assuring accurate reporting on irs form 990, schedule h · assuring accurate reporting on irs form...
TRANSCRIPT

Assuring Accurate Reporting on IRS Form 990,
Schedule H
Keith Hearle
President
Verité Healthcare Consulting, LLC
September 2015

© Verité Healthcare Consulting, LLC, 2015 2
Webinar Objectives
Discuss importance of accurate IRS Form 990,
Schedule H filings
Identify issue areas (e.g., examples of potential
under-reporting) and response strategies
Questions and answers

© Verité Healthcare Consulting, LLC, 2015 3
Brief History and Context
Concerns about tax-
exempt hospitals
Redesigned form 990 and Schedule H
PPACA:
new “501(r)” requirements
501(r) Implementing
rules

© Verité Healthcare Consulting, LLC, 2015 4
Schedule H Walk-Through
Part I: Financial Assistance and Certain Other Community Benefits at Cost
Part II: Community Building Activities
Part III: Bad Debt, Medicare, & Collection Practices
Part VI: Management Companies and Joint Ventures
Part V: Facility Information
Section A. Hospital Facilities
Section B. Facility Policies and Practices
Section C. Supplemental Information for Part V, Section B
Section D. Other Health Care Facilities (not hospitals)
Part VI: Supplemental Information

© Verité Healthcare Consulting, LLC, 2015 5
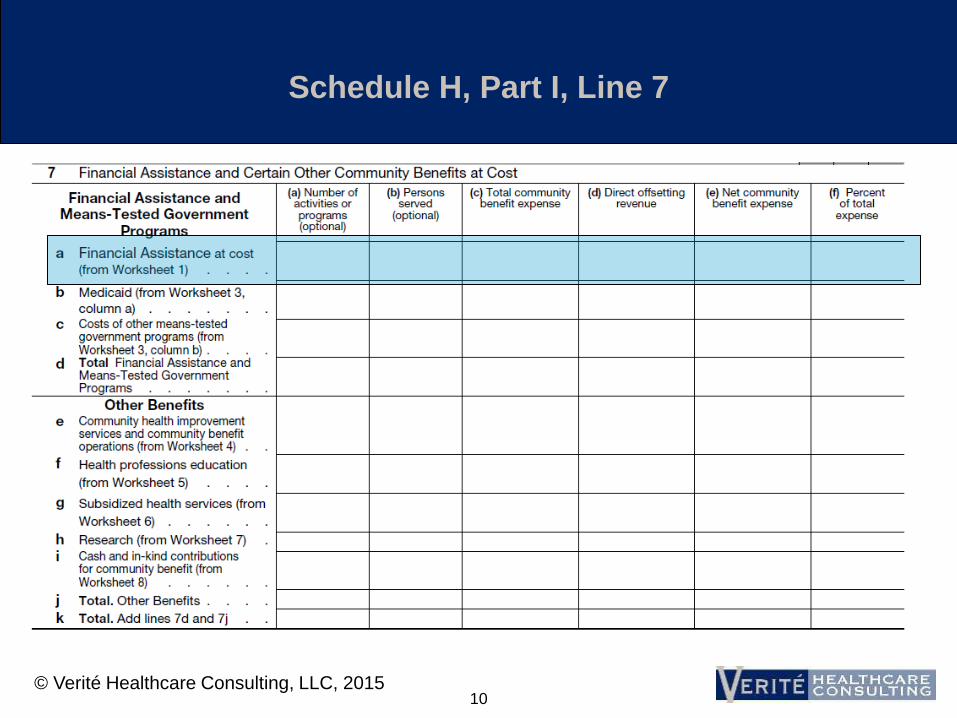
Schedule H, Part I, Line 7

© Verité Healthcare Consulting, LLC, 2015 6
IRS: What Counts as Community Benefit?
To count, a program or activity must respond to a demonstrated health/related community need and seek to achieve at least one community benefit objective:
• Improve Access to Health Services
• Enhance Public Health
• Advance Generalizable Knowledge
• Relief of a Government Burden to Improve Health

© Verité Healthcare Consulting, LLC, 2015 7
IRS: Programs that should not be counted
Activities or programs may not be reported:
• if they are provided primarily for marketing
purposes
• the program is more beneficial to the organization
than to the community; for instance,
– if the activity or program is designed primarily to
increase referrals of patients with third-party coverage,
– required for licensure or accreditation, or
– restricted to individuals affiliated with the organization.

