atorvastatin clinical study program. introduction - atorvastatin indications: atorvastatin is...
TRANSCRIPT
Atorvastatin Clinical Study Program
Atorvastatin Clinical Program
• Atorvastatin Studies fall into 3 main areas:– Lipid Efficacy and Safety Studies : ACCESS,ASSET,CHALLENGE
– Intermediate/Surrogate Endpoint Studies : ASAP, BELLES,PVD, REVERSAL,
SAGE
– Clinical Endpoint Studies : ALLIANCE, ASCOT,ASPEN,AVERT, CARDS,
4D,IDEAL, MIRACL,Saint Francis Heart Study, SPARCL, TNT
• Close to 400 atorvastatin clinical trial protocols
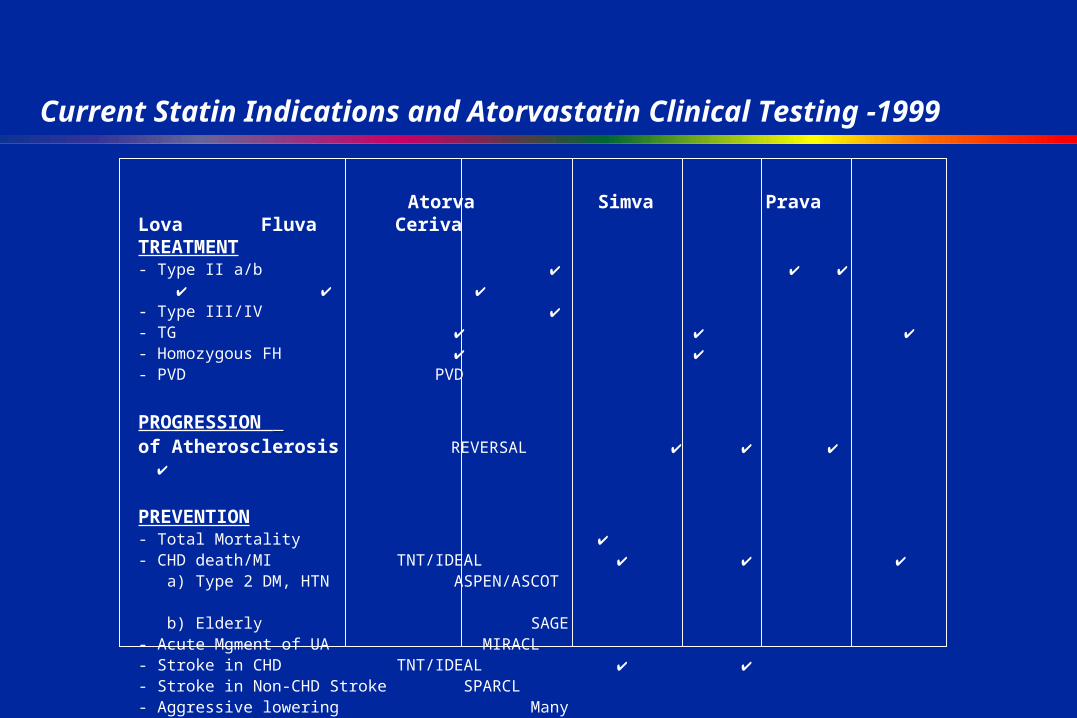
Current Statin Indications and Atorvastatin Clinical Testing -1999
Atorva Simva Prava Lova Fluva CerivaTREATMENT- Type II a/b - Type III/IV - TG - Homozygous FH - PVD PVD
PROGRESSION of Atherosclerosis REVERSAL
PREVENTION- Total Mortality - CHD death/MI TNT/IDEAL a) Type 2 DM, HTN ASPEN/ASCOT b) Elderly SAGE - Acute Mgment of UA MIRACL- Stroke in CHD TNT/IDEAL - Stroke in Non-CHD Stroke SPARCL- Aggressive lowering Many
- Indications
Major Objective of the Atorvastatin Clinical Study Program
• To provide scientific answers to many of the remaining questions in the area of lipidology and the clinical consequences of atherosclerosis.
Key Question
Is aggressive lipid lowering associated with acute event reduction in patients with unstable coronary syndromes?
MIRACL Rationale
• Background– No early separation in CHD event rates seen in major statin trials
– However, studies have systematically excluded acute patients
• 4S- entry >6 months post event
• CARE- entry 3 to 20 months post event
• LIPID- entry 3 months to 3 years post event
– Hypothesis: improved endothelial function and plaque stabilization with aggressive lipid lowering will reduce acute CHD risk
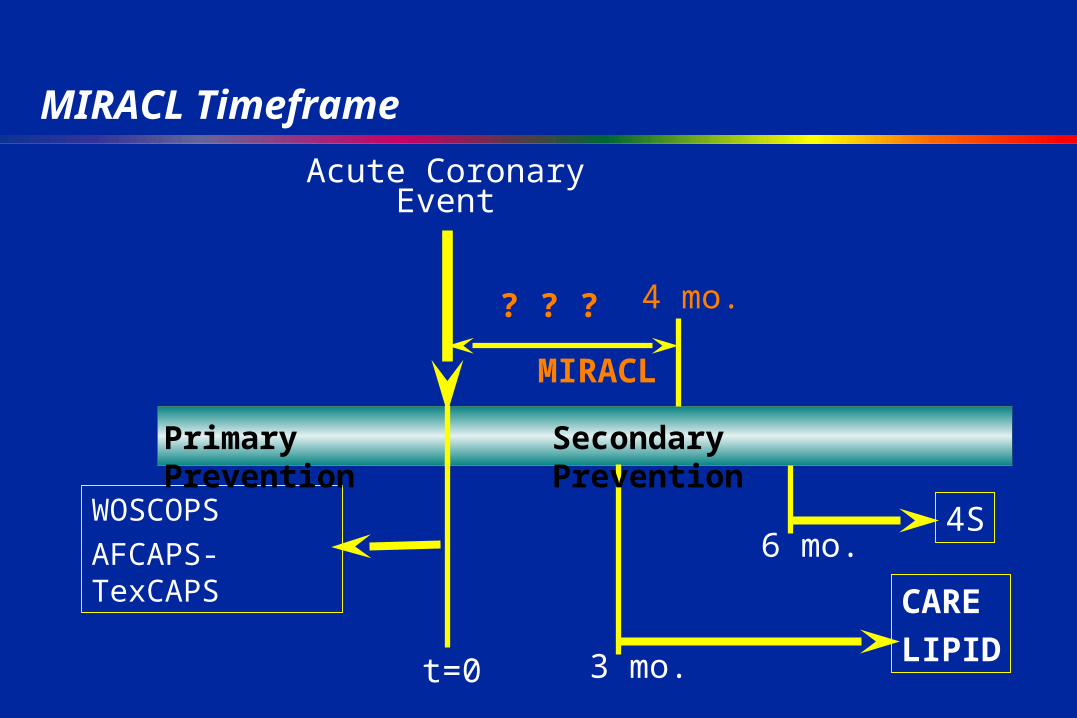
MIRACL Timeframe
Acute CoronaryEvent
MIRACL
t=0
6 mo.4SWOSCOPS
AFCAPS-TexCAPS
Primary Prevention Secondary Prevention
3 mo.
