assessment of ampicillin in the of urinary tract …
TRANSCRIPT

55
Urinary Tract Infections
AN ASSESSMENT OF AMPICILLIN IN THETREATMENT OF URINARY TRACT INFECTION
W. BRUMFITT, D. A. LEIGH, A. PERCIVAL andJ. D. WILLIAMS.
Edgware General Hospital, Edgware, Middlesex.
THE outcome of a particular infection in theindividual patient will depend upon the bal-ance between the pathogenicity of the infectingorganism and the natural defence mechanismsof the host. However, these defence mechan-isms may be impaired by the presence of astructural or functional abnormality in thehost which may then favour persistence andpossibly progression of the infection. On theother hand a chemotherapeutic substance mayalso modify the host-parasite relationship andthe effectiveness of such a substance is deter-mined primarily by the sensitivity of theinfecting organism to the concentration of thechemotherapeutic agent which can be obtainedat the site of bacterial invasion in the tissuesor body fluids. The mode of action of thechemotherapeutic substance in terms ofbactericidal or bacteriostatic effect andwhether it acts upon bacteria in both theresting and the dividing phases is probably alsoof great importance. As a model for investigat-ing the factors concerned in response to chemo-therapy, infection of the urinary tract is insome ways the easiest of infections in thehuman body to study. Although urine, beinga waste' product, varies in composition itusually supports the growth of those bacter-ial pathogens liable to invade the urinarytract and which therefore readily multiply inbladder urine. This and the ease with whichsatisfactory urine specimens can be obtained,allows accurate quantitative bacteriologicalanalysis to be carried out in order to establishprecise criteria for the presence or absence ofinfection. Furthermore, the urinary tract is
accessible to both endoscopic and radiologicalstudies which can demonstrate the presence ofeven relatively minor underlying abnormali-ties.
In view of this situation it is surprising thatrelatively little advance has been made in thelast ten years in our knowledge of the funda-mental processes governing the response ofurinary tract infections to treatment. Follow-ing the discovery of the sulphonamides, earlyreports indicated that these compounds weresuccessful in approximately 80% of patientswith urinary tract infections, (Huber 1936,Kenny, Johnson and von Haebler, 1937).Although many antibiotics have since beenused, the results of treatment with these com-pounds have been little better. It was soonrecognised that the most important factordetermining the outcome of treatment was thepresence of an underlying structural or func-tional abnormality in the patient. A review byKass (1955) showed that the failure rate inprimary uncomplicated urinary tract infectionswas 10-20% almost regardless of the chemo-therapeutic agent used, but when infection wasassociated with an underlying abnormality,approaching 90%/0 of cases failed. Therefore,the main problem in the treatment of urinarytract infection is to devise more effectivemethods for treating the 10-20% who fail theinitial conventional course of treatment aswell as those who have an underlying abnor-mality. It is important to realise that althoughthe former group will contain a substantialnumber who may subsequently be shown tohave organic lesions, in many no underlying
Protected by copyright.
