background to the falsified medicines directive and the delegated regulation
TRANSCRIPT
Susan Grieve, Principal Pharmacist, Department of Health
Background to the Falsified Medicines Directive and theDelegated Regulation
12 April 2016

2
Background to the Falsified Medicines Directive and theDelegated Regulation
Susan Grieve
3
Directive Overview• Council Directive 2011/62/EC • To reduce the occasions on which falsified medicines enter the
legitimate supply chain• A secure supply chain from excipient suppliers through
manufacturers, wholesalers, and pharmacists
4
DefinitionAny medicinal product with a false representation of: • its identity, including its packaging and labelling, its name or its
composition as regards any of the ingredients including excipients and the strength of those ingredients;
• its source, including its manufacturer, its country of manufacturing, its country of origin or its marketing authorisation holder; or
• its history, including the records and documents relating to the distribution channels used
5
6
Safety FeaturesIntroduced to enable wholesale distributors and those who supply to patients:• to verify the authenticity of the medicinal product,• to identify individual packs, • to verify, by means of a device, whether the outer packaging
has been tampered with
7
Safety features (Continued)• Unique identifier • Tamper evident packaging• Affects
• all prescription medicines (unless exempted) • no P or GSL products (unless an issue of falsification has
been notified)
8
Unique Identifier (UI)• Composition of the UI
– Sequence of alpha-numeric or numeric characters given to individual pack– Product Code enabling the identification of the name, common name, pharmaceutical form
and strength as a minimum– A serial number which is numeric or alphanumeric sequence maximum 20 characters – A national reimbursement number if required by MS– Batch number– Expiry date
• 2 dimensional data matrix barcode• Human readable format in addition• No other codes may be displayed
9
Tamper Evidence• Medicines required to include the safety features need to
include anti-tampering devices• There are already approved standards • Choice will be for the MAH/manufacturer to determine
10
Verification and Decommissioning • General provisions on the verification of the safety features
– Check the UI against the numbers held in the repository– Ensure the tamper-evident feature is intact
• At the point of supply the UI will be “checked-out” of the repository (decommissioned)
• Provision is made for– Part packs – When there are technical problems
• The UI can be checked back into the repository in certain circumstances
11
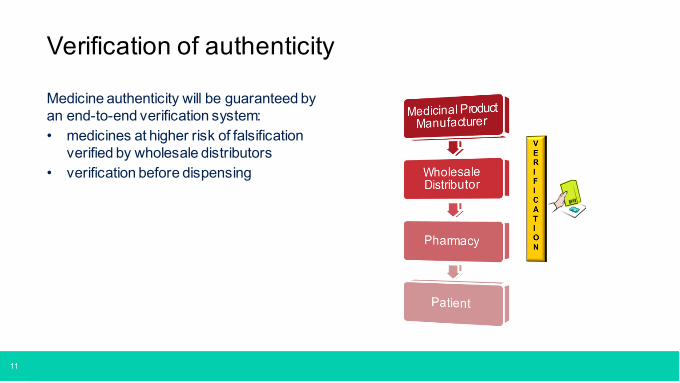
Medicine authenticity will be guaranteed by an end-to-end verification system:• medicines at higher risk of falsification
verified by wholesale distributors• verification before dispensing
Verification of authenticity

12
Establishing the Repository• Manufacturers and marketing authorisation holders (MAHs) will establish the repository• Others in the supply chain will be consulted• Managed by not-for profit legal entity• Costs of the repository will be met by MAHs and manufacturers• Central EU hub along with national or supra-national local repositories• Must be inter-operable and allow connection by pharmacies and others who supply
medicines• Data protection and ownership is accommodated• National Competent Authority (NCA) will have access
– Supervision and investigating potential incidents– Reimbursement– Pharmacovigilance or phamacoepidemiology
13
The Flexibilities – The Unique Identifier/Safety Feature • Member states may
– Extend the products to which the unique identifier/safety feature applies – Require a national reimbursement number to be within the data elements of the unique
identifier• Member states may allow
– Manufacturer to put additional information in the bar code
14
The Flexibilities – Decommissioning • Member states may require
– that a wholesaler verifies and decommissions the unique identifier before supplying the medicines to those who supply medicines to the public (however this flexibility CANNOT apply to ‘healthcare institutions’ or ‘pharmacies’).
– that a wholesaler verifies and decommissiosn the unique identifier before supplying to a healthcare institution if the healthcare institution and the wholesaler are the same legal entity. (Healthcare institution is defined).
• Where verification and decommission takes place earlier than the point of supply the integrity of anti tampering device still needs to be verified at the point of supply.
• Healthcare institutions can verify and decommissioning at any point that the medicines is in the possession of the healthcare institution.
• Provision is made for samples and medicines which cannot be supplied or returned to the wholesaler.
15
Implementation Challenges• Scale and complexity
– All parties in the supply chain– In primary care alone there nearly a billion prescriptions each one may have
more than one pack to scan• Not an ‘IT project’ but dependant on IT/connectivity/interoperability• Significant implications for business process
– decommissioning – 10 day rule
Opportunities– Aggregated codes– Use of member State flexibilities
16
Wider benefits of data captureDirect Patient Benefits: • Safety ie confirm the correct drug is dispensed • A detailed record of products supplied to a patient facilitating:
– Patient level product recalls– Monitoring a patient’s medication regime – Improved pharmacovigilance/ pharmacoepidemiology
System wide benefits include facilitating:• Monitoring patient outcomes• Opportunities to minimising the scope for fraud• Commissioning/monitoring services• Research• Targeting interventions
17
Hospital• Implications for GS1
– How does GS1 barcoding fit with FMD bar-coding?– GS1 is product specific versus FMD is unique specific– Relationship with DM&D?
• Implications of decommissioning– Not all medicines go through hospital pharmacies– ‘scan for safety’. – decommission and ‘scan’ at the point of administration?
• Implications of only 10 days to reverse decommissioning – Does this include returns from the ward? the majority is not within 10days. – If decommission at the point given to the patient less of an issue
• Implications for wholesaler dealers license
18
DH/MHRA Implementation Board• Terms of reference
To provide advice to DH and MHRA regarding the flexibilities within the Delegated Act and the key challenges facing the supply chain, public bodies, NHS and others to fully implement the requirements of the FMD and the DA.
• Members– Across the supply chain and NHS– Hospital representatives
– Iain Davidson; Andrew Davies & Boo Vadher