be healthy - patient power
DESCRIPTION
monthly health supplement focusing on health issues for African AmericansTRANSCRIPT

By all accounts, Donna Matthews is a
“good” patient. As a diabetic,
she checks her blood sugar level four to fi ve times a day – and more if she does not feel
well. She writes the numbers down in
a log that she dutifully presents at each doctor’s
appointment. Talk about patient
empowerment. “I think I’m a little OCD (obsessive-compulsive
disorder) now,” she admits. But that “OCD” serves her well. She
can name each of her medications and the dosage. She asks questions; she writes things down. To say the least, Matthews is prepared
— and clear on specifi c problems. The reason for her obsessiveness is also
clear. “I don’t want to get any worse,” she said.The notion of patient empowerment
— that patients take an active role in their care — is a growing concept. It’s not that patients are taking over; they’re just taking part. They weigh treatment options, learn about their ill-nesses and make decisions about their care.
Research has shown that patients who interact with and have a good relationship with their providers not only receive better care but are happier with that care.
If only all of Dr. Mark Drews’ patients were as good as Matthews. As an internist at Whittier Street Health Center, he averages
about 70 patients a week, and maybe he has twenty minutes with each of one of them.
But a lot has to happen in those 20 minutes.
Especially considering that primary care physicians (PCPs) are increasingly being asked to do more with less time – and with fewer doctors. PCPs are becoming such a rare commodity that in 2009 the Mas-sachusetts Medical Society concluded that the shortage of doctors of internal medicine is “severe,” and that of family medicine is “critical.”
Complicating the problem is that only 60 percent of family practitioners and a scant 44 percent of internists are ac-cepting new patients, according to the society’s Physician Workforce Study.
What’s worse, on average, patients in this area have to wait 44 days for an appointment.
Although a 2009 report in the Archives of Internal Medicine found that visits with PCPs increased from an average of 18 min-utes to almost 21 minutes, one thing remains clear: there’s not much time behind those closed doors.
Time constraints pose a problem with
specialists as well.Dr. Eldrin Lewis, a cardiologist at
Brigham and Women’s Hospital, admits he spends more time in a visit compared to some. His visits also average 20 minutes but can range as long as 40 minutes for new or com-plex conditions.
Both Drews and Lewis agree that the time is better spent if patients come prepared.
“You wouldn’t think of visiting an accoun-tant and asking if you’ll get a tax refund if you have not provided the appropriate receipts,” Lewis said. “Why would you handle a doctor’s visit any differently?”
Thirty minutes had passed and Brenda Robertson had more questions than an-swers. She was trying to fi ll out her family tree — complete with medical histories — and she soon learned that the task was nearly impossible.
Many of her relatives were dead and their medical histories — to the extent they were written down — died along with them.
That didn’t deter Robertson. The infor-mation that she could collect was a good start — and changed her life.
Both of her parents died from strokes, but it was her father’s history that particu-larly stood out. He had two strokes, and the second one was fatal. He was 44 years old when he died.
Those genes were passed down. Already, Robertson’s older sister has had a stroke, as has one of her nephews. So far, Robertson has been spared, but she is not taking any chances.
“I want to prevent these illnesses in myself,” she said.
Knowing that strokes and diabetes run in her family, Robertson has changed her lifestyle
to control those risks. She has substituted water for sugared
beverages, reduced her portion sizes and eats more vegetables. And she exercises.
“I walk a lot now,” she said.
The value of fam-ily medical histories is enormous, largely because many illnesses are passed down from generation to generation. Many diseases, such as cancer, diabetes, high blood pressure and even mental illness, have a genetic link.
