autoimmune polyendocrinopathy-candidiasis-ectodermal dysplasia
TRANSCRIPT

Autoimmune Polyendocrinopathy-Candidiasis–Ectodermal Dysplasia
Yoavanit Srivaro M.D.

Outlines
•Introduction
•Epidemiology
•Pathogenesis
•Clinical Manifestations
•Laboratory Evaluation
•Diagnosis
•Management
•Prognosis

Introduction

1st mentionedliterature by
Thorpe and Handley in 1929
CMC & HP
1929 1946
Clinical triad of 1.Chronic mucocutaneouscandidiasis 2.Hypoparathyroidism 3.Adrenal insufficiency
was reported
1956
Recognized as “Whitaker’s syndrome”
1980
Recognized as“APS-1”
Peltonen-Palotie L, Halonen M, Perheentupa J. Autoimmune polyendocrinopathy, candidiasis, ectodermal dystrophy. In: Ochs HD, Smith CI, Puck JM, editors. Primary immunodeficiency diseases: a molecular and genetic approach. 2nd ed. New York: Oxford University Press; 2007. p. 342-53.

Eisenbarth GS, Gottlieb PA. Autoimmune polyendocrine syndromes. N Engl J Med. 2004;350:2068-79.

1st mentionedliterature by
Thorpe and Handley in 1929
CMC & HP
1929 1946
Clinical triad of 1.Chronic mucocutaneouscandidiasis 2.Hypoparathyroidism 3.Adrenal insufficiency
was reported
1956
Recognized as “Whitaker’s syndrome”
1980
Recognized as“APS-1”
1990
Acronym “APECED”was introduced by Finnish pediatrician Professor JaakkoPerheentupa
Peltonen-Palotie L, Halonen M, Perheentupa J. Autoimmune polyendocrinopathy, candidiasis, ectodermal dystrophy. In: Ochs HD, Smith CI, Puck JM, editors. Primary immunodeficiency diseases: a molecular and genetic approach. 2nd ed. New York: Oxford University Press; 2007. p. 342-53.

1994 1997 2002
Analysis 1st knockout mouse models: A role for AIRE in the development of both central& peripheral tolerance.
Peltonen-Palotie L, Halonen M, Perheentupa J. Autoimmune polyendocrinopathy, candidiasis, ectodermal dystrophy. In: Ochs HD, Smith CI, Puck JM, editors. Primary immunodeficiency diseases: a molecular and genetic approach. 2nd ed. New York: Oxford University Press; 2007. p. 342-53.
APECED locus was mapped in the Finnish families to 21q22.3
A novel gene, AIRE was positionallycloned.

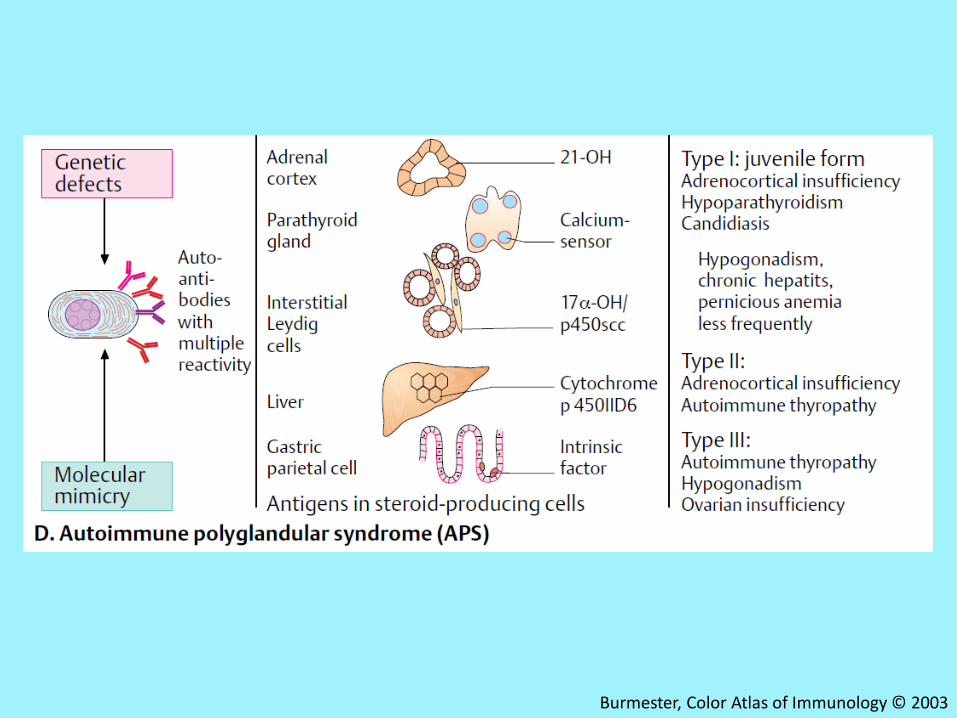
APECED
•Monogenic autosomal recessive disease
•Characterized by
1. Chronic candidiasis
2. Multiple autoimmune diseases
• Loss-of-function mutations in the autoimmune
regulator (AIRE) gene
Kisand K, Peterson P. Autoimmune polyendocrinopathy candidiasis ectodermal dystrophy. J Clin Immunol. 2015;35:463-78.
Burmester, Color Atlas of Immunology © 2003

Epidemiology

Country Prevalence
Iranian Jews 1: 9,000
Sardinians 1:14,000
Finns 1:2,5000
Slovenia 1:43,000
Norway 1:80,000
Poland 1:129,000
Kisand K, Peterson P. Autoimmune polyendocrinopathy candidiasis ectodermal dystrophy. J Clin Immunol. 2015;35:463-78.

