author: erickson, amy m an evaluation of beneficial bites ... · 2 erickson, amy m. an evaluation...
TRANSCRIPT

1
Author: Erickson, Amy M
Title: An Evaluation of Beneficial Bites: A Nutrition Education Program for
Older Adults
The accompanying research report is submitted to the University of Wisconsin-Stout, Graduate School in partial
completion of the requirements for the
Graduate Degree/ Major: MS Food & Nutritional Sciences
Research Adviser: Dr. Kerry Peterson, RD
Submission Term/Year: August, 2012
Number of Pages: 73
Style Manual Used: American Psychological Association, 6th
edition
I understand that this research report must be officially approved by the Graduate School and
that an electronic copy of the approved version will be made available through the University
Library website
I attest that the research report is my original work (that any copyrightable materials have been
used with the permission of the original authors), and as such, it is automatically protected by the
laws, rules, and regulations of the U.S. Copyright Office.
My research adviser has approved the content and quality of this paper.
STUDENT:
Amy M. Erickson DATE: 7/27/2012
ADVISER: (Committee Chair if MS Plan A or EdS Thesis or Field Project/Problem):
Kerry D. Peterson, PhD, RD DATE: 7/27/2012
---------------------------------------------------------------------------------------------------------------------------------
This section for MS Plan A Thesis or EdS Thesis/Field Project papers only
Committee members (other than your adviser who is listed in the section above)
1. CMTE MEMBER’S NAME: Carol Seaborn, PhD, RD DATE: 7/27/2012
2. CMTE MEMBER’S NAME: Elizabeth Levaro, PhD DATE: 7/27/2012
3. CMTE MEMBER’S NAME: DATE:
---------------------------------------------------------------------------------------------------------------------------------
This section to be completed by the Graduate School This final research report has been approved by the Graduate School.
Director, Office of Graduate Studies: DATE:
2
Erickson, Amy M. An Evaluation of Beneficial Bites: A Nutrition Education Program for
Older Adults
Abstract
The purpose of this study was to determine the effectiveness of Beneficial Bites, a
comprehensive nutrition education program for older adults in Barron County, Wisconsin. A
survey was administered to 63 male and female attendees of the February Beneficial Bites
presentation and data were analyzed for changes in learning about and attitudes toward food and
healthy eating as related to program participation rates and relevant sociodemographic variables.
Participants ranged in age from 47 to 93 years, were predominantly White, female, retired,
married, and high school educated. Findings in support of program effectiveness were as
follows: 1) significantly more females than males reported increased confidence in healthy
cooking, confidence in making dietary changes, and motivation to make dietary changes; 2)
approximately two-thirds of participants reported increases in learning and positive attitudes
regardless of the number of presentations attended; 3) approximately three-fourths or more of
those attending five or more Beneficial Bites presentations reported increases in all learning and
attitude parameters; and 4) positive comments about the presentations, presenters, and program
content and design outweighed any other suggestion for improvement. Based on these findings,
Beneficial Bites was effective in enhancing participants’ nutrition knowledge and promoting
positive attitudes toward food and healthy eating.
3
The Graduate School
University of Wisconsin Stout
Menomonie, WI
Acknowledgments
First and foremost, I would like to thank my committee chair, Dr. Kerry Peterson, for her
dedication, guidance, encouragement, expertise, and patience throughout this process. Much
gratitude is also owed to my graduate program advisor and committee member, Dr. Carol
Seaborn, for her continued support, extraordinary commitment, and guidance throughout this and
my entire graduate experience. I would also like to thank Dr. Elizabeth Levaro, for graciously
lending her knowledge and experience. To all of my committee members, I extend my profound
appreciation for the time you dedicated on my behalf.
I also want to thank two people without whom this would not have been possible—Leslie
Fijalkiewicz, Nutrition Program Manager at the Barron County Government Center, and Susan
Greene of UW-Stout. To Leslie, thank you for your guidance, expertise, input, and enthusiasm.
To Susan, thank you for all of your help with my data analysis and interpretation—I could not
have done this without you!
Words cannot express how grateful I am to my parents. To my dad, your support has
meant the world to me. To my mom, thank you for listening, and for simply being the person
that you are—selfless, caring beyond compare, and resilient—your strength inspires me.
Without even realizing it, you teach me and everyone around you how to be a better person.
Last, but not least, I would like thank Nick for believing in me when I did not, for
building up my confidence when I was unsure, for reassuring me in times of stress, and for
pretending to be happy with takeout.

4
Table of Contents
............................................................................................................................................. Page
Abstract ...................................................................................................................................... 2
Acknowledgements ..................................................................................................................... 3
List of Tables .............................................................................................................................. 6
Chapter I: Introduction ............................................................................................................... 7
Statement of the Problem ............................................................................................... 11
Purpose of the Study ...................................................................................................... 12
Assumptions of the Study .............................................................................................. 12
Definition of Terms ................................................................................................................... 13
Chapter II: Literature Review .................................................................................................... 15
Healthful Aging and Nutrition Education ....................................................................... 15
Perceptions of and Attitudes toward Nutrition................................................................ 16
Nutrition Education Evaluations .................................................................................... 19
Barriers .............................................................................................................. 20
Successful strategies .......................................................................................... 21
Chapter III: Methodology .......................................................................................................... 28
Subject Selection and Description .................................................................................. 28
Instrumentation.............................................................................................................. 28
Data Collection Procedures ............................................................................................ 30
Data analysis ...................................................................................................... 30
Limitations .................................................................................................................... 32

5
Chapter IV: Results ................................................................................................................... 34
Characteristics of the Sample ......................................................................................... 34
Frequency of Beneficial Bites Attendance and Use of Information Provided .................. 38
Figure 1. Frequency distribution for the total number of presentations attended ............. 38
Relation of Program Participation and Changes in Learning and Attitudes Regarding
Food and Healthy Eating ....................................................................................... 39
Comparison of Learning and Attitudes for Limited and Frequent Attendees .................. 41
Changes in Learning and Attitudes across Gender, Marital Status, Educational
Attainment, and Income Level .............................................................................. 43
Barriers to Participation, Areas of Improvement, and Future Topics .............................. 48
Chapter V: Discussion ............................................................................................................... 50
Limitations .................................................................................................................... 50
Conclusions ................................................................................................................... 52
Recommendations ......................................................................................................... 58
References ................................................................................................................................ 61
Appendix A: Institutional Review Board Approval ................................................................... 65
Appendix B: Evaluation Tool .................................................................................................... 67
Appendix C: Informed Consent ................................................................................................. 72

6
List of Tables
Table 1: Sociodemographic Characteristics of the Sample ............................................................ 37
Table 2: Proportions Reporting Changes in Learning and Attitudes as a Result of
Attending 5 or more Beneficial Bites Presentations............................................................ 40
Table 3: Frequency of Learning and Attitude Changes by Limited (8 Presentations or Fewer)
and Frequent Attendance ................................................................................................... 42
Table 4: Frequency of Learning and Attitude Changes by Limited (12 Presentations or Fewer)
and Frequent Attendance ................................................................................................... 43
Table 5: Frequency of Learning and Attitude Changes by Gender ................................................ 45
Table 6: Frequency of Learning and Attitude Changes by Marital Status ...................................... 46
Table 7: Frequency of Learning and Attitude Changes by Educational Attainment ....................... 47
Table 8: Frequency of Learning and Attitude Changes by Income Level ...................................... 48

7
Chapter I: Introduction
Coinciding with the dramatic increase in the older adult population is the need for health
promotion and nutrition services for this unique group. As the baby boomers (those born
between 1946 and 1964) begin to turn 65, the number of older persons will continue to grow
significantly over the next couple decades, increasing from 40 million in 2010 to 72 million in
2030, representing nearly 20% of the total U.S. population (Federal Interagency of Aging-
Related Statistics, 2008; United States Census Bureau, 2012). This aging population constitutes
the greatest consumers of health care resources; thus the need for primary prevention strategies
involving nutrition interventions to address the anticipated corresponding increases in health care
expenditures cannot be overemphasized (Krondl, Coleman, & Lau, 2008).
The nutritional concerns for older adults are multifactorial and unique. In general, due to
a host of factors, the probability of experiencing poor nutrition status increases with age (Kamp,
Wellman, & Russell, 2010; Kuczmarski & Weddle, 2005; Manilla, Keller, & Hedley, 2010).
Decreases in appetite and early onset of satiety can change eating patterns and frequency, which
in turn may decrease energy intake and lead to nutrient deficiencies, frailty, more frequent
hospital admissions and longer lengths of stays, increased falls and fractures, and increased
morbidity and mortality rates (Kamp et al., 2010). Declines in olfaction, taste sensitivity, and
chewing and swallowing ability are common and may contribute to reduced interest in cooking
and consuming a variety of foods (Kuczmarski & Weddle, 2005; Savoca et al., 2010). Similarly,
eating alone is a recognized risk factor for declining eating behaviors (McClelland, Bearon,
Fraser, Mustian, & Velazquez, 2001). Greater risk of malnutrition among older adults can be
attributed to all of the former as well as problems in the oral cavity causing food avoidance and
loss of functionality which affects 42% of people aged 65 years and older (Bandayrel & Wong,
8
2011; Kamp et al., 2010). In particular, the effects of oral health problems have been related to
eating fewer fruits, vegetables, and nuts, causing lower intakes of many vitamins and minerals,
and to eating more foods high in cholesterol and sodium (Savoca et al. 2010). Loss of
functionality can also greatly impact the ability to do the physical tasks necessary for grocery
shopping and food preparation (Kamp et al., 2010).
Medications can have a profound effect on nutritional status, especially among older
adults who tend to suffer from more chronic medical conditions; as a result, medication use tends
to increase with advancing age. In a recent study examining polypharmacy and nutritional status
in older adults, Heuberger and Caudell (2011) found that increased medication use was
associated with decreased fiber intake and increased sodium, glucose, and cholesterol intakes.
Furthermore, declining physical health was associated with decreasing intake of major vitamins,
minerals, and electrolytes.
At the other end of the spectrum, obesity and overweight are also common, with obesity
affecting nearly 30% of older adults (Kamp et al., 2010). Convenient, single-serving foods
requiring minimal preparation are particularly attractive to this population but are notoriously
less nutrient-dense and higher in energy, often exacerbating preexisting conditions. Indeed, age-
related physical and metabolic changes necessitate certain dietary modifications (Sahyoun, Pratt,
& Anderson, 2004). While sarcopenia is known to cause problems for this population,
sarcopenia coupled with obesity can be even more severe, and both are associated with
immobility in addition to increasing age (Kuczmarski & Weddle, 2005).
Nutritional status is affected not only by the physiological changes associated with aging,
but by psychosocial issues and mental and cognitive changes as well. Potential effects of these
changes include undernutrition, overnutrition, and food insecurity (Kamp et al., 2010; Krondl,
9
Coleman, & Lau, 2008). An often overlooked problem among the aging population is
depression, which can be caused by social isolation, loss of spouse, financial difficulties, loss of
autonomy, impaired cognition, or any combination of the former (Kamp et al., 2010). Such
constraints can also contribute to decreased interest in food and often precede the loss of
motivation to eat or to eat healthful foods.
An emerging body of evaluation literature suggests that nutrition interventions made at
later ages can improve health status and quality of life (Sahyoun et al., 2004). Although some
physiological age-related declines are unavoidable, nutritional issues can be addressed to help
promote healthful aging, including the ability to maintain low risk of disease and disease-related
disability, maintaining high mental and physical function, and promoting active engagement in
life (Krondl et al., 2008; Kuczmarski & Weddle, 2005, p. 616). Even later in life, optimal
nutrition can help with retaining independence, deterring long-term care, and improving overall
quality of life (Bandayrel & Wong, 2011). For example, supplementation of antioxidant
vitamins, certain minerals, and omega-3 fatty acids have been shown to reduce factors of
cognitive decline in the elderly, such as inflammation and the vascular disease marker
homocysteine (Williams & Kemper, 2010). In a review of nutrition education program
outcomes, Higgins and Barkley (2003) report that, while print materials and lectures can be
effective in increasing nutrition knowledge, a majority of research indicates that the use of a
combination of complementing nutrition education techniques furthers outcome improvements
such as attitudes, dietary practices, and physiologic factors.
Beneficial Bites is a nutrition education program that is composed of multiple
components. Implemented in January 2010, this community-based nutrition education program
was developed by the Registered Dietitian/Nutrition Program Manager at the Barron County

