behçet’s syndrome - vasculitis foundation · behçet’s syndrome ... • german medical journal...
TRANSCRIPT

Behçet’s SyndromeYusuf Yazıcı, MD
Assistant Professor of Medicine,NYU School of Medicine
Director, Seligman Center for Advanced Therapeutics & Behcet’s Syndrome Evaluation, Treatment and Research Center
NYU Hospital for Joint Diseases

2
History
• Hulusi Behçet described (1937) 3 patients with– aphthous mouth ulcers – genital ulceration – hypopyon uveitis
• All 3 patients studied over 17 years
• First to describe “triple symptom complex”• German medical journal (Dermatologische Wochenschrift)
• Prof. Mischner first proposed the name “Morbus Behcet” at a medical congress in Geneva (1947)

INTERNATIONAL STUDY GROUP CRITERIA FOR THE DIAGNOSIS (Classification) OF BEHÇET’S SYNDROME
3
Oral ulcers (100%)
+ 2 of the following:
a. genital ulcers (80%)b. eye lesions (50%)c. skin lesions (80%)d. pathergy (50%)

4
Distribution of Behçet’s disease

5
Symptoms

6
Demographics
• Mediterranean basin, Korea, Japan– Silk road?
‐ Very few cases in India
• Before puberty or after 6th decade, rare• Usual onset 3rd decade• Male: female equal numbers, • Worse disease in males
• 400/100,000 (16 yrs or older) in Turkey• 1‐3/100,000 in Olmstead County, MN

BS, not so rare
• Estimate the prevalence of BS in and around Paris• 26% non‐European descent• 7.1/100,000
– European 2.4– North African 17.5– Asian 34.6– Similar to rates in original countries
• Prevalence was similar regardless of age at immigration• Possibly primarily has a hereditary basis• Capture‐recapture, likely underestimates
• Interestingly, Behcet’s rates were similar to combined WG, CS and MPA combined, studied by the same group
Mahr A, et al. Arthritis Rheum 2008, in press

BS in Paris ‐ France (/100 000)
Disease Non – European European Overall
BS* frican: 35Asian: 17.5SuS. African: 5.1N-Cont. French: 6.2
2.4 7.1
1. PAN - - 3.0
2. MPA - - 2.5
3. WG - - 2.3
4. CSS - - 1.1
Total (1,2,3,4) 5.3 10.5 8.9
A Mahr et al Arthritis Rheum 2001; A Mahr et al. Arthritis Rheum in print; H Yazici et al Arhritis Rheum in print

CLINICAL MANIFESTATIONS

10
Oral ulcers• Virtually all patients
• Frequently first manifestation
• Minor aphthous ulcers are most common
– Lips, gingiva, cheeks and tongue– Unlike herpes, skin covered part of lips not involved– Usually heal in 15 days without scarring– Some complain of premenstrual activation
• Major ulcers
– Larger, may scar, lasts longer, less common– Recurrent aphthous stomatitis (RAS)
• 20% in population• Very rare for RAS to have another clinical finding• No HLA B51 association• There are no differences among the two ulcers histologically

11
Genital ulcers
• Papules or pustules that ulcerate quickly
• Punched out appearance
• Aseptic ones heal in 3 weeks, very likely to get secondary infections
• In males usually scrotum is involved, scars, and absence of lesions on glans penis is typical
– All females should have a gynecologic examination, scarring in the right clinical picture is good evidence

12
Skin manifestations of BS
• Papulopustular (acne) lesions (85%)
• Indistinguishable from acne vulgaris
• Later decades of life vs. teens• Atypical places, arms
• Acne is androgen dependent, however, androgen levels are normal• Increased severity in males?

