autoimmune hepatitis (aih) in the elderly: a systematic retrospective analysis of a large group of...
TRANSCRIPT

www.elsevier.com/locate/jhep
Journal of Hepatology 45 (2006) 575–583
Autoimmune hepatitis (AIH) in the elderly: A systematicretrospective analysis of a large group of consecutive patients
with definite AIH followed at a tertiary referral centre
Thawab Al-Chalabi, Sylvia Boccato, Bernard C. Portmann, Ian G. McFarlane,Michael A. Heneghan*
Institute of Liver Studies, King’s College Hospital, London, UK
See Editorial, pages 480–482
Background/Aims: A few reports have suggested that AIH may be less severe in the elderly and may be underdiagnosed,
but there is a paucity of data.
Methods: We have undertaken a systematic analysis of 164 consecutive patients (36 males, 128 females) with definite
AIH (median score 23, range 18–28) attending our clinics, comparing those presenting at age >60 years (Group 1,
n = 43) with those presenting at <60 years (Group 2, n = 121).Results: Median (range) duration of follow-up was 9 years (1–28) in Group 1 and 14 years (1–33) in Group 2. Median
ages (ranges) at presentation were: Group 1 = 65 (60–79) and Group 2 = 41 (6–59). Group 1 patients had a significantly
increased incidence of ascites at presentation (p < 0.001) and a lower incidence of relapse (42% vs. 70%, p = 0.002), but
there were no significant differences between the groups with respect to mode of onset (acute, insidious, asymptomatic),
other clinical signs at presentation, biochemical parameters, types or titres of autoantibodies, incidence of histological cir-
rhosis, response to therapy or related side effects. There were also no significant differences in liver-related deaths or trans-
plantation, or the frequencies of HLA DR3 or DR4 – although there was an increased frequency of the A1-B8-DR3/4haplotype in Group 2 (40% vs. 22%, p = 0.138).
Conclusions: These findings suggest that AIH often presents in older patients, who frequently have severe disease. Active
management in these patients can lead to a normal life expectancy.
� 2006 European Association for the Study of the Liver. Published by Elsevier B.V. All rights reserved.
Keywords: Autoimmune hepatitis; Old age; Immunosenescence; Cirrhosis
1. Introduction
Autoimmune hepatitis (AIH) is an uncommonchronic disease of the hepatic parenchyma which ischaracterised by hypergammaglobulinaemia, circulatingautoantibodies and the morphological changes of inter-
0168-8278/$32.00 � 2006 European Association for the Study of the Liver.
doi:10.1016/j.jhep.2006.04.007
Received 7 November 2005; received in revised form 3 April 2006;
accepted 19 April 2006; available online 16 May 2006* Corresponding author. Tel.: +44 207 3464952; fax: +44 207
3463167.E-mail address: [email protected] (M.A.
Heneghan).
face hepatitis, which is responsive to immunosuppres-sive therapy in the majority of cases [1–3]. Thepathogenesis of AIH is still unclear but the conditionappears to have an immunogenetic basis, as evidencedby its well-recognised association in northern Europeancaucasoids with inheritance of the extended HLA haplo-type A1-B8-DR3 and particularly with the DR3 andDR4 allotypes – which are also associated with otherautoimmune diseases [4,5]. The DR3 and DR4 allotypesare independent risk factors for, and are associated withdifferent clinical expressions of, the disease [6]. DR3 ismore frequently associated with a younger age at pre-sentation and greater severity of disease while DR4 is
Published by Elsevier B.V. All rights reserved.

576 T. Al-Chalabi et al. / Journal of Hepatology 45 (2006) 575–583
more prevalent among older patients with generallymilder AIH [4]. The latter is especially the case in Japan,where DR3 is rare in the normal population and the pri-mary association is with DR4 [7].
AIH was originally described in peripubertal females[8], and for many years it was considered to be a condi-tion that mainly affected young women and that it wasuncommon in older patients [9]. It is now known thatthe disease also affects males, although females predom-inate (4:1 to 6:1 in most series), and that it can present atany age [2]. Indeed, recent studies indicate that it is pre-dominantly a disease of the elderly, with a peak of pre-sentation at between 50 and 70 years of age [7,10,11].
Studies of AIH in elderly patients have, however, beenfairly limited and (perhaps in part because of the above-mentioned tendency for them to have milder disease)there has been controversy over whether or not they ben-efit from treatment [12]. One early study concluded thatelderly patients received less benefit from treatment andsuffered more adverse side effects [9], while anothershowed good responses to treatment and few adverseside effects [13]. Two more recent studies noted thatelderly patients can present with severe disease and sug-gested that this may have been due partly to delays indiagnosis and institution of therapy [11,14]. All of thesestudies have been of relatively small numbers and heter-ogeneous populations of patients, including patientswith both probable and definite AIH as well as some withfeatures of primary sclerosing cholangitis or primary bil-iary cirrhosis (so-called overlap syndromes). Additional-ly, it is possible that the earlier reports [prior to thediscovery of the hepatitis C virus (HCV)] may haveincluded patients with chronic HCV infection.
The present study was therefore undertaken in anattempt to resolve some of these issues. It has involved asystematic review of a large, and as homogeneous as pos-sible, group of consecutive patients with definite AIHwhich has provided the basis for an analysis of the influ-ence of age on presenting features, severity of disease,response to treatment and outcome by comparingpatients presenting above and below the age of 60 years.
2. Methods
Consultation of the AIH database at Kings College Hospital iden-tified 164 consecutive patients (36 males, 128 females) with definiteAIH (median score 23, range 18–28, post-treatment) according tothe revised International Autoimmune Hepatitis Group (IAIHG) scor-ing system [2], in adult hepatology clinics between 1971 and 2004 andfor whom sufficient data were available for the present analysis. Allwere seronegative for hepatitis B (HBsAg) and C (anti-HCV) virusinfection – including by retrospective testing for anti-HCV of storedsera from patients who presented prior to 1990.