on Decem
ber 30, 2021 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.40.Suppl.55 on 1 D
ecember 1964. D
ownloaded from
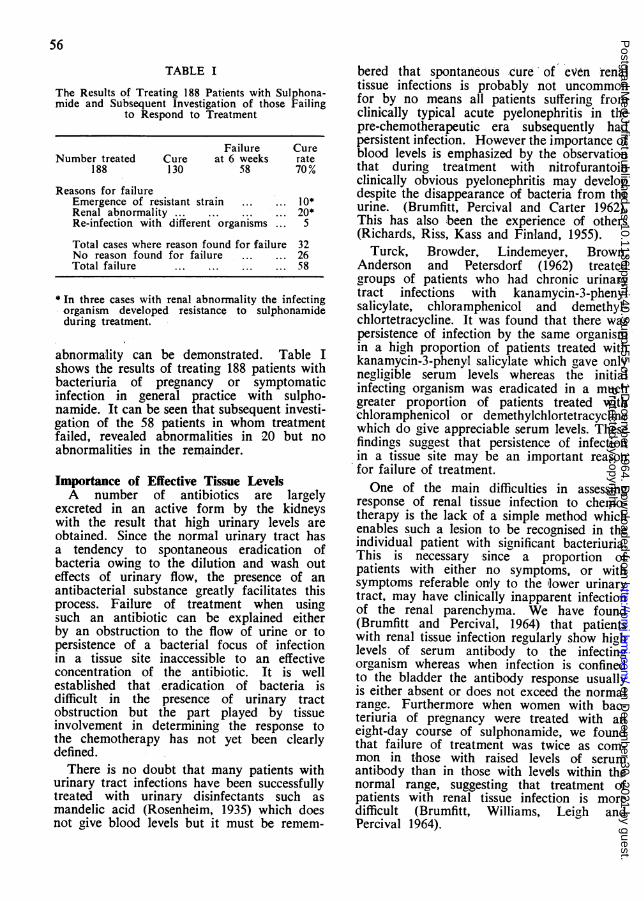
TABLE I
The Results of Treating 188 Patients with Sulphona-mide and Subsequent Investigation of those Failing
to Respond to Treatment
Failure CureNumber treated Cure at 6 weeks rate
188 130 58 70%
Reasons for failureEmergence of resistant strain ... ... 10*Renal abnormality ... ... ... ... 20*Re-infection with different organisms ... 5
Total cases where reason found for failure 32No reason found for failure ... ... 26Total failure ... ... ... ... 58
* In three cases with renal abnonnality the infectingorganism developed resistance to sulphonamideduring treatment.
abnormality can be demonstrated. Table Ishows the results of treating 188 patients withbacteriuria of pregnancy or symptomaticinfection in general practice with sulpho-namide. It can be seen that subsequent investi-gation of the 58 patients in whom treatmentfailed, revealed abnormalities in 20 but noabnormalities in the remainder.
Importance of Effective Tissue LevelsA number of antibiotics are largely
excreted in an active form by the kidneyswith the result that high urinary levels areobtained. Since the normal urinary tract hasa tendency to spontaneous eradication ofbacteria owing to the dilution and wash outeffects of urinary flow, the presence of anantibacterial substance greatly facilitates thisprocess. Failure of treatment when usingsuch an antibiotic can be explained eitherby an obstruction to the flow of urine or topersistence of a bacterial focus of infectionin a tissue site inaccessible to an effectiveconcentration of the antibiotic. It is wellestablished that eradication of bacteria isdifficult in the presence of urinary tractobstruction but the part played by tissueinvolvement in determining the response tothe chemotherapy has not yet been clearlydefined.
There is no doubt that many patients withurinary tract infections have been successfullytreated with urinary disinfectants such asmandelic acid (Rosenheim, 1935) which doesnot give blood levels but it must be remem-
bered that spontaneous cure- of even renaltissue infections is probably not uncommonfor by no means all patients suffering fromclinically typical acute pyelonephritis in thepre-chemotherapeutic era subsequently hadpersistent infection. However the importance ofblood levels is emphasized by the observationthat during treatment with nitrofurantoinclinically obvious pyelonephritis may developdespite the disappearance of bacteria from theurine. (Brumfitt, Percival and Carter 1962).This has also been the experience of others(Richards, Riss, Kass and Finland, 1955).
