association of the extension for community healthcare
TRANSCRIPT

Original Investigation | Public Health
Association of the Extension for Community Healthcare Outcomes ProjectWith Use of Direct-Acting Antiviral Treatment Among US Adults With Hepatitis CLinh Tran, BA; Roger Feldman, PhD; Thomas Riley III, MD, MS; Jeah Jung, PhD, MPH
Abstract
IMPORTANCE Direct-acting antiviral (DAA) medications are highly effective in treating hepatitis Cvirus (HCV) infection. However, use of DAAs in rural and underserved areas is low owing to limitedaccess to specialist physicians with experience in care of HCV infection. Project ECHO (Extension forCommunity Healthcare Outcomes) is a distance education model that trains primary care physiciansto improve access to care for underserved populations with complex diseases such as HCV infection.Evidence on whether Project ECHO is associated with increased DAA use is limited.
OBJECTIVE To examine the association between Project ECHO and use of DAA treatment inpatients with HCV infection.
DESIGN, SETTING, AND PARTICIPANTS This cohort study used data from Medicare beneficiarieswho newly sought care for HCV infection between January 1, 2014, and December 31, 2017. Datawere analyzed between September and December 2020.
EXPOSURES Project ECHO.
MAIN OUTCOMES AND MEASURES Use of DAA treatment. Discrete-time hazard models with stateand year fixed effects were used to examine the association between Project ECHO and DAA use inrural areas and areas with low specialist density.
RESULTS A total of 267 908 patients (mean [SD] age, 60.7 [11.5] years; 57.9% male; 66.6% Whitepatients) were included in the analysis. For every 100 clinicians attending a Project ECHO training,the odds of DAA treatment initiation among patients with HCV infection increased by 9% (adjustedodds ratio [OR], 1.09; 95% CI, 1.07-1.11; P < .001) in nonrural areas with specialist density equaling 0.The association between DAA use and Project ECHO was stronger in areas with lower vs higherspecialist density. For every additional 100 Project ECHO participants, the odds of DAA usedecreased by 1% as specialist density in the area increased (adjusted OR, 0.99; 95% CI, 0.98-1.00;P = .03). There was no association between Project ECHO and the odds of receiving DAAs amongpatients in rural vs urban areas (adjusted OR, 1.01; 95% CI, 0.99-1.02; P = .49).
CONCLUSIONS AND RELEVANCE In this cohort study, implementation of Project ECHO wasassociated with increased DAA use in areas with few specialist physicians, suggesting that ProjectECHO may enhance access to DAA treatment through expanding the capacity of primary carephysicians to treat HCV infection, especially in underserved areas.
JAMA Network Open. 2021;4(7):e2115523. doi:10.1001/jamanetworkopen.2021.15523
Key PointsQuestion Is Project ECHO (Extension
for Community Healthcare Outcomes),
a distance education model that trains
primary care physicians to improve
access to care for underserved
populations, associated with increased
use of direct-acting antiviral treatment
for hepatitis C virus (HCV) infection?
Findings In this cohort study of
267 908 patients, for every 100
additional clinicians who attended a
Project ECHO training session, the odds
that a patient with HCV infection would
receive a direct-acting antiviral agent
increased by 9%. Project ECHO was
associated with increased direct-acting
antiviral agent use in areas with few
specialist physicians compared with
areas with higher specialist density.
Meaning These results suggest that
Project ECHO may be a promising
strategy to improve access and reduce
barriers to treatment of HCV infection,
especially in underserved areas.
+ Supplemental content
Author affiliations and article information arelisted at the end of this article.
Open Access. This is an open access article distributed under the terms of the CC-BY License.
JAMA Network Open. 2021;4(7):e2115523. doi:10.1001/jamanetworkopen.2021.15523 (Reprinted) July 2, 2021 1/12
Downloaded From: https://jamanetwork.com/ on 04/06/2022

Introduction
Hepatitis C virus (HCV) infection is a public health concern, with approximately 2.7 to 3.9 millionpeople in the US having chronic infection.1 Untreated HCV infection can result in serious healthproblems, such as cirrhosis, hepatocellular cancer, and liver damage.2 Recently developed second-generation direct-acting antiviral (DAA) drugs have cure rates greater than 90%, which is higher thanthe 50% cure rate with former interferon-based treatments.3 In addition, DAAs are easy toadminister (1 pill per day), require a short treatment period (8-12 weeks), and have few adverseeffects. Direct-acting antiviral therapy is associated with a 49% to 68% reduction in HCV all-causemortality.3,4 The availability of DAAs has therefore given hope that HCV infection can be eliminated.5
The World Health Organization has set a goal of reducing the incidence of HCV infection by 80% by2030 and has recommended treating all adults with chronic HCV infection with DAAs.6,7
Despite the high cure rates of DAAs, use of DAA therapy is low at less than 50% between 2014and 2016 (the first DAA, sofosbuvir, was approved on December 1, 2013).1,8-11 Substantial rural-urbanvariation in receipt of DAA treatment exists.1 The main barriers to providing DAAs to rural populationsare the high cost of DAAs, lack of specialists with experience in care for HCV infection, and distanceand travel time.12-14 For example, patients from remote areas may wait up to 6 months and travel upto 250 miles for an appointment.13
Limited access to specialty services at community-based health centers is another reason whypatients fail to access treatment for HCV infection.13 Most primary care physicians (PCPs) do not feelcomfortable offering treatment for HCV infection owing to a lack of training, especially in resource-limited settings, and thus they often refer patients with HCV infection to specialty care.13,14
In response to the need for specialty services in rural and underserved areas, Project ECHO(Extension for Community Healthcare Outcomes), a telementoring program, was launched in 2003by the University of New Mexico Health Sciences Center.15 Project ECHO aims to reduce healthdisparities and expand access to medical care for underserved populations with complex conditions,such as HCV infection.15,16 Through the use of video conferencing technology, Project ECHO adoptsa hub-and-spoke approach to connect a specialist team (the hub) with PCPs or other health careprofessionals such as community health workers (the spokes).13,15,16 Primary care physicians canparticipate in Project ECHO at no cost.17 The only associated costs are those for technologyequipment (if needed) and time away from the clinic.17 Many Project ECHO sessions are offered inthe early morning or during lunch hours to minimize the time away from direct patient care.17 Afterparticipating in Project ECHO, PCPs can develop treatment plans and provide specialized services forpatients in their communities based on recommendations from the specialists at the hub.13,15,16
Project ECHO may be a promising approach to reduce the need for specialist referrals. Byproviding training and support for PCPs in prescribing DAAs, Project ECHO makes curative treatmentaccessible to patients living in underserved areas.18-20 Project ECHO–trained PCPs provide safe andeffective treatment for HCV infection in rural and remote areas with guidance and consultation fromspecialists.13 The quality of care for HCV infection delivered by ECHO-trained PCPs was reported tobe comparable to that of specialists.13,21
Evidence on the association of Project ECHO with DAA use is limited. One study found thatProject ECHO was associated with reduced urban-rural disparities in DAA uptake in 2 states.12
However, the results might not generalize beyond those 2 states. Thus, we extended the priorresearch by examining the association between Project ECHO and DAAs using national data fromMedicare, a federal health insurance program for older adults and those with disabilities in the US.Because many HCV-infected individuals in the US were born between 1945 and 1964,22 Medicarecovers a group with a high prevalence of HCV infection and thus has a substantial role in care for HCVinfection.