© Verité Healthcare Consulting, LLC, 2015 8
Programs that should not be counted: additional
considerations (not in IRS Instructions)
An objective, “prudent layperson” would
question whether the program was established
primarily to benefit the community
The program represents a community benefit
that does not involve a reportable expense by
the organization, e.g.
• Benefits provided by employees on their own time
• Expense is not present in Form 990, Part IX

© Verité Healthcare Consulting, LLC, 2015 9
Programs that should not be counted: additional
considerations (not in IRS Instructions)
The initiative is designed only to benefit the
organization’s own patients or covered lives, e.g.
• Programs to prevent or reduce readmissions for
discharged patients
• Programs to reduce PMPM costs for patients/
members for whom the organization bears risk (or
might participate in shared savings)
9
© Verité Healthcare Consulting, LLC, 2015 10
Schedule H, Part I, Line 7

© Verité Healthcare Consulting, LLC, 2015 11
Reporting Strategies:
Financial Assistance
Assess ratio of bad debt to charity over time
Adjust Financial Assistance Policies:
• Include medical indigency (catastrophic) provisions
• Include presumptive eligibility
• Assure discounts align with Final Rule requirements
Use predictive modeling for accounts with bad debt and without completed applications (“the unknowns”)
Accelerate decision-making process
Reverse self-pay discounts for accounts with any financial assistance
11

© Verité Healthcare Consulting, LLC, 2015 12
Ratio of Patient Care Cost to Charges
12

© Verité Healthcare Consulting, LLC, 2015 13
Reporting Strategies:
Ratio of Patient Care Cost to Charges
Accuracy Strategies:
• Adjust the ratio so that community benefit expenses
are not double counted
– Only adjust the numerator of the ratio for amounts that are in
total operating expense
Maximization Strategies:
• Cost out “nonpatient care activities” rather than using
“other operating revenue” as a proxy
• Consider using a “more accurate cost accounting
method,” as allowed by instructions
13

© Verité Healthcare Consulting, LLC, 2015 14
Schedule H, Part I, Line 7

© Verité Healthcare Consulting, LLC, 2015 15
Reporting Strategies:
Medicaid and Other Means Tested Government
Programs
Include both Medicaid fee for service and Medicaid managed
care activities – from all states
Align offsetting revenue with GAAP financial statements, but
exclude direct GME revenue and include any IME
Include expense of provider tax, fees, assessments used to
maximize federal Medicaid matching funds
Assure that Medicaid managed care recipients are accounted
for as Medicaid
Use “most accurate” cost accounting method
Discussion: how to handle DSRIP revenues and program
expenses
15

© Verité Healthcare Consulting, LLC, 2015 16
Schedule H, Part I, Line 7

© Verité Healthcare Consulting, LLC, 2015 17
Community Health Improvement Categories
Community health education outreach
Community-based clinical services where there is no patient bill
Health care support services, e.g.:
• Enrollment assistance for Medicaid and other government-funded health
programs for lower-income people
• Cost of software tools that support decision making for granting financial
assistance at the beginning of the revenue cycle
• Transportation to improve access for lower-income people (not to increase
referrals)
Social and environmental improvement activities (e.g., removing
lead, violence prevention, eliminating food deserts)
17

© Verité Healthcare Consulting, LLC, 2015 18
Community Benefit Operations Categories
Community health needs assessments
Community benefit program administration
Activities associated with fundraising or grant-
writing for community benefit programs
18

© Verité Healthcare Consulting, LLC, 2015 19
Reporting Strategies:
Community Health Improvement Services (and
Operations)
Assure that all programs and activities that can be
reported are identified (comprehensive inventory)
Assess whether certain community building programs
(Part II) qualify as community health improvement (Part
1, Line 7e)
Assure that total expense includes both direct cost and
indirect cost
Include an auditable portion of “system-office” cost
(management fee/corporate allocation) in “community
benefit operations”
19

