best practice statement - the scottish renal registry
TRANSCRIPT
Scottish Renal Nursing Strategy Group
Best Practice Statement
for the care of Arterio-Venous Fistula and Graft

This Best Practice Statement has been printed with financial and professional support from NHS Quality Improvement Scotland

1
Contents
Introduction to the statement 2
Section 1: Pre-dialysis preparation and care Section 2: Pre-operative preparation and care Section 3: Post-operative preparation and care
Section 4: Access surveillance Section 5: Cannulation Section 6: Patient information
4 5 6 7 8
12
Appendix 1/1a: Pre-operative care good practice example 13
Appendix 2: Post-operative care good practice example 15
Appendix 3: Guidelines non-functioning vascular access good practice example
17
Appendix 4: Cannulation of vascular access 18
Appendix 5: Blood flow rates & needle gauge 20
Appendix 6: Patient information 21
Glossary 22
References 24
Who was involved in developing the statement? 25
2
Introduction to the statement Over the last few years, there has been an increase in the prevalence of renal replacement therapy (RRT) for patients who reach established renal failure. The Scottish Renal Registry report of 2006 indicates that the prevalence of new patients starting renal replacement therapy has continued to increase. The annual take-in rate is approximately 600 per year. Co-morbidity has risen considerably requiring increased nursing intervention. There are ten adult renal units in Scotland with nine satellite or annexe units. In addition there is one paediatric renal unit. The Scottish Renal Nursing Strategy Group has committed to looking at ways in which the services can be developed. The largest growth area is haemodialysis. The philosophy of this group is to identify nursing priorities for renal services within Scotland to provide clear direction for nurses working within the specialty. The strategy will be developed in collaboration with representatives from all Scottish Renal units and in consultation with relevant national groups. The purpose of this best practice statement is to guide all haemodialysis nursing and technical staff in the best way to manage and preserve vascular access. Poor vascular access for haemodialysis may contribute to increased risk of infection, unnecessary repeated admissions to hospital and potentially increased mortality. The National Service Framework for Renal Services suggests that: • all children, young people and adults approaching established renal failure are
to receive timely preparation for renal replacement therapy, so the complications and progression of their disease are minimised, and their choice of clinically appropriate treatment options maximised (standard 2)
• all children, young people and adults with established renal failure are to have
timely and appropriate surgery for vascular or peritoneal access, which is monitored and maintained to achieve maximum longevity (standard 3)
Scottish Renal Association and NHS Quality Improvement Scotland (NHS QIS) standards require that: • 70% of established patients should have functioning arterio-venous fistula or
graft • 60% of new starts should have functioning arterio-venous fistula if known to renal service for more than 3 months. Why fistula first The arterio-venous fistula (AVF) remains the gold standard access to haemodialysis, showing better survival and lower complication rates than grafts and catheters (Brunori et al, 2005). The presence of a catheter and/or its complications may affect the longevity of a native fistula through its earlier utilisation or less favourable maturation (Rayner et al, 2003). The Dialysis
3
Outcomes Quality Initiative (DOQI) guideline 3 states that in order to determine which type of access is most suitable to the individual patient, an evaluation of the patient’s venous, arterial and cardiopulmonary systems must be performed. Previous placement of central venous catheter is associated with central venous stenosis. Central venous catheters should be discouraged as permanent vascular access. In the absence of factors associated with contraindications for the formation of AVF, this would be the first preference for vascular access (DOQI, 2000). Premature cannulation of a fistula may result in a higher incidence of infiltration with associated compression of the vessel by haematoma and permanent loss of the fistula (DOQI guideline 9, 2000). The AVF/graft should be: • patent • palpable with bruit present • clean and free from signs of infection • able to deliver adequate haemodialysis The success of vessel access is best assessed by its capability to supply and return blood to the general circulation at acceptable flow rates, its duration of effective function, the degree of patient discomfort and limitation, and the rate and severity of complications.

Sect
ion
1:
Pre-
dial
ysis
pre
para
tion
and
care
K
ey p
oint
: Fr
eque
nt m
onito
ring
of fi
stul
a pa
ram
eter
s is
requ
ired.
Stat
emen
t R
easo
n fo
r sta
tem
ent
How
is it
bei
ng a
chie
ved
Ref
erra
l for
vas
cula
r acc
ess
at th
e pr
e-di
alys
is s
tage
sho
uld
be m
ade
whe
n th
e pa
tient
is a
ppro
xim
atel
y si
x m
onth
s to
one
yea
r aw
ay fr
om
dial
ysis
.
Pro
gres
sion
can
be
depe
nden
t on
indi
vidu
al d
isea
se p
rogr
essi
on
(O’H
are
et a
l 200
7).
To e
nabl
e pl
anne
d in
terv
entio
n en
surin
g be
st p
erm
anen
t ac
cess
with
few
er c
ompl
icat
ions
.
This
will
als
o al
low
for a
ny re
med
ial i
nter
vent
ion
if re
quire
d.
By
impl
emen
tatio
n of
loca
l pat
ient
pat
hway
and
au
dit.
The
site
of f
istu
la s
houl
d be
iden
tifie
d an
d al
l oth
er c
o-m
orbi
ditie
s sh
ould
be
cons
ider
ed.
To re
duce
inco
nven
ienc
e to
the
patie
nt a
nd fa
cilit
ate
easi
er
care
of f
istu
la s
ite.
To fa
cilit
ate
easi
er a
cces
s of
the
fistu
la d
urin
g ca
nnul
atio
n.
To id
entif
y op
timum
site
for a
fist
ula.
By
mai
ntai
ning
and
sup
porti
ng, o
pen
com
mun
icat
ion
betw
een
patie
nt, n
ursi
ng s
taff
and
surg
eon.
Sta
ff ar
e ab
le to
iden
tify
best
pos
sibl
e fis
tula
site
s.
Pat
ient
s re
quiri
ng v
ascu
lar a
cces
s fo
r ha
emod
ialy
sis
shou
ld h
ave
thei
r vei
ns
pres
erve
d an
d no
t util
ised
for a
ny
inte
rven
tion
befo
re a
cces
s is
cre
ated
.
If ve
ssel
s ar
e ac
cess
ed fr
eque
ntly
for v
enep
unct
ure
the
vess
el b
ecom
es fr
agile
and
may
not
be
sust
aina
ble
as
adeq
uate
vas
cula
r acc
ess
for h
aem
odia
lysi
s.
Onc
e it
is id
entif
ied
that
the
patie
nt re
quire
s ac
cess
sur
gery
, all
heal
thca
re w
orke
rs s
houl
d be
ad
vise
d th
at v
esse
ls o
n “fi
stul
a” a
rm a
re n
ot u
sed
for v
enep
unct
ure/
cann
ulat
ion
or fo
r blo
od
pres
sure
.
The
patie
nt/a
dvoc
ate
shou
ld b
e ad
vise
d of
car
e of
ve
ssel
s.
Dur
ing
inpa
tient
sta
y a
loca
l mea
ns o
f id
entif
icat
ion
is a
pplie
d to
indi
cate
that
this
arm
sh
ould
not
be
used
for v
enep
unct
ure/
cann
ulat
ion
or b
lood
pre
ssur
e m
easu
rem
ent.
Key
cha
lleng
e:
Ens
urin
g re
ason
s fo
r fai
lure
to p
rogr
ess
to th
eatre
are
doc
umen
ted
and
actio
n pl
an is
impl
emen
ted.
4

Sect
ion
2
Pre-
oper
ativ
e pr
epar
atio
n an
d ca
re
Key
poi
nts:
M
inim
um o
f ure
a, e
lect
roly
tes,
full
bloo
d co
unt a
nd c
lotti
ng s
cree
n m
ust b
e ch
ecke
d be
fore
thea
tre.
Fist
ula
map
ping
may
be
impl
emen
ted
at ti
me
of s
urge
ry.
Stat
emen
t R
easo
n fo
r sta
tem
ent
How
is it
bei
ng a
chie
ved
The
patie
nt s
houl
d be
edu
cate
d re
gard
ing
acce
ss fo
rmat
ion
usin
g a
sele
ctio
n of
evi
denc
ed
base
d m
ater
ial t
ailo
red
to s
uit t
he
indi
vidu
al n
eeds
of t
he p
atie
nt.
To e
mpo
wer
the
patie
nt to
mak
e in
form
ed
deci
sion
s ab
out t
he fo
rthco
min
g pr
oced
ure
and
enco
urag
e pa
rtici
patio
n in
reco
mm
ende
d tre
atm
ent (
CS
BS
, sta
ndar
d 12
, 200
2).
Des
igna
ted
pers
on p
rovi
des
info
rmat
ion,
adv
ice
and
supp
ort f
or
patie
nt a
nd c
arer
whe
re a
ppro
pria
te b
efor
e ac
cess
form
atio
n.
A re
cord
is k
ept o
f inf
orm
atio
n di
strib
uted
to p
atie
nts
in th
e pr
e-di
alys
is p
erio
d.
Per
i-ope
rativ
e ca
re s
houl
d be
im
plem
ente
d as
per
loca
l pr
otoc
ol.
To e
nsur
e pa
tient
sui
tabi
lity
and
safe
ty d
urin
g pe
ri-op
erat
ive
perio
d.
Impl
emen
tatio
n of
loca
l pro
toco
l (ap
pend
ix 1
& 1
a).
Sta
ff in
volv
ed in
the
peri-
oper
ativ
e pe
riod
are
fam
iliar
with
loca
l pr
otoc
ol m
inim
um s
houl
d in
clud
e:
ge
nera
l hea
lth re
view
bloo
ds
dr
ugs
bl
ood
pres
sure
5

Sect
ion
3
Post
-ope
rativ
e pr
epar
atio
n an
d ca
re
Stat
emen
t R
easo
n fo
r sta
tem
ent
How
is it
bei
ng a
chie
ved
Pos
t-ope
rativ
e ca
re -
follo
win
g su
rger
y, a
ll pa
tient
s w
ill re
quire
m
onito
ring
of th
eir f
istu
la/g
raft.
