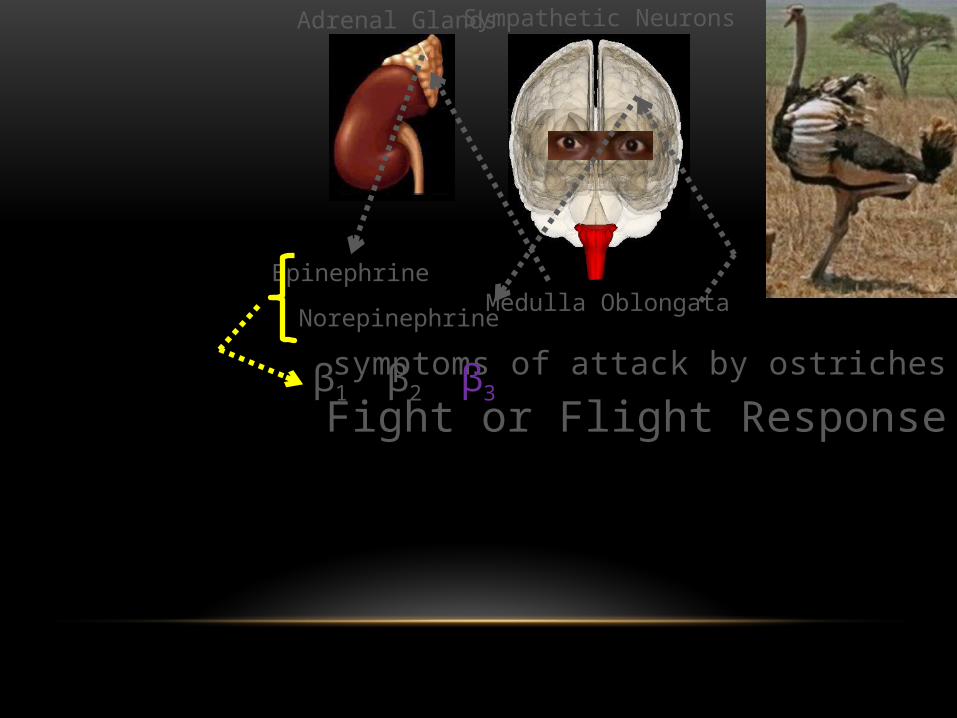
Sympathetic Neurons

symptoms of attack by ostriches
Medulla Oblongata
Adrenal Glands
Fight or Flight Response
Epinephrine
Sympathetic Neurons

symptoms of attack by ostriches
Medulla Oblongata
Adrenal Glands
Fight or Flight Response
Epinephrine
Sympathetic Neurons
Norepinephrine

symptoms of attack by ostriches
Medulla Oblongata
Adrenal Glands
Fight or Flight Response
Epinephrine
Sympathetic Neurons
Norepinephrine

symptoms of attack by ostriches
Medulla Oblongata
Adrenal Glands
Fight or Flight Response
Epinephrine
Sympathetic Neurons
Norepinephrine

symptoms of attack by ostriches
Medulla Oblongata
Adrenal Glands
Fight or Flight Response
Epinephrine
Sympathetic Neurons
Norepinephrine
β1

symptoms of attack by ostriches
Medulla Oblongata
Adrenal Glands
Fight or Flight Response
Epinephrine
Sympathetic Neurons
Norepinephrine
β1 β2
symptoms of attack by ostriches
Medulla Oblongata
Adrenal Glands
Fight or Flight Response
Epinephrine
Sympathetic Neurons
Norepinephrine
β1 β2 β3

β1 β2 β3Ep
inep
hrin
e
Nore
pine
phrin
e
Epin
ephr
ine
Nore
pine
phrin
e
Epin
ephr
ine
Nore
pine
phrin
e

β1 β2 β3Ep
inep
hrin
e
Nore
pine
phrin
e
Epin
ephr
ine
Nore
pine
phrin
e
Epin
ephr
ine
Nore
pine
phrin
e

β1 β2 β3Ep
inep
hrin
e
Nore
pine
phrin
e
Epin
ephr
ine
Nore
pine
phrin
e
Epin
ephr
ine
Nore
pine
phrin
eFight or Flight
Response Initiated

β-Blockers

β1 β2 β3
β-Blockers
β1 β2 β3
β-Blockers

β1 β2 β3
β-Blockers
Epin
ephr
ine
Nore
pine
phrin
e

β1 β2 β3
↑ ♥ Rate (Chronotropic)
↑ ♥ Force (Inotropic)
↑ ♥ Automaticity (How well ♥ cells initiate their own impulse)
↑ ♥ Output (Cardiac Output)
PUMP THAT BLOOD!!! MOVE THAT O2 NOW!!!

β1 β2 β3
↑ ♥ Rate (Chronotropic)
↑ ♥ Force (Inotropic)
↑ ♥ Automaticity (How well ♥ cells initiate their own impulse)
↑ ♥ Output (Cardiac Output)
PUMP THAT BLOOD!!! MOVE THAT O2 NOW!!!

β1 β2 β3
↑ ♥ Rate (Chronotropic)
↑ ♥ Force (Inotropic)
↑ ♥ Automaticity (How well ♥ cells initiate their own impulse)
↑ ♥ Output (Cardiac Output)

β1 β2 β3
↑ ♥ Rate (Chronotropic)
↑ ♥ Force (Inotropic)
↑ ♥ Automaticity (How well ♥ cells initiate their own impulse)
↑ ♥ Output (Cardiac Output)

β1 β2 β3
Not as much effect as β1 stimulation however
↑ ♥ Rate (Chronotropic)
↑ ♥ Force (Inotropic)
↑ ♥ Automaticity (How well ♥ cells initiate their own impulse)
↑ ♥ Output (Cardiac Output)

β1 β2 β3
Not as much effect as β1 stimulation however
↑ ♥ Rate (Chronotropic)
↑ ♥ Force (Inotropic)
↑ ♥ Automaticity (How well ♥ cells initiate their own impulse)
↑ ♥ Output (Cardiac Output)

β1 β2 β3
↑ ♥ Rate (Chronotropic)
↑ ♥ Force (Inotropic)
↑ ♥ Automaticity (How well ♥ cells initiate their own impulse)
↑ ♥ Output (Cardiac Output)

β1 β2 β3
Smooth Muscle Constriction

β1 β2 β3
Central Arterial Constriction
=↑ Blood Pressure
=↑ Blood + O2 to essential
organs
Smooth Muscle Constriction

β1 β2 β3
Central Arterial Constriction
=↑ Blood Pressure
=↑ Blood + O2 to essential
organs
Smooth Muscle Constriction
Constriction of Vessels of non essential organs(ie. Less blood to gut)
=Less digesting

β1 β2 β3
Smooth Muscle Relaxation
Central Arterial Constriction
=↑ Blood Pressure
=↑ Blood + O2 to essential
organs
Smooth Muscle Constriction
Constriction of Vessels of non essential organs(ie. Less blood to gut)
=Less digesting