© Verité Healthcare Consulting, LLC, 2015 20
Schedule H, Part I, Line 7

© Verité Healthcare Consulting, LLC, 2015 21
Reporting Strategies:
Health Professions Education
Assure Schedule H incorporates a full inventory of
all reportable health professions education programs
Assess transactions (flows of funds) between
teaching hospital and medical school (and other
affiliates) to assure that all health professions
education expense is identified
Do not include Medicare and Medicaid “Indirect
Medical Education” reimbursement in offsetting
revenue
21

© Verité Healthcare Consulting, LLC, 2015 22
Schedule H, Part I, Line 7

© Verité Healthcare Consulting, LLC, 2015 23
Subsidized Health Services
“Subsidized health services” means clinical services
provided despite a financial loss to the organization.
• The financial loss is measured after removing losses,
measured by cost, associated with bad debt, charity
care, Medicaid and other means-tested government
programs.
In addition, in order to qualify as a subsidized health
service, the organization must provide the service
because it meets an identified community need.
23

© Verité Healthcare Consulting, LLC, 2015 24
Reporting Strategies:
Subsidized Health Services
Include subsidized health services, if any are
reportable during the tax year
• Requires annual assessment using cost accounting
information
Do not report services with gains during the tax
year (even if previously reported)
Rely on “most accurate” cost accounting
methodology available
24

© Verité Healthcare Consulting, LLC, 2015 25
Schedule H, Part I, Line 7

© Verité Healthcare Consulting, LLC, 2015 26
Reporting Strategies:
Research
Assure all research studies funded by a tax-exempt
source (creating expense on the books of the
organization filing Schedule H) have been identified
Base indirect costs on NIH guidelines and not the
actual, indirect cost factor negotiated between the
organization and NIH
Consider which entity (EIN) should bear the cost of
research studies
26

© Verité Healthcare Consulting, LLC, 2015 27
Schedule H, Part I, Line 7

© Verité Healthcare Consulting, LLC, 2015 28
Cash and In-Kind Contributions
“Cash and in-kind contributions” means
contributions made by the organization to health
care organizations and other community groups
that are restricted, in writing, to one or more of
the community benefit activities described in the
Table in Part I, line 7 (or the Worksheets
thereto).
Do not include amounts involving a quid pro quo
arrangement.
28

© Verité Healthcare Consulting, LLC, 2015 29
Reporting Strategies:
Cash and In-Kind Contributions
Place restrictions on cash contributions
Include the value of time spent by staff
supporting community health work as in-kind
donation
Assure that all contributions being made by the
system and its affiliates are accounted for as
expense by the hospital organization(s)
Describe unrestricted donations/sponsorships in
Part VI
29
© Verité Healthcare Consulting, LLC, 2015 30
Part II – Community Building
Line 1: “Physical improvements and housing”
Line 2: “Economic development”
Line 3: “Community support”
Line 4: “Environmental improvements”
Line 5: “Leadership development and training for community members”
Line 6: “Coalition building”
Line 7: “Community health improvement advocacy”
Line 8: “Workforce development”
Line 9: “Other community building activities or programs”
Programs that, while not directly related to health care, provide
opportunities to address the root causes of health problems such as
poverty, homelessness, and environmental problems
30

© Verité Healthcare Consulting, LLC, 2015 31
Community Building, Continued
Change to Community Building instructions:
• 2010: “Report in this part … activities … to
protect health or safety, and that are not
reportable in Part I or III …”
• 2011: “Some community building activities may
also meet the definition of community benefit. Do
not report in Part II community building costs that
are reported on Part I, line 7 … as … a
community health improvement service
reportable on Part I, Line 7e”
31

© Verité Healthcare Consulting, LLC, 2015 32
Contact Information
Keith Hearle
President Verite Healthcare Consulting, LLC
Alexandria, VA
www.veriteconsulting.com

© Verité Healthcare Consulting, LLC, 2015 33
Questions
33

Healthcare Association of New York State www.hanys.org
HANYS’ Contacts
Schedule H Analysis: • Bob McLeod
• Pam Payette [email protected]
Community Health • Sue Ellen Wagner
• Donna Evans [email protected]
34