CARE
LIPID
4 mo.? ? ?
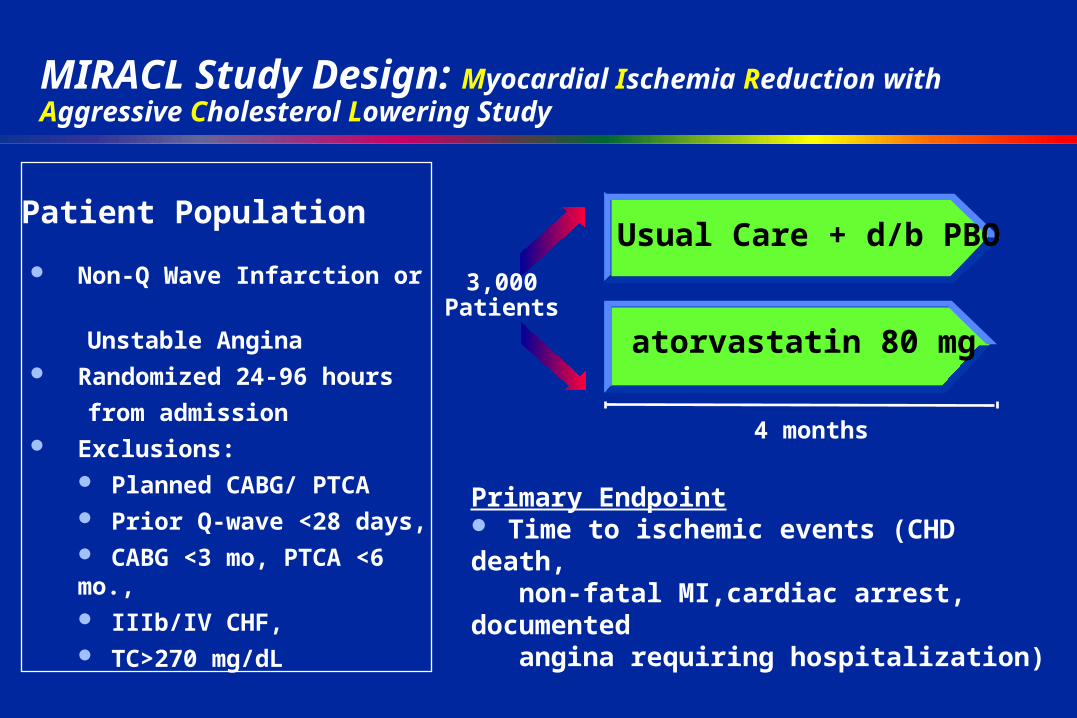
MIRACL Study Design: Myocardial Ischemia Reduction with Aggressive Cholesterol Lowering Study
4 months
atorvastatin 80 mg
3,000Patients
Usual Care + d/b PBO Non-Q Wave Infarction or
Unstable Angina Randomized 24-96 hours
from admission Exclusions:
Planned CABG/ PTCA Prior Q-wave <28 days, CABG <3 mo, PTCA <6 mo., IIIb/IV CHF, TC>270 mg/dL
Patient Population
Primary Endpoint Time to ischemic events (CHD death, non-fatal MI,cardiac arrest, documented angina requiring hospitalization)
Key Question
Does aggressive lipid lowering provide additional clinical benefits and cost-effective CHD event reductions in a managed care setting?
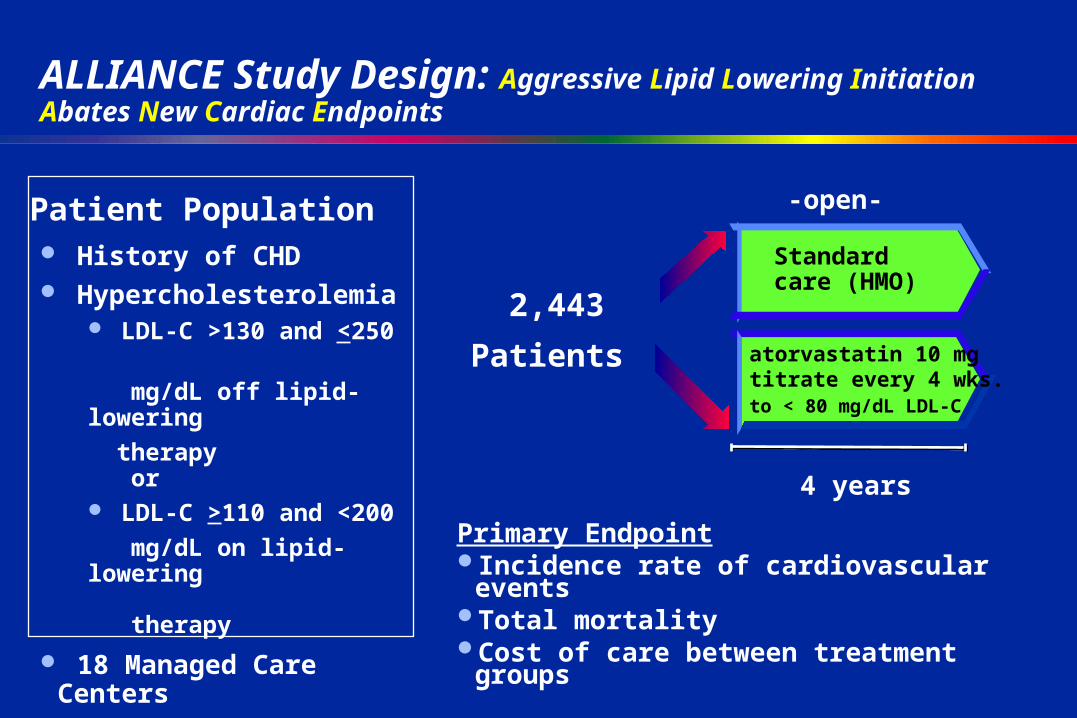
ALLIANCE Study Design: Aggressive Lipid Lowering Initiation Abates New Cardiac Endpoints
4 years
Primary EndpointIncidence rate of cardiovascular eventsTotal mortalityCost of care between treatment groups
History of CHD Hypercholesterolemia
LDL-C >130 and <250
mg/dL off lipid-lowering
therapy or LDL-C >110 and <200
mg/dL on lipid-lowering
therapy 18 Managed Care Centers
in USA
Patient PopulationStandardcare (HMO)
atorvastatin 10 mgtitrate every 4 wks.to < 80 mg/dL LDL-C
-open-
2,443 Patients
04/18/23 19:11P0168.PFIZER.Lipitor.Slide_Kit.A.dh07
Key Question
Can aggressive lipid lowering show changes in atheroma and demonstrate regression utilizing Intracoronary Ultrasound ?
