Âu 3 f¹Ã>Òq è'¡ - ntsb home · pilots and docking masters of louisiana, inc. the...
TRANSCRIPT

(
PB98-916401NTSB/MAR-98/01
NATIONALTRANSPORTATIONSAFETYBOARD
WASHINGTON, D.C. 20594
MARINE ACCIDENT REPORT
ALLISION OF THE LIBERIAN FREIGHTERBRIGHT FIELD WITH THE POYDRAS STREETWHARF, RIVERWALK MARKETPLACE, ANDNEW ORLEANS HILTON HOTEL INNEW ORLEANS, LOUISIANADECEMBER 14, 1996
E!!!k!dP., ‘e.
:--9-Q.‘ ‘..—. -. –— —’””
6885A
\U S GOWRNMEhl PRINT!% OFFICE IW 0+4!4s

Abstract: On December 14, 1996, the fully loaded Liberian bulk carrier Bright Fieldtemporarily lost propulsion power as the vessel was navigating outbound in the LowerMississippi River at New Orleans, Louisiana. The vessel struck a wharf adjacent to a populatedcommercial area that included a shopping mall, a condominium parking garage, and a hotel. Nofatalities resulted from the accident, and no one aboard the Bright Field was injured; however, 4serious injuries and 58 minor injuries were sustained during evacuations of shore facilities, agaming vessel, and an excursion vessel located near the impact area. Total property damages tothe Bright Field and to shoreside facilities were estimated at about $20 million.
The safety issues discussed in this report are the adequacy of the ship’s main engine andautomation systems, the adequacy of emergency preparedness and evacuation plans of vesselsmoored in the Poydras Street wharf area, and the adequacy of port risk assessment for activitieswithin the Port of New Orleans. This report also addresses three other issues: the actions of thepilot and crew during the emergency, the lack of effective communication (as it relates to theactions of the pilot and crew aboard the Bright Field on the day of the accident), and the delay inadministering toxicological tests to the vessel crew.
As a result of its investigation, the National Transportation Safety Board issuedrecommendations to the U.S. Coast Guard, the U.S. Army Corps of Engineers, the State ofLouisiana, the Board of Commissioners of the Port of New Orleans, International RiverCenter,Clearsky Shipping Company, New Orleans Paddlewheels, Inc., the New Orleans Baton RougeSteamship Pilots Association, the Crescent River Port Pilots Association, and Associated FederalPilots and Docking Masters of Louisiana, Inc.
The National Transportation Safety Board is an independent Federal agency dedicated topromoting aviation, railroad, highway, marine, pipeline, and hazardous materials safety. Establishedin 1967, the agency is mandated by Congress through the Independent Safety Board Act of 1974 toinvestigate transportation accidents, determine the probable causes of the accidents, issue safetyrecommendations, study transportation safety issues, and evaluate the safety effectiveness ofgovernment agencies involved in transportation. The Safety Board makes public its actions anddecisions through accident reports, safety studies, special investigation reports, safetyrecommendations, and statistical reviews.
Information about available publications may be obtained by contacting:
National Transportation Safety BoardPublic Inquiries Section, RE-51490 L’Enfant Plaza, S.W.Washington, D.C. 20594(202) 314-6551
Safety Board publications may be purchased, by individual copy or by subscription, from:
National Technical Information Service5285 Port Royal RoadSpringfield, Virginia 22161(703) 605-6000

#..+5+10"1("6*'".+$'4+#0"(4'+)*6'4$4+)*6"(+'.&"9+6*"6*'"21;&4#5"564''69*#4(."4+8'49#.-"/#4-'62.#%'."#0&
0'9"14.'#05"*+.610"*16'."+00'9"14.'#05.".17+5+#0#
&'%'/$'4"36."3;;8
MARINE ACCIDENT REPORT
Adopted: January 13, 1998Notation 6885A
0#6+10#.64#052146#6+10
5#('6;"$1#4&
9CUJKPIVQP."&0%0"427;6


iii
CONTENTS
EXECUTIVE SUMMARY .........................................................................................................vii
INVESTIGATIONSynopsis .......................................................................................................................................... 1Preaccident Events .......................................................................................................................... 1The Accident ................................................................................................................................... 5Injuries........................................................................................................................................... 10Vessel Damage.............................................................................................................................. 10Other Damage................................................................................................................................ 10Crew Information .......................................................................................................................... 14
The Pilot................................................................................................................................. 14The Master ............................................................................................................................. 14The Chief Engineer ................................................................................................................ 16The Previous Chief Engineer ................................................................................................. 17
Vessel Information ........................................................................................................................ 17Bright Field............................................................................................................................ 17
Automated Propulsion Control System .......................................................................... 18Engine Lubricating Oil System....................................................................................... 19
Cruise Ships ........................................................................................................................... 20Gaming and Excursion Vessels.............................................................................................. 20
Waterway Information................................................................................................................... 21River Stage............................................................................................................................. 21Vessel Traffic Control............................................................................................................ 21
Port Information ............................................................................................................................ 22Dredging................................................................................................................................. 22The Wharf Area...................................................................................................................... 23Federal Jurisdiction ................................................................................................................ 23
Meteorological Information .......................................................................................................... 25Toxicological Information............................................................................................................. 25Survival Aspects............................................................................................................................ 26
Bright Field............................................................................................................................ 26Enchanted Isle........................................................................................................................ 26Nieuw Amsterdam.................................................................................................................. 26Queen of New Orleans........................................................................................................... 27Creole Queen......................................................................................................................... 30Riverwalk Marketplace ..........................................................................................................32Hilton Riverside Hotel ........................................................................................................... 33
Emergency Response..................................................................................................................... 34Port of New Orleans Harbor Police ....................................................................................... 34Coast Guard Group New Orleans .......................................................................................... 35Louisiana Office of Emergency Preparedness ....................................................................... 35

iv
Police Departments ................................................................................................................ 35New Orleans Fire Department ............................................................................................... 35New Orleans Department of Health and Emergency Medical Services................................. 35
Emergency Preparedness............................................................................................................... 36Riverwalk Marketplace ..........................................................................................................36New Orleans Hilton Riverside Hotel ..................................................................................... 36Queen of New Orleans........................................................................................................... 36
Safety Briefings...............................................................................................................37Signage............................................................................................................................ 37Emergency Egress........................................................................................................... 37Drills ............................................................................................................................... 38
Creole Queen......................................................................................................................... 38Inspections, Tests, and Research................................................................................................... 38
Steering Gear.......................................................................................................................... 39Main Engine—General .......................................................................................................... 39Main Engine Lubricating Oil Sump....................................................................................... 39Main Engine Lubricating Oil Pumps/Motors......................................................................... 39Main Engine Lubricating Oil System Second Filter/Strainer ................................................ 40Main Engine Lubricating Oil Purifier .................................................................................... 40Automatic Main Engine Lubricating Oil Trip Function ........................................................ 41Alarms, Indicators, and Recorders ......................................................................................... 41Remote Engine Control Tests ................................................................................................ 41Preventive Maintenance.........................................................................................................41Reports and Recordkeeping ................................................................................................... 41Main Engine Lubricating Oil Testing and Analysis............................................................... 42Spare Parts and Calibration Tools.......................................................................................... 42Sulzer Inspection.................................................................................................................... 42Chief Engineer’s Assessment................................................................................................. 43Tests, Reports, and System Calibration ................................................................................. 43Computer Simulation ............................................................................................................. 44
Other Information.......................................................................................................................... 44Port Risk Analysis and Management—Coast Guard ............................................................. 44Port Risk Analysis and Management—Other Stakeholders .................................................. 45
Lower Mississippi River Safety Study............................................................................ 45Louisiana World Exposition ........................................................................................... 45International RiverCenter................................................................................................ 46New Orleans Aquarium of the Americas........................................................................ 46Gaming Vessel Risks and Background........................................................................... 47Operation Safe River....................................................................................................... 50
Changes Made Since the Accident......................................................................................... 51River Front Alert Network.............................................................................................. 51New Notices, Rules, and Operating Regulations............................................................ 51Steering Loss Study ........................................................................................................ 53Ship Drill Alarms............................................................................................................ 53Riverwalk Marketplace Alert System............................................................................. 53

v
Vessel Egress ..................................................................................................................54Status of the Queen of New Orleans............................................................................... 54
General .......................................................................................................................................... 55
ANALYSISAccident Overview........................................................................................................................ 55Engineering Aspects...................................................................................................................... 56
Main Engine Shutdown and Restart....................................................................................... 56Lubricating Oil Pump Operation............................................................................................ 57General Condition of the Bright Field’s Engineering Plant................................................... 57Vessel Owner’s Oversight of the Bright Field’s Engineering Plant ...................................... 58
Communication ............................................................................................................................. 59Master-Pilot Briefing at the Anchorage ................................................................................. 59Language Differences............................................................................................................. 60Information Exchange During the Emergency....................................................................... 60
Emergency Response..................................................................................................................... 62Vessel Emergency Preparedness and Evacuation Plans................................................................ 63
Vessel Evacuation .................................................................................................................. 63Emergency Drills.................................................................................................................... 65Safety Briefings and Signage ................................................................................................. 66Shoreside Emergency Alert and Response............................................................................. 67
Toxicological Testing.................................................................................................................... 68Risk Assessment and Risk Management....................................................................................... 69Findings......................................................................................................................................... 75
CONCLUSIONSFindings......................................................................................................................................... 74Probable Cause.............................................................................................................................. 76
RECOMMENDATIONS ............................................................................................................ 77
APPENDIXESAPPENDIX A--Investigation........................................................................................................ 81APPENDIX B--Chronology of Bright Field Engineering Problems ............................................ 83APPENDIX C--Voyage Data Recorders (VDRs) ......................................................................... 89


vii
Shortly after 1400 on December 14, 1996,the fully loaded Liberian bulk carrier BrightField temporarily lost propulsion power as thevessel was navigating outbound in the LowerMississippi River at New Orleans, Louisiana.The vessel struck a wharf adjacent to apopulated commercial area that included ashopping mall, a condominium parking garage,and a hotel. No fatalities resulted from theaccident, and no one aboard the Bright Fieldwas injured; however, 4 serious injuries and 58minor injuries were sustained duringevacuations of shore facilities, a gaming vessel,and an excursion vessel located near the impactarea. Total property damages to the Bright Fieldand to shoreside facilities were estimated atabout $20 million.
The National Transportation Safety Boarddetermines that the probable cause of thisaccident was the failure of Clearsky ShippingCompany to adequately manage and oversee themaintenance of the engineering plant aboard theBright Field, with the result that the vesseltemporarily lost power while navigating a high-risk area of the Mississippi River. Contributingto the amount of property damage and thenumber and types of injuries sustained duringthe accident was the failure of the U.S. CoastGuard, the Board of Commissioners of the Portof New Orleans, and International RiverCenterto adequately assess, manage, or mitigate the
risks associated with locating unprotectedcommercial enterprises in areas vulnerable tovessel strikes.
The major safety issues identified in thisinvestigation are the adequacy of the ship’smain engine and automation systems, theadequacy of emergency preparedness andevacuation plans of vessels moored in thePoydras Street wharf area, and the adequacy ofport risk assessment for activities within thePort of New Orleans. This report also addressesthree other issues: the actions of the pilot andcrew during the emergency, the lack of effectivecommunication (as it relates to the actions of thepilot and crew aboard the Bright Field on theday of the accident), and the delay inadministering toxicological tests to the vesselcrew.
As a result of its investigation of thisaccident, the Safety Board issued safetyrecommendations to the U.S. Coast Guard, theU.S. Army Corps of Engineers, the State ofLouisiana, the Board of Commissioners of thePort of New Orleans, International RiverCenter,Clearsky Shipping Company, New OrleansPaddlewheels, Inc., the New Orleans BatonRouge Steamship Pilots Association, theCrescent River Port Pilots Association, andAssociated Federal Pilots and Docking Mastersof Louisiana, Inc.
EXECUTIVE SUMMARY


1
SynopsisShortly after 1400 on December 14, 1996,
the fully loaded Liberian bulk carrier BrightField temporarily lost propulsion power as thevessel was navigating outbound in the LowerMississippi River at New Orleans, Louisiana.The vessel struck a wharf adjacent to apopulated commercial area that included ashopping mall, a condominium parking garage,and a hotel. No fatalities resulted from theaccident, and no one aboard the Bright Fieldwas injured; however, 4 serious injuries and 58minor injuries were sustained duringevacuations of shore facilities, a gaming vessel,and an excursion vessel located near the impactarea. Total property damages to the Bright Fieldand to shoreside facilities were estimated atabout $20 million.
Preaccident EventsAccording to vessel records, on September 2,
1996, the 735-foot, 36,120 gross-ton Bright Fieldcompleted loading a cargo of coal inBanjarmasin, Indonesia. On September 12, 1996,the vessel departed Indonesia with a 28-memberChinese crew bound for Davant, Louisiana. Theestimated date of arrival at Southwest Pass,Louisiana,1 (the vessel’s entrance point to theMississippi River) was October 26, 1996. Shortlyafter departure, the ship began to experienceproblems with its engineering plant, necessitatinga 3-day layover in Singapore while repairs weremade to the main engine. After the repairs werecompleted, the Bright Field continued its voyage.The trip was interrupted on several occasions bycontinuing main engine problems.
On November 21, 1996, the Bright Fieldarrived at a bulk coal-handling facility nearDavant, Louisiana (mile 55 AHP2), where it
1Southwest Pass is the westernmost of the severalentrances to the Mississippi River and is the one most oftenused.
2Distances in the Mississippi River are measured instatute miles “above head of passes” (AHP), which islocated 20 miles above Southwest Pass.
unloaded its cargo. (See figure 1.) After its holdswere prepared to load grain and after waiting fora loading berth, the Bright Field arrived atCargill Terminal, located at mile 140 AHP inReserve, Louisiana, on December 9, 1996.There the vessel loaded 56,397 metric tons ofcorn in its seven cargo holds. The vessel left theterminal at 1530 on December 11, 1996.3 Thevessel moved from the terminal area to thelower portion of La Place Anchorage at mile135 AHP, where it remained at anchor for 2days while scheduled repairs were made to themain engine’s turbocharger and air cooler.
On December 14, 1996, the vessel’s agentcontacted the New Orleans Baton RougeSteamship Pilots Association (NOBRA) andrequested that a pilot be dispatched to the vessel.4
The sailing time was set for 1030. The pilot whowas dispatched to the Bright Field stated that hewas called for duty about 0730. He said he wastold that the ship was headed to sea, whichmeant that he would take the ship to a specifiedlocation, where he would be replaced by a pilotfrom the Crescent River Port Pilots Associationfor the remainder of the trip downriver. Thepilot said he expected to be aboard the BrightField for about 3 hours.
The Bright Field third mate and chiefelectrician stated that on the morning ofDecember 14 they completed all predeparturetests for both bridge and engineering, includingtesting the bridge main engine console lights andalarms. With the successful completion of thetests, the master ordered standby engines at 0943.The pilot boarded the vessel via launch at 1040,
3At the time of departure, the draft of the vessel was11.96 meters (about 39 feet 4 inches) forward and 12.06meters (about 39 feet 8 inches) aft.
4Louisiana State law requires that a qualified andcertified State pilot be on board any vessel in foreign tradenavigating the Mississippi River in the State. AlthoughNOBRA, as well as other pilot associations, dispatchespilots, bills and collects pilotage fees, and pays associationexpenses, including staff and transportation fees, the pilotsthemselves are self-employed and contract for their servicesdirectly with vessel operators.
INVESTIGATION

2
N
0LOH473
0LOH453
0LOH433
0LOH<8
0LOH83
7R#*XOI#RI
0H[LFR#DQG
+HDG#RI#3DVVHV/$.(#3217&+$575$,1
1(:25/($16
# $
%
&
'
:
#$%&':
0#5HVHUYH0#1RUFR0#'HVWUHKDQ0#1LQH#0LOH#3RLQW0#'DYDQW0#$FFLGHQW#6LWH
/RFDWLRQ#/HJHQG
F igure 1 -- Low er M iss iss ipp i R ive r

3
and the third mate escorted him to thewheelhouse, where he was introduced to themaster at 1044.
The ship’s master spoke what the pilotdescribed as broken, but adequate, English. Thepilot said that, to facilitate communication, hespoke slowly and used simple words, and hebelieved that he and the master understood eachother. The master also stated that he wassatisfied with their ability to communicate. Thepilot said he gave helm orders in English to thehelmsman, who repeated them in English beforecarrying them out. The second mate reportedthat he also repeated (in English) the pilot’sorders and then carried them out. Other thanorders and their repetition, the pilot said he hadno verbal exchanges with the second mate or thehelmsman.
The pilot, who had not previously handledthe Bright Field, said he asked if the ship’snavigational equipment and engine were in goodworking order. He stated that the masteranswered with “just a simple ‘yes’ to bothquestions.” The master stated that he asked thepilot about the operational procedures fordeparting the anchorage.5 These were the onlyitems reported as being discussed during thepredeparture briefing. The pilot said he thenproceeded to acquaint himself with thewheelhouse layout (figure 2) and with thevessel’s posted maneuvering information. At thetime, the vessel’s main engine was beingoperated from the wheelhouse.
At 1055,6 the pilot began the normalprocedures for getting underway by ordering thefirst engineering maneuvering bell (dead slowahead). According to the third mate, he (thethird mate) attempted to execute the pilot’sorder using the wheelhouse engine controls, butthe vessel’s main engine did not start. He thencalled the engine control room and told the chiefengineer—in Chinese—that the engine did notstart. Engine control was transferred to theengine control room. Both the master and thechief engineer stated that their normal practice
5This information typically includes, among otherdetails, the location of assist tugboats and the order inwhich the two anchors are to be raised.
6Times are taken from engine bell logs.
was to transfer engine control to the enginecontrol room in the event of a nonemergencyproblem with the propulsion system.
After the engines were started (1055.5, deadslow ahead), engine control was transferredback to the wheelhouse. The pilot ordered stopengine, and the engine was stopped. At 1110,the pilot ordered dead slow ahead. Again, theengine could not be started from thewheelhouse, and again control was transferredto the engine control room, from which theengine was restarted. After the accident, thepilot stated that he had not been advised of thedifficulties in starting the engine from thewheelhouse, nor was he informed on thoseoccasions when engine control was transferredto or from the engine control room.
The Bright Field departed the La Placeanchorage at 1112. Engine maneuvering controlwas transferred back to the wheelhouse, and thepilot ordered full ahead maneuvering speed (56rpm) in order to familiarize himself with theship’s responsiveness to rudder and engineorders. He said he determined that the BrightField handled as expected for a fully loadedbulk cargo vessel operating in high-river-stageconditions.7 At 1134, the pilot ordered sea speed(72 rpm) for better ship handling. The pilot saidit was necessary to operate the ship at maximumspeed in order to obtain the best maneuverabilityin that operating environment.
Engine rpm was increased to sea speedusing wheelhouse controls. At 1159, as thevessel approached Norco, Louisiana, the pilotordered the Bright Field’s speed reduced to fullahead maneuvering speed (56 rpm). The BrightField remained at full ahead maneuvering speeduntil it reached the vicinity of Destrehan,Louisiana, when the pilot again ordered seaspeed of 72 rpm, resulting in a ground speed(speed of the ship plus speed of the current) ofabout 16 knots.
About 1300, the pilot ordered the master tosend a seaman to stand by the anchors.8 The
7On the day of the accident, the river was at high riverstage, measuring 12.5 feet on the Carrollton gauge with anapproximate 4 1/2-mph current.
8A Board of Commissioners of the Port of NewOrleans ordinance required that all vessels navigating

4
master sent the ship’s carpenter, with a handheldradio, to serve as anchor watch.9 A few milesabove Nine Mile Point, the pilot establishedVHF communications10 with an inbound towand inbound ship, both below Nine Mile Point.The vessels agreed to a starboard-to-starboardmeeting, and all three vessels met at the point.The pilot of the Bright Field said that, becausethe inbound tow was farther off the bank thananticipated, he maneuvered his ship closer to theleft descending bank of the river. The Bright
through the New Orleans Port area maintain an anchorstandby of at least one competent seaman, who was to bestationed at the anchor windless and be prepared to dropanchor if necessary.
9Serving as anchor watch was a regularly assignedduty of the Bright Field’s carpenter.
10VHF channel 67 was assigned for routine bridge-to-bridge (navigation/safety) communication in the LowerMississippi River.
Field pilot sounded the danger signal11 to alertthe workers at the Southport barge fleetingfacility12 to the proximity of the Bright Field.The Bright Field passed the area withoutincident and continued down the river at seaspeed. The master told Safety Boardinvestigators that about this time he becameconcerned that the pilot might be oversteeringthe vessel, but he said he did not voice hisconcerns to the pilot.
About 1350, the pilot made the first radiocall to the U.S. Coast Guard Gretna lightoperator.13 The Gretna light operator advised the
11Five or more shorts blasts on the ship’s whistle.12A fleet in this instance refers to one or more tiers of
barges. A fleeting facility is the geographic area along ornear a river bank where a barge mooring service is located.
13According to 33 Code of Federal Regulations (CFR)161.402(b), “Movements of vessels in vicinity of AlgiersPoint, New Orleans Harbor,” during a high river stage,
1$9,*$7,21(48,30(17
&+$577$%/(
5$'$52$53$
72#/2:(5'(&.6
+(/060$1
+$/$50#/,*+7627(/(3+21(6,
5$'$5
+(/0
*<523,/27
:,1'2:6#+8,
:+,67/(&21752/%87721
0$67(5
3257%5,'*(:,1*
:,1'2:6
6(&21'0$7(
0$18(9(5,1*/(9(52(1*,1(
25'(57(/(*5$3+:2+#(1*,1(
&21752/#&2162/(
67$5%2$5'%5,'*(:,1*
$)7
):'
Figure 2 -- navigation bridge layoutBri g ht Field

5
Bright Field that the ship was cleared to transitAlgiers Point and that a seagoing tow boat wasinbound at the Point. The pilot stated that, whilethe Bright Field was transiting under theCrescent City Connection Bridges, he allowedthe vessel to acquire a current-induced swing toport to facilitate the upcoming maneuver aroundAlgiers Point.
The AccidentThe swing to port as the ship passed under
the Crescent City Connection Bridges pointedthe vessel toward the left descending bank, theside of the river where the Poydras Street wharfand the Riverwalk Marketplace shopping mallwere located and where gaming, excursion, andcruise ships were docked. About 1406, while theBright Field was still transiting under thebridges, power output from the vessel’s mainengine dropped. At this time, the vessel’sautomated propulsion control system14 reportedlow main engine lubricating oil pressure andmain engine trip due to low oil pressure.15
The pilot said he noticed that the vessel hadgotten quiet and that the engine-induced vesselvibrations had stopped. He said he turned andsaw the master and the second mate16 standingbeside the engine order telegraph (on the otherside of the bridge from the pilot), looking downat something on the console. He said he askedthem if there was a problem, but got noresponse. He said that he did not ask a secondtime “because they didn’t answer me the firsttime.” He reported that he then looked at theengine rpm indicator and saw that engine rpm
movement of vessels around Algiers Point is controlled byseveral Coast Guard-operated and maintained traffic lights,including Gretna light at 96.6 miles AHP and GovernorNicholls light at 94.3 AHP.
14For the purposes of this report, automatedpropulsion control system and related terms will be used torefer to all main engine control, monitoring, and alarmsystems and subsystems.
15The main engine was equipped with protectiondevices that could slow down or stop the main enginedepending on the severity of the problem. See the “MainEngine Description” section of this report for informationabout the engine and its protective devices.
16The second mate had come on duty at the noonwatch to replace the third mate who had been on duty whenthe ship left the anchorage.
had dropped from about 70 to about 30,indicating to him that the vessel had experienceda significant reduction in engine power.
The master and the second mate said thatthey also noticed that the ship’s normal operatingvibrations had stopped, and they observed that themain engine rpm indicator showed a drop toabout 30 rpm. The master said the pilot “blurtedout, ‘What has happened?’” and he (the master)thought he had answered the pilot by sayingthere had been a reduction in main enginepower. The master said it was not clear to himwhy engine rpm had dropped. He said heinstructed the second mate “to call theengineroom to inquire about what happened,what’s going on. I asked the second mate todemand them to increase speed right away.” Thesecond mate said that he carried out the master’sorder immediately.
The pilot stated that when he realized that thevessel had lost power, he “jumped” out of hischair and called the Governor Nicholls Lightoperator on VHF channel 67. He said that as hemade the call he was looking out the bridgewindows and was aware that the vessel wasswinging to port and toward the docked shipsalong the left descending bank. The pilot told theGovernor Nicholls light operator that his ship hadlost power and that the operator should alerteveryone in the harbor.17
The pilot said that, after calling the lightoperator, he ordered hard starboard rudder as theship continued to swing to port. The helmsmanresponded to the order by applying hardstarboard rudder, but the new rudder setting didnothing to alter the vessel’s direction, and thepilot began sounding the danger signal using theship’s forward whistle. He said he wanted toattract the attention of the cruise ships andpublic along the left descending river bank. Thepilot stated that he ordered the master on at leasttwo occasions to have someone stand by the
17Information regarding radio transmissions usingVHF channel 67 is based on audio recordings made by thetugboat Lockmaster, located on the side of the riveropposite the Poydras Street wharf. The Lockmaster wasalso able to provide a videotape of radar images of theBright Field as it approached and struck the wharf. Thetraffic light stations were not equipped to record radiotransmissions.

6
anchors, but he did not hear the masteracknowledge the order. The pilot said he recalledthe master speaking Chinese on the radio andthat the master did not appear to be agitated, butwas “very nonchalant.”
When the pilot noted that the rpm indicatorcontinued to show a loss of power, he madeanother call to the Governor Nicholls lightoperator. He told the operator to warn the cruiseships and gaming and excursion vessels thatwere moored along the left descending bank.The Gretna light operator advised the pilot that atugboat 1 mile upriver was coming to his aid.
The chief engineer on duty in the enginecontrol room18 (figure 3) stated that,immediately before the engine lost power, anaudible alarm sounded. He said he then lookedat a computer screen in front of him and saw avisual alarm and an indication of a loss ofpressure in the lubricating oil system. (Seefigure 4.) He said he looked at the analog mainengine lubricating oil pressure gauge and sawthat the system was rapidly “depressurizing”below normal levels. He said he then noticedthat the main engine automatic slow down lightwas on, and he noticed that main engine noisewas decreasing. He reported that he alsoobserved that engine rpm had dropped from 72to between 30 and 35. He said that, as he turnedto the electrical switchboard behind him todetermine why the No. 2 lubricating oil pumphad not started automatically, the pump started.He said that, except for the low rpm, everythingseemed to him to be back to normal almostimmediately.
According to the chief engineer, he wasabout to call the bridge when the second matecalled him. He said that the second mate askedhim why the main engine was slowing down andtold him to increase the speed immediately, thatthey were transiting the bridge at that time. Thechief engineer reported that the second matespoke to him in a normal tone of voice, without
18At the time of the accident, Coast Guard regulationsdid not require that engineering spaces be manned duringtransit of the Mississippi River. Although the Bright Fieldwas classed for unattended operation of machinery spaces,company regulations required that the chief engineer andtwo other engineers be on duty in the engine control roomwhenever the vessel was entering or leaving a port.
repeating his message. The chief engineer saidhe thought the second mate was concernedabout speeding up passage of the vessel beneaththe bridges. He said he did not know the natureof the situation on the vessel’s bridge.
The chief engineer told the second mate thathe did not know the reason for the sudden dropin the No. 1 oil pump pressure, but since the No.2 pump had already come on line, thepressurization problem was solved. Neither themaster nor the second mate attempted to clearthe trip condition and restart the engine, andthus restore rpm, from the bridge controls. Thechief engineer and the second mate mutuallyagreed to transfer engine control to the enginecontrol room, and the chief engineer began theprocess of restoring engine power. He said thatengine rpm quickly reached about 52 rpm, afterwhich rpm continued to increase to about 60.According to alarm logs, main engine powerwas restored to the vessel at 1408, about 2minutes after the logs indicated that the mainengine had tripped.
In postaccident testimony, the master wasasked if it had been necessary to transfer enginecontrol from the bridge to the engine controlroom during the emergency. He said, “Undernormal circumstances, speed increase can bedone from the engine [control room] morequickly.” The master was asked why the enginecontrol room had requested that engine controlbe shifted from the bridge to the engineroom.He said that it was “because the engineeringdepartment [didn’t] realize the sense of urgencyor [that] there [was] any sense of urgency on thebridge.” He said engine control room personnelwere not initially notified of the emergencysituation but were told later when the allision19
was unavoidable even if vessel speed wereincreased.
The pilot stated that at this time he wasdevoting his attention to sounding the dangersignal to alert the moored ships along the leftdescending bank and the Riverwalk complexand that he was not immediately aware, nor was
19In marine usage, allision refers to a moving shipstriking a stationary ship or other stationary object.

7
Figure 3 -- engine control room layout showingreported positions of crewm em bers when engine powerreduction occurred.
Bright Field
0DLQ#(QJLQH*DXJHV 7HUDVDNL#0RQLWRUV
0DLQ#(QJLQH&RQWUROV
(QJLQHHU·V:RUNVSDFH 'HVN
6HFRQG#(QJLQHHU&KLHI#(QJLQHHU
7KLUG#(QJLQHHU
(OHFWULFDO#6ZLWFKERDUGV#)#0RWRU#&RQWUROOHUV
)25:$5'
(QJLQHHULQJ#FRQWURO/#PRQLWRU/#DQG#DODUP#FRQVROH
0DLQ(QJLQH5HPRWH&RQWURO&LUFXLWV
$2&
Figure 4 -- Engineering control, monitor, and alarm console

8
he made aware by the mate or the master, thatvessel power had been restored. The pilot saidthat he was not aware of what, if any, actionsthe master or the crew were taking to restorepower. The master’s orders to the second mateand the second mate’s conversations with thechief engineer were in Chinese.
The vessel continued to swing to port andtoward the left descending bank. The pilot toldthe master to prepare to drop anchors andordered the main engine full astern. The vessel’sbell logger tape, which continuously capturesdata and prints it out in 30-second intervals,recorded that the full-astern order was madefrom the bridge at 1409.5 and answered by theengine control room at 1410.0. The chiefengineer stated that he reversed the engine andran the shaft speed to 20 to 40 (fluctuating) rpmastern.
The pilot stated that, shortly thereafter, heordered the anchors dropped. The master saidthe pilot ordered only the port anchor dropped,that he concurred with that order, and thatthough he did not acknowledge the order to thepilot, he attempted to carry it out. The mastersaid that he attempted to call the carpenter onthe forecastle using the handheld radio. Thecarpenter, who was standing by the anchors,said that he could not hear radio transmissionsfrom the master because the danger signal wasstill being sounded on the ship’s whistle, whichwas located about 20 feet above his station onthe bow. The master said he made repeatedunsuccessful attempts to contact the carpenterbut did not ask the pilot to suspend the soundingof the danger signal. The pilot stated that hestopped sounding the signal only long enough tomake short radio transmissions to the trafficlight operators to urge them to call the NewOrleans Riverwalk complex and “tell the peopleto get away from the dock.”
The master stated that he rushed out to theport bridge wing and waved his arms to attractthe carpenter’s attention. When he realized thatthe carpenter did not see him, the master wentback inside the bridge. Once back inside,intermittent communications were establishedbetween the master and the carpenter. By thetime reliable communication was established,the ship had moved farther toward the wharf,and the master said he believed that dropping
the anchor at that time would cause the ship totake a sharp turn to the left and perhaps strikeone of the vessels docked there. He said hetherefore told the carpenter not to drop theanchor. The master said that after the ship hadmoved a little farther, he again contacted thecarpenter and told him to drop the anchor tokeep the ship from striking the docked vessels.The carpenter said he turned the brake wheel tolet go of the port anchor and then ran from thebow to avoid being injured in the imminentallision. Postaccident review of an amateurvideotape of the allision indicated that theanchor did not drop prior to impact.
According to statements of the pilot andcrewmembers, the pilot did not ask either themaster or second mate if the vessel’s power hadbeen restored or if the anchors had beendropped, and no one volunteered thatinformation. The pilot said he had not felt anyengine vibrations, though he expected to. Hesaid, “When that big engine turns, you feel it.”The master said the vibrations caused by theengine when it started in reverse while the shipwas still moving forward were obvious. Nofurther communications were reported betweenthe pilot and master or the pilot and the secondmate before the allision.
Meanwhile, the cruise ship Enchanted Islewas docked at the Erato Street wharf on the leftdescending bank of the river. Passengerembarkation had begun about 1230, and about200 passengers were on board. Crewmembersaboard the cruise ship did not (and were notrequired to) monitor VHF channel 67 andtherefore did not hear any radio announcementfrom the traffic light operator regarding theBright Field. They did state that they heard thevessel’s danger whistle. The third officer said hewas on the bridge as the Bright Field passedunder the Crescent City Connection Bridges andthat he knew the vessel was in trouble when heheard its whistle blow for the fifth time. Hestated that he ran out onto the outside deck andsaw the Bright Field passing his ship on a directpath to the Riverwalk area. The ship’s master,who had also heard the Bright Field’s whistle,reached the bridge as the Bright Field went past.The officers activated the public address systemand placed the bridge on standby to close thewatertight doors. The third officer said that heand the master called for the forward dock lines

9
to be tightened to protect against gangwaydisplacement as the Bright Field bow wavestruck the vessel. They also notified thegangway watchman of a possible river surge andsent two crewmen to watch over the gangwayand report any trouble back to the bridge.According to the third officer, the Bright Fieldwas clear of the Enchanted Isle throughout theaccident sequence.
Moored about 150 to 200 feet downriverfrom the stern of the Enchanted Isle was thecruise ship Nieuw Amsterdam. The ship hadbegun embarking passengers about 1330, and anestimated 200 to 300 passengers were on boardat the time of the accident. The crew did not(and was not required to) monitor VHF channel67. The second officer said he was standingbehind the port-side radar when his attentionwas drawn to a ship on the river sounding anemergency alarm. The second officer reportedthat he could not immediately determine whichvessel was sounding the alarm, so he and thechief officer went out to the port side bridgewing (the vessel was docked with its starboardside toward the wharf) and saw the Bright Fieldpassing under the Crescent City ConnectionBridges. They said they stood and watched theBright Field as it headed toward their ship andthe Poydras Street wharf area. They entered thewheelhouse to warn the on-duty third officer.
The Nieuw Amsterdam’s on-duty thirdofficer said he also had heard the multiplewhistle signals and had watched the BrightField as it passed under the bridges with its bowpointing toward his vessel. He said that theBright Field appeared to be about 1/2 nauticalmile away and moving at 8 to 10 knots. Basedon his observations of the Bright Field’sdirection of travel and the whistle sounding, hesaid, he assumed the vessel was experiencingsteering or engine failure. He immediatelywarned the master, who was in his stateroomdirectly behind the bridge.
The Nieuw Amsterdam’s master instructedthe on-duty officer to tell the security officer atthe gangway to stop the embarkation ofpassengers. The on-duty officer was then toplace the bridge on standby, close the watertightdoors, and activate the public address system.The master instructed the second and thirdofficers to go to the stern of the ship with radios
and to evacuate the Lido deck aft, then clear thedecks on the port side and monitor the situation.The crew said that after 2 or 3 minutes it wasapparent that the Bright Field would not strikethe Nieuw Amsterdam. The master and the on-duty officer followed the progress of the BrightField from the port wing bridge. They assessedthe situation and determined that the BrightField would miss the Nieuw Amsterdam byapproximately 50 meters (164 feet).
The first mate of the gaming vessel Queenof New Orleans, which was docked at thePoydras Street wharf with its bow less than1,000 feet downriver from the stern of theNieuw Amsterdam, had overheard the BrightField pilot’s call to the traffic light operator onVHF channel 67 (although the vessel was notrequired to monitor the frequency) and hadimmediately begun emergency evacuation of the637 passengers and crewmembers aboard thevessel.20 Meanwhile, the excursion vesselCreole Queen, which had been docked at theCanal Street wharf downriver from the Queen ofNew Orleans, was in the process of pullingaway from the dock with 190 passengers andcrew on board. The master said he heard thepilot of the Bright Field radio the GovernorNicholls light operator and report, “I’ve losteverything. The ship is heading toward thepassenger vessels.” The master said that hereturned the vessel to the dock and ordered anemergency evacuation.
According to the results of Safety Boardsurveys, patrons and employees of theRiverwalk Marketplace along Poydras Streetwharf and the adjacent Julia Street and CanalStreet wharves were unaware of the meaning ofthe warning whistles from the Bright Field.Several harbor police officers did recognize thewarning whistles and tried to clear the area.While they did so, some marketplace patronsand staff members noticed the Bright Fieldheading toward them, and large numbers beganto flee. Many individuals sustained injuriesduring the evacuation. The harbor police wereable to move most of the crowd away from theexpected impact area. Many of those in the area
20For a detailed discussion of all the vesselevacuations, see the “Survival Aspects” section of thisreport.

