atrial fibrillation: whole lot a shakin’ goin’ on! susan morris rnbn med cncc(c) ccn(c)
TRANSCRIPT

Atrial Fibrillation: Whole Lot a Shakin’ Goin’ On!
Susan Morris RNBN MEd CNCC(C) CCN(C)

Atrial fibrillation
• Most common arrhythmia in the world
• https://www.youtube.com/watch?v=0UITrR7uo3o
Burden of the Arrythmia
• AF places a major burden on healthcare systems, particularly as the incidence and prevalence are increasing.
• Patients with AF often need to be hospitalized and it has been estimated that United States hospitalizations have increased by 23 percent between 2000 and 2010
Perioperative Challenges of AF
• The aging population has increased the prevalence and incidence of atrial fibrillation
• Add that to the fact that we are doing elective and emergent procedures on patients well into their 80’s and possibly 90’s

Classification of AF

Incidence in the Operative Patient
• 1% with minor procedures• 5-10% after vascular or large colorectal surgery• Postoperative atrial fibrillation occurs principally
after thoracic and cardiac surgery.• Very low incidence after VATs but large
resections, pneumonectomy or esophagogastrectomy 10-30%
• CV surgery (CABG 30%) Valve (40%) and up to 50% in combined procedures

Risk factors for AF development
• Traditional risk factors: Age, HTN, male, hyperthyroidism, diabetes, CV disease and valvular dysfunction
• Emerging risk factors: obesity, obstructive sleep apnea, ETOH abuse, renal disease and with new research there is a potential genetic link
• The single most consistent predictor of AF is AGE and probably the comorbidities that go with aging


What are the Operative challenges?
• Increased hemodynamic instability
• Increased thromboembolic risk
• Management of OAC with or without heparin bridging

When Does Post Operative AF (POAF)Occur?
• 70% of AF occurs in the first four days post op and this has prompted researchers to look at surgery induced issues such as inflammation, SNS stimulation(probably most relevant), and oxidative stress (process of free radical release that causes damage to the “cell signalling” component of the cell and long term oxidative stress is thought to lead to cancer and many other diseases)
• Even though POAF is short lived its occurance increases the risk of future AF

Prognosis
• AF automatically increases mortality and morbidity because of potential for stroke, thromboembolism and CHF
• It also impairs quality of life
Complications of AF
• Stroke is the most devastating complication of AF
• AF increases stroke risk 5 fold
• If there is more than 1 risk factor for stroke then this indicates a need for OAC




Recommendation Medication
1. All AF patients be risk stratified
2. OAC for most patients > 65 or CHADS2 > 1
3. OAC for non-valvular AF NOACS: Dabigatran, rivaroxaban, apixaban or edoxaban (When approved)
4. Mechanical valves, rheumatic mitral stenosis and low creatnine clearance
Warfarin rather than the NOACS
5. Condition warrants OAC but patient refuses
ASA 81 plus clopidogrel 75 mg/day
. No risks such as age or CHADS ASA 81 mg Daily

What do we see in practice?
• Young low risk patients are often over treated• The elderly are undertreated
• The inconsistency in practice stems from a lack of knowledge of the guidelines

Case Study• Joe, 67 YO male is seen in the pre-op clinic in
preparation for aorta bifemoral bypass graft in 3 weeks time. Smokes 1PPD x 26 years, (quit 2 weeks ago and is dong well) and enjoys a daily drink (or 2) of rum, whiskey…. He is on no home medications, rarely sees a physician and his need for a bypass graft was identified when he sought attention for a gangrenous great toe. He is found to be in AF on his preop ECG, he has no complaints and can’t understand why “my stomach is being operated on to fix my toe”.

