beyond the clinic: ‘direct-to-consumer’ genomic profiling services and pharmacogenomics
TRANSCRIPT

403
Review
ISSN 1462-241610.2217/PGS.13.10 © 2013 Future Medicine Ltd Pharmacogenomics (2013) 14(4), 403–412
Beyond the clinic: ‘direct-to-consumer’ genomic profiling services and pharmacogenomics
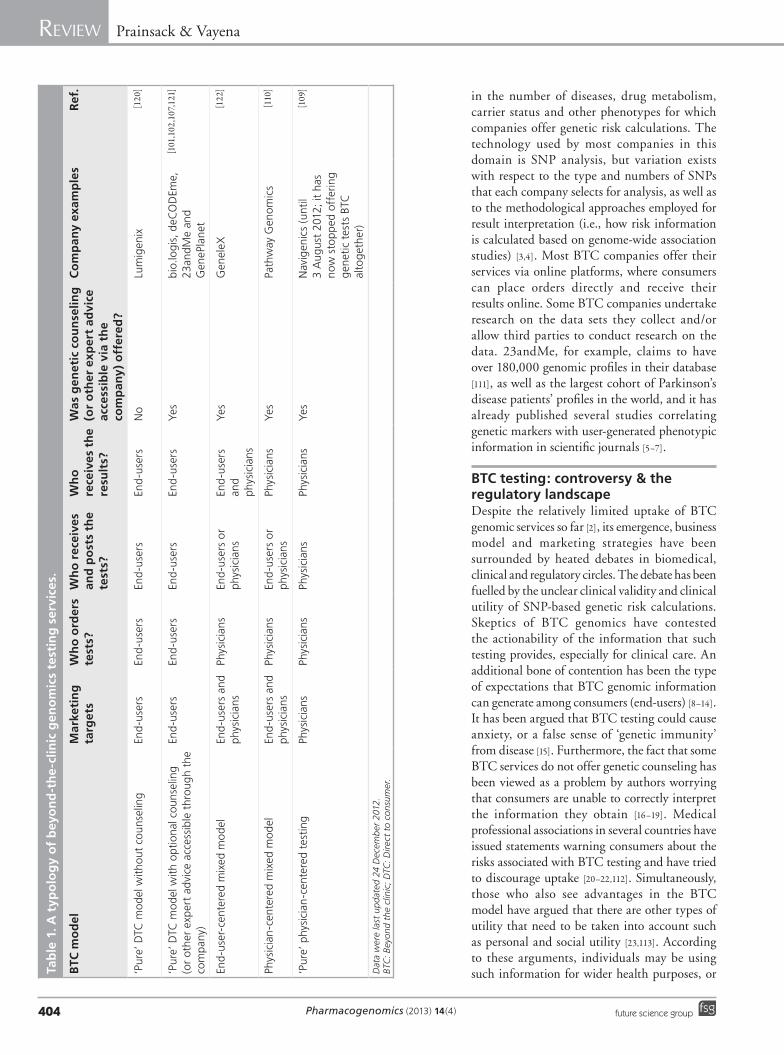
Genomic testing beyond the clinicSince the end of the last decade, genetic and genomic services have become available directly to consumers outside typical clinical settings, and often without the involvement of a medical practitioner. A relatively diverse range of companies now offer a broad spectrum of genomic profiling services including disease susceptibility for complex common diseases, ancestry, traits and pharmacogenomic information online. The first companies providing such services appeared in the USA [101] and Iceland [102], but soon thereafter, other countries around the world followed suit. More recently, the growth of new online genomics companies has slowed down, and commentators have rightly pointed out that the diversity of the services offered is now so great that the phenomenon can no longer be subsumed under the label of direct to consumer (DTC) [103,104]. There have always been variations in how companies have offered genetic tests to their consumers; for example, some have always included the option of genetic counseling in the core package of their service, while others have not. Nevertheless, what most services subsumed under the early DTC model shared in common was that tests were offered, ordered and results were received by users directly from the company, without any involvement of clinical actors. Formats have now become much more diverse (Table 1). For example, Lumigenix (Sydney, Australia) continues to represent the ‘pure’ DTC model: all stages of the testing process take place DTC [105,106]. 23andMe, deCODEme and GenePlanet (Ljubljana, Slovenia) and the personal genomics service of
bio.logis (all other services offered by bio.logis [107] are part of clinical genetic testing provision) are predominantly DTC, but offer optional genetic counseling to their customers, either for an additional fee and through a third party, as in the case of 23andMe [108], or at no additional cost. Navigenics [109] or Pathway Genomics [110] initially offered tests according to the ‘pure’ DTC model, but relatively soon resorted to only offering the tests through licensed physicians. Physicians order the kits from the company and distribute them to their patients. Practices vary as to whether patients need to go through their physicians to receive test results, or receive test results directly. Navigenics, which in 2012 was acquired by the Life Technologies Corp., a global biotechnology company with headquarters in CA, USA, required physicians to access their patients’ results; on 3 August 2012, Navigenics stopped providing genetic tests directly to consumers altogether. These examples demonstrate that instead of a single coherent DTC model, online genomics today is a cluster of practices where any or all stages of the process take place without being mediated by a clinician. We therefore use the term beyond-the-clinic (BTC) genomics to refer to this field. Besides serving as a label under which the various forms of interactions between service providers, users, and medical professionals can be subsumed, BTC genomics also captures the notion that the boundaries between genomics (and genetics more broadly) in the clinic and outside are becoming increasingly blurry [1].
While the number of BTC genomic testing companies has risen only moderately in the 2010s [2], a more steady growth can be observed
This article provides an overview of commercial pharmacogenetics and pharmacogenomics testing services offered online. The concept of ‘beyond-the-clinic’ (BTC) genomic testing is introduced to refer to the variety of formats in which these tests are offered and a typology of BTC models is developed. The authors review such models in relation to tests for individual drug response that are currently on offer. In conclusion, the authors argue that the evolving BTC domain provides opportunities for the pioneering of integrated data repositories, whose gatekeepers are patients or citizens. The authors anticipate that such developments will benefit pharmacogenomics sooner than other areas of medical practice.