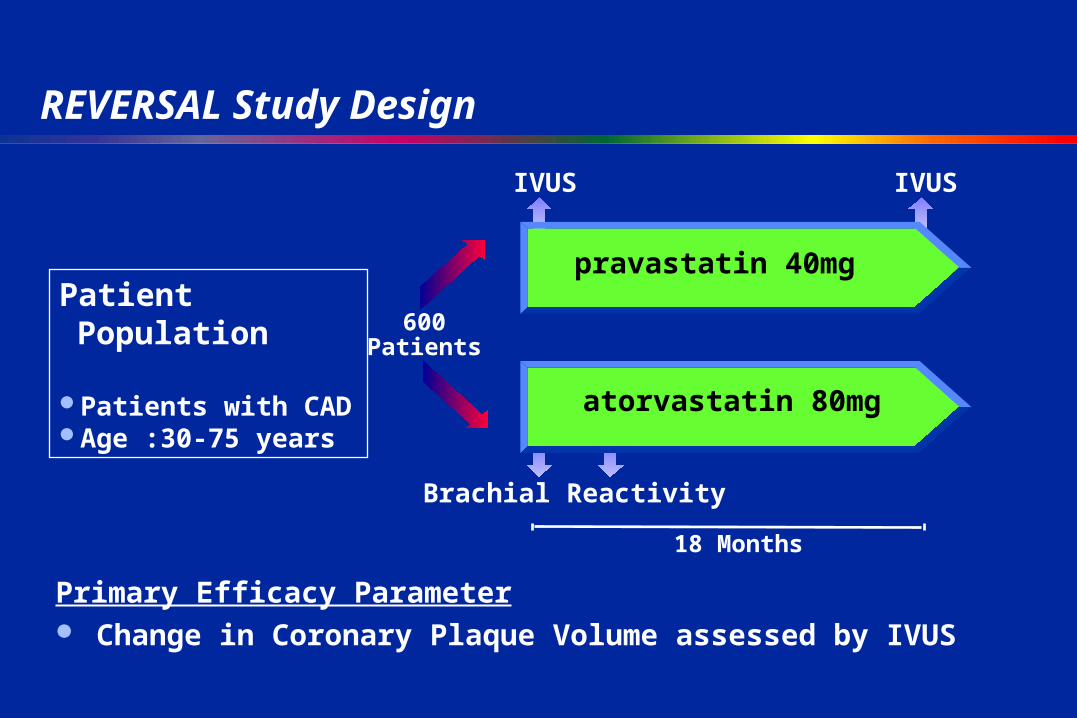
REVERSAL Study Design
IVUS
18 Months
600Patients
atorvastatin 80mg
IVUS
Brachial Reactivity
Patient Population
Patients with CAD Age :30-75 years
Primary Efficacy Parameter Change in Coronary Plaque Volume assessed by IVUS
pravastatin 40mg
Key Question
Does aggressive lipid lowering reduce coronary plaque burden more than moderate lipid lowering in post-menopausal dyslipidemic women ?
Aim : To determine whether aggressive lipid-lowering therapy with atorvastatin 80 mg/day compared with moderate treatment with pravastatin 40 mg/day can produce greater reductions in coronary artery calcification in postmenopausal women with hypercholesterolemia
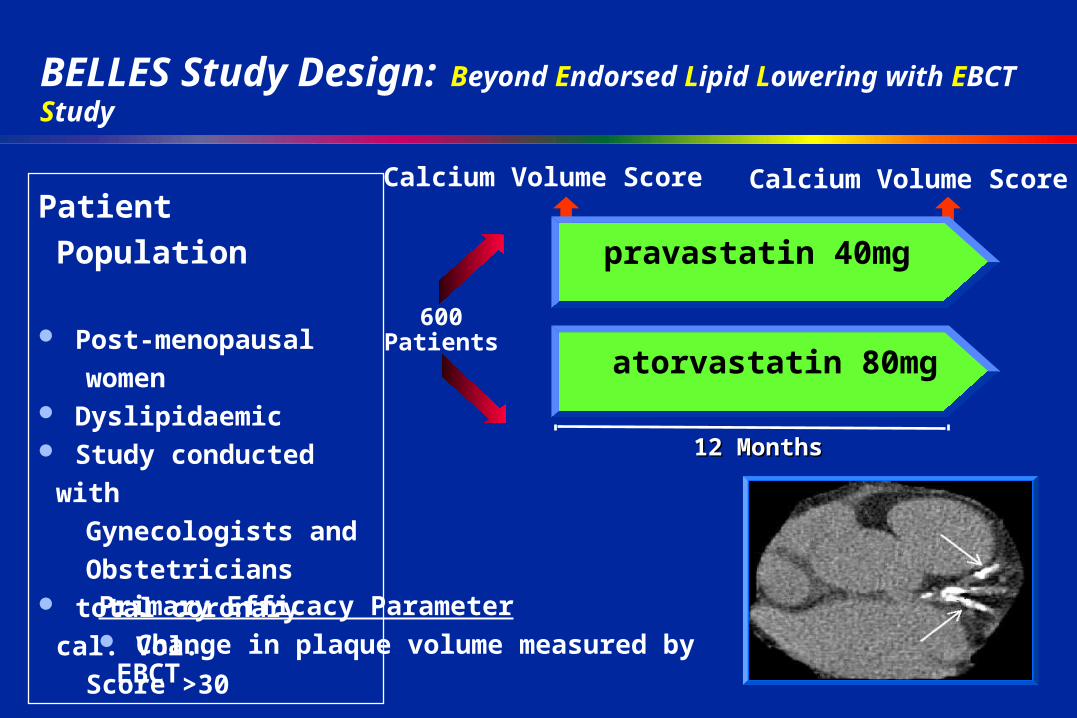
BELLES Study Design: Beyond Endorsed Lipid Lowering with EBCT Study
Calcium Volume Score
12 Months12 Months
pravastatin 40mg
600Patients
atorvastatin 80mg
Calcium Volume ScorePatient Population
Post-menopausal
women Dyslipidaemic Study conducted with
Gynecologists and
Obstetricians total coronary cal. Vol.
Score >30
Primary Efficacy Parameter Change in plaque volume measured by EBCT
BELLES Study
• EBCT : Electron Beam Computed Tomography is a noninvasive technique that is becoming the method of choice for evaluating atherosclerosis progression as a surrogate marker for atherosclerotic disease
Key Question
Does robust lipid lowering reduce ischemic events in type 2 diabetics?