10
Government Center, Wisconsin. The purpose of the program is to deliver relevant, practical,
research-based nutrition information emphasizing both why-to and how-to knowledge, all
without intimidation or reprimand (L. Fijalkiewicz, personal communication, June 6, 2012). By
featuring one functional or “powerhouse” food per month, the program emphasizes the value of
targeting small changes in the pursuit of long-term behavior change, with an ultimate goal of
increasing healthful dietary behaviors and promoting a greater understanding of the health
benefits that certain foods can provide. The featured functional foods are described by the
creator as those that provide health benefits above and beyond the usual vitamins, minerals,
protein, etc., and those with the power to prevent or improve health problems, as established by
the scientific literature and other reliable sources.
Although intended for older adults and catered to the older adult learner, the mission of
Beneficial Bites is to provide nutrition education to adults of all ages, reaching younger seniors,
as well as the broader aging community as well. Because funding for older adult nutrition
programs has not and will not keep pace with the aging population, it is an effort to promote
healthful aging and postpone the need for nutrition services later on in life among those nearing
older adulthood (L. Fijalkiewicz, personal communication, June 6, 2012).
A well-supported feature of the Beneficial Bites program is its comprehensive approach
to learning. This includes monthly nutrition education presentations involving a cooking
demonstration, food tasting, and user-friendly recipes adjusted for one or two servings, as well as
various forms of educational print materials—all focused on a functional food or specific
nutrition related topic. Each month, presentations are given by either the Nutrition Program
Manager (Registered Dietitian) or the head cook at each of five congregate meal sites or
community/senior centers in Wisconsin, including Barron, Cameron, Chetek, Cumberland, and
11
Rice Lake; a bimonthly presentation is also given at the Almena Town Hall. The educational
print materials corresponding to the monthly presentations include table tents displayed at each
of the centers, take-home recipes provided at each presentation, puzzles or games, and flyers
packaged with Meals on Wheels for delivery to homebound seniors.
Advertising for the program and presentation dates, times, and locations appear every
month in the free Barron County Senior Review newspaper, along with a Beneficial Bites article
on the topic to be presented. Participation in Beneficial Bites is free, requires no prior
registration, and provides entry into a prize drawing at each presentation, with the added
incentive of an additional entry for bringing a new participant. Although a brief, 5-item survey is
handed out to participants periodically, no formal evaluation of the program has been completed.
Statement of the Problem
Nutrition education plays an important role in promoting healthful aging by empowering
and teaching older adults how to make healthier dietary choices, strategies for cooking and
grocery shopping for just one or two, and easy, user-friendly recipes. Furthermore, participation
in community-based nutrition education programs provides increased opportunities for valuable
social interaction. Beneficial Bites is a multifaceted, community-based nutrition education
program utilizing several well-supported strategies tailored to the unique learning needs of older
adults. In the two years since its inception, no formal evaluation has been implemented to assess
the effectiveness of the program. By evaluating changes in attitudes toward food and healthy
eating and the extent of learning that has occurred among participants the Beneficial Bites staff
can make modifications to the program to increase its effectiveness.
12
Purpose of the Study
The purpose of this evaluation of the multi-component nutrition education program,
Beneficial Bites, was to determine the effectiveness of the program for enhancing participants’
knowledge of healthy eating and promoting positive attitudes toward food for better health. The
specific objectives were as follows:
1. Determine the relationship between learning about and attitudes toward food and
healthy eating and frequency of attendance at Beneficial Bites presentations
2. Compare the learning and attitude ratings between limited and frequent attendees
3. Examine the differences in learning and attitudes across gender, income level, marital
status, and educational attainment
4. Identify the prominent barriers to regular participation
5. Identify salient areas of improvement to the program
Assumptions of the Study
Several assumptions inherent to this research warrant comment. First, it was assumed
that the participants understood the survey and answered the questions truthfully. It was also
assumed that the survey respondents could reliably recall which Beneficial Bites presentations
they attended. In addition, certain survey questions aimed at measuring changes in attitudes
toward food and healthy eating were assumed to indicate changes in learning: namely, “My
confidence in healthy cooking has…”, “The belief that what I eat affects my health has…”, and
“My confidence in making changes to my diet has…” Correspondingly, it was also assumed that
nutrition knowledge and perceived benefits of dietary changes or healthy eating habits positively
influence food intake, though intake was not quantified in this research.

13
Definition of Terms
The following terms are defined here for the purpose of a better understanding of their
intended meaning for this paper.
Aging adults. To include the full range of Beneficial Bites participants and to recognize
the intent of the program, aging adults will refer to those aged 45 to 64 years, also referred to as
“younger” seniors.
Congregate nutrition sites. Community/senior centers or similar venues that serve
meals to adults aged 60 and over as provided for by the national Congregate Meal Program
(McClelland et al., 2001).
Malnutrition. A condition that occurs when the body does not receive adequate amounts
of nutrients due to a variety of reasons, including but not limited to inadequate or unbalanced
diet, problems with digestion or absorption, and certain medical conditions; both undernutrition
and overnutrition are examples (Krahn, Lengyel, and Hawranik, 2011; Zieve & Eltz, 2011).
Older adults. Most of the literature, as well as the U.S. Census Bureau, define older
adults as those aged 65 and older.
Paraprofessional. An employee trained by a professional to extend the delivery of
education and health promotion (McClelland, Irving, Mitchell, Bearon, & Webber, 2002).
Process evaluation. Data collected during implementation to support improvement of the
program (Keller, Hedley, Hadley, Wong, & Vaderkooy, 2005).
Sarcopenia. “The age-related loss of skeletal muscle mass … most often associated with
underweight” (Kuczmarski & Weddle, 2005, p. 465).

14
Successful/healthful aging. “The ability to maintain … low risk of disease and disease-
related disability, high mental and physical function, and active engagement of life” (Kuczmarski
& Weddle, 2005, p. 616; Rowe & Kahn, 1987).

15
Chapter II: Literature Review
This chapter will begin with a discussion of nutrition for successful aging, the importance
of nutrition education for older adults, and the need to evaluate those interventions. Older
adults’ perceptions of nutrition education efforts, their attitudes toward food and healthy eating,
and potential barriers to learning and participation in such programs will also be examined.
Lastly, various nutrition intervention evaluations will be described, highlighting specific
nutrition education strategies that have shown promise for older adult populations.
Healthful Aging and Nutrition Education
Nutrition plays a role in every step of disease prevention, contributing to successful aging
(Kuczmarski & Weddle, 2005; Rowe & Kahn, 1987). In primary prevention strategies, nutrition
helps to promote health and functionality. In secondary and tertiary prevention, medical
nutrition therapy is an integral part of disease management to reduce chronic disease risk, deter
disease progression, and alleviate disease symptoms. Even towards the end of the life cycle, the
goal of nutrition is to make later years healthful, enjoyable, and productive by preventing or
effectively managing chronic diseases.
Particularly for older adults, nutritional status affects functionality, independence, and
quality of life (Kamp et al., 2010). The corresponding increases in nutritional risk that occur
with aging, illnesses and chronic diseases, physical, cognitive, and social challenges, racial and
ethnic differences, and low socioeconomic status, can further complicate a situation. For these
reasons, the beneficial effects of nutrition for health promotion, risk reduction, and disease
management warrant emphasis among older adults (Krahn et al., 2011). Appropriate food and
nutrition programs including nutrition education and intervention services, adequately-funded
food assistance and meal programs, screening, assessment, counseling, therapy, monitoring,

16
evaluation, and outcomes documentation provide avenues to improve nutritional status and
ensure more healthful aging (Kamp et al., 2010). Additionally, reducing the number of risk
factors that can be avoided or modified through primary prevention and nutrition education
among middle-aged or “younger” older adults increases the probability of better health at more
advanced ages (Krondl et al., 2008).
An important component of successful aging is deterring age-related cognitive decline.
As mentioned in Chapter I, nutrition may play a role in this endeavor. In a randomized, double-
blind, placebo-controlled study by Wouters-Wesseling (2005), providing an enriched beverage
with moderate doses of all essential micronutrients to frail, elderly subjects for six months
produced significant increases in cognitive functioning, as measured by a word-learning test and
category fluency. Improvements in factors implicated in cognitive decline were also seen,
including an increase in plasma vitamin B12 concentration and a decrease in homocysteine
concentration. These data suggest that consuming foods rich in vitamins and minerals can
improve cognitive functioning even in the oldest old, providing greater impetus for designing
and promoting nutrition education for this population.
Perceptions of and Attitudes toward Nutrition
As with any intervention, it is of vital importance to assess the wants and needs of the
target audience. To explore the healthy eating perceptions of older adults in rural and northern
communities in Manitoba, Canada, Krahn et al. (2011) utilized a focus group approach. A
trained moderator conducted five focus groups of eight participants each, beginning with several
preplanned, open-ended questions posed to generate discussion for the purposes of establishing
the healthy eating perceptions of older adults and the factors influencing their food choices.

17
Findings indicated discrepancies between abstract and concrete nutrition knowledge.
Although all respondents reported that healthy eating was important and seemed to have limited
understanding of what it entails, knowledge deficits were observed regarding label reading,
understanding and visualizing portion sizes, as well as vitamin D recommendations and sources
(Krahn et al., 2011). Despite reported rates of nutritional risk of up to 68.7%, the use of food
assistance programs was minimal due to lacks of availability, transportation, or knowledge of
their existence, or individual resistance. These results indicate that there are inconsistencies
between the healthy eating perceptions and actions of older adults among this sample,
highlighting a need for nutrition education programs. This study also corroborates contentions
that information about community-based meal and nutrition education programs needs to be
more effectively communicated.
A similar study by Patacca, Rosenbloom, Kicklighter, and Ball (2004) used focus groups
to determine older adults’ opinions and attitudes toward a nutrition education program and
identify potential improvements. In this study, the nutrition education program consisted of
three nutrition lesson plans based on the Food Guide Pyramid and how to meet protein and fiber
needs, as well as self-assessment of current eating habits, a goal-setting activity, food tasting,
take-home handouts, and a question and answer session. Pre- and post-tests assessed changes in
nutrition knowledge. Six months after completion of the nutrition education program, six 45-
minute focus groups addressed opinions toward nutrition education, reasons for participating,
outcomes following the program, and suggestions for future programs.
Findings demonstrated that the majority of participants expressed a desire to learn more
about nutrition, which led to their participation in the program (Patacca et al., 2004). All
participants indicated an intent to participate in nutrition education in the future and most
18
reported wanting to participate because they found the lessons interesting and informative. A
majority reported a sustained change in their diet as a result of the nutrition education program,
with the most common changes including increased fruit and vegetable consumption and
decreased portion sizes.
Although the participants responded positively toward nutrition education, they tended to
view foods as “good” or “bad” and nutrition guidelines as “rules” or “orders” (Patacca et al.,
2004). This suggests that, in future nutrition education efforts for older adults, it may be
important to emphasize all foods can fit into a healthy diet in moderation. Despite these
connotations, most participants agreed that they would be more likely to set goals and follow
through with them if they were held accountable; in fact, the most common suggestion was to
include more goal-setting and subsequent monitoring as part of the nutrition education. Some
expressed that they would be more likely to make healthier choices if they knew a follow-up
session was ahead of them.
In a unique longitudinal study by Keller et al. (2006), a community-organized approach
was employed in the development of a nutrition education program for seniors. In this approach,
members of the target group were directly involved in the planning and delivery process to
ensure that activities and curriculum content met participant needs. Program activities included
monthly interactive food demonstrations or workshops, supplemented by a display board with
handouts and recipes, and a column in the center’s monthly newsletter. Other program
provisions included nutrition education resources for the center library and affordable fresh
produce at the center. Individual nutrition counseling, a cooking group for men, and a support
group for seniors with diabetes were added per participants’ requests.

