basic life support - grand bank / fortune …gbfambulance.webs.com/bls - master - 2012...
TRANSCRIPT

BLS Patient Care Protocols
FIELD GUIDE
Provincial Medical Oversight Program
Provincial Medical Oversight
2012 Edition Newfoundland & Labrador
BASIC LIFE SUPPORT
Patient Care Protocols

1
ACKNOWLEDGEMENT
OFFICE OF THE PROVINCIAL MEDICAL OVERSIGHT PROGRAM
Paramedicine & Medical Transport - Eastern Health
St. Clare's Mercy Hospital RM SM343
154 LeMarchant Road St. John's NL, Canada, A1C 5B8
709 – 777 – 5209
709 – 777 – 5940 FAX www.pmtnl.ca
© All Rights Reserved: No part of this publication may be reproduced or transmitted in any form or by any means, electronic or mechanical, including
photocopying, recording, or any information storage and retrieval system, without permission in writing from the Provincial Medical Oversight Program.
If found, please return to address above.
OLMC 1-877-709-3535
This OLMC line is only to be used for medical advice when actively engaged in patient care

2
AUTHORIZATION FOR PROTOCOLS
OVERVIEW These protocols were developed for the following reasons:
1. To provide the EMS provider with a quick field reference 2. As written standards of care which are consistent throughout the Province
of Newfoundland & Labrador. Users of these protocols are to have knowledge of more detailed and basic patient management principles found in EMS textbooks and literature appropriate to the EMS provider’s level of training and licensure.
3. All users must have strict adherence to these protocols.
POLICY Practitioners will work within their scope of practice specifically guided by procedures and protocols as authorized by the Provincial Medical Director or the Assistant Provincial Medical Director.
SCOPE Emergency Medical Responders and Primary Care Paramedics actively registered with the Provincial Medical Oversight Program (PMO) and who are on duty with a public ambulance service that is recognized by the Department of Health and Community Services. These protocols can be used by Advanced Care Paramedics or Critical Care Paramedics if they are working for a BLS service in the role of a BLS provider.
PURPOSE The Procedures and Protocols will be based on current best practice and evidence. These protocols are issued by the Provincial Medical Director and the Assistant Provincial Medical Director and will be supported by Regional Medical Control Physicians. These protocols govern the practice of EMS Providers who are registered with the Provincial Medical Oversight Program by the authority of Department of Health and Community Services.
REVIEW These protocols will be subject to annual review. New or revised protocols will be issued as applicable changes occur. If there are errors or omissions, please contact PMO. _________________________ _____________________________ Dr. Doug Baggs MD, FRCP(EM) Dr. Rose Mengual MD,FRCP(EM) Provincial Medical Director Assistant Provincial Medical Director Paramedicine & Medical Transport Paramedicine & Medical Transport

3
TABLE OF CONTENTS
Standards of Care 5
Airway Emergencies
Difficult Airway 7
Pediatric Respiratory Distress with Inspiratory Stridor 8
Breathing Emergencies
Adult Respiratory Distress with Bronchospasm 9
Pediatric Respiratory Distress with Bronchospasm 10
Adult Anaphylaxis 11
Pediatric Anaphylaxis 12
Circulation Emergencies
Ischemic Chest Pain 13
Symptomatic Arrhythmias 14
Pulmonary Edema 15
Cardiogenic Shock 16
Acute Stroke 17
Cardiac Arrest
Cardiac Arrest 19
Post Arrest Care 20
Traumatic Cardiac Arrest 21
Death in the Field
Obvious Death
22
Do Not Resuscitate (DNR) 23
Termination of Resuscitation (TOR) 24
Determination of Death 25
Trauma Emergencies
Burns 26
Spinal Assessment 27
Trauma Alert 29

4
Medical Emergencies
Sepsis 30
Shock Not Yet Diagnosed 31
Symptomatic Hypoglycemia 32
Treat and Release Protocol for Hypoglycemia 34
Symptomatic Hyperglycemia 35
Convulsive Seizures 36
Toxins 37
Obstetrics / Gynecology
Child Birth 38
Complications of Delivery 39
Neonatal Assessment and Resuscitation 40
Reference Material
12 Lead ECG Acquisition 42
Fluid Therapy 44
PCP/ACP Intercept 45
Non-EMS Medical Personnel On-Scene 46
Refusal of Care / Refusal of Transport 47
Potential Communicable/Quarantinable Disease 48
Mass Casualty Incident (MCI) Management 49
MCI Triage - Adult 50
MCI Triage - Pediatric 51
Communications 52
Definitions surrounding DNR, TOR, Determination of Death 53
Pediatric Reference 54
Rule of Nines 55
Glasgow Coma Scale (Adult and Pediatric) 56
Oxygen Tank Duration Charts 57
IV Rate Conversion Chart 60
Metric Conversion Chart 61
Acronyms / Abbreviations 62
Formulary 63

5
GENERAL STANDARDS OF CARE
Scene assessment (Safety issues, MOI, # of Pts, need for resources)
Application of PPE including universal precautions
Assess LOC, Airway, Breathing, Circulation
C-spine immobilization
Airway management
Administer oxygen
Establish effective ventilation
Obtain detailed history
Perform physical exam
Vital signs
Determine blood glucose level
Pulse oximetry (before and after oxygen administration if possible)
Cardiac monitor
12 lead ECG
Establish vascular access
Spinal immobilization
Perform CPR as per Heart & Stroke Guidelines
Consider differential diagnosis
Consider PCP or ACP intercept for EMR/EMR crew
Consider ACP intercept for PCP/EMR or PCP/PCP crew
Standards of trauma care to follow guidelines of International Trauma Life Support (ITLS)
Frequent reassessment, particularly after intervention
Notify receiving hospital
General standards of care should be performed if indicated and as necessary with all patients based on the registered level scope of practice for the clinician as defined by the
National Occupational Competency Profiles and PMO Policies for Paramedicine.
DOCUMENTATION
Ensure complete and thorough documentation of patient care activities.
Patient care reports should contain enough detail so that it is easily apparent why specific treatments were offered or decisions were made. Careful documentation is especially important when documenting cases including but not limited to:
Traumatic Cardiac Arrest
Obvious Death
Do-Not-Resuscitate (DNR)
Termination of Resuscitation (TOR)
Determination of Death
Spinal Assessment
Refusal of Care
If a patient care report is reviewed, your documentation should present a logical train of thought that is easily followed through the appropriate protocol or algorithm.

6
GENERAL STANDARDS OF CARE Cont’d To use these protocols as they were intended, it is necessary to know the philosophy, treatment principles, and definitions, which guided the physicians and other EMS providers who drafted these protocols:
1. Assessment and treatment should very RARELY delay transport! IV’s should be started en route except in those situations where treatment at the scene of an out-of-hospital emergency is in the patient’s best interest such as hypoglycemia, or cardiac arrest, and cardiac arrhythmia when full ACLS care is available. Delays in transport should be discussed with OLMC.
2. Inability to establish voice contact with OLMC. There are rare situations where the patient is unstable and delay in treatment threatens the patient’s life or limb. If, after good-faith attempts, the practitioner cannot contact OLMC, then the practitioner is authorized to use any appropriate treatment protocols as standing orders. Continue attempts to contact OLMC and document these attempts on the patient care record.
3. Treatments/drugs should be given in the order specified. PMO recognizes that often treatments are delivered simultaneously and more than one protocol may be used. OLMC may request treatments/drugs out of sequence for medical reasons.
EMS providers may contact OLMC in any situation in which advice is needed, not only in situations as directed by these written protocols.
Medical Authority
Medical authority is determined by the individual’s level of training. Personnel with the highest level of training shall have medical authority during ambulance responses.
Personnel with the same level of training shall have medical authority determined by the amount of experience at that training level. The person with the most experience performing at that training level shall be granted medical authority.
Personnel who have the same training level and same experience at that training level shall determine the course of treatment for the patient by mutual agreement.
If persons with the same training level and experience can not mutually agree on the course of treatment they shall contact the on line medical control physician for direction.
Failing the above, if there is a disagreement on scene, regardless of training or experience, practitioners must contact OLMC for direction.

7
DIFFICULT AIRWAY (with/without obstruction)
EMR & PCP
1. Manage airway as needed (airway maneuver and/or suction and/or adjunct).
Follow current Heart & Stroke guidelines for respiratory arrest procedure.
Utilize 100% O2 with assisted ventilation (PPV) if necessary.
Use the foreign body obstructed airway procedure as necessary. 2. Request ACP intercept if available
PCP ONLY
3. Continuous cardiac and SpO2 monitoring 4. IV during transport 5. Maintain adequate tidal volumes and ventilatory rates by monitoring chest
rise and SpO2
Difficult Bag Mask Ventilation
Predictors of Difficult Bag Mask Ventilation BOOTS
Beard Obese Older Toothless Snore/Stridor
Approach to Difficult BMV
1) Reposition airway – exaggerated head tilt or exaggerated jaw thrust. Consider adding pillow under head. If obese, position using the ear to sternum (ramping) technique (see picture below)
2) Insert oral and/or nasal airway 3) Two-person bag-mask ventilation 4) Consider alternative mask size 5) Consider foreign body 6) If cricoid pressure being applied, ease up on or release
cricoid pressure
Ramping for obese patients
Figure A shows obese patient positioned without ramping. Figure B shows the patient ramped so that her sternum and ear line up. This position should improve ventilation.

8
PEDIATRIC RESPIRATORY DISTRESS WITH INSPIRATORY STRIDOR (Laryngotracheitis/Croup)
EMR & PCP 1. Keep child as comfortable as possible, agitation may worsen condition 2. Humidified O2, with upright posture
Blow by O2 acceptable if child refuses mask 3. If needed, assist ventilations with PPV using 100% O2 4. EMR’s should request PCP or ACP intercept if available
PCP ONLY
5. Continuous cardiac and SpO2 monitoring 6. Consider nebulized epinephrine 1:1000 if indications present as per
dosing guidelines below:
Age Dose
Less than 1 year and less than 5 kg 0.5 mg (0.5mL) in 2 mL 0.9% NaCl
Less than 1 year and equal to or greater than 5 kg
2.5 mg (2.5 mL)
Greater than or equal to 1 year 5 mg (5 mL)
Indications for epinephrine:
Severe respiratory distress
AND
Current history of upper respiratory infection with a “barking cough”, stridor at rest, and suprasternal retractions with severe respiratory distress
Contact OLMC for consideration of:
Second dose of epinephrine 1:1000

9
ADULT RESPIRATORY DISTRESS WITH BRONCHOSPASM (COPD, Emphysema, Chronic Bronchitis, Asthma)
EMR & PCP 1. Manage airway as needed 2. O2 via NRB during acute distress
If needed, assist ventilations with PPV 3. EMR’s should request PCP or ACP intercept if available
PCP ONLY 4. IV access during transport 5. Continuous cardiac and SpO2 monitoring 6. Administer:
* each puff must be followed by at least 4 breaths
7. If confirmed COPD (Emphysema or Chronic Bronchitis) only and respiratory status has improved to patient’s baseline after treatment:
Consider replacing NRB with Venturi Mask or nasal cannula to maintain SpO2 90-92% if prolonged transport
If there is continued respiratory distress continue O2 via NRB
NOTES:
Patients should be treated with MDI and aerochamber unless it is deemed ineffective or patient cannot tolerate
Salbutamol or ipratropium bromide may be administered singularly if the patient has a hypersensitivity to one of the medications.
Salbutamol 4-8 puffs via MDI with aerochamber* every 5 minutes as needed to maximum of 3 administrations
AND Ipratropium Bromide 4-8 puffs via MDI with aerochamber* every 5 minutes as needed to maximum of 3 administrations
OR
Salbutamol 5 mg nebulized with O2 every 5 minutes as needed to maximum of 3 doses
AND Ipratropium Bromide 500 mcg nebulized with O2 every 5 minutes as needed to maximum of 3 doses
In cases such as status asthmaticus, where bronchospasm is not alleviated with salbutamol + ipratropium bromide, the PCP should contact OLMC to administer further salbutamol or to administer epinephrine 1:1000 0.3 mg IM