Other possible causes of liver disease, including alcohol, drugs andherbal remedies, had been carefully excluded by appropriate investiga-tions. Patients who, despite scoring as definite AIH, had evidence sug-gestive of an overlapping condition with primary sclerosing cholangitis(PSC) on endoscopic retrograde cholangio-pancreatography (ERCP)
or histological features of primary biliary cirrhosis (PBC) were exclud-ed from the analysis. Forty-three (26%) of these patients had presentedat or above the age of 60 years (Group 1; median age 65, range 60–79years), and 121 below 60 years of age (Group 2; median age 41, range6–59 years). The records of these patients were systematically reviewedand the two groups were compared with respect to clinical, laboratoryand histological features, response to therapy and outcome. The studyhas been approved by the King’s College Hospital Ethical Committee.
All patients had a full clinical and laboratory assessment at presen-tation and diagnoses were supported by histology in 162. Of the twopatients in whom liver biopsies were not performed at accession (bothin Group 2), one had several biopsies later in the course of his diseaseand in only one case was no liver histology available at any time. How-ever, both had scores (18 and 19) which were above the cut-off (17points) for post-treatment diagnosis of definite AIH [2]. Semi-quanti-tative histological assessment of the severity of chronic hepatitis wasperformed according to Batts and Ludwig [15], whereby necroinflam-matory activity is graded 0 = none, 1 = minimal or patchy, 2 = mild,3 = moderate, 4 = severe, and extent of fibrosis is staged 0 = none,1 = portal only, 2 = periportal, 3 = septal, 4 = cirrhosis. All patientshad at least grade 3 necroinflammatory activity at accession. Histolog-ical improvement was defined as a reduction by at least one grade orstage, and deterioration by an increase in at least one grade or stage.
All patients had been tested for anti-nuclear (ANA), smooth mus-cle (SMA), mitochondrial (AMA) and liver–kidney microsomal (anti-LKM1) autoantibodies by indirect immunofluorescence on sections ofrodent liver, kidney and stomach. HLA typing data were available for27 Group 1 and 92 Group 2 patients. Detailed histories relating to thepresence of other autoimmune diseases in the patients and their fami-lies were available in all cases.
Time to diagnosis was defined as the time from the first onset ofsymptoms or the first observation of deranged biochemical liver teststo the formal diagnosis of AIH. Mode of presentation was definedas ‘acute’ if symptom onset to diagnosis was 66 months, ‘insidious’>6 months, and ‘asymptomatic’ where the patient had no obvioussigns or symptoms of liver disease and their AIH was revealed inciden-tally (e.g. on the basis of abnormal liver biochemistry) on routinehealth screening or during investigation of another condition. Dura-tion of follow-up was defined as the time the patient was first diag-nosed with AIH at whichever hospital the diagnosis was made, untilthe last outpatient appointment at KCH, or death or liver transplanta-tion (LT).
All but four patients had been initially treated according to a stan-dard protocol with prednisolone 20–40 mg/daily alone or in combina-tion with azathioprine (1 mg/kg/day). The steroid dose wassubsequently individually tapered to the lowest required to maintainbiochemical remission, or eventually withdrawn and patients main-tained on azathioprine alone [16]. Initial therapy had been predniso-lone alone in 73 patients, while 87 had received combinationtherapy. Of the remaining four patients (all in Group 2), three had ini-tially received cyclophosphamide and the fourth D-penicillamine withprednisolone. Maintenance treatment regimens were prednisolonealone (5–10 mg/day) in 32 patients, prednisolone (2.5–7.5 mg/day)with azathioprine (1 or 2 mg/kg/day) in 66 patients and azathioprine(2 mg/kg/day) alone in 66 patients. Complete response to therapyand relapse during or after reduction or withdrawal of treatment weredefined according to the revised criteria of the IAIHG [2], and partialor no response to initial therapy according to the original criteria [17].Remission was defined as the absence of symptoms suggestive of arelapse and serum globulins/IgG and AST levels within the normalrange, with or without a liver biopsy showing only minimal inflamma-tion and no necrosis [16].
2.1. Statistical analysis
End-points for analyses were taken as the most recent clinic visit, orliver transplantation, or death. For quantitative data, analyses wereperformed using the Mann–Whitney and Kruskal–Wallis ANOVAtests for comparison of two and more than two independent groups,respectively. Differences in proportions were analysed by the Fisher’sexact test when the number of subjects was <5, and the Chi-square testfor 2 · 2 tables when the number of subjects in all cells was >5. Ther · c Chi-square test was used to investigate independent categories

T. Al-Chalabi et al. / Journal of Hepatology 45 (2006) 575–583 577
forming r rows and c columns where appropriate. Data are expressedas means ± standard deviations or medians and ranges as appropriate.All analyses were performed using StatsDirect (CamCode, Ashwell,Hertfordshire, England).
3. Results
Review of the records of the 164 patients revealedthat the peak age at presentation was in the fifth decadeof life, but with an almost equal number presenting inthe sixth decade (Fig. 1) and that, overall, 67% of thepatients presented at or above the age of 40 years. Themedian time to diagnosis (4 months) was identical forthe 43 patients who presented at 60 years of age orabove (Group 1) and the 121 who presented below(Group 2) this age (Table 1). There were no significantdifferences between the groups in serum biochemical orhaematological parameters at accession (Table 1) andthere was no correlation between time to diagnosisand clinical, biochemical or histological severity of dis-ease in either group. There were also no significant dif-ferences between older and younger patients withrespect to the frequencies or titres of ANA and SMA(Table 1). Overall, 88% (110/121) of patients in Group1 and 91% (38/41) patients in Group 2 who were tested,were autoantibody positive (ANA, SMA, LKM titreP40 at presentation or during follow-up). Of thepatients who were not autoantibody positive, 4/5 inGroup 1 and 5/11 in Group 2 were positive for asiagly-coprotein receptor (ASGP-R) antibodies. Eight patients(6.6%) in Group 2 had anti-LKM1 autoantibodies,which were not detected in any of the patients in Group1. Two patients had AMA, both in Group 2 (at 1:2560and 1:5120), but neither had any biochemical or histo-logical evidence of PBC either at presentation or during15 and 28 years of subsequent follow-up. Furthermore,despite deductions of four points for the presence of
< 20 20-29 30-39 40-49 50-59 60-69 70-80
Age (years)
10
30
20
40
Num
bers
of
patie
nts
50
Fig. 1. Distribution of age at presentation in 164 consecutive patients
with definite AIH.