19
To determine the impact of the program as measured by the extent of behavior change,
follow-up surveys were compared to baseline survey results from 3 years prior to the
intervention (Keller et al., 2006). Of the 251 survey respondents, 64.5% reported some level of
participation in the program, and 51% reported frequent participation in two or more activities.
From baseline to follow-up, findings demonstrated a significant decline in risk of low fruit and
vegetable intake and improved frequency of eating. Food workshops positively influenced food
practices more so than print materials, and program participants reported healthier nutrition
attitudes and beliefs compared to nonparticipants. These findings illustrate the importance of
assessing the unique needs, interests, and characteristics of each target population and
incorporating them into the planning and design of nutrition education programs to make the
content more relevant.
Nutrition Education Evaluations
Nutrition education efforts are frequently evaluated in an effort to demonstrate that
interventions made at a later age can improve health status and quality of life among older adults
(Sahyoun et al., 2004). To improve knowledge and consumption of more nutrient-dense foods
among older adults, Ellis, Johnson, Fischer, and Hargrove (2005) conducted a nutrition education
intervention directed at behaviors related to whole grain foods among congregate meal recipients
in senior centers in north Georgia. Based on the health belief model, key concepts of the
conceptual framework included perceived susceptibility to health conditions associated with low
intake of whole grains, perceived severity of these conditions that are common among older
people, perceived benefits of decreasing disease risk, perceived barriers to consuming more
whole grains, cues to action, and self-efficacy. Participants completed a pretest questionnaire
which included whole grain food consumption patterns and barriers to consumption,
20
anthropometrics, and other nutrition and health variables. Five lessons emphasized three main
messages: how to identify a whole grain food; whole grains protect against diseases; and “three
are key”—based on the MyPyramid recommendation to consume at least 3 ounces of whole
grains per day (Center for Nutrition Policy and Promotion, 2005).
Within three months after the last lesson, a post-test was administered to ascertain
knowledge and behavior changes related to whole grain foods (Ellis et al., 2005). Participants
demonstrated increased recognition of whole grain foods, increased intakes of whole grain bread,
whole grain cereal, and whole wheat crackers, as well as a stronger belief that whole grains
would reduce the risk of chronic disease. Additionally, barriers to increasing consumption were
more related to cost more so than taste or knowledge about the health benefits of whole grain
foods. Although the use recommended strategies was evident, particularly, the use of theory in
the framework of the intervention, notable limitations included self-reported outcome data,
limited information on potential barriers to whole grain food consumption, a primarily female,
Caucasian sample, and cognitive impairment among some participants.
Barriers. Just as nutritional status is subject to age-related effects, so are learning
characteristics. Besides the physical limitations experienced by older adults that may affect
learning, adult learning theory states that life-experience perceptions and social support can also
influence readiness and openness to changing behavior and motivation to learn new concepts
(Taylor-Davis et al., 2000). Using this theory Taylor-Davis et al. (2000) designed a nutrition
newsletter specifically for older adults and evaluated its effectiveness on cognitive, affective, and
behavioral domains. Two treatment groups received five biweekly nutrition newsletters. In
addition, one group received educator interaction by participating in structured process
evaluation interviews via telephone 10 to 14 days after newsletter distribution. A control group

21
completed the pretest and posttest surveys to ascertain differences in learning from the newsletter
and from the combined newsletter and telephone interviews. The telephone interviews focused
on newsletter use patterns, preferences for certain sections or topics, and short-term knowledge
gain. Pre- and post-tests assessed nutrition knowledge, willingness to answer items on a
nutrition knowledge test, perceived nutrition knowledge, interest in nutrition, food behavior, and
stages of change for dietary fat and fiber intake.
As a result of the intervention, treatment groups showed significant improvement in both
cognitive measures, both affective measures, and two behavioral measures as compared to the
control group (Taylor-Davis et al., 2000). Both treatment groups exhibited greater nutrition
knowledge, more willingness to answer nutrition knowledge test items, and greater perceived
nutrition knowledge and interest in nutrition than the control group. Furthermore, the group
receiving follow-up phone calls scored significantly better than the group receiving only
newsletters on both cognitive variables and perceived nutrition knowledge. Treatment groups
also performed better than the control on readiness to change dietary fiber intake and stages of
change to avoid dietary fats. These findings provide further evidence that older adults are not
only receptive to and benefit from nutrition education but may also experience greater benefits
still when proximal follow-up strategies are employed.
Successful Strategies. Reviews of research have identified salient program strategies
for effective nutrition education programs for aging populations (Higgins & Barkley, 2004;
Sahyoun et al., 2004). These strategies include: limiting educational messages to one or two
practical topics; emphasizing “how to” information; using interactive formats; providing hands-
on activities, incentives, cues, and frequent access to health professionals; and building upon
appropriate theories of behavior change. These strategies showed the most success in terms of
22
positive outcomes in nutrition knowledge. Notably, age was not a limiting factor in increasing
knowledge, suggesting the potential for beneficial effects of nutrition education even for the
oldest participants (Sahyoun et al., 2004).
Consistent with the Health Belief Model and increased chance of ill health among older
adults, interventions that targeted specific needs such as a health condition, provided nutrition
education to motivated persons, or addressed older adults’ unique health concerns were usually
more successful (Sahyoun et al., 2004). Other promising components consistent with those
identified in reviews by Bandayrel and Wong (2011) and Higgins and Barkley (2004) include
frequent collaboration between program participants and health professionals, individual
assessment of readiness to change, setting of achievable goals and a health plan, and the
promotion of self-efficacy. Additionally, a time frame of approximately 30 minutes for
educational sessions has been well-received in previous studies (McClelland et al., 2001).
Notably, goal-setting activities and corresponding follow-up activities that hold participants
accountable for knowledge gained and intentions to change may encourage initiation and long-
term maintenance of more healthful behaviors, as indicated in the study by Patacca et al. (2004).
Furthermore, using formative research in the initial phases of a nutrition intervention allows for
better matching of participants’ needs with the goals of the program and helps to identify
participants’ readiness to change (Sahyoun et al., 2004).
A study by Keller et al. (2005) examined the use of food workshops over a three-year
period in the Evergreen Action Nutrition Program as a useful method for providing cooking and
nutrition education for older adults. Workshops were highly interactive and involved a cooking
demonstration of a five-or-more-course menu, food tasting, and discussion of the food products,
their nutritional value, and preparation and storage techniques. Participants also received two
23
corresponding handouts—one with recipes and one with relevant nutrition and cooking
information. Two types of workshops following the aforementioned format were implemented:
single-session or stand-alone workshops and three-session series workshops following a central
theme. Process evaluation data were collected on each to determine the respective influences on
behavior change.
Several positive outcome measures were noted. A significant proportion of participants
reported an intention to change dietary behavior after attendance at a single-session workshop.
In the third year of programming, 81.5% of the participants were able to describe at least two
new things that they had learned (Keller et al., 2005). Participants of three-part series workshops
reported increased nutrition knowledge, interest in trying new foods, motivation to make dietary
changes, confidence in healthy cooking and making dietary changes, importance of healthy
eating, and increased belief that diet influences health.
Additionally, focus group data identified several program components as instrumental to
the success and empowerment of behavior change. These key components included: interactive
format, social experience, consistent high-quality education, and a small group size of less than
10 participants (Keller et al., 2005). Focus group participants also reported that the
demonstration and tasting helped to reinforce what they had learned by promoting use of the
recipes at home to ultimately change their eating behavior. Furthermore, the recipes provided
were thought to be essential to learning and relevant as they incorporated the new nutrition
information and supported concepts which included: sizing for one or two servings,
modifications for common health conditions such as diabetes and hypertension, consideration of
food cost and minimizing waste, and simplified food preparation techniques (Higgins & Barkley,
2004).
24
Another study examining the use of food tasting as a part of the larger Evergreen Action
Nutrition Program was that by Manilla et al. (2010). In an effort to promote continued interest in
food and enjoyment of eating, the purpose of this pilot study was to integrate a food-tasting
component into a nutrition education display designed for community-living older adults.
Monthly nutrition displays, which focused on practical and relevant nutrition information based
on previous feedback from senior center members and furnished recipes specific to the monthly
theme, provided the vehicle for the food-tastings. Once a month for three months during lunch at
the senior center, visitors who passed by the nutrition display were asked to sample two food
items, and those who sampled a food item were immediately asked to complete an anonymous
feedback form, for which they received a chance to win a meal at the senior center cafeteria.
Over three tasting events, 54 feedback forms were completed, representing 40% of those
who sampled the foods (Manilla et al., 2010). The number of copies of recipes taken differed
significantly for the two tasting foods at each display, suggesting that palatability or food
preference was an unavoidable factor despite preliminary recipe testing. Although 27.8%
reported that they might have made the recipe without tasting the food, 42.6% responded that
they would not have made these foods without tasting them. Among all respondents, 75.9%
indicated that they intended to prepare the sample food at home. These findings indicate that
including food tastings in nutrition education may increase the likelihood that participants will
prepare it themselves, which may in turn increase their interest in food and cooking, leading to
healthier eating behaviors and supporting autonomy. Tastings may also help to translate
nutrition messages into food behavior by promoting eating enjoyment as people age and
providing opportunities to try new foods and experiment with different flavors.
25
As nutrition educators, congregate nutrition site managers have the benefit of working
closely with the target population and being recognized as knowledgeable, caring, and willing to
help (McClelland et al., 2002). The use of such indigenous networks may prove advantageous in
nutrition education efforts involving the training of laypersons to extend the reach of health
promotion. Specifically, this established recognition may facilitate acceptance of trained
laypersons assuming an authoritative role in education by the constituency targeted for health
promotion. Based on this idea, a train-the-trainer approach, in which professionals train
paraprofessionals, may be useful in extending the reach of nutrition education programming.
To investigate this, four congregate nutrition site managers received 4 hours of training
over 2 days on an 8-week nutrition education module, “Meals on a Budget”, as well as record
keeping, survey administration, adult learning styles, and educational delivery methods
(McClelland et al., 2002). Pre- and post-tests were used to assess the level of confidence each
site manager attained in ability to teach the module. As a result of training, all site managers
reported positive changes in confidence and ability. Congregate nutrition site participants
indicated comfort with the site managers delivering the program and the majority reported high
levels of satisfaction with the nutrition information they received. Not only do these findings
suggest that trained laypersons can be effective in delivering health promotion, but also, that
nutrition program participants are receptive to education delivered by paraprofessionals.
However, this interpretation necessitates the consideration of several study limitations. As self-
report measures were subjective, focusing on participant satisfaction and comfort level, data
cannot be taken to reflect actual behavior change leading to improved nutritional status.
Correspondingly, while a rapport between educator and learner is important, relationships and
frequent contact may influence biased responses. Perhaps most importantly, observational

26
fidelity checks to determine whether the managers were implementing modules as intended were
limited to two out of eight occasions.
It is thought that congregate nutrition sites constitute an effective means of reaching older
adults and provide a convenient location for nutrition education programs (McClelland et al.,
2001). Traffic through these sites includes older adults who are likely to attend on a regular
basis, and follows a fairly predictable cycle providing some down time between arrival and
departure, usually before lunch is served. Also, the provision of meals is thought to create a
“ready audience” with a primed mindset of food and nutrition issues. Important considerations
to be made in planning the use of congregate nutrition sites as nutrition education venues include
background noise, interruptions, and other distractions.
The body of evidence describing meaningful changes in nutrition knowledge among
older adults as a result of interventions and education is growing. Optimal nutrition is integral to
successful aging and older adults have proven to be a more captive audience to this information
than previously thought. Ongoing evaluative research on nutrition education programs is needed
to further determine the most efficacious strategies for reaching this expanding population.
Therefore, the purpose of the present study was to determine the effectiveness of the
comprehensive nutrition education program, Beneficial Bites, in enhancing participants’
nutrition knowledge and promoting positive attitudes toward food and healthy eating. The
objectives were as follows: 1) to determine the relationship between learning and attitudes
regarding food and healthy eating and frequency of attendance at Beneficial Bites presentations;
2) to compare the learning and attitude ratings between limited and frequent attendees; 3) to
examine differences in learning and attitudes across gender, income level, marital status, and
27
educational attainment; 4) to identify the prominent barriers to regular participation; 5) to
describe salient areas of improvement to the program.
28
Chapter III: Methodology
This study was designed to determine the effectiveness of Beneficial Bites, a multi-
component nutrition education program, in enhancing older adults’ nutrition knowledge and
promoting positive attitudes toward food and healthy eating. In addition to assessing differences
in learning among participants, this study also sought to reveal prominent barriers to
participation, frequency of attendance at program presentations, general changes in eating
behaviors of previously unfamiliar targeted foods since participating, usefulness and interest in
the information presented, and areas of improvement. Prior to beginning, all procedures were
approved by the University of Wisconsin-Stout Institutional Review Board for the Protection of
Human Subjects (Appendix A).
Subject Selection and Description
Participants of this study included 63 attendees, aged 47 to 93, of the February Beneficial
Bites nutrition education presentation at each of five local community/senior centers in Barron
County, Wisconsin, including: Barron, Cameron, Chetek, Cumberland, and Rice Lake. To
ensure more accurate participation data, the only exclusion criterion was the incidence of short
term memory loss, or participation in the Adult Day Program at the Rice Lake Senior Center as
determined by the survey administrator/presenter for that location who was familiar with the
participants.
Instrumentation
The evaluation tool used in this study was a 13-item pen and paper survey (Appendix B),
developed by the researcher in collaboration with the Nutrition Program Manager/creator of
Beneficial Bites, and research adviser and committee member from UW-Stout. Intended to be
used for the purpose of this study only, questions were designed to gather data on Beneficial

