bevacizumab--current status and future directions
TRANSCRIPT

Review
Bevacizumab—current status and future directions
Rachel Midgley* & David Kerr
Department of Clinical Pharmacology and Cancer Therapeutics, Racliffe Infirmary, Woodstock Road, Oxford OX2 6HE, UK
Received 13 January 2005; accepted 2 February 2005
Angiogenesis is crucial to tumour initiation, survival and metastasis. Vascular endothelial growth
factor (VEGF) is one of the most important pro-angiogenic factors in cancer development. Bevacizu-
mab (a humanised monoclonal antibody against VEGF) has a reasonable safety profile and proven
efficacy in a phase III trial in advanced colorectal cancer. Efficacy of Bevacizumab also looks
promising in non small cell lung cancer, renal cancer and a variety of other solid tumours. Questions
still surround optimal dosing and the appropriate selection of patients who are most likely to benefit.
Future trials will address these questions and provide further translational insights.
Key words: angiogenesis, bevacizumab, vascular endothelial growth factor
Introduction to angiogenesis and VEGF
Angiogenesis (the growth of new blood vessels from existing
vessels) is absolutely essential during embryogenesis and in
the growth of long bones in children and adolescents. There-
after, in adult life, angiogenesis occurs in a restricted number
of pathological situations including wound healing, endome-
triosis and the growth of cancers and establishment of their
metastases.
The primary stimulus to angiogenesis is oxygen deprivation.
When this occurs pro-angiogenic factors are released which
activate the formation of new blood vessels through a number
of downstream effects, such as proliferation and migration of
vascular endothelial cells, survival of immature endothelial
cells and induction of vascular permeability in capillaries.
Candidate pro-angiogenic factors include vascular endothelial
growth factor (VEGF), basic fibroblast growth factor (bFGF)
and transforming growth factors alpha and beta (TGFa and
b), the most important of these being VEGF [1, 2]. There are
also anti-angiogenesis factors that have an opposite effect and
it is the balance of pro- and anti-angiogenic factors that deter-
mines the angiogenesis balance (Figure 1).
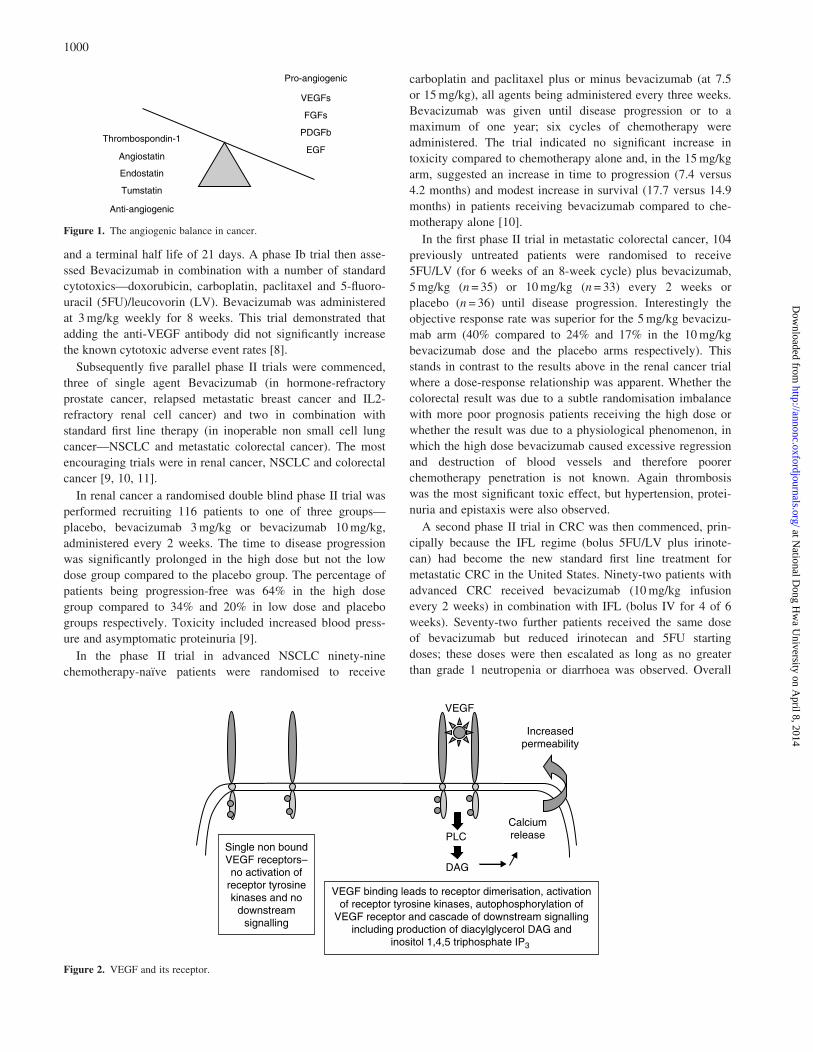
There are six described members of the VEGF family but
VEGF-A (also known as vascular permeability factor [3] or
just VEGF) appears to exert the greatest influence of angio-
genesis during the carcinogenic process. VEGF-A exerts its
influence through binding principally to the VEGF receptor-2,
expressed principally on endothelial cells (Figure 2). This
receptor shares many common characteristics with other mem-
bers of a family of receptors having tyrosine kinase activity,