KEYWORDS: beyond-the-clinic n DTC genomics n personal genomics n pharmacogenomics
Barbara Prainsack*1 & Effy Vayena2
1Department of Social Science, Health & Medicine, King’s College London, Strand, London WC2R 2LS, UK 2Institute of Biomedical Ethics, University of Zurich, Pestalozzistrasse 24, 8032 Zurich, Switzerland *Author for correspondence: Tel.: +44 7912 622901 [email protected]
part of
For reprint orders, please contact: [email protected]
Pharmacogenomics (2013) 14(4)404 future science group
Review Prainsack & Vayena
in the number of diseases, drug metabolism, carrier status and other phenotypes for which companies offer genetic risk calculations. The technology used by most companies in this domain is SNP ana lysis, but variation exists with respect to the type and numbers of SNPs that each company selects for ana lysis, as well as to the methodological approaches employed for result interpretation (i.e., how risk information is calculated based on genome-wide association studies) [3,4]. Most BTC companies offer their services via online platforms, where consumers can place orders directly and receive their results online. Some BTC companies undertake research on the data sets they collect and/or allow third parties to conduct research on the data. 23andMe, for example, claims to have over 180,000 genomic profiles in their database [111], as well as the largest cohort of Parkinson’s disease patients’ profiles in the world, and it has already published several studies correlating genetic markers with user-generated phenotypic information in scientific journals [5–7].
BTC testing: controversy & the regulatory landscapeDespite the relatively limited uptake of BTC genomic services so far [2], its emergence, business model and marketing strategies have been surrounded by heated debates in biomedical, clinical and regulatory circles. The debate has been fuelled by the unclear clinical validity and clinical utility of SNP-based genetic risk calculations. Skeptics of BTC genomics have contested the actionability of the information that such testing provides, especially for clinical care. An additional bone of contention has been the type of expectations that BTC genomic information can generate among consumers (end-users) [8–14]. It has been argued that BTC testing could cause anxiety, or a false sense of ‘genetic immunity’ from disease [15]. Furthermore, the fact that some BTC services do not offer genetic counseling has been viewed as a problem by authors worrying that consumers are unable to correctly interpret the information they obtain [16–19]. Medical professional associations in several countries have issued statements warning consumers about the risks associated with BTC testing and have tried to discourage uptake [20–22,112]. Simultaneously, those who also see advantages in the BTC model have argued that there are other types of utility that need to be taken into account such as personal and social utility [23,113]. According to these arguments, individuals may be using such information for wider health purposes, or Ta
ble
1. A
typ
olo
gy
of
bey
on
d-t
he
-clin
ic g
eno
mic
s te
stin
g s
ervi
ces.
BTC
mo
del
Mar
keti
ng
ta
rget
sW
ho
ord
ers
test
s?W
ho
rec
eive
s an
d p
ost
s th
e te
sts?
Wh
o
rece
ives
th
e re
sult
s?
Was
gen
etic
co
un
selin
g
(or
oth
er e
xper
t ad
vice
ac
cess
ible
via
th
e co
mp
any)
off
ered
?
Co
mp
any
exam
ple
sR
ef.
‘Pur
e’ D
TC m
od
el w
itho
ut c
ouns
elin
gEn
d-u
sers
End
-use
rsEn
d-u
sers
End
-use
rsN
oLu
mig
enix
[120
]
‘Pur
e’ D
TC m
od
el w
ith
opt
iona
l cou
nsel
ing
(or
othe
r ex
per
t ad
vice
acc
essi
ble
thro
ugh
the
com
pany
)
End
-use
rsEn
d-u
sers
End
-use
rsEn
d-u
sers
Yes
bio.
logi
s, d
eCO
DEm
e,
23an
dM
e an
d G
eneP
lan
et
[101
,102
, 107
,121
]
End
-use
r-ce
nter
ed m
ixed
mo
del
End
-use
rs a
nd
phys
icia
nsPh
ysic
ians
End
-use
rs o
r ph
ysic
ians
End
-use
rs
and
phys
icia
ns
Yes
Gen
eleX
[122
]
Phys
icia
n-c
ente
red
mix
ed m
od
elEn
d-u
sers
and
ph
ysic
ians
Phys
icia
nsEn
d-u
sers
or
phys
icia
nsPh
ysic
ians
Yes
Path
way
Gen
omic
s[1
10]
‘Pur
e’ p
hysi
cian
-cen
tere
d te
stin
gPh
ysic
ians
Phys
icia
nsPh
ysic
ians
Phys
icia
nsYe
s N
avig
enic
s (u
ntil
3 A
ugus
t 20
12; i
t ha
s no
w s
top
ped
off
erin
g g
enet
ic t
ests
BTC
al
tog
ethe
r)
[109
]
Dat
a w
ere
last
up
date
d 24
Dec
emb
er 2
012.
BTC
: Bey
ond
the
clin
ic; D
TC: D
irec
t to
co
nsum
er.

www.futuremedicine.com 405future science group
Beyond the clinic: ‘direct-to-consumer’ genomic profiling services & pharmacogenomics Review
for entertainment and education, for example, while the availability of aggregated data provides opportunities for research and can advance our genomic understanding of disease and health. The debate about how utility is to be understood and assessed in the BTC context is still ongoing, and has spilled over into the regulatory domain [24]. In 2010, the US FDA initiated a discussion on whether genetic tests offered online should be considered medical devices, and therefore should be subject to approval processes and regulation. Eventually hearings were held, and a US Government Accountability Office (GAO) report resulting from an ‘undercover investigation’ of online genetic and genomic testing services found a lack of standardization across different companies and even fraudulent claims [25,114,115]. It should be noted here, however, that the GAO report discussed a wide range of DTC genetic testing companies including some that are unlikely to have used genome-wide SNP assays and many that did not include pharmacogenomic testing; thus, their critique is only applicable to the topic in question to a limited extent. The GAO report, however, contributed to negative publicity of BTC companies as a whole. Since then, the FDA has issued several subsequent letters to BTC companies [116], and held an expert meeting to discuss regulation of online genetic testing in Washington (DC, USA), in 2011 [104]. Official guidance on exactly which elements of online genetic testing are under FDA authority and how the regulatory landscape should change, has so far not been issued.
