baseline report on respiratory health in the framework of...
TRANSCRIPT

December 2003
Technical Working Group on priority diseases, subgroup Respiratory Health
Baseline Report on Respiratory Health
in the framework of the European
Environment and Health Strategy
(COM(2003)338 final)
This report reflects the opinions of the members of the Working Group and it highlights the different opinions where appropriate. It shoul

Technical Working Group on priority diseases, subgroup Respiratory Health
Baseline Report on Respiratory Health
in the framework of the European
Environment and Health Strategy
(COM(2003)338 final)
file V1849-65.001
date 5 December 2003
registration number ML-MR20030787
version 1
This report reflects the opinions of the members of the Working Group and it highlights the different opinions where appropriate. It should no be considered as an official statement of the position of the European Commission.
©

5 December 2003, version 1 ML-MR20030787 - 3 -
CONTENTS PAGE
SUMMARY 5
1 INTRODUCTION 6
2 INTRODUCTION TO THE RESPIRATORY HEALTH 7 2.1 Context 7 2.2 Temporal changes 9 2.3 Impact of therapy. 9 2.4 Geographical variation 10 2.5 Multi-causality 11
3 CAUSES - PROTECTIVE FACTORS – TRIGGERS 15 3.1 Causes and triggers 15 3.2 Definitions 15
4 MODIFIERS 16 4.1 Preamble 16 4.2 Host susceptibility 16 4.2.1 Genetics 16 4.2.2 Gene/environmental interactions 17 4.3 Gender 18 4.4 Age/developmental stage 19 4.4.1 Fetal programming of lung disease in children and adults 19 4.4.2 Lung Development and Implications for disease 19 4.4.3 Unique vulnerabilities 20 4.5 Ethnic groups/Social deprivation 21
5 PROGRAMS AND STUDIES UNDERWAY 22 5.1 European programmes/ studies 22
6 HOST FACTORS 25 6.1 Infections 25 6.2 Asthma and Atopy 25 6.2.1 The Hygiene hypothesis 26 6.2.2 Diet 27 6.2.3 In utero and infant environment 28
7 OUTDOOR AMBIENT EXPOSURE/ AMBIENT AIR POLLUTION AND POLLEN 29 7.1 Introduction 29 7.2 Ambient air pollution in Europe 29 7.3 Respiratory health effects of exposure to ambient air pollution 30 7.4 Respiratory health effects of exposure to pollen 33
8 INDOOR EXPOSURE /INDOOR ENVIRONMENTAL RISK FACTORS 34 8.1 Exposure scenarios 34 8.2 Exposure 35 8.2.1 Home Environment 35 8.2.2 The School environment 38 8.2.3 Other indoor environments 39
9 GAPS IN KNOWLEDGE 40

5 December 2003, version 1 ML-MR20030787 - 4 -
10 RECOMMENDATIONS 41
11 CONCLUSIONS 42
12 REFERENCES 43
ANNEX 1 MANDATE OF THE SUB-GROUP RESPIRATORY HEALTH 54
ANNEX 2 MEMBERS OF THE SUB-GROUP RESPIRATORY HEALTH 58
COLOPHON 59

5 December 2003, version 1 ML-MR20030787 - 5 -
SUMMARY
Respiratory disease is the most common cause of mortality in children in underdeveloped economies and the commonest cause of morbidity in developed economies. Respiratory tract symptoms are particularly prevalent in young children and evidence for the relative contributions of potentially remediable environmental factors is emerging. The increased survival of children with significant lung disease, or with neuro-muscular disorders and associated respiratory impairment, is producing a growing number of young adults with increased susceptibilities to environmental hazards. Whereas some acute and chronic respiratory diseases and illnesses have clearly identifiable causes, e.g. bacterial and viral pneumonias, others including asthma and bronchitis have a variety of potential causes and environmental stressors. In this context it is important to separate potential environmental causes or initiators of diseases such as asthma from environmental “triggers” of already existing disease. Definitions of childhood respiratory disease also need to be considered as they can distort what appear to be important regional differences in disease expression. There is growing evidence that fetal life and early childhood are critical periods of development during which many diseases that present during child and adult life may have their origins. Apart from the evidence for intrauterine affects on the developing respiratory system the respiratory pattern, airway anatomy and physiology of the newborn infant are also likely to be contributory to a unique vulnerability to environmental exposure. Host factors including genes, gender age developmental stage ethnicity, social conditions and diet will influence the expression of disease and modify the effects of environmental exposures. Host factors may modify both the expression of genes and also the responses to environmental stimuli. Thus, in theory they provide a powerful place to intervene in order to prevent disease. There is clear evidence that atmospheric pollution is associated with troublesome respiratory symptoms in children but what is less clear is whether specific pollutants have a causal role in the pathogenesis of respiratory diseases. European children spend more time in indoor than outdoor environments so much so that more than 90% of their waking hours are spent indoors and the burden for many chemical substances with health consequences is much higher than outdoors. Many environmental factors thought to influence children's respiratory health remain unclear and sometimes controversial. This is especially the case with respect to asthma and allergies. Since it is likely that these conditions will increase in a number of European countries over the next decade, it is important to target research towards this area.

5 December 2003, version 1 ML-MR20030787 - 6 -
1 INTRODUCTION
Context of the study This document is part of the report that the Technical Working Group on Priority Diseases prepares in support of the European Commission’s SCALE initiative. It is based on Scientific evidence, focused on Children, meant to raise Awareness, improve the situation by use of Legal instruments and ensure a continual Evaluation of the progress made. The objective of the work of the Technical Working Group sub-group on Respiratory health (TWG_RH) has been to assess. The mandate and terms of reference of the TWG_RH are given in the Annex 1. Resources The TWG_RH has representatives from 10 countries – covering existing EU members and acceding states and northern and southern member states, industrial organisations, citizen’s organisations, the research community; the WHO and various European Commission services were also present (See Annex 2). The organisations represented have access to work carried out for/by: the WHO, the EC (DGs ENV, SANCO, RTD, JRC and the EEA), industry, public health authorities, and international research work carried out under academic or intergovernmental programmes.

5 December 2003, version 1 ML-MR20030787 - 7 -
2 INTRODUCTION TO THE RESPIRATORY HEALTH
Respiratory disease is the most common cause of mortality in children in underdeveloped economies and the commonest cause of morbidity in developed economies. Respiratory tract symptoms are particularly prevalent in young children and evidence for the relative contributions of potentially remediable environmental factors is emerging. The state of children’s respiratory health is determined by the interaction of many factors including potential stressors from their environment, patterns of exposure, individual vulnerability and genetics. Identifiable risk factors include infection, air pollution (indoors and outdoors), diet, lifestyle, social condition, occupation, and provision of medical care. They produce a multi-causal effect that has both short- and longer-term manifestations with implications for lifelong respiratory health. This effect varies with gender, developmental age and ethnicity. This report provides a succint overview of the current state of knowledge with regard to the influence of the environment on the respiratory health of children, comprising the whole array of disorders and symptoms affecting the respiratory tract ranging from rhinitis and upper respiratory tract infections to asthma and pneumonia. The target population covers the period from fetus to young adult (up to 18 years of age) in order to reflect the whole range of age-specific conditions and unique periods of vulnerability dependent on growth and development. It aims to identify the gaps in knowledge and highlight the areas where policy action at Community level would have a significant impact on improving respiratory health in the EU.
2.1 Context
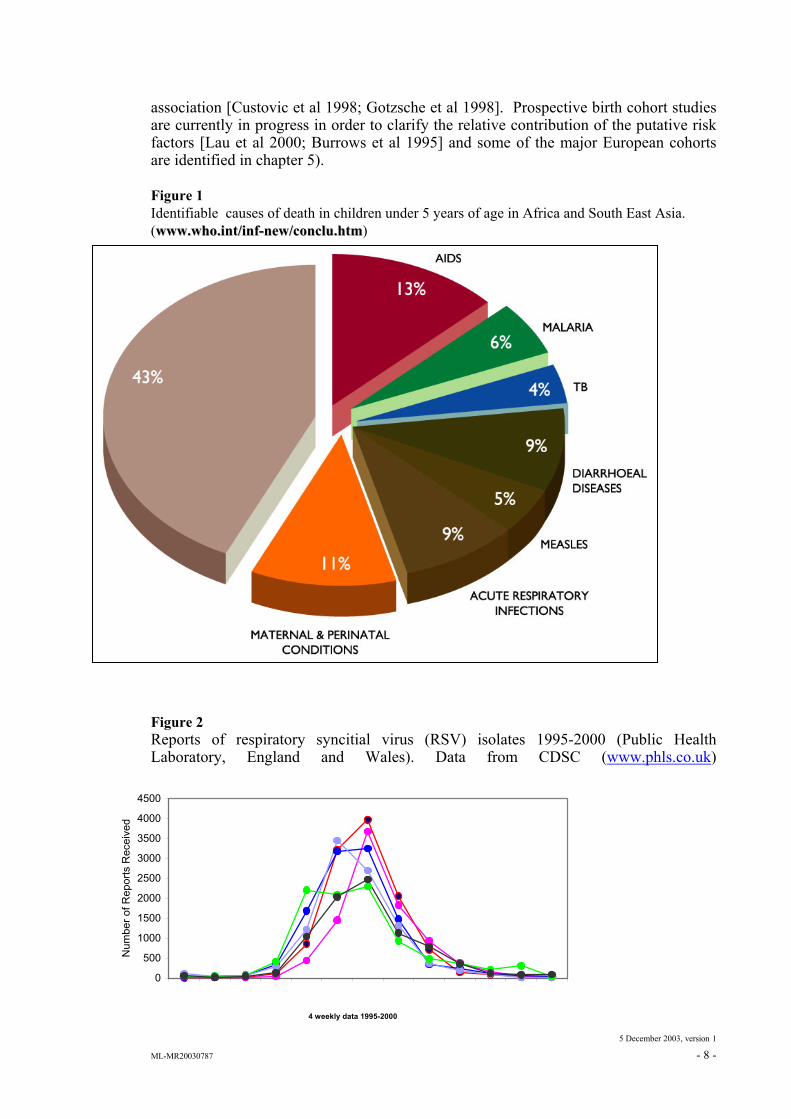
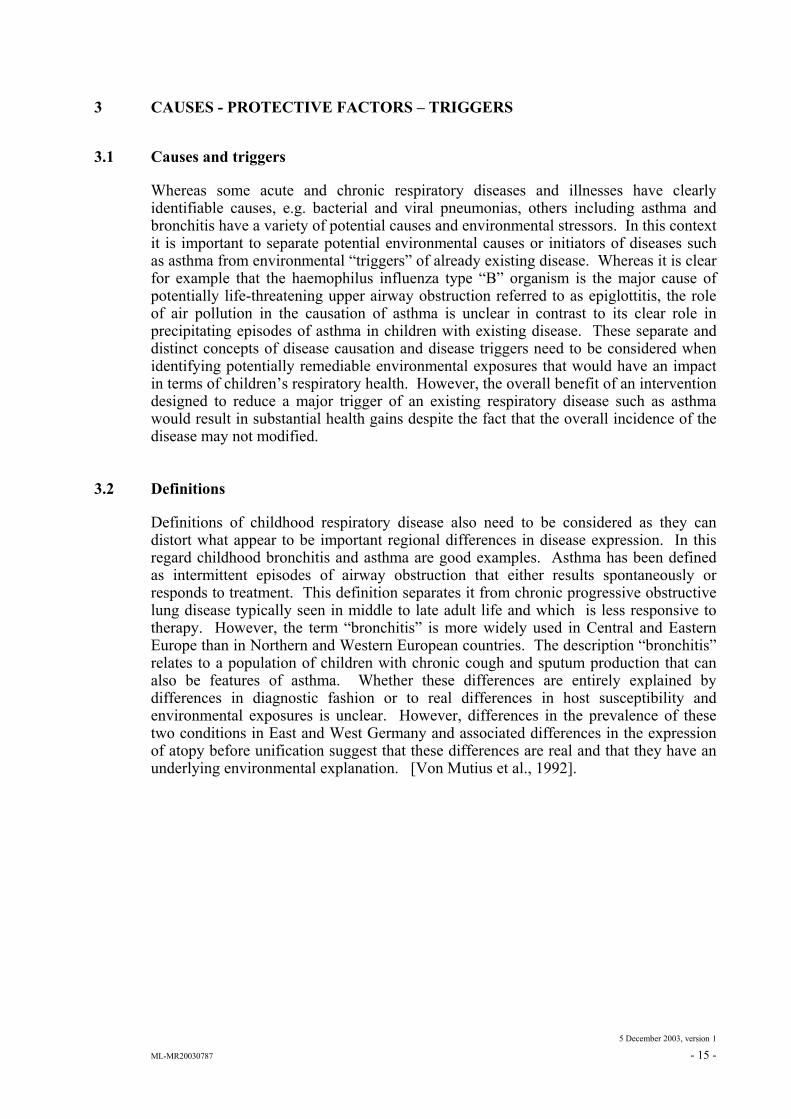
Childhood respiratory illness is the commonest cause of morbidity in industrialised countries and, acute respiratory infections (ARI) are common causes of death and serious morbidity in young children in underdeveloped and emerging economies (Figure 1). Serious morbidity is less and the causative infective agents differ in developed economies such as those in the EU in that bacterial infections, including tuberculosis, are common in underdeveloped countries while viral infections explain most ARI in developed economies. In temperate European countries there is a marked seasonality of ARI with a significant rise in prevalence in the winter months falling to relatively low levels in the summer. This pattern is evident for the respiratory syncytial virus (RSV) which is the commonest cause of the viral pneumonia labelled as “bronchiolitis” and which predominantly affects infants and very young children (Figure 2 ). Whereas serious morbidity and mortality from respiratory disease has fallen to low levels in developed economies, the total burden of respiratory disease remains high with a shift from life threatening ARI to an increased incidence of asthma and related atopic disease (rhinitis/hayfever and eczema). The reasons for what has been termed the “asthma and atopy epidemic” are not yet entirely clear although several environmental risk factors have been proposed including a reduction in the overall burden of infectious disease – the so-called hygiene hypothesis [Strachan, 1989], dietary factors including low anti-oxidant intake [Seaton et al 1994; Fogarty & Britton 2000] and greater intake of processed fats [Helms 2001]. Whereas in the last decade increased exposure to allergens and particularly those within the internal environment, including the house dust mite, were considered to be major factors, more recent data do not support this
5 December 2003, version 1 ML-MR20030787 - 8 -
association [Custovic et al 1998; Gotzsche et al 1998]. Prospective birth cohort studies are currently in progress in order to clarify the relative contribution of the putative risk factors [Lau et al 2000; Burrows et al 1995] and some of the major European cohorts are identified in chapter 5). Figure 1 Identifiable causes of death in children under 5 years of age in Africa and South East Asia. (wwwwww..wwhhoo..iinntt//iinnff--nneeww//ccoonncclluu..hhttmm) Figure 2 Reports of respiratory syncitial virus (RSV) isolates 1995-2000 (Public Health Laboratory, England and Wales). Data from CDSC (www.phls.co.uk)
0
500
1000
1500
2000
2500
3000
3500
4000
4500
4 weekly data 1995-2000
Num
ber o
f Rep
orts
Rec
eive
d

5 December 2003, version 1 ML-MR20030787 - 9 -
2.2 Temporal changes
The marked reduction in the prevalence of life threatening ARI in developed countries in the last 50 years reflects an improved standard of living, immunisation against tuberculosis, pertussis, diphtheria, measles and Haemophilus influenzae and the introduction of effective antimicrobial drugs and the relatively low rate of HIV infection. For those children with life threatening disease technological advances in managing respiratory failure have also had their impact clearly identified. Targets for further reductions in the burden of illness particularly in the youngest age groups include the elimination of RSV infection by an effective vaccine and a reduction in exposure to cigarette smoke in utero and in early childhood. Whereas the hospital work load for acute respiratory events including asthma may be diminishing the burden in primary care remains at high levels with the highest workload in the youngest age groups (Figures 3a,3b). Although sudden infant death syndrome (SIDS) is of unknown aetiology sufficient is known of its epidemiology for some practical preventive measures to have been formulated. The incidence rate in the UK increased from the 1950s (c1.6 per 1000 live births) to the 1980s (c2.5/1000) and thereafter declined to c0.65/1000 in 1996 with stability or a very slow further decline since. It is likely that this recent decline is related to a response to recommendations that infants should sleep in the supine position, since prone sleeping had been observed to be a risk. The observation in monitored infants that death or near-death is preceded by a period of severe bradycardia speaks for such factors being mediated via the autonomic nervous system and its central connections.
2.3 Impact of therapy.
In developed economies improvements in therapeutic options including age appropriate inhalation delivery devices, antibiotics and organisation of care have resulted in increasing actuarial survival for conditions that in previous generations and epochs were invariably fatal in childhood. This increased survival applies to a number of conditions including cystic fibrosis, unusual congenital anomalies such as congenital diaphragmatic hernia and respiratory complications of other conditions such as extreme prematurity and neuro-muscular disorders. In cystic fibrosis, for example, a strong cohort effect on actuarial survival, although modulated by socio-economic factors, has become apparent since the disease was first characterised in the 1940s [Britton 1989]. The increased survival of children with significant lung disease, or with neuro-muscular disorders and associated respiratory impairment, is producing a growing number of young adults with increased susceptibilities to environmental hazards.