AMA they both scored highly (19 and 24 points, respec-tively) for definite AIH.
3.1. Features at presentation
There were no significant differences in the modes ofpresentation (acute, insidious, or asymptomatic)between older and younger patients (Table 2a). The pre-senting clinical signs and symptoms were also very sim-ilar between the two groups, with painless jaundicebeing the commonest feature (Table 2a). There was,however, a significantly higher frequency of ascites(30% vs. 9%) in the older patients at presentation. Thisdid not appear to be related to the presence of cirrhosis,the incidence of which was not significantly differentbetween the two groups in the patients with ascites(8/13 vs. 5/11; p = 0.706).
The frequency of concurrent immunological disor-ders at the time of presentation was similar in bothgroups, with 37% of Group 1 and 31% of Group 2patients having at least one condition (p = 0.685). Intotal, 51 autoimmune conditions were identified eitherat presentation or during follow-up among the 43patients aged over 60 years whereas 112 conditions wereidentified among those patients <60 years. These dataare summarised in Table 2b. The commonest disorderswere thyroid disease (10 patients in Group 1, 15 inGroup 2) and rheumatoid arthritis (4 in Group 1, 8 inGroup 2). Two patients in Group 1 and four in Group2 had thyroiditis with one other concomitant extrahe-patic condition: rheumatoid arthritis, ulcerative colitis,alopecia areata, or vitiligo. However, it is noteworthythat the range of disorders in Group 1 was relativelyrestricted (thyroiditis, rheumatoid arthritis, hyperpara-thyroidism, ulcerative colitis and vitiligo). In contrast,the range of autoimmune disorders that presented inyounger patients was more diverse and included in addi-tion to those conditions specified in Group 1 type 1 dia-betes, Sjogren’s syndrome, vasculitis, multiple sclerosis,myasthenia gravis, erythema nodosum, polymyalgiarheumatica, and idiopathic thrombocytopenia purpura.
3.2. HLA markers and age
Analysis of the data for the 119 patients who had beenHLA typed revealed a higher frequency of the B8 allo-type and the A1-B8-DR3 or/and DR4 haplotype in theyounger patients but neither this trend nor differencesbetween the groups in frequencies of any other HLAmarkers were significant (Table 1). However, amongthe Group 1 patients the DR3 allotype occurred signifi-cantly more frequently in those who presented acutelythan in those with an insidious or asymptomatic presen-tation (7/11 vs. 3/16, p = 0.049). A similar associationwas not seen in the younger (Group 2) patients although,in this group, DR3 occurred significantly more frequent-

Table 1
Patient demographics and laboratory data at diagnosis
Group 1 (n = 43) Group 2 (n = 121) p
Males:Females 7:36 29:92 n.s.Age at diagnosis, median years (range) 65 (60–79) 41 (6–59) < 0.001Median months to diagnosis (range) 4 (0.5–96) 4 (0.3–108) n.s.Follow-up, median years (range) 9 (1–28) 14 (1–33) < 0.001Alkaline phosphatase, IU/L
Mean ± SD 280 ± 234 236 ± 169 n.s.Median (range) 220 (23–1435) 189 (45–1280)
Aspartate aminotransferase, IU/LMean ± SD 677 ± 548 794 ± 690 n.s.Median (range) 612 (23–2060) 620 (34–3512)
Gammaglutamyl transpeptidase, IU/LMean ± SD 266 ± 256 226 ± 197 n.s.Median (range) 172 (29–995) 174 (8–911)
Bilirubin, lmol/L ± SDMean 127 ± 149 123 ± 154 n.s.Median (range) 69 (8–609) 56 (8–1096)
Serum immunoglobulins, g/LIgG
Mean ± SD 27.11 ± 11.77 29.36 ± 11.95 n.s.Median (range) 25.65 (7.5–51.8) 27.5 (7.6–70.7)
IgMMean ± SD 2.24 ± 1.34 2.56 ± 2.16 n.s.Median (range) 2.1 (0.56–6.2) 2.2 (0.44–13.7)
IgAMean ± SD 4.31 ± 2.31 3.78 ± 2.07 n.s.Median (range) 3.6 (1.55–10.2) 3.6 (0.7–14.2)
Autoantibodies, median titres (ranges): frequencies (%)ANA 1:160 (1:40–1:5120) 1:160 (1:40–1:5120) n.s.
34/43 (79%) 95/121 (79%)SMA 1:160 (1:40–1:1280) 1:160 (1:40–1:2560) n.s.
30/43 (70%) 93/121 (77%)LKM 0 1:640 N/A
0/43 (0%) (1:160–1:2560)8/121 (7%)
HLA data (n = 27) (n = 92)A1 41% 54% n.s.B8 33% 51% n.s.DR3 41% 53% n.s.DR4 37% 36% n.s.A1-B8-DR3 or/and DR4 22% 40% n.s.
Upper normal limits: alkaline phosphatase, 130 IU/L; aspartate aminotransferase, 50 IU/L; gammaglutamyl transpeptidase, 50 IU/L; bilirubin,17 lmol/L; IgG, 18.0 g/L; IgM, 2.0 g/L; IgA, 4.0 g/L.Abbreviations: ANA, anti-nuclear antibodies; SMA, smooth muscle antibodies; LKM, type 1 liver–kidney microsomal antibodies; N/A, not
applicable.
578 T. Al-Chalabi et al. / Journal of Hepatology 45 (2006) 575–583
ly (63%) than DR4 (20%) in those with an acute presen-tation (p = 0.002). Additionally, in a separate analysis ofthe 119 patients, those who presented at or below the ageof 40 years had a significantly higher frequency of DR3(24/43 vs. 27/76, p = 0.049) and a significantly lower fre-quency of DR4 (6/43 vs. 28/76, p = 0.015) than thosewho were above 40 years of age at presentation. It wasalso noted that, in the total cohort, relapses occurred sig-nificantly more frequently in patients with DR3 than inthose without this allotype (46/59 vs. 34/60, p = 0.023).