So important is the family history that the Surgeon General in 2004 launched a Family History Initiative to en-courage families to learn more about their inherited health risks. The Surgeon General designated
Thanksgiving — a holiday when families gather — as National Family History Day. The Department of Health and Human Services has created a web-based tool at https://familyhistory.hhs.gov that allows users to enter, print out
and save the information.The family history tree is an essential tool
for patient empowerment.In the 2004 HealthyStyle survey, the
Centers for Disease Control and Prevention found that 96 percent of the respondents believe that family history is important for their own health; yet a paltry 30 percent reported that they actively collected neces-sary information. One difference was noted, however. Those with a personal history of type 2 diabetes were more likely to have col-lected information from relatives.
The family medical history tree allows a doctor to assess risks for a certain disease, determine the type and time of screening tests and judge the risk of passing the conditions on to the next generation.
For instance, women who have a history of breast cancer — especially when diagnosed at a young age — may require initiation of mammograms before the age of 40 as well as a concomitant MRI.
Donna Matthews (right), discusses her log of blood glucose levels with Dr. Mark Drews (left), a primary care physician at Whittier Street Health Center.
The root of the problemMedical histories play an essential role in determining future lifestyles
Knowing a family medical history can sometimes reduce the risk of inherited diseases through timely screenings and lifestyle changes.
PHOTO BY TONY IRVING
BE Healthy™
Patient power, continued to page 4
Family history continued to page 4
VOL. 4 • NO. 7 © March 2010
Sponsored by Boston Public Health Commission
PATIENT POWERTeam
approach
results in
better care

The beginning of the end of the national recession may be in sight, but fi nancial experts say a full recovery is still a long way off. People should be cautious with their money and look for ways to reduce their spending. This includes health care costs. Stretching health care dollars is now more essential than ever.
“Until the economy bounces back, people will be looking for ways to cut costs wherever they can,” said Dr. John Fallon, Chief Physician Executive at Blue Cross Blue Shield of Massachusetts (BCBSMA). “But when it comes to our health, we have to be smart about the decisions we make, including how we select and use our health care plans.”
Whether you sign up for a health plan through work or on your own, being a smart consumer is key. Carefully evaluate all the options available to you to fi nd the best care for your money.
Compare available plans during open enrollment periods.
Carefully compare all available options during annual open enrollment periods (often in the fall); sticking with the same plan doesn’t always make sense. If you don’t anticipate needing to see the doctor fre-quently, it may be worthwhile to select a less expensive plan with higher co-pays or a higher deductible. Most health plans have formularies listing pre-approved drugs. Often, drugs are added (and sometimes dropped) annually. Remember to check formularies annually for medications you need. Staying informed — and keeping on top of selection deadlines — can save you headaches and cash.
Compare additional incentives. Many plans offer discounts for health club memberships, smoking cessa-tion, weight loss programs and preventive screenings. Discounts may even apply to accredited complementa-ry care providers you visit, such as a dietitian, chiro-practor, masseuse, or acupuncturist. Blue Cross Blue Shield of Massachusetts offers this through the Living Healthy Naturally Program.
Once you find the right plan, follow these tips to save on costs:
1. Investigate health savings accounts. If you’re under 65 and have a high-deductible plan, you can put a portion of pretax dollars into a Health Savings Account (HSA) to pay for eligible health expenses, thus lowering your tax bill. Unused HSA funds can roll over and accumulate year to year. Alternatively, a Flexible Spending Account (FSA) offered only through employers holds pretax dollars for eligible health or dependent expenses. FSA funds not spent by year-end are forfeited. If you already have an FSA, remember to submit 2009 claims for reimbursement by March 31, 2010.
2. Stay in network. Use doctors and specialists in your health plan’s network. Out-of-network care drives up your share of the health care bill. If you’re unsure if a provider is in your plan’s network, simply give your plan a call or check online.
3. Save on prescriptions. Always ask about generics, lower-cost brand name medications and over-the-coun-ter options. Generics, which can be as effective as brand name counterparts, come on the market frequently (and big chains like Kmart, Sam’s Club, Target, and Wal–Mart price hundreds of generics under $5 for a 30-day supply). Find out if lifestyle changes — more exercise, better diet, stress reduction — might lower dosages or erase need for some medication. Always talk to your doctor or pharmacist before making any medication changes.