β1 β2 β3
Smooth Muscle Relaxation
Airways Relax=
More air with each breath=
↑ oxygenation
Central Arterial Constriction
=↑ Blood Pressure
=↑ Blood + O2 to essential
organs
Smooth Muscle Constriction
Constriction of Vessels of non essential organs(ie. Less blood to gut)
=Less digesting

β1 β2 β3
Smooth Muscle Relaxation
Airways Relax=
More air with each breath=
↑ oxygenation
Central Arterial Constriction
=↑ Blood Pressure
=↑ Blood + O2 to essential
organs
Smooth Muscle Constriction
Sweat =
Dissipate Heat
= Cools off
body
Constriction of Vessels of non essential organs(ie. Less blood to gut)
=Less digesting

β1 β2 β3
Smooth Muscle Relaxation
Airways Relax=
More air with each breath=
↑ oxygenation
Central Arterial Constriction
=↑ Blood Pressure
=↑ Blood + O2 to essential
organs
Smooth Muscle Constriction
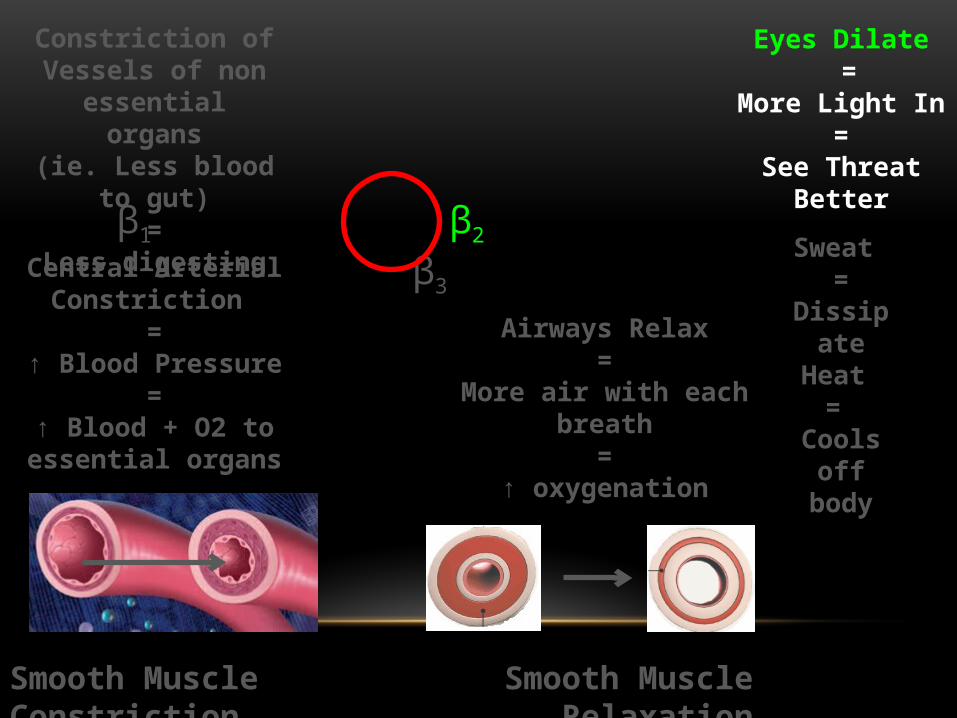
Eyes Dilate =
More Light In=
See Threat Better
Sweat =
Dissipate Heat
= Cools off
body
Constriction of Vessels of non essential organs(ie. Less blood to gut)
=Less digesting
β1 β2 β3
Smooth Muscle Relaxation
Airways Relax=
More air with each breath=
↑ oxygenation
Central Arterial Constriction
=↑ Blood Pressure
=↑ Blood + O2 to essential
organs
Smooth Muscle Constriction
Eyes Dilate =
More Light In=
See Threat Better
Sweat =
Dissipate Heat
= Cools off
body
Constriction of Vessels of non essential organs(ie. Less blood to gut)
=Less digesting

β1 β2 β3
Smooth Muscle Relaxation
Constriction of Vessels of non essential organs(ie. Less blood to gut)
=Less digesting
Airways Relax=
More air with each breath=
↑ oxygenation
Central Arterial Constriction
=↑ Blood Pressure
=↑ Blood + O2 to essential
organs
Smooth Muscle Constriction
Eyes Dilate =
More Light In=
See Threat Better
Sweat =
Dissipate Heat
= Cools off
body

β1 β2 β3
Brown Fat

β1 β2 β3
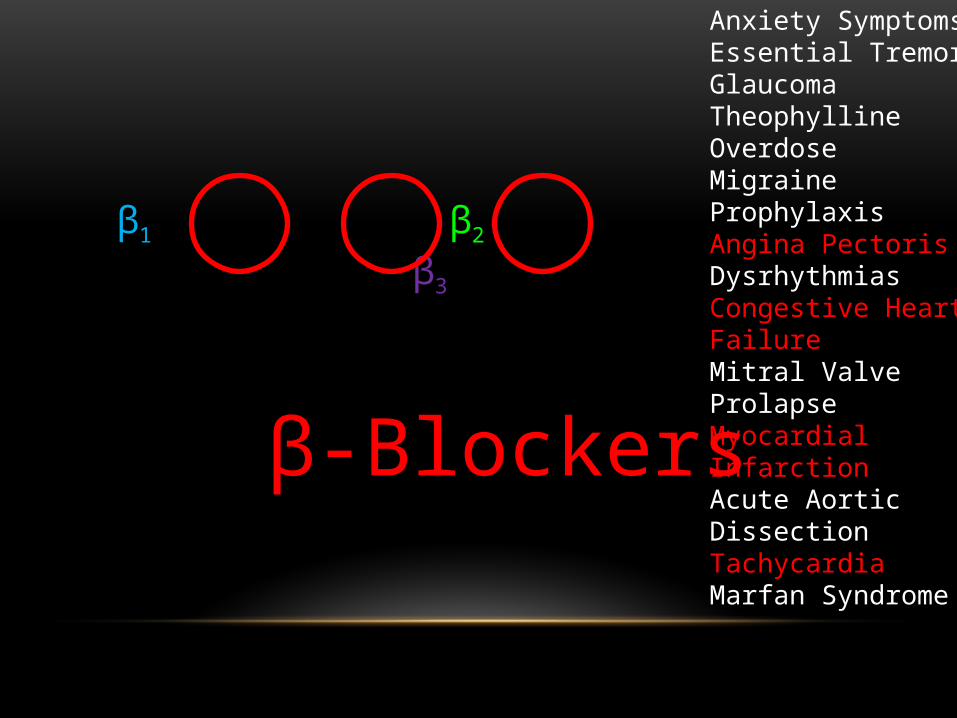
β-Blockers
Anxiety SymptomsEssential TremorGlaucomaTheophylline OverdoseMigraine ProphylaxisAngina PectorisDysrhythmiasCongestive Heart FailureMitral Valve ProlapseMyocardial InfarctionAcute Aortic DissectionTachycardia Marfan Syndrome
β1 β2 β3
β-Blockers
Anxiety SymptomsEssential TremorGlaucomaTheophylline OverdoseMigraine ProphylaxisAngina PectorisDysrhythmiasCongestive Heart FailureMitral Valve ProlapseMyocardial InfarctionAcute Aortic DissectionTachycardia Marfan Syndrome

