beneficial effect of salbutamol cardiac function in severe congestive...
TRANSCRIPT

Beneficial Effect of Salbutamol on Cardiac Functionin Severe Congestive Cardiomyopathy
Effect on Systolic and Diastolic Function of the Left Ventricle
BIM SHARMA, M.D., M.R.C.P., D.C.H. (Lond)
AND J. F. GOODWIN, M.D., F.R.C.P., F.A.C.C.
SUMMARY The effects of Salbutamol (a "selective" beta2 agonist) were studied in 12 patients with congestive car-
diomyopathy in a dose of 0.5 ,ug/min/kg. In Study A (n = 6), pressures and cardiac index (CI) were measured at rest andduring supine exercise. Study B (n = 6) was specifically designed to observe the effects of Salbutamol on the indices of leftventricular performance and diastolic pressure-volume relationships. The results of Study A revealed Salbutamol infusionsignificantly (P < 0.001) increases CI from 1.8-3.9 I/min/M2 in the resting state; the exercise CI improved from 3 to 4.5I/min/m' (P < 0.005); there was a marked decrease in left ventricular end-diastolic pressure at rest from 27-13 mm Hg(P < 0.001) and during exercise from 39-20 mm Hg (P < 0.001). There was no significant change in heart rate and bloodpressure. In Study B, there was a significant reduction in left ventricular end-diastolic volume index from 210-183 mi/M2
(P < 0.05) and left ventricular end-systolic volume index from 159-102 ml/m' (P < 0.001) with a significant increase inejection fraction from 28% to 46% (P < 0.01). Indices of myocardial performance showed significant improvement inLVdp/dt max (P < 0.02), Vpm (P < 0.001), Vmax (P < 0.01), Vce (P < 0.001), V, (P < 0.02), and V40 (P < 0.05).Salbutamol infusion significantly decreased end-diastolic circumferential wall stress (P < 0.001), total passive diastolicstiffness (P < 0.02), elastic stiffness (P < 0.001), and increased total left ventricular diastolic compliance (P < 0.01). Thisstudy indicates that Salbutamol produces significant improvement in overall cardiac function and in both systolic anddiastolic function of the left ventricle.
SYMPTOMATIC AND HEMODYNAMIC im-provement with rapidly acting parenteral vasodila-tors and inotropic agents in congestive heart failureand low cardiac output states has been well-estab-lished. -5 No single available oral agent has proven tobe consistently effective for the long-term manage-ment of these patients. Among the currently useddrugs for the management of congestive heart failureare vasodilators in sublingual, chewable, oral andtopical forms. The chief drawbacks of their use in-clude unpredictable hypotension, flushing, and head-ache, methemoglobinemia, occasionally tachyphy-laxis, and potential increase in myocardial ischemiacreated by a coronary steal effect.6 Other nonparen-teral agents that have been studied on a limited basisinclude the alpha-adrenergic blocking agents phenoxy-benzamine, the direct arteriolar dilating agentshydralazine7 and prazosin.8 However, the search forsafe, effective and long-acting nonparenteral agents^iscontinuing in order to make long-term therapy prac-tical. Salbutamol, allegedly a selective beta2 agonistdeveloped for obstructive bronchial disease, belongs tothe isoproterenol family of drugs and has beenreported to improve cardiac function in nonfailinghearts.9 This study was designed to investigate the car-diovascular effects of Salbutamol in patients withsevere heart muscle disease (congestive cardiomyop-
From the Department of Clinical Cardiology, Royal Post-Graduate Medical School, Hammersmith Hospital, London,England.
Presented in part at the 49th Scientific Sessions, American HeartAssociation, November 15-18, 1976, Miami Beach, Florida.
Address for reprints: Dr. Bim Sharma, University of Minnesota,Director, Heart Cath Laboratory, Hennepin County MedicalCenter, 701 Park Avenue, Minneapolis, Minnesota 55415.
Received January 3, 1978; revision accepted May 19, 1978.
athy) whose clinical condition warranted furthertherapeutic support despite adequate digitalis anddiuretic therapy.
Patients and Methods
Twelve patients, clinically suspected and later con-firmed by cardiac catheterization to be suffering fromsevere heart muscle disease (congestive cardio-myopathy), were studied. The average age of thegroup was 45 years (range 32-65). At the time of thestudy, despite intensive conventional anti-heart failuretreatment, all patients were in residual refractoryheart failure, and all had dyspnea. Paroxysmal noctur-nal dyspnea and ankle edema were present in fourpatients: the jugular venous pressure was raised atleast 4-5 cm above the sternal angle in the 450 supineposition in all. The liver was enlarged 3-5 cm belowthe costal margin in the mid-clavicular line in eightpatients. On auscultation, a third heart sound wasaudible in six, and a fourth heart sound in 11 patients.None had evidence of ischemia, valvular heart disease,hypertension or diabetes mellitus. All the patients hadbeen adequately treated with digoxin and diuretictherapy before the study.
Atrial fibrillation was present in one patient, and Twave inversion with or without ST depression in-dicative of some digitalis effect was present in allpatients. The chest radiographs revealed car-diomegaly; the average cardiothoracic ratio of thegroup was 64% (range 62-70%). Selective angiographyrevealed a large dilated left ventricle with generalizedhypokinesis and normal coronary arteries in eachcase, confirming the diagnosis of congestive car-diomyopathy in all. The nature and purpose of thetreatment and associated study was explained to each
449
by guest on July 10, 2018http://circ.ahajournals.org/
Dow
nloaded from

450 CIRCULATION VOL 58, No 3, SEPTEMBER 1978
TABLE 1. Indices of M11yocardial Performance at Rest in Patients with Congestive Cardiomyopathy and Effect of Salbutamol Infusion(Study B)
Congestive cardiomyopathyNormal valuest Control Subaltamol infusion
Variable (n = 6) (n - 6) (n 6)
EF 66 3 P <0.001 28 5 P <0.001 47 4
dp/dt max. 1200 + 140 P <0.02 850 130 P <0.02 1100 150mm Hg/sec
Vpm = peak (dp/dt)/psec'- 55 6 P <0.001 17 2 P <0.001 31 3(where P = total LV pressure)Peak (dp/dt)/PdSec-1 102 8 P <0.02 75 + 17 NS 88 - 13(Pd = developed pressure)VCe - peak (dp/dt)/KP--C-1 1.9 0.2 P <0.001 0.6 0.67 P <0.001 1.1 0.12
(K = 28)VCe at developed pressure 3.8 0.2 P <0.05 2.7 0.6 NS 3.1 0.5= peak (dp/dt)/KPdsec-1VmaXSec-l 108 5 P <0.001 39 3 P <0.01 53 = 4
(dp/dt)/P at zero pressureV6eec-1 90 =7 P <0.02 63 12 P <0.02 81 13= (dp/dt)/P5V40seC-1 58d3 P <0.001 18 3 P <0.05 27 4
(dp/dt)/P40Data collected for comparison from normal controls.Data expressed as mean 4 sEm.Abbreviations: P5 and P40 = developed pressure of 5 and 40 mm Hg, respectively; EF = ejection fraction; LV = left ventricular.
patient and their relatives. In all instances written con- and during mild supine exercise were studied in thesent was obtained. first six patients (Study A). In the next six patients
(Study B), the effects of Salbutamol infusion on the in-Design of Investigation dices of left ventricular (LV) systolic performance and
diastolic pressure-volume relationships (DPVR) wereThe study was designed in two parts. The investigated. Digitalis and diuretics were continued
hemodynamic effects of Salbutamol infusion at rest throughout both studies.
