basic mechanisms of pain and non- pain symptoms of fibromyalgia syndrome: impact on therapeutics...
TRANSCRIPT

Basic Mechanisms of Pain and Non-Pain Symptoms of Fibromyalgia
Syndrome: Impact on Therapeutics
Leslie J. Crofford, M.D.University of Michigan
FDA Arthritis Drugs Advisory Committee Meeting June 23, 2003

Developing Effective Treatments for Fibromyalgia Syndrome (FMS)
1. Can FMS be clinically recognized and diagnosed using current ACR criteria?• ACR criteria identify patients with predictable symptom profile• FMS patients identified by ACR criteria may contain subsets
(clinically or mechanistically defined)
2. What are the critical symptom domains in these patients that must improve for an intervention to be an effective treatment for FMS?
3. What mechanism(s) underlie FMS that may allow us to predict the types of treatments that may be effective?
4. How best can we measure improvement in response to treatment?

Fibromyalgia Symptom Domains
• Pain– Widespread MSK– Regional MSK– Visceral
• Required
• Non-Pain– Fatigue– Sleep disturbance– Cognitive dysfunction– Depression/anxiety
• Not required• Almost universally
present
Attribution of Symptom Domains to Specific Mechanisms
• Pain– Widespread clinical pain
• No mechanism implied
– ACR tender points • Tender points measure a domain that incorporates
both allodynia and non-pain domains (distress)1
– Is the pain of FMS “real”?• Psychophysical testing• Evoked potentials• fMRI
1Wolfe. Ann Rheum Dis 1997; 56:258.

Pain in FMS
• Stimulus detection normal
• Altered noxious threshold (multimodality)
• Central representation of pain confirms veracity of subjective pain complaints
• Pain cannot be explained by tissue damage– Pain generators may be common
• Implicates central factors in FMS pain

Spinal Central Sensitization orActivity-dependent Plasticity
• Neuronal plasticity in the spinal cord modifies performance of nociceptive pathways– Exaggerated or prolonged response to noxious inputs
(hyperalgesia)– Enabling normally innocuous inputs to activate nociceptive
pathways (allodynia)– Transcription independent and dependent mechanisms
• Mediators– EAA, NMDA receptors– SP and other neuropeptides, GPCR– Kinases (e.g., PKC, many others)
• Phosphorylate ion channels and receptors resulting in neuronal hyperexcitability
Descending Modulation
• Bi-directional (inhibitory and facilitatory) descending control– Serotonergic and noradrenergic pathways– Injury-induced hyperalgesia dampened by descending
pathways– Cortical and subcortical structures stimulate
facilitatory pathways– Input integrated at PAG/RVM
• Vagal afferents• HPA axis and ANS• Cortical (e.g. ACC, DLPC)
– RVM dynamic plasticity mediated by NMDA receptors

Central Modulation of PainCerebral Cortex-Goal-directed behaviors
-Attention/distraction-Expectancy-Interaction with limbic system
Sub-cortical- Stress-induced analgesia
Midbrain & Brain Stem-Integrates signals from brain and spinal cord
-Site of opiate action-Relay chemical signals to spinal cord
-Norepinephrine and serotonin

Treatment Implications for Concept of Central Pain
• Treatments usually used for “normal” musculoskeletal pain do not work well in most FMS patients
• Treatments must address the problems:– Altered pain processing in the spinal cord– Altered descending inhibition of pain signals

Attribution of Non-Pain Symptoms to Specific Mechanisms
• Non-pain symptoms form a “distress” cluster often associated with multifocal chronic pain1
– Fatigue exceptionally difficult to attribute– Sleep disturbance
• No specific alteration described, but overlap with other conditions that share symptoms2, 3
– Cognitive dysfunction• Evidence that cognitive complaints correlate with fMRI
differences
– Depression, anxiety• Marked increase in lifetime prevalence, associated with
health-care seeking
1Nisenbaum et al. Am J Epidemiol 1998; 148:72; 2Raines & Penzien. J Psychosom Res 2003; 54:77; 3Roizenblatt et al Arthritis Rheum 2001; 44:222.