29
Bites attendance, barriers to attendance, behavioral and attitudinal changes as a result of
participation, areas for improvement, and participant demographics.
Preliminary questions in the instrument determined the participant’s age and gender.
Additionally, to differentiate respondents who can actively use the presentation information and
those who attend but may rely on a caretaker for meals, questions regarding cooking and grocery
shopping responsibilities were included. To ascertain the number of presentations attended,
Question 1 included a list of the first two years of Beneficial Bites presentation topics to aid in
memory recall for respondents to indicate if they had attended. The second part of Question 1
was used to establish the prominent barriers to attendance. Respondents were asked to report, if
they had attended fewer than 5 presentations, what has prevented them from attending, and were
then asked to skip to Question 5.
Questions 2 through 4 were intended for those who had attended five or more Beneficial
Bites presentations. To determine the frequency of use of information and materials among this
sample, Question 2 asked about use of the featured recipes while Question 3 asked about
consumption and use of the featured foods/ingredients. Question 4 was modeled after an
evaluation study by Keller et al. (2005) that assessed changes in cooking/eating behavior as a
result of attending food workshops similar in design to the Beneficial Bites program. This
question contained 7 items to assess learning and attitudinal changes—such as knowledge of
nutrition and confidence and motivation to make dietary changes—which were recorded as
“increased”, “decreased”, or “not changed”.
Questions 5 and 6 were opened-ended questions aimed at collecting participant feedback.
All respondents were asked to provide their thoughts on how Beneficial Bites presentations
30
and/or attendance could be improved, as well as suggestions for topics or foods to be covered in
the future.
The remaining questions were modeled after a more detailed participant profile designed
to describe demographics for older adults (E. Levaro, personal communication, January 10,
2012). Relevant sociodemographic data including perceived health status, current employment
status, educational attainment, marital or partner status, living situation, and income were
gathered in Questions 7 through 13. A question regarding race or ethnicity was not included as
the vast majority (96.1%) of Barron County residents are Caucasian (United States Census
Bureau, 2012).
Data Collection Procedures
Survey procedures took place prior to the Beneficial Bites presentation at each location to
avoid missing potential participants due to early departure. Beginning with a short introduction
and explanation of the study, participants were familiarized with the purpose and procedures of
this research, as well as the hope to use the information gathered to improve the Beneficial Bites
program. Informed consent (Appendix C) was provided prior to survey administration and
participants were assured that involvement in the study was completely voluntary, that their
surveys would remain anonymous, and that they could withdraw at any time. Participants were
also encouraged to be as honest as possible in their answers, and to address any questions they
had along the way to the survey administrator.
Data analysis. A number of statistical analyses were used in this study to evaluate the
effectiveness of the Beneficial Bites program, as determined by differences in learning and
attitudes regarding food and healthy eating based on frequency of attendance at Beneficial Bites
presentations. The Statistical Program for Social Sciences (SPSS) version 17.0 was used to

31
analyze the data. A standard of p < 0.05 determined significance for all statistical analyses
conducted.
Frequencies were determined and reported for sociodemographic variables (age, gender,
health status, employment status, education level, marital status, household status, income level,
and income comfort level); cooking and grocery shopping responsibilities; presentations
attended; barriers to regular attendance at Beneficial Bites presentations; use of the featured
recipes and featured foods/ingredients; and changes in learning and attitudes as a result of
participating in Beneficial Bites. Similar written-in responses regarding barriers to participation,
areas of improvement, and future foods or topics were categorized and frequencies were used to
establish any patterns.
To determine if a relationship occurred between the number of presentations attended and
changes in learning and attitudes regarding food and healthy eating (increased, decreased, or no
change), Spearman’s Rho correlation was used for each of the following learning and attitude
measures: knowledge of nutrition, confidence in healthy cooking, personal value of healthy
eating, the belief that foods consumed affect health, confidence in making dietary changes, and
motivation to make dietary changes, as well as overall health compared to similarly aged
persons.
To determine differences in learning or attitudes among those who attended at least five
presentations, respondents were separated into low and high attendee groups. Low attendance
was defined in two ways: those who had attended eight or fewer of the monthly presentations in
two years, and those who had attended twelve or fewer presentations total. To obtain sufficient
observations for statistical analyses, the original rating scale for each learning and attitude
measure was collapsed into two categories: 1) increased and 2) decreased or no change.

32
Cross tabulation and Chi-square analyses were used to compare differences in the
frequencies of learning and attitude changes and overall health changes among participants who
had attended five or more presentations. Learning and attitude changes were compared for
limited and frequent attendees using Fisher’s Exact test, with limited attendance defined as eight
or fewer presentations and as twelve or fewer presentations, and frequent attendance defined as
nine or more presentations and as thirteen or more presentations.
To further determine differences in the frequency of learning and attitude changes, Cross
tabulation and Chi-square analyses with Fisher’s Exact test for statistical significance were also
conducted for each of the following sociodemographic variables: gender, marital status,
educational attainment, and income level. To obtain adequate observations, marital status,
educational attainment, and income level were each collapsed into two categories: married or
living with partner and widowed, divorced, separated, or single; high school diploma or less and
some vocational training or more; and $29,999 or less and $30,000 or more, respectively. The
same statistical analyses were attempted for income comfort level as well, however, the test
could not be performed due to a limited distribution of the data.
Limitations
The first limitation of this study was the lack of a pre/post design. In addition to the
process evaluation data presented, baseline nutrition knowledge, food frequency, and health
status data for each participant would have provided more concrete measures of the effectiveness
of the program and would have allowed absolute changes to be determined.
An additional limitation was the sampling procedure. The population for this study was
limited to participants of the Barron County Beneficial Bites presentations in February 2012. As
such, it is possible that some regular participants were unable to attend this particular month’s

33
presentation. Also, the total number of attendees was not recorded at every location, which
would have allowed the participation rate to be calculated.
The self-reported data collected by the survey was a limitation in several ways. As
alluded to in the aforementioned assumptions of this investigation, because the survey required
respondents to accurately recall which Beneficial Bites presentations they had attended,
inaccurate responses may have limited the data on survey items that depended on a certain
number of attended presentations, namely, the question regarding barriers to participation and
those aimed at measuring changes in learning and attitudes regarding food and healthy eating.
Furthermore, consistent with an inherent problem with survey methodologies, some respondents
failed to report answers to all questions for unknown reasons, limiting the data on some survey
items. Also, as surveys were administered prior to presentations to avoid missing early
departures, there may have been a perceived time constraint among respondents that prevented
them from contributing responses to open-ended questions.
An additional limitation was identified in the researcher’s instrument. Prior to Question
2, the survey instructed participants to skip to Question 5 if they had attended fewer than five
Beneficial Bites presentations, but to proceed to the following questions if they had attended
more than 5 presentations. The latter statement should have read, “If you have attended 5 or
more presentations,” to include those who had attended five presentations in the instructions to
answer the subsequent questions regarding use of the featured recipes and foods and changes in
learning and attitudes. Of the three participants who attended five presentations, only one
followed the errant survey instructions and skipped to Question 5; data collected from the other
two were included in the analyses of resulting behaviors and learning and attitudes changes of
those who had attended more than five presentations.

34
Chapter IV: Results
This chapter summarizes the results of the research study designed to evaluate the
effectiveness of Beneficial Bites, a comprehensive nutrition education program for aging and
older adults. Effectiveness of this program was determined by positive changes in learning and
attitudes regarding food and healthy eating. This research was completed to achieve the
following objectives: 1) determine the relationship between learning and attitudes regarding food
and healthy eating and frequency of attendance at Beneficial Bites presentations; 2) compare the
learning and attitude ratings between limited and frequent attendees; 3) examine differences in
learning and attitudes across gender, income level, marital status, and educational attainment; 4)
identify the prominent barriers to regular participation; and 5) describe salient areas of
improvement to the program.
This chapter presents the characteristics of the survey respondents. Findings on the
frequency of Beneficial Bites attendance, participant use of the featured foods and recipes, and
the relationship between program participation and changes in six measures of learning and
attitudes regarding food and healthy eating as well as perceived health status will be discussed.
Subsequently, analyses of changes in learning and attitudes and perceived health status in
relation to sociodemographic characteristics of the sample are examined. Lastly, the prominent
barriers to attendance are summarized, and suggestions for improvement and future foods and
topics are presented.
Characteristics of the Sample
Participants of this study included 63 attendees of the February Beneficial Bites nutrition
education presentation at each of five local community/senior centers in Barron, Cameron,
Chetek, Cumberland, and Rice Lake, of Barron County, Wisconsin. The majority (82.5%) were

35
female (n = 52) and 12.7% were male (n = 8), ranging in age from 47 to 93 years, with a mean
and median age of 74 and 75 years, respectively. The most common ages were 72 and 81 (n = 4
for each). Of the 63 survey respondents, three failed to report gender, another three failed to
report age, and one person responded with “60+”, which was removed from the age statistics.
Similarly throughout the survey, some participants failed to report answers for other
sociodemographic questions as well. However, because different sections of the survey were
sampled from to answer the research questions, all data were included in the following analyses,
regardless of survey completion.
Ten respondents failed to indicate whether they are the primary meal preparer and 14
failed to indicate whether they are the primary grocery shopper for their household. Out of 53
responses about meal preparation responsibilities, 86.8% (n = 46) reported being the primary
meal preparer. Similarly, out of 49 responses, 87.8% of (n = 43) reported being the primary
grocery shopper for their household. Fifteen participants failed to report that number of persons
they cook for; of those that did, more than half (52.1% or n = 25) reported cooking for two
people, while 37.5% (n = 18) reported cooking for one (N = 52). Two participants indicated that
they cook for three people and one subject each answered 1-2, 4-6, and 2-8 people.
A majority of participants were retired (76.2% or n = 48). Six indicated some form of
employment—part time, full time, or self-employed and two reported that they were unemployed
but looking for work.
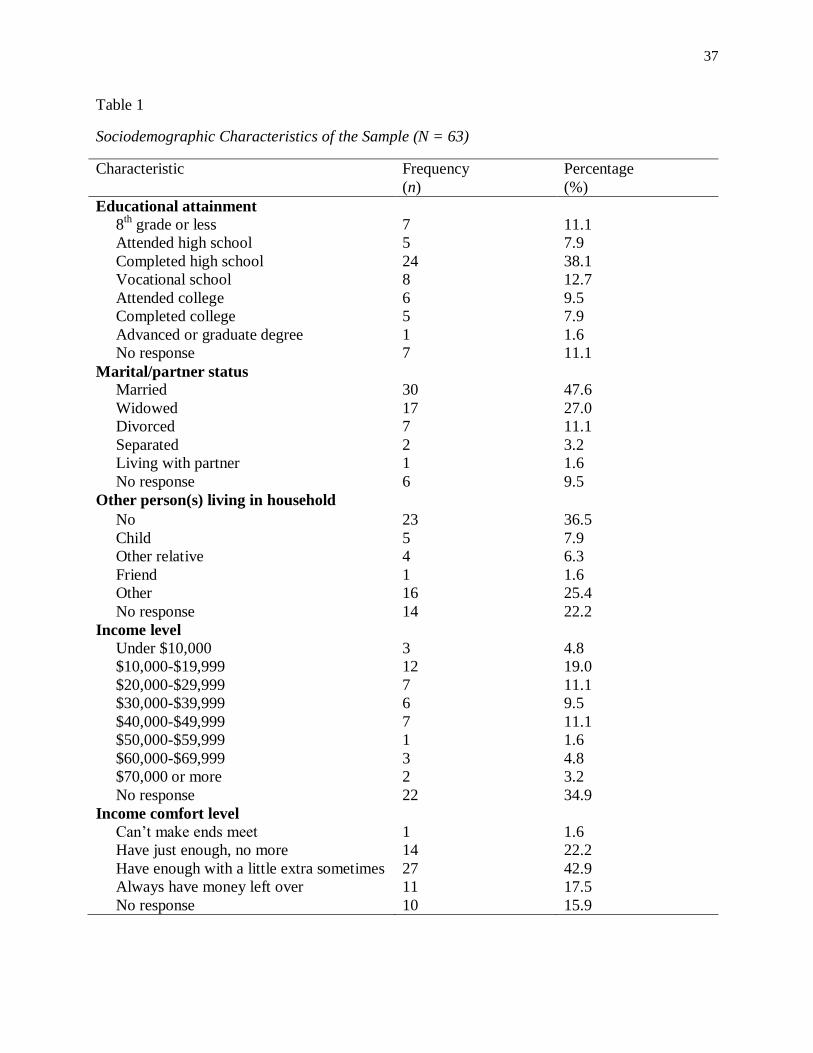
Table 1 presents a frequency distribution of other sociodemographic characteristics of the
sample. More than half of the participants (57.1%) had completed high school or less, while
31.7% had completed some college or vocational school. Nearly half were married (47.6%)
while 27.0% were widowed, 11.1% were divorced, and 3.2% were separated. A portion (36.5%)