Aim : To assess the efficacy of atorvastatin 10 mg vs placebo in the prevention of CHD in patients with type 2 diabetes with or without previous MI
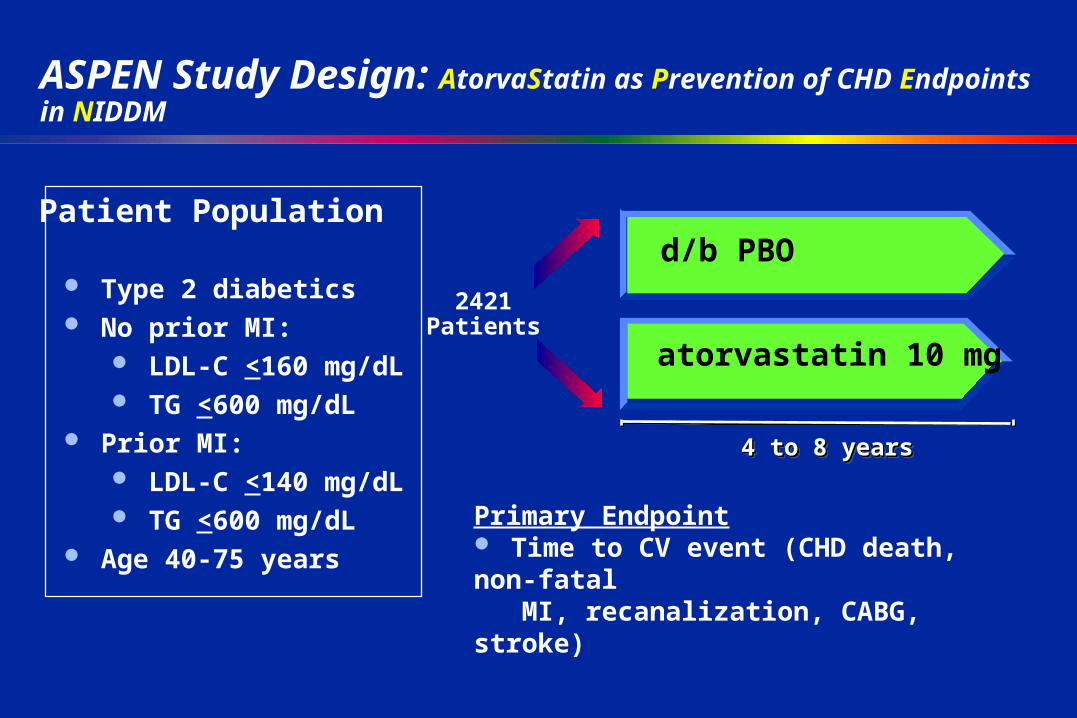
ASPEN Study Design: AtorvaStatin as Prevention of CHD Endpoints in NIDDM
4 to 8 years4 to 8 years4 to 8 years4 to 8 years
atorvastatin 10 mg
2421Patients
d/b PBO Type 2 diabetics No prior MI:
LDL-C <160 mg/dL TG <600 mg/dL
Prior MI: LDL-C <140 mg/dL TG <600 mg/dL
Age 40-75 years
Patient Population
Primary Endpoint Time to CV event (CHD death, non-fatal MI, recanalization, CABG, stroke)
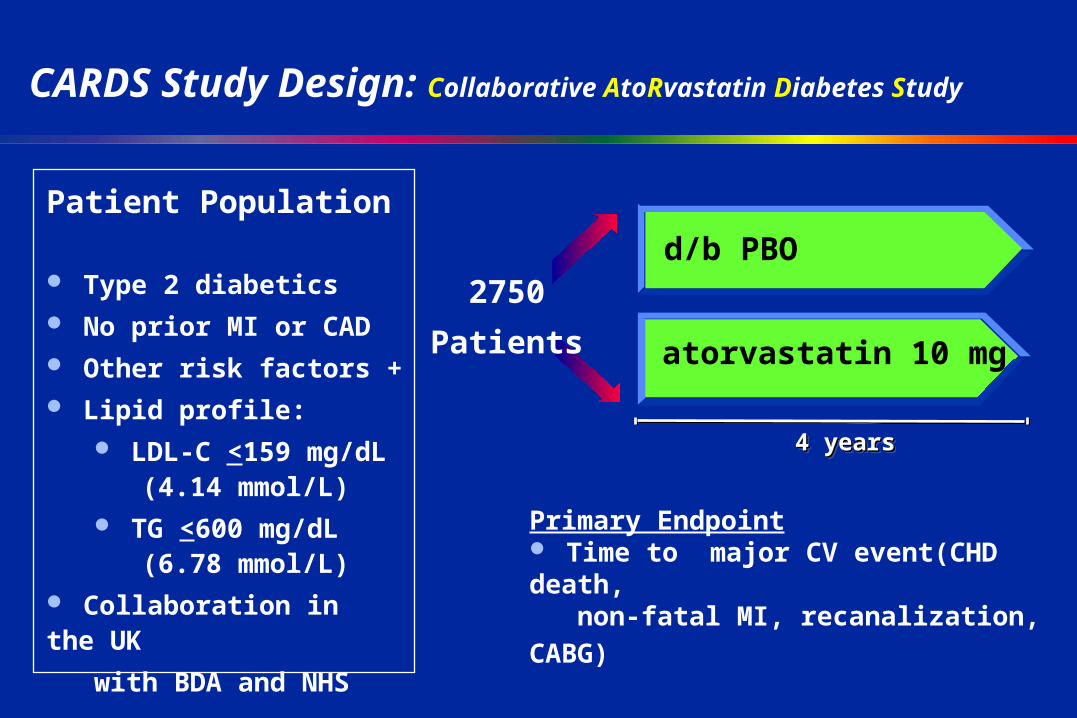
CARDS Study Design: Collaborative AtoRvastatin Diabetes Study
4 years4 years4 years4 years
atorvastatin 10 mg
2750
Patients
d/b PBO
Patient Population
Type 2 diabetics No prior MI or CAD Other risk factors + Lipid profile:
LDL-C <159 mg/dL (4.14 mmol/L) TG <600 mg/dL (6.78 mmol/L)
Collaboration in the UK
with BDA and NHS
Primary Endpoint Time to major CV event(CHD death,
non-fatal MI, recanalization, CABG)
Key Question
Does aggressive lipid lowering produce reductions in event rates for NIDDM patients with end stage renal failure ?
