audit, registry and qip: supporting the ibd standards
DESCRIPTION
Dr Ian ArnottTRANSCRIPT

Audit, Registry and QIP: supporting the IBD Standards
Ian ArnottClinical Director UK IBD AuditWednesday 18th June 2014


Setting Quality Standards





UK IBD Audit Components2006 2008 2010 2012
Organisation X X X X
Clinical X X X X
Paediatrics X X X
Primary care X
Patient experience X X
Biologics X X

Participation in 2013• 154/162 Trusts/Health
Boards participated
• 95% participation rate
• 190 hospitals
• 4359 patients with ulcerative colitis
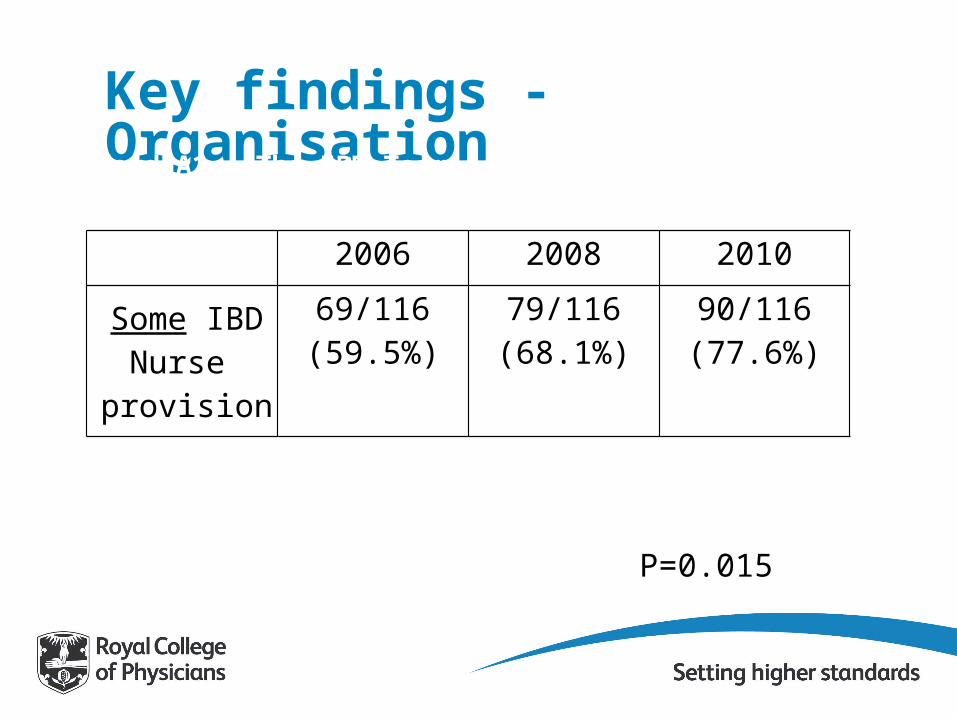
Key findings - OrganisationStandard A1 – The IBD Team
2006 2008 2010
Some IBD Nurse
provision
69/116(59.5%)
79/116(68.1%)
90/116(77.6%)
P=0.015

Key findings - Organisation
2008 2010
Written info on whom to contact when relapse?
Yes = 69% (120/174)
Yes = 80.5% (140/174)
Expect to be seen within 7 days of a relapse?
Yes = 69% (120/174)
Yes = 88.5% (154/174
Can contact an IBD Specialist by:PhoneDrop in clinicE-mail
85.7% (150/175)11.4% (20/175)40% (70/175)
94.3% (150/175)9.8% (20/175)56.3% (70/175)
Standard C2 – Rapid access to specialist advice
p<0.014
p<0.001
P=0.008P=0.615P=0.002

Results – Inpatient CareRound 2 Round 3 Round 4
Mortality 1.54% 0.92% 0.75% *
Seen by IBD nurse 27.06% 42.01% 48.35% *
Heparin 72.78% 86.21% 90.07% *
Bone protection - 66.16% 74.00% *
Surgery 12.48% 12.23% 10.76% *


Results - Re-admissions
• 27% re-admitted within 2 years• 12% re-admitted within 30 days
11% of patients were on no treatment when admitted