Based on these findings, a separate sub-analysis wasperformed with patients stratified according to a cut-off of 40 years or older. These data are summarised inTables 3a and 3b.
3.3. Immunosuppression and outcome
There were no significant differences between the twogroups with respect to the proportions of patientsreceiving the different regimens of initial or maintenancetherapy (Table 4). More than 90% of patients in eachgroup showed a complete initial response to therapy.However, relapses during corticosteroid dose reductionsor withdrawal occurred significantly more frequently inthe younger patients, who also had multiple relapses sig-nificantly more frequently (Table 4). Seven patients inGroup 1 and 13 in Group 2 had all treatment withdrawnafter 2–12 years (median 5 years) in remission onmaintenance therapy. Nine of these (3 in Group 1, 6

Table 2a
Mode of onset and presenting signs and symptoms
Group 1(n = 43)
Group 2(n = 121)
p
Mode of onsetAcute 16 (37%) 44 (36%) n.s.Insidious 18 (42%) 54 (45%) n.s.Asymptomatic 9 (21%) 23 (19%) n.s.
Signs and symptomsJaundice 28 (65%) 89 (74%) n.s.Pale stools/dark urine 23 (53%) 64 (53%) n.s.Malaise 14 (33%) 48 (40%) n.s.Abdominal pain 11 (26%) 47 (39%) n.s.Lethargy 12 (28%) 29 (24%) n.s.Pruritus 7 (16%) 25 (21%) n.s.Arthralgia 2 (5%) 14 (12%) n.s.Ascites 13 (30%) 11 (9%) < 0.001Upper GI bleed 2 (5%) 5 (4%) n.s.Encephalopathy 1 (2%) 2 (2%) n.s.
T. Al-Chalabi et al. / Journal of Hepatology 45 (2006) 575–583 579
in Group 2) have sustained remission for 3–21 years(median 7.5 years) at the time of the present analysis.The remaining 11 patients relapsed within 1–7 years(median 1 year), but all showed a complete response tore-introduction of corticosteroids. Currently, 3 patients(all Group 2) are off all immunosuppressive therapy andremain in remission after 2, 7 and 10 years, respectively.
The proportions of patients who died of any cause orrequired liver transplantation during follow-up weresimilar for both groups (Table 4). One patient in Group1 and seven in Group 2 were transplanted. Althoughtransplantation or liver-related deaths in Group 1accounted for a lower proportion (5/13 = 38%) of alldeaths/transplants in this Group than that (18/27 = 67%) in Group 2, this difference was not statistical-ly significant (p = 0.177).
The incidence of cirrhosis at presentation was very sim-ilar in the two groups (Tables 5a and 5b). However, over-all, there was a significantly lower incidence of cirrhosison index liver biopsy in patients who presented acutelythan in those with an insidious or asymptomatic presenta-tion (7/60 vs. 39/102; p < 0.001). There was no significantdifference in the incidence of cirrhosis in patients withan insidious onset compared with those who wereasymptomatic at accession (25/70 vs. 14/32; p = 0.579).
Table 2b
Frequency of concurrent immunological disorders
Disease P60 yearsn = 51 (%)
<60 yearsn = 112 (%)
p
Other AI diseases 22/51 (43.1) 37/112 (33) n.s.Diabetes 2/51 (4) 7/112 (6.2) n.s.Thyroid disease 11/51 (21.5) 10/112 (8.9) n.s.Rheumatoid arthritis 4/51 (7.8) 5/112 (4.4) n.s.Asthma 1/51 (1.9) 1/112 (0.8) n.s.Ulcerative colitis 0/51 (0) 6/112 (5.3) n.s.>2 Autoimmune diseases 7/51 (13.7) 7/112 (6.2) n.s.
Follow-up biopsies within one to three years after startingtreatment were performed in 112 patients, significantlymore frequently in Group 2 patients than those in Group1. The large majority of patients in both groups showedimprovement in necroinflammatory grade in response totreatment (Table 5b). A majority in both groups alsoshowed no change in stage of fibrosis, although 30–40%showed some progression. Of the patients with cirrhosison index biopsy in whom follow-up histology was avail-able (5/13 in Group 1, 23/33 in Group 2), no patient dem-onstrated any resolution of cirrhosis.
3.4. Adverse effects of therapy
Cushingoid facies developed significantly more fre-quently in Group 1 patients than in Group 2 (26% vs.9%, p = 0.014), but these features disappeared in allpatients who were switched to azathioprine monothera-py. Apart from this, adverse events that may have beenrelated to the drug therapy were relatively infrequentand were not significantly different between the groups.Osteoporosis developed in 12% and 8%, respectively, ofGroup 1 and 2 patients, hypertension developed in 7%and 12%, and type 2 diabetes in 2% and 7%. Cytopeniadeveloped in 5% and 10%, respectively, of Group 1 andGroup 2 patients receiving azathioprine monotherapybut all but two of these cases had cirrhosis with hyper-splenism. Only two patients, both in Group 2, developedmild steroid psychoses on prednisolone, which resolvedin both cases with reduction of the dose.
Hepatocellular carcinoma (HCC) developed in eightpatients during follow-up (4 in each group). All eightpatients who developed HCC did so on a backgroundof histological evidence of cirrhosis. The prevalence ofHCC was 10.4% among 77 cirrhotic patients. HCC wasidentified at a median follow-up of 11.5 years (range 7–28 years) following diagnosis of AIH. Extrahepatic malig-nancies were diagnosed in fifteen patients (4 in Group 1and 11 in Group 2). In Group 1, these included basal cellcarcinoma (BCC), carcinoma of the stomach, breast andcolonic carcinoma. In group 2, extrahepatic malignanciesincluded breast carcinoma in 4 patients, BCC in 2patients, squamous cell carcinoma, pharyngeal carci-noma, lung carcinoma, renal and colonic carcinoma.