Ear
ly d
etec
tion
of c
ompl
icat
ions
. To
mai
ntai
n A
VF/
graf
t pat
ency
. O
bser
vatio
ns a
re p
erfo
rmed
in a
ccor
danc
e w
ith lo
cal p
roto
col a
nd th
e ne
eds
of th
e in
divi
dual
pat
ient
(app
endi
x 2
& 2
a).
Pat
ency
of f
istu
la s
houl
d be
doc
umen
ted.
The
patie
nt is
giv
en a
vaila
ble
advi
ce fo
llow
ing
AV
F/ve
in g
raft
surg
ery.
To e
nsur
e th
at s
taff
and
patie
nt
are
awar
e of
the
appr
opria
te
afte
r car
e fo
llow
ing
acce
ss
form
atio
n.
Loca
l dev
elop
men
t of p
ost-o
pera
tive
guid
elin
es.
Cle
ar a
nd c
onci
se in
form
atio
n an
d ad
vice
sho
uld
be g
iven
rega
rdin
g co
ntin
uing
car
e an
d m
aint
enan
ce o
f fis
tula
pat
ency
(Ode
r,TF
et a
l 200
3).
Key
cha
lleng
es:
Ens
urin
g co
mpr
ehen
sive
trai
ning
and
edu
catio
n of
sta
ff.
E
nsur
ing
that
rele
vant
info
rmat
ion
rega
rdin
g ca
re o
f vas
cula
r acc
ess
acco
mpa
nies
all
patie
nts
to n
on-r
enal
are
as.
6

Sect
ion
4 A
cces
s Su
rvei
llanc
e K
ey p
oint
s:
Pat
ient
sho
uld
be a
sses
sed
pre-
oper
ativ
ely
and
post
ope
rativ
ely.
Ther
e ar
e di
ffere
nt s
tage
s in
the
proc
ess
and
to e
nsur
e ad
equa
te s
urve
illan
ce th
ese
step
s sh
ould
be
follo
wed
.
Stat
emen
t R
easo
n fo
r sta
tem
ent
How
is it
bei
ng a
chie
ved
All
patie
nts
shou
ld h
ave
vasc
ular
as
sess
men
t prio
r to
surg
ery.
To
ass
ess
pate
ncy,
ves
sel s
ize
and
suita
bilit
y fo
r cre
atio
n of
vas
cula
r ac
cess
.
• at
tend
des
igna
ted
vasc
ular
clin
ic
• du
plex
sca
n •
pre-
adm
issi
on a
sses
smen
t •
date
for s
urge
ry.
All
new
vas
cula
r acc
ess
shou
ld b
e re
view
ed w
ithin
48
hour
s of
sur
gery
by
app
ropr
iate
hea
lth p
rofe
ssio
nal.
To a
sses
s su
cces
s of
sur
gery
. Pr
e-di
alys
is p
atie
nts:
•
follo
w-u
p, 4
8 ho
urs
post
-sur
gery
as
per l
ocal
pro
toco
l.
Es
tabl
ishe
d di
alys
is p
atie
nts:
•
revi
ew w
ithin
48h
rs o
f sur
gery
by
seni
or n
urse
or n
ephr
olog
ist.
All
patie
nts:
•
follo
w-u
p, v
ascu
lar a
cces
s cl
inic
with
in s
ix w
eeks
(Kon
ner K
et a
l 20
03).
• re
peat
Dup
lex
scan
if re
quire
d.
Can
nula
tion
diffi
culti
es m
ay o
ccur
in
new
ly e
stab
lishe
d fis
tula
.
Re-
asse
ssm
ent o
f vas
cula
r acc
ess
may
be
requ
ired.
•
disc
uss
with
dia
lysi
s nu
rse
diffi
culti
es e
xper
ienc
ed d
urin
g ca
nnul
atio
n •
refe
r to
vasc
ular
acc
ess
nurs
e or
nep
hrol
ogis
t •
dupl
ex s
can
• re
-ref
er to
sur
geon
.
Rou
tine
surv
eilla
nce
of v
ascu
lar
acce
ss s
houl
d be
und
erta
ken
and
docu
men
ted.
Bea
thar
d G
200
3).
Ear
ly d
etec
tion
and
treat
men
t of
pote
ntia
l pro
blem
s w
ith e
stab
lishe
d va
scul
ar a
cces
s.
Pre-
dial
ysis
pat
ient
s:
• ro
utin
ely
asse
ss a
t low
cle
aran
ce c
linic
, onl
y re
ferr
ed b
ack
to
vasc
ular
acc
ess
nurs
e if
com
plic
atio
n oc
curs
. Es
tabl
ishe
d di
alys
is p
atie
nts:
•
min
imum
6 m
onth
ly b
lood
flow
mon
itorin
g/re
circ
ulat
ion/
trans
onic
•
rout
ine
mon
itorin
g of
arte
rial a
nd v
enou
s pr
essu
re
• hi
ghlig
ht a
ny c
ompl
icat
ion
to v
ascu
lar a
cces
s nu
rse/
neph
rolo
gist
s •
inte
rven
tiona
l Rad
iolo
gist
. w
ww
.vas
cula
racc
esss
ocie
ty.c
om/g
uide
lines
Pat
ient
s w
ith u
nexp
ecte
d no
n-fu
nctio
ning
vas
cula
r acc
ess.
R
escu
e va
scul
ar a
cces
s w
ithou
t de
lay.
•
emer
genc
y ad
mis
sion
pro
toco
l •
imm
edia
te re
ferr
al t
o va
scul
ar a
cces
s nu
rse/
neph
rolo
gist
s •
refe
r to
surg
eon
or in
terv
entio
nal r
adio
logi
st.
App
endi
x 3
Key
cha
lleng
e:
Ens
urin
g th
at re
leva
nt in
form
atio
n re
gard
ing
care
of v
ascu
lar a
cces
s ac
com
pani
es a
ll pa
tient
s to
non
-ren
al a
reas
.
7
Sect
ion
5
Can
nula
tion
Stat
emen
t R
easo
n fo
r sta
tem
ent
How
is it
bei
ng a
chie
ved
New
fist
ula
shou
ld b
e ex
amin
ed b
y ne
phro
logi
sts/
vasc
ular
sur
geon
or
desi
gnat
ed s
enio
r ren
al n
urse
prio
r to
first
ca
nnul
atio
n.
It is
ess
entia
l tha
t vas
cula
r acc
ess
shou
ld b
e:
• fre
e fro
m re
dnes
s •
free
from
sig
ns o
f inf
ectio
n •
brui
t is
pres
ent.
Stri
ct a
sept
ic te
chni
que
shou
ld b
e us
ed to
cl
ean
the
fistu
la s
ite p
rior t
o ca
nnul
atio
n, n
on-
ster
ile g
love
s sh
ould
be
wor
n du
ring
the
proc
edur
e
Firs
t and
sub
sequ
ent c
annu
latio
ns w
hile
fis
tula
is d
evel
opin
g ar
e pe
rform
ed b
y de
sign
ated
sta
ff m
embe
rs.
Cho
ice
of s
ites
is u
sual
ly d
eter
min
ed b
y th
e se
nior
rena
l nur
se.
Use
2 x
17-
gaug
e ne
edle
s O
R if
dia
lysi
s ca
thet
er in
pla
ce 1
x 1
7-ga
uge
need
le fo
r ar
teria
l lin
e an
d ca
thet
er a
s ve
nous
retu
rn
line.
Kee
p ne
edle
s a
min
imum
of 1
.5-2
cm
aw
ay fr
om a
nast
omos
is u
nles
s us
ing
butto
nhol
e te
chni
que.
To e
stab
lish
read
ines
s fo
r can
nula
tion.
To e
nsur
e co
ntin
uity
and
can
nula
tion
by s
taff
with
sui
tabl
e le
vel o
f kno
wle
dge
and
dem
onst
ratin
g be
st p
ract
ice
cann
ulat
ion
tech
niqu
e.
To p
reve
nt b
leed
ing
into
sur
roun
ding
tiss
ue.
To p
reve
nt c
onta
min
atio
n an
d m
inim
ise
trans
fer o
f ski
n flo
ra d
urin
g ca
nnul
atio
n pr
oces
s.
Aqu
eous
chl
orhe
xidi
ne 0
.25%
- 2%
is
reco
mm
ende
d fo
r cle
anin
g th
e fis
tula
site
.
All
patie
nts
shou
ld w
ash
thei
r han
ds a
nd
fistu
la a
rm w
hen
they
arr
ive
at th
e di
alys
is
unit.
To p
reve
nt d
evel
opm
ent o
f pse
udo-
aneu
rysm
use
of ro
pe la
dder
or b
utto
nhol
e ca
nnul
atio
n is
reco
mm
ende
d (B
all L
200
6).
Sm
all g
auge
nee
dles
to m
inim
ise
risk
of
infil
tratio
n, m
inim
um d
ista
nce
away
from
an
asto
mos
is to
pre
vent
dam
age
to
anas
tom
osis
.
Loca
l pol
icy
in p
lace
for
exam
inat
ion
of n
ew fi
stul
a.
App
endi
x 4
Loca
l pol
icy
in p
lace
and
m
echa
nism
for a
ssig
nmen
t of
sta
ff to
initi
al c
annu
latio
n.
Loca
l hep
arin
pol
icy
in p
lace
. Lo
cal p
olic
y in
pla
ce, s
taff
and
patie
nt e
duca
tion
on
hand
was
hing
. U
se o
f KD
OQ
I (20
00)
guid
elin
es.
Loca
l Pol
icy
in p
lace
. S
taff
educ
atio
n.
Aud
it.
8
A to
urni
quet
sho
uld
be a
pplie
d to
the
uppe
r ar
m s
o th
at it
is ti
ght e
noug
h to
dila
te th
e ve
ssel
or i
mpe
de v
enou
s ou
tflow
(Bal
l L
2005
).