Aim : To determine whether atorvastatin 20 mg will provide greater reductions in cardiovascular mortality rates and nonfatal MI than placebo in patients with type 2 diabetes who have undergone hemodialysis for no more than 2 years
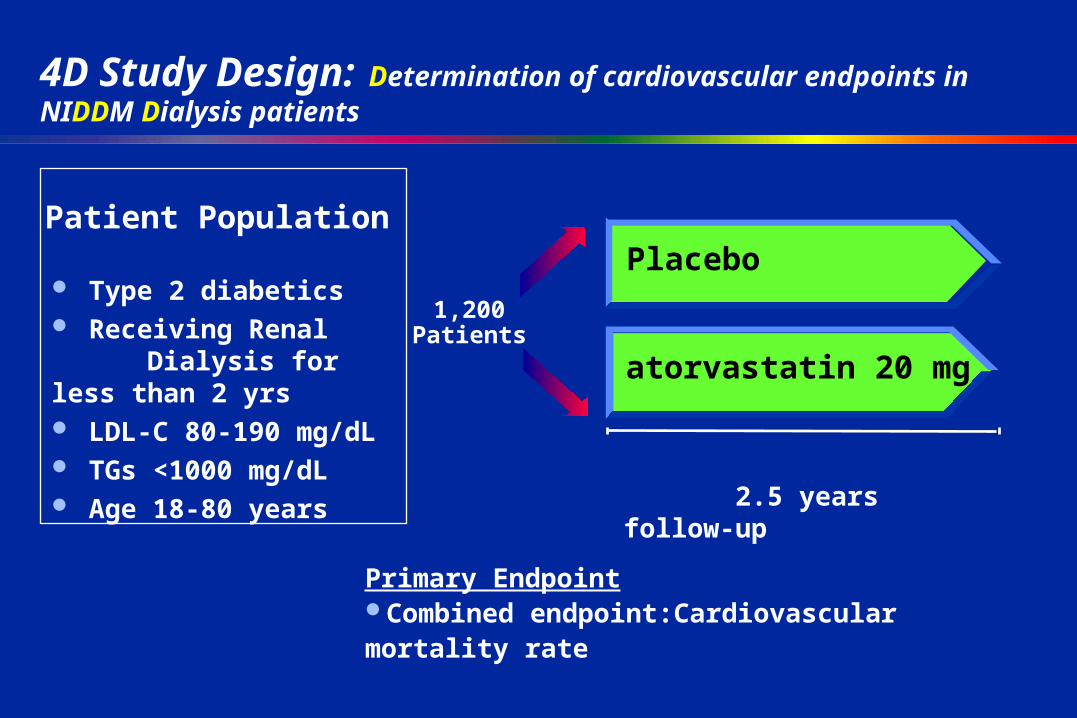
4D Study Design: Determination of cardiovascular endpoints in NIDDM Dialysis patients
atorvastatin 20 mg
Placebo
1,200Patients
Primary EndpointCombined endpoint:Cardiovascular mortality rate
Patient Population
Type 2 diabetics Receiving Renal Dialysis for less than 2 yrs LDL-C 80-190 mg/dL TGs <1000 mg/dL Age 18-80 years
2.5 years follow-up
Key Question
Does robust lipid lowering reduce ischemic events in hypertensives with “normal” cholesterol levels?
Aim : To compare the effects of atorvastatin 10 mg with placebo on the incidence of nonfatal MI and fatal CHD in hypertensive patients with TC level <= 250 mg/dL
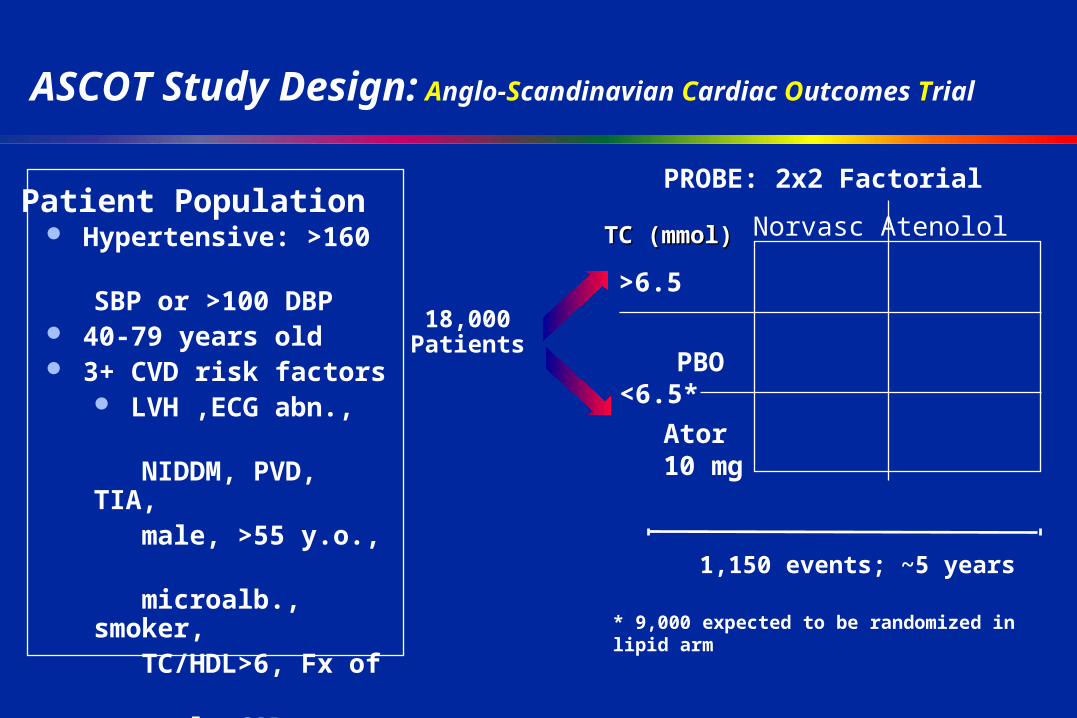
ASCOT Study Design: Anglo-Scandinavian Cardiac Outcomes Trial
1,150 events; ~5 years
18,000Patients
Hypertensive: >160 SBP or >100 DBP 40-79 years old 3+ CVD risk factors
LVH ,ECG abn., NIDDM, PVD, TIA, male, >55 y.o., microalb., smoker, TC/HDL>6, Fx of early CAD
Scandinavian and UK centers
Patient PopulationPROBE: 2x2 Factorial
Norvasc AtenololTC (mmol)TC (mmol)
>6.5
<6.5*PBO
Ator10 mg
* 9,000 expected to be randomized in lipid arm
ASCOT Study
• 1th endpoints : nonfatal MI, fatal CHD
• 2nd endpoints: all-cause mortality
» fatal and nonfatal stroke» » fatal and nonfatal heart failure
Key Question
Does robust lipid lowering reduce the occurrence of stroke in patients without CHD?