What Does “Fatigue” Mean?• General
– Decreased energy, need to rest, sleepiness or unrefreshing sleep, struggle to overcome inactivity
• Physical– Weakness, limb heaviness, post-exertional
malaise
• Emotional– Decreased motivation/interest
• Mental (cognitive)– Diminished concentration/memory
• Functional– Difficulty completing daily tasks

Possible Causes of Fatigue in FMS
• Sleep disturbance
• Depression/anxiety
• Pain
• Medications
• Deconditioning/muscle metabolism
• Neurally-mediated hypotension
• Central mechanisms, e.g. cytokines
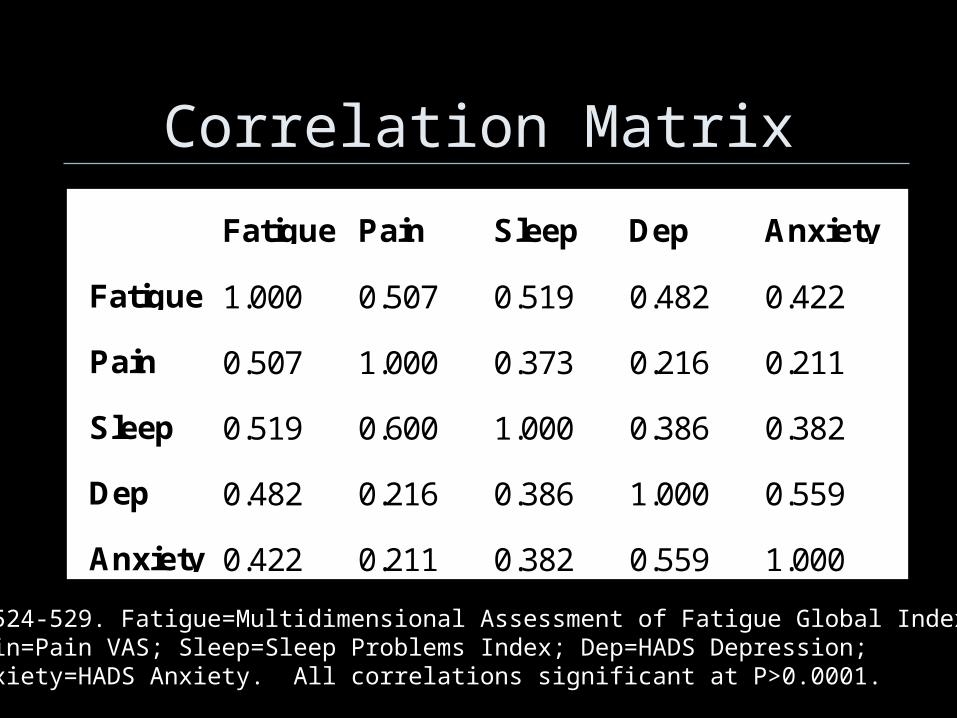
Correlation Matrix
Fatigue Pain Sleep Dep Anxiety
Fatigue 1.000 0.507 0.519 0.482 0.422
Pain 0.507 1.000 0.373 0.216 0.211
Sleep 0.519 0.600 1.000 0.386 0.382
Dep 0.482 0.216 0.386 1.000 0.559
Anxiety 0.422 0.211 0.382 0.559 1.000
N=524-529. Fatigue=Multidimensional Assessment of Fatigue Global Index;Pain=Pain VAS; Sleep=Sleep Problems Index; Dep=HADS Depression; Anxiety=HADS Anxiety. All correlations significant at P>0.0001.

