atrial fibrillation final handouts - osu center for ... - atrial fibrillation final... · 1 atrial...
TRANSCRIPT

1
Atrial FibrillationAtrial Fibrillation
Troy E. Rhodes, MD, PhDDivision of Cardiovascular Medicine, ,
ElectrophysiologyOhio State University Medical Center
Learning ObjectivesLearning Objectives• Review the growing incidence andReview the growing incidence and
importance of AF in the population• Discuss the use of anticoagulation in
AF for stroke prevention• Summarize pharmacologic and non• Summarize pharmacologic and non-
pharmacologic options for AF management

2
Atrial FibrillationAtrial Fibrillation
5 165.425.61
5
6
s
Projected Number of Adults With AF in the US
Projected Number of Adults With AF in the US
2.082.262.442.662.94
3.333.80
4.344.78
5.16
1
2
3
4
5
s w
ith
AF, M
illio
ns
0
1
Ad
ult
Year
Go et al. JAMA. 2001;285:2370-2375.

3
Costs to the Health Care SystemEstimated US cost burden 15.7 billion
annually
Costs to the Health Care SystemEstimated US cost burden 15.7 billion
annually• 35% of arrhythmia hospitalizations
• Average hospital stay = 5 days
• Mean cost of hospitalization = $18,800
• Does not include:
Costs of outpatient cardioversions
Costs of drugs/side effects/monitoring
Costs of AF-induced strokes
Quality of Life with AFQuality of Life with AF
1 Jung et al, JACC. 1999 2 Ware et al, New England Medical Center Health Survey, 1993.

4
Diagnostic EvaluationDiagnostic EvaluationMinimum Evaluation• History and physical – Sx with AF, CV
disease• Electrocardiogram – LVH, MI, BBB, WPW• Echocardiogram – LVH, LAE, LVEF, Valvesg , , ,• Labs – TSH, Renal fxn• Sleep history
AHA / ACC / ECS Guidelines 2006
Diagnostic EvaluationDiagnostic EvaluationAdditional Testing• ETT – CAD, Exercise induced SVT / AF• Holter / Event Monitor – Confirm AF and
Sxs• TEE – LA clot• EPS – SVT triggered AF • Sleep Study
AHA / ACC / ECS Guidelines 2006

5
Incidence of AF Based on Presence or Absence of OSA
Incidence of AF Based on Presence or Absence of OSA
20 –
15 –
10 –
5 –
CumulativeFrequencyof AF (%)
OSA
No OSA
Gami et al. JACC 2007;49:565-71
0 –
Years0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15
Number at RiskOSANo OSA
8442,209
7091,902
5691,616
4781,317
3971,037
333848
273641
214502
173393
134296
110217
94195
70130
4694
2969
828
Heart Rhythm 2011; 8: 157-176.

6
Fi t
Classification of Atrial FibrillationACC/AHA/ESC Guidelines
Classification of Atrial FibrillationACC/AHA/ESC Guidelines
Paroxysmal(Self-
First Detected
Persistent(Not self-
terminating)
Permanent
terminating)
Maintenance of SR Stroke preventionRate control
Treatment OptionsTreatment Options
Pharmacologic Nonpharmacologic
Class IA Class ICClass III
Catheter ablationSurgery (MAZE)Pacing
Pharmacologic• Warfarin• Thrombin inhibitor• Aspirin
Nonpharmacologic• Removal / isolation
LA d
Pharmacologic• Ca2+ blockers• β-blockers• Digitalis• Amiodarone
Nonpharmacologicβ-blocker
gLA appendage
p g• Ablate and pace
Prevent remodeling ACE-IARB
Adapted from Prystowsky, Am J Cardiol. 2000;85:3D-11D.

