assessment of community based integrated management … · assessment of community based integrated...
TRANSCRIPT

Assessment of Community Based Integrated Management of Neonatal and Childhood Illness Program
2
World Health Organization (WHO)
UN house, Pulchowk, Lalitpur, Nepal
Submitted By Nepal Development Research Institute Shree Durbar Tole, Pulchowk, Lalitpur, Nepal
Submission date: 28th April, 2017

3
This report is a product of research on“Assessment of Community Based Integrated
Management of Neonatal and Childhood Illness Program“carried out by Nepal Development Research Institute with the financial support of World Health
Organization from November 2016 to March 2017
Study Team • Mr. Bhim Prasad Shrestha, Team Leader
• Dr. Nisha Manandhar, Consultant Expert
• Dr. Pranil Man Singh Pradhan, Consultant Expert
• Dr. Jaya Kumar Gurung, Project Coordinator
• Ms. Usha Sing, Research Associate
• Ms. Kristina Parajuli, Research Associate
• Mr. Rajendra Khatri , Field and data coordinator
Report By:
Nepal Development Research Institute
Shree Durbar Tole, Pulchowk, Lalitpur

4
Table of Contents
Acknowledgement .................................................................................................................................... 8
Acronyms ................................................................................................................................................ 10
Executive summary ................................................................................................................................. 12
1 Introduction ........................................................................................................................................ 15
1.1 Background ................................................................................................................................. 15
1.2 Rationale and Objective of the Study ......................................................................................... 16
1.3 Methodology ..................................................................................................................................... 17
1.3.1 Sample design and sample selection ...................................................................................... 17
1.5 Data Collection .................................................................................................................................. 22
1.6 Data Analysis and Presentation ........................................................................................................ 26
1.7 Limitation of the Study...................................................................................................................... 28
2 Survey Findings ................................................................................................................................... 30
1. Survey Findings for District Focal Person ........................................................................................ 30
2. Survey Findings for HF Interview ........................................................................................................ 33
2.1 Availability of service readiness in the HF .................................................................................. 33
2.2 Availability of services in the health facilities ............................................................................. 34
2.3 Availability of equipments......................................................................................................... 35
2.4 Availability of drugs and commodities....................................................................................... 36
2.5 Availability of guidelines/IEC/BCC materials .............................................................................. 36
2.6 Recording ................................................................................................................................. 37
2.7 Reporting ................................................................................................................................. 42
3. Survey Findings for HSP ...................................................................................................................... 49
3.1 Designation of Health service provider ...................................................................................... 49
3.2 Service readiness of HSP in HF focusing on CB-IMNCI ................................................................ 49
3.3 Knowledge of HSP (< 2 months children) .................................................................................. 50
3.4 Knowledge of HSP (2-59 months children) ................................................................................ 53
3.5 Perception of HSPs on FCHV's role ............................................................................................ 58
3.6 Knowledge of SBA ..................................................................................................................... 58
3.7 Referral .................................................................................................................................... 59

5
4. Survey Findings for Follow up visit Results ......................................................................................... 64
4.1 Distance from the HF to the residence ...................................................................................... 64
4.2 Waiting time to get health services ............................................................................................ 65
4.3 Presenting complains of the children coming to the HF for consultation .................................... 65
4.4 Reasons for taking to the HF ..................................................................................................... 66
4.5 Assessment of weight and temperature .................................................................................... 66
4.6 Health services provided during the follow up visit .................................................................... 67
4.7 Quality of services received by the clients ................................................................................. 69
5. Survey Findings for Exit Interview ....................................................................................................... 71
5.1 Distance from the HF to the residence ...................................................................................... 71
5.2 Waiting time to get health services ............................................................................................ 72
5.3 Presenting complains of the children coming to the HF for consultation .................................... 72
5.4 Assessment of weight and temperature .................................................................................... 73
5.5 Health services provided during visit to the HF .......................................................................... 73
5.6 Quality of services received by the clients ................................................................................. 75
6. Survey Findings for Female Community Health Volunteer (FCHV) Interview .................................... 77
6.1 Trainings of the Female Community Health Volunteer ............................................................... 77
6.2 Knowledge of the FCHVs ........................................................................................................... 78
6.3 Volume of service provided to the children < 5 years age for diarrhea ....................................... 81
6.4 Available stocks of ORS, Zinc and Chlorhexidine at present ....................................................... 82
3. Summary of the Findings .................................................................................................................... 84
4. Conclusion and Recommendation ...................................................................................................... 89
Bibliography ................................................................................................................................................ 91
ANNEX ......................................................................................................................................................... 92
Annex 1. District selection ...................................................................................................................... 92
Annex 2. Detail field plan and facility allocation to each field reasearchers .......................................... 96
Annex 3. Training schedule ..................................................................................................................... 98
Annex 4. Final questionnaire for the survey ......................................................................................... 101
Annex 5. Glimpse of the survey: ........................................................................................................... 151

6
List of tables:
Table 1: Sample size of the study ................................................................................................................ 22Table 2: Types of Health faciliies in each study districts ............................................................................. 33Table 3: Training of services to health staffs .............................................................................................. 34Table 4: Availability of Servicesin Health facilities ...................................................................................... 34Table 5: Availability of equipments ............................................................................................................. 35Table 6: Availaability of Drugs and commodities in health facilities .......................................................... 36Table 7: Availability of guidelines/ IEC/BCC/ materials .............................................................................. 37Table 8: Component observed in register .................................................................................................. 38Table 9: Place where PSBI cases recoreded ................................................................................................ 39Table 10: Component observed in register for ARI/pneumonia ................................................................ 40Table 11: Component observed in register for diarrhea ............................................................................ 41Table 12: Reporting ..................................................................................................................................... 43Table 13: Training ........................................................................................................................................ 50Table 14: Treatment of PSBI cases .............................................................................................................. 52Table 15: Diagnisis of Pneumonia ............................................................................................................... 54Table 16: HSP response to treatment of Pneumonia ................................................................................. 55Table 17: HSP response to diagnosis of diarrhea ........................................................................................ 56Table 18: HSP response to classification of diarrhea .................................................................................. 56Table 19: HSP response to treatment of diarrhea ...................................................................................... 57Table 20: Response on SBA on services given to newborn after birth ....................................................... 59
List of figures
Figure 1: CB-IMNCI implementation status ................................................................................................ 18Figure 2: CB-NCP disrtict and CB-IMNCI implementation approach .......................................................... 19Figure 3: District selection in Ecological region .......................................................................................... 20Figure 4 : Sample Selection Techniques ...................................................................................................... 21Figure 5: Designation for HSP ..................................................................................................................... 49Figure 6: Designation for HSP ..................................................................................................................... 49Figure 7: Assessment done to diagnose PSBI ............................................................................................. 50Figure 8: Ways to Diagnosis of PSBI cases .................................................................................................. 51Figure 9: Management of PSBI .................................................................................................................... 53Figure 10: General danger sign ................................................................................................................... 53Figure 11: HSP perception on FCHV role .................................................................................................... 58Figure 12: Condition for referral ................................................................................................................. 59Figure 13: Problem faced by HSP in diagnosis of PSBI ................................................................................ 60

7
Figure 14: Problem faced by HSP in managing PSBI cases .......................................................................... 61Figure 15: Problem faced by HSP in diagnosis of ARI/pPneumonia and diarrhea ...................................... 62Figure 16: Problem faced by HSP in management of Pneumonia .............................................................. 62Figure 17: problem faced by HSP while treating Diarrhea ......................................................................... 63Figure 18: distace from HF to residence ..................................................................................................... 64Figure 19: Waiting time at HFs .................................................................................................................... 65Figure 20: Presesnting complians of the children coming to HF ................................................................ 66Figure 21: Assessment according disease type ........................................................................................... 66Figure 22: Information and services received by caretakers ...................................................................... 67Figure 23: Caretakers satisfaction with the quality of the health services received .................................. 70Figure 24: Distance from HF to residence ................................................................................................... 71Figure 25: Waiting time to get health services ........................................................................................... 72Figure 26: Presenting complians of the children coming to the HF ............................................................ 72Figure 27: Assessment according to disease type ...................................................................................... 73Figure 28: Information and services received by caretakers ...................................................................... 74Figure 29: care takers satisfaction with the quality of health service received ......................................... 76Figure 30: distance from HF to residence ................................................................................................... 77Figure 31: Types of training received by FCHV ........................................................................................... 77Figure 32: PNC visit by FCHV to mothers .................................................................................................... 78Figure 33: Information provided by FCHV .................................................................................................. 79Figure 34: Signs assessed in < 2 months children by FCHVs for referral .................................................... 80Figure 35: Service provided to <5 children for diarrhea ............................................................................. 81Figure 36: Available stocks of ORS, Zinc, CHX and paracetamol at present ............................................... 82

8
Acknowledgement It is a great pleasure for Nepal Development Research Institute (NDRI) to accomplish
this research in collaboration with the WHO and Child Health Division/Nepal. We thank
WHO for entrusting NDRI and making congenial environment for this research work.
It's immense pleasure to acknowledge the representatives of Nepal Government's
agencies particularly Dr. Rajendra Pant, Director, Child Health Division; Mr. Parsuram
Shrestha, CB-IMNCI Head; Mr. Deepak Jha, Child Health Division, Department of Health
services and the representatives of WHO particularly Dr. Meera Thapa Upadhaya,
National Professional Officer, Dr. Chahana Singh (UNICEF) for their invaluable
cooperation into various ways; valuable inputs in the inception phase of project,
contribution in training to field researchers, arranging the district health facilities for
their cooperation, and providing suggestions for improvement.
NDRI highly appreciates Mr. Bharat Ban –National Program Manager (Save the Children)
and Mr. Deepak Joshi (Save the Children) for their kind cooperation in designing
research tools, their valuable inputs in data analysis and finally in shaping this report.
NDRI offers gratitude to the entire research team: Mr. Bhim Prasad Shrestha, Team
Leader; Dr. Nisha Manandhar Kunwar, Consultant Expert; Dr. Pranil Man Singh Pradhan,
Consultant Expert; Ms. Usha Singh, Research Associate; Ms. Kristina Parajuli, Research
Associate for their hard work from the inception period to project accomplishment.
With great appreciation, I would particularly like to acknowledge the contribution of all
our field supervisors and enumerators; without their contribution this study would not
have been accomplished. Active contribution of Mr. Rajendra Khatri for entire
administrative and financial management incurred to this project is acknowledged as
well.

9
We would also like to extent our sincere thanks to all DHO/DPHO in relevant districts
for their valuable co-operations. Last but not the least, we would also like to thank all
the respondent service recipients for providing the information regarding the service
qualities during the exit interview, the in-charge and staffs of relevant Primary Health
Care Center, health posts and the Female Community Health Volunteers for providing
information and their cooperation during questionnaire survey.
……………………………
Dr. Jaya Kumar Gurung Executive Director Nepal Development Research Institute (NDRI)

10
Acronyms AHW Auxiliary Health Worker
ARI Acute Respiratory Infection
ANM Auxiliary Nurse Midwife
BCC Behavior Change Communication
CB-IMCI Community Based Integrated Management of Childhood Illness
CB-IMNCI Community Based Integrated Management of Neonatal and Childhood
Illness
CB-NCP Community Based Newborn Care Package
CDR Central Development Region
DHO District Health Office
DPHO District Public Health Office
EDR Eastern Development Region
FCHV Female Community Health Volunteer
FWDR Far Western Development Region
HA Health Assistant
HF Health Facility
HMIS Health Management and Information System
HP Health Post
HSP Health Service Provider
ICD International Classification of Disease

11
IEC Information, Education and Communication
IM Intra Muscular
LMIS Logistic Management Information System
MNH Maternal and Neonatal Health
MWDR Mid-Western Development Region
NDHS Nepal Demographic and Health Survey
OPD Out Patient Department
ORS Oral Rehydration Solution
PHCC Primary Health Care Center
PNC Post Natal Care
PSBI Possible Severe Bacterial Infection
SBCC Social and Behavior Change Communication
SBA Skilled Birth Attendant
SN Staff Nurse
WDR Western Development Region

12
Executive summary Community Based Integrated Management of Neonatal and Childhood Illness (CB-
IMNCI) program is comprised of both newborn and child survival interventions and
includes essential newborn care, counseling on breastfeeding and newborn
complications as well as treatment of Possible Severe Bacterial Infection (PSBI) at health
post (HP) and primary health care centre (PHCC). According to the Annual Report
2071/72, CB-IMNCI program has been implemented in 30 districts in the fiscal year
2071/72 (2014/15) and in 28 districts in the fiscal year 2072/73 (2015/16). This
assessment program was conducted to identify the gaps in the services, draw lessons
and bring necessary modifications in the CB-IMNCI program (phases) before it is scaled
up. The objectives of the assessment are to assess situation of service readiness in the
health facilities for IMNCI services particularly focusing on sick young infants;assess
knowledge and skills of service providers for management of sick young infants;
assess volume of service provided to sick young infants and children aged 2-59
months in the last 3 months and explore reasons for low or no service offered by
health facilities and reasons for reluctant to service delivery and explore quality of
service provided to the clients in terms of prescription of appropriate drugs,
appropriate dosing, follow-up visits by clients, referral, clients compliance etc.
The assessment adopted mix method approach; both primary qualitative and
secondary which was carried out in six districts. Districts were selected purposively on
the basis of ecological region, Community Based Newborn Care Package (CB-NCP) Vs
non CB-NCP districts, CB-IMNCI implementation year, PSBI performance and diversity
of partners. The sampling units were district focal person, HSPs, SBA, FCHV and

13
mothers/ caretakers of sick young infants. Structured and semi-structured
questionnaire and observation checklist were used as data collection tools.
The findings revealed mismatch between recording and reporting of PSBI, ARI/
Pneumonia, Diarrhea, use of cotrim, amoxicillin, gentamycin, oral rehydratation
solution (ORS) and zinc distribution. Similarly, this study also found discrepancy in
knowledge of healths service providers and their practice in recording and reporting.
Out of 68 health workers interviewed, it was found that 64.7% had actually received
training on CB-IMNCI. In addition, the findings also showed that only 30.6% of total 72
female community health volunteers (FCHVs) had received training on CB-IMNCI. The
result of this study showed that only 9 health facilities treated 15 PSBI cases in last 3
months. About 48% service providers reported the reason for not providing services
was mothers/ caretakers prefer to take their newborns to private clinics.
More than 30% of health facilities experienced stock out in last 3 months for essential
CB-IMNCI drugs. Similarly, more than 20% of health facilities did not have Inj.
gentamycin and antibiotics (cotrim P and Amoxicillin). The mothers/ care takers follow
up interview revealed that about 14% had to wait for 30 minutes or more to get access
to health service after reaching the health facilities. Nearly, 20% of the mothers/
caretakers reported that their child’s weight was no taken. There was 82.8%
improvement in the sick child after treatment whereas out of the remaining, 6.9%
consulted private medical shop.
The findings suggested that there is requirement of CB-IMNCI training among the
service providers, health workers and FCHVs. There is a need of logistic strengthening
and improvement in the essential drugs supply chain. And for recording and reporting

14
of different cases/ use of essential CB-IMNCI drugs, the health workers should give
attention on proper recording and reporting practice.

15
1 Introduction
1.1 Background The revised CB-IMNCI program was first introduced in Rasuwa, Nuwakot and
Nawalparasi districts in late 2014 with all the training delivered in a single phase i.e.
HF and community level training done typically over a period of less than 6 months.
Unlike Community Based Integrated Management of Childhood Illness (CB-IMCI) and
CB-NCP programs where implementation was done at a single phase, in CB-IMNCI, it is
implemented in three phase. The first phase consists of situation analysis, district
planning and trainings to selected health workers, orientations (remaining Health
workers, Dhami/Jhakri, mothers group etc.), community level trainings, onsite
coaching and implementation of Social and Behavior Change Communication (SBCC)
activities. The second phase consists of training of remaining health workers, reviews,
onsite coaching and monitoring and the third phase consist of review of activities
carried out in previous two phases.
With the phase wise approach, within one year, program has been introduced in 30
districts, with all phases completed including up to community level in 15 districts.
CB-IMNCI program is comprised of both newborn and child survival interventions and
includes essential newborn care, counseling on breastfeeding and newborn
complications as well as treatment of PSBI at HP and PHCC.
From Nepal Demographic and Health Survey (NDHS) 2011, only 25% of infants under
12 months of age with symptoms of fever or cough over the preceding 2 weeks had
been taken nowhere outside the home for treatment . Health Management Information
System (HMIS) data for the recently available year found 12,000 in-patients admissions

16
of newborns; two third of these cases were reported as being for possible sepsis and
an additional 5% of pneumonia, yielding a total of about 8,500 admitted cases of PSBI.
Still there remain important gaps on the proportions of cases of PSBI getting treatment
when they’re already at death’s door and proportions receiving safe and effective
treatment. It is to find the segment of population where effective coverage is markedly
lower. To what extent are drug and dosages accurately determined based on weight
and how adequate is the follow-up in more remote communities. The specific barriers
that families are encountering which prevent receipt of timely and appropriate
treatment still remains as a big gap for health service delivery.
1.2 Rationale and Objective of the Study This assessment program was conducted to identify the gaps in the service, draw
lessons and bring necessary modifications in the CB-IMNCI program (phases) before it
is scaled up. The assessment determined the current status with regard to
management of cases of child and newborn at PHCC, HP and community levels,
considering level of utilization and quality, and factors influencing utilization and
quality, focusing primarily on ARI, diarrhea and young infants PSBI. Moreover, the
specific objectives of the assessment are as follows.
1. Assess situation of service readiness in the health facilities for IMNCI services
particularly focusing on sick young infants (availability of trained human
resource in IMNCI, drugs and syringe, guidelines, recording and reporting tools
etc.)
2. Assess knowledge and skills of service providers for management of sick
young infants (e.g. recognition of danger signs, method of assessment,
treatment protocol, confidence, referral etc.)

17
3. Assess volume of service provided to sick young infants and children aged 2-
59 months in the last 3 months and explore reasons for low or no service
offered by health facilities and reasons for reluctant to service delivery.
4. Explore quality of service provided to the clients in terms of prescription of
appropriate drugs, appropriate dosing, follow-up visits by clients, referral,
clients compliance etc.
1.3 Methodology The assessment adopted mix method approach; both primary qualitative and
secondary quantitative data was collected. In addition review of secondary data from
HMIS and Logistic Management Information System (LMIS) was done. Methods of data
collection included document review, observation of records and store and in-depth
interviews with health service providers and mothers.
1.3.1 Sample design and sample selection
District Selection
Nepal is divided into into three ecological zones namely Mountain, Hill and Terai and
these ecological zones are further divided into five development regions namely
Eastern Development Region (EDR), Central Development Region (CDR), Western
Development Region (WDR), Mid-Western Development Region (MWDR) and Far
Western Development Region (FWDR). For nationwide representation, two districts from
each ecological zone were selected. Similarly, other criteria such as CB-NCP Vs non
CB-NCP districts, CB-IMNCI implementation year, PSBI performance and diversity of
partners were taken into consideration while selecting districts. The list of selected
18
districts based on aforementioned criteria is shown in Annex 1. The PSBI performance
was calculated by using formula
Percentage of PSBI performance= x 100
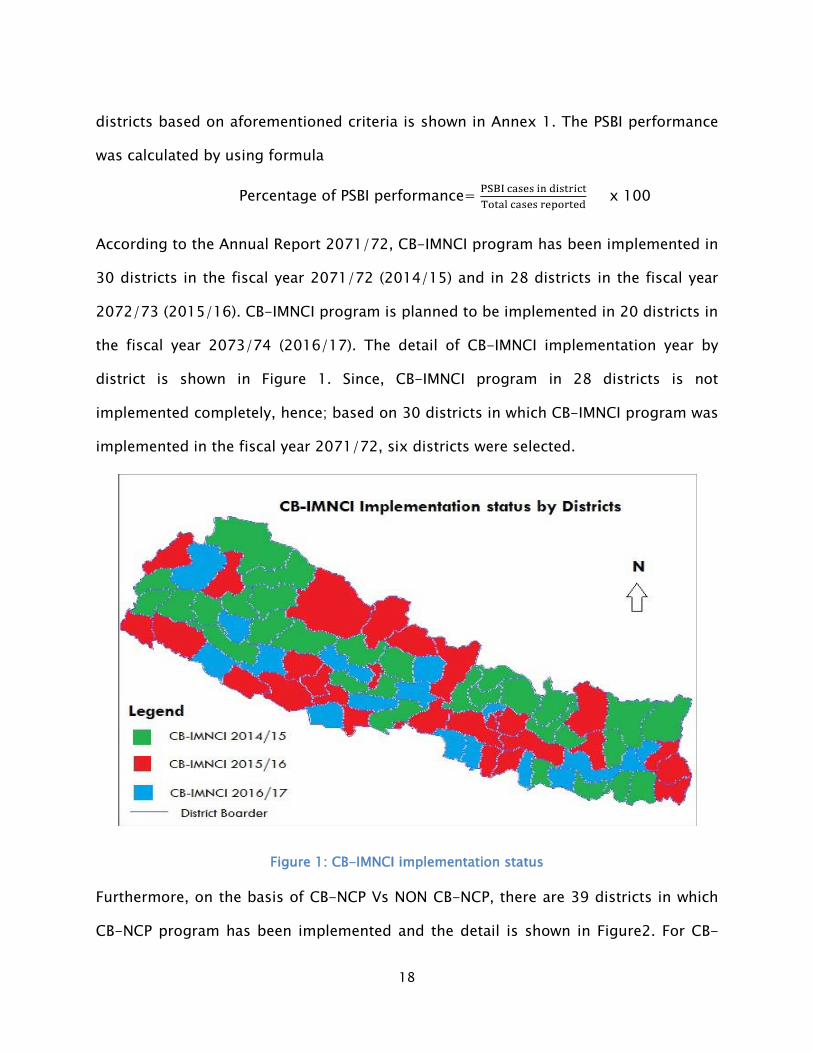
According to the Annual Report 2071/72, CB-IMNCI program has been implemented in
30 districts in the fiscal year 2071/72 (2014/15) and in 28 districts in the fiscal year
2072/73 (2015/16). CB-IMNCI program is planned to be implemented in 20 districts in
the fiscal year 2073/74 (2016/17). The detail of CB-IMNCI implementation year by
district is shown in Figure 1. Since, CB-IMNCI program in 28 districts is not
implemented completely, hence; based on 30 districts in which CB-IMNCI program was
implemented in the fiscal year 2071/72, six districts were selected.
Figure 1: CB-IMNCI implementation status
Furthermore, on the basis of CB-NCP Vs NON CB-NCP, there are 39 districts in which
CB-NCP program has been implemented and the detail is shown in Figure2. For CB-

19
IMNCI implementation approach, CB-IMNCI program was first implemented in Rasuwa,
Nuwakot and Nawalparasi districts as shown in Figure 2.
Figure 2: CB-NCP disrtict and CB-IMNCI implementation approach
Therefore, considering criteria as mentioned above, six districts namely Taplejung and
Sindhupalchowk from Mountain region, Syangja and Baitadi from Hill region and
Saptari and Nawalparasi from Terai region were selected and is illustrated in Figure 3.

20
Figure 3: District selection in Ecological region
Selection of Health Facilities
On the basis of ToR, health facilities were selected in this study. For the selection of
health facilities, at first interview with each selected district's focal person on CB-IMNCI
or MNH was conducted. Likewise, review of HMIS 9.2 and consultation with statistician
of District Public Health Office (DPHO) or DHO (District Health Office) was carried out
for ruling out less or no PSBI cases in the health facilities distance of the health
facilities, presence of private providers and type of health facilities. The detail of
selection criteria is displayed in Figure 4. Based on the criteria shown, six health
facilities (five health posts and one PHCC) from each sampled districts were selected.