36
reported living alone, while 25.4% indicated one other person in their household (usually the
spouse) and 7.9% still had a child living with them. Most participants (19.0%) reported an
income under $20,000; 11.1% reported an income between $20,000 and $29,999 and $40,000
and $49,999 each. Regarding ability to get along on their income, most participants reported
having enough with a little extra sometimes, followed by having just enough and no more,
always having money left over, and unable to make ends meet.
37
Table 1
Sociodemographic Characteristics of the Sample (N = 63)
Characteristic Frequency
(n)
Percentage
(%)
Educational attainment
8th
grade or less
Attended high school
Completed high school
Vocational school
Attended college
Completed college
Advanced or graduate degree
No response
Marital/partner status
Married
Widowed
Divorced
Separated
Living with partner
No response
Other person(s) living in household
7
5
24
8
6
5
1
7
30
17
7
2
1
6
11.1
7.9
38.1
12.7
9.5
7.9
1.6
11.1
47.6
27.0
11.1
3.2
1.6
9.5
No 23 36.5
Child 5 7.9
Other relative 4 6.3
Friend 1 1.6
Other 16 25.4
No response 14 22.2
Income level
Under $10,000
$10,000-$19,999
$20,000-$29,999
$30,000-$39,999
$40,000-$49,999
$50,000-$59,999
$60,000-$69,999
$70,000 or more
3
12
7
6
7
1
3
2
4.8
19.0
11.1
9.5
11.1
1.6
4.8
3.2
No response 22 34.9
Income comfort level
Can’t make ends meet
Have just enough, no more
Have enough with a little extra sometimes
Always have money left over
1
14
27
11
1.6
22.2
42.9
17.5
No response 10 15.9
38
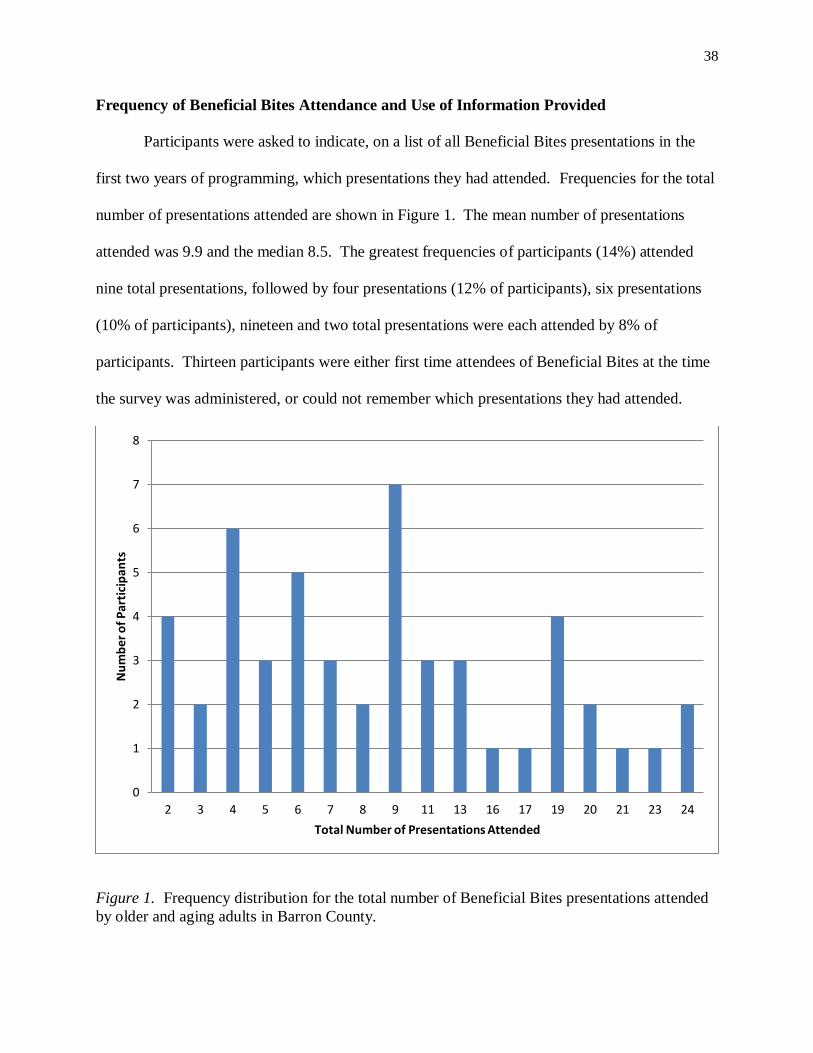
Frequency of Beneficial Bites Attendance and Use of Information Provided
Participants were asked to indicate, on a list of all Beneficial Bites presentations in the
first two years of programming, which presentations they had attended. Frequencies for the total
number of presentations attended are shown in Figure 1. The mean number of presentations
attended was 9.9 and the median 8.5. The greatest frequencies of participants (14%) attended
nine total presentations, followed by four presentations (12% of participants), six presentations
(10% of participants), nineteen and two total presentations were each attended by 8% of
participants. Thirteen participants were either first time attendees of Beneficial Bites at the time
the survey was administered, or could not remember which presentations they had attended.
Figure 1. Frequency distribution for the total number of Beneficial Bites presentations attended
by older and aging adults in Barron County.
0
1
2
3
4
5
6
7
8
2 3 4 5 6 7 8 9 11 13 16 17 19 20 21 23 24
Nu
mb
er o
f P
arti
cip
ants
Total Number of Presentations Attended

39
Although the survey intended to measure featured recipes and food use of participants
who had attended five or more Beneficial Bites presentations, some participants answered
regardless. Of the 33 that responded to recipe use, the largest number reported using the featured
recipes once a month (n = 21), followed by once a week (n = 7). One person reported using the
recipes three times a week and four reported never using the recipes. Use of the featured
foods/ingredients followed a similar pattern. Of the 36 that responded to the question, most
reported eating or cooking with the featured foods/ingredients once a month (n = 17), followed
by once a week (n = 10). Two people reported eating or cooking with the foods three times a
week and seven reported never consuming the featured foods.
Relation of Program Participation and Changes in Learning and Attitudes Regarding Food
and Healthy Eating
Six survey questions assessed changes in learning and attitudes regarding food and
healthy eating as a result of participating in Beneficial Bites. An additional question assessed
any change in overall health. Table 2 presents the proportions of participants reporting changes.
A majority of participants—nearly two thirds or more—reported increases in every category.
The greatest proportions of participants reported increases in nutrition knowledge, motivation to
make dietary changes, importance of healthy eating, and belief that what one eats affects one’s
health. More respondents consistently chose “no change” over “decreased”. Overall health,
confidence in making dietary changes, and confidence in healthy cooking showed the greatest
proportions of participants reporting no change at 33.3%, 23.8%, and 16.3%, respectively.

40
Table 2
Proportions Reporting Changes in Learning and Attitudes as a Result of Attending 5 or more
Beneficial Bites Presentations (N= 63)
Learning and attitude measures Increased
(%)
Decreased
(%)
Unchanged
(%)
Knowledge of nutrition (n = 42) 88.1 2.4 9.5
Confidence in healthy cooking (n = 43) 79.1 4.7 16.3
Importance of healthy eating in my life (n = 43) 86.0 14.0
Belief that what I eat affects my health (n = 40) 85.0 15.0
Confidence in making dietary changes (n = 42) 73.8 2.4 23.8
Motivation to make dietary changes (n = 42) 88.1 11.9
Overall health (n = 42) 61.9 4.8 33.3
Note. Percentages are out of those who responded (n).
This study aimed to examine the relationship between the frequency of Beneficial Bites
participation and learning and attitude ratings (increased, decreased, or unchanged). Spearman’s
Rho correlation analyses showed no significant association between the total number of
presentations attended and any of the following learning or attitude ratings: nutrition knowledge
(rs = 0.04, p > 0.05), confidence in healthy cooking (rs = 0.01, p > 0.05), personal importance of
healthy eating (rs = 0.08, p > 0.05), belief that foods consumed affect health (rs = -0.01, p >
0.05), motivation to make dietary changes (rs = 0.05, p > 0.05), or overall health (rs = -0.08, p >
0.05).

41
Comparison of Learning and Attitudes for Limited and Frequent Attendees
Another objective of this study was to compare changes in learning and attitudes for
limited and frequent attendees. Of those who attended five or more Beneficial Bites
presentations and answered the questions regarding learning and attitude changes (n = 40-43),
limited attendance in two years of programming was defined as one-third or fewer presentations,
and one-half or fewer presentations. To acquire adequate observations in learning and attitude
ratings, the categories were collapsed to increased and decreased or unchanged for analyses and
reporting of results. Because no precedent was found for defining limited attendance for a
similar ongoing nutrition education program, frequencies for learning and attitude changes were
compared twice for limited and frequent attendees in two years of programming, with limited
and frequent attendance defined as 8 or fewer presentations and 9 or more (Table 3) and 12 or
fewer presentations and 13 or more (Table 4). Greater differences were expected between the
groups attending half or less and more than half of the presentations as the most frequent
attendees were assumed to acquire more nutrition knowledge. Per Fisher’s Exact test, no
significant differences were observed in learning or attitude changes between limited and
frequent attendees—either with limited defined as eight or fewer presentations, or twelve or
fewer—as evaluated by Cross tabulation and Chi-square analyses.

42
Table 3
Frequency of Learning and Attitude Changes by Limited (8 Presentations or Fewer) and
Frequent Attendance
Learning and attitude measures Total number of presentations attended
8 or fewer 9 or more
Nutrition knowledge (n = 41)
No change or decreased
Increased
1 (5.9)
16 (94.1)
3 (12.5)
21 (87.5)
Confidence in healthy cooking (n = 42)
No change or decreased
Increased
4 (23.5)
13 (76.5)
5 (20.0)
20 (80.0)
Importance of healthy eating in my life (n = 42)
No change or decreased
Increased
2 (11.8)
15 (88.2)
4 (16.0)
21 (84.0)
Belief that what I eat affect my health (n = 39)
No change or decreased
Increased
2 (12.5)
14 (87.5)
4 (17.4)
19 (82.6)
Confidence in making dietary changes (n = 41)
No change or decreased
Increased
6 (35.3)
11 (64.7)
5 (20.8)
19 (79.2)
Motivation to make dietary changes (n = 41)
No change or decreased
Increased
2 (11.8)
15 (88.2)
3 (12.5)
21 (87.5)
Overall health (n = 42)
No change or decreased
Increased
6 (33.3)
12 (66.7)
10 (41.7)
14 (58.3)
Note. Numbers in parentheses are percentages of respondents (n).
Although there were no statistically significant differences between the limited and
frequent attendees, some interesting patterns arose. With limited attendance defined as eight or
fewer presentations over the course of 2 years (Table 3), 79% of frequent attendees indicated an
increase in confidence in making dietary changes compared to 65% of limited attendees. The
same trend occurred when limited attendance was defined as twelve or fewer presentations
(Table 4): 87% of frequent attendees reported an increase in confidence in making dietary
changes compared to 65% of the limited attendees. Conversely, 71% of frequent attendees

43
indicated increased overall health compared to 57% of limited attendees only when limited
attendance was defined as 12 or fewer presentations.
Table 4
Frequency of Learning and Attitude Changes by Limited (12 Presentations or Fewer) and
Frequent Attendance
Learning and attitude measures Total number of presentations attended
12 or fewer 13 or more
Nutrition knowledge (n = 41)
No change or decreased
Increased
3 (11.1)
24 (88.9)
1 (7.1)
13 (92.9)
Confidence in healthy cooking (n = 42)
No change or decreased
Increased
6 (22.2)
21 (77.8)
3 (20.0)
12 (80.0)
Importance of healthy eating in my life (n = 42)
No change or decreased
Increased
4 (14.8)
23 (85.2)
2 (13.3)
13 (86.7)
Belief that what I eat affects my health (n = 39)
No change or decreased
Increased
4 (16.0)
21 (84.0)
2 (14.3)
12 (85.7)
Confidence in making dietary changes (n = 41)
No change or decreased
Increased
9 (34.6)
17 (65.4)
2 (13.3)
13 (86.7)
Motivation to make dietary changes (n = 41)
No change or decreased
Increased
3 (11.1)
24 (88.9)
2 (14.3)
12 (85.7)
Overall health (n = 42)
No change or decreased
Increased
12 (42.9)
16 (57.1)
4 (28.6)
10 (71.4)
Note. Numbers in parentheses are percentages of respondents (n).
Changes in Learning and Attitudes across Gender, Marital Status, Educational
Attainment, and Income Level
An additional aim of this study was to examine the differences in learning and attitude
changes regarding food and healthy eating based on gender, marital status, educational
attainment, and income level. Because of a limited sample distribution across five categories for
marital status, seven for educational attainment, and eight for income level, the categories for

44
each variable were collapsed as follows: married or living with partner, and widowed, divorced,
separated, or single; high school or less and vocational training or more; and $29,999 or less and
$30,000 or more.
Table 5 presents the frequency of learning and attitude changes by gender. Cross
tabulation and Chi-square analyses showed significant differences between males and females in
three learning and attitudes parameters: confidence in healthy cooking [p = 0.016, Fisher’s Exact
test (FET)], confidence in making dietary changes (p = 0.028, FET), and motivation to make
dietary changes (p = .019, FET). More specifically, 85% of females reported increased
confidence in healthy cooking compared to 33% of males. Similarly, 79% of females reported
increased confidence in making dietary changes compared to 33% of males. Motivation to make
dietary changes showed similar results, with 91% of females reporting increases compared to
50% of males.