In addition to using national data, our study examined the association of Project ECHO withaccess to treatment for HCV infection in underserved areas with low specialist physician density.Although some states have discontinued their Project ECHO, trained PCPs may still be able to use
JAMA Network Open | Public Health Extension for Community Healthcare Outcomes Project and Hepatitis C Treatment
JAMA Network Open. 2021;4(7):e2115523. doi:10.1001/jamanetworkopen.2021.15523 (Reprinted) July 2, 2021 2/12
Downloaded From: https://jamanetwork.com/ on 04/06/2022

medical knowledge gained from past clinic sessions to deliver high-quality care to patients with HCVinfection in their own communities. Therefore, we measured Project ECHO by the cumulativenumber of attendees in HCV-specific ECHO sessions since its implementation in each state. Weexamined the association between Project ECHO and DAA treatment in a national cohort of Medicarebeneficiaries with HCV infection and evaluated whether that association was larger in underservedand rural areas.
Methods
DataThis cohort study used data from patients with HCV infection identified using Medicare claims forinpatient, skilled nursing facility, hospital outpatient, and physician services from January 1, 2013, toDecember 31, 2017 (2013 data were used only to ensure that patients did not seek care for HCVinfection in 2013). The initiation of DAAs was identified from Medicare Part D data from January 1,2014, to December 31, 2017. The institutional review board of the Pennsylvania State Universityapproved the study, and a waiver for informed consent was provided owing to the use of the existingadministrative data. This study followed the Strengthening the Reporting of Observational Studiesin Epidemiology (STROBE) reporting guideline.
We requested information on the annual number of physicians attending HCV-specific ProjectECHO clinic sessions from 2006 to 2017 from the University of New Mexico Health Sciences Center(data before 2006 were not available). Additional information on Project ECHO is availableelesewhere.23 We obtained patient demographic characteristics, health risks, and death dates fromMaster Beneficiary Summary Files; state-level total and rural population aged 45 years or older fromthe American Community Survey; county-level specialist density and number of PCPs from the AreaHealth Resources Files; and ZIP-level rurality of residence based on Rural-Urban CommutingArea codes.24
Study SampleThe study sample included fee-for-service Medicare beneficiaries who newly sought care for HCVinfection between January 1, 2014, and December 31, 2017, after a 1-year washout period. Thiscriterion identified patients who were at a relatively similar stage of seeking care for HCV infection.An index date for each beneficiary was the date of their first HCV-related claim after a 1-year periodwith no HCV-related claims. Patients with HCV infection were identified by the standard algorithmused by the Centers for Medicare & Medicaid Services25: at least 1 inpatient or skilled nursing facilityclaim or at least 2 hospital outpatient or physician claims for HCV infection in a given year. HepatitisC virus–related claims were identified using International Classification of Diseases, Ninth Revisioncodes 070.44, 070.54, 070.70, 070.71 or International Statistical Classification of Diseases andRelated Health Problems, Tenth Revision codes B18.2, B19.20, B19.21.
Although the first DAA (sofosbuvir) was approved by the US Food and Drug Administration inlate 2013, patients were required to take sofosbuvir and ribavirin with pegylated interferon.Interferon-based regimens were usually provided by specialists because of frequent adverse effects,suboptimal response rates, and long durations of treatment.19 Thus, patients who took sofosbuvirwith interferon were excluded from our analysis. We excluded patients residing in New Mexicobecause ECHO was first launched in New Mexico, and individuals from this state account for almosthalf of the cumulative number of attendees. This exclusion helped prevent the results from beingoverly affected by a single state. We included patients from New Mexico in a sensitivity analysis.
We excluded patients who died within 12 months after the index date because DAAs are notrecommended for patients with less than 1-year life expectancy.26 We excluded patients who did nothave continuous coverage in Medicare Part A (hospital and post–acute care), Part B (outpatientmedical care), and Part D (outpatient prescription drugs) throughout the entire year; those who
JAMA Network Open | Public Health Extension for Community Healthcare Outcomes Project and Hepatitis C Treatment
JAMA Network Open. 2021;4(7):e2115523. doi:10.1001/jamanetworkopen.2021.15523 (Reprinted) July 2, 2021 3/12
Downloaded From: https://jamanetwork.com/ on 04/06/2022
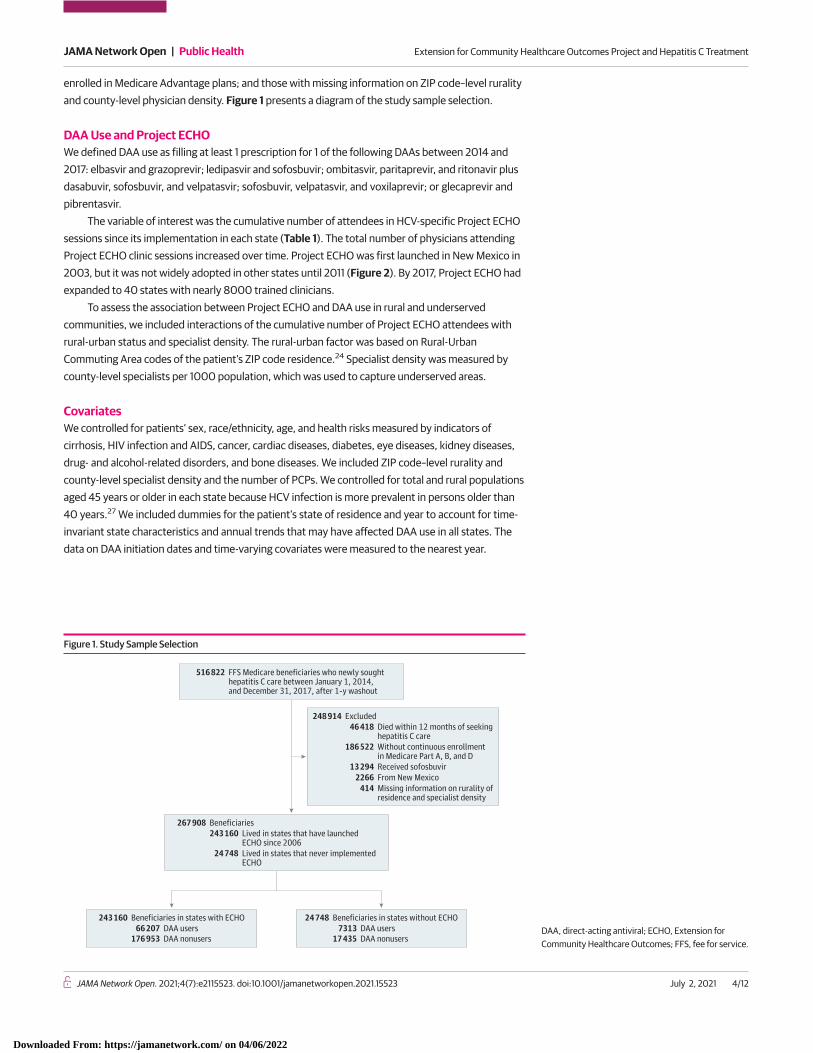
enrolled in Medicare Advantage plans; and those with missing information on ZIP code–level ruralityand county-level physician density. Figure 1 presents a diagram of the study sample selection.