10
PEDIATRIC RESPIRATORY DISTRESS WITH BRONCHOSPASM EMR & PCP
1. Manage airway, assist ventilations as necessary 2. O2 as appropriate 3. EMR’s should request PCP or ACP intercept if available
PCP ONLY 4. Continuous cardiac and SpO2 monitoring 5. Administer salbutamol based on dosing below
Age MDI (100 mcg/puff) with
aerochamber*
Nebulized (dilute with 0.9% NaCl to a total
volume of 2.5 ml)
Less than 5 years 5 puffs 2.5 mg
Greater than or equal to 5 years
10 puffs 5 mg
Repeat as needed to maximum of 3 doses (3 x 5 puffs, or 3 x 2.5 mg nebulized if less than 5 years or 3 x 10 puffs or 3 x 5 mg nebulized if greater than 5 years)
* each puff must be followed by at least 4 breaths
6. Consider ipratropium bromide administration with 2nd and 3rd dose of salbutamol as per dosing guidelines below
Age MDI (20 mcg/puff) with
aerochamber*
Nebulized (co-administer with salbutamol and
dilute with 0.9% NaCl to a total volume of 2.5 ml)
All ages 3 puffs 500 mcg
Repeat as needed 3 puffs via MDI with aerochamber every 5 minutes to a maximum of 3 doses (3 x 3 puffs, or 3 x 500 mcg nebulized)
* each puff must be followed by at least 4 breaths
7. If patient condition deteriorates, PCP’s should request ACP intercept (if available).
NOTES:
Patients should be treated with MDI and aerochamber unless it is deemed ineffective or patient cannot tolerate
Salbutamol or ipratropium bromide may be administered singularly if the patient has a hypersensitivity to one of the medications.
In cases such as status asthmaticus, where bronchospasm is not alleviated with salbutamol and/or ipratropium bromide, the PCP should contact OLMC to administer further salbutamol or to administer epinephrine 1:1000 0.01 mg/kg IM to a maximum of 0.3 mg

11
ADULT ANAPHYLAXIS
EMR & PCP
1. Manage airway, assist ventilations as necessary 2. O2 as appropriate 3. EMR’s should request PCP or ACP intercept if available 4. Assess patient for findings of anaphylaxis (see below) 5. If patient has their own anaphylaxis kit (EpiPen), EMR’s may assist
administration if patient meets anaphylaxis criteria.
PCP ONLY
6. Continuous cardiac and SpO2 monitoring 7. If findings of anaphylaxis present (see table below), administer
epinephrine 1:1000 0.3 mg IM.
Epinephrine 1:1000 0.3 mg IM may be repeated once if symptoms are not improving after 5 minutes
8. If wheezing present, administer salbutamol
4-8 puffs via MDI with aerochamber every 5 minutes as needed to a maximum of 3 administrations
OR
5 mg nebulized with O2 every 5 minutes to a maximum of 3 doses. 9. IV during transport 10. If shock present, perform fluid challenge (see Fluid Therapy Protocol,
page 44)
NOTE: Patients should be treated with MDI and aerochamber unless it is deemed ineffective or patient cannot tolerate
Findings of Anaphylaxis Acute onset (minutes to hours) of two or more of the following after exposure to likely allergen:
Skin (hives, itching, flushing)
Oropharyngeal edema (lips, tongue, uvula)
Respiratory compromise (dyspnea, wheeze, stridor, hypoxemia)
Gastrointestinal symptoms (crampy abdominal pain, vomiting, diarrhea)
Reduced blood pressure or associated symptoms (hypotonia, collapse, syncope) OR
Hypotension alone after exposure to a known allergen for that patient

12
PEDIATRIC ANAPHYLAXIS
EMR & PCP
1. Manage airway, assist ventilations as necessary 2. O2 as appropriate 3. EMR’s should request PCP or ACP intercept if available 4. Assess patient for findings of anaphylaxis (see below) 5. If patient has their own anaphylaxis kit (EpiPen), EMR’s may assist
administration if patient meets anaphylaxis criteria
PCP ONLY
6. Continuous cardiac and SpO2 monitoring 7. If findings of anaphylaxis present (see table below), administer
epinephrine 1:1000 0.01 mg/kg IM to a maximum of 0.3 mg.
Epinephrine 1:1000 may be repeated once if symptoms are not improving after 5 minutes
8. If wheezing present, administer salbutamol as per dosing guidelines below:
Age MDI (100 mcg/puff) with
aerochamber
Nebulized (dilute with 0.9% NaCl to a total
volume of 2.5 ml)
Less than 5 years 5 puffs 2.5 mg
Greater than or equal to 5 years
10 puffs 5 mg
Repeat as needed to maximum of 3 doses
9. IV during transport 10. If shock present, perform fluid challenge (see Fluid Therapy Protocol,
page 44)
NOTE: Patients should be treated with MDI and aerochamber unless it is deemed ineffective or patient cannot tolerate
Findings of Anaphylaxis Acute onset (minutes to hours) of two or more of the following after exposure to likely allergen:
Skin (hives, itching, flushing)
Oropharyngeal edema (lips, tongue, uvula)
Respiratory compromise (dyspnea, wheeze, stridor, hypoxemia)
Gastrointestinal symptoms (crampy abdominal pain, vomiting, diarrhea)
Reduced blood pressure or associated symptoms (hypotonia, collapse, syncope) OR
Hypotension alone after exposure to a known allergen for that patient

13
ISCHEMIC CHEST PAIN (Adult) (If SBP is less than or equal to 90 mmHg see Cardiogenic Shock Protocol, page 16)
EMR & PCP
1. Manage airway 2. O2 as appropriate 3. ASA 160 – 162 mg PO (chewed) 4. EMR’s should request PCP or ACP intercept if available
PCP ONLY
5. IV during transport 6. Continuous cardiac and SpO2 monitoring 7. Obtain 12 lead ECG pre and post intervention 8. Nitroglycerin 0.4 mg SL every 5 minutes to a maximum 6 sprays until
chest pain is relieved or SBP falls below 100 mmHg
If no effect from nitroglycerin after three sprays, discontinue use. 9. Request ACP intercept if available
Contact OLMC for repeat administration of nitroglycerin (beyond 6 sprays)
Inferior wall Myocardial Infarction
Nitroglycerin is NOT to be administered if an inferior wall Myocardial Infarction is suspected or confirmed by 12 Lead, and/or patients SBP has been less than 100 mmHg at any time during current event.
Fluid therapy should not be used to increase SBP to administer nitroglycerin.
STEMI Alert
1. Notify receiving facility of patient with possible STEMI if the printout identifies a possible *****Acute MI Suspected***** or left bundle branch block in patient experiencing chest pain.
2. Transmit 12 Lead ECG prior to facility arrival when possible. 3. ASA 160 – 162 mg PO if not already administered 4. Establish second IV during transport 5. Complete Thrombolytic Checklist for STEMI
Serial 12 Leads
12 lead ECG must be completed and repeated as outlined below:
1. On scene (prior to treatment) 2. In ambulance just prior to transport 3. Every 15 minutes during transport 4. Anytime patient condition or ECG changes

14
SYMPTOMATIC ARRHYTHMIAS (Adult) (Suspected cardiac origin, non-traumatic)
EMR & PCP
1. Manage airway as appropriate 2. O2 as appropriate 3. Treat symptoms based on standards of care 4. Observe & Transport 5. Request for ACP intercept if available
PCP ONLY
6. Continuous cardiac and SpO2 monitoring 7. 12 lead ECG 8. IV during transport
Symptoms associated with arrhythmias:
Chest pain Diaphoresis Dyspnea Decreased LOC Syncope Orthopnea
Hypotension Signs of Shock Pulmonary congestion Tachypnea Palpitations Nausea and Vomiting
Bradycardia Atrial Fibrillation with heart rate greater than 120 Wide Complex Tachycardia Atrial Flutter Narrow Complex Tachycardia

15
PULMONARY EDEMA (Adult) If initial systolic SBP less than or equal to 90 mmHg see Cardiogenic Shock Protocol (page 16)
EMR & PCP 1. Manage airway 2. O2 100% via non-rebreather mask. Assist ventilations (PPV) if needed 3. Assess for shock. If SBP greater than 100 mmHg, place in sitting position 4. EMR’s should request PCP or ACP intercept if available
PCP ONLY 5. Continuous cardiac and SpO2 monitoring 6. 12 Lead ECG 7. IV during transport 8. Nitroglycerin 0.4 mg SL every 5 minutes to a maximum 6 sprays until
symptoms are relieved or SBP falls below 100 mmHg 9. Request ACP intercept if available
Contact OLMC for repeat administration of nitroglycerin
(beyond six sprays)
Signs & Symptoms of Pulmonary Edema Severe Respiratory Distress
Orthopnea
Crackles
Diaphoresis
Nocturnal Dyspnea
Jugular Vein Distention
Cough that may contain foamy, blood tinged sputum
Peripherial Edema

16
CARDIOGENIC SHOCK
EMR & PCP
1. Manage Airway 2. O2 as appropriate (Assist ventilations with PPV if needed) 3. EMR’s should request PCP or ACP intercept if available
PCP ONLY
4. Continuous cardiac and SpO2 monitoring 5. 12 Lead ECG 6. IV during transport 7. Request ACP intercept if available 8. Treat symptoms based on standards of care
Criteria for Cardiogenic Shock
1) Hypotension
AND
2) Chest pain OR pulmonary edema OR cardiac dysrhythmia OR known
cardiomyopathy
AND
3) No history of trauma or infection or dehydration
Signs & Symptoms of Cardiogenic Shock
Altered level of consciousness
Cool skin
Pale or mottled skin
Diaphoresis
Hypotension
Pulmonary edema (left heart failure)
Sinus tachycardia or other dysrhythmia
Decreased urine output
For OPTION of Fluid challenge, contact OLMC with full description of history and clinical findings including:
vital signs
lung sounds
cardiac rhythm
pedal edema assessment
Carefully observe for signs of fluid overload. Auscultate chest for crackles every 250 mL. If crackles present, stop bolus

17
ACUTE STROKE EMR & PCP
1. Manage airway 2. O2 as appropriate 3. Establish and document Last Seen Normal (LSN) time
PCP ONLY
4. Continuous cardiac, SpO2, and BP monitoring 5. 12 Lead ECG 6. Measure blood glucose 7. Determine if patient is candidate for direct transport to a Stroke Centre
using Paramedic Prompt Card (page 18) 8. IV during transport
If no Stroke Centre identified within your area, transport to closest ER
If at any time during your patient contact there is airway compromise or patient’s condition becomes unstable, transport to the closest Emergency Department.

18
ACUTE STROKE Cont’d (PCP ONLY)
Paramedic Prompt Card for Acute Stroke Protocol
Indications for Direct Transport to a Stroke Centre
Direct transport to a designated Stroke Centre will be considered for patients who meet both of the following requirements:
1) Present with new onset of at least one of the following symptoms suggestive of the onset of an acute stroke:
Unilateral arm and/or leg weakness or drift
Slurred speech or inappropriate words or unable to speak
Unilateral facial droop
AND
2) Can be transported to arrive at a designated Stroke Centre within 3.5 hours of a clearly determined time of symptoms onset or the time the patient was “Last Seen Normal” (in usual state of health).
Contraindications for Direct Transport to a Stroke Centre
Any of the following conditions exclude a patient from being transported directly to a Stroke Centre when there is a closer hospital available:
Uncorrected Airway, Breathing, or Circulatory Problem
GCS less than 10
Blood Sugar less than 3 mmol/L
Seizure at onset of symptoms or observed by paramedics
Terminally ill or palliative care
Pregnancy
Symptoms of stroke completely resolved prior to paramedic arrival or assessment*
No Stroke Centre identified within your area
Any history of:
Previous brain hemorrhage
Brain tumor, arteriovenous malformation (AVM), or brain aneurysm
Stroke or brain surgery within last 3 months
*Patients whose symptoms improve significantly or resolve during transport will continue to be transported to a Designated Stroke Centre If there is uncertainty whether the patient is a candidate for Direct Transport to a
Stroke Center, contact OLMC without delay

19
CARDIAC ARREST
EMR & PCP
1. Manage Airway 2. O2 100%. Ventilate as required with PPV 3. Confirm Vital Signs Absent (VSA) 4. Request highest level intercept if available 5. Treat cardiac arrest as per guidelines listed below
PCP ONLY
6. Continuous cardiac and SpO2 monitoring 7. Consider treatable causes such as Hypoxia, Hypovolemia, Drug Overdose,
Hypothermia, Hypoglycemia
If VSA is confirmed, and DNR (page 23) or Obvious Death (page 22) protocols not applicable:
Initiate compression immediately: C-A-B Sequence
Begin CPR - 5 cycles of 30 compressions:2 breaths. (2 rescuer CPR for pediatrics 15 compressions:2 breaths) with BVM and 100% O2 and proceed directly to AED. Minimize interruptions in CPR. Allow chest to fully recoil during compressions. Rotate rescuers every 2 minutes if possible.
Attach AED and analyze for shockable rhythm o If shock advised, give one shock and resume 5 cycles CPR immediately o If no shock advised, resume 5 cycles CPR immediately
Analyze rhythm o If shock advised, give one shock and resume 5 cycles CPR immediately o If no shock advised, resume 5 cycles CPR immediately
Analyze rhythm o If shock advised, give one shock and resume 5 cycles CPR immediately o If no shock advised, resume 5 cycles CPR immediately
After third rhythm analysis, ascertain if patient meets Termination of Resuscitation (PCP ONLY) protocol (page 24). If TOR not met, transport patient. DO NOT withhold CPR
Analyze patient every 10 minutes thereafter unless there has been three consecutive “no shock advised” then no further analysis required. Continue CPR.
Continue with above steps until arrival to hospital or ACP intercept
If patient has a return to spontaneous pulse see Post Arrest Care Protocol (page 20).
If re-arrest occurs during transport, resume Cardiac Arrest Protocol.
Pediatric patients less than or equal to 8 years of age require pediatric pads.
Hypothermic patients are to be resuscitated as per protocol above. Cardiac Arrest Protocol will be continued until active re-warming has returned core temperature to normal or there has been a ROSC.