Pathogenesis

Burmester, Color Atlas of Immunology © 2003

Burmester, Color Atlas of Immunology © 2003

Abbas AK, Lichtman AH, Pillai S. Cellular and molecular immunology. 8th ed.Philadelphia, W.B. Saunders Company.2015
FIGURE 2-10 Morphology of the thymus.

FIGURE 8-18 Maturation of T cells in the thymus.
Abbas AK, Lichtman AH, Pillai S. Cellular and molecular immunology. 8th ed.Philadelphia, W.B. Saunders Company.2015

Abbas AK, Lichtman AH, Pillai Shiv. Cellular and molecular immunology. 8th ed.Philadelphia, W.B. Saunders Company.2015.
FIGURE 15-2 Central T cell tolerance.

FIGURE2Thymocyte-intrinsic pathways required for negative selection.
Siggs OM, Makaroff LE, Liston A. The why and how of thymocyte negative selection. Curr Opin Immunol. 2006;18:175-83.

Abbas AK, Lichtman AH, Pillai Shiv. Cellular and molecular immunology. 8th ed.Philadelphia, W.B. Saunders Company.2015.
FIGURE 15-2 Central T cell tolerance.

Abbas AK, Lichtman AH, Pillai Shiv. Cellular and molecular immunology. 8th ed.Philadelphia, W.B. Saunders Company.2015.
FIGURE 15-3 The function of AIRE in deletion of T cells in the thymus.

Abbas AK, Lichtman AH, Pillai Shiv. Cellular and molecular immunology. 8th ed.Philadelphia, W.B. Saunders Company.2015.
FIGURE 15-3 The function of AIRE in deletion of T cells in the thymus.

Eisenbarth GS, Gottlieb PA. Autoimmune polyendocrine syndromes. N Engl J Med. 2004;350:2068-79.

Abbas AK, Lichtman AH, Pillai Shiv. Cellular and molecular immunology. 8th ed.Philadelphia, W.B. Saunders Company.2015.

The AIRE gene is located in chromosome 21 region q22.3
Kisand K, Peterson P. Autoimmune polyendocrinopathy candidiasis ectodermal dystrophy. J Clin Immunol. 2015;35:463-78.

Peterson P, Org T, Rebane A. Transcriptional regulation by AIRE: molecular mechanisms of central tolerance. Nat Rev Immunol. 2008;8:948-57.
AIRE protein: 545–amino acid protein, molecular weight of 57.5 kDa

Figure 1 AIRE gene and AIRE 1 protein
Proust-Lemoine E, Saugier-Veber P, Wemeau JL. Polyglandular autoimmune syndrome type I. Presse Med. 2012;41:e651-62.

Figure 1 AIRE gene and AIRE 1 protein
Proust-Lemoine E, Saugier-Veber P, Wemeau JL. Polyglandular autoimmune syndrome type I. Presse Med. 2012;41:e651-62.

Proust-Lemoine E, Saugier-Veber P, Wemeau JL. Polyglandular autoimmune syndrome type I. Presse Med. 2012;41:e651-62.
HSR
NLS
SAND
PHD1
PRR
PHD2
Homogeneously Staining Region
Nuclear Localisation Signal
DNA liaison domain
Plant HomeoDomain
ProlineRich Region
Plant HomeoDomain
LXXLL motifs: motifs of nuclear receptor liaison

Kisand K, Peterson P. Autoimmune polyendocrinopathy candidiasis ectodermal dystrophy. J Clin Immunol. 2015;35:463-78.
Fig. 1 In the medullary thymic epithelial cells (mTEC) AIRE promotesthe expression of tissue specific antigens by interacting with largechromatin-associated complex.

AIRE Protein
•Restricted expression pattern
1. Mainly present in
:Medullary thymic epithelial cells (mTECs)
2. Rare present in
:Dendritic-like cells in the lymph nodes & tonsils
Heino M, Peterson P, Kudoh J, Nagamine K, Lagerstedt A, Ovod V, et al. Autoimmune regulator is expressed in the cells regulating immune tolerance in thymus medulla. Biochem Biophys Res Commun. 1999;257:821–5.
Poliani PL, Kisand K, Marrella V, Ravanini M, Notarangelo LD, Villa A, et al. Human peripheral lymphoid tissues contain autoimmune regulator-expressing dendritic cells. Am J Pathol. 2010;176: 1104–12.

Peltonen-Palotie L, Halonen M, Perheentupa J. Autoimmune polyendocrinopathy, candidiasis, ectodermal dystrophy. In: Ochs HD, Smith CI, Puck JM, editors. Primary immunodeficiency diseases: a molecular and genetic approach. 2nd ed. New York: Oxford University Press; 2007. p. 342-53.

Peltonen-Palotie L, Halonen M, Perheentupa J. Autoimmune polyendocrinopathy, candidiasis, ectodermal dystrophy. In: Ochs HD, Smith CI, Puck JM, editors. Primary immunodeficiency diseases: a molecular and genetic approach. 2nd ed. New York: Oxford University Press; 2007. p. 342-53.

FIG. 1. Expression of AIRE in thymus medulla
Heino M, Peterson P, Kudoh J, Nagamine K, Lagerstedt A, Ovod V, et al. Autoimmune regulator is expressed in the cells regulating immune tolerance in thymus medulla. Biochem Biophys Res Commun. 1999;257:821-5.