4. Dial a help line. Find out if your plan has nurse help lines to advise you on whether you should see a doctor or can self-treat using simple remedies like fl uids, fever-relievers and rest. For example, members who have a plan under BCBSMA can call experienced nurses staffi ng the 24–hour Blue Care Line. Often a call can save an unnecessary trip to the hospital or doctor’s offi ce—and your co-pay. Ask your plan what resources may be available to you.
5. Participate in wellness programs. Hit the jackpot with healthy choices. Exercising, losing weight and quitting smoking dramatically lower your risks for asthma, diabetes, cancer and heart problems, signifi cantly improving your health while cutting your health care bills. Many health plans offer wellness program discounts, rebates and fabulous online tools like personalized weight loss or workout plans. Free and low-cost community programs may be available through the Boston Parks and Recreation Department, senior centers and community education centers.
Making every dollar count
The ABC’s of health insuranceHMO, PCP, PPO, POS — feel like you’re wading through alphabet soup? Read on for translations of common terms.
• Health maintenance organizations (HMO) require you to choose a primary care physician (PCP), who coordinates all of your care, including visits to specialists.
• Preferred provider organizations (PPO) let you make your own choices from a network of preferred providers (in some plans, you can pay a higher fee for out-of-network care) and may not require you to have a primary care physician.
• Point-of-service plans (POS) let you choose between receiving care from participating providers (you’ll be reimbursed more for this), or non-participating providers(you’ll be reimbursed less for this).
Some plans offer lower premiums (monthly pay-ments) in exchange for a higher yearly deductible (the amount you must pay personally before insurance provides any coverage). Some plans require co-pays, a set fee you pay for health care visits or medications. Others ask you to pay co-insurance, which means you’re responsible for a portion (20 percent, for example) of eligible expenses charged by a provider or the amount the insurer agrees to pay for specifi c services.
Many plans require preauthorization or precertifi ca-tion for certain services, such as surgery or visits to a specialist. Some pick up the tab on preventive care ser-vices, such as fl u shots, cholesterol tests, or colonoscopy. Most have formularies that list pre-approved, commonly prescribed drugs.
How to Pick a Plan Health plans are never one–size–fi ts–all.To choose wisely, evaluate your specifi c needs.
• Who needs coverage? Are you single or married, or do you have a domestic partner? Do you have children who need coverage?
• What are your health needs? Let’s say you’re healthy and rarely need to visit the doctor. You may benefi t from a plan that couples lower monthly premiums with a higher deduct-ible, the amount you must pay personally before insurance provides any coverage. If you have chronic illnesses requir-ing frequent care like diabetes, asthma, or heart disease, a no-deductible policy might be a better choice.
• Are your current doctors in the network? Call or check online for which health plans your doctor accepts.
• Do you pay a lot monthly for prescription drugs? A plan that has prescription drug coverage — or lets you opt out of it — may offer considerable cost savings. Some plans have tiers (groupings) of co–pays (set fees) for medications. Generic drugs are least expensive. Brand name drugs are grouped into increasingly expensive tiers. For example, a 30–day supply of tier–one generic high blood pressure pills may cost $10; tier-two brand name pills may cost $20; and tier-three brand name pills may cost $30.
PHOTO: NATIONAL CANCER INSTITUTE
BE Healthy • http://behealthy.baystatebanner.com2
1. Why is it so important to know exactly what medications you are taking and the dosage?
The doctor must know all the medications you are taking in or-der to prevent unwanted or harmful medication interactions. In addition, the provider can better evaluate if the medications are benefi cial or if a higher dose or different medication would be better.
2. Is the Internet a good source of medical information?The Internet provides good medical information on such
sites as WebMD and MedlinePlus. However, you have to be careful because not all Internet sites are reputable. Look to see if the authors are experts on the subject and that the information is current. Check with your doctor if you have questions.