5 December 2003, version 1 ML-MR20030787 - 10 -
Figure 3a Total workload in Scottish General (Primary care) Continuous morbidity reporting practices 2000 in the whole population showing the significant proportion of respiratory problems at all ages particularly in young children .
2.4 Geographical variation
There are important differences in the prevalence of childhood respiratory diseases in different European countries; as a generalization, there is more asthma and allergy in the prosperous west and more infective disease in the poorer East. There are also North-South differences in the prevalence of asthma and allergies. These speak for important and perhaps correctable environmental factors either in their causation or in their triggering. The diseases of greatest interest affecting the child’s respiratory system in a European context are pneumonia, viral bronchiolitis, measles, tuberculosis, HIV infection, sudden infant Death Syndrome (SIDS), cystic fibrosis and asthma/allergies. With the exception of SIDS, these fall into two categories, primarily infectious and primarily genetic diseases.
Female
0
500
1000
1500
2000
2500
3000
3500
4000
4500
5000
<1 04 08 12 16 20 24 28 32 36 40 44 48 52 56 60 64 68 72 76 80
Wor
kload
/100
0 Pa
tient
s
Agein Years
Male
0
500
1000
1500
2000
2500
3000
3500
4000
4500
5000
Wor
kload
/100
0 Pa
tient
s
Respiratory Symptom Other Illnesses

5 December 2003, version 1 ML-MR20030787 - 11 -
Figure 3b Respiratory Disease workload per 1000 patients.URTI = upper respiratory tract infection. LTRI=lower respiratory tract infection. Data from Scottish continuous morbidity reporting practices 2000.
2.5 Multi-causality
Figure 4 [from EEA, 1999] identifies and locates the 3 main clusters of causal factors usually involved in disease and ill health viz: The “genetics” of the individual. The “host condition” of the individual, which contains most of the factors usually described as “lifestyle” that can affect nutritional, immune and health status. Many ‘lifestyle’ risk factors are partly determined by wider issues that are largely outside the control of the individual, such as societal choices over energy; transport; the built environment and the food manufacturing and distribution systems. This cluster also includes income, employment and housing, as well as age: sensitivities to environmental stressors vary greatly with age, for example, from day one after conception to 90+years. Host condition factors contribute to ill health both directly, by providing a specific link in the causal chain, (such as extensive use of the contraceptive pill, obesity, and late childbirth), and indirectly, by modifying the extent to which environmental stressors interfere with health.
0
200
400
600
800
1000
1200
1400
1600
1800
2000
<1 04 08 12 16 20 24 28 32 36 40 44 48 52 56 60 64 68 72 76 80
Male
Wor
kload
/100
0 pa
tient
s
URTI
Other
LRTI/Bronchitis
Asthma
Age in Years
0
200
400
600
800
1000
1200
1400
1600
1800
2000Female
Wor
kload
/100
0 pa
tient
s

5 December 2003, version 1 ML-MR20030787 - 12 -
“Environmental stressors”. This cluster includes environmental exposures from air, water, food, soil, other surfaces, and consumer products, as well as the exposures to climate, radiation, noise, damp, housing, etc. that arise from some of the host conditions; factors such as transport, food and planning policies. These stressors can vary from large and ‘acute’ exposures, to small, yet continuous ’chronic’ exposures over many years. Usually, exposures are mixtures of physical, biological and chemical agents that vary with the emissions and the concentrations of the agents. Their impacts are determined by their abilities to deliver biologically effective doses, which of course vary with both the genetics and the host state of the people exposed. Knowledge about specific exposures are usually difficult to obtain but generic exposures can usually be inferred from the production of stressors, such as thousands of tons of pollutants emitted to the environments that people inhabit, or from proxy indicators such as the consumption of tobacco as a proxy measure for exposure to the 3000+ chemicals in tobacco smoke. Figure 4
9 G: sdi/slides/DGE/Missions 2003/EEA cont.to the EH Strategy.ppt
MultiMulti--causality and Complexitycausality and Complexity
HOST GENETICS
HOST STATE EXPOSURES/DOSES EFFECTS
• Genotypes and phenotypes
+ + = =>
• Nutritional status
• Immune status
• Health status (lifestyle)
• Age etc.
• Multiple exposures/doses• Via several exposure
routes (skin, inhalation, ingestion)
• Environmental – indoor• Environmental – outdoor• Occupational • Low doses and/or peaks• 24 hours continuous• Or single dose at critical
times• Pre- and post-natal doses• Lifetime and cumulative• ‘Target’ organ dose• Biologically effective
dose• Often unknown doses
• Initiating• Promoting• Retarding• Suppressing• CausingChanges in • Cells, tissues,• Hormones• Organs• Functions;• ‘normal’
‘distributions of bio-functions.
• Infections• Skin • Cancer• Neurotoxicity• Respiratory• Circulatory• Reproductive• Developmental
health impacts• Other adverse
HARM

5 December 2003, version 1 ML-MR20030787 - 13 -
Most diseases, such as cancers, asthma and the neurological or endocrine mediated diseases are the result of different combinations of factors arising from all three clusters e.g. genes, the host condition and environmental stressors, involving a genetic /environment interaction which is mediated by the condition of the host body (e.g. foetus, child, adult) before it receives the environmental stressors. Many different and specific combinations of factors are responsible both for individual cases of disease and for particular fractions of total disease. It follows that there are many cause-effect combinations in differently configured causal chains. Such multi-causality provides many obstacles to understanding the mechanisms and factors in the causal chain but it also provides many opportunities for removing links in the chain and thereby preventing harm, particularly where there are inter-dependencies between causal factors, such that removing even small links can reduce the impact of both those causal factors and others that may depend on them. The simple model in Figure 4 is less clear cut on closer analysis because the boundaries between the 3 clusters are fuzzy: for example the environment can influence genes, and genes can influence lifestyle choices, which, in turn, affect both the host conditions and the stressors that it receives. In most cases neither “Nature” (genetics) nor “Nurture” (environment) is an independent cause of harm –both are usually necessary. [Hogben, 1933]. In other words: “the genes provide the bullets but the environment provides the triggers”; and “Biology is not necessarily destiny”. A more dynamic, circular and iterative illustration of these three clusters of causal factors is provided in Figure 5. Despite its simplicity, the clustering of many interacting causes into the three groups of Figure 5 can be a useful tool to help policymakers and the public respond to the complexities of the multi-causal realities that characterise the four diseases targeted in the EU Environment and Health Strategy: childhood asthma, childhood cancer, endocrine mediated diseases and neurological diseases.

5 December 2003, version 1 ML-MR20030787 - 14 -
Figure 5
Multi-causality Framework for Environment and Health
Genes Host Conditions
Exposure
Effects
Harm
Source: EEA/TRC/ TWG Resp.
5 December 2003, version 1 ML-MR20030787 - 15 -
3 CAUSES - PROTECTIVE FACTORS – TRIGGERS
3.1 Causes and triggers
Whereas some acute and chronic respiratory diseases and illnesses have clearly identifiable causes, e.g. bacterial and viral pneumonias, others including asthma and bronchitis have a variety of potential causes and environmental stressors. In this context it is important to separate potential environmental causes or initiators of diseases such as asthma from environmental “triggers” of already existing disease. Whereas it is clear for example that the haemophilus influenza type “B” organism is the major cause of potentially life-threatening upper airway obstruction referred to as epiglottitis, the role of air pollution in the causation of asthma is unclear in contrast to its clear role in precipitating episodes of asthma in children with existing disease. These separate and distinct concepts of disease causation and disease triggers need to be considered when identifying potentially remediable environmental exposures that would have an impact in terms of children’s respiratory health. However, the overall benefit of an intervention designed to reduce a major trigger of an existing respiratory disease such as asthma would result in substantial health gains despite the fact that the overall incidence of the disease may not modified.
3.2 Definitions
Definitions of childhood respiratory disease also need to be considered as they can distort what appear to be important regional differences in disease expression. In this regard childhood bronchitis and asthma are good examples. Asthma has been defined as intermittent episodes of airway obstruction that either results spontaneously or responds to treatment. This definition separates it from chronic progressive obstructive lung disease typically seen in middle to late adult life and which is less responsive to therapy. However, the term “bronchitis” is more widely used in Central and Eastern Europe than in Northern and Western European countries. The description “bronchitis” relates to a population of children with chronic cough and sputum production that can also be features of asthma. Whether these differences are entirely explained by differences in diagnostic fashion or to real differences in host susceptibility and environmental exposures is unclear. However, differences in the prevalence of these two conditions in East and West Germany and associated differences in the expression of atopy before unification suggest that these differences are real and that they have an underlying environmental explanation. [Von Mutius et al., 1992].

5 December 2003, version 1 ML-MR20030787 - 16 -
4 MODIFIERS
4.1 Preamble
Host factors including genes gender age developmental stage ethnicity and social conditions will modify the effects of environmental exposure. One of the most prominent and obvious examples in this regard is asthma and related atopy. In these conditions there is a genetic component in that children of affected parents have two to threefold increased risk of disease expression which is modified and influenced by environmental factors as evidenced by the large increases in prevalence over the past three to four decades.
4.2 Host susceptibility
4.2.1 Genetics
Pulmonary disease may accompany a number of genetic disorders in children and some pulmonary diseases have a genetic basis, although this is seldom based on simple Mendelian inheritance but may have polygenic or multifactorial aetiology. A clear exception to this is cystic fibrosis, which results from a variety of mutations in a single gene located on chromosome 7q that encodes the CFTR protein . Asthma is a complex, polygenic disease that results from the exposure of genetically susceptible individuals to environmental triggers, possibly at critical stages of development, for the disease to be expressed. Linkage studies and genome-wide searches have identified a number of potential candidate genes for asthma and atopy [Anderson & Morrison, 1998] but no single gene accounts for a major part of the expression of the disease. Also, the rate of increase in asthma prevalence in the United Kingdom and other western countries is inconsistent with major shifts in population genetics. Therefore, attention has focussed on identification of environmental exposures that may be causally implicated in the aetiology of asthma and atopy and in triggering episodes . Other pulmonary diseases that have a genetic basis but rarely present during childhood include interstitial lung disease in association with collagen disorders, such as lupus erythematosus, and sarcoidosis. There is increasing interest in the origins of chronic obstructive pulmonary disease (COPD), which has been demonstrated in several studies to cluster within families, independent of smoking status. It is possible that mechanisms such as oxidative lung injury due to deficiencies of components of the anti-oxidant defences, such as superoxide dysmutase and glatathione-S-transferases, are responsible for respiratory morbidity in childhood and that could be the antecedent of COPD in adults. Increasing knowledge of the genetic and cellular regulation of pulmonary inflammation and defence is likely to lead to new insights into the origins of pulmonary diseases. The challenge will be to recognise individuals at risk and develop effective interventions to prevent the onset or alter the natural history of some of these conditions. While genetic factors predispose children to develop asthma, convincing evidence demonstrates that a number of environmental factors – environmental tobacco smoke, poor indoor/outdoor climate and some allergens – contribute to the onset of allergic

5 December 2003, version 1 ML-MR20030787 - 17 -
disease. Once the disease is established, these factors may also trigger symptoms. This points towards an interaction of genetic and environmental factors. The results of genome screens for asthma-related traits in several populations have identified already at least 18 regions of the genome that probably house asthma/atopy genes [Cookson, 2002; Xu et al, 2001; Yokouchi et al, 2000; Hakonarson et al, 2002]. The most consistently replicated regions are on chromosomes 2q, 5q, 6p, 7q, 11q, 12q, 13q, 14q and 17q. Positional cloning projects are ongoing in laboratories around the world to identify the asthma susceptibility loci in these regions. In addition, many candidate genes have been associated with asthma phenotypes, such as the genes in the IL-4/IL-13 pathway. A research team in the UK and USA found multiple polymorphisms in the ADAM33 gene, which were associated significantly with an increased risk of asthma but no for atopy [Eerdewegh et al, 2002]. Substantial research efforts are made in US, Europe and Japan to elucidate the genetic background for the development of allergies and asthma. Asthma researchers perform gene-environment investigations by correlating genes important for asthma and allergy to the environmental exposures considered significant to immune system ontogeny and asthma symptoms phenotypes [Young Kreeger, 2003]. The scientific efforts in this area are facilitated by rapid technological developments in molecular biology (gene arrays, high-throughput screening systems). Steven Kleeberger, of the U.S. National Institute of Environmental Health Sciences (NIEHS), found regions on chromosome 17 and 11 that are important contributors to ozone allergen susceptibility, as manifested by inflammation in the murine model's lung. The candidate gene is TNF-* on chromosome 17, a potent pro-inflammatory cytokine [Kleeberger et al, 1997]. Kleeberger and colleagues have also showed a link between the phenotype of ozone-induced increased permeability of lung tissue in a murine model and the Toll receptor Tlr-4 gene, which determines susceptibility to decreased lung epithelial cell function [Kleeberger et al, 2000]. If there is a mutation in Tlr-4, the mouse is protected against ozone-induced lung hyperperme- ability. Interestingly, Tlr-4 is also turned on during an endotoxin response. This evidence points to a critical role of the innate immune system in asthma. Tarja Laitinen, of the University of Helsinki, and colleagues conducted a genome scan of a homogenous population from the Kainuu province of Finland. They found linkage in a region of chromosome 7 for three phenotypes: asthma, a high level of immunoglobulin E (IgE), and a combination of the two, with the strongest being the IgE level [Laitinen et al, 2001]. IgE is the most well-known molecular marker for allergies. Currently her group is trying to narrow the region on chromosome 7 to find a candidate gene. Along with colleagues at the Karolinska Institute in Stockholm, the Helsinki group is conducting an epidemiological study of young children in Finland and Sweden; they are looking for environmental triggers in conjunction with the chromosome 7 genotype.
4.2.2 Gene/environmental interactions
A recent study in Norway showed the significance of the joint effect of parental atopy and exposure to environmental tobacco smoke for asthma disease aggravation in children. This phenomenon – effect modification of environmental exposure by genetic constitution, or gene by environment interaction – suggests that certain genetic markers could indicate susceptibility to environmental factors [Jaakkola et al, 2001]. Starting in 2003, the Global Allergy and Asthma European Network (GALEN), co-funded by the European Commission (in the context of FP6) will bring together epidemiological, basic and clinical researchers to investigate allergy and asthma across the life course,

5 December 2003, version 1 ML-MR20030787 - 18 -
including intra-uterine life and foeto-maternal interface; interaction between genetic and environmental factors in early life, translation of allergic sensitisation into disease and persistence of disease. Genetic characterisation is also combined with epidemiology. An example of this is a US NIEHS funded project, which is approaching the causes of asthma by studying how and why different populations have such vastly different prevalences of the disease. Small cohorts in Southern California are compared with populations in Wuhan, China (where asthma prevalence is low) and Mexico City (where prevalence is slightly higher than in China but still lower than in the United States) to analyse how life patterns as well as exposures to known asthma-promoters such as ozone are implicated in the complex causation of the disease.
4.3 Gender
Asthma is initiated in childhood with the majority of cases starting starting less than 5 years. In early childhood there is a male excess of asthma cases with a male:female ratio of 2:1. During adolescence this ratio reverses to a female predominance. Further evidence for these sex patterns is apparent in hospital admissions with asthma. This characteristic pattern may be informative in understanding the origins of this complex disease and in formulating novel therapies. The timing of the sex reversal suggests a role for sex hormones in the expression of asthma. Despite the epidemiological evidence of sex predispositions, to date there are few data relating sex steroids to the pathogenesis of asthma. The powerful role played by sex hormones in the field of autoimmunity is already well established. This knowledge has led me to speculate the stimulatory properties of female hormones and the suppressant effects of male hormones on the immune system may explain the sex reversal in asthma. The effects of sex steroids on T helper cells, which initiate and perpetuate inflammatory responses, may influence the expression of asthma.