DAA Use and Project ECHOWe defined DAA use as filling at least 1 prescription for 1 of the following DAAs between 2014 and2017: elbasvir and grazoprevir; ledipasvir and sofosbuvir; ombitasvir, paritaprevir, and ritonavir plusdasabuvir, sofosbuvir, and velpatasvir; sofosbuvir, velpatasvir, and voxilaprevir; or glecaprevir andpibrentasvir.
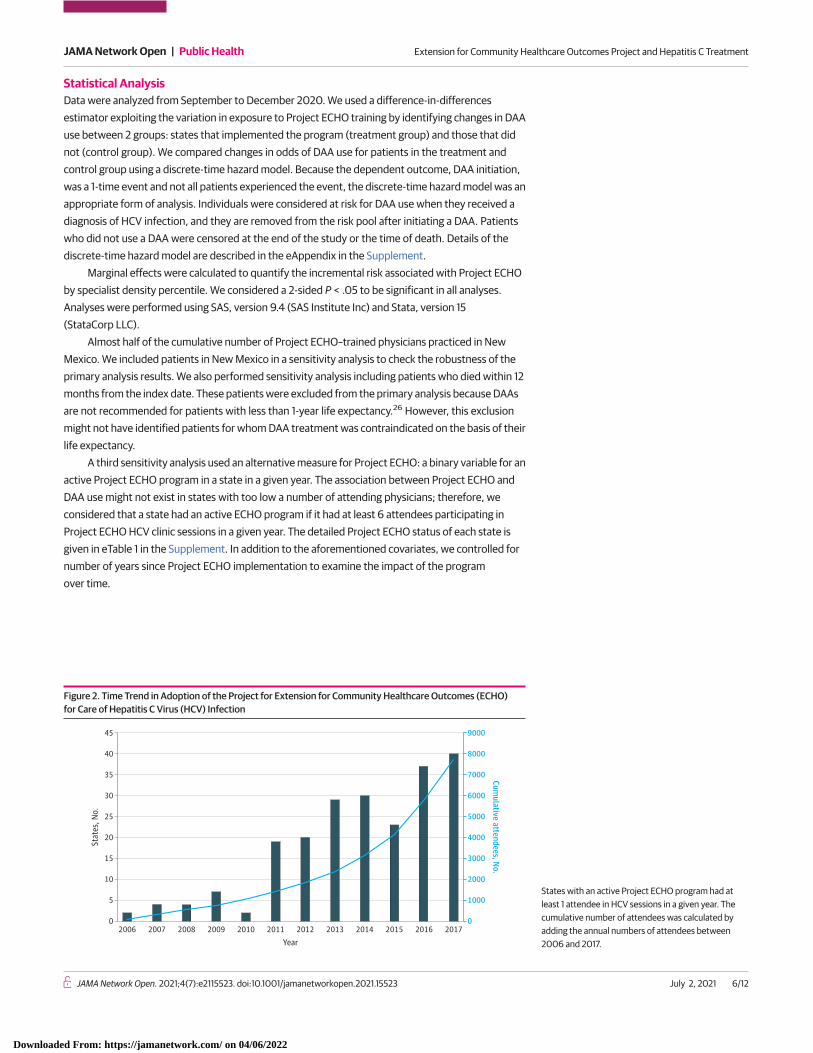
The variable of interest was the cumulative number of attendees in HCV-specific Project ECHOsessions since its implementation in each state (Table 1). The total number of physicians attendingProject ECHO clinic sessions increased over time. Project ECHO was first launched in New Mexico in2003, but it was not widely adopted in other states until 2011 (Figure 2). By 2017, Project ECHO hadexpanded to 40 states with nearly 8000 trained clinicians.
To assess the association between Project ECHO and DAA use in rural and underservedcommunities, we included interactions of the cumulative number of Project ECHO attendees withrural-urban status and specialist density. The rural-urban factor was based on Rural-UrbanCommuting Area codes of the patient’s ZIP code residence.24 Specialist density was measured bycounty-level specialists per 1000 population, which was used to capture underserved areas.
CovariatesWe controlled for patients’ sex, race/ethnicity, age, and health risks measured by indicators ofcirrhosis, HIV infection and AIDS, cancer, cardiac diseases, diabetes, eye diseases, kidney diseases,drug- and alcohol-related disorders, and bone diseases. We included ZIP code–level rurality andcounty-level specialist density and the number of PCPs. We controlled for total and rural populationsaged 45 years or older in each state because HCV infection is more prevalent in persons older than40 years.27 We included dummies for the patient’s state of residence and year to account for time-invariant state characteristics and annual trends that may have affected DAA use in all states. Thedata on DAA initiation dates and time-varying covariates were measured to the nearest year.
Figure 1. Study Sample Selection
516 822 FFS Medicare beneficiaries who newly soughthepatitis C care between January 1, 2014,and December 31, 2017, after 1-y washout
248 914 Excluded46 418 Died within 12 months of seeking
hepatitis C care186 522 Without continuous enrollment
in Medicare Part A, B, and D13 294 Received sofosbuvir
2266 From New Mexico414 Missing information on rurality of
residence and specialist density
267 908 Beneficiaries243 160 Lived in states that have launched
ECHO since 200624 748 Lived in states that never implemented
ECHO
243 160 Beneficiaries in states with ECHO66 207 DAA users
176 953 DAA nonusers
24 748 Beneficiaries in states without ECHO7313 DAA users
17 435 DAA nonusersDAA, direct-acting antiviral; ECHO, Extension forCommunity Healthcare Outcomes; FFS, fee for service.