7
Atrial Fibrillation and StrokeAtrial Fibrillation and Stroke• 5 fold increased risk of CVA• AF accounts for 1 out of every 6 CVAsy• Paroxysmal same risk as persistent• Thromboemboli originating from LAA
Stroke Risk Assessment in AF: CHADS2 Score
Stroke Risk Assessment in AF: CHADS2 Score
CHADS Annual Stroke NNTClinical Parameter PointsCHF 1Hypertension 1Age > 75yo 1Diabetes 1Stroke 2
CHADS2Score
Annual Stroke Risk %
NNT
0 1.9 4171 2.8 1252 4.0 813 5.9 334 8.5 27
Gage et al, JAMA 2001; 285:2864.
5 or 6 12-18 44

8
Stroke Risk Assessment in AF: CHADS2 Score
Stroke Risk Assessment in AF: CHADS2 Score
Clinical Parameter PointsCHF 1Hypertension 1Age > 75yo 1Diabetes 1Stroke 2
CHADS2 Score Treatment0 ASA1 ASA or Warfarin (INR 2-3)2+ Warfarin (INR 2-3)
Gage et al, JAMA 2001; 285:2864.
AnticoagulationAnticoagulation• Overall CHADS2
SEvents per 100 person- NNT
62% reduction with warfarin19% with ASA
• AFFIRM80% of CVAs
Score yearsWarfarin No Warfarin
0 0.25 0.49 417
1 0.72 1.52 125
2 1.27 2.50 81
3 2 20 5 27 33occurred after coumadin was stopped or was subtherapeutic
3 2.20 5.27 33
4 2.35 6.02 27
5 or 6 4.60 6.88 44
9
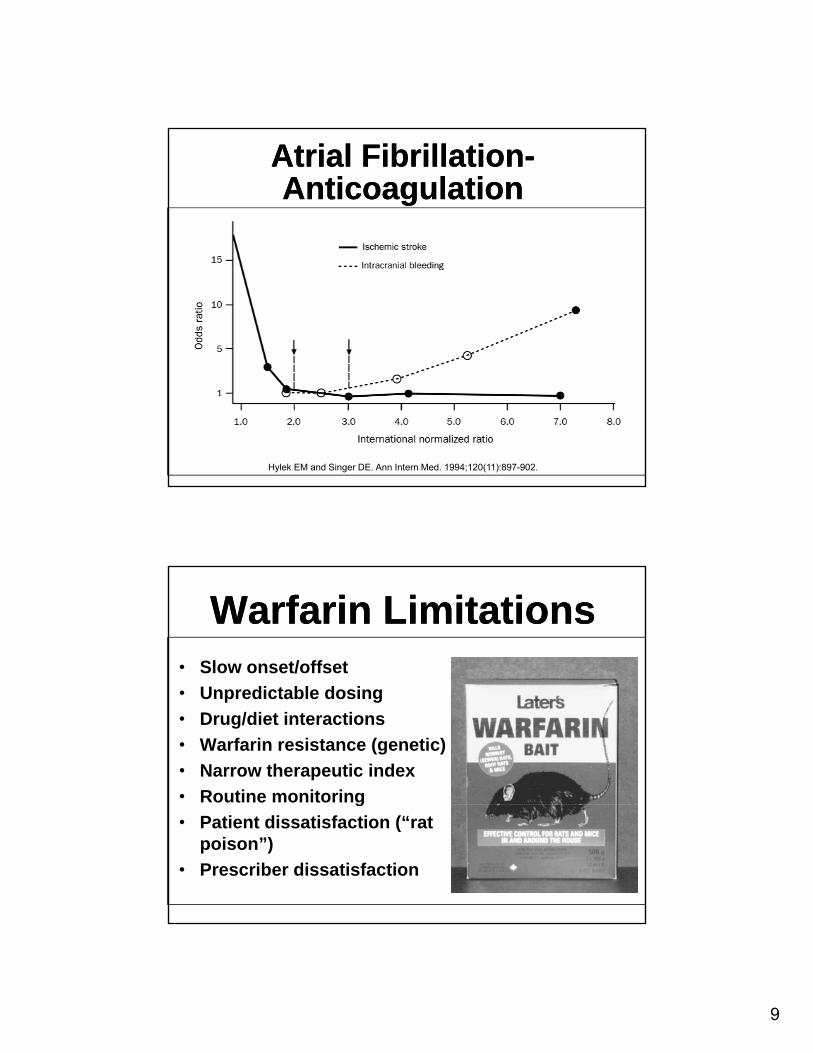
Atrial Fibrillation-Anticoagulation
Atrial Fibrillation-Anticoagulation
Hylek EM and Singer DE. Ann Intern Med. 1994;120(11):897-902.
• Slow onset/offset
Warfarin LimitationsWarfarin Limitations
• Unpredictable dosing• Drug/diet interactions• Warfarin resistance (genetic)• Narrow therapeutic index• Routine monitoringg• Patient dissatisfaction (“rat
poison”)• Prescriber dissatisfaction