β1 β2 β3
β-Blockers
Use With Caution In

β1 β2 β3
β-Blockers
Use With Caution InRenal ImpairmentHepatic Impairment

β1 β2 β3
β-Blockers
Use With Caution InRenal ImpairmentHepatic Impairment Metabolized by liver and excreted by kidneys

β1 β2 β3
β-Blockers
Use With Caution InRenal ImpairmentHepatic ImpairmentDiabetes Mellitus

β1 β2 β3
β-Blockers
Use With Caution InRenal ImpairmentHepatic ImpairmentDiabetes Mellitus
β-blockers mask hypoglycemia symptoms

β1 β2 β3
β-Blockers
Use With Caution InRenal ImpairmentHepatic ImpairmentDiabetes Mellitus Geriatrics

β1 β2 β3
β-Blockers
Use With Caution InRenal ImpairmentHepatic ImpairmentDiabetes Mellitus Geriatrics
Enhanced effects

β1 β2 β3
β-Blockers
Use With Caution InRenal ImpairmentHepatic ImpairmentDiabetes MellitusGeriatricsAsthma Patients
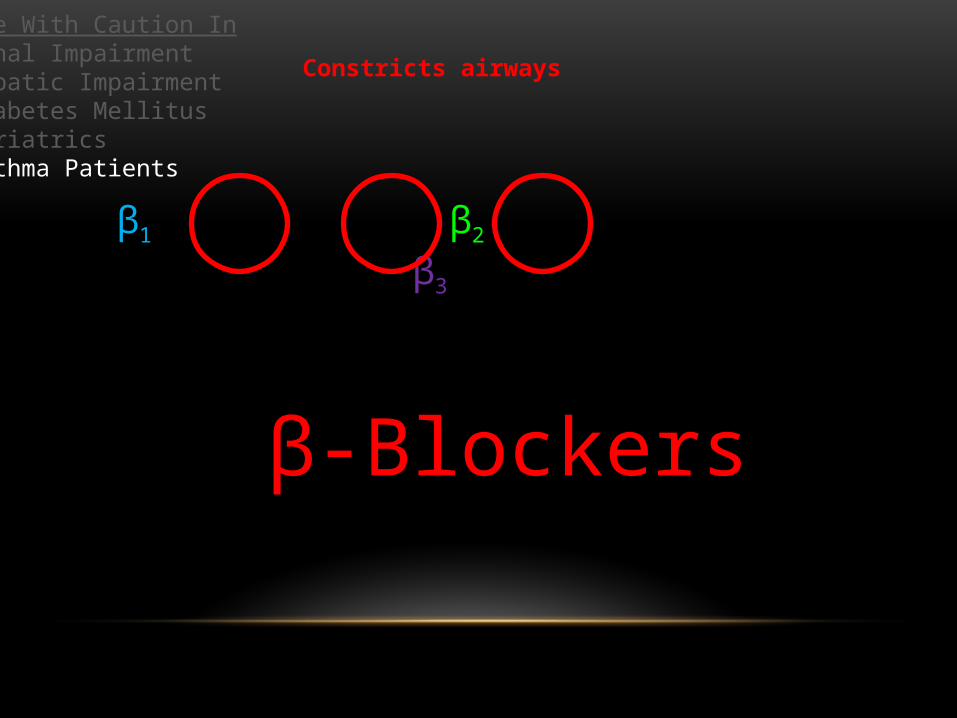
β1 β2 β3
β-Blockers
Use With Caution InRenal ImpairmentHepatic ImpairmentDiabetes MellitusGeriatricsAsthma Patients
Constricts airways

β1 β2 β3
β-Blockers
Contraindications
Use With Caution InRenal ImpairmentHepatic ImpairmentDiabetes MellitusGeriatricsAsthma Patients

β1 β2 β3
β-Blockers
ContraindicationsUncompensated CHFPulmonary edemaCardiogenic shockBradycardiaHeart Block
Use With Caution InRenal ImpairmentHepatic ImpairmentDiabetes MellitusGeriatricsAsthma Patients

β1 β2 β3
β-Blockers
ContraindicationsUncompensated CHFPulmonary edemaCardiogenic shockBradycardiaHeart Block
May ↑ these labs
Use With Caution InRenal ImpairmentHepatic ImpairmentDiabetes MellitusGeriatricsAsthma Patients

β1 β2 β3
β-Blockers
ContraindicationsUncompensated CHFPulmonary edemaCardiogenic shockBradycardiaHeart Block
May ↑ these labsBUNSerum LipoproteinK+TriglyceridesUric Acid LevelsANA titersBlood Glucose Levels
Use With Caution InRenal ImpairmentHepatic ImpairmentDiabetes MellitusGeriatricsAsthma Patients

β1 β2 β3
β-Blockers
ContraindicationsUncompensated CHFPulmonary edemaCardiogenic shockBradycardiaHeart Block
May ↑ these labsBUNSerum LipoproteinK+TriglyceridesUric Acid LevelsANA titersBlood Glucose Levels
Use With Caution InRenal ImpairmentHepatic ImpairmentDiabetes MellitusGeriatricsAsthma Patients
Primarily labs monitoring liver function

β1 β2 β3
β-Blockers
ContraindicationsUncompensated CHFPulmonary edemaCardiogenic shockBradycardiaHeart Block
↑ myocardial depression
May ↑ these labsBUNSerum LipoproteinK+TriglyceridesUric Acid LevelsANA titersBlood Glucose Levels
Use With Caution InRenal ImpairmentHepatic ImpairmentDiabetes MellitusGeriatricsAsthma Patients

β1 β2 β3
β-Blockers
ContraindicationsUncompensated CHFPulmonary edemaCardiogenic shockBradycardiaHeart Block
↑ myocardial depressionGeneral anesthesia
IV PhenytoinVerapamil
May ↑ these labsBUNSerum LipoproteinK+TriglyceridesUric Acid LevelsANA titersBlood Glucose Levels
Use With Caution InRenal ImpairmentHepatic ImpairmentDiabetes MellitusGeriatricsAsthma Patients

β1 β2 β3
β-Blockers
ContraindicationsUncompensated CHFPulmonary edemaCardiogenic shockBradycardiaHeart Block
↑ myocardial depressionGeneral anesthesia
IV PhenytoinVerapamil
↑ Bradycardia
May ↑ these labsBUNSerum LipoproteinK+TriglyceridesUric Acid LevelsANA titersBlood Glucose Levels
Use With Caution InRenal ImpairmentHepatic ImpairmentDiabetes MellitusGeriatricsAsthma Patients