5 December 2003, version 1 ML-MR20030787 - 19 -
4.4 Age/developmental stage
4.4.1 Fetal programming of lung disease in children and adults
There is growing evidence that fetal life and early childhood are critical periods of development during which many diseases that present during child and adult life may have their origins. In humans and other long-gestation species, the development of lung architecture occurs during fetal and early postnatal life. A number of epidemiological studies have demonstrated associations between prenatal factors that restrict intrauterine growth and respiratory symptoms in infancy. This observation led to speculation that factors, which impair fetal growth, may also constrain fetal lung development resulting in permanent changes to lung architecture. Barker et al (1991) described an association between low birth weight and lung function decrements in over 5000 adult males. Furthermore, respiratory infection during early childhood was associated with further decrements in adult lung function in this population, suggesting that either impaired lung function at birth was associated with predisposition to pulmonary infections during infancy or that respiratory infections, such as pneumonia and whooping cough, cause airway and lung remodelling which further impairs lung function. A follow up study of lung function in infancy has demonstrated reduced forced expiratory flows at the age of 2 months in infants who subsequently developed pneumonia [Castro Rodriguez et al, 1999] supporting a role for predisposition to infections in infants who already have pre-existing lung function impairment. Other epidemiological studies have confirmed an association between respiratory infections during infancy and early childhood and later functional abnormalities consistent with airway obstruction in adults [Shaheen et al, 1995]. In this context the typical U shaped distribution of symptomatic respiratory disease seen in whole populations (figure 3a) may in part reflect a link between the expression of early respiratory symptoms and the development of respiratory disease in late adult life. Although lung diseases that have a clearly defined and identifiable genetic basis are rare in childhood there is increasing interest in the origins of chronic obstructive pulmonary disease (COPD), which has been demonstrated in several early studies to cluster within families, independent of smoking status [Kueppers et al 1977, Larson et al 1970]. It is possible that mechanisms such as oxidative lung injury due to deficiencies of components of the anti-oxidant defences, such as superoxide dysmutase and glutathione-S-transferases, are responsible contribute to respiratory morbidity in childhood [Fryer et al 2000, Gilliland et al 2002] and may continue as risk factors for COPD in adults [Ishii et al 1999]. Increasing knowledge of the genetic and cellular regulation of pulmonary inflammation and defence is likely to lead to new insights into the origins of pulmonary diseases. The challenge will be to recognise individuals at risk and develop effective interventions to prevent the onset or alter the natural history of some of these conditions.
4.4.2 Lung Development and Implications for disease
The links between development and disease are well illustrated in the respiratory system. Although anatomically there is no sudden change at the time of birth, enormous alterations in function occur during subsequent growth and development. The observation that respiratory illness has high prevalences in infancy and early childhood
5 December 2003, version 1 ML-MR20030787 - 20 -
and again in late adult life points to possible links between early adverse environmental exposures and lifelong respiratory health [Barker 1991, Burrows 1980]. The most clearly identified adverse exposure at a whole population level is fetal tobacco smoke exposure associated with maternal smoking in pregnancy. Whereas postnatal or environmental tobacco smoke (ETS) exposure has a significant influence or respiratory morbidity in the young [Taylor & Wadsworth 1987] the effects of prenatal exposure are likely to be more long lasting. Studies which have assessed lung function soon after birth, when the effects of ETS would be expected to be small have shown evidence of reduced airway function [Hanrahan et al 1992, Young et al 1991]. Whereas it is clearly not possible to identify the exact mechanisms of these effects in humans, animal studies have shown that fetal ETS significantly reduces cell division in the lung as evidenced by reduced DNA, alveolar number and connective tissue within the lung [Collins et al1985, Vidic et al 1989].
4.4.3 Unique vulnerabilities
Apart from the evidence for intrauterine affects on the developing respiratory system the respiratory pattern, airway anatomy and physiology of the newborn infant are also likely to be contributory to a unique vulnerability to environmental exposure. The increasing metabolic demands of the rapidly growing infant requires a high ventilatory turnover. Infants have the same tidal volume as the adult on a per kilogram body weight basis but have an approximately three-fold increase in respiratory rates [Polgar & Weng 1979]. The consequence is an approximate three-fold increase in alveolar ventilation relative to body mass. Combined with a greater likelihood of sedimentation of respirable particulates in the conducting airways [Hislop et al 1972]. It should therefore not be surprising that exposures in fetal and life have lifelong implications for respiratory health.

5 December 2003, version 1 ML-MR20030787 - 21 -
4.5 Ethnic groups/Social deprivation
Using the World Bank definition of $1/person/day, it is estimated that 2.1 billion of the world’s population live in conditions of absolute poverty below this threshold. Diseases associated with poverty are primarily infectious diseases, which are linked to inadequate income, lack of access to clean water and sanitation, malnutrition and poor access to medical services. In developing countries, the commonest causes of death in children under 5 years of age are lower respiratory infections, diarrhoeal illnesses and measles. Acute lower respiratory tract infections account for 2.1 million deaths annually in young children in the developing world with approximately 40% estimated to be related to malnutrition [WHO Report on Childhood Illnesses, 1997; State of the World’s Children 2000, UNICEF]. Some developing countries have achieved lower rates of poverty related ill health by government interventions in health, education and social security and also by active programmes to increase the levels of female literacy in their populations. In the United Kingdom, adults and children of lower socio-economic status have also been demonstrated to be at higher risk of communicable diseases, particularly respiratory infections [Cohen, 1999]. A longitudinal study of a U.K. cohort born in 1946 demonstrated that a poor home environment, parental bronchitis and atmospheric pollution were the best predictors of lower respiratory infections in the first two years after birth and these factors together with later smoking and childhood respiratory infections were the best predictors of lower respiratory tract diseases in adults [Mann et al, 1992]. It is possible that increased infections in socially disadvantaged populations are related to crowding and increased exposure to infectious agents or to alterations in host immunity, possibly related to nutritional status. One of the characteristic diseases of social deprivation, tuberculosis, has recently shown a reversal of the decline in notified cases in England. (Public Health Laboratory Service (http://www.phls.co.uk)) with the largest number of cases reported from urban regions. Studies of variations in tuberculosis rates between electoral wards in inner cities have suggested that the country of birth was the single most explanatory variable, with measures of poverty being of only secondary importance [Beckhurst et al, 2001; Bennett et al, 2001].

5 D
ecem
ber 2
003,
ver
sion 1
M
L-M
R200
3078
7 - 2
2 -
5
PRO
GR
AM
S A
ND
ST
UD
IES
UN
DE
RW
AY
5.1
Eur
opea
n pr
ogra
mm
es/ s
tudi
es
Tab
le o
f ong
oing
/maj
or o
r re
leva
nt st
udie
s on
resp
irat
ory
heal
th
Stud
y na
me
Popu
latio
n (d
escr
iptio
n an
d nu
mbe
r)
Age
of
po
pula
tion
Des
ign
stud
y/ty
pe
Cou
ntry
/Reg
ion
Expo
sure
fact
or
Beg
inni
ng
date
En
d da
te
(exp
ecte
d)
Con
tact
per
son
Res
pons
ible
org
anis
atio
n
ASM
A
asth
mat
ic
child
ren
(n~4
00)
6-12
ye
ars
old
cros
s sec
tiona
l Fr
ance
sm
okin
g 19
95
Prof
. Dr.
R. L
iard
IN
SER
M P
aris
BA
MSE
ne
wbo
rn (n
~400
0)
co
hort
Swed
en
soci
al fa
ctor
s, in
door
clim
ate
1994
Pr
of. D
r. M
. Wic
kman
n En
v. H
ealth
Dep
t., S
tock
holm
C
ount
y C
ounc
il
LISA
ne
wbo
rn (n
~200
0)
co
hort
Ger
man
y V
OC
, bio
aero
sols
, TSP
and
PM
1998
2006
Prof
. D
r. O
. H
erba
rth,
Prof
. Dr.
H.-E
. Wic
hman
n
UFZ
-Cen
tre
for
Envi
ronm
enta
l R
esea
rch,
G
SF-E
nviro
nm.
&
Hea
lth
Res
earc
h C
ente
r
LEIP
I cl
inic
al c
ases
0-
18
inte
rven
tion
stud
y G
erm
any
mou
ld
1999
2005
Prof
. D
r. O
. H
erba
rth,
Prof
. Dr.
G. M
etzn
er
UFZ
-Cen
tre
for
Envi
ronm
enta
l R
esea
rch
and
Uni
vers
ity o
f Lei
pzig
KIG
A
&
KIG
A-E
NV
ki
nder
garte
n ch
ildre
n (n
~120
0)
6 cr
oss s
ectio
nal
Ger
man
y an
d A
rgen
tina
VO
C, T
SP a
nd P
M, P
AH
19
9320
05Pr
of. D
r. O
. Her
barth
UFZ
an
d U
nive
rsid
ad
Men
doza
and
Uni
vers
idad
La
Plat
a
LAR
S ne
wbo
rn
(at
risk)
(n
~475
)
coho
rt G
erm
any
indo
or e
xpos
ure
1995
2004
Prof
. Dr.
O. H
erba
rth a
nd
PD D
r. M
. Bor
te
UFZ
-Cen
tre
for
Envi
ronm
enta
l R
esea
rch
and
Uni
vers
ity o
f Lei
pzig
LISS
sc
hool
ch
ildre
n (n
~350
0)
6 an
d 8
repe
ated
cro
ss se
ctio
nal
Ger
man
y in
door
re
late
d ac
tiviti
es,
infe
ctio
n 19
9720
05Pr
of. D
r. O
. Her
barth
U
FZ-C
entre
fo
r En
viro
nmen
tal R
esea
rch
MA
S ne
wbo
rn (n
~130
0)
co
hort
Ger
man
y nu
tritio
n 19
90
Prof
. Dr.
U. W
ahn
Hum
bold
t U
nive
rsity
Ber
lin,
Cha
rite

5 D
ecem
ber 2
003,
ver
sion 1
M
L-M
R200
3078
7 - 2
3 -
PIA
MA
ne
wbo
rn (n
~400
0)
co
hort
The
Net
herla
nds
hom
e ris
k fa
ctor
s: m
ite
1996
D
r. H
. Sm
it
Nat
iona
l In
stut
e of
Pu
blic
H
ealth
and
the
Envi
ronm
ent
CO
PSA
in
ewbo
rns (
n~40
0)
0-15
yea
r co
hort
Den
mar
k am
bien
t and
indo
or a
ir po
llutio
n,
othe
r ris
k fa
ctor
s 19
9920
04Pr
of. D
r. H
. Bis
gaar
d U
nive
rsity
of C
open
hage
n
AIR
ALL
ERG
new
born
s fr
om
BA
MSE
, GIN
I, LI
SA,
PIA
MA
coho
rt
Swed
en,
Ger
man
y,
The
Net
herla
nds
indo
or a
nd o
utdo
or a
ir po
llutio
n20
0120
05Pr
of. B
. Bru
nekr
eef
Inst
itute
of
Ris
k A
sses
smen
t St
udie
s, Th
e N
ethe
rland
s
PATY
sc
hool
chi
ldre
n (n
~70
000)
5-
15 y
ear
cros
s sec
tiona
l
Aus
tria,
B
ulga
ria,
Ger
man
y, I
taly
, H
unga
ry,
the
Net
herla
nds,
Pola
nd,
Rus
sia,
C
zech
R
epub
lic,
Slov
akia
, Sw
itzer
land
, U
SA a
nd U
K.
outd
oor p
ollu
tion
2002
2004
Dr.
T. F
letc
her
Lond
on S
choo
l of
Hyg
iene
an
d Tr
opic
al M
edic
ine
Bitt
erfe
ld st
udy
scho
ol c
hild
ren
(n
~5 0
00)
5-14
yea
r cr
oss s
ectio
nal
Ger
man
y ou
tdoo
r pol
lutio
n 19
92
Prof
. Dr.
M. W
ickm
ann
GSF
-Env
ironm
. &
H
ealth
R
esea
rch
Cen
ter
Fren
ch
Six
City
Stu
dy
scho
ol
child
ren
(n~7
000)
cros
s sec
tiona
l Fr
ance
in
door
and
out
door
air
pollu
tion
1999
D
r. I.
Ann
esi-M
aesa
no
INSE
RM
Par
is
Osl
o B
irth
Coh
ort
new
born
(~40
00)
co
hort
Nor
way
ou
tdoo
r pol
lutio
n 19
9220
06D
r. P.
Naf
stad
N
orw
eign
Ins
tute
for
Pub
lic
Hea
lth
SCA
RPO
L sc
hool
chi
ldre
n
cros
s sec
tiona
l Sw
itser
land
in
door
and
out
door
air
pollu
tion
1998
2004
Prof
. C. B
raun
-Fah
rland
erU
nive
rsity
of B
asel
SEA
TON
N
ewbo
rn (
n~18
00)
4-5
C
ohor
t Sc
otla
nd U
K
Mat
erna
l (In
pre
ganc
y)an
d C
hild
D
iet
1998
2004
Prof
P H
elm
s D
r Ger
aldi
ne M
cNei
ll U
nive
rsity
of A
berd
een