45
Table 5
Frequency of Learning and Attitude Changes by Gender
Learning and attitude measures Male (n = 6) Female (n = 34)
Nutrition knowledge
Decreased or no change
Increased
2 (33.3)
4 (66.7)
2 (5.9)
32 (94.1)
Confidence in healthy cooking
Decreased or no change
Increased
4 (66.7)
2 (33.3)
5 (14.7)
29 (85.3)
Importance of healthy eating in my life
Decreased or no change
Increased
2 (33.3)
4 (66.7)
4 (11.8)
30 (88.2)
Belief that what I eat affects my health
Decreased or no change
Increased
2 (33.3)
4 (66.7)
4 (11.8)
27 (79.4)
Confidence in making dietary changes
Decreased or no change
Increased
4 (66.7)
2 (33.3)
6 (17.6)
27 (79.4)
Motivation to make dietary changes
Decreased or no change
Increased
3 (50.0)
3 (50.0)
2 (5.9)
31 (91.2)
Overall health Decreased or no change
Increased
3 (50.0)
2 (33.3)
12 (35.3)
22 (64.7)
Note. Numbers in parentheses are percentages.
No significant differences were observed between changes in learning and attitudes and
any of the other sociodemographic variables as evaluated by Cross tabulation and Chi-square
analyses. The frequency of learning and attitude changes by marital status, educational
attainment, and income level are each presented in Tables 6, 7, and 8, respectively.
Albeit nonsignificant, some notable differences arose between the coupled and single
groups in learning and attitude changes (Table 6). Although more of those who were married or
living with a partner indicated increases in the belief that foods consumed affect health and
overall health compared to cohorts, more of those who were widowed/widowers, divorced,
separated, or single indicated increases in confidence about making dietary changes.

46
Table 6
Frequency of Learning and Attitude Changes by Marital Status
Learning and attitude measures Married or living
with partner
Widowed, divorced,
separated, or single
Nutrition knowledge (n = 37)
Decreased or no change
Increased
1 (5.9)
16 (94.1)
2 (10.0)
18 (90.0)
Confidence in healthy cooking (n = 38)
Decreased or no change
Increased
4 (23.5)
13 (76.5)
5 (23.8)
16 (76.2)
Importance of healthy eating in my life (n = 38)
Decreased or no change
Increased
2 (11.8)
15 (88.2)
4 (19.0)
17 (81.0)
Belief that what I eat affects my health (n = 35)
Decreased or no change
Increased
1 (6.3)
15 (93.8)
4 (21.1)
15 (78.9)
Confidence in making dietary changes (n = 37)
Decreased or no change
Increased
5 (29.4)
12 (70.6)
3 (15.0)
17 (85.0)
Motivation to make dietary changes (n = 37)
Decreased or no change
Increased
2 (11.8)
15 (88.2)
2 (10.0)
18 (90.0)
Overall health (n = 36)
Decreased or no change
Increased
5 (31.3)
11 (68.8)
9 (45.0)
11 (55.0)
Note. Numbers in parentheses are percentages of respondents (n).
Despite the lack of statistical significance, educational attainment seemed to have an
effect on some learning and attitude measures, (Table 7). Namely, slightly greater proportions of
participants with a high school education or less reported increases in nutrition knowledge (96%
versus 86%), the belief that foods consumed influence health (91% versus 79%), and overall
health (71% versus 42%) compared to their more educated cohorts.

47
Table 7
Frequency of Learning and Attitude Changes by Educational Attainment
Learning and attitude measures High school or less Vocational training
or more
Nutrition knowledge (n = 37)
Decreased or no change
Increased
1 (4.3)
22 (95.7)
2 (14.3)
12 (85.7)
Confidence in healthy cooking (n = 38)
Decreased or no change
Increased
6 (25.0)
18 (75.0)
3 (21.4)
11 (78.6)
Importance of healthy eating in my life (n = 38)
Decreased or no change
Increased
4 (16.7)
20 (83.3)
2 (14.3)
12 (85.7)
Belief that what I eat affects my health (n = 35)
Decreased or no change
Increased
2 (9.5)
19 (90.5)
3 (21.4)
11 (78.6)
Confidence in making dietary changes (n = 37)
Decreased or no change
Increased
6 (26.1)
17 (73.9)
2 (14.3)
12 (85.7)
Motivation to make dietary changes (n = 37)
Decreased or no change
Increased
3 (13.0)
20 (87.0)
1 (7.1)
13 (92.9)
Overall health (n = 36)
Decreased or no change
Increased
7 (29.2)
17 (70.8)
7 (58.3)
5 (41.7)
Note. Numbers in parentheses are percentages of respondents (n).
Consistent with the other sociodemographic variables, although none of the learning or
attitude differences between income categories was statistically significant, some interesting
patterns emerged (Table 8). Greater proportions of participants with less income reported a
decrease or no change in all learning and attitude variables. Notably, 80% of those with more
income indicated an increase in overall health since participating in Beneficial Bites, compared
to 59% of those in the lesser income category.
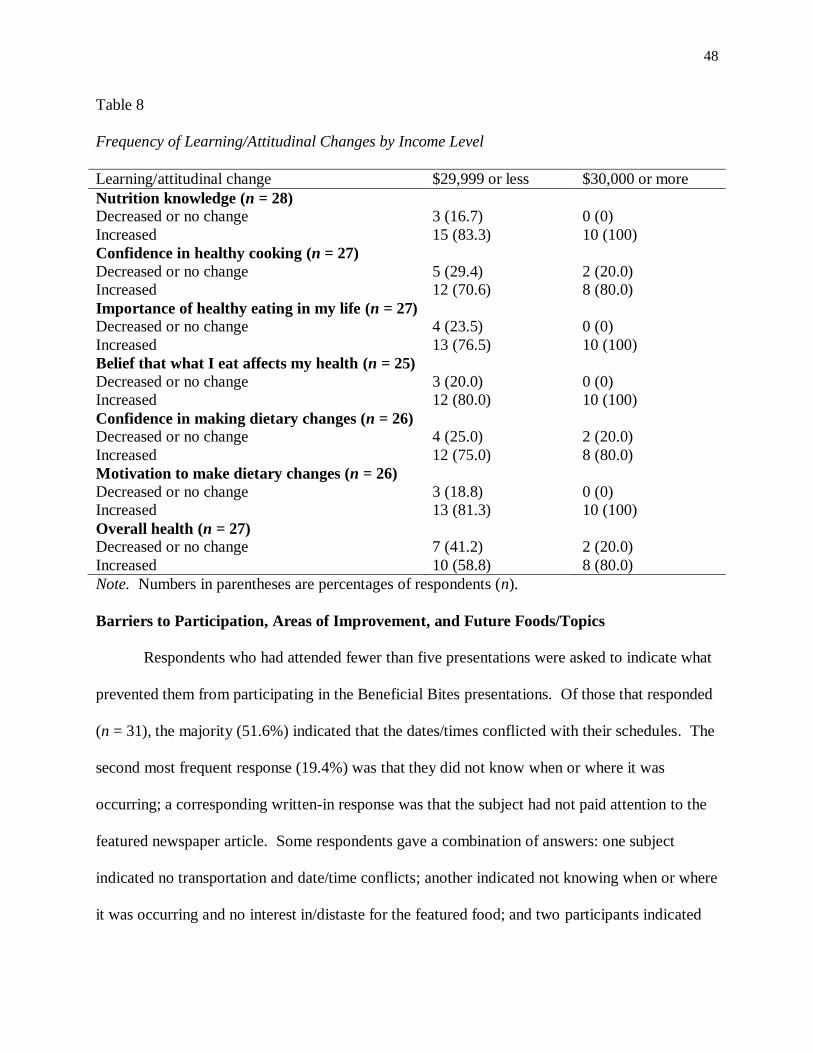
48
Table 8
Frequency of Learning/Attitudinal Changes by Income Level
Learning/attitudinal change $29,999 or less $30,000 or more
Nutrition knowledge (n = 28)
Decreased or no change
Increased
3 (16.7)
15 (83.3)
0 (0)
10 (100)
Confidence in healthy cooking (n = 27)
Decreased or no change
Increased
5 (29.4)
12 (70.6)
2 (20.0)
8 (80.0)
Importance of healthy eating in my life (n = 27)
Decreased or no change
Increased
4 (23.5)
13 (76.5)
0 (0)
10 (100)
Belief that what I eat affects my health (n = 25)
Decreased or no change
Increased
3 (20.0)
12 (80.0)
0 (0)
10 (100)
Confidence in making dietary changes (n = 26)
Decreased or no change
Increased
4 (25.0)
12 (75.0)
2 (20.0)
8 (80.0)
Motivation to make dietary changes (n = 26)
Decreased or no change
Increased
3 (18.8)
13 (81.3)
0 (0)
10 (100)
Overall health (n = 27)
Decreased or no change
Increased
7 (41.2)
10 (58.8)
2 (20.0)
8 (80.0)
Note. Numbers in parentheses are percentages of respondents (n).
Barriers to Participation, Areas of Improvement, and Future Foods/Topics
Respondents who had attended fewer than five presentations were asked to indicate what
prevented them from participating in the Beneficial Bites presentations. Of those that responded
(n = 31), the majority (51.6%) indicated that the dates/times conflicted with their schedules. The
second most frequent response (19.4%) was that they did not know when or where it was
occurring; a corresponding written-in response was that the subject had not paid attention to the
featured newspaper article. Some respondents gave a combination of answers: one subject
indicated no transportation and date/time conflicts; another indicated not knowing when or where
it was occurring and no interest in/distaste for the featured food; and two participants indicated

49
date/time conflicts and no interest in/distaste for the featured food. The most frequent written-in
response was “I forgot” (n = 4, 12.9%), followed by “I wasn’t living here at the time” (n = 2,
6.5%).
Regarding participant suggestions for improvement to the program, four major themes
emerged from the 22 written-in responses. The majority of responses (36.4%, or n = 8) were not
suggestions but positive comments about the presentations, recipes, and/or presenters. Six
participants (27.3%) identified the need for more advertising, such as in the local newspapers
rather than just the Barron County Senior Review. Three participants commented on distracting
background noise from the kitchen and dining room staff, two of which suggested that the
presenter use a microphone. Three participants made suggestions regarding presentation times:
one proposed changing the time from morning or afternoon to evening and two suggested
scheduling them close to other senior/community center activities.
Suggestions for future topics or foods were varied. The greatest number of requests (n =
11) were for specific vegetables, five of which were specifically for potatoes. The second
greatest request (n = 8) was for fruits, followed by spices/herbs (n = 4) and tips for eating out (n
= 4). Specialty diets, desserts, hotdishes, proteins, and breakfast items were each requested three
times, followed by dairy products, which were requested twice. Five participants wrote in
“anything” or “everything”.

50
Chapter V: Discussion
This study was conducted to appraise the effectiveness of Beneficial Bites—a
comprehensive nutrition education program for older and aging adults—for the purpose of
further program development. This chapter will discuss limitations throughout the research
process—particularly as related to the findings and conclusions of the study, summarize notable
findings and conclusions of the present study in correlation to previous findings in nutrition
education evaluations, and propose recommendations for future nutrition education evaluation
research as well as for the Beneficial Bites program in particular.
Limitations
The limitations of this study have been previously discussed in detail in Chapter III.
Several methodological limitations have particular relevance to the interpretations and
conclusions drawn from this study. The first limitation of this study was the lack of a pre/post
design. In addition to the process evaluation data presented, baseline nutrition knowledge, food
frequency, and health status data for each participant would have provided more objective
measures of the effectiveness of the program and would have allowed identification of absolute
changes. Food frequency data in particular would have provided a more objective measure of
dietary changes.
An additional limitation was in the sampling procedure. The population for this study
was limited to participants of the Barron County Beneficial Bites presentations in February 2012.
As such, it is possible that some regular participants were unable to attend this particular month’s
presentation. Data collection should have continued over the subsequent months to obtain a
more inclusive sample of Beneficial Bites participants.
51
The self-reported data collected by the survey was a limitation in several ways. Because
the survey required respondents to accurately recall which Beneficial Bites presentations they
had attended, inaccurate responses may have limited the data on survey items that depended on a
certain number of attended presentations, namely, the question regarding barriers to participation
and those aimed at measuring changes in learning and attitudes regarding food and healthy
eating. A desire to look good, or give the “right” answer also may have influenced positive
responses to learning and attitude measures. Despite assurances that responses would be kept
anonymous, participants may have responded positively in an effort to please the researcher,
survey administrator, or program coordinator.
Correspondingly, consistent with an inherent problem with survey methodologies, failure
to report answers to all questions for unknown reasons limited the data on some survey items.
The multiple categories for several of the sociodemographic questions, numbering up to eight for
income level, may have overwhelmed the respondents, making choosing more difficult. Thus,
rather than describing the sample in more detail as intended, too many choices may have led
respondents to skip the question. Using a consistent number of options for each
sociodemographic variable would not only have streamlined the survey, facilitating readability,
but it may have also increased the data collected from each question, which in turn may have
contributed to variability in responses.
An additional limitation was identified in the researcher’s instrument (Appendix B).
Prior to Question 2, the survey instructed participants to skip to Question 5 if they had attended
fewer than five Beneficial Bites presentations; those who had attended more than 5 presentations
were instructed to proceed through the subsequent questions. The latter statement should have
read, “If you have attended 5 or more presentations,” to specifically include those who had
52
attended five presentations in the instructions to answer the subsequent questions regarding use
of the featured recipes and foods and changes in learning and attitudes. Of the three participants
who attended five presentations, only one followed the errant survey instructions and skipped
Questions 2 through 4; data collected from the other two participants were included in the
analysis of resulting behaviors and learning and attitude changes of those who had attended more
than five presentations.
Final blanket limitations were the lack of a pilot study and use of the specific population.
First, direction of a pilot study may have allowed for improvements to the research design and
corrections to the aforementioned limitations, which may have strengthened the statistical
significance of results. Second, the convenience sampling methodology, small sample size, and
primarily White female sample limit the ability to generalize findings to other nutrition education
initiatives.
Conclusions
Despite the limited statistical significance of many of the study findings, interesting
patterns emerged warranting further discussion. Patterns in learning and attitudes regarding food
and healthy eating related to frequency of Beneficial Bites attendance are discussed, followed by
further discussion of patterns observed in learning and attitudes changes for limited versus
frequent attendees. Changes in learning and attitudes across gender, marital status, educational
attainment, and income level will follow. Finally, conclusions regarding prominent barriers to
regular participation and corresponding areas of improvement will be discussed.
No relationship was established between changes in learning or attitudes and frequency
of program participation. It should be noted, however, that most participants (nearly two thirds
or more) reported increases in learning about and positive attitudes toward food and healthy
53
eating, regardless of the amount of presentations attended. Similarly, reported knowledge gains
are common in the literature, despite varied attendance rates for other nutrition education
presentations, lessons, or food workshops (Ellis et al., 2005; Keller et al., 2005). Ellis et al.
(2005) found similar increases in positive attitudes and behavior changes after a five-lesson
pre/post intervention. As a result of 51% of participants attending three or more lessons, at least
75% reported trying to follow a healthier diet, eating more whole grain foods with the belief that
they were good for them, and/or feeling more strongly than before that eating whole grain foods
would reduce the risk of chronic disease.
In the present study, no significant differences were observed in learning or attitude
changes between limited and frequent attendees. As mentioned previously, this was likely due to
the limited variation observed in responses, namely, most participants reported increases in
learning and attitudes. However, an interesting pattern occurred when limited attendance was
defined as 12 presentations or fewer compared to 8 or fewer. A greater proportion of frequent
attendees participating in 13 or more presentations tended to report increased confidence in
making dietary changes—a trend that did not change when frequent attendance was decreased to
9 or more presentations. This may suggest that greater confidence in making dietary changes is
possible with even moderate participation in nutrition education programs. Similarly, Keller et
al. (2005) found increases in confidence in making dietary changes, as well as motivation to
make dietary changes and confidence in healthy cooking when participants attended only one of
a three-session series food workshop (44.3% compared to 31.4% attending all three sessions and
24.3% attending two sessions). Notably, nutrition knowledge, interest in trying new foods,
importance of healthy eating, and increased belief that diet influences health also increased.