TABLE 2. Pressure-Volume Data; Indices of Left Ventricular Diastolic Compliance Before and After Salbutamol Infusion in Con-gestive Cardiomyopathy (Study B)
Normal values Congestive cardiomyopathyRest Control Salbutamol
Variable (n = 6) (n = 6) (n = 6)
LVEDP(mmHg) 9 1 P <0.001 28 3 P <0.01 13 2LV end-diastolic volume (LVEDV) ml/M2 84 5 P <0.001 210 10 P <0.05 183 9LV end-systolic volume (LVESV) ml/m2 30 2 P <0.001 159 6 P <0.001 102 8Total LV diastolic compliance 0.196 0.01 P <0.02 0.022 0.05 P <0.01 0.109 0.04Index-(Av/Ap)/LVESV
LVEDP/LVEDV ratio 0.062 0.009 P <0.01 0.097 = 0.008 P <0.02 0.075 0.007mm Hg/ml/m2
Total passive diastolic stiffness 0.014 = 0.004 P <0.01 0.035 - 0.009 P <0.02 0.017 0.009Index-(Ap/Av)/p
LV volume mass ratio 0.94 0.04 P <0.01 1.46 - 0.10 NS 1.36 0.05VED/VW ratio
Mid circumferential end-diastolic wall 12.2 1.2 P 0. <001 86 5 P <0.001 46 5.2stress (am)dyne/cm2 X 103
Peak systolic stress 350 20 NS 370 - 30 NS 360 25dyne/cm2 X 103
Stiffness constant K 14.3 3 NS 19.9 = 4 NS 19.3 * 3(K = 3 + 3 loge 2.33 (LVEDP))
Elastic stiffness (Em) 205 22 P <0.001 1710 = 392 P <0.001 890 = 275X 103 dyne/cm2
(Em = K.am)Data expressed as mean iSEM.Abbreviations: LVEDP = left ventricular end-diastolic pressure; LV = left ventricular; LVEDV - left ventricular end-diastolic volume; LVESV =
left ventricular end-systolic volume.
by guest on July 10, 2018http://circ.ahajournals.org/
Dow
nloaded from
SALBUTAMOL IN CONGESTIVE CARDIOMYOPATHY/Sharma and Goodwin
Protocol for the Patients (n = 6) in Study A
During the control period patients were studied atrest and during supine pedaling exercise. The cardiacoutput (CO) and intracardiac pressures weremeasured simultaneously at rest as well as during thefinal 2 minutes of exercise. After 20 minutes of restfollowing exercise, control resting measurements ofCO and pressures were made at 5 and 10 minutesbefore the infusion of Salbutamol. Then a continuousintravenous infusion of Salbutamol was given to eachpatient using an electromechanical pump (Harvard) ina dose of 0.5 ,ug/min/kg body weight. Resting cardiacoutputs and simultaneous pressures were measured at5, 10, 20, 30 and 40-minute intervals during infusion ofSalbutamol. Supine bicycle exercise was then repeated40 minutes after the resting data had been collectedwhile patients were still on continuous Salbutamol in-fusion.
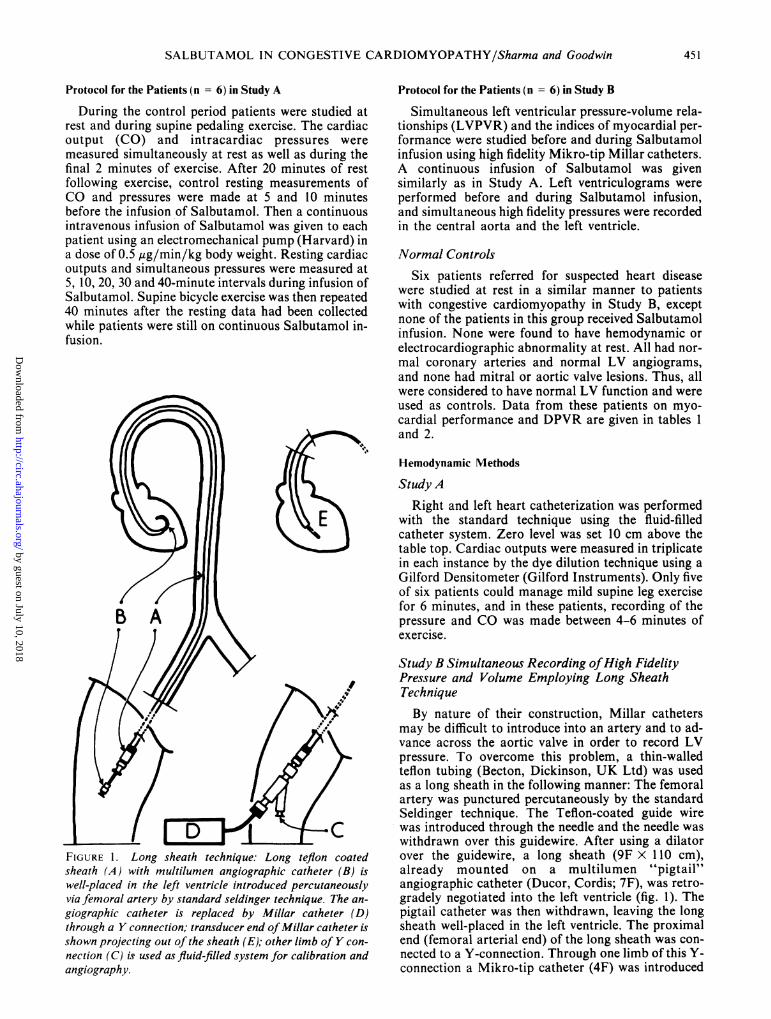
FIGURE 1. Long sheath technique: Long teflon coatedsheath (A) with multilumen angiographic catheter (B) iswell-placed in the left ventricle introduced percutaneouslyvia femoral artery by standard seldinger technique. The an-
giographic catheter is replaced by Millar catheter (D)through a Y connection; transducer end ofMillar catheter isshown projecting out of the sheath (E); other limb of Y con-
nection (C) is used as fluid-filled system for calibration andangiography.
Protocol for the Patients (n = 6) in Study B
Simultaneous left ventricular pressure-volume rela-tionships (LVPVR) and the indices of myocardial per-formance were studied before and during Salbutamolinfusion using high fidelity Mikro-tip Millar catheters.A continuous infusion of Salbutamol was givensimilarly as in Study A. Left ventriculograms wereperformed before and during Salbutamol infusion,and simultaneous high fidelity pressures were recordedin the central aorta and the left ventricle.
