berger - drug development with cdx 2015 - final
TRANSCRIPT
________________________________________
Drug Development With Companion Diagnostics:
Regulatory and Reimbursement Aspects of New Business Models
Edward E. Berger, Ph.D.
Larchmont Strategic Advisors
Tufts CSDD Postgraduate Course Feb. 4, 2015
________________________________________
Definition
2
Companion diagnostic – A diagnostic test used to predict the likely clinical effectiveness and/or safety of a particular therapeutic intervention for a specific individual; the term is most often used to describe a molecular diagnostic test that stratifies a patient population with regard to the likelihood of response to, or the safety of, a pharmacologic therapy.
________________________________________
An Ongoing Medical Revolution
• “Personalized medicine” / “Precision Medicine”– The right treatment (Tx)– For the right patient– In the right amount– At the right time
• Diagnostic (Dx) is the key to Tx success
3
________________________________________
Limits of Traditional Medicine
• Tx success is frequently probabilistic– Protocols based on population-wide data– Non-response rates are high– Complication rates are high– Determinants of success are poorly known
• Informed guessing yields– Delays in identifying effective Tx– Exposure to unnecessary risks– Enormous financial, time and opportunity costs
4
________________________________________
Pharma Has a Parallel Problem
• Lengthy and expensive product development process– Size and duration of clinical trials is a major
factor• Painfully low yield rate on compounds
screened• High failure rate in clinical trials• Phase IV (and beyond) safety issues
5
________________________________________
Companion Diagnostics (CDx)
• Can yield substantial improvements in clinical care
• Promise major efficiencies and savings in drug development
• Contribute to more effective and efficient use of society’s investment in health care
6
________________________________________
In the Clinic …