13
Acne and arthritis in BS
• 44 patients with BS and arthritis
• 42 patients with BS without arthritis • 21 patients with RA • 33 healthy controls
•Acne scores were very significantly higher among BS patients with arthritis
E Diri et al Ann Rheum Dis 2001

14
Target organ associations in BS
• An Analysis of 272 consecutive patients
• Factor I : • oral ulcers + genital ulcers+ erythema nodosum
• Factor II: • superficial vein thrombosis + deep vein thrombosis
• Factor III: • Uveitis
• Factor IV: • acne + arthritis
Tunc R, et al J Rheumatol 2002

Enthesopathy and BS
• To test if enthesopathy was increased in the acne/arthritis cluster
• 35 BS with acne/arthritis– 38 BS without arthritis– 37 AS– 25 RA– 25 HC
• 5 enthesal sites by US– Sup/inf poles of patella– Tibial tuberosity
Hatemi G et al, Arthritis Rheum 2008

Enthesopathy
Hatemi G et al, Arthritis Rheum 2008

17
Nodular lesions of BS
• 60 % of patients• 50% e.nodosum like lesions (more
common in women)• 50% superficial thrombophlebitis
(associated with major vessel involvement)
• Difficult to tell one from the other.

18
CNS involvement in BS
• CNS involvement has a frequency of 4 % in prospective, cross‐sectional studies.
• The frequency goes up to 10 % in longer follow‐up.
• Peripheral neuropathy is distinctly rare.
• CNS involvement has two distinct forms:A. Parenchymal disease (80%, bad prognosis)B. Dural sinus thrombi (20%, favourable prognosis)
‐ A and B rarely co‐exist

CNS disease differential diagnosis
Brainstem, diancephelon and pontobulbar regions mainly effected Peripheral neuropathy very rare CNS lesions do not follow a specific vascular pattern Isolated cerebellar disease rare Meningeal symptoms and on ocasion convulsions can be seen Multiple sclerosis, and on occasion sarcoidosis can cause problems
19

Behçet’s Syndrome vs Multiple Sclerosis
MS BSHeadache ± +++
Optic neuritis +++ ±Sensory problems +++ ±PV and SC lesions +++ ±Brainstem lesions Small, no upward
extensionLarge, with upward extension
Spinal cord lesions +++ +
Inflammatory CSF ± +++
OCB > 90% ~ 10%

21
Pulmonary Artery Aneurysms
Unique complication of BS Diagnosed mainly at postmortem until 1980 – the most frequent arterial
complication today Strongly associated with venous thrombosis Large proximal branches of pulmonary arteries

22
Mortality in PAA
• Survival rate: 62% at 5 years (new cohort)• 70% of the deaths occurred within 1 year following emergence of PAA
Hamuryudan V, et al Am J Med 2004

23
BS vs. Crohn’s Disease
Korman U, et al Abdominal Imaging 2003

24
Pathergy reaction
• Non‐specific hyperreactivity to minor trauma
• Can also be seen in pyoderma gangrenosum
• Standard technique– 20 gauge needle– Papule or pustule in 48 hours– Induration required– More common in Middle East
• Interestingly PPD is not augmented in BS patients
– Hatemi G et al. Rheumatology 2008

25
Eye disease in BS• Most serious when considering frequency and morbidity
• Leading cause of non‐traumatic blindness after DM in Japan, Israel
• Non‐granulomatous panuveitis and retinal vasculitis
• Over all 50%– 70% of males <25 yr
• Frequently present at onset or first 2‐3 yrs– Rare after 5 years of disease
• Bilateral in 90%
• Hypopyon is classical finding in eye disease (20%)– Almost always accompanied by severe retinal vasculitis

26

27
Thrombophilia in BS
• 1/3 of patients have thrombophlebitis
• Abundant evidence for functional impairment of the vessel wall;• an autoinflammatory
endothelitis?
• Abnormalities in the coagulation cascade?

28
DVT
• DVT in BS is an inflammatory reaction to the endothelium
• It is a sticky and very hard clot, no trailing tail formation
• Very rare for it to break off and embolise
• ? Anti‐coagulation in DVT with BS

29
Long‐term mortality and morbidity of BS: Two decade outcome study
• 428 (286M / 142F) BS patients registered at Cerrahpaşa BS Multidisciplinary Outpatient Clinic between 1977‐1992
• Found to have died: 42(9.8 %) ‐ 39M / 3F
• Could not be reached: 41(9.6 %) ‐24M /17F)
Seyahi E, et al. Medicine (Baltimore) 2003

30
STANDARDIZED MORTALITY RATIOS OF 286 MALE PATIENTS WITH BS STRATIFIED AS TO THE AGE OF ONSET AND EVALUATED AT 7 YEAR INTERVALS
2.04
4.91
17.85
2.46
5.59
23.03
3.97
6.99
28.73
1.11
3.02
10.22
1.25
3.20
12.87
1.823.21
13.20
0.531.73
5.28
0.541.65
6.42
0.671.18
4.84
0
5
10
15
20
25
30
35
14-24 25-34 35-50 14-24 25-34 35-50 14-24 25-34 35-50
7 YEARS
14 YEARS
20 YEARS

