association between proton pump inhibitor therapy and ... · class) for an association between ppi...
TRANSCRIPT

Association between Proton Pump Inhibitor Therapy andClostridium difficile Infection: A ContemporarySystematic Review and Meta-AnalysisImad M. Tleyjeh1,2,3,4*, Aref A. Bin Abdulhak5., Muhammad Riaz6., Faisal A. Alasmari1, Musa A. Garbati1,
Mushabab AlGhamdi1, Abdur Rahman Khan7, Mohamad Al Tannir6, Patricia J. Erwin8, Talal Ibrahim9,
Abed AlLehibi1, Larry M. Baddour3, Alex J. Sutton10
1 Department of Medicine, King Fahad Medical City, Riyadh, Saudi Arabia, 2 College of Medicine, AlFaisal University, Riyadh, Saudi Arabia, 3 Division of Infectious Diseases,
Mayo Clinic, Rochester, Minnesota, United States of America, 4 Division of Epidemiology, Mayo Clinic, Rochester, Minnesota, United States of America, 5 Department of
Internal Medicine, University of Missouri-Kansas City, Kansas City, Missouri, United States of America, 6 Research and Scientific Publication Center, King Fahad Medical City,
Riyadh, Saudi Arabia, 7 Department of Internal Medicine, University of Toledo Medical Center, Toledo, Ohio, United States of America, 8 Mayo Medical Library, Mayo Clinic,
Rochester, Minnesota, United States of America, 9 Department of Orthopedic and Trauma Surgery, Hamad Medical Corporation Doha, Qatar, 10 Department of Health
Sciences, University of Leicester, University of Leicester, Leicester, England
Abstract
Introduction: Emerging epidemiological evidence suggests that proton pump inhibitor (PPI) acid-suppression therapy isassociated with an increased risk of Clostridium difficile infection (CDI).
Methods: Ovid MEDLINE, EMBASE, ISI Web of Science, and Scopus were searched from 1990 to January 2012 for analyticalstudies that reported an adjusted effect estimate of the association between PPI use and CDI. We performed random-effectmeta-analyses. We used the GRADE framework to interpret the findings.
Results: We identified 47 eligible citations (37 case-control and 14 cohort studies) with corresponding 51 effect estimates.The pooled OR was 1.65, 95% CI (1.47, 1.85), I2 = 89.9%, with evidence of publication bias suggested by a contour funnelplot. A novel regression based method was used to adjust for publication bias and resulted in an adjusted pooled OR of 1.51(95% CI, 1.26–1.83). In a speculative analysis that assumes that this association is based on causality, and based on publishedbaseline CDI incidence, the risk of CDI would be very low in the general population taking PPIs with an estimated NNH of3925 at 1 year.
Conclusions: In this rigorously conducted systemic review and meta-analysis, we found very low quality evidence (GRADEclass) for an association between PPI use and CDI that does not support a cause-effect relationship.
Citation: Tleyjeh IM, Bin Abdulhak AA, Riaz M, Alasmari FA, Garbati MA, et al. (2012) Association between Proton Pump Inhibitor Therapy and Clostridium difficileInfection: A Contemporary Systematic Review and Meta-Analysis. PLoS ONE 7(12): e50836. doi:10.1371/journal.pone.0050836
Editor: Markus M. Heimesaat, Charite, Campus Benjamin Franklin, Germany
Received August 23, 2012; Accepted October 24, 2012; Published December 7, 2012
Copyright: � 2012 Tleyjeh et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permitsunrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Funding: The authors have no funding or support to report.
Competing Interests: The authors have declared that no competing interests exist.
* E-mail: [email protected]
. These authors contributed equally to this work.
Introduction
Proton pump inhibitors (PPIs) are one of the most prescribed
groups of drugs globally [1]. PPIs are effective for the treatment of
all acid-related disorders. They are also indicated ICU patients
with coagulopathy, patients on mechanical ventilation, and
patients with history of peptic ulcer disease, (particularly those
on NSAID or antiplatelet therapy) [2].
The use of PPIs has increased dramatically [1] despite concerns
that PPIs are overprescribed both in primary care [3] and in
hospitals, both in the in-patient setting [4–7] and on discharge [8].
Moreover, concerns have been raised about the potential long-
term effects of these drugs. PPIs have been associated with
significant interaction with other drugs [9,10] and fractures [11],
interstitial nephritis [12], pneumonia [13] and enteric infections
[14,15], namely Clostridium difficile infection (CDI).
CDI has recently emerged as a major public health problem
with current estimates suggesting a point prevalence of 13.1/1000
in-patient population [16]. Studies have reported increases in both
incidence and mortality of CDI [17–20]. The increase in incidence
of CDI has been attributed to an aging population, increase in use
of antibiotics and acid suppressive drugs. PPIs are postulated to
increase the proliferation of spores and change the acidic milieu of
the stomach that permits spores to survive intraluminally.
The role of gastric acid suppression therapy has gained much
interest recently as a risk factor for CDI. Four recently published
meta-analyses have suggested an association between gastric acid
suppression therapy with proton pump inhibitors (PPI) and CDI
PLOS ONE | www.plosone.org 1 December 2012 | Volume 7 | Issue 12 | e50836

[15,21,22,23]. The United States Food and Drug Administration
(FDA) recently warned the public about a possible association
between CDI and PPI use [19]. Nevertheless, these reviews had
important limitations such as missing a large number of published
studies [15,19,22,23], using only unadjusted data from observa-
tional studies [15,22,23], not exploring heterogeneity and the
effect of publication bias and over-interpreting the findings. We,
therefore, performed a systematic review and meta-analysis that
addressed the role of PPIs in CDI. We used the MOOSE [24] and
PRISMA guidelines [25] for reporting systematic reviews. We
include new studies published after the previous meta-analyses and
added unique approaches to adjust for publication bias as well as
explore the potential effect of unknown confounders. We use the
Grades of Recommendation, Assessment, Development and
Evaluation (GRADE) framework [26] to interpret our findings.
Methods
Study Search StrategyThe search strategy and subsequent literature searches were
performed by a medical reference librarian (PJE) with 38 years of
experience. The initial strategy was developed in Ovid MEDLINE
(1990 through January 2012), using MeSH (Medical Subject
Headings) controlled vocabulary, and then modified for Ovid
EMBASE (1990 through January 2012). The search was intended
to capture all acid suppression studies. Primary terms were:
enterocolitis, pseudomembranous/AND the therapeutic agents of
interest: explode omeprazole, explode proton pump inhibitors,
anti-ulcer agents, and explode histamine H2 antagonists (Explode
allows including all of the specific drugs, without having to use all
of the various terms, synonyms, brands and generic names.)
Articles were limited to randomized controlled trials, cohort
studies, and/or case-control studies. The same process was used
with Ovid EMBASE with alterations as necessary to accommodate
EMBASE’s more granular subject headings. ISI Web of Science
and Elsevier Scopus use textwords: (difficile OR pseudomembra-
nous OR pseudo-membranous) AND (omeprazole OR ‘‘proton
pump’’ OR ranitidine OR h2 OR h-2 OR ‘‘acid suppression’’ OR
antacid*)) AND (random* OR trial* OR blind* OR cohort* OR
controlled OR prospective).
There was no restriction on language. All results were downloaded
into EndNote 7.0 (Thompson ISI Research soft, Philadelphia,
Pennsylvania), a bibliographic database manager, and duplicate
citations were identified and removed. Two authors (A.B.A. and
F.A.) independently assessed the eligibility of identified studies.
Study SelectionTo be included, a study had to: (1) be an analytical study; and (2)
have examined the association between PPI use and incidence of CDI.
Data CollectionA data collection form was developed and used to retrieve
information on relevant features and results of pertinent studies.
Two reviewers (A.B.A. and F.A.) independently extracted and
recorded data on a predefined checklist. Disagreements among
reviewers were discussed with two other reviewers (I.M.T. and
M.A.), and agreement was reached by consensus. Data included
the following: study characteristics (i.e., country and year of study),
characteristics of the study, PPI intake definition and ascertain-
ment, and outcome. We also collected adjusted effect estimates
and 95% confidence intervals (CI) based on the multivariable
regression model used in each study, and the list of variables
considered for inclusion in the multivariate analysis.
We used the Newcastle-Ottawa Quality Assessment Scale for cohort
and case-control studies [27] which is intended to rate selection bias,
comparability of the exposed and unexposed groups of each cohort,
outcome assessment, and attrition bias. Two reviewers (A.B.A. and
F.A.) independently assessed the methodological quality of selected
studies using the Newcastle-Ottawa Quality Assessment Scale for
cohort and case-control studies. Disagreement among reviewers was
discussed with 2 other reviewers (I.M.T. and M.A.), and agreement
was reached by consensus.