including several extracellular Ig-like domains, a transmem-
brane region and an intracellular tail with tyrosine kinase
activity. Induction of the kinase activity by VEGF binding
causes a cascade of phosphorylation of at least 46 signalling
molecules.
In the pathogenesis of cancer, VEGF has a number of key
roles. It stimulates excessive angiogenesis, allowing the
tumour to embark upon its exponential growth phase. This
vascularisation also provides an exit route for haematogenous
metastases and allows them to establish themselves at their
final destination. The critical importance of VEGF during
tumorigenesis has been illustrated by a number of obser-
vations: VEGF expression is elevated in the tissues or circula-
tion in many solid tumours [4]; a significant correlation has
been found between plasma VEGF levels and disease stage or
metastasis [5]; pre-clinical experiments showed that anti-
VEGF antibodies inhibited the growth of human tumour cell
lines injected into nude mice [6].
History of bevacizumab
Given this key role, it is not surprising that much effort has
been made to develop agents that block the effects of VEGF,
in an attempt to abrogate the carcinogenic process. The most
well developed of these to date is Bevacizumab (Avastinw),
which is a humanised murine monoclonal antibody against the
VEGF molecule.
The first phase I trial of Bevacizumab began in 1997 [7].
Twenty-five patients with measurable or assessable solid
tumours (sarcoma = 8, renal cell carcinoma (RCC) = 7, breast
cancer = 5, lung cancer = 2) were enrolled and five dose levels
were assessed—0.1, 0.3, 1.0, 3,0 and 10mg/kg. Bevacizumab
was delivered intravenously over 90 minutes on days 0, 28, 35
and 42. One patient with RCC achieved a minor response
with an approximate 25% reduction in the sum of perpendicu-
lar diameters of the pulmonary and lymph node metastases.
48% of the remaining patients achieved disease stabili-
sation. Bevacizumab showed a linear pharmacokinetic profile
*Correspondence to: Dr R. Midgley, Cancer Research UK, ChurchillHospital, Headington, Oxford, UK, OX3 7LJ.E-mail: [email protected]
Annals of Oncology 16: 999–1004, 2005
doi:10.1093/annonc/mdi208
Published online 6 June 2005
q 2005 European Society for Medical Oncology
at National D
ong Hw
a University on A
pril 8, 2014http://annonc.oxfordjournals.org/
Dow
nloaded from
and a terminal half life of 21 days. A phase Ib trial then asse-
ssed Bevacizumab in combination with a number of standard
cytotoxics—doxorubicin, carboplatin, paclitaxel and 5-fluoro-
uracil (5FU)/leucovorin (LV). Bevacizumab was administered
at 3mg/kg weekly for 8 weeks. This trial demonstrated that
adding the anti-VEGF antibody did not significantly increase
the known cytotoxic adverse event rates [8].