In European countries, regulatory approaches to BTC testing vary greatly [26–28]. BTC companies are not allowed to operate from within the territory of certain countries (such as Switzerland) although residents of these countries are not prohibited from ordering such services online; the law is addressed to, and thus binding for, service providers, not end-users. A recent report by the European Academies of Medical Sciences called for harmonized regulation of BTC genomics in Europe and took a strong stance against ‘the DTC model’ by recommending strict regulation against it [112]. The problematic clinical utility of online genomic testing services is the most central concern, and it cuts across all aspects of BTC genomic services including pharmacogenetic and pharmacogenomic information.
The marketing strategies of BTC companies have been an additional target of criticism. BTC companies have so far focused mainly on three key messages: consumer empowerment,
self-knowledge and personal responsibility for health [12,29–30]. Unsurprisingly, it has been the mobilization of these concepts, in conjunction with the fact that BTC companies bypass, at least partly, the traditional gatekeepers of genetic information in the health domain, which has caused concern. Some of the critique of online genetic testing also seems to stem from deep-seated skepticism of devolving agency to individuals without professional training [8,10,31–33]. However, other contributions provide a more disinterested ana lysis of the tensions that are lying at the heart of the empowerment rhetoric. For example, Juengst and colleagues recently emphasized the fact that more access to information on genetic susceptibility and prevention also means more responsibility for individuals [30]. These authors also point out that the mere presence of more data does not automatically empower patients, or users of BTC services. Whether data actually empower anybody depends, as a recent report by the European Science Foundation (ESF) also highlighted, on how these data are contextualized to become meaningful and potentially actionable [117]. This clearly indicates that utility cannot be understood merely as clinical utility in the narrow sense. As box 1 illustrates, and as preliminary evidence from interviews of users of BTC testing also shows [34–36], the motivations for using BTC tests and the ways in which test results obtain meaning and utility in individual’s lives, reach far beyond the boundaries of the clinic.
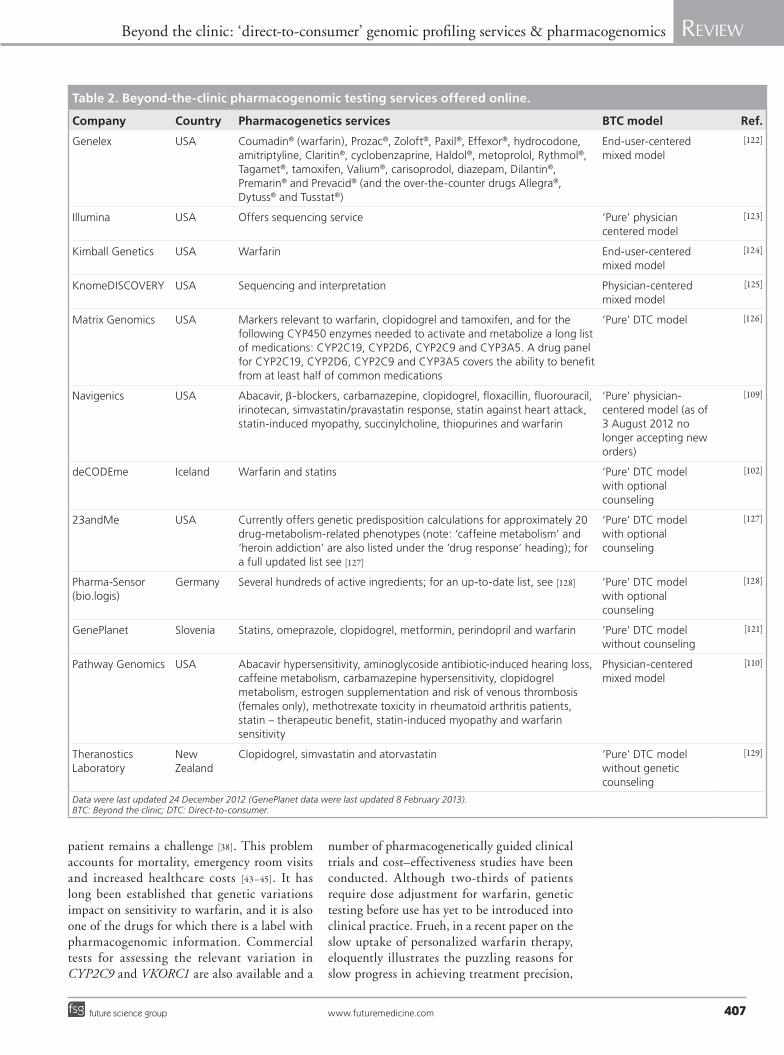
State of the art of BTC pharmacogenomic testing Many BTC companies today also offer pharmacogenomic or pharmacogenetic tests. There is, however, significant variation among them regarding what specific drug responses they have chosen to include in their respective portfolios, as well as the technology platforms used for analyses, the type of gene variants and the alleles they genotype. A recent review of nine BTC websites by Chua and Kennedy described services in the BTC pharmacogenomics domain as ‘patchy and quite limited’ [37]. We reviewed additional websites, expanding on the Genetics and Public Policy Center’s list of DTC genetic testing companies (Table 2) [118]. In the total of 29 company websites that we reviewed we observed a pattern similar to the one described by Chua and Kennedy; pharmacogenomic testing services vary substantially among companies. The companies reviewed provided genetic and genomic

Pharmacogenomics (2013) 14(4)406 future science group
Review Prainsack & Vayena
information relevant to 31 compounds (Table 2). There is more consistency across BTC companies regarding the disease phenotypes they test for, than with regard to drug-related information. Nevertheless, most companies offer testing for abacavir sensitivity, antidepressant response, b-blocker response, carba mazepine sensi tivity, statin- induced myo pathy, simvastatin/pravastin response, clopido grel (sensitivity and efficacy) and warfarin sensitivity.
Companies typically do not offer explanations for how they select the phenotypes they include in their ana lysis or how they compare to other services. The aforementioned review by Chua and Kennedy uses the list of FDA-approved drugs with pharmacogenetic and pharmacogenomic information already on their labels as a means of identifying the best candidate gene–drug pairs for inclusion in the BTC services. According to this comparison only a small range of the information related to drugs that BTC companies are currently including in their test battery could have clinical utility [37,38]. The authors further argue that a lack of effective guidance on how to interpret test results accounts for the limited value of the information. This problem, of course, is not confined to the realm of pharmacogenomics.