5 December 2003, version 1 ML-MR20030787 - 25 -
6 HOST FACTORS
Host factors may modify both the expression of genes and also the responses to environmental stimuli. Thus, in theory they provide a powerful place to intervene in order to prevent disease. There is already much evidence that environmental factors can modify host factors with respect to the expression of a number of important childhood respiratory diseases. All conditions result from interactions between genes and the environment. Even primarily genetic conditions such as cystic fibrosis may be influenced importantly by environmental factors while environmental conditions such as pneumonia may have genetic pre-determinants. In this section we consider the more important respiratory conditions, asthma, infections, cot death and cystic fibrosis.
6.1 Infections
Infectious diseases in Europe exemplify the effectiveness of classical public health action in dealing with known risk factors. Even before antibiotics and immunisation, tuberculosis declined as a consequence of case finding, segregation of infectious people into sanatoria and improvement of housing, nutrition and living standards, with reduction of overcrowding. Immunisation with BCG is an effective method of reducing the expression of childhood tuberculosis and of preventing the important complications such as meningitis in countries where the infection is still prevalent. The incidence of measles has responded to mass immunisation programmes, although resurgence may be expected in response to public fears of vaccination, echoing the early days of the prevention of smallpox. In terms of deaths caused, pneumonia is the most important childhood respiratory disease. The immediate cause is infection but poverty, poor housing, overcrowding, malnutrition and poor medical services are contributory causes. Similar factors contribute to viral bronchiolitis of childhood. It should be noted that the benefits of antibiotics since the 1950s in treating infectious diseases of childhood have to some extent been countered by a growing problem of antibiotic resistance and the development of organisms, particularly Staphylococcus aureus and Mycobacterium tuberculosis, resistant to multiple drugs. Much of this may be attributed to inappropriate use of antibiotics. Despite the obvious benefits of antibiotics there is some evidence that their early administration may be a factor in the rise in allergic disease [Helms 2001].
6.2 Asthma and Atopy
Unlike most of the conditions mentioned above, asthma and allergies have become increasingly frequent in the prosperous countries of Western Europe, although they remains much less common in the Eastern part of the continent. A number of genetic polymorphisms have been described (see section 4.2.1) as associated with the risk of asthma, but the change in prevalence over a short period of two or three decades and the variation from country to country within Europe and the wider world speaks for important environmental determinants. In the broadest sense, this appears to be something associated with increasing national prosperity (not "westernisation", since it has been observed, for example, in Saudi Arabia). Two plausible hypothetical

5 December 2003, version 1 ML-MR20030787 - 26 -
explanations have been advanced for increasing population susceptibility to allergic disease - changes in patterns of exposure to micro-organisms (the hygiene hypothesis) and alterations in diet and energy output.
6.2.1 The Hygiene hypothesis
The hygiene hypothesis was originally based on an inverse relationship between infections and hayfever. leading the concept that protection of younger infants may be derived from infections passing round the family, altering their immune development from one primarily allergic (mediated by T helper 2 lymphocytes) to an anti-infective T helper 1 lymphocyte response. This concept has to answer two important objections. First, there has in fact also been an increase in T helper 1 associated diseases such as diabetes, and the two types of disease are not mutually exclusive. Secondly, the immunological features of the family size effect appear to be present in cord blood before the child is born, suggesting that the effect is unrelated to infections acquired in post-natal life, but is more likely due to the mother's increasing immune tolerance of her children in utero. Nevertheless, there is evidence that some infections early in childhood, including measles and hepatititis A and possibly tuberculosis, may protect against later allergies and perhaps asthma. Recent research along these lines has investigated the possibility of temporal changes in the species of micro-organisms colonising the gut as patterns of early diet change, altering immune programming in the infant - in fact, a variant of the dietary hypothesis. Strachan (1989) first proposed the 'hygiene hypothesis' that infections in early childhood prevented the development of allergic diseases. An inverse relationship was observed between family size, particularly the presence of older siblings, and features of allergic disease, including hay fever and positive skin prick test responses, but not with asthma. Recent observations that the prevalence of allergy is reduced in farming communities [von Ehrenstein et al, 2000] might also be explained by increased exposure to infections in early life in this setting, although other differences in lifestyle between rural farming and urban communities are possible confounders of this relationship. T cell responses may be central to the mechanisms of these observed associations. Activated T lymphocytes are important in maintaining lung inflammation in adults with asthma and the demonstration of increased concentrations of soluble interleukin 2 receptors in children with asthma suggests that activated T cells are important in this context also. Atopy in children has been proposed to represent persistence of fetal Th2 responses [Prescott et al, 1999] with the production of type 2 cytokines (interleukins 4, 5, 6, 10, 13) in response to allergens. Infections may be important in early childhood by stimulating Th1 predominant responses (IL 2, interferon, TNF). Survivors of a measles epidemic in Guinea-Bissau were found to have decreased prevalence of atopy compared with immunised children [Shaheen et al, 1996], although the possibility that children with impaired Th1 responses were more susceptible to dying during the epidemic has been raised. Also, exposure to tuberculosis has been shown to result in lower prevalence of atopy, but not asthma, in a large Finnish study [Von Hertzen et al, 1999]. The potential for immune modulation of T helper response by bowel flora and the effect of antibiotics on bowel colonisation has also been studied. These clinical observations together with laboratory studies of T cell sensitisation have led to the development of strategies to modulate the switch from Th2 to Th1 predominant responses, either by allergen avoidance from early gestation [Jones et al, 1998] or by the development of vaccines, Th1 selective adjuvants or immunotherapy.

5 December 2003, version 1 ML-MR20030787 - 27 -
In addition to potential protective effects on later development of asthma, viral respiratory infections have also been proposed as contributors to the development of obstructive airways disease. A number of studies have reported persistent or recurrent wheezing after RSV bronchiolitis in infants . However, there is still debate about whether RSV causes asthma or whether severe RSV infection is a manifestation of pre-existing risk factors for both bronchiolitis and asthma [Sigurs, 2001]. It is hoped that randomised control trials of RSV prophylaxis will be able to address some of these questions but these are currently restricted to high-risk infants.
6.2.2 Diet
The prenatal effects of maternal famine were studied in a Dutch population exposed to the famine of 1944-45. The prevalence of obstructive airways diseases in the offspring of famine-exposed mothers was higher, particularly when the exposure occurred in early gestation. This effect did not appear to be mediated through increased prevalence of atopic disease in this population, suggesting that impairment of fetal lung development was an important factor. A number of dietary constituents have been examined in relation to their potential role in the aetiology of lung diseases, including fatty acids, anti-oxidants and sodium intake. The observation that Eskimos had a low prevalence of lung disease and a diet high in oily fish prompted speculation that n-3 fatty acids, which competitively inhibit the metabolism of arachidonic acid, may be protective against asthma [Schwartz, 2000]. However, there is only weak evidence for this and no intervention studies have yet been done. Oxidative damage to the lungs, mediated through oxygen free radicals, is believed to be important in the pathogenesis of asthma and chronic obstructive pulmonary disease (COPD). Fruit is a major source of antioxidant vitamins and epidemiological associations between fruit intake and lung function in adults have been established. A positive association between fresh fruit consumption and lung function has also been demonstrated in children [Cook et al, 1997]. Selenium is essential to the activity of glutathione peroxidase enzymes that are involved in the lung's antioxidant defences. Low serum concentrations of selenium have been demonstrated in subjects with asthma but it is unclear whether selenium deficiency contributes to the development of asthma or if selenium consumption occurs as a consequence of oxidant injury. A recent ecological study of asthma and allergy (ISAAC) did not demonstrate an increased prevalence in countries in which selenium deficiency is endemic [Moreno-Reyes et al, 1998] compared with areas with abundant dietary selenium sources. Low dose vitamin A supplementation has been examined for its possible protective role in the development of lower respiratory infections in children. Two intervention studies in developing countries have suggested that this effect is strongly related to nutritional status with decreased acute lower respiratory infections observed in underweight children only [Sempertegui al, 1999; Fawzi et al, 2000] and adverse effects noted in children of normal nutritional status. Regional differences in asthma mortality have been correlated with table salt purchase, leading to the possibility that dietary sodium may be an important factor in asthma pathogenesis. However, dietary salt intake in children has been associated with

5 December 2003, version 1 ML-MR20030787 - 28 -
increased bronchial responsiveness to methacholine but not with a diagnosis of asthma or with exercise induced bronchospasm [Demissie et al, 1996].
6.2.3 In utero and infant environment
There is evidence that intra-uterine factors influence risks of asthma and allergies, but not always in the same direction. The strongest associations are with allergic rhinitis, the risks of which are increased in the children of young mothers and decreased in premature and low birthweight children. In contrast, asthma is more likely in children of older mothers and less likely in high birthweight children. Maternal smoking in pregnancy is associated with lower birthweight, reduced lung function and increased respiratory symptoms in the infant, but the effects on longer-term risks of asthma and allergies are equivocal. Breast-feeding, if prolonged for about 6 months or more, appears to protect against early respiratory symptoms, possibly by transfer of immunity, but again effects on longer-term risks of asthma and allergy are equivocal.

5 December 2003, version 1 ML-MR20030787 - 29 -
7 OUTDOOR AMBIENT EXPOSURE/ AMBIENT AIR POLLUTION AND POLLEN
7.1 Introduction
There is clear evidence that atmospheric pollution is associated with troublesome respiratory symptoms in children but what is less clear is whether specific pollutants have a causal role in the pathogenesis of respiratory diseases. The principal pollutants of the external (outdoor) environment include nitrogen oxides (NO, NO2), ozone, sulphur dioxide (SO2) and particulatesThe well documented rise in the prevalence of asthma in industrialised countries has coincided with a general increase in the density of road traffic in the majority of these countries. Therefore a number of studies have investigated the possibility that traffic pollution is an exposure that is associated with respiratory health in children. The following section gives an overview of the current situation and the trends in ambient air pollution in Europe over the recent years for a number of key pollutants (particulate matter, ozone, sulphur dioxide, nitrogen dioxide) and the emissions from road traffic and industry (7.2). This is followed by a description of the respiratory health effects associated with these ambient air pollutants (7.3). Lastly, the respiratory health effects of exposure to pollen are briefly addressed (7.4).
7.2 Ambient air pollution in Europe
Particulate Matter (PM) Concentrations of particulate matter with a cut off size of 10 µm (PM10) in ambient air show a downward tendency between 1996 and 2000. Violations of currently recommended PM10 limit values are widespread in urban areas in Europe, as well in rural areas in some countries [Larsen 2003]. The new EU annual average of 40 µg/m3 that is to be introduced from 2005 has been exceeded at several traffic hot-spots and may de difficult to achieve at such locations . The limit value for average 24-hour concentrations (50 µg/m3 not to be exceeded more than 35 times in a year) was exceeded also at a number of urban and rural background stations. An increase of the PM10 concentration from rural to urban to traffic hot-spot areas is evident. The situation in Russia is likewise of concern: in 1998, 30% of Russian cities did not comply with the World Health Organisation limits for particulate matter [EEA 2003]. The available data for other PM categories such as PM2.5, PM1.0 and the number of ultra fine particles, are still too scarce to draw firm conclusions. Ozone (O3) For ground level ozone the tendency is towards an increasing level for annual average concentrations and a stable level for short term peak concentrations. Violations of the ozone target value are widespread in Europe. Of 1207 stations recorded in AirBase, 275 stations in 12 countries measured levels in excess of the target value, and another 371 had levels above an upper classification level of 100 µg/m3 (as 26th highest daily 8-hour value). Violations occur mainly in South European countries, as well as in Central and Eastern Europe (Switzerland, Austria, South and East Germany, Czech Republic, Slovakia and Poland) [Larsen 2003]. Nitrogen Dioxide (NO2)
5 December 2003, version 1 ML-MR20030787 - 30 -
NO2 shows in Western Europe a downward trend between 1996 and 2000, both for annual and the short-term peak concentrations. The large difference in concentrations from rural to urban to hot-spot is clear. The annual EU limit value is mostly exceeded at traffic sites, and to a lesser extent at some urban background sites. [Larsen 2003]. Sulphur Dioxide (SO2) The urban and local SO2 concentration continues to decrease in most areas in Western Europe, but elevated 24-hour average concentrations of SO2 still represents an air pollution problem in some cities and locations in Europe. In some industrial cities the daily SO2 concentration is still high even at urban background locations. At some hot-spot (industrial type) stations violations of the limit value for 24-hour average occur [Larsen 2002]. Traffic related air pollution NO2, PM10 and PM2.5 are often used as indicators for traffic-related air pollution. In a study in Amsterdam, outdoor levels of these pollutants were 15-22% higher at homes located in high traffic intensity streets compared to low traffic homes [Fischer et al., 2000]. A substantially larger contrast (about a factor 2) was found for components of the particulate matter like polycyclic aromatic hydrocarbons and soot, and gas-phase components like benzene. Difference of a similar magnitude were also found in the indoor air of these homes. Recent studies in a number of European cities have shown that the foreseen limit value for benzene of the EC directive (5 µg/m3 by 2010) is likely to be met in most of Europe except in hot-spot locations and in Eastern and Southern European cities [Jantunen et al., 1998, MACBETH and RESOLUTION projects]. Industry-related air pollution The concentration levels of industry-related air pollution depends on the type of industry, the level of process technology and emission control, as well as the emission conditions. Sulphur dioxide, particulate matter and heavy metals are the most significant pollutants emitted from industrial sources. In most of the EU and EFTA countries, efforts to clean up industrial emissions have substantially reduced such problems, but industrial areas with air pollution exposure exceeding WHO-AQGs still exist. High levels of SO2 exposure occur, for example, in Zlatna and Baia Mare (Romania), Asenovgrad (Bulgaria), Sokolov and Teplice regions (Czech Republic) and in Toru’n (Poland) with annual averages around 500 µg/m3. Non-ferrous metal (cadmium and aluminium) industries and coal-fired power plants are those industries most often responsible for very high local industrial pollution in Europe [EEA, 1995]. PM10 levels in adjacent residential areas near certain types of industrial installations can exceed the urban background by a factor of 2. The areas with elevated concentrations can reach one to several square kilometres. Although the size of the population exposed is limited, the total population in Europe affected may be significant in number since there are several hundreds of such installations all around Europe [CAFE WG on PM 2003].
7.3 Respiratory health effects of exposure to ambient air pollution
There is increasing evidence that levels of the most common air pollutants (PM, O3, NO2 and SO2) adversely affect the respiratory health of children. These health effects vary from post neonatal respiratory mortality [Bobak, 1992; Bobak, 1999] and respiratory mortality in infants (< 5 years) [Saldiva, 1994; Conceicao, 2001], decreased exercise capacity, increased respiratory symptoms, lung inflammation, increased airway
5 December 2003, version 1 ML-MR20030787 - 31 -
reactivity and decreases in lung functions [ATS, 1995]. Recently, the respiratory health effects of the traffic-related part of the air pollution mixture has become the focus of interest [Brauer, 2002]. These health effects have been shown both due to short-term exposures (daily variations in air pollution levels) and due to long-term exposures to air pollution. Currently the role of particles is receiving attention as these may be a major component of the adverse effects of air pollution. . A large number of epidemiological studies have focussed on the respiratory health effects due to short-term exposures to air pollution in non-symptomatic children and in children with asthma or chronic respiratory symptoms. Overall, there is an association between the level of air pollution and the prevalence of respiratory symptoms in both healthy and symptomatic children, although some studies have shown conflicting results [Roemer et al., 1998]. The relationship between exposure to air pollution and the exacerbation of childhood asthma has been well studied although until recently, relatively few studies have focused on traffic-related air pollution. Although short-term increases in air pollution levels have been associated with acute reductions in lung function and increased reporting of respiratory symptoms in children, including asthmatic symptoms , it is not clear whether these effects occur exclusively in asthmatic children, or whether, they also adversely affect children without underlying respiratory disease . Information on the health effects of long-term exposures to air pollution is scarce. In a study in the former East Germany, an association between air pollution levels in the city of residence, presence of chronic respiratory (especially bronchitic) symptoms and lung function growth was found [Frye, 2003]. A study conducted in Switzerland [Braun-Fahrlander, 1997] also found increased occurrence of symptoms with increased air pollution levels in children. Several other studies [Ware et al., 1986; Dockery et al., 1989; Dockery et al., 1996; Raizenne et al., 1996; Baldi et al., 1999] have also found increased bronchitic but not asthmatic symptoms in children and lower lung function at higher air pollution levels. Based on a review of datat from several studies Kuenzli et al. [2000] estimated a 10 µg/m3 increase of the long-term average PM10 concentration was associated with a 31% increase in the prevalence of bronchitic symptoms in children. Studies that have specifically assessed the role of traffic on adverse respiratory health of children suggest that children attending schools located close to major roads and/or living in their vicinity show adverse respiratory health effects. The health effects reported include reduced lung function, higher prevalence of respiratory symptoms including wheeze and higher asthma rates (Wjst et al. 1993; Duhme et al. 1996; Brunekreef et al. 1997). An attempt to quantify this was made in the study by Künzli et al. (Kunzli et al. 2000), who analysed the public health impact of traffic-related air pollution for Switzerland, France and Austria (with a total population of 74 million inhabitants). The authors estimated that in an average year and in the three countries more than 290 000 episodes of bronchitis and more than 160 000 asthma attacks were attributable to exposure to traffic related air pollution Experimental and epidemiological studies among adults have suggested that antioxidant supplementation could modulate the acute change in lung functions observed among people exposed to photo-oxidants [Chatham et al. 1987, Trenga et al., 2001, Grievink et al. 1997, Grievink et al., 1999, Samet et al., 2001]. There is only one study that has