Normal Controls
Six patients referred for suspected heart diseasewere studied at rest in a similar manner to patientswith congestive cardiomyopathy in Study B, exceptnone of the patients in this group received Salbutamolinfusion. None were found to have hemodynamic orelectrocardiographic abnormality at rest. All had nor-mal coronary arteries and normal LV angiograms,and none had mitral or aortic valve lesions. Thus, allwere considered to have normal LV function and wereused as controls. Data from these patients on myo-cardial performance and DPVR are given in tables 1and 2.
Hemodynamic Methods
Study ARight and left heart catheterization was performed
with the standard technique using the fluid-filledcatheter system. Zero level was set 10 cm above thetable top. Cardiac outputs were measured in triplicatein each instance by the dye dilution technique using aGilford Densitometer (Gilford Instruments). Only fiveof six patients could manage mild supine leg exercisefor 6 minutes, and in these patients, recording of thepressure and CO was made between 4-6 minutes ofexercise.
Study B Simultaneous Recording ofHigh FidelityPressure and Volume Employing Long SheathTechniqueBy nature of their construction, Millar catheters
may be difficult to introduce into an artery and to ad-vance across the aortic valve in order to record LVpressure. To overcome this problem, a thin-walledteflon tubing (Becton, Dickinson, UK Ltd) was usedas a long sheath in the following manner: The femoralartery was punctured percutaneously by the standardSeldinger technique. The Teflon-coated guide wirewas introduced t-hrough the needle and the needle waswithdrawn over this guidewire. After using a dilatorover the guidewire, a long sheath (9F x 110 cm),already mounted on a multilumen "pigtail"angiographic catheter (Ducor, Cordis; 7F), was retro-gradely negotiated into the left ventricle (fig. 1). Thepigtail catheter was then withdrawn, leaving the longsheath well-placed in the left ventricle. The proximalend (femoral arterial end) of the long sheath was con-nected to a Y-connection. Through one limb of this Y-connection a Mikro-tip catheter (4F) was introduced
451
by guest on July 10, 2018http://circ.ahajournals.org/
Dow
nloaded from

VOL 58, No 3, SEPTEMBER 1978
into the ventricle, leaving its tip outside the longsheath. The other limb of the Y-connection was usedfor the calibration of Millar catheter with fluid-filledsystem and also for the calibration of the contrastmaterial for left ventriculography. This technique hasbeen found to be safe, easy and reliable. There hasbeen no incidence of local thrombosis or excessivehemorrhage in any patient studied. By this long sheathtechnique, LV pressure and volume were recordedsimultaneously using only one percutaneous arterialpuncture. Another Mikro-tip catheter (4F) was alsoplaced through a long sheath (6F X 100 cm) intoascending aorta via percutaneous brachial arterypuncture for the simultaneous recording of aorticpressure.The timing of each cine film exposure during ven-
triculography was electronically integrated withpressure by means of a battery operated photo celldevice, so that a calculated volume could be related toa time of the cardiac cycle and instantaneous pressure(fig. 2). Left ventriculograms were performed in 450right arterior oblique plane during inspiration at acamera speed of 48 frames/sec.
Measurements, Calculations and Statistical Analyses
Mean systolic pressure was estimated byplanimetric integration of the pressure and aorticpressure pulse component over five cardiac cycles. LVstroke work was calculated as the product of strokevolume and mean systolic pressure.'0 Oxygen uptakewas derived as the product of atrioventricular (AV)difference of oxygen content and CO. Systemic andpulmonary vascular resistances were calculated withresponse to surface area."The LV volumes were calculated from the first three
beats during angiography by the area lengthmethod.'2' '3 In addition to frame-by-frame analysis ofvolume, measurements were made of the long axis,and midwall internal radius and midwall externalradius. Ejection fraction (%) was calculated as
LVEDV-LVESV X 100LVEDV
where LVEDV and LVESV are left ventricular end-diastolic and left ventricular end-systolic volumes,respectively.The measurements and calculations of the pressure-
related indices of myocardial performance -
LV dp/dt Max, Vpm, Vce, Vmax, Peak (dp/dt)Pd KPd
Peak dp/dt, V, and V40 were made as shown in ap-pendix A,-A6. The total diastolic compliance index(,AV/AP/LVESV) where AV equals diastolic volumechanges measured as stroke index and AP equalschanges in the LV diastolic pressure measured fromthe lowest early diastolic pressure to left ventricularend-diastolic pressure (LVEDP). The first three beatswere analyzed for AV/AP for each patient before andduring Salbutamol. Since initial volume affects thefunctional passive volume curve, the value forobserved compliance was normalized by dividing byLVESV.'4 15 Total passive diastolic stiffness index(LAP/AV)/P is the reciprocal of ventricular com-pliance. Previous studies in canine heart have shownthat instantaneous first derivative (dp/dv) related tothe simultaneous LV pressure (p) is a linear function,the slope of which provides a quantitative index of LVstiffness, independent of volume and largely dependentof ventricular geometry.'6 The approach has been ex-
. . tSSii| NI*ZABhIiU1**h&AA*AAA 1 tAB11 11 )1 t' .1 I LLI.L' .L
FIGURE 2. A record ofhigh fidelity left ventricular (L V) pressure (high gain and low gain), aortic pressure,cineangiographic frame maker, electrocardiogram at a paper speed of 125 mm/sec. Cineframe maker hasbeen shown to drop down ImV, which indicates the time of the contrast injection. Pressure 0-25 for highgain L Vpressure and 0-150 for low gain L Vand aortic pressures. A = atrial wave; b = post A wave (whereL V end-diastolic pressure has been measured; b to c = isovolumic contraction phase; c to d = ejectionphase; e-early diastolic pressure of the left ventricle.