• Stratify patient population on the basis of validated indicators of Tx effectiveness and/or safety– Increase response rates– Decrease complication rates
• Better and safer drugs (Rx) • Less time and money wasted
7

________________________________________
In Drug Development …
• Targeted screening of compounds allows better choices for clinical development
• Ability to recruit patients who are likely responders yields smaller clinical trials with higher probability of success
• Economics of process transformed (?)– Development time and cost reduced– Blockbuster model severely threatened
8
________________________________________
For Society …
• Targeted Tx selection means higher return on health care investment– Less ineffective or unnecessary care– Fewer complications and adverse events– Healthier population– Lower health insurance costs?– Control of health care share of GDP?
9
________________________________________
Success Ought to Follow
• All affected parties seem to benefit• Essential enabling technologies are
advancing– Pharmacogenomics and proteomics– Bioinformatics– Molecular pathology testing– Health information technology / electronic
health records
10
________________________________________
Many Positive Signs
• Drug and diagnostics companies are deeply engaged
• Venture capital is being invested – Diagnostics; Bioinformatics tools; HIT
• IPO window is open• Regulatory agency (FDA) is on board• A dominant business model has emerged
11
________________________________________
DHHS Is Supportive
• Secretary’s Advisory Committee on Genetics, Health and Society– http://www4.od.nih.gov/oba/SACGHS.HTM
• Dedicated website– http://www.hhs.gov/myhealthcare/
• “Personalized Health Care: Opportunities, Pathways, Resources”, Sept. 2007– http://www.hhs.gov/myhealthcare/news/
presonalized-healthcare-9-2007.html
12
________________________________________
FDA Resources for Industry
• Paving the Way for Personalized Medicine (Oct. 2013)– http://www.fda.gov/downloads/ScienceResearc