10
DabigatranDabigatran• Direct thrombin inhibitor
R ibl bi diReversible bindingFree & clot-bound thrombin
• Inhibits platelet aggregation• Inhibits tissue factor-induced
thrombin generation• Renally cleared• No antidote
FDA-Approved LabelingFDA-Approved Labeling• Who it’s for:
Non-valvular AF patients for strokeNon-valvular AF patients for stroke prevention
• Who it’s NOT for:Mechanical heart valvesPEPEDVTProphylaxis for knee/hip replacementsHIT

11
Management of AFManagement of AF
ANTITHROMBOTIC RX
RHYTHM RATE
AND
RHYTHMCONTROL
RATECONTROL
OR ?
Rate ControlRate Control

12
Atrial FibrillationAtrial FibrillationRate control – Drug TherapyRate control – Drug Therapy
Digoxin – controls resting rate, OK in CHF patients.
Beta, Calcium channel blockers – controls resting and exercise rates.
Best therapy – combination of beta blockerand digoxin.
Primary Goal – Avoid Tachycardia InducedCardiomyopathy
What is optimum rate control?What is optimum rate control?• AFFIRM trial
Resting heart rate less than 80 bpmPeak heart rate less than 110 bpm
• RACE II

13
RACE IIRACE II• 614 patients
L i t C t l (<110 b )• Lenient Control (<110 bpm) versus strict control (<80 at rest, <110 at peak).
• Mean follow up 2 years.• Primary Outcomes of death, CHF,
stroke embolism, life threatening arrhythmias
The RACE II Investigators. N Engl J Med. 2010;362: 1363-1373.
Rate ControlRate Control• No significant difference in two groups
The RACE II Investigators. N Engl J Med. 2010;362:.