Iwo 0
..dmmmmmmw0
452 CIRCULATION
it
1040 . ..
by guest on July 10, 2018http://circ.ahajournals.org/
Dow
nloaded from

SALBUTAMOL IN CONGESTIVE CARDIOMYOPATHY/Sharma and Goodwin
TABLE 3. Circulatory Studies in Patients with Severe Heart Muscle Disease (Congestive Cardiomyopathy) Before and During Intra-venous Infusion of Salbutamol (Study A)
Control (n = 6) Salbutamol Infusion (0.5 ug/min/kg body wt) (n = 6)Variable - 10 min -5min 5 min 10 min 20 min 30 min 40 min
Oxygen uptake(ml/min/m2) 146 10 140 9 158=12 160 12 160 13 158 8 158 11
AV difference(vol %) 8.1 0.9 7.8 0.8 4.2 - 0.6t 4.2 0.6t 4.2 0.3t 4.1 0.2§ 4.1 0.3§
Cardiac output(1/min/m2) 1.8 0.2 1.8 0.2 3.8 0.21 3.8 0.21 3.8 0.31 3.9 0.3¶ 3.9 0.2¶
Heart rate(beats/min) 91 2 92 6 100 6 97 7 98 6 99 6 99 6
Stroke volume(ml/min/m2) 21 4 20 4 38 3§ 40 3§ 39 4§ 40 3§ 40 3§
Systemic arterialpressure (mm Hg)
Systolic 128 6 127 6 120= 5 119 - 5 120 6 120 5 120 =5Diastolic 81 3 80 3 78 3 75=3 75 2 75 3 75 3Mean 101 6 98 6 98 5 98 6 98 6 99 5 98 6
Pulmonary arterymean pressure(mm Hg) 35 6 34 6 25 5* 24 4t 25 4* 25 5* 25 5*
Vascular resistance(dyne-sec-cm-5/m2)
Systemic 4530 340 4530 330 2060 210¶ 2050 210¶ 2060 200§ 2040 210§ 2050 22§Pulmonary 470 110 470 100 160 20t 165 i 20t 160 30t 158 30t 158 20t
LV end-diastolicpressure(mm Hg) 27 2 27 2 12 31 13 31 12*21 13 31 13 31
LV stroke work(g-M/m2) 26 6 26 i5 50 * 51 52 - 5¶ 54i 6 52i51 52 61Data expressed as mean 4 SEM.Probability relate to comparison of group mean.*P <0.05.tP <0.02.P <0.01.IP <0.005.¶P <0.001.Abbreviations: AV = systemic-pulmonary arterial blood oxygen content difference; LV = left ventricular.
tended to the relation of AP/AV to mean LV pressure(p).17 The LV volume mass ratio (Ved/Vw), mid-circumferential wall stress (arn) and elastic stiffnesswere calculated as shown in appendix A7-A,0. Volumemass ratio was calculated because elastic stiffness(Em) has been shown to be dependent on it."8 The Emconstant K, calculated as shown in the appendix, is asimplified expression for constant K in the clinicalsituation.'9
Probability of statistical significance within thegroup was calculated by the Student t test for paireddata, and statistical significance in between the groupwas calculated by the umpaired t test.
Results
Each patient's electrocardiogram was continuouslymonitored throughout the study and did not revealany arrhythmias or any other change during or afterSalbutamol infusion. No side effects of the drug wereobserved in any of the patients studied.
Hemodynamic Changes in Study A (table 3 and 4)
At Rest (fig. 3)Individual hemodynamic characteristics in this
group of patients were similar. Before Salbutamol in-
fusion, patients with cardiomyopathy had a lowresting cardiac index (1.8 ± 0.2 1/min/M2) and highheart rate (91 ± 2/min), LVEDP (27 ± 2 mm Hg),and pulmonary artery mean pressure (35 ± 6 mmHg), indicating severe heart failure. Responses to in-travenous Salbutamol were similar in all patients.There was a significant increase in stroke volume(P < 0.005) and CO (P < 0.001), a consistent fall inLVEDP (P < 0.001), with a concomitant reduction inthe pulmonary artery mean pressure (P < 0.05).Although there were individual variations in the heartrate and systemic arterial pressure, there was nosignificant change in these two factors as a group dur-ing Salbutamol infusion. Since there was no change inthe aortic dynamic and mean pressure, the significantfall in the calculated systemic (P < 0.001) andpulmonary vascular resistance (P < 0.02) primarilyreflected changes in the CO. These changes weremaintained throughout the 40-minute period ofSalbutamol infusion.
During Exercise (fig. 4)Only five of six patients were able to perform light
supine leg exercise. The hemodynamic findings inthese patients and their response to exercise, beforeand during Salbutamol infusion, were again
453
by guest on July 10, 2018http://circ.ahajournals.org/
Dow
nloaded from

VOL 58, No 3, SEPTEMBER 1978
TABLE 4. Circulatory Response to Mild Supine Exercise in Patients with Severe Heart Muscle Disease (Con-gestive Cardiomyopathy) Before and During Intravenous Infusion of Salbutamol (Study A)
Supine leg exercise(n =5
During salbutamolVariable Control infusion
Oxygen uptake ml/min/M2 292 20 NS 305 22
AV difference (vol %7) 9.7 0.8 P <0.01 6.8 - 0.7
Cardiac output (I/min/M2) 3.0 0.4 P <0.001 4.5 - 0.2
Heart rate (beats/min) 123 6 NS 129 - 3
Stroke volume (ml/min/m2) 25 4 P <0.01 36 - 3
Systemic arterial pressure (mm Hg)Systolic 188 12 NS 169 5Diastolic 102 10 NS 91= 6Mean 138 6 NS 123 8
Pulmonary artery pressure - mean (mm Hg) 48 6 P <0.01 35 7
LV end-diastolic pressure (mm Hg) 39 4 P <0.001 20 2
Vascular resistance (dyne-sec-cm-5/m2)Systemic 4030 640 P <0.01 2210 130Pulmonary 330 80 P <0.02 160 20
LV stroke work (g-m/m2) 42 + 6 P <0.01 64 4
Data expressed as mean rt sEm.Abbreviation: LV = left ventricular.
remarkably consistent. In the control study the exer-cise cardiac index (3 ± 4 1/min/M2) and stroke index(25 ± 4 ml/beat/M2) were severely impaired. TheLVEDP (39 ± 4 mm Hg) and pulmonary artery meanpressure (48 ± 6 mm Hg) were raised significantly.Salbutamol infusion during exercise resulted in nosignificant change in the heart rate and systemicarterial pressure compared with the control exercisedata. The rise in the LVEDP in response to exerciseduring Salbutamol infusion was significantly lessmarked (P < 0.001) than the values obtained duringthe control exercise study. There was also significantincrease in cardiac index (P < 0.001) and stroke index(P < 0.01) and a significant fall in pulmonary arterymean pressure (P < 0.01) and pulmonary resistance(P < 0.02) during Salbutamol infusion in thesepatients.
Effect on Modified Frank-Starling Left VentricularFunction Curve
The relationship between LV stroke work andLVEDP before and during Salbutamol infusion is il-lustrated in figure 5. Infusion of Salbutamol wasfollowed by a large reduction in end-diastolic pressure(both at rest and during exercise P < 0.001) and asignificant increase in stroke work output (rest P <0.001; exercise P < 0.01) without significant change inthe heart rate and systemic arterial pressure, in-dicating significant improvement in the LV function.
105_
E 95
A95 _
15113 r
5 4.U
S Ei0
c3.
2.0
30
20FIGURE 3. All patients had low cardiac output andsignificantly raised left ventricular end-diastolic pressure(LVEDP) during control period. During 40 minutes ofSalbutamol infusion there was sustained improvement incardiac output and L VEDP without significant change in theheart rate and systemic arterial pressure.
p * NS
E 1, 1 p NS
, I.