JAMA Network Open | Public Health Extension for Community Healthcare Outcomes Project and Hepatitis C Treatment
JAMA Network Open. 2021;4(7):e2115523. doi:10.1001/jamanetworkopen.2021.15523 (Reprinted) July 2, 2021 4/12
Downloaded From: https://jamanetwork.com/ on 04/06/2022

Table 1. Extension for Community Healthcare Outcomes Cumulative Number of Attendees in Hepatitis CSessions by State, 2014-2017
State
Attendees, No.a
2014 2015 2016 2017
Alabama NA NA 3 13
Arkansas 18 40 57 76
Arizona 95 137 201 256
California 60 102 244 403
Colorado 22 32 53 68
Connecticut 124 170 221 275
District of Columbia 15 15 15 15
Florida 1 1 3 4
Georgia 6 6 11 17
Hawaii 5 6 6 6
Idaho 93 124 148 179
Illinois 36 163 383 608
Indiana NA NA 3 9
Iowa 2 2 2 2
Kansas NA NA 2 8
Kentucky 7 7 7 7
Louisiana 8 14 33 44
Maine NA NA 3 11
Maryland 3 3 5 7
Massachusetts 21 29 64 117
Michigan 1 1 3 10
Minnesota 25 31 43 57
Mississippi NA NA 1
Missouri 6 6 37 94
Montana 74 114 156 195
Nebraska 3 5 6 7
Nevada 2 5 8 11
New Hampshire NA NA 1
New Jersey 15 15 17 17
New Mexico 2066 2308 2658 3008
New York 13 13 46 92
North Carolina 1 1 1 1
North Dakota 3 7 21 31
Ohio 4 4 6 8
Oklahoma 24 61 165 257
Oregon 41 68 95 138
Pennsylvania 7 17 23 23
Rhode Island NA NA NA 2
South Carolina NA NA NA 3
South Dakota 7 7 16 22
Tennessee 1 1 3 10
Texas 85 178 286 380
Utah 91 142 196 275
Virginia 25 25 25 26
Washington 101 223 454 746
West Virginia NA NA 74 134
Wyoming 30 45 63 78
Abbreviation: NA, not available.a The value of cumulative number of attendees in
hepatitis C sessions depended on when thebeneficiary entered the study. For example, if 1patient entered the study in 2014 and anotherpatient in the same state entered in 2017, they wouldhave different values for the exposure of interest.
JAMA Network Open | Public Health Extension for Community Healthcare Outcomes Project and Hepatitis C Treatment
JAMA Network Open. 2021;4(7):e2115523. doi:10.1001/jamanetworkopen.2021.15523 (Reprinted) July 2, 2021 5/12
Downloaded From: https://jamanetwork.com/ on 04/06/2022
Statistical AnalysisData were analyzed from September to December 2020. We used a difference-in-differencesestimator exploiting the variation in exposure to Project ECHO training by identifying changes in DAAuse between 2 groups: states that implemented the program (treatment group) and those that didnot (control group). We compared changes in odds of DAA use for patients in the treatment andcontrol group using a discrete-time hazard model. Because the dependent outcome, DAA initiation,was a 1-time event and not all patients experienced the event, the discrete-time hazard model was anappropriate form of analysis. Individuals were considered at risk for DAA use when they received adiagnosis of HCV infection, and they are removed from the risk pool after initiating a DAA. Patientswho did not use a DAA were censored at the end of the study or the time of death. Details of thediscrete-time hazard model are described in the eAppendix in the Supplement.
Marginal effects were calculated to quantify the incremental risk associated with Project ECHOby specialist density percentile. We considered a 2-sided P < .05 to be significant in all analyses.Analyses were performed using SAS, version 9.4 (SAS Institute Inc) and Stata, version 15(StataCorp LLC).
Almost half of the cumulative number of Project ECHO–trained physicians practiced in NewMexico. We included patients in New Mexico in a sensitivity analysis to check the robustness of theprimary analysis results. We also performed sensitivity analysis including patients who died within 12months from the index date. These patients were excluded from the primary analysis because DAAsare not recommended for patients with less than 1-year life expectancy.26 However, this exclusionmight not have identified patients for whom DAA treatment was contraindicated on the basis of theirlife expectancy.
A third sensitivity analysis used an alternative measure for Project ECHO: a binary variable for anactive Project ECHO program in a state in a given year. The association between Project ECHO andDAA use might not exist in states with too low a number of attending physicians; therefore, weconsidered that a state had an active ECHO program if it had at least 6 attendees participating inProject ECHO HCV clinic sessions in a given year. The detailed Project ECHO status of each state isgiven in eTable 1 in the Supplement. In addition to the aforementioned covariates, we controlled fornumber of years since Project ECHO implementation to examine the impact of the programover time.
Figure 2. Time Trend in Adoption of the Project for Extension for Community Healthcare Outcomes (ECHO)for Care of Hepatitis C Virus (HCV) Infection
45
40
35
25
30
20
15
5
10
0 0
2000
1000
9000
8000
7000
6000
5000
4000
3000
Stat
es, N
o.
Cumulative attendees, N
o.
Year2006 2007 2008 2009 2010 2011 2012 2013 2014 2015 2016 2017
States with an active Project ECHO program had atleast 1 attendee in HCV sessions in a given year. Thecumulative number of attendees was calculated byadding the annual numbers of attendees between2006 and 2017.