31
Main causes of death among 42 patients
• Vascular disease: 17 (venous 5)• CNS disease: 5• Amyloidosis: 3• Malignancy: 4• Suicide: 2• Misc: 11
• PAA– Main reason for mortality
– Frequently associated with thrombi in inferior vena cava and iliac‐femoral system
– Presents with hemoptysis, may look similar to PE
– Anticoagulation contraindicated

32
Onset of eye disease in males
2 (1%)4 (2%)
16 (9%)
6 (3%)5 (3%)
98 (54%)
27 (16%)
8 (4%) 10 (6%)4 (2%)
0
20
40
60
80
100
120
-1 0 1 2 3 4 5 6-10 11-20 21-30
OD
Years
%

33
Other manifestations
Beginning End
OU (%) 345 (100.0) 220 (63.7)*
GU (%) 310 (89.9) 90 (26.1)*
EN (%) 223 (64.4) 88 (25.5)*
Arthritis (%) 140 (40.6) 34 (9.9)*
* P=0.001

34
Disease course in BS
• The disease burden of BS decreases with the passage of time
• During the disease course the occurrence of all manifestations seem decrease in frequency accept for CNS disease and major vascular pathology.
• This disease course is unlike what has been reported for RA and SLE.
• It’s biological meaning remains to be understood.

35
Differential diagnosis
• Sacroiliitis and spinal joint involvement are not features of BS
• Skin lesions do not include psoriasis
• Urethral discharge is not a feature of BS
• GI involvement with ileocaecal ulceration and sometimes colonic perforation is distinct from typical IBD

36
Clinical evidence for autoimmunity in BS?
Uncommon/not seen in BS: Sjögren’s syndrome Association with other
autoimmune diseases Raynaud’s phenomenon Polyserositis Hemolytic anemia Sun sensitivity No autoantibodies
Unique to BS: Pathergy Genital ulcers – scrotal Pulmonary artery aneurysms Clinical course

37
Autoinflammatory?(FMF as the prototype)
Epidemiology - Mediterranean vs. Japan
Rare and almost all defined from the West
- Children vs. adults
Clinical findings
Genetic aspects- HLA B51 - Pyrin
Response to treatment (colchicine story) Well defined mutations (TNF-receptor, pyrin or CARD/NOD) and
transmission Usually a non - abating course

38
CAD in Patients with Severe Vascular Disease of BS
24 males Age: 37.5 ± 4.5 yrs. Disease duration: 13.2 ± 3.9 yrs. Smoking: 88% Steroid use: 63% 3/24 (12.5%) had angina pectoris
Coronary calcification and stenosis: 3/24 (12.5%)
Seyahi-Kural E et al. Rheumatology, 2004

39
Prevalence of carotid artery plaques in male patients vshealthy controls
*: Mean age for BS: 40 ±7, RA: 46 ± 7, AS: 39 ± 7, HC: 38 ± 8 years
**: Adjusted for age and presence or absence of diabetes mellitus and hypertension
Diseases * n (%) Adjusted**
OR (95%CI)
p
BS (n =162)
RA (n = 24)
AS (n =58)
HC (n = 83)
31 (19)
11 (46)
9 (16)
10 (12)
1.5 (0.7- 3.4)
3.5 (1.1- 10.9)
1.3 (0.5- 3.5)
-
0.33
0.033
0.64
-
Kural-Seyahi et al Ann Rheum Dis, 2008

Genetics of Behcet
• HLA B51– ? HLA A26 in Japanese and Turkish
• GWAS– IL‐10
• IL‐10 knockout mice intestinal inflammation• UC, Crohn’s• Increasing IL‐10 may restore imbalance and control hyperinflmmation
– Interferon?‐aplha ?– IL‐23R , shared between Japanese and Turks
• Also found in spondyloarthritis group– AS, IBD, psoriasis– Genetic variants don’t overlap
– IL‐12RB2
Gul A. Clin Exp Rheumatol 2011