We used the GRADE framework to interpret our findings. The
Cochrane Collaboration has adopted the principles of the
GRADE system [28] for evaluating the quality of evidence for
outcomes reported in systematic reviews.
For purposes of systematic reviews, the GRADE approach
defines the quality of a body of evidence as the extent to which one
can be confident that an estimate of effect or association is close to
the quantity of specific interest. Quality of a body of evidence
involves consideration of within-study risk of bias (methodological
quality), directness of evidence, heterogeneity, precision of effect
estimates and risk of publication bias.
Statistical AnalysesMeta-analyses. The primary effect measures used in the
meta-analysis were Odds Ratios (OR) (46 observations), and
Hazard Ratios (HR) (5 observations) which were assumed to
reasonably estimate the same association between CDI and PPIs
because of low CDI incidence and are pooled together. Adjusted
effect estimates were primarily used for this analysis. Unadjusted
effect estimates were used as alternatives if studies did not observe
an association on univariate comparison and did not therefore
pursue adjustment or did not report adjusted estimates. We
performed meta-analyses for all studies together and separately for
different subgroups such as case-control studies and cohort studies.
Effect estimates from all included studies were pooled in a meta-
analysis using the DerSimonian and Laird random effects model [29].
Exploring heterogeneity. Homogeneity among studies was
estimated by calculation of the variation across studies attributable
to heterogeneity rather than chance (I2). The influence of a range
of a-priori selected study-level and aggregated individual-level
parameters on the observed effect estimate was investigated by
means of meta-regressions. In these analyses, the log odds ratio
from each study was regressed on the potential confounders in
univariate and multivariate weighted linear regressions, weighted
according to the inverse standard error and the residual between-
study variance. Nine potential confounders were considered. Six
variables were categorical: design of the study (case-control vs.
cohort), country of publication, setting (single center vs. multicen-
ter), method of ascertainment of antibiotic use, method of effect
measure (OR vs. RR/HR) and effect estimate (adjusted vs.
unadjusted). Three continuous variables were: the impact factor of
the journal where the study was published, number of variables the
effect measure was adjusted for and proportion of cases that were
exposed to antibiotics.
Publication bias. The possible influence of publication bias
was graphically assessed with the novel method of contour-
enhanced funnel plot [30] where log-transformed odds ratios were
plotted against standard errors. This method examines whether
any funnel plot asymmetry is likely to be due to publication bias
compared with other underlying causes of funnel plot asymmetry.
The contours help to indicate whether areas of the plot, where
studies are perceived to be missing, are where studies would have
statistically significant effect sizes or not and thus decrease or
increase the evidence that the asymmetry is due to publication
bias. The presence of funnel plot asymmetry was also assessed
Proton Pump Inhibitors and C. difficile Infection
PLOS ONE | www.plosone.org 2 December 2012 | Volume 7 | Issue 12 | e50836

using Egger’s test [31]. To adjust for the impact of publication bias
on the pooled effect estimate, we used a novel regression based
adjustment method recently suggested by Moreno et al [32]. An
adjusted pooled effect estimate for an ideal study of a very large
size (i.e. with zero standard error) is obtained from the fitted
weighted linear regression equation, plotted with a regression line
on the contour enhanced funnel plot. This method of regression is
a modified version of conventional Egger’s regression test for
publication bias where the log of effect estimate is regressed by its
variance rather than the standard error and weights are assigned
according to the inverse of the variance. This model has been
shown to consistently outperform the conventional trim and fill
method [32].
Residual confounding. Finally, the possible influence of
unknown confounders (residual confounding) was investigated
with a rule-out approach described by Schneeweiss [33]. This
approach stipulates the influence of a hypothetical confounder and
determines what characteristics this confounder must have to fully
account for the observed association between use of PPIs and
occurrence of CDI. The hypothetical confounder is characterized
by its association to PPIs use (OREC, odds ratio of exposure to the
confounder) and its association to the outcome (RRCO, relative
risk of outcome in individuals exposed to the confounder vs. non-
exposed). For this analysis, the absolute risk in the pooled non-
exposed group was used for conversion of odds ratio to relative risk
using the method described by Zhang and Yu [34]. Separate
analyses were performed to demonstrate what levels of OREC and
RRCO would be required to fully explain the observed association
between PPIs and CDI for different hypothetical prevalence of the
unknown confounder (i.e. PC = 0.2, PC = 0.5) before and after
adjustment for publication bias as described above.
In all analyses, results associated with p-values ,0.05 (two-sided
test) were considered statistically significant. All statistical analyses
were performed using Stata version12 statistical software (Stata
Corp, College Station, Texas).
Results
Yield of Search Strategy and Eligible StudiesThe search strategy yielded 287 publications of which 242 were
not eligible for inclusion based on title/abstract review. Reference
lists of all eligible articles were systematically searched and 7
additional studies were identified that were not captured by our
search strategy. A total of 47 citations, 4 of which reported data on
4 different populations, that examined the association between PPI
therapy and CDI were eligible for this review. Figure 1
summarizes the study selection process and is presented in the
appendix.
Figure 1. Flow diagram of eligible studies.doi:10.1371/journal.pone.0050836.g001
Proton Pump Inhibitors and C. difficile Infection
PLOS ONE | www.plosone.org 3 December 2012 | Volume 7 | Issue 12 | e50836

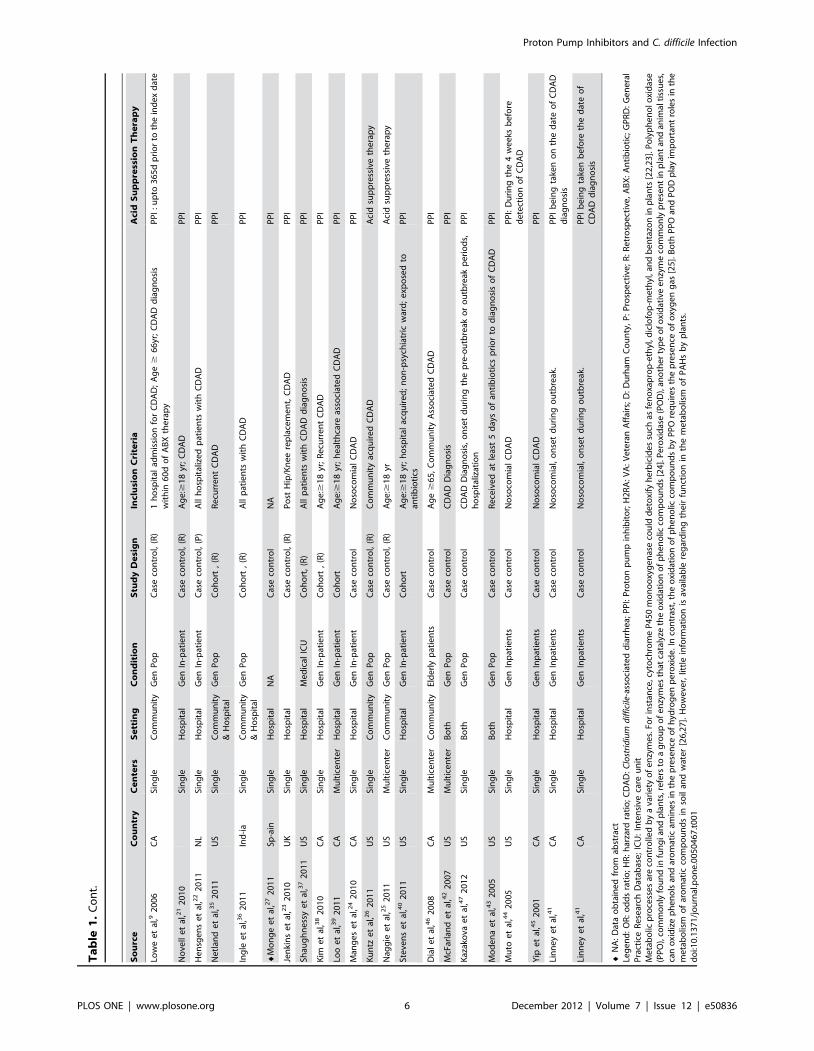
Characteristics of the Included StudiesTable 1 summarizes characteristics of the included studies.
Studies were conducted in Asia, Europe, North America (Canada
and USA). One citation reported both a case-control and cohort
designs on 2 different patient populations [35]. Three citations
[36–38] reported two different case control analyses per each
citation. Forty analyses were single-centre, nine were multi-centre,
and two from a general practice research database (GPRD). Thirty
seven analyses were of case-control design and 14 were of cohort
design. Among these, 8 exclusively addressed community-acquired
CDI, 37 hospital-acquired and 6 both hospital- and community-
acquired CDI. Table S1 and S2 summarizes the CDI case
ascertainment and control or non-exposed group selection method
for all studies.