Turck, Browder, Lindemeyer, Brown,Anderson and Petersdorf (1962) treatedgroups of patients who had chronic urinarytract infections with kanamycin-3-phenylsalicylate, chloramphenicol and demethyl-chlortetracycline. It was found that there waspersistence of infection by the same organismin a high proportion of patients treated withkanamycin-3-phenyl salicylate which gave onlynegligible serum levels whereas the initialinfecting organism was eradicated in a muchgreater proportion of patients treated withchloramphenicol or demethylchlortetracyclinewhich do give appreciable serum levels. Thesefindings suggest that persistence of infectionin a tissue site may be an important reasonfor failure of treatment.One of the main difficulties in assessing
response of renal tissue infection to chemo-therapy is the lack of a simple method whichenables such a lesion to be recognised in theindividual patient with significant bacteriuria.This is necessary since a proportion ofpatients with either no symptoms, or withsymptoms referable only to the 'lower urinarytract, may have clinically inapparent infectionof the renal parenchyma. We have found(Brumfitt and Percival, 1964) that patientswith renal tissue infection regularly show highlevels of serum antibody to the infecting,organism whereas when infection is confinedto the bladder the antibody response usuallyis either absent or does not exceed the normalrange. Furthermore when women with bac-teriuria of pregnancy were treated with aneight-day course of sulphonamide, we foundthat failure of treatment was twice as com-mon in those with raised levels of serumantibody than in those with levdls within thenormal range, suggesting that treatment ofpatients with renal tissue infection is moredifficult (Brumfitt, Williams, Leigh andPercival 1964).
56P
rotected by copyright. on D
ecember 30, 2021 by guest.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.40.S
uppl.55 on 1 Decem
ber 1964. Dow
nloaded from

57
70
60
50
40
0 30o Range of M.I.Cs.m 20 for Esch. coli.
10
0 4 12 24Time/hrs.
FIG. 1.-Relationship of sulphamethoxydiazine blood levels to the M.I.Cs.for Esch. coli following a single oral dose of 1.0 gram.
3
2 Range of M.I.Cs.for Esch. coli.
0
0
0 1 2 3 4 5 6
Time/hrs.
FIG. 2.-Relationship of tetracycline blood levels to the M.I.Cs. for Esch.coli following a single oral dose of 500 mg.
Relation of Minimum Inhibitory Concentrationof Antibiotics to Attainable Blood LevelsFor successful treatment of a renal tissue
infection, the concentration in the tissue of thechemotherapeutic agent used should exceed the
minimum inhibitory concentration (M.I.C.) forthe infecting organism. Since very little isknown about tissue levels obtained duringtreatment with antibiotics, it is often assumedthat the serum levels are similar if not identi-
Protected by copyright.
on Decem
ber 30, 2021 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.40.Suppl.55 on 1 D
ecember 1964. D
ownloaded from

58
13
12 IM.
10 -------- ---------- .
9
8 Range of M.I.Cs.7 | for Esch. coli.0 6
5'0o 4
3
2
--- - - - - ---- ~Staph.aureus Au /ml.0 1 2 3 4 5 6
Time/hrs.FIG. 3.-Relationship of ampicillin blood levels to the M.I.Cs. for Esch.
coli following a single dose (oral and intramuscular) of 500 mg.
6
5
o 1 Range of M.I.Cs.- for Esch. coli.
0 2 3 4 5 6
Time/hrs.
FIG. 4.-Relationship of colistin methane sulphonate (polymyxin E) bloodlevels to the M.I.Cs. for Esch. coli following a single intramuscularinjection of II million units.
cal to the tissue levels. This assumption maynot always be valid especially in the renalmedullary tissues where diffusion from thetubules could theoretically lead to tissue levelshigher than those in the serum, since the con-centration of antibiotic in the renal tubules may
be several hundred times greater than that inthe serum. On the other hand, a substantialproportion of some antibiotics is bound toserum protein and may not be available fordiffusion into tissues. Therefore, the serumlevel may give a false indication of the con-
Protected by copyright.