FIG. 2. Intracellular expression of AIRE in vivo and in vitro.
Heino M, Peterson P, Kudoh J, Nagamine K, Lagerstedt A, Ovod V, et al. Autoimmune regulator is expressed in the cells regulating immune tolerance in thymus medulla. Biochem Biophys Res Commun. 1999;257:821-5.

AIRE Gene Mutation
•More than 50 mutations
: Deletions
: Insertions
: Missense point mutations
: Nonsense point mutations
Proust-Lemoine E, Saugier-Veber P, Wemeau JL. Polyglandular autoimmune syndrome type I. Presse Med. 2012;41:e651-62.

Finnish mutation
English mutation
Sardinainmutation

Anderson MS, Casanova JL. More than Meets the Eye: Monogenic Autoimmunity Strikes Again. Immunity. 2015;42:986-8.

Husebye ES, Perheentupa J, Rautemaa R, Kampe O. Clinical manifestations and management of patients with autoimmune polyendocrinesyndrome type I. J Intern Med. 2009;265:514–29

Clinical Manifestations

Husebye ES, Perheentupa J, Rautemaa R, Kampe O. Clinical manifestations and management of patients with autoimmunepolyendocrine syndrome type I. J Intern Med. 2009;265:514–29

• Chronic Mucocutaneous Candidiasis
• Endocrine Manifestations
• Gastrointestinal Manifestations
• Ectodermal Manifestations
• Tubulo-Interstitial Nephritis
• Interstitial Lung Disease
• Other Manifestations

• Chronic Mucocutaneous Candidiasis
• Endocrine Manifestations
• Gastrointestinal Manifestations
• Ectodermal Manifestations
• Tubulo-Interstitial Nephritis
• Interstitial Lung Disease
• Other Manifestations

Chronic Mucocutaneous Candidiasis
• Heterogeneous group of syndromes
1. Common features
: Chronic noninvasive Candida infections of the
skin,nails, and mucous membranes
2. Associated autoimmune manifestations

Proust-Lemoine E, Saugier-Veber P, Wemeau JL. Polyglandular autoimmune syndrome type I. Presse Med. 2012;41:e651-62.
Finn Sardinian2006 201291 (%) 22 (%)
88 69
84 77
100 97
33 5
31
18 27
39
31
22

Perheentupa J. Autoimmune polyendocrinopathy-candidiasis-ectodermal dystrophy. J Clin Endocrinol Metab. 2006;91:2843-50.

Perheentupa J. Autoimmune polyendocrinopathy-candidiasis-ectodermal dystrophy. J Clin Endocrinol Metab. 2006;91:2843-50.

Collins SM, Dominguez M, Ilmarinen T, Costigan C, Irvine AD. Dermatological manifestations of autoimmune polyendocrinopathy-candidiasis-ectodermal dystrophy syndrome. Br J Dermatol. 2006;154:1088-93.

Collins SM, Dominguez M, Ilmarinen T, Costigan C, Irvine AD. Dermatological manifestations of autoimmune polyendocrinopathy-candidiasis-ectodermal dystrophy syndrome. Br J Dermatol. 2006;154:1088-93.
• Less than 10% of cases : limited to the skin & often localized. • Up to 100% of cases :mainly affects the oral mucous membranes.• 2/3 of cases : mainly affects the nails.

Collins SM, Dominguez M, Ilmarinen T, Costigan C, Irvine AD. Dermatological manifestations of autoimmune polyendocrinopathy-candidiasis-ectodermal dystrophy syndrome. Br J Dermatol. 2006;154:1088-93.
• More rarely : Genitals candidiasis• 15 to 22% of cases:Oeosophageal candidiasis

Perheentupa J. Autoimmune polyendocrinopathy-candidiasis-ectodermal dystrophy. J Clin Endocrinol Metab. 2006;91:2843-50.

Milner JD, Holland SM. The cup runneth over: lessons from the ever-expanding pool of primary immunodeficiency diseases. Nat Rev Immunol. 2013;13:635-48.
FIGURE 4 Defects in immunity to Candida albicans.

Milner JD, Holland SM. The cup runneth over: lessons from the ever-expanding pool of primary immunodeficiency diseases. Nat Rev Immunol. 2013;13:635-48.
FIGURE 4 Defects in immunity to Candida albicans.


Puel A, Doffinger R, Natividad A, Chrabieh M, Barcenas-Morales G, Picard C, et al. Autoantibodies against IL-17A, IL-17F, and IL-22 in patients with chronic mucocutaneous candidiasis and autoimmune polyendocrine syndrome type I. J Exp Med. 2010;207:291-7.

Gouda MR, Al-Amin A, Grabsch H, Donnellan C. A multidisciplinary approach to management of autoimmune polyendocrinopathy candidiasis ectodermal dystrophy (APECED). BMJ Case Rep. 2013;2013.

Sivabalan S, Mahadevan S, Srinath MV. Recurrent oral thrush. Indian J Pediatr. 2014;81:394-6.

• Chronic Mucocutaneous Candidiasis
• Endocrine Manifestations
• Gastrointestinal Manifestations
• Ectodermal Manifestations
• Tubulo-Interstitial Nephritis
• Interstitial Lung Disease
• Other Manifestations

Burmester, Color Atlas of Immunology © 2003

Endocrine Manifestations
•Hypoparathyroidism
•Adrenocortical failure
•Hypergonadotropic hypogonadism
•Type 1 diabetes
•Autoimmune thyroiditis
•Pituitary failure and growth hormone deficiency
Kisand K, Peterson P. Autoimmune polyendocrinopathy candidiasis ectodermal dystrophy. J Clin Immunol. 2015;35:463-78.