3. What’s the value of keeping a health journal?A health journal — a complete record of your health — al-
lows you to present a complete and current medical history when visiting your doctor. The journal, which includes your ill-nesses, hospitalizations and medications, will expedite your visit and allow the physician more time to concentrate on other parts of the medical visit.
4. Can a patient safely assume that the doctor knows or remembers his or her medical history?
No. Physicians treat many patients and sometimes do not see them for months at a time. It is diffi cult for them to remem-ber all of their patients’ medical histories. Even with paper or electronic charts, a doctor can still lack certain information. It is always best to remind your physician of your medical history.
5. Is it necessary to mention herbal or over-the-counter (OTC) medications since they are non-prescription?
Yes. Herbal medicines, such as Saw Palmetto (for pros-tate) and OTC drugs can be quite powerful. There is a com-mon misconception that, because they are available without a doctor’s prescription, they are not really strong. However, many drugs now available OTC were prescription drugs at one time. Their ease of access has not necessarily reduced their potency. In addition, non-prescription drugs may counter the effect of a prescription drug, so it is important to mention all medications, whether or not they require a prescription.
6. If you have bad side effects from a drug prescribed by your doctor, should you stop taking them?
Not without your doctor’s consent. If you have bad side effects from a drug prescribed by your doctor, you should call your doctor’s offi ce as soon as possible and inform him or her of your symptoms. Some side effects will resolve over time as you continue the medication. There are other side effects, however, which are potentially life threatening. It is always best to speak to your doctor about what the best course of action should be.
7. Should you talk to your doctor about life changes, such as stress, divorce or depression?
Most defi nitely. Certain life changes can affect your overall health. For example, stress can worsen or trigger many problems such as heart disease, hypertension and obesity. The physician can evaluate you and refer you to get some help.
8. If the doctor’s offi ce does not call a patient regarding test results, is it safe to assume that the tests were negative?
You should never assume that everything is normal if you do not get a call from the doctor’s offi ce. It is always best to contact the offi ce yourself if you have not heard anything.
The information presented in BE HEALTHY is for educational purposes only, and is not intended to take the place of consultation with your private physician. We recommend that you take advantage of screenings appropriate to your age, sex, and risk factors and make timely visits to your primary care physician.
Michelle Johnson, M.D.InternistWhittier Street Health Center
Questions & Answers
Looking for reliable sources of health information? Here are a few...
Government Agencies
• National Cancer Institutewww.cancer.gov
• MedlinePlushttp://medlineplus.gov
• Centers for Disease Control and Preventionwww.cdc.gov
• U.S. Department of Health and Human Serviceswww.healthfi nder.gov
Non–profi t Organizations/HMOs
• American Cancer Societywww.cancer.org
• American Heart Associationwww.heart.org
• American Diabetes Associationwww.diabetes.org
• Blue Cross Blue Shield of Massachusettswww.ahealthyme.com
INHERITED RISKS
There are several diseases that run in families and are passed down from generation to generation. A family history does not guarantee an illness; it raises the odds. Examples of inherited diseases are:
• Prostate cancer• Ovarian and breast cancer• Colorectal and uterine cancer• Diabetes• Heart disease• Stroke• High blood pressure• High cholesterol
• Kidney disease• Depression and dementia• Alcoholism and other substance abuse• Miscarriage and stillbirth• Birth defects and infertility• Asthma• Alzheimer’s disease
1. What is the test for?
2. How many times have you done this [procedure]?
3. When will I get the results?
4. Why do I need this surgery?
5. Are there any alternatives to surgery?
6. What are the possible complications?
7. Which hospital is best for my needs?
8. How do you spell the name of that drug?
9. Are there any side effects?
10. Will this medicine interact with medicines that I’m already taking?
You won’t learn the answer if you don’t ask the question
Below is a list of questions you should always ask when the situation arises:
Source: Agency for Healthcare Research and Quality www.ahrq.gov/questionsaretheanswer
BE Healthy • http://behealthy.baystatebanner.com 3
Medicines cause a major concern. Doctors cannot prescribe a new drug without knowing what a person is already taking. “Less than one–third of patients will know what they take,” Lewis said. “Others will have just a general idea, but don’t know the name or dose of the drug. They assume that I know.”