Sleep Disturbances in FMS
• Alpha-delta sleep– First objective alteration described in FMS1
– Non-specific, not universal
• Reduced slow-wave (stage 3-4) sleep– Non-specific, not universal– No spectral analyses reported to examine
delta power in FMS
• “Psychophysiologic” insomnia– Altered sensitivity to environmental stimuli
1Moldofsky et al. Psychosom Med 1975; 37:341
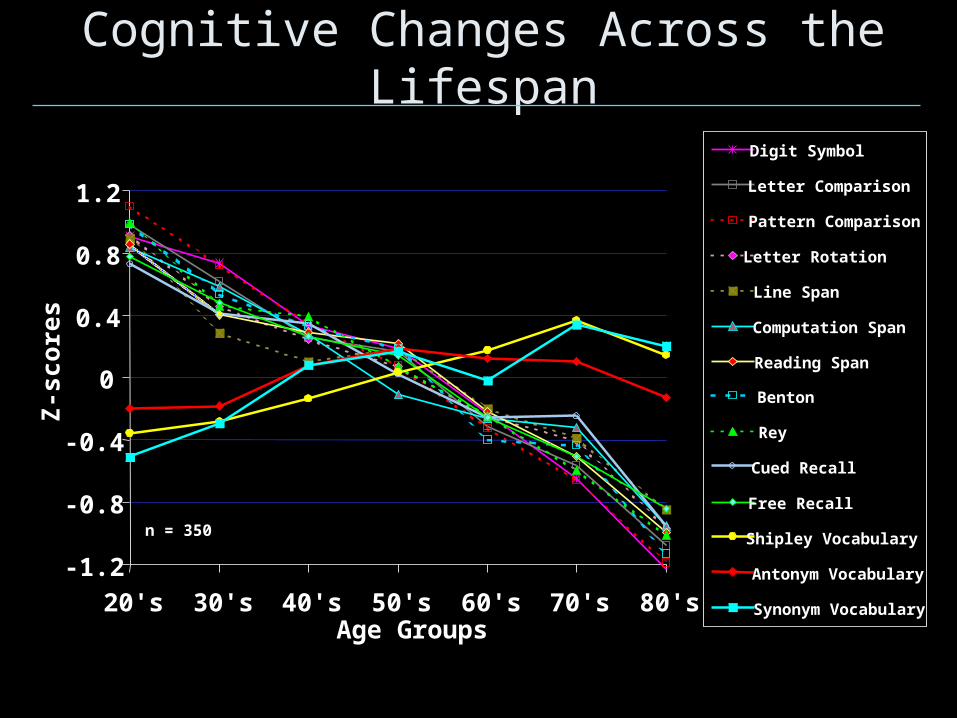
Cognitive Changes Across the Lifespan
-1.2
-0.8
-0.4
0
0.4
0.8
1.2
20's 30's 40's 50's 60's 70's 80's
Digit Symbol
Letter Comparison
Pattern Comparison
Letter Rotation
Line Span
Computation Span
Reading Span
Benton
Rey
Cued Recall
Free Recall
Shipley Vocabulary
Antonym Vocabulary
Synonym Vocabulary
Age Groups
Z-s
core
s
n = 350

Information Processing Speed: FM are as fast as Age-matched controls
80
90
100
110
120
130
140
150
FM Older Controls Age-MatchedControls
Num
ber
Cor
rect
p < .80FM vs AMC

Working Memory:FM perform like older adults
101214161820222426283032
FM Older Controls Age-MatchedControls
Num
ber
Cor
rect
Tri
als
p < .039FM vs AMC