Risk stratification:What should we give him?What other factors come in to play in the decision making process here?
Perioperative,PACU and Surgical Nurses
• Your patients are most likely high risk and now the added complexity of determining who can be taken off of their OAC in preparation for the OR, who needs a heparin bridge, who takes antiplatelet therapy such as ASA or clopidagril (plavix) and who remembered to stop taking these medications when they were supposed to

POAF: Amiodarone is the drug of choice

• Amiodarone should be used with caution in patients with low pulmonary reserve as it is associated with acute pulmonary toxicity when given in higher doses
• Important tip: one of the largest drug interactions is between amiodarone and wafarin. Amio decreases the effectiveness of warfarin but then when it is discontinued the INR will significantly elevate

Prevention
• Prophylactic betablockers > 1 week preop
• Prophylactic amiodarone pre op
• IV magnesium if the patient is hypomagnesemic

How Decisions are Made for Holding & Bridging in the Elective Pre-op Patient





So what does all of this mean for the nurse?
• Assisting in identifying the high risk patient…..we do the history on most patients!!
• Nurses need to understand when medications will be restarted and be able to assess postop bleeding risks and report this prior to the restart of medications
• **Nurses need to be able to do a good neuro exam: recovery, ICU or post op floor

What about these New OAC’s (NOAC’s)
• There are 3 important considerations for peri-operative management of patients taking a NOAC:
• 1) Reliable laboratory tests to confirm the absence of a residual anticoagulant effect of NOACs are not widely available.
• 2) Half-lives of NOACs differ and increase with worsening renal function, affecting when the drug should be stopped before surgery.
• 3) NOACs have rapid onset of action, with a peak anticoagulant effect occurring 1-2 hours after oral intake.

Noac’s and Coagulation Tests?
• Vitamin K antagonists such as warfarin have a well recognized test for determining “degree” of anticoagulation but NOAc’s do not.
• Also NOACs do not have reversal agents such as Vit K or octaplex
Drug of Choice for Bridging
• No evidence for unfractionated heparin over Enoxaparin
• Often the physician preference dictates• Heparin is often preferred for high risk
patients, especially mechanical valve patients as we can monitor the effectiveness via pTT but with LMWH there is no simple test to determine effectiveness

Just ASA

Case Studies
• Template:• 1. Does the patient have Atrial Fibrillation• 2. Is it paroxysmal (<7days), persistent (new onset but >7 days) or
permanent (confirmed on multiple visits with HCP)
• 3. What type of anticoagulation is the patient on?• 4. Determine the risk based on the procedure• 5. Is there a medication that needs to be held (safely)?• 6. Is bridging anticoagulation needed during warfarin
interruption?• 7. What is the drug of choice for bridging

Mrs Black pre op assessment
• 54 year old female• Elective abdominal hysterectomy• PMHx: syncope NYD, T&A and appendectomy
as a child. Type II diabetes• Home medications: metoprolol 50 for irregular
heart rate and ASA 81 mg• Routine ECG:

Mrs Black

• 1. Does the patient have Atrial Fibrillation• 2. Is it paroxysmal (<7days), persistent (new onset but >7 days) or
permanent (confirmed on multiple visits with HCP) We have to ask some targeted questions
• 3. What type of anticoagulation is the patient on?• None just antiplatelet: ASA• 4. Determine the risk based on the procedure intermediate• 5. Is there a medication that needs to be held (safely)?• Yes for 7 days perop• 6. Is bridging anticoagulation needed during warfarin
interruption? No as she was not on warfarin• 7. What is the drug of choice for bridging N/A
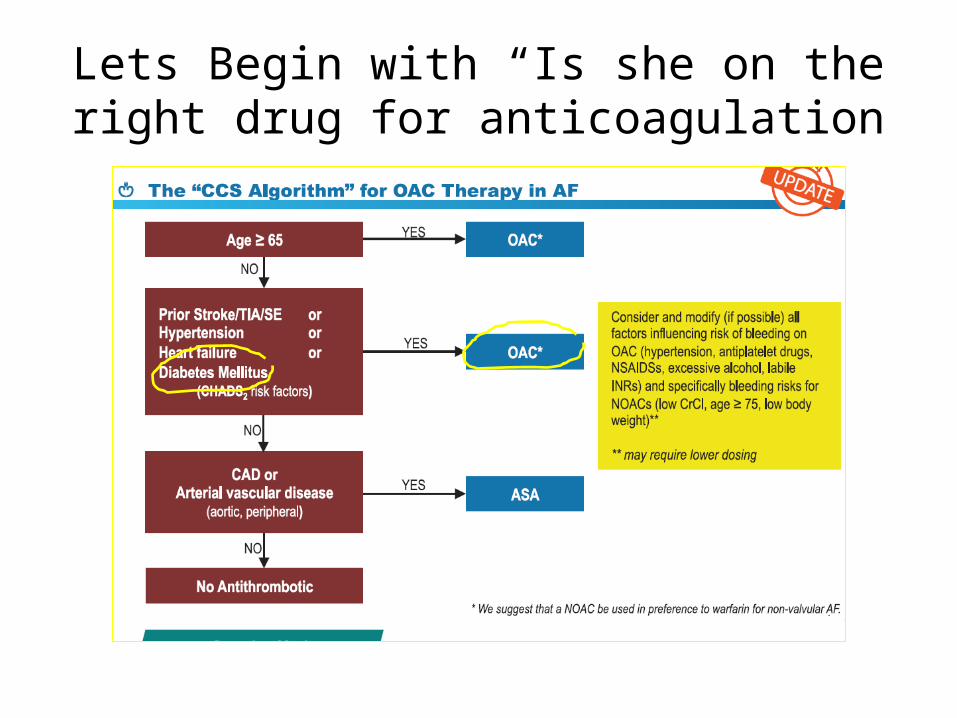
Lets Begin with “Is she on the right drug for anticoagulation