20
POST ARREST CARE
EMR & PCP
1. Manage Airway 2. O2 100%, Ventilate as required 3. If AED was used, leave pads in place 4. Request highest level intercept if available
PCP ONLY
5. Continuous cardiac (not via defib pads) and SpO2 monitoring 6. 12 lead ECG 7. IV during transport 8. Consider treatable causes (Hypoxia, Hypovolemia, Drug Overdose,
Hypothermia, Hypoglycemia)
Be sure to leave a copy of the code summary and PCR with the receiving facility

21
TRAUMA CARDIAC ARREST
EMR & PCP
When a patient is found to be Vital Signs Absent (VSA) and has sustained trauma, the EMR/PCP must identify the category:
If no obvious external signs of significant trauma or if unsure of mechanism of injury, consider medical cardiac arrest and treat according to appropriate
medical Cardiac Arrest Protocol (page 19)
Proceed with the Determination of Death Protocol (page 25) if no resuscitative
efforts are ongoing.
Blunt Trauma Confirm cardiac arrest by absence of spontaneous respiration and palpable pulse in a patient with obvious external signs of significant blunt trauma consistent with the Trauma Alert Activation Criteria in the Trauma Alert Protocol (page 29). If criteria met: No resuscitative effort is to be provided.
Penetrating Trauma Confirm cardiac arrest by absence of spontaneous respiration and palpable pulse in a patient with obvious external signs of penetrating trauma. Initiate management and CPR as per BLS resuscitation standards and attach AED:
Unshockable Rhythm: If unshockable + absent pupillary response + no spontaneous movement AND Nearest hospital is greater than 20 minutes away - terminate resuscitation.
If unshockable AND nearest hospital is less than 20 minutes away - continue resuscitation and initiate rapid transport (do not delay for intervention on scene)
Shockable Rhythm: If shockable – continue resuscitation and initiate rapid transport
Limit to ONLY ONE SHOCK ON SCENE unless patient entrapped or other unforeseen circumstance

22
OBVIOUS DEATH
The EMR or PCP will NOT start resuscitation of a patient of any age that is suffering from cardiac arrest (not breathing and no palpable pulse) if any of the following signs of obvious death are present:
1. Rigor mortis 2. Dependant lividity 3. Decapitation 4. Transection of the torso 5. Decomposition 6. Confirmed submersion greater than 60 minutes 7. Obvious destruction of brain, heart, or lungs that is incompatible with life 8. Other catastrophic injury that is incompatible with life
Proceed with the Determination of Death Protocol (page 25) when appropriate.

23
DO NOT RESUSUSCITATE (DNR)
This DNR Protocol CANNOT be implemented by an EMR or PCP in situations related to:
Trauma (see Traumatic Cardiac Arrest Protocol, page 21)
Suicide attempt
Sudden reversible events such as, choking, asphyxia, anaphylaxis, submersion less than 60 minutes, drowning, poisoning, overdose, hypothermia, and toxicity.
The EMR or PCP will NOT start (or if already started will terminate) resuscitation of a patient of any age that is suffering from cardiac arrest (not breathing and no palpable pulse) in either of the following circumstances.
1. A Valid Do Not Resuscitate Order* or Advance Health Care Directive* is presented AND a reasonable effort has been made to verify the identity of the patient named on the document.
2. A legally recognized Substitute Health Care Decision Maker* (SHCDM) is present and states that the patient expressed a desire not to be resuscitated in this type of circumstance OR presents reasons why the patient should not be resuscitated while maintaining the patients best interest.
- AND - The EMR or PCP must not have any concerns about the appropriateness of withholding resuscitation based on:
A. Doubts about the patients best interest B. The validity of the DNR order or Advance Health Care Directive C. The identity of the person making the request as a SHCDM D. The patients family that are present being unable to reach an agreement
about withholding resuscitation Note: *See Reference Section (page 53)
If the above is met, proceed with the Determination of Death Protocol (page 25)
If a request to DNR is made prior to the patient suffering a complete cardiac arrest – provide supportive care (oxygen, airway support, and comfort measures) and contact OLMC with transport to hospital as appropriate.
If the EMR or PCP has any concerns – full resuscitative efforts as per protocol will be started and contact made with OLMC if necessary with transport to hospital as appropriate.

24
TERMINATION OF RESUSCITATION (PCP ONLY)
This TOR Protocol CANNOT be implemented by the PCP in situations related to:
1) Pediatrics (Age less than 18 years) 2) Pregnancy 3) Hypothermia 4) Electrocution including lightning strike 5) Traumatic cardiac arrest (see Traumatic Cardiac Arrest protocol, page 21) 6) Poisoning or drug overdose 7) Sudden reversible event (anaphylaxis, choking, drowning with submersion
less than 60 minutes, asphyxia)
In these cases resuscitation and transport must proceed as per usual cardiac arrest protocols.
If the PCP has any concerns – full resuscitative efforts as per protocol will be started and contact made with OLMC if necessary with transport to hospital as appropriate.
Note: *See Reference Section (page 53)
Termination of resuscitation is to be applied when resuscitation of cardiac arrest has been initiated and prior to transport decision. A PCP will terminate resuscitative efforts of a patient that is suffering from a cardiac arrest (not breathing and no palpable pulse) if ALL of the following criteria are met:
1) Cardiac arrest unwitnessed by EMS provider or medical first responder 2) No Return of Spontaneous Circulation (ROSC) after 3 full rounds of CPR and rhythm
analyses at any point during resuscitation 3) No shock(s) advised or delivered by EMS provider or medical first responder
If the above is met, proceed with the Determination of Death Protocol (page 25)

25
DETERMINATION OF DEATH
This Protocol is for implementation by the EMR or PCP AFTER the completion of the TOR Protocol (page 24), Trauma Arrest Protocol (page 21), or the DNR Protocol (page 23), and in certain situations, in whole or in part, after the Obvious Death Protocol (page 22).
NOTE: *See Reference Section (Page 53)
Determine death by assessment for AND Documentation of: 1. No palpable carotid pulse (assess for 60 seconds) 2. No spontaneous respiratory effort (assess for 60 seconds) 3. Non-reactive pupils
If the death meets the criteria of a *Reportable Death:
Do not disturb the scene – limit access only to essential responders
Leave ALL disposable medical equipment and supplies used in the resuscitation in place – do not remove from the scene
Leave IV’s, defibrillation pads, and airway adjuncts in place
Leave the deceased in position – do NOT cover the body
Exit the scene of the death immediately using the same pathway as was used to enter
Do not permit anyone entrance into the scene
Notify police
If death was an *Expected Death:
Notify family physician, if unavailable contact OLMC, or the police.
Post-Death Care: 1. Comfort of the bereaved
a. Inform simply and directly with warmth and compassion b. Listen and empathize c. Assist locating support – relative, friend, clergy, victim support group
2. If an expected death allow the bereaved to see the body if they wish; a. Prepare the deceased – clean-up medical supplies, cover with blanket, place
pillow under head, close eyes, wipe body fluids from the face, etc. b. Prepare the bereaved for what they will see, and answer any questions c. Do not rush the bereaved
Remain on scene until appropriate supports arrive for the bereaved, AND / OR: 1. Family physician, coroner, or the police arrive and assume control of the deceased. 2. If requested to respond to another life-threatening time-dependant emergency call.
Transport of the deceased shall be completed by: 1. A licensed funeral director
OR 2. An ambulance, if in a public place whereby the funeral director will be extensively
delayed (1 hour), as directed by police or OLMC

26
BURNS
EMR & PCP
1. Manage Airway 2. O2 as appropriate 3. Stop the burning process –
Remove involved clothing
Brush off powdered chemicals and copious irrigation of any other chemical exposure
Remove all items including jewelry that have the potential to become constrictive to the neck, extremities or digits
4. Warm ambient temperature to avoid hypothermia 5. Estimate % Total Body Surface Area (TBSA) affected using Rule of Nines
(Page 55)
Less than 5%TBSA
Cover with saline soaked or moist burn dressing.
5% - 20% TBSA
Cover with clean, dry sheet or commercial dressing.
Greater than 20% TBSA
Cover with clean, dry sheet or commercial dressing.
IV fluid administration as per Parkland Formula.
PCP ONLY
6. IV during transport (avoid placing IV in burned skin if possible) 7. Cardiac monitor (avoid placing leads on burned skin) and SpO2 8. Administer fluid based on Parkland Formula if burns greater than 20% BSA 9. Request ACP intercept if available
The Parkland Formula Fluid for first 24 hours (mL) = 4 X Patient's weight in kg X %TBSA
The first half of this amount is delivered in the first 8 hours, and the remaining half is delivered in the remaining 16 hours.
Carefully observe for signs of fluid overload. Auscultate chest for crackles every 250ml. If crackles present, stop bolus
Caution
Hypothermia – efforts must be made to prevent heat loss.