PC 0.001
p< 0.001
10
-10 -5 5 10 20TIHE (min)
HAEMODYNAMIC EFFECTS OF SALBUFAMOL INFUSION AT RESTIN PATIENTS WITH HEART MUSCLE DISEASE in *6)
Salbuafmol 10. 5pgWglmin)
30 40
454 CIRCULATION
9(A4A
w
-Ccc
9c4i
3Ev
A nk
igm4.11V)
2.-ja :Jr(A e< eCl
cni
I.,
IL
i 100II 11I.
ip I Iyol70 w L. y
by guest on July 10, 2018http://circ.ahajournals.org/
Dow
nloaded from

SALBUTAMOL IN CONGESTIVE CARDIOMYOPATHY/Sharma and Goodwin
LEFT VENTRICULAR FUNCTION
70Contmo Salbutamol (infusion)
130
p- NSI-
E
E
V.'3.
5C-Z
50
40
30
'II
p * NS
p<(0.05
FIGURE 4. Patients with congestive cardiomyopathy inStudy A showed a significant increase in cardiac output
(CO) and a decrease in left ventricular end-diastolic pressure(L VEDP) with no significant change in the heart rate (HR)and mean aortic pressure (MAP) during Salbutamol infu-sion.
Effect ofSalbutamol on the Pressure-RelatedParameters of Myocardial Performance(table 1, fig. 6)
In Study B, ejection fraction and LV dp/dt maxwere severely depressed, indicating myocardial dis-ease. During Salbutamol infusion these values rose
significantly (P < 0.001 and P < 0.02, respectively).The total LV pressure-related parameters of contrac-tility (Vpm, Vce and Vmax) were severely depressedduring the control rest period and rose significantlyduring the Salbutamol infusion (P < 0.001, P < 0.001,and P < 0.01, respectively). Similarly, the values offorce velocity parameters related to the LV developed
pressure (Peak P/ , Vce, V, and V40) were far lower
than normal values. Of these parameters there was
statistically significant improvement in V5 and V40(P < 0.02 and P < 0.05, respectively). Thus, in StudyB patients all the parameters of contractility measured
1-i-
// SALBUTAMOL
I
* Resto Exercise
o-FCONTROL
I ILV
0 10 20 30 40 50
LEFT VENTRICULAR END DIASTOLIC PRESSURE (mmHg)
FIGURE 5. Effects of Salbutamol infusion on the Starlingrelation between left ventricular stroke work and end-diastolic pressure in patients with congestive car-diomyopathy.
were depressed during the control resting period, in-dicating severe heart muscle disease. Also, there wassignificant improvement in the majority of myocardialcontractility parameters during Salbutamol infusionwithout significant change in the heart rate andsystemic arterial pressure.
Effect ofMidcircumferential Wall Stress (table 2,fig. 7)
In Study B, the end-diastolic midcircumferentialwall stress at rest was significantly elevated (86 ± 5dyne/cm2 X 103), as compared to the normal values(12.2 ± 1.2 dyne/cm2 X 103). Salbutamol significant-ly lowered this stress (P < 0.001) in these patients.The midwall peak systolic circumferential stress wasnormal at control rest and did not change significantlyduring Salbutamol infusion. However, when LV wallstress (tension) was plotted against time duringsystole, these patients showed an abnormal response.Instead of the usual normal rapid fall in wall stressduring the mid and late ejection period, four patientsshowed sustained or increasing wall stress throughoutthe ejection period. During Salbutamol infusion thisabnormal response was abolished in all four patients.
L VEDP- Volume Relation and VentricularCompliance (table 2 and fig. 8)At rest the average LVEDV in normal subjects was
84 ± 5 ml/ml (average ± SEM). The average LVEDVin patients with congestive cardiomyopathy (210 ± 10ml/M2) was significantly higher (P < 0.001) than nor-mals. During Salbutamol infusion the average value ofLVEDV (183 ± 9 ml/M2) was significantly lower
HAEMODYNAMIC EFFECTS OF SALBUTAMOL INFUS ION
DURING EXERCISE IN PATIENTS WVITH HEART FAILURE
H.R. per min
C.O. I/min
M.A.P. mm
L.V.E.D. P.
mmHg
10
455
A
by guest on July 10, 2018http://circ.ahajournals.org/
Dow
nloaded from

VOL 58, No 3, SEPTEMBER 1978
IA_Umk time amu o WPM I/-P wrw Lii V.iticulr wusur.
3
CONROL
so
FIGUREL6.LVdp/dt haseenplot g EFT WNWRICUIAR PSSUE mmHgFIGLJRE 6. L Vdp /dthas been plotted against left ventricular (L V) pressure in all six patients (as shown bydifferent symbols) with congestive cardiomyopathy in Study B. Descending limb of each curve is ex-trapolated to the zero L V pressure (dotted line) in order to calculate Vmax (see text). Note low value ofVmax during control period and its significant improvement during Salbutamol infusion.
(P < 0.05) than control value. The average LVEDPfor the cardiomyopathy group was 28 ± 3 mm Hg(P < 0.001), which was significantly higher (P < 0.01)when compared to the normal group (table 2). Inpatients with congestive cardiomyopathy, the averagevalue of LV diastolic compliance index (0.022 ± 0.05)was significantly reduced (P < 0.02) when comparedwith the average value in normals (0.196 ± 0.01), in-dicating significant reduction in ventricular disten-sibility in patients with congestive cardiomyopathy.During infusion of Salbutamol this index of ventric-ular distensibility was nearly normal (0.109 ± 0.04).
The total passive diastolic compliance index, P/AVP
was significantly higher in patients with congestivecardiomyopathy (P < 0.01) when compared with thevalues obtained in normal subjects. During the infu-sion of Salbutamol the average value of this stiffnessindex decreased significantly (P < 0.02). There was nosignificant difference between the normal value andthe value obtained during Salbutamol infusion inpatients with congestive cardiomyopathy. TheLVEDV-mass ratio (Ved/Vw) was significantly higherin cardiomyopathic patients (P < 0.01) and did notchange significantly during the infusion ofSalbutamol.The stiffness constant K during the control rest in
patients with congestive cardiomyopathy was19.9 ± 4. This was not significantly different from thevalue achieved during Salbutamol infusion (19.3 ± 3)and the normal group (14.3 ± 3). Em was markedlyelevated (1710 ± 392 dyne/cm2 X 103) in patientswith congestive cardiomyopathy (P < 0.001) and wassignificantly reduced (890 ± 275 dyne/cm2 X 103) dur-ing Salbutamol infusion (P < 0.001), yet remainedsignificantly higher than normal value (205 ± 22dyne/cm2 X 103). In figure 8, Em was plotted against
end-diastolic stress. This indicated that patients withcongestive cardiomyopathy, before and duringSalbutamol infusion, were operating at different stresslevels of the same stiffness-stress curve.