on Decem
ber 30, 2021 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.40.Suppl.55 on 1 D
ecember 1964. D
ownloaded from

59
centration of antibiotic available for tissuepenetration. However, at the present time,since tissue levels can be measured only withdifficulty in experimental animals, and usuallynot at all in the patient, serum levels are thebest indication which we have of tissue levels ofantibiotic.The minimum inhibitory concentration of
some antibiotics for various strains of Esclh.coli in relation to the blood levels attainableon conventional therapeutic dosage are shownin-Figs. 1-4. Fig. 1 shows that with sulphame-thoxydiazine most Esch. coli strains isolatedfrom women with bacteriuria of pregnancyand patients with symptomatic infections ingeneral practice were inhibited by 40 yg. perml. and blood levels capable of inhibitinggrowth of the infecting organisms were com-monly obtained following standard dosage.Similar results are obtained for tetra-cycline (Fig. 2) but following a conventionaloral dose of ampicillin (500 mg.) a far greaterproportion of Esch. coli strains isolated frompatients with urinary tract infections fall out-side the therapeutic range as judged by com-parison of the M.I.C. and serum level (Fig. 3).It can be seen that much better levels can beobtained by the parental administration of asimilar dose of ampicillin (Fig. 3) or colistinmethane sulphonate (Fig. 4). The serum levelfollowing parenteral injection is also morepredictable as the variation in absorption whichoccurs following oral dosage is avoided.These findings which are relevant to the gene-
ral problem of treatment of systemic infectionsdue to Gram negative bacteria, suggest a rea-son for the difficulty in treating renal tissueinfections since with all the chemotherapeuticagents so far available the peak serum levelsbarely exceed the M.I.C. for many of theinfecting organisms and often levels above theM.I.C. are not obtained at all. The resultsexpressed in Figs. 1-4 apply to organismsfound to be sensitive by conventional paperdisc testing and therefore it should be remem-bered that a proportion of organisms havebeen excluded by this procedure. In contrast,treatment of systemic infections due to Grampositive organisms presents no such difficultiesbecause the M.I.C. of the effective antibioticsfor sensitive Gram positive organisms are somuch lower than with Gram negative bacteria(Fig. 3).
AmpicillinAmpicillin is active against many strains of
Esch. coli, Proteus mirabilis and Strept. fccalis
(Rolinson and Stevens, 1961) and like otherpenicillins, it has low toxicity and is bacteri-cidal. The development of resistant variantsduring treatment is very uncommon (Brum-fitt and others 1962, Trafford, McLaren,Lillicrapp and Barnes, Houston and Knox,1962) and activity in the urine is little affectedby pH variation (Brumfitt and Percival1962). In our view these properties suggestedthat ampicillin was a suitable agent for thetreatment of urinary tract infections due tosensitive organisms and in particular for thosein whom there is infection of the renal tissue.We therefore, decided to assess the value ofampicillin in treatment and have now used itin three different groups of patients.
TABLE II
The Results of Treatment of Urinary Tract Infectionsusing Ampicillin as the Initial Therapy
Failure CureOrganism Total Cure at 6 weeks rate
Esch. coli 30 25 5 83%Proteus mirabilis 1 1 8 3 73%Paracolon spp. 3 3 0Total for all 44 36 8 82%,'
organisms
Ampicillin in Initial Treatment of UrinaryTract InfectionThe results of treating 44 patients from
hospital and domiciliary practice with 500 mg.ampicillin eight hourly for five days areshown in Table II. All organisms were sensi-tive to 10 ug. ampicillin per ml. or less. Theoverall cure rate, as judged by clinical andbacteriological cure when examined six weeksafter the end of treatment, was 82% andsimilar results have been obtained by others(Trafford et al. 1962, Anderson, Kennedy,Plorde, Shulman and Petersdorf 1964). Noattempt was made to follow the eventualclinical progress of the patients who failed orto establish reasons for failure.
Ampicillin in the Treatment of UrinaryInfections which have Failed to Respond toSulphonamide
Because of the cheapness, low toxicity andsatisfactory serum and urinary levels obtainedwith sulphonamides and because a high pro-portion of the infecting organisms in patientsfrom general practice or in women with bac-teriuria of pregnancy are sensitive we use theshort acting sulphonamide sulphadimidine orthe long acting compound sulphamethoxydia-zine initially in these patients (Brumfitt et cal.