27
SPINE ASSESSMENT (PCP ONLY)
This clinical decision tool was developed to detect c-spine injuries among patients who are alert and stable but at risk for neck injury due to trauma.
Practitioner judgment, in favor of immobilization, should always override the result of the clinical decision tool in situations of uncertainty over interpretation of the tool or perceived risk to the patient. In any situation of uncertainty, practitioner must default towards immobilization of the patient.
Prior to applying the decision tool you must determine if patient is eligible for application of the tool by evaluating Inclusion and Exclusion Criteria.
1. Does patient meet ALL inclusion criteria?
INCLUSION CRITERIA
Age greater than 16
Alert (GCS = 15, converses spontaneously, FULLY oriented and follows commands)
Cooperative (Willingly follows commands and is not agitated)
Stable (SBP greater than or equal to 90 mmHg, respiratory rate 10-24 per minute on arrival)
YES – evaluate for exclusion criteria NO – can’t use decision tool, MUST immobilize
2. Does patient have ANY exclusion criteria?
YES – can’t use decision tool, MUST immobilize NO – APPLY THE DECISION TOOL ON NEXT PAGE
EXCLUSION CRITERIA
Age greater than or equal to 65 years
Numbness or tingling or paralysis
Any high risk mechanism of injury
Fall from greater than 1 m or 5 stairs
MVC greater than 100 km/h , and/or Roll-over, and/or Ejection from vehicle
Recreational vehicle crash
Pedestrian struck by vehicle
Axial load injury
Bicycle crash
Penetrating neck trauma
Known vertebral disease (ankylosing spondylitis, rheumatoid arthritis, spinal stenosis, previous c-spine surgery)
Pregnancy
Alcohol or drug ingestion
Greater than 8 hours since injury
If patient meets ALL Inclusion Criteria AND has NONE of the Exclusion Criteria then proceed with application of the decision tool to determine if immobilization is necessary
28
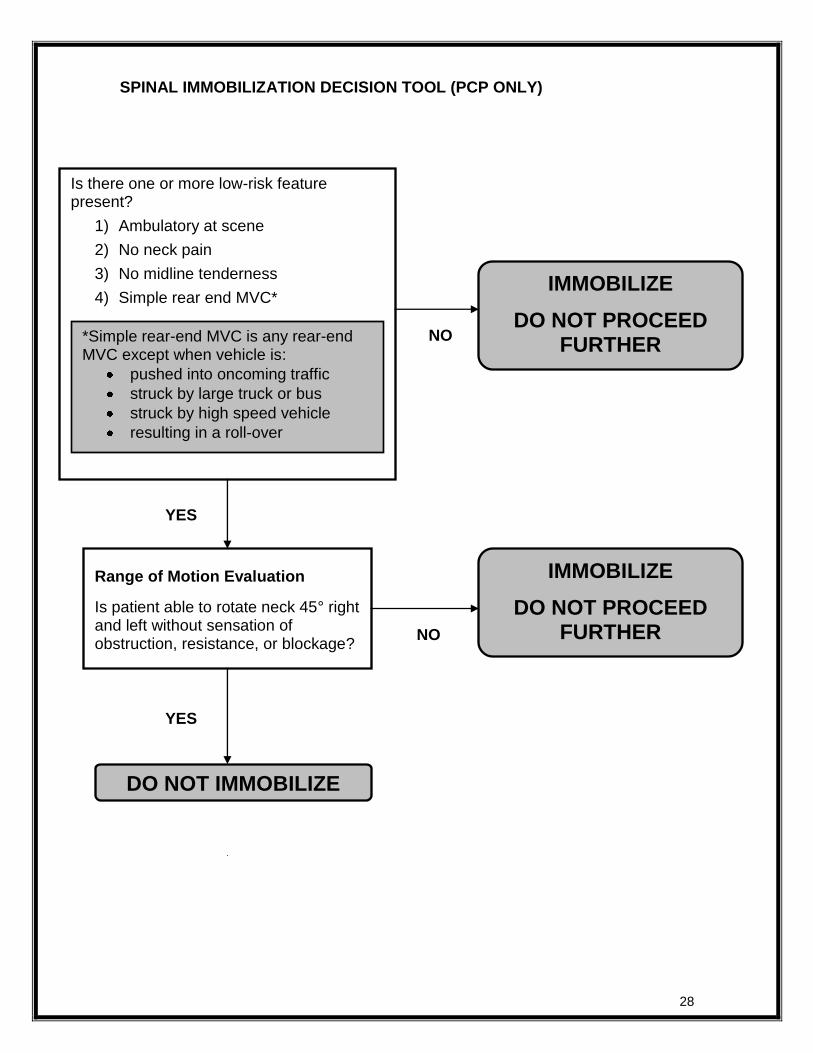
SPINAL IMMOBILIZATION DECISION TOOL (PCP ONLY)
Is there one or more low-risk feature present?
1) Ambulatory at scene
2) No neck pain
3) No midline tenderness
4) Simple rear end MVC*
DO NOT IMMOBILIZE
Range of Motion Evaluation
Is patient able to rotate neck 45° right and left without sensation of obstruction, resistance, or blockage?
IMMOBILIZE
DO NOT PROCEED FURTHER
YES
YES
NO
*Simple rear-end MVC is any rear-end MVC except when vehicle is:
pushed into oncoming traffic
struck by large truck or bus
struck by high speed vehicle
resulting in a roll-over
IMMOBILIZE
DO NOT PROCEED FURTHER
NO
29
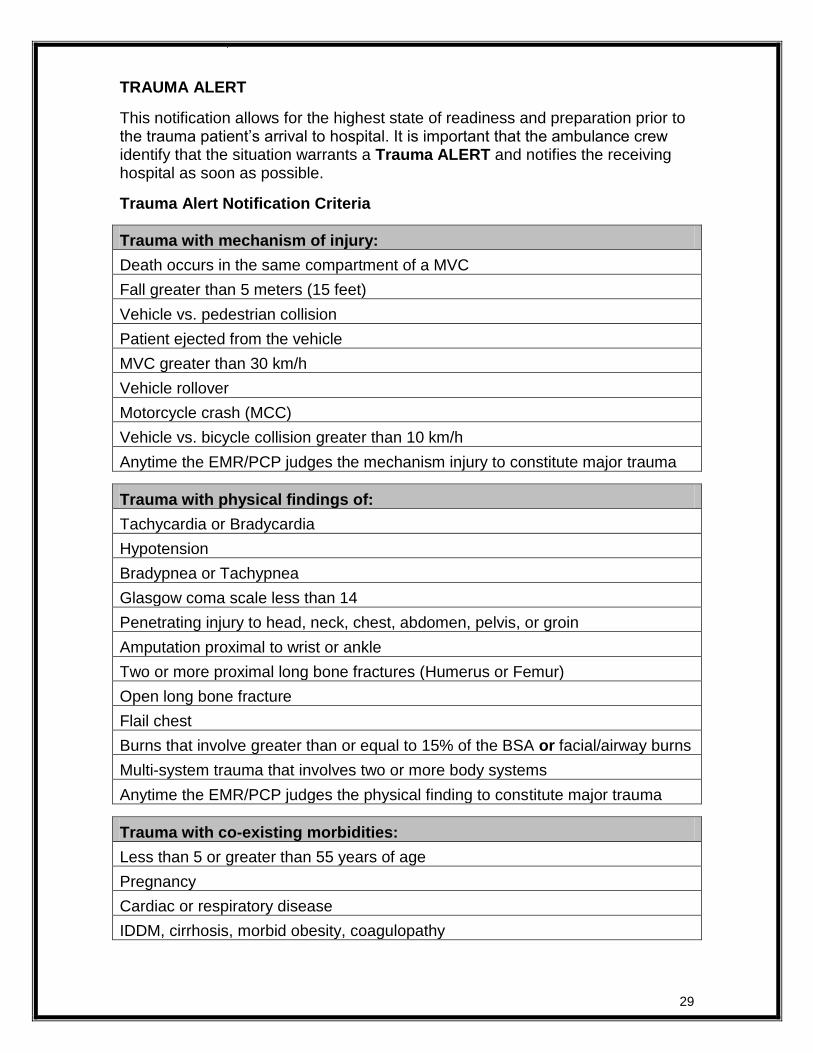
TRAUMA ALERT
This notification allows for the highest state of readiness and preparation prior to the trauma patient’s arrival to hospital. It is important that the ambulance crew identify that the situation warrants a Trauma ALERT and notifies the receiving hospital as soon as possible.
Trauma Alert Notification Criteria
Trauma with mechanism of injury:
Death occurs in the same compartment of a MVC
Fall greater than 5 meters (15 feet)
Vehicle vs. pedestrian collision
Patient ejected from the vehicle
MVC greater than 30 km/h
Vehicle rollover
Motorcycle crash (MCC)
Vehicle vs. bicycle collision greater than 10 km/h
Anytime the EMR/PCP judges the mechanism injury to constitute major trauma
Trauma with physical findings of:
Tachycardia or Bradycardia
Hypotension
Bradypnea or Tachypnea
Glasgow coma scale less than 14
Penetrating injury to head, neck, chest, abdomen, pelvis, or groin
Amputation proximal to wrist or ankle
Two or more proximal long bone fractures (Humerus or Femur)
Open long bone fracture
Flail chest
Burns that involve greater than or equal to 15% of the BSA or facial/airway burns
Multi-system trauma that involves two or more body systems
Anytime the EMR/PCP judges the physical finding to constitute major trauma
Trauma with co-existing morbidities:
Less than 5 or greater than 55 years of age
Pregnancy
Cardiac or respiratory disease
IDDM, cirrhosis, morbid obesity, coagulopathy

30
SEPSIS
EMR & PCP
1. Manage Airway 2. O2 100% via non-rebreather mask 3. EMR’s should request PCP or ACP intercept if available
PCP ONLY
4. Continuous cardiac and SpO2 monitoring 5. 12 Lead ECG 6. Two large bore IV’s during transport 7. Treat symptoms based on standards of care 8. If patient meets Sepsis Inclusion Criteria*:
Provide fluid bolus of 20 mL/kg
regardless of blood pressure
Sepsis Inclusion Criteria*
History of infection AND any TWO of the following:
Temperature less than 36° C or greater than 38° C
Tachypnea (greater than 20 BPM)
Tachycardia (HR greater than 100)
If patient remains hypotensive after administration of IV fluid, he/she is considered to be in Septic Shock. Contact OLMC for consideration of the following:
Continuous fluid bolus to achieve a SBP of greater than 90 mmHg for adults or normotensive for pediatrics (see pediatric reference page 54).
Carefully observe for signs of fluid overload. Auscultate chest for crackles every 250 mL. If adventitious breath sounds present, stop bolus and contact OLMC.

31
SHOCK – Not Yet Diagnosed
EMR & PCP
1. Manage Airway 2. O2 100% via non-rebreather mask 3. Control external bleeding 4. EMR’s should request PCP or ACP intercept if available
PCP ONLY
5. Two large bore IV’s (limit to one attempt on scene) 6. Continuous cardiac and SpO2 monitoring 7. If shock present, give a fluid challenge based on Fluid Therapy Protocol
(page 44)
STAGES OF SHOCK
Vital Signs
Signs and Symptoms
Compensated Shock Uncompensated
shock Irreversible Shock
Heart Rate Mild Tachycardia Moderate Tachycardia Bradycardia, Severe
dysrhythmias
Level of Consciousness
Lethargy, confusion, combativeness
Confusion, unconsciousness
Coma
Skin Delayed capillary refill,
cool skin
Delayed capillary refill, cold extremities,
cyanosis
Pale, cold, clammy skin
Blood Pressure Normal or slightly
elevated Decreased systolic
and diastolic pressure Frank hypotension
If patient remains hypotensive after two liters of NS, contact OLMC for consideration of second bolus.
Note: Trendelenburg positioning is not indicated in the treatment of shock, and is not to
be utilized as a treatment option.

32
SYMPTOMATIC HYPOGLYCEMIA
EMR & PCP
1. Manage airway as needed 2. O2 100% via non-rebreather mask 3. Administer oral glucose or sugared beverage if
symptomatic Hypoglycemia Treatment Indications met* for the EMR or is confirmed by blood glucose testing by the PCP.
4. EMR’s should request PCP or ACP intercept if available
ORAL GLUCOSE
Indications: Symptomatic Hypoglycemia and patient is conscious, awake, and able to swallow and cough
Contraindications: Altered consciousness, Unable to cough, Unable to swallow or protect own airway
Precautions: Monitor for aspiration
Dose: ONE of the following options:
5 tablets Dex 4® 20 grams PO
Two tubes of Dex 4® 15 gram paste PO
Insta-glucose® 30 gram tube
1 cup (250 mL) fruit juice or regular pop (if available at scene and deemed more palatable by patient)
4 teaspoons (20 mL) or 4 packets of table sugar dissolved in water (if available at scene and deemed more palatable by patient)
*Hypoglycemia Treatment Indications for the EMR
Patient is a known diabetic who is conscious, awake, and able to swallow and cough and is showing the following:
1. Irritability 2. Confusion 3. Weakness 4. Profuse sweating 5. Low blood sugar according to family or patient
If patient is unconscious, not awake, or unable to cough or swallow, DO NOT
administer oral glucose or sugared beverage