Genetic ? Environmental ?
Japanese living in Hawaii Hirohata et al. Hawaii Med J , 1975
Turkish immigrants vs Germans in Berlin NG Papoutsiset al. Clin Exp Rheumatol 2006
Arabs/Druzes vs Jews in Israel I Krause et al. Clin Rheumatol 2007
North African immigrants vs Europeans in Paris A Mahr et al. A Mahr et al. Arthritis Rheum, 2008
41

42
Treatment

Systematic literature search: 2402 articles Exclusions:
Duplications Review articles Editorials Case reports Studies where the results for BD was not given separately
137 articles 20 randomized controlled trials 43

44
Colchicine in BS

45
Corticosteroids

46
Corticosteroids in BS(Skin‐Mucosa Manifestations)

47
Azathioprine in BS (I)
Prevents emergence of eye disease in the unaffected (p < 0.01)
Prevents eye disease becoming bilateral (p < 0.001)
Prevents eye disease getting severe (thus leading to withdrawal from the study) among the affected (p < 0.001)
Less frequent attacks of hypopyon (p < 0.001)
Preserves vision
Yazici H, et al New Engl J Med 1990

48
Azathioprine in BS (II)
Less frequent oral ulcers (p<0.005)
Less frequent genital ulcers (p<0.001)
Less frequent arthritis (p<0.02)
Less frequent thrombophlebitis (p<0.10>0.05)
Yazici H, et al New Engl J Med 1990

49
Azathioprine in BS (III)Reassesment after 8 years
Total loss of vision more in those initially allocated to placebo (p = 0.02)
Beneficial effects on visual acuity mainly among those who had been allocated to azathioprine within 2 years of onset of eye disease (p = 0.05 and 0.07 for either eye)
A trend for less frequent extraocular manifestations among the groups that received azathioprine
Hamuryudan V, et al Arhtritis Rheum 1997

50
Azathioprine in BS (IV)
Data avaliable had been for the 2.5 mg /kg/day dose!
Onset of action is slow (> 3 months)
Leukopenia with azathioprine + interferon

51
Interferon – α in BS Effective in controlling oro-genital ulceration
Alpsoy E et al Arch Dermatol 2002
Most probably effective in controlling acute eye disease (eyes improved in 5/6 patients in the Alpsoy study)
In the retracted paper the significant effects were seen only after the drug was stopped.
IFN alpha and corticosteroids 45 pt since 1988 Mean treatment duration 30m 26/79 (of 90 eyes) had recurrance
Krause L et al. J Rheum 2008
The time of onset of effect? Concurrent administration with immunosuppresives? Problems: Flu like illness, leucopenia, psoriasis, autoimmune disease, hair loss,
itching and depresion

52
Effect of etanercept on mucocutaneous manifestations of BS
• 40 males with mainly mucocutaneous BS were randomised to receive either etanercept (25 mg sc. 2x/wk) or placebo for 4 weeks.
• Weekly assessments were made as well as a 3 month evaluation after the trial ended.
• Pathergy reaction and the dermal response to MSU crystals were also measured before and after the trial.
Melikoğlu M et al. J Rheumatol, 2002

53
Effect of etanercept on mucocutaneous manifestations of BS
• There was 40% chance of remaining oral ulcer (OU) free in the etanercept arm versus 5% in the placebo arm (plog=0.002) at the end of 4 weeks.
• There were also significant decreases in the number OU, nodular lesions, acne lesions and arthritis with the expected exacerbations at 3 months after the trial ended.
• No effect on the pathergy reactions.
Melikoğlu M, et al J Rheumatol 2002

54
Infliximab for severe and treatmentresistant uveitis of BS
4 studies (open): – Fast (<24 hours) onset of action – Complete (attack free) remission:
31 – 75%– Infusions need to be continued
for sustained remission
Ohno S et al J Rheumatol 2004Sfikakis P et al. Ann Intern Med 2004Lindstedt EW et al. Br J Ophthalmol 2005Tugal‐Tutkun I et al. Arthritis Rheum 2005

55
Infliximab
• Active uveitis despite treatment– Azathioprine, steroids, cyclosporine
• Infliximab treatment for 13 patients– All male, all bilateral uveitis
• Weeks 0‐22=infusion period• Weeks 23‐54=observation period
Tugal-Tutkun I e al Arthritis Rheum. 2005 Aug;52(8):2478-84.