DiscussionAn assessment of myocardial function apart from
studying the performance of the heart as a pump is ofcontinuing interest to clinical cardiologists. Variouscompensatory mechanisms may mask pump failureuntil late in the course of the disease. Therefore, theknowledge of both systolic performance and diastolicproperties is important for an accurate diagnosis ofmyocardial dysfunction, and for the evaluation of themechanisms of action of a particular therapeuticagent. Study B was specifically designed for this pur-pose. Data from this study indicate that patients withcongestive cardiomyopathy have depressed myocar-dial contractility, decreased LV compliance, increasedend-diastolic stress and elevated Em. These findingsare in agreement with the pressure-volume datareported by Gaasch et al.'9
Salbutamol infusion in patients with congestive car-diomyopathy improved cardiac function (at rest aswell as during mild supine exercise), increased LVdiastolic compliance and decreased Em. Also,Salbutamol decreased end-diastolic wall stress andimproved the stress-time curve relationship duringsystole. With this improvement in myocardial func-tion, Salbutamol infusion in a dose of 0.5 g/kg/mindid not significantly change heart rate and systemicarterial pressure in these patients. Previous studieshave shown Salbutamol infusion to produce an im-provement in patients with valvular heart diseasewithout heart failure9 and cardiogenic shock.20 Thisstudy has indicated its further usefulness in severeheart muscle disease.
CIRCULATION456
by guest on July 10, 2018http://circ.ahajournals.org/
Dow
nloaded from

SALBUTAMOL IN CONGESTIVE CARDIOMYOPATHY/Sharma and Goodwin
WASUREINT OF CIRCUWERNEIAL MIDWALL STIESSIN A PATENT WITH CONGESTIVE CARDIOMYOPATHY
* BeXre
oAfter Salbuamol
FIGURE 7. Effect of Salbutamol on
midwall stress time curve in a patient withcongestive cardiomyopathy.
* lul lmm~0 80 160 240 320 400 480 560
Time (msec)
The claims for increased myocardial contractilitymay be questioned because there are disadvantages at-tached to all the various measurements of cardiac con-tractility. In order to overcome some of these objec-tions, this study was designed to influence manyaccepted derived parameters of contractility. The ma-jority of these indices (Vpm, Vce, Vmax, V40 and V5)have shown consistent unidirectional changes before
20
-b 16-sn*c
r
i 12-
CD
8-
tn
Xu 4-lii
0
0
0
0
Control Congestive
Salbutamol Cardiomyopathy
and during Salbutamol infusion. Vpm, which isregarded as one of the reliable indices of contractilityand is independent of changes in preload, afterload,and CO,21 was found to be consistently low in the con-trol period and consistently increased duringSalbutamol infusion. The decision of whether a giventherapeutic agent is an inotropic agent or a vaso-dilator can be difficult when a study is carried out in
FIGURE 8. Elastic stiffness (Em) has beenplotted against end-diastolic wall stressbefore and during Salbutamol infusion inpatients with congestive cardiomyopathy.
P; 200
2I
0
II I I I
20 40 60 80 100 120Mid wall end diastolic stress CGm (103dynes/cm)
457
PL F.G.
by guest on July 10, 2018http://circ.ahajournals.org/
Dow
nloaded from

VOL 58, No 3, SEPTEMBER 1978
man. Since heart rate, preload and afterload, if notcontrolled, can be affected equally by both agents,these simple, easily obtainable parameters cannot beused reliably to distinguish a vasodilator from an ino-tropic agent. Although concomitant vasodilator effectis difficult to exclude, Salbutamol has been shown toincrease stroke volume, ejection fraction and otherdirect indices of myocardial contractility. Salbutamolhas also been shown to increase those indices ofmyocardial contractility which are known to be leastaffected by preload and afterload. Other sensitive andreliable indices of contractility, as described in theliterature, are maximum rate of change of aorticblood flow and maximum rate of change in LVpower.22 Recently, other investigators in this field havestudied the effect of Salbutamol and nitroprusside onthese two parameters in nine patients after cardiacsurgery and demonstrated that Salbutamol signifi-cantly augments the maximum acceleration of aorticblood flow and maximum rate of change in LVpower,23 while nitroprusside does not change the ac-celeration and reverses the effect of Salbutamol onmaximum rate of change in LV power. Thus, fromthis and other studies,23 it may be suggested thatSalbutamol enhances the inotropic state of the leftventricle.
Alterations in LV compliance are affected by manyfactors other than elastic properties of the myocar-dium. Most accepted factors related to the left ventri-cle itself altering compliance are ventricular geometry,initial volume, hypertrophy, wall thickness, ventric-ular filling rate 15, 17, 19, 24-26 and ventricular stiffness.Changes in the behavior of the anatomical constraintsto the LV distension, including right ventricularchamber,27 the pericardium and the pleural cavity28associated with altered pressure and volume-loadingconditions, have also been suggested to contribute tothe observed displacement of the LV pressure-volumecurves. Another constraint to the LV pressures, vol-ume and shifting pressure-volume relationship,without directly altering ventricular stiffness, is theperfusion pressure within the coronary vascularbed.29' 30 However, in this study it is unlikely that thecompliance changes with Salbutamol infusion havebeen produced by the changes in the ventriculargeometry or hypertrophy. Although pleural pressureswere not measured, Alderman et al.28 did suggest thatchanges in the pleural pressure may slightly affectpressure-volume relations between patients, butindividual patients under identical respiratory con-ditions have pleural pressures which are similar andwould not account for a significant shift of pressure-volume relation. Thus, with Salbutamol infusion animprovement in the pressure-volume relationship maybe attributed to changes either in the elastic propertiesof the myocardium or to alteration of the physicalconstraints to the LV distension produced by the rightventricle, pericardium and/or perfusion pressurewithin the coronary vasculature. Since myocardialcontractility in itself does not directly affect ven-tricular compliance,31' 32 it might be suggested that animprovement in the LV diastolic dysfunction could be
due to an action of Salbutamol, independent from itsinotropic action.The acute effects of an inotropic agent on LV
diastolic compliance in congestive cardiomyopathyhave not been well-documented. Although previousclinical observations suggested an improvement in thepulmonary hemodynamics in congestive heart failureafter the use of an inotropic agent, this may be relatedto improved compliance with consistent alteration inpassive pressure-volume relation in addition toenhancement of cardiac contractile property. Changesin ventricular compliance related to ischemia may becorrected," and observations in LV compliance andchronic volume overload may at least be partiallyreversible, as shown in children after closure of aVSD33 and in certain patients after surgical correctionof aortic regurgitation.34 This study suggests thatSalbutamol infusion has acutely improved the long-standing and profoundly abnormal pressure-volumecharacteristics of the diseased left ventricle of con-gestive cardiomyopathy.The potential of Salbutamol as a therapeutic agent
for heart failure or congestive cardiomyopathy has notbeen established. This study indicates Salbutamol in-fusion may be an effective means of improving pumpfailure, abnormal wall stress, ventricular complianceand Em properties of the left ventricle. Oral prepara-tions of this drug, currently used in the treatment ofobstructive airways disease, should be investigatedfurther. Combined therapy with such an inotropicagent and vasodilator drug may be a potenttherapeutic combination for severe intractable heartfailure.