21
Selection of Health Service Providers and FCHVs
Two HSPs: Health Facility (HF) In-charge and Skilled Birth Attendant (SBA) who were
involved in providing CB-IMNCI services from each HF will be interviewed resulting into
72 health workers. For selection of FCHV, two FCHVs (one living near to the HF and one
living far from the HF) were interviewed from each sampled health facilities.
Selection of mother or carter takers of children
For follow up and exit interview, two mothers whose young infants had been sick in
last three months and received services from the sampled health facilities were
interviewed.
Sample Size
Health Facilities were visited on the basis of certain criteria, stated above. In each HF,
HF survey was conducted along with interviews of two service providers (HF in charge
and SBA). Similarly, two FCHVs were interviewed. In the same way, two follow up cases
Figure 4 : Sample Selection Techniques
Less or No PSBI service provided
Interview with District Focal
Person
6 Health Facilities in
Each District Remoteness
Presence of Private Provider
Type of Health Facilities

22
(0-6 months) two exit interviews were conducted. So, a total of 324 (interviews and
Survey) were conducted. The details are provided in Table1.
Table 1: Sample size of the study
Sample size
Ecological Zone
Districts
Health
Facilities
(Selected)
HF Surve
y / Obser
v.
HS Provide
r Interview/SB
A
FCHV Intervie
w
Client F/U
visits
Exit intervi
ew
Total
Mountain
Taplejung 6 6 12 12 12 12 54 Sindhupalchowk
6 6 12 12 12 12 54
Hills Syangja 6 6 12 12 12 12 54 Baitadi 6 6 12 12 12 12 54
Terai Nawalparasi 6 6 12 12 12 12 54 Saptari 6 6 12 12 12 12 54
Total 36 36 72 72 72 72 324
1.5 Data Collection Both qualitative and quantitative methods i.e. mixed method was approached for data
collection. A semi structured questionnaire was drafted for data collection on the basis
of objectives stated.
HF Assessment (Quantitative and Observation)
For this, a close observation of health facilities including its store was conducted. Apart
from this, availability of commodities such as drugs and syringe, trained human
resource in IMNCI, guidelines, recording and reporting tools were closely monitored. In
addition, the stocks of drugs responsible for treatment of ARI, Diarrhea, Pneumonia

23
and PSBI were closely observed. Availability and expiry dates of drugs such as
Cotrimoxazole, Amoxicillin, Gentamycin, Vitamin A capsule, Ampicillin, Ciprofloxacin,
Chlorhexidine, IV fluids, Zinc and ORS were closely observed. Needles and Syringes
were also checked for its availability and expiry date. For recording and reporting,
CBIMCI register, general OPD register, MRN were reviewed and HMIS 9.2 at the HF level.
The uppermost priority was given to the recording of PSBI cases in young infants as
they are the major cause for other secondary infections. And if such cases were not
recorded then the HSP were further asked to clarify for non-availability of such clients.
Interview with HSPs
HSPs included interview with HF In charge and SBA. They were interviewed about the
training received by them either pre-service or in-service. They will be interviewed for
assessing knowledge on CB-IMNCI program especially focusing on diseases like
pneumonia/ ARI, Diarrhea, and PSBI and difficulties faced by health workers while
diagnosing, treatment and referral of aforementioned diseases.
Interviews with FCHVs
Female Community Health Volunteers (FCHVs) were interviewed on the basis of
following checklists:
i. To what extent are they still involved in ARI or diarrhea treatment?
ii. How are severe cases managed?
iii. Is there provision of referral cases? If yes, what types of arrangements are
conducted?
iv. The state of availability of certain medications such as ORS, zinc and so on.
v. Degree of Stock out

24
vi. Lag in service due to distance
vii. Involvement in training (pre-service or in-service) if any
viii. State of increased demand corresponding to less service delivery.
Exit Interviews and Follow-up visits Interviews
Exit Interviews were conducted with at least two mother/care-takers of clients who had
visited HF for IMNCI services (only from ARI, pneumonia, diarrhea and PSBI) Mothers/
caretakers were asked details about the index child such as date of birth, details about
the birth of the child, what the newborn was fed and how it was cared for and details
of the child’s sickness. Details about interventions at home and subsequent visits to
health facilities were also collected.
While conducting In Depth Interviews with mother/care takers of sick young infants
following checklist was prepared:
i. Clients’ perception regarding the quality of service provided.
ii. Clients view regarding their degree of satisfaction in terms of behavior of
HSPs and their duration of treatment on the basis of disease incubation
period
iii. Clients’ perception regarding prescription and dosing of appropriate drugs by
the HSP.
iv. The process of referral system in the facility.
v. The Level of Compliance in clients.
vi. Follow up visits by clients

25
In case of Follow up Visits of clients, the quality of service provided by the HSP was
closely observed. For this, two young infants (0-6 months) who had been sick in the
last three months and had obtained services from the HF were followed up.
Recruit and train field staff enumerators and data entry
All the selected 12 enumerators were trained before commencing data collection.
Three days training starting from 21st – 23rd December, was carried out in three
sessions. The training focused on familiarizing filed staffs on brief description of
project, objectives of the study, study design, sampling strategy, data collection and
quality procedures and research ethics to be strictly followed by field staffs. In addition
to the classroom training, field practice and mock interviews were conducted to gain
familiarity with the questionnaires and experience in interviewing. Along with training
on the questionnaires, the field staffs were also made familiar about their survey
districts and respective health facilities. The resource people involved in the training
and the detailed schedule of the training session is provided in the Annex.
Pilot Survey
The pre-test of the survey was conducted on 26th December, 2016. In this pre-testing
session all the trained enumerators and group leaders participated. Two groups were
made (six enumerators in each group) and pre-testing was conducted in health
facilities and community level (FCHV and mother) of Nuwakot district. After the pre-
testing, all the field staffs including group leaders were gathered for the discussion of
confusions and problems encountered in the field. The problems occurred during pre-
testing were addressed by technical experts. The results of the pilot survey were used
to further refine the questionnaire and pre-empt pitfalls during the survey process.

26
Finalization of the Survey Questionnaire
The draft questionnaire which was prepared was further refined by incorporating all
problems and feedbacks from the training session and also from findings during pre-
testing. The final version of the survey questionnaire was translated in Nepali language
and is provided in Annex 4.
Mobilization of the field staffs
A total of 12 field enumerators were deployed to the field. In each district, two field
enumerators were mobilized. The number of health facilities to be surveyed and
number of FCHVs and mothers to be interviewed by each enumerator and districts
allocated to them were designed and provided to each of them before deploying them
to the field as shown in Annex 2. Further, field staffs were provided letter from Child
Health Divison (CHD) to facilitate data collection from the health facilities.
1.6 Data Analysis and Presentation Data processing was done in three phases namely data entry program development,
data entry and data cleaning. The following process was carried out for overall data
management:
Development of coding system
A scientific coding system was developed using alphabets and numbers denoting
questionnaire IDs, ecological region, districts, and type of health facilities of survey.
Selection of software, data masking and data entry
SPSS was used for the data entry. In case of data masking, all the variables used in the
questionnaire was properly labeled along with the corresponding value codes in
English and entered in the SPSS database. During the data entry process, strict data

27
quality control procedures, codes and checks were undertaken. For example, a feature
in data validation called data entry to a whole number within limits was used to define
restrictions on what data should be entered in a cell. This prevented the users from
entering invalid data. The data validation also allowed input messages to define what
input we expect for the cell, and instructions to help data entry operators correct any
errors. Also, random re-checking of data entered with the field data was carried out.
Data cleaning and reporting
Two sources of detectable errors i.e. data entry errors (such as mistyping responses,
entering data out of range or leaving an answer blank when a valid response was
included) and enumerator errors (such as failing to accurately follow a skip pattern,
writing a response that is difficult to interpret or providing false answers) were both
considered while cleaning the data. The SPSS Descriptive was used to run an initial
check on the data to show the minimum and maximum values for each variable in the
file such that data entered out of range could be easily seen. For checking the data
errors in skip patterns, a few SPSS syntax was written. For this a new variable was
created and a logical statement was provided to identify cases violating the skip
patterns. From here we were able to identify the case ID of each violating case and go
back to the questionnaire and fix the problem.
Data analysis
As per requirements, some intervening variables were developed for cross-tabulations.
The cross-tabulations were done to examine the relationship between two variables.
While doing cross tabulations independent and dependent variables was identified and
percentage values and observed values (frequency) was calculated for each category of
the independent variable. For multiple response data, where the respondents can

28
choose or provide more than one response, multiple response analysis was done. The
multiple responses was organized in multiple dichotomy (i.e. 1=yes and 2= no). The
multiple responses were defined for all questions where multiple responses were
expected. Then the crosstab option was used to obtain frequencies or percentages
according to number of respondents/responses. (The syntax used is: Analyze -
multiple responses - define variable sets. Create the sets. Then going back to the
command: Analyze -multiple responses - frequencies or crosstabs). The analyzed data
was presented into tabular and graphical forms while drafting the report.
1.7 Limitation of the Study The research tool along with the sample designing for this survey has been revised
several times such that the output/ findings from the survey could be representative.
However, the research contains some limitations which were out of control.
• The total interviews for the assessment were taken from the six districts which
may be a small sample for the representation nationwide.
• Purposive sampling method for the selection of the service provider,
mothers/caretakers is used which itself is a limitation in the study.
• The proposed categorization of the age group <2 months and 2-59 months for
data collection of the PBSI, Diarrhea and ARI/Pneumonia could not be met
during the health facility interview (exit and follow up) due to unavailability of
cases.
• The data for the mother/ caretakers interview could be biased as they were truly
based on the perceptions of the mothers/caretakers which may a limitation of
the study.

29
• In Baitadi and Saptari were first phase implementation districts for CB-IMNCI.
Therefore, all the health workers in the helath facilities and FCHVs of these
districts were not trained in the CB-IMNCI.
• This study is limited to three diseases namely PSBI, ARI/ Pneumonia and
Diarrhea.

30
2 Survey Findings
1. Survey Findings for District Focal Person In the selected 6 districts, the first contact was made with the district focal person. An
interview was taken with the CB-IMNCI focal person in the District Health Office
/District Public Health Office of the 6 selected districts. Among which, 1 DPHO and 5
DHOs were visited in the six districts.
The focal persons were asked whether they received medicine and commodities as per
the district demand on time. Out of the 6, half of them answered yes and among them,
only 2 (33.3%) were positive that it was enough to cover the daily services in all the
health facilities within the district. They further said that they supply the medicines and
commodities to the peripheral health facilities on demand (66.7%) and on quarterly
basis (33.3%).
All the 6 focal persons said that there was regular staff meeting held in the district
office and 5 of them (83.3%) said that they discuss the issues of CB-IMNCI in the
meetings. Half of them answered that they received supervision visits from the higher
level focusing in the CB-IMNCI program whereas all 6 focal persons said that went for
the supervision visit to the peripheral health institutions (PHCC and HP). There were
Health Facility Operation and Management Committee (HFOMC) present in all the HF.
There were 100% availability of the HMIS tools/forms and formats for supplying the
health facilities whereas 5 out of 6 replied that they have the HMIS user manuals
available. All the staffs involved in CB-IMNCI were oriented in HMIS tools and 5 out of 6
had timely reporting from the HFs.
31
The focal persons were asked about the activities they carried out for strengthening
the CB-IMNCI program. They responded with various answers.
“ANM-training on CB-IMNCI is given first priority. Birthing center has now been
upgraded and improved. FCHV have the duty to refer child of under 5 to HF. And
school education on childhood diseases has been provided. These are the activities
being done.”
“Basic training and refresher training are needed here but there is need for more
budget. For now, we review of indicator and do analysis (quarterly and annually) and
also conduct meeting in HP every month”
“We are doing joint monitoring and onsite coaching of the staffs for filling the register.
The reports that we receive are checked and then we give feedback to the health
facilities. Training are also being given for management of emergency condition of the
children.”
While asking how they monitored the CB-IMNCI program, they said they focused on
recording, correcting the weakness seen in recording, give feedback and provide
supervision on medicines and other equipments. The monitoring sheets for the
diseases are supervised and feedback is given and reviewing the register and going for
observation of the HSP. They also focused on strengthening the reporting system as
reporting is weak and also have meetings with FCHVs to get ideas about the referral
cases.
Evaluation of the CB-IMNCI program were being done through HMIS register and report
analysis, see how records were kept and updated, getting feedbacks from the annual
register and keep a check on percentage of neonatal death and infant mortality.

32
The reasons for less/no reporting of the PSBI cases among young infants in last 3
months from the health facilities as explained by the focal persons were that the PSBI
cases usually go to the private or the higher HF other than the PHCCs. There is lack of
trained man power in the CB-IMNCI in the health posts, so no PSBI cases are seen there
and parents prefer to take their child to private centers in emergency.
According to the focal persons, the major priority issues for service availability and
quality of CB-IMNCI program could be providing basic training and refresher training
more frequently, availability of equipments and essential drugs with timely monitoring
and supervision. Proper allocation of the budget and review workshops needed to be
organized with review meetings every trimester and quarterly. They suggested fulfilled
staffs with improve logistic supply and requirement of special trainings for the focal
person.

33
2. Survey Findings for HF Interview A total of 36 health facilities, 6 from each selected districts were included in this study.
Out of 36 health facilities, 29 (81%) of health facilities were health posts and 7 (19%) of
health facilities were PHCC. Details of health facilities in each district are shown in
Table 2.
Table 2: Types of Health faciliies in each study districts
Type of HF
Name of the District
Total Taplejung Sindhupal
chowk Syangja Baitadi Saptari Nawalprasi PHC 1 2 1 1 1 1 7 (19.4%) HP 5 4 5 5 5 5 29 (80.6%)
Total 6 6 6 6 6 6 36 (100%)
2.1 Availability of service readiness in the HF Human resources
The findings revealed that more than 30% of staffs working in the health facilities were
auxiliary nurse midwife (ANM) followed by auxiliary health worker (AHW) which
accounted for 27.3%. However, only 3.4% of staffs were staff nurse. About 26.1% of
staffs working in the HF come under other category which included doctor, health
assistant, administrative officer, lab assistant and peon. The reason for greater number
of ANM and AHW working in the health facilities than doctors is because more than
80% of health facilities chosen in this study were HPs.
Training and provision of CB-IMNCI services in the health facilities
The number of staffs receiving CB-IMNCI and CB-IMCI were nearly equal to 24%.
However, only 61 (16%) staffs received training on CB-NCP. Even though, only 93
34
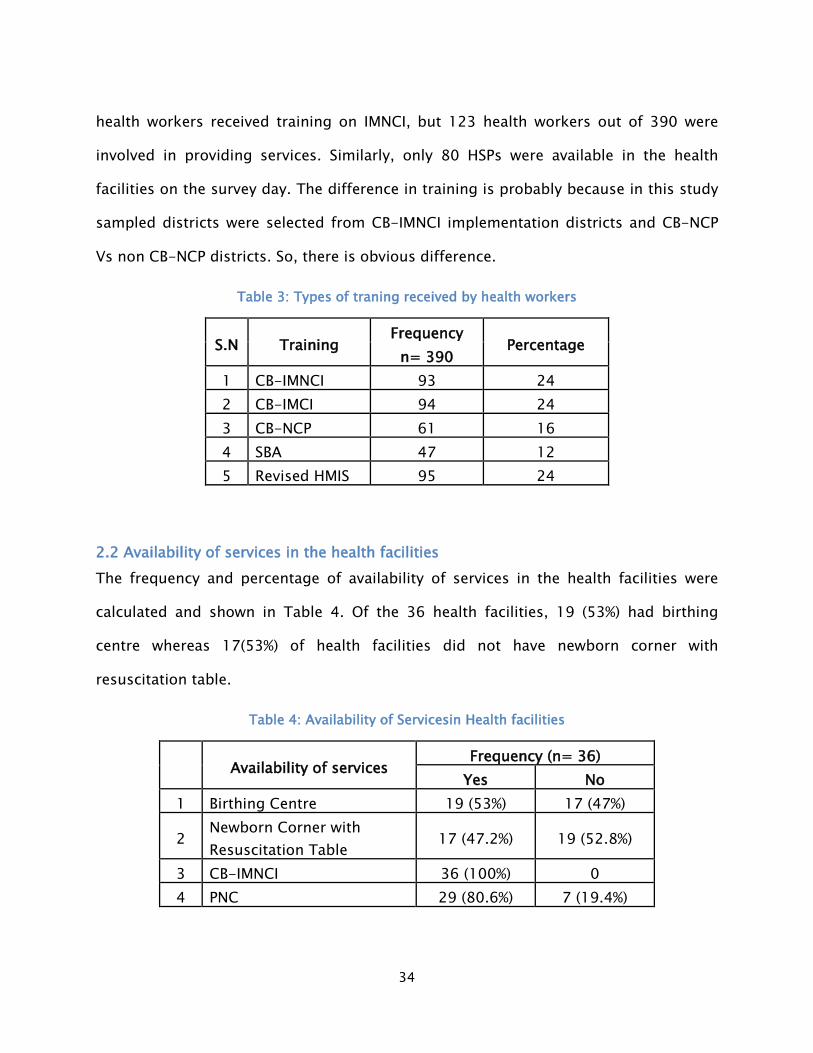
health workers received training on IMNCI, but 123 health workers out of 390 were
involved in providing services. Similarly, only 80 HSPs were available in the health
facilities on the survey day. The difference in training is probably because in this study
sampled districts were selected from CB-IMNCI implementation districts and CB-NCP
Vs non CB-NCP districts. So, there is obvious difference.
Table 3: Types of traning received by health workers
S.N Training Frequency
Percentage n= 390
1 CB-IMNCI 93 24 2 CB-IMCI 94 24 3 CB-NCP 61 16 4 SBA 47 12 5 Revised HMIS 95 24
2.2 Availability of services in the health facilities The frequency and percentage of availability of services in the health facilities were
calculated and shown in Table 4. Of the 36 health facilities, 19 (53%) had birthing
centre whereas 17(53%) of health facilities did not have newborn corner with
resuscitation table.
Table 4: Availability of Servicesin Health facilities
Availability of services
Frequency (n= 36) Yes No
1 Birthing Centre 19 (53%) 17 (47%)
2 Newborn Corner with Resuscitation Table
17 (47.2%) 19 (52.8%)
3 CB-IMNCI 36 (100%) 0 4 PNC 29 (80.6%) 7 (19.4%)

35
2.3 Availability of equipments Health facilities were visited for the availability and proper functioning of equipments.
The list of equipments which were observed in the health facilities are illustrated in
Table 5. It is seen that equipments such as BP instruments, stethoscope and
penguin/delee Suction were available in the all the birthing centres. More than 80%
percent of the bithing centres contained equipments like salter scale, pan scale ARI
timer and neborn bag and mask. However, 5 (30%) non birthing centres did not contain
ARI timer.
Table 5: Availability of equipments
Avaialbility of equipments
Birthing Centre (n1= 19) Non Birthing Centre (n2= 17) Yes,
Functioning Yes, Not
Functioning No Yes,
Functioning Yes, Not
Functioning No
Salter Scale 16 (84%) 0 3
(16%) 6 (35%) 1 (6%) 10
(59%)
Pan Scale 16 (84%) 1 (5%) 2
(11%) 8 (47%) 0 9
(53%) Mercury Thermometer 11 (58%) 2 (10%)
6 (32%) 8 (47%) 0
9 (53%)
Digital Thermometer 18 (95%) 1 (5%) 0 12(70%) 1 (6%)
4 (24%)
Sthethoscope 19 (100%) 0 0 17 (100%) 0 0 BP Instrument 19 (100%) 0 0 17 (100%) 0 0
ARI Timer 17 (90%) 1 (5%) 1
(5%) 12(70%) 4 (24%) 1 (6%) Penguin/Delee Suction 19 (100%) 0 0 3 (18%) 0
14 (82%)
Newborn Bag and Mask 18 (95%) 0
1 (5%) 4 (24%) 0
13 (76%)

36
2.4 Availability of drugs and commodities From the Table 6, it is found that more than 30% of health facilities experienced stock
out for the antibiotics (cotrimP and Amoxicillin) (38.9%), paracetamol 500mg (33.3%)
and injection gentamycin (30.6%). Similarly, more than 20 % of health facilities did not
have Inj. gentamycin (27.8%) and antibiotics (22.2%). Eventhough, the questionnaire
did not mention about medicines in syrup but this study found that many health
facilities lack syrup paracetamol.
Table 6: Availaability of CB-IMNCI Drugs in health facilities
Availability of medicines/
commodities
Current status(n= 36) Stock out in last 3
months (n=36) Yes less than 1 month
Yes, for 1 month No Yes No
ORS Packets 3 (8.3) 32 (88.9) 1 (2.8) 6 (16.7) 30 (83.3)
Antibiotics 8 (19.4) 21 (58.3) 7 (22.3) 14 (38.9) 22 (61.1) Vitamin A Capsule 4 (11.1) 32 (88.9) 0 3 (8.3) 33 (91.7) Albendazole 400mg 7 (19.4) 28 (77.8) 1 (2.8) 6 (16.7) 30 (83.3) Paracetamol 500mg 8 (19.4) 22 (61.1) 6 (16.7) 12 (33.3) 24 (66.7) Gentamycin Injection 2 (5.6) 24 (66.7) 10 (27.8) 11 (30.6) 25 (69.4) Zinc Tablet 3 (8.3) 24 (66.7) 9 (25) 8 (22.2) 28 (77.8) Chlorhexidine gel 3 (8.3) 29 (80.6) 4 (11.1) 7 (19.4) 29 (80.6)
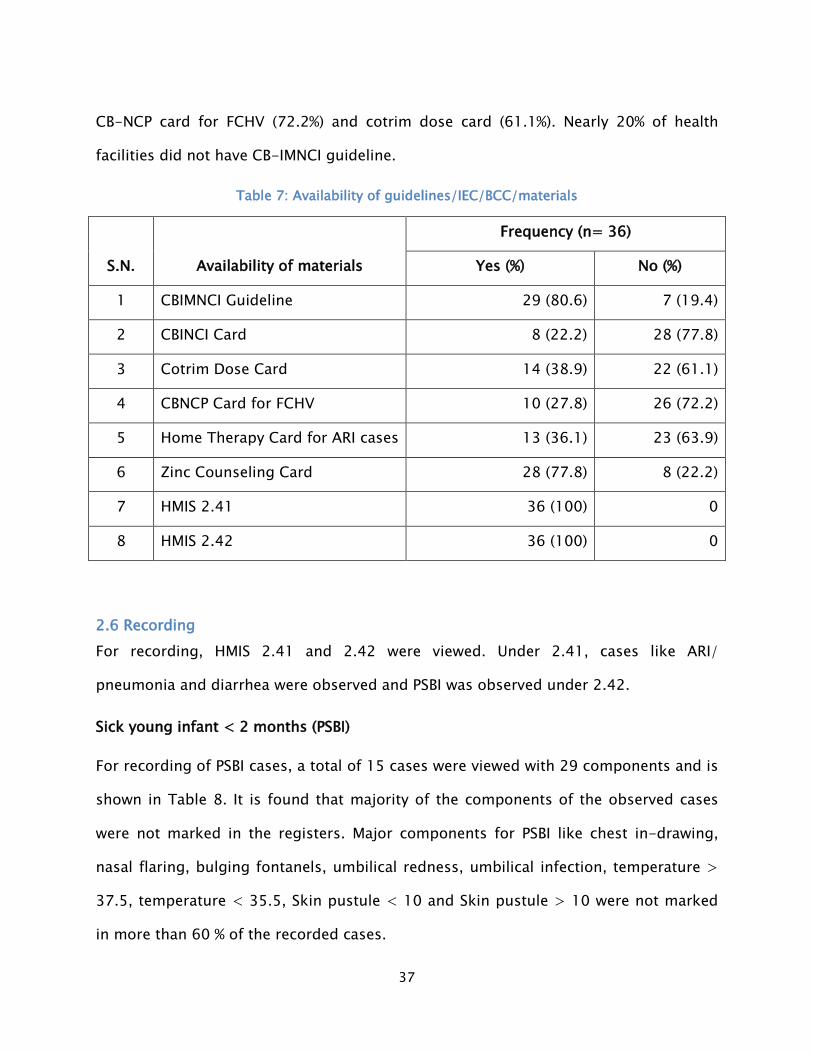
2.5 Availability of guidelines/IEC/BCC materials Table 7 shows the availability of materials and guidelines in the health facilities. From
the table it is seen that all the health facilities contained HMIS 2.41 and HMIS 2.42
registers. About 28 (77.8%) of health facilities did not contain CB-IMCI card followed by
37
CB-NCP card for FCHV (72.2%) and cotrim dose card (61.1%). Nearly 20% of health
facilities did not have CB-IMNCI guideline.
Table 7: Availability of guidelines/IEC/BCC/materials
S.N. Availability of materials
Frequency (n= 36)
Yes (%) No (%)
1 CBIMNCI Guideline 29 (80.6) 7 (19.4)
2 CBINCI Card 8 (22.2) 28 (77.8)
3 Cotrim Dose Card 14 (38.9) 22 (61.1)
4 CBNCP Card for FCHV 10 (27.8) 26 (72.2)
5 Home Therapy Card for ARI cases 13 (36.1) 23 (63.9)
6 Zinc Counseling Card 28 (77.8) 8 (22.2)
7 HMIS 2.41 36 (100) 0
8 HMIS 2.42 36 (100) 0
2.6 Recording For recording, HMIS 2.41 and 2.42 were viewed. Under 2.41, cases like ARI/
pneumonia and diarrhea were observed and PSBI was observed under 2.42.
Sick young infant < 2 months (PSBI)
For recording of PSBI cases, a total of 15 cases were viewed with 29 components and is
shown in Table 8. It is found that majority of the components of the observed cases
were not marked in the registers. Major components for PSBI like chest in-drawing,
nasal flaring, bulging fontanels, umbilical redness, umbilical infection, temperature >
37.5, temperature < 35.5, Skin pustule < 10 and Skin pustule > 10 were not marked
in more than 60 % of the recorded cases.