5 December 2003, version 1 ML-MR20030787 - 32 -
assessed the effect of antioxidant dietary supplementation on decrements in pulmonary function associated with exposure to air pollution in children. Romieu et al. [2002] evaluated whether acute effects of ozone, nitrogen dioxide, and PM10 could be attenuated by antioxidant vitamin supplementation. 158 Children with asthma living in Mexico City were randomly given a daily supplement of vitamins (50 mg/day of vitamin E and 250 mg/day of vitamin C) or a placebo. In children with moderate and severe asthma, ozone levels were inversely associated significantly with lung function in the placebo group, while no association between ozone and lung functions was observed in the supplement group. The results suggest that supplementation with antioxidants might modulate the impact of ozone exposure on the small airways of children with moderate to severe asthma. Overall, there is sufficient evidence that exposure to ambient air pollution levels has deleterious respiratory health effects in children. Intervention studies have provided strong circumstantial evidence of the health gains from clean air. One of the best examples is a labour dispute that shut down a large steel mill in Utah Valley [Pope, 1989]. Respiratory hospital admissions in children substantially decreased during the strike and increased to pre strike levels after the dispute was ended. In Hong Kong in 1990 a fuel restriction was introduced that required all power plants and road vehicles to use fuel oil with a sulfur content of not more than 0,5 % by weight. Prevalences of bronchial hyperreactivity in children living in different polluted districts declined on average from 25% to 15% after the fuel restriction [Wong et al 1998]. Another example is the study carried out during the 1996 Summer Olympic Games in Atlanta in which the impact of changes in transportation and community behaviours on air quality and childhood asthma was investigated [Friedman et al 2001]. During these games an alternative transportation strategy was implemented resulting in lower traffic emissions. During the period of the Olympic Games a reduction (41.6%) in the number of childhood asthma acute care events was observed. A study with 110 children investigated whether changes in air quality caused by relocation were associated with changes in lung function growth rates [Avol et al 2001]. As a group, subjects who had moved to areas of lower air pollution levels showed increased growth in lung function and subjects who moved to communities with higher air pollution levels showed decreased growth in lung function [Avol et al 2001]. A stronger trend was found for subjects who had migrated at least 3 years before the follow-up visit than for those who had moved in the pervious 1-2 years [Avol et al 2001]. Another example are several studies on the reduction in respiratory health effects in association with the reduced air pollution levels over several years in the former German Democratic Republic. These studies report a decrease in the prevalence of bronchitis [Heinrich et al 2000, Herbarth et al., 2001], a decrease in prevalence of non-allergic respiratory symptoms [Heinrich et al 2002] and an increase in the mean forced capacity and forced expiratory volume in 1 second in children [Frye et al 2003]. Although the evidence for the contribution of air pollution to exacerbations in children with pre-existing asthma is compelling what is less clear is whether such exposures make any contribution to the cause of asthma. A landmark study of this aspect of lung disease in children was undertaken following the German reunification in 1989. This allowed a study of two genetically similar populations exposed to different levels of atmospheric pollution with higher concentrations of industrial pollutants (SO2 and particulates) in Leipzig, East Germany compared with Munich, West Germany where traffic density was higher. The results of this study demonstrated a higher lifetime prevalence of asthma and a greater prevalence of sensitisation to common aeroallergens

5 December 2003, version 1 ML-MR20030787 - 33 -
in the West German population compared with the East German population, suggesting that prolonged exposure to “classical” air pollutants was not associated with the development of asthma or allegy [von Mutius et al, 1992]. Although the epidemiological evidence is inconclusive, there are data to support a possible role for air pollutants as adjuvants in the process of airway sensitisation to common inhalent allergens The results from some recent studies [Salvi, Frew, Holgate 1999; Diaz-Sanchez et al., 1999 and Janssen et al., 2003] suggest that ambient air pollution, in particular diesel-related compounds, may enhance allergic sensitisation or may increase the allergic response among children who are already sensitised to common allergens.
7.4 Respiratory health effects of exposure to pollen
Specific aeroallergens released from pollen cause hypersensitivity and lead to the allergic diseases rhinoconjunctivitis and urticaria). In Europe pollen allergens may account for 10-20% of allergic disease, particularly rhinoconjunctivitis [D’Amato 1998] although their role in the causation of asthma is unclear. The main allergies are to grasses and birch pollens in Northern and Central Europe, ragweed in Central and Eastern Europe and olive and cypresses in Southern Europe. The burden of IgE-mediated allergic diseases is related to the length of the pollen season, the total pollen counts and the number and level of the pollen peaks and allergen bioavailability [Huynen and Menne, 2003]. Ambient air pollution may increase the prevalence of pollen allergies in highly polluted areas [Ishizaki 1987]. However, no direct correlation has been observed among pollen release, emission peaks of NOx, SO2 and atmospheric fine dust [Behrendt 1991; Ring 2001In a recent study, no additional pro-inflammatory effect of air pollution among children was observed in the pollen season, which suggests that air pollution does not facilitate allergen-induced inflammatory responses [Steerenberg et al., 2003]. There is a growing evidence that global climate change as changing temperature and precipitation might facilitate the geographical spread of particular plant species to new areas which become climatically suitable. Warming is likely to further cause an earlier onset and may extend the duration of flowering and pollen season for some species. The impact of the climate change on the spatial distribution of the incidence and on the severity of allergic disorders is uncertain [Huynen and Menne, 2003].

5 December 2003, version 1 ML-MR20030787 - 34 -
8 INDOOR EXPOSURE /INDOOR ENVIRONMENTAL RISK FACTORS
European children spend more time in indoor than outdoor environments so much so that more than 90% of their waking hours are spent indoors and the burden for many chemical substances with health consequences is much higher than outdoors. The effects of indoor air pollution are of special interest in relation to respiratory health and allergic disorders including asthma. Here the main concern centers around the question as to what extent different exposures give rise to different effects and to what extent these effects in turn translate to health risks. Allergic diseases are, therefore, included in the following report where they are relevant to respiratory health . The coexistence of allergic disease for example in children with asthma is associated with an increased risk of persistence into adult life. [Wolfe et al 2000].
8.1 Exposure scenarios
Depending on the age of the children, the effects of different air pollution exposure conditions can differ widely. As far as indoor exposures are concerned, 3 different environments can be distinguished: 1) the home environment, 2) the child’s outside-the-home environment (day care, Kindergarten, school), 3) environment of recreational activities (swimming pools, etc.) The pollution burden of these different environments, where a child’s daily activities take place, can vary considerably. We have to assume, however, and this has been confirmed in environmental epidemiological studies, that exposure in the home-environment is very important considering the time spent in this environment. Exposure where ′recreational activities‘ take place are specific to that environment and may be recognised as ′hot spots‘ where the exposure burden exceeds the recommended limits. Pollution sources Indoor air pollutants can be classified into chemical, biological or physical agents. It should, however, be pointed out that these may occur as mixtures, be present as a background or may arise simultaneously. Sources of indoor pollution are outdoor emission sources, permanent indoor sources or intermittent indoor sources (e.g., mainly due to human activities or lifestyle habits) Background indoor sources include hazardous building materials and contamination of indoor furnishings, such as furniture and carpets. Intermittent sources are due to human activities and habits, such as smoking, cooking, home renovations or the use of cleaning agents disinfectants or air-fresheners. In addition, the continuous stress on energy-saving policies in environmental politics leads to the situation that less and less air exchange occurs in our homes and office buildings. Thus, to the above mentioned source-dependent pollutants mites, moulds and bacteria may be added. These problems not only arise in the ′cold‘ climates of Central and Northern Europe, but due to the increased use of air conditioners also in the warmer climatic zones of Southern Europe. Respiratory health effects Respiratory illnesses can be acute and short lived or chronic and persistent. Important indoor-pollution-associated diseases include infections of the upper and lower respiratory tract, and non-obstructive pulmonary diseases (simple chronic bronchitis) , irritation of the airways and with respect to allergic disease manifestations rhino

5 December 2003, version 1 ML-MR20030787 - 35 -
conjunctivitis and exacerbations of asthma. Particular indoor-pollution-associated symptoms which may occur include wheezing, cough and bronchial hypersecretion. Current data do not allow a detailed comparison overview in Europe. The reason lies not only in the fact that specific studies in important areas are missing but Europe is plagued with the habit of still not using uniform diagnostic criteria. Although there appears to be a gradient for symptomatic asthma from north west to south east Europe (see section 1) there is considerable overlap in the expression of the disease and for hay fever in the main European regions (Table) [ISAAC, 1998]. region 6-7 years old children 13-14 years old children Wheezing Hay fever Asthma Wheezing Hay fever Asthma North and Eastern Europe
7.3-10.9 0.9-7.5 1.6-8.0 8.1-16.0 3.9-27.4 2.4-10.4
Central and Western Europe
7.2-18.4 2.9-10.6 2.9-22.9 11.6-32.2 11.7-34.8 4.2-20.7
Southern Europe 6.2-13.2 5.3-9.3 5.4-11.0 3.7-10.3 5.9-15.8 4.5-12.1 Data are from ISAAC 1998 expressed as % prevalence ranges. Europe-wide, only a few studies have been concerned with the effects of complex indoor pollution on the respiratory system of children, despite the fact that the dose resulting from a stay indoors generally is above the outdoors-related dose. Examples of these types of studies are: ASMA Asthma study [Liard et al., 2002] BAMSE Barn Allergi Miljö i Stockholm- en Epidemiologisk undersökning (Children
Allergy Environment in Stockholm- an Epidemiological survey [Wickmann et al., 2002]
ECA Environment and Childhood Asthma [Lodrup Carlsen, 2002] KIGA Kindergarten Children Study on Allergies and Airway Diseases [Herbarth et
al., 2001, 1998] LARS Allergy Risk Children Study [Diez et al., 2003; Herbarth et al., 1999] LISA Lifestyle-ImmuneSystem-Allergy Study [Lehmann et al., 2001] MAS Multicentre Allergy Study [Lau et al., 2002] PIAMA Prevention and Incidence of Asthma and Mite Allergy [Brunekreef et al., 2002] A summary presentation of studies can be found under AIRNET (http://airnet.iras.uu.nl/inventory/index.php)
8.2 Exposure
8.2.1 Home Environment
Cigarette smoke Passive smoking or environmental tobacco smoking (ETS) is the indoor pollution variable that has been most intensively studied. Not only does smoking in the presence of a child have an effect on the manifestation of respiratory symptoms but also has an adverse effect on the developing fetus of mothers who smoke. [Burr 1999, Burr et al., 1999]. Exposure to cigarette smoke in utero and in the immediate post natal period is

5 December 2003, version 1 ML-MR20030787 - 36 -
also a major risk factor for sudden infant death (SIDS) (see below). During childhood, wheezing is the most pronounced symptom [Diez et al., 2000, OIE et al., 1999, Zacharasiewicz 1999]. ETS, particularly in utero, leads to a decrease in pulmonary function, increased asthmatic symptoms and an increase in bronchial hyper responsiveness [Lodrup Carlsen 2002, Lodrup Carlsen et al., 2001, Bogacka 2002, Liard et al., 2002]. Whereas postnatal or environmental tobacco smoke (ETS) exposure has a significant influence or respiratory morbidity in the young [Taylor & Wadsworth 1987] the effects of prenatal exposure are likely to be more long lasting. Studies which have assessed lung function soon after birth, when the effects of ETS would be expected to be small have shown evidence of reduced airway function [Hanrahan et al 1992, Young et al 1991]. Whereas it is clearly not possible to identify the exact mechanisms of these effects in humans, animal studies have shown that fetal ETS significantly reduces cell division in the lung as evidenced by reduced DNA, alveolar number and connective tissue within the lung [Collins et al1985, Vidic et al 1989]. A recent systematic review demonstrated a consistent relationship between parents’ smoking and respiratory illnesses and symptoms and middle ear disease in children with odds ratios between 1.2 and 1.6 [Cook & Strachan, 1999]. The odds are greater for preschool children and higher for maternal compared with paternal smoking. The latter observation might be explained by increased exposure to maternal rather than paternal smoking among preschool children. Alternatively, a prenatal effect of maternal smoking on the developing fetal lungs might be responsible. One of the difficulties of disentangling the interrelationships of prenatal and postnatal tobacco smoke exposure on children’s respiratory symptoms in epidemiological studies is the observation that prenatal maternal smoking is almost always associated with postnatal tobacco smoke exposure. However whatever the mechanism it is clear that environmental tobacco smoke exposure (ETS) is an important and potentially remediable cause of respiratory morbidity in the young. Several studies have demonstrated an association between prenatal tobacco smoke exposure and decrements in pulmonary function in infants soon after delivery and before the onset of symptoms. Such decrements appear to be associated with respiratory symptoms during the first year after birth [Martinez et al, 1988; Stick et al, 1996; Dezateux et al, 1999] and it seems likely that in utero smoke exposure causes growth restraint of fetal airways. The longer term effects of such fetal growth restraint have yet to be determined. Recent studies have attempted to examine the differential effects of intrauterine and postnatal tobacco smoke exposure on the outcomes of asthma and wheezing in later childhood. Gilliland and colleagues (2001) have demonstrated associations between in utero exposure and physician diagnosed asthma in later childhood but, although current or past environmental (postnatal) exposure was related to wheezing symptoms, there was not a significant relationship with asthma. The authors speculated that environmental exposure may act as a cofactor for attacks of wheezing but did not appear to be a factor that induced asthma in this population. Parental smoking has also been demonstrated in several case control and cohort studies [Mitchell, 1995] to be significantly associated with sudden infant death syndrome (SIDS). Maternal smoking was associated with increased risk and a dose response effect has been demonstrated in several studies, suggesting a casual relationship, and, although smoking rates vary with socio-economic status, the risk appears to be