h/SpecialTopics/PersonalizedMedicine/UCM372421.pdf
– Contains extensive list of FDA Guidances pertaining to personalized medicine
• In Vitro Companion Diagnostic Devices Draft Guidance, July 14, 2011– http://www.fda.gov/MedicalDevices/DeviceRegu
lationandGuidance/GuidanceDocuments/ucm262292.htm
• “Table of Valid Genomic Biomarkers” http://www.fda.gov/drugs/scienceresearch/researchareas/pharmacogenetics/ucm083378.htm
13

________________________________________
Pharmacogenomic Markers in Drug Labeling
• Genomic biomarker information in labeling may describe …– Drug exposure and clinical response
variability– Drug interactions– Adverse event risk– Genotype-specific dosing– Mechanisms of action– Polymorphic drug target and disposition
genes 14
________________________________________
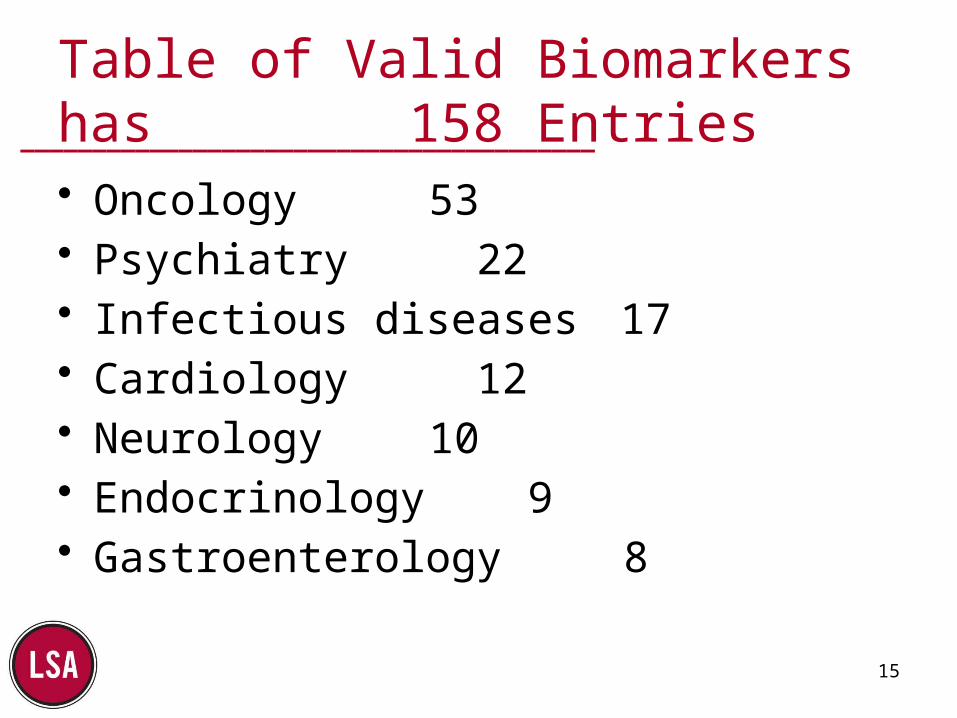
Table of Valid Biomarkers has 158 Entries• Oncology 53• Psychiatry 22• Infectious diseases 17• Cardiology 12• Neurology 10• Endocrinology 9• Gastroenterology 8
15
________________________________________
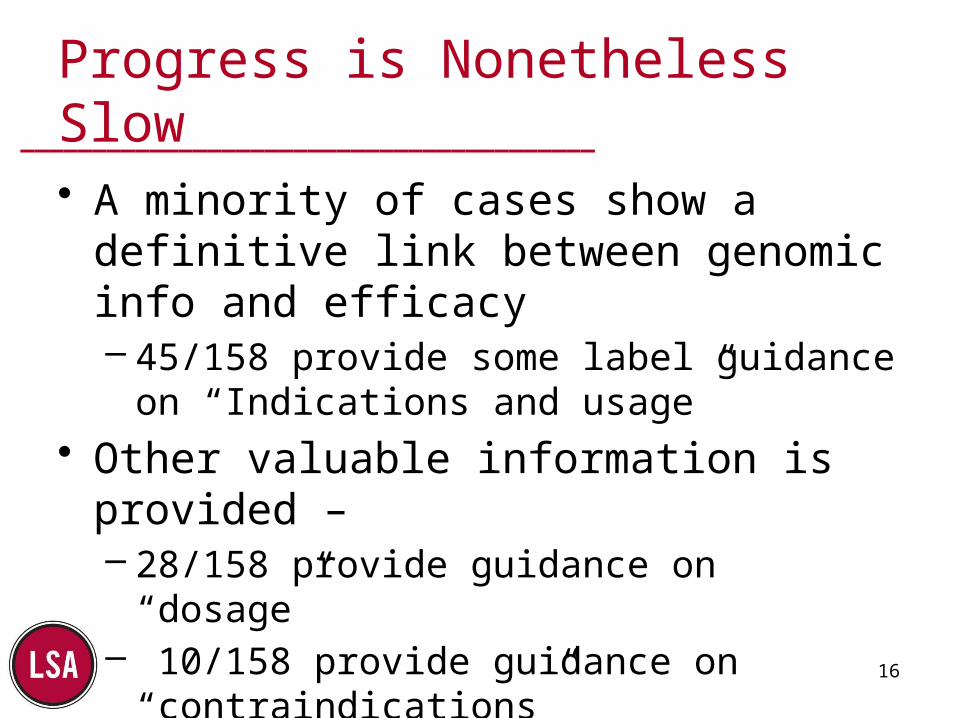
Progress is Nonetheless Slow
• A minority of cases show a definitive link between genomic info and efficacy– 45/158 provide some label guidance on
“Indications and usage”• Other valuable information is provided –
– 28/158 provide guidance on “dosage”– 10/158 provide guidance on
“contraindications”– 35/ 158 provide guidance on “drug
interactions” 16

________________________________________
Significant Rate-Limiting Factors
• Genomic and proteomic influence on Rx efficacy is more complex than at first envisioned– 1/1 cases of effectiveness are rare
• Complexity of the regulatory pathway remains an impediment– Despite FDA clarification of guidance
• Dominant business model may not be scientifically/clinically optimal
17
________________________________________
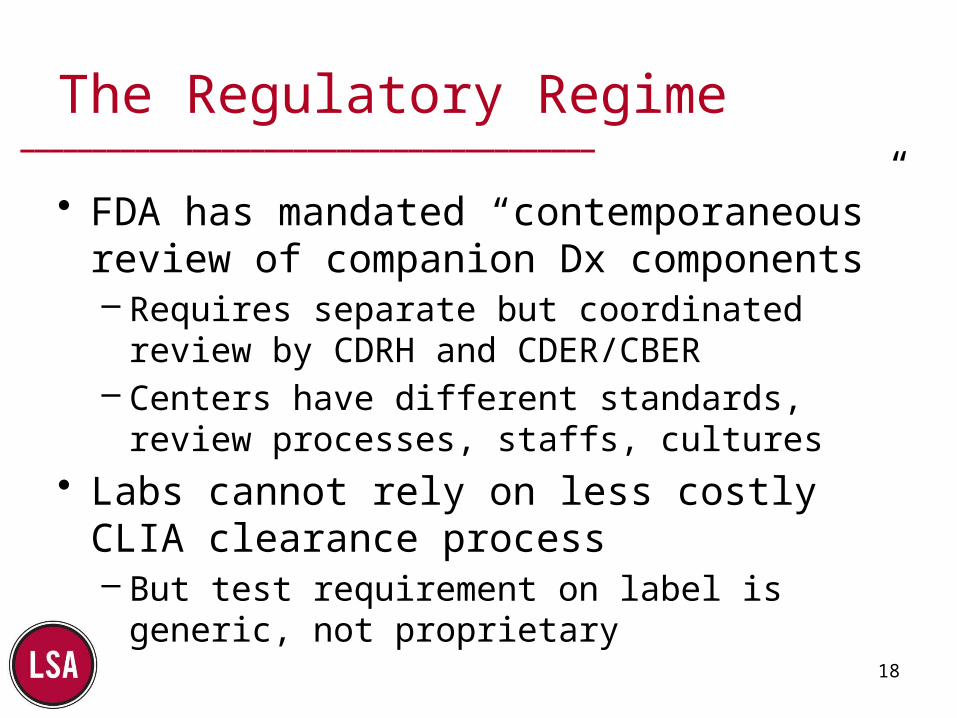
The Regulatory Regime
• FDA has mandated “contemporaneous” review of companion Dx components– Requires separate but coordinated review by