So we discover she is not properly risk stratified. Is her surgery high risk for bleeding? What do
we do with the ASA?

Case Study #2 Mr. Jack Daniels
• 74 year old male admitted for repair of AAA• PMHx: MI in 1998, 2008, 2014 with CABG x4 in
2014. Diabetes, HTN, mild COPD, atrial fibrillation on warfarin
• Meds: Coumadin 2.5 MWF 2.0mg Sat and Sun 1 mg Tues thurs. Metoprolol 50 BID Crestor 20mg OD Altace 10 OD, nitro spray prn
• ECG:


Who wants to:
• A: synchronized cardioversion
• B: give metoprolol 2.5 mg IV pushstat
• C. Amiodarone 300 mg IV push stat
• D. Monitor the BP and assess a little longer

1. Does the patient have Atrial Fibrillation: Yes documented in previous charts and visits2. Is it paroxysmal (<7days), persistent (new onset but >7 days) or permanent (confirmed on multiple visits with
HCP) Patient is in Sinus brad right now but we can assume it is permanent as he is on coumadin3. What type of anticoagulation is the patient on? VKA warfarin4. Determine the risk based on the procedure: AAA is high risk5. Is there a medication that needs to be held (safely)? Yes the warfarin
6. Is bridging anticoagulation needed during warfarin interruption?yes7. What is the drug of choice for bridging: If we go with heparin then he must be in hospital 3 days preop, LMWH can be given by extramural, family physician etc

Case #3: Suzie Smirnoff
• 64 year old poor historian admitted to the OR from emerg for emergent bowel resection.
• In her medication bag she has hydrochlorathiazide OD, dabigitran BID, metoprolol OD, but has no idea why she takes them.
• ECG:


1. Does the patient have Atrial Fibrillation2. Is it paroxysmal (<7days), persistent (new onset but >7 days) or permanent (confirmed on multiple visits with HCP)3. What type of anticoagulation is the patient on?4. Determine the risk based on the procedure5. Is there a medication that needs to be held (safely)?6. Is bridging anticoagulation needed during warfarin interruption?7. What is the drug of choice for bridging

A note about NOAC’s and reversibility
• Although we lack peer-reviewed, full-length, patient data–based publications to guide us in this situation, here is what we do know:
• Dabigatran has a half-life of approximately 12 hours in patients with normal (greater than 50 mL/min) creatnine clearance, 18 hours when the creatnine clearance is 30 to 50 mL/min, and 27 hours when the creatnine clearance is less than 30 mL/min
• There no true antidote (eg, such as vitamin K for warfarin) for dabigatran (coming soon I hear).– Time: Since the half-life is 12 hours, each 12 hours from dosing will halve
the concentration and anticoagulant effect to allow surgery.– May need charcol if recently ingested– Dialysis – Supportive care: FFP, platelets and managing – Regarding laboratory testing for dabigatran effect: no definative test
at this time

Questions??