33
SYMPTOMATIC HYPOGLYCEMIA Cont’d
PCP ONLY
5. IV access 6. Measure blood glucose 7. If blood glucose is less than 4 mmol/L, administer either of the following
medications based on patient:
DEXTROSE 10, 25 & 50% (if IV established)
Indications: Symptomatic Hypoglycemia with IV access
Contraindications: None in emergency setting
Precautions: May cause local venous irritation, tissue necrosis in the event of extravasation
Dose:
Weight Dose
Greater than 40 kg 50 mL (25 g) of 50% Dextrose SIVP
20 – 40 kg 1 mL/kg of 50% Dextrose to a max of 50 mL (25 g) SIVP
10 – 20 kg 2 mL/kg of 25% Dextrose (dilute D50 1:1 with NS) SIVP
Less than 10 kg 5 mL/kg of 10% Dextrose (dilute D50 1:4 with NS) SIVP
GLUCAGON (unable to establish IV)
Indications: Symptomatic Hypoglycemia without IV access
Contraindications: Hypersensitivity
Precautions: Hx of Pheochromocytoma
Dose: Adult (greater than 20 kg) 1.0 mg IM Pediatric (less than 20 kg) 0.5 mg IM
8. Repeat glucose measurement in 10 minutes if dextrose administered or at 20 minutes if glucagon administered.
9. Repeat step 7 once if necessary
Contact OLMC:
to repeat dose if BG remains less than 4 mmol/L after second dose
for any patient that refuses transport or meets criteria for Treat and Release.
34
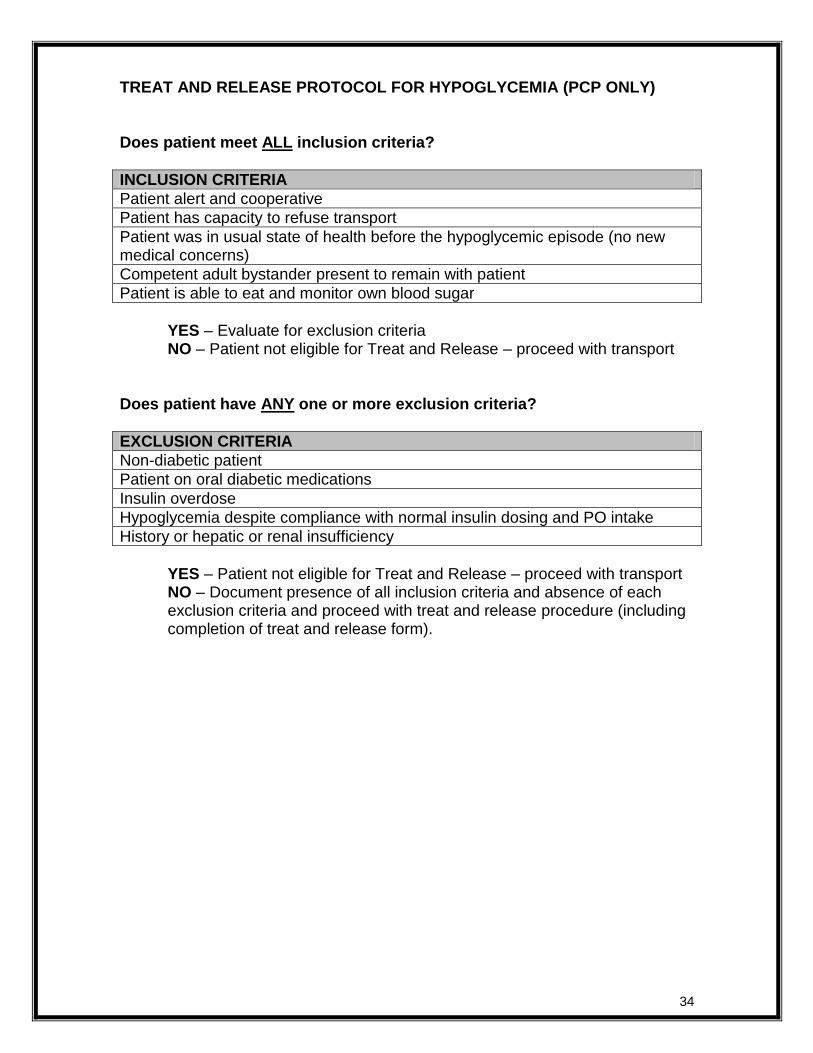
TREAT AND RELEASE PROTOCOL FOR HYPOGLYCEMIA (PCP ONLY) Does patient meet ALL inclusion criteria?
INCLUSION CRITERIA
Patient alert and cooperative
Patient has capacity to refuse transport
Patient was in usual state of health before the hypoglycemic episode (no new medical concerns)
Competent adult bystander present to remain with patient
Patient is able to eat and monitor own blood sugar
YES – Evaluate for exclusion criteria NO – Patient not eligible for Treat and Release – proceed with transport
Does patient have ANY one or more exclusion criteria?
EXCLUSION CRITERIA
Non-diabetic patient
Patient on oral diabetic medications
Insulin overdose
Hypoglycemia despite compliance with normal insulin dosing and PO intake
History or hepatic or renal insufficiency
YES – Patient not eligible for Treat and Release – proceed with transport NO – Document presence of all inclusion criteria and absence of each exclusion criteria and proceed with treat and release procedure (including completion of treat and release form).

35
SYMPTOMATIC HYPERGLYCEMIA
EMR & PCP
1. Manage airway as needed 2. O2 as appropriate 3. EMR’s should request PCP or ACP intercept if available
PCP ONLY
4. IV during transport 5. Measure blood glucose 6. If blood glucose is greater than 15 mmol/L, AND patient shows signs of
dehydration (see box below), Initiate IV bolus at:
10 mL/kg for pediatrics
20 mL/kg for adults 7. Continuous cardiac and SpO2 monitoring 8. Repeat glucose measurement every 20 minutes
Contact OLMC for consideration of further fluid bolus.
Symptoms Associated with Hyperglycemia:
Diuresis Warm, dry skin Dry mucous membranes Tachycardia Postural hypotension Polyuria Polydipsia Abdominal pain Dehydration Confusion
Signs and Symptoms of Dehydration: Adult: Dry mucous membranes Tachycardia Skin Tenting Weakness or Lethargy Decreased urine output Pediatric: Dry mucous membranes Tachycardia Mottled skin Weakness or Lethargy Decreased urine output Delayed capillary refill

36
CONVULSIVE SEIZURES
EMR & PCP
1. Manage airway 2. O2 100% via non-rebreather mask 3. Spinal immobilization if unprotected fall to ground and seizure has stopped 4. If actively seizing, place patient supine and protect patient from injury. If
postictal, place in left lateral recumbent position and maintain airway. 5. EMR’s should request PCP or ACP intercept if available
PCP ONLY
6. Continuous cardiac and SpO2 monitoring 7. IV during transport 8. Measure blood glucose 9. Request ACP intercept for active seizures or recurrent seizures (Status
Epilepticus).

37
TOXINS
EMR & PCP
1. Scene safety: protect rescuers and patients from immediate danger and contamination.
Toxic exposures might require special precaution, including HAZMAT precautions, before patient treatment begins.
2. Manage Airway 3. O2 as appropriate 4. EMR’s should request PCP or ACP intercept if available
PCP ONLY
5. IV during transport 6. Continuous cardiac and SpO2 monitoring 7. 12 lead ECG 8. Request ACP intercept if available
Contact OLMC for guidance if required

38
CHILD BIRTH
EMR & PCP
1. Maintain airway, assist ventilations as necessary 2. O2 as appropriate 3. If no crowning, place patient in left lateral recumbent position and
discourage patient from bearing down and initiate transport 4. If crowning prepare for imminent delivery
PCP ONLY
5. Continuous cardiac, SpO2, and BP monitoring if possible 6. IV Access
APGAR SCORE 0 1 2 Appearance, color Blue, pale Centrally pink Completely pink
Pulse, heart rate None Less than 100 Greater than 100
Grimace, reflex No response Grimace Cough, gag, cry
Activity, attitude Flaccid/limp muscle tone Some flexion Well-flexed/active motion
Respiratory effort None Weak, irregular irritable Good, crying
Imminent delivery:
1. Call for ALS support or second unit 2. Warm ambient temperature 3. Prepare equipment:
- Airway equipment – suction, BVM - Blankets - Clamps and scissors to cut umbilical cord - Bag for placenta
4. Apply gentle pressure using a cupped hand to the perineum (skin stretched between the vagina and the rectum) and encourage a controlled (non-explosive) delivery.
5. Sweep your finger around newborn neck to determine if nuchal cord present 6. If nuchal cord:
Attempt to guide loop of cord over newborn head prior to delivery of shoulders If tight cord and unable to guide over newborn’s head double clamp the cord
approximately 2.5 cm apart and cut cord 7. Gently guide anterior shoulder followed by posterior shoulder as newborn delivers –
keep baby below level of cord 8. Double clamp umbilical cord approximately 8 cm from baby and cut between clamps 9. Dry, warm and stimulate baby 10. If baby is pre-term, unconscious and/or poor tone or respiratory distress and/or apnea,
proceed with Neonatal Assessment and Resuscitation Protocol (Page 40) 11. If full-term, breathing and/or crying spontaneously and has good tone, wrap baby, place
on mother’s chest and encourage breast feeding 12. Calculate APGAR at 1 and 5 minutes 13. Prepare for delivery of placenta – do not pull on umbilical cord 14. When placenta delivers place in plastic bag along with umbilical cord

39
COMPLICATIONS OF DELIVERY (Cont’d from Childbirth Protocol)
EMR & PCP
Shoulder Dystocia (the situation in which the head has been born but the shoulders cannot be delivered by the usual methods)
Place patient in a Semi-Fowler’s and “Knee-chest” position. o With hips flexed have patient pull knees up towards the chest o Remove legs from stirrups and have assistant push on bottom of feet to bring knees
as close as possible to the chest in order to increase the AP diameter of the pelvis as much as possible
Have assistant stand beside the patient and facing the feet, use the heel of your hand to apply downward suprapubic pressure (just above pubic bone) to encourage the anterior shoulder to slip beneath pubis
During contraction, encourage mom to push while assistant continues application of suprapubic pressure – attempt to deliver the anterior shoulder from under the pubic bone
Limb presentation
Knee-chest position
Keep prolapsing limb warm and moist
Discourage mother from pushing with contractions
Prolapsed Cord
Place the patient in the “Knee-Chest” or Trendelenberg position with the hips elevated and the head positioned low
C-section is the delivery method of choice
Manually elevate the presenting part off of the umbilical cord and maintain until instructed to stop in the operating room
Instruct mother NOT to push
Keep the prolapsed portion of the cord warm and moist with saline soaked towel
Breech Presentation
Place patient in a Semi-Fowler’s and “Knee-chest” position. o With hips flexed have patient pull knees up towards the chest o Remove legs from stirrups and have assistant push on bottom of feet to bring knees
as close as possible to the chest in order to increase the AP diameter of the pelvis as much as possible
Sweep out legs
Allow the buttocks and trunk to deliver spontaneously
Support the body with your dominant forearm positioned under the baby’s torso

40
NEONATAL ASSESSMENT AND RESUSCITATION
EMR & PCP
Request PCP/ACP intercept if available
If baby is full term AND breathing and/or crying AND has good tone: 1. Clear airway if necessary 2. Warm and dry 3. Continue ongoing evaluation
If baby is pre-term OR unconscious and/or poor tone OR respiratory distress or apnea:
1. Clear airway if necessary – suction the mouth, oropharynx, and then nose
2. Warm, dry and stimulate baby
If gestational age is less than 28 weeks, dry and warm as normal on delivery then cover baby from neck down in plastic wrap blanket to prevent evaporative heat loss. Do NOT WRAP PLASTIC AROUND baby. Then wrap baby in a warm blanket - cover the head while still keeping the face exposed.
3. Check heart rate immediately.
Greater than 100: routine care.
Less than 100 or gasping or apnea or central cyanosis: Immediately provide PPV with 100% oxygen at 40 – 60 breaths per minute.
4. After 30 seconds, recheck heart rate:
Greater than 100: routine care.
Less than 100: Attempt to improve ventilation.
5. After 30 seconds, recheck heart rate:
Less than 60: Initiate chest compressions coordinated with PPV at ratio of 3 compressions : 1 ventilations with a goal of 90 compressions and 30 breaths per minute
Reassess patient every 30 seconds
CPR Guidelines
Two-thumb encircling chest technique preferred
3:1 ratio of compressions to ventilations with a goal of 90 compressions and 30 bpm.
If providing PPV alone
Rate should be 40 – 60 breaths per minute
Temperature Control
Warm ambient temperature in anticipation of delivery (greater than 26°C)
Use warmed blankets if possible
Wrap in warm blanket or skin on skin with mother and cover both with a blanket

41
PAGE INTENTIALLY LEFT BLANK FOR FUTURE PROTOCOL

42
12-LEAD ECG ACQUISITION PROTOCOL (PCP ONLY)
NOTES:
Acquiring a 12-lead ECG tracing will not normally prolong scene time or transport more than 2 minutes.
The procedure should be performed concurrent with other assessment and care and should not interfere with other treatment protocols.
12 lead printouts should be clearly labeled with patients surname or MCP number and one copy must be attached (stapled if possible) to the PCR at receiving facility. The second copy should be kept with the service records.
12 Lead ECG Acquisition Criteria
For males greater than 35 years old and females greater than 40 years old, or diabetics of any age experiencing, but not limited to, any of the following:
Or anytime the paramedic feels a patient warrants a 12 lead ECG (regardless of age)
Chest pain
Jaw pain
Left arm pain
Epigastric pain
Dyspnea
Presyncope or Syncope
CVA
Diaphoresis disproportionate to the environment
Palpitations
Weakness
Dysrhythmias
Shortness of Breath
Abdominal pain
Pulmonary edema
Overdose or toxic ingestion
Non-traumatic back pain
Suspected electrolyte disturbances
Nausea / vomiting
Serial 12 Leads
12 lead ECG must be completed and repeated as outlined below:
1. On scene (prior to treatment) 2. In ambulance just prior to transport 3. Every 15 minutes during transport 4. Anytime patient condition or ECG changes

43
12-LEAD ECG ACQUISITION PROTOCOL (Cont’d) Procedure:
1. Place the patient in a supine or semi-sitting position. 2. Bare the patient’s chest enough to acquire a 12-lead ECG. Take all steps
necessary and possible to protect the patient’s dignity and privacy. 3. Prep the skin with alcohol or other wipe. Remove excess chest hair where
needed for good contact. If patent is large breasted or obese, be sure to place leads correctly.
4. Attach the four limb, chest, and precordial leads in the following correct anatomical position:
5. Reduce causes of artifact. Stop patient movement. If en-route to hospital, stop ambulance to acquire ECG.
6. Provide the receiving facility with a copy of the 12-lead ECG. Attach a copy to the PCR, and document the device interpretation on the PCR.