Quality Assessment of Included StudiesQuality assessment of all included studies was done using the
validated Newcastle-Ottawa Quality Assessment Scale [27] for
cohort and case control studies (Table S3 and Table S4). Most
studies were of good quality with no evidence of selection bias, and
with good comparability of the exposed and unexposed groups of
each cohort, and outcome assessment. Fifty-one individual effect
estimates from 47 eligible citations were extracted. We identified 2
outliers and excluded them from the final analyses as per the
Cochrane Handbook for Systematic Reviews [39]. The 2 outliers
were: Bajaj et al [40] because of a high OR = 37.6, and Wilcox
et al [41] because of large SE (SE log OR = 3.59). Final
interpretation was based on analyses of the 51 observations.
Meta-analysisAssociation between PPI and CDI. Fifty one individual
effect estimates from 47 eligible studies were extracted. Figure 2
shows the results of the pooled estimates for the 51 observations.
The pooled OR for the 51 observations was 1.65, 95% CI (1.47,
1.85), I2 = 89.9%. Table 2 summarizes the pooled estimates and
associated heterogeneity for different subgroups. All estimates
supported an association between PPI therapy and CDI.
Exploring heterogeneity. The influence of a range of a-
priori selected study-level and aggregated individual-level param-
eters on the observed effect estimate was investigated by means of
meta-regressions. Table S5 summarizes the meta-regression
analyses for all 51 results and is presented in the appendix. We
observed that studies that used interviews to ascertain PPI
exposure had on average lower effect estimates that studies that
used medical records 1.17 (0.91, 1.51) vs. 1.89 (1.45, 2.45), p for
interaction = 0.05 (Table 2). We also observed that studies that
used adjusted effect estimates [1.76 (95% CI, 1.54, 2.00)] had
higher pooled estimates than those that used unadjusted effect
estimates [1.27 (95% CI, 0.93, 1.72)], p = 0.07.
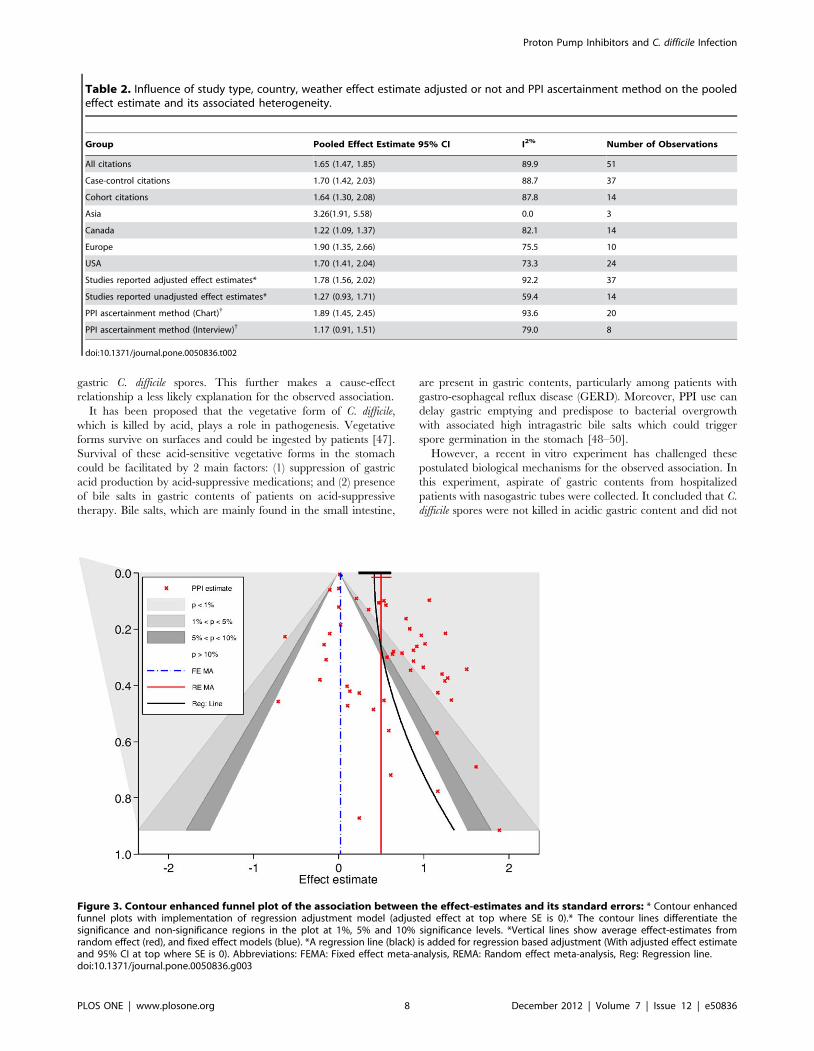
Publication bias. Figure 3 displays a contour-enhanced
funnel plot with the corresponding fixed (FE) and random effect
(RE) meta-analyses pooled estimates providing a weighted average
of effect size across studies of 1.02 (95% CI, 1.01–1.03) and 1.65
(95% CI, 1.47–1.85) respectively. There was visual evidence of
funnel asymmetry and Egger’s test for publication bias, P = 0.001.
Hence, a novel regression based method was used to adjust for
publication bias.
The fitted regression line plotted in Figure 3 corresponds to the
regression-based adjustment method. The adjusted estimate is
obtained by extrapolating the line with a standard error of 0 (at the
top of the funnel plot). This produced an adjusted average effect
estimate (RE model) of 1.51 (95% CI, 1.26–1.83).
Residual confounding. The results of the residual confound-
ing analysis are presented in Figure 4. Panel A refers to a
confounder with a prevalence of 0.20 and at this prevalence level,
even a strong confounder causing a 2.5-fold increased risk of CDI
would have to be imbalanced between acid-suppression users and
non-users (OREC = 3.8) to fully account for the observed adjusted
RR of 1.32 (adjusted for publication bias). For a very common
confounder with a prevalence of 0.50 (Panel B) and causing a 2.5-
fold increased risk of CDI, it would have to be distinctly
imbalanced between acid-suppression users and non-users
(OREC = 5.38) to fully account for the observed adjusted RR of
1.32.
Number Needed to HarmThe number needed to harm (NNH) was estimated by using the
pooled OR from the meta-analysis [42]. This analysis is only
speculative as it assumes there is a cause-effect relationship
between PPI and CDI. A recent large prospective hospital cohort
[43] reported the incidence of CDI at 14 days after hospital
admission in patients receiving antibiotics or not: which was 42/
1,000 and 5.4/1000, respectively. Based on these reported baseline
risks, the number needed to harm (NNH) was 50, 95% CI (31, 97)
and 367, 95% CI (226, 718), respectively. For the general
population, the NNH at 1 year was 3925, 95% CI (2412, 7698) at
1 year, based on a baseline incidence of CDI of 48/100,000
person-years [39].
Discussion
FindingsIn this rigorously conducted systemic review and meta-analysis,
we observed a weak association between PPI use and risk of CDI.
This association was further weakened by the presence of
significant heterogeneity. Although we adjusted for publication
bias and ruled out a strong effect of an unmeasured confounder,
the cumulative evidence provided by this systematic review
constitutes only very low quality evidence (as per GRADE
framework) in favor of this association. Factors that negatively
influence the quality of the evidence include the observational
design, inconsistency of results, and evidence of publication bias.
Moreover, even if we assume that the pooled effect estimate is valid, the
absolute risk of CDI would be very low in the general population
with an estimated NNH of 3925 at 1 year. In contrast, the risk
would behighest in hospitalized patients receiving antibiotics with
an estimated NNH of 50 at 2 weeks.
Comparison to Other StudiesSeveral systematic reviews [15,21–23,44,45] examining this
association have been published previously; however, our review is
the most comprehensive and is unique in its analytical approach
and interpretation and thus adds substantially to the cumulative
evidence. Table 3 summarizes the differences between our
systematic and those recently published. First, our review
identified the largest number of studies published to date. For
example, our review has 36% more studies than the largest meta-
analysis by Kowk et al [21] and 90% more studies that the recent
FDA review published in February 2012. Second, our meta-
analysis included adjusted effect estimates of the association
between PPI and CDI. Third, we used meta-regression to explore
sources of heterogeneity. None of the published analyses used this
method. Fourth, we examined the effect of publication bias using a
novel approach of contour-enhanced funnel plot [46]. The largest
and most recent analysis by Kowk et al. [21] did not examine the
effect of publication bias. Fifth, we used a novel regression-based
method to adjust the pooled estimate for publication bias and we
Proton Pump Inhibitors and C. difficile Infection
PLOS ONE | www.plosone.org 4 December 2012 | Volume 7 | Issue 12 | e50836

Ta
ble
1.