β1 β2 β3
β-Blockers
ContraindicationsUncompensated CHFPulmonary edemaCardiogenic shockBradycardiaHeart Block
↑ myocardial depressionGeneral anesthesia
IV PhenytoinVerapamil
↑ BradycardiaDigoxin
May ↑ these labsBUNSerum LipoproteinK+TriglyceridesUric Acid LevelsANA titersBlood Glucose Levels
Use With Caution InRenal ImpairmentHepatic ImpairmentDiabetes MellitusGeriatricsAsthma Patients
β1 β2 β3
β-Blockers
ContraindicationsUncompensated CHFPulmonary edemaCardiogenic shockBradycardiaHeart Block
↑ myocardial depressionGeneral anesthesia
IV PhenytoinVerapamil
↑ BradycardiaDigoxin
↑ HTN
May ↑ these labsBUNSerum LipoproteinK+TriglyceridesUric Acid LevelsANA titersBlood Glucose Levels
Use With Caution InRenal ImpairmentHepatic ImpairmentDiabetes MellitusGeriatricsAsthma Patients

β1 β2 β3
β-Blockers
ContraindicationsUncompensated CHFPulmonary edemaCardiogenic shockBradycardiaHeart Block
↑ myocardial depressionGeneral anesthesia
IV PhenytoinVerapamil
↑ BradycardiaDigoxin
↑ HTNOther antihypertensives
Acute –OH ingestionnitrates
May ↑ these labsBUNSerum LipoproteinK+TriglyceridesUric Acid LevelsANA titersBlood Glucose Levels
Use With Caution InRenal ImpairmentHepatic ImpairmentDiabetes MellitusGeriatricsAsthma Patients
β1 β2 β3
β-Blockers
ContraindicationsUncompensated CHFPulmonary edemaCardiogenic shockBradycardiaHeart Block
↑ myocardial depressionGeneral anesthesia
IV PhenytoinVerapamil
↑ BradycardiaDigoxin
↑ HTNOther antihypertensives
Acute –OH ingestionnitrates
Unopposed α adrenergic stimulation
May ↑ these labsBUNSerum LipoproteinK+TriglyceridesUric Acid LevelsANA titersBlood Glucose Levels
Use With Caution InRenal ImpairmentHepatic ImpairmentDiabetes MellitusGeriatricsAsthma Patients

β1 β2 β3
β-Blockers
ContraindicationsUncompensated CHFPulmonary edemaCardiogenic shockBradycardiaHeart Block
↑ myocardial depressionGeneral anesthesia
IV PhenytoinVerapamil
↑ BradycardiaDigoxin
↑ HTNOther antihypertensives
Acute –OH ingestionnitrates
Unopposed α adrenergic stimulationAmphetamines
CocaineEphedrine
EpinephrinePhenylephrine
pseudophedrine
May ↑ these labsBUNSerum LipoproteinK+TriglyceridesUric Acid LevelsANA titersBlood Glucose Levels
Use With Caution InRenal ImpairmentHepatic ImpairmentDiabetes MellitusGeriatricsAsthma Patients

β1 β2 β3
β-Blockers
Side Effects/Adverse Rxns
β1 β2 β3
β-Blockers
Extension of therapeutic effect
Side Effects/Adverse Rxns

β1 β2 β3
β-Blockers
Side Effects/Adverse Rxns FatigueWeaknessArrhythmiasBradycardiaCHFPulmonary EdemaErectile dysfunctionAnaphylaxis (rare)Nasal StuffinessBronchospasm/wheezingOrthostatic hypotension
Extension of therapeutic effect

β1 β2 β3
β-BlockersSymptoms of Toxicity
Side Effects/Adverse Rxns FatigueWeaknessArrhythmiasBradycardiaCHFPulmonary EdemaErectile dysfunctionAnaphylaxis (rare)Nasal StuffinessBronchospasm/wheezingOrthostatic hypotension

β1 β2 β3
β-BlockersSymptoms of ToxicityBradycardiaSevere DizzinessFaintingSevere DrowsinessDyspneaBluish FingernailsSeizures
Side Effects/Adverse RxnsFatigueWeaknessArrhythmiasBradycardiaCHFPulmonary EdemaErectile dysfunctionAnaphylaxis (rare)Nasal StuffinessBronchospasm/wheezingOrthostatic hypotension

β1 β2 β3
β-BlockersSymptoms of ToxicityBradycardiaSevere DizzinessFaintingSevere DrowsinessDyspneaBluish FingernailsSeizures
AssessmentSide Effects/Adverse Rxns FatigueWeaknessArrhythmiasBradycardiaCHFPulmonary EdemaErectile dysfunctionAnaphylaxis (rare)Nasal StuffinessBronchospasm/wheezingOrthostatic hypotension

β1 β2 β3
β-BlockersSymptoms of ToxicityBradycardiaSevere DizzinessFaintingSevere DrowsinessDyspneaBluish FingernailsSeizures
Side Effects/Adverse Rxns FatigueWeaknessArrhythmiasBradycardiaCHFPulmonary EdemaErectile dysfunctionAnaphylaxis (rare)Nasal StuffinessBronchospasm/wheezingOrthostatic hypotension
AssessmentMonitor BP and HR

β1 β2 β3
β-BlockersSymptoms of ToxicityBradycardiaSevere DizzinessFaintingSevere DrowsinessDyspneaBluish FingernailsSeizures
AssessmentMonitor BP and HR hold med, call MD, if apical pulse is <50bpm
Side Effects/Adverse Rxns FatigueWeaknessArrhythmiasBradycardiaCHFPulmonary EdemaErectile dysfunctionAnaphylaxis (rare)Nasal StuffinessBronchospasm/wheezingOrthostatic hypotension

β1 β2 β3
β-BlockersSymptoms of ToxicityBradycardiaSevere DizzinessFaintingSevere DrowsinessDyspneaBluish FingernailsSeizures
AssessmentMonitor BP and HR hold med, call MD, if apical pulse is <50bpm
Assess for orthostatic hypotension
Side Effects/Adverse Rxns FatigueWeaknessArrhythmiasBradycardiaCHFPulmonary EdemaErectile dysfunctionAnaphylaxis (rare)Nasal StuffinessBronchospasm/wheezingOrthostatic hypotension

β1 β2 β3
β-BlockersSymptoms of ToxicityBradycardiaSevere DizzinessFaintingSevere DrowsinessDyspneaBluish FingernailsSeizures
AssessmentMonitor BP and HR hold med, call MD, if apical pulse is <50bpm
Assess for orthostatic hypotension teach pt to stand up slowly
Side Effects/Adverse Rxns FatigueWeaknessArrhythmiasBradycardiaCHFPulmonary EdemaErectile dysfunctionAnaphylaxis (rare)Nasal StuffinessBronchospasm/wheezingOrthostatic hypotension

β1 β2 β3
β-BlockersSymptoms of ToxicityBradycardiaSevere DizzinessFaintingSevere DrowsinessDyspneaBluish FingernailsSeizures
AssessmentMonitor BP and HR hold med, call MD, if apical pulse is <50bpm
Assess for orthostatic hypotension teach pt to stand up slowlyMonitor I/O and daily weights
Side Effects/Adverse Rxns FatigueWeaknessArrhythmiasBradycardiaCHFPulmonary EdemaErectile dysfunctionAnaphylaxis (rare)Nasal StuffinessBronchospasm/wheezingOrthostatic hypotension