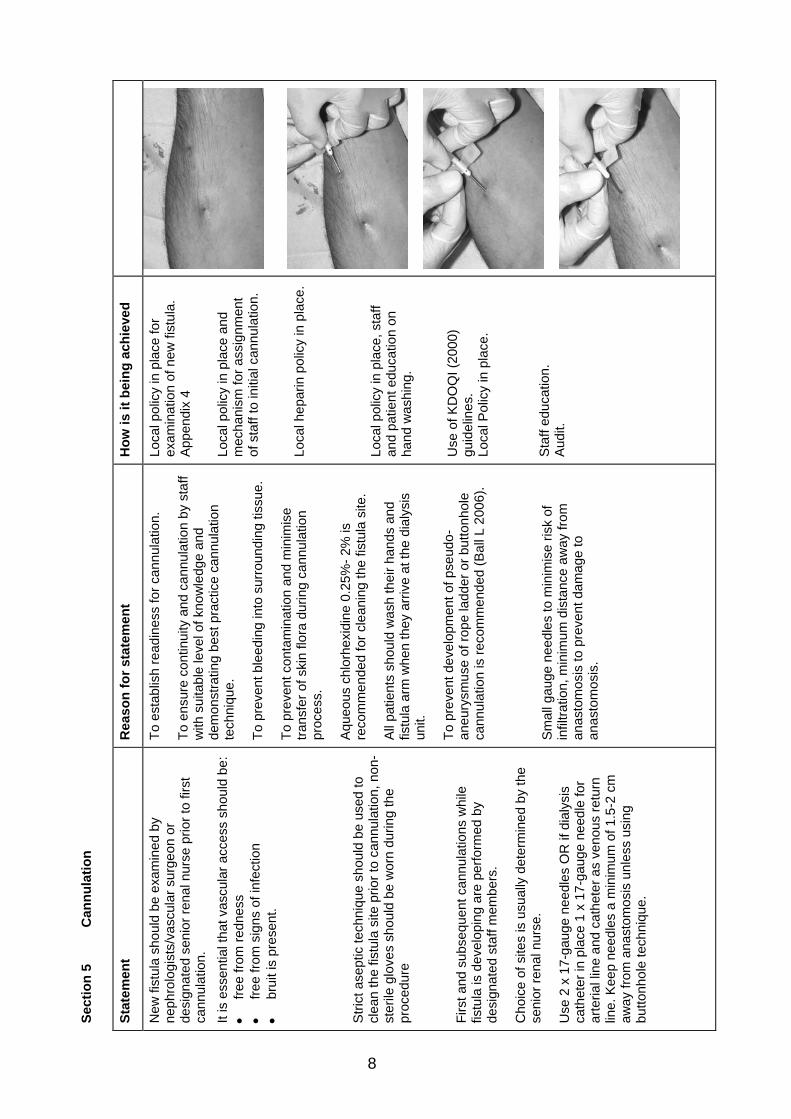
The
patie
nt m
ay b
e en
cour
aged
to g
rip th
eir
fistu
la a
rm in
stea
d of
usi
ng a
tour
niqu
et.
Gen
tly p
ull t
he s
kin
in th
e op
posi
te d
irect
ion
to th
e ne
edle
inse
rtion
and
can
nula
te th
e fis
tula
usi
ng a
25-
degr
ee a
ngle
, with
the
beve
l of t
he n
eedl
e U
P. T
ape
need
le a
t the
an
gle
of in
serti
on
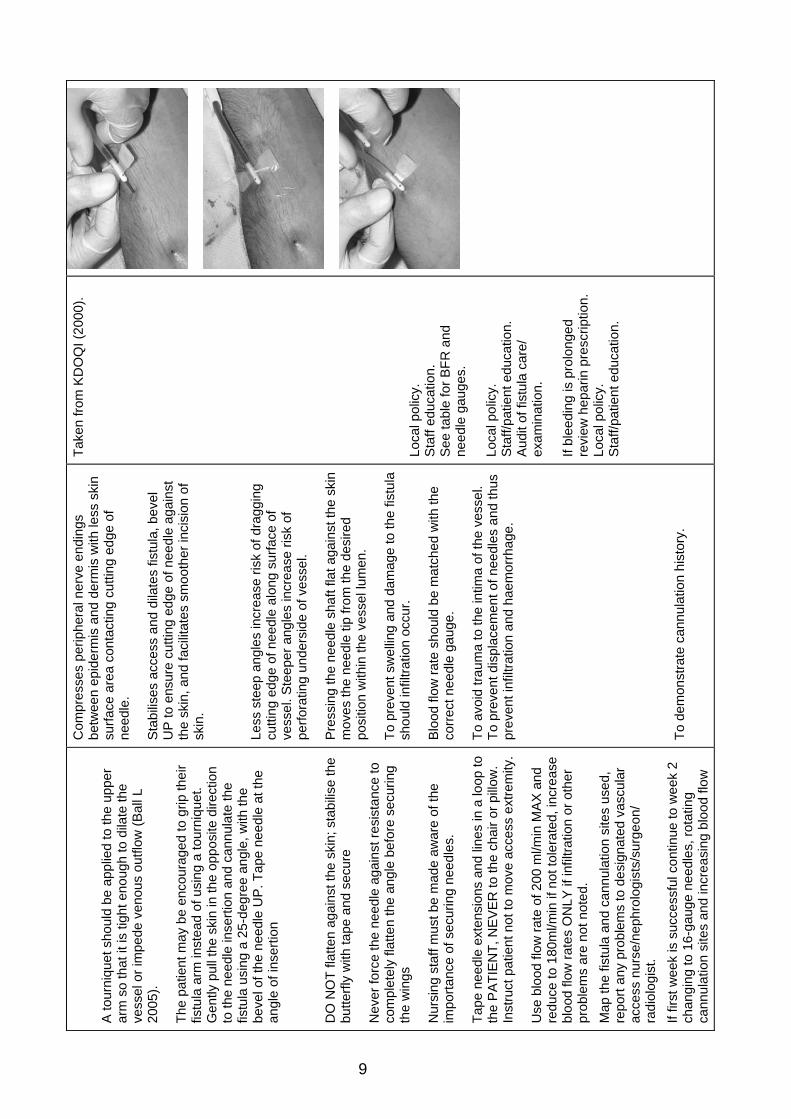
DO
NO
T fla
tten
agai
nst t
he s
kin;
sta
bilis
e th
e bu
tterfl
y w
ith ta
pe a
nd s
ecur
e
Nev
er fo
rce
the
need
le a
gain
st re
sist
ance
to
com
plet
ely
flatte
n th
e an
gle
befo
re s
ecur
ing
the
win
gs
Nur
sing
sta
ff m
ust b
e m
ade
awar
e of
the
impo
rtanc
e of
sec
urin
g ne
edle
s.
Tape
nee
dle
exte
nsio
ns a
nd li
nes
in a
loop
to
the
PA
TIE
NT,
NE
VE
R to
the
chai
r or p
illow
. In
stru
ct p
atie
nt n
ot to
mov
e ac
cess
ext
rem
ity.
Use
blo
od fl
ow ra
te o
f 200
ml/m
in M
AX
and
re
duce
to 1
80m
l/min
if n
ot to
lera
ted,
incr
ease
bl
ood
flow
rate
s O
NLY
if in
filtra
tion
or o
ther
pr
oble
ms
are
not n
oted
. M
ap th
e fis
tula
and
can
nula
tion
site
s us
ed,
repo
rt an
y pr
oble
ms
to d
esig
nate
d va
scul
ar
acce
ss n
urse
/nep
hrol
ogis
ts/s
urge
on/
radi
olog
ist.
If fir
st w
eek
is s
ucce
ssfu
l con
tinue
to w
eek
2 ch
angi
ng to
16-
gaug
e ne
edle
s, ro
tatin
g ca
nnul
atio
n si
tes
and
incr
easi
ng b
lood
flow
Com
pres
ses
perip
hera
l ner
ve e
ndin
gs
betw
een
epid
erm
is a
nd d
erm
is w
ith le
ss s
kin
surfa
ce a
rea
cont
actin
g cu
tting
edg
e of
ne
edle
.
Sta
bilis
es a
cces
s an
d di
late
s fis
tula
, bev
el
UP
to e
nsur
e cu
tting
edg
e of
nee
dle
agai
nst
the
skin
, and
faci
litat
es s
moo
ther
inci
sion
of
skin
.
Less
ste
ep a
ngle
s in
crea
se ri
sk o
f dra
ggin
g cu
tting
edg
e of
nee
dle
alon
g su
rface
of
vess
el. S
teep
er a
ngle
s in
crea
se ri
sk o
f pe
rfora
ting
unde
rsid
e of
ves
sel.
Pre
ssin
g th
e ne
edle
sha
ft fla
t aga
inst
the
skin
m
oves
the
need
le ti
p fro
m th
e de
sire
d po
sitio
n w
ithin
the
vess
el lu
men
.
To p
reve
nt s
wel
ling
and
dam
age
to th
e fis
tula
sh
ould
infil
tratio
n oc
cur.
Blo
od fl
ow ra
te s
houl
d be
mat
ched
with
the
corr
ect n
eedl
e ga
uge.
To a
void
trau
ma
to th
e in
tima
of th
e ve
ssel
. To
pre
vent
dis
plac
emen
t of n
eedl
es a
nd th
us
prev
ent i
nfilt
ratio
n an
d ha
emor
rhag
e.
To d
emon
stra
te c
annu
latio
n hi
stor
y.
Take
n fro
m K
DO
QI (
2000
).
Loca
l pol
icy.
S
taff
educ
atio
n.
See
tabl
e fo
r BFR
and
ne
edle
gau
ges.
Lo
cal p
olic
y.
Sta
ff/pa
tient
edu
catio
n.
Aud
it of
fist
ula
care
/ ex
amin
atio
n.
If bl
eedi
ng is
pro
long
ed
revi
ew h
epar
in p
resc
riptio
n.
Loca
l pol
icy.
S
taff/
patie
nt e
duca
tion.
9

rate
. W
eek
3: a
s w
eek
2 or
if to
lera
ted
wel
l in
crea
se to
14/
15-g
auge
nee
dles
and
re
quire
d B
FR.
Infil
tratio
n gu
idel
ines
: •
if th
e fis
tula
infil
trate
s le
t it r
est f
or 1
wee
k th
en g
o ba
ck to
sm
alle
r gau
ge n
eedl
es.