Ch
arac
teri
stic
so
fth
eIn
clu
de
dSt
ud
ies.
So
urc
eC
ou
ntr
yC
en
ters
Se
ttin
gC
on
dit
ion
Stu
dy
De
sig
nIn
clu
sio
nC
rite
ria
Aci
dS
up
pre
ssio
nT
he
rap
y
Ku
tty
et
al(V
A),1
20
10
US
Mu
ltic
en
ter
Co
mm
un
ity
Ge
nP
op
Cas
e-c
on
tro
lA
ge
:$
18
yr;
Co
mm
un
ity
on
set
CD
AD
PP
Ie
xpo
sure
3m
op
rio
rto
test
Ku
tty
et
al(D
),1
20
10
US
Mu
ltic
en
ter
Co
mm
un
ity
Ge
nP
op
Cas
e-c
on
tro
lA
ge
:$
18
yr;
Du
rham
resi
de
nce
;C
om
mu
nit
yo
nse
tC
DA
DP
PI
exp
osu
re3
mo
pri
or
tote
st
Sou
the
rne
tal
,22
01
0U
SM
ult
ice
nte
rH
osp
ital
Ab
d-s
urg
ery
pts
Cas
e-C
on
tro
lP
osi
tive
CD
wit
hin
30
daf
ter
surg
ery
;d
iarr
he
aP
PI:
exp
osu
rew
ith
in1
0d
be
fore
surg
ery
Nat
he
tal
,31
99
4C
ASi
ng
leH
osp
ital
He
m-o
nco
log
yp
tsC
ase
-co
ntr
ol
Ad
ult
;In
-pat
ien
t.
3d
Aci
dsu
pp
ress
ive
the
rap
y
Jaya
tila
kae
tal
,42
00
7U
SSi
ng
leH
osp
ital
Ge
nIn
-pat
ien
tC
ase
-co
ntr
ol
Ag
e.
18
PP
Ip
reo
rd
uri
ng
adm
issi
on
Jaya
tila
kae
tal
,42
00
7U
SSi
ng
leH
osp
ital
Ge
nIn
-pat
ien
tC
ase
-co
ntr
ol
Ag
e.
18
PP
I:p
ost
adm
issi
on
Bra
nch
et
al,5
20
07
US
Sin
gle
Ho
spit
alG
en
In-p
atie
nt
Cas
e-c
on
tro
lA
ge
$1
8yr
;In
-pat
ien
tP
PI:
3d
be
fore
test
ing
or
7d
wit
hin
the
last
mo
nth
;b
efo
reh
osp
ital
izat
ion
Al-
Tu
reih
ie
tal
,62
00
5U
SSi
ng
leH
osp
ital
LTC
Fp
tsC
ase
-co
ntr
ol
Po
siti
veC
Dto
xin
;d
ocu
me
nte
dd
iag
no
sis/
AB
Xfo
rC
DA
DP
PI
Shah
et
al(D
),82
00
0U
KSi
ng
leH
osp
ital
Ge
nIn
-pat
ien
tC
ase
-co
ntr
ol
Ag
e.
65
yr;
Ge
nm
ed
ical
/e
lde
rly
care
war
ds
PP
I:u
pto
16
wk
be
fore
dia
rrh
ea
Dia
le
tal
,11
20
05
UK
GP
RD
Co
mm
un
ity
Ge
nP
op
Cas
e-c
on
tro
lA
ge
$1
8yr
;A
tle
ast
2yr
so
fre
cord
sin
the
GP
RD
pri
or
toin
de
xd
ate
;fi
rst
occ
urr
en
ceo
fC
DA
DP
PI:
90
dp
rio
rto
the
ind
ex
dat
e
Akh
tar
et
al,1
22
00
7U
SSi
ng
leH
osp
ital
Ge
nIn
-pat
ien
tC
ase
-co
ntr
ol
Afr
o-A
me
rica
n/
His
pan
icp
tsad
mit
ted
wit
hd
iarr
he
ap
osi
tive
CD
PP
I:3
mb
efo
red
iarr
he
a
Dia
le
tal
,13
20
06
UK
GP
RD
Co
mm
un
ity
Ge
nP
op
Cas
e-c
on
tro
lA
llp
tsw
ith
firs
tp
resc
rip
tio
no
ral
Van
com
ycin
;N
op
revi
ou
sad
mis
sio
n1
yrb
efo
rein
de
xd
ate
PP
I:9
0d
pri
or
toth
ein
de
xd
ate
Ass
eri
et
al,1
42
00
8U
SSi
ng
leH
osp
ital
Ge
nIn
-pat
ien
tC
ase
-co
ntr
ol
Ag
e$
18
Yr;
Inp
tfo
r$
3d
PP
I:at
leas
t3
db
efo
reC
DA
D
Cu
nn
ing
ham
et
al,1
52
00
3U
KSi
ng
leH
osp
ital
Ge
nIn
-pat
ien
tC
ase
-co
ntr
ol
NR
PP
I:p
rece
din
g2
mo
Du
bb
erk
ee
tal
,16
20
07
US
Sin
gle
Ho
spit
alG
en
In-p
atie
nt
Cas
eC
on
tro
lP
tsad
mit
ted
for
.4
8h
rb
etw
ee
nst
ud
yp
eri
od
we
rein
clu
de
dP
PI
Dia
le
tal
,17
20
04
CA
Sin
gle
Ho
spit
alG
en
In-p
atie
nt
Cas
e-c
on
tro
l,(P
)In
-p
tsw
ith
CD
AD
;P
osi
tive
toxi
nre
sult
du
rin
go
rw
ith
inm
afte
rth
ein
de
xad
mis
sio
nP
PI
:at
leas
t3
db
efo
red
iarr
he
a;
3d
inh
osp
ital
ifn
od
iarr
he
a
Loo
et
al,1
82
00
5U
KSi
ng
leH
osp
ital
Ge
nIn
-pat
ien
tC
ase
-co
ntr
ol
Ho
spit
alA
cqu
ire
dC
DA
D;
PP
I:6
wk
be
fore
dia
gn
osi
s
Sun
dra
me
tal
,19
20
09
UK
Sin
gle
Ho
spit
alG
en
In-p
atie
nt
Cas
e-c
on
tro
lA
du
ltH
osp
ital
Acq
uir
ed
CD
AD
PP
I:6
wk
pri
or
too
nse
to
fC
DA
D
Ho
we
lle
tal
,29
20
07
US
Sin
gle
Ho
spit
alG
en
In-p
atie
nt
Co
ho
rtA
ge
$1
8yr
;LO
S$
3d
;O
nly
firs
td
iag
no
sis
Dai
lyP
PI
Dal
ton
et
al,3
02
00
9C
AM
ult
ice
nte
rH
osp
ital
Me
d/S
urg
ical
Sub
spe
cial
tyC
oh
ort
,(R
)A
ge
:$
18
yr;
Min
imu
m7
-dLO
S;A
BX
exp
osu
reP
PI
Day
s:1
8.7
62
1.5
Du
bb
erk
et
al,3
12
00
7U
SSi
ng
leH
osp
ital
Ge
nIn
-pat
ien
tC
oh
ort
,(R
)A
llp
tsad
mit
ted
toB
JHfo
rm
ore
than
48
ho
urs
PP
I
Pe
pin
et
al,3
22
00
5C
ASi
ng
leH
osp
ital
Ge
nIn
-pat
ien
tC
oh
ort
,(R
)A
du
ltIn
-pat
ien
tP
PI
Be
aulie
ue
tal
,33
20
07
CA
Sin
gle
Ho
spit
alM
ed
ical
ICU
Co
ho
rtLO
Sin
ICU
.2
4h
r;
Dia
rrh
ea
.2
4h
ran
dp
osi
tive
CD
toxi
nb
etw
ee
n2
dto
2m
oaf
ter
dis
char
ge
PP
I
Pe
led
et
al,3
42
00
7IL
Sin
gle
Ho
spit
alG
en
In-p
atie
nt
Co
ho
rt,
(P)
CD
test
ing
du
rin
g4
mp
eri
od
;A
BX
wit
hin
40
dp
rio
rto
dia
rrh
ea
PP
I
Dia
le
tal
,17
20
04
CA
Sin
gle
Ho
spit
alM
ed
/CT
surg
ical
war
ds
Co
ho
rtP
har
mac
yd
atab
ase
;A
BX
du
rin
gst
ud
yp
eri
od
;p
osi
tive
toxi
nin
the
infe
ctio
nco
ntr
ol
reg
istr
yP
PI
Lin
sky
et
al,2
82
01
0U
SM
ult
ice
nte
rC
om
mu
nit
y&
Ho
spit
alG
en
Po
pC
oh
ort
,(R
)Fi
rst
po
siti
veC
Dto
xin
,V
Ah
eal
thca
resy
ste
mu
sefo
r1
yrb
efo
reo
raf
ter
the
ind
ex
CD
AD
PP
I:C
on
curr
en
tw
ith
CD
AD
Tre
atm
en
t
Bax
ter
et
al,7
20
08
US
Sin
gle
Ho
spit
alG
en
In-p
atie
nt
Cas
eco
ntr
ol
In-p
atie
nt
PP
I:6
0d
be
fore
ind
ex
dat
e
De
bas
te
tal
,20
20
09
NL
Sin
gle
Ho
spit
al*
Ge
nIn
-pat
ien
tC
ase
con
tro
lA
ge
:$1
8yr
;C
DA
DP
PI:
Inth
ep
ast
3m
o
Ye
arsl
ey
et
al,1
02
00
6U
KSi
ng
leH
osp
ital
Ge
nIn
-pat
ien
tC
ase
con
tro
l,(P
)A
ge
.1
8yr
PP
I:3
mp
rio
rto
stu
dy
en
try
Proton Pump Inhibitors and C. difficile Infection
PLOS ONE | www.plosone.org 5 December 2012 | Volume 7 | Issue 12 | e50836
Ta
ble
1.