β1 β2 β3
β-BlockersSymptoms of ToxicityBradycardiaSevere DizzinessFaintingSevere DrowsinessDyspneaBluish FingernailsSeizures
AssessmentMonitor BP and HR hold med, call MD, if apical pulse is <50bpm
Assess for orthostatic hypotension teach pt to stand up slowlyMonitor I/O and daily weights assess chest sounds and for edema
Side Effects/Adverse Rxns FatigueWeaknessArrhythmiasBradycardiaCHFPulmonary EdemaErectile dysfunctionAnaphylaxis (rare)Nasal StuffinessBronchospasm/wheezingOrthostatic hypotension

β1 β2 β3
β-BlockersSymptoms of ToxicityBradycardiaSevere DizzinessFaintingSevere DrowsinessDyspneaBluish FingernailsSeizures
AssessmentMonitor BP and HR hold med, call MD, if apical pulse is <50bpm
Assess for orthostatic hypotension teach pt to stand up slowlyMonitor I/O and daily weights assess chest sounds and for edema
Vitals q5-15 post parenteral administration
Side Effects/Adverse Rxns FatigueWeaknessArrhythmiasBradycardiaCHFPulmonary EdemaErectile dysfunctionAnaphylaxis (rare)Nasal StuffinessBronchospasm/wheezingOrthostatic hypotension

β1 β2 β3
β-BlockersSymptoms of ToxicityBradycardiaSevere DizzinessFaintingSevere DrowsinessDyspneaBluish FingernailsSeizures
AssessmentMonitor BP and HR hold med, call MD, if apical pulse is <50bpm
Assess for orthostatic hypotension teach pt to stand up slowlyMonitor I/O and daily weights assess chest sounds and for edema
Vitals q5-15 post parenteral administrationadminister atropine if needed
Side Effects/Adverse Rxns FatigueWeaknessArrhythmiasBradycardiaCHFPulmonary EdemaErectile dysfunctionAnaphylaxis (rare)Nasal StuffinessBronchospasm/wheezingOrthostatic hypotension

β1 β2 β3
β-BlockersSymptoms of ToxicityBradycardiaSevere DizzinessFaintingSevere DrowsinessDyspneaBluish FingernailsSeizures
AssessmentMonitor BP and HR hold med, call MD, if apical pulse is <50bpm
Assess for orthostatic hypotension teach pt to stand up slowlyMonitor I/O and daily weights assess chest sounds and for edema
Vitals q5-15 post parenteral administrationadminister atropine if needed
Side Effects/Adverse Rxns FatigueWeaknessArrhythmiasBradycardiaCHFPulmonary EdemaErectile dysfunctionAnaphylaxis (rare)Nasal StuffinessBronchospasm/wheezingOrthostatic hypotension For pulse <40bpm, ↓CO = atropine 0.25-0.5 mg IV

β1 β2 β3
β-BlockersSymptoms of ToxicityBradycardiaSevere DizzinessFaintingSevere DrowsinessDyspneaBluish FingernailsSeizures
AssessmentMonitor BP and HR hold med, call MD, if apical pulse is <50bpm
Assess for orthostatic hypotension teach pt to stand up slowlyMonitor I/O and daily weights assess chest sounds and for edema
Vitals q5-15 post parenteral administrationadminister atropine if needed
Patient and Family Teaching
Side Effects/Adverse Rxns FatigueWeaknessArrhythmiasBradycardiaCHFPulmonary EdemaErectile dysfunctionAnaphylaxis (rare)Nasal StuffinessBronchospasm/wheezingOrthostatic hypotension

β1 β2 β3
β-BlockersSymptoms of ToxicityBradycardiaSevere DizzinessFaintingSevere DrowsinessDyspneaBluish FingernailsSeizures
AssessmentMonitor BP and HR hold med, call MD, if apical pulse is <50bpm
Assess for orthostatic hypotension teach pt to stand up slowlyMonitor I/O and daily weights assess chest sounds and for edema
Vitals q5-15 post parenteral administrationadminister atropine if needed
Patient and Family TeachingAbrupt withdrawal can cause life
threatening arrhythmias, HTN or MI
Side Effects/Adverse Rxns FatigueWeaknessArrhythmiasBradycardiaCHFPulmonary EdemaErectile dysfunctionAnaphylaxis (rare)Nasal StuffinessBronchospasm/wheezingOrthostatic hypotension

β1 β2 β3
β-BlockersSymptoms of ToxicityBradycardiaSevere DizzinessFaintingSevere DrowsinessDyspneaBluish FingernailsSeizures
AssessmentMonitor BP and HR hold med, call MD, if apical pulse is <50bpm
Assess for orthostatic hypotension teach pt to stand up slowlyMonitor I/O and daily weights assess chest sounds and for edema
Vitals q5-15 post parenteral administrationadminister atropine if needed
Patient and Family TeachingAbrupt withdrawal can cause life
threatening arrhythmias, HTN or MI
Check pulse and BP 2x/wkIf HR <50bpm, hold dose and call MD
Side Effects/Adverse Rxns FatigueWeaknessArrhythmiasBradycardiaCHFPulmonary EdemaErectile dysfunctionAnaphylaxis (rare)Nasal StuffinessBronchospasm/wheezingOrthostatic hypotension
β1 β2 β3
β-BlockersSymptoms of ToxicityBradycardiaSevere DizzinessFaintingSevere DrowsinessDyspneaBluish FingernailsSeizures
AssessmentMonitor BP and HR hold med, call MD, if apical pulse is <50bpm
Assess for orthostatic hypotension teach pt to stand up slowlyMonitor I/O and daily weights assess chest sounds and for edema
Vitals q5-15 post parenteral administrationadminister atropine if needed
Patient and Family TeachingAbrupt withdrawal can cause life
threatening arrhythmias, HTN or MI
Check pulse and BP 2x/wkIf HR <50bpm, hold dose and call MD
Notify if having difficulty breathing, wheezing, coldHands/feet, confusion, dizzy
Side Effects/Adverse Rxns FatigueWeaknessArrhythmiasBradycardiaCHFPulmonary EdemaErectile dysfunctionAnaphylaxis (rare)Nasal StuffinessBronchospasm/wheezingOrthostatic hypotension

β1 β2 β3
β-BlockersSymptoms of ToxicityBradycardiaSevere DizzinessFaintingSevere DrowsinessDyspneaBluish FingernailsSeizures
AssessmentMonitor BP and HR hold med, call MD, if apical pulse is <50bpm
Assess for orthostatic hypotension teach pt to stand up slowlyMonitor I/O and daily weights assess chest sounds and for edema
Vitals q5-15 post parenteral administrationadminister atropine if needed
Patient and Family TeachingAbrupt withdrawal can cause life
threatening arrhythmias, HTN or MI
Check pulse and BP 2x/wkIf HR <50bpm, hold dose and call MD
Notify if having difficulty breathing, wheezing, coldHands/feet, confusion, dizzy
Change positions slowly
Side Effects/Adverse Rxns FatigueWeaknessArrhythmiasBradycardiaCHFPulmonary EdemaErectile dysfunctionAnaphylaxis (rare)Nasal StuffinessBronchospasm/wheezingOrthostatic hypotension