Aim : To determine whether aggressive cholesterol-lowering therpy with atorvastatin 80 mg can reduce the incidence of cerebrovascular endpoints compared with placebo in patients with out a history of CHD who have experienced a prior stroke or TIA
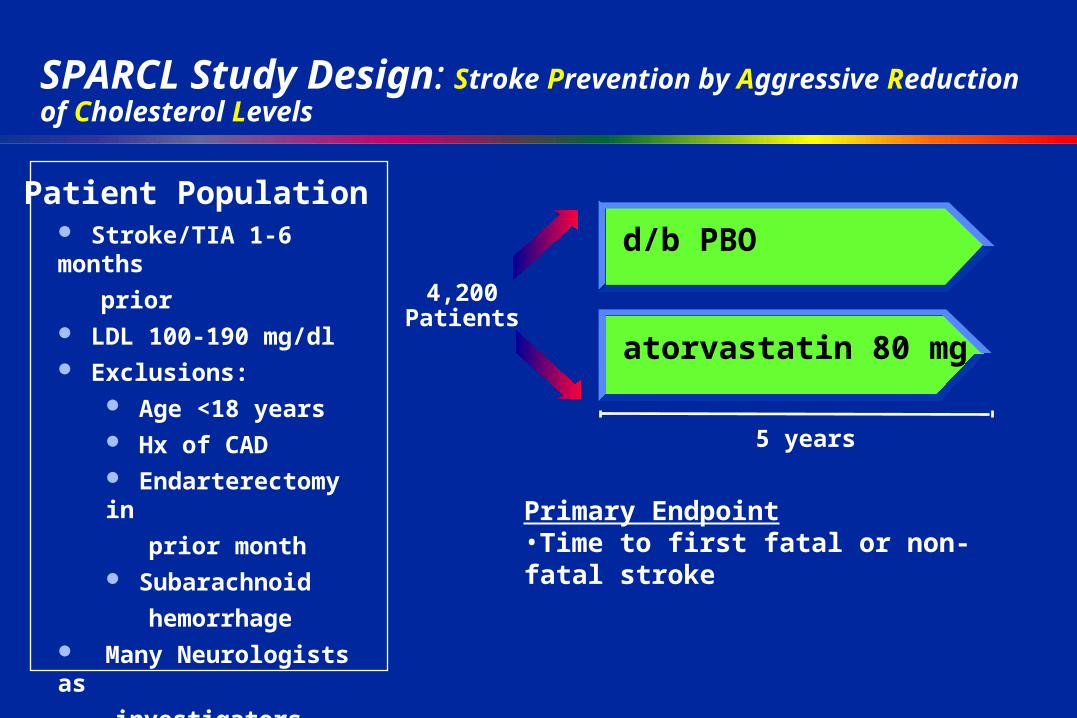
SPARCL Study Design: Stroke Prevention by Aggressive Reduction of Cholesterol Levels
5 years
atorvastatin 80 mg
4,200Patients
d/b PBO Stroke/TIA 1-6 months
prior LDL 100-190 mg/dl Exclusions:
Age <18 years Hx of CAD Endarterectomy in
prior month Subarachnoid
hemorrhage Many Neurologists as
investigators
Patient Population
Primary Endpoint•Time to first fatal or non-fatal stroke
Key Question
Does aggressive lipid lowering produce additional coronary benefit beyond that shown with other therapy or currently recommended guidelines ?
Aim : To assess whether reducing LDL-C aggressively to 75 mg/dL will provide a greater reduction in CHD events than lowering LDL-C more moderately to 100 mg/dL
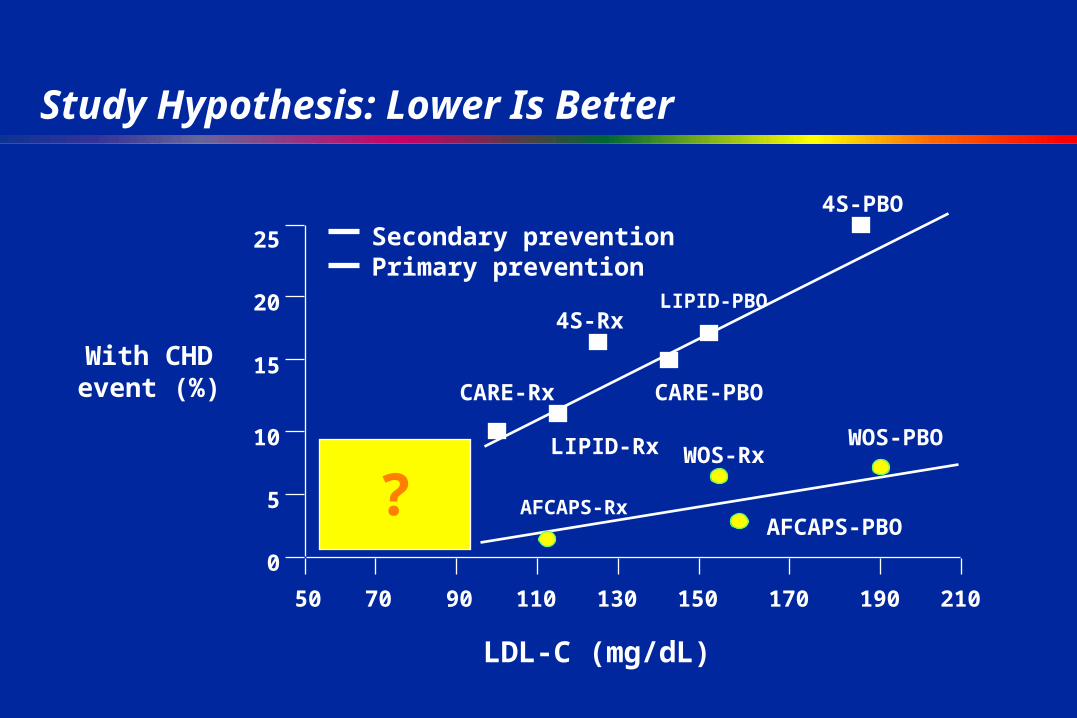
Study Hypothesis: Lower Is Better
With CHDevent (%)
50 70 90 110 130 150 170 190 210
0
5
10
15
20
25
LIPID-Rx
CARE-PBOCARE-Rx
4S-RxLIPID-PBO
4S-PBO
AFCAPS-Rx
WOS-RxWOS-PBO
AFCAPS-PBO
LDL-C (mg/dL)
Secondary preventionPrimary prevention
?