10
said that they did not know what was happening,and because they had had so little advancenotice of a potential hazard, they did not havethe opportunity to obtain information from mallemployees or security officers.
About 1411, the port bow of the BrightField struck the Poydras Street wharf at alocation between the docked Nieuw Amsterdamand Queen of New Orleans. (See figure 5.) Thevessel struck the wharf at what witnesses saidwas a 40- to 45-degree angle, went into thewharf up to the end of the forecastle deck (about50 to 60 feet), and then made a sidewaysmovement. The bow portion of the vesselscraped and collapsed portions of the buildingson the Poydras Street wharf, including a portionof the Riverwalk Marketplace shopping mall, acondominium parking garage, and part of theHilton Riverside Hotel. The ship came to restagainst the wharf with its stern about 200 feetfrom the stern of the Nieuw Amsterdam and itsbow about 70 feet from the bow of the Queen ofNew Orleans. (See figure 6.) The pilot orderedthe engine stopped, after which several tugboatsarrived to hold the ship against the dock. About3 minutes had elapsed from the time the pilotmade his first emergency call to the Coast Guardlight operator until the ship struck the wharf.
InjuriesThe accident resulted in 4 serious and 58
minor injuries to persons in the Riverwalk area,aboard the Queen of New Orleans, or aboard theexcursion vessel Creole Queen, which was
docked near the Queen of New Orleans. (Seetable 1.)
Vessel DamageAfter striking the wharf, the bow of the
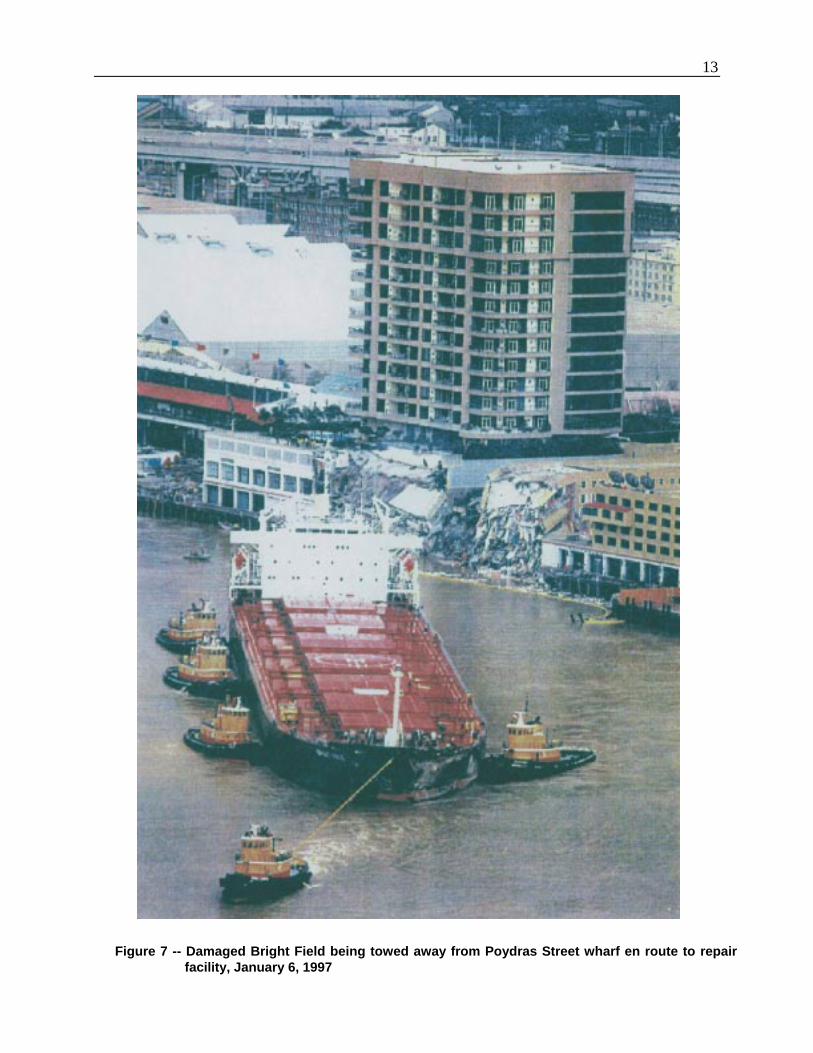
Bright Field grated along the concrete and steelwharf structure for a distance of about 600 feet.The allision damaged the port side of the bow.The hull of the vessel sustained two horizontalgashes about 100 feet long that penetrated theport side of the ship and extended down the portside from the fore peak (bow) ballast tank andinto the No. 1 cargo hold. Both the breachedfore peak tank and the No. 1 cargo hold flooded.A diver found a 100-foot section of the forwardhull resting on the river bottom adjacent to thePoydras Street wharf. Total damages to theBright Field were estimated to be about $2million. (See figure 7.) The vessels that hadbeen docked in the allision area did not sustainsignificant damage.
Other DamageThe One River Place condominium
building, located on the Poydras Street wharf,sustained damage to its valet parking garage.Residents of the building were evacuatedbecause of a loss of power and water. TheRiverwalk Marketplace, a mall with 100 stores,3 restaurants with outdoor seating, and a largewharf walkway, sustained damage to more than350 feet of its wharf frontage. About 10 percentof the mall shops and restaurants were affected.The New Orleans Hilton Riverside Hotel, partof which was situated on the Poydras Street
Table 1 -- Injuries Sustained in Bright Field Allision1
+0,74+'5 4KXGTYCNM"#TGC 3WGGP"QH"0GY"1TNGCPU %TGQNG"3WGGP 7PMPQYP 6QVCN
(#6#. 2 2 2 2 2
5'4+175 3 4 3 2 6
/+014 38 32 5 4; 7:
010' 5 2 2 4 7
616#. 42 34 6 53 89
1Table based on the injury criteria (49 CFR 830.2) of the International Civil Aviation Organization, which the
Safety Board uses in accident reports for all transportation modes.

11
N
$/*,(563RLQW#
0LOH#<717 0LOH#<8
)HUU\7HUPLQDO
0,66,66,33,5LYHU#)ORZ
7R#*XOI#RI0H[LFR
)HUU\#7HUPLQDO
&UHROH4XHHQ
:ROGHQEHUJ3DUN
:RUOG#7UDGH&HQWHU#EXLOGLQJ
1121#+LOWRQ
5LYHUZDON
4XHHQ#RI#1HZ2UOHDQV
1HZ#2UOHDQV&RQYHQWLRQ#)([KLELWLRQ&HQWHU
&UHVFHQW#&LW\&RQQHFWLRQ#%ULGJHV
0LOH<81:
&$1$/#671
-DFNVRQ#6TXDUH)UHQFK#4XDUWHU
7RXORXVH#6W:KDUI%LHQYLOOH#6W1:KDUI
&DQDO#6W1:KDUI
3R\GUDV#6W1:KDUI
-XOLD#6W1:KDUI
(UDWR#6W1:KDUI
7XJ#/RFNPDVWHU/RFDWLRQ
1LHXZ#$PVWHUGDP
(QFKDQWHG,VOH
%ULJKW#)LHOG
%ULJKW#)LHOG
Fig ure 5 -- Path of Bri g ht Field (not to scale)
$TXDULXP

13
Figure 7 -- Damaged Bright Field being towed away from Poydras Street wharf en route to repair facility, January 6, 1997

14
wharf, sustained damage to 40 of its 1,600rooms. Total damages to all facilities wereestimated to be about $18 million. (See figures 8and 9.)
Crew InformationThe Pilot -- The Bright Field pilot, age 46,
had been a NOBRA pilot for about 17 years. Hebegan his maritime career in 1969 when hestarted working on the Mississippi River duringcollege summer vacations. He served as adeckhand aboard the Delta Queen, apaddlewheel passenger vessel, and as adeckhand and mate aboard other passengervessels, including the Mississippi Queen and theNatchez. He also worked for a barge lineoperating on the Illinois River between St. Louisand Chicago.
In 1975, the pilot graduated from a 2-yearprogram at the National River Academy inHelena, Arkansas. The program consisted ofperiods of 2 months of classroom instructionfollowed by 2 months on a river vessel. Heobtained his first Coast Guard license, an inlandmate’s license, in 1975. He was commissionedby the New Orleans Baton Rouge State PilotsCommission as a pilot on January 16, 1980. Atthe time of the accident, he was a licensed rivermaster and first class pilot. The most recentrenewal of his license had been on May 5, 1995.
The pilot said that he had piloted on most ofthe vessel types transiting the Mississippi River.He said he navigated primarily foreign flagvessels anywhere from the New Orleans generalanchorage to Baton Rouge. The majority ofthese were deep-draft vessels, although he saidhe occasionally worked a seagoing tug andbarge. He said he averaged about 7 vesselassignments per week, totaling between 200 and300 ships each year. He stated that he had notattended any ship simulator training, and hebelieved that only one NOBRA pilot hadattended such training. He said he had notreceived any bridge resource management(BRM)21 training and was, in fact, unfamiliarwith the term and the concept.
21Bridge resource management entails effective use ofall available resources to achieve safe operations.
The pilot stated he had been involved inthree previous accidents. In 1983, the vessel hewas piloting struck a bridge when acrewmember raised a boom too high. Thesecond event occurred when the vessel he waspiloting lost steering shortly after he cameaboard. The vessel moved hard to starboard andhit a ship launch dock. The third event tookplace in spring 1996, when the pilot wasworking on board a vessel that lost ruddercontrol and struck the river bank.
For the 4 days prior to the accident, the pilotsaid, he had kept essentially the samesleep/wake schedule, arising shortly afterdaylight, about 0700, and retiring between 2230and 2300. He reported that he had slept well thenight before the accident, did not have any sleepabnormalities, and did not suffer from anyillnesses. He said he was not sick and that hehad taken no medications on the day of theaccident.
The Master -- The Bright Field master, age35, had been in the maritime industry for 14years. He began as an able seaman beforebecoming an apprentice officer. He thenprogressed from third, to second, to first, tochief officer, and then to master. He had been amaster for a little more than 1 1/2 years and hadserved on three different ships. He said he hadbeen master of the Bright Field for about 15weeks at the time of the accident (since August25, 1996). During his time with the Bright Field,he had spent about 3 months at sea and about 1month in port. He said he had been to NewOrleans twice before, in 1983 and 1989;however, this was his first trip as master. Hesaid he had never, on any vessel, experienced areduction in engine rpm of the kind thatoccurred just prior to this accident.
The master attended the Dalien MaritimeAcademy in China for 4 years and graduated inAugust 1982. His training involved more than40 deck officer-related courses. It also includedcomputer-based simulator training in shiphandling and maneuvering. He said he hadreceived additional simulator training on twooccasions at the Qingdao Mariner’s TrainingSchool. The first occasion involved radarplotting and ship handling to qualify for hisradar observer’s endorsement. The secondinvolved the handling of large vessels and

15
Figures 8 and 9 -- Postaccident scenes

16
occurred after he had passed his master’sexamination.
The master held a People’s Republic ofChina Marine Certificate of Competency, whichcertified that he was qualified to be a master ofships of 1,600 gross tons or more. The mostrecent endorsement of that certificate had beenon April 20, 1995. He also held a Republic ofLiberia license certifying his competence as amaster and radar observer on oceangoing vesselsof any gross tonnage. The most recentendorsement of that license had been on October3, 1996. Both licenses are valid for 5 years.
The master indicated he had receivedtraining that emphasized coordination amongthe bridge team, including the pilot. He said histraining covered the duties and responsibilitiesof each individual and stressed the need to beable to communicate with one another and assistone another in the performance of their duties.He said the training also stressed the integrationof the various responsibilities.
The master noted that, since he had held theposition of master, he had overruled pilots onfour occasions. On this trip he said,
I…instructed the carpenter not to dropthe anchor, which in effect…overruledthe pilot, because the pilot [had]instructed [me] to drop the anchor. [I]instructed the carpenter not to drop theanchor because [it] would [cause theBright Field to] swerve towards thepassenger ship. That, in effect, is a wayof overruling the pilot.
The master said he did not confer with thepilot about the change in the timing of the drop-anchor order because there was “no time.”
The master reported that he began to learnEnglish when he entered the maritime academy.He characterized his English language skills as“not bad among Chinese,” though he noted thathis ability to read the language was better thanhis ability to speak it. He said he did not haveany difficulty understanding the pilot on thistrip.
The master stated that he was required to beavailable 24 hours a day but that his normalschedule involved going to bed at midnight andarising at 0700 each day. He said he had keptthis schedule on the night before the allision,arising about 0715 after a complete night’ssleep. He reported that he was not sufferingfrom any long-term illnesses and that he was notsick and took no medications on the day of theaccident.
The Chief Engineer -- The Bright Field’schief engineer, age 34, began his maritimecareer in 1979. He studied marine engineering atthe Jimei Maritime School, graduating in 1982.He said he had been sailing aboard ships as anengineer since his graduation. He said he hadbeen a chief engineer for 4 years, had been withhis current employer for 1 month, and had beenchief engineer aboard the Bright Field for 3weeks prior to the allision. He came aboard theBright Field for the first time on November 21,1996, to replace the vessel’s previous chiefengineer (see below), who had been relieved ofduty upon the vessel’s arrival in New Orleans.
The chief engineer stated that he had servedon ships with both more and less automatedengineering equipment than the Bright Field andthat he was comfortable with the Bright Field’sautomation. He also said he had receivedtraining on automated ship systems at the DalienMaritime Academy in 1993 and that the lastship he served on before the Bright Field wasequipped with a similar system. While aboardthe Bright Field, he had been underway on shorttransits on four occasions for a total of 11 hours.During those occasions he said there were noengine casualties or automation problems,although various main engine repairs had beenmade while the ship was at anchor during the 3weeks he had been aboard.
The chief engineer held a People’s Republicof China Marine Certificate of Competency,which certified that he was qualified as a chiefengineer of ships of 3,000 kw (kilowatt, or4,023 hp) propulsion power or more. The mostrecent endorsement of that certificate had beenon October 27, 1993. He also held a Republic ofLiberia license certifying his competence as achief engineer on motor vessels of anypropulsion power. The most recent endorsement

17
of that license had been on May 23, 1995. Bothlicenses are valid for 5 years.
The chief engineer reported that his normalwork day began at 0800 and ended at 1700. Hisnormal sleep schedule was to go to bed at 2300and arise at 0700. In the 2 days prior to theallision, the Bright Field was at anchor, and theengineer was involved in some repairs. OnDecember 12, the turbocharger was repaired.Work began in the evening and was completedat 0220 the following morning, December 13.The chief engineer said he then went to bed andgot up shortly after 1000. That night he went tobed before 2300 and was awakened just after0600 on December 14 by the air coolertechnician, who needed his signature. He said heremained awake, but he did not actually startworking for the day until about 0920.
The chief engineer reported that he was notsuffering from any long-term illnesses and thathe was not sick and had taken no medications onthe day of the accident.
The Previous Chief Engineer -- Thevessel’s previous chief engineer had joined theBright Field in April 1996. He left the vessel inNew Orleans on November 21, 1996, after beingfired for what a company representative saidwas his failure to comply with company ordersabout the maintenance and operation of theBright Field’s engineering plant.
Vessel InformationFour vessels were docked near the point at
which the Bright Field struck the wharf. TheEnchanted Isle was docked at the Erato Streetwharf, and the Nieuw Amsterdam was docked atthe Julia Street wharf. The gaming vessel Queenof New Orleans was docked at the PoydrasStreet wharf in front of the Hilton RiversideHotel. The excursion vessel Creole Queen wasdocked at the Canal Street wharf.
Bright Field --The Bright Field, a bulkcargo carrier with seven cargo holds, was builtin 1988 by Sasebo Heavy Industries Co. Ltd., ofJapan. At the time of the accident, the ship wasowned by Clearsky Shipping Company, aLiberian corporation, and operated by CoscoH.K. Shipping Company, of Hong Kong. TheLiberian-registered vessel was 735 feet long,
weighed 68,200 deadweight tons, and had amaximum breadth of 106 feet.
The Bright Field was classed22 by DetNorske Veritas (DNV) for periodicallyunattended machinery space. When the BrightField was delivered, the original owners electedto have the unattended machinery space en-dorsement include specifications for preventivemaintenance and routine testing of automaticpropulsion system components, and theprocedures were verified periodically by DNV.The current owner of the vessel elected not tocontinue the preventive maintenanceendorsement of the original class certification.
The vessel was equipped with an IHI SulzerRTA62 slow-speed, five-cylinder, two-cycle,turbocharged, reversible diesel enginemanufactured by Ishikawajima-Harima HeavyIndustries (IHI) of Aioi, Japan. The 9,655-brakehp (7,200 kw) engine was directly coupled to a24-foot-diameter, four-blade, bronze propellercapable of driving the vessel to a speed of 15.5knots at sea speed.23 A change from ahead toastern required that the engine be stopped andrestarted with shaft rotation in the oppositedirection. A high-pressure compressed-airsystem was used to start the engine in eitherdirection and also to stop its rotation during achange from ahead to astern or vice versa.
The Bright Field’s engine was fitted withprotective devices (alarms and shut downs),sensors (pressure, temperature, etc.), andautomatic control equipment. In support ofunattended machinery operation, the vessel wasequipped with engine controls located on thebridge.
The Bright Field was configured as aconventional bulk carrier with an aftengineering plant and accommodation house.The navigation bridge was fitted with a charttable, navigation equipment, and an automatic
226JG" CRRNKECDNG" &08" TWNGU" KPEQTRQTCVGF" VJG+PVGTPCVKQPCN" #UUQEKCVKQP" QH" %NCUUKHKECVKQP" 5QEKGV[IU*+#%5+"WPKHKGF"TWNGU"CPF"VJG"International Convention forthe Safety of Life at Sea (SOLAS), %JCRVGT"33/3."2CTV"'0
23Because of the relatively rapid river current on theday of the accident, the Bright Field was traveling at aneffective speed that exceeded its rated sea speed.

18
radar plotting aid (ARPA)24 in its after part.Facing toward the bow, forward of the charttable to starboard of centerline, was the enginecontrol console with engine order telegraph. Tothe left of the console on the centerline was thehelm control console, comprising the helm, gyrocompass, and magnetic periscope compass.Forward of the console and suspended from theoverhead was a rudder angle indicator andengine order indicator. Below the forwardbridge windows was a gyro repeater, radar, VHFmarine radio, and manual buttons for the ship’swhistles.
Although not required by U.S. or Interna-tional Maritime Organization regulations, thevessel was equipped with a course recorder. In-vestigators determined that, at the time of thisaccident, the unit was inoperative because ofleaking graph recording pens. Examination ofthe course recorder paper determined that theunit had probably been out of service for sometime. When in working order, the unit recordsthe ship’s gyro heading over time.
The vessel was equipped with an enginetelegraph logger that automatically recordedengine telegraph orders (date and time) from thebridge and acknowledgments of the orders fromthe engine control room. The logger also notedwhether the engine was being operated from thecontrol room or wheelhouse. The time unitswere recorded in hours, minutes, and halfminutes. The unit did not record the ship’sactual engine rpm.
Automated Propulsion Control System -- Theautomated propulsion control system aboard theBright Field used components from a number ofmanufacturers, the primary two being IHI,which provided the main engine control system,and Terasaki, which provided the engineeringplant monitoring, alarm, and recording systems.Most remote control functions affecting the op-eration of the main engine, including theautomatic engine trip features, passed throughthe IHI control system. Dual independentTerasaki computers and monitors received sig-nals from sensing probes on engineering plantequipment and provided a status report,
24ARPAs are computer-based devices that processradar signals and display selected navigation information.
including operating and fault conditions.Conditions falling outside the acceptable oper-ating ranges were alarmed to appropriatewatchstanding and engineering personnel.Sasebo Heavy Industries, the ship’s builder,assembled and connected the variouscomponents of the automated propulsion controlsystem, including the bridge and engineeringremote control consoles.
The Bright Field’s automated propulsioncontrol system provided for operation of themain engine through use of either electro-pneumatic controls from the wheelhouse orpneumatic controls from the control room. Theengine could be controlled from the bridge usinga single maneuvering lever, which also acted asan engine telegraph transmitter. Although thebridge controls allowed the Bright Fieldengineroom to be unattended, company policyrequired that the engine control room beattended during operation in restricted waterssuch as the Mississippi River. Although eachoperating location was equipped with certainengine function controls that were not availableat the other location, the main engine could bestarted, stopped, reversed, accelerated, ordecelerated from either the wheelhouse or thecontrol room. Both control locations couldprovide main engine throttle control over thevessel’s two speed ranges: maneuvering mode(from dead slow speed of 30 rpm to full speedof 56 rpm) and sea mode (speeds up to themaximum of 72 rpm).
During normal operations, the rate at whichthe rpm of the Bright Field’s main engine couldbe increased was subject to limitations imposedby two independent components of theautomated propulsion control system: anacceleration-limiting program and a scavengingair pressure25 limiter.
The automatic acceleration-limitingprogram could be activated when the engine wasbeing operated in wheelhouse control. Theprogram allowed engine rpm to increase onlygradually, in accordance with a programmed(variable) acceleration rate. The wheelhousecontrol operator could activate a switch to
25Scavenging air is that air used to evacuate exhaustgasses from the engine’s cylinders after combustion.

19
bypass this program when engine speed neededto be increased quickly. The acceleration-limiting program was automatically bypassedwhen the engine was being operated from theengine control room.
The scavenging air pressure limiterfunctioned to reduce main engine exhaustemissions. Overriding the limiter injected morefuel into the engine, thereby increasing enginerpm at a slightly faster rate. The limiter wasautomatically overridden whenever wheelhousecontrols were moved to “crash (emergency)ahead” or “crash astern.” Also, a crashmaneuvering pushbutton on the engine controlroom console enabled engineering personnel tooverride the scavenging air pressure limiter ifnecessary. According to the second engineer,the crash maneuvering pushbutton was usedonly on the orders of a bridge officer, and suchan order was not given on the day of theaccident.
Transfer of engine operating control to orfrom the wheelhouse and engine control roomrequired communication and coordinationbetween bridge and engine control roompersonnel. Transfer of propulsion control wasphysically initiated by the engineer in thecontrol room, who first matched control settingsin the control room with those on the bridge,then set a selector switch to the desired mode.Transfer of control was completed when acrewmember in the wheelhouse pressed a buttonon the bridge to acknowledge the transfer.According to the Bright Field chief engineer,the transfer normally required 20 to 30 secondsfrom the time of the initial decision to make thetransfer until the changeover was accomplished.This time was confirmed in postaccident testing.
Audible and visual alarms on the bridge andin the engine control room were designed toactivate in the event of the following emergencyconditions: start failure (wheelhouse only),emergency manual stop, automatic emergencytrip, automatic slowdown, low control airpressure, low starting air pressure, controlpower failure, telegraph power failure, andautomatic failure of wheelhouse controls (autocontrol failure).
Automatic engine slowdown interrupts andautomatic engine trip due to high cooling water
temperature could be overridden without thefault having been corrected. The other mainengine trips, including trips resulting from lowlubricating oil pressure, required that the faultsbe corrected before engine operation could beresumed.
Engine Lubricating Oil System -- The mainengine lubrication oil system circulated 30-weight high-detergent oil from the 14-cubic-meter (about 3,700 gallons) sump located in themain engine foundation. A suction line pickedup the oil from the sump and delivered it to twoseparate oil lines. These oil lines passed the oilthrough wire mesh basket strainers beforedelivering it to two (designated as No. 1 and No.2) high-capacity (180 cubic meters, or 47,550gallons, per hour) lubricating oil pumps. (Seefigure 10.) Each pump was capable of boostingthe oil pressure to approximately 4 bar.26 Thedischarge piping from each pump met at a
26One bar is equal to .995 kg/cm2 or 14.5 psi.
Figure 10 -- Bright Field No. 1 (left) and No. 2lubricating oil pumps

20
common header, from which the oil passedthrough an oil cooler and a second filter. In thesecond filter, the oil was passed through 16 fine-mesh cylindrical strainers. At this point, thesystem pressure would have dropped byapproximately 1/2 to 1 bar. Various oiltemperature and pressure sensors monitored thecondition of the oil and signaled the status to theautomated control system. After beingcirculated through the engine, the lubricating oildrained back into the crankcase sump, where thecycle began again. A separate lubricating oilpurification system drew warm oil from the oilsump, passed it through a centrifugal separatorwhere water and contaminants were removed,and then returned the cleaned oil to the mainengine sump.
The chief engineer stated that the standardconfiguration for maneuvering the Bright Fieldin restricted waters included remote enginecontrol from the wheelhouse, the No. 1lubricating oil pump running, and the No. 2lubricating oil pump on standby. If theautomated propulsion control system detectedmain engine lubricating oil pressure below 2.5bar, it was designed to sound and display analarm in the engine control room, on the bridge,and in various locations in the accommodationspaces. If the pressure dropped below 2.4 bar, apressure-activated changeover switch wouldsignal the automated control system to start thestandby oil pump. If the pressure dropped belowabout 2.3 bar, the control system would, after abrief time delay, trip (shut down) the mainengine.
Cruise Ships -- The cruise ships at the Juliaand Erato Street wharves were normally mooredat this location on weekends to disembark andembark passengers and to load supplies. Thecruise ship Enchanted Isle was owned byAlmira Enterprises, Inc., and operated by NewCommodore Cruise Lines, Inc. The vessel, builtin 1958, was 574 feet long and was 13,681 grosstons. It was powered by a steam turboelectricpropulsion system. Maximum capacity was1,198 persons.
The Nieuw Amsterdam, moored at the JuliaStreet wharf, was owned by Hal Antillen, Inc.,and operated by Holland America LineWestours, Inc. The 704-foot, 16,027-gross-ton
vessel was built in 1983 and was powered by adirect-drive diesel engine.
Gaming and Excursion Vessels -- TheQueen of New Orleans was owned by HiltonNew Orleans, Inc., and New OrleansPaddlewheels, Inc., in an association known asQueen of New Orleans Joint Venture. Thevessel operated from a dock located at thePoydras Street wharf, on the riverfront behindthe New Orleans Hilton Riverside Hotel andRiverwalk Marketplace. The vessel conductedeight scheduled 90-minute cruises each day. Thevessel left its docking facility at the wharf every3 hours, beginning each day at 0245 and endingat 2345. Passengers were allowed on board forgambling 45 minutes prior to and 45 minutesafter each cruise.
The six-deck, 1,470-gross-ton, 245-foot-long vessel was built in 1993. It was powered bya Sternwheeler Propulsion System paddlewheel.Capacity was 300 crew and 1,500 passengers,for a total capacity of 1,800. The master of thevessel stated that the vessel had four decksaccessible to passengers. The first three deckswere all gaming areas; the fourth had a forwardcafé and an aft gaming area. On a normal day,about 20 percent of the passengers would be onthe first deck. The most crowded deck would bethe second deck, with about 40 percent of thepassengers. About 30 percent of the passengerswould be on the third deck, with only about 10percent on the fourth deck. At the time of theaccident, 637 persons were on board, including14 marine crew, 96 gaming personnel, 38security, nongaming, and miscellaneouspersonnel, and 489 passengers.
The Queen of New Orleans master statedthat, on the day of the accident, the vessel wasnot scheduled to leave the dock. Under normaloperations, if the river stage is “8 feet andrising,” the vessel remains at the dock. NewOrleans Paddlewheels, Inc., has stated that thevessel:
Does not leave the dock for regularlyscheduled cruises during foul weather,including rain, thunderstorms, showers,hail, fog and mist and wind conditionsin excess of 12 mph. Additionally, thevessel does not sail during seasonal highriver stage when the Governor Nicholl’s

21
traffic light is in operation.27 Finally, theQueen of New Orleans remains at dockduring port closures issued by theMarine Safety Office. When the vesselis dockside, the vessel remains open forbusiness and passengers are permitted toremain on board.
According to the Board of Commissionersof the Port of New Orleans (Dock Board), theprovisions of the Dock Board’s EmergencyManagement Checklist and Guidelines wereapplied to the Queen of New Orleans gamingvessel and its shoreside terminal as part of apermit process. The facilities and operationswere reviewed by a Dock Board consultant priorto approval of the permit and found to be incompliance with the guidelines.
The 3-deck, 397-gross-ton Creole Queen, a1,000-passenger-capacity paddlewheel excur-sion vessel, was 190 feet long and 40 feet wide.It normally departed the Canal Street dock fortwo daily sightseeing trips and one nightlydinner cruise. The overnight mooring locationfor the vessel was the Poydras Street wharf ad-jacent to the office of New OrleansPaddlewheels, Inc., the vessel’s owner. Theberth was destroyed as a result of being struckby the Bright Field. After the accident, theovernight mooring location was moved to theCanal Street wharf.
Waterway InformationAccording to information provided by the
U.S. Army Corps of Engineers, the MississippiRiver has a Federal project depth of 45 feet fromover the bar at Southwest Pass thence to the headof the passes and to mile 233.4 AHP, or about135 miles above New Orleans. Various areas ofthe Federal project are under constantmaintenance dredging. Southwest Pass has arecommended draft limit of 45 feet.
According to records supplied to the SafetyBoard by the Corps of Engineers, between 1983and 1996, mean monthly water temperatures in
27The company has told the Safety Board that sincethis policy was developed, the traffic lights have beenplaced in full-time operation; consequently, the policy isnow interpreted to refer to those times (high water stage)when the traffic lights are actually controlling river traffic.
the Mississippi River ranged from a low of 43.2°F in January to a high of 83.3 °F in August.Mean water temperature over the period for themonth of December was 49.6 °F.
River Stage -- On average, high river stageoccurs in April and the low river stage inOctober. At New Orleans, the extremedifference between high and low stage is 17feet; the mean difference is about 8 feet. Atseveral places in the lower part of the river,counter currents or eddies often are found nearthe banks. This occurrence is especiallypronounced in the area of Algiers Point.
Records maintained by the Corps ofEngineers indicated that the Carrollton gauge atmile 102.8 AHP on December 14, 1996, read12.5 feet (above a datum at New Orleans) andwas falling. Based on this reading, the Corps ofEngineers’ best estimate of the current below theCrescent City Connection Bridges in the area ofthe accident on December 14, 1996, was 4.5 mph.
At times of extremely high river stage, theCorps of Engineers has the option of openingthe Bonnet Carré Spillway, which, by diverting1/4 million cubic feet of water per secondthrough the spillway, lowers the river byapproximately 4 feet while reducing the speedof the current. According to the Corps ofEngineers, the spillway, located about 33 milesabove Canal Street, was built in 1932 to protectcommunities downstream of the spillway fromfloods, and to lower river stages generally, bydischarging floodwaters into LakePontchartrain, then into the Gulf of Mexico.According to the Corps of Engineers, undernormal operating conditions, opening thespillway is a complex task that requires about 36hours to complete. Prior to the Bright Fieldallision, the spillway had been opened seventimes since its construction, the last time in1983.28
Vessel Traffic Control -- The onlyoperational vessel traffic control system serving
28During what the Coast Guard termed“unprecedented high waters on the Mississippi River” inearly 1997, the Bonnet Carré Spillway was opened for theeighth time on March 17, 1997, to lower the water leveland combat strong river currents. The spillway remainedopen until April 18, 1997.