14
Rhythm ControlRhythm Control
Conversion of AFConversion of AF
< 3 Months3 - 12 Months
100
Length of timein AF prior tocardioversion
Duration of AF is the best predictor of recurrent AF after cardioversion
3 12 Months> 12 Months
80
60
40
nts
in s
inus
rhyt
hm (%
)
*cardioversion
Dittrich HC. Am J Cardiol. 1989;63:193-197.
20
0Initial One month
post-CVSix months
post-CV*P = <0.02
Patie
n
15
Anticoagulation - CardioversionAnticoagulation - Cardioversion• Atrial stunning
Stunning can occur even with one hour ofeven with one hour of atrial fibrillationIf duration < 2 weeks, function may return within 24 hours to one weekweekIf duration > 2 weeks, stunning may persist for one month
Mattioli, AV. et al. Am J Cardiol 1998; 82:1368.
CardioversionCardioversion• Less than 48 hours durationLess than 48 hours duration
Cardioversion without TEEHeparin at time of cardioversionWarfarin for a month and re-evaluation as outpatient
16
CardioversionCardioversion• If greater than 48 hours
Option 1: Anticoagulate for 4 weeks andOption 1: Anticoagulate for 4 weeks and then cardiovertOption 2: TEE and if no thrombus, cardiovert
If thrombus, 4 weeks warfarin and h krecheck
Anticoagulate for minimum of one month and re-evaluate
25
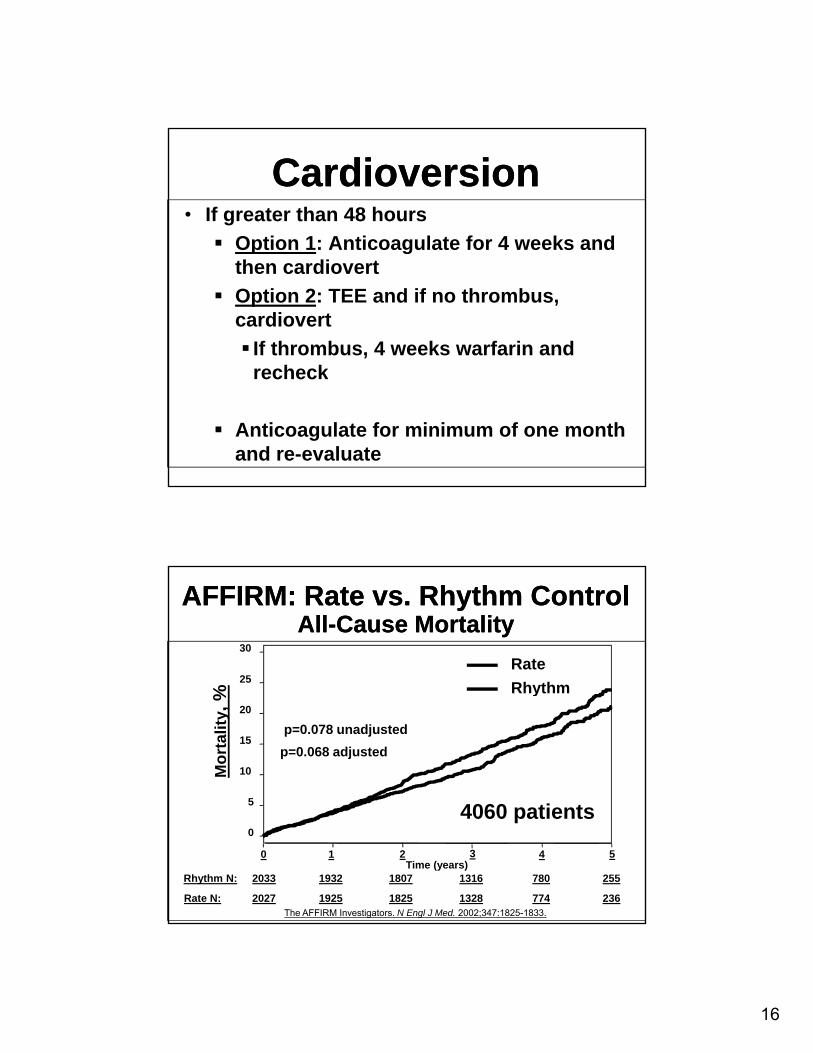
30RateRhythm
AFFIRM: Rate vs. Rhythm Control AFFIRM: Rate vs. Rhythm Control All-Cause MortalityAll-Cause Mortality
5
10
15
20
Mor
talit
y, %
Rhythm
p=0.078 unadjusted p=0.068 adjusted
4060 ti t
Rate N:
Rhythm N:
2027
2033
1925
1932
1825
1807
1328
1316
774
780
236
255
0
5
0 1 2 3 4 5Time (years)
The AFFIRM Investigators. N Engl J Med. 2002;347:1825-1833.
4060 patients

17
Rate vs. Rhythm Control Trials: Implications
Rate vs. Rhythm Control Trials: Implications
• AFFIRM demonstrated that a rate control “strategy” is an acceptable primary“strategy” is an acceptable primary therapy in a selected high-risk subgroup of AF patients
• Continuous anticoagulation seems warranted in all patients with risk factors f t kfor stroke
Asymptomatic recurrences
• AFFIRM did not define whether it is better to be in NSR.
Rhythm ControlRhythm ControlADVANTAGES DISADVANTAGESADVANTAGES• Avoids electrical and
anatomical remodeling• Improves hemodynamics• Enhanced exercise capacity • Symptom relief
I QOL
DISADVANTAGES• Ventricular proarrhythmia• Increased mortality?• Drug-induced
bradyarrhythmias• End-organ toxicity
Ad ff• Improves QOL• Restores atrial transport• Reduces thromboembolic
events?
• Adverse effects• Recurrences are likely• Asymptomatic (silent) AF

18
Heart Rhythm 2011; 8: 157-176.
CTAF Trial*: Maintenance of SRCTAF Trial*: Maintenance of SR
nce,
% 100Amiodarone 10 mg/kg/2 wk, 300 mg/4 wk, 200 mg/d (n=201)
ents
with
out r
ecur
ren 80
60
40
20
Propafenone 300-450 mg/d (n=101)
Sotalol 160 mg BID or 80 mg TID (n=101)
Roy D, et al. N Engl J Med. 2000;342:913-920.
Patie
0 1000
200 300 400 500 600
Days of follow-up
* Excluded recurrence in first 21 days.