38
Table 8: Component observed in register for PSBI cases
S.N Observed components
Frequency (n= 15)
Yes (%) No (%) 1 Ethnicity 14 (93.3) 1 (6.7) 2 Ward 12 (80) 3 (20) 3 Gender 13 (86.7) 2 (13.3) 4 Age in week 14 (93.3) 1 (6.7) 5 Weight 13 (86.7) 2 (13.3) 6 Temperature 10 (66.7) 5(33.3) 7 Referred by 15 (100) 0 8 Convulsion 3 (20) 12 (80) 9 Respiratory rate 12 (80) 3 (20) 10 Chest in-drawing 6 (40) 9 (60) 11 Nasal flaring 5(33.3) 10 (66.7) 12 Bulging fontanels 5(33.3) 10 (66.7) 13 Umbilical redness 5(33.3) 10 (66.7) 14 Umbilical infection 6 (40) 9 (60) 15 Temperature > 37.5 6 (40) 9 (60) 16 Temperature < 35.5 4 (27.7) 11(73.3) 17 Unable to feed 4 (27.7) 11(73.3) 18 Skin pustule < 10 5(33.3) 10 (66.7) 19 Skin pustule > 10 4 (27.7) 11(73.3) 20 Inactive/ unconscious 4 (27.7) 11(73.3) 21 Normal movement 5(33.3) 10 (66.7)
22 Less than normal movement 4 (27.7) 11(73.3)
23 Major classification 9 (60) 6 (40) 24 Number 3 (20) 12 (80) 25 ICD code 4 (27.7) 11(73.3) 26 Medicine 10 (66.7) 5(33.3) 27 Counseling 9 (60) 6 (40) 28 Referred to 8 (50) 8 (50) 29 Follow up 4 (27.7) 11(73.3)

39
For recording keeping, HSPs were asked where (type of register) they record PSBI cases
which were further validated by observing registers. The registers where cases had
been registered are shown in Table 9. Majority of cases were registered in IMCI register
(79.4%). 17.6% of cases were registered in IMNCI register and only 2.9% of cases were
registered in OPD register. Most of the health workers gave the reason for not
recording cases in IMNCI register was due to unavailability of IMNCI register (96.4%)
and 3.6% reported due to other reason. Out 36 health facilities, only 15 PSBI cases were
treated in last 3 months. Therefore, HSPs were asked why PSBI cases were not treated.
Most of the health workers reported due to no cases brought or reported to the HF
(94.1%) and 5.9 % reported due to lack of drugs. The reasons for not bringing to the HF
were mothers prefer to take their newborns to private clinics (47.9%), mothers do not
have confident in HF (14.6%) and others (37.5%). Others included district or zonal
hospital being near or parents take sick young infant to district or zonal hospital and
due to distance from the HF.
Table 9: Place where PSBI cases recoreded
S.N Register Frequency (n= 68) Percent 1 IMNCI register 12 17.6 2 IMCI register 54 79.4 3 OPD register 2 2.9
40
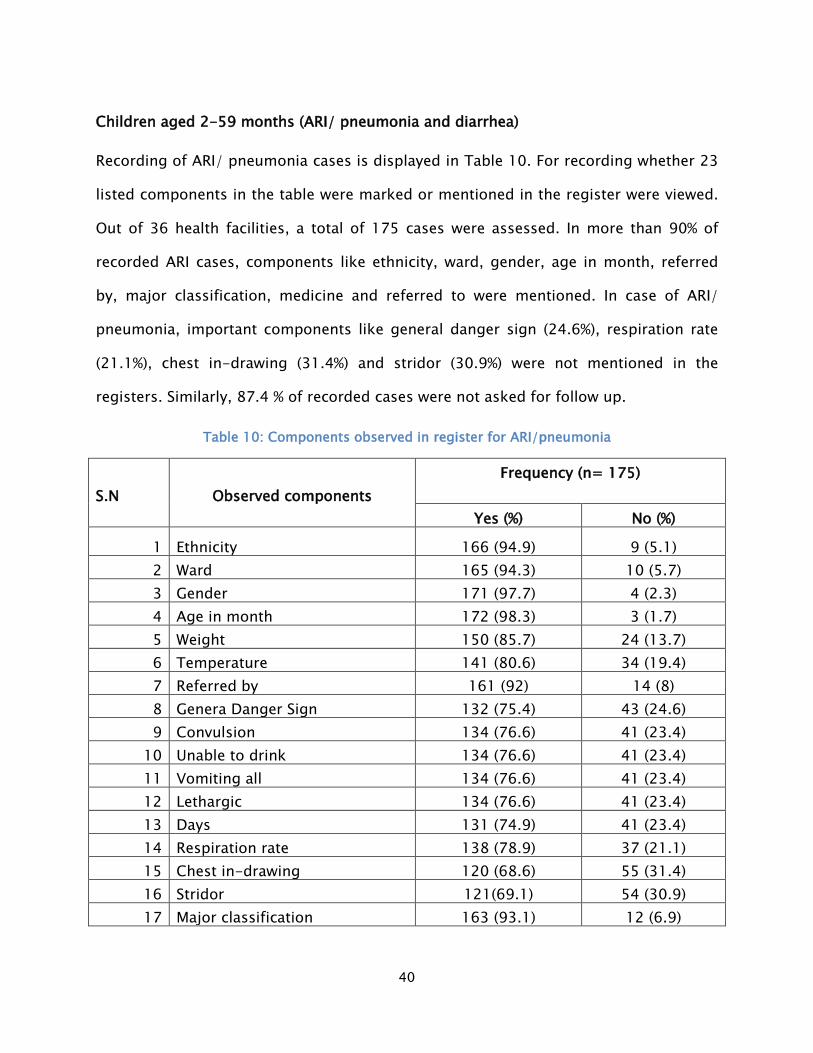
Children aged 2-59 months (ARI/ pneumonia and diarrhea)
Recording of ARI/ pneumonia cases is displayed in Table 10. For recording whether 23
listed components in the table were marked or mentioned in the register were viewed.
Out of 36 health facilities, a total of 175 cases were assessed. In more than 90% of
recorded ARI cases, components like ethnicity, ward, gender, age in month, referred
by, major classification, medicine and referred to were mentioned. In case of ARI/
pneumonia, important components like general danger sign (24.6%), respiration rate
(21.1%), chest in-drawing (31.4%) and stridor (30.9%) were not mentioned in the
registers. Similarly, 87.4 % of recorded cases were not asked for follow up.
Table 10: Components observed in register for ARI/pneumonia
S.N
Observed components
Frequency (n= 175)
Yes (%) No (%)
1 Ethnicity 166 (94.9) 9 (5.1) 2 Ward 165 (94.3) 10 (5.7) 3 Gender 171 (97.7) 4 (2.3) 4 Age in month 172 (98.3) 3 (1.7) 5 Weight 150 (85.7) 24 (13.7) 6 Temperature 141 (80.6) 34 (19.4) 7 Referred by 161 (92) 14 (8) 8 Genera Danger Sign 132 (75.4) 43 (24.6) 9 Convulsion 134 (76.6) 41 (23.4)
10 Unable to drink 134 (76.6) 41 (23.4) 11 Vomiting all 134 (76.6) 41 (23.4) 12 Lethargic 134 (76.6) 41 (23.4) 13 Days 131 (74.9) 41 (23.4) 14 Respiration rate 138 (78.9) 37 (21.1) 15 Chest in-drawing 120 (68.6) 55 (31.4) 16 Stridor 121(69.1) 54 (30.9) 17 Major classification 163 (93.1) 12 (6.9)

41
18 Number 46 (26.3) 129 (73.7) 19 ICD code 41(23.4) 134 (76.6) 20 Medicine 161 (92) 14 (8) 21 Counseling 69 (39.4) 106 (60.6) 22 Referred to 158 (90.3) 17 (9.7) 23 Follow up 22 (12.6) 153 (87.4)
In Table 11, recorded diarrhea cases are shown. For recording, a total of 169 diarrhea
cases were observed which included 24 components. From the table, it is found that
none of the components were completely mentioned in all recorded cases.
Components like general danger sign, blood, irritable, sunken eyes, cannot drink,
drinks eagerly, drinks normally, skin pinch goes slowly and skin pinch goes very slowly
were not mentioned in almost 20% of the recorded cases.
Table 11: Components observed in register for diarrhea
S.N Observed components
Frequency (n= 169)
Yes (%) No (%) 1 Ethnicity 156 (92.3) 13 (7.7) 2 Ward 154 (91.1) 15 (8.9) 3 Gender 161 (95.3) 8 (4.7) 4 Age in month 160 (94.7) 9 (5.3) 5 Weight 139 (82.2) 30 (17.8) 6 Temperature 116 (68.6) 53 (31.4) 7 Referred by 154 (91.1) 15 (8.9) 8 Days 129 (76.3) 40 (23.7) 9 General Danger Sign 135 (79.9) 34 (20.1)
10 Blood 134 (79.3) 35 (20.7) 11 Irritable 133 (78.7) 36 (21.3) 12 Sunken Eyes 135 (79.9) 34 (20.1) 13 Cannot Drink 133 (78.7) 36 (21.3) 14 Drinks eagerly 134 (79.3) 35 (20.7)

42
15 Drinks normally 137 (81.1) 32 (18.9) 16 Skin pinch goes slowly 136 (80.5) 33 (19.5) 17 Skin pinch goes very slowly 130 (76.9) 39 (23.1) 18 Major classification 148 (87.6) 21 (12.4) 19 Number 43 (25.4) 126 (74.6) 20 ICD code 34 (20.1) 135 (79.9) 21 Medicine 152 (89.9) 17 (10.1) 22 Counseling 69 (40.8) 100 (59.2) 23 Referred to 115 (68) 54 (32) 24 Follow up 26 (15.4) 143 (84.6)
For ARI/ pneumonia and diarrhea cases, 79.4 % were recorded in IMCI register, 17.6 %
were recorded in IMNCI and 2.9 % were recorded in OPD register. The reason for not
recording cases in IMNCI register was due to unavailability of IMNCI register (96.4%)
and 3.6 % reported due to other reason.
2.7 Reporting For reporting, HMIS 9.1 was reviewed. Comparison between the numbers of cases
recorded and reported in last 3 months for cases such as PSBI, ARI/Pneumonia and
diarrhea, use of cotrim, amoxicillin gentamycin first dose, gentamycin complete dose,
ORS and zinc, and was done and is shown in Table 12

43
Table 12: Reporting and recording mismatch
Mismatch No. of HF who treated cases in last 3 months
Number of cases treated
Recording and Reporting Mismatch
Record match
Under reporting
Over reporting
PSBI 9 15 5 3 1
Severe Pneumonia 6 8 2 3 1
Pneumonia 30 433 14 6 10
No Pneumonia 34 811 12 6 16
Severe dehydration 3 12 0 3 0
Some dehydration 18 52 8 3 7
No dehydration 34 324 17 6 11
Gentamycin first dose
3 3 1 1 1
Gentamycin full dose 3 3 2 0 1
Treated with ORS and Zinc
32 336 17 3 12
Treated with amoxicillin
29 455 4 17 8
Treated with cotrimoxazole
22 298 5 9 8
Sick young infant < 2 months (PSBI)
Tallying data of PSBI, mismatch in recording and reporting was found in 4 health
facilities. The reasons for mismatch were asked with service providers in depth. The
reasons were

44
“There should not have been any mistakes in the recording but as I check now, the
same single PSBI case has been reported in both 2.41 and 2.42 of the record book.
That is why, there has been 2 cases of PSBI reported. This is the reason for the
mismatch.”
“There are no PSBI cases in last three months. Here, while looking at the registered
cases, even a case of Local bacterial infection in the records has been reported as a
PSBI case.”
“Sometimes, there is no recording done. It will be mentioned in the OPD register but
we forget to mention in the record file. It is due to no sufficient staffs for the recording
and the reporting job.”
“No proper classification is done in the record files while diagnosing the cases. So it
becomes difficult for us to record and report the cases properly in the register files.”
Gentamycin first dose record mismatch
The results revealed mismatch was found in 6 cases. The reasons for mismatch were
“Many times, the parents of the sick children do not allow us to give IM injection. But
inwe do record and show it in thereporting as the DHO asks us questions why
gentamycin is not being given. So while this process, there might have been a
mismatch in the records and reports.”
“Service provider did not count properly, so there are mistakes in the register.”
“The AHW sir may not have counted properly, or else it would have been correct.”
Gentamycin full dose record mismatch

45
The results revealed that mismatch was found in 5 cases. The reasons for mismatch
were
“Marking is done in patient's prescription but not recorded in register. However, it is
mentioned in the reporting file as the complete dose has been given to the patient.
Though not recorded in the register, it is reported.”
“The AHW records all the cases of the antibiotics. He made some mistakes and
reported all the cases in amoxicillin instead.”
Children aged 2-59 months
ARI service record mismatch
From the Table 12, mismatch was found in classification of ARI/Pneumonia cases
between recorded and reported. The reasons for mismatch were asked with service
providers in depth. The reasons were
“Classification, recording and reporting are done by different staffs. Moreover, the
staffs also do not have proper knowledge and skills for the classification of the
diseases. So they do not write properly in the records and again do negligence while
reporting.”
“Most of the times I am busy, and recording and reporting are done by the other staffs
in the HF. So do not know much about this.”
“The health worker who does the recording in register is not trained and there may
also be minor counting mistakes while reporting.”

46
“There is haphazard classification of Pneumonia done in the OPD due to limited time
and more patients waiting. So there are mistakes while recording and further
reporting.”
Diarrhea service record mismatch
Tallying classification of diarrhea cases in last 3 months, mismatch was found. The
reasons for mismatch were asked with service providers in depth. The reasons were
“Usually, there is no enough time to classify the disease and record properly in IMNCI
register, so many times the cases are not recorded properly.”
“Due to no proper skills and knowledge in classifying diarrhea, it is recorded wrongly
by the another person. And further they do carelessness and counting mistakes while
reporting in the register.”
“Because of high patient flow and limited number of staffs it is difficult to record in
register at that time, and later when we record and report, there may occursome
counting mistakes”
Cotrim record mismatch
The reasons for mismatch in recording and reporting for cotrim use were asked to the
service providers and the reasons were
“We usually do not register the use of cotrim nowadays. As we are instructed not to use
cotrim, some cases might have been missed in recording the use of cotrim. “
“The over recording must have been from the Urban health centers. There is more
availability and use of cotrim which is still present in the urban health centers.”
47
“We do not have any specific person for the record keeping job. Neither anyone is
trained for the record keeping. So the mismatch may have occurred due to the lack of
trained person for recording in our HF.”
“There are not many staffs who are specified for record keeping and reporting. And
there are different staffs who record and report. The other staffs working here do not
have enough time to record in the register as the same person is looking after the
patients and the same person has to record and report.”
“The data are corrected but here the cases are wrongly reported in the register.”
“Cotrim is very commonly used therefore there might be mistake on counting.”
“Sometimes, we just happen to forget to report the cases while reporting.”
“We have limited amoxicillin here in the health post. Therefore we provide cotrim to
the needy patients but there is an order for not giving cotrim. Thus, cotrim is usually
not reported.
“Cotrim is given but not recorded, many times amoxicillin is also counted under
cotrim. That is why, there may be over reporting of the cases.”
Amoxicillin record mismatch
The results revealed that mismatch in recording and reporting was found in the health
facilities. The reasons for mismatch were
“Untrained person in IMNCI records the data in the register, the handwriting unclear
and moreover the service provider and the person filling the reporting form are the
different person, so there is mismatch in the records and reports.”

48
“There is no space for writing in reporting file, therefore many times, it is recorded in
other antibiotics’ column.”
“Not many staffs are involved in recording and reporting job, so the other staffs do not
have enough time to record and report in the register.”
“Amoxicillin is so commonly used. So many times, due to the carelessness of the
staffs, there is double counting and sometimes, they forget to count. This may be the
reason for the mismatch of the records.”
ORS and Zinc tablets record reporting mismatch
The number of cases treated with ORS and zinc tablets in last 3 months was tallied and
found mismatch in the health facilities. The reasons for mismatch were
“Sometimes recording is done in the OPD register, but however, while reporting we not
only count from the record files but also from the OPD registers. That is why, the
records in the file and the reporting in the HMIS varies sometimes.”
“ORS and zinc are given so frequent that they are not recorded in register, therefore
sometimes, we have to report by just guessing the numbers.”
“ORS and Zinc are usually given more than the actual diarrheal cases, so we do not
keep an exact count of ORS and Zinc and even do not have enough time for recording
and reporting.”
“It has been wrongly written, the number 1 is mistakenly reported as number 7. This is
the carelessness of the staffs who do the recording and reporting.”

49
2.9
14.7
2.9
22.117.6
11.8
25
2.9
05
1015202530
Designation of Health Service Provider
Percent
3. Survey Findings for HSP
3.1 Designation of Health service provider Out of 36 health
facilities, a total of 68
health workers who were
involved in providing
CB-IMNC services were
interviewed. The
designation of
interviewed HSPs is
illustrated in Figure 2.
From the figure, it is
seen that majority of the interviewed health workers were ANM (25%) followed by
senior AHW (22.1%). However, nearly 3% of medical officer and staff nurse were
interviewed. The percentage of interviewed HSPs such as AHW, HA and senior ANM
were 17.6, 14.7 and 11.8 respectively.
3.2 Service readiness of HSP in HF focusing on CB-IMNCI Training
Table 12 shows that all the HSPs are not trained on CB-IMNCI services. Only 44% of the
health workers are trained on CB-IMNCI services. Likewise, the percentage of health
workers trained on CB-IMCI was 35 and 30 for CB-NCP. About 37% of the HSP received
other trainings such as nutrition, SBA, TB modular, HMIS and family planning.
Figure 5: Designation for HSP Figure 6: Designation for HSP

50
97% 94%71%
82% 77% 72%
0%20%40%60%80%
100%120%
Assessment done to diagnose PSBI
Table 13: Training received by HSP
S.N. Training Frequency (n= 68)
Yes (%) No (%) 1 CB-IMCI 35 (51.5) 33 (48.5) 2 CB-NCP 30 (44.1) 38 (55.9) 3 CB-IMNCI 44 (64.7) 24 (35.3) 4 Others 37 (54.4) 31 (45.6)
Provision of services
Even though, health workers were not trained but they had been providing CB-IMNCI
services.
3.3 Knowledge of HSP (< 2 months children) For assessing
knowledge, HSPs were
asked question about
assessment done to
diagnose PSBI. The
responses of the HSPs
are shown in Figure 7.
More than 90% of health
workers reported that
they took temperature
and count respiratory rate for diagnosis of PSBI. Similarly, 70.6% of health workers
mentioned that they listened to breathing, 82.4% mentioned that they measured
Figure 7: Assessment done to diagnose PSBI

51
weight of child, 76.5% asked about child's feeding and 72.1 % assessed child's
movement. However, result obtained by observing 15 recorded cases showed that in
33.3% of recorded cases temperature was not marked and in 20% of recorded cases
respiratory rate was not marked. The findings revealed that there is a discrepancy in
knowledge of HSPs and recording system.
Similarly, HSPs were further asked about how they diagnose PSBI cases. 7 (10%) service
providers mentioned all the responses that ares shown in Figure 8. 51 (75%) reported
more than four responses and 10 (15%) mentioned three or less than three responses.
Figure 8: Ways to Diagnose PSBI cases
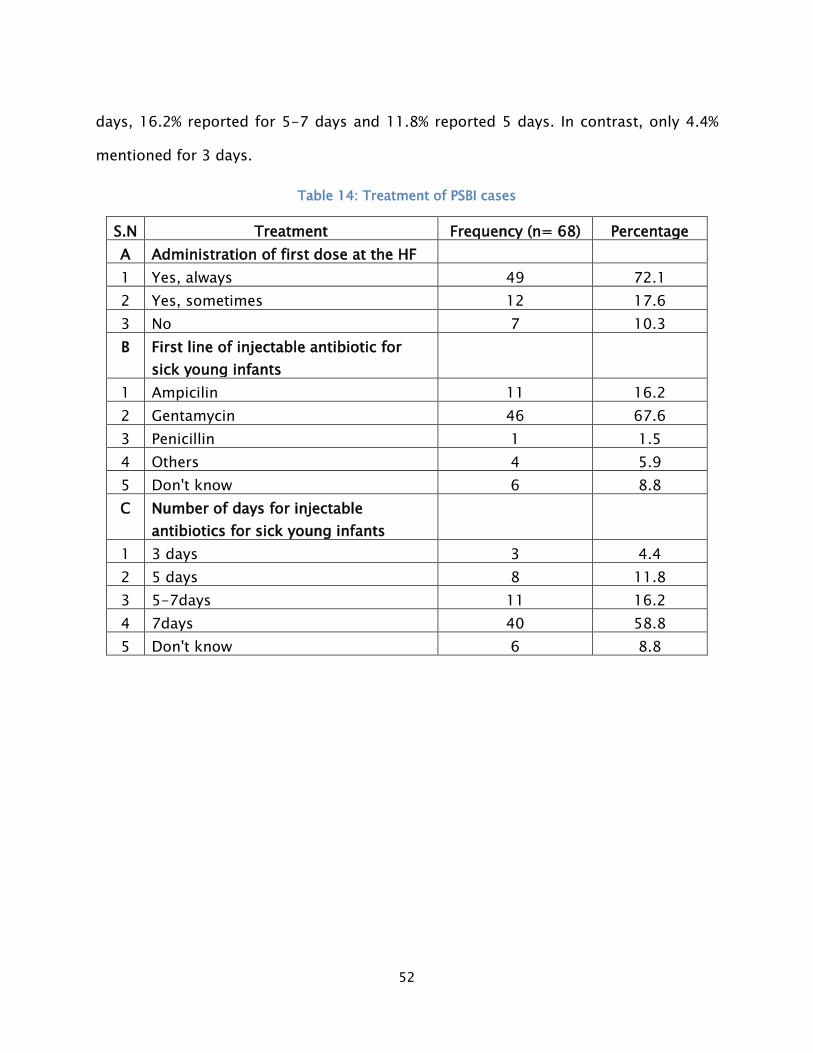
Knowledge of HSPs on treatment of PSBI cases is shown in Table 14. It was found that
72% of the health workers always administered first dose of antibiotic at HF whereas
only 12% of health workers sometimes administered first dose of antibiotic at HF. For
first line of injectable antibiotics, 67.6 % of health workers mentioned Gentamycin. For
number of days, injectable antibiotics given, 58.8% of health workers reported for 7
1168
5234
6571
6044
5352
4029
6818
0 20 40 60 80
Others/ Don't knowUnable to breastfeed
ConvulsionFast breathing
Severe chest in-drawingFever
Low body temperatureLess than normal movement
Lethargic or unconciousNo movent at all
Nasal flaringBulging Fontanelle
10 or more skin pustules or big boilUmbilicus redness or infection
How do you diagnose PSBI cases?
Percent
52
days, 16.2% reported for 5-7 days and 11.8% reported 5 days. In contrast, only 4.4%
mentioned for 3 days.
Table 14: Treatment of PSBI cases
S.N Treatment Frequency (n= 68) Percentage A Administration of first dose at the HF
1 Yes, always 49 72.1 2 Yes, sometimes 12 17.6 3 No 7 10.3 B First line of injectable antibiotic for
sick young infants 1 Ampicilin 11 16.2
2 Gentamycin 46 67.6 3 Penicillin 1 1.5 4 Others 4 5.9 5 Don't know 6 8.8 C Number of days for injectable
antibiotics for sick young infants 1 3 days 3 4.4
2 5 days 8 11.8 3 5-7days 11 16.2 4 7days 40 58.8 5 Don't know 6 8.8

53
37
6069
10
01020304050607080
Continuity of breast
feeding to prevent low
blood glucose
Skin to skin contact to
prevent heat loss
IM Gentamycin
and oral amoxicillin for 7 days
Refer
Management of PSBI
Percentage
82
68
56
26
44
10
0 50 100
Unable to …
Vomitting all
Convulsion
Unconscious/ …
Wheezing and chest …
Fever
General Danger Signs
Percentage
Figure 9 shows
responses given by
health workers in
management of PSBI
cases. Findings showed
that 69% of health
workers mentioned IM
gentamycin and oral
amoxicillin for 7 days for
management of PSBI
cases. About 32% of health workers reported others which included amoxicillin for 7
days, cotrim, health teaching, paracetamol and refer. However, 63.2% of health workers
did not mention continuity of breast feeding to prevent low blood glucose.
3.4 Knowledge of HSP (2-59 months children)
The responses given by the health workers on danger signs seen among children aged 2-59 months are shown in Figure10. About 82% of service providers mentioned unable to drink or suck breast milk, 68% reported vomiting and 56% reported convulsion.
Figure 9: Management of PSBI
Figure 10: General danger sign

54
Responses of HSP regarding their knowledge in the diagnosis, treatment and
management of ARI/ Pneumonia cases
The responses given by the HSPs are shown in Table 15. For severe pneumonia, 86.8 %
of HSP reported stridor in calm child and 32% mentioned increased respiration rate. For
pneumonia, most of the HSPs (94.1%) mentioned fast breathing. Likewise, 78%
reported chest in-drawing and 29% mentioned others which included fever and
wheezing. In case of no pneumonia, 51.5% mentioned no above signs and 50%
reported others which included common cold and fever.
Table 15: HSP respose to diagnosis of ARI/Pneumonia
S.N Diagnosis of Pneumonia Frequency (n= 68)
Yes (%) No (%) A Severe pneumonia 1 Stridor in calm child 59 (86.8) 9 (13.2) 2 Increased resporation rate 22 (32.4) 46 (67.6) 3 Lethargic/ Unconscious 9 (13.2) 59 (86.8) 4 Fever 4 (5.9) 64 (94.1) B Pneumonia N= 68 1 Chest in-drawing 53 (77.9) 15 (22.1) 2 Fast breathing 64 (94.1) 4 (5.9) 3 Fever 15 (22) 35(78) 4 Wheezing 5 (7) 63 (93) C No pneumonia N= 68 1 No above signs 35 (51.5) 33 (48.5) 2 Common cold 24 (35) 44 (65) 3 Fever 10 (15) 58(85)
Knowledge of HSPs regarding treatment of pneumonia is shown in Table 16. For severe
pneumonia, greater percentage (76.5%) of health workers reported first dose of
antibiotic followed by immediate referral which accounted 72.1%. In case of

55
pneumonia, 86.8% provided Amoxicilin 2 timesx5days, 47.1% monitored the case on
the third day and 29.4% of health workers reported use of salbutamol 3 timesx5 days.
For no pneumonia, 63% of HSPs reported home treatment and 24% paracetamol for
fever. In contrast, only 16.2% mentioned use of salbutamol 3times x 5days.
Table 16: HSP response to treatment of ARI/Pneumonia
S.N Treatment of Pneumonia Frequency (n= 68)
Yes (%) No (%) A Severe pneumonia 1 First dose of antibiotic 52 (76.5) 16 (23.5) 2 Immediate referral 49 (72.1) 19 (27.9) 3 Others 8 (12) 60 (88) B Pneumonia n= 68 1 Amoxicilin 2 timesx5days 59 (86.8) 9 (13.2) 2 Salbutamol 3 timesx5days 20 (29.4) 48 (70.6) 3 Monitor the case on third day 32 (47.1) 36 (52.9) 4 Others 10 (14.7) 58 (85.3) C No pneumonia n= 68 1 Salbutamol3timesx5days 11 (16.2) 57 (83.8) 2 Home treatment 43 (63) 25(37) 2 Paracetamol for fever 16 (24) 52 (76)
Responses of HSP regarding their knowledge in the diagnosis, sign and symptoms,
classification, treatment and management of diarrhea cases
Responses given by the health workers for diagnosis of diarrhea are shown in Table
17. For severe dehydration, the highest percentage of the health workers (88.2%)
mentioned skin pinch very slowly. 25% of service providers reported others which
included bulging frontanelle, less urine output and vomiting. For dehydration, greater
percent of health workers mentioned skin pinch slowly (90.1%) than restless or irritable

56
(55.9%). Likewise, in case of no dehydration most of the health workers reported not
enough signs (92.6%) than minor or serious dehydration (38.2%).
Table 17: HSP response to diagnosis of diarrhea
S.N Diagnosis of diarrhea Frequency (n= 68)
Yes (%) No (%) A Severe dehydration 1 Lethargic/ Unconscious 53 (77.9) 15 (22.1) 2 Sunken eyes 52 (76.5) 16 (23.5) 3 Drink poorly 50 (73.5) 18 (26.5) 4 Skin pinch very slowly 60 (88.2) 8 (11.8) 5 Others 17 (25) 51 (75) B Dehydration n= 68 1 Restless/irritable 38 (55.9) 30 (44.1) 2 Skin pinch slowly 62 (91.2) 6 (8.8) 3 Others 10 (14.7) 58 (85.3) C No Dehydration n= 68 1 Not enough signs 63 (92.6) 5 (7.4) 2 Minor dehydration 26 (38.2) 42 (61.8) 3 Others 5 (7.4) 63 (92.6)
The responses of the health workers on classification of diarrhea are shown in Table
18. For severe persistent diarrhea and persistent diarrhea, majority of the respondent
reported diarrhea for more than 14 days. For dysentery, 83.8% of the respondent
mentioned blood in stool.
Table 18: HSP response to classification of diarrhea
S.N Classification of diarrhea Frequency (n= 68)
Yes (%) No (%) A Severe persistent diarrhea n= 68 1 Diarrhea for more than 14 days 59 (86.8) 9 (13.2)