22
the Mississippi River in the New Orleans area isa series of traffic lights operated by the CoastGuard. When the river reaches 8 feet on theCarrollton gauge on the rising stage, and untilthe gauge reads 9 feet on a falling stage, themovement of all tugs with tows and all ships,whether under their own power or in tow (butexcluding tugs or towboats without tows or rivercraft of comparable size and maneuverabilityoperating under their own power) in the vicinityof Algiers Point is governed by the CoastGuard’s Governor Nicholls and Gretna trafficlights. The lights are visible throughout theentire width of the river and flash once everysecond. A green light displayed ahead of avessel (in the direction of travel) indicates thatAlgiers Point is clear and the vessel mayproceed. A red light displayed ahead of a vessel(in the direction of travel) indicates that AlgiersPoint is not clear and the vessel is not toproceed.
Port Information 29
More than 6,000 oceangoing ships and120,000 barge and tows travel through the Portof New Orleans30 each year. The port isprimarily a general cargo port. The frontage fordeep draft vessels within the port limits includesapproximately 34 miles along the riverbanks.The city of New Orleans is the majorcommercial area within the port limits. The Portof New Orleans has more than 28 miles ofpublic and private wharves and related facilities.The public docks can handle as many as 85ships at a time.
Most of the wharves along the New Orleanswaterfront are public facilities under the controlof the Dock Board. The Dock Board consists ofmembers selected by the Governor of Louisianafrom a list of nominees compiled by 18 businessand civic associations. The Dock Boardmaintains the depths of vessel berths adjacent toits public wharves from the face of the wharf to
29Information obtained from United States Coast Pilot5, from the Dock Board, and from other local and nationalreference sources.
30The Port of New Orleans extends along both sides ofthe river from mile 80.6 AHP to mile 115 AHP, andencompasses the city of New Orleans, several parishes orthe river frontage of those parishes, and a number ofsmaller communities.
100 feet into the river and assigns vessel berthsat its public wharves. The Coast Guard isprimarily responsible for control of navigationin the river, and the Corps of Engineers isprimarily responsible for approving newstructures in or on the river.
Subject to the above Federal jurisdictions,the Dock Board regulates activities related tomaritime commerce within the Port of NewOrleans and administers, controls, and regulatesthe public wharf facilities in the port. About 3/4of the wharf frontage is owned by the DockBoard and operated by private operators underoccupancy agreements from the board.
Above New Orleans, the Mississippi Riveris used by oceangoing vessels to Baton Rouge,about 135 miles above Canal Street in NewOrleans. The river channel between NewOrleans and Baton Rouge for the most part isdeep and clear. Facilities on the MississippiRiver above New Orleans to Baton Rougeinclude private and public terminals forhandling oil and other products on both sides ofthe river.
The Erato and Julia Street wharves, adjacentto the Poydras Street wharf, were used fordocking cruise ships from the Holland America,Carnival, and New Commodore cruise lines, aswell as U.S. Navy ships and, during annualMardi Gras, additional tourist ships, some ofwhich were used as hotels. The wharf area hadtwo passenger terminal buildings, a parking lot,and harbor police facilities. This wharf area wasaccessible only when cruise ships were at berthand was the only open public area not managedby a commercial tenant. Port of New OrleansHarbor Police officers were detailed to the areaand monitored police radios. In the event of anemergency, the harbor police officers providedevacuation direction and assistance in the cruiseterminal area. The remainder of the Port of NewOrleans public areas were under the control ofthe renters or lessees.
Dredging -- The Dock Board is responsiblefor dredging New Orleans Passenger Terminal(passenger/cruise ships) and Riverwalk piers toa distance of 100 feet out from the pier face. OnDecember 11, 1996, maintenance dredging wascompleted in the Riverwalk Marketplace andNew Orleans International Terminal areas. The

23
Dock Board specified that the dredging wouldextend to a 33-foot project depth. The passengerterminal was dredged only to a depth sufficientto accommodate the cruise ships that dockedthere. At the time of the accident, the depth wassufficient to accommodate the Enchanted Isle,which had a draft of 28 feet. The docking areaof the Queen of New Orleans had not beendredged since 1994 and had been left to silt in toafford the vessel protection from ramming bydeep-draft vessels. With the silting, water depthin the docking area was about 15 feet in averageriver stage conditions. Because of the dredgingand the high river stage that existed onDecember 14, 1996, the river was 45 to 48 feetdeep alongside the Poydras Street wharf in thearea of the Riverwalk Marketplace at the time ofthe accident.
The Wharf Area -- According to the DockBoard, the Canal, Poydras, and Julia Streetwharves were constructed early in this century.The wharves have been renovated or rebuiltseveral times since their original construction,but always on the same “footprint.” All of thesubstructure and first level decks of the wharveswere designed and built, and are currentlyowned, by the Dock Board. In 1977, theInternational RiverCenter (IRC) constructed acruise ship terminal on the first level of theUpper Poydras Street wharf. The terminal wasbuilt in conjunction with the development of thefirst phase of the Hilton Hotel. In 1983, the IRCcompleted the riverside expansion of the HiltonHotel, which was constructed on old warehousepiers on the river side of the levee flood wall.No additional footings or wharf extensions wereerected beneath or beyond the original piers atthe site of the Riverwalk complex.
In the early 1980s, the Louisiana WorldExposition (LWE) selected the Upper PoydrasStreet, Julia Street, and Erato Street wharves aslocations for the world’s fair’s riverfrontattractions. The last full year of cargo operationsat these wharves was 1981. In the LWE’s leaseagreement of July 1982, the Dock Board agreedto discontinue cargo operation and assignmentof lay-up vessels at the Julia, Poydras and EratoStreet wharves between May 1 and November15, 1984. The Dock Board’s lease with theLWE required that the first 15 feet of thewharves be kept unobstructed and inaccessibleto the public. Existing structures on the Julia
Street, Poydras Street, and Erato Street wharveswere significantly modified by construction offacilities for the world’s fair, however, thewharf deck profiles were not changed.
In 1986, the Rouse Company developed theRiverwalk mall on portions of the LowerPoydras, Upper Poydras, and Julia Streetwharves. The Rouse Company leased the landrights from the IRC and the city of NewOrleans. The Rouse Company was required toobtain construction permits for the RiverwalkMarketplace from the city of New Orleans andthe New Orleans Levee Board. Rouse wasgranted a consent agreement from the DockBoard to construct and operate the RiverwalkMarketplace. The Dock Board reviewed theRiverwalk mall plans to determine the extent towhich the development might affect Dock Boardactivities.
The One River Place condominium parkinggarage was constructed above the lower PoydrasStreet wharf and above the Riverwalkdevelopment. The condominiums werecompleted in 1989. One River Place was given alease agreement from the Dock Board toconstruct and operate the condominiums. OneRiver Place was required to obtain allappropriate city building permits.
In 1993, the Julia Street wharf cruise shipterminal was opened, replacing the originalterminal constructed by the IRC. Also in 1993,the Queen of New Orleans Joint Venturewidened a part of the Poydras Street wharf by50 feet and constructed a boarding tower on thewharf to accommodate a riverboat-style gamingvessel. (See figure 11.) The widened wharf andthe addition of a boarding tower were permittedby the Army Corps of Engineers, the DockBoard, and the city of New Orleans. No barrierswere constructed outboard of these structures.
The construction of wharves extending intothe navigable waters of the United States issubject to approval and issuance of a permit bythe Corps of Engineers. The Corps of Engineersrelies on the Coast Guard for any navigationalsafety concerns that such constructions mayraise.
Federal Jurisdiction -- While the CoastGuard is responsible for promoting the safety of

24

25
life and property on the navigable waters of theUnited States, the Corps of Engineers has finalauthority to approve any structure built on or inthe navigable waters of the United States,including the Mississippi River. A permit fromthe Corps of Engineers is required to situate astructure in or on any navigable waterway.Under the Rivers and Harbors Act of 1899, theCorps has jurisdiction over the establishment ofharbor lines and anchorages and themaintenance of clear passage along navigablewaterways. A permit is required to constructpiers, wharves, jetties, permanent moorings,permanently moored floating vessels, or anyother permanent or semipermanent obstacle orobstruction.
Meteorological InformationAt the time of the accident, winds were from
the east at 6 knots; clouds were scattered;visibility was 7 miles; the temperature was 70°F.31
Toxicological InformationPostaccident alcohol and drug tests were
conducted after this accident on the pilot andnine crewmembers who were on duty at the timeof the accident.32 Testing was ordered forcrewmembers assigned to the noon watch. Theship’s carpenter, who was acting as anchorwatch at the time of the accident, was notassigned to the noon watch and was not tested.
The crew’s tests were conducted by aspecimen collection and testing companyretained by the ship’s agent. The breath tests,using a portable testing device taken aboard theship, began at 2036, 6 hours and 25 minutesafter the accident. The last three tests done werethose of the helmsman at 2208, the master at2235, and the chief engineer at 2241. These testswere conducted 7 hours 57 minutes, 8 hours 24minutes, and 8 hours 30 minutes, respectively,after the accident. The results of all nine tests
31As reported from the Naval Air Station, Belle Chase,Louisiana.
32The master, second mate, helmsman, bridge lookout,chief engineer, second engineer, third engineer, electrician,and motorman.
showed 0.00 percent blood alcoholconcentration (BAC).
The same collection and testing companycollected urine specimens from the ninecrewmembers between 2030 and 2230. Thespecimens were sent to a Federally approvedtesting lab in New Orleans and tested for thepresence of five categories of illicit drugsspecified in Coast Guard and Department ofTransportation regulations.33 The specimenswere negative for the five drugs for all the testedcrewmembers.
The Safety Board requested a portion of thespecimens that remained after the lab completedits testing. Those portions were forwarded to theCenter for Human Toxicology (CHT) in SaltLake City for additional testing. The secondtesting confirmed that none of the five groups ofillicit drugs, nor any other drugs, were present inthe specimens. In addition, tests for urinealcohol concentration were negative for allspecimens. Traces of caffeine and/or smokingbyproducts were the only chemicals found insome specimens.
Urine and breath specimens for postaccidentalcohol and drug testing were obtained from thepilot about 1 1/2 hours after the accident (at1537 and at 1550, respectively). Results showeda BAC of 0.00 percent and were negative for thefive groups of illicit drugs tested. Additionaltesting requested by the Safety Board wasconducted on a portion of the urine specimen byCHT. Caffeine was the only drug found in thepilot’s specimen.
Coast Guard postaccident drug and alcoholtesting regulations (46 CFR Parts 4 and 16 and33 CFR Part 95) require specimen collection tooccur “as soon as practicable following anaccident.” The chronology of specimencollection in this accident (based onrecollections of the individuals involved) is asfollows:
1530 Ship’s agent learns of accident from thevessel charterer.
33The drugs specified in 49 CFR Part 40 aremarijuana, cocaine, opiates, amphetamines, andphencyclidine.

26
1600 Coast Guard investigator on board ship.Pilot not aboard. NOBRA was called toensure pilot was tested. NOBRA statesthat testing was in progress. Investigatorlooks for, but finds no evidence ofalcohol or drug impairment among crew.
1630 Ship’s agent representative on board.Ship’s attorney on board.
1700 Coast Guard Marine Safety Office(MSO) investigator orders ship’sattorney to test crew for drugs andalcohol.
1730 Ship’s agent general manager on board.
1834 Specimen collection and testing companycontacted by general manager when helearns that the Coast Guard wasexpecting the ship to call the drug testingcompany.
1955 First of two collectors arrives at scene.
2010 First collector arrives on board ship afterdifficulty getting past road blocks.
2030 First specimen taken.
2235 Second collector on board.
2245 Breath testing and urine specimencollection complete.
Survival AspectsBright Field -- The vessel master said the
crew was trained to respond to a particularemergency alarm that is sounded in case of afire, a pollution incident, or other emergency.The response normally entailed reporting to themain deck. The master stated the most recentfire and boat drill held aboard the Bright Field,in accordance with international and Republic ofLiberia rules, was on November 17, 1996. Hesaid fire and boat drills included the sounding ofthe emergency alarm and were normally heldweekly.
Enchanted Isle -- The Port of New OrleansHarbor Police arrived at the Enchanted Islegangway a few moments after the Bright Fieldstruck the wharf and requested that passenger
embarkation be stopped. Embarkation wasdelayed 4 to 5 minutes as the river surged andthe situation was assessed. According towitnesses, the gangway moved up and downbriefly with the swells, but no passengers wereon it at the time.
Nieuw Amsterdam -- After the Bright Fieldimpact, the second officer of the NieuwAmsterdam radioed the bridge that the BrightField had stopped moving and wasapproximately 50 meters from the stern of theNieuw Amsterdam. He said later he recalledseeing tugboats arrive within moments to keepthe Bright Field stable against the wharf. Hesaid he reported to the bridge by radio that theBright Field no longer posed a danger to theNieuw Amsterdam, after which he returned tothe bridge. Upon receiving the radio call, thethird officer and the master assessed thesituation and returned the ship to its normaloperations.
At the Safety Board’s request, the master ofthe Nieuw Amsterdam distributed aquestionnaire among the ship’s passengers.While the actual number of passengers whoreceived the questionnaire is unknown, 137 ofthem responded. Their responses are the sourceof the information that follows.
Numerous passengers who were on theNieuw Amsterdam at the time of the accidentobserved the Bright Field as it passed by theship before hitting the wharf. These passengerswere on the Lido deck, port side. They said theyheard the vessel’s whistle, then noticed itsdirection and speed. As the Bright Field passedthe Nieuw Amsterdam, most of the passengersran aft on the Lido deck, observed the BrightField strike the wharf, and watched theemergency responders arrive.
Several passengers were on the NieuwAmsterdam gangway at the time the BrightField was approaching the Poydras Street wharf.One couple first noticed the Bright Field as itpassed under the bridge because it wasrepeatedly sounding its whistle, and theybecame aware that the vessel was experiencingproblems because of the angle of its approach.When they and other passengers were abouthalfway up the gangway, ship personnelinstructed them to turn around, exit the

27
gangway, and return to the terminal. After theBright Field struck the wharf, cruise terminalemployees instructed them to go into theterminal for their own safety.
Another couple was on the dock when theyheard the Bright Field’s whistle, but they didnot understand its significance. They observedharbor police scooters driving past them withlights and sirens on. After the accident, cruiseterminal employees directed them to return tothe terminal, where they remained until theyboarded the Nieuw Amsterdam about 1/2 hourlater.
Other passengers were in the port terminalwhen the Bright Field struck the wharf. Theywere instructed to remain against the far side ofthe terminal and became aware of an emergencywhen they heard the Bright Field’s whistles,observed harbor police officers moving towardthe wharf, and saw people begin “streaming” outof the Riverwalk Marketplace. Although mostresponding passengers recalled that emergencyresponders arrived quickly, others recalled thatsome time elapsed before emergency personnelarrived.
Queen of New Orleans -- The first mate onthe Queen of New Orleans (figure 12) stated thathe was monitoring channel 67 when he heardthe call from the Bright Field pilot to theGovernor Nicholls Light operator. He said heimmediately notified the master, who was on theaft portion of the main deck. The master statedthat, when he approached the stairs to thepilothouse (on the main deck forward), he notedthe Bright Field’s location and speed. He radi-oed the first mate and instructed him toimmediately inform the deckhands to preparethe gangway for evacuation. The master saidthat, as he continued up the stairs to the pilot-house, he observed that the Bright Field washeading directly toward the Poydras Streetwharf. He said he radioed the mate to begin theemergency announcements over the loudspeak-ers. According to representatives of the vessel’sowners, the first mate initiated the first emer-gency evacuation announcements at 1410:48.The master, entering the pilothouse at the end ofthe first emergency announcements, rang thegeneral alarm bell at 1411:22. The first matemade several more emergency evacuationannouncements, after which the master in-
structed him to radio security and have them call911. The master then told the mate to instructthe chief engineer to prepare the engines forgetting underway, after which the chief engineerstarted the engines.
The ship’s director of security andsurveillance said that he was on the second deckwhen he heard the announcement instructing thepassengers to leave the vessel by the gangway.While moving toward the bow of the vessel, hebegan instructing gaming personnel to leave thevessel after the passengers. He said that at thebow of the second deck, he was blocked by acrowd of passengers trying to evacuate over thegangway. He said he looked out toward thewharf and saw the Bright Field headed towardhis vessel. He said he immediately went out aside door, then went around the crowd andbegan to distribute life jackets and help thepassengers off the vessel. He stated that it wasnot normally his responsibility during anemergency to distribute the life jackets;however, most of the team leaders, who wereresponsible for distributing life jackets, wereassisting passengers in exiting the gangway orwere caught behind the crowd trying to evacuatethe vessel. In addition, the team leaders werehaving difficulty reaching the life jackets at thegangway because of the crowd. Duringemergency drills, the passengers were usuallydivided into different “refuge areas” and werenot all in the gangway area at the same time.
A nonoperating crewmember recalledhearing the announcement to evacuate. As sheand the passengers evacuated from all threedecks, they merged together on the second deck,where the gangway was located. She said thatshe did not hear any announcements regardinglife jackets. The master said that he had notmade such an announcement because the vesselwas not scheduled to cruise that day. Theemployee said that she saw the deckhandsobtaining life jackets, but that many passengerswere not wearing them because they wererunning, and the deckhands were telling them tokeep moving. The crewmember said she didrecall hearing a horn blowing a few times, butshe said she heard this all the time on the river.She recalled that “everyone was in a panic”because they did not know what was going onuntil they went outside and saw the Bright Fieldheading toward their vessel.
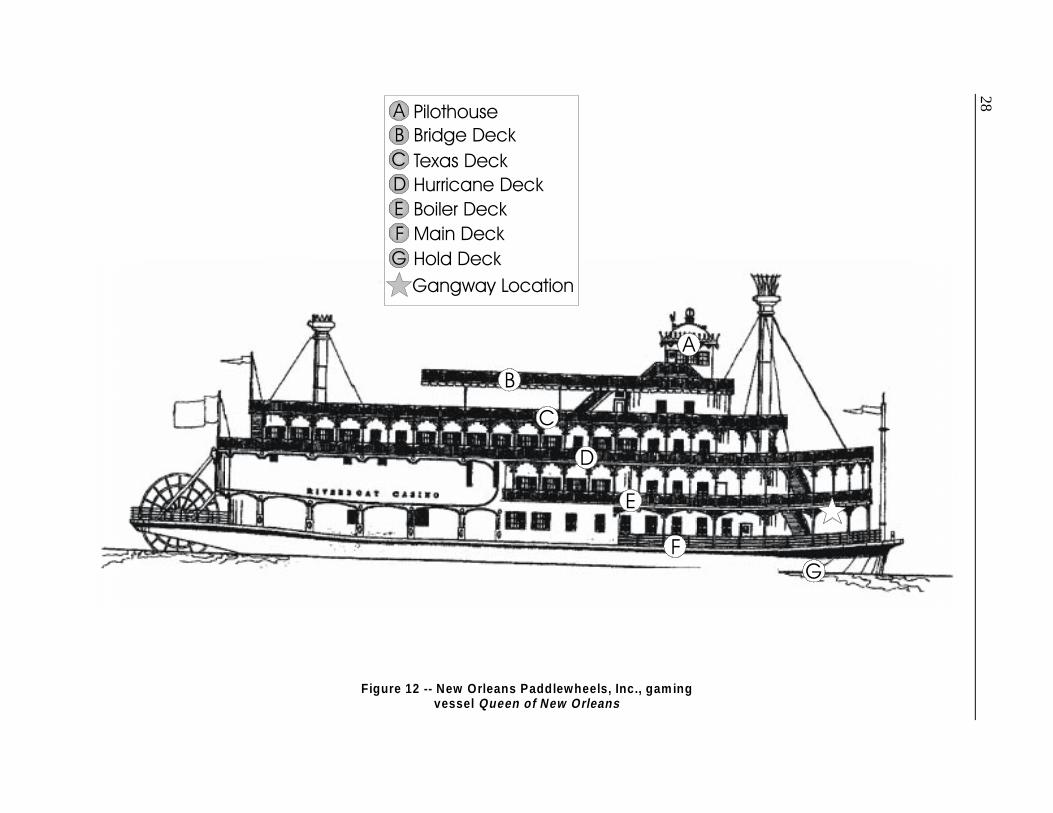
28
Figure 12 -- New Orleans Paddlewheels, Inc., gam ing vessel Queen of New Orleans
$
*)('
%&
3LORWKRXVH%ULGJH#'HFN7H[DV#'HFN+XUULFDQH#'HFN%RLOHU#'HFN0DLQ#'HFN
*DQJZD\#/RFDWLRQ+ROG#'HFN
*)
(
'
%
&
$

29
Another employee, who was on the stern ofthe second deck, recalled hearing the evacuationannouncement, after which he began instructingpassengers to proceed to the gangway. As hebegan moving forward, he said he heard thewhistle from the Bright Field. He recalledhelping one wheelchair-bound passenger out ofthe casino area, over the gangway, and to theelevators of the hotel. He said he then returnedto help clear the casino floor of passengers andmoved to the bow of the vessel, where he begandistributing life jackets to passengers andassisting those passengers who were panicking.
The only means of egress from the Queen ofNew Orleans during the evacuation was a singlegangway from the second deck to a stairway andelevator structure of the Hilton Hotel and thewharf. When the Bright Field struck the wharf,the vessel’s bow wave caused the Queen of NewOrleans to rise 4 to 6 feet. A deckhand calledthe pilothouse and informed the first mate thatthe gangway was “bouncing,” or rising up anddown, approximately 2 feet. According totestimony of the master, the gangway plateswere “jumping” up and down for about 10seconds. The master instructed the first mate,who ordered the deckhands to stop theevacuation. After about 10 to 15 seconds of“bouncing,” the gangway stabilized again. Theevacuation resumed until the gangway againbegan to bounce. The master again instructedthe deckhands to stop the evacuation, raise thegangway, and report to their mooring stations.
Upon hearing this announcement, thesecurity director, who said he was not sure whata mooring station was, assumed the instructionswere for the operating crew. He said he and afew other crewmembers instructed thepassengers to “get back” and “run to the back ofthe boat.” When the crowd became aware thatthe Bright Field was heading toward the Queenof New Orleans, people began to run toward thestern of the vessel.
Following this call, the first mate went tothe bow of the second deck to assist the crew,who had not yet raised the gangway because ithad “restabilized again.” Crewmemberscontinued the evacuation from the gangway atthis time. The mate observed a steady flow ofpassengers evacuating the gangway, whichagain began “bouncing.” At this point, the
gangway was rising approximately 1 to 2 feetabove its normal position. The mate stopped theevacuation again by stepping in front of thepassengers and physically blocking their pathfrom the vessel. After several seconds thegangway again settled, and the evacuationresumed. At this point, the Bright Field hadstopped moving down the wharf, coming to restabout 70 feet from the bow of the Queen of NewOrleans. According to the master, between 70and 80 percent of the passengers had beenevacuated. According to New OrleansPaddlewheels, security videotapes from theQueen of New Orleans showed that about 90percent of the passengers had been evacuatedwhen the Bright Field stopped moving, about 70feet from the bow of the Queen of New Orleans.
Once all the passengers had left the vessel,the master instructed several deckhands to go tothe dock and assist in crowd control andemergency response. Vessel security instructedthe remaining gaming personnel to exit thevessel, and only operating crew remainedonboard. At the same time, the first mateinstructed some deckhands to prepare thelifeboats to launch. Deckhands were alsoinstructed to conduct a search of the vessel toverify that all the passengers had beenevacuated. Another deckhand was instructed tosearch the river for any signs of a personoverboard. Three gaming and security personnelwere sent to the front of the hotel to direct theemergency responders.
Meanwhile, the master radioed the 24-hourmedic and sent him to the dock to providemedical assistance to the injured. A medic,contracted from a local ambulance service, wasaboard the Queen of New Orleans at all times toprovide medical assistance to passengers andcrew. The master called 911, and then instructedthe first mate to send several deckhands to theCreole Queen to offer assistance.
Questionnaires were sent to 74 persons whohad been either in or near the RiverwalkMarketplace when the accident occurred or whowere among the passengers and crew of theQueen of New Orleans or Creole Queen at thetime of the allision.34 A total of 12 responses
34Injury reports were the only available sources foridentifying individuals who may have been on board the

30
were received from individuals who said theyhad been aboard the Queen of New Orleanswhen the Bright Field struck the wharf. All ofthem said they had boarded the vessel between1300 and 1400. Nine of the passengers did notrecall receiving any information concerningwhat to do in the event of an emergency and didnot recall observing any safety informationplacards when they boarded the vessel. Seven ofthese passengers did not receive a life jacketwhen evacuating the vessel. Each of thesepassengers recalled first learning about theemergency when they heard the announcementfrom the first mate over the public addresssystem.
Almost all of the injuries (generally limitedto fractures, abrasions, contusions, lacerations,and back or cervical strains) occurred when thepassengers were pushed, shoved, or trampledduring the evacuation. One passenger recalledthat the crowd was “out of control, stampedinglike wild animals, pushing, shoving, andscreaming.” Another passenger said she sawpeople running and yelling, trying to get out bythe stairwell. “I even saw one man take offrunning and jump, trying to walk on people’sshoulders to get out,” she said. She said that“getting to or out of an exit to land wasimpossible,” and that she was not aware of analternate escape route from the vessel.
Another passenger believed she would neverbe able to get to the dock and decided to moveto the stern of the vessel and “pray for the best.”As she began to move aft on the starboard sideof the vessel, she said, she heard a man on thedock yelling for her to jump. She replied thatshe could not jump; however, when she turnedand saw the Bright Field still heading in thedirection of her ship, she climbed over the railand jumped to the wharf. She sustained pelvicand lower back fractures and was hospitalizedfor 6 days.
Queen of New Orleans or the Creole Queen at the time ofthe accident or who may have been inside or near theRiverwalk Marketplace when the Bright Field struck.Crewmembers of the two ships were identified throughcompany documents. Other than crewmembers, the onlyindividuals who received Safety Board questionnaires werethose who had reported being injured during or subsequentto the accident sequence.
Several passengers commented that thevessel crew also seemed to panic and did notappear to be trained for an emergency of thistype. One passenger said she observed some ofthe crew running to get off the vessel along withthe passengers. She said she perceived that therewas “no order and no one seemed in charge”during the evacuation.
According to New Orleans Paddlewheels,Inc., the comments of these passengers do notcorrespond to the surveillance videotapeshowing the evacuation. Company officials saidthe passengers may have seen somecrewmembers leaving the vessel during theevacuation, along with the passengers; however,these were the crewmembers who were notassigned to assist in the evacuation. Thecompany said crewmembers with evacuationresponsibilities remained aboard the Queen ofNew Orleans and provided assistancethroughout the evacuation. The company saidthat its security videotape “clearly showspassengers responding to announcementsimmediately, orderly, and no one running.” TheSafety Board has reviewed the tape and did notobserve, in the locations of the vessel shown,any of the passengers falling or being“trampled” or knocked down. The videotapesappear to show passengers exiting the vessel inan orderly manner without apparent panic.
Creole Queen -- The master of the CreoleQueen was monitoring two handheld radios, acompany radio with two channels and anotherradio tuned to VHF channel 67. The main radioin the wheelhouse also monitored channel 67.The master stated that, at approximately 1400,he instructed the deckhands to remove the linesfor the vessel’s second cruise. As the deckhandslet go of the lines and the master began usingthe bow thruster to move the vessel away fromthe dock, he heard the call from the Bright Fieldpilot to the Governor Nicholls Light operator.
As the master began to maneuver the vesselback to the dock, he radioed his first mate andinstructed him to go starboard on the main deck,look upriver, and report his observations. Thefirst mate reported back, “he’s headed straightfor the Riverwalk.” The master instructed thefirst mate to “put the gangway down and beginan evacuation.”

31
The first mate and a deckhand had gone tothe gate on the deck of the Creole Queen toopen it for the gangway. The first mate climbedashore and began to lower the gangway whileother deckhands tied up the vessel. Once thevessel was secure, the gangway was positionedfor the passengers to begin evacuating. The firstmate said he positioned himself on the dock sideof the gangway as the deckhands, on the vesselside of the gangway, helped the passengersevacuate.
At this time, the master began makingemergency evacuation announcements to thepassengers. He recalled announcing,
Ladies and gentlemen, this is thecaptain. Please exit the boat using thegangway. Please do not panic. Pleaseexit the boat using the same entrance aswhen you boarded. This is anemergency. Please exit immediately.
The passengers began evacuating, and themaster rang the general alarm bell. Meanwhile,the master could hear the Bright Field’s whistlegetting closer, but his view of the vessel wasobstructed by the Queen of New Orleans.
The first mate observed that the BrightField’s bow wave caused the Queen of NewOrleans to rise up “as if it were out on the oceanand hit by a wave.” He said he called to thedeckhands to stop the evacuation of thepassengers. The master said he used the publicaddress system to caution the passengers to“watch the gangway.” The master estimated thatat that time half of the passengers had evacuatedthe Creole Queen and were waiting on the dock.The bow wave and undertow from the BrightField pulled the Creole Queen away from thedock, and the gangway began to slip aft alongthe deck. The deckhands stopped theevacuation; however, three passengers were stillon the gangway at the time. As the boat rose up,it “was sucked out” away from the wharf, andthe gangway dropped off the Creole Queen anddown toward the water. The three passengers onthe gangway fell into the river between the shipand the wharf.
The deckhand and some passengers whowere on the dock began to crank up andreposition the gangway so that the evacuation
could be continued. Meanwhile, a passenger onthe main deck threw a life buoy and a child-sizelife jacket to the three passengers in the water.The first mate, from the dock, told the passengerwhere to find an adult life jacket, and thepassenger then threw an adult jacket into thewater. The first mate then instructed acrewmember on board to retrieve the ladderfrom the rescue boat on board and to place itover the side of the Creole Queen. Two of thepassengers in the water climbed the ladder andentered the vessel. The third passenger, a 61-year-old man, suffered a hip injury when he fellinto the water, and he was unable to climb overthe railing and into the vessel. The first mateclimbed onto the vessel from the dock andassisted the crewmember in easing the passengerinto a Stokes Basket. They then pushed thebasket from the vessel over to the dock. Whilethis was underway, the master was attempting toreposition the vessel to the fallen gangway. Ashe was maneuvering the vessel, he continued tomake emergency announcements to thepassengers until the gangway was re-positionedand the evacuation could be resumed.
Once the evacuation was complete, themaster requested, via the company radio to theQueen of New Orleans’s first mate, that the 24-hour medic be dispatched to assist some of theinjured Creole Queen passengers. The mate onthe Queen of New Orleans told him that themedic was already assisting the injured from theQueen of New Orleans. The master later told theSafety Board that one of the problems heencountered during the accident was the lengthof time it took for emergency medicaltechnicians to arrive on scene. He recalled thatafter he made this complaint to another personafter the accident, he was informed that thedelay in ambulances responding to the dockwhere the Creole Queen was moored was due todamage done by the Bright Field to the normalemergency response access route to the wharf.
Three respondents to the Safety Boardquestionnaire were individuals who said theyhad been on the Creole Queen at the time of theaccident.35 One passenger recalled boarding the
35Questionnaires were sent only to the three CreoleQueen passengers who had reported being injured in theaccident. All three individuals responded.