Out-patient care• 70% of patients with established UC were
seen in outpatients before admission• Median 35 days (IQR 9-104).
• In those with active disease, who were not admitted
• Treatment was not changed in 42%
• 16% of patients on steroids >3/12• Steroids sparing therapies tried in 22%
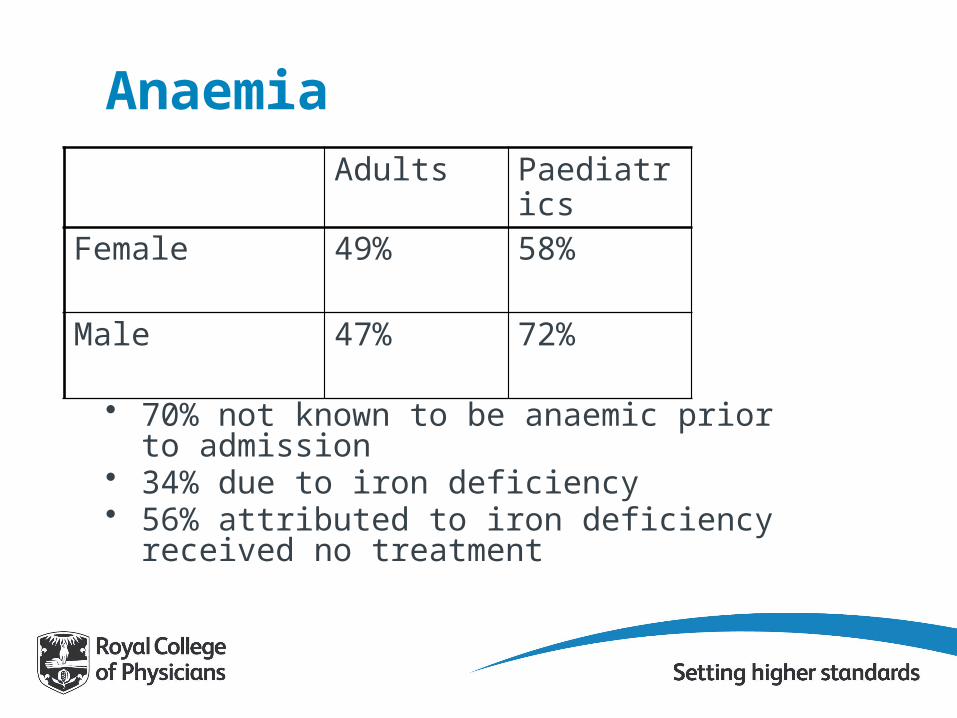
AnaemiaAdults Paediatrics
Female 49% 58%
Male 47% 72%
• 70% not known to be anaemic prior to admission• 34% due to iron deficiency• 56% attributed to iron deficiency received no
treatment
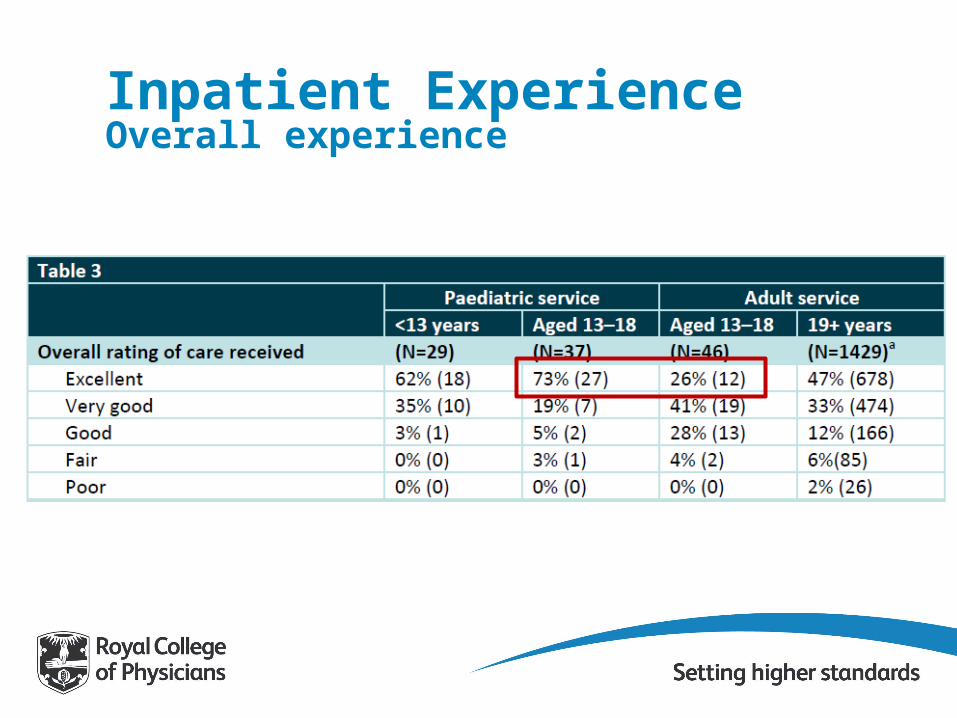
Inpatient ExperienceOverall experience
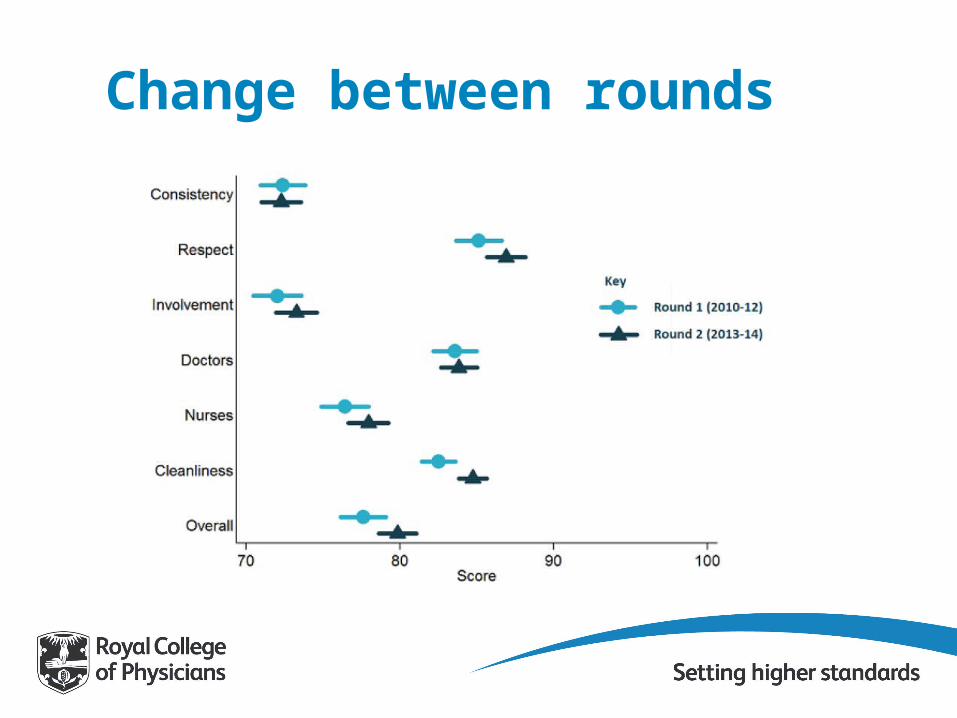
Change between rounds

Challenges
Clinical burdenAudit fatigueSupporting quality improvementSources of bias
esp. Case selection and reportingCeiling of improvementBeing responsive to clinical need

The Future• HQIP funding ensured until Feb 2015
• Focus on quality improvement• Regional meetings, patient report, action
plans• Biologics is only data collected
• Re-tendering process represents a key time point• Integration• Modernisation and simplification

Conclusion• Audit continues to drive quality
improvement• Much remains to be done• Opportunities to collaborate/come
together• HQIP funding• Key role for registry• Barriers to overcome• Benefits for all

AcknowledgementsCEEu
– Aimee Protheroe– Susan Murray– Kajal Mortier– Hannah Evans– Kevin Stewart– Rhona Buckingham– Jane Ingram
CCUK– David Barker– Elaine Steven
BSG– John Williams– Jon Rhodes– Ian Forgacs
NHSE– Mike Glynn
Contact: [email protected]
020 3075 1566/1565
www.rcplondon.ac.uk