54
In a review evaluating nutrition education intervention results, Sahyoun et al. (2004)
found that knowledge gains were the most frequently reported outcome. Correspondingly,
Taylor-Davis et al. (2000) demonstrated the use of theory-based nutrition education newsletters
and follow-up telephone interviews in increasing nutrition knowledge, willingness to answer
nutrition knowledge test items, confidence in nutrition knowledge, and interest in nutrition.
Treatment groups also performed better than the control on readiness to change dietary fiber
intake and stages of change to avoid dietary fats. Lesson plans incorporating self-assessment of
current eating habits, goal-setting activities, food tasting, take home handouts, and question-and-
answer with a nutrition educator have also shown success in increasing nutrition knowledge and
positive dietary changes (Patacca et al., 2004).
Increases in overall health may require more regular participation in nutrition education.
A greater proportion of frequent attendees participating in 13 or more Beneficial Bites
presentations reported increased overall health; however, the same trend did not uphold for 9 or
more presentations. This is consistent with the more varied evidence for behavior change and
positive nutrition-related biochemical and anthropometric outcomes as a result of nutrition
education (Bandayrel & Wong, 2011; Sahyoun et al., 2004).
Findings of the present research established significant differences in learning and
attitude changes according to gender. Specifically, more females than males reported increased
confidence in healthy cooking, confidence in making dietary changes, and motivation to make
dietary changes. This may be explained by differences in the austerity of gender roles that older
cohorts are accustomed to, particularly those involving meal preparation and grocery shopping
responsibilities. From this perspective, women, especially older adult women, may have more
experience with selecting and preparing food. Moreover, consistently more females than males
55
in the present study were also found to report increases in their nutrition knowledge, personal
value for healthy eating, belief that foods consumed affect health, and overall health compared to
cohorts. These collective findings appear to agree with the observation by Krondl et al. (2008)
that recent widowers exhibit greater nutritional risk with subsequent impact on their health
compared to women living alone.
In discussion of this finding of gender differences in learning and attitudes, it should also
be noted that a majority of the sample was female (83%). A majority also reported being the
primary meal preparer (86%) and primary grocery shopper (88%). Approximately one-third of
Beneficial Bites presentation content is devoted to the selection, storage, handling, cooking, and
serving of the featured food. Additionally, an assortment of take-home recipes featuring the
food/ingredient of the month is always provided at each presentation. Thus, participants who
remain actively engaged in meal preparation and food selection and procurement at home may
constitute a more captive audience; as a result, they may ultimately become better equipped (i.e.
more confident and motivated) to actively make and maintain behavioral changes such as diet
modifications and cooking healthier meals.
Although no significant differences were observed in learning or attitude changes as
related to marital status, some interesting patterns surfaced. More of those who were married or
living with a partner tended to report increases in the belief that foods consumed affect health as
well as increases in overall health compared to cohorts. In contrast, more of those who were
widowed/widowers, divorced, separated, or single reported increases in confidence regarding
dietary changes. While the former trend seems to coincide with previous research, the latter does
not. Varying forms of social isolation have been consistently linked to negative changes in
eating habits among the elderly: bereavement of spouse, depression due to an array of factors,
56
lack of transportation, rural residences, and disability or loss of functionality may all limit an
older adult’s interaction with others (Kamp et al., 2010; Krondl et al., 2008; Kuczmarski &
Weddle, 2005). Furthermore, elderly adults living alone experience greater rates of food
insecurity (Kuczmarski & Weddle, 2005).
No significant differences were established between educational attainment and learning
and attitude changes. An unexpected pattern occurred in that greater proportions of those who
completed high school or less tended to indicate increased overall health, nutrition knowledge,
and belief that foods consumed influence health compared to those who had vocational training
or more. This may be due to the limited variation observed in educational attainment—namely,
that most had only a high school education or less. Contrary to this pattern, Krondl et al. (2008)
have proposed that the younger generation of the future elderly population is likely to be more
health conscious and better educated, and as such may be more receptive to knowledge-based
interventions and nutrition education. As mentioned in Chapter I, Beneficial Bites targets not
only older adults, but also “younger” seniors, or the future older adult population in an effort to
promote healthful aging and postpone the need for nutrition services later on in life. This is not
only in recognition of the need for primary and secondary prevention of chronic disease among
this subgroup, but also in recognition of an aging population that continues to outpace funding
for its respective nutrition programs.
Other interesting patterns occurred in the frequency of learning and attitude changes by
income category. Namely, more participants with less income tended to report a decrease or no
change in each learning and attitude measure, as well as in overall health. This corroborates the
previous findings by Ellis et al. (2005) suggesting that barriers to increasing healthful behaviors
regarding whole grain foods consumption are more likely to include financial constraints than

57
knowledge about the respective health benefits. Krondl et al. (2008) also recognize that older
adults on fixed incomes may be forced to limit allocations for nutritious food. Because a
majority of the sample in the present study was retired, fixed incomes may explain the lack of
changes in attitudes toward food and healthy eating. Although data on income comfort level
were insufficient for statistical analysis, most participants indicated having either “no more than
just enough” or “enough with a little extra sometimes”.
A major theme identified in participant suggestions for improvement to Beneficial Bites
was the need for more advertising; this was consistent with the second most prominent barrier to
participation—not knowing when or where the presentations were occurring. Further, 13 of the
63 participants were possible first-time attendees, as concluded from no recalled presentations
attended, which may suggest that as much as 21% of participants only recently became aware of
the program. Judging from this perspective, a majority of the potential target audience may be
unaware of the program. This was consistent with findings from Manilla et al. (2010) in which
14.8% of participants in an educational food tasting activity had learned of the activity from the
monthly newsletter compared to 42% who had no prior knowledge of the activity, suggesting
that advertising strategies relying chiefly on monthly newsletters are insufficient for attracting
larger scales of older adult audiences.
The purpose of this study was to evaluate the effectiveness of Beneficial Bites—a
comprehensive nutrition education program featuring well-supported strategies for teaching
older adults. Several findings support the conclusion that Beneficial Bites is effective at
promoting nutrition knowledge gains and positive attitudes toward food and healthy eating
among the target audience. Significantly more females than males reported increased confidence
in healthy cooking, confidence in making dietary changes, and motivation to make dietary
58
changes. Most participants (nearly two thirds or more) reported increases in knowledge and
positive attitudes regarding food and healthy eating regardless of the amount of presentations
attended. Of those who did attend five or more Beneficial Bites presentations, approximately
three-fourths or more reported increases in nutrition knowledge, confidence in healthy cooking
and making dietary changes, motivation to make dietary changes, the personal value of healthy
eating, and the belief that foods consumed affect health. Additionally, positive comments about
the presentations, presenters, and program content and design outnumbered any other suggestion
for improvement.
Despite the lack of an established, statistically significant relationship between the
frequency of Beneficial Bites attendance and changes in learning and attitudes regarding food
and healthy eating, similar findings of varied nutrition education attendance rates producing
overall knowledge gains have also been reported. Further comparisons of limited and frequent
attendees revealed a trend such that greater proportions of frequent attendees tended to report
increased confidence in making dietary changes.
The lack of significant findings may be explained by the lack of a pre/post design and
small sample size. Also, participants with lower incomes tended to report a decrease or no
change in each learning and attitude measure, as well as in overall health, suggesting that a
barrier to increasing healthful behaviors in this sample may relate to financial constraints. This
may be explained by the greater proportion of retirees within the sample, who may be limited by
a fixed income.
Recommendations
Nutrition education is especially important to older adults who are, for a multitude of
reasons, uniquely susceptible to nutritional risk. Because so many factors may contribute to this

59
risk, ongoing nutrition education programs for older adults require regular assessment or
evaluations to ensure that the needs of the target population are being met and to further program
development. Thus, regular formative evaluations or assessments of Beneficial Bites
programming are recommended to continue to identify potential areas for improvement.
Furthermore, nutritional risk and eating habits could be assessed using a validated tool to identify
priorities for programming.
This study was unable to establish a significant relationship between changes in learning
and attitudes and frequency of attendance. A recommended approach for future nutrition
education evaluation research is a pre/post research design in which baseline and follow-up
nutrition knowledge, food frequency, health status, and nutritional risk for each participant are
measured. This would provide more objective measures of knowledge and behavioral changes
as a result of program participation.
A prominent barrier to regular participation, corresponding with a common suggestion
for improvement, was the need for more advertising of presentation dates, times, and locations.
Although Beneficial Bites is advertised monthly in the free Barron County Senior Review, which
has a circulation of 4,500, only about 100 are actually mailed out. Subscriptions are available to
those who are unable to pick one up where they are normally distributed throughout the county
(grocery stores, banks, senior apartment buildings, senior centers, etc.), or to those who do not
automatically receive one as a recipient of Meals on Wheels, however, many are to those who no
longer live in the area. A recommended advertising resource recognized by current attendees is
local newspapers in the respective towns where Beneficial Bites presentations take place. Other
advertising for Beneficial Bites occurs in the form of flyers and postings at local
community/senior centers; however, the reach of this strategy is limited to those who visit the

60
centers. Posting flyers in public spaces in each locality may increase access to the broader
potential audience for which the program is intended. Further investigation of specific barriers
to participation in this and other ongoing nutrition education programs is needed to determine
strategies for reaching more of the potential audience.
With respect to future research, it is recommended that the survey used for data collection
in the present study be revised in several ways. Given the varied response rate, the number of
choices for sociodemographic questions should be consistent and limited to four to facilitate
readability and reduce respondent burden. This population may also require more detailed
instructions during survey administration to address any points of confusion. A further
recommendation would be to evaluate the potential sociodemographic factors of nutritional
risk—such as income and living situation—separately, using a reliable, validated tool.