Co
nt.
So
urc
eC
ou
ntr
yC
en
ters
Se
ttin
gC
on
dit
ion
Stu
dy
De
sig
nIn
clu
sio
nC
rite
ria
Aci
dS
up
pre
ssio
nT
he
rap
y
Low
ee
tal
,92
00
6C
ASi
ng
leC
om
mu
nit
yG
en
Po
pC
ase
con
tro
l,(R
)1
ho
spit
alad
mis
sio
nfo
rC
DA
D;
Ag
e$
66
yr;
CD
AD
dia
gn
osi
sw
ith
in6
0d
of
AB
Xth
era
py
PP
I:u
pto
36
5d
pri
or
toth
ein
de
xd
ate
No
vell
et
al,2
12
01
0Si
ng
leH
osp
ital
Ge
nIn
-pat
ien
tC
ase
con
tro
l,(R
)A
ge
:$1
8yr
;C
DA
DP
PI
He
nsg
en
se
tal
,22
20
11
NL
Sin
gle
Ho
spit
alG
en
In-p
atie
nt
Cas
eco
ntr
ol,
(P)
All
ho
spit
aliz
ed
pat
ien
tsw
ith
CD
AD
PP
I
Ne
tlan
de
tal
,35
20
11
US
Sin
gle
Co
mm
un
ity
&H
osp
ital
Ge
nP
op
Co
ho
rt,
(R)
Re
curr
en
tC
DA
DP
PI
Ing
lee
tal
,36
20
11
Ind
-ia
Sin
gle
Co
mm
un
ity
&H
osp
ital
Ge
nP
op
Co
ho
rt,
(R)
All
pat
ien
tsw
ith
CD
AD
PP
I
¤M
on
ge
et
al,2
72
01
1Sp
-ain
Sin
gle
Ho
spit
alN
AC
ase
con
tro
lN
AP
PI
Jen
kin
se
tal
,23
20
10
UK
Sin
gle
Ho
spit
alC
ase
con
tro
l,(R
)P
ost
Hip
/Kn
ee
rep
lace
me
nt,
CD
AD
PP
I
Shau
gh
ne
ssy
et
al,3
72
01
1U
SSi
ng
leH
osp
ital
Me
dic
alIC
UC
oh
ort
,(R
)A
llp
atie
nts
wit
hC
DA
Dd
iag
no
sis
PP
I
Kim
et
al,3
82
01
0C
ASi
ng
leH
osp
ital
Ge
nIn
-pat
ien
tC
oh
ort
,(R
)A
ge
:$1
8yr
;R
ecu
rre
nt
CD
AD
PP
I
Loo
et
al,3
92
01
1C
AM
ult
ice
nte
rH
osp
ital
Ge
nIn
-pat
ien
tC
oh
ort
Ag
e:$
18
yr;
he
alth
care
asso
ciat
ed
CD
AD
PP
I
Man
ge
se
tal
,24
20
10
CA
Sin
gle
Ho
spit
alG
en
In-p
atie
nt
Cas
eco
ntr
ol
No
soco
mia
lC
DA
DP
PI
Ku
ntz
et
al,2
62
01
1U
SSi
ng
leC
om
mu
nit
yG
en
Po
pC
ase
con
tro
l,(R
)C
om
mu
nit
yac
qu
ire
dC
DA
DA
cid
sup
pre
ssiv
eth
era
py
Nag
gie
et
al,2
52
01
1U
SM
ult
ice
nte
rC
om
mu
nit
yG
en
Po
pC
ase
con
tro
l,(R
)A
ge
:$1
8yr
Aci
dsu
pp
ress
ive
the
rap
y
Ste
ven
se
tal
,40
20
11
US
Sin
gle
Ho
spit
alG
en
In-p
atie
nt
Co
ho
rtA
ge
:$1
8yr
;h
osp
ital
acq
uir
ed
;n
on
-psy
chia
tric
war
d;
exp
ose
dto
anti
bio
tics
PP
I
Dia
le
tal
,46
20
08
CA
Mu
ltic
en
ter
Co
mm
un
ity
Eld
erl
yp
atie
nts
Cas
eco
ntr
ol
Ag
e$
65
,C
om
mu
nit
yA
sso
ciat
ed
CD
AD
PP
I
McF
arla
nd
et
al,4
22
00
7U
SM
ult
ice
nte
rB
oth
Ge
nP
op
Cas
eco
ntr
ol
CD
AD
Dia
gn
osi
sP
PI
Kaz
ako
vae
tal
,47
20
12
US
Sin
gle
Bo
thG
en
Po
pC
ase
con
tro
lC
DA
DD
iag
no
sis,
on
set
du
rin
gth
ep
re-o
utb
reak
or
ou
tbre
akp
eri
od
s,h
osp
ital
izat
ion
PP
I
Mo
de
na
et
al,4
32
00
5U
SSi
ng
leB
oth
Ge
nP
op
Cas
eco
ntr
ol
Re
ceiv
ed
atle
ast
5d
ays
of
anti
bio
tics
pri
or
tod
iag
no
sis
of
CD
AD
PP
I
Mu
toe
tal
,44
20
05
US
Sin
gle
Ho
spit
alG
en
Inp
atie
nts
Cas
eco
ntr
ol
No
soco
mia
lC
DA
DP
PI:
Du
rin
gth
e4
we
eks
be
fore
de
tect
ion
of
CD
AD
Yip
et
al,4
52
00
1C
ASi
ng
leH
osp
ital
Ge
nIn
pat
ien
tsC
ase
con
tro
lN
oso
com
ial
CD
AD
PP
I
Lin
ne
ye
tal
,41
CA
Sin
gle
Ho
spit
alG
en
Inp
atie
nts
Cas
eco
ntr
ol
No
soco
mia
l,o
nse
td
uri
ng
ou
tbre
ak.
PP
Ib
ein
gta
ken
on
the
dat
eo
fC
DA
Dd
iag
no
sis
Lin
ne
ye
tal
,41
CA
Sin
gle
Ho
spit
alG
en
Inp
atie
nts
Cas
eco
ntr
ol
No
soco
mia
l,o
nse
td
uri
ng
ou
tbre
ak.
PP
Ib
ein
gta
ken
be
fore
the
dat
eo
fC
DA
Dd
iag
no
sis
¤N
A:
Dat
ao
bta
ine
dfr
om
abst
ract
Leg
en
d:
OR
:o
dd
sra
tio
;H
R:
har
zard
rati
o;
CD
AD
:C
lost
rid
ium
dif
fici
le-a
sso
ciat
ed
dia
rrh
ea;
PP
I:P
roto
np
um
pin
hib
ito
r;H
2R
A:
VA
:V
ete
ran
Aff
airs
;D
:D
urh
amC
ou
nty
,P
:P
rosp
ect
ive
;R
:R
etr
osp
ect
ive
,A
BX
:A
nti
bio
tic;
GP
RD
:G
en
era
lP
ract
ice
Re
sear
chD
atab
ase
;IC
U:
Inte
nsi
veca
reu
nit
Me
tab
olic
pro
cess
es
are
con
tro
lled
by
ava
rie
tyo
fe
nzy
me
s.Fo
rin
stan
ce,c
yto
chro
me
P4
50
mo
no
oxy
ge
nas
eco
uld
de
toxi
fyh
erb
icid
es
such
asfe
no
xap
rop
-eth
yl,d
iclo
fop
-me
thyl
,an
db
en
tazo
nin
pla
nts
[22
,23
].P
oly
ph
en
olo
xid
ase
(PP
O),
com
mo
nly
fou
nd
infu
ng
ian
dp
lan
ts,r
efe
rsto
ag
rou
po
fe
nzy
me
sth
atca
taly
zeth
eo
xid
atio
no
fp
he
no
licco
mp
ou
nd
s[2
4].