Subsequently five parallel phase II trials were commenced,
three of single agent Bevacizumab (in hormone-refractory
prostate cancer, relapsed metastatic breast cancer and IL2-
refractory renal cell cancer) and two in combination with
standard first line therapy (in inoperable non small cell lung
cancer—NSCLC and metastatic colorectal cancer). The most
encouraging trials were in renal cancer, NSCLC and colorectal
cancer [9, 10, 11].
In renal cancer a randomised double blind phase II trial was
performed recruiting 116 patients to one of three groups—
placebo, bevacizumab 3mg/kg or bevacizumab 10mg/kg,
administered every 2 weeks. The time to disease progression
was significantly prolonged in the high dose but not the low
dose group compared to the placebo group. The percentage of
patients being progression-free was 64% in the high dose
group compared to 34% and 20% in low dose and placebo
groups respectively. Toxicity included increased blood press-
ure and asymptomatic proteinuria [9].
In the phase II trial in advanced NSCLC ninety-nine
chemotherapy-naı̈ve patients were randomised to receive
carboplatin and paclitaxel plus or minus bevacizumab (at 7.5
or 15mg/kg), all agents being administered every three weeks.
Bevacizumab was given until disease progression or to a
maximum of one year; six cycles of chemotherapy were
administered. The trial indicated no significant increase in
toxicity compared to chemotherapy alone and, in the 15mg/kg
arm, suggested an increase in time to progression (7.4 versus
4.2 months) and modest increase in survival (17.7 versus 14.9
months) in patients receiving bevacizumab compared to che-
motherapy alone [10].
In the first phase II trial in metastatic colorectal cancer, 104
previously untreated patients were randomised to receive
5FU/LV (for 6 weeks of an 8-week cycle) plus bevacizumab,
5mg/kg (n= 35) or 10mg/kg (n= 33) every 2 weeks or
placebo (n = 36) until disease progression. Interestingly the
objective response rate was superior for the 5mg/kg bevacizu-
mab arm (40% compared to 24% and 17% in the 10mg/kg
bevacizumab dose and the placebo arms respectively). This
stands in contrast to the results above in the renal cancer trial
where a dose-response relationship was apparent. Whether the
colorectal result was due to a subtle randomisation imbalance
with more poor prognosis patients receiving the high dose or
whether the result was due to a physiological phenomenon, in
which the high dose bevacizumab caused excessive regression
and destruction of blood vessels and therefore poorer
chemotherapy penetration is not known. Again thrombosis
was the most significant toxic effect, but hypertension, protei-
nuria and epistaxis were also observed.
A second phase II trial in CRC was then commenced, prin-
cipally because the IFL regime (bolus 5FU/LV plus irinote-
can) had become the new standard first line treatment for
metastatic CRC in the United States. Ninety-two patients with
advanced CRC received bevacizumab (10mg/kg infusion
every 2 weeks) in combination with IFL (bolus IV for 4 of 6
weeks). Seventy-two further patients received the same dose
of bevacizumab but reduced irinotecan and 5FU starting
doses; these doses were then escalated as long as no greater
than grade 1 neutropenia or diarrhoea was observed. Overall
Figure 1. The angiogenic balance in cancer.
Figure 2. VEGF and its receptor.
1000
at National D
ong Hw
a University on A
pril 8, 2014http://annonc.oxfordjournals.org/
Dow
nloaded from

the complete response rate, partial response rate and stabilis-
ation rate were 5.4%, 38% and 36% respectively, giving a
promising overall disease control rate of 79.4% [12].