Burmester, Color Atlas of Immunology © 2003

Proust-Lemoine E, Saugier-Veber P, Wemeau JL. Polyglandular autoimmune syndrome type I. Presse Med. 2012;41:e651-62.
Finn Sardinian2006 201291 (%) 22 (%)
88 69
84 77
100 97
33 5
31
18 27
39
31
22

Perheentupa J. Autoimmune polyendocrinopathy-candidiasis-ectodermal dystrophy. J Clin Endocrinol Metab. 2006;91:2843-50.

Perheentupa J. Autoimmune polyendocrinopathy-candidiasis-ectodermal dystrophy. J Clin Endocrinol Metab. 2006;91:2843-50.

Hypoparathyroidism
•Symptoms are related to hypocalcemia
: Muscle cramps, mild paresthesia and clumsiness
Husebye ES, Perheentupa J, Rautemaa R, Kampe O. Clinical manifestations and management of patients with autoimmunepolyendocrine syndrome type I. J Intern Med. 2009;265:514–29

Endocrine Manifestations
•Hypoparathyroidism
•Adrenocortical failure
•Hypergonadotropic hypogonadism
•Type 1 diabetes
•Autoimmune thyroiditis
•Pituitary failure and growth hormone deficiency
Kisand K, Peterson P. Autoimmune polyendocrinopathy candidiasis ectodermal dystrophy. J Clin Immunol. 2015;35:463-78.

Burmester, Color Atlas of Immunology © 2003

Proust-Lemoine E, Saugier-Veber P, Wemeau JL. Polyglandular autoimmune syndrome type I. Presse Med. 2012;41:e651-62.
Finn Sardinian2006 201291 (%) 22 (%)
84 69
88 77
100 97
33 5
31
18 27
39
31
22

Perheentupa J. Autoimmune polyendocrinopathy-candidiasis-ectodermal dystrophy. J Clin Endocrinol Metab. 2006;91:2843-50.

Perheentupa J. Autoimmune polyendocrinopathy-candidiasis-ectodermal dystrophy. J Clin Endocrinol Metab. 2006;91:2843-50.

Addison’s disease
•Mediated by autoreactive cytotoxic T-cells
•Adrenal hormone deficiencies do not manifest
clinically until at least 90 % of the functional
adrenocortical cells have been destroyed
Kisand K, Peterson P. Autoimmune polyendocrinopathy candidiasis ectodermal dystrophy. J Clin Immunol. 2015;35:463-78.

Addison’s disease
•Characteristic symptoms include
:Fatigue, salt craving, hypotension, weight loss and
an increased pigmentation of the skin and mucous
membranes
Kisand K, Peterson P. Autoimmune polyendocrinopathy candidiasis ectodermal dystrophy. J Clin Immunol. 2015;35:463-78.

Endocrine Manifestations
•Hypoparathyroidism
•Adrenocortical failure
•Hypergonadotropic hypogonadism
•Type 1 diabetes
•Autoimmune thyroiditis
•Pituitary failure and growth hormone deficiency
Kisand K, Peterson P. Autoimmune polyendocrinopathy candidiasis ectodermal dystrophy. J Clin Immunol. 2015;35:463-78.

Burmester, Color Atlas of Immunology © 2003

Hypergonadotropic hypogonadism
•Ovarian insufficiency
•Testicular insufficiency
Husebye ES, Perheentupa J, Rautemaa R, Kampe O. Clinical manifestations and management of patients with autoimmunepolyendocrine syndrome type I. J Intern Med. 2009;265:514–29

Ovarian insufficiency
•Start early with arrested pubertal development
•Manifest as premature menopause
Husebye ES, Perheentupa J, Rautemaa R, Kampe O. Clinical manifestations and management of patients with autoimmunepolyendocrine syndrome type I. J Intern Med. 2009;265:514–29

Testicular insufficiency
• Less frequent
•Affects approximately 10 % of male patients
•Usually develops during adulthood
Husebye ES, Perheentupa J, Rautemaa R, Kampe O. Clinical manifestations and management of patients with autoimmunepolyendocrine syndrome type I. J Intern Med. 2009;265:514–29

Endocrine Manifestations
•Hypoparathyroidism
•Adrenocortical failure
•Hypergonadotropic hypogonadism
•Type 1 diabetes
•Autoimmune thyroiditis
•Pituitary failure and growth hormone deficiency
Kisand K, Peterson P. Autoimmune polyendocrinopathy candidiasis ectodermal dystrophy. J Clin Immunol. 2015;35:463-78.

Proust-Lemoine E, Saugier-Veber P, Wemeau JL. Polyglandular autoimmune syndrome type I. Presse Med. 2012;41:e651-62.
Finn Sardinian2006 201291 (%) 22 (%)
80 69
87 77
100 97
33 5
31
22
39
18 27
31

Perheentupa J. Autoimmune polyendocrinopathy-candidiasis-ectodermal dystrophy. J Clin Endocrinol Metab. 2006;91:2843-50.

Perheentupa J. Autoimmune polyendocrinopathy-candidiasis-ectodermal dystrophy. J Clin Endocrinol Metab. 2006;91:2843-50.

Endocrine Manifestations
•Hypoparathyroidism
•Adrenocortical failure
•Hypergonadotropic hypogonadism
•Type 1 diabetes
•Autoimmune thyroiditis
•Pituitary failure and growth hormone deficiency
Kisand K, Peterson P. Autoimmune polyendocrinopathy candidiasis ectodermal dystrophy. J Clin Immunol. 2015;35:463-78.