Not
ify v
ascu
lar a
cces
s nu
rse/
neph
rolo
gist
• if
it in
filtra
tes
a se
cond
tim
e re
st fo
r 2
wee
ks a
nd th
en re
duce
nee
dle
size
. N
otify
vas
cula
r acc
ess
nurs
e/ne
phro
logi
st
•
if in
filtra
tion
occu
rs a
third
tim
e no
tify
desi
gnat
ed v
ascu
lar a
cces
s nu
rse/
co-
ordi
nato
r/nep
hrol
ogis
t/rad
iolo
gist
/ su
rgeo
n.
To re
ach
optim
um d
eliv
ered
blo
od fl
ow a
nd
dial
ysis
ade
quac
y.
To p
reve
nt fu
rther
dam
age
to fi
stul
a, a
nd
allo
w h
ealin
g.
Con
secu
tive
infil
tratio
n co
uld
sign
ify a
pr
oble
m w
ith th
e fis
tula
whi
ch re
quire
s ra
diol
ogic
al o
r sur
gica
l int
erve
ntio
n.
Loca
l pol
icy.
A
ccur
ate
docu
men
tatio
n at
al
l sta
ges.
A
ppen
dix
5
10
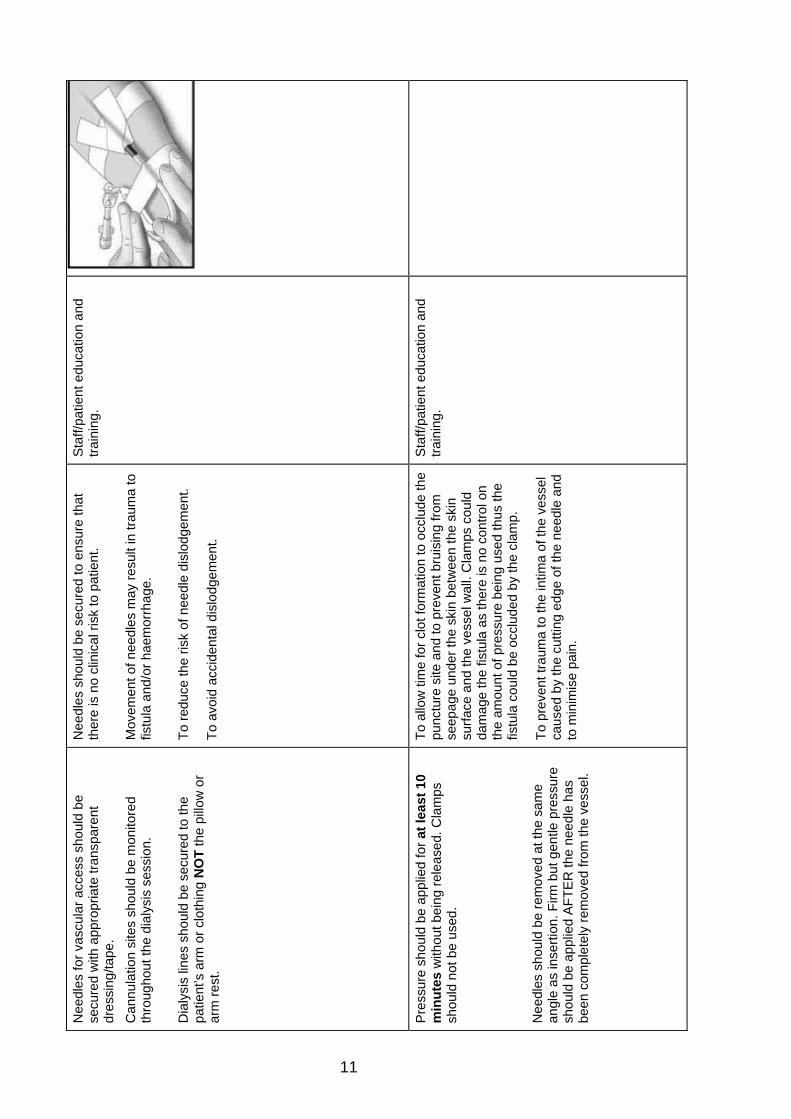
Nee
dles
for v
ascu
lar a
cces
s sh
ould
be
secu
red
with
app
ropr
iate
tran
spar
ent
dres
sing
/tape
. C
annu
latio
n si
tes
shou
ld b
e m
onito
red
thro
ugho
ut th
e di
alys
is s
essi
on.
Dia
lysi
s lin
es s
houl
d be
sec
ured
to th
e pa
tient
’s a
rm o
r clo
thin
g N
OT
the
pillo
w o
r ar
m re
st.
Nee
dles
sho
uld
be s
ecur
ed to
ens
ure
that
th
ere
is n
o cl
inic
al ri
sk to
pat
ient
. M
ovem
ent o
f nee
dles
may
resu
lt in
trau
ma
to
fistu
la a
nd/o
r hae
mor
rhag
e.
To re
duce
the
risk
of n
eedl
e di
slod
gem
ent.
To a
void
acc
iden
tal d
islo
dgem
ent.
Sta
ff/pa
tient
edu
catio
n an
d tra
inin
g.
Pre
ssur
e sh
ould
be
appl
ied
for a
t lea
st 1
0 m
inut
es w
ithou
t bei
ng re
leas
ed. C
lam
ps
shou
ld n
ot b
e us
ed.
Nee
dles
sho
uld
be re
mov
ed a
t the
sam
e an
gle
as in
serti
on. F
irm b
ut g
entle
pre
ssur
e sh
ould
be
appl
ied
AFT
ER
the
need
le h
as
been
com
plet
ely
rem
oved
from
the
vess
el.
To a
llow
tim
e fo
r clo
t for
mat
ion
to o
cclu
de th
e pu
nctu
re s
ite a
nd to
pre
vent
bru
isin
g fro
m
seep
age
unde
r the
ski
n be
twee
n th
e sk
in
surfa
ce a
nd th
e ve
ssel
wal
l. C
lam
ps c
ould
da
mag
e th
e fis
tula
as
ther
e is
no
cont
rol o
n th
e am
ount
of p
ress
ure
bein
g us
ed th
us th
e fis
tula
cou
ld b
e oc
clud
ed b
y th
e cl
amp.
To p
reve
nt tr
aum
a to
the
intim
a of
the
vess
el
caus
ed b
y th
e cu
tting
edg
e of
the
need
le a
nd
to m
inim
ise
pain
.
Sta
ff/pa
tient
edu
catio
n an
d tra
inin
g.
11
12
Sect
ion
6
Patie
nt In
form
atio
n St
atem
ent
Rea
son
for s
tate
men
t H
ow is
it b
eing
ach
ieve
d
All
patie
nts
shou
ld b
e in
form
ed
abou
t sim
ple
emer
genc
y pr
oced
ures
and
how
to b
est c
are
for t
heir
dial
ysis
acc
ess.
Pat
ient
mus
t be
awar
e of
wha
t ac
tion
to ta
ke in
eve
nt o
f ha
emor
rhag
e.
Pat
ient
pla
ys a
n im
porta
nt ro
le in
th
e de
velo
pmen
t and
pr
eser
vatio
n of
the
fistu
la a
nd in
ea
rly d
etec
tion
of c
ompl
icat
ions
.
Com
plic
atio
ns m
ay in
clud
e th
e fo
llow
ing:
infe
ctio
n
haem
orrh
age
thro
mbo
sis
is
chae
mia
para
sthe
sia
(Ste
al
synd
rom
e)
Pat
ient
sho
uld
be p
rovi
ded
with
info
rmat
ion
rega
rdin
g th
eir a
cces
s si
te th
roug
h ea
sily
und
erst
ood
verb
al a
nd w
ritte
n co
mm
unic
atio
n.
A re
cord
is k
ept o
f inf
orm
atio
n gi
ven
to p
atie
nts.
12

13
Appendix 1 Vascular access creation – Pre-dialysis patients
(LA/GA - Day Cases)
FISTULA CREATION – CHECK LIST
Patient referred to vascular surgeon from low clearance clinic when creatinine: > 300 umol/l diabetic
> 400 umol/l non diabetic
Patient reviewed by vascular surgeon: • vascular access assessed • further investigations/tests
arranged
Surgeon’s secretary arranges admission list for access creation and informs: • day surgery unit (DSU) • anaesthetic secretary • renal unit sister • pre-dialysis nurse/vascular access nurse • pre-dialysis patients highlighted and LA/GA indicated
- LA/GA indicated
1. Pre-dialysis/vascular a nurse will: • contact patient to discuss admission details • arrange for patient to attend renal department (Fri) prior to theatre (Tues) for pre-theatre assessment
o Us and Es, bone profile, glucose and FBC o coagulation screen o MRSA screening o fluid assessment o medication check
• arrange a pre-operative visit to DSU • give stress ball & explain pre- and post-operative access care to patient • inform SHO of blood results and arrange for doctor’s assessment • arrange for anaesthetic assessment GA: 12 lead ECG, chest x-ray and review by anaesthetist
arm block: review by anaesthetist 2. SHO will:
• document patients blood results and general condition in case notes and act on results • arrange admission to ward if patients condition/blood results require • commence appropriate antiplatelet medication if admitted, ward staff will liaise with DSU – • if patient is diabetic and having a local anaesthetic, fasting is not required on morning of theatre - breakfast can be
taken as normal • anaesthetist will assess whether GA patients require to be admitted/fasted prior to theatre • if patient is well & blood results stable then patient can go home and attend DSU as previously arranged • vascular surgeon will gain consent from patient in DSU just prior to theatre
DSU will inform patient in writing re: admission details and provide any advice/instructions that are required (DSU Booklet sent out to patient).
1. Patient attends DSU for surgery. 2. Patient will be reviewed by vascular surgeon and anaesthetist post-operative (if required). 3. GA patients may be required to remain in DSU until early evening for post-operative observations. 4. Upon discharge DSU staff will provide patients with:
• guidelines for care of fistula – post-op & long term care • vascular out-patient clinic appointment for fistula review with vascular access surgeon 2-4 weeks post-op • emergency contact numbers • arrangements for district nurse to review wound 3 days post-operative.