Long-Term MemoryFree Recall: FM Perform like older adults
15
17
19
21
23
25
27
29
31
FM Older Controls Age-MatchedControls
Num
ber
of W
ords
Rec
alle
d
p < .025FM vs AMC
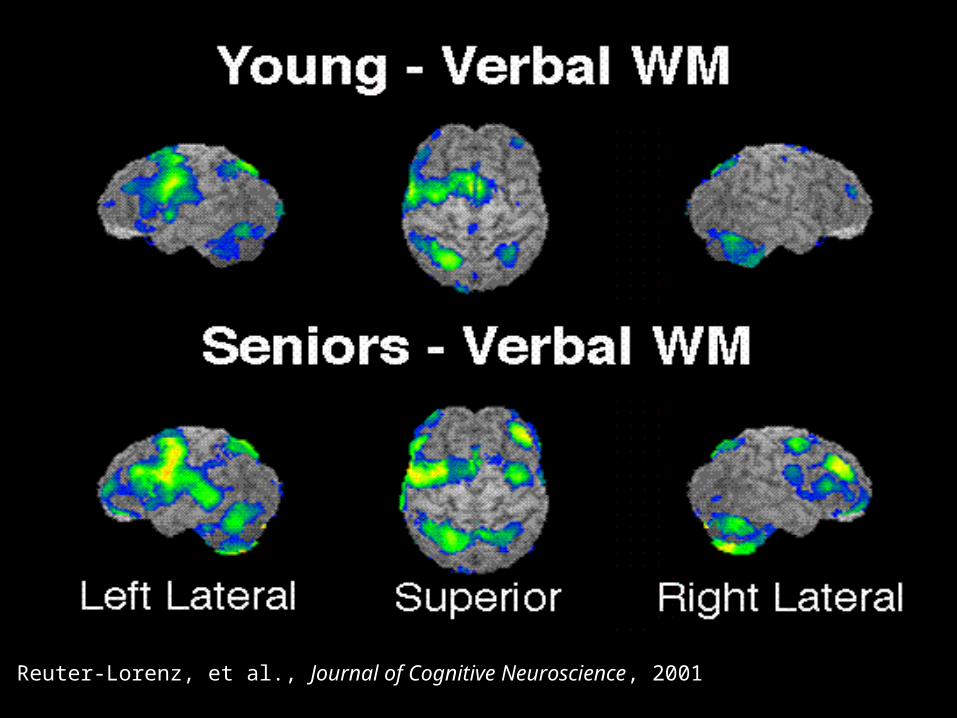
Reuter-Lorenz, et al., Journal of Cognitive Neuroscience, 2001
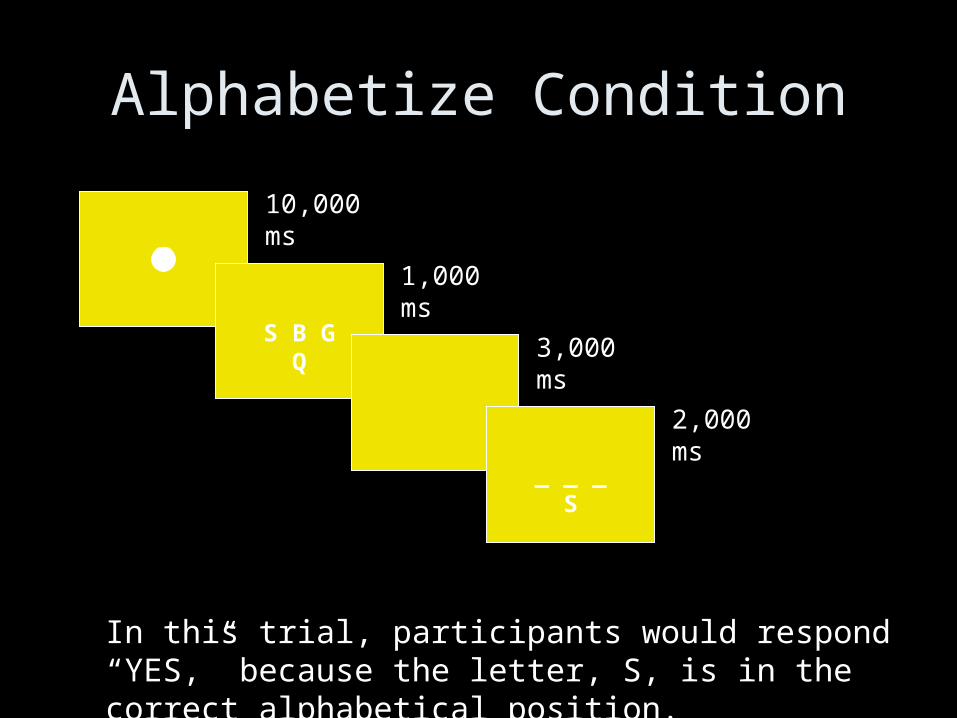
Alphabetize Condition
S B G Q
_ _ _ S
10,000 ms
1,000 ms
3,000 ms
2,000 ms
In this trial, participants would respond “YES,” because the letter, S, is in the correct alphabetical position.