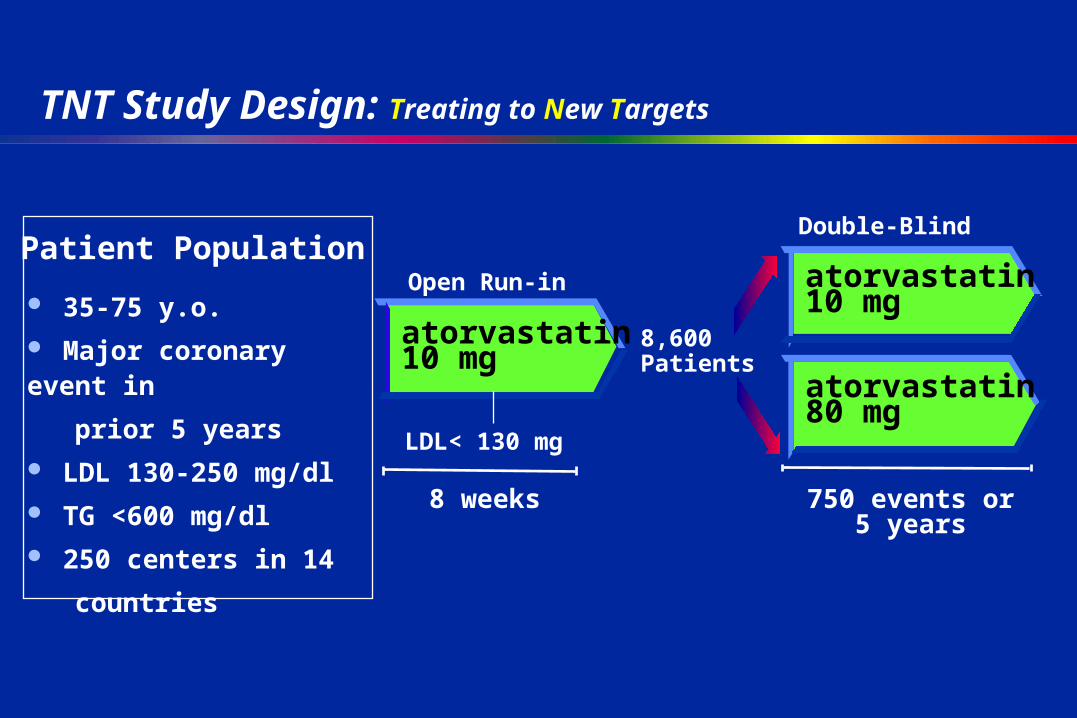
TNT Study Design: Treating to New Targets
750 events or5 years
atorvastatin 80 mg
atorvastatin 10 mg 35-75 y.o.
Major coronary event in
prior 5 years
LDL 130-250 mg/dl
TG <600 mg/dl
250 centers in 14
countries
Patient Population
atorvastatin 10 mg
LDL< 130 mg
Open Run-in
Double-Blind
8,600Patients
8 weeks
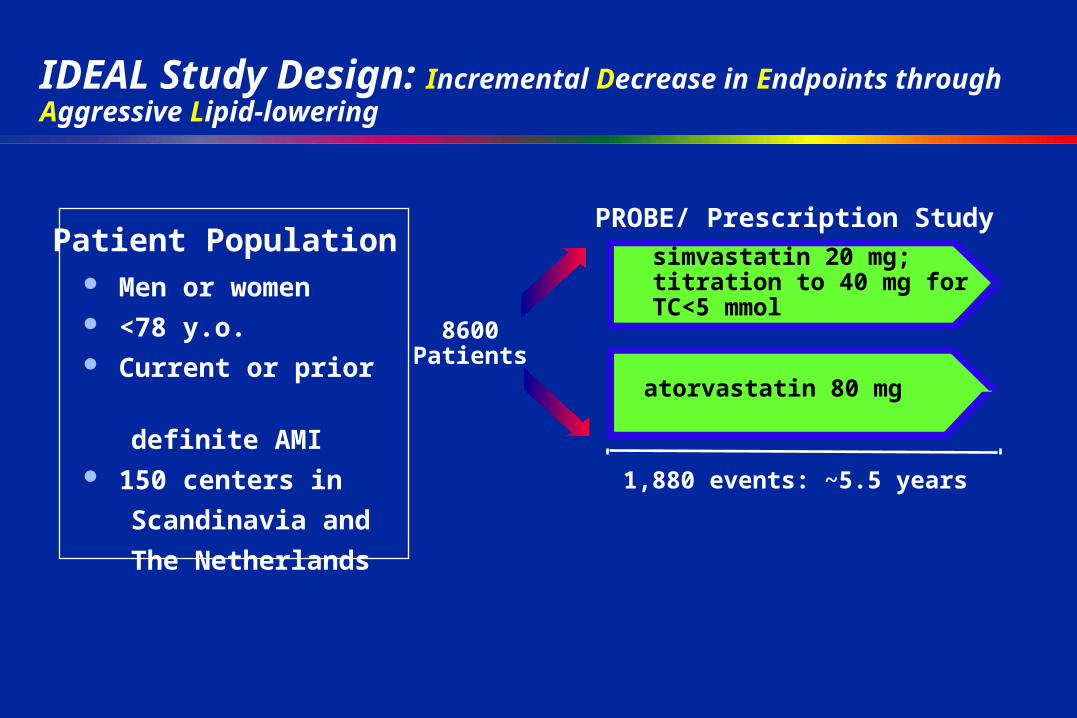
IDEAL Study Design: Incremental Decrease in Endpoints through Aggressive Lipid-lowering
1,880 events: ~5.5 years
atorvastatin 80 mg
8600Patients
simvastatin 20 mg; titration to 40 mg for TC<5 mmol
Men or women <78 y.o. Current or prior
definite AMI 150 centers in
Scandinavia and
The Netherlands
Patient PopulationPROBE/ Prescription Study
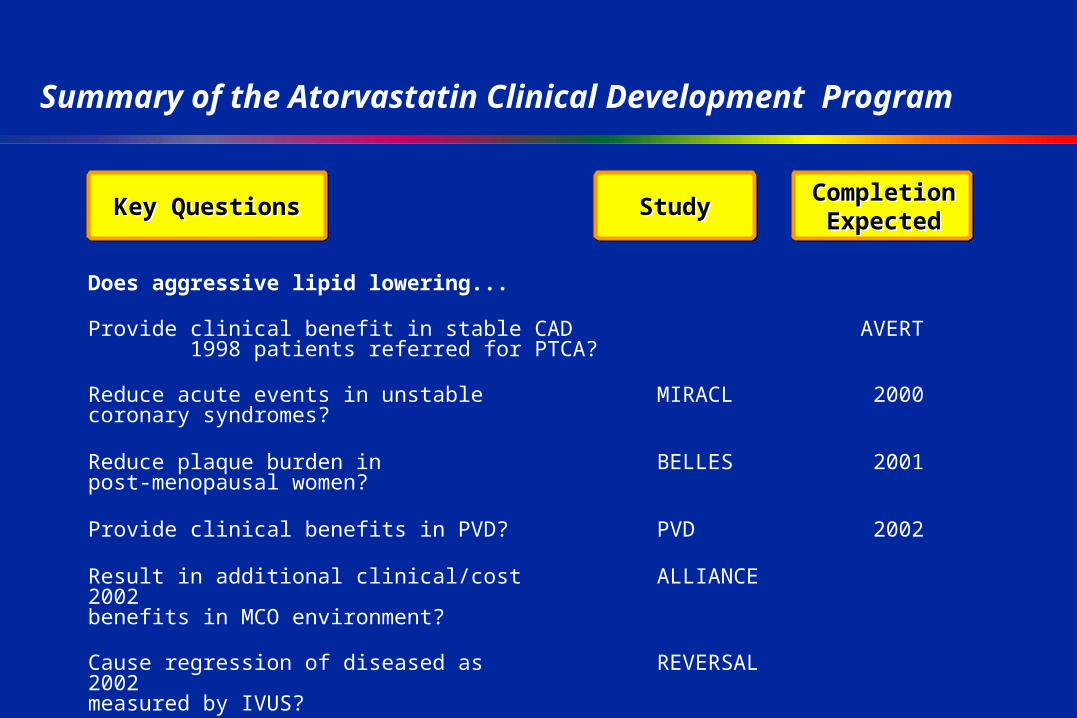
Summary of the Atorvastatin Clinical Development Program
Completion Expected
Completion ExpectedStudyStudyKey QuestionsKey Questions
Does aggressive lipid lowering...