19
AF AntiarrhythmicTherapy
AF AntiarrhythmicTherapy
• Treatment goalsTreatment goals ↓ frequency of recurrences↓ duration of recurrences↓ severity of recurrencesNot to abolish every episode
• Safety is primary concern• Minimize risk of proarrhythmia
Drug-Induced Proarrhythmia -Torsades
Drug-Induced Proarrhythmia -Torsades

20
Factors Which InfluenceVentricular Proarrhythmia Risk
Factors Which InfluenceVentricular Proarrhythmia Risk
• Hypokalemia, hypomagnesemia• Long QT at baseline• CHF / Decreased EF• Ventricular hypertrophy • Bradycardia
F l d• Female gender• Reduced drug metabolism or
clearance • Amiodarone has lowest risk
Alternatives to Drug Therapy“Non-Pharmacologic Therapy”Alternatives to Drug Therapy
“Non-Pharmacologic Therapy”
C di LAA l (W t h )Coumadin – LAA closure (Watchman)
Rate Control – AVN RFA + PCMK
AAR Adj ti AFL RFAAARx – Adjunctive AFL RFA
AARX – Curative Afib RFA
21
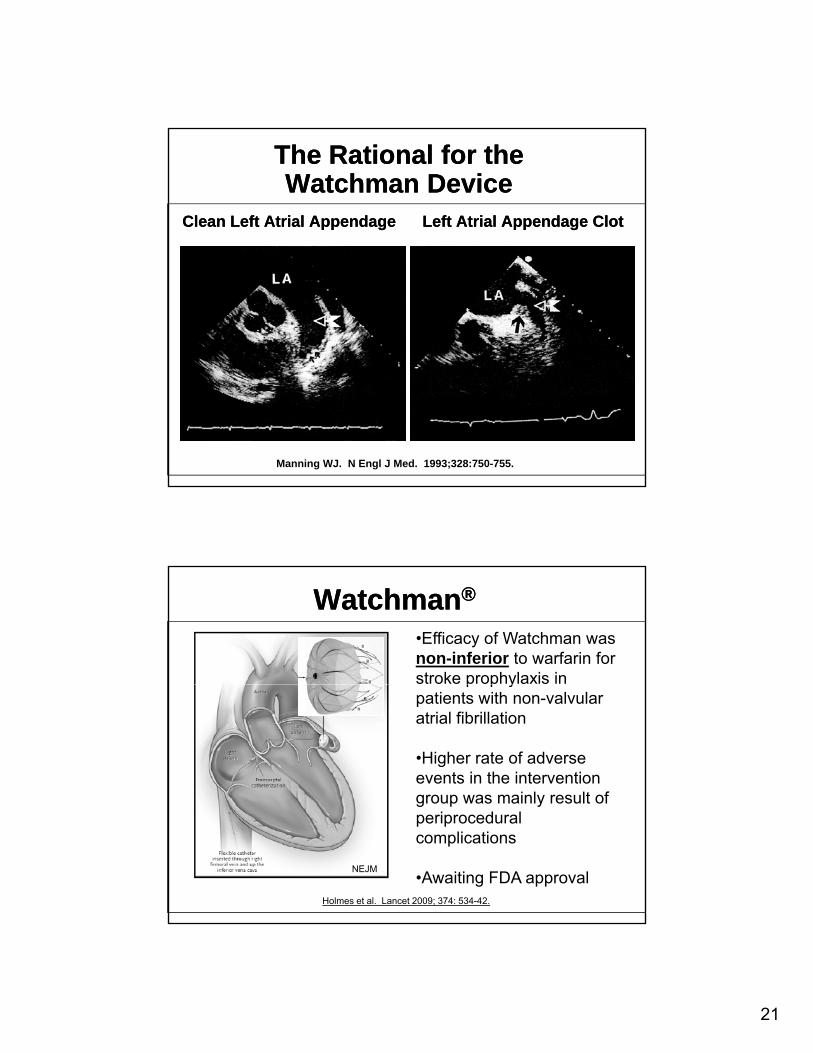
The Rational for the Watchman Device
The Rational for the Watchman Device
Clean Left Atrial Appendage Left Atrial Appendage ClotClean Left Atrial Appendage Left Atrial Appendage Clot
Manning WJ. N Engl J Med. 1993;328:750-755.
Watchman®Watchman®
•Efficacy of Watchman was non-inferior to warfarin for stroke prophylaxis in p p ypatients with non-valvular atrial fibrillation
•Higher rate of adverse events in the intervention group was mainly result of
NEJM
g p yperiprocedural complications
•Awaiting FDA approvalHolmes et al. Lancet 2009; 374: 534-42.