FM Patients: Alphabetizing - Maintenance
•FM’s show bilateral activation in middle frontal gyrus while alphabetizing (BA 6)
•Increased activation in the right superior parietal lobe (BA 7, 39)
•An area specialized for the processing of spatial location of objects; processing of meaning; storage of items during working memory tasks
•Midline medial frontal gyrus (BA 8) - Associated with Frontal Eye Fields; Facilitates eye movements and visual reflexes (e.g., pupil constriction/dilation)
•Overall, FM’s show more activation when alphabetizing

FM Patients: Alphabetizing - Maintenance
An additional region bordering the right inferior frontal gyrus and the precentral gyrus (involving BA 6, 9, and 44) was found in FMs.
•Right BA 44 is the homologue to Broca’s area in the left hemisphere
•BA 9 is thought to be involved in reasoning

Controls: Alphabetizing - Maintenance
The normal controls did not show more activation in any part of the brain. Only a small, nonsignificant region was identified at the posterior junction of the occipital and parietal lobes.
Control subjects did not have to work harder to alphabetize compared to maintenance.

Depression and Anxiety in Fibromyalgia
• Neither necessary nor sufficient for diagnosis of FM
• Higher point prevalence than in the general population
• Lifetime prevalence in a tertiary care population1
– Depression 68%– Any anxiety disorder 35%
• Health-care seeking associated with psychiatric comorbidity
1Epstein et al, Psychosomatics, 1999; 2Bradley et al. Arthritis Rheum 1996; 39:436


“Stress is life and life is stress”- Hans Selye
• Stressors are forces that disturb homeostasis– Acute physical, chronic physical, psychological,
anticipatory
• Counterbalanced by adaptive forces– Central adaptation, peripheral adaptation
• Hypothalamic-pituitary-adrenal (HPA) axis and autonomic nervous system (ANS) are critical components of the coordinated physiologic response to stress
• Physical, behavioral, and psychological symptoms linked to HPA axis and ANS abnormalities

What is a “Healthy” HPA Axis?
• Circadian variation with high cortisol in am and low cortisol in pm
• High responsiveness to physiologic and stressful stimuli
• Sensitivity to dexamethasone suppression
• “Responsive and resilient”

Low-Dose oCRH/Dex Suppression Protocol
Day 1 Day 2 Day 3 Day 4 Day 5 Day 6 Day 7
AM PM AM PM AM PM AM PM AM PM AM PM
Saliva Collections
Dex 0.25 mg Dex 0.50 mg
GCRC for Low-Dose(0.3 ug/kg) oCRH

Mean ACTH ± SEM Following Low Dose oCRH (0.3 ug/kg) Stimulation in FM (n=14) and Controls (n=12)
0
5
10
15
20
25
30
35
40
-15 -8 0 5 15 30 60 90 120
Time from oCRH administration (min)
AC
TH
(p
mo
l/mL
)
FM Control
p = 0.047