JAMA Network Open | Public Health Extension for Community Healthcare Outcomes Project and Hepatitis C Treatment
JAMA Network Open. 2021;4(7):e2115523. doi:10.1001/jamanetworkopen.2021.15523 (Reprinted) July 2, 2021 6/12
Downloaded From: https://jamanetwork.com/ on 04/06/2022
Results
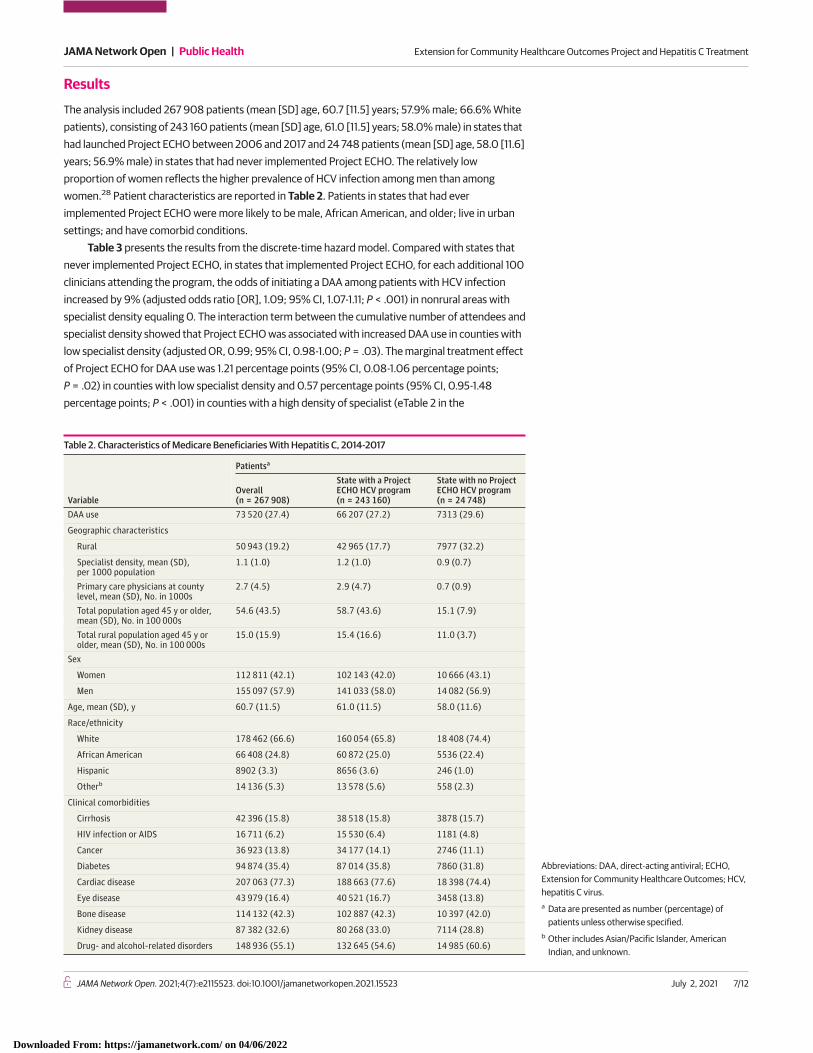
The analysis included 267 908 patients (mean [SD] age, 60.7 [11.5] years; 57.9% male; 66.6% Whitepatients), consisting of 243 160 patients (mean [SD] age, 61.0 [11.5] years; 58.0% male) in states thathad launched Project ECHO between 2006 and 2017 and 24 748 patients (mean [SD] age, 58.0 [11.6]years; 56.9% male) in states that had never implemented Project ECHO. The relatively lowproportion of women reflects the higher prevalence of HCV infection among men than amongwomen.28 Patient characteristics are reported in Table 2. Patients in states that had everimplemented Project ECHO were more likely to be male, African American, and older; live in urbansettings; and have comorbid conditions.
Table 3 presents the results from the discrete-time hazard model. Compared with states thatnever implemented Project ECHO, in states that implemented Project ECHO, for each additional 100clinicians attending the program, the odds of initiating a DAA among patients with HCV infectionincreased by 9% (adjusted odds ratio [OR], 1.09; 95% CI, 1.07-1.11; P < .001) in nonrural areas withspecialist density equaling 0. The interaction term between the cumulative number of attendees andspecialist density showed that Project ECHO was associated with increased DAA use in counties withlow specialist density (adjusted OR, 0.99; 95% CI, 0.98-1.00; P = .03). The marginal treatment effectof Project ECHO for DAA use was 1.21 percentage points (95% CI, 0.08-1.06 percentage points;P = .02) in counties with low specialist density and 0.57 percentage points (95% CI, 0.95-1.48percentage points; P < .001) in counties with a high density of specialist (eTable 2 in the
Table 2. Characteristics of Medicare Beneficiaries With Hepatitis C, 2014-2017
Variable
Patientsa
Overall(n = 267 908)
State with a ProjectECHO HCV program(n = 243 160)
State with no ProjectECHO HCV program(n = 24 748)
DAA use 73 520 (27.4) 66 207 (27.2) 7313 (29.6)
Geographic characteristics
Rural 50 943 (19.2) 42 965 (17.7) 7977 (32.2)
Specialist density, mean (SD),per 1000 population
1.1 (1.0) 1.2 (1.0) 0.9 (0.7)
Primary care physicians at countylevel, mean (SD), No. in 1000s
2.7 (4.5) 2.9 (4.7) 0.7 (0.9)
Total population aged 45 y or older,mean (SD), No. in 100 000s
54.6 (43.5) 58.7 (43.6) 15.1 (7.9)
Total rural population aged 45 y orolder, mean (SD), No. in 100 000s
15.0 (15.9) 15.4 (16.6) 11.0 (3.7)
Sex
Women 112 811 (42.1) 102 143 (42.0) 10 666 (43.1)
Men 155 097 (57.9) 141 033 (58.0) 14 082 (56.9)
Age, mean (SD), y 60.7 (11.5) 61.0 (11.5) 58.0 (11.6)
Race/ethnicity
White 178 462 (66.6) 160 054 (65.8) 18 408 (74.4)
African American 66 408 (24.8) 60 872 (25.0) 5536 (22.4)
Hispanic 8902 (3.3) 8656 (3.6) 246 (1.0)
Otherb 14 136 (5.3) 13 578 (5.6) 558 (2.3)
Clinical comorbidities
Cirrhosis 42 396 (15.8) 38 518 (15.8) 3878 (15.7)
HIV infection or AIDS 16 711 (6.2) 15 530 (6.4) 1181 (4.8)
Cancer 36 923 (13.8) 34 177 (14.1) 2746 (11.1)
Diabetes 94 874 (35.4) 87 014 (35.8) 7860 (31.8)
Cardiac disease 207 063 (77.3) 188 663 (77.6) 18 398 (74.4)
Eye disease 43 979 (16.4) 40 521 (16.7) 3458 (13.8)
Bone disease 114 132 (42.3) 102 887 (42.3) 10 397 (42.0)
Kidney disease 87 382 (32.6) 80 268 (33.0) 7114 (28.8)
Drug- and alcohol-related disorders 148 936 (55.1) 132 645 (54.6) 14 985 (60.6)
Abbreviations: DAA, direct-acting antiviral; ECHO,Extension for Community Healthcare Outcomes; HCV,hepatitis C virus.a Data are presented as number (percentage) of
patients unless otherwise specified.b Other includes Asian/Pacific Islander, American
Indian, and unknown.
JAMA Network Open | Public Health Extension for Community Healthcare Outcomes Project and Hepatitis C Treatment
JAMA Network Open. 2021;4(7):e2115523. doi:10.1001/jamanetworkopen.2021.15523 (Reprinted) July 2, 2021 7/12
Downloaded From: https://jamanetwork.com/ on 04/06/2022

Supplement). The interaction term between the number of ECHO-trained health care professionalsand the rural-urban indicator suggested that Project ECHO was not associated with the odds of DAAuse among patients in rural vs urban areas (adjusted OR, 1.01; 95% CI, 0.99-1.02; P = .49).