Based on the results of these two phase II trials and some
ongoing concerns about the safety of the IFL regime, a double
blind randomised phase III three arm study was commenced.
Patients received IFL plus placebo (n= 411), IFL plus bevaci-
zumab (n = 402) or 5FU/LV plus bevacizumab (n= 110).
When acceptable safety of the IFL/bevacizumab combination
was established the third arm stopped recruitment. The
results of the trial are summarised in Table 1. The addition of
bevacizumab to IFL chemotherapy produced significant
improvements in response rate (44.8 versus 34.8%; P = 0.004),
time to progression (10.6 versus 6.2 months; P<0.001) and
median survival (20.3 versus 15.6 months; P<0.001) [13].
Toxicity is still of some concern with this combination. IFL
alone produces grade 3/4 toxicity rates of 30% and 25% for
neutropenia and diarrhoea respectively. Adding bevacizumab
significantly increased grade 3 hypertension rates (11% versus
2.3%, P<0.01), but interestingly did not impact significantly
upon the rates of proteinuria, thrombosis and bleeding. One
major concern was six gastrointestinal perforations occurring
in patients receiving IFL/bevacizumab and this possibility
needs to be highlighted to clinicians who are using the combi-
nation and potential symptom profiles outlined to patients to
allow early intervention.
A number of re-analyses of the toxicity data from these
combined trials were presented at ASCO 2004 (see Table 2).
The authors looked at thrombo-embolism in the phase II and
III CRC trials in more detail and found that although arterial
thrombo-embolism may be slightly increased with bevacizu-
mab (10% versus 4.8% and 3.3% versus 1% in the phase II
and phase III trials respectively), incidence of venous
thrombo-embolism was not increased. They also assessed
whether remaining on bevacizumab during subsequent full
dose anti-coagulation increased the risk of bleeding and,
although numbers were small, there was no evidence to
suggest this. The authors also re-analysed wound healing and
bleeding complications in patients who had undergone pri-
mary cancer surgery between 28 and 60 days prior to com-
mencing bevacizumab therapy. 187 subjects on chemotherapy
plus bevacizumab had undergone surgery compared to 155
subjects on receiving chemotherapy alone. The incidence of
grade 3/4 wound healing problems/bleeding was 1 patient
(0.65%) in the bolus IFL alone arm, 3 patients in the bevaci-
zumab plus IFL arm and no subjects in the bevacizumab plus
5FU/LV arm, revealing no statistically significant difference.
Table 1. Results of the Phase III trial of IFL ± bevacizumab in first line
treatment of advanced colorectal cancer [13]
IFL plusplacebo
IFL plusbevacizumab
P value
Median survival (months) 15.6 20.3 <0.001
One year survival rate (%) 63.4 74.3 <0.001
Progression-freesurvival (months)
6.2 10.6 <0.001
Overall response rate—CR + PR (%)
34.8 44.8 0.004
Median duration of response(months)
7.1 10.4 0.001
Table 2. Bevacizumab at ASCO 2004
Abstract no. and authors Questions addressed and trial type Summary of results
3529 Holmgren et al. Thrombo-embolism re-appraisal withBev (from phase II and phase III trials)
Slight increase risk of arterial embolismbut not venous embolism
3530 Scappaticci et al. Wound healing and bleeding re-appraisal withBev post-surgery (from phase II/III trials)
No increase in rate if start treatmentbetween 28 and 60 days post op
578 Wedam et al. ? Bev with chemo for neoadjuvant therapy ofinflammatory breast ca (exploratory)
Good efficacy and MRI evidence of reducedblood flow with Bev alone
3589 Willett et al. Combination Bev plus chemoradiation inneoadjuvant rectal ca (phase I)
No DLT and excellent efficacy
5539 Mauer et al. Combination Bev + erlotinib for advancedSCC head and neck (phase I)
No DLT even at 15mg/kg/3 weeks.Good disease control rate
2000 Sandler et al. Combination Bev + erlotinib advanced NSCLCpreviously treated (phase I/II)
34 treated in phase II part (15mg/kg/3 weeks Bev)PR 22.5%; MR 5%; SD 35%
4502 Hainsworth et al. Combination Bev (10mg/kg/2weeks) + erlotinibadvanced RCC (phase II)
40 evaluable for efficacy PR 25%;MR 15%; DS 47%. Well tolerated
9012 D’Adamo et al. Combination Bev (15mg/kg/3 weeks) + Doxadvanced soft tissue sarcomas (phase II)
13 patients evaluable PR 14%; SD 59%
3013 Yao et al. Bev versus PEG IFNa in carcinoid tumours (phase II) Too immature for efficacy results. fCT showedrapid reduction tumour blood flow
4009 Kindler et al. Bev (10mg/kg/2weeks) + gemcitabine in chemo-naı̈veadvanced pancreatic cancer (phase II)
42 patients evaluable PR21%; SD 45%.Reasonable tolerability
See text for more detail.