5 December 2003, version 1 ML-MR20030787 - 37 -
consistent across socio-economic groups. Fleming and colleagues (1996) in a study of sudden infant death after the ‘Back to Sleep’ campaign in the United Kingdom calculated an odds ratio of SIDS for maternal smoking during pregnancy of 2.1 with an additional independent effect of paternal smoking. The mechanisms for this effect has not been elucidated but fetal lung growth restraint or effects of smoking on neurological responses to thermal, hypoxic or hypercapnic stress have been postulated. ETS also contributes to exacerbation of allergic symptoms [Baier et al., 2002, Diez et al., 2000]. Pre- and post natal ETS exposure increases a child’s sensitisation to food allergens [Kulig et al., 1999, 1999] and changes in the nasal mucous membrane have been observed in genetically predisposed children [Vinke et al., 1999]. Many studies have concentrated on the respiratory health effects of passive exposure to tobacco smoke in children. However, active smoking by children remains a significant health problem. A recent survey of 14-16 year old children revealed that 30% had been active smokers in the previous 12 months, with 14.1% reporting regular smoking [Withers et al, 2000]. Damp housing with mould growth, mite infestation, cockroaches and toxins Due to the ever increasing energy-saving standards, the air exchange between indoor and outdoor air is really limited. The consequence is a build-up of humidity indoors. This promotes the growth of micro-organisms as well as their associated allergens and toxins. The most important role play mites and moulds and occasionally bacterial- and mould-secreted toxins. Indoor allergens are associated with atopic disorders [Timonen et al., 2002] and an increase in adverse respiratory health effects with mites and moulds being the most important [Muller et al., 2002, Burr 2001, Savilahti et al., 2000, Meklin et al., 2002, Jedrychowski et al., 1997, Zureik et al., 2002]. Furthermore, an increase in wheezing, asthma and bronchial hyperresponsiveness [Lau et al., 2000, Zacharasiewicz 1999, 2000] as well as indoor-allergen-associated changes in lung function [Langley et al., 2003] were being observed. Endo- as well as mycotoxins affect allergic and non-allergic airway diseases, whereby endotoxins are assumed to may have a protective effect on the development o allergic sensitisation [Gereda et al., 2002]. An effect of mycotoxins on the immune-competent cells, on the other hand, could experimentally be demonstrated [Wichmann et al., 2002], which allows to conclude that a direct effect on atopic disorders is possible. As far as the lifetime age range for these exposures is concerned, it appears that exposures in the first 3 years have the greatest effect. With increased likelyhood of flooding consequent upon intense periods of rainfall in association with climate change, exposure of children to the conditions of damp housing may increase in the coming years. Presence of pets and other animals The keeping of pets and other animals is being discussed controversially in the literature. On the one hand, findings suggest that pets/animals are associated with an increase in sensitisation towards allergens but, on the other hand, allergy-protective effects have been reported [for an overview see de Blay et al., 2003]. Part of this observed protective effect may be due to avoidance strategies by the parents whose children suffer from hay fever or are already sensitised [Anyo 2002]. Other authors report on marginal effects of animal allergens or no effect at all [Foucard et al., 2000]. Nevertheless, animals with a proven effect on sensitisation rates are pets such as cats and dogs [Langley et al., 2003, Reijonen et al., 2000]. Reijonen and colleagues report especially the effect on dermatitis and asthma. This current controversy may in part be

5 December 2003, version 1 ML-MR20030787 - 38 -
explained by the timing of exposure to animals. Exposure in utero and/or in infancy may result in tolerance to associated animal allergens whereas later exposure to sensitisation and expression of allergic symptoms. Use of polluting fuels for cooking or heating Cooking and heating, particularly, with gas has been found to affect respiratory illnesses in children. Responsible are obviously the NOx. Observed effects were an increase in respiratory diseases [Burr 1999] and respiratory infections, an increase in the susceptibility to asthma [de Marco, 2001] and the occurrence of bronchial asthma and allergic disease [Bogacka, 2002] as well as changes in lung function [Corbo et al., 2001]. It can be assumed that especially the extensive use of cleaning agents may influence the respiratory health of children. Studies about it do not exist. There are some indications that these substances (occupational environment) may affect the respiratory system of adults. Indoor chemicals from building materials, paintings, carpets and furniture Indoor chemicals are found in any indoor environment. High concentrations occur especially following renovation activities or renewal of the furnishings. Exposure to these chemicals affect airway diseases, in particular, wheezing, respiratory symptoms and asthma, as well as allergic disorders in children [Diez et al., 2003, 2000; Herbarth et al., 2003; Clarisse et al., 2002; Jaakola et al., 2000; de Blay et al., 1999]. Important here is early exposure, possibly even exposure during pregnancy [Herbarth et al., 2003]. Critical is that parents, more often than not, carry out these home renovation activities just in time when they are expecting a baby and that just before birth. The effects of volatile organic compounds (VOC) on the immune system could experimentally be determined, which may in part explain these health effects [Lehmann et al., 2002a, 2002b, 2001]. It could also be shown that exposure to indoor chemicals during early childhood increases the risk to microbiological-dependent airway diseases [Diez et al., 2000]. This appears related to irritations of the nasal and respiratory tract mucosa, which besides VOC and SVOC may be due to the effects of among others phthalate plasticisers and flame retardants [Kimmel et al., 2000]. Aldehydes and glycol-compounds are also suspected to adversely affect the respiratory system.
8.2.2 The School environment
Day-care and preschool children The influence of the non-domestic indoor environment on the respiratory health of infants and young children in day care and Kindergartens has not been extensively investigated, but it is likely that the same factors as those described for the home environment will operate. Consequently, efforts should be directed at controlling or reducing exposure to environmental tobacco smoke, allergens (including moulds), gases originating from cooking and heating appliances, and VOCs from cleaning agents, disinfectants, building materials and outdoor (traffic) air pollution. School children Similar considerations apply to children of school age. With increasing age, appropriate preventive efforts should be conducted to prevent and delay the initiation of tobacco smoking. This should include a total ban on smoking in school premises, including by

5 December 2003, version 1 ML-MR20030787 - 39 -
teachers and staff. The detrimental effects of cannabis smoking on the respiratory tract should not be ignored. In adolescents, a special attention should be devoted to pupils following vocational or technical education. Practical classes and on-the-job training may involve hazardous exposures (e.g. welding, woodworking, food industry, animal handling) for which appropriate legislative, technical and educational provisions should be available. The teaching of preventive attitudes in these pupils is likely to be of critical importance for their future careers. Occupational asthma has been shown to occur already in students and apprentices in at risk jobs (bakers, hair dressers, spray painters, animal technicians). Competent school health services should be available to provide appropriate counseling for choosing a particular type of education and future job that is compatible with the child’s health state (atopy, asthma, cystic fibrosis).
8.2.3 Other indoor environments
Recreation and sports It is well known that physical exercise during play and sports results in a higher exposure of the airways and lungs to higher amounts of pollutants, such as ozone, than at rest. It is, therefore, of importance that sports can take place in areas with the cleanest possible environment. The practice of sports in cold areas has been shown to affect asthma. During recreation, children may also spend time indoors in youth clubs, sports halls, and swimming pools, etc. Recent studies have indicated that the release of chloramines in the air of chlorinated swimming pools may represent a significant hazard for respiratory health [Bernard et al. 2003].
5 December 2003, version 1 ML-MR20030787 - 40 -
9 GAPS IN KNOWLEDGE
• Constituents of the indoor environment that impact on respiratory health of children. Focus on new building materials and agents used within the home.
• Interaction between external and internal (home) environments. • European definitions of chronic childhood respiratory symptoms particularly
bronchitis and asthma. • Evidence based reviews of environmental hazards possibly relevant to childhood
respiratory health. • Important gene/environmental interactions and identification of susceptible
population sub groups. • Medium to long term effects of exposures for respiratory health (Birth and child
cohorts). • Effects of exposure to indoor and outdoor air pollution at different stages of
development.
5 December 2003, version 1 ML-MR20030787 - 41 -
10 RECOMMENDATIONS
General • We should recommend other TWG’s to look at Multicausality as thiscould form
a good overall introduction to all diseases TWG’s. Research Needs
• Development of appropriate biomarkers and methodologies for identification of individual genetic susceptibility to respiratory disorders.
• Identification of genes associated with respiratory disorder manifestation and determination of polymorphisms in differentially expressed genes, which would predispose individuals to exacerbate respiratory disorders in the presence of specific environmental triggers and promoters.
• Medium to long term consequences of exposures in early life. Indicators for environmental respiratory health
• Genetic susceptibility data accounting for regional and ethnic differences in the EU population. This set of indicators would help identify “intelligent” cost-effective strategies for prevention of the onset and exacerbation of children respiratory health disorders.
• Where is the evidence sufficient for public health action?

5 December 2003, version 1 ML-MR20030787 - 42 -
11 CONCLUSIONS
Environmental factors play an important role in altering host resistance to respiratory diseases in childhood. It is likely that the accession of a number of former Soviet Union countries to the European Community will be accompanied by changes in the patterns of disease among children in those countries. These are likely to include increases in asthma and allergic conditions and decreases in serious and life threatening infections. It is recommended that prospective research be targeted at such changes in order to establish likely causative factors and methods of intervention. The factors most likely to be associated with benefits to children's respiratory health are those with other general benefits, namely good housing and nutrition, avoidance of exposure to cigarette smoke, active encouragement of physical exercise in a clean air environment and avoidance of obesity, and good health care including immunization programmes. It is recommended that steps be taken to encourage physical activity and a good balanced diet in children, with adequate amounts of fresh fruit and vegetables, to discourage parental smoking and to provide maintain clean air both in the internal (home) and external environment. Many environmental factors thought to influence children's respiratory health remain unclear and sometimes controversial. This is especially the case with respect to asthma and allergies. Since it is likely that these conditions will increase in a number of European countries over the next decade, it is important to target research towards this area. Hence the recommendations to investigate the influence of the environmental and potentially modifiable factors while recognising that the risk factors may differ between the respiratory diseases and symptoms of childhood. Once these issues have been clarified, it is recommended that Community-wide intervention trials be carried out. It is highly unlikely that there is any single measure that will reverse the rise in asthma and allergies in prosperous countries, since these diseases have multiple interacting causes. There is therefore a need to address all the identifiable risk factors and to establish the evidence base for whole population interventions by systematic reviews of existing evidence and by further research in the areas of uncertainty including the medium to long term outcomes of exposures in early life.

5 December 2003, version 1 ML-MR20030787 - 43 -
12 REFERENCES
Amato D’, (1998). D’Amato G., Spieksma F., Liccardi G. et al. Pollen-related allergy in Europe. Allergy, Vol 53, pp. 567-78. Anderson GG, Morrison JFJ. 1998; Molecular biology and genetics of allergy and asthma. Arch Dis Child 78: 488-96. Anderson HR, Pottier AC, Strachan DP., (1992) Asthma from birth to age 23: incidence and relation to prior and concurrent atopic disease. Thorax;47:537-42.
Anyo G, Brunekreef B, de Meer G, Aarts F, Janssen NA, van Vliet P., (2002). Early, current and past pet ownership: associations with sensitization, bronchial responsiveness and allergic symptoms in school children. Clin Exp Allergy, Mar;32(3):361-6. ATS, (1995). American Thoracic Society, Health effects of outdoor air pollution. Am J Avol EL, Gauderman WJ, Tan SM, London SJ, Peters JM., (2001). Respiratory effects of relocating to areas of differing air pollution levels. American Journal of Critical Care Medicine, 164: 2067-2072. Baier G, Stopper H, Kopp C, Winkler U, Zwirner-Baier I., (2002). Respiratory diseases and genotoxicity in tobacco smoke exposed children. Laryngorhinootologie, Mar;81(3):217-25. Barker D, Godfrey K, Fall C, Osmond C, Winter P, Shaheen S., (1991). Relation of birth weight and childhood respiratory infection to adult lung function and death from chronic obstructive airways disease. Br.Med.J., 303:671-5. Behrendt, (1991). Behrendt H., Frierichs K., Kainka-Stanicke E., Darsow U., Becker W., Tomingas R. Allergens and pollutants in the air a complex interaction. Ring J, Prybilla B (eds) New Trends in Allergy III, pp 467-478. Bieber, (1992). Bieber T, De la Salle H., Wollenberg A., Hakimi J., Chizzonite R., Ring J., Hanau D., De la Salle C. Human Langerhans cells express the high affinity receptor for immunoglobulin E (FcERI). J Exp med, 175: 1285-1290. Blay F. de, Birba E., (2003). Controlling indoor allergens. Curr Opin Allergy Clin Immunol, Jun;3(3):165-8. Blay F. de, Lieutier-Colas F., (1999). Domestic pollution (other than tobacco). Allerg Immunol (Paris), Oct;31(8):268-77. Bobak M, Leon DA, (1992). Air pollution and infant mortality in the Czech Republic, 1986-88. Lancet, 340 (8826): 1010-4. Bobak M, Leon DA, (1999). The effect of air pollution on infant mortality appears specific for respiratory causes in the post-neonatal period. Epidemiology, 10 (6): 666-70.

5 December 2003, version 1 ML-MR20030787 - 44 -
Bogacka E., (2002). Health threats for children in the modern building trade. Pol Merkuriusz Lek. Feb;12(68):143-6. Brauer M, Hoek G, Van Vliet P, Meliefste K, Fischer PH, Wijga A, et al, (2002). Air pollution from traffic and the development of respiratory infections and asthmatic and allergic symptoms in children. Am J Respir Crit Care Med, 166 (8): 1092-8. Braun-Fahrlander C, Vuille JC, Sennhauser FH, Neu U, Kunzle T, Grize L, Gassner M, Minder C, Schindler C, Varonier HS, Wuthrich B. Respiratory health and long-term exposure to air pollutants in Swiss schoolchildren. Britton JR., (1989). Effects of social class, sex and region of residence on age at death from cystic fibrosis. Br.Med.J., 298:483-7. Brunekreef B, Janssen NA, De Hartog J, Harssema H, Knape M, Van Vliet P, (1997). Air pollution from truck traffic and lung function in children living near motorways. Epidemiology, 8: 298-303. Brunekreef B, Smit J, de Jongste J, Neijens H, Gerritsen J, Postma D, Aalberse R, Koopman L, Kerkhof M, Wilga A, van Strien R., (2002). The prevention and incidence of asthma and mite allergy (PIAMA) birth cohort study: design and first results. Pediatr Allergy Immunol, 13 Suppl 15:55-60. Burr ML, Anderson HR, Austin JB, Harkins LS, Kaur B, Strachan DP, Warner JO, (1999). Respiratory symptoms and home environment in children: a national survey. Thorax, Jan; 54(1):27-32. Burr ML., (1999). Indoor air pollution and the respiratory health of children. Pediatr Pulmonol Suppl, 18:3-5. Burr ML., (2001). Health effects of indoor molds. Rev Environ Health, Apr-Jun;16(2):97-103. Burrows B, Martinez FD, Cline MG, Lebowitz MD., (1995). The relationship between parental and children's serum IgE and asthma. American Journal of Respiratory & Critical Care Medicine, 152: 1497-500. Burrows B,.Taussig LM, (1980). As the twig is bent, the tree inclines (perhaps). Am.Rev.Respir.Dis.,122:813-6. CAFE WG on PM, (2003). Second Position Paper on Particulate Matter. CAFE Working Group on Particulate Matter, Draft version August 20th, 2003. Castro-Rodriguez J, Holberg C, Wright A, et al, (1999). Association of radiologically ascertained pneumonia before age 3 years with asthma like symptoms and pulmonary function during childhood: a prospective study. Am J Respir Crit Care Med, 159: 1891-97. Clarisse B, Seta N, El Hasnaoui A, Terrioux P, Momas I., (2002). How to describe indoor environment in epidemiological studies dealing with respiratory diseases. Rev Epidemiol Sante Publique, Apr;50(2):179-200.