Drews agrees.Trying to get the details from some patients
doesn’t always work. “The response — ‘The heart doctor gave me a new pill. It’s white.’ — is not much help,” Drews said. “ ‘Let me call my wife at home. She can read the label’ — is better. But that doesn’t tell the entire story.”
He offers a solution: “Put all your pills in a bag and bring them with you.”
That helps in more ways than one. Not only can he determine what you’re on, he can determine what you’re no longer on. People tend to keep medications they stopped taking — or they have three different doses of the same medication, according to Drews. “It helps to have the actual bottles,” he said.
He makes a larger point. “This is a national safety issue,” Drews said, referring to the thousands of accidental overdoses and allergic reactions to all types of drugs.
Lewis agreed that he prefers to see the medications directly and not rely solely on the medical record. “It could be wrong,” he noted.
He knows his time is limited. In those 20 minutes Lewis must hear and inter-pret a patient’s problems, ask questions, perform a physical examination and develop strategies for treatment. “You don’t want to lose ten minutes trying to fi gure out medications,” he remarked.
Both doctors mentioned pet peeves or irritations that impede good care: not taking medicine but thinking that you’re going to get better; not telling the doctor when you don’t understand; being too embarrassed to raise an issue; showing up late for appoint-ments; relying on a family member’s advice instead of the doctor’s.
For his part, Drews does his homework to make the most of his time and he expects the same from his patients. During the visit, he expects participation and good interaction from his patients. He encourages questions. And he expects honesty. Hiding information and pro-viding just part of a picture can be detrimental. He welcomes a family member or friend at the visit to help fi ll in the gaps.
For the patient’s part, it takes three steps to achieve the ultimate visit. The fi rst is preparation. Don’t go to the doctor empty-handed. Take your drugs with you — includ-
ing over-the-counter and herbal drugs, and vitamins; write a list of your symptoms and complaints; and prioritize the three or four most troublesome.
The American Academy of Family Physi-cians recommends developing a health journal that includes a history of illnesses and injuries, hospitalizations, surgeries, allergies and drugs.
The second step is the actual visit. Discuss your complaints; update the doctor of any changes since the last visit, including life changes, such as divorce; answer questions honestly; ask questions if you do not under-stand and write down information.
The third step is follow-up. Call if you experience problems after the visit, such as side effects from medications, deterioration of your symptoms, or failure to receive the results of tests.
Lewis emphasizes the need for patients to take charge. “Most treatment occurs in between doctor visits,” he said. “You have to understand what you’ve been told and then do it.”
Be a part of the team. Ask why you’re tak-ing the drug. If you are on three different medications for apparently the same diagnosis, ask why. When you have your blood pres-sure taken, write down the results. “That’s a patient’s job,” he said.
He fi nds that some people are a little bit more involved in their care, but not as much as he’d like to see. People of African American descent, he noted, tend to not ask ques-tions as often.
One thing he stresses. If you and your doctor have a relationship that works,
that goes a long way. “You don’t have to be friends, but you should feel secure that he or she has your best interest,” he said. “If not, fi nd another doctor.”
Apparently, Matthews’ fastidiousness and her close working relationship with Drews have paid off. She sees the improvements.
“My A1C — a test that refl ects the aver-age blood sugar level for the past two to three months — used to be in the 9’s,” she said. “Now it’s in the 6’s.”
It is recommended that the A1C for dia-betics not exceed 6.9.
Matthews is living proof of several stud-ies that suggest that African Americans can improve blood glucose levels when in strong partnership with their doctor.