Bev = bevacizumab; DLT= dose limiting toxicity; chemo= chemotherapy; SCC= squamous cell carcinoma; NSCLC=non small cell lung cancer;
RCC= renal cancer; MR=minor response rate; PR= partial response rate; DS = disease stabilisation rate; fCT= functional CT.
1001
at National D
ong Hw
a University on A
pril 8, 2014http://annonc.oxfordjournals.org/
Dow
nloaded from

This augurs well for the use of bevacizumab in the adjuvant
setting in the future.
Current status of bevacizumab
Based on the results of this phase III trial the IFL/bevaci-
zumab (5mg/kg) combination gained FDA approval for the
first line treatment of advanced CRC by the FDA in the Uni-
ted States in February 2004. However much of the rest of the
academic community are awaiting confirmatory evidence
and evaluation of the combination of bevacizumab with better
tolerated chemotherapy regimes. A phase III trial in combi-
nation with oxaliplatin, 5FU and LV is ongoing.
What about patients that are not fit for irinotecan in the first
line treatment of advanced colorectal cancer? The companion
trial to the phase III trial described above randomised 209
patients to receive Roswell Park 5FU/LV (6 of 8 weeks) plus
placebo or bevacizumab 50mg/kg every 2 weeks [11]. The
addition of bevacizumab produced a statistically significant
prolongation of progression-free survival and a trend towards
improved response rate and survival. However again there was
a 2% gastrointestinal perforation rate in the bevacizumab arm
and this needs careful consideration when assessing the risks
and benefits of the addition of bevacizumab in this population.
In the adjuvant setting of colorectal cancer, bevacizumab is
being assessed in combination with capecitabine (1000mg/m2,
14 of 21 days) and irinotecan (250mg/m2 every three weeks)
in the United Kingdom QUASAR 2 trial.
In advanced breast cancer the first phase III trial (n = 462)
comparing capecitabine plus or minus bevacizumab as third
line chemotherapy (after anthracyclines and taxanes) demon-
strated an improved response rate with bevacizumab but no
impact upon progression-free or overall survival [14]. It is
now being assessed in first line metastatic breast cancer in
combination with paclitaxel. Bevacizumab is also being
assessed in a phase III trial in NSCLC (with carboplatin and
paclitaxel); and in the first line treatment of advanced renal
cancer in combination with interferon-a (CALGB 90 206)
where the dose of bevacizumab will be 10mg/kg based on the
phase II trial data for this disease.
Bevacizumab at ASCO 2004
A number of studies related to bevacizumab were presented at
ASCO this year. These can be divided into exploratory, phase
I and phase II trials (Table 2, reference 15).