56
Infliximab

Apremilast
Hatemi G, et al. EULAR 2013

OU
28.6%
50.0%
70.9%
89.1%
0
10
20
30
40
50
60
70
80
90
100
Complete Response Partial Response
Per
cent
Placebo
30 mg BID

OU time to response
0.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
wk0 wk2 wk4 wk6 wk8 wk10 wk12 wk14 wk16 wk18 wk20 wk22 wk24 wk26 wk28Placebo 2.9 1.7 1.9 1.9 1.6 1.4 2.1 0.4 0.4 0.6 0.5 0.3 0.4 1.3 1.630 mg BID 2.7 0.3 0.7 0.5 0.5 0.7 0.5 0.6 0.6 0.6 0.7 0.2 0.6 1.9 1.7
Mea
n N
umbe
r of O
ral U
lcer
s All patients in the PBO group switched to APR from week 12 visit

OU Pain over time
0.0
10.0
20.0
30.0
40.0
50.0
60.0
wk0 wk2 wk4 wk6 wk8 wk10 wk12 wk14 wk16 wk18 wk20 wk22 wk24 wk26 wk28Placebo 51.7 29.8 37.4 36.7 30.7 23.5 35.0 7.9 7.9 7.3 7.2 6.6 9.6 17.2 21.030 mg BID 54.3 12.0 10.2 10.5 13.0 8.8 9.4 9.9 5.8 7.1 8.1 3.4 9.7 23.2 27.2
Mea
n O
ral U
lcer
Pai
n VA
S



EULAR Guidelines Ann Rheum Dis 2008
• Inflammatory eye disease with posterior segment involvement should be on azathioprine+corticosteroids
• Severe eye disease, retinal disease– Cyclosporine or infliximab added– Interferon alpha
• No firm guidelines for major vascular disease– DVT= immunosupression– PAA and peripheral aneurysm= CYC+corticosteroids
• No data about use of anticoagulants, anti‐platelet agents but not recommended
• No evidence base for GI treatment– Immunosupression, TNF
• In most patients, arthritis can be managed with colchicine
63

EULAR guidelines (2)
• No data on CNS disease management– AZA, CYC preferred, IFN alpha, TNF inhibitors
• Cyclosporine should not be used in CNS, unless needed for eye inflammation
• Mucocutaneous lesions, systemic treatment if resistant to topical measures
64

65
Management in 2013• Consider natural course, age, sex • Steroids: not for long‐term use• Colchicine:
• arthritis (M+F)• e. nodosum (M+F)• genital lesions among the females
• Thalidomide: – Good for all mucocutaneous lesions• toxicity precludes long‐term use
• Azathioprine• slow‐acting, usually under‐dosed
• Cyclosporine • fastest acting agent for eye disease; CNS toxicity?
• Interferon: • masked studies in eye disease needed
• TNF inhibitors• Quick response, use in combination
• Plaquenil, MTX, Cellcept,...
No anticoagulation for thrombophilia

What have we learned?
We have agents that can rather satisfactorily control the eye, skin‐mucosa, arthritis and, to some extent, major vascular problems of Behçet’s syndrome patients.
Earlier treatment is better.
Females not only have less severe disease but respond better to treatment.

What have we not learned?• How to manage CNS disease, thrombophilia and GI disease
• Whether there is a subset of patients that respond to colchicine
• Comparative efficacy (including time of onset of action)/safety of cyclosporin, interferon and a‐TNF agents in controlling eye disease
• Role of high dose corticosteroids in disease control
• Role of other biologicals • Prophylactic drug use (the young male) How long to continue treatment

NYU HJD Behçet’s Syndrome Evaluation, Treatment and Research Center
68
• Started in 2005
• ~700 patient seen
• ABDA
• RCT

Methods
• Patients were analyzed as the whole cohort and then also separated into to 2 groups:
– Non‐Ethnic= Patients with ethnic background in northern Europe and North America and /or self declared Caucasians without background around the Mediterranean and/or the Far East
– Ethnic= Patients with an ethnic background in the Mediterranean, Middle East, North Africa, and Far East.
• Israel 42, Italy 42, Arabic 23, Far East 23, Turkish 18, G k 9