Some patient factors were significantly associated with the odds of DAA initiation. Being femalewas associated with 10.6% lower odds of DAA initiation (adjusted OR, 0.89; 95% CI, 0.88-0.91;P < .001). The odds of DAA use were 54% higher among African American patients (adjusted OR,1.54; 95% CI, 1.51-1.58; P < .001) compared with White patients. The presence of certaincomorbidities, such as cancer (adjusted OR, 0.81; 95% CI, 0.79-0.83), diabetes (adjusted OR, 0.93;95% CI, 0.91-0.95), cardiac disease (adjusted OR, 0.73; 95% CI, 0.71-0.74), bone disease (adjustedOR, 0.97; 95% CI, 0.95-0.98), kidney disease (adjusted OR, 0.60; 95% CI, 0.59-0.61), and drug- andalcohol-related disorders (adjusted OR, 0.60; 95% CI, 0.59-0.61) was associated with lower odds ofDAA initiation (all P < .001). Patients with cirrhosis (adjusted OR, 2.09; 95% CI, 2.05-2.13), HIV/AIDS(adjusted OR, 1.08; 95% CI, 1.04-1.12), and eye diseases (adjusted OR, 1.12; 95% CI, 1.09-1.14) weremore likely to use DAAs (all P < .001). Beneficiaries with cirrhosis had twice the odds of initiating aDAA than those without cirrhosis. Residing in rural areas (adjusted OR, 1.00; 95% CI, 0.97-1.03;P = .79) and specialist density (adjusted OR, 1.01; 95% CI, 0.99-1.02; P = .42) were not associatedwith the odds of receiving DAAs (Table 3).
The findings from the analysis including patients residing in New Mexico were similar, and inmany cases identical, to those of the main analysis (eTable 3 in the Supplement). In this analysis,
Table 3. Adjusted Odds Ratios of Direct-Acting Antiviral Treatment Initiation Among 267 908 Beneficiariesa
Variable Odds ratio (95% CI) P valueProject ECHO program, 100 physicians attending Project ECHO 1.09 (1.07-1.11) <.001
Interaction
Project ECHO program × rural 1.01 (0.99-1.02) .49
Project ECHO program × specialist density 0.99 (0.98-1.00) .03
Geographic characteristics
ZIP code level
Urban 1 [Reference] NA
Rural 1.00 (0.97-1.03) .79
County level
Specialist density, per 1000 population 1.01 (0.99-1.02) .42
PCPs, No. in 1000s 1.00 (0.99-1.00) <.001
State level
Total population aged 45 y or older, No. in 100 000s 0.96 (0.95-0.97) <.001
Total rural population aged 45 y or older, No. in 100 000s 0.89 (0.77-1.03) .13
Women 0.89 (0.88-0.91) <.001
Age 1.00 (1.00-1.00) .18
Race/ethnicity
White 1 [Reference]
<.001African American 1.54 (1.51-1.58)
Hispanic 0.91 (0.87-0.96)
Otherb 0.79 (0.76-0.82)
Clinical comorbidities
Cirrhosis 2.09 (2.05-2.13)
<.001
HIV infection or AIDS 1.08 (1.04-1.12)
Cancer 0.81 (0.79-0.83)
Diabetes 0.93 (0.91-0.95)
Cardiac disease 0.73 (0.71-0.74)
Eye disease 1.12 (1.09-1.14)
Bone disease 0.97 (0.95-0.98)
Kidney disease 0.60 (0.59-0.61)
Drug- and alcohol-related disorders 0.60 (0.59-0.61)
Abbreviations: ECHO, Extension for CommunityHealthcare Outcomes; NA, not available; PCP, primarycare physician.a Includes 403 228 person-years.b Includes Asian/Pacific Islander, American Indian,
and unknown.
JAMA Network Open | Public Health Extension for Community Healthcare Outcomes Project and Hepatitis C Treatment
JAMA Network Open. 2021;4(7):e2115523. doi:10.1001/jamanetworkopen.2021.15523 (Reprinted) July 2, 2021 8/12
Downloaded From: https://jamanetwork.com/ on 04/06/2022

Project ECHO was associated with increased DAA use (adjusted OR, 1.08; 95% CI, 1.07-1.10; P < .001).The interaction between Project ECHO and specialty density also showed a negative association withDAA use (adjusted OR, 0.99; 95% CI, 0.99-1.00; P = .02). The results from the analysis includingpatients who died within 12 months from the index date were similar to those of the main analyses(eTable 4 in the Supplement).
The results from the analysis using a Project ECHO variable (whether the state had >5 ECHOattendees in a given year) were also similar to those of the primary analysis. Although the resultssuggest that Project ECHO was not associated with DAA use (adjusted OR, 1.01; 95% CI, 0.96-1.06;P = .98) (eTable 5 in the Supplement), Project ECHO was associated with 3% increased odds ofinitiating a DAA in areas with low specialist density (adjusted OR, 0.97; 95% CI, 0.95-0.99; P = .007).
Discussion
In this cohort study, implementation of Project ECHO was associated with improved access to DAAtreatment. An additional 100 PCPs participating in Project ECHO HCV sessions was associated with9% increased odds of DAA use after adjusting for patient demographic characteristics, comorbidities,and geographic characteristics.
Project ECHO was associated with increased odds of DAA use in areas with few specialistphysicians compared with areas with higher specialist density. Although the magnitude of theassociation was small, this finding suggests that Project ECHO can potentially address 1 of the majorbarriers to expanding access to treatment of HCV infection: specialist shortages. After attendingtelementoring sessions, PCPs in resource-limited settings are able to deliver specialized care forcomplex health conditions such as HCV infection in community-based clinics where specialistservices were previously unavailable.16 As a result, access to DAA treatment is less restricted bylimited numbers of hepatologists, gastroenterologists, and infectious diseases specialists inunderserved areas. Even though we did not find an association between Project ECHO and DAA usein rural areas compared with urban areas, our results showed that the number of health careprofessionals attending Project ECHO HCV clinic sessions was associated with increased DAA use.