Pe
roxi
das
e(P
OD
),an
oth
er
typ
eo
fo
xid
ativ
ee
nzy
me
com
mo
nly
pre
sen
tin
pla
nt
and
anim
alti
ssu
es,
can
oxi
diz
ep
he
no
lsan
dar
om
atic
amin
es
inth
ep
rese
nce
of
hyd
rog
en
pe
roxi
de
.In
con
tras
t,th
eo
xid
atio
no
fp
he
no
licco
mp
ou
nd
sb
yP
PO
req
uir
es
the
pre
sen
ceo
fo
xyg
en
gas
[25
].B
oth
PP
Oan
dP
OD
pla
yim
po
rtan
tro
les
inth
em
eta
bo
lism
of
aro
mat
icco
mp
ou
nd
sin
soil
and
wat
er
[26
,27
].H
ow
eve
r,lit
tle
info
rmat
ion
isav
aila
ble
reg
ard
ing
the
irfu
nct
ion
inth
em
eta
bo
lism
of
PA
Hs
by
pla
nts
.d
oi:1
0.1
37
1/j
ou
rnal
.po
ne
.00
50
46
7.t
00
1
Proton Pump Inhibitors and C. difficile Infection
PLOS ONE | www.plosone.org 6 December 2012 | Volume 7 | Issue 12 | e50836

examined the potential effect of a residual confounding on the
observed association using the rule-out approach.
Finally, we interpret the results in the context of observed
limitations and therefore, draw more careful conclusions. Contrary
to other reviews and FDA alert, we conclude that current
cumulative data constitutes very low quality evidence. Our results
are helpful for guidelines writing committees and policy makers
that use the GRADE framework when formulating recommenda-
tions for use of PPI for different clinical indications.
Biologic PlausibilityThe mechanism by which PPI therapy contributes to an
increased risk of CDI is unclear, because gastric acid does not kill
Figure 2. Forest Plot of the Meta analyses of The Association Between CDI and Proton Pump Inhibitors Based on 51 Observations.doi:10.1371/journal.pone.0050836.g002
Proton Pump Inhibitors and C. difficile Infection
PLOS ONE | www.plosone.org 7 December 2012 | Volume 7 | Issue 12 | e50836
gastric C. difficile spores. This further makes a cause-effect
relationship a less likely explanation for the observed association.
It has been proposed that the vegetative form of C. difficile,
which is killed by acid, plays a role in pathogenesis. Vegetative
forms survive on surfaces and could be ingested by patients [47].
Survival of these acid-sensitive vegetative forms in the stomach
could be facilitated by 2 main factors: (1) suppression of gastric
acid production by acid-suppressive medications; and (2) presence
of bile salts in gastric contents of patients on acid-suppressive
therapy. Bile salts, which are mainly found in the small intestine,
are present in gastric contents, particularly among patients with
gastro-esophageal reflux disease (GERD). Moreover, PPI use can
delay gastric emptying and predispose to bacterial overgrowth
with associated high intragastric bile salts which could trigger
spore germination in the stomach [48–50].
However, a recent in vitro experiment has challenged these
postulated biological mechanisms for the observed association. In
this experiment, aspirate of gastric contents from hospitalized
patients with nasogastric tubes were collected. It concluded that C.
difficile spores were not killed in acidic gastric content and did not
Table 2. Influence of study type, country, weather effect estimate adjusted or not and PPI ascertainment method on the pooledeffect estimate and its associated heterogeneity.
Group Pooled Effect Estimate 95% CI I2% Number of Observations
All citations 1.65 (1.47, 1.85) 89.9 51
Case-control citations 1.70 (1.42, 2.03) 88.7 37
Cohort citations 1.64 (1.30, 2.08) 87.8 14
Asia 3.26(1.91, 5.58) 0.0 3
Canada 1.22 (1.09, 1.37) 82.1 14
Europe 1.90 (1.35, 2.66) 75.5 10
USA 1.70 (1.41, 2.04) 73.3 24
Studies reported adjusted effect estimates* 1.78 (1.56, 2.02) 92.2 37
Studies reported unadjusted effect estimates* 1.27 (0.93, 1.71) 59.4 14
PPI ascertainment method (Chart){ 1.89 (1.45, 2.45) 93.6 20
PPI ascertainment method (Interview){ 1.17 (0.91, 1.51) 79.0 8
doi:10.1371/journal.pone.0050836.t002
Figure 3. Contour enhanced funnel plot of the association between the effect-estimates and its standard errors: * Contour enhancedfunnel plots with implementation of regression adjustment model (adjusted effect at top where SE is 0).* The contour lines differentiate thesignificance and non-significance regions in the plot at 1%, 5% and 10% significance levels. *Vertical lines show average effect-estimates fromrandom effect (red), and fixed effect models (blue). *A regression line (black) is added for regression based adjustment (With adjusted effect estimateand 95% CI at top where SE is 0). Abbreviations: FEMA: Fixed effect meta-analysis, REMA: Random effect meta-analysis, Reg: Regression line.doi:10.1371/journal.pone.0050836.g003
Proton Pump Inhibitors and C. difficile Infection
PLOS ONE | www.plosone.org 8 December 2012 | Volume 7 | Issue 12 | e50836

Figure 4. Influence of a hypothetical dichotomous confounder present in 20% (panel A) and 50% (panel B) of the study population,unaccounted for in the adjustments already performed in the individual studies. The graphs indicate what combinations of OREC and RRthat would be necessary for the confounder to fully account for the observed association between proton pump inhibitor (PPI) use and CDAD afteradjustment for publication bias. Abbreviations: OREC, odds ratio of exposure to the confounder in PPI non-users vs. acid-suppression users; RRCD,relative risk of CDAD in individuals exposed to the confounder vs. non-exposed.doi:10.1371/journal.pone.0050836.g004
Proton Pump Inhibitors and C. difficile Infection
PLOS ONE | www.plosone.org 9 December 2012 | Volume 7 | Issue 12 | e50836

germinate in gastric contents of hospitalized patients on PPI.
Germination occurred with the addition of taurocholic acid [51].
LimitationsThere are limitations to our work. First, observational studies
are subject to inherent limitations in the study design leading to
unmeasured differences in the study population and unmeasured
confounders despite all possible adjustments. PPIs use may be a
surrogate of comorbidities and thus, the observed association may
have been affected by selective overuse of PPIs in high risk groups.
For example, the potential interaction between PPIs and
Clopidogrel found in observational studies was refuted in
randomized controlled trials [52]. Second, the use of PPIs was
based on electronic and prescription records, rather than by actual
use by the patient. Third, there is presence of publication bias, and
substantial amount of heterogeneity in the included studies. There
are many patient level parameters which may have led to
substantial heterogeneity. Nevertheless, investigating these vari-
ables is only possible with individual patient data meta-analysis.
Fourth, all statistical methods used to assess for publication bias or
residual confounding are subject to certain assumptions and have
inherent limitations. For example, funnel plot asymmetry can be
due to between studies heterogeneity rather than publication bias
[31].
Given these limitations, focus on hand hygiene as one of the
cornerstones of prevention of nosocomial transmission of C. difficile
is warranted. Several studies have documented the reduction of
rates of hospital acquired infection by improvement in the
compliance with hand washing by healthcare workers between
episodes of contact with patients [53].
ConclusionsIn this rigorously conducted systemic review and meta-analysis,
we found very low quality evidence in support of an association
between PPI use and risk of CDI. This association was weakened
by the presence of significant heterogeneity and publication bias.
Our findings are re-assuring that PPIs use in the general
population does not pose a significant CDI risk. On the other
hand, our findings warrant judicious and evidence-based use of
PPI in patients at high risk for CDI.
Supporting Information
Table S1 The Association between PPI use and Devel-opment of Clostridium difficile infection in Case-controlCitations.
(DOCX)
Table S2 The Association between PPI use and Devel-opment of Clostridium difficile infection from Cohortcitations.
(DOCX)
Table S3 Meta-regression analysis to explore sources ofheterogeneity.
(DOCX)
Table S4 Forest plot of the meta-analysis of theproportion of Clostridium difficile cases that wereexposed to antibiotics.
(DOCX)
Table S5 Modified Newcastle-Ottawa Quality Assess-ment Scale for Case-control studies included in theMeta-analysis.