Demographics
• Total of 471 (female 365, 77%)
• 296 meet ISBD criteria (63%)– 237 (80% female)
• Non‐ethnic: 163 (55%)• Ethnic: 133 (45%)
• Caucasian: 240 (81%), Hispanic 24(8%), Asian 13 (4%), other 11 (4%), African American 10 (3%)
• Patients from 45 states

Demographics (3)
Non‐Ethnic Ethnic Total
N Mean SD N Mean SD N Mean SD p
Age (Years) 163 37.1 13.7 133 35.3 11.9 296 36.3 12.9 0.167
Female (%) 162 140 86.4% 133 97 72.9% 295 237 80.3% 0.004
Married (%) 163 79 48.5% 133 62 46.6% 296 141 47.6% 0.752
Duration (Years) 146 3.6 6.0 127 3.8 6.0 273 3.7 6.0 0.932
Symptom Duration (Years) 149 9.1 8.6 126 8.5 7.6 275 8.8 8.2 0.919
Education (Years) 148 14.7 3.5 122 15.3 3.4 270 15.0 3.5 0.075
Function [0‐10] 159 1.9 1.9 129 1.6 1.8 288 1.7 1.9 0.212
Pain [0‐10] 156 4.9 3.2 130 4.4 3.1 286 4.6 3.2 0.217
Global [0‐10] 152 5.1 2.9 126 4.8 2.9 278 5.0 2.9 0.474
Fatigue [0‐10] 155 6.0 3.3 127 5.3 3.3 282 5.6 3.3 0.075
RAPID3 [0‐30] 150 11.8 7.1 125 10.7 6.8 275 11.3 7.0 0.186
BSAS [0‐100] 61 46.1 23.0 52 48.0 20.4 113 47.0 21.8 0.631
Adjusted Critical Value p=0.025
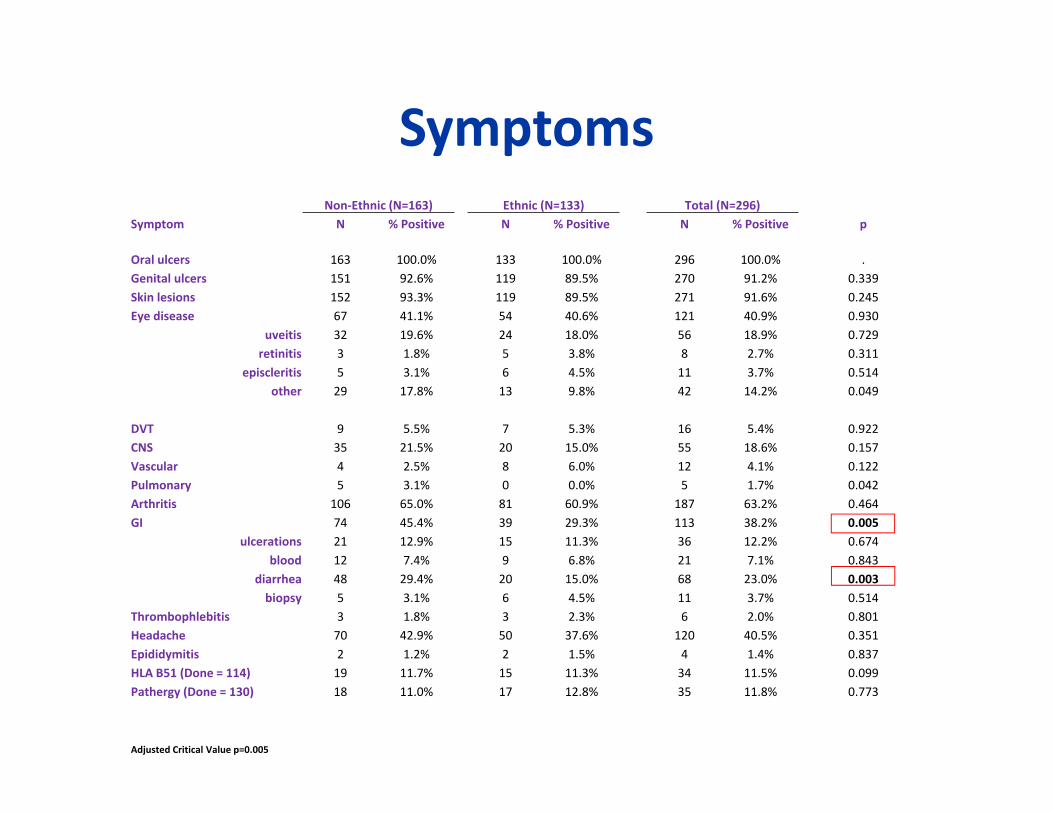
SymptomsNon‐Ethnic (N=163) Ethnic (N=133) Total (N=296)
Symptom N % Positive N % Positive N % Positive p
Oral ulcers 163 100.0% 133 100.0% 296 100.0% .Genital ulcers 151 92.6% 119 89.5% 270 91.2% 0.339Skin lesions 152 93.3% 119 89.5% 271 91.6% 0.245Eye disease 67 41.1% 54 40.6% 121 40.9% 0.930
uveitis 32 19.6% 24 18.0% 56 18.9% 0.729retinitis 3 1.8% 5 3.8% 8 2.7% 0.311
episcleritis 5 3.1% 6 4.5% 11 3.7% 0.514other 29 17.8% 13 9.8% 42 14.2% 0.049
DVT 9 5.5% 7 5.3% 16 5.4% 0.922CNS 35 21.5% 20 15.0% 55 18.6% 0.157Vascular 4 2.5% 8 6.0% 12 4.1% 0.122Pulmonary 5 3.1% 0 0.0% 5 1.7% 0.042Arthritis 106 65.0% 81 60.9% 187 63.2% 0.464GI 74 45.4% 39 29.3% 113 38.2% 0.005
ulcerations 21 12.9% 15 11.3% 36 12.2% 0.674blood 12 7.4% 9 6.8% 21 7.1% 0.843
diarrhea 48 29.4% 20 15.0% 68 23.0% 0.003biopsy 5 3.1% 6 4.5% 11 3.7% 0.514
Thrombophlebitis 3 1.8% 3 2.3% 6 2.0% 0.801Headache 70 42.9% 50 37.6% 120 40.5% 0.351Epididymitis 2 1.2% 2 1.5% 4 1.4% 0.837HLA B51 (Done = 114) 19 11.7% 15 11.3% 34 11.5% 0.099Pathergy (Done = 130) 18 11.0% 17 12.8% 35 11.8% 0.773
Adjusted Critical Value p=0.005