5. Pre-dialysis nurse will follow patient up at home and at clinics.
Assessment letter/report sent to: • referring Physician • pre-dialysis nurse • vascular access nurse • RDU Sister
14
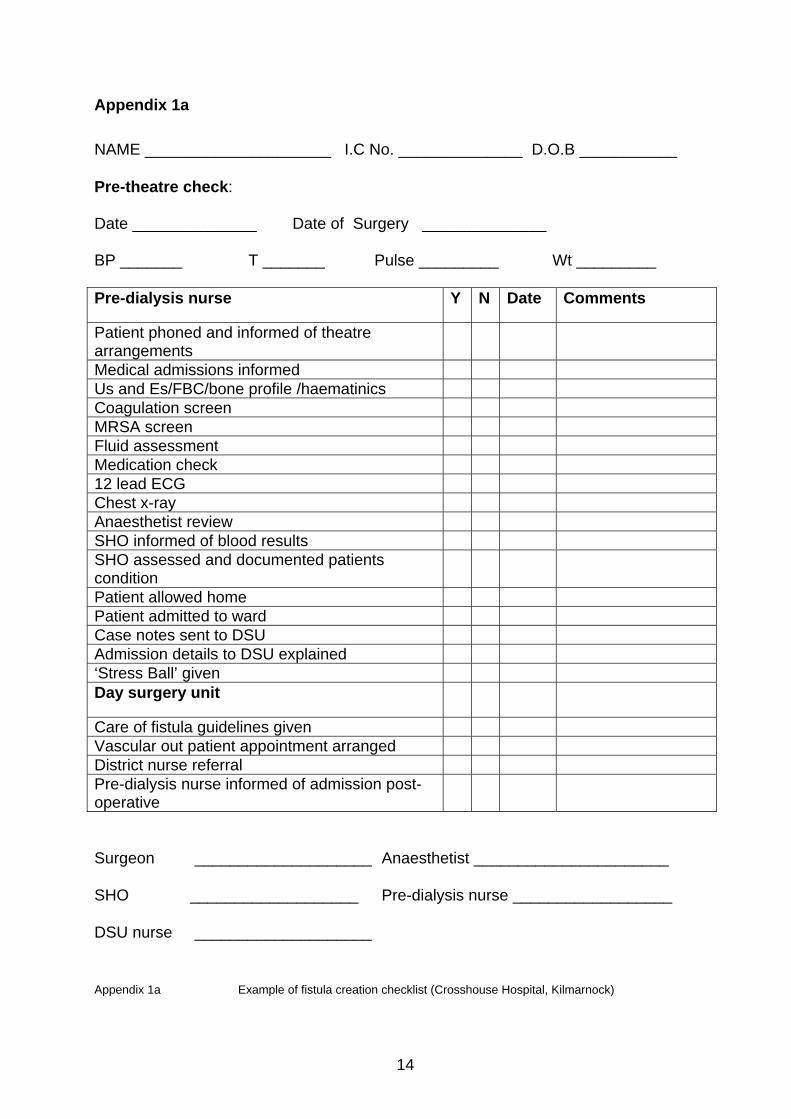
Appendix 1a
NAME _____________________ I.C No. ______________ D.O.B ___________ Pre-theatre check: Date ______________ Date of Surgery ______________ BP _______ T _______ Pulse _________ Wt _________ Pre-dialysis nurse
Y N Date Comments
Patient phoned and informed of theatre arrangements
Medical admissions informed Us and Es/FBC/bone profile /haematinics Coagulation screen MRSA screen Fluid assessment Medication check 12 lead ECG Chest x-ray Anaesthetist review SHO informed of blood results SHO assessed and documented patients condition
Patient allowed home Patient admitted to ward Case notes sent to DSU Admission details to DSU explained ‘Stress Ball’ given Day surgery unit
Care of fistula guidelines given Vascular out patient appointment arranged District nurse referral Pre-dialysis nurse informed of admission post-operative
Surgeon ____________________ Anaesthetist ______________________ SHO ___________________ Pre-dialysis nurse __________________ DSU nurse ____________________ Appendix 1a Example of fistula creation checklist (Crosshouse Hospital, Kilmarnock)
15
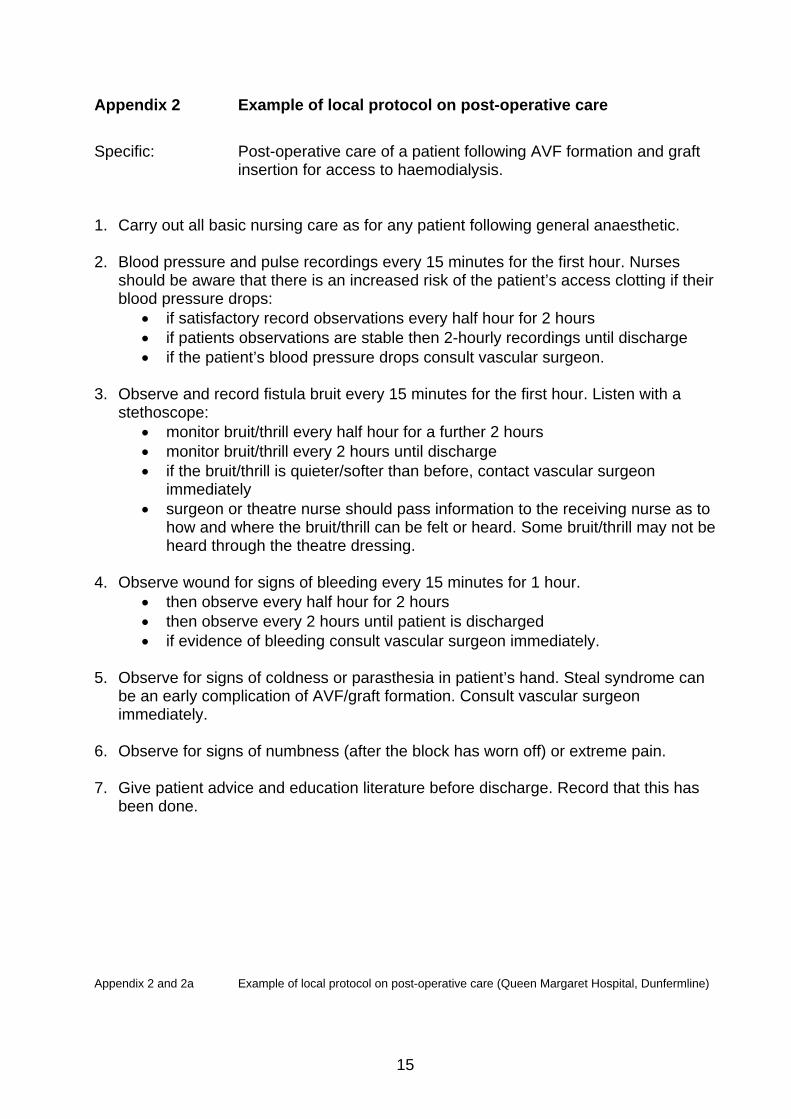
Appendix 2 Example of local protocol on post-operative care
Specific: Post-operative care of a patient following AVF formation and graft
insertion for access to haemodialysis.
1. Carry out all basic nursing care as for any patient following general anaesthetic. 2. Blood pressure and pulse recordings every 15 minutes for the first hour. Nurses
should be aware that there is an increased risk of the patient’s access clotting if their blood pressure drops:
• if satisfactory record observations every half hour for 2 hours • if patients observations are stable then 2-hourly recordings until discharge • if the patient’s blood pressure drops consult vascular surgeon.
3. Observe and record fistula bruit every 15 minutes for the first hour. Listen with a
stethoscope: • monitor bruit/thrill every half hour for a further 2 hours • monitor bruit/thrill every 2 hours until discharge • if the bruit/thrill is quieter/softer than before, contact vascular surgeon
immediately • surgeon or theatre nurse should pass information to the receiving nurse as to
how and where the bruit/thrill can be felt or heard. Some bruit/thrill may not be heard through the theatre dressing.
4. Observe wound for signs of bleeding every 15 minutes for 1 hour.
• then observe every half hour for 2 hours • then observe every 2 hours until patient is discharged • if evidence of bleeding consult vascular surgeon immediately.
5. Observe for signs of coldness or parasthesia in patient’s hand. Steal syndrome can be an early complication of AVF/graft formation. Consult vascular surgeon immediately.
6. Observe for signs of numbness (after the block has worn off) or extreme pain. 7. Give patient advice and education literature before discharge. Record that this has
been done.