β1 β2 β3
β-BlockersSymptoms of ToxicityBradycardiaSevere DizzinessFaintingSevere DrowsinessDyspneaBluish FingernailsSeizures
AssessmentMonitor BP and HR hold med, call MD, if apical pulse is <50bpm
Assess for orthostatic hypotension teach pt to stand up slowlyMonitor I/O and daily weights assess chest sounds and for edema
Vitals q5-15 post parenteral administrationadminister atropine if needed
Patient and Family TeachingAbrupt withdrawal can cause life
threatening arrhythmias, HTN or MI
Check pulse and BP 2x/wkIf HR <50bpm, hold dose and call MD
Notify if having difficulty breathing, wheezing, coldHands/feet, confusion, dizzy
Change positions slowly
Don’t double dose if you miss one Take ASAP or up to 4 hours before the next dose
Side Effects/Adverse Rxns FatigueWeaknessArrhythmiasBradycardiaCHFPulmonary EdemaErectile dysfunctionAnaphylaxis (rare)Nasal StuffinessBronchospasm/wheezingOrthostatic hypotension

β1 β2 β3
β-BlockersSymptoms of ToxicityBradycardiaSevere DizzinessFaintingSevere DrowsinessDyspneaBluish FingernailsSeizures
AssessmentMonitor BP and HR hold med, call MD, if apical pulse is <50bpm
Assess for orthostatic hypotension teach pt to stand up slowlyMonitor I/O and daily weights assess chest sounds and for edema
Vitals q5-15 post parenteral administrationadminister atropine if needed
Patient and Family TeachingAbrupt withdrawal can cause life
threatening arrhythmias, HTN or MI
Check pulse and BP 2x/wkIf HR <50bpm, hold dose and call MD
Notify if having difficulty breathing, wheezing, coldHands/feet, confusion, dizzy
Change positions slowly
Don’t double dose if you miss one Take ASAP or up to 4 hours before the next dose
Take as directed, even if you feel well
Side Effects/Adverse Rxns FatigueWeaknessArrhythmiasBradycardiaCHFPulmonary EdemaErectile dysfunctionAnaphylaxis (rare)Nasal StuffinessBronchospasm/wheezingOrthostatic hypotension

β1 β2 β3
β-BlockersSymptoms of ToxicityBradycardiaSevere DizzinessFaintingSevere DrowsinessDyspneaBluish FingernailsSeizures
AssessmentMonitor BP and HR hold med, call MD, if apical pulse is <50bpm
Assess for orthostatic hypotension teach pt to stand up slowlyMonitor I/O and daily weights assess chest sounds and for edema
Vitals q5-15 post parenteral administrationadminister atropine if needed
Patient and Family TeachingAbrupt withdrawal can cause life
threatening arrhythmias, HTN or MI
Check pulse and BP 2x/wkIf HR <50bpm, hold dose and call MD
Notify if having difficulty breathing, wheezing, coldHands/feet, confusion, dizzy
Change positions slowly
Don’t double dose if you miss one Take ASAP or up to 4 hours before the next dose
Take as directed, even if you feel well
Monitor glucose closely. ↓ glucose symptoms may be masked
Side Effects/Adverse Rxns FatigueWeaknessArrhythmiasBradycardiaCHFPulmonary EdemaErectile dysfunctionAnaphylaxis (rare)Nasal StuffinessBronchospasm/wheezingOrthostatic hypotension

β1 β2 β3
AcebutololAtenololBetaxololBisprolol
CeliprololEsmololMetoprololNebivolol

β1 β2 β3
AlprenololBucindololCarteololCarvedilolLabetalolNadololOxprenololPenbutololPindololPropranololSotalolTimolol
AcebutololAtenololBetaxololBisprolol
CeliprololEsmololMetoprololNebivolol

β1 β2 β3
AlprenololBucindololCarteololCarvedilolLabetalolNadololOxprenololPenbutololPindololPropranololSotalolTimolol
AcebutololAtenololBetaxololBisprolol
CeliprololEsmololMetoprololNebivolol

β1 β2 β3
β-BlockersMetoprolol PO
Beloc, Beloc-ZOK, betaloc Durules, Betaloc-Zok, lopresor, Lopresor SR, Lopressor, Metoprol, Novo-metoprol, Seloken-ZOK, Toprol

β1 β2 β3
β-BlockersMetoprolol PO

β1 β2 β3
β-BlockersMetoprolol PO
…effects of ↓♥rate, ↓BP, suppression of arrhythmias
β1 β2 β3
β-BlockersMetoprolol PO
Labeled Uses
…effects of ↓♥rate, ↓BP, suppression of arrhythmias

β1 β2 β3
β-BlockersMetoprolol PO
Labeled UsesManagement of HTNPrevention and mgmt of MIMgmt of stable, symptomatic Class 1, 3 ♥ failureAngina
…effects of ↓♥rate, ↓BP, suppression of arrhythmias

β1 β2 β3
β-BlockersMetoprolol PO
Labeled UsesManagement of HTNPrevention and mgmt of MIMgmt of stable, symptomatic Class 1, 3 ♥ failureAngina
Off Label Uses
…effects of ↓♥rate, ↓BP, suppression of arrhythmias

β1 β2 β3
β-BlockersMetoprolol PO
Labeled UsesManagement of HTNPrevention and mgmt of MIMgmt of stable, symptomatic Class 1, 3 ♥ failureAngina
Off Label UsesVentricular arrhythmiasVentricular tachycardia
Migraine prophylaxisDrug induced akathisia
Aggressive behaviorTremorsanxiety…effects of ↓♥rate, ↓BP, suppression of arrhythmias

β1 β2 β3
β-BlockersMetoprolol PO
Labeled UsesManagement of HTNPrevention and mgmt of MIMgmt of stable, symptomatic Class 1, 3 ♥ failureAngina
…effects of ↓♥rate, ↓BP, suppression of arrhythmias
25mg, 50mg, 100mg
Off Label UsesVentricular arrhythmiasVentricular tachycardia
Migraine prophylaxisDrug induced akathisia
Aggressive behaviorTremorsanxiety

β1 β2 β3
β-BlockersMetoprolol PO
Labeled UsesManagement of HTNPrevention and mgmt of MIMgmt of stable, symptomatic Class 1, 3 ♥ failureAngina
…effects of ↓♥rate, ↓BP, suppression of arrhythmias
25mg, 50mg, 100mg 15 min onsetUnknown peak5-8 hr duration3-7 hr ½ life
Off Label UsesVentricular arrhythmiasVentricular tachycardia
Migraine prophylaxisDrug induced akathisia
Aggressive behaviorTremorsanxiety

β1 β2 β3
β-BlockersMetoprolol PO
Labeled UsesManagement of HTNPrevention and mgmt of MIMgmt of stable, symptomatic Class 1, 3 ♥ failureAngina
…effects of ↓♥rate, ↓BP, suppression of arrhythmias
25mg, 50mg, 100mg 15 min onsetUnknown peak5-8 hr duration3-7 hr ½ lifeFull effect not seen for 3-4 weeksMostly metabolized by liverAdminister with meals
Off Label UsesVentricular arrhythmiasVentricular tachycardia
Migraine prophylaxisDrug induced akathisia
Aggressive behaviorTremorsanxiety