An exploratory study in inflammatory breast cancer patients
assessed response and angiogenesis after treatment with
bevacizumab (15mg/kg). Sixteen patients received a cycle of
bevacizumab alone followed by six cycles of neoadjuvant
bevacizumab, doxorubicin and docetaxel. Post-mastectomy
and radiation, patients were administered eight further cycles
of bevacizumab (plus or minus hormone therapy depending on
ER status). Tumour biopsies and dynamic contrast-enhanced
MRI were obtained prior to treatment, after the single cycle
of bevacizumab alone and then after cycles 4 and 7 of
combination treatment. Of 10 evaluable patients, nine
achieved a partial response and one demonstrated progressive
disease. Preliminary data suggested a decrease in vascular per-
meability (MRI) and endothelial cell proliferation (Cd31/Ki67
expression) even after the single cycle of bevacizumab alone.
In responding patients there was a trend towards a decrease in
VEGF after bevacizumab alone and in tumour cell prolifer-
ation (Ki67) after chemotherapy and bevacizumab. This is an
interesting mechanistic study and suggests that bevacizumab
warrants further exploration in this setting where treatment is
often difficult and inadequate.
Also presented were two phase I trials. The first was a
study of neoadjuvant bevacizumab, 5FU and radiation fol-
lowed by surgery for primary rectal cancer in nine patients
with T3 or T4, Nx, Mo tumours. Patients received bevaci-
zumab at a dose of 5mg/kg (n= 6) or 10mg/kg (n= 3) every
2 weeks, with bevacizumab therapy commencing 2 weeks
prior to chemoradiation. Surgery was performed 7 weeks after
completion of all therapy. All patients to date had completed
the course of treatment without DLT and pathological review
of the surgical specimens of six of the seven evaluable
patients showed only limited microscopic disease (in keeping
with the lack of macroscopic disease visualised on follow-up
endoscopy prior to surgery). These results demonstrate safety
of the combination and significant clinical activity, again
suggesting that further investigation would be appropriate.
The second phase I study assessed the combination of beva-
cizumab and an epidermal growth factor receptor (EGFR)
inhibitor erlotinib in patients with advanced squamous cell car-
cinoma of the head and neck cancer receiving no more than
one previous therapy for their disease. The rationale for the
combination lies in the observation in pre-clinical studies that
resistance to EGFR inhibitors appears related to angiogenesis.
A fixed dose of erlotinib (150mg orally daily) was adminis-
tered with an escalating dose of bevacizumab (5, 10 and
15mg/kg every 3 weeks). 10 patients were enrolled. Grade 3
diarrhoea, skin rash and lymphopenia were seen in one patient
each. Grade 4 haemorrhage from a tongue tumour was
observed in one patient. No dose limiting toxicity was seen.
One patient gained a partial response with 7 patients achieving
disease stabilisation and a phase II trial is now underway.
The combination was similarly assessed in advanced/recur-
rent NSCLC. A phase I trial first set a maximum tolerated
dose (MTD) of 15mg/kg bevacizumab every 3 weeks in com-
bination with erlotinib 150mg once daily orally. Thirty-four
patients were treated at the MTD in the phase II portion of the
trial. Twenty-four of these patients had received at least two
chemotherapeutic regimes. The partial response rate was
22.5% with minor response in a further 5% and stable disease
in 35%, giving an overall disease control rate of 62.5%, which
compares very well with historical controls treated in this set-
ting. A randomised phase II trial is now planned in a similar
cohort of patients.
Another group assessed the same combination in advanced
renal cancer who had received a maximum of one previous
regimen. Bevacizumab was given at a dose of 10mg/kg every
1002
at National D
ong Hw
a University on A
pril 8, 2014http://annonc.oxfordjournals.org/
Dow
nloaded from

2 weeks and erlotinib 150mg once daily until progression.
Fifty-seven patients were treated, 40 of which were evaluable
for efficacy (at least 8 weeks of therapy). Progression-free sur-
vival at 6 months was 71% with a partial response rate of
25%, a minor response rate of 15% and a disease stabilisation
rate of 47%. Grade 3/4 toxicity rates were low—hypertension
11%, diarrhoea 9%, rash 7% and nausea/vomiting 7%. Again
the substantial clinical activity means that randomised phase
II or even phase III trials should now be initiated.