Protected by copyright.
on Decem
ber 30, 2021 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.40.Suppl.55 on 1 D
ecember 1964. D
ownloaded from

60
TABLE IIIResults of Treatment using either Ampicillin or Tetracycline in Cases of Urinary Tract
Infection which Failed to Respond to Sulphonamide
AMPICILLIN TETRACYCLINEFailures Cure Failures Cure
Organism No. at 6/52 rate No. at 6/52 rateEsch. coli 26 11 58%, 11 7 36%Proteus mirabilis 2 1 0Paracolon spp. 2 0 - 1 0Aerobacter aerogenes - - 2 0Total for all organisms 30 12 60% 14 7 50%Renal abnormalities 7 (58%) 2 (30%)on follow up
1964). However, if these patients fail torespond a second course of sulphonamideis usually unsuccessful even though theorganism remains sensitive. In a series of 10patients with sensitive organisms who failed torespond to sulphonamide only two (20%) werecleared of infection by a second course ofsulphonamide and we have discontinued thisregime of treatment.
If sulphonamide failures were treated withampicillin (500 mg. eight hourly for sevendays) the cure rate was 60% which thoughlower than the 82% when ampicillin wasused initially was nevertheless substantial. Ifblood and urine levels of oral ampicillin andsulphonamide are compared and these resultsrelated to the M.I.C. of the organisms treated(Figs. 1 and 3) the reason for success ofampicillin and failure of sulphonamide is notimmediately clear since blood levels in relationto M.I.C. are more satisfactory with sulphona-mide. The possibility that the better resultswith ampicillin may have been a reflection ofthe greater effectiveness of a bactericidalrather than a bacteriostatic antibiotic is notsupported by the finding that treatmentof sulphonamide failures with tetracycline gaveresults apparently almost as good as ampicillin(Table III). However, investigation of thepatients in whom infection by the sameorganism persisted despite treatment withsulphonamide and then either ampicillin ortetracycline showed the presence of underlyingabnormalities in seven out of 12 failuresin the ampicililin group and two out ofseven in the tetracycline group (Table III). Theabnormalities found included renal calculi andcongenital lesions such as calyceal cyst anddouble ureter and pelvis.Parenteral AmpicillinWhere it was felt necessary to obtain blood
levels in excess of the M.I.C. of the infectingorganisms, we have treated a number of hospi-
tal patients with ampicillin given by intramus-cular injection (500 mg. six hourly for fivedays).
Patients were divided into three groupsaccording to the presenting features and thegroups and results of treatment are shown inTable IV. In eight patients with clinical featuresof acute pyelonephritis a rapid response wasobtained and all patients showed clinical andbacteriological cure at follow-up examinationsix weeks after the end of treatment. On theother hand, only seven of the 14 patients withpersistent infection by the same organismassociated with an underlying renal abnorma-lity were successfully treated and five of thesesuccesses had become infected by a differentorganism during the six week follow-up period.The results were somewhat better where per-sistent infection was not associated with ademonstrable abnormality, six of nine patientsbeing cured but in two of these infection by adifferent organism had occurred whenexamined six weeks after the end of treatment.ConclusionsInitial Treatment of Urinary Tract Infection
If the high incidence of chronic renal diseaseresulting from urinary tract infection is to bereduced effective treatment of the primaryattack is required and because of the unrelia-bility of symptoms as a guide to the presenceof infection (Mond, Percival, Williams andBrumfitt 1964) a specimen of urine should .betaken before starting empirical treatment andtherapy immediatdly adjusted where the organ-ism is found to be resistant. Patients knownto be susceptible to urinary tract infection,e.g. pregnant women, diabetics, should havethe urine screened for bacteriuria. Since mostpatients remain ambulant and a number areat work some form of oral therapy is desirablein the first instance.As the majority of strains of Esch. coli and
Proteus mirabilis which cause spontaneous
Protected by copyright.
on Decem
ber 30, 2021 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.40.Suppl.55 on 1 D
ecember 1964. D
ownloaded from

61
TABLE IVThe Results of Using Intramuscular Ampicillin in 3 Groups of Patients
Number Immediate Result Follow-upstudied Success Failure Success Failure
Group I Acute pyelonephritis 8 8 0 8 0needing urgent treatment.