44
FLUID THERAPY (PCP ONLY)
When IV medication or fluid therapy maybe required, start a peripheral IV line or lock using 0.9% Normal Saline solution. The drip rate will be set at TKVO rate.
TKVO rate for patients less than 8 years of age is 15 ml/hr.
TKVO rate for patients greater than 8 years of age is 60-100 ml/hr.
Fluid bolus should be initiated if specified by protocol.
ADULT
Trauma:
20 mL/kg bolus. There is no limit to the amount of fluid a paramedic may administer to maintain an optimal SBP of 90 mmHg. If head and/or spinal cord injury is suspected, maintain an optimal SBP of 110-120 mmHg.
Non Trauma:
20 mL/kg bolus. Can be repeated to maximum of 2000 mL.
PEDIATRIC
Trauma:
20 mL/kg bolus. There is no limit to the amount of fluid a paramedic may administer to achieve and/or maintain hemodynamic stability. If head and/or spinal cord injury is suspected, maintain an optimal SBP of 80 mmHg for preschool and 90 mmHg for older children.
Non-Trauma
20 mL/kg bolus (10 mL/kg if hyperglycemia). Can be repeated X 1
Carefully observe for signs of fluid overload. Auscultate chest for crackles every 250 mL in adults, every 10 mL/kg in pediatrics. If crackles present, stop bolus
Intraosseous Therapy is not to be initiated at the PCP scope of Practice.
A buratrol or syringe should be used when fluid bolusing pediatric patients when at all possible (mandatory in children less than 8 years).

45
PCP/ACP INTERCEPT
EMR/EMR Crew Configuration
If identified by protocol, or when the EMR deems it necessary, an ALS Intercept may be requested. Based on patient presentation and/or protocol, EMR’s can request PCP Intercept if an ACP crew is not available.
EMR/PCP or PCP/PCP Crew Configuration If identified by protocol, or when the PCP deems it necessary, an ALS Intercept may be requested.
Intercepts should be activated as early as possible. They may be cancelled by the requesting crew if reassessment determines that it is not required.
The following list of conditions indicate the need for an ALS intercept:
Abdominal pain with unstable vital signs
Accident/assault victims with multiple trauma or high-risk injuries and/or unstable vital signs
Airway compromise/potential compromise
Altered LOC: unstable or declining
Anaphylaxis: unresponsive to initial treatment
Arrest: cardiac or respiratory
Chest pain or cardiac problems
GI bleed with unstable vital signs
Hemorrhage: internal/external – uncontrollable or with signs of shock
Respiratory distress unresponsive to initial treatment
Seizures: ongoing (greater than 5 minutes) or repetitive
Abnormal vital signs
*** DO NOT delay patient transport to await the arrival of an intercepting unit ***
Intercept Documentation
The original responding crew is to document the call up to the point of transfer of care, including all billing information and patient assessments / care provided, on the initial PCR (primary claim). Once care is transferred to the intercepting medic, the intercepting medic will complete a new PCR documenting their patient assessment and any treatment rendered as well as administrative patient information and will include the Primary Claim ID number of the initial PCR.
The crew originally assigned to the call must record the PCR number of the intercepting crew in the narrative portion of the PCR.
This information is essential to linking the two PCR’s

46
NON-EMS MEDICAL PERSONNEL ON SCENE
The medical care provided at the scene is the responsibility of the highest level of pre-hospital care provider who has responded by usual dispatch systems to that scene. Bystanders who stop to help, even though possibly more highly trained than the system providers, may not assume responsibility (except as outlined below) but may be allowed to help in care at the discretion of the lead provider. Any healthcare provider (MD, RN, off duty EMR/Paramedic, etc.) who is not an active member of the responding unit, and who is either at the scene at the time of the ambulance arrival or arrives after an EMR/Paramedic has initiated care, and who desires to continue to participate, should be put in touch with the on-line medical control physician.
An on-scene physician who is providing medical care outside the scope of practice of the attending practitioner must agree to take responsibility for patient care, be willing to document their involvement on the Patient Care Report (PCR), and accompany the patient to the hospital. Any disagreements between the responding ambulance crew and the on-scene physician should be discussed with the help of OLMC.
Individuals shall not intervene in the provision of care unless the individual is:
1. Permitted by the attending EMR or Paramedic, and 2. Is capable of assisting or delivering more extensive emergency medical
care, and 3. Can provide proof of licensure in Newfoundland & Labrador
Off-duty practitioners must obtain errors and omissions insurance coverage through one of the following means*:
a) A pre-existing written Memorandum of Understanding (MOU) specifically granting errors and omission coverage during off-duty hours and for when a practitioner is placed in a humanitarian situation in the province when your skill set will improve patient care
b) Contact your supervisor or employer for extension of errors and omission coverage prior to provision of care
*Off-duty practitioners who do not adhere to the above may be held personally liable for all provision of care interventions if they do not obtain coverage for errors and omissions insurance.
At no time should an EMR/Paramedic provide care outside of their
patient care protocols.

47
REFUSAL OF CARE / REFUSAL OF TRANSPORT
Policy Competent adult patients (or a mature minor*) have a right to refuse pre-hospital assessment, management, or transport. These patients must sign a Refusal of Care Form provided they meet the criteria outlined below.
Procedure 1. Assess the patient for and document on the record:
a) The ability to make medical decisions and understand consequences (e.g. alert and oriented, GCS = 15, no evidence of suicidal ideation/attempt, no evidence of intoxication with drugs or alcohol, ability to communicate an understanding of the consequences of refusal).
b) The understanding of risks to refusing treatment/transport. c) Lack of evidence of medical conditions that may affect ability to make
decisions (e.g. hypoglycemia, hypoxia, hypotension)
2. If it is determined that the patient is capable of making and understanding the consequences of medical decisions and there is no indication to contact OLMC, then: a) Explain possible consequences of refusing treatment/transport to the
patient. b) Have patient and witness sign the Refusal Form. c) Educate patient/family to call back if patient worsens or changes decision d) Recommend that the patient/family contact the patient’s family physician e) Offer assistance in arranging alternative transportation.
3. Patients who are minors (under age 18, and not considered to be a mature minor*) cannot refuse care. However, if the minor’s parent or legal guardian demonstrates understanding and are willing to assume responsibility for the minor’s care or lack of care must sign the “Refusal of Care” form on behalf of these minors.
4. If the individual refuses assessment, management, or transport, and you believe he/she is suicidal, and/or is in immediate danger of bodily injury to themselves or others as a result of mental illness and/or is intoxicated and in need of medical treatment, OLMC must be contacted or the police must be contacted as per the Mental Health Care and Treatment Act.
Mature Minor*
When a teenager has reached the point where he or she has sufficient intelligence and understanding to appreciate the nature and consequences of what medical treatment is proposed, the individual is considered a mature minor.

48
POTENTIAL COMMUNICABLE/QUARANTINABLE DISEASE
Indicators of Potential Communicable/Quarantinable Disease
Fever (38° C or greater) with any of the following:
Appearing obviously unwell
Multiple ill travelers aboard conveyance
Shortness of breath (recent onset)
Persistent cough / coughing blood
Persistent vomiting or diarrhea
Headache
Confusion (recent onset)
Skin rash
Bruising or bleeding (without previous injury)
1. If the patient meets the above indicators of a potential communicable disease, alert all emergency responding agencies of appropriate personal protective equipment (PPE) requirements (to include, but not limited to: gloves, gown, goggles and N95 mask for the emergency responder; mask and appropriate draping for the patient).
2. If the patient meets the potential communicable/quarantinable indicators or involves a known quarantinable disease (box below) AND is an international traveler being picked up at a port of entry (air or sea) notify the Quarantine Officer (QO) before leaving the vessel / passing customs (902-873-7659) for further direction.
3. Notify receiving facility of potential Communicable/Quarantinable disease. 4. Notify dispatch that transport vehicle will be unavailable after transport until
decontamination has occurred (confer with local hospital Infection Control)
Known Quarantinable Diseases
Active pulmonary tuberculosis Measles Anthrax Meningococcal meningitis Argentine hemorrhagic fever Meningococcemia Bolivian hemorrhagic fever Pandemic influenza type A Botulism Plague Brazilian hemorrhagic fever Poliomyelitis Cholera Rift Valley fever Crimean-Congo hemorrhagic fever Severe Acute Respiratory Syndrome Diphtheria Smallpox Ebola hemorrhagic fever Tularemia Lassa fever Typhoid fever Marburg hemorrhagic fever Venezualan hemorrhagic fever Yellow fever
Quarantine Officer- Atlantic Region 902-873-7659

49
MASS CASUALTY INCIDENT MANAGEMENT
Organization:
1. Incident Command and Triage is established by the first arriving unit. Roles may change as additional personnel arrive.
2. Scene size up
Incident Command:
1. Estimate number of victims, and notify dispatch 2. Request appropriate number of responding units, special equipment,
mutual aid units, and additional resources as needed 3. Identify staging area, access and egress routes 4. Identify treatment area 5. Assign other positions as additional crews and help arrive:
a. Treatment c. Litter bearers/extrication teams b. Transport d. Assign other duties as required
Triage Coordinator (Lowest trained personnel) 1. Direct all walking wounded to a designated area.
a. If possible, direct a few people to remain in the triage area and assist victims as required.
2. Triage of victims should be initiated immediately using the START* or JumpSTART** system. (see Triage reference page 50 or 51)
3. Perform only the most life saving measures (open airway, stop bleeding) 4. Oversee and direct litter bearers to transport patients from the triage area
to the treatment area according to triaged priority.
Treatment Coordinator (Highest trained personnel) 1. Establish treatment areas.
If incident is large, designate separate treatment areas for each triage level, including a morgue separate from other victims.
2. Ensure aggressive treatment and rapid packaging of patients 3. Assign and supervise treatment teams 4. Assign transport priorities (transport highest priority first) and communicate
this to transport coordinator.
Transport Coordinator: 1. Establish Staging area as well as access and egress routes 2. Establish and supervise the patient loading zone 3. Assign and supervise the quick and efficient loading of patients 4. Ensure smooth flow of ambulances and avoid congestion of vehicles 5. Maintain a log containing the victim’s name, injuries, time transported,
destination, and triage tag number 6. Notify the receiving facility of patient transports, including a brief description
of injuries
There must be adequate medical personnel working in the treatment area prior to initiating transportation of patients to receiving facilities.
All personnel are to restrict radio communications

50
MASS CASUALTY INCIDENT TRIAGE - Adult
The purpose of the Simple Triage And Rapid Treatment (START) system is to efficiently triage and transport the victims of a multiple or mass casualty incident. This is used when the number of injured exceed the capabilities of the first arriving units or for large scale incidents.
*START Triage System
Triage of victims should take no longer than 60 seconds each. Assess their “RPM” Respirations, Perfusion and Mental Status. Tags of the appropriate color should be placed on the upper extremity or in a visible location. Reassessments may be conducted and priority changed once all have been triaged 1. Walking Wounded
Voice triage should be used to direct walking wounded to designated area.
Tag GREEN minor 2. Respiratory
If the respiratory rate is over 30/min, tag Red immediate.
If the victim is not breathing, position airway, assess for breathing. If the victim is still not breathing, tag Black deceased.
3. Perfusion
If there is no radial pulse, tag Red immediate. 4. Mental Status
If the victim cannot follow simple commands, is unconscious or disoriented, tag Red immediate.
5. All other patients
Tag Yellow delayed

51
MASS CASUALTY INCIDENT TRIAGE - Pediatric
The purpose of the Simple Triage And Rapid Treatment (START) system is to efficiently triage and transport the victims of a multiple or mass casualty incident. This is used when the number of injured exceed the capabilities of the first arriving units or for large scale incidents.
**JumpSTART Triage System (for 1-8 years of age)
Triage of victims should take no longer than 60 seconds each. Assess their “RPM” Respirations, Perfusion and Mental Status. Tags of the appropriate color should be placed on the upper extremity or in a visible location. Reassessments may be conducted and priority changed once all have been triaged
1. Walking Wounded
Voice triage should be used to direct walking wounded to designated area.
Tag GREEN minor
2. Respiratory
If the respiratory rate is under 15/min or over 40/min tag Red immediate
If the victim is not breathing, position airway, assess for breathing. o If breathing resumes tag Red immediate. o If the victim is still not breathing, check pulse. If no pulse, tag Black
deceased. o If the victim is still not breathing, but has a pulse, perform 15 seconds
(5 ventilations) of mouth to mask ventilations. If respirations resume, tag Red immediate. If no respirations, tag Black deceased.
3. Perfusion
If there is no radial/brachial pulse, tag Red immediate.
4. Mental Status
Assess using the AVPU scale. o If alert, responsive to verbal stimuli, or appropriately responsive to
pain, tag Yellow delayed. o If unresponsive, or inappropriately responsive to pain, tag Red
immediate.