Autoimmune thyroiditis
•Hypothyroidism also develops during adulthood
:Dx in one-fourth of patients
•Hyperthyroidism is very rare and transient
Kisand K, Peterson P. Autoimmune polyendocrinopathy candidiasis ectodermal dystrophy. J Clin Immunol. 2015;35:463-78.

Endocrine Manifestations
•Hypoparathyroidism
•Adrenocortical failure
•Hypergonadotropic hypogonadism
•Type 1 diabetes
•Autoimmune thyroiditis
•Pituitary failure and growth hormone deficiency
Kisand K, Peterson P. Autoimmune polyendocrinopathy candidiasis ectodermal dystrophy. J Clin Immunol. 2015;35:463-78.

Pituitary failure and Growth hormone deficiency
•Rare manifestations
•Higher prevalence in certain populations
Meloni A, Willcox N, Meager A, Atzeni M, Wolff AS, Husebye ES, et al. Autoimmune polyendocrine syndrome type 1: an extensive longitudinal study in Sardinian patients. J Clin Endocrinol Metab. 2012;97:1114–24.

Meloni A, Willcox N, Meager A, Atzeni M, Wolff AS, Husebye ES, et al. Autoimmune polyendocrine syndrome type 1: an extensive longitudinal study in Sardinian patients. J Clin Endocrinol Metab. 2012;97:1114-24.
Sardinians 25 %

• Chronic Mucocutaneous Candidiasis
• Endocrine Manifestations
• Gastrointestinal Manifestations
• Ectodermal Manifestations
• Tubulo-Interstitial Nephritis
• Interstitial Lung Disease
• Other Manifestations

Gastrointestinal Manifestations
Husebye ES, Perheentupa J, Rautemaa R, Kampe O. Clinical manifestations and management of patients with autoimmunepolyendocrine syndrome type I. J Intern Med. 2009;265:514–29

Proust-Lemoine E, Saugier-Veber P, Wemeau JL. Polyglandular autoimmune syndrome type I. Presse Med. 2012;41:e651-62.
Finn Sardinian2006 201291 (%) 22 (%)
80 69
87 77
100 97
33 5
31
18 27
39
31
22

Gastrointestinal Manifestations
Husebye ES, Perheentupa J, Rautemaa R, Kampe O. Clinical manifestations and management of patients with autoimmunepolyendocrine syndrome type I. J Intern Med. 2009;265:514–29

Proust-Lemoine E, Saugier-Veber P, Wemeau JL. Polyglandular autoimmune syndrome type I. Presse Med. 2012;41:e651-62.
Finn Sardinian2006 201291 (%) 22 (%)
80 69
87 77
100 97
33 5
31
18 27
39
31
22

Gastrointestinal Manifestations
Husebye ES, Perheentupa J, Rautemaa R, Kampe O. Clinical manifestations and management of patients with autoimmunepolyendocrine syndrome type I. J Intern Med. 2009;265:514–29

Proust-Lemoine E, Saugier-Veber P, Wemeau JL. Polyglandular autoimmune syndrome type I. Presse Med. 2012;41:e651-62.

Gastrointestinal Manifestations
Husebye ES, Perheentupa J, Rautemaa R, Kampe O. Clinical manifestations and management of patients with autoimmunepolyendocrine syndrome type I. J Intern Med. 2009;265:514–29

• Chronic Mucocutaneous Candidiasis
• Endocrine Manifestations
• Gastrointestinal Manifestations
• Ectodermal Manifestations
• Tubulo-Interstitial Nephritis
• Interstitial Lung Disease
• Other Manifestations

Ectodermal Manifestations
Husebye ES, Perheentupa J, Rautemaa R, Kampe O. Clinical manifestations and management of patients with autoimmunepolyendocrine syndrome type I. J Intern Med. 2009;265:514–29

Proust-Lemoine E, Saugier-Veber P, Wemeau JL. Polyglandular autoimmune syndrome type I. Presse Med. 2012;41:e651-62.
Finn Sardinian2006 201291 (%) 22 (%)
80 69
87 77
100 97
33 5
31
18 27
39
31
22

FIGURE. 6-13 Autoimmune polyendocrinopathy-candidiasis-ectodermal dystrophy (APECED) syndrome.
A.Erythematous candidiasis diffusely involving the dorsal tongue of a 32-year-old man.
B.Same patient showing nail dystrophy.
C.Corneal keratopathy
http://pocketdentistry.com/6-fungal-and-protozoal-diseases

Ectodermal Manifestations
Husebye ES, Perheentupa J, Rautemaa R, Kampe O. Clinical manifestations and management of patients with autoimmunepolyendocrine syndrome type I. J Intern Med. 2009;265:514–29

Proust-Lemoine E, Saugier-Veber P, Wemeau JL. Polyglandular autoimmune syndrome type I. Presse Med. 2012;41:e651-62.

FIGURE 2 Dental Enamel hypoplasia
Winer KK, Merke DP. Picture of the month. Autoimmune polyglandular syndrome type 1. Arch Pediatr Adolesc Med. 2000;154:745-6.

Ectodermal Manifestations
Husebye ES, Perheentupa J, Rautemaa R, Kampe O. Clinical manifestations and management of patients with autoimmunepolyendocrine syndrome type I. J Intern Med. 2009;265:514–29

Proust-Lemoine E, Saugier-Veber P, Wemeau JL. Polyglandular autoimmune syndrome type I. Presse Med. 2012;41:e651-62.
Finn Sardinian2006 201291 (%) 22 (%)
80 69
87 77
100 97
33 5
31
18 27
39
31
22

Fig 3a: hyperpigmentation and periorificial vitiligo in a 23 year-old female patient
Proust-Lemoine E, Saugier-Veber P, Wemeau JL. Polyglandular autoimmune syndrome type I. Presse Med. 2012;41:e651-62.