4. Discussion
In the present study, all patients had histologicallymoderate to severe AIH and may not therefore be typi-cal of a wider spectrum of disease seen in general gastro-enterology practice. Nonetheless, with 67% of ourpatients presenting at 40 years of age or above and26% presenting in their sixth decade of life, the findingsconfirm recent reports that AIH is predominantly a dis-ease affecting peri- and post-menopausal women

Table 3a
Summary of significant differences between patients presenting at or below age 40 years compared with those presenting at age 40 years or greater
Median 640 Range Median >40 Range p
Follow-up (years) 15 1–33 11 1.5–29 0.003Gammaglutamyl transpeptidase (IU/L) 103.5 8–820 190 29–995 0.04Histological stage at initial biopsy 1 0–4 4 0–4 0.001Histological grade on follow-up 2 1–2.25a 2 2–3a 0.022Histological stage on follow-up 3 1–4a 4 3–4a 0.008Median number of relapses 2 0–7 1 0–6 0.002
a Expressed as interquartile range.
580 T. Al-Chalabi et al. / Journal of Hepatology 45 (2006) 575–583
[7,10,11]. That one -third of our patients were under 40years of age is probably a reflection of referral bias to aspecialist centre, as has been suggested previously [10],and is very similar to the age distribution of patientsattending another specialist centre [11]. The present find-ings do not, however, confirm previous suggestions thatdiagnosis of AIH in the elderly is often delayed [11].Indeed, although the range was very wide, the mediantime to diagnosis was identical for patients presentingat or above (Group 1) and below (Group 2) the age of60 years.
Presenting features were very similar between the twogroups, including the frequency of concurrent immuno-logical disorders – although there was a wider range ofthese conditions in the younger patients. The only signif-icant difference was in the proportion of patients withascites at accession, which was greater in the olderpatients. The reason for this is unclear, but it was notobviously due to either a higher incidence of cirrhosisin older patients or a difference in the incidence of hyp-oalbuminaemia between the two groups. However, apossible explanation for the increased incidence of asci-tes in Group 1 patients is an enhanced susceptibility tothe physiological effects of fibrosis/cirrhosis withincreasing age. This concept is supported by the recentobservations that senescence is associated with pseudo-capillarization of the hepatic sinusoidal endothelium,and that this in turn results in increased rigidity of thesinusoid and increased resistance to blood flow [18,19].These findings could in part explain the increased prev-alence of ascites, without cirrhosis being apparent onbiopsy specimens. Alternatively, it could be explainedsimply by sampling variation within biopsy specimens,with the prevalence of cirrhosis being underestimated.
In this series we also identified 2 patients with detect-able anti-mitochondrial antibodies. In general, the find-
Table 3b
Summary of differences between patient groups when stratified according to ag
Patients 640 year, N
Cirrhosis on index biopsy 11 (19)Proportion of patients with any relapse 41 (69)Splenomegaly at presentation 19 (32)Spider naevi/palmar erythema at presentation 17 (29)
ing of detectable AMA is presumed to relate to eitherthe diagnosis of PBC or an overlap syndrome. Fromour data, it appears that occasional patients do existwith definite AIH who are positive for AMA, but,who lack evidence of either PBC or features of overlap.It is notable that M2 subtyping was not available foreither patient. However, neither patient demonstratedbiochemical or histological features of cholestasis overa long follow-up period, and responded completely toimmunosuppressive therapy without the addition ofursodeoxycholic acid.
Response to immunosuppressive therapy was excel-lent in both groups, with more than 90% showing a com-plete initial response, which was confirmed by theimprovement in histological grade in the 94% of patientswho had at least one follow-up liver biopsy. Follow-upbiopsies were performed significantly more frequentlyin the younger patients. This may have been due in partto a greater reluctance among older patients to undergothe procedure, but was more likely due to clinical indica-tions relating to the higher relapse rate in the youngerage group, although the overall outcome was not signif-icantly different between the groups. Thirty and thirty-seven percent, respectively, of patients in Group 1 andGroup 2 demonstrated progression of fibrosis on fol-low-up histology despite conventional treatment. Theapparent high incidence of progression of fibrosis mayreflect in part, tertiary referral centre bias, since manypatients with severe or difficult to control disease aremore likely to be referred to this centre. In addition,other studies have found progression of fibrosis inpatients on treatment [20].
The higher relapse rate in the younger patients wasthe most striking difference between the groups, withthe younger patients relapsing (and having multiplerelapses) during reduction or withdrawal of corticoste-
e >40 years
= 59 No. (%) Patients >40, N = 105 No. (%) p
35 (33) 0.08262 (59) 0.0918 (17) < 0.02548 (46) < 0.05
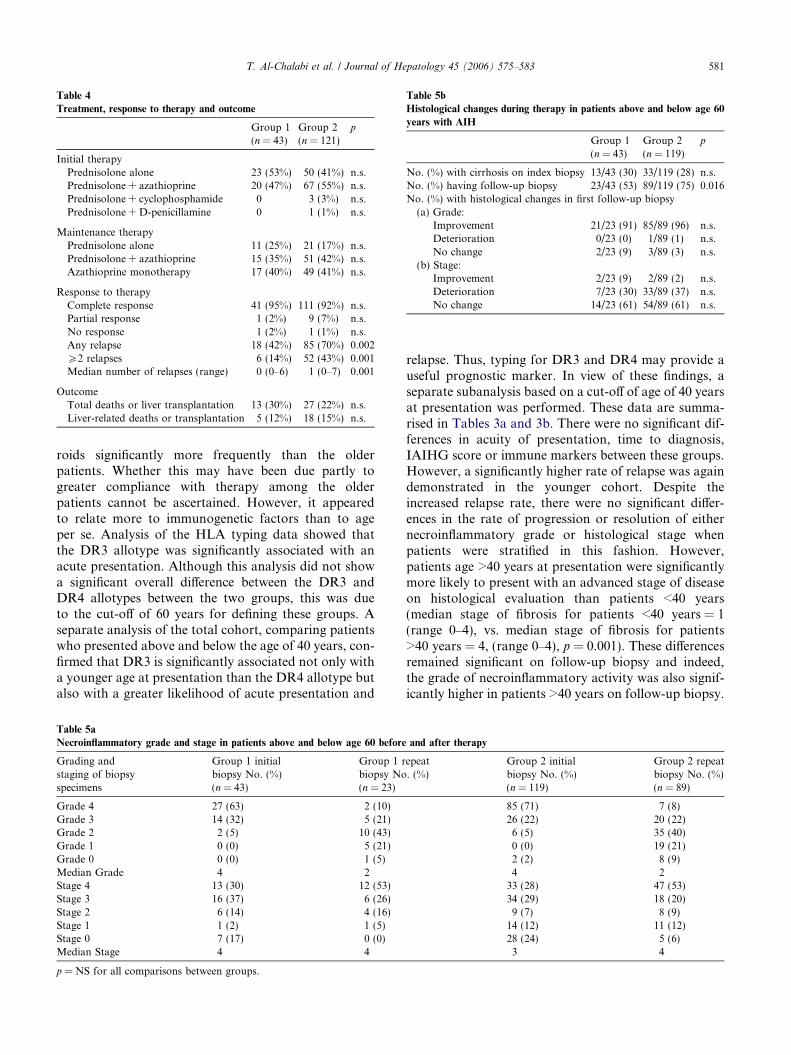
Table 4
Treatment, response to therapy and outcome
Group 1(n = 43)
Group 2(n = 121)
p
Initial therapyPrednisolone alone 23 (53%) 50 (41%) n.s.Prednisolone + azathioprine 20 (47%) 67 (55%) n.s.Prednisolone + cyclophosphamide 0 3 (3%) n.s.Prednisolone + D-penicillamine 0 1 (1%) n.s.