Appendix 2 and 2a Example of local protocol on post-operative care (Queen Margaret Hospital, Dunfermline)
16
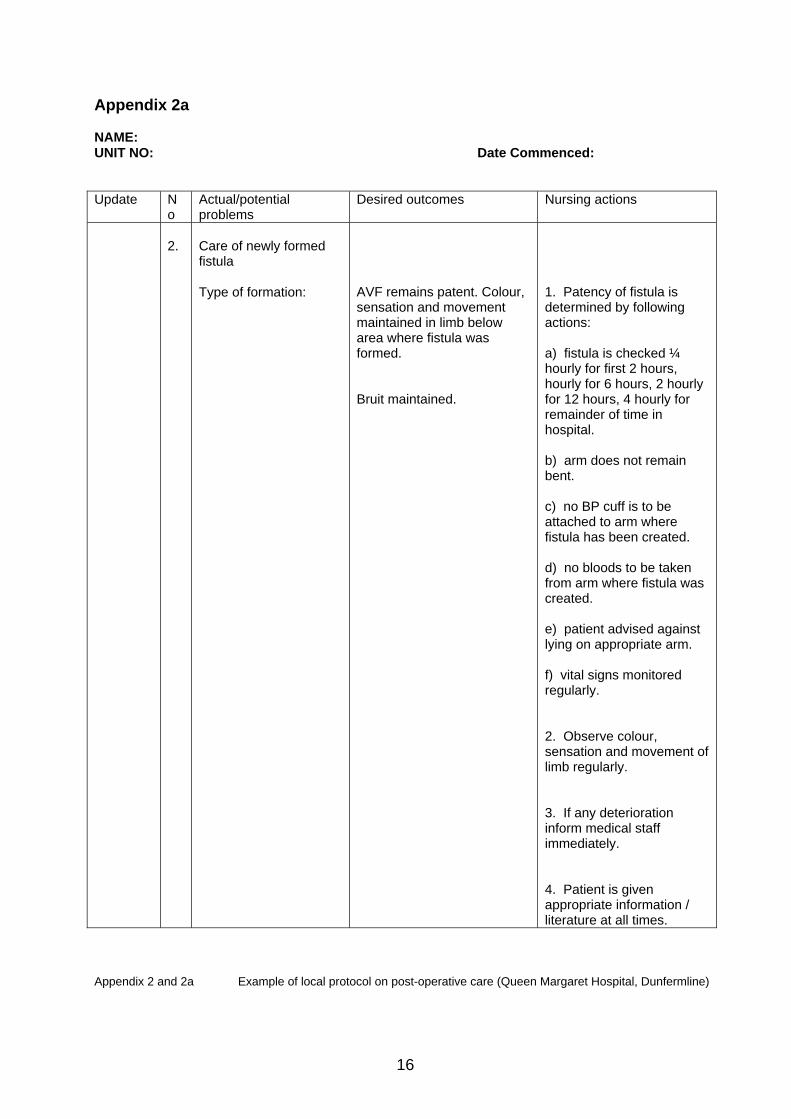
Appendix 2a NAME: UNIT NO: Date Commenced: Update N
o Actual/potential problems
Desired outcomes Nursing actions
2.
Care of newly formed fistula Type of formation:
AVF remains patent. Colour, sensation and movement maintained in limb below area where fistula was formed. Bruit maintained.
1. Patency of fistula is determined by following actions: a) fistula is checked ¼ hourly for first 2 hours, hourly for 6 hours, 2 hourly for 12 hours, 4 hourly for remainder of time in hospital. b) arm does not remain bent. c) no BP cuff is to be attached to arm where fistula has been created. d) no bloods to be taken from arm where fistula was created. e) patient advised against lying on appropriate arm. f) vital signs monitored regularly. 2. Observe colour, sensation and movement of limb regularly. 3. If any deterioration inform medical staff immediately. 4. Patient is given appropriate information / literature at all times.
Appendix 2 and 2a Example of local protocol on post-operative care (Queen Margaret Hospital, Dunfermline)
17
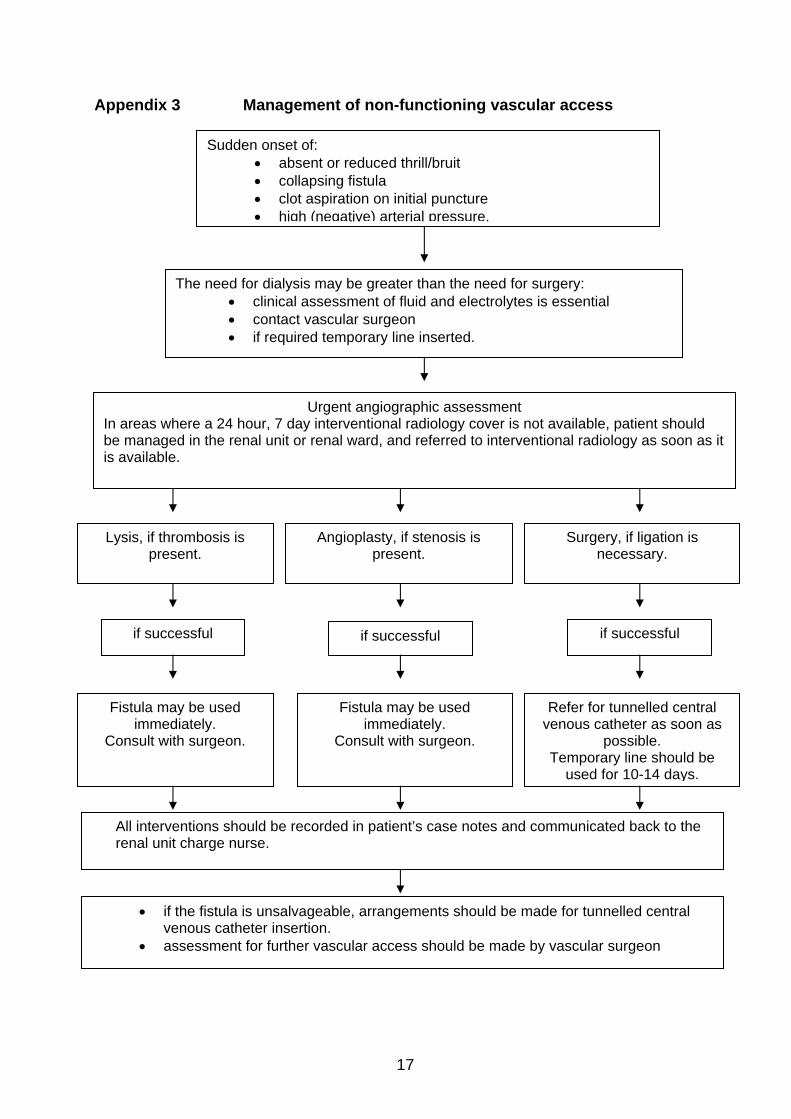
Appendix 3 Management of non-functioning vascular access
Appendix 4
Sudden onset of: • absent or reduced thrill/bruit • collapsing fistula • clot aspiration on initial puncture • high (negative) arterial pressure.
The need for dialysis may be greater than the need for surgery: • clinical assessment of fluid and electrolytes is essential • contact vascular surgeon • if required temporary line inserted.
Urgent angiographic assessment In areas where a 24 hour, 7 day interventional radiology cover is not available, patient should be managed in the renal unit or renal ward, and referred to interventional radiology as soon as it is available.
Lysis, if thrombosis is present.
Angioplasty, if stenosis is present.
Surgery, if ligation is necessary.
Fistula may be used immediately.
Consult with surgeon.
Fistula may be used immediately.
Consult with surgeon.
Refer for tunnelled central venous catheter as soon as
possible. Temporary line should be
used for 10-14 days.
if successful if successful if successful
• if the fistula is unsalvageable, arrangements should be made for tunnelled central venous catheter insertion.
• assessment for further vascular access should be made by vascular surgeon
All interventions should be recorded in patient’s case notes and communicated back to the renal unit charge nurse.

18
Appendix 4 Cannulation of new AVFs and grafts Purpose: To successfully cannulate new AVF and to prevent infiltration. Policy:
Newly created primary AVFs shall be allowed to develop for at least 8 to 12 weeks prior to cannulation. Initial attempts to perform dialysis via new fistulas shall proceed with caution. Without exception, fistulas shall not be progressed faster than these guidelines without consultation with vascular surgeon, vascular access nurse or nephrologist. All healthcare professionals are responsible for implementing this policy. Procedure: 1. Obtain order from vascular surgeon or nephrologist to begin cannulation of fistula 8
to 12 weeks after creation. All new fistulas should be examined by surgeon, nephrologist and designated staff member before cannulation is initiated.
2. Only staff identified as demonstrating best cannulation practice techniques should be assigned to cannulate newly developing fistulas.
3. Always use a tourniquet, even with well-developed fistulas. No exceptions.
4. Explain procedure to patient.
5. Educate patient on: • checking the access daily for a thrill and for signs and symptoms of infection • performing fistula exercises to promote maturation process • understanding that haematoma could occur most likely during the first two weeks
of using the access • for infiltrations, provide written materials about icing, elevation, and heat
application.
19
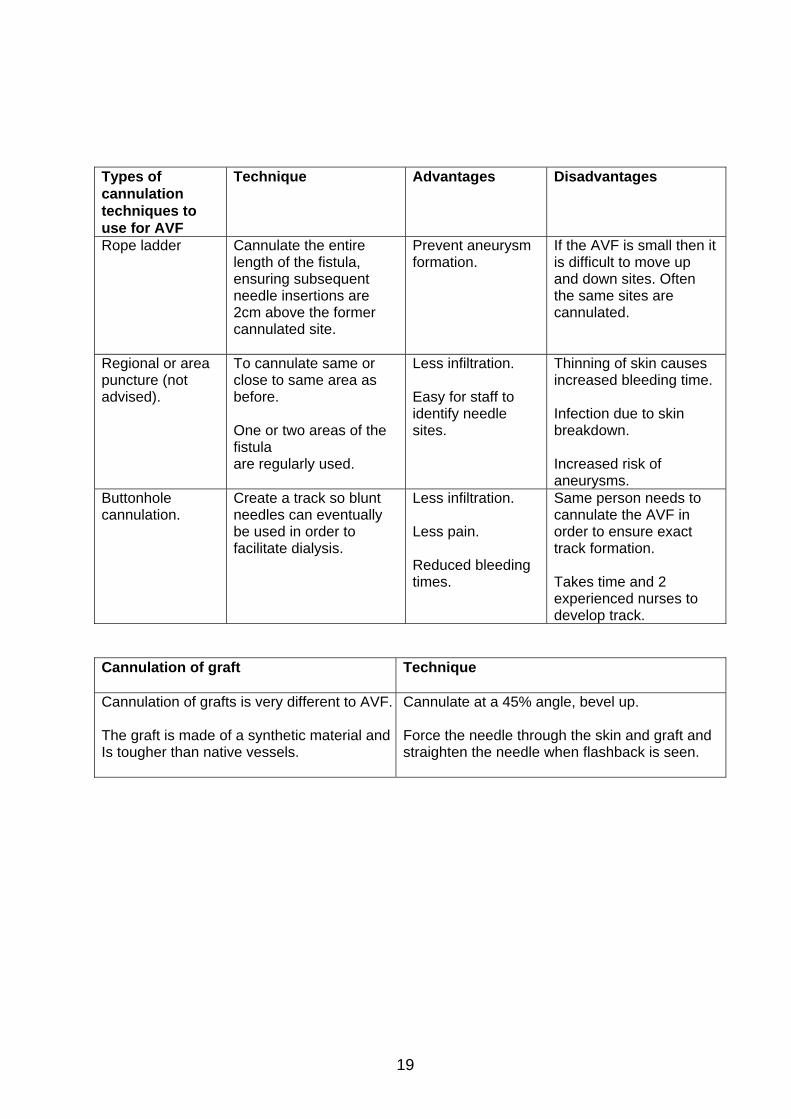
Types of cannulation techniques to use for AVF
Technique Advantages Disadvantages
Rope ladder Cannulate the entire length of the fistula, ensuring subsequent needle insertions are 2cm above the former cannulated site.