We found that the odds of DAA use were higher among African American patients comparedwith White patients. This is consistent with a prior study, which suggested that increased DAA useamong African Americans may reflect pent-up demand for treatment for HCV infection because ofpoor tolerance for interferon-based therapy.8 The fight to eradicate HCV infection in the US has beenongoing for many years without success. Despite the recommendation of the World HealthOrganization to treat all adults with chronic HCV infection with DAAs,29 only 27% of Medicarepatients with HCV infection in our study initiated an interferon-free DAA. This finding is consistentwith those of previous studies of Medicare populations with HCV infection.8,12,30 A major reason forlow DAA uptake is the insufficient numbers of physicians with experience in cases of HCV infection,especially in rural and underserved areas.12 However, with task-shifting treatment models such asProject ECHO, access to DAA treatment has become less limited by the shortage of specialists. Ourstudy suggests that Project ECHO is associated with increased availability of and access to DAAtherapy, particularly in resource-limited settings, moving a step closer to the HCV infection treatmenttarget set by the World Health Organization.6
LimitationsThis study has limitations. First, we could not obtain information on how many patients with HCVinfection were treated by rural physicians who participated in Project ECHO or the percentage ofrural PCPs who attended Project ECHO HCV sessions. Thus, we may not have fully captured the roleof the intervention in the care of HCV infection in rural areas. Second, health care professionals wereeligible to receive continuing medical education credits if they participated in all Project ECHO HCVsessions or 70% of the sessions within a series. This may have influenced whether the physicianswere prepared to provide specialized care to their patients with HCV infection. We did not have
JAMA Network Open | Public Health Extension for Community Healthcare Outcomes Project and Hepatitis C Treatment
JAMA Network Open. 2021;4(7):e2115523. doi:10.1001/jamanetworkopen.2021.15523 (Reprinted) July 2, 2021 9/12
Downloaded From: https://jamanetwork.com/ on 04/06/2022
information on ECHO completion for each participant. Third, we did not know whether health careprofessionals trained before 2014 continued to treat patients with HCV infection when DAAs becameavailable. These physicians may have retired, moved to other states, or died or may not have adopteduse of DAAs. Therefore, we may have underestimated the association between Project ECHO andDAA use. Fourth, owing to limitations of claims data, we did not have detailed clinical informationsuch as viral clearance; thus, some patients treated with DAAs in our analysis may not have beencured of their HCV infection. Fifth, our study was limited to fee-for-service Medicare beneficiaries;thus, the results may not apply to other populations.
Conclusions
The results of this cohort study suggest that implementation of ECHO was associated with improvedaccess to DAA treatment, suggesting that Project ECHO may be a promising strategy to improveaccess and reduce barriers to HCV treatment, especially in underserved areas. Expansion of ProjectECHO may help mitigate unmet needs for DAA treatment and expand capacity of care for patientswith HCV infection in resource-limited settings. More research is needed to evaluate whether ProjectECHO improves access to other recommended care for patients with HCV infection.
ARTICLE INFORMATIONAccepted for Publication: April 29, 2021.
Published: July 2, 2021. doi:10.1001/jamanetworkopen.2021.15523
Open Access: This is an open access article distributed under the terms of the CC-BY License. © 2021 Tran L et al.JAMA Network Open.
Corresponding Author: Linh Tran, BA, Department of Health Policy and Administration, Pennsylvania StateUniversity College of Health and Human Development, 501 G Ford Building, University Park, PA 16802([email protected]).
Author Affiliations: Department of Health Policy and Administration, Pennsylvania State University College ofHealth and Human Development, University Park, State College (Tran, Jung); Division of Health Policy andManagement, University of Minnesota School of Public Health, Minneapolis (Feldman); Department of Medicine,Pennsylvania State University College of Medicine, Hershey (Riley).
Author Contributions: Ms Tran and Dr Jung full access to all of the data in the study and take responsibility for theintegrity of the data and the accuracy of the data analysis.
Concept and design: All authors.
Acquisition, analysis, or interpretation of data: All authors.
Drafting of the manuscript: Tran, Riley.
Critical revision of the manuscript for important intellectual content: All authors.
Statistical analysis: Tran, Feldman.
Obtained funding: Feldman, Jung.
Administrative, technical, or material support: Tran.
Supervision: Feldman, Riley, Jung.
Conflict of Interest Disclosures: Dr Feldman reported owning a small amount of stock in Gilead Sciences. Dr Rileyreported receiving grants from the National Institutes of Health during the conduct of the study. Dr Jung reportedreceiving grants from the National Institute on Aging, National Institutes of Health during the conduct of the study.No other disclosures were reported.
Funding/Support: This project was supported by grant R01 AG055636-01A1 from the National Institute on Aging,National Institutes of Health (Dr Jung).
Role of the Funder/Sponsor: The funder had no role in the design and conduct of the study; collection,management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; anddecision to submit the manuscript for publication.
JAMA Network Open | Public Health Extension for Community Healthcare Outcomes Project and Hepatitis C Treatment
JAMA Network Open. 2021;4(7):e2115523. doi:10.1001/jamanetworkopen.2021.15523 (Reprinted) July 2, 2021 10/12
Downloaded From: https://jamanetwork.com/ on 04/06/2022

Disclaimer: The content is solely the responsibility of the authors and does not necessarily represent the officialviews of the National Institute on Aging, National Institutes of Health.
Meeting Presentation: This study was presented as a poster at the Virtual Academy Health Research Conference;June 14, 2021.
REFERENCES1. Njei B, Esserman D, Krishnan S, et al. Regional and rural-urban differences in the use of direct-acting antiviralagents for hepatitis C virus: the Veteran Birth Cohort. Med Care. 2019;57(4):279-285. doi:10.1097/MLR.0000000000001071
2. US Centers for Disease Control and Prevention. Viral hepatitis: hepatitis C information. Published October 27,2020. Accessed October 29, 2020. https://www.cdc.gov/hepatitis/hcv/index.htm
3. Kalidindi Y, Jung J, Feldman R, Riley T III. Association of direct-acting antiviral treatment with mortality amongMedicare beneficiaries with hepatitis C. JAMA Netw Open. 2020;3(7):e2011055. doi:10.1001/jamanetworkopen.2020.11055
4. Backus LI, Belperio PS, Shahoumian TA, Mole LA. Direct-acting antiviral sustained virologic response: impact onmortality in patients without advanced liver disease. Hepatology. 2018;68(3):827-838. doi:10.1002/hep.29811
5. Saeed S, Strumpf EC, Moodie EE, et al; Canadian Co-Infection Cohort Study. Disparities in direct acting antiviralsuptake in HIV-hepatitis C co-infected populations in Canada. J Int AIDS Soc. 2017;20(3). doi:10.1002/jia2.25013
6. World Health Organization. Combating hepatitis B and C to reach elimination by 2030. Accessed October 29,2020. https://www.who.int/hepatitis/publications/hep-elimination-by-2030-brief/en/
7. Wiktor S. How feasible is the global elimination of HCV infection? Lancet. 2019;393(10178):1265-1267. doi:10.1016/S0140-6736(18)32750-8
8. Jung J, Du P, Feldman R, Kong L, Riley T III. Racial/ethnic and socioeconomic disparities in use of direct-actingantivirals among Medicare beneficiaries with chronic hepatitis C, 2014-2016. J Manag Care Spec Pharm. 2019;25(11):1236-1242. doi:10.18553/jmcp.2019.25.11.1236
9. Gidwani R, Barnett PG, Goldhaber-Fiebert JD, et al. Uptake and utilization of directly acting antiviralmedications for hepatitis C infection in US veterans. J Viral Hepat. 2015;22(5):489-495. doi:10.1111/jvh.12344
10. Spradling PR, Xing J, Rupp LB, et al; Chronic Hepatitis Cohort Study (CHeCS) Investigators. Uptake of andfactors associated with direct-acting antiviral therapy among patients in the Chronic Hepatitis Cohort Study, 2014to 2015. J Clin Gastroenterol. 2018;52(7):641-647. doi:10.1097/MCG.0000000000000857
11. Kanwal F, Kramer JR, El-Serag HB, et al. Race and gender differences in the use of direct acting antiviral agentsfor hepatitis C virus. Clin Infect Dis. 2016;63(3):291-299. doi:10.1093/cid/ciw249
12. Du P, Wang X, Kong L, Jung J. Can telementoring reduce urban-rural disparities in utilization of direct-actingantiviral agents? Telemed J E Health. 2020.