22
Pacemaker + AV Node Ablation Pacemaker + AV Node Ablation
http://www.heartrhythmcenter.com/myweb2/av_nodal_ablation2.htmhttp://www.nlm.nih.gov/medlineplus/ency/images/ency/fullsize/19566.jpg
AVN RF AblationAVN RF Ablation

23
70
mean
55
50 mean
Objective Benefits of AV Nodal AblationObjective Benefits of AV Nodal Ablation
60
50
40
30
LVEF
(%)
mean54 + 7
p < 0.001
mean43 + 8
45
35
30
LVES
D (m
m)
mean34 + 5
p < 0.003
mean40 + 5
40
25
Rodriguez LM. Am J Cardiol. 1993;72:1137-1141.
A Left ventricular ejection fraction (%)
B Left ventricular end systolic diameter (mm)
20Before After
20Before After
25
AVN Ablation AVN Ablation Advantages:
100% efficacy85% symptomatic improvement85% symptomatic improvementImproved EF (LV remodeling)Eliminates need for rate control drugs
Disadvantages:Pacemaker dependant
Good Candidates:Good Candidates:Tachy / Brady SyndromePPM present – CHF with BiV deviceMedication refractory / intolerantElderly

24
IC Antiarrhythmic Induced Atrial Flutter1:1 Conduction
IC Antiarrhythmic Induced Atrial Flutter1:1 Conduction
Atrial Flutter CircuitAtrial Flutter Circuit

25
Approximately 15% of AF patients treated with an AARx will develop AFL
Atrial Flutter AblationAtrial Flutter Ablation
Advantages:95% efficacy≈ 80% arrhythmia control if AARx continuedAs primary Tx RFA more effective than AARx
Disadvantages: Invasivesad a tages as e
Good Candidates:Typical AFL (IVC / TV isthmus)Primary or AARx related Atrial Flutter
• 94% of AF RA LA
Focal Origin of Atrial FibrillationHassaiguerre M, NEJM, 1998
Focal Origin of Atrial FibrillationHassaiguerre M, NEJM, 1998
triggers from Pulmonary Veins
• “90-95% of all AF FO
SVC
Pulmonary Veins
is initiated by PV ectopy”
CS
IVC 6 11