32
vessel at 1310 and receiving informationconcerning emergency procedures. He statedthat, about 1315, the first mate announced that,if the passengers were required to immediatelyevacuate the vessel, they should follow theinstructions announced over the public addresssystem. This passenger considered thoseinstructions of great value because theevacuation was not a typical situation; itinvolved little time to don life preservers, formgroups, or disembark to the pier or lifeboats. Heobserved placards posted on the salon andobservation decks that provided emergencyinformation regarding the location of life jacketsand the procedures for donning them.
A couple, a 61-year-old man and 59-year-old woman, both sustained injuries when theyfell into the water when the gangway collapsed.They said they boarded the Creole Queen about1350, and they did not recall receiving anyinformation about what to do in the event of anemergency, nor did they observe any placardsthat provided this information. The femalepassenger recalled the master announcing theywere returning to the dock to disembark, and themale passenger recalled six to eight repeatedcalls for “abandon ship.” They observed peopleon the Riverwalk running toward the SpanishPlaza. The male passenger recalled thatpassengers were confused when they heard“abandon ship”; they were unsure whether tojump into the water or remain on board, and thecrew was shouting, “get the life preservers,where are the life preservers?” He recalled thatit seemed “like a continuous shouting match”while the crew was attempting to find lifejackets and the three passengers remained in thewater.
Riverwalk Marketplace -- In a letter to theSafety Board, a couple said they were in a caféon the second level of the marketplace whenthey heard the Bright Field’s whistles. Thehusband got up from the table and went to thewindow to see what was happening on the river.When he had almost reached the window, theBright Field struck the wharf, then brokethrough the window of the cafe. Patrons seatednear the window “ran screaming and runningout of the café.” The man and his wife said theyheard a waitress yelling “get out” twice as theyran to the restaurant doors. They turned aroundand watched the ceiling and floor above crash
down and fold over the entire room, as theBright Field continued to crash through the cafe.They immediately left the area to evacuate themall.
As they attempted to go up to another level,“the only route out of the mall [away from thedirection of the river],” they ran into a“bottleneck,” a large crowd attempting to usethe escalators to reach the higher floors toevacuate. As they were climbing up the “down”escalator, they said, they feared a gas explosionbecause they smelled gas. When they made it upto another mall level, many mall customers onthe upper floors were still shopping, unaware ofthe accident. At this time, the couple noticedthat they had not yet heard any alarms or publicaddress announcements, even though it had beenseveral minutes since the vessel struck the cafe.They encountered security guards who did notallow them to use emergency exits to evacuate.They said they believed they were “strictly onour own. The mall management apparently hadmade no disaster plans for its merchants andcustomers; if such plans existed, they were acomplete failure.”
The Safety Board received responses from15 individuals who said they were either patronsor employees of the Riverwalk Marketplacewhen the accident occurred. One patron recalledthat she was on the first level of the RiverwalkMarketplace, alongside the wharf, when sheheard the Bright Field’s whistle sounding. Shebelieved that the noise was “normal river noise”and did not take notice. She then heard peoplebegin screaming “run,” and “get out.” She saidshe turned around and saw the Bright Fieldcoming into the wharf area. She said that, whenshe turned to run out of the store, she wasknocked down by the crowd. She tried severaltimes to get up, and was repeatedly knockeddown. After the wharf was struck, a securityguard came to assist her, and he helped her outof the store and over to a triage area. She wastaken to the hospital and admitted for bluntabdominal trauma.
A family was shopping in a mall grocerystore at the time of the accident. They said theyheard the Bright Field’s whistles but did notknow the whistles were a warning signal. Theythought that a vessel was arriving, so they wentto the glass window on the wharf to watch the

33
Bright Field approaching the dock. They saidthey did not know that they were in danger untilthey realized the vessel was not docking but wasactually striking the wharf. They said the storeclerk did not appear to be aware of what theship’s warning whistles meant and did not knowthat the store should be evacuated.
As the vessel struck the wharf, the familyturned to flee the store. As the customers wererunning, the store was collapsing behind themand the roof began falling in. As the collapsingwalls shifted furniture, the doorway becameblocked, and they could not escape until thefalling ceiling shattered the front glass displaywindow. When they attempted to leave the mall,by going up to the third floor, they could not goup the escalators because there were too manypeople exiting the same way. One of the familymembers hit the stop button on the “down”escalator, and they went up to the third floor viathat escalator. They said that when they left thefront of the Riverwalk Marketplace, they werenot given instructions on which way to evacuate.Not until they were leaving the marketplace didthey see a police officer, and they did notobserve any other emergency responders.Overall, the family recalled that there appearedto be a lack of preparedness for an emergencyevacuation and that crowding was a problem infinding an exit away from the damaged wharf.
Another couple was in a restaurant on thewharf when they saw other people screamingand running out of the mall. They did not hearan emergency whistle from the Bright Field orgeneral mall emergency announcements; theydid hear a fire alarm ringing after the BrightField struck the mall shops. The couple wereinjured when they were knocked down and“trampled” by shoppers who were fleeing themall. The couple recalled the activities of themall personnel relating to visitor safety as“poor,” both during and after the accident. Theyrecalled that the police and Coast Guard arrivedimmediately, and that the fire departmentarrived about 10 minutes later.
Riverwalk Marketplace has providedvideotapes to the Safety Board which companyofficials say “show the mall being evacuatedwithin a matter of minutes with virtually nosignificant personal injuries suffered by any of
the persons evacuated.” The Safety Boardviewed the tapes, which showed variouslocations in the mall during the allisionsequence. The tapes were recorded by securitycameras using a loop system that recordedframes from all camera locations on a singletape. Continuous footage from a single locationwas not available, and the frames from the tapeloop were made at intervals of about 4 seconds.These videotapes do not appear to show patronsbeing “trampled” or knocked down during theevacuation.
In addition to providing videotapes to theSafety Board, Riverwalk Marketplace also hasstated that public safety officers did blockcertain emergency exits in accordance withprotocol and the evacuation plans andprocedures. “To allow individuals to exit freelyfrom any exit they chose might have placedthem in greater peril,” the company said. As forthe smell of gas reported by the patrons, thecompany said that a member of the Marketplaceengineering department was on the wharf justprior to the accident, saw that the allision wasinevitable, and immediately shut off all utilityservice to the mall, including natural gas, toprevent an explosion. The company said thatfire alarms did not sound prior to the allisionbecause of the absence of any alert or warningprior to impact. The security central monitoringstation printouts showed the fire alarmssounding at 1411:42 and 1414:11.
Hilton Riverside Hotel -- When the BrightField struck the Hilton Riverside Hotel, thepublic safety dispatcher received several 52 F(fire) activation alarms, and housekeepingcalled to inform the dispatcher that a vessel hadstruck the riverside hotel. The dispatchernotified the local fire and police agencies andcalled the Director and Assistant Director ofPublic Safety and Security. The hotelEmergency Disaster Procedures Plan was putinto effect and the hotel emergency responseteam was notified. The security supervisor onduty received a call that a possible fireemergency had occurred in the riverboat casino;when he arrived in the hotel lobby, he“discovered that a panic crowd was runningaway from the area.” He instructed officers tocalm the crowd down and clear the lobby. Heattempted to use the radio to communicate withother officers, but when the vessel struck the

34
building, it knocked out the power and,therefore, communication capabilities. So heinstructed the officers in the lobby to assist himin evacuating guests from the riverside building.
Meanwhile, a security officer who wasreturning to his post from lunch was in theRiverwalk parking lot when he was met by alarge crowd that informed him that a freighterhad hit the Riverwalk and many people by thestairs in the rear lot were injured. He ran to thelocation and observed people “falling down thestairs and bleeding.” He attempted to stop thepeople from running but to no avail. He found aperson with a cellular phone and called 911 toreport the emergency. He then assisted theinjured until the emergency medical servicesarrived. He was then assigned to assist withtraffic control.
Another security officer, who was in frontof the hotel, heard a call from another officerthat a possible fire emergency had occurred onthe riverboat casino. He ran, along with otherofficers, to the area and observed that a largeship with heavy damage to the front section was“docked” near the casino riverboat and that asection of the Riverwalk mall and the hotel hadcollapsed. They attempted to radio the securitysupervisor on duty, but all communications hadbeen lost due to a power failure in the riversidehotel building. So, the officers proceeded to thedamaged area of the hotel to evacuate everyonefrom the building. They encountered theemergency response team on the fifth floor asthey were responding to a report of a trappedfemale guest.
This emergency response team consisted ofthe security, maintenance, and engineeringdepartments. When the Bright Field struck thehotel, the maintenance person on duty washeaded to the first floor when the building beganto shake violently. The engineering supervisorwas in the carpenter shop when he was notifiedby the dispatcher that a vessel had struck thebuilding. He, the housekeeping supervisor, andthe maintenance person on duty, along withhotel security officers, conducted a floor-by-floor search of the hotel. A housekeeperinformed them that a female guest was trappedin her room. They attempted to open the frontdoor to the room; however, it was blocked bycollapsed ceiling damage from the freighter’s
allision. They had to use a claw hammer tobreak in the hallway wall to reach the guest. Theteam was able to open a large hole in the wall ofthe fifth floor, and the trapped guest wasevacuated from her room by 1425. According tothe emergency response team, the guest statedthat “there was no one else in room 5085 andthat she did not think that she was injured.”Meanwhile, other members of the emergencyresponse team completed the evacuation searchby 1418, when the New Orleans Fire and PoliceDepartments arrived at the hotel. Anotherintensive search of the hotel was conducted byseparate groups of local response agencies andthe hotel emergency response team.
At 1435, the Director of Security arrived atthe hotel, and set up a command post with thefire, police, and harbor police inside of Kabby’srestaurant. A printout of the occupied guestsuites was delivered, and all departmentsverified the number and locations of theiremployees. Once this information was collected,a third search of the building was conducted. Noother guests were found trapped in their rooms.According to Hilton Riverside Hotel, noemployees of the hotel were injured during theBright Field allision. The riverside building wascompletely evacuated. The engineeringdepartment had notified the security directorthat the team secured all utility lines, includinggas and electrical lines, and placed the buildingon the back-up generator; power andcommunications were restored once thisgenerator was hooked up to the repeater.
Emergency ResponsePort of New Orleans Harbor Police --
Harbor police officers were the first responderson scene. They initiated rescue effortsimmediately, ordered emergency units, andbroadcast a description of the incident via policeradio. The harbor police were responsible forimmediate scene stabilization, traffic control,pedestrian control, and support for the NewOrleans Fire Department. A triage center wasestablished at a Riverwalk Marketplace securitypost, and emergency medical services units werestaged near the rear apron roadway. TheMedical Center of Louisiana’s Charity andUniversity campuses were notified of theincident and designated as the primary treatmentfacilities. The director of public safety and

35
security for the Port of New Orleans authorizedthe request for additional enforcement andrescue assistance from several surroundingparish police and sheriff’s departments and fromthe Louisiana State police. For the first 48 hoursafter the accident, all available harbor policeofficers and six recruits were called in toprovide security in both interior and perimeterareas of the Poydras, Julia, and Canal Streetwharf area.
Coast Guard Group New Orleans -- Theon-duty officer at Coast Guard MSO NewOrleans was notified of the accident at 1420 bythe Gretna traffic light operator. The initialreport indicated possible persons in the waterand significant damage to the Bright Field andPoydras Street wharf buildings, resulting inother casualties. At 1421, the MSO on-dutyofficer designated Coast Guard Group NewOrleans as the search and rescue missioncoordinator. Group New Orleans requested animmediate search and rescue responsedetachment from Coast Guard Station NewOrleans to search for possible persons in thewater.
At 1422, the Mississippi River was closed atmile 96 AHP in the vicinity of the accident. At1430, a Coast Guard helicopter was dispatchedby the search and rescue coordinator to pick upa rescue swimmer and report to the scene of theaccident. The MSO on-duty officer notified boththe captain of the port (COTP) and the chief ofport operations of the accident. At 1435, theMSO notified the office of the commander ofthe Eighth Coast Guard District.
The MSO chief of port operationsimmediately went to the scene. After consultingwith the incident commander, he assessed thedamage and began searching for leaking fuel orother dangerous conditions. He observed thatthe ship was not secured to the wharf, and hedirected crewmembers and firefighters to attachbow mooring lines.
At 1445, the MSO emergency responseteam arrived and boarded the vessel, and theCoast Guard on-duty officer also dispatched fireand hazardous materials teams to the scene. At1447, the helicopter was on scene and searchingthe river for persons in the water. At 1550, twoCoast Guard infrared search teams were
dispatched to help search for persons in thedebris of the collapsed Poydras Street wharf. At1750, the Coast Guard received an update thatno fatalities had been confirmed and that 100injuries had been reported. All search andrescue activities were terminated at 1000 onDecember 16, 1996.
Louisiana Office of EmergencyPreparedness -- About 1500, the LouisianaOffice of Emergency Preparedness responded tothe Bright Field accident, dispatching theassistant director and the chief of operations tothe scene to offer State support and assistance.At approximately 1630, a request was made forlight sets for possible night operations. TheLouisiana Army National Guard provided lightslater that evening.
Police Departments -- The New OrleansPolice Department assisted the harbor police instabilizing the scene, controlling traffic andpedestrians, and supporting the New OrleansFire Department in this accident. The initial callwas received at 1414 to assist the Harbor PoliceDepartment with “unknown trouble...largecrowd of people running inside...possiblebuilding cave in.”
New Orleans Fire Department -- Theinitial call to the fire department dispatcher wasreceived at 1413. The initial response was afirst-alarm response. When the incidentescalated into a three-alarm response, more than40 units and 110 people responded. The firedepartment established an incident commandsystem to oversee operations, evacuate theaffected areas, remove the injured persons,triage and treat the injured, search for andrescue trapped persons, control natural gas leaksand utilities, and make arrangements forperimeter security through the New OrleansPolice Department, the Coast Guard, and thePort of New Orleans Harbor Police.
New Orleans Department of Health andEmergency Medical Services -- The NewOrleans Health Department, EmergencyMedical Services Division, assessed injuries,treated and transported the injured to localhospitals, and coordinated additional treatmentand transportation with area private providers.The initial call was received at 1414 by theLevee Board police dispatcher, and the first

36
emergency medical services responder arrivedon scene at 1417.
Emergency PreparednessRiverwalk Marketplace -- According to
Riverwalk Marketplace figures, approximately13,500 persons visit the mall daily. TheRiverwalk Marketplace had a mallemergency/catastrophe plan in place thatincluded emergency procedures and mapsindicating the locations of sprinkler systems andzones, fire extinguishers and standpipes, smokedetectors, chemical and hazardous materialsstorage, main entrance feeders and disconnects,gas shutdowns, water mains, and primary andsecondary emergency exits. Each emergencyexit from the Riverwalk Marketplace wasmarked by a lighted sign with the words“Emergency Exit” in white letters on a redbackground.
The emergency procedures instructed mallemployees to first call the local fire departmentin the event of an emergency, and then followup with calls to the management office. Acommand post, if necessary, was to bedesignated, and the emergency manager was todetermine, along with fire department officials,whether to evacuate the mall.
The “Emergency Organization Guidelines”in the Mall Security Plan manual listedprocedures for security officers on duty at thetime of an emergency. This manual provided aseparate emergency evacuation plan for eachlevel of the marketplace and specified duties andresponsibilities for security officers, dispatchers,and public safety supervisors during anemergency evacuation.
In documents provided to the Safety Boardon November 13, 1997, the RiverwalkMarketplace stated that the Riverwalk policy“is, and always has been,” that the seniormanager on duty at the time of any event isresponsible for determining whether to evacuatethe mall, or certain portions of the mall. In theabsence of the management, the senior securitysupervisor on duty has the authority to call foran evacuation of all or part of the mall,depending on the circumstances. The decision toevacuate is based upon an evaluation of thesafety threat posed to patrons and employees in
the mall. The company said that, once thedecision to evacuate is made, evacuation iscommenced prior to the arrival of firefighters orpolice on the scene. Notification of the fire orpolice departments, as necessary, is madeinstantaneously and coincidentally with thedecision to evacuate the mall.
The company said that, for an emergencyinvolving a vessel striking the wharf, specificemergency instructions were based on theseverity of the allision. Immediate procedureswere to contact the harbor police, identify thedamage to the wharf as major or minor,immediately report the accident to a supervisor,determine if city services were needed, andbegin safety measures.
New Orleans Hilton Riverside Hotel -- Theemployee manual of the New Orleans HiltonRiverside Hotel details the procedures to befollowed during a fire or other emergency.Included in the manual are the duties andresponsibilities of the hotel emergency responseteam; the hotel management; the securitydepartment; and the engineering, front desk,bellstaff, catering, and housekeeping personnel.
The emergency directions includenotification of the fire department,establishment of a command center, detailing ofevacuation procedures, and notification ofHilton Hotel headquarters management. Sampleemergency announcement messages areprovided, as are crisis communicationguidelines for on-duty management personnel.
The decision whether to evacuate the hotelis to be made by the senior manager on dutyprior to the arrival of fire or police officials. Thedecision is to be based on the threat of injury tohotel guests and employees, the extent of theemergency, and the need to remain in control ofthe evacuation while fire or police officialsassess the emergency. The New Orleans HiltonRiverside Hotel did not have a section in theemergency procedures or evacuation planmanual that covered a vessel striking the wharf.
Queen of New Orleans -- The Queen ofNew Orleans Emergency EvacuationProcedures in Moored Conditions manualprovided instructions for evacuation routes,including alternates, in the event of an

37
emergency. Each deck had a different escaperoute for a specific number of passengers, basedon the number of persons permitted on that deckand the space available for the exits. All primaryand alternate deck exit routes led to thegangway located at the bow of the second deck.This 12-foot-wide gangway led to a stairwayand elevator structure, then into the NewOrleans Hilton Riverside Hotel, or down to thewharf. The master stated that the time wasinsufficient during the Bright Field accident touse the procedures outlined in the manual.
The Safety and Vessel Operation Manualfor the Queen of New Orleans provided safetyinformation for the operating crew and otherpersonnel working on the vessel. It includeddetails concerning the evacuation of the vessel,a description of the sounding of the alarm bells,and an explanation of each alarm. It alsodescribed the responsibilities of eachcrewmember and specified the refuge area,muster area, and designated team leader for eachposition. According to the manual, thenonoperating crew were responsible formustering passengers, warning passengers,directing them to refuge areas, assisting themwith life jackets, keeping order in the stairwaysand passageways, and generally controlling themovement of passengers and maintaining theirsafety.
Safety Briefings -- Based on companydocuments and the master’s statements, theQueen of New Orleans broadcast a vessel safetyvideotape on two 27-inch television monitors inthe Hilton Hotel lobby and on one 27-inchmonitor on the boarding structure ramp. Themonitors in the hotel lobby were positioned justbelow the ceiling on the wall adjoining the wallthrough which a door led to the boarding ramp.The monitor screens were visible to personspassing through the door to the ramp if theylooked up and to the right. The boarding rampmonitor was centered overhead at a point abouthalfway up the ramp. The safety videotapeplayed continuously on the monitors anddemonstrated the donning of a life jacket andthe dangers of the river.
Before each cruise, a safety announcementinformed the passengers of the appearance andlocations of the boxes containing life jackets.According to the master, an oral announcement
about life jackets was not made prior to theBright Field accident because the vessel was notscheduled to leave the dock. He stated that thevessel is “an extension of the dock when we’renot underway.”
In responding to Safety Boardquestionnaires, a number of passengers on boardthe Queen of New Orleans on the day of theaccident, some of whom had been on the vesselseveral times before, did not recall ever havingnoticed the video monitors.
Signage -- The Queen of New Orleans hademergency, safety, and life jacket signs postedin various locations throughout the vessel.According to the master’s testimony, the vesselhad overhead signage, including lightedoverhead exit signs at every exit door, directingpassengers to the exits of the vessel. The masterstated that he did not recall any signage near thefloor at designated exits that provided exitinstructions. He said signs were postedthroughout the vessel advising passengers whichlevel they were on and how to get to otherlevels.
The information placards were covered withthin, clear laminate and attached to the light-colored bulkheads. An emergency evacuationplacard and casino station bill were posted onthe first and second decks, and three station billsand an emergency evacuation placard wereposted on the hold deck. Life jacket placardswere found on the inside of the cover of all lifejacket boxes. The placards displayedinstructions for donning life jackets, along witha photo displaying a properly donned life jacket.An emergency evacuation placard and stationbill were posted on the fourth deck; a station billand emergency evacuation placards were postedon the third deck. According to 46 CFR 199.80(8)(c), vessel emergency instructions “must beposted in each passenger cabin and in spacesoccupied by persons other than crew, and mustbe conspicuously displayed at each musterstation.”
Emergency Egress -- The Safety and VesselOperation Manual described both “dry” and“wet” evacuations. The wet evacuation involvedputting passengers into the water with lifejackets and other emergency equipment. Dryevacuations involved assisting passengers to

38
embarkation areas where they would disembarkvia an emergency evacuation ramp/slide. Thelocation of this ramp/slide was not shown on thevessel diagram in the manual, and no otherreference to the equipment was made.According to company documents, at the timethe vessel was under construction, the ownersexperimented with the slide, but they were notsatisfied with its safety and performance;therefore, the slide was not incorporated into thevessel design. According to the company, threeportable emergency gangways were maintainedaboard the vessel at all times and were designedto be used in the event the main gangwaybecame inoperable.
Drills -- According to the company, fire drillsfor the Queen of New Orleans operatingcrewmembers were held twice per week, one percrew, with active participation mandatory. Atleast weekly, each marine crew participated inrescue boat drills in which the rescue boat davitand motor were tested and the boat was loweredinto the water. To facilitate documentation andmanagement of the drills, a safety team leaderwas designated for each area of the vessel. Thesafety team leader assisted the master withcoordination and control of the drills. First aidand CPR training were required for all securitysupervisors, mates, masters, engineers, and leaddeckhands.
According to the master, the deckhandsparticipated in fire and emergency drills, and theevacuation drills were incorporated into thesafety and security meetings. Detailed minutesof the safety meetings were not kept, although abrief description was included on special safetyand fire drill forms. During these meetings,deckhands were instructed in the handling of theflow of passengers through the vessel during anemergency. The master stated that thepassengers “have to get out of the casinothemselves or walk out themselves, and then wecan direct them to the exit of the vessel.”Security crew were instructed to assist in theevacuation procedures as well. The master saidthat passengers were not involved in the weeklydrills, so the crew had not practiced physicallymoving passengers.
According to the master, the gaming staffdid not take part in the regularly scheduledevacuation training. Instead, the safety team
leaders participated in the drills. Two safetyteam leaders were assigned on each level of thecasino except on the fourth and first levels,where there were few passengers and where oneteam leader was assigned. The security staff wasinvolved with the safety meetings, as weresupervisory gaming employees. Thesesupervisors were instructed to inform theremaining gaming staff about the content of themeetings. According to the master, no formalprocedure existed for verifying that thisinformation was being relayed to gamingemployees. The master said he had randomlychecked gaming employees to verify that theyknew of the nearest safety equipment, knewwhich exits to use, and knew how to don a lifejacket.
Creole Queen -- The Creole Queenoperations manual covered emergencyevacuations, emergency egress, and firefightingprocedures. The station bill section of themanual required that a life jacket demonstrationbe given before each cruise. The station bill alsoincluded instructions regarding the sounding ofthe vessel’s whistle and ringing of the generalalarm for emergency situations such as fire,abandon ship, man overboard, and dismissalfrom drills. The station bill also included adescription of the duties and responsibilities ofeach crewmember during each of theseemergencies.
Inspections, Tests, and ResearchSeveral days after the accident, Safety
Board investigators boarded a fully loadedvessel that was similar to the Bright Field insize, displacement, and power. During a transitdownriver in high water conditions similar tothose on the day of the accident, the pilot didnot use full speed to maneuver the ship.
Safety Board investigators boarded theBright Field shortly after the accident toexamine shipboard systems. Because the BrightField was still alongside the damaged wharf atthis time and could not be moved, its direct-drive engine could not be started during initialtests and inspections. After conducting a generalsurvey of the engineering plant, Safety Boardinvestigators focused their efforts on theengineering systems most closely associatedwith the ship’s propulsion plant and related

39
control systems. These systems included thesteering gear, the main engine and associatedmain engine auxiliary subsystems, theautomated propulsion control system, and themaintenance and management infrastructure forthe vessel’s engineering plant.
Steering Gear -- The Bright Field’s electro-hydraulic steering gear consisted of a tiller, tworams, four cylinders, two electric hydraulicpumps, and an electro-hydraulic control system.During the investigation, the steering unit wasinspected externally and was operationallytested by timing the rudder movements inaccordance with SOLAS ’74 steeringperformance standards. The Bright Field’ssteering system functioned normally.
Main Engine—General -- Because the mainengine could not be started and run during initialinspections, the initial survey of the condition ofthe engine was based on visual inspection,testimony of crewmembers, and review ofmaintenance and operating documentation.Visual inspection of the main engine revealednothing unusual. The second engineer statedthat the engine’s exhaust gas temperatures ranabnormally high and that, as a result, the crewhad had to replace pistons and cylinder linersseveral times since July 1996. His maintenancerecords confirmed this fact. The repairs to theair turbocharger and air cooler made during thevessel’s New Orleans port call were an effort bythe vessel owners to correct the problem. Theengineering crew stated that the main engineoperated normally during the trip downriver onthe day of the accident; however, a review of theTerasaki alarm printout for the early part of thevoyage indicated that the main engine wasexperiencing cylinder jacket water coolingalarms due to low jacket water cooling pumppressure. The tape also recorded alarmsindicating main engine lubricating oil purifiermalfunction and high second filter pressuredifferential. A more detailed review ofengineering reports, including informationreceived late in the investigation from civillitigation depositions, is contained in appendixB. From at least January 1996, the BrightField’s main engine experienced continuedproblems with component failures.
Main Engine Lubricating Oil Sump --According to engineering drawings, the engine’snormal lubricating oil sump level was 14 cubicmeters (about 3,699 gallons) when oil pumpsand machinery were off. With pumps and allmechanical equipment running, the oil level inthe sump should drop to about 10.3 cubic meters(about 2,721 gallons). The design plansindicated that the low-oil-level alarm should beset to activate at 8.16 cubic meters (about 2,156gallons). With both lubricating oil pumps andother machinery off, the oil level for the BrightField’s main engine lubricating oil sump wasmeasured by Safety Board investigators at 10.75cubic meters (about 2,840 gallons). SafetyBoard investigators examined the main enginesump and found that, with pumps andmechanical equipment running, the Bright Fieldgauge read 8.1 cubic meters (about 2,140gallons). Investigators tested the Bright Fieldlow-oil-level alarm and found that it activated atabout 7.25 cubic meters (about 1,915 gallons).The chief engineer’s log book recorded that,upon the Bright Field’s arrival at New Orleanson November 21, 1996, the main engine oilsump level was 7.5 cubic meters, with theengine running. At about the time of the allisionon December 14, 1996, the Terasaki monitoringsystem recorded a main engine low sump oillevel alarm.
Main Engine Lubricating OilPumps/Motors -- According to testimony of theengineers, both No. 1 and No. 2 (electricallydriven) oil pumps were operating at the time ofthe allision, and they had not been altered in anyway since the accident. The No. 1 oil pump wasnoisy and exhibited a periodic rumbling sound,as if the pump were cavitating.36 Lubricating oiltemperature was approximately 56 °C (about132 °F). Mean discharge pressure was about 2.8bar, however, both suction and discharge gaugeswere oscillating wildly, making it difficult toobtain a reliable reading. When pump No. 2 wasstopped, the system pressure dropped to about2.3 bar. Pump No. 2 was tested and operatedsatisfactorily.
36The pump cavitates when numerous vapor bubblesform in the oil. Subsequent collapsing of the bubbles canproduce a distinctive rumbling sound in a piping system.

40
Investigators opened and examined both oilpump basket strainers and found them intact andclear. The No. 1 oil pump was restarted, but itcontinued to produce only about 2.3 bar. Thepump was examined for possible suction-side airleaks, but all flanges, seals, and joints appearedto be intact. The pump was taken to a marineengineering repair facility for disassembly,inspection, and testing. Other than minor wear,no significant defects were found, and allclearances were within manufacturer’sspecifications. The pump was reassembled andreinstalled in the Bright Field.
During additional testing witnessed bySafety Board investigators about 2 weeks later,the No. 1 oil pump was again examined, started,and found to be running quietly. Suctionpressure was -0.3 bar, and discharge pressurewas about 4 bar by local gauges. The pumppressure relief valve was found to be operatingin accordance with the manufacture’sspecifications. The following day, investigatorsreexamined the oil pumps and found high noiselevels associated with both pumps, including the“cavitation-like” sound. No obvious leaks werefound in the flanges and openings on thesuction-side piping, and both pumps generatedrated (4 bar) pressure. Close inspection of theNo. 2 oil pump discharge stop check valverevealed that the stem was jammed in the valveyoke, and the valve would not manually closeand seat. The “check” feature of the valveappeared to function correctly when subjected toback pressure. Both oil pumps evidencednoticeable vibration and noise for the remainderof the vessel’s stay in New Orleans, and thecause of the abnormal operation could not bedetermined with certainty.
Main Engine Lubricating Oil SystemSecond Filter/Strainer -- The secondfilter/strainer was designed for working pressureof about 4 bar and a working oil temperature of45 °C (about 113 °F). The filter was equippedwith two pressure switches. One switchmonitored differential pressure across the filterand activated an automatic backwash system (toclean the strainer) if the pressure differentialreached a certain level. The other switch wasdesigned to activate an alarm in the event of adifferential pressure drop across the filtergreater than 0.9 bar.
On December 17, 1996, Safety Boardinvestigators recorded second filter/strainer inletand outlet pressures of 3.4 and 2.4 bar,respectively, with the lubricating system stillrunning in the same condition, including an oiltemperature of 56 °C, as at the time of theaccident. A high-differential-pressure alarm didnot sound. Safety Board investigatorsdetermined that the differential pressure alarmhad been set at 1.3 bar.
Safety Board investigators opened andexamined the second filter and found that theinstallation was consistent with designdrawings. No visible debris buildup or blockagewas found. The filter was cleaned, reassembled,and tested with new oil. The differentialpressure was found to be approximately 0.7 bar.The filter manufacturer recommends that thesecond filter/strainer be opened and cleanedevery 6 months. No record was found in thesecond engineer’s maintenance log to indicatethat the filter had been cleaned between lateJuly and December 1996.
Main Engine Lubricating Oil Purifier --The Bright Field third engineer told the SafetyBoard that the lubricating oil purifier wassupposed to run continuously (whether or notthe engine was running), drawing oil from theengine oil sump, removing water and sedimentfrom it by centrifugal action, and then returningthe cleaned oil to the sump. Because the purifierfunctioned with warm oil only, an auxiliaryboiler was needed to heat the oil when theengine was not running. The Bright Field chiefengineer, in a December 9, 1996, letter to thevessel owner, stated that the purifier had notbeen used because the auxiliary boiler had beeninoperative. At some point during the vessel’sstay in New Orleans, and prior to the accident,the auxiliary boiler was repaired, and thelubricating oil purifier was restarted.
On January 3, 1997, Safety Boardinvestigators were present when the oil purifierwas stopped, cleaned, and restarted. On January6, 1997, the purifier began to alarm due to lossof water seal. When the purifier was opened andexamined on January 10, 1997, investigatorsfound heavy contamination from an asphalt-likesubstance.