13. Arora S, Thornton K, Murata G, et al. Outcomes of treatment for hepatitis C virus infection by primary careproviders. N Engl J Med. 2011;364(23):2199-2207. doi:10.1056/NEJMoa1009370
14. Thomson M, Konerman MA, Choxi H, Lok ASF. Primary care physician perspectives on hepatitis C managementin the era of direct-acting antiviral therapy. Dig Dis Sci. 2016;61(12):3460-3468. doi:10.1007/s10620-016-4097-2
15. Dearing JW, Cruz S, Kee K, Larson RS, Rahm AK. Project ECHO: Review and Research Agenda. DiffusionAssociates; 2019.
16. Komaromy M, Duhigg D, Metcalf A, et al. Project ECHO (Extension for Community Healthcare Outcomes):a new model for educating primary care providers about treatment of substance use disorders. Subst Abus. 2016;37(1):20-24. doi:10.1080/08897077.2015.1129388
17. ATM Health. Project ECHO. Accessed February 5, 2021. https://health.tamu.edu/echo/index.html
18. Terrault NA. Hepatitis C elimination: challenges with under-diagnosis and under-treatment. F1000Res.2019;8. doi:10.12688/f1000research.15892.1
19. Yoo ER, Perumpail RB, Cholankeril G, Jayasekera CR, Ahmed A. Expanding treatment access for chronichepatitis C with task-shifting in the era of direct-acting antivirals. J Clin Transl Hepatol. 2017;5(2):130-133. doi:10.14218/JCTH.2016.00059
20. Syed TA, Bashir MH, Farooqui SM, et al. Treatment outcomes of hepatitis C-infected patients in specialty clinicvs. primary care physician clinic: a comparative analysis. Gastroenterol Res Pract. 2019;2019:8434602. doi:10.1155/2019/8434602
21. Kattakuzhy S, Gross C, Emmanuel B, et al; ASCEND Providers. Expansion of treatment for hepatitis C virusinfection by task shifting to community-based nonspecialist providers: a nonrandomized clinical trial. Ann InternMed. 2017;167(5):311-318. doi:10.7326/M17-0118
JAMA Network Open | Public Health Extension for Community Healthcare Outcomes Project and Hepatitis C Treatment
JAMA Network Open. 2021;4(7):e2115523. doi:10.1001/jamanetworkopen.2021.15523 (Reprinted) July 2, 2021 11/12
Downloaded From: https://jamanetwork.com/ on 04/06/2022

22. Reid M, Price JC, Tien PC, Hepatitis C virus infection in the older patient. Infect Dis Clin North Am. 2017;31(4):827-838. doi:10.1016/j.idc.2017.07.014
23. The University of New Mexico School of Medicine. Project ECHO. Accessed October 2, 2020. https://hsc.unm.edu/echo/
24. US Department of Agriculture. Rural-urban commuting area codes. Accessed November 18, 2020. https://www.ers.usda.gov/data-products/rural-urban-commuting-area-codes.aspx
25. Chronic Conditions Data Warehouse. Condition categories. Accessed June 25, 2020. https://www2.ccwdata.org/web/guest/condition-categories
26. Hepatitis C Online. Making a decision on when to initiate HCV therapy. Accessed June 25, 2020. https://www.hepatitisc.uw.edu/go/evaluation-treatment/treatment-initiation-decision/core-concept/all
27. Nakashima K, Ikematsu H, Hayashi J, Kishihara Y, Mutsutake A, Kashiwagi S. Intrafamilial transmission ofhepatitis-C virus among the population of an endemic area of Japan. JAMA. 1995;274(18):1459-1461. doi:10.1001/jama.1995.03530180053030
28. Baden R, Rockstroh JK, Buti M. Natural history and management of hepatitis C: does sex play a role? J InfectDis. 2014;209(suppl 3):S81-S85. doi:10.1093/infdis/jiu057
29. World Health Organization. Hepatitis C. Accessed November 12, 2020. https://www.who.int/news-room/fact-sheets/detail/hepatitis-c
30. Du P. Use of new hepatitis C drugs in Medicare: persistent urban-rural disparities and potential interventions.Innov Aging. 2019;3(suppl 1):S13. doi:10.1093/geroni/igz038.047
SUPPLEMENT.eAppendix. Discrete-Time Hazard AnalysiseTable 1. Status of Extension for Community Healthcare Outcomes (ECHO) Status for Hepatitis C Care by State,2014-2017eTable 2. Marginal Effects of Extension for Community Healthcare Outcomes (ECHO) on Direct-Acting Antiviral(DAA) Initiation by Specialist Density PercentileeTable 3. Adjusted Odd Ratios of Direct-Acting Antiviral (DAA) Initiation(Including Patients from New Mexico)eTable 4. Adjusted Odd Ratios of Direct-Acting Antiviral (DAA) Initiation (Including Patients Died within 12 Monthsfrom The Index Date*)eTable 5. Adjusted Odd Ratios of Direct-Acting Antiviral (DAA) Initiation
JAMA Network Open | Public Health Extension for Community Healthcare Outcomes Project and Hepatitis C Treatment
JAMA Network Open. 2021;4(7):e2115523. doi:10.1001/jamanetworkopen.2021.15523 (Reprinted) July 2, 2021 12/12
Downloaded From: https://jamanetwork.com/ on 04/06/2022