5 December 2003, version 1 ML-MR20030787 - 45 -
Collins MH, Moessinger AC, Kleinerman J, Bassi J, Rosso P, Collins AM et al, (1985). Fetal lung hypoplasia associated with maternal smoking: a morphometric analysis. Pediatr.Res., 19:408-12. Conceicao GM, Miraglia SG, Kishi HS, Saldiva PH, Singer JM., (2001). Air pollution and child mortality: a time-series study in Sao Paulo, Brazil. Environ Health Perspect, 109 Suppl 3: 347-50. Cookson W., (2002). Genetics and genomics of asthma and allergic diseases, Immunol Rev, 190:195-206. Corbo GM, Forastiere F, Agabiti N, Dell'Orco V, Pistelli R, Aebischer ML, Valente S, Perucci CA., (2001). Effect of gas cooking on lung function in adolescents: modifying role of sex and immunoglobulin E. Thorax, Jul;56(7):536-40. Custovic A, Simpson A, Chapman MD, Woodcock A., (1998). Allergen avoidance in the treatment of asthma and atopic disorders. Thorax, 53: 63-72. Dawson B, Illsley R, Horobin G, Mitchell R., (1969). A survey of childhood asthma in Aberdeen. Lancet.; 1 :827-30. Diez U, Kroessner T, Rehwagen M, Richter M, Wetzig H, Schulz R, Borte M, Metzner G, Krumbiegel P, Herbarth O., (2000). Effects of indoor painting and smoking on airway symptoms in atopy risk children in the first year of life results of the LARS-study. Leipzig Allergy High-Risk Children Study. Int J Hyg Environ Health, Mar;203(1):23-8. Diez U, Rehwagen M, Rolle-Kampczyk U, Wetzig H, Schulz R, Richter M, Lehmann I, Borte M, Herbarth O., (2003). Redecoration of apartments promotes obstructive bronchitis in atopy risk infants--results of the LARS Study. Int J Hyg Environ Health, Jun;206(3):173-9. Dodge RR,.Burrows B., (1980). The prevalence and incidence of asthma and asthma-like symptoms in a general population sample. Am.Rev.Respir.Dis. ; 122 :567-75.
Duhme H, Weiland SK, Keil U, Kraemer B, Schmid M, Stender M, Chambless L., (1996). The association between self-reported symptoms of asthma and allergic rhinitis and self-reported traffic density on street of residence in adolescents. Epidemiology, 578-582. EEA, (1995). Stanners D. and Philippe P. (Eds.). Europe's Environment. The Dobris Assessment. EEA, (1999), Europe’s Environment at the Turn of the Century. Health Chapter, European Environment Agency: Copenhagen EEA, (2003). Europe’ environment: the third assessment. Eerdewegh P.V. et al, (2002). Association of the ADAM33 gene with asthma and bronchial hyperresponsiveness. Nature, 418:426-30

5 December 2003, version 1 ML-MR20030787 - 46 -
Fischer PH, Hoek G, Reeuwijk H van, Briggs DJ, Lebret E, Wijen JH van, Kingham S, Elliott PE., (2000). Traffic-related differences in outdoor and indoor concentrations of particles and volatile organice compounds in Amsterdam. Atmospheric Environenment, 34 3713-3722. Fogarty A, Britton J., (2000). The role of diet in the aetiology of asthma. Clin.Exp.Allergy, 30: 615-27. Foucard T., (2000). Is prevention of allergy and asthma possible? Acta Paediatr Suppl., Sep;89(434):71-5. Friedman MS, Powell KE, Hutwagner L, Graham LM, Teague WG., (2001). Impact of changes in transportation and commuting behaviours during the 1996 summer Olympic games in Atlanta on air quality and childhood asthma. The Journal of the American Medical Association, 285: 897-905. Frye C, Hoelscher B, Cyrys J, Wjst M, Wichmann HE, Heinrich J., (2003). Association of lung function with declining ambient air pollution. Environmental Health Perspectives, 111(3):383-387. Fryer AA, Bianco A, Hepple M, Jones PW, Strange RC, Spiteri MA. Polymorphism at the glutathione S-transferase GSTP1 locus, (2000). A new marker for bronchial hyperresponsiveness and asthma. American J Respir Cril Care Med., 161:1437-42. Gehring U, Cyrys J, Sedlmeir G, Brunekreef B, Bellander T, Fischer P, Bauer CP, Reinhardt D, Wichmann HE, Heinrich J., (2002). Traffic-related air pollution and respiratory health during the first 2 yrs of life. European Respiratory Journal, 19: 690-698. Gereda JE, Leung DY, Thatayatikom A, Streib JE, Price MR, Klinnert MD, Liu AH, (2000). Relation between house-dust endotoxin exposure, type 1 T-cell development, and allergen sensitisation in infants at high risk of asthma. Lancet, May 13;355(9216):1680-3. Gilliland FD, Rappaport EB, Berhane K, Islam T, Dubeau L, Gauderman WJ et al, (2002). Effects of glutathione S-transferase P1, M1, and T1 on acute respiratory illness in school children. Am J Respir Crit Care Med., 166:346-51. Gotzsche PC, Hammarquist C, Burr M., (1998). House dust mite control measures in the management of asthma: Meta-analysis. British Medical Journal, 317: 1105-10. Hakonarson H. et al., (2002). A major susceptibility gene for asthma maps to chromosome 14q24. Am J Hum Genet, 71:483-91. Hanrahan JP, Tager IB, Segal MR, Tosteson TD, Castile RG, Van Vunakis H et al, (1992). The effect of maternal smoking during pregnancy on early infant lung function. Am.Rev.Respir.Dis., 145:1129-35. Heinrich J, Hoelscher B, Frye C, Meyer I, Pitz M, Cyrys J, Wjst M, Neas L, Wichmann HE, (2002). Improved air quality in reunified Germany and decreases in respiratory symptoms. Epidemiology, 13(4):394-401.

5 December 2003, version 1 ML-MR20030787 - 47 -
Heinrich J, Hoelscher B, Wichmann HE, (2000). Decline of ambient air pollution and respiratory symptoms in children. American Journal of Respiratory and Critical Care Medicine, 161(6):1930-1936. Helms PJ., (2001). Early environmental influences in the development of asthma and atopic disease. Monaldi Arch Chest Dis: 56: 265-269. Herbarth O, Fritz G, Diez U, Rehwagen M, Borte M, Schulz R, Richter M, Krumbiegel P, Müller A., (1998). Effect of volatile organic compoundas in- and outdoors on allergies. Air Pollution VI Ed. CA Brebbia, CF Ratto, H Power, WITPress Boston, Southhampton. Herbarth O, Fritz G, Krumbiegel P, Diez U, Franck U, Richter M., (2001). Effect of sulfur dioxide and particulate pollutants on bronchitis in children - a risk analysis. Environ Toxicol, Jun;16(3):269-76. Herbarth O, Fritz G, Lehmann I., (2003). Influence of indoor chemical exposure in early childhood on allergic symptoms and disorders. Epidemiology, 14(5) Suppl. 53. Herbarth O., (2003). Epidemiology of air pollution associated allergies children. Bundesgesundheitsbl., 46:732-738. Hislop A, Muir DC, Jacobsen M, Simon G, Reid L., (1972). Postnatal growth and function of the pre-acinar airways. Thorax, 27:265-274. Hogben, L., (1933), Nature and Nurture. Williams and Norgate: London. ISAAC Steering Committee, (1998). Worldwide Variation in Prevalence of Symptoms of Asthma, Allergic Rhinoconjunctivitis, and Atopic Eczema: ISSAC. The Lancet, 351, 1225-1232. Ishii T, Matsuse T, Teramoto S, Matsui H, Miyao M, Hosoi T et al, (1999). Glutathione S-transferase P1 (GSTP1) polymorphism in patients with chronic obstructive pulmonary disease. Thorax, 54:693-6. Ishizaki, (1987). Ishizaki T., Koizumi K., Ikemori R., Ishiyama Y., Kushibiki E. Studies of prevalence of Japanese cedar pollinosis among the residents in a densely cultivared area. Ann Allergy, 58: 265-270 Jaakkola JJ, Verkasalo PK, Jaakkola N., (2000). Plastic wall materials in the home and respiratory health in young children. Am J Public Health, May;90(5):797-9. Jaakkola JJK, Nafstad P, Magnus P, (2001). Environmental tobacco smoke, parental atopy, and childhood asthma. Environmental Health Perspectives, 109:579-582. Jantunen MJ, Hänninen O, Katsouyanni K, Knöppel H, Kuenzli N, Lebret E, Maroni M, Saarela K, Sram R, Zmirou D, (1998). Air pollution exposure in European cities: The "Expolis"-study. JEAEE, 8 (4): 495-518.

5 December 2003, version 1 ML-MR20030787 - 48 -
Jedrychowski W, Flak E., (1997). Respiratory tract symptoms in school children exposed to indoor and outdoor air pollution. Pneumonol Alergol Pol., 65(11-12):741-8. Kay, (2001), Kay A 2001. Allergy and allergic diseases. First of two parts. N Engl J Med, 344: 30-37. Kimmel R, Dartsch PC, Hildenbrand S, Wodarz R, Schmahl FW., (2000). Insufficient ventilation as the etiology of illness perception in an elementary school. Gesundheitswesen, Dec;62(12):660-4. Kjellström et al, (1999),. Late Lessons from Early Warnings. The Precautionary Principle 1896-2000. Ref. From B.P. No 2, EEA, 2001: Copenhagen Kleeberger S.R. et al., (1997). Linkage analysis of susceptibility to ozone-induced lung inflammation in inbred mice. Nature Genetics, 17:475-8. Kleeberger S.R. et al., (2000). Genetic susceptibility to ozone-induced lung hyperpermeability: Role of the toll-like receptor 4 (Tlr4). Am J Respir Cell Mol Biol, 22:620-7. Kueppers F, Miller RD, Gordon H, Hepper NG, Offord K., (1977). Familial prevalence of chronic obstructive pulmonary disease in a matched pair study. Am.J.Med., 63:336-42. Kulig M, Luck W, Lau S, Niggemann B, Bergmann R, Klettke U, Guggenmoos-Holzmann I, Wahn U., (1999). Effect of pre- and postnatal tobacco smoke exposure on specific sensitization to food and inhalant allergens during the first 3 years of life. Multicenter Allergy Study Group, Germany. Allergy, Mar;54(3):220-8. Kulig M, Luck W, Wahn U., (1999). The association between pre- and postnatal tobacco smoke exposure and allergic sensitization during early childhood. Multicentre Allergy Study Group, Germany. Hum Exp Toxicol, Apr;18(4):241-4. Kunzli N, Kaiser R, Medina S, Studnicka M, Chanel O, Filliger P, et al, (2000). Public-health impact of outdoor and traffic-related air pollution: a European assessment. Lancet, 356 (9232): 795-801. Laitinen T. et al., (2001). A susceptibility locus for asthma-related traits on chromosome 7 revealed by genome-wide scan in a founder population. Nature Genetics, 28:87-91. Langley SJ, Goldthorpe S, Craven M, Morris J, Woodcock A, Custovic A., (2003). Exposure and sensitization to indoor allergens: association with lung function, bronchial reactivity, and exhaled nitric oxide measures in asthma. J Allergy Clin Immunol, Aug;112(2):362-8. Larsen 2002. Larsen S. (Ed.), Barrett K.J., Fiala J., Goodwin J., Hagen L.O., Henriksen J.F., de Leeuw F. and Tarrason L., (2003). Air Pollution in Europe, State and Trends 1990-99. European Environment Agency, Topic Report 4/2002.

5 December 2003, version 1 ML-MR20030787 - 49 -
Larsen 2003. Larsen S. (Ed.), Adams M.L., Barrett K.J., Bolscher M.vh., de Leeuw F. and Pulles T., (2003). Air Pollution in Europe, 1990-2000. European Environment Agency, Final Draft – 20 June 2003. Larson RK, Barman ML, Kueppers F, Fudenberg HH., (1970). Genetic and environmental determinants of chronic obstructive pulmonary disease. Ann.Intern.Med., 72:627-32. Lau S, Illi S, Sommerfeld C, Niggemann B, Bergmann R, von Mutius E, Wahn U., (2000). Early exposure to house-dust mite and cat allergens and development of childhood asthma: a cohort study. Multicentre Allergy Study Group. Lancet, Oct 21;356(9239):1392-7. Lau S, Nickel R, Niggemann B, Gruber C, Sommerfeld C, Illi S, Kulig M, Forster J, Wahn U, Groeger M, Zepp F, Kamin W, Bieber I, Tacke U, Wahn V, Bauer CP, Bergmann R, von Mutius E; MAS Group, (2002). The development of childhood asthma: lessons from the German Multicentre Allergy Study (MAS). Paediatr Respir Rev, 3(3):265-72. Lehmann I, Rehwagen M, Diez U, Seiffart A, Rolle-Kampczyk U, Richter M, Wetzig H, Borte M, Herbarth O; Leipzig Allergy Risk Children Study, (2001). Enhanced in vivo IgE production and T cell polarization toward the type 2 phenotype in association with indoor exposure to VOC: results of the LARS study. Int J Hyg Environ Health, Dec;204(4):211-21. Lehmann I, Thoelke A, Rehwagen M, Rolle-Kampczyk U, Schlink U, Schulz R, Borte M, Diez U, Herbarth O., (2002). The influence of maternal exposure to volatile organic compounds on the cytokine secretion profile of neonatal T cells. Environ Toxicol, 17(3):203-10. Lehmann I, Thoelke A, Weiss M, Schlink U, Schulz R, Diez U, Sierig G, Emmrich F, Jacob B, Belcredi P, Bolte G, Heinrich J, Herbarth O, Wichmann HE, Borte M., (2002). T cell reactivity in neonates from an East and a West German city--results of the LISA study. Allergy, Feb;57(2):129-36. Leonardi GS, Houthuijs D, Nikiforov B, Volf J, Rudnai P, Zejda J, et al, (2002). Respiratory symptoms, bronchitis and asthma in children of Central and Eastern Europe. Eur Respir J, 20 (4): 890-8. Liard R, Soussan D, Zureik M, Touron D, Lepage T, Martinat Y, Rogeaux Y, Neukirch F., (2002). Development over 3 years of asthma recently diagnosed in a cohort of children (ASMA study). Factors related to improvement in clinical. Presse Med, 13;31(14):637-43 LIFE RESOLUTION project : Final results of Paris campaign. AIRPARIF, February 2003. Lodrup Carlsen KC, (2002). The environment and childhood asthma (ECA) study in Oslo: ECA-1 and ECA-2. Pediatr Allergy Immunol, 13 Suppl 15:29-31.