41
Automatic Main Engine Lubricating OilTrip Function -- According to statements fromthe chief engineer and other engineeringcrewmembers, the normal practice for the BrightField while operating in restricted waters was tohave the No. 1 lubricating oil pump running andthe No. 2 pump on automatic standby and thatthe vessel was operating in this configuration onthe day of the accident. On January 4, 1997,Safety Board investigators tested the oil pumpautomatic changeover feature by reducing thelubricating oil pressure sensed by the device.During these tests, the pressure switch failed toactivate the standby pump. While investigatorswere conducting tests of other systemcomponents, Bright Field engineeringcrewmembers examined and further tested thepressure switch. When Safety Boardinvestigators retested the pump changeoverfeature a few days later, the switch functionedand started the standby pump automatically. Theoriginal pressure switch was removed from thevessel for laboratory testing. Test conclusionswere that, “the contact resistance is abnormallyhigh,” and could, under certain conditions,“cause a problem; i.e., giving erroneous …orfaulty readings.”
Alarms, Indicators, and Recorders --Safety Board investigators examined wheel-house and control room engineering alarm lightsand found that the wheelhouse automatic slow-down alarm light was burned out. In tests of thewheelhouse and control room audible and visualalarms using the manufacture’s test plan, thesystem worked as designed.
The Terasaki monitoring and alarm systemwas designed to record and print out alarmconditions and propulsion control system eventsthat were activated by the automated system.Manual actions taken by the operating crewwere displayed on video monitors in the enginecontrol room, but no printed record was made ofthose actions. The alarm log printout for the dayof the accident showed engine trip due to lowoil pressure at 1406. The printout did notindicate automatic starting of the No. 2lubricating oil pump.
Investigators compared lubricating oilpressure readings displayed on local analoggauges with those recorded by the Terasakisystem. While the analog gauges displayed the
same readings, the monitoring and alarm systemrecorded pressures that were higher than thegauge readings by about 0.3 bar.
Remote Engine Control Tests -- OnJanuary 5 and 10, 1997, with representatives ofIHI, the Bright Field engineering and navigationcrew, and the Coast Guard in attendance, SafetyBoard investigators observed testing of theremote engine control using an IHI simulationplan dated December 29, 1996. Control wassuccessfully shifted between the wheelhouseand the control room, and the control roomanswered all telegraph commands from thewheelhouse. No unexplained anomalies werenoted at either control station. Similar tests werelater conducted with the vessel underway, andall controls worked as designed. In testimony,neither the chief engineer nor the chiefelectrician could explain the two engine-startinganomalies experienced by the vessel onDecember 14 on the downriver voyage. Duringtesting, the problem could not be reproduced.
Preventive Maintenance -- The BrightField was provided with owners’ instructions,dated August 28, 1995, that describedrequirements for periodic (based on enginehours) inspection and repair of the vessel’s mainengine, auxiliary, and electrical equipment(exclusive of equipment associated with theautomated propulsion control system). OnOctober 25, 1995, the owners, concerned about“frequent cylinder liner cracks in the past 1 or 2years,” instituted additional operating policy forthe maintenance of the Bright Field mainengine. Safety Board investigators were unableto find evidence that the vessel’s crew(s)complied with the periodic maintenancerequirements developed by the owner.
Reports and Recordkeeping --Engineering personnel on the Bright Fieldmaintained several types of records that werereviewed by investigators. The secondengineer’s daily log book recorded work doneon the vessel’s machinery. The log wastranslated by the second engineer each monthand sent to the owner with other vessel reports.
The owner received periodic telexes fromthe master documenting the severity ofengineering problems, delays in schedulingresulting from the engineering problems, and

42
the inability of the engineering crew to makepermanent repairs. See appendix B for a detailedchronologies of engineering problemsreferenced in the monthly engineering reportsand in the master’s telexes to the Bright Field’sowner.
Main Engine Lubricating Oil Testing andAnalysis -- The Bright Field’s lubricating oilswere supplied by British Petroleum (BP) onlong-term contract. BP also periodicallyprocessed oil samples provided by the owner fortest and analysis.
In a January 20, 1996, analysis of a BrightField main engine bearing oil sample, BP founda reduced flash point and recommendedcorrective action. Analysis by BP of an August24, 1996, sample showed increased viscosityand reduced flash point. BP oil analystsconcluded that the oil was contaminated by fueloil leaking from the main engine. The reportrecommended immediately replacing the mainengine lubricating oil and correcting the fuelleak. The second engineer stated that hechanged the main engine lubricating oil onNovember 5, 1996, after the main enginealarmed and went into emergency slowdownbecause of a high density of oil mist in thecrankcase. The second engineer stated that hesuspected fuel oil contamination of thelubricating oil system.
The engine manufacturer recommended tothe Bright Field’s owners in November 1996that the engine oil be tested as soon as possibleto check for contamination by water and fuel.The sample was drawn by the chief engineer onNovember 20, but was not tested by BP untilJune 1997. BP analysis of the oil indicatedelevated water content and viscosity comparedwith BP’s oil specifications and the enginedesigner’s recommended range of acceptable oilproperties. The analysis also recorded elevatedinsolubles due to combustion byproductsentering the lubricating oil.
A December 18, 1996, sample collected bythe Bright Field’s chief engineer was tested bySaybolt, Inc. The analysis indicated excessivewater content and high viscosity whencompared to a clean sample of the BP oil.Saybolt reported that the oil sample alsocontained a significant amount of suspended
particulates. Additional analysis of lubricatingoil samples collected by Safety Boardinvestigators and analyzed by JET-CAREInternational, Inc., confirmed elevated viscosityand water content in excess of BP and Sulzerspecifications.
Spare Parts and Calibration Tools -- Thesecond engineer’s maintenance record andtelexes from the master noted that spare partsfor the main engine, auxiliary boiler, watermaker, and other engineering equipment wereeither in short supply, of poor quality, or notavailable at all. According to the records, thelack of readily available spare parts meant thatengineering personnel had to reuse worn ordamaged parts that could be made serviceable.Calibration tools necessary to set the timing ofthe main engine fuel pump were missing andcould not be located.
Sulzer Inspection -- A representative ofNew Sulzer Diesel, the designer of thepropulsion diesel engine, had inspected theengine shortly after the Bright Field arrived atNew Orleans in November 1996. He identifiedseveral sources of possible lubricating oilcontamination and noted the following problemswith the main engine:
• Cracked cylinder liners;
• Missing, worn, dirty, carbon-contaminatedcomponents, including piston rings;
• Clogged cylinder inlet ports and pistoncooling passages;
• Clogged, dirty, damaged components tocharge air receiver; water leaks observed;
• Fuel oil pump drain clogged and leakingfuel oil into main engine lubricating oilsump (recommended testing oil as soon aspossible);
• Missing main engine turbocharger filtersand dirty internals;
• Control air system valves clogged withcondensation;
• Worn, loose, misaligned fuel oil pumps andlinkages.

43
Chief Engineer’s Assessment -- OnDecember 9, 1996, the new chief engineercorresponded with the Bright Field’s owners,confirming the seriousness of engineeringproblems observed by the Sulzer technician inlate November and indicating the status ofrepairs. He reported the following:
• Scavenging box showed serious accumula-tion of sludge and carbon with blocked airvents;
• Charge air cooler separation panels pol-luted, blocked, and rusted;
• Scavenging box nonreturn air valvesblocked with sludge;
• Missing, loose, worn piston rings; sparepiston rings of low quality;
• High-pressure fuel oil pump residuedischarge pipes blocked, leaking fuel oilinto lubricating oil sump;
• Cracked, welded cracks in No. 2 cylinderliner; renewed piston head (only 360 hoursof operation since this cylinder liner waslast pulled);
• No. 5 piston rings replaced;
• Control air system contaminated;
• One Terasaki computer monitor out ofcommission; second monitor distorted;
• Auxiliary boiler out of commission; fuel oilpump not working and numerous plugged(with debris) tubes from lack ofmaintenance; main engine’s main bearinglubricating oil not being purified;
• Abnormal main engine cylinder cooling;
• Smoke exhaust from main engine darkbecause of problems with turbochargerand/or charge air cooler;
• Improper main engine fuel oil injectiontiming;
• Serious noise and vibration from both mainengine lubricating oil pumps;
• Numerous auxiliary pumps, engines, andmotors not working or working poorly.
Safety Board investigators examined theengineering plant following the accident anddetermined that the vessel had sailed onDecember 14, 1996, with the followinguncorrected engineering conditions:
• Severe noise and vibration in both mainengine lubricating oil pumps;
• Defective Terasaki monitoring equipment;
• High differential pressure across the secondfilter;
• Poorly calibrated sensors (automated pro-pulsion control system); and
• Main engine lubricating oil quality andquantity that did not meet specifications.
Tests, Reports, and System Calibration --The chief electrician’s log book reflectedelectrical work completed, tests conducted,problems encountered, and electrical machinery(cranes, winches, motors) used each day. Thereports were translated by the chief electricianand included with the vessel’s monthly reports.(See appendix B for a record of problemsassociated with the automated propulsioncontrol system.)
The chief electrician also conductedquarterly testing of engineering safety devices,such as alarms and sensors, and submitted areport on their operation to the owner. Thequarterly testing did not evaluate the conditionof engineering safety control devices, such asthe pressure switch for starting the standbylubricating oil pump. Also excluded were thetrip and slowdown set points. The chiefelectrician stated that neither he nor the chiefengineer tested the calibration of the automatedpropulsion control system set points.
The Bright Field was originally deliveredwith a complete DNV-approved set ofautomated propulsion control system testprocedures for periodically validating theoperability of the control system. The BrightField’s engineering crew stated that they were

44
unaware of any test procedures and did notregularly test or calibrate the system. Theengineering crew could not produce a set ofautomation test procedures. Copies of post-delivery automation test procedures were foundin the crew’s library.
Technical manuals covering eachcomponent of the automated propulsion controlsystem were on board the Bright Field. Most ofthe manuals were found in the staterooms ofindividual engineering officers.
Computer Simulation -- The VehiclePerformance Division of the Safety Board’sOffice of Research and Engineering digitizedand analyzed data retrieved from a video madeby the tugboat Lockmaster as the vessel’s radartracked the Bright Field. Engineers attempted tocompute vessel motion parameters; however, theradar data were of low resolution and did notprovide an accurate depiction of the BrightField’s movement. The Safety Board contractedwith the Corps of Engineers to perform anengineering computer simulation to determinethe path of the Bright Field during the accidentsequence. The simulation was based oncomputer modeling of the Bright Field and theMississippi River at the accident site. Becauseof the limited number of parameters availableupon which to base the simulation, the Corps ofEngineers simulation results were alsoinconclusive.
Other InformationPort Risk Analysis and Management—
Coast Guard -- The Coast Guard, under thePorts and Waterways Safety Act of 1972, wascharged by Congress with monitoring,managing, and communicating risk in all U.S.ports and taking actions to maintain risk at anacceptable level. The act empowers Coast GuardCOTPs to monitor the risk levels in their portareas and maintain “an acceptable level of risk.”The Coast Guard Marine Safety Manual definesthe elements of waterways risk assessment to beconsidered by the COTP as vessel properties,waterway properties, cargo properties, andenvironmental conditions.
General port risk management is theresponsibility of the Coast Guard’s Office ofMarine Safety and Environmental Protection,
which is charged with protecting the public, theenvironment, and United States economicinterests by preventing or mitigating the effectsof marine accidents and incidents. According tothe “Program Principles” section of the Officeof Marine Safety and EnvironmentalProtection’s 1996 Performance Report,37 riskmanagement is the “business” of the office. Thereport states:
Preventing low probability-highconsequence events, such as major lossof life on passenger vessels, andmedium and major oil spills, is acornerstone of our risk managementapproach. To improve our decisionmaking, we need to strike a balance,allowing field commanders to employexisting risk analysis tools for routinerisk management decisions, whileestablishing a formal program policy forhigh level risk analysis projects, such ascomprehensive port risk models.
Appendix III of the report, “RiskManagement & Risk Analysis,” defines risk as“the probability of suffering a degree of harmfrom one or more hazards.” The documentquantifies this definition with the formula:
RISK = Probability x Consequence
The document states that the risk equationimplies that some risks are greater than othersand that risk management involves choicesabout “how, and to what degree, we will try toreduce the probability and/or consequences of apotentially harmful event.” The document statesthat a complete risk management processincludes risk analysis, risk management, andrisk communication.
Risk analysis, according to the document, isthe process of systematically identifying,estimating, and ranking risks according to theirprobabilities and consequences. From thatranking of risk, a risk-ranking matrix (figure 13)can be developed. The document states that the
37The 1996 report on the office’s progress towardgoals contained in Commandant Instruction 16000.2(series), Business Plan for Marine Safety andEnvironmental Protection.

45
Office of Marine Safety and EnvironmentalProtection’s overall risk management strategyusing this matrix is to select the higher risks thatcan be influenced and try to reduce theirfrequency and/or consequence in order tominimize their contribution to overall risk in thewaterway.
Risk management, according to thedocument, is the systematic selection of optionsfor treating different risks. “Options mayinclude measures aimed at reducing theprobability and/or consequences of particularrisks, eliminating risks, shifting risks in spaceand/or time, or tolerating risks.”
The document defines risk communicationas the “continuous, two-way process ofcommunicating with stakeholders38 about therisks associated with [the] system of concern.”
Port Risk Analysis and Management—Other Stakeholders -- During the past 20 years,various stakeholders in the greater New Orleansport area have commissioned numerous riskassessment and reduction studies.
38Stakeholders refers to parties of interest, from bothpublic and private sectors, in the Port of New Orleans area.
Lower Mississippi River Safety Study -- Theobjective of this 1981 study by Louisiana StateUniversity was to develop recommendationsconcerning the way in which communications,electronics surveillance, aids to navigation, andtraffic management could best be used toenhance river safety and protect theenvironment. The study identified problemsamong port and waterway uses, determinedtraffic patterns and volume in the area,synthesized accident data from the Coast Guardand other sources, identified areas of hazardcreated by natural and artificial conditions andstructures on the river, surveyed those who usethe river to ascertain their opinions about riversafety and what was needed to improve it, anddeveloped a prototype system to enhance riversafety.
Louisiana World Exposition -- Prior to the startof the 1984 world’s fair, LWE officials preparedan environmental impact statement thataddressed safety concerns associated withmarine accidents. An analysis of vesselincidents between January 1973 and September1981 revealed that only one vessel had struckthe Julia Street wharf during that period, with noinjuries reported. The Poydras, Julia, and EratoStreet wharves were determined to be the areasleast associated with vessel strikes.
/RZ
&RQVHTXHQFH 0HGLXP
&RQVHTXHQFH
+LJK
&RQVHTXHQFH
+LJK
3UREDELOLW\
0HGLXP
3UREDELOLW\
/RZ
3UREDELOLW\
Figure 13 -- Coast Guard risk-rankin g
0DMRU#3DVVHQJHU 9HVVHO#&DVXDOW\ 0DMRU#2LO#6SLOO

46
LWE officials recognized that fair structuresand activities could adversely affect safenavigation along the Mississippi River. Forexample, fair officials were concerned thatnighttime illuminations, including fireworksdisplays, could interfere with the night vision ofmariners. To minimize these risks, the LWErequested that the COTP establish a “safetyzone,” within which the Coast Guard wouldregulate marine traffic when the fair held specialevents on the river. The safety zone wasestablished, and mariners received notices fromthe Coast Guard cautioning them to navigatevessels with extreme care in the vicinity of theworld’s fair.
The Dock Board refused to allow theberthing of barges and houseboats at the Julia,Erato, and Poydras Street wharves during thefair. The Dock Board rejected the LWE’srequest to place exhibit pavilions (that would beexpected to have large numbers of visitors) onfloating barges moored along the river.39 TheDock Board did permit the mooring of tall ships,oceangoing passenger vessels, largesternwheelers, and visiting foreign warships inthe area.
International RiverCenter -- Prior to theexpansion of the Hilton Hotel, the IRC wasrequired to obtain construction permits from thecity of New Orleans, the Corps of Engineers,and the New Orleans Levee Board. The DockBoard required that the plans be submitted forreview and executed a lease with the IRC for thedevelopment. The Dock Board reviewed theplans to determine the extent to which thedevelopment might interfere with Dock Boardactivities.
According to the IRC, during the time whenthe IRC was negotiating a lease with the DockBoard, the Dock Board advised the IRC thatvessels had had allisions with wharves withinthe Port of New Orleans, but that no allisionshad occurred at the Lower Poydras Street wharf.The IRC representatives were shownphotographs of the allisions at other wharves.
39Information regarding activities of the Dock Boardduring the fair was provided by the Dock Board andconfirmed by a former Dock Board chief executive officer.
These photographs, according to the IRC,“depicted only minimal damage.”
An IRC official was not aware of anypreconstruction risk assessments that werecarried out in connection with the Hilton Hotelexpansion in the early 1980s, and the IRC wasunable to provide the Safety Board with anyother information regarding previouslycompleted risk assessments regarding theirproperties built on the river side of the levee.The damaged properties, including portions ofthe Riverwalk Marketplace mall, thecondominium parking garage, and the HiltonHotel are being rebuilt on the same footprint. Nophysical barriers against accidents involvingriver traffic have been constructed at thislocation.
New Orleans Aquarium of the Americas --In1987, before construction of the Aquarium ofthe Americas, the Audubon Institute contractedfor a risk analysis for construction of theaquarium on the riverfront outboard of thelevee. The contractor was asked to assess thesafety risk from marine traffic at the site of theproposed Riverfront Park, including aquariumstructures and park area. The scope of workincluded a study of 20 years of Port of NewOrleans records documenting damage towaterfront facilities at and near the site of theproposed Riverfront Park, as well as thepotential consequences of an allision of a vessel,barge tow, or boat with Port of New Orleanswharves such as the Bienville Street wharf,where the proposed aquarium was to be located.
The report concluded that vessels and towsmoving downriver, with the current, have lesswater moving across the rudder, rendering themless maneuverable and their pilots less able toadjust to emergency situations. This hazardincreases with higher river stages, which deliverfaster currents. The study concluded that, if anoutbound ship or tow were to lose steering,power, or control, or if it were to becomeslightly out of shape to navigate the bend aroundAlgiers Point, the Bienville Street wharf areawould be less likely to be damaged, since thedownriver current would probably carry thevessel past this area. Vessel damage would morelikely occur in the areas of the GovernorNicholls, Esplanade, or Mandeville Streetwharves, which are located in the Algiers Point

47
bend of the river, about 3/4 mile below theBienville Street wharf. According to the report,because Bienville Street wharf is high in thebend, it faced low risk of being struck by anoutbound vessel.
A Port of New Orleans review of records for1967 through 1987 indicated that the Bienvilleand adjacent Toulouse Street wharves hadreceived no major vessel strikes; however,major vessel strikes had occurred along thewharves at and downriver from GovernorNicholls Street.
Analysis of wharf damage from ship, barge,and tow strikes revealed that such damage rarelypenetrated beyond 25 to 50 feet inward of thefender line. The shock from such an accidentcould be felt for a distance along the wharf; butthe impact load was not sufficient tocompromise the overall stability of the wharf.
The report concluded that any majorstructure located 100 feet or more from the edgeof the wharf would not be in danger from rivermarine traffic. The report recommended that thearea within 50 to 100 feet of the wharf beconsidered a buffer zone that, while open topedestrian traffic, should be free of buildingstructures. The report stated that this buffer zonecould be most effectively isolated from the innerwharf area by a motion control joint, installedparallel to the fender line, that would reduce anyvibrations from a ship strike.
Gaming Vessel Risks and Background -- In1991, the Dock Board initiated a series ofplanning initiatives related to riverboat gaming.These initiatives included commissioning theCoast Guard and the Louisiana State UniversityNational Ports and Waterways Institute toconduct a navigation risk assessment. The DockBoard also contracted with a safety consultant toreview the safety of Dock Board properties andto develop guidelines for gaming vesseloperation. The consultant’s study addressedpublic-safety aspects of riverboat gaming,focusing on fire protection, police response, andemergency medical services. It focusedparticular attention on ways of ensuring thatgaming vessels had adequate access and egress.
The Coast Guard COTP determined thatabout 350 incidents of steering and power loss
were reported annually in the COTP-NOLAzone.40 The COTP requested that the DockBoard provide a navigational risk assessment inpreparation for berthing the riverboat gamingvessels. The Dock Board contracted with theNational Ports and Waterways Institute, incooperation with the George WashingtonUniversity, to conduct the risk assessment thatwent beyond the scope of the Coast Guard’srequest to consider a wide range of safetyaspects along the Mississippi River. Theassessment incorporated input solicited fromwaterway users, including local pilots. Thestudy did not address the high-capacitypassenger cruise ships that use the Julia or EratoStreet wharves as bases of operations.
Phase I of the study, completed in July1994, concluded that the addition of gamingboats to the Mississippi River increased both theprobability of a marine casualty and thepotential impact of such a casualty. While theincrease in the probability of an incident wascomparatively small, the increase in potentialinjuries and loss of life was large in relation tocasualties involving nongaming vessels. Thestudy determined that the increased risk wasprimarily a function of the operatingenvironment, not of the vessels themselves. Thestudy asserted that restricting the conditionsunder which gaming vessels may cruise couldreduce, but could not eliminate, the risk.
Accident data (figure 14) for the Port ofNew Orleans from 1983 through 1993 (a total of166 rammings along the left descending bankbetween miles 91 and 101 AHP) were analyzedand the results tabulated to identify a mooringarea for gaming vessels of “lowest historicalallisions on the left bank.” The study stated, “Itshould be noted, however, that no area of theleft bank downbound was completely free ofallisions during the eleven year period.”
The phase I report made the followingrecommendations:
• Gaming vessels moored on the leftdescending bank of the Mississippi River
40The COTP-NOLA zone extends along theMississippi River from the Arkansas border to the Gulf ofMexico.

48
3 8 43 48 53
1 # #$80%(5 2) //,6,216
0,/(3267
)LJXUH#47#00#$OOLVLRQV#LQ#WKH#0LVVLVVLSSL#5LYHU#+WRWDO#499,#EHWZHHQ################PLOHV#<40434#$+3#+OHIW#GHVFHQGLQJ#EDQN,#4<;604<<6
<418<41<<514
<6<615
<619
<61:<714
<715<717
<719<71<<8
<818
<819<915
<916<:<:16
<:1;
<:1<<;16
<;17
<;19
<;1;
43414
43319
<:18
<816
6W1#0DXULFH#$YH1$ODER#6W1
$QGU\#6W1
3RODQG#$YH13DXOLQH#6W1 3LHW\#6W1
)3UHVV#6W1/RXLVD#6W1
0DQGHYLOOH#6W1
(VSODQGH#$YH1
7RXORVH#6W1
&DQDO#6W13R\GUDV#6W1-XOLD#6W1
(UDWR#6W1#/RZHU
(UDWR#6W1#8SSHU2UDQJH
0DUNHW6W1#$QGUHZ#6W1
)LUVW#6W1
+DUERU#3ROLFH27KLUG#6W16HYHQWK#6W1
+DUPRQ\#6W1/RXLVLDQD#$YH1#*/)/(
1DSROHRQ#$YH1#(
1DSROHRQ#$YH1#%1DSROHRQ#$YH1#$
1DVKYLOOH#$YH1
+HQU\#&OD\#$YH1
*RYHUQRU#1LFKROOV

49
should be moored in the area of lowesthistorical accident rate (Poydras Street toFirst Street);
• Gaming vessels should remain mooredduring periods of low visibility, high winds,or high river stage;
• The potential for protecting the mooredgaming vessel by allowing berths to silt inshould be investigated;
• Fully equipped rescue craft capable ofhandling the volumes of passengers shouldbe available, either through the public sectoror by contracts with the private sector;
• Contingency and disaster management plansshould be developed, and routinepreparedness drills should be held;
• The issue of providing emergency egressfrom passenger vessels to other vessels, to adock, or to a river bank should beinvestigated. The objective must be toremove passengers when underway ormoored during a crisis without havingpersons resort to leaping into the water.
The phase I study reported expert opinionthat “high river stage was an important factor inriver casualties” and stated that this opinion wassupported by casualty data. According to thatdata, casualties (allisions and collisions) show aseasonal trend, with the high water months ofFebruary, March, April, and May experiencingtwo to three times the number of casualties asthe low-water months of July through October.The phase I study did not determine thefrequency with which high-risk events werelikely to occur and thus could not provide anoverall estimate of risk for the port.
The phase II study developed methods tofurther quantify the risk levels and thus enablean evaluation of the overall risk, as well as riskreduction, due to the mitigation measuresidentified in phase I. A simulation of the Port ofNew Orleans integrated the expert assessmentsof phase I using available data, and simulationresults were validated against historical casualtystatistics. The simulation estimated that 2.24vessels incidents per month could be expected inthe port area from miles 80 to 106 AHP and
that, of these incidents, 0.75 incident per monthcould be expected between miles 90 and 95AHP.41
The phase II report reached the followingconclusions regarding gaming vessels:
• The probability of occurrence of an incidentat high river stage is 10 times greater than atlow river stage;
• A 25 percent increase in traffic in the riverwould result in a 37 percent increase in thenumber of vessel incidents that could beexpected.
One phase II study recommendation forminimizing the risk of high-capacity passengervessel operation in the Port of New Orleans wasthe following:
The Coast Guard and the Port of NewOrleans should ensure that responseplans and resources are adequate to dealwith a casualty involving a high-capacity passenger vessel. Although theprobability of an incident involving oneof these vessels can be minimized, theonly way to minimize the potentialimpact of such an event is to invest inthe resources and planning required toeffectively respond to such a casualty.
In 1993, the Governor’s Task Force onMaritime Industry, which addresses safetyissues on the Mississippi River and MississippiRiver—Gulf Outlet, formed a Marine SafetyCommittee to address the issue of gamingvessels berthing on the Mississippi River. Thecommittee was to solicit and promulgatesuggestions from local mariners regardingprotection of the areas in which gaming vesselswould be operating. The committee was latersubsumed into the Coast Guard PassengerVessel Safety Committee and other groupsformed by the Port of New Orleans to addressthe issue of minimizing casualties from acollision between a deep- or shallow-draftvessel and a gaming vessel. This committeefunctioned as an advisory group to the
41Mile 95 AHP is at the approximate location of theallision.

50
Governor’s Task Force and made the followingsuggestions:
• Assign a rescue boat to the immediatevicinity of the gaming vessels and equip itfor handling a large number of passengers incase of a casualty;
• Station in the area a fully equipped fire boat,which could be utilized as an additionalrescue boat;
• Install a weather and river monitoring sys-tem;.
• Assign a dedicated communications marineradio channel to be used by vesselstransiting the area;
• Post and otherwise publicize notices tomariners advising of this controlled zone;
• Conduct joint Coast Guard, harbor police,fire department, and police departmentemergency preparedness drills;
• Establish a fire and rescue station equippedwith a helicopter pad to provide rapidevacuation in case of a casualty;
• Ensure that all vessels are in full compliancewith classification society and Coast Guardrequirements;
• Meet with all gaming interests to reviewdesigns and recommendations of safetyprograms.
One member of the advisory grouprecommended that the area from the CrescentCity Connection Bridges to Canal Street beallowed to silt in, forming a barrier 150 to 200feet into the river to prevent deep-draft shipsfrom reaching the moored gaming vessels.
Operation Safe River -- In January 1994, CoastGuard Group New Orleans, together with theNew Orleans Port Authority Harbor Police, theCrescent River Port Pilots Association, the Cityof New Orleans Office of EmergencyPreparedness, and the Southeast LouisianaSearch and Rescue Organization, conducted ajoint search and rescue exercise on theMississippi River between the Crescent City
Connection Bridges and Algiers Point. Theexercise area included the section of the riverwhere gaming vessels were planned to berth andoperate. The exercise simulated a major marineincident in the Mississippi River involving ahigh-capacity passenger vessel. Weatherconditions during the exercise included an airtemperature of 40 °F and a water temperature of34 °F. This real-time exercise demonstrated that,during daylight hours with the resourcesavailable, only 20 to 30 percent of people in thewater could be expected to be rescued.
Based on the results of this exercise and thelarge number of vessel casualties—particularlybridge allisions—that had occurred during 1993-94, the Eighth Coast Guard Districtimplemented Operation Safe River to improvesafety on the Lower Mississippi River. Theoperation initiatives called for a higher standardof care by mariners and ordered COTPs to takea harder line on enforcement and penaltysanctions. The operation also includedinitiatives to review the riverboat gaming vesselprogram, focusing on the number of vessels andtheir docking sites, as well as ferry vessel safetypertaining to manning and operation.
According to Coast Guard officials,initiatives developed as a result of OperationSafe River have resulted in the following:
• An extension of the regulated navigationarea for barge fleeting, resulting in areduction in barge breakaway incidentsbecause of improved barge fleetingoperating practices;
• Improved reporting of vessel power andsteering losses by river pilots, and anincrease in the number of incidents in whicha pilot refuses to sail vessels withnavigational or engineering deficiencies;
• Increased awareness by owners andoperators of their responsibility for safenavigation in the river, resulting in areduction of incidents of vessel power orsteering loss;
• Better adherence by owners and operators toriver draft requirements, resulting in areduced number of mid-channel groundings;and

51
• Year-round operation of the Algiers trafficlight.
Changes Made Since the Accident --Several steps were taken after the Bright Fieldaccident to enhance safety in the Port of NewOrleans area.
River Front Alert Network -- The Coast Guardand the Dock Board, on March 11, 1997, agreedto a memorandum of understanding establishinga River Front Alert Network to provide earlywarning of potential shipping disasters in thearea of the Port of New Orleans. The RiverFront Alert Network is an 800 MHz emergencyradio alerting and communications systeminstalled at the Coast Guard’s GovernorNicholls traffic light control tower and the Portof New Orleans Harbor Police Department. Thesystem links the Governor Nicholls light, theHarbor Police Department, the Delta QueenCruise Terminal, the Riverwalk Marketplace,the Hilton Hotel, One River Place condomini-ums, and the Aquarium of the Americas.
The River Front Alert Network is designedto provide a capability to directly notify the Portof New Orleans Harbor Police Department andPort of New Orleans property tenants of apotential threat caused by vessels navigating inthe vicinity of Algiers Point. Under thememorandum of understanding, the alert signalis initiated by the Governor Nicholls lightoperator, who contacts the harbor policedispatcher and the security officers of theriverfront properties whenever an abnormalityor irregularity that could affect the riverfrontproperties is identified or reported by a vessel inthe Algiers Point regulated navigation area. Thelight operator is to transmit a short warningmessage over the network describing thesituation. The dispatcher and the securityofficers are to monitor the situation on themarine radio and make their own judgmentsabout the appropriate response at theirproperties. The network system is to beactivated as early as possible to provide themaximum advance notice to the riverfrontproperties. Once the situation is no longer athreat, an “all clear” message is to be initiatedby the light operator.
Under the memorandum, the Dock Board isresponsible for installing and maintaining the
River Front Alert Network system hardware,including system design, maintenance, support,problem identification, and repair. The Port ofNew Orleans is responsible for coordinating aprogram to regularly test the network, includingthe scheduling, participation, conduct, analysis,and corrective action required to ensure thesystem is functioning properly. The harborpolice are to implement standard operatingprocedures defining the actions to be takenwhen the network is activated during a possibleemergency incident, situation, or condition. Theport is to coordinate with the property tenants todefine the emergency actions to be taken whenthe network is activated.
According to documentation provided bythe Dock Board on November 3, 1997, the boardhas worked with the property tenants whoparticipate in the River Front Alert Network todevelop and implement standard operatingprocedures for emergency evacuations. TheDock Board reports that property tenants withinthe River Front Alert Network zone haveupdated their emergency plans to incorporatethe network alarm system and to provideinstructions for security officers to follow in theevent the Coast Guard light operator activatesthe River Front Alert Network radio. Under theupdated procedures, security officers are tolisten to the broadcast from the Coast Guardlight operator, monitor VHF channels 16 or 67,visually assess the situation on the river, and onthe basis of this information, determine whetherto order an evacuation of the property. Thesecurity officers are authorized to initiate anevacuation immediately based on the nature andimmediacy of the apparent river danger. Upondetermination that an evacuation is necessary,security officers are to make public addressannouncements of the evacuation andimplement those evacuation procedures thathave been established for their particularlocations.
New Notices, Rules, and Operating Regulations --In January 1997, the New Orleans COTPidentified passenger vessels deemed to be at riskfrom allisions and issued written COTP ordersdirecting these vessels to (1) maintain a constantbridge watch whenever passengers areembarked, (2) maintain a constant monitoringwatch on VHF-FM channel 16 or otherappropriate emergency and bridge-to-bridge

52
radio frequency, and (3) be able to alertpassengers and other crewmembers and have theability to direct initial action in the event of anemergency.
Also in January 1997, the New OrleansCOTP issued a notice that on vessels of morethan 1,600 gross tons, the anchors are to be keptready for immediate release and that, while theanchor watch is in effect, effectivecommunications are to be provided between thebridge and the foredeck.
On March 21, 1997, the commander of theEighth Coast Guard District issued temporaryrules applying new operating requirements toself-propelled vessels of 1,600 gross tons ormore operating in the Mississippi River betweenthe South and Southwest Passes and mile 233.9AHP. According to the Coast Guard, the newrequirements were prompted by the Bright Fieldaccident and by subsequent unprecedented highwater levels in the river, which had led to “amarked increase in vessel accidents.” Thesetemporary rules were extended twice; thesecond extension was set to expire on October31, 1997.
Before the expiration of the temporary rules,the Coast Guard, on October 30, 1997,published the new requirements as an interimrule (33 CFR Part 165) in the Federal Register.Interested parties have until December 29, 1997,to comment. In its discussion of the rule, theCoast Guard stated that the new requirementswere needed to “protect vessels, bridges,shoreside facilities, commercial businesses andthe public from a safety hazard created by deep-draft vessel operations along the LowerMississippi River.” The Coast Guard noted thatduring 1995 and 1996, more than 300 self-propelled vessels of 1,600 gross tons or greaterexperienced loss of power, loss of steering, orengine irregularities while operating in theMississippi River. It stated that the new ruleswould enhance safe navigation of the river byrequiring that masters and engineers takemeasures to minimize the risk of steeringcasualties or engine failures/irregularities.
Under interim 33 CFR 165.810(e),passengers vessels with one or more passengerson board that are anchored or moored in theLower Mississippi River below mile 233.9 AHP
are required to keep a continuously mannedpilothouse,42 and to
monitor river activities and marine VHFemergency and working frequencies ofthe port so as to be immediatelyavailable to take necessary action toprotect the vessel, crew and passengersin the event that an emergency radiobroadcast, danger signal or visualindication of a problem is received ordetected.
Under interim 33 CFR 165.810(f), self-propelled vessels of 1,600 gross tons or moreoperating in the regulated area are to complywith the following:
(1) The engine room shall bemanned at all times while un-derway in the RNA [RegulatedNavigation Area].
(2) Prior to embarking a pilot whenentering or getting underway inthe RNA, the master of eachvessel shall ensure that the ves-sel is in compliance with 33CFR Part 164 [specifying testsof steering gear, internal vesselcontrol communications, emer-gency generators, storagebatteries for emergency sys-tems, and main propulsionmachinery, ahead and astern, allof which are to be completedprior to entering or gettingunderway in U.S. navigablewaters].
(3) The master shall ensure that thechief engineer has certified thatthe following additional oper-ating conditions will besatisfied so long as the vessel isunderway in the RNA:
(i) The main propulsion plantis in all respects ready for
42The rule exempts ferryboats and small passengervessels of less than 49-passenger capacity from thisrequirement to maintain a manned pilothouse.