52
COMMUNICATIONS REFERENCE
Radio Report to Receiving Hospital
Radio reports should be kept as brief as possible. A short, concise report can be given over the radio and followed by a more detailed report at the hospital. The purpose of the radio report is to provide an opportunity for the receiving facility to activate the appropriate resources and services given the patient presentation
Radio Report Structure
Unit identification
Age and gender of patient
Chief complaint or reason for transport (CTAS If known, Alert status if applicable)
History of present illness/injury with vital signs
Very brief pertinent medical history (one sentence if possible)
Treatment rendered
Estimated time of arrival
The receiving facility should be contacted at the earliest available opportunity during critical cases.
Communications with OLMC (1-877-709-3535) Upon establishing communication with physician, present the following information in a clear and concise manner:
Level of practice and registration number (e.g. ACP - A12345)
Patients age and gender
Chief complaint
History of current illness
Past medical history
Medications
Present medical condition and vital signs
Treatment rendered
Request for orders and/or advice (you must speak directly to OLMC)
MUST repeat order(s) for clarification
Communications Failure In case of a communications failure with medical control due to equipment (radio, cell phone, landline) malfunction or due to incident location, the following will apply:
Personnel may, within the limits of their certifications, perform necessary procedures, that are contained within the protocols that would require a direct physician order under normal circumstances.
These procedures shall be the minimum necessary to prevent the loss of life or the critical deterioration of a patient’s condition.
All procedures performed under this order and the conditions that created the communications failure need to be thoroughly documented.
Attempts must be made to establish contact with medical control.
Such instances must be reported to Quality & Learning during the next business day. A Communication Failure Form must be completed and submitted at that time.
53
DEFINITIONS SURROUNDING DNR, TOR AND DETERMINATION OF DEATH
Reportable Death Criteria
Death as a result of violence, accident or suicide
An unexpected death when the person was in good health
Where the person was not under the care of a physician
The death is obviously of a suspicious nature
Where the cause of death is undetermined
Death is the result of improper or suspected negligent treatment by another person
Expected Death
Does NOT meet Reportable Death Criteria
SHCDM – Substitute Health Care Decision Maker
Means the person appointed by the Maker of an advance health care directive to make health care decisions on his or her behalf. The first named person or a member of the category of persons on the following list may, if he or she is at least 19 years of age, act as a SHCDM; the incompetent person's:
(a) Appointed substitute decision maker, or a guardian that has been appointed for the purpose by a court and named on the advance health care directive
(b) Spouse (c) Children (d) Parents (e) Siblings (f) Grandchildren (g) Grandparents (h) Uncles and aunts (i) Nephews or nieces (j) Another relative
(k) Health care professional who is responsible for the proposed health care
Valid AHCD – Advance Health Care Directive
Means a document in which a maker sets out that Maker's instructions or the maker's general principles regarding his or her health care treatment or in which a Maker appoints a substitute decision maker or both (Maker means a person who makes an advance health care directive). An advance health care directive shall be:
1. In writing 2. Witnessed by at least 2 independent persons 3. Signed by the Maker
Valid DNR – Do Not Resuscitate
Is a written order issued and signed by a physician that resuscitation should not be attempted if a person suffers cardiac or respiratory arrest. Such an order may be instituted on the basis of an advance health care directive from a person, or from a substitute health care decision maker, or by a physician, and it is designed to prevent unnecessary suffering.
54
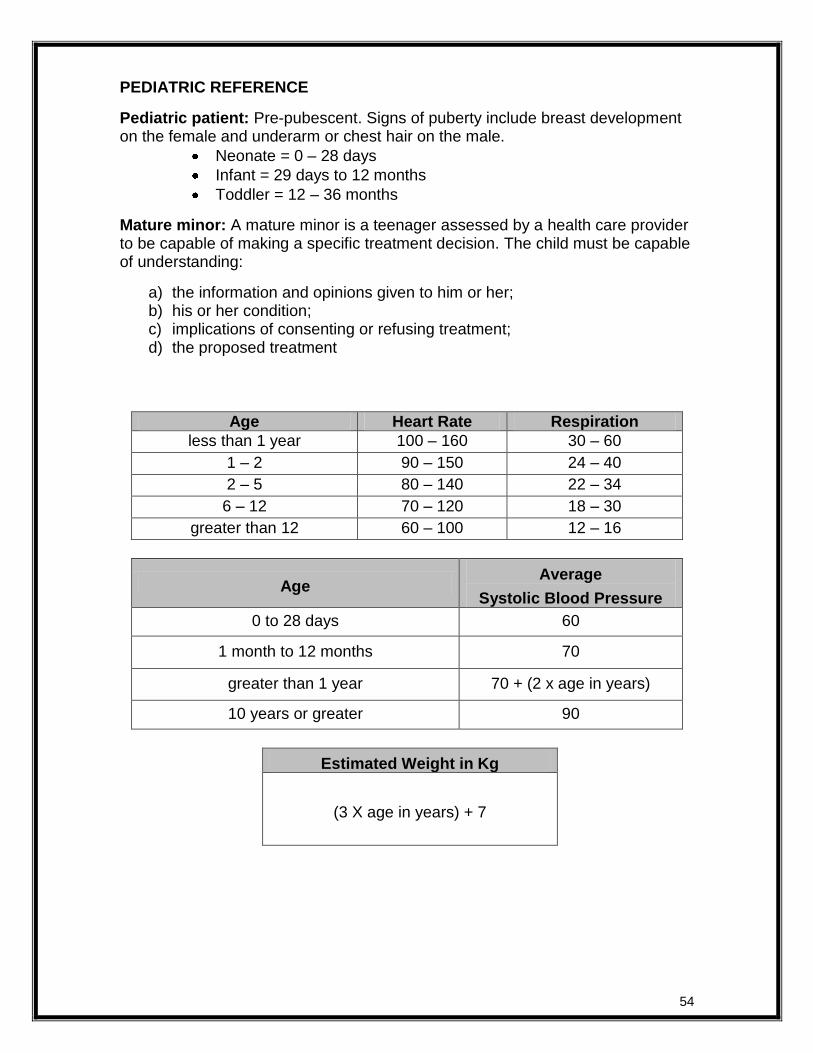
PEDIATRIC REFERENCE
Pediatric patient: Pre-pubescent. Signs of puberty include breast development on the female and underarm or chest hair on the male.
Neonate = 0 – 28 days
Infant = 29 days to 12 months
Toddler = 12 – 36 months
Mature minor: A mature minor is a teenager assessed by a health care provider to be capable of making a specific treatment decision. The child must be capable of understanding:
a) the information and opinions given to him or her; b) his or her condition; c) implications of consenting or refusing treatment; d) the proposed treatment
Age Heart Rate Respiration
less than 1 year 100 – 160 30 – 60
1 – 2 90 – 150 24 – 40
2 – 5 80 – 140 22 – 34
6 – 12 70 – 120 18 – 30
greater than 12 60 – 100 12 – 16
Age Average
Systolic Blood Pressure
0 to 28 days 60
1 month to 12 months 70
greater than 1 year 70 + (2 x age in years)
10 years or greater 90
Estimated Weight in Kg
(3 X age in years) + 7

55
RULE OF NINES
A method to estimate burn injury that divides the total body surface area (BSA) into segments that are multiples of 9%.
This method provides a rough estimate of burn injury size and is most accurate for adults and children older than 10 years of age.
If burns are irregularly shaped or has a scattered distribution throughout the body, the rule of palms is a better indicator of percentage. The surface of the patient’s hand (palm and fingers) equals about 1% of the total BSA.

56
GLASGOW COMA SCALE
The Glasgow Coma Scale a clinical tool used to assess the degree of consciousness and neurological functioning - and therefore severity of brain injury - by testing motor responsiveness, verbal response and eye opening.
ADULT CHILDREN INFANTS
EYE
OPENING
4 spontaneously spontaneously spontaneously
3 to command to command to command
2 to pain to pain to pain
1 no response no response no response
BEST VERBAL
RESPONSE
5 oriented oriented, appropriate coos, babbles, smiles
4 confused confused Irritable cries
3 inappropriate
words
inappropriate words inappropriate cries,
screams
2 incomprehensible incomprehensible words
or nonspecific sounds
moans in response to pain
1 no response no response no response
BEST MOTOR
RESPONSE
6 obeys commands spontaneous spontaneous
5 localizes pain localizes pain localizes pain
4 withdraws from
pain
flexion withdrawal flexion withdrawal
3 abnormal flexion abnormal flexion abnormal flexion
2 extension extension extension
1 no response no response no response

57
OXYGEN TANK DURATION CHARTS
Time in minutes
D Cylinder - Minus safe residual of 200 PSI P
SI
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
20
00
28
8
14
4
96
72
58
48
41
36
32
29
26
24
22
21
19
19
00
27
2
13
6
91
68
54
45
39
34
30
27
25
23
21
19
18
18
00
25
6
12
8
85
64
51
43
37
32
28
26
23
21
20
18
17
17
00
24
0
12
0
80
60
48
40
34
30
27
24
22
20
18
17
16
16
00
22
4
11
2
75
56
45
37
32
28
25
22
20
19
17
16
15
15
00
20
8
10
4
69
52
42
35
30
26
23
21
19
17
16
15
14
14
00
19
2
96
64
48
38
32
27
24
21
19
17
16
15
14
13
13
00
17
6
88
59
44
35
29
25
22
20
18
16
15
14
13
12
12
00
16
0
80
53
40
32
27
23
20
18
16
15
13
12
11
11
11
00
14
4
72
48
36
29
24
21
18
16
14
13
12
11
10
10
10
00
12
8
64
43
32
26
21
18
16
14
13
12
11
10
9
9
90
0
11
2
56
37
28
22
19
16
14
12
11
10
9
9
8
7
80
0
96
48
32
24
19
16
14
12
11
10
9
8
7
7
6
70
0
80
40
27
20
16
13
11
10
9
8
7
7
6
6
5
60
0
64
32
21
16
13
11
9
8
7
6
6
5
5
5
4
50
0
48
24
16
12
10
8
7
6
5
5
4
4
4
3
3
40
0
32
16
11
8
6
5
5
4
4
3
3
3
2
2
2
30
0
16
8
5
4
3
3
2
2
2
2
1
1
1
1
1
20
0
0
0
0
0
0
0
0
0
0
0
0
0
0
0
0
PS
I
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
← Liters per minute →

58
Time in minutes
E Cylinder - Minus safe residual of 200 PSI P
SI
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
20
00
50
4
25
2
16
8
12
6
10
1
84
72
63
56
50
46
42
39
36
34
19
00
47
6
23
8
15
9
11
9
95
79
68
60
53
48
43
40
37
34
32
18
00
44
8
22
4
14
9
11
2
90
75
64
56
50
45
41
37
34
32
30
17
00
42
0
21
0
14
0
10
5
84
70
60
53
47
42
38
35
32
30
28
16
00
39
2
19
6
13
1
98
78
65
56
49
44
39
36
33
30
28
26
15
00
36
4
18
2
12
1
91
73
61
52
46
40
36
33
30
28
26
24
14
00
33
6
16
8
11
2
84
67
56
48
42
37
34
31
28
26
24
22
13
00
30
8
15
4
10
3
77
62
51
44
39
34
31
28
26
24
22
21
12
00
28
0
14
0
93
70
56
47
40
35
31
28
25
23
22
20
19
11
00
25
2
12
6
84
63
50
42
36
32
28
25
23
21
19
18
17
10
00
22
4
11
2
75
56
45
37
32
28
25
22
20
19
17
16
15
90
0
19
6
98
65
49
39
33
28
25
22
20
18
16
15
14
13
80
0
16
8
84
56
42
34
28
24
21
19
17
15
14
13
12
11
70
0
14
0
70
47
35
28
23
20
18
16
14
13
12
11
10
9
60
0
11
2
56
37
28
22
19
16
14
12
11
10
9
9
8
7
50
0
84
42
28
21
17
14
12
11
9
8
8
7
6
6
6
40
0
56
28
19
14
11
9
8
7
6
6
5
5
4
4
4
30
0
28
14
9
7
6
5
4
4
3
3
3
2
2
2
2
20
0
0
0
0
0
0
0
0
0
0
0
0
0
0
0
0
PS
I
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
← Liters per minute →