The literature addressing pharmacogenomic tests within the BTC domain specifically is very limited. However, most of the issues that have been raised in connection with BTC genomic testing more generally also apply to BTC pharmacogenomics. Data confidentiality [39], the problem of the shifting of responsibility from societies (or, in countries where healthcare is publicly funded, from healthcare systems) on individuals [30,40–41] and worries that ‘lay’ people may misunderstand test results are clearly relevant to BTC pharmacogenomic testing.
The utility of BTC pharmacogenomic testingIt is mainly the notion of clinical utility that sets BTC pharmacogenomic testing aside from BTC testing for complex diseases, carrier status and ‘recreational’ traits (e.g., bitter taste perception, hair curl, ‘athlete genes’). Any genetic information that affects drug response will be clinically relevant in some respect, for the mere reason that decisions on drug therapy are solidly anchored in the clinical domain. One particular concern that has been put forward is the confusion that pharmacogenomic information could cause for consumers. Such confusion, it has been argued, will be generated by the discrepancy between BTC companies’ bypassing, at least in part, traditional clinical gatekeepers on the one hand, and the presumed need for consumers to discuss the results of their pharmacogenetic and pharmacogenomic tests with professional experts on the other. Commentators have argued that BTC pharmacogenomic testing does not offer any actual benefits to test takers [17]. If individuals need their physicians to make treatment decisions, get prescriptions, and adjust doses, so the argument continues, they should turn to their physician to initiate genetic testing, instead of accessing tests DTC. This is a compelling argument if we see the doctor–patient relationship as a closed system in which information travels primarily in one way, namely from the physician to the patient [42]. In light of the slow introduction of pharmacogenomics into clinical practice, however, informed patients can bring useful and actionable information to the decision-making process about their health. Warfarin is a case in point. Warfarin is an anticoagulant that has been used in the clinic for more than 50 years, yet determining the appropriate dose for each
Box 1. Examples for indirect utility of beyond-the-clinic pharmacogenomic testing.
A user of beyond-the-clinic services learned that her genotype indicated that she would show a reduced response to clopidogrel. This was calculated by the company on the basis of five markers in the CYP2C19 gene: rs4244285 (AG); rs4986893 (GG); rs28399504 (AA); rs41291556 (TT); and rs12248560 (CC) [58–61]. Although this user did not use any blood thinners herself, a biological relative of this user used clopidogrel. This relative, despite taking the drug, suffered some minor ischemic stroke events. Although the relative was never tested herself, she was prescribed different blood thinners after learning that her close relative was likely to be a poor responder to clopidogrel. No further ischemic strokes occurred.
Clearly we cannot claim any causal relationship between the change of drugs and the stabilization of her health. What this short vignette shows, however, is that the effects of beyond-the-clinic test results can unfold in more complex ways than what is captured by the notion of clinical utility. The utility observed here is tentative, indirect and nonimmediate, yet it was perceived as very valuable for the individuals involved. Other examples include those who find information on a higher genetic predisposition to Alzheimer’s disease useful for planning ahead for the eventuality of their suffering from dementia in the future, together with their families [Prainsack B, Vayena E, Unpublished Data].
www.futuremedicine.com 407future science group
Beyond the clinic: ‘direct-to-consumer’ genomic profiling services & pharmacogenomics Review
patient remains a challenge [38]. This problem accounts for mortality, emergency room visits and increased healthcare costs [43–45]. It has long been established that genetic variations impact on sensitivity to warfarin, and it is also one of the drugs for which there is a label with pharmacogenomic information. Commercial tests for assessing the relevant variation in CYP2C9 and VKORC1 are also available and a
number of pharmacogenetically guided clinical trials and cost–effectiveness studies have been conducted. Although two-thirds of patients require dose adjustment for warfarin, genetic testing before use has yet to be introduced into clinical practice. Frueh, in a recent paper on the slow uptake of personalized warfarin therapy, eloquently illustrates the puzzling reasons for slow progress in achieving treatment precision,
Table 2. Beyond-the-clinic pharmacogenomic testing services offered online.
Company Country Pharmacogenetics services BTC model Ref.
Genelex USA Coumadin® (warfarin), Prozac®, Zoloft®, Paxil®, Effexor®, hydrocodone, amitriptyline, Claritin®, cyclobenzaprine, Haldol®, metoprolol, Rythmol®, Tagamet®, tamoxifen, Valium®, carisoprodol, diazepam, Dilantin®, Premarin® and Prevacid® (and the over-the-counter drugs Allegra®, Dytuss® and Tusstat®)
End-user-centered mixed model
[122]
Illumina USA Offers sequencing service ‘Pure’ physician centered model
[123]
Kimball Genetics USA Warfarin End-user-centered mixed model
[124]
KnomeDISCOVERY USA Sequencing and interpretation Physician-centered mixed model
[125]
Matrix Genomics USA Markers relevant to warfarin, clopidogrel and tamoxifen, and for the following CYP450 enzymes needed to activate and metabolize a long list of medications: CYP2C19, CYP2D6, CYP2C9 and CYP3A5. A drug panel for CYP2C19, CYP2D6, CYP2C9 and CYP3A5 covers the ability to benefit from at least half of common medications
‘Pure’ DTC model [126]
Navigenics USA Abacavir, b-blockers, carbamazepine, clopidogrel, floxacillin, fluorouracil, irinotecan, simvastatin/pravastatin response, statin against heart attack, statin-induced myopathy, succinylcholine, thiopurines and warfarin
‘Pure’ physician-centered model (as of 3 August 2012 no longer accepting new orders)
[109]
deCODEme Iceland Warfarin and statins ‘Pure’ DTC model with optional counseling
[102]
23andMe USA Currently offers genetic predisposition calculations for approximately 20 drug-metabolism-related phenotypes (note: ‘caffeine metabolism’ and ‘heroin addiction’ are also listed under the ‘drug response’ heading); for a full updated list see [127]
‘Pure’ DTC model with optional counseling
[127]
Pharma-Sensor (bio.logis)
Germany Several hundreds of active ingredients; for an up-to-date list, see [128] ‘Pure’ DTC model with optional counseling
[128]
GenePlanet Slovenia Statins, omeprazole, clopidogrel, metformin, perindopril and warfarin ‘Pure’ DTC model without counseling
[121]
Pathway Genomics USA Abacavir hypersensitivity, aminoglycoside antibiotic-induced hearing loss, caffeine metabolism, carbamazepine hypersensitivity, clopidogrel metabolism, estrogen supplementation and risk of venous thrombosis (females only), methotrexate toxicity in rheumatoid arthritis patients, statin – therapeutic benefit, statin-induced myopathy and warfarin sensitivity
Physician-centered mixed model
[110]
Theranostics Laboratory
New Zealand
Clopidogrel, simvastatin and atorvastatin ‘Pure’ DTC model without genetic counseling
[129]
Data were last updated 24 December 2012 (GenePlanet data were last updated 8 February 2013).BTC: Beyond the clinic; DTC: Direct-to-consumer.