53
operations including themain propulsion air startsystems, fuel systems,lubricating systems, coolingsystems and automationsystems;
(ii) Cooling, lubricating andfuel oil systems are atproper operating tempera-tures;
(iii) Automatic or load limitingmain propulsion plantthrottle systems are oper-ating in manual mode withengines available to im-mediately answer maneu-vering commands; and
(iv) Main propulsion standbysystems are ready to beimmediately placed inservice.
Steering Loss Study -- After the Bright Fieldaccident, a number of maritime, portcommunity, and public stakeholders in the Portof New Orleans began to work together toaddress mutual concerns. One result was a studyof propulsion and steering losses experienced inthe Lower Mississippi River, which wasexpanded as a national issue for the CoastGuard’s Navigation Safety Advisory Council(NAVSAC). In April 1997, the NAVSACNavigation Equipment Committee concludedthat loss of propulsion and steering by vesselswhile navigating the Mississippi River is anational problem and that the nature of theseincidents is of great concern to all stakeholders.The committee is exploring solutions, regulatoryand nonregulatory, that can be implemented tohelp prevent steering and propulsion casualties.
Another area of concern to stakeholders wasdevelopment of objectives for a vessel trafficsystem (VTS) for the Lower Mississippi River.After the Bright Field allision, an ad hoccommittee produced in January 1997 a“foundation of needs,” which addressed anumber of government, industry, and publicobjectives for improved river safety. Accordingto the Coast Guard, it has designated the Lower
Mississippi River as the location of ademonstration project for a new “silent” VTSsystem that is expected to begin limitedoperation in mid-1998. Under the silent VTSsystem, vessels will be equipped withtransponders that will transmit a wide range ofvessel description and position information thatcan be displayed on computer screens aboardany vessel in the area. The system will provideinstantaneous and positive vessel informationwhile reducing VHF radio traffic.
Ship Drill Alarms -- Immediately following theBright Field accident, the president of the Portof New Orleans issued a letter to the cruise lineowners at the Julia Street wharf asking them tosuspend the sounding of their ships’ whistlesduring drills in order to avoid confusion aboutthe source and meaning of the whistle. Theletter requested that the cruise lines suspend thedrills and whistle soundings until they havedeparted the Julia Street wharf. In addition, thePort of New Orleans revised its general rulesand regulations to read:
No vessel, whether a cruise ship or anexcursion boat, shall sound a distress,fire or emergency alarm as part of itspreparation drills while it is docked ator near the Board’s wharves from RobinStreet to Governor Nicholls Streetexcept for such alarms required as partof a vessel’s quarterly drills required tomaintain U.S. Coast Guard certification.In the latter event, each vessel shallnotify in advance of such, thesurroundings of the Board’s HarborPolice Department, the Hilton Hotel,One River Place and the New OrleansRiverwalk Associates. To the extent thata vessel needs to familiarize passengerswith the sounds of such alarms as partof its on-board safety drills, theseexercises should be conducted when thevessel is either below the GovernorNicholls Street wharf or above theRobin Street wharf.
Riverwalk Marketplace Alert System -- Accordingto minutes taken during a public Dock Boardmeeting on February 6, 1997, the RiverwalkMarketplace plans to install three cameras thatwill monitor and display river traffic to all mallmerchants. The River Front Alert Network

54
provides an alarm to the Riverwalk securitydesk, which then monitors maritime activities bymarine radio and visual monitoring. Thesecurity desk determines the appropriate courseof action, including the sounding of evacuationalarms. In addition, representatives of thecomplex proposed the installation of a color-coded alarm system display monitor that willnotify merchants of the type of evacuationprotocol to follow in the event of an emergency.
According to representatives of theRiverwalk Marketplace, the public addresssystem in place at the time of the accidentoperated through the mall’s Simplex alarmsystem, which used speakers mounted at alarmlocations throughout the mall interior.Emergency instructions were broadcast throughthese speakers. Since the accident, the systemhas been modified so that emergency messagescan be broadcast throughout the mall via thebackground music system. Riverwalk isinvestigating the possibility of a dual strobe-horn combination alarm system that would alertthe mall tenants, employees, and patrons to thetype of evacuation required under variousemergency scenarios.
In an August 22, 1997, letter to the SafetyBoard, a Dock Board official stated that theDock Board had encouraged the IRC to widenthe remaining portion of the Upper PoydrasStreet wharf by 50 feet to match the portion ofthe wharf that was previously widened toaccommodate gaming vessels. The Dock Boardalso recommended that silt be allowed toaccumulate under the wharf as an additionalsafety factor. The letter noted that the DockBoard has no authority to compel the IRC tocarry out these modifications.
Vessel Egress -- The Dock Board, in itsPublic Protection and Emergency ManagementGuidelines for Gaming Vessels and BerthingAreas, states that “a powered mobile elevatingplatform suitable for emergency access orcasualty removal from upper decks is
conveniently available in the wharf area.” Alsoin its August 22, 1997, letter, the Dock Boarddescribed how the gaming vessel located at thePoydras Street wharf has complied with theDock Board’s guidelines. The letter stated thatthe Queen of New Orleans had provided anelevator-equipped gangway and a wharf-mounted crane.
The same guidelines state that “forpassenger use, at least two regular gangwaysleading directly to the wharf are necessary.”This guidance applies to all three vessels ownedby New Orleans Paddlewheels, Inc., (the Queenof New Orleans, the Creole Queen, and theCajun Queen). In its August 22, 1997, letter, theDock Board stated that:
The excursion vessels have aluminumgangways as a secondary means ofegress in addition to their primarygangways. The Flamingo (Queen ofNew Orleans) has such emergencygangways at all levels. The CreoleQueen and the Cajun Queen havesecondary emergency gangways andadditional gangways are currently onorder.
According to the Dock Board’s letter, boththe board and the Coast Guard require thatriverboat gaming vessels, excursion vessels,riverfront commercial properties, andoceangoing cruise ships prepare their ownemergency response plans and conduct relatedtraining and drills. The Dock Board stated that ithad recently reviewed all such plans.
Status of the Queen of New Orleans --According to documentation received by theSafety Board on October 22, 1997, the gaminglicense of the Queen of New Orleans expired onSeptember 30, 1997, and the vessel was notexpected to resume operations in the Port ofNew Orleans. Arrangements were reportedlyunderway to have the vessel moved from thePoydras Street wharf.

55
GeneralThe following factors were determined not
to have been causal or contributory to theaccident involving the Bright Field: weather,fatigue, malfunctioning of vessel steering gearor equipment on the bridge, and alcohol or otherdrugs. (See “Toxicological Testing” section ofthis report for additional information.) The pilotwas properly licensed and certified by the Stateof Louisiana and was qualified to serve in hisposition. All officers of the Bright Field wereproperly licensed and certified by the Liberiangovernment and were qualified to serve in theirpositions.
The Bright Field was not, nor was itrequired to be, equipped with a voyage datarecorder (VDR). (See appendix C.) Had it beenequipped with a fully configured VDR, valuableinformation such as the vessel’s exact position,course, rudder setting, throttle setting, enginespeed, and vessel speed at each point along theaccident track may have been available toinvestigators. Such information could have beenused to perform a comprehensive computersimulation that might have proved helpful inevaluating engineering and human performanceon the day of the accident.
The major safety issues identified in thisinvestigation and discussed in this analysis arethe adequacy of the ship’s main engine andautomation systems, the adequacy of emergencypreparedness and evacuation plans for vesselsmoored in the Poydras Street wharf area, and theadequacy of port risk assessment for activitieswithin the Port of New Orleans. This analysisalso addresses three other issues: the actions ofthe pilot and crew during the emergency, thelack of effective communication (as it relates tothe actions of the pilot and crew aboard theBright Field on the day of the accident), and thedelay in administering toxicological tests to thevessel crew.
Accident OverviewThe event that precipitated this accident, the
sudden and unexpected reduction in enginepower at a critical point in the Bright Field’snavigation down the Mississippi River, was ofrelatively short duration. However, thecombination of vessel speed, vessel direction,river current, and high river stage left littlemargin for error in responding to the emergency.The Bright Field struck the wharf in an areabetween two docked vessels, missing one ofthem by less than 170 feet and coming to restonly about 70 feet from the other. Thus, bysheer chance, an allision with an occupiedpassenger, gaming, or excursion vessel—and theassociated high risk of numerous seriousinjuries—was barely averted. Even so, patronsof a popular commercial district were placed injeopardy when the Bright Field struck portionsof shoreside buildings or undermined theirfoundation supports. Had this accident occurredduring the evening, at night, or in the morninghours, most of the hotel rooms that weredestroyed in the accident would probably havebeen occupied. It is unlikely that even the RiverFront Alert Network would have been able toawaken the sleeping guests, alert them to thedanger, and evacuate them in time to preventserious injury or possible death.
The significant reduction in the BrightField’s engine power resulted from low mainengine lubricating oil system pressure and thenonautomatic starting of the backup (No. 2)lubricating oil pump. With main engine powerreduced and the ship swinging toward theRiverwalk, the time and options available to thepilot and crew to avoid an allision were limited.The options involved pulling ahead andmaneuvering out of danger, slowing and steeringaway, or stopping; however, exercising any ofthese options would have required more time,propulsion power, or steering control than wereavailable to the Bright Field in the momentsbefore the allision. The Safety Board couldtherefore not determine whether the pilot orcrew could have done anything to prevent thisaccident. The same constraints on power and
ANALYSIS

56
control that hindered efforts to prevent theaccident also may have rendered ineffective theactions that the pilot and crew did take prior tothe allision. Thus, the final rest position of theBright Field may have resulted from thecombined forces of the ship and the river ratherthan from the efforts of the pilot or crew. Thesubstantial role played by chance in thisaccident has important implications forassessing risk in and around the river, as will bediscussed below.
The investigation of this accident revealed ahistory of maintenance and operationalproblems associated with the main propulsionengine of the Bright Field. These problems wereknown to the vessel’s owners, who did notcorrect them in a timely fashion. On the opensea, in good weather, temporary malfunctions inthe vessel’s main engine may be tolerable;however, in the close quarters of the MississippiRiver, where safe maneuvering is directlydependent upon a responsive main engine, a lossof power can, as it did in this instance, presentan immediate threat to other vessels and toshoreside facilities.
Complicating the emergency created by theloss of engine power on the Bright Field was theinteraction between the river pilot and the ship’smaster and crew on the vessel’s bridge. Atseveral points prior to and during the BrightField emergency, the pilot, master, and crew ofthe vessel did not exchange importantinformation about the nature of the emergencyand its potential outcome. In slightly differentcircumstances, the limited communicationbetween the pilot and the ship’s crew could havecompromised the vessel’s ability to recoverfrom a threatening situation.
Some of the injuries resulting from theaccident were sustained by gaming andexcursion vessel passengers as they attempted toescape what appeared to be an imminentallision. The lack of adequate numbers ofreadily available egress routes, in addition to thelack of effective evacuation procedures andplans aboard the vessel on which numerousinjuries occurred, contributed to the number andseverity of injuries. The lack of advancewarning to the patrons and employees of theRiverwalk Marketplace also contributed to thenumber of injuries.
This accident demonstrates the riskrepresented by heavily loaded, (relatively) high-speed vessels navigating a twisting waterwaybordered both by populated wharves andmooring areas for passenger vessels. While theabsolute elimination of all risk associated withthis operating environment would be impossible,in the view of the Safety Board, opportunitiesexist to reduce the risk of vessel collisions andallisions and to reduce the vulnerability ofshoreside facilities.
Engineering AspectsMain Engine Shutdown and Restart --
About 1406 on the day of the accident, as theBright Field was passing under the CrescentCity Connection Bridges, the vessel’s automatedpropulsion control system reported low mainengine lubricating oil pressure and main enginetrip (shutdown) due to low lubricating oilpressure. The chief engineer stated that, whenthe alarms sounded, he noted that the lubricatingoil system had depressurized.
The complete shutdown of the main enginewas not immediately apparent to those on thebridge or in the control room because the“windmilling” effect as the vessel movedthrough the water kept the propeller (and thusthe directly connected engine) turning at about30 rpm. In fact, the engine probably did notcome to a complete stop before the chiefengineer cleared the fault indication andrestarted the engine. The alarm log printoutindicated that the power reduction was the resultof main engine trip due to low main enginelubricating oil system pressure.
When Safety Board investigators boardedthe Bright Field 2 days after the accident, boththe No. 1 and No. 2 lubricating oil pumps wererunning. Had the oil pump backup system beenfunctioning on the day of the accident, and hadit been set to automatic mode, the No. 2 oilpump would have started automatically whenthe system sensed a drop in main engine oilpressure. The system alarm log printout for thatday, however, did not indicate the automaticstarting of the second pump. Moreover, SafetyBoard tests showed that the pressure switch thatwould have automatically started the secondpump may have been inoperative on the day ofthe accident and therefore would have been

57
unable to effect the changeover, even with theNo. 2 oil pump set on automatic standby. On theday of the accident, then, either the automatedpropulsion control system was not set up forautomatic starting of the standby lubricating oilpump or the switch that accomplishes thechangeover failed to respond properly to thedrop in system pressure.
During interviews with Safety Boardinvestigators, no crewmember acknowledgedmanually starting the No. 2 pump; however, thepump could only have been started eitherautomatically—which would have beenrecorded on the alarm log printout—ormanually. The evidence indicates, therefore, thata crewmember did, in fact, manually start (byeither turning the switch to auto start or byinitiating a manual start on the pump motorcontrol panel when the changeover switchfailed) the standby oil pump after the BrightField’s main engine shut down because of lowlubricating oil pressure. The restoration ofsufficient oil pressure allowed the engine to berestarted.
Lubricating Oil Pump Operation --Although the main engine lubricating oil systempressure with the No. 1 lubricating oil pumprunning was consistently observed over a periodof several days after the accident to be about 2.3bar, the exact cause of the low pressure in thelubricating oil system could not be determined.Following teardown, cleaning, adjustment, andreassembly of the No. 1 lubricating oil pump,the outlet pressures reached the rated pressure of4 bar. Shortly after the pump was reinstalled, itagain displayed the vibration and noisyoperation that had been noted in earlierinspections and that had been reported to thevessel owners by the chief engineer before theaccident. The source of the vibration and noisecould not be determined; however, the No. 1lubricating oil pump continued to produce ratedpressure.
According to the system monitor printout, at1400 on the day of the accident, main enginelubricating oil pressure was 2.64 bar. Althoughsystem pressure was in the acceptable range, itwas critically close to the system’s low-pressure-alarm level. This slight differentialbetween the system’s operating pressure and thealarm/trip pressure settings (2.5/2.3 bar) was
due primarily to the pressure drop across thesecond filter, which resulted when contaminantsin the oil clogged the fine mesh screen of thesecond filter’s strainers. This determination isconsistent with the repeated second filter high-differential-pressure alarms recorded during theDecember 14 voyage as well as with the resultsof testing of the second filter.
At 1406, the pressure had dropped below2.3, as evidenced by the protection system’stripping the main engine off line. Several causesof this sudden pressure drop were considered,then discounted, because they would haveproduced outcomes that were inconsistent withinformation gathered in the investigation. Thosecauses include heavy pump cavitation fromaeration of the lubricating oil; failure of the No.2 oil pump’s discharge stop check valve, whichwould have allowed “backflow” of oil throughthe No. 2 pump; a faulty pressure relief valve onthe No. 1 pump, which would have allowed oilto backflow to the suction side of the No. 1pump; catastrophic failure of the main enginelubricating oil system’s piping; and manualintervention.
Several other possible causes of the suddendrop in lubrication oil system pressure could notbe discounted. These included the vibration andnoise problem in both oil pumps that had beennoted by the chief engineer weeks before theaccident and was never corrected and theabnormally low level of lubricating oil in themain engine sump. Incessant pump and pipingvibration could have precipitated a transient airleak in the fittings associated with the No. 1 oilpump. Or the No. 1 oil pump may have becomeairbound after pulling in air through the oilsump suction pipe inlet because of the low levelof oil in the sump. Either condition would haveallowed air to be drawn into the suction side ofthe pump, resulting in the rapid oil systemdepressurization observed by the chief engineer.In such an event, unless the standby pump isstarted immediately, the depressurization canresult in engine trip; as previously noted, theNo. 2 pump was either not on automaticstandby, or the automatic switching mechanismfailed to operate on the day of the accident.
General Condition of the Bright Field’sEngineering Plant -- Safety Boardinvestigators’ examination of the engineering

58
plant and maintenance records for the BrightField revealed, as noted earlier, enginelubricating oil that was not within the allowablespecifications of the oil supplier or enginedesigner, excessive differential pressure acrossthe second oil filter, and uncorrected vibrationand noise from both main engine lubricating oilpumps. Among other deficiencies identifiedwere marginal lubricating oil sump level,incorrectly calibrated sensing devices, reuse ofworn parts, and numerous other problemsassociated with the main engine and variousauxiliary systems/machinery. While many of thedeficiencies noted by the New Sulzer Dieseltechnician and chief engineer were correctedbefore the December 14 voyage, the vesselsailed with several significant engineeringproblems uncorrected.
A review of the vessel’s records dating backto January 1996 revealed that the engineeringcrew responded to recurring engineering failureswith repairs that were sufficient to keep thevessel operating most of the time. However, thecrew apparently was not able to makepermanent repairs to the vessel’s main engineand associated engineering systems; as a result,these problems became a continuing source ofvoyage disruptions. In the 3 months prior to theaccident, the Bright Field added about 1 monthto its schedule due to delays attributed toengineering problems.
The crew was not required to use theautomated propulsion control test proceduresthat were delivered with the vessel in 1988 or toperiodically test the functional operability of theautomated propulsion control system. Theengineering plant on the Bright Field wasequipped with a number of safety devices, andthe chief electrician submitted a reportconcerning the status of these devices to thevessel’s owners quarterly. But the report wasbased only on a survey of alarms and sensors.No one regularly performed operational testingand maintenance of safety control devices suchas the oil pressure switch that was supposed tostart the standby oil pump in case of a drop inmain engine lubricating oil pressure.
While the Bright Field’s owners providedeach vessel in their fleet with generalrequirements for periodic testing andmaintenance of the main engine, including
regular analysis of the main engine lubricatingoil, Safety Board investigators determined thatcritical main engine components were run untilfailure occurred and that periodic preventivemaintenance was not routinely accomplished.
The Safety Board concludes that the BrightField showed evidence of recurring engineeringproblems that affected vessel main enginereliability, and had all engineering systems beenkept in good repair and regularly tested, thevessel may not have unexpectedly lost powerduring its voyage down the Mississippi River.The Safety Board believes that ClearskyShipping Company should perform a baselineengineering assessment of the Bright Field’sengineering plant and correct all conditions notin conformance with manufacturer’sspecifications.
Vessel Owner’s Oversight of the BrightField’s Engineering Plant -- The Bright Field’sowners, Clearsky Shipping Company, receivedregular engineering and maintenance reports onthe Bright Field and thus had knowledge of thevessel’s engineering problems. Seriousengineering problems were reported to theowners as early as January 1996. In addition toreports from the engineering crew, the ownershad received periodic telexes from the masterdocumenting the severity of engineeringproblems, delays in scheduling resulting fromthe engineering problems, and the inability ofthe engineering crew to make permanent repairs.The Safety Board acknowledges that, on at leastone occasion in 1996, the Bright Field’sowners’ representatives visited the vesselbecause of concerns about the operation of theengineering plant. The owners also replaced theBright Field’s chief engineer when the vesselarrived in New Orleans on November 21because, they said, the engineer had beenunresponsive to the owners’ orders. Thedocumented problems with the Bright Field’sengineering plant, however, existed at least asearly as 1995, which predated the arrival onboard of the previous chief engineer. Theseengineering deficiencies are indicative of long-term, recurring problems that cannot be tied tothe competence or job performance of a singleindividual.
The Safety Board concludes that the BrightField owners’ oversight of testing and

59
maintenance of the vessel’s engineering systemswas inadequate and led to unreliableperformance of the engineering plant andcontributed to the shutdown of the mainpropulsion engine on the day of the accident.The Safety Board believes that ClearskyShipping Company should institute anengineering testing, maintenance, repair, andcompany oversight program for the Bright Fieldthat will ensure safe and reliable operation ofthe vessel’s engineering plant.
CommunicationQuite by chance, the Bright Field came to
rest between two docked ships in a space notsignificantly larger than the ship itself. Whilethe actions of the pilot and crew during theemergency may have been reasonable, theiractions were not well coordinated. Because acomputer simulation of the accident scenariowas inconclusive, the Safety Board could notdetermine how changes in the nature or timingof the crew’s actions may have affected theoutcome. The Safety Board therefore concludesthat insufficient information was available todetermine whether any actions taken by the pilotand crew of the Bright Field would have beeneffective in preventing the allision or mitigatingits effects. The Safety Board also concludes,however, that at several points prior to andduring the Bright Field emergency, the pilot,master, and crew of the vessel did not exchangeinformation that under other circumstancescould have prevented or at least mitigated theeffects of the accident.
In the view of the Safety Board, theperformance of the Bright Field pilot and crewcould have benefited from effective applicationof the principles of BRM, which entailseffective use of all available resources toachieve safe operations. The Safety Board haslong supported mariners’ use of BRMtechniques and has advocated professionaltraining in BRM.
Underlying effective BRM is anunderstanding that every officer, crewmember,and pilot on board a vessel is responsible foracting and for using resources in closecoordination with others on the watch. Themaster, pilot, and conning officer use leadershipskills and command authority to integrate the
resources for any given passage or watch. At thesame time, they must convey their receptivity tooperating information that originates withsubordinates. The role of those on the watch isto perform their assigned tasks responsibly, toknow about or participate in determining theplans for navigation of the vessel, to be alert todepartures from plans or from the expectedperformance of others, and to make thosediscrepancies known in time to avert anoperational error. The practice of BRM by pilotsand crew can be handicapped by intercultural orlanguage differences, but these can often beovercome by deliberate and clearmaster/pilot/crew briefings.
Master-Pilot Briefing at the Anchorage --The pilot of the Bright Field did not advise themaster of his plans for making the river transit,including the fact that he intended to operate theship at sea speed. Had the pilot offered, or hadthe master requested, information on the transitplans, not only would both men, as well as thebridge crew, have known when and where toexpect various actions, but the flow ofinformation could have enhanced coordinationand confidence between the pilot, master, andcrew.
If, for example, the master had asked, or thepilot had offered, information on the pilot’sintended transit speed, that issue could havebeen discussed, and together they could haveevaluated the operational consequences ofproceeding at sea speed. Navigational situationscan develop at any time for which an increase inspeed (to improve rudder control or avoidcollision) is a viable option, but, when a ship isalready operating at top speed, that option is nolonger available. If the pilot and master haddiscussed the intended speed, they could havereached a consensus on the best way to operate.
Although a discussion of intended actionscan take place at any time during a transit,predeparture discussions generally provide thegreatest latitude in both time and options. Apredeparture discussion also avoids some of thepractical logistical problems (related toobtaining another pilot) that could arise if aserious disagreement occurs between a masterand a pilot once a trip begins. Thus, discussingand agreeing on transit plans before gettingunderway is more efficient.

60
A transit plan should include intendedspeeds, areas of high risk due to trafficconcentration, shoreside structures, or river flowcharacteristics, and actions to be taken in theevent of various ship power or controldifficulties. According to their statements, eachman felt confident of his own abilities andassumed that the other was qualified to performany duties that might be required. The lack ofdiscussions between the master and pilotregarding emergency maneuvering proceduresdid not cause this accident. Still, if the actions tobe taken in an emergency had been established,cooperation and coordination in the emergencythat developed would probably have beenenhanced, tasks could have been clearlydelineated, and orders (such as the order to dropanchor) could perhaps have been given andcomplied with more quickly.
While the pilot was not forthcoming withinformation about his transit plans, the masterdid not tell the pilot of the inability to start themain engine from the bridge either at 1055 orwhen the same difficulty was encountered at1110. In each case, engine control had to betransferred to the engine control room and back,but this information was not made known to thepilot. Had the pilot been made aware of thesituation, he and the master could havediscussed options, including the location ofengine control (control room or wheelhouse) oruse of tug escorts. If the pilot and master couldnot agree, the pilot could have refused to getunderway from the anchorage.
Language Differences -- Even though theship’s master and crew were Chinese and spoketheir native language among themselves,interchanges between the crew and the pilottook place in English. The language differencebetween the pilot and the crew does not appearto have been a significant impediment tocommunications on the bridge.
The fact that the crew spoke Chinese amongthemselves, however, eliminated an adjunctsource of information for the pilot. For example,because conversations between master and crewwere in Chinese, the pilot was not aware of theengine starting difficulties, the content of thesecond mate’s conversation with the chiefengineer, or the master’s order to drop theanchor. Of course, critical operational
information should be clearly stated, and nooperations should depend exclusively onoverhearing a conversation. But the languagedifferences on the bridge, combined with thefact that the ship was sailing in restricted waters,made it even more important that the master andcrew convey all operations-related informationto the pilot. If the master and crew did not takethis initiative, then the pilot should havespecifically requested that he be kept informedof all activities and conversations on the bridgeaffecting vessel operation. Such ongoingcommunication did not occur on the bridge ofthe Bright Field.
Information Exchange During theEmergency -- If more information had beenexchanged during the brief period after powerreduction and before the allision, the actions ofthe pilot and crew could have been bettercoordinated and perhaps more timely. Eventhough the eventual outcome would probablyhave been the same in this case, in differentcircumstances, more effective communicationcould have helped avoid or mitigate an accident.
When the pilot noticed the cessation ofvibration in the vessel, he asked if there was aproblem. Even though he stated that neither themaster nor the mate responded, he did not ask asecond time. By not following up andattempting to determine the exact nature of theproblem, the pilot denied himself informationthat may have influenced the nature or thetiming of his navigational decisions and orders.
When the pilot realized that the vessel had,in fact, lost power, he again did not conversewith the master or mate. Consequently, he wasunaware of what they were doing or could do toaddress the problem. Although the master andthe mate were attempting to restore engine rpm,they did not tell the pilot of their actions.
A limited information exchange took placeamong the master, second mate, and chiefengineer. The master instructed the second mateto call the engine control room and demand animmediate increase in speed. The second matecomplied. In response, the chief engineer said heunderstood what had happened (a sudden dropin the pressure of the lubricating oil pump), butnot why it happened, and told the second mateso. He also told the second mate the

61
pressurization problem had already been solvedby the No. 2 pump coming on line. He thenasked if the second mate wanted to switchengine control from the bridge to the enginecontrol room. The second mate said yes, and thetransfer of control began.
During the postaccident investigation, themaster explained why engine control wastransferred. He said it was standard procedure togive the engineroom control whenever aproblem occurred that involved the engine, andthat under normal circumstances, the engine rpmcould be brought up more quickly from theengineroom. Following this normal procedurewould seem to make sense, since the masteracknowledged that he did not know the nature ofthe problem that caused the rpm reduction.However, the transfer of control takes 20 to 30seconds and must be completed before enginespeed can begin to be restored.
In this case, since the pressurizationproblem had already been corrected, the rpmcould have been restored from the bridge asquickly as from the engineroom. If that had beendone, the transfer time could have been saved.However, the second mate apparently did notrecognize the implication of the chief engineer’scomment, which was that the second engineercould increase rpm himself. So when the chiefengineer asked if engine control should betransferred, the second mate agreed. The secondmate was quite likely simply following themaster’s order to have “them” (the chiefengineer and his staff) increase speed. If thechief engineer had supplied information to thebridge about the time necessary for him toassume control and restore engine rpm, thisinformation may have altered the nature andtiming of the master’s and pilot’s orders.
The second mate also did not immediatelypass on the information about the lubricating oilrepressurization to the master. If he had, themaster may have recognized his option toincrease rpm from the bridge, and the normalpractice of sending engine control to the enginecontrol room in the event of engine-relatedproblems may not have been followed, therebysaving the control transfer time. Likewise, if thesecond mate had given the chief engineeradditional information about the direction inwhich the ship was headed, the chief engineer
could have made a more informed decisionconcerning the options for increasing rpm, suchas activating the crash maneuvering feature orperhaps not transferring engine control to theengine control room. After the accident, themaster testified that the engineering crew wasnot made aware of the emergency situation untilthe allision was unavoidable.
Had the above additional information beensupplied during these exchanges, it may nothave altered the outcome. Nevertheless,additional information should have beenexchanged to facilitate decisions.
Another information exchange between thepilot and master affected the order to dropanchor. During the accident sequence, the pilotfirst ordered the master to have someone standby the anchors and, later, to drop the anchors.The orders were heard and understood by themaster, though the pilot was unaware of thatbecause the master did not acknowledge eitherorder. The master attempted to carry out theorder to drop anchor, but his radiocommunications with the carpenter at the bowwere impeded by the sound of the ship’swhistle. The master did not tell the pilot of thecommunication problem created by the whistle;instead, he went out to the bridge wing and triedto attract the carpenter’s attention by waving hisarms. When this effort failed, the master triedthe radio again, finally establishing intermittentcontact. He still did not tell the pilot of hisdifficulties.
In the meantime, the pilot did not realizethat he was preventing his own order from beingcarried out by continuing to sound the ship’swhistle. Transmission of the order was delayedso long that when the master finally reached thecarpenter on the radio, he deemed dropping theanchor to be an inappropriate order andcountermanded it. By the time the masterdecided to drop the anchor, the carpenter couldmake only a brief effort to carry out the orderbefore having to flee to escape injury in theimminent allision. As a result, and as confirmedby an amateur video of the accident, the anchorwas not dropped before the Bright Field struckthe wharf.
The fact that the pilot issued the order todrop anchor indicates that he believed that some

62
value, however small, could be gained bydropping one or both anchors. Had he notbelieved that dropping anchors could mitigatethe emergency, he was obligated to relay thatinformation to the master so the carpenter couldbe told to abandon the anchor watch and removehimself to a safer position. Yet the pilot madeno real effort to determine if his order had beencarried out, even when he saw the master go tothe bridge wing and wave his arms. If he did notrecognize that effort as an attempt tocommunicate with the anchor watch, he shouldhave inquired about the meaning of the master’sunusual actions at such a critical time.
The lack of information exchange andfeedback on the part of the master is alsonotable. For example, he did not tell the pilotthat he had countermanded the drop-anchororder, only to reissue it a little later. Earlier inthe accident sequence, he did not ensure that thepilot was fully aware of the actions he wastaking to restore engine rpm. While the pilotcould have inferred the master’s actions fromthe rpm indicator, the master should haveremoved any ambiguity by advising the pilot ofwhat he was doing at all times. Likewise themaster could have given the pilot an estimate ofthe time it might take to restore engine power. Ifhe did not know the amount of time needed, hecould have asked the chief engineer. The pilotcould have used each of these pieces ofinformation as he determined which orders toissue at what time.
The need to exchange information andensure that orders are heard, understood, andcarried out is basic to the operation of anyvessel. These needs are not new and have longbeen familiar to mariners; however, they have inrecent years been formalized as central elementsof BRM. The Safety Board concludes that use ofBRM precepts on board the Bright Field wouldhave enhanced the exchange of information andthe coordination of actions among the pilot,master, and crew during the accident sequence.The Safety Board has issued severalrecommendations concerning BRM since 1991.Due in part to those recommendations and theefforts of the Coast Guard, the InternationalMaritime Organization (IMO) has issuedamendments to its Standards of Training,Certification and Watchkeeping thatincorporate BRM training for watch officers
effective February 1, 1997. A 5-year phase-inperiod (from February 1, 1997) to certifylicensed watch officers will follow. Signatorycountries are to have plans for such trainingprograms in place by February 1, 1998. Allsignatory countries, including the United Statesand Liberia (flag of the Bright Field), willrequire officers of vessels such as the BrightField to have BRM training. Pilots will not besubject to the same training unless they hold aCoast Guard license.
Training in BRM typically includes fivegeneric categories of knowledge and skilldevelopment: (1) the development and perform-ance of watch or pilot briefings; (2)maintenance of situational awareness; (3) identi-fication of error chains (and error trapping); (4)implementation of effective bridge/vessel com-munication; and (5) integration (coordination)of bridge/vessel resources. In whole or in part,most of theses elements were missing during theBright Field’s December 14, 1996, voyage.
The Safety Board believes that NOBRAshould encourage its members to participate ininitial and recurrent BRM training thatemphasizes team coordination between the pilotand crew. The Safety Board further believes thatClearsky Shipping Company should provide itsbridge and engineroom watchstanding officersand crewmembers with initial and recurrentBRM training that includes communication andcoordination between pilots and members of thebridge and engineroom watches and thataddresses their use of bridge and engineroomsystems.
Emergency ResponseAfter the allision, rescue efforts were
initiated at once, and emergency units wereordered. The harbor police dispatcher notifiedthe city of New Orleans Fire, Police, and Healthand Emergency Services Departments. Morethan 25 agencies responded; fire, police, andemergency medical service units arrived onscene within minutes. After being contacted bythe Gretna light operator, the Coast Guard beganan immediate search and rescue response. Inaddition to providing assistance throughmultiple city agencies, the city of New Orleanscontacted the Louisiana Office of Emergency