Acknowledgment
The authors would like to thank Drs. Howard Burchell, MorrisonHodges, Gary Francis and Barbara Nelson for their help in prepar-ing this paper, and the staffs of the Cardiac CatheterizationLaboratory and Hammersmith Hospital, London, for theirtechnical assistance. Authors are also indebted to the British HeartFoundation for the generous grant for this work.
References1. Majid PA, Sharma B, Taylor SH: Phentolamine for
vasodilator treatment of severe heart failure. Lancet 2: 719,1971
2. Majid PA, Sharma B, Meeran MKM. Taylor SH: Insulin andglucose in the treatment of heart failure. Lancet 2: 937, 1972
3. Sriussadaporn S, Cohn JN: Inotropic properties of an iso-quinoline derivative (NC 7197) in man. Am Heart J 85: 374,1973
4. Akhtar N, Chaudhry MH, Cohn JN: Dobutamine: selectiveinotropic action in patients with heart failure. Circulation 48(suppl IV): IV-136, 1973
5. Guiha NH, Cohn JN, Mikulig E, Franciosa JA, Lima CJ:Treatment of refractory heart failure with infusionnitroprusside. N Engl J Med 291: 587, 1974
6. Forman R, Kirk ES, Downey JM, Sonnenblick EH:Nitroglycerin and heterogeneity of myocardial blood flow:reduced subendocardial blood flow and ventricular contractileforce. J Clin Invest 52: 905, 1973
7. Franciosa J, Cohn JN: Hemodynamic improvement withhydralazine in left heart failure. Clin Res 24: 217, 1976
8. Miller RR, Awan NA, Maxwell KS, Mason DT: Sustainedreduction of cardiac impedance and preload in congestive heart
458 CIRCULATION
by guest on July 10, 2018http://circ.ahajournals.org/
Dow
nloaded from

SALBUTAMOL IN CONGESTIVE CARDIOMYOPATHY/Sharma and Goodwin
failure with the antihypertensive vasodilator prazosin. N Engl JMed 297: 303, 1977
9. Gibson GD, Coltart DJ: Hemodynamic effects of intravenoussalbutamol in patients with mitral valve disease: comparisonwith isoprenaline and atropine. Postgrad Med 47 (suppl 40):40-4, 1971
10. Dexter L, Whittenberger JL, Haynes FW, Goodale WT, GorlinR, Sawyer CG: Effect of exercise on circulatory dynamics ofnormal individuals. J Appl Physiol 3: 439, 1951
11. Taylor SH, Sutherland GR, Hutchinson DE, Kidd , Robert-son PC, Kennedy BM, Donald KW: Effects of intravenousguanethidine on the systemic and pulmonary circulation inman. Am Heart J 63: 239, 1962
12. Kasser IS, Kennedy TW: Measurement of left ventricularvolume in man by single plane cine angiography. Invest Radiol4: 83, 1969
13. Sharma B, Goodwin JF, Raphael MJ, Steiner RE, RainbowRG, Taylor SH: Left ventricular angiography on exercise: anew method of assessing left ventricular function in ischemicheart disease. Br Heart J 38: 59, 1976
14. Smith M, Ratshin RA, Harrell FE: Early sequential changes inleft ventricular dimensions and filling pressure in patients aftermyocardial infarction. Am J Cardiol 33: 363, 1974
15. Miller RR, DeMaria AN, Amsterdam EA, Mailander MM,Zelis R, Lurie AJ, Mason DT: Improvement of reduced leftventricular diastolic compliance in ischemic heart disease aftersuccessful coronary artery bypass surgery. Am J Cardiol 35: 11,1975
16. Diamond G, Forrester JS, Hargis J, Parmley WW, Danzig R,Swan HJC: Diastolic pressure volume relationship in the canineleft ventricle. Circ Res 29: 267, 1971
17. Diamond G, Forrester JS: Effect of coronary artery disease andacute myocardial infarction in left ventricular compliance inman. Circulation 45: 11, 1972
18. Mirsky I, Parmley WW: Evaluation of passive elastic stiffnessfor the left ventricle and isolated heart muscle. In CardiacMechanics, edited by Mirsky I, Ghista DN, Sandler H. NewYork, John Wiley & Sons, Inc, 1976, p 331
19. Gaasch WH, Battle WE, Oboler AA, Banas JS, Levine HS:Left ventricular stress and compliance in man. Circulation 45:746, 1972
20. Lal S, Savidge RS, Davies DM, Ali MM, Soni V: Intravenoussalbutamol and cardiogenic shock. Lancet 1: 853, 1972
21. Mirsky I, Parmley WW: Force velocity studies in isolated andintact heart muscle. In Cardiac Mechanics, edited by Mirsky I,Ghista DN, Sandler H. New York, John Wiley & Sons Inc,1974, p 89
22. Noble MIM, Trenchard D, Guz A: Left ventricular ejection inconscious dogs: 1. Measurement and significance of the max-imum acceleration of blood from the left ventricle. Circ Res 19:139, 1966
23. Pool-Wilson PA, Lewis G, Angerpourter T, Malcolm AD,Williams BJ: Hemodynamic effects of salbutamol in patientsneeding circulatory support after open heart surgery. Br HeartJ 39: 721, 1977
24. Forrester JS, Diamond G, Parmley WW, Swan HJC: Early in-crease in left ventricular compliance after myocardial infarc-tion. J Clin Invest 51: 598, 1972
25. Covell JW, Taylor RR, Ross J Jr: Series elasticity in the leftventricle determined by quick release technique. Fed Proc 26:382, 1967
26. Spotnitz HM, Sonnenblick EH: Structural conditions in thehypertrophied and failing heart. Am J Cardiol 32: 398, 1973
27. Bemis CE, Serun JR, Borkenlagen D, Sonnenblick EH,Urschel CW: Influence of right ventricular filling pressure onleft ventricular pressure and dimension. Circ Res 34: 498, 1974
28. Alderman EL, Glantz SA: Acute hemodynamic interventionsshift the diastolic pressure-volume curve in man. Circulation54: 664, 1976
29. Bacamer M, Connoly JR, Bruns D: Coronary blood flow as acritical determinant of cardiac performance and cardiac size.Am J Med 30: 392, 1961
30. Salisbury TF, Cross CE, Rieben TA: Influence of coronaryartery pressure upon myocardial elasticity. Circ Res 8: 794,1960
31. Windenthal K, Mullin CB, Harris MD, Mitchell JH: Left ven-tricular end-diastolic distensibility after non-epinephrine andpropranolol. Am J Physiol 217: 821, 1969
32. Templeton GH, Ecker RR, Mitchell JH: Left ventricularstiffness during diastole and systole: the influence of changes involume and inotropic state. Cardiovasc Res 6: 95, 1972
33. Jarmakani JMM, Graham TP, Canent RV Jr, Capp MP:Effect of corrective surgery on left heart volume and mass inchildren with VSD. Am J Cardiol 27: 254, 1971
34. Gault JH, Covell JW, Braunwald E: Left ventricular perfor-mance following correction free aortic regurgitation. Circula-tion 42: 773, 1970
Appendix1. Calculation of the Pressure-Related Parametersof Myocardial Contractility:Maximum rate of pressure rise in the left ventricle(LV dp/dt max) was derived by the R-c differentiatingcircuit connected to the left ventricular LV pressure.By simultaneously recording LV pressure with itsderivative and aortic pressure, the following indiceswere calculated in Study B:
Vpm Peak (dp/dt)Sec-lVpm =Pealk PA1
Where p is the instantaneous LVpressure.