Mean Salivary Cortisol Concentration ± SEM Pre & Post Graded Low-dose Dexamethasone
Suppression in Controls & FM
0
1
2
3
4
5
6
7
8
AM PM AM PM AM PM AM PM AM PM AM PM
DAY 2 DAY 3 DAY 4 DAY 5 DAY 6 DAY 7
Co
rtis
ol (
mg
/dL
)
FM Control
p = 0.22
p < 0.01
p = 0.03
p = 0.01
Dex 0.25 mg Dex 0.50 mg
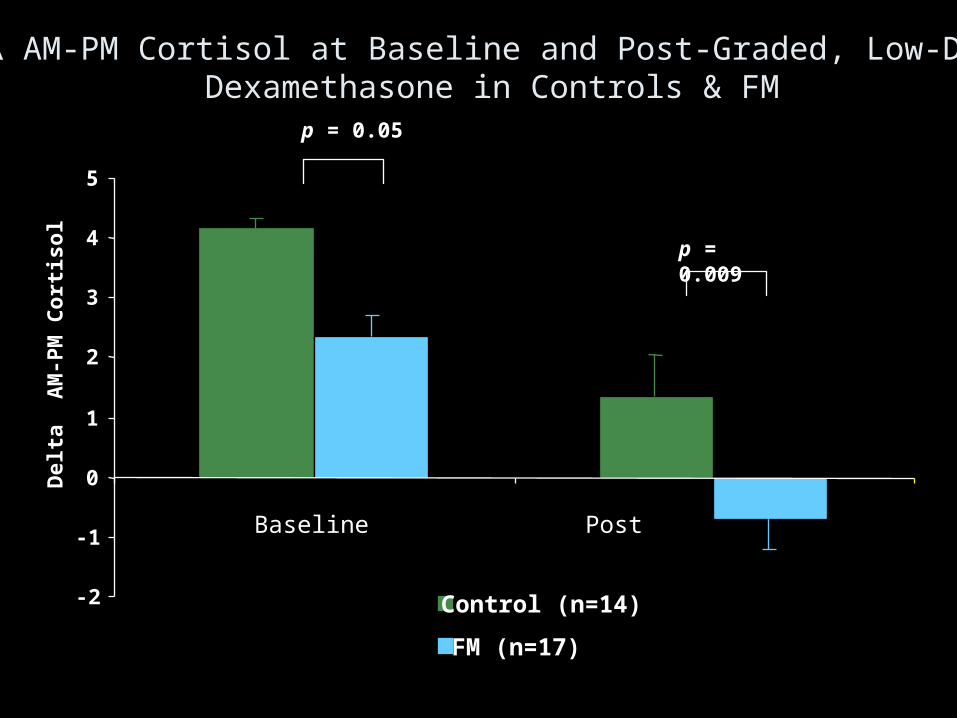
AM-PM Cortisol at Baseline and Post-Graded, Low-DoseDexamethasone in Controls & FM
-2
-1
0
1
2
3
4
5
Del
ta A
M-P
M C
ort
iso
l
Control (n=14)
FM (n=17)
p = 0.05
p = 0.009
Baseline Post

Autonomic Nervous System
• Number of studies also suggesting altered sympathetic and sympathoadrenal dynamic variability1
– Reduced heart rate variability2
– Altered stimulus-induced blood flow3
– Altered stimulus-induced ANS4
1 Petzky & Clauw Curr Rheum Rep 2000; 2:116; 2Martinez-Lavin A&R 1998; 41:1966;3Granges & Littlejohn J Rheumtol 1993;20:344; 4Adler et al. Am J Med 1999;106:534

Altered Dynamic Function of Stress-Response Systems
• Hypo- and hyper-responsiveness may cause similar symptoms– Concept of allostat
• Function may differ under different physical and psychosocial stress– Concept of allostatic load
• Strong drive to maintain overall hormone levels• Current therapies influence expression of key
components of system– TCA and SSRI influence expression of MR/GR in
CNS– Exercise modulates “set point” of allostat
Implications for Drug Therapy• FMS is a clinically recognizable syndrome
– Does not exclude the likelihood of subsets of patients with different underlying mechanisms
• Clinically important improvements in pain are likely to occur in response to treatments addressing central mechanisms– Reduced pain is likely to improve HR-QOL
• Non-pain symptoms are also important to HR-QOL, health-care seeking/utilization– Non-pain symptoms often cluster with central pain
and neurobiological mechanisms may be shared– Clinically significant improvement in non-pain
symptoms likely to result in global improvement