63
Preparedness to provide notification and requeststandby for possible assistance.
Passengers aboard the cruise ships and thegaming and excursion vessels, as well as severalRiverwalk Marketplace patrons, in response toSafety Board questionnaires recalled theemergency response as prompt and efficient.Although initial access to the area was hinderedby damage occurring when the Bright Fieldstruck the wharf, the emergency responderswere able to locate and use an acceptablealternate route to respond to the incident, assistthe injured, and provide crowd control. TheSafety Board concludes that the response to theBright Field accident by local emergencyresponse agencies was timely and appropriate.
Vessel Emergency Preparedness andEvacuation Plans
Four vessels were docked alongside thewharf in the area of the Bright Field accident:the Enchanted Isle, the Nieuw Amsterdam, theQueen of New Orleans, and the Creole Queen.In the view of the Safety Board, the actions ofthe captains and crews aboard the cruise shipsEnchanted Isle and Nieuw Amsterdam in themoments preceding the allision were adequatefor the circumstances. An emergency evacuationwas not attempted because of the limitedamount of time that elapsed from the firstawareness of the emergency until the BrightField passed clear of the two vessels.
Vessel Evacuation -- According to SafetyBoard surveys of passengers, when the firstmate of the Queen of New Orleans made theinitial evacuation announcement, somepassengers did not respond immediately. Whena second announcement was made ordering theimmediate evacuation of the vessel, passengersand nonoperating crewmembers began runningtoward the gangway. About this time, the BrightField struck the wharf and was continuing tomove toward the bow of the Queen of NewOrleans. Even though the bow wave from theBright Field’s approach destabilized the seconddeck gangway of the Queen of New Orleansseveral times during the evacuation process,passengers were not provided with analternative means of access to the dock.
According to the Queen of New Orleans’Emergency Evacuation Plan for MooredConditions, the vessel can be exited only fromthe bow section of the second deck. The planstates that to evacuate the vessel in anemergency, every passenger is to be directed tothis gangway. The owner of the vessel notedthat three portable emergency gangways, whichare designed to be used in the event the maingangway is inoperable, were aboard the vessel.The vessel’s emergency evacuation plan,however, does not refer to these portablegangways, or provide instructions on how tomake them operable in an emergency, or giveguidance for directing passengers to them. Theevacuation plan also does not take into accountthe time needed to alert the crew to take actionor for crewmembers to stage the portablegangways and ensure their safe operation.Because the emergency gangways were not usedduring the Bright Field accident, the only exitavailable was the second deck bow gangway.
New Orleans Paddlewheels, Inc., providedsecurity camera videotapes that show areas ofthe vessel being evacuated in what companyofficials call “a calm and orderly evacuation.”The Safety Board did not see, on these tapes,any passengers sustaining injuries during theevacuation. Nonetheless, some passengers wereinjured, as documented by medical records.While the Safety Board recognizes that thenumber of questionnaire responses was smallrelative to the number of passengers aboard thevessel, the responses are neverthelessmeaningful and illustrate the panic inducedwhen the crowd was confronted with no meansof escape from a vessel directly threatened by anoncoming freighter. Furthermore, had the vesselbeen filled to its capacity of 1,800 passengersand crewmembers, the number of personsunable to evacuate in time could have beensignificantly higher. The ensuing panic mostlikely would have been more hazardous,possibly resulting in a higher number of, andmore severe, injuries. The Safety Boardconcludes that evacuation of the Queen of NewOrleans was hampered, and passenger riskincreased, by the fact that only one gangwaywas made available for passenger egress duringthe emergency.
The Creole Queen, a New OrleansPaddlewheels, Inc., excursion vessel with a

64
capacity of 1,000 passengers and crew, wasdocked astern of the Queen of New Orleans. Atthe time of the accident, 190 passengers andcrewmembers were aboard. Following themaster’s instructions to evacuate, passengersexited the vessel across a single docksidegangway. When the bow wave from the BrightField passed the Creole Queen, the gangwaydropped from the side of the vessel, and threepassengers on the gangway fell into the river.One passenger was seriously injured; the othertwo sustained minor injuries. By this time,approximately one half of the Creole Queen’spassengers had been evacuated. The remainingpassengers could not exit the vessel until thegangway was repositioned.
The Safety Board acknowledges the effortsof the senior officers of both vessels to evacuatea large number of passengers. Even so, if the36,000-ton Bright Field had struck the Queen ofNew Orleans, the remaining passengers still onboard the gaming vessel, regardless of the exactnumber, would have been in grave danger.
The Safety Board believes that New OrleansPaddlewheels, Inc., must make better provisionsfor all its vessels in the event of an impendingallision or other emergency. Consequently, theSafety Board issued the following safety rec-ommendations to New Orleans Paddlewheels,Inc., on September 5, 1997:
Work with the U.S. Coast Guard toreview the Emergency Evacuation Planfor Moored Conditions of the Queen ofNew Orleans and amend it regardingcurrent evacuation procedures and thenumber of immediately accessiblegangways and disembarkation locations,to ensure timely and orderly exiting ofpassengers in the event of emergencyevacuation. (M-97-62)
Work with the U.S. Coast Guard todevelop and implement procedures forevacuation under moored or dockedconditions for all your excursion vesselsto ensure that passengers can exit eachvessel in a timely and orderly mannershould an emergency evacuation benecessary. (M-97-63)
In a September 29, 1997, letter to the SafetyBoard, New Orleans Paddlewheels, Inc., repliedthat its emergency evacuation plan for theQueen of New Orleans in moored conditions
addresses the evacuation of all areas onboard the vessel. We purposely did notinclude portable gangways because theyare to be used only when the primaryevacuation gangway is inoperable. Ourdeck crew is regularly trained anddrilled on how to use these portablegangways in multiple locations.
Portable gangways were not used in thisemergency. The Safety Board is concerned thatthe evacuation plan for the Queen of NewOrleans does not provide a readily availableadditional means of escape that does not requirestaging in an emergency. The Safety Board’sintent in issuing Safety Recommendation M-97-62 was to prompt New Orleans Paddlewheels,Inc., to amend the Queen of New Orleans’sEvacuation Plan for Moored Conditions notonly to enhance evacuation procedures, but alsoto address the need to provide for more than oneimmediately accessible disembarkation locationto ensure a timely and orderly exiting ofpassengers.
Further, although the September 29 letterstates that the deck crew is trained and drilledon use of the portable gangways, the letter doesnot address the training of the nonoperatingcrewmembers, who are responsible for assistingpassengers to the egress areas of the vesselduring emergencies. The Evacuation Plan forMoored Conditions provides no guidance on theuse of portable gangways to the numerousnonoperating crew on board the vessel who areresponsible for directing passengers andassisting their escape. Moreover, the specificplan to which all crewmembers are to look forguidance in responding to emergency situationsdoes not provide any information on thesegangways or how to guide passengers to them.Based on the failure of New OrleansPaddlewheels, Inc., to effectively address theseconcerns, the Safety Board classifies SafetyRecommendation M-97-62 “Closed--Unacceptable Action.” New OrleansPaddlewheels, Inc., has not responded to SafetyRecommendation M-97-63 concerning thedevelopment of evacuation procedures for

65
moored or docked conditions for all itsexcursion vessels. Therefore, SafetyRecommendation M-97-63 remains classified“Open--Await Response.”
The Safety Board, also on September 5,1997, issued the following safety recommenda-tion to the Coast Guard:
Work with New Orleans Paddlewheels,Inc., to review and amend the Emer-gency Evacuation Plan for MooredConditions of the Queen of NewOrleans regarding current evacuationprocedures and the number of immedi-ately accessible gangways anddisembarkation locations, and todevelop and implement procedures forevacuation under moored or dockedconditions for all New Orleans Paddle-wheels, Inc., excursion vessels to ensurethat passengers can exit each vessel in atimely and orderly manner should anemergency evacuation be necessary.(M-97-59)
In a November 18, 1997, letter, the CoastGuard responded that the New Orleans COTPhad already required a review of evacuationprocedures for all high-capacity gaming vessels,but that the Coast Guard believes this safetyrecommendation should be expanded to coverall passenger vessels operating in theMississippi River in the New Orleans area. Theletter stated the Coast Guard’s belief that,
It would be prudent to developreasonable, practical and appropriateevacuation criteria for the differenttypes of passenger vessels based upontheir type, configuration, passenger andcrew capacity, and the extent whichpassengers are normally aboard thevessel while dockside. To this end, wehave discussed the expansion of thisrecommendation with Captain of thePort New Orleans and will requirefurther review and development of thisinitiative.
The Safety Board is pleased that the CoastGuard has not only addressed the specific intentof Safety Recommendation M-97-59 regardingthe Queen of New Orleans, but has also
expanded the scope of the recommendation tocover all high-capacity passenger vesselsoperating within the Port of New Orleans. Whilethe Coast Guard response does not specificallyaddress evacuation plans for New OrleansPaddlewheels excursion vessels, the SafetyBoard notes that these vessels will be coveredby the evacuation criteria the Coast Guard plansto develop for all passenger vessels operating inthe New Orleans area of the Mississippi River.Pending further information from the CoastGuard regarding the proposed review ofevacuation plans for such vessels, andspecifically those vessels belonging to NewOrleans Paddlewheels, Inc., the Safety Boardclassifies Safety Recommendation M-97-59“Open--Acceptable Response.”
Emergency Drills -- The companyoperating manuals and station bills for both theQueen of New Orleans and the Creole Queenclearly stated that nonoperating crewmemberswere responsible for distributing life jackets,keeping order in the stairways and passageways,and controlling the movement of passengers toensure their safety. During the Bright Fieldemergency, however, several nonoperatingcrewmembers experienced difficulty inperforming their duties. For example, when thefirst mate directed the crewmembers to go totheir mooring stations during the evacuation ofthe Queen of New Orleans, the vessel’s directorof security did not understand or appreciate theimplications of this announcement. Also,nonoperating crewmembers did not distributelife jackets to passengers aboard the CreoleQueen during the emergency.
Drills held aboard the Queen of NewOrleans had not simulated an evacuation whilemoored. Moreover, the drills and trainingsessions that were held involved onlysupervisory gaming staff, who were expected toinform other gaming staff crewmembers of theircontent. No formal methods were used to verifywhether the nonoperating crewmembers wereadvised of the content of the safety meetings orthe nature of drills performed. Unless it requiresaccountability for the flow of safety informationfrom supervisory gaming staff to the rest of thenonoperating staff, management cannot ensurethat the latter receive safety information thatcould be critical in an emergency. The SafetyBoard concludes that nonoperating crewmem-

66
bers of the Queen of New Orleans and theCreole Queen had not received training coveringthe full range of emergency scenarios and wereunprepared to properly carry out theirresponsibilities in this accident.
As a result of its investigation of a 1994 fireaboard the small passenger vessel ArgoCommodore,43 the Safety Board issued thefollowing recommendation to the PassengerVessel Association (PVA):
Develop and provide to your memberscrew drills for on-board crew emer-gency procedures/standards that includepreincident planning for a variety ofshipboard emergencies, including fires,and the deployment of crew resourcesfor proper response to the emergencywithout compromising passenger safety.(M-95-43)
This recommendation was later placed onthe Safety Board’s list of Most Wanted SafetyImprovements. In 1997, the PVA made availableto the Safety Board its recently publishedTraining Manual for Passenger Vessel Safety,which incorporates a “Non-marine Crew Train-ing” section that outlines a comprehensivetraining program for nonoperating crewmem-bers. The introduction to this section states thatspecialized safety training for nonoperatingemployees “makes sense when managementrealizes that, more often than not, [theseemployees] will be the first person[s] on thescene in any kind of emergency.”
Based on the PVA’s support for the conceptof comprehensive training for nonoperatingemployees and its development of the trainingmanual, the Safety Board classified SafetyRecommendation M-95-43 “Closed--AcceptableAction.” The Safety Board notes that NewOrleans Paddlewheels, Inc., which is a PVAmember, has apparently not yet implementedthe training program for nonoperatingcrewmembers set forth by the PVA in itstraining manual. The Safety Board believes thatNew Orleans Paddlewheels, Inc., should, in
43Marine Accident Report--Fire Aboard U.S. SmallPassenger Vessel Argo Commodore in San Francisco Bay,California, December 3, 1994 (NTSB/MAR-95/03).
accordance with the guidance published by thePVA, require that nonoperating crewmemberson all its vessels participate in formalemergency training and drills in the properhandling of emergencies that have the potentialto affect the persons in their charge. Thecompany should also maintain written records toverify nonoperating crew proficiency levels andskill retention.
Safety Briefings and Signage -- Accordingto the vessel master, when the Queen of NewOrleans was to remain moored, he did not makeany safety announcements because he believedthe vessel was an extension of the dock whennot underway. The Queen of New Orleansbroadcast a vessel safety videotape throughoutthe vessel’s queuing area; however, a significantnumber of passengers on board the vessel on theday of the accident, some of whom had been onthe vessel several times before, did not recallever having seen or heard the safety broadcast.Because the scheduled cruise had been canceledowing to the high river stage, no safety briefingswere provided prior to the Bright Field accident.However, the master stated that he hadinstructed the engineer to start the engines toprepare for leaving the dock to avoid beingstruck by the Bright Field. Had the vessel leftthe dock, the master probably would not havehad time to provide passengers with such basicinstructions as the location of life jackets.
The Safety Board concludes that the lack ofeffective recurring safety briefings foroccupants of the Queen of New Orleansregarding emergency and evacuation proceduresmay have contributed to the confusion and panicreported among passengers and crew during thevessel evacuation. The Safety Board believesthat New Orleans Paddlewheels, Inc., shouldreview the existing methods of providing safetyinformation to boarding passengers and makethe necessary improvements to ensure that allvessel occupants receive recurring safetybriefings, regardless of whether the vessel isscheduled to leave the dock.
Emergency instruction placards and signaboard the Queen of New Orleans were notconspicuously displayed and were not readilyvisible during the emergency. The safetyinstructions, printed on plain white paper withclear laminate, were subject to destruction in an

67
emergency such as that involving fire.Moreover, the paper on which the instructionswere printed was similar to the color of thewalls upon which they were affixed, negatingtheir effectiveness in an emergencycharacterized by haste, panic, or reducedvisibility. According to a number of the vessel’spassengers on the day of the accident, they didnot see emergency instruction signage or egressdiagrams.
The Safety Board concludes that theinstruction placards and signage aboard theQueen of New Orleans were ineffective indisseminating emergency instructions and vesselinformation to passengers. The Safety Boardtherefore believes that New OrleansPaddlewheels, Inc., should post, on all itsvessels, emergency instructions that are printedon fire- and heat-resistant material and that areclearly visible to all passengers both undernormal conditions and during emergencies whenlighting and visibility may be diminished.
Shoreside Emergency Alert andResponse -- Under River Front Alert Networkprocedures established after this accident,individual riverfront commercial propertieswere to make their own determinations aboutthe proper actions to be taken after receivingnotification of an emergency involving a vesselon the river. According to evacuation plans thatwere initially in effect for property tenants, alengthy procedural chain of command was inplace that could delay a decision to evacuate. Inthe view of the Safety Board, such a potentialfor delay could endanger the employees andpatrons of riverfront properties. Therefore, onSeptember 5, 1997, the Safety Board issued thefollowing safety recommendation to the NewOrleans Dock Board:
Develop, as part of the River Front AlertNetwork, an emergency evacuationannouncement for broadcast by theharbor police department dispatcherusing a public address system linked toriver front properties that provides for atimely and efficient evacuation in theevent of an impending collision or otheremergency. (M-97-60)
Documentation received by the SafetyBoard on November 3, 1997, outlining the
actions to be taken in the event of the activationof the River Front Alert Network appears toaddress the Safety Board concerns thatprompted the issuance of SafetyRecommendation M-97-60. Under the specificevacuation protocols developed for respondingto the activation of the River Front AlertNetwork, the procedural chains of commandwithin each property’s evacuation plans havebeen eliminated, and property security officershave been given authority to initiate anevacuation immediately upon hearing a RiverFront Alert Network broadcast and assessing thedanger. Because these revised evacuation plansmeet the intent of the safety recommendation,the Safety Board classifies SafetyRecommendation M-97-60 “Closed--AcceptableAction.”
The River Front Alert Network system didnot require that vessels docked or moored in itsvicinity monitor the alert broadcast from theCoast Guard traffic light operator to the harborpolice dispatcher indicating a vessel irregularityor loss of steering in the vicinity of theriverfront properties. The Safety Board wasconcerned that, unless these vessels monitoredthe network for emergency broadcasts, vesseloccupants would be subject to delays innotification similar to those that occurred in thisaccident and that contributed to the disorderlyevacuation and numerous injuries. Therefore, onSeptember 5, 1997, the Safety Board issued thefollowing safety recommendation to the NewOrleans Dock Board:
Require all vessels which dock or moorin the area encompassed by the RiverFront Alert Network to monitor theRiver Front Alert Network radio for anyemergency broadcast to provide maxi-mum advance notice of an emergency.(M-97-61)
In a September 15, 1997, reply to the SafetyBoard, the Dock Board said that the intent ofthis safety recommendation should be met bythe postaccident COTP order requiring that alllarge passenger vessels docked in the area havea manned pilothouse and that they monitor allemergency and working marine channels. Whileagreeing that monitoring working andemergency radio channels should give mooredpassenger vessels advance warning of

68
potentially hazardous situations on the river, theSafety Board noted that the COTP orderrequiring such monitoring was an interim, andpossibly temporary, measure. The Coast Guardhas since published an interim rule that, whenissued as a final rule, will make permanent theCOTP order. In anticipation that the interim ruleregarding manned pilothouses and radiomonitoring will become permanent as 33 CFR165.810(e), the Safety Board classifies SafetyRecommendation M-97-61 “Closed--No LongerApplicable.”
Also on September 5, 1997, the SafetyBoard issued the following safety recommenda-tion to the Coast Guard:
Require that all commercial vessels thatoperate within the River Front AlertNetwork zone participate in the networkand notify the U.S. Coast Guard trafficlight operator whenever they experiencean irregularity or abnormality that couldresult in a safety risk to the Port of NewOrleans area. (M-97-58)
In its November 18, 1997, letter to theSafety Board, the Coast Guard stated thatexisting regulations and local marine practiceare now serving to meet the intent of this safetyrecommendation. The letter stated that,
[Title] 33 CFR 160.215 requires vesselsto immediately notify the nearestMarine Safety Office or Group ofhazardous conditions aboard or causedby the vessel. Currently, the vessels inthe vicinity of the traffic light notify thetraffic light operator who is responsibleto the Marine Safety Office. Through 33CFR 26.03 or existing Captain of thePort orders, ALL vessels, includingmoored passenger vessels, must monitorChannel 67 VHF. Therefore, when ahazardous condition is reported to thetraffic light operator, he activates theRiverfront Alert Network by calling theHarbor Police on the Network radio.The police then notify the impactedparticipating facilities and vessels.Between the Channel 67 notificationsand subsequent Riverfront AlertNetwork radio calls, ALL vessels andfacilities are notified.
Based on this response, the Safety Boardclassifies Safety Recommendation M-97-58“Closed--Acceptable Action.”
Toxicological TestingTwo Coast Guard regulations (33 CFR Part
95 and 46 CFR Part 4) require that postaccidentalcohol tests be conducted on the pilot andBright Field crewmembers directly involved inthis accident. Those regulations specify thatmarine employers or their representatives are toensure that urine specimens (for drug testing)and breath or blood specimens (for alcoholtesting) are obtained as soon as is practicablefollowing an accident.
In this case, the self-employed pilot suppliedboth breath and urine specimens in a timelymanner. His specimens were negative foralcohol and drugs. Bright Field crewmembersalso supplied breath and urine specimens, andthe results were negative.44 The Safety Board isconcerned, however, that breath testing, whichis a time-sensitive procedure, was not conductedin a timely fashion on some Bright Fieldpersonnel and, in fact, was conducted too late tohave any practical value. Because of the rate atwhich humans metabolize alcohol,45 evidence ofalcohol consumption is usually eliminated fromthe body in about 8 hours. For example, anindividual could be legally intoxicated (0.10percent BAC) at the time of an accident andhave a 0.00 percent BAC about 8 hours later.Consequently, to produce meaningful results,testing should occur within that time span.
In this case, tests of the master, chiefengineer, and helmsman were conductedbetween 7 hours and 57 minutes and 8 hours and30 minutes after the accident. Given that amountof time, it cannot be clearly determined throughthese tests whether alcohol had a role in thisaccident, although no other informationsuggested that alcohol was a factor. On thecontrary, the first Coast Guard investigatoraboard observed the crew by sight, sound, and
44The results of the alcohol tests on the pilot and ninecrew members showed .000 percent BAC.
45The elimination rate ranges between about .015percent and .020 percent per hour.

69
smell for signs of alcohol or other impairmentand found none.
Postaccident testing could have begunsooner. The ship’s agent learned of the accident1 hour and 20 minutes after it occurred, and heand the ship’s attorney were aboard in about 21/2 hours. The first Coast Guard investigatorwent aboard 2 hours after the accident, and anhour later (3 hours after the accident), heordered the ship’s attorney to have the crewtested. Either of them could have facilitatedinitiation of the testing process. Instead, theship’s agent general manager came aboard 3 1/2hours after the allision and was there for anotherhour before he arranged for testing. Tests werenot started sooner because the general managererroneously thought the Coast Guard wouldmake the arrangements. Further delay wasincurred in locating someone to conduct thetests, which finally began 6 1/2 hours after theaccident. Each of these delays diminished thevalue of the tests. Further, by conducting thebreath tests of the helmsman, master, and chiefengineer last, 8 hours or more after the accident,the value of those tests was essentially negated.
Besides arranging for the testing, the agenthad to decide whom to test. The regulationsstate that he should do so by determining whowas directly involved in the incident. The shipagent’s decision was to test all crewmembersassigned to the noon watch, which was on dutyat the time of the allision. However, the ship’scarpenter, who was acting as the anchor watch,was not tested. He was apparently inadvertentlyoverlooked for testing because he was notregularly assigned to the noon watch. Since notesting of the carpenter was done, no definitiveconclusions can be made about drugs or alcoholwith respect to his activities, though as with theother crewmembers, no information wasobtained that would suggest that either had arole.
Arrangements for and timing of the alcoholtesting illustrate several problems. For example,the Coast Guard investigator was fully aware ofthe agent’s responsibilities, but the agent wasnot. Time was lost until the agent became fullyaware. Additional time was lost while aqualified tester was contacted and broughtaboard. Also, the regulations themselves do notadequately address the physiological need to
conduct alcohol testing within 8 hours if theresults are to be meaningful.
The Safety Board has observed these sameproblems in previous accidents, and severalpotential solutions exist. One recent accidentinvolved the vessel Julie N, which struck abridge support in Portland, Maine, on December4, 1996. Because the problems and solutionsassociated with the timing of postaccident drugand alcohol testing were explored in a March13-15, 1997, public hearing on that accident andwill be comprehensively addressed in the SafetyBoard’s upcoming Julie N accident report, theyare not further discussed here.
Risk Assessment and Risk ManagementThis accident demonstrates that the many
and diverse stakeholders in the area of the Portof New Orleans, including the Coast Guard, theState of Louisiana, the Dock Board, the pilotorganizations, and the owners and operators ofriverfront properties and nearby mooredpassenger ships, did not adequately prepare foror mitigate the risk of a marine casualtyaffecting people and property within the Port ofNew Orleans. Some of the stakeholders, mostnotably the Dock Board, had commissionedpartial risk assessment studies at various timesfor the assets in the harbor area. Despite theirlimitations (in either geography or scope), thesestudies did provide adequate information for thestakeholders to recognize the possibility of anaccident similar to the one involving the BrightField.
For example, risk assessment projectspredicted an increase in accidents involvingcollisions, rammings, and groundings due toincreased river traffic. The Louisiana StateUniversity risk assessment project, in 1994,concluded that no sections of the Port of NewOrleans waterfront were free of ship allisions,including the area where the high-capacitypassenger vessels, gaming vessels, andriverfront properties were located. Analysis ofaccident data for the Port of New Orleans from1983 through 1993 (a total of 166 rammingsalong the left descending bank between miles 91and 101 AHP) identified a mooring area forgaming vessels that had seen the fewest“historical allisions on the left bank.” The studyacknowledged, however, that no area of the left

70
descending bank of the river had beencompletely free of vessel strikes during the 11-year period studied.
Port stakeholders did take risk managementinitiatives such as providing barriers andcontrols for some of their assets. At the time ofthe planning for the Louisiana world’s fair in theearly 1980s, a proposal was made to tie upbarges (exhibit pavilions with large numbers ofpatrons or visitors) along the riverfront fair siteat the location now occupied by the RiverwalkMarketplace. The Dock Board rejected the plan.The Audubon Institute, as a result of apreconstruction risk assessment in 1987,decided to construct the Aquarium of theAmericas some 100 feet behind the levee so thatit would be safe from vessel strikes. Morerecently, the mooring areas for the gaming,excursion, and ferry vessels were silted in topossibly protect these vessels from ramming byother ships.
Despite this history of some sensitivity torisk within the port area, the Riverwalkcomplex, including the condominium garageand the Hilton Hotel Riverside, wereconstructed on old warehouse piers on the riverside of the levee. This location offered no“crush zone” that could absorb the impact of amarine ramming, and despite the fact that thepiers themselves were not built to withstandbeing struck by a heavy vessel, no physicalbarriers were constructed outboard of the newbuildings to offer them protection. According tothe IRC, during the time when the IRC wasnegotiating a lease with the Dock Board, theDock Board advised the IRC that vessels hadhad allisions with wharves within the Port ofNew Orleans, but no allisions had occurred atthe Lower Poydras Street wharf. The IRCrepresentatives were shown photographs of theallisions at other wharves, but these photographsdepicted only minimal damage. The IRCapparently did no further risk assessment, andneither the initial construction of the mall northe initial construction of the riverside portionof the Hilton Hotel resulted in any new structureextending farther into the Mississippi River.Rather, these structures were built entirely ontop of existing wharves.
In contrast, the 1987 Audubon Institute-sponsored risk assessment similarly determined
that there had been few allisions at the BienvilleStreet wharf and that because it is high up in thebend, it faced low risk of being struck by anoutbound vessel. Nonetheless, recognizing lowincidence, but a potential for high consequences,the Audubon Institute placed the Aquarium ofthe Americas behind the levee with a 100-footbuffer zone to protect the shoreside structure.No similar safety feature was considered orconstructed for the Hilton Hotel or theRiverwalk Marketplace.
The IRC obtained construction permits forthe riverside expansion of the hotel from the cityof New Orleans, the Corps of Engineers, and theNew Orleans Levee Board. In addition, theconstruction plans were approved by the DockBoard. According to the Dock Board, it maymake recommendations to the IRC or otherstakeholders in the area to widen the wharf, toallow silt to accumulate, or to further increasethe robustness of construction in the areaimmediately outbound of their structures;however, it has no authority to compel suchaction. Currently, the damaged portions of theRiverwalk Marketplace mall, the parking deck,and the Hilton Hotel are being rebuilt in thesame location. No physical barriers have beenincluded in the rebuilding of these facilities. Aswith the initial construction, all permits weregranted, and all plans were approved.
Given the hazardous operating environmentin the Port of New Orleans and the number ofinstances of loss of propulsion and steering, anynumber of which could have resulted in similaraccidents or far more serious ones, the SafetyBoard does not understand the property owners’reluctance to provide adequate barriers toprotect their assets in the port area. Although theRiver Front Alert Network is a commendableeffort to alert the harbor police and securityofficers in the event of a need to evacuate thearea, such efforts are unlikely to result in acomplete evacuation under even slightlydifferent circumstances. For example, the BrightField rammed the Hilton Hotel during daylighthours when, fortunately, few guests wereoccupying rooms and no cleaning personnelwere in the immediate area. Had this accidentoccurred during the evening, at night, or in themorning hours, most of the rooms wouldprobably have been occupied. It is unlikely thateven the River Front Alert Network would have

71
been able to awaken the sleeping guests, alertthem to the danger, and evacuate them in time toprevent serious injury or possible death.
The Safety Board is concerned that, despitethe historical record of marine incidents andaccidents in that section of the MississippiRiver, the Dock Board permitted the placementof a commercial facility within about 20 feet ofan unprotected wharf. More than 13,500 peoplea day visit the Riverwalk Marketplace. Thosevisitors have a reasonable expectation that thePort of New Orleans will assert its responsibilityto protect their safety by exercising the power todisapprove a building plan that does notadequately account for a known risk. The SafetyBoard concludes that the IRC and the DockBoard did not conduct adequate risk assessmentnor perform adequate safety managementoversight to protect their properties and thepeople that use them from an allision such asthat involving the Bright Field.
While the construction of a shopping malland a hotel in such a high-risk area was ill-advised, the Safety Board recognizes thateconomy and practicality argue againstattempting to correct the error by relocatingthose facilities. Nonetheless, the Bright Fieldaccident highlights the risk to shoresidestructures within the Port of New Orleans andthe need to consider that risk in the approvalprocess for future construction there. The SafetyBoard believes that the Dock Board, as part ofthe permit-approval process for new commercialand residential development along the wharveswithin its jurisdiction, should require that anynew construction of occupied space be sitedbehind a buffer zone sufficient to protectpersons and property by safely absorbing theimpact should a vessel strike a wharf.
After this accident, the Dock Board, ineffect, identified a buffer zone for the RiverwalkMarketplace. The Dock Board “encouraged” theIRC to widen the Upper Poydras Street wharf by50 feet. The company had already widened thewharf by that amount in one area toaccommodate a gaming vessel, and the DockBoard suggested that the remainder of the wharfbe extended as well. The Safety Board concursin this suggestion and believes that the IRCshould enhance the safety of the patrons andemployees of the Riverwalk complex by
immediately undertaking to widen, by aminimum of 50 feet, that length of the PoydrasStreet wharf that has not previously beenextended. Such an extension prior to thisaccident would have added a “crush zone” thatwould probably have prevented the structuraldamage and threat to persons that resulted fromthe Bright Field accident.
Several passenger vessels, includinggaming, tour, and cruise vessels, were allowedto dock along the left descending bank, the sideof the river at highest risk. Had the Bright Fieldlost power some time later and the sameaccident scenario evolved, the ship would likelyhave rammed the gambling vessel, resulting insubstantial loss of life. The cruise vessels, whichhad even less warning time, would quite likelyalso have sustained serious passenger injuries orloss of life.
While silting around the vessels’ dockingareas may offer some protection from rammingby deep-draft vessels at average river stages, thesilt layer did not reduce water depth sufficientlyto retard a runaway ship when the river washigh, as it was on the day of the Bright Fieldaccident, nor did it protect the moored vesselsfrom ramming by shallow-draft vessels such astows and barges. The Safety Board is not awareof any engineering evaluations conducted toassess the effectiveness of the silting efforts.
The property owners and other stakeholderswithin the Port of New Orleans clearly had theresponsibility to establish and maintain areasonable level of safety in the port area. TheSafety Board concludes that the Coast Guard,the Dock Board, and the property owners didnot adequately address the risks posed tomoored vessels along the Erato, Julia, Poydras,and Canal Street wharves; as a result, undercertain conditions, those vessels were vulnerableto ramming by other marine traffic. The SafetyBoard believes that the Coast Guard and theDock Board should reassess the risk of locatingpassenger vessels along the left descending bankof the Mississippi River and determine whetherto remove the vessels to a less vulnerablelocation or put in place procedural, operational,or physical barriers that will protect them fromramming by riverborne traffic.