(DOCX)
Ta
ble
3.
Sum
mar
yo
fre
vie
ws
of
the
asso
ciat
ion
be
twe
en
PP
Iu
sean
dC
lost
rid
ium
Dif
fici
lein
fect
ion
.
Stu
dy
Se
arc
hE
ng
ine
sD
ate
Aci
dsu
pp
ress
ion
Nu
mb
er
of
ob
serv
ati
on
sP
oo
led
eff
ect
est
ima
tes
He
tero
ge
ne
ity
Ex
plo
rin
gh
ete
rog
en
eit
yP
ub
lica
tio
nb
ias
ass
ess
me
nt
Re
sid
ua
lco
nfo
un
din
g
Tle
yje
he
tal
(Pre
sen
tre
vie
w)
Med
line
EMB
ASE
ISI
Web
of
Scie
nce
and
Else
vier
Sco
pu
sJa
n2
01
2P
PI
51
1.6
5(1
.47
,1
.85
)I2
=8
9.9
%M
eta
-re
gre
ssio
nC
on
tou
r-e
nh
ance
dfu
nn
el
plo
tas
ymm
etr
yR
ule
-ou
tap
pro
ach
FDA
Ale
rt,
44
No
tav
aila
ble
NR
PP
I2
8Sy
ste
mat
icre
vie
wo
nly
No
me
ta-a
nal
ysis
NA
NA
NA
NA
Kw
ok
et
al,2
12
01
2M
ed
line
EMB
ASE
De
c2
01
1P
PI
39
1.7
4(1
.47
–2
.85
)I2
=8
5%
Sen
siti
vity
anal
yse
s:-C
ase
-co
ntr
ol
-Co
ho
rt-L
ab.
Co
nfi
rmat
ion
-In
pat
ien
t-
Co
mm
un
ity
or
mix
ed
-A
dju
ste
de
stim
ate
s
No
tas
sess
ed
No
tas
sess
ed
Bav
ish
ian
dD
up
on
t,2
32
01
1M
ed
line
May
20
11
PP
I2
7Sy
ste
mat
icre
vie
wo
nly
No
me
ta-a
nal
ysis
NA
NA
NA
NA
Jan
arth
anan
et
al,4
52
01
2M
ed
line
De
c2
01
0P
PI
23
1.6
9(1
.39
5–
1.9
74
)I2
=9
1.9
%Su
bg
rou
pan
alys
is:
Cas
e-
con
tro
l-C
oh
ort
Fun
ne
lp
lot:
po
ssib
leas
ymm
etr
yN
ot
asse
sse
d
De
shp
and
ee
tal
,22
20
12
Me
dlin
eC
INA
HL
Co
chra
ne
We
bo
fSc
ien
cean
dSc
op
us
Oct
20
10
PP
I3
02
.15
(1.8
1–
2.5
5)
Un
ad
just
ed
da
taI2
=8
7%
-Cas
e-c
on
tro
l-C
oh
ort
-%an
tib
ioti
cu
sed
Fun
ne
lp
lot:
no
asym
me
try
No
tas
sess
ed
Leo
nar
de
tal
,15
20
07
Me
dlin
eC
INA
HL
EMB
ASE
D2
00
5P
PI
11
2.0
5(1
.47
–2
.85
)U
na
dju
ste
dd
ata
P,
0.0
01
No
tas
sess
ed
Fun
ne
lp
lot:
no
asym
me
try
No
tas
sess
ed
Leg
en
d:
PP
I:P
roto
np
um
pin
hib
ito
r;N
A:
No
tav
aila
ble
.d
oi:1
0.1
37
1/j
ou
rnal
.po
ne
.00
50
83
6.t
00
3
Proton Pump Inhibitors and C. difficile Infection
PLOS ONE | www.plosone.org 10 December 2012 | Volume 7 | Issue 12 | e50836

Figure S1 Forest plot of the meta-analysis of theproportion of Clostridium difficile cases that wereexposed to antibiotics.
(DOCX)
Author Contributions
Analyzed the data: IMT AJS MR ABA MAA MAG. Wrote the paper:
IMT MR ARK ABA MAA MAG MA. Study concept and design: IMT
AJS MR PJE. Data abstraction: ABA FAA MA AA TI MAG. Quality
assessment: FAA ABA MAG. Revision of the manuscript: IMT AJS MR
ABA FAA MAA AA TI MAG ARK LMB.
References
1. IMS Health (2005) Leading 20 therapeutic classes by U.S. sales, Available: http:
//www.imshealth.com/ims/portal/front/articleC/0,2777,6599_73915261_
77140565,00.html. Accessed 2006 June.
2. Yachimski PS, Farrell EA, Hunt DP, Reid AE (2010) Proton Pump Inhibitors forProphylaxis of Nosocomial Upper Gastrointestinal Tract BleedingEffect of
Standardized Guidelines on Prescribing Practice. Arch Intern Med. 2010;170(9):779–783.
3. Batuwitage BT, Kingham JGC, Morgan NE, Bartlett RL (2007) Inappropriate
prescribing of proton pump inhibitors in primary care. Postgrad Med J 83: 66–
68.
4. Cahir C, Fahey T, Teeling M, Teljeur C, Feely J, et al. (2010) Potentiallyinappropriate prescribing and cost outcomes for older people: a national
population study. Br J Clin Pharmacol 69(5): 543–552.
5. Mat Saad AZ, Collins N, Lobo MM, O’Connor HJ (2005) Proton pumpinhibitors: a survey of prescribing in an Irish general hospital. Int J Clin Pract 59:
31–34.
6. Niklasson A, Bajor A, Bergendal L, Simren M, Strid H, et al. (2003) Overuse of
acid suppressive therapy in hospitalized patients with pulmonary diseases. RespirMed 97: 1143–1150.
7. Scagliarini R, Magnani E, Pratico A, Bocchini R, Sambo P, et al. (2005)
Inadequate use of acid-suppressive therapy in hospitalized patients and itsimplications for general practice. Dig Dis Sci 50: 2307–2311.
8. Ahrens D, Chenot JF, Behrens G, Grimmsmann T, Kochen MM (2010)
Appropriateness of treatment recommendations for PPI in hospital dischargeletters. Eur J Clin Pharmacol 66(12): 1265–1271.
9. US Food and Drug Administration (2009) Information for healthcare
professionals: update to the labeling of clopidogrel bisulfate (marketed as Plavix)
to alert healthcare professionals about a drug interaction with omeprazole(marketed as Prilosec and Prilosec OTC). U.S. Department of Health and
Human Services, 11/17/2009. http: //www.fda.gov/Drugs/Drug Safety/Postmarket Drug Safety Information for Patients and Providers/Drug Safety
Information for Heath,care Professionals/ucm190787.htm. Accessed 9/23/
2010.
10. Charlot M, Grove EL, Hansen PR, Olesen JB, Ahlehoff O, et al. (2011) Protonpump inhibitor use and risk of adverse cardiovascular events in aspirin treated
patients with first time myocardial infarction: nation-wide propensity score-matched study. BMJ 342: d2690.
11. Eom CS, Park SM, Myung SK, Yun JM, Ahn JS (2011) Use of acid suppressive
drugs and risk of fracture: a meta-analysis of observational studies. Ann Fam
Med 9(3): 257–267.
12. Sierra F, Suarez M, Rey M, Vela MF (2007) Systematic review: proton pumpinhibitor-associated acute interstitial nephritis. Aliment Pharmacol Ther 26:
545–553.
13. Johnstone J, Nerenberg K, Loeb M (2010) Meta-analysis: proton pump inhibitoruse and the risk of community-acquired pneumonia. Aliment Pharmacol Ther
31(11): 1165–1177.
14. Dial MS. (2009) Proton pump inhibitor use and enteric infections.Am J Gastroenterol (suppl 2): S10–S16.
15. Leonard J, Marshall JK, Moayyedi P (2007) Systematic review of the risk of
enteric infection in patients taking acid suppression. Am J Gastroenterol 102:
2047–2056.
16. Jarvis WR, Schlosser J, Jarvis AA, Chinn RY (2009) National point prevalence ofClostridium difficile in US health care facility inpatients, 2008. Am J Infect
Control 37: 263–270.
17. Archibald LK, Banerjee SN, Jarvis WR (2004) Secular trends in hospital-acquired Clostridium difficile disease in the United States. J Infect Dis 189:
1585–1589.
18. McDonald LC, Owings M, Jernigan JB (2006) Clostridium difficile infection in
patients discharged from US short-stay hospitals, 1996–2003. Emerg Infect Dis12: 409–415.