57
2 Severe/some dehydration 18 (26.5) 50 (73.5) 3 Others 14 (20.6) 54 (79.4) B Persistent diarrhea n= 68 1 Diarrhea for more than 14 days 66 (97.1) 2 (2.9) 2 Others 13 (19.1) 55 (80.9) C Dysentery n= 68 1 Blood in stool 57 (83.8) 11 (16.2) 2 Others 27 (39.7) 41 (60.3)
Table 19 shows responses of the health workers for the treatment of diarrhea. For
severe persistent diarrhea, most of the respondent reported treat dehydration (72%)
centre, whereas in case of persistent diarrhea and dysentery majority of the
respondent mentioned provision of ORS and zinc for 10 days.
Table 19: HSP response to treatment of diarrhea
S.N Treatment of diarrhea based on its classification Frequency (n= 68)
Yes (%) No (%) A Severe persistent diarrhea 1 Treat dehydration 49 (72.1) 19 (27.9) 2 Refer to treatment centre 39 (57.4) 29 (42.6) 3 Single dose of Vitamin A 46 (67.6) 22(32.4) B Persistent diarrhea n= 68 1 Single dose of Vitamin A 27 (39.7) 41 (60.3) 2 ORS and Zinc tablet for 10 days 61 (89.7) 7 (10.3) 3 Monitor on 5th day 35 (51.5) 33 (48.5) C Dysentery n= 68 1 Ciprofloxacin for 3 days 42 (61.8) 26 (38.2) 2 ORS and Zinc tablet for 10 days 54 (79.4) 14 (20.6) 3 Monitor on the third day 48 (70.6) 20 (29.4)

58
94
79
78
68
74
24
25
16
9
0 20 40 60 80 100
Refer to the health facility
Supply iron/folic tablets
Educate on newborn care
Educate on danger sigs …
Advise on the need for …
Treatment by cotrim
ORS/ zinc distribution
Counseling on home care
Others
HSP perception on FCHV role
Percentage
3.5 Perception of HSPs on FCHV's role The responses given by
health workers are
illustrated in Figure 11.
About 94% health workers
reported to refer to the
higher facility. More than
70% of service providers
reported educate on
newborn care, advice on need
for immediate consultation.
However, only 25% of service providers mentioned distribution of ORS and zinc.
Majority of HSPs (79.4%) believed that the role of FCHV's does not depend on distance.
Similarly, 82.4% health workers mentioned that FCHVs working in distance 2 hrs or
more have the same role as those living near HF. However, 17.6% reported that their
role was different.
3.6 Knowledge of SBA Out of 68 interviewed HSPs, 22 were SBA. The responses given by the SBA are
illustrated in Table 20. More than 90% of SBA mentioned immediate drying of
newborns immediately after birth. For care given to the mother after child's birth, 86%
of SBA reported ensure placenta is fully delivered and check for bleeding.
For danger signs in newborn, all the respondent reported unable to suck milk, 68.2%
mentioned severe chest in-drawing, unconscious/ lethargic. About 50% mentioned
other danger signs such as skin rashes or umbilical infection.
Figure 11: HSP perception on FCHV role
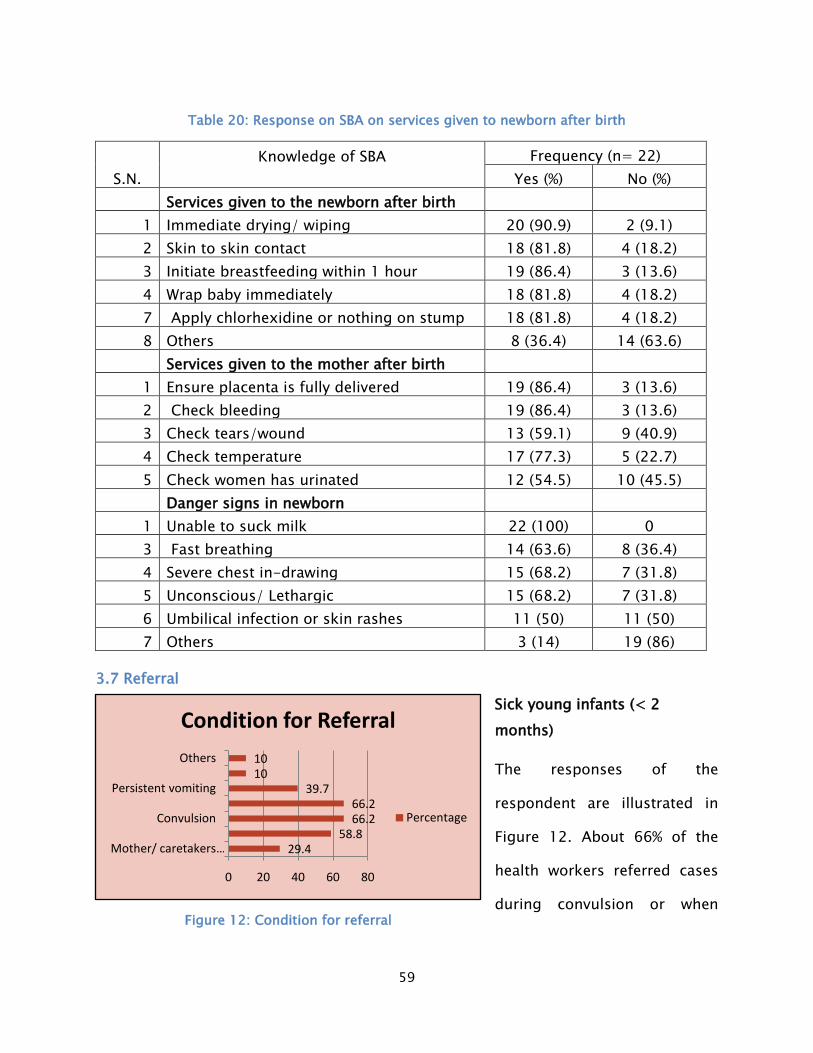
59
29.458.8
66.266.2
39.71010
0 20 40 60 80
Mother/ caretakers …
Convulsion
Persistent vomiting
Others
Condition for Referral
Percentage
Table 20: Response on SBA on services given to newborn after birth
S.N. Knowledge of SBA
Frequency (n= 22)
Yes (%) No (%)
Services given to the newborn after birth
1 Immediate drying/ wiping 20 (90.9) 2 (9.1) 2 Skin to skin contact 18 (81.8) 4 (18.2) 3 Initiate breastfeeding within 1 hour 19 (86.4) 3 (13.6) 4 Wrap baby immediately 18 (81.8) 4 (18.2) 7 Apply chlorhexidine or nothing on stump 18 (81.8) 4 (18.2) 8 Others 8 (36.4) 14 (63.6)
Services given to the mother after birth
1 Ensure placenta is fully delivered 19 (86.4) 3 (13.6) 2 Check bleeding 19 (86.4) 3 (13.6) 3 Check tears/wound 13 (59.1) 9 (40.9) 4 Check temperature 17 (77.3) 5 (22.7) 5 Check women has urinated 12 (54.5) 10 (45.5)
Danger signs in newborn
1 Unable to suck milk 22 (100) 0 3 Fast breathing 14 (63.6) 8 (36.4) 4 Severe chest in-drawing 15 (68.2) 7 (31.8) 5 Unconscious/ Lethargic 15 (68.2) 7 (31.8) 6 Umbilical infection or skin rashes 11 (50) 11 (50) 7 Others 3 (14) 19 (86)
3.7 Referral Sick young infants (< 2 months)
The responses of the
respondent are illustrated in
Figure 12. About 66% of the
health workers referred cases
during convulsion or when Figure 12: Condition for referral

60
17.5
22.5
12.5
47.5
0 50
Irritable child
Lack of …
Limited number …
Untrained health …
Problems faced by HSP
Percent
child is lethargic or unconscious. And 58.8% of the respondent reported when there is
no improvement on the third day. About 85.3% of health worker provided pre-referral
dosing before referral. For pre-referral dosing, 84.5% respondent provided first dose
of gentamycin and ampicillin and 15.5% respondent reported provision of other
medicines. The highest cases were referred to district hospital (59%). About 21% of
cases were referred to zonal hospital and sub-regional hospital, 10% to the PHC and
private hospital.
Children aged 2-59 months (Pneumonia cases)
Health workers were asked question when they referred cases in pneumonia. Nearly
84% of the service providers reported in severe pneumonia and 16% reported if the
condition is not improved.
Problem faced by health workers in diagnosis of PSBI
Sick young infant (< 2 months)
Of 68 interviewed health workers,
26.5% did not have problem while
diagnosing PSBI cases and 14.7%
had not seen cases. Thus, a total of
40 service providers faced
difficulties while diagnosing PSBI
cases and the difficulties faced by
them is displayed in Figure 13.
Most of respondent faced problems due to untrained health personnel (47.5%) followed
by lack of equipment and lab facility (22.5%). 17.5% of the service providers faced
problems due to irritable child and 12.5% mentioned due to limited number of staffs.
Figure 13: Problem faced by HSP in diagnosis of PSBI

61
15.4
15.4
17.935.9
15.4
0 20 40
Caretakers don't …
Irritable child
Medicine compliance
Unavailability of …
Untrained health …
Problems faced by HSP
Percent
Problem faced by health workers in managing of PSBI
A total of 39 HSPs faced
difficulties while treating PSBI
cases which are illustrated in
Figure 7. Of those, 35.9% of
health workers faced problem
because of unavailability of
medicine. 15.4% of service
providers faced difficulties due
to untrained health personnel, irritable child and lack of trust on service providers.
Children aged 2-59 months (ARI/ pneumonia and diarrhea cases)
Problem faced by the HSPs in the diagnosis of ARI/pneumonia and diarrhea is shown in
Figure 15. Almost 34 (50%) interviewed health workers faced difficulties while
diagnosing ARI/ pneumonia cases. Out of which, majority of the respondent reported
due to lack of equipments (41.2%). In contrast, in case of diarrhea 37.9% of health
workers faced problems because of untrained health personnel.
Figure 14: Problem faced by HSP in managing PSBI cases

62
6%
42%
24%
8%
20%
0%5%
10%15%20%25%30%35%40%45%
Antibiotic resistant
Difficult to give
medicine to child
Lack of medicine
No follow up
Untrained health
personnel
Problems faced by HSP
Percent
Figure 15: Problem faced by HSP in diagnosis of ARI/Pneumonia and diarrhea
Problem faced by HSP in managing Pneumonia
Problems faced by the
HSPs while managine
ARI/pneumonia and
diarrhea is shown in
Figure 16. For
ARI/pneumonia, 50
respondents felt problem
while treating. About 42%
of service providers faced
problem while giving medicine to child and 24% felt because of lack of medicine.
29.4
41.2
5.9
23.5
31
24.1
6.9
37.9
0
5
10
15
20
25
30
35
40
45
Irritable child Lack of equipments
Unavailability of sufficient staffs
Untrained health
personnel
Problems faced by HSP
ARI/Pneumonia (%)
Diarrhea (%)
Figure 16: Problem faced by HSP in management of Pneumonia

63
For diarrhea, 40 health workers reported of having problems while treating diarrhea
cases. Majority of the service providers faced problems due to insufficient supply of
ORS and zinc (40%). Nearly 13 % of service providers felt problem because of difficulty
to feed medicine and no follow up.
Figure 17: problem faced by HSP while treating Diarrhea
12.5%7.5%
40.0%
12.5%
27.5%
0.0%5.0%
10.0%15.0%20.0%25.0%30.0%35.0%40.0%45.0%
Difficulty to feed
medicine
Guardians don't trust
public health facility
Insufficient supply of ORS and
Zinc
No follow up
Untrained health
personnel
Problems faced by HSP
Percent
N= 40

64
55%
45%
Distance from the HF to residence
<30 minutes
>=30 minutes
4. Survey Findings for Follow up visit Results A total of 58 caretakers were interviewed, out of which, 56 cases were from the age
group of 2-59 months children and the rest 2 cases were below 2 months. The
children who were presenting to the HF came with the illnesses such as ARI/pneumonia
35 (60%), Diarrhea 20 (35%) and PSBI 3 (5%). And there were majority of
Brahmin/Chhetri ethnicity (48.3%) followed by Janajati (29.3%). Out of the 58 cases, 50
(86.2%) children were brought to the HF by their mothers, 5(8.6%) were brought by
their fathers with remaining 3 (5.2%) brought by other members of the family.
4.1 Distance from the HF to the residence Out of the total 58 caretakers,
32 (55%) lived at the distance
of less than 30 minutes from
the HF whereas the other 26
(45%) lived at a distance of 30
minutes or more.
Figure 18: distace from HF to residence

65
86%
14%
Waiting time at the HF
<30 minutes
>=30 minutes
4.2 Waiting time to get health services In a total of 58 caretakers who
visited the HF for follow up visits for
their sick children, 50 (86.2%) said
that they had to wait less than 30
minutes to get the health service
after reaching the facility while 8
(13.8%) said they had to wait for 30
minutes or more to get the health
service.
It was seen that 13.8% of the caretakers still had to wait for 30 minutes or more to
receive the health service after reaching the HF.
4.3 Presenting complains of the children coming to the HF for consultation Figure shows the presenting complains that the children had for which they had come
to the HF for consultation. A maximum of 42 (72.4%) out of 58, had come with the
complaints of fever followed by 29(50%) with difficulty in breathing. A total of 24
(34.5%) children had come due to diarrhea and 14 (24.1%) had come due to inability to
feed.
Figure 19: Waiting time at HFs

66
2
16
29
2
19
32
0
10
20
30
40
Assessment according disease type
Weight
Temperature
Figure 20: Presesnting complians of the children coming to HF
4.4 Reasons for taking to the HF The total of 58 caretakers were asked about their reasons for going to the HF which
they visited and 44 of them (76%) replied that they went to the HF because it was near.
The other reasons were availability of services (9%), availability of quality services (7%)
and good behavior of the
staffs and others (8%) of the
HF.
4.5 Assessment of weight and temperature Asa part of the examination, the caretakers were interviewed asking them if the health
workers examined the weight and temperature. From the Figure, it is seen that for the
72.4
50
24.1
5.2
34.5
8.615.5
3.40
20
40
60
80
Presenting complains of the children coming to the HF
Percentage
Figure 21: Assessment according disease type

67
76%
41%
59%
31%
40%
0% 10% 20% 30% 40% 50% 60% 70% 80%
Medicines
Newborn care
Breast feeding
Immunization
Nutrition and Home care
Information and servecies received by caretakers
cases of ARI/ Pneumonia and Diarrhea weight was not measured than compared to
temperature.
4.6 Health services provided during the follow up visit The caretakers were
asked about the
information and
services they received
during their visit to the
HF apart from other
knowledge they
received. Figure 22
shows that about 76%
of the caretakers were
provided with
medicines, 22% were
given immunization
services. Around 41% were given the information about essential newborn care, 59%
about breastfeeding and 31% about the immunization.
For <2 months age group children
Information regarding the danger signs
Among the total 58 children, a total of 7 were <2 months of age out of whom, 6 were
given information regarding the danger signs of newborn by the health worker.
Figure 22: Information and services received by caretakers

68
Among the total of 6 caretakers, all were provided information about hypothermia and
out of 6, 5 were given information on fever as a danger sign, 4 were given information
on fast breathing and unable to breastfeed and 2 were informed about the red
umbilicus. However, no caretakers were given information about the occurrence of skin
pustules as danger signs of newborn.
Client compliance
Understanding of the information given by the health worker
The caretakers were asked if they understood all the information provided by the
health worker. Around 83% said that they understood all the information provided and
the rest said that they understood some information provided to them.
The results on the understanding of all the information provided by the health worker
were based on the perception of the mothers/caretakers which depict their view of
understanding all or some information given to them.
Giving medicines/complete course of doses as prescribed by the health worker
All the 58 (100%) caretakers responded that they gave medicines to their children just
as prescribed by the health worker. Asking about the complete course of doses, 56
(96.6%) of the caretakers responded that they gave the complete course of drugs as
prescribed by the health worker.
Care of child advised by the health worker
The caretakers were asked whether they cared for their sick children as advised by the
health worker to which 57 (98.3%) of the caretakers responded that they cared as they
were advised by the health worker.
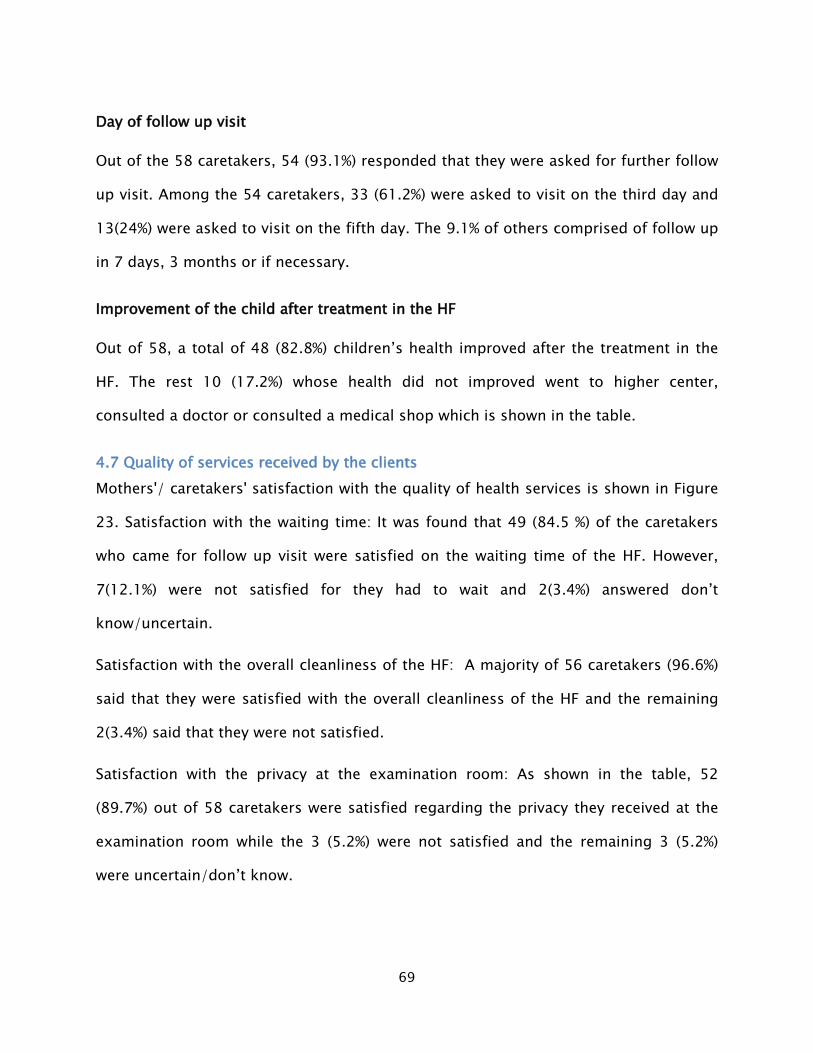
69
Day of follow up visit
Out of the 58 caretakers, 54 (93.1%) responded that they were asked for further follow
up visit. Among the 54 caretakers, 33 (61.2%) were asked to visit on the third day and
13(24%) were asked to visit on the fifth day. The 9.1% of others comprised of follow up
in 7 days, 3 months or if necessary.
Improvement of the child after treatment in the HF
Out of 58, a total of 48 (82.8%) children’s health improved after the treatment in the
HF. The rest 10 (17.2%) whose health did not improved went to higher center,
consulted a doctor or consulted a medical shop which is shown in the table.
4.7 Quality of services received by the clients Mothers'/ caretakers' satisfaction with the quality of health services is shown in Figure
23. Satisfaction with the waiting time: It was found that 49 (84.5 %) of the caretakers
who came for follow up visit were satisfied on the waiting time of the HF. However,
7(12.1%) were not satisfied for they had to wait and 2(3.4%) answered don’t
know/uncertain.
Satisfaction with the overall cleanliness of the HF: A majority of 56 caretakers (96.6%)
said that they were satisfied with the overall cleanliness of the HF and the remaining
2(3.4%) said that they were not satisfied.
Satisfaction with the privacy at the examination room: As shown in the table, 52
(89.7%) out of 58 caretakers were satisfied regarding the privacy they received at the
examination room while the 3 (5.2%) were not satisfied and the remaining 3 (5.2%)
were uncertain/don’t know.

70
Satisfaction with the time given by the HSP: Here, 53(91.4%) of the caretakers were
satisfied with the time given by the HSPs to them. However, 2(3.4%) and 3 (5.2%) said
they were not satisfied and did not know/uncertain respectively.
Satisfaction with the behavior of the HSP: Almost 95% caretakers were satisfied with the
behavior of the HSPs during their follow up visit. The remaining 2(3.4%) were not
satisfied and 1(1.7%) said they were uncertain.
Satisfaction with the overall service of the health: The overall satisfaction regarding the
health services were expressed by 50 (86.2%) caretakers whereas 5 (8.6%) said they
were not satisfied with the service they received and 3 (5.2%) said they did not know
and were uncertain about the service.
Figure 23: Caretakers satisfaction with the quality of the health services received
84.596.6
89.7 91.4 94.886.2
12.13.4 5.2 3.4 3.4 8.63.4 0 5.2 5.2 1.7 5.2
0
20
40
60
80
100
120
Caretakers Satisfaction
Satisfied
Not satisfied
Don't know

71
51%
49%
Distance from the HF to residence
<30 minutes
>=30 minutes
5. Survey Findings for Exit Interview For the exit interview of the caretakers, 61 caretakers were interviewed, out of which,
54 cases were from the age group of 2-59 months children and the rest 7 cases were
below 2 months. The caretakers were from the age group 20-53 years. The sick
children were presented with ARI/pneumonia 36 (59%), diarrhea 22 (36%) and PSBI 3
(5%). And there was a majority of Brahmin/Chhetri (52.4%) followed by Janajati (21.3%).
Out of the 61 cases, 58 (95.1%) children were brought to the HF by their mothers and
the remaining 3 (4.9%) brought by their fathers.
5.1 Distance from the HF to the residence Out of the total 61 caretakers, 31
(50.8%) lived at the distance of
less than 30 minutes from the HF
whereas the other 30 (49.2%)
lived at a distance of 30 minutes
or more.
Figure 24: Distance from HF to residence

72
93%
7%
Waiting time at the HF
<30 minutes
>=30 minutes
62.350.8
18
1.6
36.127.9
19.78.2 4.9
010203040506070
Presenting complains of the children coming to the HF
Percentage
5.2 Waiting time to get health services In a total of 61 caretakers who
visited the HF for check up, 57
(93.4%) said that they had to
wait less than 30 minutes to get
the health service after reaching
the facility while 4 (6.6 %) said
they had to wait for 30 minutes
or more to get the health service.
Health seeking behavior of the caretakers
When asked if the caretakers brought their children to the same HF usually when they
get sick, 56 (91.8%) answered yes and the remaining 5 (8.2%) who answered no said
that they went for the private clinics (4.9%) and others (3.3%).
5.3 Presenting complains of the children coming to the HF for consultation Figure 26 shows
the presenting
complains that
the children had
for which they
had come to the
HF for
consultation.
Figure 25: Waiting time to get health services
Figure 26: Presenting complians of the children coming to the HF

73
1
22
33
3
19
33
0
10
20
30
40
PSBI diarrhea ARI/pneumonia
Assessment according disease type
Weight
Temperature
A maximum of 38 (62.3%) had come with the complaints of fever followed by 31
(50.8%) who had come with difficulty in breathing. A total of 22(36.1%) children had
come due to diarrhea and 11 (18%) had come with complains of being unable to feed.
Lethargic-unconsciousness 17 (27.9 %), cough and cold (19.7 %), weakness (8.2%) and
earache (4.9%) were the other complains.
5.4 Assessment of weight and temperature As a part of the
examination, the
caretakers were
interviewed asking them if
the health workers
examined the weight and
temperature during their
visit. From the Figure 27,
it is found that out of 3 PSBI cases, weight of 2 cases was not taken. However, for ARI/
Pneumonia cases weight and temperature was measured for equal number of cases.
5.5 Health services provided during visit to the HF The caretakers were asked about the information and services they received during
their visit to the HF. Figure 28 shows that 41 (67%) of the caretakers were provided
with medicines. There were 25 (41%) caretakers who were given the information about
essential newborn care, 49% were given information about breastfeeding and 39%
about the immunization.
Figure 27: Assessment according to disease type

74
Figure 28: Information and services received by caretakers
For <2 months age group children
Information regarding the danger signs
Among the total of 15 caretakers, all said that they were informed about the danger
signs in newborn. Among which, only 2 were provided the information of the danger
signs as being unable to breastfeed, hypothermia, fast breathing, red umbilicus and
occurrence of skin pustules. And 3 were given information that fever is a danger sign
and 2 about other signs.
Day of Follow up visit
Out of the 61 cases, 50 (82 %) said that they were asked for further follow up visit.
Among the 50 cases, 32 (52.5%) were asked to visit on the third day and 1(1.6 %) were
asked to visit on the fourth day and 14(23%) on the fifth. The 4.9% of others comprised
of follow up if necessary.
67%
41%
49%
39%
15%
0% 10% 20% 30% 40% 50% 60% 70% 80%
Medicines
Newborn care
Breast feeding
Immunization
Nutrition and home care
Information and services received by caretakers

75
5.6 Quality of services received by the clients Mothers'/ caretakers' satisfaction with the quality of health services is shown in Figure
29. Satisfaction with the waiting time: It was found that 56 (91.8 %) of the caretakers
who came for visit to the HF were satisfied with the waiting time of the HF. However,
5 (8.2%) answered they didn’t know and were uncertain.
Satisfaction with the overall cleanliness of the HF: A majority of 57 caretakers (93.4%)
said that they were satisfied with the overall cleanliness of the HF and 3 (4.9%) said
they were not satisfied and the remaining 1 (1.6 %) answered uncertain.
Satisfaction with the privacy at the examination room: As shown in the table, 50 (82 %)
out of 61 caretakers were satisfied regarding the privacy they received at the
examination room while the 7 (11.5 %) were not satisfied and the remaining 4 (6.6%)
were uncertain and didn’t know.
Satisfaction with the information given by the HSP: Here, 55 (90.2%) of the caretakers
were satisfied with the information that was provided by the HSPs to them. However, 6
(9.8 %) said they were not certain.
Satisfaction with the behavior of the HSP: Almost 97% caretakers were satisfied with the
behavior of the HSPs during their visit. The remaining 2 (3.3 %) said they were
uncertain about the behavior of the HSP.
Satisfaction with the overall service of the health: The overall satisfaction regarding the
health services were expressed by 56 (91.8%) caretakers whereas 5 (8.2%) said they did
not know and were uncertain about the service.