Maintenance therapyPrednisolone alone 11 (25%) 21 (17%) n.s.Prednisolone + azathioprine 15 (35%) 51 (42%) n.s.Azathioprine monotherapy 17 (40%) 49 (41%) n.s.
Response to therapyComplete response 41 (95%) 111 (92%) n.s.Partial response 1 (2%) 9 (7%) n.s.No response 1 (2%) 1 (1%) n.s.Any relapse 18 (42%) 85 (70%) 0.002P2 relapses 6 (14%) 52 (43%) 0.001Median number of relapses (range) 0 (0–6) 1 (0–7) 0.001
OutcomeTotal deaths or liver transplantation 13 (30%) 27 (22%) n.s.Liver-related deaths or transplantation 5 (12%) 18 (15%) n.s.
Table 5b
Histological changes during therapy in patients above and below age 60
years with AIH
Group 1(n = 43)
Group 2(n = 119)
p
No. (%) with cirrhosis on index biopsy 13/43 (30) 33/119 (28) n.s.No. (%) having follow-up biopsy 23/43 (53) 89/119 (75) 0.016No. (%) with histological changes in first follow-up biopsy
(a) Grade:Improvement 21/23 (91) 85/89 (96) n.s.Deterioration 0/23 (0) 1/89 (1) n.s.No change 2/23 (9) 3/89 (3) n.s.
(b) Stage:Improvement 2/23 (9) 2/89 (2) n.s.Deterioration 7/23 (30) 33/89 (37) n.s.No change 14/23 (61) 54/89 (61) n.s.
T. Al-Chalabi et al. / Journal of Hepatology 45 (2006) 575–583 581
roids significantly more frequently than the olderpatients. Whether this may have been due partly togreater compliance with therapy among the olderpatients cannot be ascertained. However, it appearedto relate more to immunogenetic factors than to ageper se. Analysis of the HLA typing data showed thatthe DR3 allotype was significantly associated with anacute presentation. Although this analysis did not showa significant overall difference between the DR3 andDR4 allotypes between the two groups, this was dueto the cut-off of 60 years for defining these groups. Aseparate analysis of the total cohort, comparing patientswho presented above and below the age of 40 years, con-firmed that DR3 is significantly associated not only witha younger age at presentation than the DR4 allotype butalso with a greater likelihood of acute presentation and
Table 5a
Necroinflammatory grade and stage in patients above and below age 60 before
Grading andstaging of biopsyspecimens
Group 1 initialbiopsy No. (%)(n = 43)
Group 1 rbiopsy No(n = 23)
Grade 4 27 (63) 2 (10)Grade 3 14 (32) 5 (21)Grade 2 2 (5) 10 (43)Grade 1 0 (0) 5 (21)Grade 0 0 (0) 1 (5)Median Grade 4 2Stage 4 13 (30) 12 (53)Stage 3 16 (37) 6 (26)Stage 2 6 (14) 4 (16)Stage 1 1 (2) 1 (5)Stage 0 7 (17) 0 (0)Median Stage 4 4
p = NS for all comparisons between groups.
relapse. Thus, typing for DR3 and DR4 may provide auseful prognostic marker. In view of these findings, aseparate subanalysis based on a cut-off of age of 40 yearsat presentation was performed. These data are summa-rised in Tables 3a and 3b. There were no significant dif-ferences in acuity of presentation, time to diagnosis,IAIHG score or immune markers between these groups.However, a significantly higher rate of relapse was againdemonstrated in the younger cohort. Despite theincreased relapse rate, there were no significant differ-ences in the rate of progression or resolution of eithernecroinflammatory grade or histological stage whenpatients were stratified in this fashion. However,patients age >40 years at presentation were significantlymore likely to present with an advanced stage of diseaseon histological evaluation than patients <40 years(median stage of fibrosis for patients <40 years = 1(range 0–4), vs. median stage of fibrosis for patients>40 years = 4, (range 0–4), p = 0.001). These differencesremained significant on follow-up biopsy and indeed,the grade of necroinflammatory activity was also signif-icantly higher in patients >40 years on follow-up biopsy.
and after therapy
epeat. (%)
Group 2 initialbiopsy No. (%)(n = 119)
Group 2 repeatbiopsy No. (%)(n = 89)
85 (71) 7 (8)26 (22) 20 (22)6 (5) 35 (40)0 (0) 19 (21)2 (2) 8 (9)4 2
33 (28) 47 (53)34 (29) 18 (20)9 (7) 8 (9)
14 (12) 11 (12)28 (24) 5 (6)3 4

582 T. Al-Chalabi et al. / Journal of Hepatology 45 (2006) 575–583
Frequently, uncertainty exists regarding the optimalduration of therapy required to maintain remission inpatients with AIH. In this study, for patients whorelapsed following drug withdrawal, this occurred onlyin the context of a treatment withdrawal trial, and inthat regard, the rate of relapse was 87% (26/30) ofpatients in whom therapy was withdrawn, from a cohortof patients who had been in remission from 1.5 to 9years [21]. In a report by Kanzler et al., of 28/103patients withdrawn from treatment, only sevenremained in remission over a mean follow-up of 8 years(range, 1.5–18 years) [22]. They concluded that treat-ment withdrawal should not be attempted before fouryears of continued therapy, and not at all if there wasany evidence of ongoing disease activity. They alsofound a higher relapse rate in patients with HLA A1-B8-DR3 and suggested that this should be taken intoaccount prior to stopping therapy. In this study, 9 of20 patients withdrawn from therapy remained in remis-sion, and HLA DR3 allotype was associated withincreased frequency of relapse, consistent with the previ-ous report.