19. Elixhauser A, Jhung M (2008) Clostridium difficile-associated disease in US
hospitals, 1993–2005. HCUP statistical brief No. 50, April 2008. US Agency forHealthcare Research and Quality, Rockville, MD. Available at: http: //www.
hcup-us.ahrq.gov/reports/statbriefs.sb50.pdf. Accessed February 16, 2009.
20. Redelings MD, Sorvillo F, Mascola L (2007) Increase in Clostridium difficile-related mortality rates, United States, 1999e2004. Emerg Infect Dis 13(9): 1417–
1419.
21. Kwok CS, Arthur AK, Anibueze CI, Singh S, Cavallazzi R, et al. (2012) Risk of
Clostridium difficile Infection With Acid Suppressing Drugs and Antibiotics: Meta-Analysis. Am J Gastroenterol 107(7): 1011–1019.
22. Deshpande A, Pant C, Pasupuleti V, Rolston DD, Jain A, et al. (2012) Association
between proton pump inhibitor therapy and Clostridium difficile infection in ameta-analysis. Clin Gastroenterol Hepatol 10(3): 225–233.
23. Bavishi C, Dupont HL (2011) Systematic review: the use of proton pump
inhibitors and increased susceptibility to enteric infection. Aliment Pharmacol
Ther 34(11–12): 1269–1281.
24. Stroup DF, Berlin JA, Morton SC, Olkin I, Williamson GD, et al. (2000) Meta-analysis of Observational Studies in Epidemiology: A Proposal for Reporting.
JAMA 283: 2008–2012.
25. Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gøtzsche PC, et al. (2009) ThePRISMA statement for reporting systematic reviews and meta-analyses of studies
that evaluate healthcare interventions: explanation and elaboration. BMJ
2009;339: b2700.
26. Guyatt GH, Oxman AD, Vist G, Kunz R, Falck-Ytter Y, et al. (2008) Rating
quality of evidence and strength of recommendations GRADE: an emerging
consensus on rating quality of evidence and strength of recommendations. BMJ336: 924–926.
27. Wells G, Shea B, O’Connell D, Peterson J, Welch V et al. The Newcastle-
Ottawa scale (NOS) for assessing the quality of non-randomized studies in meta-analysis. Ottawa, Ontario: The Ottawa Health Research Institute. Available:
http: //www.ohri.ca/programs/clinicalepidemiology/nosgen.doc. Accessed on2011 September 13.
28. Higgins JPT, Altman DG (2008) Chapter 8: Assessing risk of bias in included
studies. In: Higgins JPT, Green S, editors. Cochrane Handbook for Systematic
Reviews of Interventions Version 5.0.1 [updated September 2008] TheCochrane Collaboration, 2008. Available: www.cochrane-handbook.org. Ac-
cessed 2010 December 15.
29. DerSimonian R, Laird N (1986) Meta-analysis in clinical trials. Control ClinTrials 7(3): 177–188.
30. Peters JL, Sutton AJ, Jones DR, Abrams KR, Rushton L (2008) Contour-
enhanced meta-analysis funnel plots help distinguishing publications bias fromother causes of asymmetry. J Clin Epidemiol 61: 991–996.
31. Egger M, Davey Smith G, Schneider M, Minder C (1997) Bias in meta-analysis
detected by a simple, graphical test. BMJ 315: 629–634.
32. Moreno SG, Sutton AJ, Ades AE, Stanley TD, Abrams KR, et al. (2009)Assessment of regression-based methods to adjust for publication bias through a
comprehensive simulation study. BMC Med Res Methodol 9: 2.
33. Schneeweiss S (2006) Sensitivity analysis and external adjustment for
unmeasured confounders in epidemiologic database studies of therapeutics.Pharmacoepidemiol Drug Saf 15: 291–303.
34. Zhang J, Yu KF (1998) What’s a relative risk? A method of correcting the odds
ratio in cohort studies of common outcomes. JAMA 280: 1690–1691.
35. Dial S, Alrasadi K, Manoukian C, Huang A, Menzies D (2004) Risk ofClostridium difficile diarrhea among hospital inpatients prescribed proton pump
inhibitors: cohort and case-control studies. CMAJ 171(1): 33–38.
36. Kutty PK, Woods CW, Sena AC (2010) Risk Factors for and EstimatedIncidence of Community-associated Clostridium difficile Infection, North Carolina,
USA. Emerg Infect Dis 16(2): 197–204.
37. Jayatilaka S, Shakor R, Eddi R, Bakaj G, Baddoura WJ, et al. (2007) Clostridium
difficile Infection in an Urban Medical Centre: Five-year Analysis of Infection
Rates among Adults admissions and Association with the Use of Protein Pump
Inhibitors. Ann Clin Lab Sci 37(3): 241–247.
38. Linney S, Fernandes T, Einarson T, Sengar A, Walker JH, et al. (2010)Association Between Use of Proton Pump Inhibitors and a Clostridium difficile–
Associated Disease Outbreak: Case–Control Study. Can J Hosp Pharm 63(1):31–37.
39. http: //www.cochrane-net.org/openlearning/html/mod14-2.htm.
40. Bajaj JS, Ananthakrishnan AN, Hafeezullah M, Zadvornova Y, Dye A, et al.
(2010) Clostridium difficile is Associated With Poor Outcomes in Patients WithCirrhosis: A National and Tertiary Center Perspective. Am J Gastroenterol 105:
106–113.
41. Wilcox CM, Martin T, Phadnis M, Mohnen J, Worthington J, et al. (2008)Absence of gastrointestinal infections in a cohort of patients with Zollinger-
Ellison syndrome and other acid hypersecretors receiving long-term acid
suppression with lansoprazole. BMC Gastroenterol 8: 18.
42. Lowe DO, Mamdani MM, Kopp A, Low DE, Juurlink DN (2006) Proton pumpinhibitors and hospitalization for Clostridium difficile–associated disease: a
population-based study. Clin Infect Dis 43(10): 1272–1276.
43. Howell MD, Novack V, Grgurich P, Soulliard D, Novack L, et al. (2010)Iatrogenic Gastric Acid Suppression and the Risk of Nosocomial Clostridium
difficile Infection. Arch Intern Med 170(9): 784–790.
44. Available: http: //www.fda.gov/Drugs/DrugSafety/ucm290510.htm.Accessed2012 February 14.
45. Janarthanan S, Ditah I, Adler DG, Ehrinpreis MN (2012) Clostridium difficile-
Associated Diarrhea and Proton Pump Inhibitor Therapy: A Meta-Analysis.
Am J Gastroenterol 107(7): 1001–1010.
Proton Pump Inhibitors and C. difficile Infection
PLOS ONE | www.plosone.org 11 December 2012 | Volume 7 | Issue 12 | e50836

46. Moreno SG, Sutton AJ, Turner EH, Abrams KR, Cooper NJ, et al. (2009)
Novel methods to deal with publication biases: secondary analysis of
antidepressant trials in the FDA trial registry database and related journal
publications. BMJ 339: b2981.
47. Jump RL, Pultz MJ, Donskey CJ (2007) Vegetative Clostridium difficile survives in
room air on moist surfaces and in gastric contents with reduced acidity: a
potential mechanism to explain the association between proton pump inhibitors
and C. difficile-associated diarrhea? Antimicrob Agents Chemother 51: 2883–
2887.
48. Wilson KH (1983) Efficacy of various bile salt preparations for stimulation of
Clostridium difficile spore germination. J Clin Microbiol 18: 1017–1019.
49. Theisen J, Nehra D, Citron D, Johannson J, Hagen J, et al. (2000) Suppression
of gastric acid secretion in patients with gastroesophageal reflux disease results in
gastric bacterial overgrowth and deconjugation of bile acids. J Gastrointest Surg
4: 50–54.50. Thorens J, Froehlich F, Schwizer W, Saraga E, Bille J, et al. (1996) Bacterial
overgrowth during treatment with omeprazole compared with cimetidine: a
prospective randomized double blind study. Gut 39: 54–59.51. Nerandzic MM, Pultz MJ, Donskey CJ (2009) Examination of Potential
Mechanisms To Explain the Association between Proton Pump Inhibitors andClostridium difficile Infection. Antimicrob Agents Chemother 53(10): 4133–4137.
52. Bhatt DL, Cryer BL, Contant CF, Cohen M, Lanas A, et al. (2010) Clopidogrel
with or without omeprazole in coronary artery disease. N Engl J Med; 363:1909–1917.
53. Boyce JM, Pittet D (2002) Healthcare Infection Control Practices AdvisoryCommittee; HICPAC/SHEA/APIC/IDSA Hand Hygiene Task Force.
MMWR Recomm Rep. 25;51(RR-16): 1–45.
Proton Pump Inhibitors and C. difficile Infection
PLOS ONE | www.plosone.org 12 December 2012 | Volume 7 | Issue 12 | e50836