76
Figure 29: care takers satisfaction with the quality of health service received
91.8 93.482
90.2 96.7 91.8
04.9
11.5 0 0 08.2 1.6 6.6 9.8 3.3 8.2
0
20
40
60
80
100
120
Caretakers Satisfaction
Satisfied
Not satisfied
Don't know

77
39%
61%
Distance from the HF to residence
<30 minutes
>=30 minutes
31%42% 43%
0%
20%
40%
60%
CB-IMNCI CB-NCP CB-IMCI
Types of trainings received by FCHV
6. Survey Findings for Female Community Health Volunteer (FCHV) Interview A total of 72 FCHVs were interviewed for the survey. The FCHVs were from the age
group 24 years to 61 years. Majority were Brahmin/Chhetri (50%), followed by Janajati
(23.6%), Madhesi (22.2%) and Dalit (4.2%).
Out of the 72 FCHVs, 28 (38.9%) lived near to the HF that is within the walking distance
of less than 30 minutes to the HF from their residence and the 44 (61.1%) others said
that they lived at a distance of more or equal to 30 minutes from the HF.
Figure 30 shows that the
majority of FCHVs were
providing services in the
community even staying far
from the respective HF which
they report to.
6.1 Trainings of the Female Community Health Volunteer The FCHVs had taken different
trainings of which 22 (31%) out of
the 72 were trained in CB-IMNCI, 30
(42%) out of 72 FCHVs were trained
on CB-NCP, 31 (43%) were trained
on CB-IMCI. The training received by
FCHVs is shown in Figure 31. The
reason for FCHVs less trained in CB-
IMNCI is because in Baitadi and Saptari districts first phase of CB-IMNCI program is
Figure 30: distance from HF to residence
Figure 31: Types of training received by FCHV

78
47%
35%
7%1%
10%
0%
10%
20%
30%
40%
50%
On the day of birth
on the third day of birth
on the 7th day of birth
on the 29th day of birth
dont know
PNC Visit by FCHV
running and the FCHVs belonging to these districts are not provided training on CB-
IMNCI.
6.2 Knowledge of the FCHVs Meeting the mother and the newborn after delivery
The FCHVs were asked
about the postnatal
visits they had made
for the women who
recently delivered and
are shown in Figure
32. Asking about the
day of the visits, 34
(47%) of the FCHVs
had visited the mother and the newborn on the day of birth. Similarly, 25 (35%) had
made visits on the third day of birth, 5 (7%) on the 7th day of birth and 1 (1.4%) on the
29th day of birth. However, there were 7 (10%) of FCHVs who said that they did not
know about their postnatal care visits.
Figure 32: PNC visit by FCHV to mothers

79
61%
86%74%
54%
94%
54%
22% 25%
0%10%20%30%40%50%60%70%80%90%
100%
Information provided by FCHV
Information provided during the post natal visit
The FCHVs were
interviewed about the
information they
provided the mothers
during their post natal
visit and details are
shown in Figure 33.
The FCHVs gave
information about the
post natal care (61%),
they informed about the danger signs of newborn (86%) and about the danger signs of
mothers (74%). The FCHVs also gave information about the chlorhexidine gel
application to 39 (54%) and information about breastfeeding (94%) and family planning
(54%).
Referral to the HF
The FCHVs were asked if they refer the case that they see to the HF. Out of the 72
FCHVs, almost all i.e. 72 (100%) responded that they referred the patients to the
hospital if complications arise.
Place of referral
The FCHVs were asked where did they usually refer the cases to which, 66 (92%) out of
72 said that they referred to the respective health facilities in their wards/VDCs and 6
Figure 33: Information provided by FCHV

80
(8.3%) said that they referred to other centers as the district hospital (6.9%) and the
zonal hospital (1.4%).
Signs to assess in the < 2 months child for referral to the HF
The FCHVs were asked about the signs that they assessed in a newborn less than 2
months to refer to the HF. Here, 57 (79%) said that they assess whether the baby drinks
poorly, 55(76%) said that they checked there was difficulty in breathing and the 46
(64%) said that they assessed chest indrawing for referral. Unconsciousness/ lethargic
conditions were assessed by 42(58%) for referral and 59 (82%) and 20 (28%) assessed
fever and bulging frontanelle respectively for referral.
Figure 34: Signs assessed in < 2 months children by FCHVs for referral
79 76 64 5882
28 19 80
20406080
100
Signs to assess for referral in <2 moths children
Percentage

81
9276
3819 11
020406080
100
Services Provided
Percentage
6.3 Volume of service provided to the children < 5 years age for diarrhea There were 67 (93%) of
the FCHVs who said that
they provided service to
the under 5 years
children suffering from
diarrhea. In the last 3
months, they treated a
maximum up to 40 cases of diarrhea. The various services provided were distribution
of oral rehydration solution (ORS) which was among 66 (92%) FCHVs, zinc tablets
among 55 (76%) and counseling for breastfeeding continuity (38%). The other services
provided were advice on hygiene and sanitation (11%) and home remedies (19%) are
shown in Figure 35.
Treatment of ARI/Pneumonia
The FCHVs were asked if they provided services for the treatment of ARI/Pneumonia
for under 5 children. Among all, 42% said that they provided treatment for the
ARI/Pneumonia in under 5 children and the remaining 58% did not provide treatment
for ARI/Pneumonia.
Reasons for no treatment of ARI/Pneumonia
The 58% of FCHVs who said that they did not provide treatment for ARI/Pneumonia
were because of the reasons as Cotrim not being advised nowadays (11%), no
medicines available (13%), no cases of pneumonia (1%), no training available (8%) and
the reasons due to referral to the nearby HF directly (25%).
Figure 35: Service provided to <5 children for diarrhea

82
6.4 Available stocks of ORS, Zinc and Chlorhexidine at present The FCHVs said that they provided Chlorhexidine gel to the pregnant mothers and it
was found that 50% provided and 50% did not. The reasons for not providing
Chlorhexidine gel were 9.7% having no stock at that time and 20.8% said that the HF
was near and they referred pregnant women for institutional delivery.
The FCHVs were further asked if they have current available stocks of ORS, Zinc and
Chlorhexidine gel and is shown in Figure. For the ORS packets, 83% had stocks
available with them at present. Of the total FCHVs, 63% said that they had current
available stocks of zinc tablets and 50% currently have stocks of Chlorhexidine gel with
49% available stock of paracetamol at present.
Figure 36: Available stocks of ORS, Zinc, CHX and paracetamol at present
83
63
50 49
0102030405060708090
ORS Zinc Chlorhexidine Paracetamol
Available Stock
Percentage
N= 72

83
FCHV meetings register update and reporting to the HF
The FCHVs were asked if they had conducted mothers’ group meeting last month and
all the 72 (100%) FCHVs said they conducted the meeting last month. Regarding the
ward register update, all 72 (100%) said that they have updated their ward register.
And they said that they all submit the report to the HF once a month.
Role of the FCHVs given in the CB-IMNCI program
The FCHVs were asked about their role in the CB-IMNCI program and whether they
were satisfied with the role given to them by the CB-IMNCI program. Out of the total
72 FCHVs, 60 (83.3%) said that they were satisfied with their role in the CB-IMNCI
program. The remaining had their reasons for their unsatisfaction. Out of the 12
(16.7%) FCHVs, 5 (6.9%) expressed the need of more trainings to be conducted for the
FCHVs to run the CB-IMNCI better. The 4 (5.6%) said that it was difficult for them to
travel to different places to the wards, so it would have been better, if they were
provided with some incentives and the remaining 3 (4.2%) said that they were
unsatisfied as the medicines were not all made available to them to be able to give
better services, especially for the children of <2 months.

84
3. Summary of the Findings An assessment study of the CB-IMNCI program was carried out in the six districts
covering the different ecological zones. It focused on the three diseases of the CB-
IMNCI program viz. PSBI, ARI/Pneumonia and Diarrhea. Firstly, the CB-IMNCI focal
person from each districts were visited and interviewed. They were asked about the
logistics (receiving and supplying the medicines and commodities) and regular staff
meetings, monitoring and supervision and how they evaluated the CB-IMNCI program.
The HMIS manual presence (83.3%), adequate tool supply (100%), orientation of staffs
towards HMIS (66.7%), timely reporting (83.3%) and reasons for not reporting of PSBI
cases were enquired.
The Health facilities were then chosen as per the less/ no PSBI cases treated in last
three, remoteness, presence of private clinics and types of HF (Health post and Primary
Health Care Center). A total of 36 health facilities from 6 districts were visited out of
which 7 were PHCC and 29 HPs. There was equal percentage of CB-IMNCI and CB-IMCI
trained personnel in the health facilities. Out of the 36 HF, 19 (52.8%) were birthing
centers and 17 (47.2%) had newborn corner with resuscitation table. For the availability
of equipments, all health facilities had BP instrument and stethoscope. More than 30%
of the health facilities experienced stock out in the last three months for the months
for the drugs such antibiotics (Amoxicillin and Cotrim P) and Tab. Paracetamol 500 mg,
Inj. Gentamycin. The current status of the drugs showed there were 27.8% health
facilities did not have Inj. Gentamicin and 22.2% did not have antibiotics.
Health service provider's interview was taken among 68 health workers working in 36
HF. It was found that auxillary health workers had the most toll (22.1%) followed by
least of 2.9% of medical officers and staff nurses. Out of the 68 health workers, 44

85
(64.7%) were CB-IMNCI trained persons. The knowledge was determined using the
semi-structured questionnaire where assessment of the different diseases was done
on the basis of signs and symptoms, diagnosis, treatment and referral. In diagnosing
PSBI, 94.1% of the HSP had known about respiratory rate, 97.1% about taking
temperature and 82.4% on weighing the child. Further, 70.6% had known about fever,
64.7% about severe chest indrawing, 51.5% about convulsion and 67.6% about skin
pustules as different signs and symptoms. For the management of PSBI, 61.1% of
health workers reported IM Gentamycin and oral Amoxicillin for 7 days, 60.3% reported
skin to skin contact to heat loss. However, only 36.8% reported continuity of
breastfeeding for the management of PSBI. The knowledge of the HSP on the danger
signs of children aged 2 – 59 months showed that 82.4% reported unability to
drink/suck milk and 67.6% reported vomiting as a danger sign. More than 80% of
service providers had knowledge on classification of diarrhea. For severe persistent
diarrhea, 86.8% HSP said diarrhea for more than 14 days and for dysentery, 83.8% said
blood in stool. The cases of severe pneumonia were diagnosed as 86.8% HSP said
presence of stridor in calm child; and 94.1% HSP said fast breathing and chest
indrawing (77.9%) for the diagnosis of pneumonia.
Among the total 68 HSP, 22 SBAs were assessed on services given to the newborn and
mothers immediately after birth and the danger signs in newborn. More than 90 % of
the SBA had knowledge on immediate drying of baby. On the referring the sick young
infant, 66% of HSP said referral is required when convulsions occur and if the baby is
lethargic and unconscious. Moreover, 58.8% of HSP refer the cases when there is no
improvement on the third day of treatment. Out of total, 40 service providers faced
problems in diagnosing PSBI cases which were due to untrained health workers (47.5%)

86
and lack of equipments and lab facility (22.5%) whereas for the treatment, problems
were due to unavailability of drugs (35.9%) and 17.9% with drug inadherence. The
problems in diagnosing ARI/pneumonia were due to lack of equipments (41.2%) and
irritable child (29.4%) whereas in diarrhea, untrained health worker (37.9%) was the
major problem faced.
About 80% HSP expressed that the role of FCHV does not vary on the distance from the
HF to their residence. According to the HSP, the role of FCHVs in CB-IMNCI is to refer
(94.1%) and more than 70% in roles such as supply iron/folic acid, educate on newborn
care and advice on need for immediate consultation.
For the follow up visits, 58 care takers were interviewed. Out of which, 86.2% of
children were brought by their mothers and rest by other care takers. Regarding the
distance to the health facilities, 55.2% of the caretakers lived less than 30 minutes
from the HF. In order to get the health services, 13.8% care takers said that they had to
wait for 30 minutes or more in the HF. The reason for going to the particular HF was
75.9% HF being near and 6.9% for availability of quality health service. The presenting
complains of the children coming to the HF were 72.4% fever, 50% difficulty in
breathing, 34.5% diarrhea and 24.1% unable to feed. The various information and
services provided comprised of giving medicines 75.9%, information on breast feeding
58.6%, information on essential new born care 41.1% and information regarding
immunization 39%. For the information provided on danger signs for less than 2
months children, out of 7 under 2 months children, 6 were given information on
danger signs. Based on care takers perspective, 82.8% said that they understood all the
information given by the health workers, 96.6% gave complete course of doses and
98.3% cared their child as advised.
87
Out of 58, 54 (93.1%) were asked for follow up and 56.9% were asked to visit on the
third day and 22.4% on the fifth. When asked, 82.8% said that their child improved
after treatment and the rest 17.2% who did not improve, went to higher facility (8.6%),
consulted to a doctor (5.2%) and consulted private medical shop (6.9%). For the quality
of the services, 84.5% of the care takers were satisfied with the waiting time, 96.6%
were satisfied with the cleanliness of the HF and 89.7% satisfied with privacy of room.
More than 90% were satisfied on the time given and the behavior of HSP and 86.2%
were satisfied on the overall health service.
A total of 61 care takers were interviewed for the exit interview, where 95.1% children
were brought to the HF by the mothers. About 50% lived at a distance of less than 30
minutes and 93.4% of caretakers had to wait only for less than 30 minutes in the HF.
All the caretakers of children <2 months were given information on the danger signs
and 93.1% were asked for further follow up.
Regarding the role of distance in the service provided by FCHVs, 44 (61.2%) of the total
72 FCHVs interviewed lived at a distance of 30 minutes or more to the nearest HF.
About 30 % of them had received training on CB-IMNCI and 42.2 % said that they meet
the mother and the child on the very day of birth for postnatal visit. While the postnatal
visit, 94.4% said they give information about breastfeeding to the mothers, 86.1% said
that they give information about the dangers signs of the newborn and 73.6% on the
danger signs of the mother. Among all the 72 FCHVs, 91.7% said that they usually refer
the patients to the respective HF. The FCHVs provided service as distributing ORS
(91.7%) and distributing zinc tablet (76.4%). Around 42% said that they provided
treatment for ARI/Pneumonia. The reasons for not providing treatment were referring
to the HF nearby (42.8%), medicines not available (21.5%), adviced not to give tab.

88
Cotrim (19%). There was 83.3% stock availability of ORS at present day, 62.5% stock
available for zinc, 50% for chlorhexidine gel and 48.8% paracetamol.
All the FCHVs said they conducted mothers’ group meeting last month and all had
their ward register updated and that they submit the report once a month. The FCHV
were almost (83.3%) satisfied with their role in the CB-IMNCI. The remaining expressed
their need for more training to be conducted for the FCHVs and more availability of
medicines for them to give better services.

89
4. Conclusion and Recommendation An assessment study of the CB-IMNCI program was conducted in six districts namely
Taplejung, Sindhupalchowk, Syangja, Baitadi, Saptari and Nawalprasi. The district focal
person was the first point of contact and health facilities were selected accordingly. A
total of 7 PHCC and 20 HP were visited for assessing service readiness in the health
facilities and knowledge and skills of the HSP regarding the management of sick young
infants. The volume of the services was measured among under 2 months infants and
children aged 2-59 months in the last 3 months and the reasons for low or no service,
recording and reporting mismatch were explored. The perceptions of quality of
services received by the mothers/ care takers during their visit to health facilities and
during follow up visits were explored. The role of FCHVs for the effectiveness of CB-
IMNCI program was assessed.
The findings revealed mismatch between recording and reporting of PSBI, ARI/
Pneumonia, Diarrhea, use of cotrim, amoxicillin, gentamycin, ORS and zinc
distribution. And the reasons for the mismatch were asked in depth, adding to the
significance of recording and reporting of cases/ drugs for further planning. Similarly,
the study also found that there is a discrepancy in knowledge of HSPs and recording
system. Hence, health workers should give attention on proper recording and reporting
practice.
The findings also showed that only 15 PSBI cases were treated in 9 helath facilities. The
reason for less PSBI cases treated is that no cases were brought to the health facilities.
The reason for not bringing cases to the health facility was mothers/ caretakers prefer
their newborns to take private clinics. Therefore, it would be better if Government of
Nepal bring private clinics into the CB-IMNCI policy and strategy.

90
Out of 68 health workers interviewed, it was found that 64.7% had actually received
training on CB-IMNCI, depicting the fact that 35% of the health workers providing CB-
IMNIC services were in need of training. In addition, the findings also showed that only
30.6% of total 72 FCHVs had received training on CB-IMNCI. The findings suggested
that there is requirement of CB-IMNCI training among the service providers, health
workers and FCHVs.
More than 30% of health facilities experienced stock out in last 3 months for essential
CB-IMNCI drugs. Similarly, more than 20% of health facilities did not have Inj.
gentamycin antibiotics which suggested that there is a dire requirement of
improvement of drug supply chain and logistic strengthening.
During follow up visit, it was difficult to find sick children by their names only. It would
be better if the name of mother/ caretaker is included in the register.

91
Bibliography
Ministry of Health and Population. Annual Report 2071/72 (2014/2015). Departmen of Health Services, Kathmandu, Nepal, 2016
MOHP and New ERA. Nepal Demographic and Health Survey (NDHS) 2011. Ministry of Health and Population, New Era, and ICF International, Calverton, Maryland, 2011
Evaluation report of the Integrated Management of Childhood Illness (IMCI) strategy in the District of Kirehe, Eastern Province in Rwanda, November 2008
WHO Ghana. IMCI Documentation : Experiences, Progress and Lessons Learnt, WHO Ghana Report, May 2004
USAID. Quality Assurance Project . Assessing Health Worker Performance of IMCI in Kenya;, 2000
WHO. Health Facility Survey- Tool to evaluate the quality of care delivered to sick children attending outpatients facilities using IMCI clinical guideliness as best practice, Family and Community Health Cluster, 2003
MoHP / DoHS CB-IMCI FCHV training manual 2069
Murray J, Manoncourt S. Integrated Health Facility Assessment Manual: Using Local Planning to Improve the Quality of Child Care at Health Facilities, 1998
UNICEF / Solutions consultant Pvt.ltd. Survey on Assessing Effectiveness of CB-IMCI program: Comparative Study in Kaski and Tanahu Febreaury 2004,
MoHP / DoHS / CHD , CBIMNCI Treatment chart booklet 2071.
WHO. National Health Facility Survey on the quality of Outpatient Primary Child Healthcare service: IMCI Health Facility Survey, Morocco.2007
MoHP/ DoHS / CHD. CB-IMCI Annual Report 2005-2006
Development of Integrated Management of Childhood Illness ( IMCI) in Nepal ( June 1995 – June 2002

92
ANNEX
Annex 1. District selection
CB-IMNCI Sample Distrct Selection
Sn.
Ecological
Zone
CBIMNCI Covered
GoN and Partners
CBNCP Covered
PSBI Perfoma
nce
CBIMNCI Implementa
tion
CBNCP / Non
CBNCP]
1 Mountain Taplejung
Suaahara/USAID Taplejung 3.57 2nd Phase
2 Mountain
Sankhuwashabha
Suaahara/USAID
Sankhuwasabha 14.50 2nd Phase
3 Mountain Solukhumbu GoN 2nd Phase
4 Mountain Dolakha
Suaahara/USAID 2.83 2nd Phase
5 Mountain
Sindhupalchowk GoN* 2.34 2nd Phase
6 Mountain Rasuwa SCF 4.04 1st Phase
7 Mountain Manang GoN 2nd Phase
8 Mountain Mustang GoN 2nd Phase
9 Mountain Dolpa UNICEF Dolpa 2nd Phase
10
Mountain Jumla UNICEF Jumla 18.66 2nd Phase
11
Mountain Kalikot UNICEF 28.33 2nd Phase
12
Mountain Humla UNICEF Humla 14.60 2nd Phase
13
Mountain Mugu UNICEF Mugu 18.44 2nd Phase
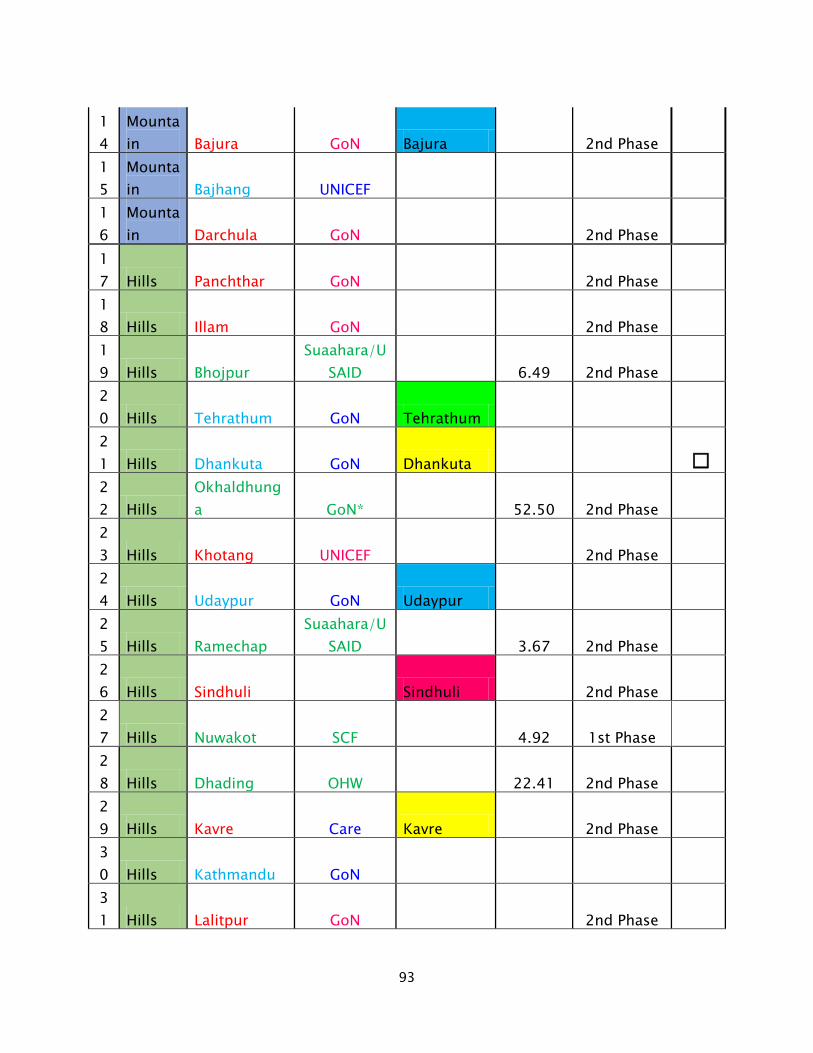
93
14
Mountain Bajura GoN Bajura 2nd Phase
15
Mountain Bajhang UNICEF
16
Mountain Darchula GoN 2nd Phase
17 Hills Panchthar GoN 2nd Phase 18 Hills Illam GoN 2nd Phase 19 Hills Bhojpur
Suaahara/USAID 6.49 2nd Phase
20 Hills Tehrathum GoN Tehrathum 21 Hills Dhankuta GoN Dhankuta 22 Hills
Okhaldhunga GoN* 52.50 2nd Phase
23 Hills Khotang UNICEF 2nd Phase 24 Hills Udaypur GoN Udaypur 25 Hills Ramechap
Suaahara/USAID 3.67 2nd Phase
26 Hills Sindhuli Sindhuli 2nd Phase 27 Hills Nuwakot SCF 4.92 1st Phase 28 Hills Dhading OHW 22.41 2nd Phase 29 Hills Kavre Care Kavre 2nd Phase 30 Hills Kathmandu GoN 31 Hills Lalitpur GoN 2nd Phase

94
32 Hills Bhaktapur GoN 2nd Phase 33 Hills Makwanpur Makwanpur 2nd Phase 34 Hills Gorkha GoN 2nd Phase 35 Hills Lamjung GoN Lamjung 36 Hills Tanahu GoN 37 Hills Kaski GoN 1.00 2nd Phase 38 Hills Syangja GoN 1.09 2nd Phase 39 Hills Myagdi
Suaahara/USAID Myagdi 11.61 2nd Phase
40 Hills parbat GoN 2nd Phase 41 Hills Baglung GoN Baglung 42 Hills
Arghakhanchi GoN
Arghakhanchi 2nd Phase
43 Hills Gulmi GoN 7.58 2nd Phase 44 Hills Palpa
Suaahara/USAID Palpa
45 Hills Rukum GoN 21.46 2nd Phase 46 Hills Rolpa GoN 2nd Phase 47 Hills Pyuthan JSI / USAID Pyuthan 2nd Phase 48 Hills Salyan GoN Salyan 49 Hills Surkhet GoN 31.13 2nd Phase

95
50 Hills Dailekh
Suaahara/USAID Dailekh
51 Hills Jajarkot
ADRA /GoN* 39.86 2nd Phase
52 Hills Accham GoN 32.52 2nd Phase 53 Hills Doti GoN Doti 24.10 2nd Phase 54 Hills Baitadi GoN Baitadi 15.73 2nd Phase 55 Hills Dadeldhura Care Dadeldhura 70.08 2nd Phase 56 Terai Jhapa GoN 2nd Phase 57 Terai Morang PLAN * Morang 69.00 2nd Phase 58 Terai Sunsari PLAN * Sunsari 32.52 2nd Phase 59 Terai Saptari UNICEF 5.39 2nd Phase 60 Terai Siraha GoN 61 Terai Dhanusha GoN 7.29 2nd Phase 62 Terai Mohattari SCF Mohattari
63 Terai Sarlahi UNICEF Sarlahi 2nd Phase 64 Terai Chitwan GoN Chitwan 2nd Phase 65 Terai Parsa GoN Parsa 66 Terai Bara GoN Bara 67 Terai Rautahat Rautahat 2nd Phase