61
References
Bandayrel, K., & Wong, S. (2011). Systematic literature review of randomized control trials
assessing the effectiveness of nutrition interventions in community-dwelling older adults.
Journal of Nutrition Education and Behavior, 43(4), 251-262.
Center for Nutrition Policy and Promotion. (2005). MyPyramid—Getting started. Retrieved from
http://www.choosemyplate.gov/food-groups/downloads/MyPyramid_Getting_Started.pdf
Ellis, J., Johnson, M. A., Fischer, J. G., & Hargrove, J. L. (2005). Nutrition and health education
intervention for whole grain foods in the Georgia Older Americans Nutrition Program.
Journal of Nutrition for the Elderly, 24(3), 67-83. doi: 10.1300/J052v24n03_06
Federal Interagency Forum on Aging-Related Statistics. (2008). Population. Retrieved from
http://www.agingstats.gov/agingstatsdotnet/Main_Site/Data/2010_Documents/Population
.aspx
Heuberger, R., & Caudell, K. (2011). Polypharmacy and nutritional status in older adults: a
cross-sectional study. Drugs & Aging, 28(4), 315-323. doi:10.2165/11587670-
000000000-00000
Higgins, M. M., & Barkley, M. C. (2003). Evaluating outcomes and impact of nutrition
education programs designed for older adults. Journal of Nutrition for the Elderly, 22(4),
69-81.
Higgins, M. M. & Barkley, M. C. (2004). Improving effectiveness of nutrition education
resources for older adults. Journal of Nutrition for the Elderly, 23(3), 69-81.
Kamp, B. J., Wellman, N. S., & Russell, C. (2010). Position of the American Dietetic
Association, American Society for Nutrition, and Society for Nutrition Education: Food

62
and nutrition programs for community-residing older adults. Journal of the American
Dietetic Association, 110, 463-472. doi: 10.1016/j.jada.2009.12.009
Keller, H. H., Hedley, M., Hadley, T., Wong, S., & Vanderkooy, P. (2005). Food workshops,
nutrition education, and older adults: A process evaluation. Journal of Nutrition for the
Elderly, 24(3), 5-23. doi: 10.1300/J052v24n03_03
Keller, H. H., Hedley, M. R., Wong, S. S-L., Vanderkooy, P., Tindale, J., & Norris, J. (2006).
Community organized food and nutrition education: Participation, attitudes, and
nutritional risk in seniors. The Journal of Nutrition, Health, & Aging, 10(1): 15-20.
Krahn, V. M., Lengyel, C. O., & Hawranik, P. (2011). Healthy eating perceptions of older adults
living in Canadian rural and northern communities. Journal of Nutrition in Gerontology
and Geriatrics, 30, 261-273. doi: 10.1080/21551197.2011.591270
Krondl, M., Coleman, P., & Lau, D. (2008). Helping older adults meet nutritional challenges.
Journal of Nutrition for the Elderly, 27(3/4), 205-219.
Kuczmarski, M. F. & Weddle, D. O. (2005). Position Paper of the American Dietetic
Association: Nutrition across the spectrum of aging. Journal of the American Dietetic
Association, 105, 616-633. doi: 10.1016/j.jada.2005.02.026
Manilla, B., Keller, H. H., & Hedley, M. R. (2010). Food tasting as nutrition education for older
adults. Canadian Journal of Dietetic Practice and Research, 71(2), 99-102. doi:
10.3148/71.1.2010.99
McClelland, J. W., Bearon, L. B., Fraser, A. M., Mustian, D. R., & Velazquez. (2001). Reaching
older adults with nutrition education: Lessons learned during the partners in wellness
pilot project. Journal of Nutrition for the Elderly, 21(2), 59-72.

63
McClelland, J. W., Irving, L. M., Mitchell, R. E., Bearon, L. B., & Webber, K. H. (2002).
Extending the reach of nutrition education for older adults: Feasibility of a train-the-
trainer approach in congregate nutrition sites. Journal of Nutrition Education and
Behavior, 34, S48-S52.
Patacca, D., Rosenbloom, C. A., Kicklighter, J. R., & Ball, M. (2004). Using a focus group
approach to determine older adults’ opinions and attitudes toward a nutrition education
program. Journal of Nutrition for the Elderly, 23(3), 55-72. doi: 10.1300/J052v23n03_04
Rowe, J. W., & Kahn, R. L. (1987). Human aging: Usual and successful. Science (New York,
N.Y.), 237(4811), 143-149.
Sahyoun, N. R., Pratt, C. A., & Anderson, A. (2004). Evaluation of nutrition education
interventions for older adults: A proposed framework. Journal of the American Dietetic
Association, 104(1), 58-69. doi: 10.1016/j.jada.2003.10.013
Savoca, M. R., Arcury, T. A., Leng, X., Chen, H., Bell, R. A., Anderson, A. M., … & Quandt, S.
A. (2010). Food avoidance and food medication practices due to oral health problems
linked to the dietary quality of older adults. Journal of the American Geriatric Society,
58(7), 1225-1232. doi: 10.1111/j/1532-5415.2010.02909.x
Taylor-Davis, S., Smiciklas-Wright, H., Warland, R., Achterberg, C., Jensen, G. L., Sayer, A., &
Shannon, B. (2000). Responses of older adults to theory-based nutrition newsletters.
Journal of the American Dietetic Association, 100(6), 656-664.
United States Census Bureau. (2012, January 17). State & county QuickFacts. Retrieved from
http://quickfacts.census.gov/qfd/states/55000.html

64
Williams, K. & Kemper, S. (2010). Exploring interventions to reduce cognitive decline in aging.
Journal of Psychosocial Nursing and Mental Health Services, 48(5), 42-51. doi:
10.3928/02793695-20100331-03
Wouters-Wesseling, W., Wagenaar, L. W., Rozendaal, M., Deijen, J. B., de Groot, L. C.,
Bindels, J. G., & van Staveren, W. A. (2005). Effect of an enriched drink of cognitive
function in frail elderly persons. The Journals of Gerontology. Series A: Biological
Sciences and Medical Sciences, 60(2), 265-270.
Zieve, D. & Eltz, D. R. (2011, June 14). Malnutrition. Retrieved from
http://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0001441/
65
Appendix A: Institutional Review Board Approval Letter
January 25, 2012
Amy Erickson
Food and Nutrition Department
UW-Stout
Title: “An evaluation of Beneficial Bites: A nutrition education program for older adults”
Subject: Protection of Human Subjects
Dear Amy,
In accordance with Federal Regulations, your project, “An evaluation of Beneficial Bites: A
nutrition education program for older adults” was reviewed on January 25, 2012, by a member
of the Institutional Review Board and was approved under Expedited Review through January
24, 2013.
If your project involves administration of a survey or interview, please copy and paste the
following message to the top of your survey/interview form before dissemination:
If you are conducting an online survey/interview, please copy and paste the following message to
the top of the form:
“This research has been approved by the UW-Stout IRB as required by the Code of
Federal regulations Title 45 Part 46.”
Responsibilities for Principal Investigators of IRB-approved research:
1. No subjects may be involved in any study procedure prior to the IRB approval date or
after the expiration date. (Principal Investigators and Sponsors are responsible for
initiating Continuing Review proceedings.)
2. All unanticipated or serious adverse events must be reported to the IRB.

66
3. All protocol modifications must be IRB approved prior to implementation, unless they
are intended to reduce risk.
4. All protocol deviations must be reported to the IRB.
5. All recruitment materials and methods must be approved by the IRB prior to being used.
6. Federal regulations require IRB review of ongoing projects on an annual basis.
Thank you for your cooperation with the IRB and best wishes with your project.
Should you have any questions regarding this letter or need further assistance, please contact the
IRB office at 715-232-1126 or email [email protected].
Sincerely,
Susan Foxwell
Research Administrator and Human Protections Administrator,
UW-Stout Institutional Review Board for the Protection of Human Subjects in Research (IRB)
*NOTE: This is the only notice you will receive – no paper copy will be sent.

67
Appendix B: Evaluation tool
Beneficial Bites Evaluation
Thank you for taking a moment to fill out this evaluation.
1. Please check which Beneficial Bites presentations you have attended:
___ Rosemary ___ Dark Chocolate ___ Dry Beans
___ Kiwifruit ___ Flaxseed ___ Garlic
___ Yogurt ___ Tomatoes ___ Basil
___ Squash ___ Cranberries ___ Cinnamon
___ Cabbage Family ___ Walnuts & Almonds ___ Reading the
Food Label
___ Whole Grains ___ Asparagus ___ Apricots
___ Green Peas ___ Corn ___ Bell Peppers
___ Apples ___ Sweet Potatoes ___ Healthy
Holiday Foods
Age _____
Gender ____
Are you the primary meal preparer for your household? ______
If so, how many people do you cook for? ______
Are you the primary grocery shopper for your household? ______

68
If you have attended fewer than 5 presentations, what has prevented you from
participating? (Circle the most common reason)
a. Illness
b. Lack of transportation
c. I didn’t know when or where it was occurring
d. Dates/times did not work for me
e. I didn’t like or wasn’t interested in the featured food
f. Other (please explain):
___________________________________________________________
___________________________________________________________
___________________________________________________________
If you have attended less than 5 Beneficial Bites presentations, please skip to
question 5.
If you have attended more than 5 Beneficial Bites presentations, please answer the
following questions:
2. How often do you use the featured recipes?
NEVER ONCE A MONTH ONCE A WEEK 3 TIMES A WEEK
3. Of the featured foods/ingredients that you were unfamiliar with, how often do you
eat or cook with them now?
NEVER ONCE A MONTH ONCE A WEEK 3 TIMES A WEEK
4. As a result of participating in Beneficial Bites, indicate if any of the following have
changed:
a. My knowledge of nutrition has:
INCREASED DECREASED NOT CHANGED
b. My confidence in healthy cooking has:
INCREASED DECREASED NOT CHANGED
c. The importance of healthy eating in my life has:

69
INCREASED DECREASED NOT CHANGED
d. The belief that what I eat affects my health has:
INCREASED DECREASED NOT CHANGED
e. My confidence in making changes to my diet has:
INCREASED DECREASED NOT CHANGED
f. My motivation to make changes to my diet has:
INCREASED DECREASED NOT CHANGED
g. My overall health, compared to other persons my age has:
INCREASED DECREASED NOT CHANGED
5. What would you suggest to improve the presentations or attendance?
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
__________________________________________________________________
6. What topics or foods would you like to be covered in the future?
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
7. Compared to other persons your age, would you say that your health is
___ excellent ___ good ___fair ___ poor
70
8. What is your employment status?
___ retired
___ not employed but looking for work
___ not employed and not looking
___ employed part-time (34 or fewer hours per week)
___ employed full-time (35 or more hours per week)
___ self-employed part-time or full-time (circle one)
9. What is the highest grade in school that you completed?
___ completed 8th grade or less
___ attended high school
___ completed high school
___ vocational training after high school
___ attended college
___ completed college
___ completed advanced or graduate degree
10. What is your current marital or partner status?
___ married, living with spouse
___ widowed
___ divorced
___ separated
___ single, never married
___ living with a partner
11. Is there anyone else besides you currently living in your household?
___ no, I live alone
___ child/children or stepchild/children
___ grandchild/children or step grandchild/children
___ other relative(s)
___ friend(s)
71
___ other person(s) (please explain) ________________________________
12. Which of the following represents your total combined household income before
deductions during the last 12 months?
___ Under $10,000
___ $10,000 - $19,999
___ $20,000 - $29,999
___ $30,000 - $39,999
___ $40,000 - $49,999
___ $50,000 - $59,999
___ $60,000 - $69,999
___ $70,000 or more
13. Which of the following best describes your ability to get al.ong on your income?
___ I can’t make ends meet
___ I have just enough, no more
___ I have enough with a little extra sometimes
___ I always have money left over

72
Appendix C: Consent form
Consent to Participate In UW-Stout Approved Research
Title: An evaluation of Beneficial Bites: A nutrition education program for older adults
Investigator: Amy Erickson
218-343-0241
Research Sponsor: Dr. Kerry D. Peterson
Food and Nutrition Department, UW-Stout
220 Heritage Hall
Description: This study is intended to evaluate the effectiveness of the Beneficial Bites nutrition education
program by gathering information on attendance and participants, as well as gaining insight on
areas of improvement. It is hoped that the results will be used to increase the usefulness of
programming, and increase participation and regular attendance.
Risks and Benefits: There are no major risks associated with participating in this study. When completing the
demography portion of this survey you may feel minor emotional discomfort or personal
feelings. There are no direct benefits for participating in this study. However, by completing
this survey you will help us to improve future Beneficial Bites presentations by identifying
barriers to attendance and areas for further development.
Time Commitment: It is expected that the survey for this study should take you no more than 10 minutes to complete.
Confidentiality: Your name will not be included on any documents and therefore you cannot be identified from
any of the information gathered for this study.
Right to Withdraw: Your participation in this study is entirely voluntary. You may choose not to participate without
any adverse consequences to you. You have the right to stop the survey at any time. However,
should you choose to participate and later wish to withdraw from the study, there is no way to
identify your anonymous document after it has been turned into the investigator. If you are
participating in an anonymous online survey, once you submit your response, your data cannot
be identified for withdrawal.
IRB Approval: This study has been reviewed and approved by The University of Wisconsin-Stout's Institutional
Review Board (IRB). The IRB has determined that this study meets the ethical obligations
required by federal law and University policies. If you have questions or concerns regarding this
study please contact the Investigator or Advisor. If you have any questions, concerns, or reports
regarding your rights as a research subject, please contact the IRB Administrator.

73
Investigator: IRB Administrator Amy Erickson Sue Foxwell, Director, Research Services
218-343-0241 152 Vocational Rehabilitation Bldg.
[email protected] UW-Stout
Menomonie, WI 54751
Advisor: 715-232-2477
Kerry D. Peterson [email protected]
715-232-1408
Statement of Consent: By completing the following survey you agree to participate in the project entitled, “An
evaluation of Beneficial Bites: A nutrition education program for older adults