266 US vs 93 JPN BS patients

Treatment
• Significantly more patients had been treated with azathioprine, methotrexate, and TNF inhibitors among US patients
• Significantly more patients in JPN received sulfasalazine, and • Differences were noted for colchicine, corticosteroids, or cyclosporine use
among cohorts.

BSAS
BSAS consists of 10 questions, each scored 0-10.
Patient reported measures
VAS for patient’s level of discomfort oral ulcers, genital ulcers, skin lesions or acne, and current disease activity.
The BSAS also categorizes the number of oral ulcers, genital ulcers, and acne lesions present, and records if there is GI involvement, vascular involvement, or eye involvement.

Table 1‐ Pearson correlations between the measures
BSAS BDCAF QoL
r p r p r p
BDCAF 0.597 <0.0001
QoL 0.489 <0.0001 0.388 0.0012
MD Global 0.276 0.019 0.299 0.014 0.507 <0.0001
76

MDHAQ in Behcet’s

MDHAQ in Behcet’s

Current studies
• Apremilast– OU, double blind, placebo controlled
• Xoma IL‐1– NIH
• Abatacept– OU, open label
• Tocilizumab– OU, double blind, placebo controlled
• Neurology NYU HJD and NIH– Functional imaging

80
Conclusions
• BS is not very rare.
• It has distinct features from “connective tissue” diseases
• Disease clusters
• In many patients it is a mild disease which can also go away by
itself.
• We can successfully manage a substantial majority of the
remaining patients.
• CNS disease and thrombophilia are still problems.
• We are doing considerably better now than did 20 years ago

Thank you
• Hasan Yazici, MD
• Maria Filopoulos• Thalia Gooden, DO• Pamela Sharaf• Monalyn De Los Reyes Labitigan, MD• Chelsey Forbess, MD• Nicole Moses, MD• Johannes Nowatzky, MD
• Hui Zhan• Ranit Shriky