Pharmacogenomics (2013) 14(4)408 future science group
Review Prainsack & Vayena
even when technically it is within reach [46]. Lengthy and rather fruitless controversies over the clinical utility and cost–effectiveness of pharmacogenetic testing for warfarin have prevented the adoption of such testing in the clinic, despite compelling evidence of its utility [46]. Other reasons that are not specific to warfarin but apply more broadly include: outsourcing of genotyping by clinics to private companies resulting in high costs; physicians’ limited pharmacogenetic knowledge; and the fact that many drugs that are widely used are off-patent and therefore there is limited commercial interest in pharmacogenomic studies of their efficacy [47,48]. Against this backdrop it is rather unsurprising that warfarin sensitivity testing is included in the services of all BTC companies with a pharmacogenomics portfolio. Given the apparent clinical utility of warfarin sensitivity testing and its unavailability in the clinic, it is hard to argue against the choice of consumers to obtain and use this information. Yet, this option raises the notorious question of reimbursement [47] and unequal access; a situation where only those who can afford to pay for BTC pharmacogenomics testing out-of-pocket are protected from the danger of over- or under-dosing is highly problematic.
Pharmacogenetics BTC: danger of self-medicationAnother concern is that pharmacogenetic testing, in conjunction with platforms such as Cure Together [119] that allow people to see what kinds of treatments are most effective in patients most similar to them (both in terms of personal characteristics such as ethnicity, sex and age, and in terms of the kinds and severity of symptoms), will encourage people to make treatment and dosage decisions on their own. This scenario is more likely to materialize in contexts where access to clinical care is more expensive, in terms of out-of-pocket-expenditure, than in countries where such access does not incur any immediate costs to the patient. It could be objected here, of course, that the risk of people self-medicating (or adjusting their dose on the basis of a BTC pharmacogenomic test) is alleviated by the fact that most drugs that can cause serious side effects or adverse reactions require a prescription by a licensed physician. While this is certainly a valid argument, it must also be noted that the internet now enables individuals to access prescription drugs – including, unfortunately, counterfeit variants – outside of the traditional clinical routes. In addition, strong arguments in
favor of a ‘right to self medication’ have recently been made within bioethics [49].
The risk that people could self-medicate, or unilaterally change the dosage of their medication, is not a sufficient justification to limit access to BTC pharmacogenomic testing. From our perspective, the main argument against putting up regulatory barriers against BTC pharmacogenomic and pharmacogenetic testing is the fact that BTC testing has raised public awareness of the relevance of genome ana-lysis to drug response [37]. Moreover, some of the companies offering BTC pharmacogenomic and pharmacogenetic testing also include warnings on their website that patients should not adjust dosage, or stop taking a drug altogether, without consulting with experts. Who the experts are, however, is a different question altogether; the urgent need to provide information and education to clinicians on the scientific underpinnings and practical implications of pharmacogenomics has been highlighted by many authors recently [38,42,50–54]. Recent surveys of physicians’ knowledge and use of pharmacogenomic testing revealed that only 10.3–13% felt adequately informed about pharmacogenomics and a similarly small percentage had ordered a pharmacogenomic test recently [54,55]. At the same time, a telephone survey of 1139 US residents carried out by Haga and colleagues found very high levels of interest (≥73%) in pharmacogenetic testing (unless there was a chance that their DNA sample or test results could be disclosed to others without their permission) [56].
Conclusion & future perspectiveWe deem it a timely endeavor to expand the discussion on BTC genomic testing to questions of reimbursement and access. As the utility of pharmacogenomic testing in the BTC domain is already evidenced in some contexts, rather than focusing only on what individuals will do when they receive their test results, we should ask the question of whether there are any groups for whom we should facilitate access to BTC testing. Examples of groups who may benefit from learning about their genetic predisposition to a wide variety of conditions and traits include egg and sperm donors and adoptees without a family medical history. Regarding pharmacogenetic testing specifically, we would include anyone who needs to decide whether or not to take a drug with serious side effects and where pharmacogenetic testing allows for meaningful probabilistic inferences regarding

www.futuremedicine.com 409future science group
Beyond the clinic: ‘direct-to-consumer’ genomic profiling services & pharmacogenomics Review
drug metabolism. We can no longer merely assume that traditional clinical gatekeepers are the sole experts on any health-related test. As Chua and Kennedy summarize, ‘healthcare professionals are generally ill-prepared for incorporating pharmacogenetics into their practice’ [37]. Simultaneously, we should also make sure that the current knowledge vacuum in this field does not provide patients with an incentive to make rash decisions regarding their choice of drug, or dosage, on the basis of online information alone. This scenario can best be avoided by public awareness measures that highlight the need to consult clinicians for any decision on prescription drugs; yet such measures should also refrain from demonizing online-based services and platforms.
Two developments that will impact on the future of pharmacogenomics testing in general are genome sequencing and gene expression prof iling. Both will also inf luence BTC pharmacogenomics services. Exome sequencing and – further down the line – whole-genome sequencing, is expected to increase the predictive value, and thus the immediate clinical utility, of pharmacogenomics and pharmacogenetic tests.