She relies on her doctor for expertise and support but relies more heavily on herself to follow through with “her” health plan.
She says that Whittier Street Health Center is good at calling her to inform her of test results. If they didn’t, she explained, she would anyway.
“I’d be too scared not to,” she says.
Patient power continued from page 1
“The biggest concerns are cancer and heart disease, especially in the young,” said Dr. Mark Drews, an internist at Whittier Street Health Center. “If you’re 40 and your brother died of cancer at 40, you should know which cancer. If it was prostate cancer, you need to start screening now. If it was lung cancer and he was a heavy smoker, there is less concern.”
An ideal family history includes at least three generations. Primary relatives — parents, children and siblings — are most important. But grandparents, aunts, uncles and cousins should not be overlooked.
What should trigger attention is a disease that occurs at an earlier age than expected, a disease in more than one close relative, a disease that is atypical for that gender — for instance breast cancer in a male — and certain combinations of diseases, such as breast and
ovarian cancer. It takes a bit of detective work to com-
plete the history. Ask questions, review death certifi cates and available medical records. Determine age of diagnosis and age and cause of death. List ethnic backgrounds as well.
The history is a work in progress and should be corrected and edited as new infor-mation comes to light. Most important is to pay attention to what’s been revealed.
Lifestyle changes — healthy diet, exercise, and smoking cessation — will not change your genes, but can reduce the risk of the diseases. The fact that your family has a certain history is not a guarantee that you will likewise be affl icted.
Originally from the West Indies, Rob-ertson readily admits she is not through with her history. “I’m going home this year,” she said. “I can get more information from my family then.”