FIGURE 1 Depigmented patchs around both eyes were noted
Winer KK, Merke DP. Picture of the month. Autoimmune polyglandular syndrome type 1. Arch Pediatr Adolesc Med. 2000;154:745-6.

FIGURE 1 Dermatological manifestations of autoimmune polyendocrinopathy–candidiasis– ectodermal dystrophy syndrome
Oral candidiasis
Halo naevi
Candidalonychomycosis & paronychia
Poliosis
Collins SM, Dominguez M, Ilmarinen T, Costigan C, Irvine AD. Dermatological manifestations of autoimmune polyendocrinopathy-candidiasis-ectodermal dystrophy syndrome. Br J Dermatol. 2006;154:1088-93.

FIGURE 1 Dermatological manifestations of autoimmune polyendocrinopathy–candidiasis– ectodermal dystrophy syndrome
Oral candidiasis
Halo naevi
Candidalonychomycosis & paronychia
Poliosis
Collins SM, Dominguez M, Ilmarinen T, Costigan C, Irvine AD. Dermatological manifestations of autoimmune polyendocrinopathy-candidiasis-ectodermal dystrophy syndrome. Br J Dermatol. 2006;154:1088-93.

Ectodermal Manifestations
Husebye ES, Perheentupa J, Rautemaa R, Kampe O. Clinical manifestations and management of patients with autoimmunepolyendocrine syndrome type I. J Intern Med. 2009;265:514–29

Proust-Lemoine E, Saugier-Veber P, Wemeau JL. Polyglandular autoimmune syndrome type I. Presse Med. 2012;41:e651-62.
Finn Sardinian2006 201291 (%) 22 (%)
80 69
87 77
100 97
33 5
31
18 27
39
31
22

Fig 3 b: alopecia of the scalp (note the absence of eyelashes and eyebrows) in a 34 year-old subject
Proust-Lemoine E, Saugier-Veber P, Wemeau JL. Polyglandular autoimmune syndrome type I. Presse Med. 2012;41:e651-62.

Ectodermal Manifestations
Husebye ES, Perheentupa J, Rautemaa R, Kampe O. Clinical manifestations and management of patients with autoimmunepolyendocrine syndrome type I. J Intern Med. 2009;265:514–29

Proust-Lemoine E, Saugier-Veber P, Wemeau JL. Polyglandular autoimmune syndrome type I. Presse Med. 2012;41:e651-62.

FIGURE 3 Nail pitting
Winer KK, Merke DP. Picture of the month. Autoimmune polyglandular syndrome type 1. Arch Pediatr Adolesc Med. 2000;154:745-6.

• Chronic Mucocutaneous Candidiasis
• Endocrine Manifestations
• Gastrointestinal Manifestations
• Ectodermal Manifestations
• Tubulo-Interstitial Nephritis
• Interstitial Lung Disease
• Other Manifestations

Tubulo-Interstitial Nephritis
•Serious but rare manifestation
•Affecting up to 10 % of patients
• Serum Cr , ESR, Abn UA , Proteinuria & Glycosuria
•Permanent renal dysfunction, H/D, KT
•Biopsy T cell infiltration & antiproximal tubular autoab.
Kisand K, Peterson P. Autoimmune polyendocrinopathy candidiasis ectodermal dystrophy. J Clin Immunol. 2015;35:463-78.

• Chronic Mucocutaneous Candidiasis
• Endocrine Manifestations
• Gastrointestinal Manifestations
• Ectodermal Manifestations
• Tubulo-Interstitial Nephritis
• Interstitial Lung Disease
• Other Manifestations

Interstitial Lung Disease
•Rare ,Affecting less than 5%of patients
• It can lead to chronic respiratory failure
•Chronic cough, dyspnea, thoracic pain & recurrent
LRTI
• Lung bx severe peribronchiolar lymphoid infiltrate
•Two autoantibodies :KCNRG, BPIFB1
Kisand K, Peterson P. Autoimmune polyendocrinopathy candidiasis ectodermal dystrophy. J Clin Immunol. 2015;35:463-78.

• Chronic Mucocutaneous Candidiasis
• Endocrine Manifestations
• Gastrointestinal Manifestations
• Ectodermal Manifestations
• Tubulo-Interstitial Nephritis
• Interstitial Lung Disease
• Other Manifestations

Other Manifestations
•Asplenia
•Chronic inflammatory demyelinating polyneuropathy
•Sjögren’s syndrome
•Rheumatoid arthritis
•Cutaneous vasculitis
Kisand K, Peterson P. Autoimmune polyendocrinopathy candidiasis ectodermal dystrophy. J Clin Immunol. 2015;35:463-78.

Other Manifestations
•Scleroderma
•Metaphyseal osteodysplasia
•Amyotrophic lateral sclerosis
•Retinal pigment degeneration
•Celiac disease
Kisand K, Peterson P. Autoimmune polyendocrinopathy candidiasis ectodermal dystrophy. J Clin Immunol. 2015;35:463-78.

Asplenia
•Presenting in up to 20 % of adult patients
• Impaired immune responses to encapsulated
bacteria
•Pathogenesis of asplenia remains unknown
Kisand K, Peterson P. Autoimmune polyendocrinopathy candidiasis ectodermal dystrophy. J Clin Immunol. 2015;35:463-78.