β1 β2 β3
β-BlockersMetoprolol PO
Labeled UsesManagement of HTNPrevention and mgmt of MIMgmt of stable, symptomatic Class 1, 3 ♥ failureAngina
Off Label UsesVentricular arrhythmiasVentricular tachycardia
Migraine prophylaxisDrug induced akathisia
Aggressive behaviorTremorsanxiety…effects of ↓♥rate, ↓BP, suppression of arrhythmias
25mg, 50mg, 100mg 15 min onsetUnknown peak5-8 hr duration3-7 hr ½ lifeFull effect not seen for 3-4 weeksMostly metabolized by liverAdminister with meals
Anti-Anginal/HTN25mg/day → 100mg/day
May ↑ After 1 week

β1 β2 β3
β-BlockersMetoprolol PO
Labeled UsesManagement of HTNPrevention and mgmt of MIMgmt of stable, symptomatic Class 1, 3 ♥ failureAngina
Off Label UsesVentricular arrhythmiasVentricular tachycardia
Migraine prophylaxisDrug induced akathisia
Aggressive behaviorTremorsanxiety…effects of ↓♥rate, ↓BP, suppression of arrhythmias
25mg, 50mg, 100mg 15 min onsetUnknown peak5-8 hr duration3-7 hr ½ lifeFull effect not seen for 3-4 weeksMostly metabolized by liverAdminister with meals
Anti-Anginal/HTN25mg/day → 100mg/day
May ↑ After 1 week
Heart Failure12.5mg → 25mg/day
Can be doubled q2 weeksMax 200mg

β1 β2 β3
β-BlockersMetoprolol PO
Labeled UsesManagement of HTNPrevention and mgmt of MIMgmt of stable, symptomatic Class 1, 3 ♥ failureAngina
Off Label UsesVentricular arrhythmiasVentricular tachycardia
Migraine prophylaxisDrug induced akathisia
Aggressive behaviorTremorsanxiety…effects of ↓♥rate, ↓BP, suppression of arrhythmias
25mg, 50mg, 100mg 15 min onsetUnknown peak5-8 hr duration3-7 hr ½ lifeFull effect not seen for 3-4 weeksMostly metabolized by liverAdminister with meals
Anti-Anginal/HTN25mg/day → 100mg/day
May ↑ After 1 week
Heart Failure12.5mg → 25mg/day
Can be doubled q2 weeksMax 200mg
MI Treatment25mg → 50mg 15 min after last IV dose
Every 6 hrs for 48 hrsThen 100mg 2x daily for 3mo min.

β1 β2 β3
β-BlockersMetoprolol PO
Labeled UsesManagement of HTNPrevention and mgmt of MIMgmt of stable, symptomatic Class 1, 3 ♥ failureAngina
Off Label UsesVentricular arrhythmiasVentricular tachycardia
Migraine prophylaxisDrug induced akathisia
Aggressive behaviorTremorsanxiety…effects of ↓♥rate, ↓BP, suppression of arrhythmias
25mg, 50mg, 100mg 15 min onsetUnknown peak5-8 hr duration3-7 hr ½ lifeFull effect not seen for 3-4 weeksMostly metabolized by liverAdminister with meals
Anti-Anginal/HTN25mg/day → 100mg/day
May ↑ After 1 week
Heart Failure12.5mg → 25mg/day
Can be doubled q2 weeksMax 200mg
MI Treatment25mg → 50mg 15 min after last IV dose
Every 6 hrs for 48 hrsThen 100mg 2x daily for 3mo min.
Migraine Prevention50-100mg, 2-4x/day

β1 β2 β3
β-BlockersMetoprolol IV
β1 β2 β3
β-BlockersMetoprolol IV
…effects of ↓♥rate, ↓BP, suppression of arrhythmias

β1 β2 β3
β-BlockersMetoprolol IV
Labeled UsePrevention and mgmt of MI
…effects of ↓♥rate, ↓BP, suppression of arrhythmias

β1 β2 β3
β-BlockersMetoprolol IV
Labeled UsePrevention and mgmt of MI
…effects of ↓♥rate, ↓BP, suppression of arrhythmias
1mg/mL

β1 β2 β3
β-BlockersMetoprolol IV
Labeled UsePrevention and mgmt of MI
…effects of ↓♥rate, ↓BP, suppression of arrhythmias
1mg/mL
For MI, suggested dose is 5mg q2 min for 3 doses, followed by oral dosing.
Following this order, how many total mLs of metoprolol would be administered?

β1 β2 β3
β-BlockersMetoprolol IV
Labeled UsePrevention and mgmt of MI
…effects of ↓♥rate, ↓BP, suppression of arrhythmias
1mg/mL
For MI, suggested dose is 5mg q2 min for 3 doses, followed by oral dosing.
Following this order, how many total mLs of metoprolol would be administered?
5mg x 3 = 15mg
15mg/1 x 1mL/1mg = 15mL

β1 β2 β3
β-BlockersMetoprolol IV
Labeled UsePrevention and mgmt of MI
…effects of ↓♥rate, ↓BP, suppression of arrhythmias
1mg/mLImmediate onset20 min peak6-12 hr duration3-7 hr ½ life

β1 β2 β3
β-BlockersMetoprolol IV
Labeled UsePrevention and mgmt of MI
…effects of ↓♥rate, ↓BP, suppression of arrhythmias
1mg/mLImmediate onset20 min peak6-12 hr duration3-7 hr ½ lifeAdminister undilutedAdminister over 1 minute

β1 β2 β3
β-BlockersMetoprolol IV
Labeled UsePrevention and mgmt of MI
…effects of ↓♥rate, ↓BP, suppression of arrhythmias
1mg/mLImmediate onset20 min peak6-12 hr duration3-7 hr ½ lifeAdminister undilutedAdminister over 1 minute
MI Treatment5mg q2min for 3 doses
Followed by oral dosing

β1 β2 β3
β-BlockersMetoprolol IV
Labeled UsePrevention and mgmt of MI
…effects of ↓♥rate, ↓BP, suppression of arrhythmias
1mg/mLImmediate onset20 min peak6-12 hr duration3-7 hr ½ lifeAdminister undilutedAdminister over 1 minute
MI Treatment5mg q2min for 3 doses
Followed by oral dosing
Get calculations VERIFIED

β1 β2 β3
β-BlockersCarvedilol PO

β1 β2 β3
β-BlockersCarvedilol PO
Coreg, Coreg CR

β1 β2 β3
β-BlockersCarvedilol PO
β1 (myocardial) & β2 (pulmonary, vascular)

β1 β2 β3
β-BlockersCarvedilol PO
Labeled Uses
β1 (myocardial) & β2 (pulmonary, vascular)

β1 β2 β3
β-BlockersCarvedilol PO
Labeled UsesManagement of HTNCHF (ischemic cardiomyopathies)Left ventricular dysfunction after MI
β1 (myocardial) & β2 (pulmonary, vascular)