Provide clinical benefit in stable CAD AVERT 1998 patients referred for PTCA?
Reduce acute events in unstable MIRACL 2000coronary syndromes?
Reduce plaque burden in BELLES 2001post-menopausal women?
Provide clinical benefits in PVD? PVD 2002
Result in additional clinical/cost ALLIANCE 2002benefits in MCO environment?
Cause regression of diseased as REVERSAL 2002measured by IVUS?
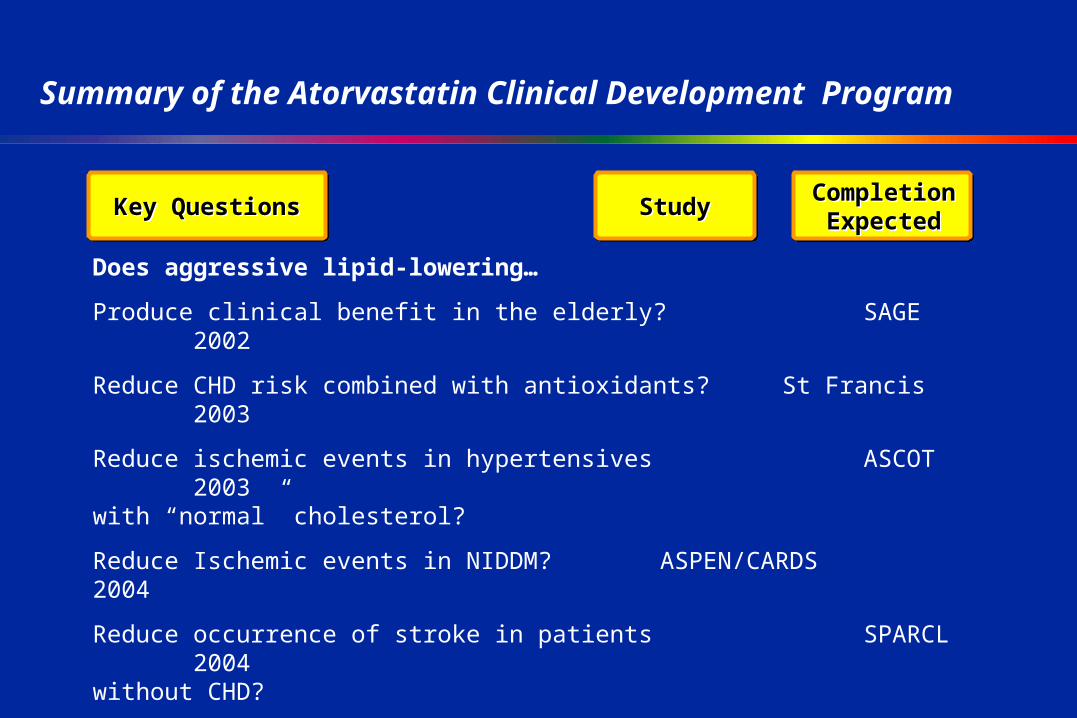
Summary of the Atorvastatin Clinical Development Program
Completion Expected
Completion ExpectedStudyStudyKey QuestionsKey Questions
Does aggressive lipid-lowering…
Produce clinical benefit in the elderly? SAGE 2002
Reduce CHD risk combined with antioxidants? St Francis 2003
Reduce ischemic events in hypertensives ASCOT 2003with “normal” cholesterol?
Reduce Ischemic events in NIDDM? ASPEN/CARDS 2004
Reduce occurrence of stroke in patients SPARCL 2004without CHD?
Produce additional CV benefit beyond IDEAL/TNT 2004/5that shown with other therapies (IDEAL) or beyond current recommended guidelines (TNT)?
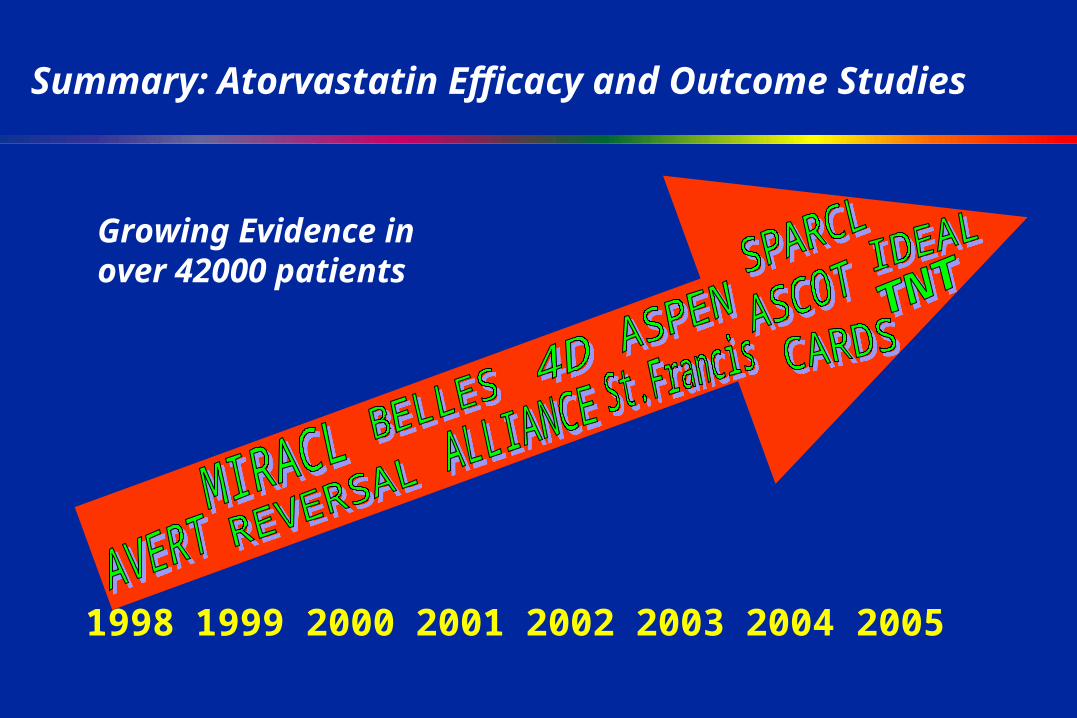
Summary: Atorvastatin Efficacy and Outcome Studies
1998 1999 2000 2001 2002 2003 2004 2005
Growing Evidence in over 42000 patients