96
68 Terai Nawalparasi SCF
Nawalparasi 13.29 1st Phase
69 Terai Rupandehi JSI / USAID Rupandehi 2nd Phase 70 Terai Kapilbastu GoN Kapilbastu 71 Terai Dang GoN Dang 2nd Phase 72 Terai Banke Banke 2nd Phase 73 Terai Bardiya SCF Bardiya 74 Terai Kailali SCF Kailali 2nd Phase 75 Terai Kanchanpur GoN Kanchanpur 2nd Phase 75 39
Annex 2. Detail field plan and facility allocation to each field reasearchers
ll
Sn.
Distrcts
Disctrict
Focal Person IMNCI
HF survey/ Observatio
n
Service Providers
/ SBA interview
FCHV
FU Visits
Exit Interview
s
Total
1 Taplejung 1 6 12 12 12 12 55
2 Sindhupalchowk 1 6 12 12 12 12 55
3 Syangja 1 6 12 12 12 12 55 4 Baitadi 1 6 12 12 12 12 55 5 Saptari 1 6 12 12 12 12 55 6 Nawalparasi 1 6 12 12 12 12 55
Total 6 36 72 72 72 72 330

97
Sn. Distrcts Name of
Enumerator Tel.No
1 Taplejung Subhash Lamichane 9849093447
Bishnu Patel 9845425868
2 Sindhupalchowk Bhim Prasad Shrestha 9841802157
Thuma Rawat 9848186800
3 Syangja Kristina Parajuli 9841411038 Surakhsha Sharma 9843692061
4 Baitadi Usha Singh 9861538491 Sujata Gurung 9800913169
5 Saptari
Divya Laxmi Devkota 9849197719
Rukmani Chaudhary 9841539875
6 Nawalparasi Bhawana Bhandari 9868214062 Alina Rai 9808936856
Replacement
Dr. Nisha Manandhar 9841857333
Rajendra Khatri 9841180963 Total

98
Annex 3. Training schedule
Assessment of Community – Based Integrated Management of Neonatal and Childhood Illness (CB-IMNCI) Program
Training Program
(CHD/WHO/NDRI, December 2016)
(Venue: Training Hall NDRI, Hall , Pulchowk , Lalitpur )
DATE TIME SN. ACTIVITIES RESPONSIBLE
DAY 1
Wednesday, 21 Dec. 2016
08.30 – 09.00
1. Registration All Participants
09.00 – 09.10
2. Introduction All Participants
09.10 – 09.20
3. Welcome Speech Dr. Jaya Kumar Gurung
09.20 – 10.00
4. Introduction CB-IMNCI Bhim Prasad Shrestha
10.00 – 10.20
5. Objectives of data collection
Bhim Prasad Shrestha
10.20 – 11.00
6. Sample Size & Methodology
Rajendra Khatri
11.00 – 11.30
7. Data and Interview Bhim Prasad Shrestha
11.30 – 12.30
8. District level Focal Person Interview discussion
Dr. Nisha Manadhar Kunwar
12.30 – 13.30
9. Lunch Break
13.30 – 16.40
10. Health Facilities Survey / Observation
Usha Singh , Kristina Parajuli and Bhim P. Shrestha
16.40 – 17.00
11. Re cape of Day I Dr. Nisha Manandhar Kuwar
08.30 – 09.00
1. Registration All Participants

99
DAY 2
Thursday , 22
Dec. 2016
09.00 – 09.15
2. Review of the day 1 Dr. Nisha Manandhar Kunwar
09.15 – 09.45
3. Service Providers/ SBA / HP in-charge
Bhim Prasad Shrestha
12.00 – 12.30
4. In- depth-Interview – ( Service providers/SBA)
Bhim Prasad Shrestha
12.30 – 13.30
5. Lunch
13.30 – 15.00
6. In- depth-Interview – ( Service providers/SBA)
Kristina Parajuli
15.00 – 16.50
7. FCHV Interview Usha Singh
16.50 – 17.00
8. Pretest notice Rajendra Khatri
DAY 3 Pretest
Friday, 23 Sep. 2016
09.00 – 09.15
1. Registration All Participants
09.15 – 15.00
2. Pre-test ( in different Health Facilities)
All Participant
15.00 – 16.30
3. Discussion - Pretest All Participant , Finalizing tools
DAY 4 Saturday,
24 Sep. 2016
09.30 – 10.00
1. Registration All Participants
10.00 – 12.30
2. Exit interview / Follow up
Dr. Nisha Manadhar Kunwar
12.30 – 13.30
3. Lunch
13.30 – 14.00
4. Role Play All participiants
13.31 – 14.00
5. District Allocation Rajendra Khatri

100
14.00 – 14.20
6. Admin and Financial Manisha Raymajhi / Rajendra Khatri
14.20 – 15.20
7. Other preparation

101
Annex 4. Final questionnaire for the survey
dGh'/L
gd:t], d]/f] gfd ………………………………………………xf] . :jf:Yo dGqfno÷ljZj :jf:Yo ;+u7g÷Save the Children÷g]=lj=c=k|=4f/f ;+o'St ?kdf ;+rflnt CB-IMNCI sfo{s|dsf] cWoogdf d sfo{/t 5' . PHCC, HP / ;d'bfo:t/df aRrf / gjhft lzz'sf] Joj:yfkg nufot pkof]u / u'0f:t/sf] :t/ / ARI, kvfnf, PSBI s]lGb«t ltgsf k|efljt sf/sx?sf] jt{dfg cj:yf lgwf{/0f ug'{ o; cWoogsf] p2]Zo /x]sf] 5 .
xfdL cfk"lt{ Joj:yfkg -Logistics management_, lgl/If0f, ;dGjosfo,{ cg'udg tyf d'Nof+sg, CB-IMNCI sfo{s|dsf] /]sl8{ª / l/kf]l6{ª 6'n h:tf CB-IMNCI ;DalGwt ;Dk'0f{ hfgsf/L lbg ;Sg] lhNnf CB-IMNCI Focal Personsf] cGtjf{tf lng rfxG5f} . xfdL o; cGtjf{tfnfO{ cufl8 a9\g cf}krfl/s ;xdlt rfxG5f}+ .
tkfO{n] lbg' ePsf] hfgsf/L uf]Ko /flvg]5 / s]an kl/of]hgf ljZn]if0fsf nflu dfq k|of]u ul/g]5 . o; sfo{s|dsf nflu xfdLnfO{ ;xof]u ug'{x'g] JolSt tyf ;3+;+:yfk|lt :jf:Yo dGqfno÷ljZj :jf:Yo ;+u7g÷Save the Children÷g]=lj=c=k|= xflb{s s[t¡ftf k|s6 ub{5 . tkfO{sf] ;xeflutf :j}lR5s (Voluntarily) x'g]5 / olb tkfO{n] efu lng grfx]df glng ;Sg' x'g]5 / o;n] s'g} c;/ ug]{ 5}g . olb tkfO{ ;xdt x'g'x'G5 eg] s[kof ;lx ul/lbg'xf]nf .
s] d cGtjf{tf ;'? ug]{ cg'dlt kfpg ;S5' <
5 ====================
5}g ==================
pQ/bftfsf] x:tfIf/ ldlt
;d'bfodf cfwfl/t gjhft tyf afn/f]usf] Plss[[t Joj:yfkgsf] d'Nof+sg cWoog
@)&#÷&$
:jf:Yo dGqfno÷ljZj :jf:Yo ;+u7g÷Save the Children÷g]=lj=c=k|=
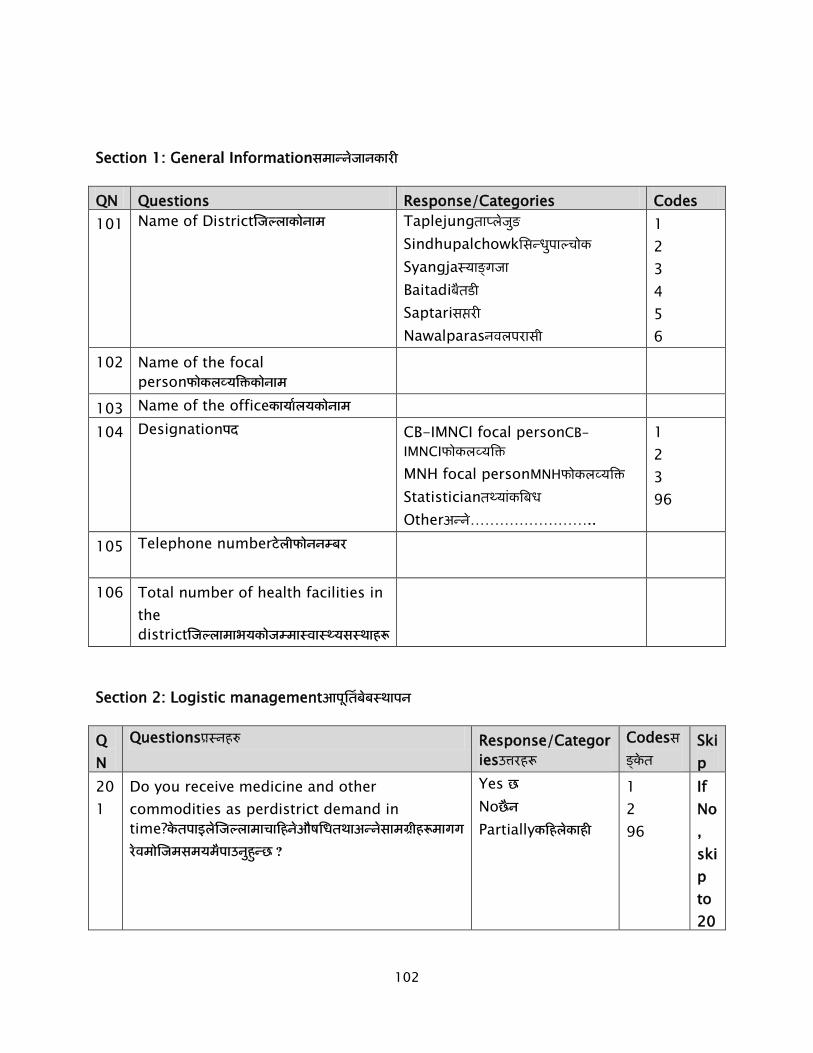
102
Section 1: General Information
QN Questions Response/Categories Codes 101 Name of District Taplejung
Sindhupalchowk Syangja Baitadi Saptari Nawalparas
1 2 3 4 5 6
102 Name of the focal person
103 Name of the office 104 Designation CB-IMNCI focal personCB-
IMNCI MNH focal personMNH Statistician
Other ……………………..
1 2 3 96
105 Telephone number
106 Total number of health facilities in the district
Section 2: Logistic management
QN
Questions Response/Categories
Codes
Skip
201
Do you receive medicine and other commodities as perdistrict demand in time?
Yes
No Partially
1 2 96
If No, skip to 20
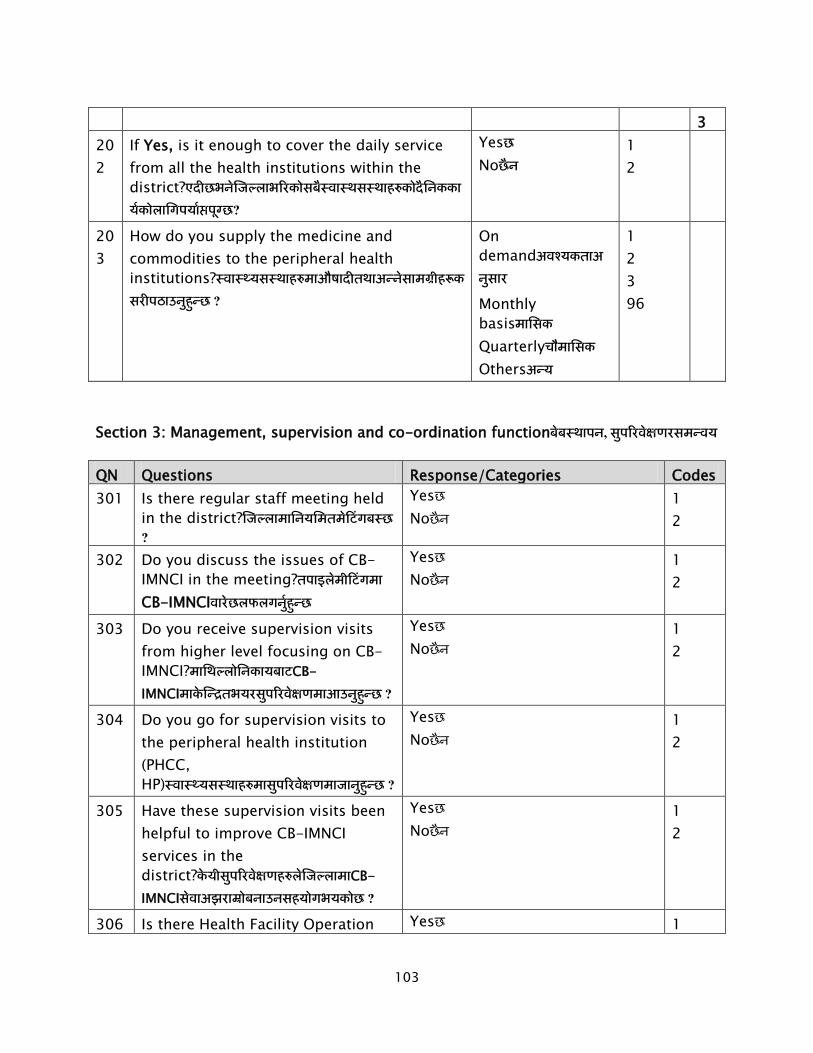
103
3 202
If Yes, is it enough to cover the daily service from all the health institutions within the district?
Yes No
1 2
203
How do you supply the medicine and commodities to the peripheral health institutions?
On demand
Monthly basis Quarterly Others
1 2 3 96
Section 3: Management, supervision and co-ordination function
QN Questions Response/Categories Codes 301 Is there regular staff meeting held
in the district?
Yes No
1 2
302 Do you discuss the issues of CB-IMNCI in the meeting? CB-IMNCI
Yes No
1 2
303 Do you receive supervision visits from higher level focusing on CB-IMNCI? CB-IMNCI
Yes No
1 2
304 Do you go for supervision visits to the peripheral health institution (PHCC, HP)
Yes No
1 2
305 Have these supervision visits been helpful to improve CB-IMNCI services in the district? CB-IMNCI
Yes No
1 2
306 Is there Health Facility Operation Yes 1

104
and Management Committee (HFOMC) in all HF?
No Don't know
2 98
Section 4: Monitoring and evaluation
QN. 401: What are the activities do you do for strengthening the CB-IMNCI program?CB-IMNCI
......................................................................................................................................
......................................................................................................................................
......................................................................................................................................
......................................................................................................................................
......................
QN. 402: How do you monitor the CB-IMNCI program?CB-IMNCI
......................................................................................................................................
......................................................................................................................................
......................................................................................................................................
......................................................................................................................................
.....................
QN. 403: What are the new things that you do for assessing CB-IMNCI program?CB-IMNCI
......................................................................................................................................
......................................................................................................................................
......................................................................................................................................
......................................................................................................................................
......................
QN. 404: How do you evaluate the CB-IMNCI program? CB-IMNCI

105
......................................................................................................................................
......................................................................................................................................
......................................................................................................................................
......................................................................................................................................
......................
Section 5: Recording and reporting tools
QN
Questions Response/Categories Codes
501
Does the copies of HMIS user manuals available?HMIS ?
Yes No
1 2
502
Did you have adequate supply of HMIS tool/ form and formats for supplying to the health institutions? HMIS
Yes No
1 2
503
Are all staff involved in CB-IMNCI oriented on HMIS tools?CB-IMNCI
HMIS
Yes No
1 2
504
Is there timely reporting from the health facilities?
Yes No
1 2
505
What are the number of health facilities that did not report PSBI cases among young infants (0-2 months) in the last fiscal year? PSBI
………………………………………………..
506
If many, why so many health facilities of the district did not report PSBI cases among young infants in the last fiscal year? PSBI
…………………………………………………
50 What are the measures taken to improve …………………………………

106
7 recording and reporting of PSBI cases?PSBI
…………..... ………………………………………………… …………………………………………………
Section 6: Need for improvement
What are the most priority issues you want to address immediately so that service availability and quality of CB-IMNCI services can be improved in your district?
CB-IMNCI
......................................................................................................................................
......................................................................................................................................
......................................................................................................................................
......................................................................................................................................
......................................................................................................................................
.................................................

107
dGh'/L
gd:t], d]/f] gfd ………………………………………………xf] . :jf:Yo dGqfno÷ljZj
:jf:Yo ;+u7g÷Save the Children÷g]=lj=c=k|=4f/f ;+o'St ?kdf ;+rflnt CB-IMNCI d'NofGsg
sfo{s|dsf] cWoogdf d sfo{/t 5' . PHCC, HP / ;d'bfo:t/df aRrf / gjhftlzz'sf] Joj:yfkg
nufot pkof]u / u'0f:t/sf] :t/ / Zjf;g ;+s|d0f, kvfnf, PSBI s]lGb«t ltgsf k|efljt sf/sx?sf]
jt{dfg cj:yf lgwf{/0f ug'{ o; cWoogsf] p2]Zo /x]sf] 5 .
xfdL :jf:Yo ;+:yfdf pknJw;]jf, pks/0f dfgj ;+dzfwg cf}iflw / CB-IMNCI lgb{]lzsf / IEC/BCCaf/]
cjnf]sg /cGtjf{tf lng rfxG5f}+ . xfdL yk hfgsf/L klg lbg]5f}+ / cufl8 a9\g cf}krfl/s ;xdlt rfxG5f}+ .
tkfO{4f/f k|bfg ul/Psf hjfkm uf]Ko /flvg]5 / s]an kl/of]hgf ljZn]if0fsf nflu k|of]u ul/g]5 . o; sfo{s|dsf nflu xfdLnfO{ ;xof]u ug'{x'g] JolSt tyf ;3+;+:yfk|lt :jf:Yo dGqfno xflb{s s[t¡ftf k|s6 ub{5 . tkfO{sf] ;xeflutf :j}lR5s 5 / olb tkfO{ efu lng grfx]df o:sf] s]lx kl/0ffd x'g] 5}g . tkfO{sf] a'´fO{ / ;xdltnfO{ hgfpg oxfF hgfOPsf] 5 .
s] d cGtjf{tf ;'? ug]{ cg'dlt kfpg ;S5' <
5 ……………………………………..
5}g ……………………………………..
pQ/bftfsf] x:tfIf/ ldlt
;d'bfodf cfwfl/t gjhft tyf afn/f]usf] Plss[[t Joj:yfkgsf] d'Nof+sg cWoog
@)!^÷!&
:jf:Yo dGqfno÷ljZj :jf:Yo ;+u7g÷Save the Children÷g]=lj=c=k|=

108
v08 !: :jf:Yo ;'ljwfsf] ;fdfGo hfgsf/L k|Zg.g+. klxrfg ljj/0f k|ltls|of/ljefu sf]8 5f]8\g]
!)! lhNnfsf] gfd Tffkn]h'g l;Gw'kfNrf]s :ofGemf a}6l8 ;ktl/ gjnk/fl;
! @ # $ % ^
!)@ Uff= lj= ;/ gu/kflnsf !)# j8f gDa/ !)$ :jf:Yo ;+:yfsf] gfd !)% :jf:Yo ;+:yfsf] k|sf/ k|fylds :jf:Yo pkrf/ s]Gb|
:jf:Yo rf}sL !
@
!)^ :jf:Yo ;+:yfdf sfd ug{] sd{rf/Lsf] ;+Vof :jf:Yo ;xfos................................... :6fkm g;{................................. c= x]= j =............................... c=g= ld............................. c?..........................................
!)& k|ltjflbsf] gfd
!)* k|ltjflb OGrfh{ xf] ls xf]Og? xf] xf]Og
! @
!)( k|ltjflbsf] kb d]l8sn clws[t :jf:Yo ;xfos(HA) :6fkm g;{ jl/i7 c= x]= j jl/i7 c=g= ld c= x]= j c=g= ld c? (lglb{i6)…………………….
! @ # $ % ^ & (^
!!) :jf:Yo ;'ljwf lbg] OGrfh{sf] gfd !!! :jf:Yo ;+:yfsf] 6]lnkmf]g gDa/

109
v08 @: ;]jfsf] pknAwtf
k|Zg.g+. ;]jf k|ltls|of/ljefu sf]8
@)! Birthing Centrea/lyË ;]G6/ 5 5}g
s'g} ;]jf 5}g ;fGble{s 5}g
! @ * (
@)@ gahft l;;' sIfsf] ;fy l/;l:6];g 6]an
Newborn corner with a resuscitation table
5 5}g
s'g} ;]jf 5}g ;fGble{s 5}g
! @ * (
@)# CB-IMNCI 5 5}g
s'g} ;]jf 5}g ;fGble{s 5}g
! @ * (
@)$ PNC 5 5}g
s'g} ;]jf 5}g ;fGble{s 5}g
! @ * (
v08 #: pks/0f pknAwtfAvaibility of Equipment
k|Zg.g+. pks/0f sfd ug{] xf] sfd
gug{] 5}g
;fGble{s
5}g
#)! Birthing Centre ;fN6/ :s]n ! @ # $
#)@ Pan scaleKofg :s]n ! @ # $
#)# Mercury Thermometer d/s/L ydf{dL6/ ! @ # $
#)$ Digital Thermometerl8lh6n ydf{dL6/ ! @ # $
#)% Stethoscope:6]yf]:sf]k ! @ # $
#)^ BP instrumentaLlk ;fwg ! @ # $
#)& ARI Timer P Pf/ cfO{ 6fO{d/ ! @ # $

110
k|Zg.g+. pks/0f sfd ug{] xf] sfd
gug{] 5}g
;fGble{s
5}g
#)* Penguink]+u'Og/ Delee suction lbn];S;g ! @ # $
#)( Newborn Bag and Maskgjhftsf] Jofu PG8
df:s
! @ # $
v08 $: dfgj ;+dzfwgHuman Resource
k|Zg.g+. k|Zg
$)! slt hgf sd{rf/Ln] tflnd lnPsf
5g\:
CBIMNCI CBIMCI CBNCP SBA Revised HMIS
$)@ slt hgf sd{rf/Ln]CB IMNCI
;'ljwfdf ;]jf k|wfg ub{5g\?
$)# cfh slt hgf sd{rf/Ln]CB IMNCI
;'ljwfdf ;]jf k|wfg ul//x]sf 5g\?

111
v08 %: cf}ifw / ;/;fdfgDrugs and Commodities
k|Zg.g+. cf}ifw/;/;fdfg
jt{dfg l:ylt
kl5Nnf] # dlxgf :6s ;lsP
sf] cg'ej
]5, sDtLdf lg Ps rf]6L
5, sDtLdf lg Ps dlxgf(EOP1
5}g
)
5 5}g
%)! ORS packets ! @ # ! @
%)@ Cotrimoxazole tablets (P) 250mg ! @ # ! @
%)# Vitamin A Capsule ! @ # ! @
%)$ Albendazole 400 mg ! @ # ! @
%)^ Amoxicillin Tablets 250 mg ! @ # ! @
%)& Metronidazole 200 mg ! @ # ! @
%)* Paracetamol 500 mg ! @ # ! @
%)( Gentamycin Injection ! @ # ! @
%!) Zinc Tablets ! @ # ! @
%!! Chlorhexidine gel ! @ # ! @
%!@ Dexamethosone injection 4 mg/ml in 1 ml ! @ # ! @
%!# Salbutamol ! @ # ! @
%!$ Inj. R/L ! @ # ! @
%!% Inj. N/S ! @ # ! @
%!^ Syringe
1 EOP – Emergency Order Point which means the HF has to have one month stock.