59
Time in minutes
M Cylinder - Minus safe residual of 200 PSI P
SI
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
20
00
28
08
14
04
93
6
70
2
56
2
46
8
40
1
35
1
31
2
28
1
25
5
23
4
21
6
20
1
18
7
19
00
26
52
13
26
88
4
66
3
53
0
44
2
37
9
33
2
29
5
26
5
24
1
22
1
20
4
18
9
17
7
18
00
24
96
12
48
83
2
62
4
49
9
41
6
35
7
31
2
27
7
25
0
22
7
20
8
19
2
17
8
16
6
17
00
23
40
11
70
78
0
58
5
46
8
39
0
33
4
29
3
26
0
23
4
21
3
19
5
18
0
16
7
15
6
16
00
21
84
10
92
72
8
54
6
43
7
36
4
31
2
27
3
24
3
21
8
19
9
18
2
16
8
15
6
14
6
15
00
20
28
10
14
67
6
50
7
40
6
33
8
29
0
25
4
22
5
20
3
18
4
16
9
15
6
14
5
13
5
14
00
18
72
93
6
62
4
46
8
37
4
31
2
26
7
23
4
20
8
18
7
17
0
15
6
14
4
13
4
12
5
13
00
17
16
85
8
57
2
42
9
34
3
28
6
24
5
21
5
19
1
17
2
15
6
14
3
13
2
12
3
11
4
12
00
15
60
78
0
52
0
39
0
31
2
26
0
22
3
19
5
17
3
15
6
14
2
13
0
12
0
11
1
10
4
11
00
14
04
70
2
46
8
35
1
28
1
23
4
20
1
17
6
15
6
14
0
12
8
11
7
10
8
10
0
94
10
00
12
48
62
4
41
6
31
2
25
0
20
8
17
8
15
6
13
9
12
5
11
3
10
4
96
89
83
90
0
10
92
54
6
36
4
27
3
21
8
18
2
15
6
13
7
12
1
10
9
99
91
84
78
73
80
0
93
6
46
8
31
2
23
4
18
7
15
6
13
4
11
7
10
4
94
85
78
72
67
62
70
0
78
0
39
0
26
0
19
5
15
6
13
0
11
1
98
87
78
71
65
60
56
52
60
0
62
4
31
2
20
8
15
6
12
5
10
4
89
78
69
62
57
52
48
45
42
50
0
46
8
23
4
15
6
11
7
94
78
67
59
52
47
43
39
36
33
31
40
0
31
2
15
6
10
4
78
62
52
45
39
35
31
28
26
24
22
21
30
0
15
6
78
52
39
31
26
22
20
17
16
14
13
12
11
10
20
0
0
0
0
0
0
0
0
0
0
0
0
0
0
0
0
PS
I
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
← Liters per minute →

60
IV RATE CONVERSION CHART
Drip rate
mL/hr 10 gtt 15 gtt 20 gtt 60 gtt
30 5 8 10 30
40 7 10 13 40
60 10 15 20 60
100 17 25 33 100
125 21 31 42 125
150 25 38 50 150
175 29 44 58 175
200 33 50 67 200
250 42 63 83 250
300 50 75 100 300
← g
tt/m
in →
350 58 88 117 350
400 67 100 133 400
450 75 113 150 450
500 83 125 167 500
550 92 138 183 550
600 100 150 200 600
650 108 163 217 650
700 117 175 233 700
750 125 188 250 750
800 133 200 267 800
850 142 213 283 850
900 150 225 300 900
950 158 238 317 950
1000 167 250 333 1000
Total amount (mL) X drop factor = drops/minute
Total time (in minutes)

61
METRIC CONVERSION CHARTS
TEMPERATURE WEIGHT WEIGHT
°F °C Lbs Kg Lbs Kg
106 41.1 396 180 66 30
105 40.6 385 175 64 29
104 40 374 170 62 28
103 39.4 363 165 59 27
102 38.9 352 160 57 26
101 38.3 341 155 55 25
100 37.8 330 150 53 24
99 37.2 319 145 51 23
98.6 37 308 140 48 22
97 36.1 297 135 46 21
96 35.6 286 130 44 20
95 35 275 125 42 19
94 34.4 264 120 40 18
93 33.9 253 115 37 17
92 33.3 242 110 35 16
91 32.8 231 105 33 15
90 32.2 220 100 31 14
89 31.7 209 95 29 13
88 31.1 198 90 26 12
87 30.6 187 85 24 11
86 30 176 80 22 10
85 29.4 165 75 20 9
84 28.9 154 70 18 8
83 28.3 143 65 15 7
82 27.8 132 60 13 6
81 27.2 121 55 11 5
80 26.7 110 50 9 4
79 26.1 99 45 7 3
78 25.5 88 40 4 2
77 25 77 35 2 1

62
ACRONYMS / ABBREVIATIONS
ACLS Advanced Cardiac Life Support LPM Liters Per Minute
ACP Advanced Care Paramedic Lt Left
AED Automated External Defibrillator MCC Motorcycle Crash
ALS Advanced Life Support mcg Micrograms
AMI Acute Myocardial Infarction MD Medical Doctor
AP Anterior Posterior MDI Metered Dose Inhaler
APGAR Activity, Pulse, Grimace, Appearance, Respiration min Minute
ASA Acetylsalicylic Acid mL Milliliter
BG Blood Glucose mmHg Millimeters of Mercury
BLS Basic Life Support mmol/L Millimoles Per Liter
BP Blood Pressure MOI Mechanism of Injury
BPM Breaths Per Minute MVC Motor Vehicle Crash
BSA Body Surface Area NRP Neonatal Resuscitation Program
BVM Bag Valve Mask NS Normal Saline
C Celsius/Centigrade NYD Not Yet Diagnosed
CCP Critical Care Paramedic OLMC Online Medical Control
COPD Chronic Obstructive Pulmonary Disease PCP Primary Care Paramedic
CPR Cardiopulmonary Resuscitation PCR Patient Care Report
CVA Cerebral Vascular Accident PMCP Provincial Medical Control Program
D25 Dextrose 25% PO Per Os (by mouth, orally)
D50 Dextrose 50% PPE Personal Protective Equipment
DHCS Department of Health and Community Services PPV Positive Pressure Ventilation
DNR Do Not Resuscitate PSI Pounds per Square Inch
ECG Electrocardiogram Pt. Patient
EMR Emergency Medical Responder q Every
F Fahrenheit RA Right Arm
GCS Glasgow Coma Scale RL Right Leg
GI Gastrointestinal ROM Range of Motion
Gtt(s) Drop(s) ROSC Return of Spontaneous Circulation
HAZMAT Hazardous Materials RR Respiratory Rate
HHNK Hyperosmolar Hyperglycemia Non-Ketotic Rt Right
HR Heart Rate SBP Systolic Blood Pressure
HTN Hypertension SC Subcutaneous
Hx History SHCDM Substitute Health Care Decision Maker
IDDM Insulin-Dependent Diabetes Mellitus SIVP Slow Intravenous Push
IM Intramuscular SL Sublingual
IV Intravenous SpO2 Saturation of Peripheral Oxygen
kg Kilogram STEMI ST Elevation Myocardial Infarction
LA Left Arm TKVO To Keep Vein Open
lbs Pounds TOR Termination of Resuscitation
LL Left Leg VSA Vital Signs Absent
LOC Level Of Consciousness

63
FORMULARY

64
DEXTROSE 10, 25 & 50% (if IV in place)
Indications: Symptomatic Hypoglycemia with IV access
Contraindications: None in emergency setting
Precautions: May cause local venous irritation, tissue necrosis in the event of extravasation
Dose:
Weight Dose
Greater than 40 kg 50 mL (25 g) of 50% Dextrose SIVP
20 – 40 kg 1 mL/kg of 50% Dextrose to a max of 50 mL (25 g) SIVP
10 – 20 kg 2 mL/kg of 25% Dextrose (dilute D50 1:1 with NS) SIVP
Less than 10 kg 5 mL/kg of 10% Dextrose (dilute D50 1:4 with NS) SIVP
EPINEPHRINE 1:1000
Indications: Anaphylaxis, Status Asthmaticus, Pediatric Laryngotracheitis / Croup
Contraindications: HR greater than 150 for adults, HR greater than 180 for pediatrics
Precautions: Pregnancy, HTN, Active ischemic heart disease
Dose: Anaphylaxis, Status Asthmaticus: Adult: 0.3 mg IM Pediatric: 0.01 mg/kg IM to a maximum of 0.3 mg
Pediatric Laryngotracheitis / Croup:
Age Dose
Less than 1 year and less than 5 kg 0.5 mg (0.5mL) in 2 mL 0.9% NaCl
Less than 1 year and equal to or greater than 5 kg
2.5 mg (2.5 mL)
Greater than or equal to 1 year 5 mg (5 mL)
ASA
Indications: Ischemic Chest Pain
Contraindications: Hypersensitivity, active GI bleed, Hx of blood clotting disorder
Dose: 160 – 162 mg PO (chewed)

65
GLUCAGON
Indications: Symptomatic Hypoglycemia without IV access
Contraindications: Hypersensitivity
Precautions: Hx of Pheochromocytoma
Dose: Adult (greater than 20 kg) 1.0 mg IM Pediatric (less than 20 kg) 0.5 mg IM
IPRATROPIUM BROMIDE
Indications: Respiratory Distress with wheezing due to bronchospasm
Contraindications: Hypersensitivity, symptomatic tachycardia (greater than 150 HR in adults, greater than 180 for pediatrics), Ischemic chest pain.
Adult Dose: 4-8 puffs via MDI with aerochamber every 5 minutes as needed to a maximum of 24 puffs
OR 500 mcg nebulized with O2 every 5 minutes to maximum of 3 doses (1500 mcg)
Pediatric Dose: 3 puffs via MDI with aerochamber every 5 minutes as needed to a maximum of 9 puffs
OR 500 mcg nebulized with O2 every 5 minutes to a maximum of 3 doses (1500 mcg)
GLUCOSE (Oral)
Indications: Symptomatic Hypoglycemia and patient able to protect own airway
Contraindications: Unable to swallow or protect own airway
Precautions: Airway compromise due to consistency of medication.
Dose: ONE of the following options:
5 tablets Dex 4® 20 grams PO
Two tubes of Dex 4® 15 gram paste PO
Insta-glucose® 30 gram tube
1 cup (250 mL) fruit juice or regular pop (if available at scene and deemed more palatable by patient)
4 teaspoons (20 mL) or 4 packets of table sugar dissolved in water (if available at scene and deemed more palatable by patient)

66
NITROGLYCERIN
Indications: Ischemic chest pain
Contraindications: Hypersensitivity, decreased LOC, SBP less than 100 mmHg, HR less than 60, HR greater than 150, Patient taking erectile dysfunction drugs within 48 hrs.
Dose: 0.4 mg SL every 5 minutes to a maximum 6 sprays until chest pain is relieved or SBP falls below 100 mmHg
SALBUTAMOL
Indications: Respiratory Distress with wheezing due to bronchospasm
Contraindications: Hypersensitivity, symptomatic tachycardia (greater than 150 HR in adults, greater than 180 for pediatrics), Ischemic chest pain.
Adult Dose:
4-8 puffs via MDI every 5 minutes as needed to maximum 24 puffs
OR 5 mg nebulized with O2 every 5 minutes to maximum of 3 doses
Pediatric Dose:
Age MDI (100 mcg/puff) with
aerochamber*
Nebulized (dilute with 0.9% NaCl to a total
volume of 2.5 ml)
Less than 5 years 5 puffs 2.5 mg
Greater than or equal to 5 years
10 puffs 5 mg
Repeat as needed to maximum of 3 doses (3 x 5 puffs, or 3 x 2.5 mg nebulized if less than 5 years or 3 x 10 puffs or 3 x 5 mg nebulized if greater than 5
years)

67
NOTES

68
NOTES

69
NOTES