26
Atrial Fibrillation AblationAtrial Fibrillation AblationAtrial ShellAtrial Shell Cardiac MRICardiac MRI
Comparison of Antiarrhythmic Drug Therapy and Radiofrequency Catheter Ablation in Patients with Paroxysmal Atrial Fibrillation: A Randomized Controlled Trial
Comparison of Antiarrhythmic Drug Therapy and Radiofrequency Catheter Ablation in Patients with Paroxysmal Atrial Fibrillation: A Randomized Controlled Trial
66%vs.
16%
JAMA 2010
Major Adverse Events: Ablation 4.9% vs. AARx 8.8%Repeat Ablation in 12.6% of patients
27
Current State of CurativeCatheter-Based RFA
Who is a good candidate?
Current State of CurativeCatheter-Based RFA
Who is a good candidate?Symptomatic / Frequent AFLimited Heart Dz
EF > 35%LA < 5.5cmNo MS / Rheumatic Dz
Younger PatientsNo LA thrombus or Hx of CVAMedically Refractory / Intolerant
(Ablation now second line therapy)
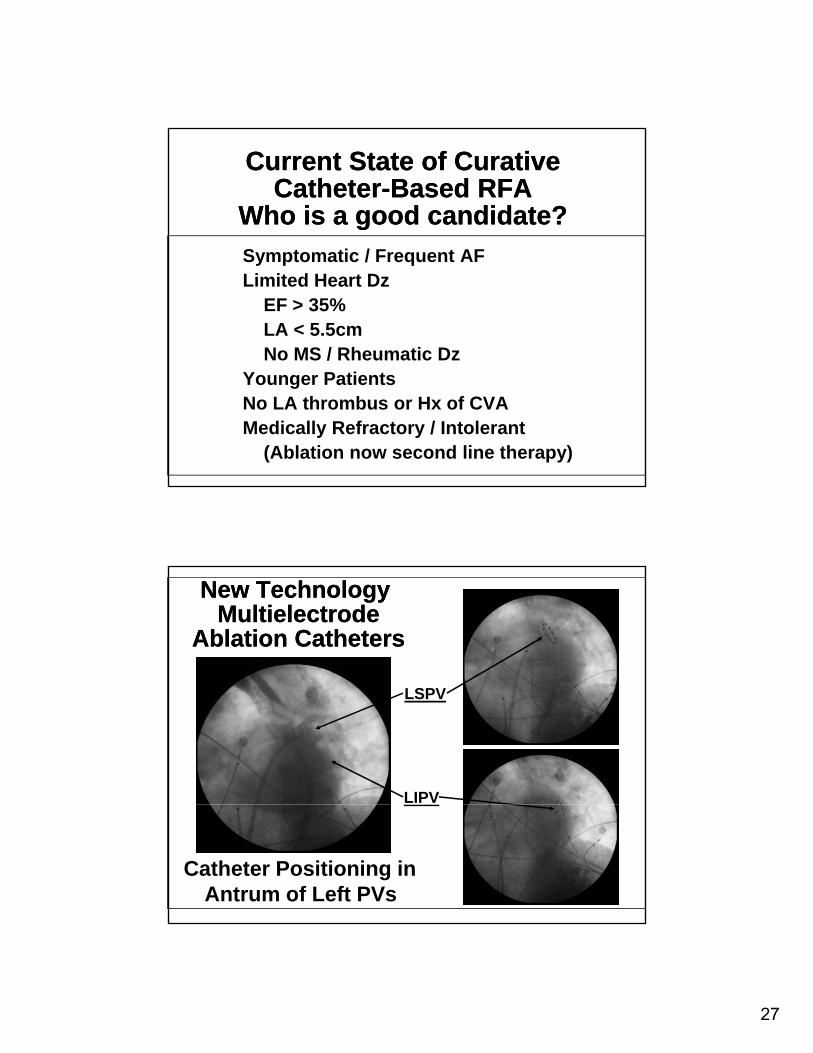
New TechnologyMultielectrode
Ablation Catheters
New TechnologyMultielectrode
Ablation Catheters
LSPV
LIPV
Catheter Positioning in Antrum of Left PVs

28
Balloon TechnologyBalloon TechnologyRSPVRSPV LSPVLSPV
StereotaxisRemote Magnetic Control
StereotaxisRemote Magnetic Control
29
Atrial FibrillationNew Technology / Studies at
Ohio State University
Atrial FibrillationNew Technology / Studies at
Ohio State UniversityStereotaxis – Magnetic Catheter Navigation
New Catheter Design / Energy Sources High Intensity Focused Ultrasound (HIFU)Ablation Frontiers – Circular CathetersCryoablationLaser Ablation
Cabana trial – Drug vs Ablation (including primary therapy)
Watchman – Left Atrial Appendage ClosureSurgical vs Catheter Ablation