112
v08 ^:lgb{]lzsfpknlJw/IEC/BCC ;fdfu|LGuidelines/IEC/BCC Materials
k|Zg.g+. lgb{]lzsf/IEC/BCC ;fdfu|L
5 5}g
^)! CB-IMNCI Guideline lgb{]lzsf ! @
^)@ @ b]lv % aif{sf afnaflnsfnfO{ {CB-IMNCI sf8{ ! @
^)# CBNCP sf8{ FCHVsf] nfuL ! @
^)$ Cotrim Dose sf8{ ! @
^)% { Home Therapy Card for ARI casesxf]d y]/fkL sf8{ ! @
^)^ lh+s k/fdz{ sf8{ ! @
^)& HMIS 2.41 (@ dlxgf b]lv %( dlxgf) ! @
^)* HMIS 2.42 (@ dlxgf eGbf a9L) ! @
v08 &:HMISdf /]s8{ ug{]
cg';Gwfgstf{x?n] kl5Nnf] % a6f P= cf/= cfO(ARI)/ lgdf]lgof (Pneumonia)/ emf8fkvfnf
(Diarrhea)/ @ a6f lk= P;= lj= cfO (PSBI)caseHMISkmf/d 2.41/ HMIS 2.42df /]s8{ ul/Psf] ÷
gul/Psf] cfjnf]sg ug{] .
jf8{sf] hfgsf/L ug{, cg';Gwfgstf{x?n] df:6/ /]lh:6/ 6«ofs (Master register
tracking) ;Fu Pd= cf/= Pg= sf]8 (MRN)sf] x]g'{ kg{} 5 .
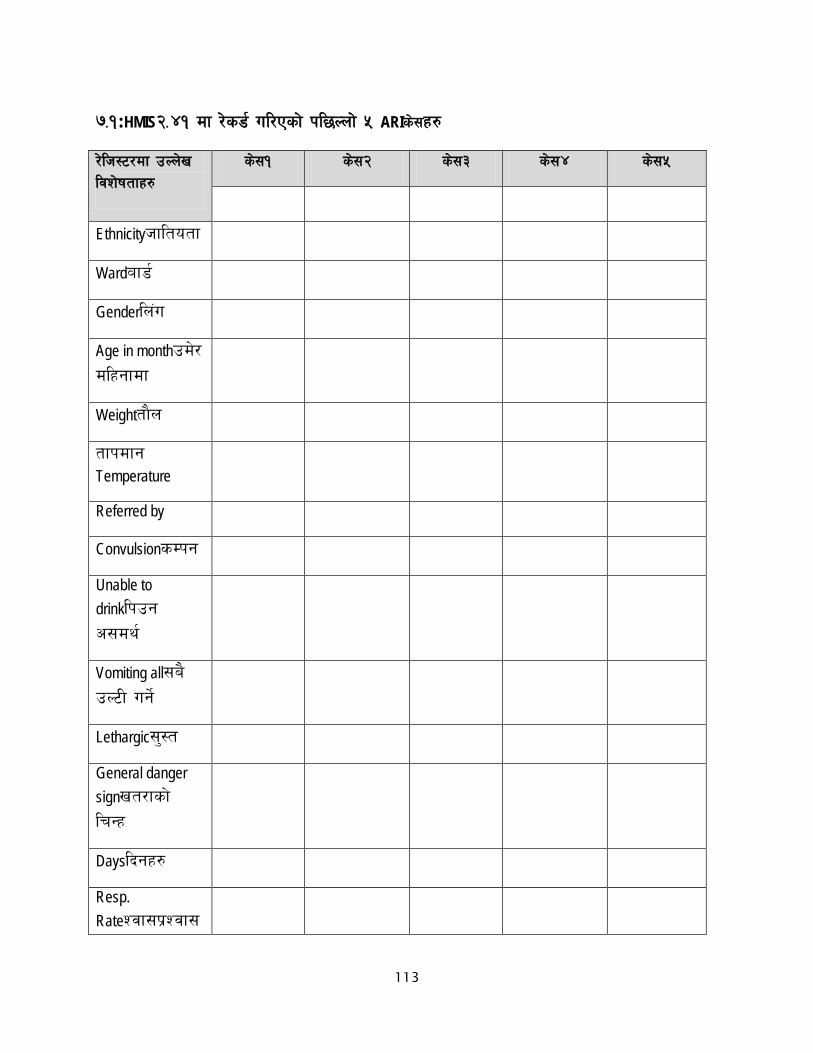
113
&=!:HMIS@=$! df /]s8{ ul/Psf] kl5Nnf] % ARIs];x?
/]lh:6/df pNn]v ljz]iftfx?
s];! s];@ s];# s];$ s];%
Ethnicityhfltotf
WardJff8{
Genderln+u
Age in monthpd]/ dlxgfdf
WeightTff}n
Tffkdfg Temperature
Referred by
ConvulsionsDkg
Unable to drinklkpg c;dy{
Vomiting all;a} pN6L ug{]
Lethargic;':t
General danger signvt/fsf] lrGx
Dayslbgx?
Resp. RateZjf;k|Zjf;

114
b/
Chest in drawingsf]vf xfGg]
Stridor :6«fO8/
Major Classificationk|d'v juL{s/0f
NumbergDa/
ICD codecfO{l;l8 sf]8
Medicinecf};lw
Counseling k/fdz{
Referred to
Follow up kmnf]ck

115
&=@:kl5Nnf] % HMIS @=$! df /]s8{ ul/psf] Diarrheas];x?
laz]iftfx? s]; ! s]; @ s]; # s]; $ s]; %
Ethnicityhfltotf
WardJff8{
Genderln+u
Age in monthdlxgfdf pd]/
Weightjhg
TemperatureTffkdfg (C)
Referred by
sDkg
lkpg c;dy{
;a} pN6L ug{]
;':t
vt/fsf] lrGx
/ut
lkGr]Irritable
cfFvf
u9\g'Sunken Eyes
lkpg c;dy{

116
;fdfGotf k]oDrinks Normally
k]6sf] 5fnf cf}+nfn] tfg]/ 5f]8\8f la:tf/} kmls{g]
k]6sf] 5fnf cf}+nfn] tfg]/ 5f]8\8f w]/} la:tf/} kmls{g]
emf8fkvfnf
k|d'v juL{s/0f
gDa/
ICD sf]8
cf};lw
k/fdz{
Referred to
Follow Up

117
&=#:kl5Nnf] HMIS@=$@ df /]s8{ ul/sf] @ PSBIs];x?
laz]iftfx? s];! s]; @
Hfltotf Ethnicity
Jff8{
ln+u
xKtfdf pd]/
jhg
Tffkdfg (C)
Referred By
sDkg Convulsion
Zjf;k|Zjf; b/Respiratory Rate
sf]vf xfGg] Chest Indrawing
gfssf] kf]/f km'Ng]
Tffn' pS;]sf]
gfO6f]sf] /ftf]kg
5fnf, gfO6f] ;ªs|d0f
tfkdfg>37.5
tfkdfg <35.5
v'jfpg c;dy{

118
5fnfsf] kmf]sf -!) eGbf sd_
5fnfdf w]/} kmf]sfx?!) eGbf a9L
;':t/ a]xf]z
;fdfGo rng
;fdfGo eGbf sd rng
k|d'v juL{s/0f
gDa/
ICD sf]8
cf};lw
k/fdz{Counselling
Referred To
Follow Up
v08 *:cg';Gwfgstf{x?n] dflysf] /]sl8{ªdf cfwfl/t k|Zgx? pTkGg ug{'kg]{5, / ;]jfug{]
sfo{df ;f]wk'5 ug{'kg{] 5 .
k|Zg=g+= klxrfg ljj/0f k|ltls|of/ljefu sf]8 *)! PSBI s];x?df
rnfO{PsfInjectionGentamycinsf;a} Dose/lh;6df /]s8{ ul/Psf] 5?
5 5}g
! @
*)@
olb ;a} 8f]h /]s8 5}g eg], lsg /lh:6/df ;a} 8f]hx? /]s8{ gug{' ePsf]?

119
Health Service Provider Interview
:
Medical Officer
HA SN
Sr AHW
CB-IMNCI
……………………….
CB-IMCI CB NCP CB IMNCI

120
:
Count respiratory rate
Listen to breathing
Assess child
movement/consciousness
Respiratory rate timer
Stethoscope
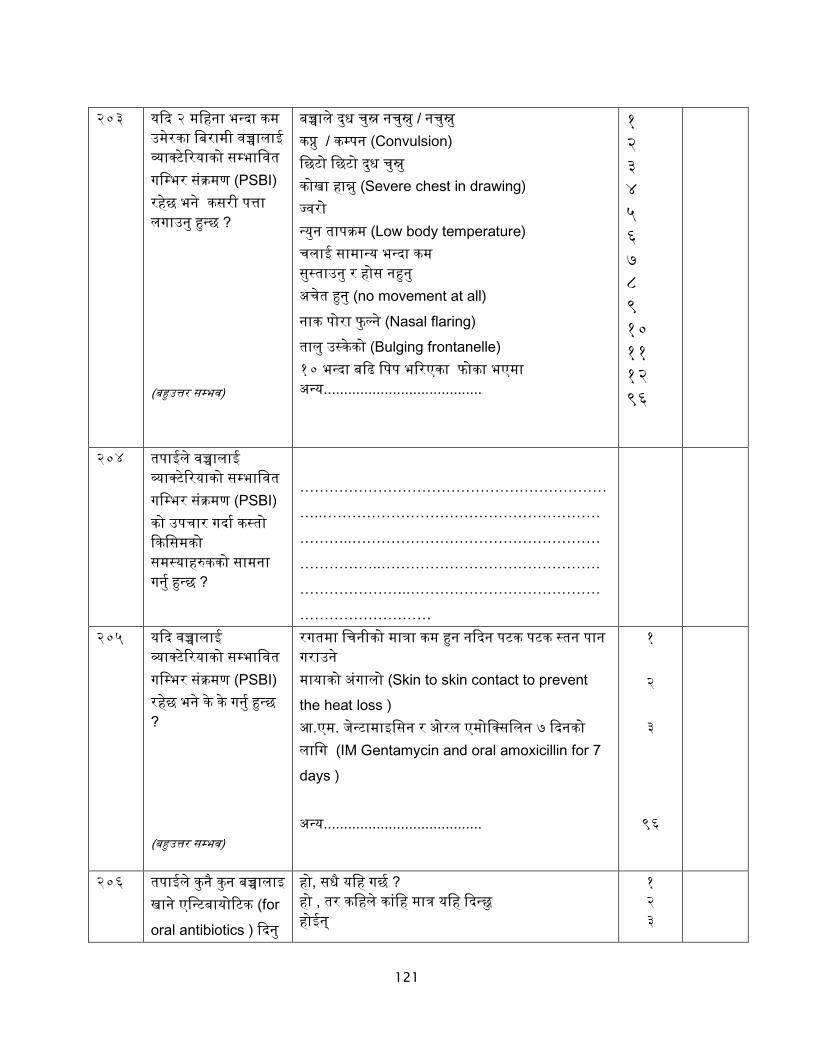
121
PSBI
Convulsion
Severe chest in drawing
Low body temperature
no movement at all Nasal flaring
Bulging frontanelle
PSBI
…………………………………………………………..…………………………………………………………..…………………………………………………………..…………………………………………………………..…………………………………………………………
PSBI
Skin to skin contact to prevent
the heat loss
IM Gentamycin and oral amoxicillin for 7 days
for
oral antibiotics

122
-
injectable antibiotic
Ampicillin Gentamicin
Penicillin
………………………………………………………………………………………………………………………………………………………………………………………
<
………………………………………………………………………………………………………………………………………………………………………………………
PSBI
-
(IM)Give first dose of gentamicin (IM) and ampicillin (IM)

123
PSBI
PSBI
……………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………
LBI
LBI
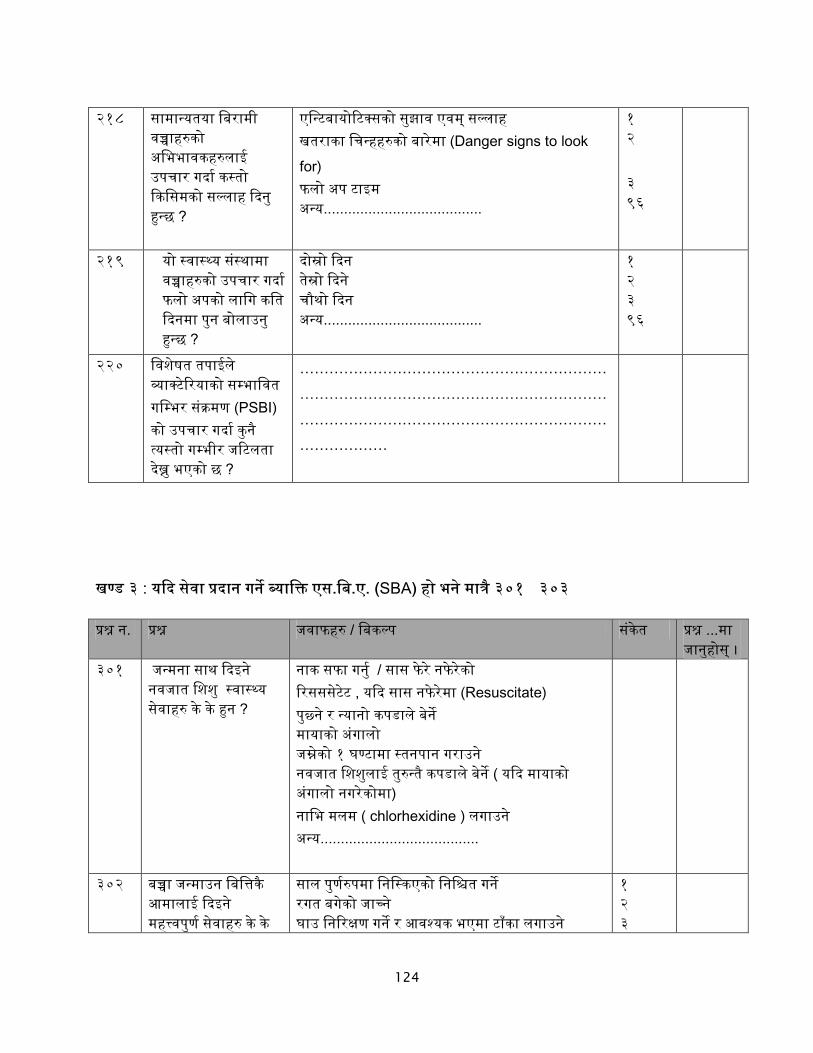
124
Danger signs to look
for
PSBI
………………………………………………………………………………………………………………………………………………………………………………………
: SBA
Resuscitate
chlorhexidine
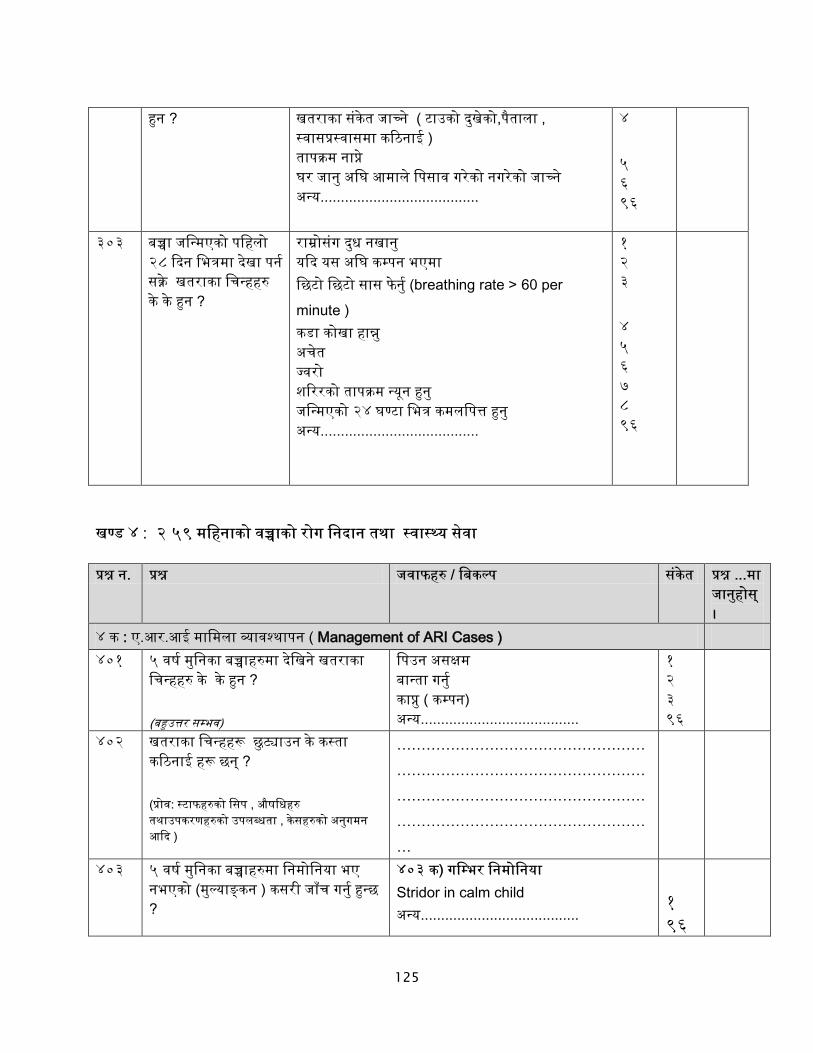
125
breathing rate > 60 per minute
:
: Management of ARI Cases )
………………………………………………………………………………………………………………………………………………………………………………………
Stridor in calm child

126
Prompt for
classification
………………………………………………………………………………………………………………………………………………….
x x (if
wheezing also)
x (if wheezingpresent )
………………………………………………
Prompt for classification
……………………………………………….. ……………………………………………………………………………………………….

127
: Management of Diarrheal Case
)
)
)
1 2 96 1 96 1 96
………………………………………………………………………………………………………………………………………

128
………………………………………………
)
……………………………
)
…………………………
)
……………………………
………………………………………………………………………………………………………………………………………………………………………………………
:
CB-IMNCI

129
………………………
................................................................... ………………………………………………. ………………………………………………..
:
: CB IMNCI
PSBI
IMNCI
Other register PSBI cases
PSBI IMNCI
IMNCI
IMNCI …............................
PSBI
PSBI

130
PSBI ........................... PSBI
PSBI
….................................
PSBI
PSBI
PSBI …................................
PSBI
.............................................
ARI
IMNCI
Other register PSBI cases
ARI IMNCI
IMNCI
IMNCI …............................
ARI
ARI
ARI
...........................
ARI
ARI

131
….................................
ARI
ARI
…................................
diarrhea
IMNCI
Other register diarrhea cases
diarrhea IMNCI
diarrhea
IMNCI …............................
diarrhea
diarrhea
diarrhea
...........................
diarrhea
diarrhea
….................................

132
diarrhea
…................................
: CB IMNCI
Record
Severe Bacterial infection
Local Bacterial Infection
No. of infants receiving cotrimoxazole
No. of infants receiving first dose of gentamycin
No. of infants receiving complete dose of gentamycin
No. of infants referred
Record

133
ARI/Pneumonia
Severe Pneumonia
Pneumonia
Common cold/ No Pneumonia
Diarrhea
Blood in stool
Persistent diarrhea
Severe dehydration
Some dehydration
No dehydration
Treatment
No. of infants treated with cotrimoxazole
ORS zinc tablets
No. of infants treated with ORS and zinc tablets
ORS
No. of infants treated with ORS
Referral ARI
No. of ARI referred cases
diarrhea

134
No. of diarrhea referred cases
:
:PSBI
:ARI
----------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------
:diarrhea
:ARI
:diarrhea
----------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------

135
:
----------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------
:
----------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------
:
----------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------
:ORS zinc tables
----------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------

136
Exit Interview
dGh'/L
gd:t], d]/f] gfd ………………………………………………xf] . :jf:Yo dGqfno÷ljZj
:jf:Yo ;+u7g÷Save the Children÷g]=lj=c=k|=4f/f ;+o'St ?kdf ;+rflnt CB-IMNCI d'NofGsg
sfo{s|dsf]cWoogdf d sfo{/t 5' . PHCC, HP / ;d'bfo:t/df aRrf / gjhftlzz'sf] Joj:yfkg nufot
pkof]u / u'0f:t/sf] :t/ / Zjf;g ;+s|d0f, kvfnf, PSBI s]lGb«t ltgsf k|efljt sf/sx?sf] jt{dfg
cj:yf lgwf{/0f ug'{ o; cWoogsf] p2]Zo /x]sf] 5 .
xfdL la/fdL lzz'sf] /]vb]v / pgLx?sf] pkrf/df ;+nUg cfdf / ;';f/];Fu cGtjf{tf lng rfxG5f}+ . xfdL yk hfgsf/L klg lbg]5f}+ / cufl8 a9\g cf}krfl/s ;xdlt rfxG5f}+ .
tkfO{4f/f k|bfg ul/Psf hjfkm uf]Ko /flvg]5 / s]an kl/of]hgf ljZn]if0fsf nflu k|of]u ul/g]5 . o; sfo{s|dsf nflu xfdLnfO{ ;xof]u ug'{x'g] JolSt tyf ;3+;+:yfk|lt :jf:Yo dGqfno xflb{s s[t¡ftf k|s6 ub{5 . tkfO{sf] ;xeflutf :j}lR5s 5 / olb tkfO{ efu lng grfx]df o:sf] s]lx kl/0ffd x'g] 5}g . tkfO{sf] a'´fO{ / ;xdltnfO{ hgfpg oxfF hgfOPsf] 5 .
s] d cGtjf{tf ;'? ug]{ cg'dlt kfpg ;S5' <
5 ……………………………………..
5}g ……………………………………..
;d'bfodf cfwfl/t gjhft tyf afn/f]usf] Plss[[t Joj:yfkgsf] d'Nof+sg cWoog
@)&#÷&$
:jf:Yo dGqfno÷ljZj :jf:Yo ;+u7g÷Save the Children÷g]=lj=c=k|=
PSBI-@ dlxgf _ jf emf8fkvfnf jf lgdf]lgofaf6 la/fdL k/]sf % jif{sf d'lgsf lzz'sf
cfdf÷x]/rfx ug{] JolQm;Fusf] Exit Interview

137
k[i7e"ld hfgsf/L
k|Zg ;+Vof k|Zgx? k|ltls|of sf]8 s}lkmot 101 lhNnf tfKn]h'ª 1
l;Gw'kfNrf]s 2 :ofª\hf 3 a}t8L 4 ;Kt/L 5 gjnk/f;L 6
102 :jf:Yo;+:yfsf] gfd
103 :jf:Yo ;+:yfsf] k|sf/ PHCC 1
HP 2
104 lzz'sf] pd]/ @ dlxgf eGbf sd 1 @–%( dlxgf 2
105 /f]usf] k|sf/ PSBI 1 emf8fkvfnf 2 P=cf/=cfO=÷lgdf]lgof 3
106 lzz'sf] x]/rfO ug{] JolQmsf] gfd
107 lzz'sf]] x]/rfO ug{] JolQmsf] pd]/
jif{
108 lzz'sf] x]/rfO ug{] JolQmsf] hfltotf
blnt 1 hghflt 2 dw];L 3 d'l:nd 4 a|flXd0f÷If]qL 5 cGo 96
109 x]/rfO ug{] JolQmsf];Fu lzz'sf]] gftf
cfdf 1 A'faf 2 cGo 96
110 :jf:Yo ;+:yf b]lv tkfO{+sf] 3/sf] b'/L slt 5 <
ldg]6 306f
111 :jf:Yo ;]jf kfpgsf nflu cfh tkfO{n] slt a]/ s'g'{ k¥of] <
ldg]6

138
v08 !M;]jf pkof]u
k|Zg ;+Vof k|Zgx? k|ltls|of sf]8 s}lkmot 201 lzz'sf] pd]/ slt xf] < dlxgf lbg
202 tkfO{n] lzz'nfO{ sxfF hGd lbg' ePsf] lyof] <
lhNnf c:ktfn 1 lghL c:ktfn 2
PHCC 3
HP 4 olx+ :jf:Yo ;'ljwf 5 3/ 6 cGo 96
203 hGdsf] ;dodf tkfO{sf] lzz'sf] tf}n slt lyof] <
………………….. u|fd yfxf 5}g 8
204 s] tkfO{ cfˆgf] la/fdL aRrfnfO{ k|foM olx+ :jf:Yo ;+:yfdf Nofpg' x'G5 <
xf] 1 olb xf] eg] 106 df hfg'xf]nf .
xf]Og 2
205 olb xf]Og eg] tkfO{ cfˆgf] la/fdLaRrfnfO{{ sxfF n}hfg'x'G5 <
lghL SnLlgs 1 c:ktfn 2 k/Dk/fut lrlsT;f 3 cGo 96
206 aRrfdf s:tf] vfnsf] nIf0f÷ladf/L b]lvPsf] 5 <
Hj/f] 1 ;f; km]g{ ufx|f] 2 vfg g;Sg] 3 hl08; 4 emf8fkvfnf 5 cr]t 6 cGo 96
207 :jf:YosdLn] tkfO{sf] aRrfsf] lgDg hfFr u/]sf] lyof] < tf}n < tfks|d < 5ftLsf] hfFr <
lyof] lyPg tf}n tfks|d 5ftLsf] hfFr
1 2 1 2
1 2
1 2
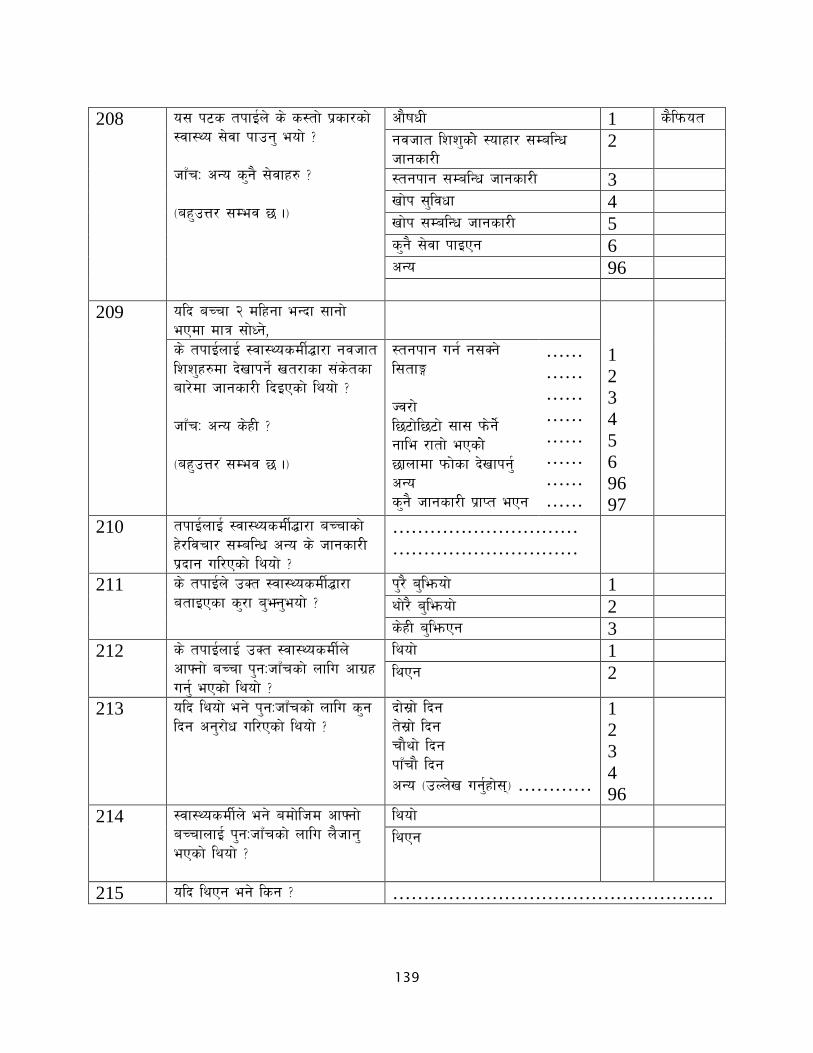
139
208 o; k6s tkfO{n] s] s:tf] k|sf/sf] :jf:Yo ;]jf kfpg' eof] < hfFrM cGo s'g} ;]jfx? < -ax'pQ/ ;Dej 5 ._
cf}ifwL 1 s}lkmot gjhft lzz'sf]] :ofxf/ ;DalGw hfgsf/L
2
:tgkfg ;DalGw hfgsf/L 3 vf]k ;'ljwf 4 vf]k ;DalGw hfgsf/L 5 s'g} ;]jf kfOPg 6 cGo 96
209
olb aRrf @ dlxgf eGbf ;fgf] ePdf dfq ;f]Wg],
1 2 3 4 5 6 96 97
s] tkfO{nfO{ :jf:YosdL{4f/f gjhft lzz'x?df b]vfkg]{ vt/fsf ;+s]tsf af/]df hfgsf/L lbOPsf] lyof] < hfFrM cGo s]xL < -ax'pQ/ ;Dej 5 ._
:tgkfg ug{ g;Sg] l;tfË Hj/f] l56f]l56f] ;f; km]g]{] gfle /ftf] ePsf]] 5fnfdf kmf]sf b]vfkg'{ cGo s'g} hfgsf/L k|fKt ePg
…… …… …… …… …… …… …… ……
210 tkfO{nfO{ :jf:YosdL{4f/f aRrfsf] x]/ljrf/ ;DalGw cGo s] hfgsf/L k|bfg ul/Psf] lyof] <
………………………… …………………………
211 s] tkfO{n] pSt :jf:YosdL{4f/f atfOPsf s'/f a'‰g'eof] <
k'/} a'l´of] 1 Yff]/} a'l´of] 2 s]xL a'l´Pg 3
212 s] tkfO{nfO{ pSt :jf:YosdL{n] cfˆgf] aRrf k'gMhfFrsf] nflu cfu|x ug'{ ePsf] lyof] <
lyof] 1 lyPg 2
213 olb lyof] eg] k'gMhfFrsf] nflu s'g lbg cg'/f]w ul/Psf] lyof] <
bf];|f] lbg t];|f] lbg rf}yf] lbg kfFrf} lbg cGo -pNn]v ug'{xf];\_ …………
1 2 3 4 96
214 :jf:YosdL{n] eg] adf]lhd cfˆgf] aRrfnfO{ k'gMhfFrsf] nflu n}hfg' ePsf] lyof] <
lyof] lyPg
215 olb lyPg eg] lsg < …………………………………………….