72
Additionally, no tugboats were used eitheras escorts or as a “barrier” to prevent a runawayship from ramming the shore or colliding withanother marine asset. And no environmentalcontrols, such as the Corps of Engineers’opening of the Bonnet Carré Spillway, were putin place to reduce river flow or current.
On the river itself, the Bright Field wasoperating at full speed in high-river and high-current conditions. Apparently, neither the pilotnor crew considered procedures that might beemployed to maximize the time available torespond to an emergency. For example, the mainengines were being operated in bridge control,and although this may have created a timepenalty in responding to an emergency, the pilotand bridge crew did not discuss engine controllocation prior to commencing the tripdownriver. In his testimony, the pilot claimedthat it was necessary to operate the Bright Fieldat maximum speed to attain reasonablemaneuverability of the vessel in the operatingenvironment of high water, rapid current, and aheavily laden ship designed to be maneuverableat lower speeds.
Several days after the accident, SafetyBoard investigators boarded a fully loadedvessel of similar size, displacement, and powerto the Bright Field that was operatingdownbound in similar high water conditions.During this transit, the pilot did not use fullspeed to maneuver the ship. Each ship handlesdifferently, but the operation of the Bright Fieldat full speed left no margin for error. Forexample, the main engine tripped off linebecause of a temporary loss of lubricating oilpressure. The oil pressure and engine operationwere restored within about 2 minutes, which is areasonable amount of time. However, operatingat full speed in high-river conditions, the shiphad no room to maneuver out of the emergency.The Safety Board concludes that operating avessel at full speed in the restricted waters of theMississippi River may not allow sufficient timeor distance to recover from an emergency. TheSafety Board believes that the Coast Guardshould take the lead in working with the pilotassociations serving the Port of New Orleans toevaluate the impact of operating vessels at fullspeed in the Mississippi River and incorporatethat information in its risk-management andrisk-reduction strategies for the port area.
High-river conditions are repeatedly cited ascause for concern. For example, various portrisk assessments cite local experts, in interviewsand in response to questionnaires, clearlyexpressing that high river stage is an importantfactor in river casualties. This opinion isstrongly supported by available data. Elevenyears of casualty data from the Port of NewOrleans and the Coast Guard clearly show aseasonal trend to river casualties. The highwater months of February, March, April, andMay experience two to three times the casualtiesthat occur during the low-water months of Julythrough October.
In addition, the studies point out that theCoast Guard acknowledges the fast MississippiRiver current and low seasonal watertemperatures as creating a very hostileenvironment. No matter how many Coast Guard,State, local, and other resources respond to acasualty involving a large number of persons inthe water, it would be difficult to rescueeveryone. The Coast Guard 1994 search andrescue exercise lead to the conclusion that,under adverse conditions, the Coast Guard couldexpect to rescue and save only a smallpercentage of the people in the water. Thisfinding should be unacceptable to the CoastGuard and the Port of New Orleans, and the twoagencies should consider alternative means todeal with this emergency. For example, prior tothe Bright Field accident, the Bonnet CarréSpillway had only been opened seven times toalleviate high water conditions, apparentlybecause of the cumbersome and lengthy tasksnecessary to do so. Nonetheless, the risksassociated with high water and rapid currentwere considered “unusual” enough that inMarch 1997, the spillway was opened for theeighth time. The Port of New Orleans, the CoastGuard, and the Corps of Engineers mightconsider more aggressive use of the BonnetCarré Spillway to alleviate these high waterconditions and to deal with the safety issuescreated by them. Further, if the majorimpediment to opening the spillway is the timeand effort it takes to do so, it may be appropriatefor the Corps of Engineers to consider ways tomake the spillway more usable and to employ itfor risk mitigation as well as for flood control.
No practical physical barrier aboard shipexists that will safely stop a runaway vessel. In

73
such an emergency, a safe outcome depends onthe successful interaction of several physicaland operational factors. For example, if mainengine power is lost, adequate steering canusually be maintained until the ship slowsenough for the anchors to be dropped. If a vesselloses its steering, engine power can be used toeither slow the vessel (astern power) or, if it is atwin-screw vessel, to maneuver the ship.
Anchors are perceived as providing somelevel of protection by serving as “brakes” thatwill stop or at least slow a ship. But anchors areneither designed nor adequate for stopping aheavily loaded ship traveling at high speed. Hadthe Bright Field’s anchors been released, theanchor chain would quite likely have payed outat a speed that could not be controlled by thewindlass brake, and the chain would simplyhave continued to run out until it parted fromthe ship. In this accident, the dropping of theanchor and paying out of chain could not havebeen expected to significantly slow, let alonestop, the ship.
Since this accident, the Coast Guard hasplaced renewed emphasis on having anchors atthe ready (backed out of the hawsepipe,disengaged from the windlass, and being held bythe brake), with a two-person forecastle watch.While having the anchors manned and at theready may prove beneficial in certaincircumstances, it is unlikely to achieve anythingmeaningful aboard a heavy vessel operating atrelatively high speeds in the Mississippi River.Further, “increased emphasis” on having theanchors at the ready may even provide a falsesense of security without effectively addressingthe dangers inherent in operating heavy vesselsat high speed in proximity to shoresidebusinesses and passenger vessels.
The notable characteristic of all previousrisk assessment studies commissioned by theCoast Guard or the Dock Board was theirlimited scope. Most were conducted in light ofspecific proposals, such as the addition ofgaming vessels to the port. Investigatorsdetermined that no comprehensive study hasbeen done that considers all types of risks to allport properties and people. The Safety Boardconcludes that the stakeholders within the Portof New Orleans, including Federal, State, andlocal agencies; private commercial entities;
shipowners; and pilot associations have notdetermined the overall level of risk associatedwith the full range of activities within the portarea and have not provided adequate protectionfor persons and property in that area.
The Coast Guard has overall responsibilityfor maintaining public safety in the Port of NewOrleans area. Under the Ports and WaterwaysSafety Act of 1972, the Congress charged theCoast Guard with monitoring and managing riskin all U.S. ports and taking actions to maintainrisk at an acceptable level. In carrying out thisrole, the Coast Guard must assess and managethe risk that is inherent in all commercialactivities within U.S. ports. In fact, in its 1996Performance Report, the Coast Guard’s Officeof Marine Safety and Environmental Protectionasserts that managing risk is its primary mission.The Safety Board concurs with this assessmentand notes that the Coast Guard has the authority,the responsibility, and the experience to direct acomprehensive assessment of risk in the Port ofNew Orleans.
The Safety Board believes that the CoastGuard, with the cooperation of all stakeholderswithin the Port of New Orleans, should conducta comprehensive risk assessment that considersall activities, marine and shoreside, within theport area. In addition to those risk factorsdiscussed earlier, this assessment shouldconsider the risks to people and property,including shoreside businesses and passengervessels, that are associated with relatively high-speed navigation of the river, high river stageand rapid river current, railroad and highwaybridges spanning the waterway,46 and thecarriage of cargoes such as bulk oil or otherhazardous materials or chemicals that can causepollution, fire, or explosion.
The Safety Board notes that many of therisk factors associated with river commercewithin the port area have already been identifiedin previous risk assessment studies and, further,that these factors may be amenable to knownrisk-reduction or risk-mitigation initiatives.
46For more information, see Highway-MarineAccident Report--U.S. Towboat Chris Collision with theJudge William Seeber Bridge, New Orleans, Louisiana,May 28, 1993 (NTSB/HAR-94/03).

74
Such initiatives might include reducing vesselspeed, opening the Bonnet Carré Spillway on amore regular basis, using tugboats either asescorts or as a “barrier” to protect marine assets,adequately assessing the protection afforded bysilting-in of vulnerable areas, and moving thepassenger vessels to a safer location. The SafetyBoard believes that the Coast Guard should, incooperation with the appropriate stakeholders,including Federal, State, and local agencies;private commercial entities; shipowners; andpilot associations, implement risk-managementand risk-mitigation initiatives that will ensurethe safety of people and property within the Port
of New Orleans. The Safety Board furtherbelieves that the Corps of Engineers, the Stateof Louisiana, the Dock Board, the IRC(including the New Orleans Hilton RiversideHotel), New Orleans Paddlewheels, Inc., theNew Orleans Baton Rouge Steamship PilotsAssociation, the Crescent River Port PilotsAssociation, and Associated Federal Pilots andDocking Masters of Louisiana, Inc., shouldparticipate with other stakeholders in institutingrisk management and mitigation initiatives thatwill ensure the safety of people and propertywithin the Port of New Orleans.

75
Findings1. The following factors were not causal or
contributory to the accident involving theBright Field: weather, fatigue, malfunc-tioning of either the vessel’s steering gear orequipment on the bridge, alcohol or otherdrugs, crew health, crew qualifications, orcrew experience.
2. The Bright Field showed evidence ofrecurring engineering problems that affectedvessel main engine reliability, and had allengineering systems been kept in goodrepair and regularly tested, the vessel maynot have unexpectedly lost power during itsvoyage down the Mississippi River.
3. The Bright Field owners’ oversight oftesting and maintenance of the vessel’sengineering systems was inadequate and ledto unreliable performance of the engineeringplant and contributed to the shutdown of themain propulsion engine on the day of theaccident.
4. Insufficient information was available todetermine whether any actions taken by thepilot and crew of the Bright Field wouldhave been effective in preventing theallision or mitigating its effects.
5. At several points prior to and during theBright Field emergency, the pilot, master,and crew of the vessel did not exchangeinformation that under other circumstancescould have prevented or at least mitigatedthe effects of the accident.
6. Use of bridge resource managementprecepts on board the Bright Field wouldhave enhanced the exchange of informationand the coordination of actions among thepilot, master, and crew during the accidentsequence.
7. The response to the Bright Field accident bylocal emergency response agencies wastimely and appropriate.
8. Evacuation of the Queen of New Orleanswas hampered, and passenger risk increased,by the fact that only one gangway was madeavailable for passenger egress during theemergency.
9. Nonoperating crewmembers of the Queen ofNew Orleans and the Creole Queen had notreceived training covering the full range ofemergency scenarios and were unpreparedto properly carry out their responsibilities inthis accident.
10. The lack of effective recurring safety brief-ings for occupants of the Queen of NewOrleans regarding emergency and evacua-tion procedures may have contributed to theconfusion and panic reported among pas-sengers and crew during the vesselevacuation.
11. The instruction placards and signage aboardthe Queen of New Orleans were ineffectivein disseminating emergency instructions andvessel information to passengers.
12. The International RiverCenter and theBoard of Commissioners of the Port of NewOrleans did not conduct adequate riskassessment nor perform adequate safetymanagement oversight to protect theirproperties and the people that use them froman allision such as that involving the BrightField.
13. The U.S. Coast Guard, the Board ofCommissioners of the Port of New Orleans,and the property owners did not adequatelyaddress the risks posed to moored vesselsalong the Erato, Julia, Poydras, and CanalStreet wharves; as a result, under certain
CONCLUSIONS

76
conditions, those vessels were vulnerable toramming by other marine traffic.
14. Operating a vessel at full speed in therestricted waters of the Mississippi Rivermay not allow sufficient time or distance torecover from an emergency.
15. The stakeholders within the Port of NewOrleans, including Federal, State, and localagencies; private commercial entities;shipowners, and pilot associations have notdetermined the overall level of riskassociated with the full range of activitieswithin the port area and have not providedadequate protection for persons andproperty in that area.
Probable CauseThe National Transportation Safety Board
determines that the probable cause of thisaccident was the failure of Clearsky ShippingCompany to adequately manage and oversee themaintenance of the engineering plant aboard theBright Field, with the result that the vesseltemporarily lost power while navigating a high-risk area of the Mississippi River. Contributingto the amount of property damage and thenumber and types of injuries sustained duringthe accident was the failure of the U.S. CoastGuard, the Board of Commissioners of the Portof New Orleans, and International RiverCenterto adequately assess, manage, or mitigate therisks associated with locating unprotectedcommercial enterprises in areas vulnerable tovessel strikes.

77
As a result of its investigation of thisaccident, and in addition to the safetyrecommendations issued previously to the U.S.Coast Guard, to the Board of Commissioners ofthe Port of New Orleans, and to New OrleansPaddlewheels, Inc., the National TransportationSafety Board makes the following safetyrecommendations:
--to the U.S. Coast Guard:
In cooperation with the Board ofCommissioners of the Port of NewOrleans, reassess the risk of locatingpassenger vessels along the leftdescending bank of the MississippiRiver and determine whether to removethe vessels to a less vulnerable locationor put in place procedural, operational,or physical barriers that will protectthese vessels from ramming byriverborne traffic. (M-98-1)
Conduct, with the cooperation of allstakeholders, a comprehensive riskassessment that considers all activities,marine and shoreside, within the Port ofNew Orleans. (M-98-2)
Take the lead in working with the pilotassociations serving the Port of NewOrleans to evaluate the impact ofoperating vessels at full speed in theMississippi River and incorporate thatinformation in your risk-managementand risk-reduction strategies for the portarea. (M-98-3)
In cooperation with the appropriatestakeholders, including Federal, State,and local agencies; private commercialentities; shipowners; and pilot associa-tions, implement risk-management andrisk-mitigation initiatives that will en-sure the safety of people and propertywithin the Port of New Orleans.(M-98-4)
--to the U.S. Army Corps of Engineers:
Participate with the U.S. Coast Guardand other stakeholders in a comprehen-sive risk assessment that considers allactivities, marine and shoreside, withinthe Port of New Orleans. (M-98-5)
In cooperation with the appropriatestakeholders, including Federal, State,and local agencies; private commercialentities; shipowners; and pilot associa-tions, implement risk-management andrisk-mitigation initiatives that will en-sure the safety of people and propertywithin the Port of New Orleans.(M-98-6)
--to the State of Louisiana:
Participate with the U.S. Coast Guardand other stakeholders in a comprehen-sive risk assessment that considers allactivities, marine and shoreside, withinthe Port of New Orleans. (M-98-7)
In cooperation with the appropriatestakeholders, including Federal, State,and local agencies; private commercialentities; shipowners; and pilot associa-tions, implement risk-management andrisk-mitigation initiatives that will en-sure the safety of people and propertywithin the Port of New Orleans.(M-98-8)
--to the Board of Commissioners of the Portof New Orleans:
As part of the permit-approval processfor new commercial and residentialdevelopment along the wharves withinyour jurisdiction, require that any newconstruction of occupied space be sitedbehind a buffer zone sufficient toprotect persons and property by safelyabsorbing the impact should a vesselstrike the wharf. (M-98-9)
RECOMMENDATIONS

78
In cooperation with the U.S. CoastGuard, reassess the risk of locatingpassenger vessels along the leftdescending bank of the MississippiRiver and determine whether to removethe vessels to a less vulnerable locationor put in place procedural, operational,or physical barriers that will protectthese vessels from ramming byriverborne traffic. (M-98-10)
Participate with the U.S. Coast Guardand other stakeholders in a comprehen-sive risk assessment that considers allactivities, marine and shoreside, withinthe Port of New Orleans. (M-98-11)
In cooperation with the appropriatestakeholders, including Federal, State,and local agencies; private commercialentities; shipowners; and pilot associa-tions, implement risk-management andrisk-mitigation initiatives that will en-sure the safety of people and propertywithin the Port of New Orleans.(M-98-12)
--to International RiverCenter:
As previously suggested by the Board ofCommissioners of the Port of NewOrleans, immediately enhance the safetyof the patrons and employees of theRiverwalk complex by widening, by aminimum of 50 feet, that length of thePoydras Street wharf that has notpreviously been extended. (M-98-13)
Participate with the U.S. Coast Guardand other stakeholders in a comprehen-sive risk assessment that considers allactivities, marine and shoreside, withinthe Port of New Orleans. (M-98-14)
In cooperation with the appropriatestakeholders, including Federal, State,and local agencies; private commercialentities; shipowners; and pilot associa-tions, implement risk-management andrisk-mitigation initiatives that will en-sure the safety of people and propertywithin the Port of New Orleans.(M-98-15)
--to Clearsky Shipping Company:
Perform a baseline engineering assess-ment of the Bright Field’s engineeringplant and correct all conditions not inconformance with manufacturer’s speci-fications. (M-98-16)
Institute an engineering testing, mainte-nance, repair, and company oversightprogram for the Bright Field that willensure safe and reliable operation of thevessel’s engineering plant. (M-98-17)
Provide your bridge and engineroomwatchstanding officers and crewmem-bers with initial and recurrent bridgeresource management training that in-cludes communication and coordinationbetween pilots and members of thebridge and engineroom watches and thataddresses their use of bridge and en-gineroom systems. (M-98-18)
--to New Orleans Paddlewheels, Inc.:
In accordance with the guidancepublished by the Passenger VesselAssociation, require that nonoperatingcrewmembers on all your vesselsparticipate in formal emergency trainingand drills in the proper handling ofemergencies that have the potential toaffect the persons in their charge.Maintain written records to verifynonoperating crew proficiency levelsand skill retention. (M-98-19)
Review the existing methods ofproviding safety information toboarding passengers and make thenecessary improvements to ensure thatall vessel occupants receive recurringsafety briefings, regardless of whetherthe vessel is scheduled to leave thedock. (M-98-20)
On all your vessels, post emergencyinstructions that are printed on fire- andheat-resistant material and that areclearly visible to all passengers bothunder normal conditions and duringemergencies when lighting and visibilitymay be diminished. (M-98-21)

79
Participate with the U.S. Coast Guardand other stakeholders in a comprehen-sive risk assessment that considers allactivities, marine and shoreside, withinthe Port of New Orleans. (M-98-22)
In cooperation with the appropriatestakeholders, including Federal, State,and local agencies; private commercialentities; shipowners; and pilot associa-tions, implement risk-management andrisk-mitigation initiatives that will en-sure the safety of people and propertywithin the Port of New Orleans.(M-98-23)
--to the New Orleans Baton RougeSteamship Pilots Association:
Encourage your members to participatein initial and recurrent bridge resourcemanagement training that teaches theprinciples of resource management andthat emphasizes team coordinationbetween the pilot and crew. (M-98-24)
Participate with the U.S. Coast Guardand other stakeholders in a comprehen-sive risk assessment that considers allactivities, marine and shoreside, withinthe Port of New Orleans. (M-98-25)
In cooperation with the appropriatestakeholders, including Federal, State,and local agencies; private commercialentities; shipowners; and pilot associa-tions, implement risk-management andrisk-mitigation initiatives that will en-sure the safety of people and property
within the Port of New Orleans.(M-98-26)
--to the Crescent River Port PilotsAssociation:
Participate with the U.S. Coast Guardand other stakeholders in a comprehen-sive risk assessment that considers allactivities, marine and shoreside, withinthe Port of New Orleans. (M-98-27)
In cooperation with the appropriatestakeholders, including Federal, State,and local agencies; private commercialentities; shipowners; and pilot associa-tions, implement risk-management andrisk-mitigation initiatives that will en-sure the safety of people and propertywithin the Port of New Orleans.(M-98-28)
--to Associated Federal Pilots and DockingMasters of Louisiana, Inc.:
Participate with the U.S. Coast Guardand other stakeholders in a comprehen-sive risk assessment that considers allactivities, marine and shoreside, withinthe Port of New Orleans. (M-98-29)
In cooperation with the appropriatestakeholders, including Federal, State,and local agencies; private commercialentities; shipowners; and pilot associa-tions, implement risk-management andrisk-mitigation initiatives that will en-sure the safety of people and propertywithin the Port of New Orleans.(M-98-30)

80
BY THE NATIONAL TRANSPORTATION SAFETY BOARD
JAMES E. HALLChairman
ROBERT T. FRANCIS IIVice Chairman
JOHN A. HAMMERSCHMIDTMember
JOHN J. GOGLIAMember
GEORGE W. BLACK, JR.Member
January 13, 1998

81
APPENDIX A
Investigation
The Safety Board learned of the accident involving the Bright Field about 1700 onDecember 14, 1996. A five-person investigation team consisting of an investigator-in-charge, an engineering specialist, an operations specialist, a human performancespecialist, and a survival factors specialist arrived on scene on December 15, 1996,accompanied by representatives from the Safety Board’s Offices of General Counsel andPublic Affairs. Member Hammerschmidt was the Board Member on scene.
This accident was investigated jointly by the Safety Board and the U.S. Coast Guardunder the authority of section 304(a)(1)(E) of the Independent Safety Board Act of 1974 andin accordance with 49 CFR 850, “Coast Guard-NTSB Marine Casualty Investigations.” TheCoast Guard invited the Government of Liberia to participate in the investigation, inaccordance with the IMO resolution A637, “Co-Operation in Maritime CasualtyInvestigations.” The Government of Liberia accepted the invitation and a representativeparticipated fully in all aspects of the investigation.
Hearing / DepositionThe Safety Board did not conduct a public hearing in connection with this accident.
However the Safety Board was a participant in the U.S. Coast Guard Marine Board ofInvestigation public hearings held in New Orleans, Louisiana, on December 17-21, 1996;January 6-11 and 29-30, 1997; and March 19-20, 1997.


83
APPENDIX B
Chronology of Bright Field Engineering Problems
October 1995
25th Owner notes concern about continuing cracking problems on Sulzer RTA62 main enginesand attributes problem to design, material, manufacturer, operation and handling.Provides specific instructions to masters and chief engineers about operation andmaintenance parameters.
January 1996
1st Chief engineer reports to owner about serious engineering problems on the Bright Fieldincluding cracked main engine cylinder liners, and loss of power while transiting thePanama Canal due to low main engine lubrication oil system pressure because of anexcessive pressure drop across the second filter.
February 1996
2nd Master telexes owner that he has to run at reduced rpms because of main engineoverheating problems and frequent “auto slowdowns”.
March 1996
Master telexes owner that engineering equipment malfunctions frequently due to the ageand condition.
April 1996
Bright Field dry docked in Nan Tung, China.
May 1996
20th Master telexes owner about severe damage to the main engine’s No. 2 cylinder andpiston. No spare parts available.

Appendix B—Cont.84
June 1996
2nd Second engineer’s maintenance log reports repairs to the main engine’s No. 2 and 3cylinder liners and pistons.
July 1996
5th 0900, arrived Long Beach, California.
23rd Anchored, Japan.
26th Renewed #2 piston, cylinder liner and rings to main engine.
August 1996
3rd Trouble with a pneumatic control valve 14B in automated propulsion pneumatic logiccontrol.
4th Removed #5 piston and cylinder liner to main engine, replaced cylinder liner.
5th Removed #4 cylinder liner and piston rings to main engine, replaced piston rings with“used” rings.
6th 1500, departed for Indonesia.
16th 0440, arrived Pulau Laut, Indonesia.
18th 1245, departed Pulau Laut, Indonesia for Hong Kong.
26th Arrived Hong Kong. Owner’s representative boards vessel.
27th Repaired main engine pneumatic control valve 38A
28th 0005, departed Hong Kong
September 1996
2nd Arrived Banjarmasin, Borneo, Indonesia to load cargo of steaming coal.
3rd Renewed #1 cylinder liner and piston to main engine (liner cracked, piston head burnt anddented).
5th Master informs owner must purchase fresh water, evaporator can only make 10 metrictons, vessel consumes 15 metric tons daily.
6th Owner telexes Bright Field that main engine lubrication oil analysis shows low flashpoint and high viscosity with possible fuel oil leakage into sump.
9th Ordered replacement parts for main engine fuel injection pump, cracked valve
12th Departed Banjarmasin, Indonesia, enroute Davant, Mississippi River (e.t.a. Oct 26th)
17th 0400, #4 piston rings seized and broken, running at reduced speed (65 rpms). Masterhopes to make Singapore for repairs. Chief engineer recommends lifting out #4 piston forrepairs.

Appendix B—Cont. 85
18th 0500, drifting while repairing rings to #4 piston, changed piston crown to #4 brokenpiston crown bolts and no more spares. Also found water leakage in #4 cylinder by pistoncrown damage. Discovered ring damage to #1, 2, 4, 5 pistons, found blocked holds wherecylinder oil is injected. #5 cylinder not working correctly, found cylinder liner cracks. Notenough spare parts for piston ring and cylinder liner repairs, Master telexes owner,“Serious trouble! Except for #1, all cylinder liners leaking gas. Not sure of safety”.
18th 0448, stopped main engine for repairs. Renewed #4 piston rings and piston crown.Welded cracked in cylinder liner.
19th Rough seas main engine still under repair. Notes high level of impurity in main engineand blockage of filters.
20th Master reports vessel in area of typhoon. Main engine damage is serious with no spareparts available. Welded cracks in #5 cylinder liner. Replaced #4 cylinder liner with oldused liner (old #1). Engineering crew exhausted.
21st Dirty air cooler. Can not dismantle to clean because of sea conditions.
22nd 1600, completed temporary main engine repairs. #4 cylinder liner still leaking, running atreduced rpms enroute Spore, Singapore for repairs main engine, air cooler e.t.a. 30 Sept.
25th High main engine scavenging temp due to malfunctioning sea water cooler and mainengine air cooler.
26th Repairs to both main high pressure air compressors.
28th Evaporator out of commission due to faulty pump.
29th Main engine slowdown.30th , 0700 arrived Spore, Singapore.
October 1996
1st Chief electrician tests some temp/pressure sensors.
2nd Telephone conversation between second engineer and owner concerning the quality of themain engine’s lubrication oil. In telex to owner, master reports that the chief engineer hasincreased main engine cylinder oil flow rate.
3rd Owner’s representative boards vessel and reports concern about poor operating conditionof Bright Field’s main engine and lack of confidence in chief engineer. Master telexesrepairs completed, enroute Devant, LA, via Suez Canal, e.t.a. 15 Nov
4th Urgent request for spare parts at Suez for high pressure air compressor, boiler fuel oilburning pump, evaporator.
7th Revised e.t.a. Devant, LA, Nov 21th.
9th Mmaster requested permission to reduced main engine speed to 63 rpms due to highexhaust gas temps and ‘overloads’. Reports continued cylinder cracking problems ifspeed isn’t reduced.
10th Main engine temp problems due to air/electrical valve in speed control system. Chiefengineer overhauls 14A, 4B, and 7D pneumatic control valves.1st , renewed #1 pistonrings. Renewed #4 cylinder liner.

Appendix B—Cont.86
11 Main engine fuel timing cannot be adjusted.
17th Response to owner message, can’t increase speed more.
21st 1400, arrived Suez Canal.
21st No. 2 & 3 cylinder leaking past piston rings and stuffing boxes. #2 piston found to havedented head, planned to lift out #2 and #3 pistons to inspect/change damaged rings beforedeparture from Suez.
23rd Renewed #2 and #3 piston rings.
24th Main engine repairs completed. Ring damage attributed to poor quality of rings. mainengine cylinder oil consumption is 1.32 g/hp-h. Departed Port Said, e.t.a. Devant, LA isNov 16th.
28th Second engineer looking for tools to set main engine fuel oil injecting timing.30th Main engine calibration tools found on board surveyed in response to owner request.
November 1996
4th Reduced rpm to 61 due to high exhaust gas temperatures (508C vs. alarm at 515C).Request repair of CRT monitors and main engine fuel injection pump timing.
5th 2200, slow down caused by the high crank case oil mist alarm. Heavy smoke emittedfrom main engine, repair work underway.
6th 1800, stopped main engine, found hole in #5 piston head cracked and leaking exhaustgases through stuffing box into crank case, contaminating lube oil. Found #5 main enginepiston head burn through. Replaced with old used piston head. Engineering crew renewsmain engine sump lubricating oil due to concern about low flash point of oil. Onlyreplaced 8.4 cubic meters of oil (all that was in storage). Owner informed main enginesump was cleaned.
7th 2300 underway again running at reduced speed (61 rpms) due to high exhausttemperatures.
8th Request for spare parts: 2 piston heads, piston rings, main engine fuel injection valve.Request for 14 tons of main engine lubrication oil (no spare), 10 tons for storage and 4tons to be added to the main engine sump. New e.t.a is Nov 20th.
12th Chief engineer notes that vessel does not have proper tools to set main engine fuel oilpump timing correctly. Consulting instruction books. 1200 hours stopped to try to adjustfuel pump timing based on instructions from owner. 1800 work completed underwayagain.
13th New e.t.a. Nov 21st
14th Requesting 14,000 liters of main engine lube oil on arrival Davant. Auxiliary boiler FOboost pump ooc (requested spare parts on August 27th ), no spare parts. Must use dieseloil instead of bunker fuel oil every time main engine and G/Es are started and stopped.
14th Master requests main engine expert meet vessel to solve problems, no one on boardknows how to fix problems. Attempted to increase rpms from 61. At 63 turbochargerinlet temp rose to 510 (alarm at 515C). Reduced speed to 61 rpms.

Appendix B—Cont. 87
15th Master notes last d/d 04-28-96 and last special survey 17-09-95.
20th Second engineer still looking for missing tool to set main engine fuel oil injector timing.
21st 0610 at sea buoy, set manned engine room. Chief engineer relieved of duty and replaced.1630 along side Davant coal dock to off load coal.
21st Sulzer technical representative checks main engine. Identifies several sources of possiblelube oil contamination. Notes many serious problems with the main engine.
22nd Master reports results of Sulzer survey to owner.
24th Tested main engine emergency shut downs.
25th 0849 coal discharge completed, anchored Mississippi River to clean cargo holds.
25th Overhauled #2 main engine cylinder, new piston head.26th Bunkering fuel oil and diesel oil.
27th Vessel fails cargo hold inspection. Engineering crew rebuilds main engine injector pumpsand set timing with help of Sulzer technical representative. Vessel receives approximately8,000 liters of main engine lubrication oil.
28th Overhauled #5 main engine cylinder, replaced piston rings, found three small cracks inliner.
30th Repaired defective main engine emergency stop valve.
December 1996
1st Master requests engineering spare parts. Notes status of repair work; #2 and #5 cylinderscracked and piston rings worn (poor quality), cleaned stuffing boxes and scavenging airboxes, air/water separator for air cooler and exhaust manifold, M/E fuel oil pump timingwith assistance of Sulzer, main engine emergency stop system repaired 3 control airvalves.
2nd Crew attempted unauthorized repair to Terasaki monitors.
5th Vessel passed hold inspection. Repaired main engine control air supply pressure reducers(A-124HA,124HB).
7th Tested main engine with sea trial data and found continued high turbocharger inlet temps.Recommended repairs to turbocharger and /or air cooler.
9th Chief engineer sends notice to owner confirming seriousness of engineering problemsobserved by Sulzer technician. At 1200, along side Cargil (Reserve) grain loading facilityto load cargo.
11th Found turbocharger rotor rings worn. 1317 completed loading corn.
12th Renewed #5 cylinder piston rings. Chief engineer sends off main engine lube oil sample.12th Anchored Mississippi River for repairs to turbocharger and air cooler by local
engineering repair service.
13th ETD December 14, 0800. Next port of call is Cristobal, Panama with an ETA ofDecember 19th at 1600.
14th 0700, engineering repairs completed, 0945, vessel underway from Reserve, sailed from

Appendix B—Cont.88
anchorage at 1112, draft forward 11.96m, draft aft 12.06m., ETA Kashima, Japan onJanuary 18, 1997.
14th 1055 and 1110, main engine will not start in W/H control.
14th 1158 and 1235, main engine experiences overheating alarms/problems due to jacket watercooling problems.
14th 1406, loss of main engine lube oil pressure. Failure of standby lube oil pump to start. Lowpressure alarm and main engine trip.
89
APPENDIX C
Voyage Data Recorders (VDRs)
The Safety Board has long considered that marine VDRs (also known as voyage eventrecorders, or VERs), when used as management oversight tools, can provide valuableinformation, not only on engineering plant performance, but on crew performance and trainingneeds. Use of a VDR to monitor crew performance can provide management with a means ofmeasuring training effectiveness and identifying needed changes in training or procedures. Whenused as accident reconstruction tools, VDRs help investigators determine how an accidentoccurred so that they can develop measures to help prevent similar accidents.
The Safety Board has promoted the use of VDRs of various types since the 1970s and is onrecord in support of the value of these systems as management tools as well as accidentinvestigation tools. Safety Board staff has been extensively involved in aviation and surfacevehicle data recorder readout, data analysis, rulemaking, and technical standards development forVDRs. The Safety Board has been working closely with the Coast Guard for more than 1 year inan effort to develop International Maritime Organization (IMO) carriage requirements andtechnical standards for VDRs.
The IMO’s Navigation Subcommittee has requested that the InternationalElectrotechnical Commission (IEC) develop an international technical testing standard for VDRs.The standard will be based on the IMO recommendations. The IEC working group (TC-80/WG-11) commenced work in March 1997 and expects to publish a standard in 1999. Representativesfrom the Safety Board are working with the IEC group to develop the standard.
The IMO is expected to require the installation of VDRs on roll-on roll-off (RORO)passenger ferries as early as 1998, followed by a requirement for VDRs on all vessels of morethan 1,600 gross tons within the next 4 to 5 years. While the Safety Board would prefer moretimely deployment of VDRs, it is encouraged that this significant issue is finally receivinginternational attention and action.