• Include at least three generations if possible• Note the relative’s age at diagnosis and the age and cause of death• Watch for a disease that occurs in more than one relative• Look for diseases that occur at an earlier age than expected• View death certifi cates, family bibles and family medical histories• Get input from as many relatives as you can• Continue to update and correct the tree as new information becomes available• Share the information with your doctor and relatives
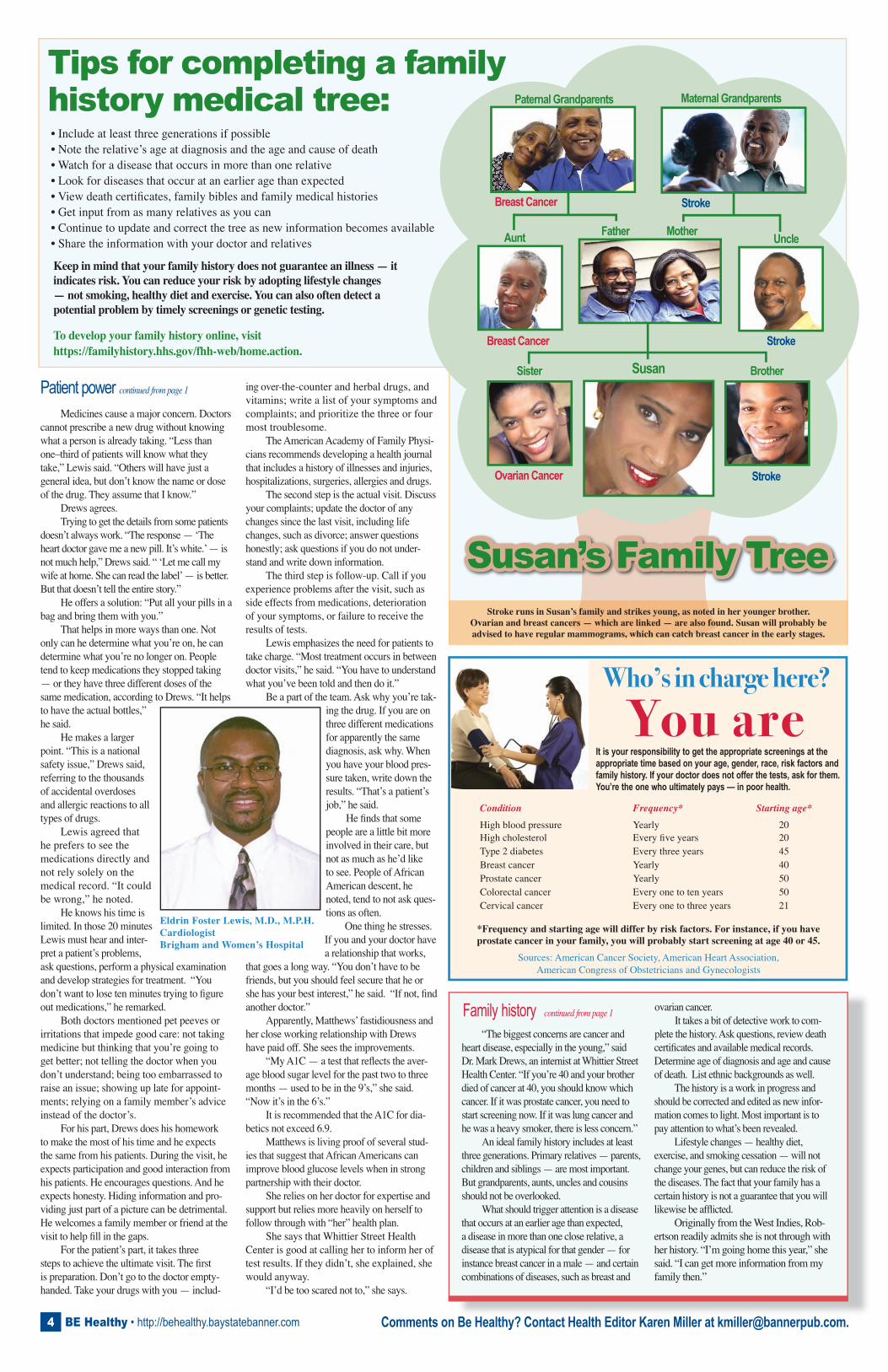
Paternal Grandparents Maternal Grandparents
Father Mother
Susan
Aunt
Sister
Ovarian Cancer
Breast Cancer
Breast Cancer
Brother
Stroke
Stroke
Uncle
Stroke
Tips for completing a family history medical tree:
Keep in mind that your family history does not guarantee an illness — it indicates risk. You can reduce your risk by adopting lifestyle changes — not smoking, healthy diet and exercise. You can also often detect a potential problem by timely screenings or genetic testing.
To develop your family history online, visithttps://familyhistory.hhs.gov/fhh-web/home.action.
Susan’s Family TreeStroke runs in Susan’s family and strikes young, as noted in her younger brother.
Ovarian and breast cancers — which are linked — are also found. Susan will probably be advised to have regular mammograms, which can catch breast cancer in the early stages.
Eldrin Foster Lewis, M.D., M.P.H.CardiologistBrigham and Women’s Hospital
Comments on Be Healthy? Contact Health Editor Karen Miller at [email protected].
Condition Frequency* Starting age*
High blood pressure Yearly 20High cholesterol Every fi ve years 20Type 2 diabetes Every three years 45Breast cancer Yearly 40Prostate cancer Yearly 50Colorectal cancer Every one to ten years 50Cervical cancer Every one to three years 21
Family history continued from page 1
Who’s in charge here?You are
It is your responsibility to get the appropriate screenings at the appropriate time based on your age, gender, race, risk factors and family history. If your doctor does not offer the tests, ask for them. You’re the one who ultimately pays — in poor health.
*Frequency and starting age will differ by risk factors. For instance, if you haveprostate cancer in your family, you will probably start screening at age 40 or 45.
Sources: American Cancer Society, American Heart Association,American Congress of Obstetricians and Gynecologists
BE Healthy • http://behealthy.baystatebanner.com4