The situation will be complicated, however, by our increasing knowledge of the importance of gene expression [57], as well as immunological and other aspects impacting on drug efficacy. As the BTC domain is not bound by the software-related, taxonomic and logistical infrastructures of the clinic, it has the potential to pioneer integrated data repositories for multiple genomic, epigenetic, demographic and other environmental data sets whose gatekeepers are individual patients.
AcknowledgementsThe authors gratefully acknowledge helpful comments from D Gurwitz, D Vorhaus and three anonymous referees.
Financial & competing interests disclosureThe authors have no relevant affiliations or financial involvement with any organization or entity with a finan-cial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.
Executive summary
� Since the end of the last decade, genetic and genomic tests have become widely available outside typical clinical settings. Services are offered in a wide range of formats, ranging from those including no involvement of health professionals to the online services that are available only through physicians.
� We introduce the terms beyond-the-clinic (BTC) genetics and genomics to accommodate the various forms of interactions between service providers, users and health professionals.
� The controversy about online BTC genetics is ongoing. While opponents continue to worry about whether end-users are capable of adequately understanding and acting upon test results, supporters increasingly call for the need to acknowledge that genetic and genomic information often have personal and social utility for individuals.
� The main points of the controversy about the value and utility of BTC pharmacogenetic testing are similar to those characterizing the debate about BTC genetic testing more generally.
� Currently, BTC companies offer testing for various compounds, with warfarin and clopidogrel being included in most testing services.
� As the uptake of pharmacogenetic testing in the clinic is slow, commercial providers offering tests BTC may attract users who have the funds to pay for it out of pocket. Governmental agencies and payers should consider the implications of this scenario, and any unintended consequences that this is likely to have. We call for the discussion on BTC pharmacogenetics, and BTC genetics more broadly, to be expanded to address questions of reimbursement and access.
ReferencesPapers of special note have been highlighted as:n of interestnn of considerable interest
1 Topol E. The Creative Destruction of Medicine: How the Digital Revolution Will Create Better Health Care. Basic Books, NY, USA (2012).
n Provides a big picture view by discussing current shifts in medical research and practice that are relevant to understanding the development of beyond-the-clinic (BTC) pharmacogenetics and pharmacogenomics.
2 Wright C, MacArthur DG. Direct to consumer genetic testing. In: Molecular Genetics and Personalized Medicine – Molecular and Translational Medicine. Best DH, Swensen JJ (Eds). Springer, NY, USA (2012).
3 Imai K, Kricka LJ, Fortina P. Concordance study of 3 direct-to-consumer genetic-testing services. Clin. Chem. 57, 518–521 (2011).
4 Zehnbauer B. Direct-to-consumer genetics testing – fair comparisons? Clin. Chem. 57, 369–371 (2011).
5 Eriksson N, Macpherson JM, Tung JY et al. Web-based, participant-driven studies yield novel genetic associations for common traits. PLoS Genet. 6, e1000993 (2010).
6 Do CB, Tung JY, Dorfman E et al. Web-based genome-wide association study identifies two novel loci and a substantial genetic component for Parkinson’s disease. PLoS Genet. 7(6), e1002141 (2011).
7 Tung JY, Do CB, Hinds DA et al. Efficient replication of over 180 genetic associations with self-reported medical data. PLoS ONE 6(8), e23473 (2011).
Pharmacogenomics (2013) 14(4)410 future science group
Review Prainsack & Vayena
8 Howard HC, Borry P. Direct-to-consumer genetic testing: More questions than benefits? Per. Med. 5(4), 317–320 (2008).
9 Feero WG, Guttmacher AE, Collins FS. The genome gets personal – almost. JAMA 299, 1351–1352 (2008).
10 Hunter DJ, Khoury MJ, Drazen JM. Letting the genome out of the bottle – will we get our wish? N. Engl. J. Med. 358(2), 105–107 (2008).
11 Kraft P, Hunter DJ. Genetic risk prediction – are we there yet? N. Engl. J. Med. 360(17), 1701–1703 (2009).
12 Caulfield T, McGuire AL. Direct-to-consumer genetic testing: perceptions, problems, and policy responses. Annu. Rev. Med. 63, 23–33 (2012).
13 Khoury MJ, Berg A, Coates R et al. The evidence dilemma in genomic medicine. Health Aff. (Millwood) 27(6), 1600–1611 (2009).
14 Caulfield T. Direct-to-consumer genetics and health policy? A worst-case scenario? Am. J. Bioeth. 9(6), 48–50 (2009).
15 James KM, Cowl CT, Tilburt JC et al. Impact of direct-to-consumer predictive genomic testing on risk perception and worry among patients receiving routine care in a preventive health clinic. Mayo Clin. Proc. 86(10), 933–940 (2011).
16 Nordgren A. Neither as harmful as feared by critics nor as empowering as promised by providers: risk information offered direct to consumer by personal genomics companies. J. Community Genet. doi:10.1007/s12687–012–0094–0090) (2012) (Epub ahead of print).
17 Howard H, Borry P. Direct-to-consumer pharmacogenomic testing. Pharmacogenomics 12(10), 1367–1370 (2011).
n Voices ethical concerns about pharmacogenomic testing beyond the clinic.
18 Leighton JW. The general public’s understanding and perception of DTC genetic test results. Public Health Genomics 15, 11–21 (2012).
19 Vayena E, Mauch F.Personal genomics: are we debating the right issues? Praxis (Bern 1994) 101(15), 961–964 (2012).
20 Hudson K, Javitt G, Burke W, Byers P; ASHG Social Issues Committee. ASHG statement* on direct-to-consumer genetic testing in the United States. Am. J. Hum. Genet. 81(3), 635–637 (2007).
21 European Society of Human Genetics (ESHG). Statement of the ESHG on direct-to-consumer genetic testing for health-related purposes. Eur. J. Hum. Genet. 12, 1271–1273 (2010).
22 Committee on Genetics, American College of Obstetricians and Gynecologists;
Committee on Ethics, American College of Obstetricians and Gynecologists. ACOG Committee Opinion No. 409: direct-to-consumer marketing of genetic testing. Obstet. Gynecol. 111(6), 1493–1494 (2008).