Vce = Peak (dp/dt)Sec 1Kp
A2
Where K is the series elastic constant.A value of 28 mm sec muscle-lengthwas used for k appropriate to theprevious studies in isolated heart.
Vmax =dp/dtPo
A3
dp/dt at LV zero pressure (Po) wasobtained by computer extrapolation ofthe descending limb of (dp/dt) curve
to zero pressure employing an ex-ponential curve fit to the formula y =
a + bc where a, b and c are constantsdetermined from a nonlinear regres-sion analysis.
Similarly, Peak (dp/dt) and (dp/dt)Pd KPd A4
were calculated employing developedpressure (Pd) in the left ventriclewhich in turn was calculated as in-stantaneous LV pressure minus LVend-diastolic pressure.
Since Vmax at zero developed pressure-approachedinfinity the following measurements were made:
A5V5 = (dp/dt)Sec-1P5
V40 = (dp/dt)Sec-1P40
A6
459
by guest on July 10, 2018http://circ.ahajournals.org/
Dow
nloaded from

VOL 58, No 3, SEPTEMBER 1978
Where P5 and P40 are developed pressure of 5and 40 mm Hg during isovolumic systole.
2. Calculation of L V Volume-Mass Ratio. (V/ Vw),Mideircumferential Wall Stress (am) and ElasticStiffness:'8
Volume-mass ratio Ved/Vw - Ved 4wr 03-a3)3 A7
Where Ved is end-diastolic volume, Vw isLV-muscle volume, a and b are internal andexternal radii, respectively.
Midcircumferential wall stress (am) = P (V/Vw)
(1 + b3)2R3 A8
where p is LV pressure, V is instantaneousLV volume, b is external radius and R is(a + b) where (a) is internal radius.2
Elastic Stiffness (Em) = K crm A9
where K = is elastic stiffness constant whichin turn is calculated as:"9
K = 3 + 3 1oge 2.33 (LVEDP) Alo
Aortic Input Impedance in Heart Failure
CARL J. PEPINE, M.D., WILMER W. NICHOLS, Ph.D., AND C. RICHARD CONTI, M.D.
SUMMARY The input impedance of the systemic circulation was calculated from recordings of pulsatile pressure andflow in the ascending aorta of 20 patients. Ten patients had clinical and hemodynamic evidence of heart failure. The other 10subjects had no clinical evidence of heart failure and were used as a control group. In the heart failure patients, both inputresistance and characteristic impedance (index of aortic distensibility) were significantly increased compared to pressure-
and age-matched control subjects. Oscillations of impedance moduli, represented by the difference between maximum andminimum moduli, were also significantly increased in the heart failure patients compared with the control subjects. The in-creased characteristic input impedance in these heart failure patients suggests that the human aorta is stiffer in heart failure,and the larger oscillations in the impedance spectrum indicate an increase in pressure and flow wave reflections. Fromreflected wave theory in elastic tubes, reflected pressure waves add to the amplitude of incident pressure waves at the en-
trance of the system, whereas reflected flow waves subtract from the magnitude of the forward flow. Thus, changes in aorticdistensibility could have an important influence on the pulsatile function of the failing left ventricle.
THE AORTA AND LARGE ARTERIES of thesystemic circuit are not rigid pipes, but constitute adistensible elastic buffering chamber. These elasticproperties permit a damping mechanism throughwhich pulsatile blood flow waves ejected from the leftventricle are converted to a near-constant blood flowfor resistance vessels to distribute to systemiccapillaries. Elastic properties of these large vessels canbe modified by autonomic nervous effects on vascularsmooth muscle cells with only minor changes in vesseldimensions.' Recent studies in our laboratoriessuggest that age and the presence of atherosclerosismay also be important in modifying the elastic proper-ties of large vessels.2
In heart failure, previous studies have emphasizedabnormal ventricular and peripheral hemodynamic
From the Division of Cardiovascular Medicine, University ofFlorida, Shands Teaching Hospital and Gainesville Veterans Ad-ministration Hospital, Gainesville, Florida.
$upported in part by grant HL 17717-02 from the NIH and agrant from the Veterans Administration.
Address for reprints: Carl J. Pepine, M.D., Division of Car-diovascular Medicine, P.O. Box J-277, JHM Health Center,Gainesville, Florida 32610.
Received December 19, 1977; revision accepted May 5, 1978.
responses.' The peripheral responses consist of ab-normal vasoconstriction both at rest and during exer-cise.' The latter changes were thought to be compen-satory and possibly important in maintaining regionalblood flow.5 6 Recent interest in these so-called"compensatory" changes in vascular resistance hasemerged due to the application of vasodilator therapyin patients with heart failure.7 These studies suggestthat the failing ventricle's pump performance ismarkedly influenced by alterations of the mean com-ponent of the total resistive load. Alterations of aorticdistensibility also have the potential to alter thedynamic or pulsatile component of the vascularload.2, 8-10 This alteration could be deleterious in thepatient with a failing ventricle. A study of this part ofthe ventricular afterload in patients with heart failurehas not been reported. In this investigation we studiedthe total impedance spectrum at the input to thesystemic arterial system in patients with heart failure.These findings were compared to measurements madein age-matched subjects with similar aortic pressurewho had no evidence of heart failure. These findingsmay also be useful in providing a basis for future in-vestigation of agents designed to reduce the pulsatilecomponent of afterload.
CIRCULATION460
by guest on July 10, 2018http://circ.ahajournals.org/
Dow
nloaded from

B Sharma and J F GoodwinEffect on systolic and diastolic function of the left ventricle.
Beneficial effect of salbutamol on cardiac function in severe congestive cardiomyopathy.
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1978 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/01.CIR.58.3.449
1978;58:449-460Circulation.
http://circ.ahajournals.org/content/58/3/449.citationthe World Wide Web at:
The online version of this article, along with updated information and services, is located on
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer information about this process is available in the
located, click Request Permissions in the middle column of the Web page under Services. FurtherEditorial Office. Once the online version of the published article for which permission is being requested is
can be obtained via RightsLink, a service of the Copyright Clearance Center, not theCirculationpublished in Requests for permissions to reproduce figures, tables, or portions of articles originallyPermissions:
by guest on July 10, 2018http://circ.ahajournals.org/
Dow
nloaded from