β1 β2 β3
β-BlockersCarvedilol PO
Labeled UsesManagement of HTNCHF (ischemic cardiomyopathies)Left ventricular dysfunction after MI
β1 (myocardial) & β2 (pulmonary, vascular)
3.125mg, 6.25mg, 12.5mg, 25mg
β1 β2 β3
β-BlockersCarvedilol PO
Labeled UsesManagement of HTNCHF (ischemic cardiomyopathies)Left ventricular dysfunction after MI
β1 (myocardial) & β2 (pulmonary, vascular)
3.125mg, 6.25mg, 12.5mg, 25mg Within 1 hr onset1-2 hr peak12 hr duration7-10 hr ½ life

β1 β2 β3
β-BlockersCarvedilol PO
Labeled UsesManagement of HTNCHF (ischemic cardiomyopathies)Left ventricular dysfunction after MI
β1 (myocardial) & β2 (pulmonary, vascular)
3.125mg, 6.25mg, 12.5mg, 25mg Within 1 hr onset1-2 hr peak12 hr duration7-10 hr ½ life98% protein binding Excreted in feces and urine
β1 β2 β3
β-BlockersCarvedilol PO
Labeled UsesManagement of HTNCHF (ischemic cardiomyopathies)Left ventricular dysfunction after MI
β1 (myocardial) & β2 (pulmonary, vascular)
3.125mg, 6.25mg, 12.5mg, 25mg Within 1 hr onset1-2 hr peak12 hr duration7-10 hr ½ life98% protein binding Excreted in feces and urineCYP2D6 metabolized

β1 β2 β3
β-BlockersCarvedilol PO
Labeled UsesManagement of HTNCHF (ischemic cardiomyopathies)Left ventricular dysfunction after MI
β1 (myocardial) & β2 (pulmonary, vascular)
3.125mg, 6.25mg, 12.5mg, 25mg Within 1 hr onset1-2 hr peak12 hr duration7-10 hr ½ life98% protein binding Excreted in feces and urineCYP2D6 metabolizedFood decreases absorption

β1 β2 β3
β-BlockersCarvedilol PO
Labeled UsesManagement of HTNCHF (ischemic cardiomyopathies)Left ventricular dysfunction after MI
β1 (myocardial) & β2 (pulmonary, vascular)
3.125mg, 6.25mg, 12.5mg, 25mg Within 1 hr onset1-2 hr peak12 hr duration7-10 hr ½ life98% protein binding Excreted in feces and urineCYP2D6 metabolizedFood decreases absorption
Anti-Anginal80mg/day → 320mg/day
In 2-4 divided doses

β1 β2 β3
β-BlockersCarvedilol PO
Labeled UsesManagement of HTNCHF (ischemic cardiomyopathies)Left ventricular dysfunction after MI
β1 (myocardial) & β2 (pulmonary, vascular)
3.125mg, 6.25mg, 12.5mg, 25mg Within 1 hr onset1-2 hr peak12 hr duration7-10 hr ½ life98% protein binding Excreted in feces and urineCYP2D6 metabolizedFood decreases absorption
Anti-Anginal80mg/day → 320mg/day
In 2-4 divided doses
Anti-HTN120mg → 240mg
Twice daily

β1 β2 β3
β-BlockersCarvedilol PO
Labeled UsesManagement of HTNCHF (ischemic cardiomyopathies)Left ventricular dysfunction after MI
β1 (myocardial) & β2 (pulmonary, vascular)
3.125mg, 6.25mg, 12.5mg, 25mg Within 1 hr onset1-2 hr peak12 hr duration7-10 hr ½ life98% protein binding Excreted in feces and urineCYP2D6 metabolizedFood decreases absorption
Anti-Anginal80mg/day → 320mg/day
In 2-4 divided doses
Anti-HTN120mg → 240mg
Twice daily
Anti-Arrhythmic10mg-30mg
3-4 times a day

β1 β2 β3
β-BlockersCarvedilol PO
Labeled UsesManagement of HTNCHF (ischemic cardiomyopathies)Left ventricular dysfunction after MI
β1 (myocardial) & β2 (pulmonary, vascular)
3.125mg, 6.25mg, 12.5mg, 25mg Within 1 hr onset1-2 hr peak12 hr duration7-10 hr ½ life98% protein binding Excreted in feces and urineCYP2D6 metabolizedFood decreases absorption
Anti-Anginal80mg/day → 320mg/day
In 2-4 divided doses
Anti-HTN120mg → 240mg
Twice daily
Anti-Arrhythmic10mg-30mg
3-4 times a day
MI Prevention180mg-240mg
Divided doses daily

β1 β2 β3
β-BlockersCarvedilol PO
Labeled UsesManagement of HTNCHF (ischemic cardiomyopathies)Left ventricular dysfunction after MI
β1 (myocardial) & β2 (pulmonary, vascular)
3.125mg, 6.25mg, 12.5mg, 25mg Within 1 hr onset1-2 hr peak12 hr duration7-10 hr ½ life98% protein binding Excreted in feces and urineCYP2D6 metabolizedFood decreases absorption
Anti-Anginal80mg/day → 320mg/day
In 2-4 divided doses
Anti-HTN120mg → 240mg
Twice daily
Anti-Arrhythmic10mg-30mg
3-4 times a day
MI Prevention180mg-240mg
Divided doses daily
Vascular HA Prev.1mg-3mg
May be repeated after 2 min and again in 4 hours
References
Deglin, J., Vallerand, A., & Sanoski, C. (2011). Davis's drug guide for nurses. (12 ed., p. 1043). Philadelphia, Pennsylvania: F.A. Davis Company.
(n.d.). Retrieved from elevenwarriors.com/2012/02/catching-up-with-tyler-moeller
(n.d.). Retrieved from 1.bp.blogspot.com/_1p20WdeXKKs/TM_tELEfsNI/AAAAAAAAKKI/bNymO _rAnBw /s1600/AsthmaThermoplasty.gif
(n.d.). Retrieved from blogs.mcgill.ca/ossstudents/files/2012/09/adrenal-glands2.jpg
(n.d.). Retrieved from commons.wikimedia.org/wiki/File:Medulla_oblongata.png
(n.d.). Retrieved from focuseducation.com.au/CoolStuff/project/brainfront.jpg
(n.d.). Retrieved from foodandthecity.com/3-things-we-think-men-want-us-to-do-but-they-think-is-gross/
(n.d.). Retrieved from giglig.com/family/education/what-is-circulatory-system
(n.d.). Retrieved from health-for-you.biz/aromatherapy-for-bladder-infections.php
(n.d.). Retrieved from images.wisegeek.com/internal-organs.jpg
(n.d.). Retrieved from jogdoc.files.wordpress.com/2010/11/running_legs1.jpg
(n.d.). Retrieved from menshealth.com/sweat/avoid-embarassing-stains.php
(n.d.). Retrieved from mynyp.org/images/my_health/ei_2396.jpg
(n.d.). Retrieved from opm.phar.umich.edu/protein.php?pdbid=2y02
(n.d.). Retrieved from romeljoseph.files.wordpress.com/2012/01/stage-fright1.jpg
(n.d.). Retrieved from worldresources.tripod.com/image-hypertension/21.phototake_ rm_photo_of_arteries.jpg