Prevent aneurysm formation.
If the AVF is small then it is difficult to move up and down sites. Often the same sites are cannulated.
Regional or area puncture (not advised).
To cannulate same or close to same area as before. One or two areas of the fistula are regularly used.
Less infiltration. Easy for staff to identify needle sites.
Thinning of skin causes increased bleeding time. Infection due to skin breakdown. Increased risk of aneurysms.
Buttonhole cannulation.
Create a track so blunt needles can eventually be used in order to facilitate dialysis.
Less infiltration. Less pain. Reduced bleeding times.
Same person needs to cannulate the AVF in order to ensure exact track formation. Takes time and 2 experienced nurses to develop track.
Cannulation of graft
Technique
Cannulation of grafts is very different to AVF. The graft is made of a synthetic material andIs tougher than native vessels.
Cannulate at a 45% angle, bevel up. Force the needle through the skin and graft and straighten the needle when flashback is seen.

20
Appendix 5 Blood flow rates (BFR) are recommendations and can be modified based on centre-specific guidelines. Only increase BFR if no evidence of infiltration or other problems noted. Report any cannulation or BFR problems to the charge nurse. Week two:
• if the first week is successful, cannulate with 16 gauge needles, rotating cannulation sites if not using buttonhole.
• blood flow rate recommended: 300 ml/min. Week three:
• either repeat procedure for week 2, or may attempt to progress to prescribed BFR and needle gauge. When increasing BFR, recommend matching needle gauge to BFR as shown in chart below,
• recommended needle placement: arterial retrograde (toward the arterial anastomosis), venous antegrade (toward the venous anastomosis). (this policy may vary based on policies and procedures of specific units)
Infiltration instructions
If the fistula infiltrates, let it “rest” for one week and then go back to smaller gauge needles. Notify charge nurse, vascular access nurse or nephrologist. If the fistula infiltrates a second time, wait another two weeks and then go back to smaller gauge needles. Notify charge nurse, vascular access nurse or nephrologist. If the fistula infiltrates a third time, notify surgeon and nephrologist.
RECOMMENDED: It is important to match needle gauge to blood flow rate. BLOOD RECOMMENDED FLOW RATE NEEDLE GAUGE
<300 ml/min
17-gauge
300 – 350 ml/min
16-gauge
>350-450 ml/min
15-gauge
> 450 ml/min
14-gauge
Note: These are minimum recommended gauges for the stated BFR settings. Larger needles, when feasible, will reduce (make less negative) pre-pump arterial pressure and increase delivered blood flow.

21
Appendix 6 Patient information - care of your fistula/graft Following Theatre: • for 24 hours following your anaesthetic it is important to adhere to the following
instructions: o do not drive o do not operate machinery, cookers or kettles o avoid alcohol and do not take sleeping tablets o do not make important decisions or sign legal documents
• if you feel any discomfort following surgery, painkillers may be taken as prescribed –
paracetamol/panadol
• you may be given some medication that helps to prevent your fistula/graft from clotting, it is very important that you take this medication as prescribed
• if any bleeding occurs, apply pressure with a clean cloth. If bleeding continues beyond 15 minutes, contact the Ward or attend your nearest A&E department
• your top theatre bandage can be removed 24-hours following surgery leaving a small white dressing over your wound
• keep this dressing clean and dry. If it gets wet or dirty please contact the pre-dialysis nurse.
• following surgery it is very important that you check your fistula/graft twice daily. This is done by placing your other hand gently on top of the dressing to feel a slight buzzing sensation. This means that your fistula/graft is working properly. If you do not feel this please contact the ward, pre-dialysis nurse or vascular access nurse for advice immediately.
• a district nurse will visit and assess your wound 3 days after surgery
• your stitches are self-dissolving, therefore do not need to be removed
• observe your wound regularly for any signs of redness, swelling or leakage
• ensure hands are washed prior to touching your fistula/graft wound
• once your dressing is removed you may bath/shower as normal, avoid using soap or talcum powder over the wound until the wound is completely healed
• you will be required to attend an outpatient clinic 2-4 weeks following surgery just to ensure there are no problems with your fistula/graft. You will receive an appointment through the post following discharge from the DSU.
• gentle hand exercises may be commenced once all dressings have been removed. These will help strengthen and build up the vein in your fistula/graft. Commence by squeezing your stress ball gently for several minutes 2-3 times/day. Increase the frequency of these exercises over the next few weeks.
22
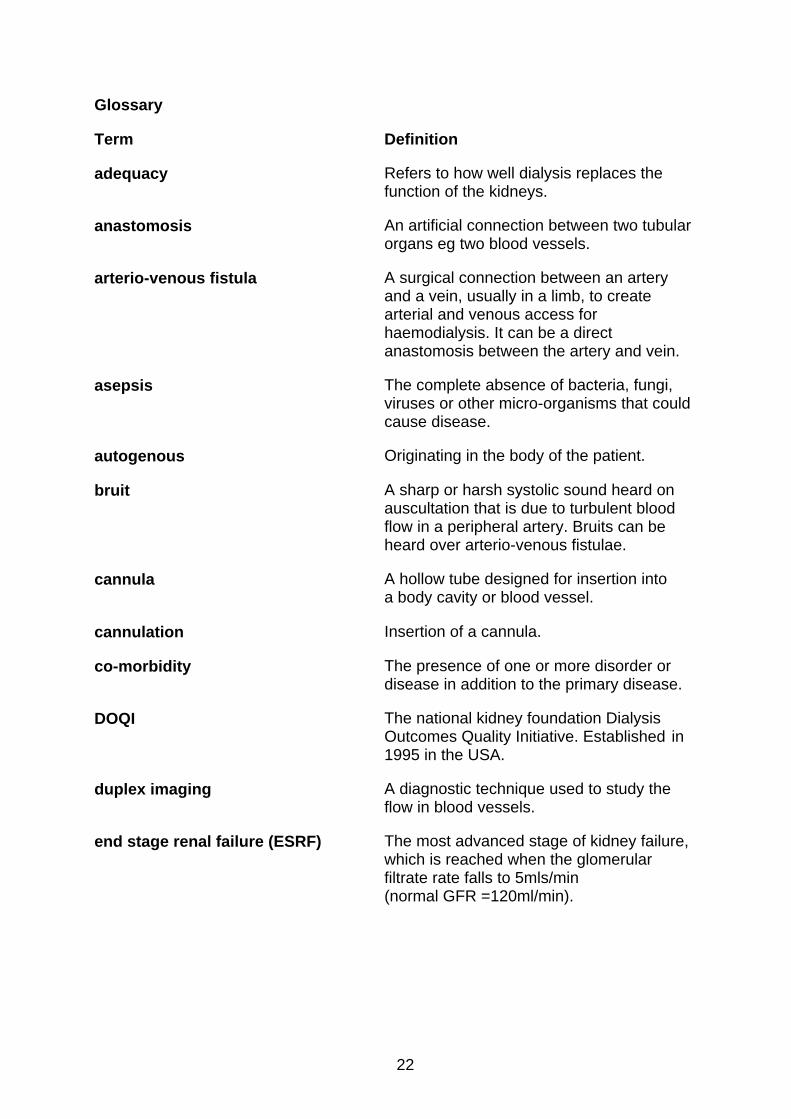
Glossary Term
Definition
adequacy Refers to how well dialysis replaces the function of the kidneys.
anastomosis
An artificial connection between two tubular organs eg two blood vessels.
arterio-venous fistula
A surgical connection between an artery and a vein, usually in a limb, to create arterial and venous access for haemodialysis. It can be a direct anastomosis between the artery and vein.
asepsis
The complete absence of bacteria, fungi, viruses or other micro-organisms that could cause disease.
autogenous
Originating in the body of the patient.
bruit
A sharp or harsh systolic sound heard on auscultation that is due to turbulent blood flow in a peripheral artery. Bruits can be heard over arterio-venous fistulae.
cannula
A hollow tube designed for insertion into a body cavity or blood vessel.
cannulation
Insertion of a cannula.
co-morbidity
The presence of one or more disorder or disease in addition to the primary disease.
DOQI The national kidney foundation Dialysis Outcomes Quality Initiative. Established in 1995 in the USA.
duplex imaging A diagnostic technique used to study the flow in blood vessels.
end stage renal failure (ESRF) The most advanced stage of kidney failure, which is reached when the glomerular filtrate rate falls to 5mls/min (normal GFR =120ml/min).