140
v08 @M:jf:Yo ;]jf ;'ljwf k|lt x]/rfx ug{] JolQmsf] ;Gt'li6
k|Zg ;+Vof k|Zgx? k|ltls|of ;Gt'i6 yfxf 5}g÷clglZrt c;Gt'i6
201 ;]jf kfpgsf nflu s'g'{ k/]sf] cj:yfk|lttkfO{ ;Gt'i6 x'g'x'G5 <
1 2 3
202 :jf:Yo ;+:yfsf] ;/;kmfOk|lt tkfO{ sltsf] ;Gt'i6 x'g'x'G5 <
1 2 3
203 hfFRg] sf]7fsf] uf]klgotfk|lt tkfO{ sltsf] ;Gt'i6 x'g'x'G5 <
1 2 3
204 :jf:Yo sdL{n] lbg] hfgsf/Laf6 tkfO{ sltsf] ;Gt'i6 x'g'x'G5 <
1 2 3
205 :jf:YosdL{sf]] Jojxf/af6 tkfO{ sltsf] ;Gt'i6 x'g'x'G5 <
1 2 3
206 :jf:Yo;+:yfaf6pknAw ;]jfaf6 tkfO{ sltsf] ;Gt'i6 x'g'x'G5 <
1 2 3

141
k'gMhfFr ;]jfu|fxL cGtjf{tf
dGh'/L
gd:t], d]/f] gfd ………………………………………………xf] . :jf:Yo dGqfno÷ljZj
:jf:Yo ;+u7g÷Save the Children÷g]=lj=c=k|=4f/f ;+o'St ?kdf ;+rflnt CB-IMNCI sfo{s|dsf]
cWoogdf d sfo{/t 5' . PHCC,HP / ;d'bfo:t/df aRrf / gjhftlzz'sf] Joj:yfkg nufot pkof]u /
u'0f:t/sf] :t/ /ARI, kvfnf, PSBI s]lGb«t ltgsf k|efljt sf/sx?sf] jt{dfg cj:yf lgwf{/0f ug'{ o;
cWoogsf] p2]Zo /x]sf] 5 .
xfdL la/fdL lzz'sf] /]vb]v / pgLx?sf] pkrf/df ;+nUg cfdf / lzz'sf] x]/rfx ug]{ JolQmsf] cGtjf{tf lng rfxG5f}+ .xfdL yk hfgsf/L klg lbg]5f}+ / cufl8 a9\g cf}krfl/s ;xdlt rfxG5f}+ .
tkfO{n] lbg' ePsf] hfgsf/L uf]Ko /flvg]5 / s]an kl/of]hgf ljZn]if0fsf nflu dfq k|of]u ul/g]5 . o; sfo{s|dsf nflu xfdLnfO{ ;xof]u ug'{x'g] JolSt tyf ;3+;+:yfk|lt:jf:Yo dGqfno÷ljZj :jf:Yo
;+u7g÷Save the Children÷g]=lj=c=k|= xflb{s s[t¡ftf k|s6 ub{5 . tkfO{sf] ;xeflutf
:j}lR5s(Voluntarily)x'g]5 / olb tkfO{n] efu lng grfx]df glng ;Sg' x'g]5 / o;n] s'g} c;/ ug]{ 5}g .
olb tkfO{ ;xdt x'g'x'G5 eg] s[kof ;lx ul/lbg'xf]nf .
s] d cGtjf{tf ;'? ug]{ cg'dlt kfpg ;S5' <
5 ……………………………………..
5}g ……………………………………..
pQ/bftfsf] x:tfIf/ ldlt
;d'bfodf cfwfl/t gjhft tyf afn/f]usf] Plss[[t Joj:yfkgsf] d'Nof+sg cWoog
@)&#÷&$
:jf:Yo dGqfno÷ljZj :jf:Yo ;+u7g÷Save the Children÷g]=lj=c=k|=
% jif{sf d'lgsf la/fdL lzz'sf cfdf÷ lzz'sf] x]/rfx ug]{ JolQm;Fusf] k|ZgfjnL

142
v08 !M k[i7e"ld
k|Zg ;+Vof k|Zgx? k|ltls|of sf]8 s}lkmot !)! lhNnf tfKn]h'ª !
l;Gw'kfNrf]s @ :ofª\hf # a}t8L $ ;Kt/L % gjnk/f;L ^
!)@ :jf:Yo ;+:yfsf] gfd !)# :jf:Yo ;+:yfsf] k|sf/ PHCC !
HP @ !)$ lzz'sf] pd]/ @ dlxgf eGbf sd !
@–%( dlxgf @ !)% /f]usf] k|sf/ PSBI !
emf8fkvfnf @ P=cf/=cfO=÷lgdf]lgof #
!)^ lzz'sf] x]/rfx ug]{ JolQmsf] gfd
!)& lzz'sf]] x]/rfx ug]{ JolQmsf] pd]/
jif{
!)* x]/rfx ug]{ JolQmsf] hfltotf
blnt ! hghflt @ dw];L # d'l:nd $ a|flXd0f÷If]qL % cGo (^
!)( x]/rfx ug]{ JolQm;Fu lzz'sf]] gftf
cfdf ! A'faf @ cGo (^
!!) :jf:Yo;+:yfb]lv tkfO{+sf] 3/sf] b'/L slt 5 <
ldg]6 306f
!!! :jf:Yo ;]jf kfpgsf nflu tkfO{n] slt a]/ s'g'{ k¥of] <
ldg]6

143
v08 @M;]jf k|fjwfg
k|Zg ;+Vof k|Zgx? k|ltls|of sf]8 s}lkmot @)! lzz'sf] pd]/ slt xf] < dlxgf lbg @)@ hGdsf] ;dodf tkfO{sf] aRrfsf]
tf}n slt lyof] < ………………….. u|fd yfxf 5}g *
@)# aRrfdf s] s:tf] :jf:Yo ;d:ofx? b]vf k/]/ :jf:Yo ;+:yfdf Nofpg' ePsf] xf] < -ax'pQ/ ;Dej 5 ._
Hj/f] ! ;f; km]g{ ufx|f] @ vfg g;Sg] # hl08; $ emf8fkvfnf % cr]t ^ cGo (^
@)$ tkfO{n] s] sf/0fn] oxL :jf:Yo ;+:yfdf cfˆgf] la/fdL aRrfnfO{ Nofpg' ePsf] xf] <
3/af6 glhs ! ;]jf;'ljwf ;DkGg @ u'0f:tl/o ;]jf;'ljwf # sd{rf/Lsf] /fd|f] Jojxf/ $ cGo (^
@)% s] :jf:YosdL{n] tkfO{sf] aRrfsf] lgDg hfFr u/]sf] lyof] <
lyof] lyPg ! @
tf}n < tf}n ! @ tfks|d < tfks|d ! @ 5ftLsf] hfFr < 5ftLsf] hfFr ! @
@)^ ;fdfGo hfFr afx]s tkfO{n] cGo s] s] hfgsf/L / ;]jfx? kfpg' ePsf] lyof] < hfFrM cGo s'g} ;]jfx? < -ax'pQ/ ;Dej 5 ._
cf}ifwL ! gjhft lzz'sf]] :ofxf/ ;DalGw hfgsf/L
@
:tgkfg ;DalGw hfgsf/L # vf]k ;'ljwf $ vf]k ;DalGw hfgsf/L % s'g} ;]jf kfOPg ^ cGo (^

144
@)& olb lzz @ dlxgf eGbf ;fgf] ePdf
dfq ;f]Wg],
s] tkfO{nfO{ :jf:YosdL{4f/f gjhft lzz'x?df b]vfkg]{ vt/fsf ;+s]tsf af/]df hfgsf/L lbOPsf] lyof] <
lyof] ! lyPg @
@)* olb lyof] eg] s:tf] hfgsf/L lbOPsf] lyof] < hfFrM cGo s]xL < -ax'pQ/ ;Dej 5 ._
:tgkfg ug{ g;Sg] l;tfª Hj/f] l56f]l56f] ;f; km]g]{] gfle /ftf] ePsf]] 5fnfdf lkk el/Psf] kmf]sf b]vfkg'{ cGo s'g} hfgsf/L k|fKt ePg
! @ # $ % ^ (^ (&
@)( s] tkfO{n] :jf:YosdL{4f/f atfOPsf s'/f a'‰g'eof] <
k'/} a'l´of] ! yf]/} a'l´of] @ a'l´Pg #
@!) s] tkfO{n] :jf:YosdL{sf] ;Nnfx adf]lhdsf] cf}ifwL cfˆgf] aRrfnfO{ lbg'eof] <
lbP ! lbOg @
@!! olb lbg' ePg eg] lsg < @!@ s] tkfO{n] :jf:YosdL{sf] ;Nnfx
adf]lhd cf}ifwLsf] 8f]h k'/f ug'{ eof] <
u/] ! ul/g @
@!# olb ug{' ePg eg] lsg < la;]{/ ! cf}ifwL vl/b ug{ g;s]/ @ aRrfsf] :jf:Yodf ;'wf/ cfP/ # 8f]hsf] dfqf k'¥ofpg' k5{ eGg] gnfu]/
$
cGo (^ @!$ s] tkfO{nfO{ :jf:YosdL{n] cfˆgf]
la/fdL aRrfsf] 3/df klg x]/rfx ug{ ;Nnfx lbg' ePsf] lyof] <
lyof] ! lyPg @
@!% s] tkfO{n]{ cfˆgf] la/fdL aRrfsf] x]/rfx :jf:YosdL{sf] ;Nnfx adf]lhd lbg'eof] <
lbP ! lbOg @
@!^ olb lbg' ePg eg] lsg < la;]{/ ! ;do lbg g;s]/ @ dxTjk'0f{ gnfu]/ #

145
c?n] gug'{ eg]/ $ cGo (^
@!& s] tkfO{nfO{ :jf:YosdL{n] cfˆgf] aRrf k'gMhfFrsf] nflu cfu|x ug'{ ePsf] lyof] <
lyof] ! lyPg @
@!* olb lyof] eg] s'g lbgsf] nflu cfpg eGg' ePsf] lyof] <
bf];|f] lbg t];|f] lbg rf}yf] lbg kfFrf} lbg cGo -pNn]v ug'{xf];\_ ………
! @ # $ (^
@!( s] tkfO{n] cg'/f]w u/] adf]lhd cfˆgf] aRrfnfO{ k'gMhfFrsf] nflu n}hfg' ePsf] lyof] <
lyof] ! lyPg @
@@) olb lyPg eg] lsg < la;]{/ ! 6f9f eP/ @ dxTjk'0f{ gnfu]/ # ga' ]́/ $ cGo -pNn]v ug'{xf];\_ ……… (^
@@! pkrf/kl5 s] tkfO{n] aRrfsf] :jf:Yodf ;'wf/ kfpg' eof] <
kfP ! kfOg @
@@@ olb kfpg' ePg eg] cGo s] s] pkfo ckgfpg' eof] < hfFrM cGo s]xL < -ax'pQ/ ;Dej 5 ._
7'nf] c:ktfndf uP 8fS6/;Fu ;Nnfx lnP lghL (Private) d]l8sndf uP wfdL÷´fls|sf]df uP 3/df g} pkrf/ u/] cGo -pNn]v ug'{xf];\_ ………
! @ # $ % (^

146
v08 #M:jf:Yo ;]jf ;'ljwf k|lt ;]jfu|fxLsf] ;Gt'li6
k|Zg ;+Vof k|Zgx? k|ltls|of #)! s] tkfOn]{ ;]jf kfpgsf] nflu s'g'{ k/]sf] cj:yfk|lt
;Gt'i6 x'g'x'G5 < ;Gt'i6 c;Gt'i6
yfxf 5}g÷clglZrt
! @ #
#)@ :jf:Yo s]Gb«sf] ;/;kmfOk|lt tkfO{ sltsf] ;Gt'i6 x'g'x'G5 <
;Gt'i6 c;Gt'i6
yfxf 5}g÷clglZrt
! @ #
#)# hfFRg] sf]7fsf] uf]klgotfk|lt tkfO{ sltsf] ;Gt'i6 x'g'x'G5 <
;Gt'i6 c;Gt'i6
yfxf 5}g÷clglZrt
! @ #
#)$ :jf:YosdLn]] lbPsf] ;do af/] tkfO{ sltsf] ;Gt'i6 x'g'x'G5 <
;Gt'i6 c;Gt'i6
yfxf 5}g÷clglZrt
! @ #
#)% :jf:YosdL{sf] Jojxf/k|lt tkfO{ sltsf] ;Gt'i6 x'g'x'G5 <
;Gt'i6 c;Gt'i6
yfxf 5}g÷clglZrt
! @ #
#)^ :jf:Yo ;+:yfn] lbPsf] ;]jfaf6 tkfO{ sltsf] ;Gt'i6 x'g'x'G5 <
;Gt'i6 c;Gt'i6
yfxf 5}g÷clglZrt
! @ #

147
dGh'/L
gd:t], d]/f] gfd ………………………………………………xf] . :jf:Yo dGqfno÷ljZj
:jf:Yo ;+u7g÷Save the Children÷g]=lj=c=k|=4f/f ;+o'St ?kdf ;+rflnt CB-IMNCI sfo{s|dsf]
cWoogdf d sfo{/t 5' . PHCC, HP / ;d'bfo:t/df aRrf / gjhftlzz'sf] Joj:yfkg nufot pkof]u /
u'0f:t/sf] :t/ / Zjf;g ;+s|d0f, kvfnf, PSBI s]lGb«t ltgsf k|efljt sf/sx?sf] jt{dfg cj:yf lgwf{/0f
ug'{ o; cWoogsf] p2]Zo /x]sf] 5 . . xfdL dlxnf ;fd'bflos :jf:Yo :j+o;]ljsf;Fu cGt{/jftf{ lng rfxG5f} hf] % jif{ d'gLsf
lj/fdL aRrfx?sf] pkrf/sf] lg0f{o lng ;xeflu x'g'x'G5 . xfdLn] w]/} ;"rgfx? k|bfg ug]{ 5f}, o; k|of]hgsf nflu s] tkfO{ cg'dlt lbg'x'G5 .
tkfO{4f/f k|bfg ul/Psf hjfkm uf]Ko /flvg]5 / s]an kl/of]hgf ljZn]if0fsf nflu k|of]u ul/g]5 . o; sfo{s|dsf nflu xfdLnfO{ ;xof]u ug'{x'g] JolSt tyf ;3+;+:yfk|lt :jf:Yo dGqfno xflb{s s[t¡ftf k|s6 ub{5 . tkfO{sf] ;xeflutf :j}lR5s 5 / olb tkfO{ efu lng grfx]df o:sf] s]lx kl/0ffd x'g] 5}g . tkfO{sf] a'´fO{ / ;xdltnfO{ hgfpg oxfF hgfOPsf] 5 .
s] d cGtjf{tf ;'? ug]{ cg'dlt kfpg ;S5' <
5 ……………………………………..
5}g ……………………………………..
pQ/bftfsf] x:tfIf/ ldlt
;d'bfodf cfwfl/t gjhft tyf afn/f]usf] Plss[[t Joj:yfkgsf] d'Nof+sg cWoog
@)&#÷&$
:jf:Yo dGqfno÷ljZj :jf:Yo ;+u7g÷Save the Children÷g]=lj=c=k|=
dlxnf ;fd'bflos :jf:Yo :j+o;]ljsf;Funflu k|Zgkq

148
Background Information ;"rgfsf] k[i6e"dL
Q.N. Questions k|Zgx? Response/Categories pQ/÷jlu{s/0f ;+s]t df hfg]
A01 DistrictlhNnf TaplejungtfKn]h'Ë Sindhupalchowk l;Gw'kfNrf]s Syangja:ofUhf Baitadij}t8L Saptari ;Kt/L Nawalparasi gjnk/f;L
! @ # $ % ^
A02 Name of the HF:jf:Yo ;]jfs]Gb|sf] gfd
A03 Type of the HF:jf:Yo ;]jfs]Gb|sf] k|sf/ PHCCk|fylds :jf:Yo ;]jf s]Gb| HP :jf:Yo ;]jf s]Gb|
! @
A04 Location of FCHV dlxnf ;fd'bflos :jf:Yo :j+o;]ljsf] lbzf
Near to the HF :jf:Yo ;]jf s]Gb|jf6 ghLs Far from HF:jf:Yo ;]jf s]Gb|jf6 6f9f
! @
A05 Name of the FCHV dlxnf ;fd'bflos :jf:Yo :j+o;]ljsf] gfd
A06 Age of FCHVdlxnf ;fd'bflos :jf:Yo :j+o;]ljsf pd]/ Years jif{
A07 Ethnicity of FCHV dlxnf ;fd'bflos :jf:Yo :j+o;]ljsf] hfltotf
Dalitblnt Janajati hghftL Madhesidw]zL Muslim d'lZnd Brahmin/chhetrijf|Dd0f÷If]qL Others …cGo………………….
! @ # $ % (^
A08
What is the distance from HF to your residence?tkfO{sf] 3/af6 :jf:Yo ;]jf;Dd k'Ug slt b'/L 5 <
ldg]6
A09 Type of training received lnPsf] tfnLdsf] k|sf/
Yes 5 No5}g
CB IMNCI;L= aL=cfO{=Pd=Pg= ;L= cfO{= CB NCP;L= aL= Pg= ;L=kL= CB IMCI;L= aL=cfO{=Pd= ;L= cfO{= Others cGo
! @ ! @ ! @ ! @
(^
A10
Telephone number6]nLkmf]g g+=
;]S;g 1: IMNCI ;Dalgw sfo{qmddf ;fdflhs dlxnf :jf:Yo :jo+;]ljsfsf] 1fg / cEof;
Q.N. k|Zgx? pQ/÷jlu{s/0f ;+s]t df hfg]
!)! gjhft lzz'sf] hGd eO{;s]kl5 cfdf / jRrfsf] e]6 slxn] jf s'g lbgdf eof] <
hGd]sf] lbgdf....................... hGd]sf] t];|f] lbgdf.............. hGd]sf] ;ftf} lbgdf................ hGd]sf] @( lbgdf............. yfxf 5}g………………………..
! @ # $ (*

149
!)@ tkfO{n] e|d0fsf] qmddf cfdfnfO{ s]
s:tf ;"rgf lbg' eof] < k|f]jM s]xL cGo jx'pQ/ ;Dej 5
;'Ts]/L gjhft lzz'df vt/f lrGx cfdf vt/f lrGx gfeL dnd -Snf]/ x]ShLl8g h]n_ :tgkfg kl/jf/ lgof]hg cGo
! @ # $ % ^ (^
!)# s] tkfO{ gjhft lzz' / cfdfnfO{ l/km/ ug'{x'G5 <
x'G5 x'Gg
! @
!)$ tkfO{ tkfO{sf] ;d'bfodf ePsf cfdf / gjhft lzz'nfO{ sxfF l/km/ ug'{x'G5 <
cfˆg} :jf:Yo ;]jf s]Gb| lghL d]l8sn k;n cGo………………………………..
! @ (^
!)% olb tkfO{n] tkfO{sf] :jf:Yo ;]jfdf l/km/ ug'{x'Gg eg] lsg <
……………………………………………………………………………………………………………………………………………………………………………..
!)^ gjhft lzz'nfO / @ dlxgf d'gLsf aRrfdff s:tf vfnsf lrGx b]vf k/]df tkfO{ l/km/ ug'{x'G5 <
sd vfPdf jf sd lkPdf Zjf; k|Zjf;df ;d:of ePdf sf]vf xfg]df cr]t÷;':t ePdf Hj/f] tfn' pS;g'-jNsLg'_ cGo
! @ # $ % ^ (^
!)& s] tkfO{ % jif{ d'gLsf aRrfx?nfO{ kvfnf ePdf pkrf/ ;]jf k|bfg ug'{x'G5 <
x'G5 x'Gg
! @
x'Gg cfPdf !!$ df hfg]
!)* tkfO{n] ljut # dlxgfdf kvfnfsf slt 36gfx?sf] pkrf/ ug'{eof] <- olb ;+Dej ePdf xflh/ skLjf6 /]s8{ x]g'{xf];_
cases36gf
!)( tkfO{n] k|bfg u/]sf pkrf/x? s] s] lyP <
hLjghn lhÍ hlt ;Dej 5 nuftf/ ?kdf :tgkfg u/fpg] k/fdz{ lbg] cGo……………………………………….
! @ # (^
!!) kvfnfsf] nflu tkfO{n] hLjghn ljt/0f ug'{ePg eg] lsg ljt/0f gug'{ePsf] <
hLjghnsf] e08f/0f gePsfn] :jf:Yo ;]jf glhs ePsfn] hLjghnsf] nflu jf:Yo ;]jfdf l/km/ u/]sf] :jf:Yo sfo{stf{n] glbg' eGg] cfb]z ePsfn] cGo-v'nfpg]xf];_…………
! @ # (^
!!! kvfnfsf] nflu tkfO{n] lhÍ ljt/0f ug'{ePg eg] lsg ljt/0f gug'{ePsf] <
lhÍ e08f/0f gePsfn] :jf:Yo ;]jf glhs ePsfn] lhÍ nflu :jf:Yo ;]jfdf l/km/ u/]sf] :jf:Yo sfo{stf{n] glbg' eGg] cfb]z ePsfn] cGo-v'nfpg]xf];_…………
! @ # (^
!!@ % jif{ d'gLsf jfnjflnsfnfO{ tkfO{n] P=cf/=cfO{=÷lgdf]gLofsf] pkrf/ ;]jf k|bfg ug'{ ePsf] 5 <
5 5}g
! @
5}g cfPdf !!^df hfg]
!!# tkfO{ P=cf/=cfO{=÷lgdf]gLofsf 36gfdf s'g cf}ifwL k|of]u ug'{x'G5 <
………………………………………………………………………………………………………………….

150
!!$ olb tkfO{n] P=cf/=cfO{=÷lgdf]gLofsf]
pkrf/ ug'{ePg eg], lsg tkfO{n] pkrf/ k|bfg ug'{ePg <
dlxnf ;fd'bflos :jf:Yo :jo+;]ljsfn] pkrf/ k|bfg ug{ c;xof]u u/]sfn] ………………………………………………………………………………………………………………….
!!% tkfO{sf] ;d'bfodf tkfO{n] ue{jtL cfdfx?nfO{ gfeL dnd -Snf]/ x]ShLl8g h]n_ k|bfg ug'{eof] <
5 5}g
! @
5}g cfPdf !!(df hfg]
!!^ ljut # dlxgfdf gfeL dnd -Snf]/ x]ShLl8g h]n_ slt cfdfx?nfO{ pknAw u/fpg' eof] <
!!& olb tkfO{n] gfeL dnd -Snf]/ x]ShLl8g h]n_ ue{jtL cfdfx?nfO{ ljt/0f ug'{ePg eg], lsg tkfO{n] ljt/0f ug'{ePg <
gfeL dnd -Snf]/ x]ShLl8g h]n_e08f/0f gePsfn] :jf:Yo ;]jf glhs ePsfn] gfeL dnd -Snf]/ x]ShLl8g h]n_ nflu jf:Yo ;]jfdf l/km/ u/]sf] :jf:Yo sfo{stf{n] glbg' eGg] cfb]z ePsfn] cGo-v'nfpg]xf];_…………
! @ # $ (^
!!* tkfO{n] cTofjZos a:t'x?sf] clxn] k|of{Kt e08f/0f ug'{ ePsf] 5 <
hLjghn lhÍ gfeL dnd -Snf]/ x]ShLl8g h]n_ Kof/f l;6fdf]n
! @ # $
!!( ljut dlxgfdf tkfO{n] cfdf ;d'xsf] j}7ssf] cfof]hgf ug'{eof] < - HMIS-4.2 sf] cjnf]sg_
5 5}g
! @
!@) olb 5}g eg], To;sf] sf/0f s] xf]nf < ………………………………………………………………………………………………………………………………………………
!@! dlxnf ;fd'bflos :jf:Yo :jo+;]ljsf] jf8{ ;lhi6/ cWofjlws lyof] < - HMIS-4.2 sf] cjnf]sg_
5 5}g
! @
!@@ :jf:Yo ;]jfdf(health post,PHCC) tkfO{ cfˆgf] l/kf]{6 a'emfpg' x'G5 <
5 5}g
! @
5}g cfPdf !@^df hfg]
!@# :jf:Yo ;]jfdf (health post,PHCC)tkfO{n] slxn] cfˆgf] l/kf]{6 a'emfpg' eof] <
dlxgfdf Ps rf]6L dlxgfdf b'O{ rf]6L
! @
!@$ olb 5}g eg], To;sf] sf/0f s] xf]nf < ………………………………………………………………………………………………………………………………………………………………
!@% cf= Pd= Pg= ;L= cfO{= (IMNCI)n]
lbO{Psf] e"ldsf k|lt tkfO{ ;Gt'i6 x'g'x'G5 <
!@^ olb 5}g eg] lsg <
----------------------

151
Annex 5. Glimpse of the survey:
Health facility observation
Follow up Visit Interview

152
FCHV Interview
HSP Interview

153
Observation of registers (HMIS 2.41, 2.42 and 9.1)