23 Foster MW, Mulvihill JJ, Sharp RR. Evaluating the utility of personal genomic information. Genet. Med. 11(8), 570–574 (2009).
24 Myers MF. Health care providers and DTC access and advertising of genetic testing in the US. Genome Med. 3(12), 81 (2011).
25 Udesky L. The ethics of direct-to-consumer genetic testing. Lancet 376(9750), 1377–1378 (2010).
26 Colaiacovo M, Grimaldi KA. Personal genetics, the European regulations maze and the way out. Per. Med. 9(5), 515–522 (2012).
27 Borry P, van Hellemondt RE, Sprumont D et al. Legislation on direct-to-consumer genetic testing in seven European countries. Eur. J. Hum. Genet. 20(7), 715–721 (2012).
28 Soini S. Genetic testing legislation in western Europe – a fluctuating regulatory target. J. Community Genet. 3(2), 143–153 (2012).
29 Lee SS, Crawley L. Research 2.0: social networking and direct-to-consumer (DTC) genomics. Am. J. Bioeth. 9(6), 35–44 (2009).
30 Juengst ET, Flatt, MA, Settersten RA Jr. Personalized genomic medicine and the rhetoric of empowerment. Hastings Cent. Rep. 35, 34–40 (2012).
n Careful analysis of the rhetoric of patient empowerment in the domain of genetics beyond the clinic.
31 Howard HC, Borry P. Is there a doctor in the house? The presence of physicians in the direct-to-consumer genetic testing context. J. Community Genet. 3(2), 105–112 (2012).
32 Evans JP, Berg JS. Next-generation DNA sequencing, regulation, and the limits of paternalism: the next challenge. JAMA 306(21), 2376–2377 (2011).
33 Howard HC, Borry P. To ban or not to ban? Clinical geneticists’ views on the regulation of direct-to-consumer genetic testing. EMBO Rep. 13(9), 791–794 (2012).
34 McBride CM, Wade CH, Kaphingst KA. Consumers’ views of direct-to-consumer genetic information. Annu. Rev. Genomics Hum. Genet. 11, 427–446 (2010).
35 McGowan ML, Fishman JR, Lambrix MA. Personal genomics and individual identities: Motivations and moral imperatives of early users. New Genet. Soc. 29(3), 261–290 (2010).
36 Vayena E, Gourna E, Streuli J, Hafen E, Prainsack B. Early users of direct-to-consumer genomics in Switzerland. Public Health Genomics 15(6), 352–362 (2012).
37 Chua EW, Kennedy MA. Current state and future prospects of direct-to-consumer pharmacogenetics. Front. Pharmacol. 3, 152 (2012).
nn Provides a review and critical discussion of direct-to-consumer pharmacogenetic testing services currently on the market.
38 Kitzmiller JP, Groen DK, Phelps MA, Sadee W. Pharmacogenomics testing: relevance in medical practice. Cleve. Clin. J. Med. 78(4), 243–257 (2011).
nn Overview of the benefits of pharmacogenomics testing for clinicians.
39 Gurwitz D, Bregman-Eschet Y. Personal genomics services: whose genomes? Eur. J. Hum. Genet. 17(7), 883–889 (2009).
40 Rose N. The Politics of Life Itself: Biomedicine, Power, and Subjectivity in the Twenty-First Century. Princeton University Press, NJ, USA (2008).
41 Prainsack B, Reardon J, Hindmarsh R, Gottweis H, Naue U, Lunshof JE. Misdirected precaution? Nature 456, 34–35 (2008).
42 Gurwitz D, Lunshof JE. Personalized participatory medicine: sharing knowledge and uncertainty. Genome Med. 3(10) 69(2011).
43 Wysowski, DK, Nourjah P, Swartz L. Bleeding complications with warfarin use: a prevalent adverse effect resulting in regulatory action. Arch. Intern. Med. 167, 1414–1419 (2007).
44 Budnitz DS, Pollock DA, Weidenbach KN, Mendelsohn AB, Schroeder TJ, Annest JL. National surveillance of emergency department visits for outpatient adverse drug events. JAMA 296, 1858–1866 (2007).
45 Kim MM, Metlay J, Cohen A et al. Hospitalization costs associated with warfarin- related bleeding events among older community-dwelling adults. Pharmacoepidemiol. Drug Saf. 19, 731–736 (2010).
46 Frueh F. On rat poison and human medicines: personalizing warfarin therapy. Trends Mol. Med. 18(4), 201–205 (2012).
n Excellent overview of the issues relating to the introduction of pharmacogenetic testing for warfarin.
47 Cohen JP. Overcoming regulatory and economic challenges facing pharmacogenomics. New Biotechnology 29(6), 751–756 (2012).
48 Harper AR, Topol EJ. Pharmacogenomics in clinical practice and drug development. Nat. Biotechnol. 30(11), 1117–1124 (2012).
49 Flanigan J. Three arguments against prescription requirements. J. Med. Ethics 38(10), 579–586 (2012).
www.futuremedicine.com 411future science group
Beyond the clinic: ‘direct-to-consumer’ genomic profiling services & pharmacogenomics Review
www.futuremedicine.com
50 Higgs JE, Andrews J, Gurwitz D, Payne K, Newman W. Pharmacogenetics education in british medical schools. Genomic Med. 2(3–4), 101–105 (2008).
51 Gurwitz D. Pharmacogenetics education: 10 years of experience at Tel Aviv University. Pharmacogenomics 11(5), 647–649 (2010).
52 Dias MM, Depala K, Ward HM et al. Reforming pharmaceutical education to enhance the global uptake of pharmacogenomics and personalized medicine. Curr. Pharmacogenomics Person. Med. 10(3), 231–238 (2012).
53 Lunshof JE, Gurwitz D. Pharmacogenomic testing: Knowing more, doing better. Clin. Pharmacol. Ther. 91(3), 387–389 (2012).
nn Discussion of the need for more education and training for medical professionals in the area of pharmacogenomics.
54 Stanek EJ, Sanders CL, Taber KA et al. Adoption of pharmacogenomic testing by US physicians: results of a nationwide survey. Clin. Pharmacol. Ther. 91(3), 450–458 (2012).