Bevacizumab was also assessed in phase II trials in a num-
ber of new indications, including soft tissue sarcoma, carci-
noid tumours and advanced pancreatic cancer. Bevacizumab
(15mg/kg) was combined with doxorubicin (75mg/m2), both
given every 3 weeks, in the treatment of soft tissue sarcomas.
The response rate of 14% was no better than historical con-
trols treated with doxorubicin alone; however the authors felt
that the disease stabilisation rate of 59% was encouraging and
warranted further investigation.
Carcinoid tumour patients were randomly assigned to either
bevacizumab (dose not given in abstract) or PEG interferon
2a for the first 18 weeks followed by the combination of the
two. Tumour blood flow was assessed by functional CT. The
early results demonstrated a rapid decrease in tumour blood
flow in patients treated with bevacizumab as opposed to PEG
interferon 2a but the data were too immature to draw any
conclusions about efficacy.
Updated results from a phase II trial of gemcitabine
(1000mg/m2 weekly for 3 out of 4 weeks)/bevacizumab
(10mg/kg every 2 weeks) in chemotherapy-naı̈ve advanced
pancreatic cancer patients were also presented. Forty-two
patients were evaluable for response with a median follow-up
of 5.7 months. The partial response rate was 21% with a dis-
ease stabilisation rate of 45%. Six-month survival was 74%.
There were two deaths, one due to a gastrointestinal bleed and
one secondary to bowel perforation, so clearly these toxicities
are not confined to patients with colorectal cancer. A random-
ised phase III CALGB study is now under development.
Future considerations for bevacizumaband other VEGF inhibitors
It is clear from the studies presented above that the repertoire
of diseases for which bevacizumab may be applicable is
rapidly expanding. It is also apparent that performing properly
designed randomised phase II trials in this ever expanding
area of novel biological agents might reduce the duplication
of studies and allow quicker translation of the most promising
agents into the phase III setting.
In order to increase our ability to select the most promising
anti-angiogenesis drugs overall, and in particular for indivi-
dual patients a number of surrogate endpoints for effect have
been explored. These include treatment-induced depression in
plasma VEGF, reduction in tumour blood flow on functional
CT or MRI or biopsy proof of a decrease in angiogenesis but
to date none of these has been performed in an adequate num-
ber of patients or been correlated in any statistically robust
way with response to promote routine clinical use. An area of
exploration for the future will be studying polymorphisms of
the VEGF molecule itself or its receptor and attempting to
correlate these with tumour response.
One area of confusion surrounding bevacizumab has been
the differential dosing seemingly required for different
tumours, with colorectal cancers requiring only 5mg/kg/
2 weeks compared to 10mg/kg or greater for NSCLC and
renal cancers. It must be remembered that the dose defined for
colorectal cancer was based on a relatively small phase II
study (about 35 patients/arm) and was defined according to
efficacy. With these numbers a slight swing of two or three
patients in either direction (responders being non-responders
or vice versa) would result in a completely different con-
clusion. In the future consideration should be given to dose-
confirmation for biological agents being integrated into large
randomised phase III trials, perhaps posed in a 2�2 factorial
fashion to reduce the numbers of patients required.
One final question has been the conversion of dosing of
bevacizumab into a three-weekly schedule to fit in with other
chemotherapy regimes. At ASCO this year results from the
CRC and NSCLC phase II trials were combined to assess the
pharmacokinetic effect of two-weekly (5mg/kg) versus three-
weekly (7.5mg/kg) dosing on tumour exposure to bevaci-
zumab. The authors concluded that observed and simulated
drug exposure were similar in both arms, due to the slow
clearance and long elimination half life of 20 days for bevaci-
zumab. This answers any concern about the three weekly
schedule and allows QUASAR 2 and other large phase III
trials to proceed without further deliberation.