CDRH and CDER/CBER– Centers have different standards, review
processes, staffs, cultures• Labs cannot rely on less costly CLIA
clearance process– But test requirement on label is generic, not
proprietary 18
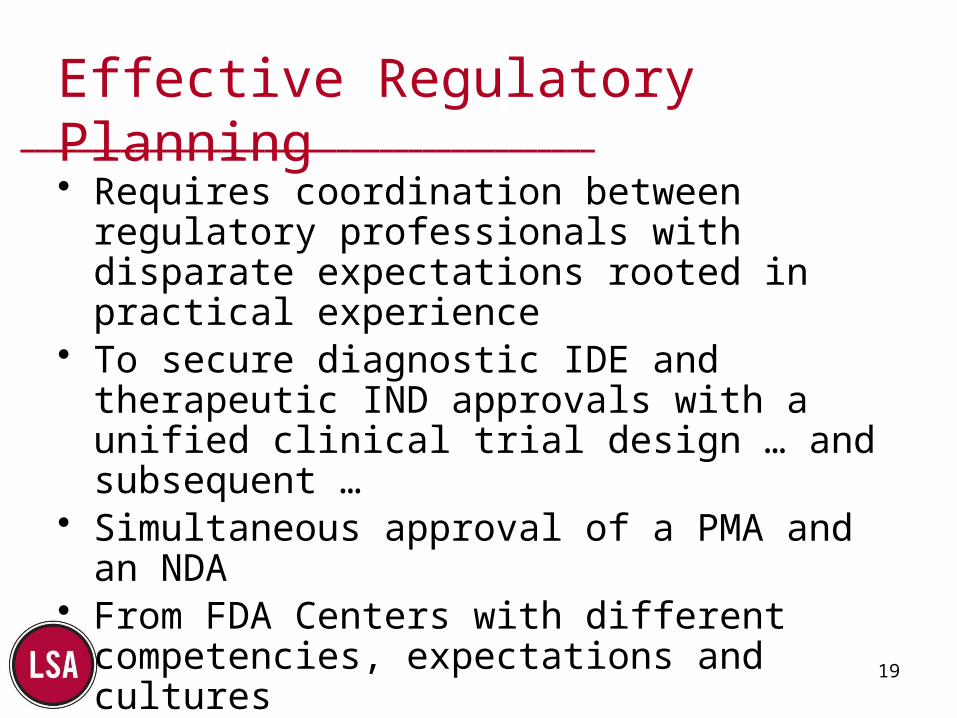
________________________________________Effective Regulatory Planning• Requires coordination between regulatory
professionals with disparate expectations rooted in practical experience
• To secure diagnostic IDE and therapeutic IND approvals with a unified clinical trial design … and subsequent …
• Simultaneous approval of a PMA and an NDA• From FDA Centers with different competencies,
expectations and cultures• With mutually agreed division of responsibility
and cost19
________________________________________
The Business Model Problem
• Regulatory framework and underlying business requirements mandate Dx / Rx co-development
• Pharma and diagnostics have diverse, possibly incompatible, business processes and cultures– Product development timeframes and costs– ROI expectations– Regulatory and reimbursement regimes– Workplace cultures
• Customer requirements are ill-defined and evolving
20
________________________________________
Structuring the CDx Effort
• Some Pharma tried to bring Dx development capability in-house through acquisition or internal startup– Choice between immediate culture clash and
long incubation period– Many internal operational / financial / political
issues• Partnership for co-development dominates
– More fruitful and less traumatic
21

________________________________________
CDx Partnering Deals
22
256 deals January 2007 – September 2013*
*Current Partnering. Companion Diagnostics Partnering Terms and AgreementsReport Code CP2106
________________________________________
Partnering Activity Remains High
• Dako, an Agilent Technologies company, announced today it has entered into a master framework agreement with Merck to develop companion diagnostic tests for oncology drugs currently in Merck’s development pipeline Jan. 9, 2014.