5 December 2003, version 1 ML-MR20030787 - 50 -
Lodrup Carlsen KC, Carlsen KH., (2001). Effects of maternal and early tobacco exposure on the development of asthma and airway hyperreactivity. Curr Opin Allergy Clin Immunol, Apr;1(2):139-43. Luyt DK, Burton PR, Simpson H., (1993). Epidemiological study of wheeze, doctor diagnosed asthma, and cough in preschool children in Leicestershire. BMJ 1993; 306:1386-90.
MACBETH project : Cocheo, V., De Saeger, E., Pérez Ballesta, P. et al, (2000). Urban benzene and population exposure. Nature 404, 141-142, 9 March. Marco R. de, (2001). Contribution of epidemiologic research to the knowledge on the etiology of asthma. Recenti Prog Med., Sep;92(9):513-20. Meklin T, Husman T, Vepsalainen A, Vahteristo M, Koivisto J, Halla-Aho J, Hyvarinen A, Moschandreas D, Nevalainen A., (2002). Indoor air microbes and respiratory symptoms of children in moisture damaged and reference schools. Indoor Air, Sep;12(3):175-83. Metzeger, (1984). Metzger H, Rivnay B, Henkart M, Kanner B, Kinet J, Perez-Monfort R. Analysis of the structure and function of the receptor for immunoglobulin. Mol Immunol, 21: 1167-1173 Muller A, Lehmann I, Seiffart A, Diez U, Wetzig H, Borte M, Herbarth O., (2002). Increased incidence of allergic sensitisation and respiratory diseases due to mould exposure: results of the Leipzig Allergy Risk children Study (LARS). Int J Hyg Environ Health, Feb;204(5-6):363-5. Mutius E. von, Fritzsch C, Weiland SK, Röll G, Magnussen H. 1992; Prevalence of asthma and allergic disorders among children in united Germany: a descriptive comparison. BMJ 305: 1395-99. Oie L, Nafstad P, Botten G, Magnus P, Jaakkola JK., (1999). Ventilation in homes and bronchial obstruction in young children. Epidemiology, May;10(3):294-9. Osman M., (2003) Therapeutic implications of sex differences in asthma and atopy. Arch.Dis.Child.;88:587-90.
Peat, (1996). Peat J.K. , Tovey E., oelle B.G., et al. House dust mite allergens: A major risk factor for childhood asthma in Australia. AmJ Respir Crit Care Med, Vol 1532, pp 141-6. Polgar G, Weng TR., (1979). The functional development of the respiratory system. Am Rev Respir Dis, 120:625-695. Pope CA, 3rd., (1989). Respiratory disease associated with community air pollution and a steel mill, Utah Valley. American Journal of Public Health, 79: 623-628. Price, (1992). Price S, Wilson L. Pathophysiology: Clinical concepts of disease processes. Mosby Year Book, St. Louis.

5 December 2003, version 1 ML-MR20030787 - 51 -
Reijonen TM, Kotaniemi-Syrjanen A, Korhonen K, Korppi M., (2000). Predictors of asthma three years after hospital admission for wheezing in infancy. Pediatrics, Dec;106(6):1406-12. Respir Crit Care Med, Vol 153, pp. 3–50. Ring, (2001). Ring J., Kramer U., Schafer T., Behrendt H. Why are allergies increasing? Curr Opin Immunol, 13:701-708. Saldiva PH, Lichtenfels AJ, Paiva PS, Barone IA, Martins MA, Massad E, et al, (1994). Association between air pollution and mortality due to respiratory diseases in children in Sao Paulo, Brazil: a preliminary report. Environ Res, 65 (2): 218-25. Savilahti R, Uitti J, Laippala P, Husman T, Roto P., (2000). Respiratory morbidity among children following renovation of a water-damaged school. Arch Environ Health, Nov-Dec;55(6):405-10. SCARPOL Team, (1997). Swiss Study on Childhood Allergy and Respiratory Symptoms with Respect to Air Pollution, Climate and Pollen. Am J Respir Crit Care Med., Mar; 155(3):1042-9. Seaton A, Godden DJ, Brown K., (1994). Increase in asthma: A more toxic environment or a more susceptible population? Thorax, 49: 171-4. Senna, (1997). Senna G., Dama A., Crivellaro M., Gani F., Mezzelani P. The epidemiology of allergic respiratory disease. Many questions, few answer. Rec Prog in Med, Vol 88 N 7-8 pp 303-8. Shaheen SO, Barker DJ, Holgate ST., (1995). Do lower respiratory tract infections in early childhood cause chronic obstructive pulmonary disease? Am J Respir Crit Care Med, 151: 1649-51. Strachan DP, (1989). Hay fever, hygiene and household size. BMJ: 299: 1259-60. Taking a world view of asthma, (2002). Environmental Health Perspectives, vol. 110(9): A514-515. Talal N., (1992) Sex Hormones and Immunity. In Roitt I, ed. Encyclopedia of Immunology, pp 1369-71. Academic Press.
Taylor B,.Wadsworth J., (1987). Maternal smoking during pregnancy and lower respiratory tract illness in early life. Arch.Dis.Child, 62:786-91. Timonen KL, Schwartz J, Nielsen J, Brunekreef B., (2002). Associations between markers of respiratory morbidity in European children. Eur Respir J., Mar;19(3):479-86. Venn A, Lewis S, Cooper M, Hill J, Britton J., (1998). Questionnaire study of effect of sex and age on the prevalence of wheeze and asthma in adolescence. BMJ; 316:1945-6. Vidic B, Ujevic N, Shabahang MM, van de Zande F., (1989). Differentiation of interstitial cells and stromal proteins in the secondary septum of early postnatal rat: effect of maternal chronic exposure to whole cigarette smoke. Anat.Rec., 223:165-73.

5 December 2003, version 1 ML-MR20030787 - 52 -
Vinke JG, KleinJan A, Severijnen LW, Fokkens WJ., (1999). Passive smoking causes an 'allergic' cell infiltrate in the nasal mucosa of non-atopic children. Int J Pediatr Otorhinolaryngol, Dec 5;51(2):73-81. Wahn, (1997). Wahn U ., Bergmann R., Kulig M., et al. The natural course of sensitisation and atopic diseases in infancy and childhood. Pediatr Allergy immunol, Vol 8 (suppl 10), pp. 16-20. Whitacre, CC, Reingold SC, O'Looney PA., (1999). A gender gap in autoimmunity. Science ;283 :1277-8.
Wichmann G, Herbarth O, Lehmann I., (2002). The mycotoxins citrinin, gliotoxin, and patulin affect interferon-gamma rather than interleukin-4 production in human blood cells. Environ Toxicol, 17(3):211-8. Wickmann M, Kull I, Pershagen G, Nordvall SL., (2002). The BAMSE project: presentation of a prospective longitudinal birth cohort study. Pediatr Allergy Immunol, 13 Suppl 15: 11-13. Wjst M, Reitmeier P, Dold S, Wulff A, Nicolai T, von Loeffelholz-Colberg EF, von Mutius E., (1993). Raod traffic and adverse effects on respiratory health in children. British Medical Journal, 307: 596-600. Wong CM, Lam TH, Peters J, Hedley AJ, Ong SG, Tam AY, Liu J, Spiegelhalter DJ., (1998). Comparison between two districts of the effects of an air pollution intervention on bronchial responsiveness in primary school children in Hong Kong. Journal of Epidemiology and Community Health, 52(9):571-578. Xu J. et al., (2001). Genomewide screen and identification of gene-gene interactions for asthma-susceptibility loci in three US populations: Collaborative study on the genetics of asthma. Am J Hum Genet, 68:1437-46. Yokouchi Y. et al., (2000). Significant evidence for linkage of mite-sensitive childhood asthma to chromosome 5q31-q33 near the interleukin 12 B locus by a genome-wide search in Japanese families. Genomics, 66:152-60. Young Kreeger K., (2003). Asthma, genetics and the environment. The Scientist 17(7). Young S, Le Souef PN, Geelhoed GC, Stick SM, Turner KJ, Landau LI., (1991). The influence of a family history of asthma and parental smoking on airway responsiveness in early infancy. N.Engl.J.Med., 324:1168-73. Zacharasiewicz A, Zidek T, Haidinger G, Waldhor T, Suess G, Vutuc C., (1999). Indoor factors and their association to respiratory symptoms suggestive of asthma in Austrian children aged 6-9 years. Wien Klin Wochenschr, Nov 12;111(21):882-6. Zacharasiewicz A, Zidek T, Haidinger G, Waldhor T, Vutuc C, Zacharasiewicz A, Goetz M, Pearce N., (2000). Symptoms suggestive of atopic rhinitis in children aged 6-9 years and the indoor environment. Allergy, Oct;55(10):945-50. Zureik M, Neukirch C, Leynaert B, Liard R, Bousquet J, Neukirch F; European Community Respiratory Health Survey, (2002). Sensitisation to airborne moulds and

5 December 2003, version 1 ML-MR20030787 - 53 -
severity of asthma: cross sectional study from European Community respiratory health survey. BMJ, Aug 24;325(7361):411-4.

5 December 2003, version 1 ML-MR20030787 - 54 -
ANNEX 1 MANDATE OF THE SUB-GROUP RESPIRATORY HEALTH
DRAFT (16.9.2003) Mandate : “Indicators and priority diseases”
Introduction The EU Environment and Health Strategy puts a particular emphasis on improving understanding of the links between environmental factors and key diseases and conditions. For the first cycle, three priority disease areas have been identified: childhood cancers, neurodegenerative diseases, and respiratory diseases, asthma and allergies. The underlying environmental factors, determinants and risks which contribute to these diseases are similar. Moreover, in addressing the diseases and developing actions in the Community framework, a similar set of instruments is being used.
The development of indicators and the identification of priority diseases is closely linked. The work on European Health and Environment indicators will therefore take place as part of the developing European health information system.
Work on these issues will therefore be taken forward in an integrated way. One overall group on ‘Indicators and priority diseases’ will be created to ensure that synergies between the different areas are properly explored. The meetings will include breakout sessions to discuss specific issues related to the different subject areas (see specific sub-mandates).
Tasks In all areas set out below, a similar structure of work will be pursued: Step 1 : definition of the baseline
The WG should first provide a Baseline Report (end of December 2003) on indicators and on the priority diseases, including :
an overview of the existing state of knowledge and activities, including an appraisal of problems and deficits of current activities
advantages of developing work at EU level;
requirements for EU activities;
Assess the adequacy/scope of proposed actions/priorities
Step 2 : establishment of options for action & recommendations
On the basis of the outcome of the previous tasks, the Working Group will then establish options for action and recommendations for the Commission’s “AP 2004-2010”.
Links with other TWGs should be ensured in step 1 as well as in step 2.
Chairs The Working Group will be chaired by the Commission (M. Rajala, DG SANCO) and co-chaired by … Co-ordinators will be appointed to follow work in the four specific areas (see attached sub-mandates).
Members, Location The list of members will be established after the Preliminary Meeting of the Consultative Group on 10/9. They will include members nominated by the High Level Committee on Health and the EU Health Forum. Moreover, the European Environment Agency and other Commission

5 December 2003, version 1 ML-MR20030787 - 55 -
services (ENV, RTD, JRC…) will be invited to attend. Technical support will be provided through a contract concluded by DG ENV.
The meetings will take place in Luxembourg (possibly also in Brussels or Ispra). Co-ordination, work methods, planning and deliverables Guidelines and requirements common to all groups are specified in the Framework Mandate and in the Co-ordination Mandate.
Detailed planning is to be established by the chair and co-chair, and the co-ordinators, in consultation with the Commission services.
***

5 December 2003, version 1 ML-MR20030787 - 56 -
Sub-Mandate : “Childhood respiratory diseases, asthma, allergies” INTRODUCTION An estimate of mortality due to long-term exposure in 124 European cities (for a total of 80 million inhabitants), showed that around 60 000 deaths per year may be associated with the long-term exposure to particulate air pollution exceeding the level1 in the 124 cities with particulate matter data. Children are particularly affected. Over the last few decades, asthma and allergies have increased throughout Europe. On average, 10% of children suffer from asthmatic symptoms. For 1995-1996, the International Study of Asthma and Allergies in Childhood (ISAAC) found an 11.5% annual average prevalence of self-reported asthma symptoms in children aged 13–14 years. In Western Europe, the symptom rate is up to ten times than in eastern countries. This suggests that a western lifestyle is associated with allergic diseases in childhood. Environmental tobacco smoke and air pollution are among the major threats to respiratory health, especially early in life, and are likely to worsen asthma. Environmental tobacco smoke increases the risk of lung cancer in non-smokers by 20-30 %.2 Also women are particularly exposed to passive smoking. It is estimated that the majority of the 1000 deaths/year from lung cancer in non-smokers in the 15 EU countries are females. Problems identified Improve understanding of the links between environmental factors and respiratory diseases, and to develop specific actions which could be taken up in the first cycle of the European Environment and Health action plan. Objectives/Tasks of the Group Step 1 : definition of the baseline The Group will first define a baseline including :
• Providing an overview of the studies or programmes in the Member States and Acceding Countries investigating childhood respiratory diseases, asthma and allergies and its relationship to environmental exposures.
• Identifying gaps in knowledge regarding environmental exposures and childhood respiratory diseases and allergies.
• Assessing the identification of unrecognised causal links between environmental agents and childhood allergies, respiratory diseases and asthma.
The result of this first step will be a « Baseline Report » to be presented by the end of December 2003.
Step 2 : establishment of options for action & recommendations
On the basis of the outcome of the first step, the Group will then :
1 equivalent to particulate matter 10 = 5mg/m3. “Europe’s environment: the third assessment”
European Environment Agency, Copenhagen (2003)
2 “Europe’s environment: the third assessment” European Environment Agency, Copenhagen (2003)

5 December 2003, version 1 ML-MR20030787 - 57 -
• Establishing options for actions and recommendations for the Commission’s “AP 2004-2010”. In particular proposals for :
– preventive actions
– the establishment of monitoring/epidemiological surveillance programmes in areas at risk
– gaps in knowledge.
• Each recommendation or option presented will be accompanied by a justification of the choices, the practicability, the estimated impacts and costs involved, the time lines and the interlinkages with other measures or policies.
The links with other TWGs (e.g. dioxins, heavy metals, …) and the work in other sub-groups of the indicators and priority diseases group should be ensured.
Chairs The co-ordinator for this area will be …………, assisted by …
Members Members will be assigned after the Preliminary Meeting of the Consultative Group on 10/9.
Co-ordination, work methods, planning and deliverables Guidelines and requirements common to all groups are specified in the Framework Mandate and in the Co-ordination Mandate.
Detailed planning is to be established by the chair and co-chair, in consultation with the Commission services.
***

5 December 2003, version 1 ML-MR20030787 - 58 -
ANNEX 2 MEMBERS OF THE SUB-GROUP RESPIRATORY HEALTH
TWG Members (participating in the writing of the baseline report) Name Organization Jan Zejda (chair) Medical University of Silesia, Poland Peter Helms (co-chair) University of Aberdeen, UK Silvia Brini APAT, National Agency for Environment and
Technical Services, Italy David Gee EEA, European Environment Agency, Denmark Danny Houthuijs RIVM, Netherlands Dirk Pallapies BASF AG Benoit Nemery Katholieke Universiteit Leuven, Belgium Anthony Seaton IOM Edinburgh, UK Isabella Annesi-Maesano INSERM, France Daniela Parola Universita La Sapienza, Italy Denis Sarigiannis Europ. Commission JRC Giovanni De Santi European Commisssion, DG JRC Bettina Menne WHO Olf Herbarth UFZ Center for Environmental Research Leipzig-
Halle Ulrich Wahn EAACI, European Academy of Allergology and
Clinical Immunology, Denmark

5 December 2003, version 1 ML-MR20030787 - 59 -
COLOPHON
ML-MR20030787
Client : Error! Reference source not found. Project : Baseline Report on Respiratory Health in the framework of
the European Environment and Health Strategy (COM(2003)338 final)
File : V1849-65.001 Length of report : 59 pages Contributions : TWG Respiratory health Coordinators : Peter Helms, Jan Zejda Technical secretary : Peter van den Hazel, Anders van der Velden Date : 5 December 2003 Name/Initials :