Of interest, only 2 of our patients (both <60 andfemale) were reported to have steatosis in their liverbiopsies. Neither patient had been found to have steato-sis on their index biopsy, only in their follow-up biop-sies. Steatosis therefore in this cohort at least does notaccount for differences in relapse rates between thetwo groups of patients. However, as type II AIH is asso-ciated with an increased severity of disease and relapserate, the higher incidence of type II AIH in the youngercohort (8 patients in Group 2, and 0 patients in Group1) may in part account for the observed greater frequen-cy of relapses in patients <60 compared with patients>60.
Adverse effects and complications, which may havebeen due to therapy, were relatively infrequent.Although the incidence of side effects is relatively lowin both groups, it is important that these side effectsare actively managed. Despite this, the risk of such co-morbidities should not deter therapy in post-menopaus-al patients, given the known poor survival associatedwith untreated AIH. The use of steroids, with or withoutazathioprine, as maintenance therapy was similar inboth groups. In addition, whereas the incidence of ste-roid related effects such as hypertension and diabeteswas more common in younger patients, the developmentof Cushingoid facies associated with steroid usage wasmore common in older patients. Therefore, steroid relat-ed adverse events cannot be ascribed to differences insteroid doses between the two groups, however, differentage groups appear to be more susceptible to differentsteroid side effects. It has been traditional in some prac-tices to avoid or limit steroid usage in older patientsbecause of concerns of increased risks of medically sig-nificant adverse effects. Our results suggest that younger
patients are in fact more susceptible to hypertension anddiabetes than older patients. Whilst agreeing at least inpart with Verslype et al. that steroid therapy should beindividualized in elderly patients, it reiterates the needto introduce azathioprine earlier rather than later inpatient management, so that complete steroid withdraw-al can be facilitated in a timely manner [16,23]. Regard-ing osteoporosis as a specific side effect, the prevalencereported in this study is likely an underestimate, as bonemineral density (BMD) scans were not routinely per-formed in patients. Published Guidelines for the preven-tion of osteoporosis in chronic liver disease advocateBMD scans in all patients with cirrhosis or with anyother risk factors for osteoporosis at accession and bian-nually thereafter, even in patients with a normal scan[24].
An interesting observation in this report is the higherthan heretofore reported prevalence of HCC amongstpatients with established cirrhosis and AIH. In a previ-ous report from this institution, from a cohort of 217patients with AIH, 8 patients were identified (4% of cir-rhotic patients) who developed HCC [25]. Of thesepatients, 6/8 had evidence of HCV infection. In the pres-ent study, 10.4% of patients with cirrhosis at diagnosisdeveloped HCC during follow-up. This current seriesexcluded these previous eight patients and included onlypatients with definite AIH based on IAIHG criteria.Seven of the 8 current patients with HCC were main-tained on azathioprine +/� prednisolone as immuno-suppression. It is difficult to assess the significance ofazathioprine as a risk factor for the development ofHCC, since cumulative doses of azathioprine were sim-ilar in patients with and without cancer. Moreover, alco-hol ingestion does not explain the incidence of HCC,since only three patients of the complete cohort drankany alcohol in follow-up, of whom none developedHCC. In this current series, the prevalence of cirrhosismay have been underestimated, since it is based on his-tological criteria alone, and not all patients had histo-logical follow-up. Although there are no randomisedcontrolled trials evaluating the benefits of screening incirrhosis, current practice advocates screening inpatients with cirrhosis related to chronic HCV andHBV infection [26]. No formal guidelines exist regardingscreening for development of HCC among patients withautoimmune liver diseases [26,27]. Based on these preli-minary observations, we recommend routine HCCscreening in patients with AIH and known cirrhosis.
In a recent study [14], it was found that treatment hadbeen withheld in 42% of older patients with AIH, despiteevidence of relatively severe disease – suggesting that,outside of specialist centres, therapy is often inappropri-ately withheld from older patients. Untreated, the surviv-al rate for severe AIH approaches 40% within 6 monthsand 27% after 10 years [28,29]. Given the excellentresponse to therapy and overall outcome in this report,

T. Al-Chalabi et al. / Journal of Hepatology 45 (2006) 575–583 583
it is imperative that the disease be recognised and appro-priately treated. Although aging is associated with areduction in overall immune function described as immu-nosenescence, there is also experimental evidence ofimpaired hepatic regeneration following hepatic insultand injury in a number of model systems [30–33]. Forthat reason, though the severity of AIH may bedecreased in the older patient, as demonstrated by fewerrelapses, since hepatic regeneration may be impaired,hepatic injury may be less likely to be reversible furtheremphasizing the need for active treatment in the elderly.
References
[1] Ludwig J, McFarlane IG, Rakela J. Terminology of chronichepatitis. International Working Party. Am J Gastroenterol1995;90:181–189.
[2] Alvarez F, Berg PA, Bianchi FB, Bianchi L, Burroughs AK,Cancado EL, et al. International Autoimmune Hepatitis GroupReport: review of criteria for diagnosis of autoimmune hepatitis. JHepatol 1999;31:929–938.
[3] Heneghan MA, McFarlane IG. Current and novel immunosup-pressive therapy for autoimmune hepatitis. Hepatology2002;35:7–13.
[4] Donaldson PT, Doherty DG, Hayllar KM, McFarlane IG,Johnson PJ, Williams R. Susceptibility to autoimmune chronicactive hepatitis: human leukocyte antigens DR4 and A1-B8-DR3are independent risk factors. Hepatology 1991;13:701–706.