Rash with fever
•One of the first signs of APECED
• It usually develops before the age of 5 years
•Skin bx : Presence of vasculitis
Kisand K, Peterson P. Autoimmune polyendocrinopathy candidiasis ectodermal dystrophy. J Clin Immunol. 2015;35:463-78.

Perheentupa J. Autoimmune polyendocrinopathy-candidiasis-ectodermal dystrophy. J Clin Endocrinol Metab. 2006;91:2843-50.

Perheentupa J. Autoimmune polyendocrinopathy-candidiasis-ectodermal dystrophy. J Clin Endocrinol Metab. 2006;91:2843-50.

Perheentupa J. Autoimmune polyendocrinopathy-candidiasis-ectodermal dystrophy. J Clin Endocrinol Metab. 2006;91:2843-50.

Perheentupa J. Autoimmune polyendocrinopathy-candidiasis-ectodermal dystrophy. J Clin Endocrinol Metab. 2006;91:2843-50.

Meloni A, Willcox N, Meager A, Atzeni M, Wolff AS, Husebye ES, et al. Autoimmune polyendocrine syndrome type 1: an extensive longitudinal study in Sardinian patients. J Clin Endocrinol Metab. 2012;97:1114-24.
• 22 patients from 17 Sardinian families with APS1
• Female/male :13/9
• Median current age : 30.7yr (1.8–46yr)
• Median early disease onset : 3.5 yr (0.3–10 yr)

Meloni A, Willcox N, Meager A, Atzeni M, Wolff AS, Husebye ES, et al. Autoimmune polyendocrine syndrome type 1: an extensive longitudinal study in Sardinian patients. J Clin Endocrinol Metab. 2012;97:1114-24.

Meloni A, Willcox N, Meager A, Atzeni M, Wolff AS, Husebye ES, et al. Autoimmune polyendocrine syndrome type 1: an extensive longitudinal study in Sardinian patients. J Clin Endocrinol Metab. 2012;97:1114-24.
• Classic triad : 58%
• First sign with CMC : 18 patients
• First sign with HP : 3 patients
• CMC : 95%
• HP :77%
• AD :68%

Meloni A, Willcox N, Meager A, Atzeni M, Wolff AS, Husebye ES, et al. Autoimmune polyendocrine syndrome type 1: an extensive longitudinal study in Sardinian patients. J Clin Endocrinol Metab. 2012;97:1114-24.
• Major nonsense mutation, R139X :93%
• Died during follow-up : 3 patients
:Hyperacute AIH (aged 5–12 yr) : 2 patients
:Unrelated HIV infection: 1 patients

Laboratory Evaluation

• Immunologic Evaluation
• Endocrine Work Up
• Gastrointestinal Work Up
• Serum autoantibody Work Up

• Immunologic Evaluation
• Endocrine Work Up
• Gastrointestinal Work Up
• Serum autoantibodies Work Up

Picard C, Al-Herz W, Bousfiha A, Casanova JL, Chatila T, Conley ME, et al. Primary Immunodeficiency Diseases: an Update on the Classification from the International Union of Immunological Societies Expert Committee for Primary Immunodeficiency 2015. J Clin Immunol. 2015.

• Immunologic Evaluation
• Endocrine Work Up
• Gastrointestinal Work Up
• Serum autoantibodies Work Up

Endocrine Work Up

• Immunologic Evaluation
• Endocrine Work Up
• Gastrointestinal Work Up
• Serum autoantibodies Work Up

Gastrointestinal Work Up
Husebye ES, Perheentupa J, Rautemaa R, Kampe O. Clinical manifestations and management of patients with autoimmunepolyendocrine syndrome type I. J Intern Med. 2009;265:514–29

• Immunologic Evaluation
• Endocrine Work Up
• Gastrointestinal Work Up
• Serum autoantibodies Work Up

Husebye ES, Perheentupa J, Rautemaa R, Kampe O. Clinical manifestations and management of patients with autoimmune polyendocrinesyndrome type I. J Intern Med. 2009;265:514–29

Kisand K, Peterson P. Autoimmune polyendocrinopathy candidiasis ectodermal dystrophy. J Clin Immunol. 2015;35:463-78.

Meloni A, Willcox N, Meager A, Atzeni M, Wolff AS, Husebye ES, et al. Autoimmune polyendocrine syndrome type 1: an extensive longitudinal study in Sardinian patients. J Clin Endocrinol Metab. 2012;97:1114-24.

Meloni A, Willcox N, Meager A, Atzeni M, Wolff AS, Husebye ES, et al. Autoimmune polyendocrine syndrome type 1: an extensive longitudinal study in Sardinian patients. J Clin Endocrinol Metab. 2012;97:1114-24.

Diagnosis

Husebye ES, Perheentupa J, Rautemaa R, Kampe O. Clinical manifestations and management of patients with autoimmunepolyendocrine syndrome type I. J Intern Med. 2009;265:514–29

Management

Treatment
•Require continuous hormone replacement therapy
•Calcium and vitamin D supplements
•Systemic antibiotics for candidal infections
• Immunosuppressive therapy
Peltonen-Palotie L, Halonen M, Perheentupa J. Autoimmune polyendocrinopathy, candidiasis, ectodermal dystrophy. In: Ochs HD, Smith CI, Puck JM, editors. Primary immunodeficiency diseases: a molecular and genetic approach. 2nd ed. New York: Oxford University Press; 2007. p. 342-53.

Hormone replacement therapy
•Hydrocortisone 20 mg /day (divided in three dose)
•Cortisone acetate 25 mg /day (divided in three dose)
Proust-Lemoine E, Saugier-Veber P, Wemeau JL. Polyglandular autoimmune syndrome type I. Presse Med. 2012;41:e651-62.