Group II Persistent infection with 14 9 5 7* 7abnormality
Group III Persistent infection no 9 7 2 6 3renal abnonnality
*Two patients in group 3 and five in group 2 have become re-infected with a different organisminfection in domiciliary practice are sensitiveto sulphonamide (Mond et al., 1964) weusually recommend this therapy in the firstinstance and the patient is seen three dayslater when the results of culture and sensi-tivity tests are available. If the organism issensitive to sulphonamide this treatment iscontinued for a further 5-10 days and theurine re-examined four days after the end oftreatment and again six weeks later if clearof infection. Patients with a history of sulpho-namide sensitivity are given ampicillin 500mg. t.d.s., for seven days as primary treat-ment.The Treatment of Sulphonamide FailuresSulphonamides are successful in eradication
of primary infections due to sensitive organ-isms in about 75% of patients. Of those whofail, most are due to the persistence of sulpho-namide sensitive strains within the renal tractalthough development of resistant mutantsduring treatment occurs in some cases. Fortreatment of these failures we use oral ampi-cillin which is bactericidal, there is littletendency to development of resistance and itis little affected by pH variation of the urine.With regard to the blood level found afteroral administration, there is evidence that thisfrequently does not exceed the M.I.C. ofinfecting Esch. coli strains (Brumfitt etal., 1962; Neumann, 1962). However, theextent of diffusion of antibiotics in the renaltissues is at present unknown but the satisfac-tory clinical results with ampicillin usingdosages which give blood levels which barelyreach the M.I.C. of the infecting organismsuggests that concentration of the antibioticmay occur in the renal tissues as well as inthe urine (Brumfitt, Percival and Williams1964).In summary we use oral ampicillin for treat-
ing urinary tract infections due to sensitiveorganisms in the following circumstances:
1. As initial treatment for patients who
have a history of hypersensitivity tosulphonamide or when the infectingorganism is resistant to sulphonamide.
2. In patients who have typical clinicalfeatures of pyelonephritis (indicatingextensive renal involvement).
3. Where treatment with sulphonamide hasfailed.
It must be emphasized that the duration oftherapy should not depend upon the relief ofsymptoms and a minimum of seven daystherapy should be given no matter how quicklysymptoms subside. Over half the patients inour series who failed to respond to sulphona-mide and ampicillin were found to haveorganic abnormalities which in many caseswere amenable to surgical treatment. There-fore failure to respond to both sulphonamideand ampicillin is a clear indication for furtherinvestigation by the radiologist and genito-urinary surgeon.
Parenteral AmpicillinThe persistence of infection without organic
abnormality means that the renal lesion ismore inaccessible and parenteral therapyaimed at producing higher blood levels isindicated. The substances available forthis purpose are colistin methane sulphonate,streptomycin and kanamycin and parenteralampicillin. Which of these antibiotics is mosteffective in treating severe and persistentrenal infections remains to be elucidated.
Injections of 500 mg. ampicillin are re-quired at intervals of six hours or less tomaintain adequate blood levels and thereforetreatment is best given in hospital. We consi-der the indications for parenteral therapy to beas follows:-
(a) For patients who have been given anadequate trial of oral therapy, butinfection by the same organism persistsin the absence of a demonstrable renallesion.
Protected by copyright.
on Decem
ber 30, 2021 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.40.Suppl.55 on 1 D
ecember 1964. D
ownloaded from

62
(b) For patients with pronounced clinicalfeatures of acute pyelonephritis whererapid control to limit renal damage isdesirable.
(c) For patients known to have extensiverenal damage where there is a dangerof infection precipitating renal failureas well as extending the renal lesion.
(d) Post-operative patients where oraltherapy is impracticable or whereabsorption is in doubt.