[5] Czaja AJ, Donaldson PT. Genetic susceptibilities for immuneexpression and liver cell injury in autoimmune hepatitis. ImmunolRev 2000;174:250–259.
[6] Donaldson PT, Czaja AJ. Genetic effects on susceptibility, clinicalexpression, and treatment outcome of type 1 autoimmunehepatitis. Clin Liver Dis 2002;6:419–437.
[7] Toda G, Zeniya M, Watanabe F, Imawari M, Kiyosawa K,Nishioka M, et al. Present status of autoimmune hepatitis in Japan-correlating the characteristics with international criteria in an areawith a high rate of HCV infection. Japanese National StudyGroup of Autoimmune Hepatitis. J Hepatol 1997;26:1207–1212.
[8] Reuben A. A sheep in wolf’s clothing. Hepatology2003;38:1596–1601.
[9] Lebovics E, Schaffner F, Klion FM, Simon C. Autoimmunechronic active hepatitis in postmenopausal women. Dig Dis Sci1985;30:824–828.
[10] Parker DR, Kingham JG. Type I autoimmune hepatitis isprimarily a disease of later life. QJM 1997;90:289–296.
[11] Schramm C, Kanzler S, Meyer zum Buschenfelde KH, Galle PR,Lohse AW. Autoimmune hepatitis in the elderly. Am J Gastro-enterol 2001;96:1587–1591.
[12] Yarze JC, Meyer zum Buschenfelde K-H, Lohse AW. Autoim-mune hepatitis. N Engl J Med 1996;334:923–924.
[13] Selby CD, Toghill PJ. Chronic active hepatitis in the elderly. AgeAgeing 1986;15:350–356.
[14] Newton JL, Burt AD, Park JB, Mathew J, Bassendine MF, JamesOF. Autoimmune hepatitis in older patients. Age Ageing1997;26:441–444.
[15] Batts KP, Ludwig J. Chronic Hepatitis. An update on terminol-ogy and reporting. Am J Surg Pathol 1995;19:1409–1417.
[16] Johnson PJ, McFarlane IG, Williams R. Azathioprine for long-term maintenance of remission in autoimmune hepatitis. N Engl JMed 1995;333:958–963.
[17] Johnson PJ, McFarlane IG. Meeting report: International Auto-immune Hepatitis Group. Hepatology 1993;18:998–1005.
[18] Hilmer SN, Cogger VC, Fraser R, McLean AJ, Sullivan D, LeCouteur DG. Age-related changes in the hepatic sinusoidalendothelium impede lipoprotein transfer in the rat. Hepatology2005;42:1349–1354.
[19] Huet PM, Villenueve JP. Microcirculation of the aging liver: isgetting old like having cirrhosis?. Hepatology 2005;42:1248–1251.
[20] Czaja AJ, Carpenter HA. Progressive fibrosis during corticoste-roid therapy of autoimmune hepatitis. Hepatology2004;39:1631–1638.
[21] Hegarty JE, Nouri Aria KT, Portmann B, Eddleston AL,Williams R. Relapse following treatment withdrawal in patientswith autoimmune chronic active hepatitis. Hepatology1983;3:685–689.
[22] Kanzler S, Gerken G, Lohr H, Galle PR, Meyer zum Buschen-felde KH, Lohse AW. Duration of immunosuppressive therapy inautoimmune hepatitis. J Hepatol 2001;34:354–355.
[23] Verslype C, George C, Buchel E, Nevens F, van Steenbergen W,Fevery J. Diagnosis and treatment of autoimmune hepatitis at age65 and older. Aliment Pharmacol Ther 2005;21:695–699.
[24] Collier JD, Ninkovic M, Compston JE. Guidelines on themanagement of osteoporosis associated with chronic liver disease.Gut 2002;50 (Suppl. 1):i1–i9.
[25] Ryder SD, Koskinas J, Rizzi PM, McFarlane IG, Portmann BL,Naoumov NV, et al. Hepatocellular carcinoma complicatingautoimmune hepatitis: role of hepatitis C virus. Hepatology1995;22:718–722.
[26] Fattovich G, Stroffolini T, Zagni I, Donato F. Hepatocellularcarcinoma in cirrhosis: incidence and risk factors. Gastroenterol-ogy 2004;127:S35–S50.
[27] Ryder SD. Guidelines for the diagnosis and treatment of hepato-cellular carcinoma (HCC) in adults. Gut 2003;52 (Suppl. 3):iii1–iii8.
[28] Soloway RD, Summerskill WH, Baggenstoss AH, Geall MG,Gitnick GL, Elveback IR, et al. Clinical, biochemical, andhistological remission of severe chronic active liver disease: acontrolled study of treatments and early prognosis. Gastroenter-ology 1972;63:820–833.
[29] Kirk AP, Jain S, Pocock S, Thomas HC, Sherlock S. Late resultsof the Royal Free Hospital prospective controlled trial ofprednisolone therapy in hepatitis B surface antigen negativechronic active hepatitis. Gut 1980;21:78–83.
[30] Hakim FT, Flomerfelt FA, Boyiadzis M, Gress RE. Aging,immunity and cancer. Curr Opin Immunol 2004;16:151–156.
[31] Wang X, Kiyokawa H, Dennewitz MB, Costa RH. The ForkheadBox m1b transcription factor is essential for hepatocyte DNAreplication and mitosis during mouse liver regeneration. Proc NatlAcad Sci USA 2002;99:16881–16886.
[32] Wang X, Krupczak-Hollis K, Tan Y, Dennewitz MB, Adami GR,Costa RH. Increased hepatic Forkhead Box M1B (FoxM1B)levels in old-aged mice stimulated liver regeneration throughdiminished p27Kip1 protein levels and increased Cdc25B expres-sion. J Biol Chem 2002;277:44310–44316.
[33] Conboy IM, Conboy MJ, Wagers AJ, Girma ER, Weissman IL,Rando TA. Rejuvenation of aged progenitor cells by exposure to ayoung systemic environment. Nature 2005;433:760–764.