Acknowledgement
This article first appeared in Japanese in Gan Bunshi-Hyoteki
Chiryo and is published here in English with permission of
the copyright holder. Citations to this article should be to Gan
Bunshi-Hyoteki Chiryo 2005; 3: 124–132.
References
1. Yancapoulos GD, Davis S, Gale NW et al. Vascular specific growth
factors and blood vessel formation. Nature 2000; 407: 242–248.
2. Jain RK. Molecular recognition of vessel maturation. Nat Med 2003;
9: 685–93.
3. Ferrara N. VEGF: an update on biological and therapeutic aspects.
Curr Opin Biotechnol 2000; 11: 617–624.
4. Brown LF, Berse B, Jackman RW et al. Vascular stroma formation in
carcinoma in situ, invasive carcinoma and,metastatic carcinoma of the
breast. Clin Cancer Res 1999; 5: 1041–1056.
5. Karayiannakis AJ, Bolanaki H, Syrigos KN et al. Serum vascular
endothelial growth factor levels in pancreatic cancer patients correlate
with advanced and metastatic disease and poor prognosis. Cancer Lett
2003; 194: 119–124.
6. Kim KJ, Li B, Winer J et al. Inhibition of vascular endothelial growth
factor-induced angiogenesis suppresses tumour growth in vivo. Nature
1993; 362: 841–844.
7. Gordon MS, Margolin K, Talpaz M. Phase I safety and pharmaco-
kinetic study of recombinant human anti-vascular endothelial growth
1003
at National D
ong Hw
a University on A
pril 8, 2014http://annonc.oxfordjournals.org/
Dow
nloaded from

factor in patients with advanced cancer. J Clin Oncol 2001; 19(3):
843–850.
8. Margolin K, Gordon MS, Holmgren E. Phase Ib trial of intravenous
recombinant humanised monoclonal antibody to vascular endothelial
growth factor in combination with chemotherapy in patients with
advanced cancer: Pharmacologic and longterm safety data. J Clin
Oncol 2001; 19(3) 851–856.
9. Yang JC, Haworth L, Sherry RM et al. A randomised trial of bevaci-
zumab, an antivascular endothelial growth factor antibody for meta-
static renal cancer. N Engl J Med 2003; 349: 427–434.
10. Johnson DH, Fehrenbacher L, Novotny WF et al. Randomised phase
II trial comparing bevacizumab plus carboplatin and paclitaxel with
carboplatin and paclitaxel alone in previously untreated metastatic or
locally advanced non small cell lung cancer. J Clin Oncol 22(11):
2184–2191.
11. Kabbinavar F, Hurwitz H, Fehrenbacher L et al. Phase II randomised
trial comparing Bevacizumab plus 5FU/LV with 5FU/LV alone in
patients with metastatic colorectal cancer. J Clin Oncol 2003; 21(1):
60–65.
12. Giantonio BJ, Levy D, O’Dwyer PJ et al. Bevacizumab plus IFL as
frontline therapy for advanced colorectal cancer: Results from ECOG
study 2200. Proc Am Soc Clin Oncol 2003; 22: 1024.
13. Hurwitz H, Fehrenbacher L, Novotny W et al. Bevacizumab plus
irinotecan, flurouracil and leucovorin for metastatic colorectal cancer.
N Engl J Med 2004; 350(23): 2335–2342.
14. Miller KD et al. Phase III trial of capecitabine plus bevacizumab
versus capecitabine alone in women with metastatic breast cancer pre-
viously treated with an anthracycline and a taxane. Breast Cancer Res
76: S37.
15. Assorted authors. Proc Am Soc Clin Oncol 2004. See Table 2.
1004
at National D
ong Hw
a University on A
pril 8, 2014http://annonc.oxfordjournals.org/
Dow
nloaded from