55 Haga S, Burke W, Ginsburg G, Mills R, Agans R. Primary care physicians’ knowledge and experience with pharmacogenomics testing. Clin. Genet. 82(4), 388–394 (2012).
56 Haga SB, O’Daniel JMO, Tindall GM, Lipkus IR, Agans R. Survey of US public attitudes towards pharmacogenetic testing. Pharmacogenomics J. 12, 197–105 (2011).
57 Mesko B, Zahuczky G, Nagy L. The triad success in personalised medicine: pharmacogenomics, biotechnology and regulatory issues from a central European perspective. Nat. Biotechnol. 29(6), 741–750 (2012).
58 Paré G, Mehta SR, Yusuf S et al. Effects of CYP2C19 genotype on outcomes of clopidogrel treatment. N. Engl. J. Med. 363(18), 1704–1714 (2010).
59 Mega JL, Simon T, Colleet JP et al. Reduced-function CYP2C19 genotype and risk of adverse clinical outcomes among patients treated with clopidogrel predominantly for PCI. JAMA 304(16), 1821–1830 (2010).
60 Simon T, Verstuyft C, Mary-Krause M. Genetic determinants of response to clopidogrel and cardiovascular events. N. Engl. J. Med. 360(4), 363–375.
61 Mega JL, Close SL, Wiviott SD et al. Cytochrome p-450 polymorphisms and response to clopidogrel. N. Engl. J. Med. 360(4), 354–362 (2009).
n Websites101 Genetic testing for health disease and
ancestry. www.23andMe.com
102 Genetic testing for diseases, common conditions and health. www.deCODEme.com
103 Vorhaus D. The Past, Present and Future of DTC Genetic Testing Regulation. Genomics Law Report (5 August 2010). www.genomicslawreport.com/index.php/2010/08/05/the-past-present-and-future-of-dtc-genetic-testing-regulation (Accessed 25 October 2012)
104 Vorhaus, D. Looking Ahead After the FDA’s DTC Meeting. Genomics Law Report (9 March 2011). www.genomicslawreport.com/index.php/2011/03/09/looking-ahead-after-the-fdas-dtc-meeting/#more-5406 (Accessed 23 December 2012)
105 Vorhaus, D. Clearing a Path for DTC Oversight. Genomics Law Report (7 March 2012). www.genomicslawreport.com/index.php/2011/03/07/charting-a-path-for-dtc-oversight (Accessed 25 October 2012)
106 Vorhaus D, MacArthur D, Jostins L. DTC Genetic Testing and the FDA: is there an end in sight to the regulatory uncertainty? Genomics Law Report (16 June 2011). www.genomesunzipped.org/2011/06/dtc-genetic-testing-and-the-fda-is-there-an-end-in-sight-to-the-regulatory-uncertainty.php#more-3681 (Accessed 22 October 2012)
107 bio.logis. www.bio.logis.de
108 Informed Medical Decisions Inc. http://informeddna.com/index.php/23andme/schedule-appointment-23.html (Accessed 25 October 2012)
109 Navigenics. www.navigenics.com
110 Genetic DNA reports. www.pathway.com
111 Rochman B. Test Your DNA for Diseases – No Doctor Required. Time (23 October 2012). http://healthland.time.com/2012/10/23/drugstore-genomes-whos-pushing-the-sequencing-industry/#ixzz2HMFKx9Bm (Accessed 8 January 2013)
112 European Academies Scienctific Advisory Council (EASAC). Direct-To-Consumer Genetic Testing. www.easac.eu/fileadmin/Reports/EASAC_Genetic_Testing_Web_complete.pdf (Accessed 23 October 2012)
113 Vorhaus D. The Scientific Foundation for Personal Genomics: Recommendations from the Joint NIH-CDC Workshop. Genomics Law Report (18 August 2009).
www.genomicslawreport.com/index.php/2011/03/09/looking-ahead-after-the-fdas-dtc-meeting/#more-5406 (Accessed 23 December 2012)
114 US Government Accountability Office (GAO). Direct-to-consumer genetic tests: misleading test results are further complicated by deceptive marketing and other questionable practices. GAO-10–847T (22 July 2010). www.gao.gov/assets/130/125079.pdf (Accessed 22 October 2012)
115 Jostins L, Morley K, MacArthur D. A missed opportunity: what the GAO report could have told us about DTC genetic testing. Genomics Law Report (19 August 2010). www.genomesunzipped.org/2010/08/ a-missed-opportunity-what-the-gao-report-could-have-told-us-about-dtc-genetic-testing.php (Accessed 22 October 2012)
116 US FDA. Letters to Industry (29 November 2012). www.fda.gov/MedicalDevices/ResourcesforYou/Industry/ucm111104.htm (Accessed 23 December 2012)
117 European Science Foundation (ESF). Personalised Medicine for the European Citizen – towards more precise medicine for the diagnosis, treatment and prevention of disease. ESF, Strasbourg, France (2012). www.esf.org/activities/forward-looks/medical-sciences-emrc/current-forward-looks-in-medical-sciences/personalised-medicine-for-the-european-citizen.html (Accessed 24 December 2012)
n Final report of the European Science Foundation’s Forward Look on Personalized Medicine, which contains aspects relevant to beyond-the-clinic pharmacogenetics and pharmacogenomics.
118 Genetics and Public Policy Center. Updated List of DTC Genetic Testing Companies. www.dnapolicy.org/resources/DTCTableAug2011Alphabydisease.pdf (Accessed 27 December 2012)
119 Cure together. www.curetogether.com
120 Genetic testing for health, disease and ancestry. www.lumigenix.com/
121 Gene Planet. www.geneplanet.com
122 Genelex. http://genelex.com/
123 Illumina. www.illumina.com
124 Kimball. Genetic testing in preventative medicine. www.kimballgenetics.com

Pharmacogenomics (2013) 14(4)412 future science group
Review Prainsack & Vayena
125 Knome. The human genome interpretation company. www.knome.com
126 Matrix genomics. www.matrixgenomics.com
127 23andme. www.23andme.com/you/health/drug_response/
128 Bio.logis – personal genomics services. www.bio.logis.de/pharma-sensor/index
129 Theranostics Laboratory. www.theranostics.co.nz