23
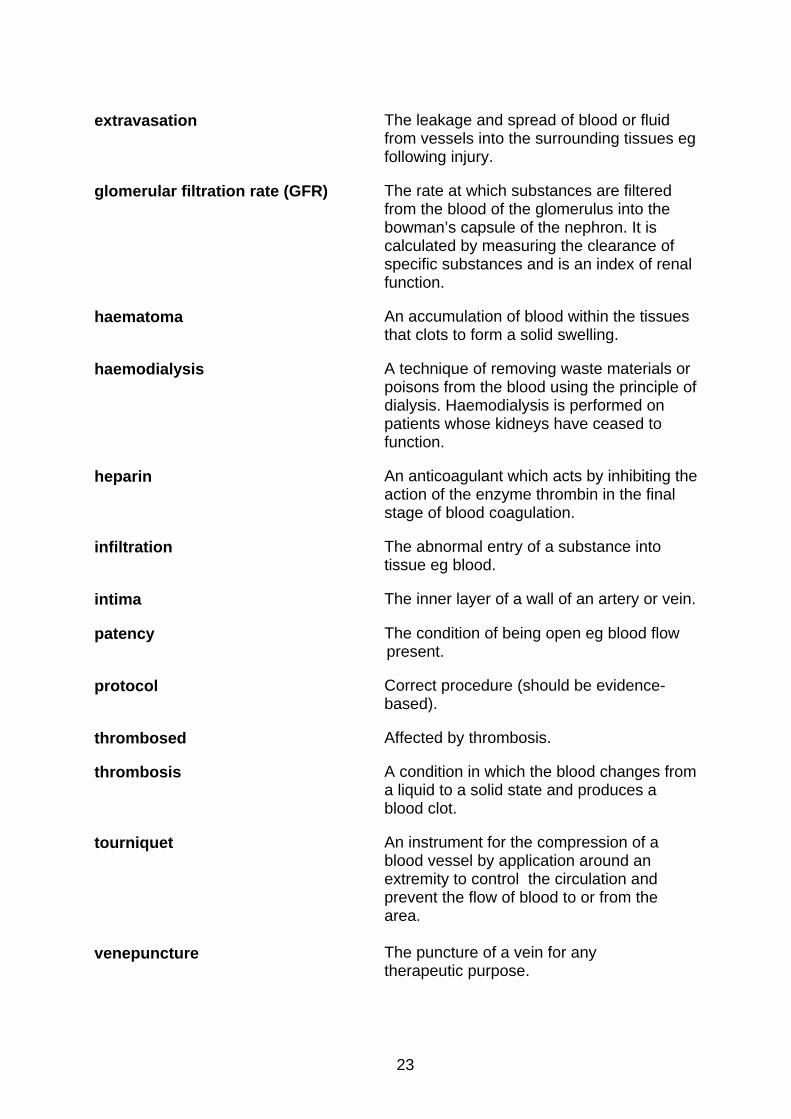
extravasation The leakage and spread of blood or fluid
from vessels into the surrounding tissues eg following injury.
glomerular filtration rate (GFR) The rate at which substances are filtered from the blood of the glomerulus into the bowman’s capsule of the nephron. It is calculated by measuring the clearance of specific substances and is an index of renal function.
haematoma An accumulation of blood within the tissues that clots to form a solid swelling.
haemodialysis A technique of removing waste materials or poisons from the blood using the principle of dialysis. Haemodialysis is performed on patients whose kidneys have ceased to function.
heparin An anticoagulant which acts by inhibiting the action of the enzyme thrombin in the final stage of blood coagulation.
infiltration The abnormal entry of a substance into tissue eg blood.
intima
The inner layer of a wall of an artery or vein.
patency The condition of being open eg blood flow present.
protocol Correct procedure (should be evidence-based).
thrombosed Affected by thrombosis.
thrombosis
A condition in which the blood changes from a liquid to a solid state and produces a blood clot.
tourniquet
An instrument for the compression of a blood vessel by application around an extremity to control the circulation and prevent the flow of blood to or from the area.
venepuncture
The puncture of a vein for any therapeutic purpose.
24
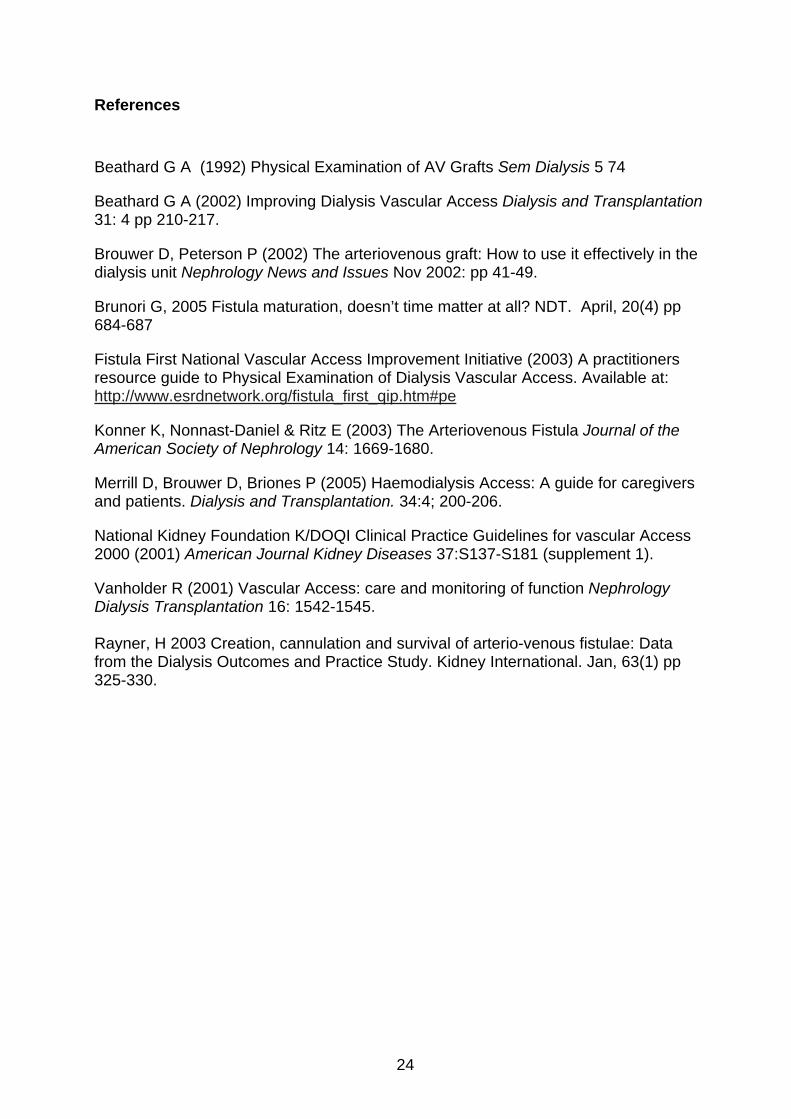
References
Beathard G A (1992) Physical Examination of AV Grafts Sem Dialysis 5 74
Beathard G A (2002) Improving Dialysis Vascular Access Dialysis and Transplantation 31: 4 pp 210-217.
Brouwer D, Peterson P (2002) The arteriovenous graft: How to use it effectively in the dialysis unit Nephrology News and Issues Nov 2002: pp 41-49.
Brunori G, 2005 Fistula maturation, doesn’t time matter at all? NDT. April, 20(4) pp 684-687
Fistula First National Vascular Access Improvement Initiative (2003) A practitioners resource guide to Physical Examination of Dialysis Vascular Access. Available at: http://www.esrdnetwork.org/fistula_first_qip.htm#pe
Konner K, Nonnast-Daniel & Ritz E (2003) The Arteriovenous Fistula Journal of the American Society of Nephrology 14: 1669-1680.
Merrill D, Brouwer D, Briones P (2005) Haemodialysis Access: A guide for caregivers and patients. Dialysis and Transplantation. 34:4; 200-206.
National Kidney Foundation K/DOQI Clinical Practice Guidelines for vascular Access 2000 (2001) American Journal Kidney Diseases 37:S137-S181 (supplement 1).
Vanholder R (2001) Vascular Access: care and monitoring of function Nephrology Dialysis Transplantation 16: 1542-1545. Rayner, H 2003 Creation, cannulation and survival of arterio-venous fistulae: Data from the Dialysis Outcomes and Practice Study. Kidney International. Jan, 63(1) pp 325-330.

25
Who was involved in developing the statement? Working group members Carol Latta Ward Manager, RDU Gartnavel General Hospital, NHS
Greater Glasgow
Caroline Arnott Ward Manager, Renal Unit, Queen Margaret Hospital, Dunfermline
Anne Allan Clinical Ward Manager, Renal Unit Raigmore Hospital, Inverness
Anne Petherick Education Co-ordinator, Renal Unit, Edinburgh Royal Infirmary
Barbara Killoran Lecturer, Adult Nursing, University of Paisley, Paisley
Geraldine Ovens Renal Education Facilitator, Renal Unit, NHS Ayrshire & Arran
Ippy Brown Clinical Nurse Manager, Renal Unit, NHS Greater Glasgow
Julie English Clinical Educator, Renal Unit, Raigmore Hospital, Inverness
Laurie Kirkland Pre-dialysis Nurse, NHS Ayrshire & Arran
Margaret Boyd Clinical Facilitator, Renal Unit, Monklands General Hospital
Morag McGhee Clinical Nurse Manager, Renal Unit, Monklands General Hospital
Noreen McMahon Ward Manager, Crosshouse Hospital, Kilmarnock
Rhona Lochiela Vascular Access Nurse, Edinburgh Royal Infirmary
Temby Chigaru Clinical Educator, Queen Margaret Hospital, Dunfermline
Sean McCartney Senior Charge Nurse, Renal Unit, Ninewells Hospital, Dundee
Jacqueline Ross Acting Ward Manager, Renal Unit, Aberdeen Royal Infirmary
Jacqueline Annand Senior Staff Nurse, Renal Unit, Aberdeen Royal Infirmary
Jane Rodriguez Ward Manager Renal Unit, Falkirk Royal Infirmary

26
Wider reference group Sister Aileen Heminglsey HD sister Monklands Hospital, Airdrie Dr W Smith Consultant Monklands Hospital, Airdrie Dr M Hand Consultant Monklands Hospital, Airdrie Dr I Shilliday Consultant Monklands Hospital, Airdrie Dr H Oun Associate Specialist Monklands Hospital, Airdrie Dr M McGregor Consultant Crosshouse Hospital Kilmarnock Dr K Simpson Consultant Glasgow Royal Infirmary Dr C Brunton Consultant Aberdeen Royal Infirmary,
Aberdeen Dr A Severn Consultant Ninewells Hospital Dundee Dr R Peel Consultant Raigmore Hospital, Inverness Dr S Lambie Consultant Raigmore Hospital, Inverness Dr M Wood Consultant Queen Margaret Hospital, Dunfermline Dr K McBride Consultant Queen Margaret Hospital, Dunfermline Dr S Rodger Consultant Western Infirmary, Glasgow Ms L Buist Consultant Western Infirmary, Glasgow Ms Alison Wilkinson Patient Representative Ninewells Hospital, Dundee