Finally, we do not wish to claim thatampicillin is superior to all other drugs inthe treatment of urinary tract infection. Morecomparative trials are needed before thesuperiority of one antibiotic over another canbe established.
REFERENCESANDERSON, K. N., KENNEDY, R. P., PLORDE, J. J.,
SHULMAN, J. A., and PETERSDORF, R. G. (1964):J. Amer. med. Ass., 187, 555.
BRUMFITr, W., and PERCIVAL, A. (1962): Lancet, i,186
BRUMFITT, W., PERCIVAL, A., and CARTER, M. J.(1962): Lanicet, i, 130.
BRUMFIrr, W., and PERCIVAL, A. (1964): 2nd Inter-national Pyelonephritis Symposium. To bepublished.
BRUMFITr, W., WILLIAMS, J. D., LEIGH, D. A.. andPERCIVAL, A. (1964): 2nd International Pyelone-phritis Symposium. To be published.
BRUMFITr, W. PERCIVAL, A., and WILLIAMS, J. D.(1964): Brit. J. clin. Pract., 18, 503.
HUBER, H. G. (1936): Muncheni. med. Wochenschr.,83, 2014.
KASS, E. H. (1955): Amer. J. Med., 18, 764.KENNY, M., JOHNSON, F. D., and VON HAEBLER, T.
(1937): Lancet, ii, 119.MoND, N. C., PERCIVAL, A., WILLIAMS, J. D., and
BRUMFITr, W. (1964): In the press.RICHAODS, W. A., RIss, E., KASS, E. H., and FINLAND,
M. (1955): Arch. intern. Med., 96, 437.ROLINSON, G. N., and STEVENS, S. (1961): Brit.
med. J., , 191.ROSENHEIM, M. L. (1935): Lancet, L, 1032.TRAFFORD, J. A. P., MCLAREN, D. M., LILLICRAP,
D. A., BARNES, R. D. S., HOUSTON, J. C., andKNOX, R. (1962): Lancet, i, 987.
TURCK, M., BROWDER, A. A., LINDERMEYER, R. I..BROWN, N. K., ANDERSON, K. N., and PETERS-DORF, R. G. (1962): New Engl. J. med., 267, 999.
TREATMENT OF URINARY TRACT INFECTIONSWITH AMPICILLIN
PETER NAUMANNFrom the Inslitute of Clinical Bacter-iology and
Serology of the University of Hamburg.(Director: Professor G. B. Roemer).
THE therapeutic evaluation of a new anti-biotic should not be carried out solelyaccording to clinical criteria. The course ofa bacterial infection depends on too manyindividual factors and imponderables. Thetherapeutic value of an antibiotic cannot,therefore always be assessed objectively bycomparing clinically cured or improved caseswith those who failed to respond. After all,a not inconsiderable number of infections iscured without any or with only inadequatetherapy and may then be quoted as evidencein favour of a preparation which actually is in-effective. On the other hand, failure to respondmay be wrongly ascribed to an "ineffective" anti-biotic, even though the bacterial process hasbeen controlled, or is capable of being con-trolled, provided the drug is given inadequately high doses. "Clinical cure" is acomplex event which depends on the defen-
sive potential of the body as a whole, and itis not always easy to make a true assess-ment of the part played by the antibiotic---both in the cured case and in that which failsto respond. This applies particularly toinfections of the urinary tract, for even aftersuccessful eradication of one organisnm re-ihfection by an unrelated bacterial strainfrequently results in apparent failure of therapy.For this reason assessment of a drug such asampicillin should not be based on the number of"clinical cures", but primarily on the con-sideration whether the bacteriological effecthas been attained which should. be expectedfrom this antibiotic.
Present SeriesUsing the bacteriological examination of
the urine to diagnose the presence of infec-tion, an attempt has been made during 1963
Protected by copyright.
on Decem
ber 30, 2021 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.40.Suppl.55 on 1 D
ecember 1964. D
ownloaded from