• Foundation Medicine and Clovis Oncology Expand Collaboration to Develop Novel Companion Diagnostic for Rucaparib in Ovarian Cancer April 3, 2014
• Thermo Fisher Scientific Announces Agreement with GlaxoSmithKline and Pfizer to Develop Oncology Companion Diagnostics Using Next-Generation Sequencing (NGS) September 25, 2014
• QIAGEN N.V. … has entered into a master collaboration agreement with … Novartis AG … development and commercialization of companion diagnostics to be paired with existing Novartis pharmaceutical products as well as compounds in its development pipeline. November 11, 2014
23
________________________________________
Dynamic Market Growth Projected*
• The global CDx market ($8.7 billion in 2014) will see CAGR of 22.9% over the next ten years;
• > 10 million tests/year by 2024.• Companion drugs generated estimated revenues of more
than $26 billion in 2013, with six drugs achieving blockbuster status.
• Rich CDx pipeline - more than 75 drugs being co-developed with predictive biomarkers.
• Partnership seems to be the most preferred model for development; since January 2011, there have been more than 90 collaborations between pharmaceutical and
diagnostic companies.*Companion Diagnostic Market 2014-2024.Roots Analysis Private Ltd.,June 2014
24
________________________________________
The Reimbursement Regime
• In traditional fee-for-service settings, Dx and Rx will be subject to separate coverage and payment determinations, often by different entities– Will insurer pay for Dx required by PBM to
secure payment for Rx?– Label requirement helps, but the payer
entities need to coordinate• Capitation changes this dynamic
25
________________________________________
Coding is Critical to Reimbursement
• Broken Molecular Pathology Coding System has been Fixed– Molecular diagnostic tests had been coded by
processes, not by analyte; a single test required “stacking” of multiple processes and repetitions
– Prevented electronic claim processing– Hard to identify test performed, analyze
utilization, etc.• New codes effective Jan. 1, 2013 address
the problem26
________________________________________
Progress on Coding Continues
•New MolPath codes facilitate electronic processing, utilization analysis, and test-specific fee setting for some tests
– Tier 1 - Unique identifiers for 99 high volume tests– Tier 2 – Nine resource intensity group codes– CPT 81479 for Unlisted molecular pathology procedure
• NGS codes effective January 1, 2015 address large scale multi-analyte sequencing procedures
• Payment uncertainty remains an impediment to use
27
________________________________________
Payer Coverage Status
• Generally aware of pharmacogenomic developments– Coverage for Dx/Rx pairs is case-by-case– Traditional decision criteria have worked so far– Limited experience no commitment to a model– Critical mass not yet reached
• Great majority of 158 entries in FDA table are advisory only
• Some PBMs understand the issues well– Uniquely positioned to evaluate and manage the
financial benefits of companions– Report more receptivity from self-insured employers
than from third party insurers28
________________________________________
Priorities for Gaining Coverage
• Understand the traditional coverage criteria– “Reasonable and necessary” standard
• Integrate reimbursement planning into clinical development plan– Leverage FDA process and outcome
• Recognize the primacy of the therapeutic goal– Focus on clinical utility of Dx
29
________________________________________
Leverage FDA Process For …
• Unequivocal confirmation of biomarker validity – both analytic and clinical
• Demonstration of objective basis for stratification of patient population
• Empirical evidence of clinical utility– link between Dx status and Tx success – Minimization of probabilistic element
• Dx/Rx tied by label indications
30
________________________________________
Conclusions (1)
• The CDx value proposition is clear and well understood– Clinical value – efficacy and safety– Cost-effectiveness
• Co-developed Dx/Rx pairings increase probability of success and reduce total costs– Other Dx development models are financially
and operationally problematic up until now …
31
________________________________________
Conclusions (2)
• Pharma and diagnostics developers need further experience working together– Close the expectations and culture gaps– Gain positive experiences to build on
• Regulators and payers are moving – if slowly – to adapt to and facilitate CDx development and utilization
• CDx presence in clinical practice will inexorably accelerate …
32
________________________________________
33
Edward E. Berger, Ph.D.PrincipalLarchmont Strategic Advisors2400 Beacon St. #203Chestnut Hill, MA 02467
Tel: (617)645-8452
Email: [email protected]