Calcium and vitamin D supplements
•Elementary Ca 100–500 mg 2–3 daily doses
•Ca-citrate is preferable
Proust-Lemoine E, Saugier-Veber P, Wemeau JL. Polyglandular autoimmune syndrome type I. Presse Med. 2012;41:e651-62.

Calcium and vitamin D supplements
•Dihydrotachysterol (T½ 7 days)
•Alphacalcidol (T½ 2 days)
•Calcitriol (T½ 1 day)
Proust-Lemoine E, Saugier-Veber P, Wemeau JL. Polyglandular autoimmune syndrome type I. Presse Med. 2012;41:e651-62.

Antibiotics for candidal infections
•Oral mucositis
: First, 1–2 mL of nystatin suspension oral 4 times daily
: Then, Amphotericin B lozenge oral 4 times daily
for 4 to 6 weeks or for at least 1 week after the
resolution of symptoms
Proust-Lemoine E, Saugier-Veber P, Wemeau JL. Polyglandular autoimmune syndrome type I. Presse Med. 2012;41:e651-62.

Antibiotics for candidal infections
•Recurrent candidosis
: Pulse prophylaxis
: 1-week course of either of the polyenes q 3 week.
: 3 mL of nystatin suspension oral 3 times daily
: Chlorhexidine mouth rinse 2 times daily
Proust-Lemoine E, Saugier-Veber P, Wemeau JL. Polyglandular autoimmune syndrome type I. Presse Med. 2012;41:e651-62.

Antibiotics for candidal infections
• Infected corners of the mouth
: Natamycin
: Amorolphine hydrochloride cream
: Nonalcoholic chlorhexidine gel
: Miconazole gel
several times daily continuing for 4–5 days after the
corners have healed.
Proust-Lemoine E, Saugier-Veber P, Wemeau JL. Polyglandular autoimmune syndrome type I. Presse Med. 2012;41:e651-62.

Antibiotics for candidal infections
•Failure of the topical therapy & Severe oral mucositis
:Fluconazole adults 200–300 mg once daily
for 1-week course of high dose
Proust-Lemoine E, Saugier-Veber P, Wemeau JL. Polyglandular autoimmune syndrome type I. Presse Med. 2012;41:e651-62.

Antibiotics for candidal infections
•Fingernail candidosis
:Amorolphine nail lacquer 40%
:Urea paste with the help of a podiatrist.
:Itraconazole continued for up to 6 weeks.
Proust-Lemoine E, Saugier-Veber P, Wemeau JL. Polyglandular autoimmune syndrome type I. Presse Med. 2012;41:e651-62.

Immunosuppressive treatments
•Hepatic involvement
•Severe malabsorption
Proust-Lemoine E, Saugier-Veber P, Wemeau JL. Polyglandular autoimmune syndrome type I. Presse Med. 2012;41:e651-62.

Kisand K, Peterson P. Autoimmune polyendocrinopathy candidiasis ectodermal dystrophy. J Clin Immunol. 2015;35:463-78.

Kisand K, Peterson P. Autoimmune polyendocrinopathy candidiasis ectodermal dystrophy. J Clin Immunol. 2015;35:463-78.

Immunization
• Live virus vaccines must be avoided
Peltonen-Palotie L, Halonen M, Perheentupa J. Autoimmune polyendocrinopathy, candidiasis, ectodermal dystrophy. In: Ochs HD, Smith CI, Puck JM, editors. Primary immunodeficiency diseases: a molecular and genetic approach. 2nd ed. New York: Oxford University Press; 2007. p. 342-53.

General considerations on follow-up
•Regular follow-up serum alanine aminotransferase
(ALT) activity to monitor liver function
Peltonen-Palotie L, Halonen M, Perheentupa J. Autoimmune polyendocrinopathy, candidiasis, ectodermal dystrophy. In: Ochs HD, Smith CI, Puck JM, editors. Primary immunodeficiency diseases: a molecular and genetic approach. 2nd ed. New York: Oxford University Press; 2007. p. 342-53.

General considerations on follow-up
• F/U with endocrinologist and an oral specialist at
least once annually
•An SOS Emergency Bracelet
•Need professional support to avoid depression,
social isolation and alcoholism.
Husebye ES, Perheentupa J, Rautemaa R, Kampe O. Clinical manifestations and management of patients with autoimmunepolyendocrine syndrome type I. J Intern Med. 2009;265:514–29

Prognosis

Perheentupa J. Autoimmune polyendocrinopathy-candidiasis-ectodermal dystrophy. J Clin Endocrinol Metab. 2006;91:2843-50.

Perheentupa J. Autoimmune polyendocrinopathy-candidiasis-ectodermal dystrophy. J Clin Endocrinol Metab. 2006;91:2843-50.

Meloni A, Willcox N, Meager A, Atzeni M, Wolff AS, Husebye ES, et al. Autoimmune polyendocrine syndrome type 1: an extensive longitudinal study in Sardinian patients. J Clin Endocrinol Metab. 2012;97:1114-24.

Take Home Message
•Rare autosomal recessive disease
•Autoimmune Regulator (AIRE) gene mutations

Take Home Message
•Diagnosis :based on presence of at least two
out of three ‘‘majors’’ criterions
1. Candidiasis
2. Autoimmune hypoparathyroidism
3. Adrenal insufficiency

Take Home Message
•Hormone replacement therapy
•Candidiasis and other infections should be
carefully screened and treated

Take Home Message
•Potentially letal components :treated by
immunosuppressors
:Hepatitis
:Intestinal malabsorption
